 Elin Kindstedt1,2*
Elin Kindstedt1,2* Charlotte de Vries3
Charlotte de Vries3 Magnus Wänman1
Magnus Wänman1 Barbara Aleksandra Potempa4Jan Potempa4,5Susanne Lindquist6
Barbara Aleksandra Potempa4Jan Potempa4,5Susanne Lindquist6 Anders Esberg7
Anders Esberg7 Karin Lundberg3
Karin Lundberg3 Pernilla Lundberg1
Pernilla Lundberg1- 1Department of Odontology, Section for Molecular Periodontology, Umeå University, Umeå, Sweden
- 2Wallenberg Centre for Molecular Medicine, Umeå University, Umeå, Sweden
- 3Division of Rheumatology, Department of Medicine Solna, Karolinska Institutet and Center for Molecular Medicine, Karolinska University Hospital, Stockholm, Sweden
- 4Department of Oral Immunology & Infectious Diseases, University of Louisville School of Dentistry, Louisville, KY, United States
- 5Department of Microbiology, Faculty of Biochemistry, Biophysics and Biotechnology, Jagiellonian University, Krakow, Poland
- 6LipumAB, Umeå, Sweden
- 7Department of Odontology, Umeå University, Umeå, Sweden
Introduction: Periodontitis is associated with rheumatoid arthritis (RA). One hypothesis posits that this connection arises from the formation of autoantibodies against citrullinated proteins (ACPA) in inflamed gums, possibly triggered by Porphyromonas gingivalis. We previously demonstrated an increased antibody response to P. gingivalis arginine gingipains (anti-Rgp IgG), not only in individuals with severe periodontitis compared to controls, but in RA versus controls, with an association to ACPA. In the present study, we set out to further explore the relationship between anti-Rgp IgG, ACPA and periodontitis, including clinical periodontal parameters, in the large and well-characterized PerioGene North case-control study.
Methods: We measured serum levels of anti-Rgp and ACPA IgG by enzyme-linked immunosorbent assay (ELISA), in 478 patients with periodontitis and 509 periodontally healthy controls within PerioGene North. Subsequently, anti-Rgp IgG levels and ACPA status were analysed in relation to periodontitis and clinical periodontal parameters.
Results: Serum anti-Rgp IgG levels were elevated in cases versus controls (p< 0.001). However, receiver operating characteristic (ROC) curve analysis revealed that anti-Rgp IgG could not efficiently discriminate cases from controls (AUC= 0.63; 95% CI: 0.60 – 0.66). Among cases, increased anti-Rgp IgG levels associated with high periodontal inflammation and advanced alveolar bone loss (p<0.001 for both). An ACPA response was detected in 15 (3.1%) cases and 6 (1.2%) controls (p=0.033), but no association to periodontitis was evident after adjustment for age and smoking and anti-Rgp IgG levels did not differ between ACPA-positive and ACPA-negative individuals.
Conclusion: We show that anti-Rgp IgG identifies a subgroup of periodontitis patients with high degree of periodontal inflammation and advanced alveolar bone loss, but we do not find support for a link between periodontitis or anti-Rgp IgG and ACPA status in PerioGene North. Given the association between anti-Rgp and alveolar bone loss, the mechanistic role of gingipains in bone resorption should be experimentally explored.
1 Introduction
Periodontitis is an oral condition that is characterized by progressive destruction of the tooth supporting tissues, including both collagenous connective tissue of the gingiva and the tooth anchoring jawbone (1). In periodontally healthy states, indigenous polymicrobial communities at mucosal surfaces maintain an ecological balance via inter-microbial and host-microbial interactions. However, genetic and acquired factors, most notably smoking, but also obesity, immune deficiencies, immunoregulatory defects, diabetes mellitus and other systemic diseases may disrupt this homeostatic balance, leading to selective growth of species with the potential for destructive inflammation. This condition, known as dysbiosis, underlies the development of periodontitis in susceptible hosts. The pathogenic process is not linear, but involves a positive-feedback loop between a dysbiotic microbiota on the tooth surface below the gum line and the host inflammatory response (2). The molecular pathways underpinning tissue destruction have not been clarified, and there are currently no biomarkers available to help clinicians predict onset of periodontitis or identify individuals at risk of a more aggressive disease course.
Besides the local and detrimental effects on the periodontium that jeopardize tooth retention, the disease is strongly connected to a number of other non-communicable diseases, including rheumatoid arthritis (RA) (3). Different models for a causal and reciprocal relationship between periodontitis and RA have been described (4). In support of a causal link between periodontitis and RA, results from experimental studies show that periodontitis can exacerbate arthritis (5). Our findings of increased alveolar bone loss in individuals with high levels of anti-citrullinated protein antibodies (ACPA), before RA onset, imply that periodontitis predates the onset of ACPA-positive RA (6). However, it remains elusive whether there is a causative link.
The gram-negative anaerobic oral bacterium Porphyromonas gingivalis (P. gingivalis) is frequently detected in subgingival plaque of periodontitis patients (7). P. gingivalis expresses multiple virulence factors for its growth, survival, and immune evasion (8), including the arginine gingipains (Rgp), potent extracellular cysteine proteases which efficiently degrade host proteins by cleaving polypeptides C-terminal of arginine (9, 10). Protein degradation by gingipains can facilitate further enzymatic processing by Porphyromonas peptidylarginine deaminase, resulting in citrullinated neoepitopes (11). Gingipains have also been described to contribute directly to the inflammatory response by cleavage of protease activated receptor-2 on the neutrophil surface, triggering formation of neutrophil extracellular traps with the release of endogenously citrullinated proteins (12). Notably, citrulline-reactive B cells have been successfully isolated from gingival tissue of periodontitis patients, suggesting that break of tolerance and ACPA production in RA may take place in inflamed gums (13). Moreover, gingipains are highly immunogenic (14), and we have previously shown an increased anti-Rgp antibody response, not only in individuals with periodontitis compared to controls, but also in RA, especially ACPA-positive RA, compared to controls even before RA onset (15, 16). We have previously demonstrated associations between anti-Rgp IgG and alveolar bone loss, as well as presence of ACPA in PAROKRANK, a case-control study including patients hospitalized for a first myocardial infarction. Interestingly, we also found a particularly strong association between anti-Rgp IgG and severe periodontitis in a subfraction of PerioGene North study (17). Therefore, P. gingivalis antibodies, more specifically gingipain antibodies, are gaining increased attention as a potential biomarker for individuals with periodontitis and concomitant risk for systemic autoimmunity (13, 16–18).
In summary, accumulating evidence suggests that periodontitis is linked to RA-specific autoimmunity through a loop in which P. gingivalis promotes ACPA formation. In the present study, we address this link by analysing the association between periodontal clinical parameters, anti-Rgp IgG and ACPA in 987 individuals within the large and well-characterized PerioGene North case-control study (19).
2 Material and methods
2.1 Study design
PerioGene North is a multicentre case-control study consisting of 526 periodontitis cases and 532 periodontally healthy controls. Study participants were consecutively recruited between 2007 and 2019, from specialist clinics and general dental care within the counties of Västerbotten, Gävleborg, Uppsala and Västmanland in northern Sweden. Cases were examined by senior consultants in periodontology and controls were examined by general dentists. To validate the absence of alveolar bone loss in controls, all radiographs were reviewed by senior consultants in periodontology.
2.2 Clinical data collection
All participants underwent a complete oral and periodontal examination, including registration of periodontal inflammation, measured as bleeding on probing (BoP), and periodontal probing pocket depth (PPD), at six sites per tooth using a PCP-12, 3-6-9-12 (Hu-Friedy) dental probe. Furcation involvement was assessed but not registered in the study protocol. Alveolar bone loss was assessed for each tooth using dental radiographs (bitewing and apical images). Information regarding number of teeth per quadrant with PPD (< 4 mm, 4-6 mm and > 6 mm) and degree of alveolar bone loss (< 1/3, ≥ 1/3 to ≤ 2/3 or > 2/3 of the root length) was registered in the study protocol. Data collection was conducted before the present classification for periodontitis was introduced (20). By using a proposed framework for applying the 2018 periodontal status classification on completed epidemiological studies, we concluded that all cases fulfilled the stage III criteria and 87 cases (18.2%) with <20 teeth could be classified as stage IV (21). This means that all cases presented with severe periodontitis. Cases were further subcategorized based on level of BoP (high ≥20%, low <20%), PPD and alveolar bone loss according to previous studies (22).
Degree of periodontal inflammation: A low degree of periodontal inflammation was defined as having BoP < 20%. High degree of periodontal inflammation was defined as having BoP ≥ 20%.
Level of periodontal pocket depth and alveolar bone loss: Each tooth was given a score of 1-3 depending on the PPD/alveolar bone loss value. A PPD < 4 mm or alveolar bone loss < 1/3 of the root length was given the score 1. A PPD between 4 and 6 mm or alveolar bone loss between ≥ 1/3 to ≤ 2/3 of the root length was given the score 2. A PPD > 6 mm or alveolar bone loss > 2/3 of the root length was given the score 3. The total score for the entire dentition was summed up and then divided by the number of teeth. In the present study, a score between 1.01 - 1.49 was referred to as a low degree of periodontal probing depth or alveolar bone loss, 1.50 – 1.99 as moderate, and over 2.0 as a high level.
Information about sex, birth country, past and/or current tobacco use, education level and awareness of parent with periodontitis (self-reported heredity) was recorded. Information about height and weight was obtained for calculation of body mass index (BMI). Information about general health (diseases according to ICD-10 categories) was obtained from registries of the National Board of Health and Welfare in Sweden.
2.3 Inclusion and exclusion criteria
Inclusion criteria for cases were i) having at least one tooth in each quadrant with alveolar bone loss ≥ 1/3 of the root length and ii) having ≥15 remaining teeth, or ≥8 if teeth were only present in one jaw. Cases with alveolar bone loss that could be explained by local aggravating factors such as root fractures or pulpal infections were excluded. The cases were included after being refered to specialist clinics from generel dental care and had received previous periodontal treatment to various extent. Inclusion criteria for controls were i) no alveolar bone loss, i.e. <3 mm distance from the cementoenamel junction to the bone crest, ii) PPD <4 mm, iii) having ≥24 remaining teeth and iv) being ≥ 34 years of age. Participants with known contagious blood diseases were excluded.
2.4 Blood sampling
A venous blood sample of 3 x 10 mL was collected from all participants at inclusion. The participants were not fasted at the time of sampling. Collection and handling of blood samples, including fractionation into plasma, serum, and buffy coat, and storage at -80°C followed the standardized routines at the Medical Biobank of Northern Sweden, Västerbotten County Council, Sweden.
2.5 Antibody measurements
Anti-Rgp IgG in serum were measured using a previously described in-house enzyme-linked immunosorbent assay (ELISA) (15, 17), with purified, recombinant hexahistidine-tagged RgpB protein as coating agent (23). To compare serum samples analysed on different ELISA plates, anti-Rgp IgG levels were presented as arbitrary units (AU) with interquartile ranges (IQR) calculated from a standard curve (a pool of anti-Rgp IgG positive sera in 1:1 x7 serial dilution) included on all plates. Serum samples were analysed in duplicates and blank wells were included on all plates to account for background signal.
Presence ACPA was measured as anti-cyclic citrullinated peptide2 (CCP2) IgG, using the Immunoscan CCPlus® test kit (Svar Life Science, Malmö, Sweden), according to manufacturer’s instructions. Serum samples were analysed in single wells, with positive samples (≥25U/mL) re-analysed in duplicates.
2.6 Statistical methods
Descriptive analyses were used for frequency distributions of categorical variables, whereas median values with interquartile range were calculated for continuous variables. Group comparisons were conducted utilizing chi-square tests (categorical variables) or the non-parametric Mann-Whitney U test or Kruskal-Wallis test (continuous variables). Log-transformed anti-Rgp IgG levels were analyzed in relation to periodontitis, periodontal inflammation, periodontal pocket probing depth and alveolar bone loss, using a linear regression model, adjusted for age, age2, sex and smoking. Results are presented as Exp(B) = exponential B (interpretable as multiplicative effect), with 95% confidence interval (CI) and p-value. Adjustment for multiple testing was performed with Tukey’s method. P-values <0.05 were considered statistically significant. Receiver operating characteristic curves (ROC) was used to evaluate the discriminatory performance of anti-Rgp IgG to distinguish cases from controls and to determine the area under the curve (AUC). Youden’s J statistic was used to determine the cutoff with highest sensitivity and specificity.
Statistical Package for Social Sciences (SPSS), version 26 (IBM Corporation, Armonk, NY, USA), and R, version 4.2.3 (R foundation for statistical computing, Vienna, Austria), with packages: tidyverse, magrittr, haven, psych, cutpointr, pRoc, emmeans, gtsummary, and brglm2, were used for the analyses.
3 Results
3.1 Study population characteristics
Among 1,058 enrolled study participants, 60 were excluded in the present study due to missing clinical data or missing serum, and eleven were excluded due to not fulfilling the inclusion criteria, resulting in 478 study participants with periodontitis (referred to as cases) and 509 periodontally healthy (referred to as controls). The distribution of men and women was similar between cases and controls, but cases were older and had a higher proportion of smokers. Two controls and three cases were diagnosed with rheumatoid arthritis (Table 1). A comprehensive description of the study population characteristics has been published previously (19).
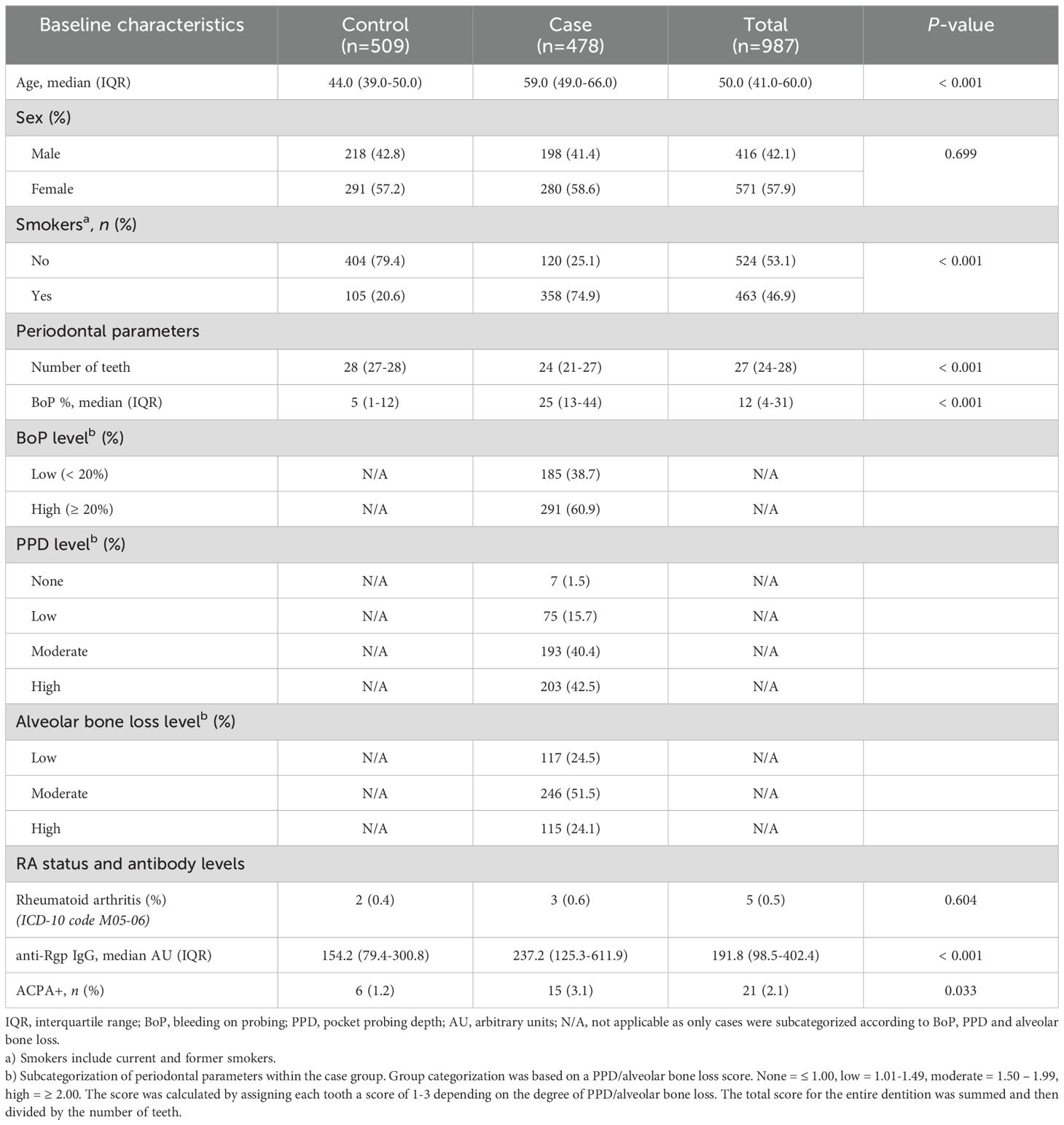
Table 1. Study participant characteristics in PerioGene North.
3.2 High anti-Rgp IgG levels are associated with periodontitis, but show poor potential to discriminate between cases and controls
An antibody response towards P.gingivalis Rgp was evident in both periodontitis cases and controls, with higher median anti-Rgp IgG values for cases (237.2 AU; IQR= 125.3-611.9) than controls (154.2 AU; IQR= 79.4-300.8), p<0.001 (Table 1 and Figure 1A). The average increase of anti-Rgp IgG levels in cases versus controls was 71% (p<0.001) when adjusted for age, age2, sex and smoking (Table 2). A ROC curve analysis showed that anti-Rgp IgG levels could separate cases from controls with a sensitivity of 37.5% and specificity of 83.1% (AUC=0.63; 95% CI: 0.60 – 0.66), demonstrating a weak discriminatory ability (Figure 1B).
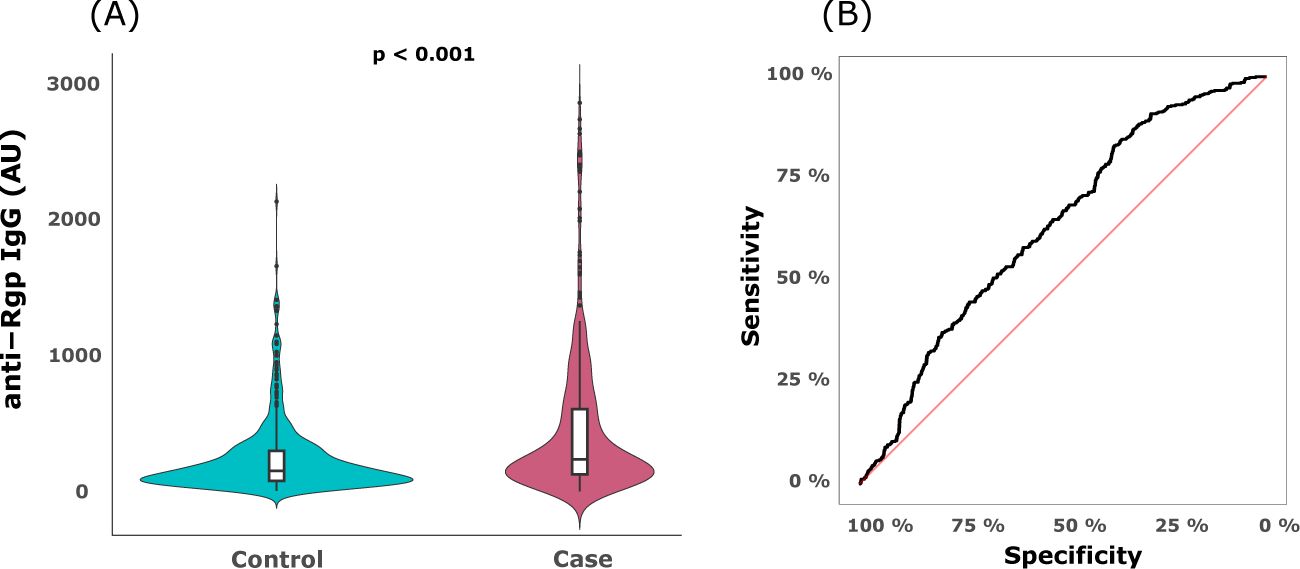
Figure 1. Serum anti-Rgp IgG levels are elevated in periodontitis, but do not discriminate cases from controls. (A) The violin plot shows distribution of serum anti-Rgp IgG levels in PerioGene North cases (n=478) and controls (n=509). Integrated box plots show median AU values and 25th and 75th percentiles as horizontal lines; whiskers indicate the 10th to 90th percentile; outliers plotted as dots. (B) Receiver operating characteristic (ROC) curve for prediction of cases and controls based on serum levels of anti-Rgp IgG. Rgp = arginine gingipain; AU = arbitrary units.
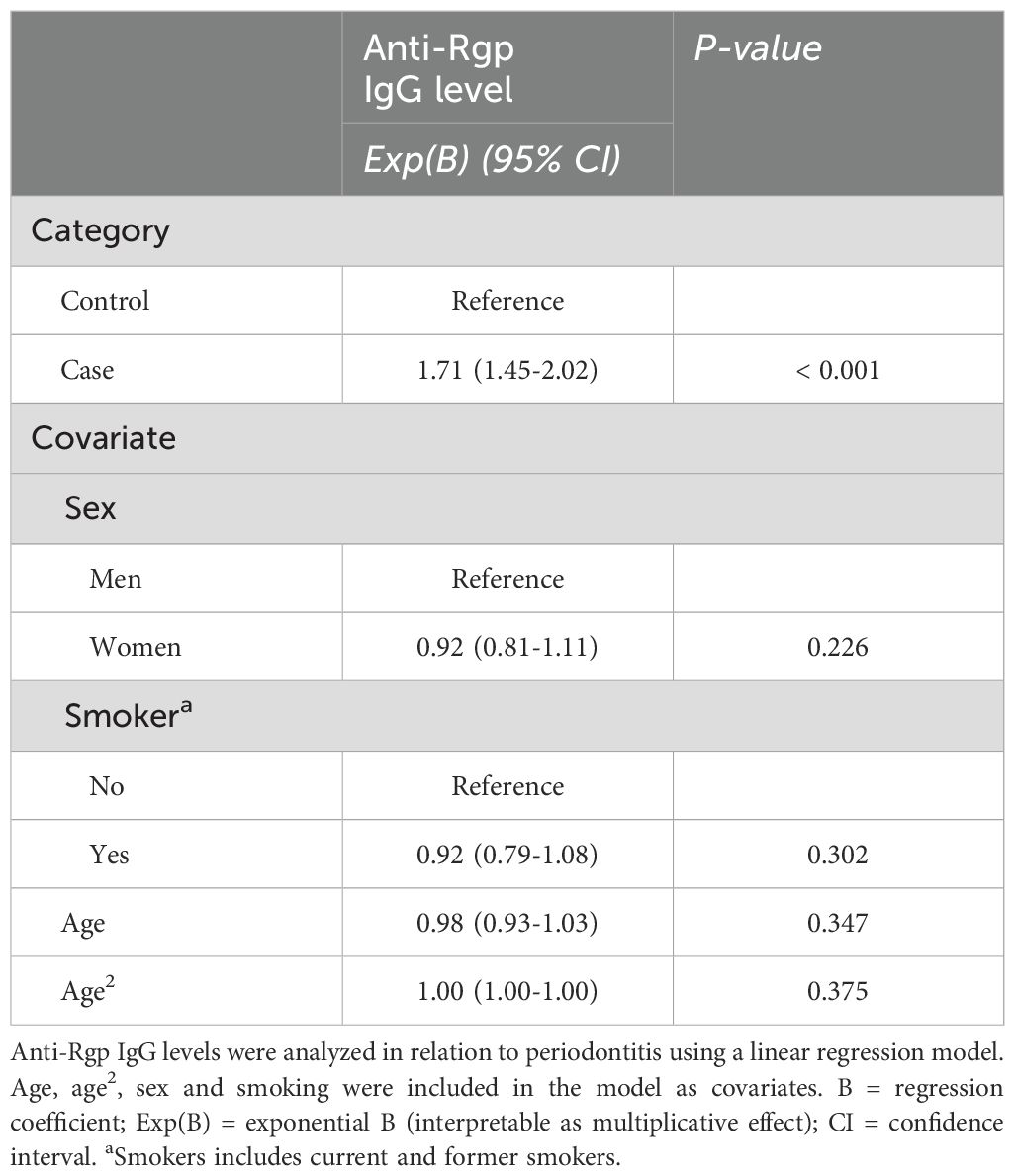
Table 2. Association between serum anti-Rgp IgG and periodontitis.
3.3 Anti-Rgp IgG levels associate with periodontal inflammation and alveolar bone loss
Next, we analyzed anti-Rgp IgG levels in relation to different clinical periodontal parameters; periodontal inflammation, measured as bleeding on probing, (BoP), periodontal probing pocket depth (PPD), and alveolar bone loss. We detected significantly higher anti-Rgp IgG levels in cases with high periodontal inflammation (Figure 2A). The average increase in anti-Rgp IgG levels in cases with high versus low periodontal inflammation was 50%, p<0.001 (Table 3). We also found higher anti-Rgp IgG levels in cases with high level of alveolar bone loss (Figure 2B). For cases with high versus low level of alveolar bone loss, the average increase of anti-Rgp IgG levels was 65%, p<0.002 (Table 3), and here we also observed a significant increase (40%) when comparing cases with high versus moderate level of alveolar bone loss, p=0.042. We found no association between anti-Rgp IgG levels and level of PPD (Figure 2C, Table 3). These analyses were adjusted for the confounding effects of age, age2, sex and smoking.
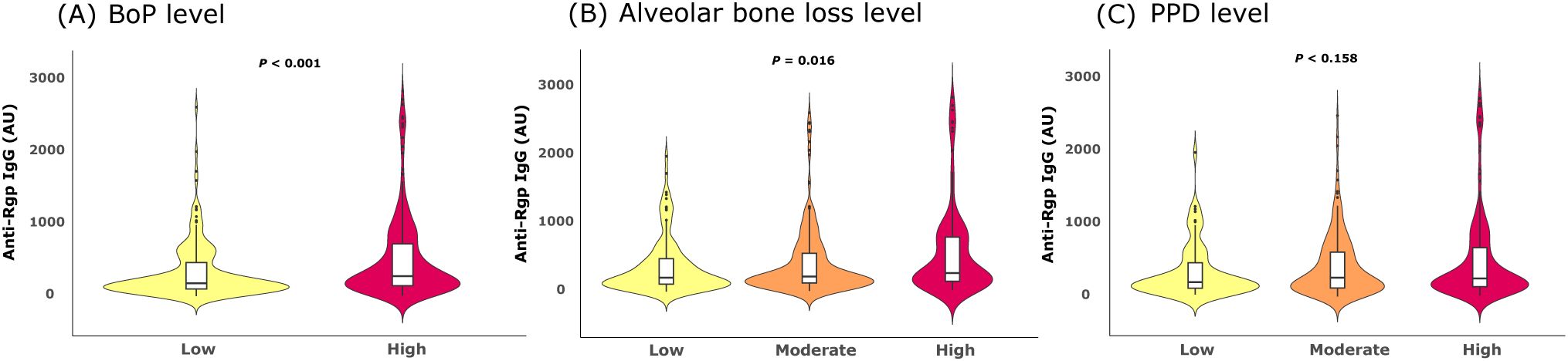
Figure 2. Anti-Rgp IgG levels are elevated in cases with periodontal inflammation and advanced alveolar bone loss. Violin plots show distribution of Rgp IgG levels in PerioGene North cases, based on: (A) degree of periodontal inflammation, measured as bleeding on probing (BoP); (B) level of alveolar bone loss and (C) periodontal pocket probing depth (PPD) level. Integrated box plots show median AU values and 25th and 75th percentiles as horizontal lines; whiskers indicate 10th to 90th percentile; outliers are plotted as dots. Rgp = arginine gingipain; AU = arbitrary units.
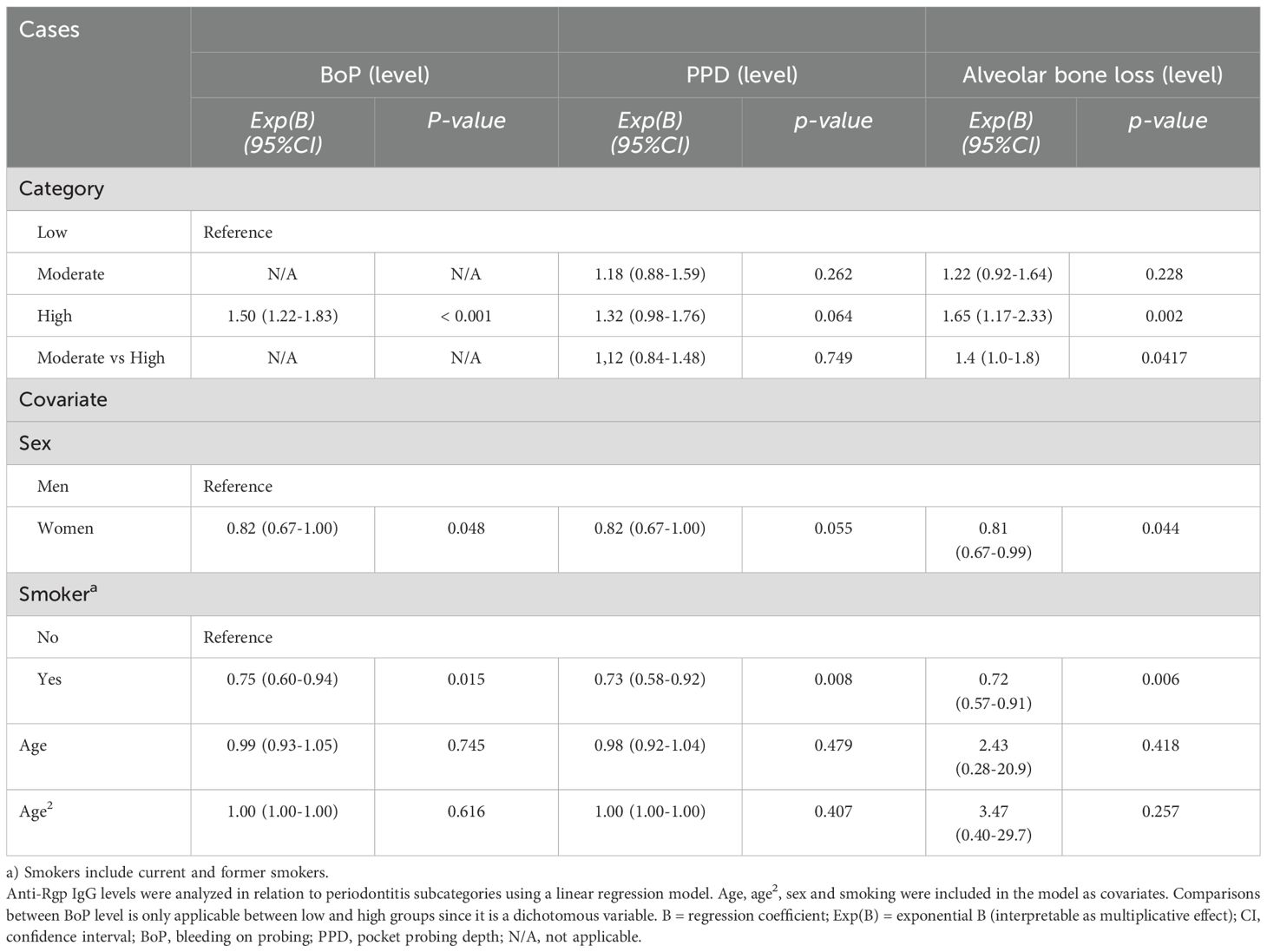
Table 3. Average increase in anti-Rgp IgG levels between different clinical subgroups of periodontitis cases.
3.4 RA-specific autoimmunity does not associate with periodontitis or anti-Rgp IgG
Next, we analyzed the presence of ACPA IgG in PerioGene North. When applying the manufacturer’s suggested cutoff value of ≥25 U/mL, 21 individuals were considered ACPA-positive. Notably, 15 of these had periodontitis, giving a frequency of 3.1% ACPA-positive cases and 1.2% ACPA-positive controls, p=0.003 (Table 1). Among the ACPA-positive participants, 1 case and 2 controls had been diagnosed with RA. Yet, there was no significant association between periodontitis and ACPA after adjusting for age and smoking (data not shown). Furthermore, anti-Rgp IgG levels did not differ significantly between ACPA-positive and ACPA-negative individuals (data not shown).
4 Discussion
In this study, we demonstrate that serum anti-Rgp IgG levels cannot clearly discriminate individuals with periodontitis from periodontally healthy but define a subgroup of periodontitis patients with high periodontal inflammation and advanced alveolar bone loss. Moreover, we find no strong support for a link between periodontitis or anti-Rgp IgG and RA-specific autoimmunity, e.g. ACPA.
Antibodies against periodontal pathogens have been investigated for many years (24). In particular, antibodies against P. gingivalis have been shown to associate with periodontitis (25), and among 29 different P. gingivalis antigens, Hirai and co-authors recently showed that the gingipains elicited the most sensitive and specific IgG responses in patients with periodontitis (14), supporting the use of Rgp in our study.
The data presented herein clearly show that individuals with periodontitis present with higher anti-Rgp IgG levels than periodontally healthy controls, which is in accordance with our previous findings (17). It should be noted that high anti-Rgp IgG levels were also detected among some of the controls. Studies have suggested that periodontally healthy individuals are able to produce highly functional antibodies, protecting against P. gingivalis colonization, whereas periodontitis patients produce less functional antibodies with lower avidity (26). Hence, we speculate that the presence of anti-Rgp antibodies in periodontally healthy controls in our study reflects a healthy immune response, while high levels of anti-Rgp IgG that we see in a subset of periodontitis patients indicate high P. gingivalis counts and high pathogenic gingipain load. In support of this scenario, several studies showed decreased anti-P. gingivalis antibody levels in response to successful periodontal treatment, following lower bacterial counts (27–29).
Our previous data (17), based on 41 cases and 39 controls from PerioGene North, indicated a very good capacity for anti-Rgp antibodies to discriminate cases from controls (AUC=0.79). Thus, we wanted to further validate our data in the entire cohort. However, in the present study, anti-Rgp IgG had poor discriminatory ability to distinguish cases from controls (AUC=0.63). The discrepant data between the two studies suggests that the sub-cohort is unrepresentative of the entire PerioGene North cohort. Moreover, the results in the present study are in agreement with our previous findings in PAROKRANK, a case-control study designed to investigate periodontal health in relation to myocardial infarction, where anti-Rgp IgG also could not separate periodontitis patients from controls efficiently, but was still significantly elevated in individuals with severe forms of periodontitis compared to controls (17).
In here, we present significant associations between anti-Rgp IgG and specific clinical periodontal parameters, periodontal inflammation and alveolar bone loss. Thus, collectively, these data indicate that anti-Rgp antibodies are not likely to perform well as predictive biomarkers for periodontitis per se, while they may still be valuable indicators of risk for severe periodontal damage.
Gingipains are known for their proteolytic capacity, including the degradation of components of the complement system and extracellular matrix structures (30). They can directly contribute to gingival bleeding and tissue breakdown by degrading fibrinogen (31). Interestingly, gingipains have also been shown to promote osteoclastogenesis in vitro, thus implicating a possible role in bone resorption (32). Noteworthy, both gingipain vaccines and gingipain-inhibitors have been used successfully to prevent P. gingivalis-induced periodontal damage in experimental models (33, 34). Moreover, we have previously shown elevated anti-Rgp antibody levels in RA versus controls (15), and given the results in the present study – demonstrating an association between high anti-Rgp antibody levels and advanced alveolar bone loss – anti-Rgp IgG levels should potentially also be examined in relation to articular bone loss in RA. Notably, a recent study links oral bacteremia to RA flares (35), and other studies have detected P. gingivalis DNA in RA synovial joints (36, 37). Thus, the mechanistic role of gingipains in inflammation-mediated bone resorption should be further explored.
Several studies have linked periodontitis and periodontal pathogens to ACPA-positive RA (15, 35, 38), including a recently published meta-analysis demonstrating that RA patients with periodontitis have significantly higher ACPA levels than RA patients without periodontitis (39). However, until now, it has not been clear if periodontitis alone is sufficient to elicit a systemic ACPA response, as previous studies are sparse and present conflicting results. The present study is, to the best our knowledge, the first to investigate ACPA status in a large and well-characterized periodontitis case-control study. Although we observed a higher frequency of ACPA-positivity among periodontitis patients compared to controls, in line with our previous report (17), this was not significant after adjustment for the confounding effects of smoking and age. Given that only 15 of 478 individuals with periodontitis were ACPA-positive, we were underpowered to analyze ACPA in relation to periodontal parameters.
In accordance with the data herein, a cross-sectional study by Lew and co-authors did not find differences in ACPA levels when comparing periodontitis patients without RA and healthy controls (40). In here, we did not find an association between ACPA status and anti-Rgp. Similarly, Svard et al. found no association between anti-Rgp antibodies in saliva and periodontitis or ACPA status (41). In summary, the data we present are based on a large and well-characterized periodontitis cohort and suggest that there is not convincing evidence for that a systemic ACPA response is connected to periodontitis, or elevated anti-Rgp IgG levels in periodontitis patients. Still, this does not rule out that locally produced ACPA in inflamed gingival tissue are involved in onset and/or progression of RA in susceptible individuals. Notably, ACPA have been detected in gingival crevicular fluid from non-RA individuals (42).
The main strength with the present study is the significant power of PerioGene North, owing to its large number of study participants and the high resolution clinical periodontal data provided by trained specialists. Within this material, we have previously described serum levels of hs-CRP that are in line with results presented in a meta-analysis (43), implying that PerioGene North is well suited for investigating, and detecting, serum markers associated with periodontitis. Unlike the periodontitis cases in PAROKRANK, where more than half were affected by myocardial infarction, the overall presence of general diseases in PerioGene North is low (19). Therefore, the elevated anti-Rgp IgG levels observed in PerioGene North are less likely to be affected by the presence of other systemic diseases.
A limitation with our study was that the case group, due to the original purpose of PerioGene North to study genetic polymorphisms, were not matched to controls on age. However, all controls were 34 years or older, which is a strength as many other studies have included young adults as periodontally healthy controls. Still, this resulted in an older case group and all analyses were subsequently adjusted for age as well as for smoking, both well-known risk factors for periodontitis (44, 45). In our previous report (19), post-hoc analysis within different age groups confirmed that the distinguishable protein profile was not a result of the case group being older.
In conclusion, our data show that periodontitis per se is not associated with the presence of a systemic ACPA response and that ACPA-positive individuals in this cohort do not have an increased antibody response to Pg virulence factor arginine gingipain. While anti-Rgp IgG showed poor ability to separate patients with periodontitis from periodontally healthy in an efficient manner, elevated levels associate significantly with the subset of patients that have active periodontal inflammation and advanced alveolar bone loss. Prospective studies could reveal whether high anti-Rgp IgG levels can serve as a biomarker to predict a more aggressive disease course. Future studies should also address the actions of gingipains in the context of bone resorption, to clarify molecular mechanisms, and further explore whether blocking gingipains could be a future treatment for periodontitis.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Regional Ethical Review Board at Umeå University, the Regional Ethical Review Board at Uppsala University and the Swedish Ethical Review Authority. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in the study.
Author contributions
EK: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Visualization, Writing – original draft, Writing – review & editing. Cd: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. MW: Formal analysis, Investigation, Methodology, Writing – review & editing. BP: Methodology, Resources, Writing – review & editing. JP: Funding acquisition, Methodology, Resources, Writing – review & editing. SL: Methodology, Project administration, Writing – review & editing. AE: Formal analysis, Methodology, Supervision, Writing – review & editing. KL: Conceptualization, Funding acquisition, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing. PL: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The County Council of Västerbotten Spjutspetsmedel funded this research, grant number RV 396172146 (PLU), the County Council of Västerbotten Internal Research Foundation, grant number RV 396172134 (PLU), and Wallenberg Centre for Molecular Medicine (WCMM), grant number RV 813051 (EK). Work conducted by CV and KL was funded by King Gustav V 80-year foundation, grant numbers: FAI-2020-0646 and FAI-2021-0771, and the Swedish Rheumatism foundation, grant number: R-969194. JP acknowledges support by grant from: US NIH/NIDCR (DE 022597). None of the funding bodies influenced the study design, data collection, analysis, interpretation, or manuscript writing.
Acknowledgments
First and foremost, we acknowledge and express our sincere gratitude to all study participants and to the senior consultants in periodontology and resident and general dentists and dental nurses within the participating counties of Västerbotten, Gävleborg, Uppsala, and Västmanland. A special thanks to Britt-Inger Nordell for your invaluable efforts. We acknowledge the support provided by The Clinical Research Center at Norrlands University Hospital and the Medical Biobank of Northern Sweden. The authors also wish to thank MSc student Sabrina Kunz at Karolinska Institutet.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor TV declared a past co-authorship with the author JP.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Pihlstrom BL, Michalowicz BS, Johnson NW. Periodontal diseases. Lancet. (2005) 366:1809–20. doi: 10.1016/S0140-6736(05)67728-8
2. Hajishengallis G. Periodontitis: from microbial immune subversion to systemic inflammation. Nat Rev Immunol. (2015) 15:30–44. doi: 10.1038/nri3785
3. Fuggle NR, Smith TO, Kaul A, Sofat N. Hand to mouth: A systematic review and meta-analysis of the association between rheumatoid arthritis and periodontitis. Front Immunol. (2016) 7:80. doi: 10.3389/fimmu.2016.00080
4. Kaur G, Mohindra K, Singla S. Autoimmunity-Basics and link with periodontal disease. Autoimmun Rev. (2017) 16:64–71. doi: 10.1016/j.autrev.2016.09.013
5. Cantley MD, Haynes DR, Marino V, Bartold PM. Pre-existing periodontitis exacerbates experimental arthritis in a mouse model. J Clin Periodontol. (2011) 38:532–41. doi: 10.1111/j.1600-051X.2011.01714.x
6. Kindstedt E, Johansson L, Palmqvist P, Koskinen Holm C, Kokkonen H, Johansson I, et al. Association between marginal jawbone loss and onset of rheumatoid arthritis and relationship to plasma levels of RANKL. Arthritis Rheumatol. (2017) 70(4):508–15. doi: 10.1002/art.40394
7. Rafiei M, Kiani F, Sayehmiri K, Sayehmiri F, Tavirani M, Dousti M, et al. Prevalence of anaerobic bacteria (P.gingivalis) as major microbial agent in the incidence periodontal diseases by meta-analysis. J Dent (Shiraz). (2018) 19:232–42.
8. Zheng S, Yu S, Fan X, Zhang Y, Sun Y, Lin L, et al. Porphyromonas gingivalis survival skills: Immune evasion. J Periodontal Res. (2021) 56:1007–18. doi: 10.1111/jre.12915
9. Guo Y, Nguyen KA, Potempa J. Dichotomy of gingipains action as virulence factors: from cleaving substrates with the precision of a surgeon’s knife to a meat chopper-like brutal degradation of proteins. Periodontol. (2010) 54:15–44. doi: 10.1111/j.1600-0757.2010.00377.x
10. Hocevar K, Potempa J, Turk B. Host cell-surface proteins as substrates of gingipains, the main proteases of Porphyromonas gingivalis. Biol Chem. (2018) 399:1353–61. doi: 10.1515/hsz-2018-0215
11. McGraw WT, Potempa J, Farley D, Travis J. Purification, characterization, and sequence analysis of a potential virulence factor from Porphyromonas gingivalis, peptidylarginine deiminase. Infection Immun. (1999) 67:3248–56. doi: 10.1128/IAI.67.7.3248-3256.1999
12. Bryzek D, Ciaston I, Dobosz E, Gasiorek A, Makarska A, Sarna M, et al. Triggering NETosis via protease-activated receptor (PAR)-2 signaling as a mechanism of hijacking neutrophils function for pathogen benefits. PloS Pathog. (2019) 15:e1007773. doi: 10.1371/journal.ppat.1007773
13. Sherina N, de Vries C, Kharlamova N, Sippl N, Jiang X, Brynedal B, et al. Antibodies to a citrullinated porphyromonas gingivalis epitope are increased in early rheumatoid arthritis, and can be produced by gingival tissue B cells: implications for a bacterial origin in RA etiology. Front Immunol. (2022) 13:804822. doi: 10.3389/fimmu.2022.804822
14. Hirai K, Yamaguchi-Tomikawa T, Eguchi T, Maeda H, Takashiba S. Identification and modification of porphyromonas gingivalis cysteine protease, gingipain, ideal for screening periodontitis. Front Immunol. (2020) 11:1017. doi: 10.3389/fimmu.2020.01017
15. Kharlamova N, Jiang X, Sherina N, Potempa B, Israelsson L, Quirke AM, et al. Antibodies to porphyromonas gingivalis indicate interaction between oral infection, smoking, and risk genes in rheumatoid arthritis etiology. Arthritis Rheumatol. (2016) 68:604–13. doi: 10.1002/art.39491
16. Johansson L, Sherina N, Kharlamova N, Potempa B, Larsson B, Israelsson L, et al. Concentration of antibodies against Porphyromonas gingivalis is increased before the onset of symptoms of rheumatoid arthritis. Arthritis Res Ther. (2016) 18:201. doi: 10.1186/s13075-016-1100-4
17. de Vries C, Ruacho G, Kindstedt E, Potempa BA, Potempa J, Klinge B, et al. Antibodies to porphyromonas gingivalis are increased in patients with severe periodontitis, and associate with presence of specific autoantibodies and myocardial infarction. J Clin Med. (2022) 11. doi: 10.3390/jcm11041008
18. Bender P, Burgin WB, Sculean A, Eick S. Serum antibody levels against Porphyromonas gingivalis in patients with and without rheumatoid arthritis - a systematic review and meta-analysis. Clin Oral Investigations. (2017) 21:33–42. doi: 10.1007/s00784-016-1938-5
19. Wanman M, Betner S, Esberg A, Holm CK, Isehed C, Holmlund A, et al. The perioGene north study uncovers serum proteins related to periodontitis. J Dental Res. (2024) 103(10):999–1007. doi: 10.1177/00220345241263320
20. Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Periodontol. (2018) 89 Suppl 1:S159–S72. doi: 10.3390/jcm11041008
21. Holtfreter B, Kuhr K, Borof K, Tonetti MS, Sanz M, Kornman K, et al. ACES: A new framework for the application of the 2018 periodontal status classification scheme to epidemiological survey data. J Clin Periodontol. (2024) 51:512–21. doi: 10.1111/jcpe.13965
22. Holmlund A, Hedin M, Pussinen PJ, Lerner UH, Lind L. Porphyromonas gingivalis (Pg) a possible link between impaired oral health and acute myocardial infarction. Int J Cardiol. (2011) 148:148–53. doi: 10.1016/j.ijcard.2009.10.034
23. Veillard F, Potempa B, Guo Y, Ksiazek M, Sztukowska MN, Houston JA, et al. Purification and characterisation of recombinant His-tagged RgpB gingipain from Porphymonas gingivalis. Biol Chem. (2015) 396:377–84. doi: 10.1515/hsz-2014-0304
24. Murayama Y, Nagai A, Okamura K, Kurihara H, Nomura Y, Kokeguchi S, et al. Serum immunoglobulin G antibody to periodontal bacteria. Adv Dent Res. (1988) 2:339–45. doi: 10.1177/08959374880020022401
25. Dye BA, Herrera-Abreu M, Lerche-Sehm J, Vlachojannis C, Pikdoken L, Pretzl B, et al. Serum antibodies to periodontal bacteria as diagnostic markers of periodontitis. J Periodontol. (2009) 80:634–47. doi: 10.1902/jop.2009.080474
26. Takahashi J, Saito A, Nakagawa T, Yamada S, Ishihara K, Okuda K. Dynamics of serum immunoglobulin G avidity for porphyromonas gingivalis in adult periodontitis. J Periodontol. (1998) 69:367–73. doi: 10.1902/jop.1998.69.3.367
27. Nakayama Y, Ogata Y, Hiromatsu Y, Imamura K, Suzuki E, Saito A, et al. Clinical usefulness of novel immunochromatographic detection device for porphyromonas gingivalis in evaluating effects of scaling and root planing and local antimicrobial therapy. J Periodontol. (2016) 87:1238–47. doi: 10.1902/jop.2016.160147
28. Morozumi T, Yashima A, Gomi K, Ujiie Y, Izumi Y, Akizuki T, et al. Increased systemic levels of inflammatory mediators following one-stage full-mouth scaling and root planing. J Periodontal Res. (2018) 53:536–44. doi: 10.1111/jre.2018.53.issue-4
29. Kudo C, Naruishi K, Maeda H, Abiko Y, Hino T, Iwata M, et al. Assessment of the plasma/serum IgG test to screen for periodontitis. J Dent Res. (2012) 91:1190–5. doi: 10.1177/0022034512461796
30. Ruggiero S, Cosgarea R, Potempa J, Potempa B, Eick S, Chiquet M. Cleavage of extracellular matrix in periodontitis: gingipains differentially affect cell adhesion activities of fibronectin and tenascin-C. Biochim Biophys Acta. (2013) 1832:517–26. doi: 10.1016/j.bbadis.2013.01.003
31. Ally N, Whisstock JC, Sieprawska-Lupa M, Potempa J, Le Bonniec BF, Travis J, et al. Characterization of the specificity of arginine-specific gingipains from porphyromonas gingivalis reveals active site differences between different forms of the enzymes. Biochemistry. (2003) 42:11693–700. doi: 10.1021/bi0349726
32. Mo W, Luo H, Wu J, Xu N, Zhang F, Qiu Q, et al. Gingipains promote RANKL-induced osteoclastogenesis through the enhancement of integrin beta3 in RAW264.7 cells. J Mol Histol. (2020) 51:147–59. doi: 10.1007/s10735-020-09865-w
33. Huang N, Shimomura E, Yin G, Tran C, Sato A, Steiner A, et al. Immunization with cell-free-generated vaccine protects from Porphyromonas gingivalis-induced alveolar bone loss. J Clin Periodontol. (2019) 46:197–205. doi: 10.1111/jcpe.2019.46.issue-2
34. Dominy SS, Lynch C, Ermini F, Benedyk M, Marczyk A, Konradi A, et al. Porphyromonas gingivalis in Alzheimer’s disease brains: Evidence for disease causation and treatment with small-molecule inhibitors. Sci Adv. (2019) 5:eaau3333. doi: 10.1126/sciadv.aau3333
35. Brewer RC, Lanz TV, Hale CR, Sepich-Poore GD, Martino C, Swafford AD, et al. Oral mucosal breaks trigger anti-citrullinated bacterial and human protein antibody responses in rheumatoid arthritis. Sci Transl Med. (2023) 15:eabq8476. doi: 10.1126/scitranslmed.abq8476
36. Totaro MC, Cattani P, Ria F, Tolusso B, Gremese E, Fedele AL, et al. Porphyromonas gingivalis and the pathogenesis of rheumatoid arthritis: analysis of various compartments including the synovial tissue. Arthritis Res Ther. (2013) 15:R66. doi: 10.1186/ar4243
37. Reichert S, Haffner M, Keysser G, Schafer C, Stein JM, Schaller HG, et al. Detection of oral bacterial DNA in synovial fluid. J Clin Periodontol. (2013) 40:591–8. doi: 10.1111/jcpe.2013.40.issue-6
38. Potempa J, Mydel P, Koziel J. The case for periodontitis in the pathogenesis of rheumatoid arthritis. Nat Rev Rheumatol. (2017) 13:606–20. doi: 10.1038/nrrheum.2017.132
39. Eezammuddeen NN, Vaithilingam RD, Hassan NHM. Influence of periodontitis on levels of autoantibodies in rheumatoid arthritis patients: A systematic review. J Periodontal Res. (2023) 58:29–42. doi: 10.1111/jre.13065
40. Lew PH, Rahman MT, Safii SH, Baharuddin NA, Bartold PM, Sockalingam S, et al. Antibodies against citrullinated proteins in relation to periodontitis with or without rheumatoid arthritis: a cross-sectional study. BMC Oral Health. (2021) 21:360. doi: 10.1186/s12903-021-01712-y
41. Svard A, Kastbom A, Ljungberg KR, Potempa B, Potempa J, Persson GR, et al. Antibodies against Porphyromonas gingivalis in serum and saliva and their association with rheumatoid arthritis and periodontitis. Data from two rheumatoid arthritis cohorts in Sweden. Front Immunol. (2023) 14:1183194. doi: 10.3389/fimmu.2023.1183194
42. de Smit MJ, Rahajoe PS, Raveling-Eelsing E, Lisotto P, Harmsen HJM, Kertia N, et al. Influence of oral microbiota on the presence of igA anti-citrullinated protein antibodies in gingival crevicular fluid. Front Oral Health. (2022) 3:904711. doi: 10.3389/froh.2022.904711
43. Paraskevas S, Huizinga JD, Loos BG. A systematic review and meta-analyses on C-reactive protein in relation to periodontitis. J Clin Periodontol. (2008) 35:277–90. doi: 10.1111/j.1600-051X.2007.01173.x
44. Leite FRM, Nascimento GG, Scheutz F, Lopez R. Effect of smoking on periodontitis: A systematic review and meta-regression. Am J Prev Med. (2018) 54:831–41. doi: 10.1016/j.amepre.2018.02.014
Keywords: periodontitis, alveolar bone loss, periodontal inflammation, cysteine peptidase gingipain B, anti-citrullinated protein antibodies
Citation: Kindstedt E, de Vries C, Wänman M, Potempa BA, Potempa J, Lindquist S, Esberg A, Lundberg K and Lundberg P (2025) The PerioGene North study reveals that periodontal inflammation and advanced jawbone loss in periodontitis associate with serum gingipain antibodies but not with systemic autoimmunity. Front. Immunol. 15:1504975. doi: 10.3389/fimmu.2024.1504975
Received: 01 October 2024; Accepted: 19 December 2024;
Published: 14 January 2025.
Edited by:
Teun J. De Vries, VU Amsterdam, NetherlandsReviewed by:
Josefine Hirschfeld, University of Birmingham, United KingdomJeffrey Ebersole, University of Nevada, Las Vegas, United States
Copyright © 2025 Kindstedt, de Vries, Wänman, Potempa, Potempa, Lindquist, Esberg, Lundberg and Lundberg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elin Kindstedt, ZWxpbi5raW5kc3RlZHRAdW11LnNl