 Andrea Alemany1,2,3
Andrea Alemany1,2,3 Núria Balanza1,4
Núria Balanza1,4 Pere Millat-Martinez1
Pere Millat-Martinez1 Dan Ouchi1,2Marc Corbacho-Monné2,3,5
Dan Ouchi1,2Marc Corbacho-Monné2,3,5 Cristian Morales-Indiano3,6
Cristian Morales-Indiano3,6 Gema Fernández Rivas7
Gema Fernández Rivas7 Ignacio Blanco3,6Oriol Mitjà2,3
Ignacio Blanco3,6Oriol Mitjà2,3 Ruth Aguilar1,4,8
Ruth Aguilar1,4,8 Carlota Dobaño1,4,8
Carlota Dobaño1,4,8 Quique Bassat1,4,9,10,11,12,13
Quique Bassat1,4,9,10,11,12,13 Gemma Moncunill1,4,8Bàrbara Baro1* and COnV-ert BMK STUDY GROUP
Gemma Moncunill1,4,8Bàrbara Baro1* and COnV-ert BMK STUDY GROUP- 1ISGlobal, Barcelona, Spain
- 2Fight Infectious Diseases Foundation, Badalona, Spain
- 3Hospital Universitari Germans Trias i Pujol, Badalona, Spain
- 4Facultat de Medicina i Ciències de la Salut, Universitat de Barcelona (UB), Barcelona, Spain
- 5Hospital Universitari Parc Taulí, Sabadell, Spain
- 6Clinical Laboratory Metropolitana Nord, Badalona, Spain
- 7Microbiology Department, Clinical Laboratory Metropolitana Nord, Barcelona, Spain
- 8CIBER Enfermedades Infecciosas (CIBERINFEC), Instituto de Salud Carlos III, Madrid, Spain
- 9CIBER de Epidemiología y Salud Pública, Instituto de Salud Carlos III, Madrid, Spain
- 10Consorcio de Investigación Biomédica en Red de Epidemiología y Salud Pública (CIBERESP), Madrid, Spain
- 11ICREA, Pg Lluís Companys 23, Barcelona, Spain
- 12Pediatrics Department, Hospital Sant Joan de Déu, Universitat de Barcelona, Esplugues, Barcelona, Spain
- 13Centro de Investigação em Saúde de Manhiça (CISM), Maputo, Mozambique
Introduction: Evidence on the association of biomarkers of host response to infection with COVID-19 clinical outcomes has focused mainly on hospitalized patients. We investigated the prognostic performance of 39 immune and endothelial activation markers measured early in the course of disease to predict the development of severe COVID-19 and hospitalization.
Methods: We conducted a nested case-control study from a randomized clinical trial evaluating the efficacy of COVID-19 convalescent plasma in outpatients aged 50 years or older presenting with mild-to-moderate COVID-19. We selected participants who were hospitalized within 28 days (cases) and who were not (controls) to compare their biomarker levels in plasma samples collected at enrolment.
Results: A total of 42 cases and 42 controls were included in this study. The levels of CRP, IL6, IP10, ferritin, IFNα, IL8, IL1RA, MCP1, and RANTES, determined within 7 days of symptoms onset, showed good individual prognostic performance for COVID-19 associated hospitalization by day 28. The biomarkers CRP, IL6, IP10, IL8, IL1RA, and suPAR showed good individual prognostic performance for severe COVID-19. CRP, IL6 and IP10 had the most robust association with both hospitalization and severe COVID-19, with CRP having the highest discriminatory capacity with hospitalization, and IL6 for severe COVID-19.
Discussion: Our study shows good prognostic performance of CRP and IL6 for 28-day hospitalization in patients with mild-to-moderate COVID-19, in the absence of clinical criteria for admission upon enrolment. These findings confirm the value of these biomarkers at early stages of COVID-19 disease in the outpatient setting to support management decisions.
Introduction
COVID-19 can rapidly progress to severe disease, leading to acute respiratory distress, multi-organ failure, and death, particularly in individuals with underlying conditions, weakened immune systems, and unvaccinated (1). COVID-19 symptoms and risk factors have shown poor specificity and thus limited accuracy for early identification of patients at risk (1–3), hence the role of host biomarkers in predicting severe outcomes has been investigated to enhance triaging strategies. Several biomarkers of inflammation, thrombosis, blood count and coagulation, end-organ damage, as well as immune and endothelial activation have shown to be associated with oxygen requirement, non-invasive ventilation, intensive care admission, and in-hospital mortality.
Most of the evidence has focused on hospitalized patients at a severe stage of the disease. Meta-analyses compiling the initial evidence, mainly based on retrospective studies involving hospitalized patients in China, highlighted the association of disease severity and mortality with lymphopenia, thrombocytopenia, elevated levels of C-reactive protein (CRP), procalcitonin (PCT), lactate dehydrogenase (LDH), D-dimer, ferritin, interleukin 6 (IL6), E-selectin, vascular cell adhesion molecule 1 (VCAM1), and Angiopoietin 2 (Angpt2), among others (4–8). These meta-analyses showed high heterogeneity between studies in severity outcomes, which hindered interpretation of biomarkers’ utility. Prospective studies of hospitalized patients confirmed these associations, also for markers related to immune activation such as interleukin 8 (IL8), soluble urokinase plasminogen activator receptor (suPAR), and soluble triggering receptor expressed on myeloid cells 1 (sTREM1) (9–12). Of note, a large prospective cohort of 1,484 admitted patients showed strong association with disease severity and death of elevated levels of IL6 and tumour necrosis factor (TNF) on admission (13). In a smaller prospective cohort of 187 inpatients, IL6 and suPAR showed the best area under the receiver operating characteristic curve (AUROC) for predicting severe COVID-19 (14), although their performance was nearly comparable to that of age and the National Early Warning Score 2.
Evidence on early biomarkers assessment prior to the onset of severe COVID-19 and hospitalization is rather scarce. A prospective study of 76 patients presenting to an emergency department with mild, moderate, or severe COVID-19 showed strong prognostic accuracy for sTREM1 and IL6, with sTREM1 having the best AUROC for intubation/mortality (0.86; 95% CI: 0.77-0.95) and IL6 for oxygen requirement (0.84; 95% CI: 0.74-0.94) (15). Another prospective study of 426 patients with moderate COVID-19 presenting to two hospitals in India developed and validated three clinical prediction models (particularly useful for resource-limited settings) using age, sex, SpO2, and either neutrophil to lymphocyte ratio, suPAR, or IL6 levels to identify patients unlikely to need supplemental oxygen and hence suitable for safely discharge and community management (16). Hence, it remains to be further demonstrated the prognostic value of these promising biomarkers in early mild COVID-19, to confirm their potential to guide triage and management decisions.
The main aim of this study was to investigate the prognostic performance of 39 immune and endothelial activation markers, measured in patients with mild-to-moderate COVID-19 within 7 days of symptoms onset and discharged home after first clinical assessment, to predict progression to hospitalization and severe COVID-19.
Methods
Study design
We conducted an unmatched nested case-control study from a multicenter, double-blind, randomized, placebo-controlled trial assessing the efficacy of COVID-19 convalescent plasma in preventing severe COVID-19 and hospitalization up to day 28 in patients infected with SARS-CoV-2 with mild-to-moderate illness (COnV-ert trial, NCT04621123) (17). Recruitment was conducted between November 2020 and July 2021 in four health-care centers in Spain.
The COnV-ert trial and the blood sample analysis were approved by the Ethics Committee at Hospital Germans Trials i Pujol (number PI 20-313) and the institutional review boards of all participating centers. All participants provided written informed consent before enrolling in the study.
Study population
Eligible participants for the COnV-ert study were aged 50 years or older, regardless of other risk factors for severe disease, and with confirmed SARS-CoV-2 infection within 5 days from enrolment. All patients were non-hospitalized and with mild-to-moderate COVID-19 upon first presentation, with symptom onset within the previous 7 days. A total of 376 participants were enrolled in the COnV-ert study; and hospitalization up to 28 days occurred in 43/376 participants (11.4%), with no significant differences between the convalescent plasma and the placebo groups.
For this study, we selected participants from the COnV-ert study based on hospitalization status up to day 28 for additional biomarker investigation in plasma samples collected at enrolment and day 7. We included all cases who required hospitalization for COVID-19 progression within 28 days after enrolment and who had available baseline plasma sample. For the control group, we randomly selected participants who did not require hospitalization for COVID-19 up to 28 days at a 1:1 ratio.
Clinical and laboratory evaluation
As part of the COnV-ert study procedures, baseline demographic and clinical characteristics, including risk factors and COVID-19 symptoms and severity, were collected using standardized questionnaires and recorded using a structured electronic case report form. Follow-up visits were performed on days 3, 7, 14, 28, and 60, to assess hospitalization status and disease severity. Severity of COVID-19 was assessed using the WHO Clinical Progression Scale, a validated score that ranges from 0 (not infected), 1-3 (ambulatory mild disease), 4-5 (hospitalized with moderate disease), 6-9 (hospitalized with severe disease) and 10 (dead) (18). Blood samples for biomarker assessment were collected at enrolment, before administration of interventional product, and 7 days after enrolment and administration of interventional product, using EDTA coated tubes.
Blood levels of the inflammatory biomarkers D-dimer, ferritin, IL6, lymphocytes, CRP, and pre-albumin for all participants included were quantified on the same day at the centralized clinical laboratory of Hospital Universitari Germans Trias i Pujol. Plasma D-dimer concentration was measured using a latex-enhanced immunoassay (ACL TOP 750 analyzer, Instrumentation Laboratory), IL6 levels by electrochemiluminiscent immunoassay of paramagnetic particles (Unicel DxI 800 analyzer, Beckman Coulter), CRP, ferritin and pre-albumin were determined by immunoturbidimetry assay (AU5800 analyzer, Beckman Coulter), and lymphocytes count was measured by VCSn technology (DxH900 analyzer, Beckman Coulter). Procedures were performed according to manufacturers’ instructions and blinded to clinical data.
Additional biomarker quantification was retrospectively performed at a centralized laboratory in ISGlobal for the participants included in this study, on samples stored at -80°C without freeze-thaw until batch analyte quantification. The concentrations of a panel of 30 cytokines, chemokines and growth factors were measured in plasma samples by Luminex using the Cytokine Human Magnetic 30-Plex Panel LHC6003M from Life Technologies™. This panel included the following analytes which are involved in inflammatory or immune responses: epidermal growth factor (EGF), eotaxin, fibroblast growth factor (FGF), granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), hepatocyte growth factor (HGF), interferon-alpha (IFNα), IFNγ, interleukin-1 receptor agonist (IL1RA), IL1β, IL2, IL2R, IL4, IL5, IL6, IL7, IL8, IL10, IL12 (p40/p70), IL13, IL15, IL17, IFNγ induced protein 10 (IP10), monocyte chemoattractant protein 1 (MCP1), monokine induced by IFNγ (MIG), macrophage inflammatory protein 1α (MIP1α), MIP1β, Regulated upon Activation, Normal T Cell Expressed and Presumably Secreted (RANTES), Tumor necrosis factor (TNF), and vascular endothelial growth factor (VEGF). Briefly, 25 μL of plasma were tested, applying a modification to the manufacturer’s protocol by using half the volume of all reagents including the standards. This modification was previously tested and showed no difference in assay performance compared to the original protocol and has been used in prior studies (19–21). Each plate included 16 serial dilutions (2-fold) of a standard sample with known concentrations of each analyte and two blanks. In addition, concentrations of Angpt2, IL8, PCT, sTREM1, and suPAR were also measured in plasma samples by Luminex using a custom-developed panel from R&D Systems (LXSAHM) following manufacturer instructions. Each plate included 11 serial dilutions (2-fold) of a standard sample with known concentrations of each analyte and two blanks. For both kits, samples were acquired on a Luminex®100/200™ instrument and analyzed with xPONENT® software 3.1. The concentration of each analyte was obtained by interpolating the median fluorescent intensity (MFI) to a 5-parameter logistic regression curve and reported as pg/mL using the drLumi R package. Limits of quantification (LOQ) were estimated based on cut-off values of the 30% coefficient of variation (CV) of the standard curve for each analyte. When the value of an analyte was below the lower LOQ (LLOQ), a random value between the LLOQ and the LLOQ/2 was assigned. One biomarker from the 30-plex panel (interleukin 15) was excluded from the analyses as more than 30% of the values were under the LLOQ.
Study endpoints
The primary endpoint was hospitalization due to COVID-19 progression within 28 days of enrolment (WHO Clinical Progression scale score 4 to 10). Secondary endpoints included (1) hospitalization with severe COVID-19, defined as hospitalization with requirement of oxygen by non-invasive ventilation or high flow, intubation and mechanical ventilation, or death (WHO Clinical Progression scale score 6 to 10) within 28 days of enrolment, and (2) hospitalization with moderate disease, either with no need for oxygen therapy or with oxygen by mask or nasal prongs (WHO Clinical Progression scale score 4 to 5).
The decision to hospitalize was based on clinical judgement and national guidelines, which were standardized across all study sites, without the use of biomarker information. The secondary endpoint of severe COVID-19, presented with lower frequency, was added as it provides standard definition of severity and allows greater generalizability across different settings.
Statistical methods
All analyses were performed in all study participants with complete baseline biomarker information for all analytes of interest, defining the analysis population. Descriptive data were summarized using medians [interquartile range, IQR] or counts (%).
To investigate the association of the concentration of biomarkers with primary and secondary endpoints, we performed several analyses. Biomarker data were log-transformed for inclusion in all regression models. First, we selected the best discriminatory biomarkers for further exploration using nonparametric statistical methods to compare levels of 39 biomarkers at baseline with hospitalization and severe COVID-19 up to day 28. The Kruskal-Wallis test and post-hoc comparisons with Dunn’s test were used to assess differences in biomarker levels between the three groups: i) non-hospitalized, ii) hospitalized with moderate disease (WHO Clinical Progression scale score 4 to 5), and iii) hospitalized with severe disease (WHO Clinical Progression scale score 6 to 10), with p-values adjusted for multiple comparisons using Holm’s method. We presented a heatmap with the median levels of the biomarkers for each group, and a dendrogram clustering the biomarkers using Ward’s D2 method with Euclidean distances. Second, logistic models were used to estimate odds ratios (ORs) for hospitalization and severe COVID-19 of the selected biomarkers. For logistic models, we estimated univariable and multivariable models accounting for relevant covariates. Third, the discrimination capacity of each biomarker was assessed using AUROCs, which were analyzed nonparametrically and compared pairwise using the algorithm suggested by DeLong et al. (22). Fourth, for the best biomarkers, performance metrics associated with different cut-off levels were calculated. We used cut-offs described in the literature and derived the best ones for our cohort according to the maximum Youden index.
As a secondary aim, we assessed levels of biomarkers at baseline and day 7. Baseline biomarkers levels according to study endpoints were compared non-parametrically using Kruskal-Wallis tests, followed by Dunn’s tests with Holm correction in three groups. In a subset of individuals with biomarker data at day 7, biomarkers kinetics were explored by determining mean changes from baseline to day 7. The mean change of each biomarker was compared, by severity or treatment groups, through fitting linear mixed-effects models, using the individual as random effects in the intercept to adjust for intra-individual correlation and modeling time-group interaction effects. Last, correlation of biomarkers level with viral load was assessed using Spearman’s rank correlation coefficients.
All analyses were performed using Stata v16.1 (Stata Corp, College Station, TX, USA) and R statistical package version 4.3 or higher statistical packages, under a two-tailed significance level of 0.05.
Our unmatched case-control study with a total sample size of 79 participants with a 1:1 ratio (38 cases and 41 controls) has 80% statistical power to detect a minimum relative increase of 44% in the mean levels of CRP marker on log2 scale in the cases vs control group, using a two-sided significance level of 0.05.
Results
Study population characteristics
A total of 84 COnV-ert participants with available baseline plasma samples were included in this study; 42 hospitalized participants (cases) and 42 non-hospitalized (controls). 79/84 participants (38/42 cases and 41/42 controls) had complete baseline biomarker information for all 39 analytes of interest and were included in all analyses (Study flowchart – Supplementary Figure S1).
Baseline demographic and clinical characteristics were similar between cases and controls (Table 1). The median age was 58 (IQR 54 to 66) years, 37/79 (47%) were female, and obesity (39%) was the most frequent coexisting comorbidity. Viral load was significantly higher in cases than controls. The median time from symptom onset to enrolment and sample collection was 5 days (IQR 3 to 6). 42/79 (53%) participants were randomized to receive convalescent plasma infusion. Within the cohort of hospitalized participants, 13/38 (34%) fulfilled the criteria of severe COVID-19 disease according to the WHO Clinical Progression Scale (scores 6 to 10), 5/38 (13%) individuals required mechanical ventilation, and 2/38(5%) died. Median time from recruitment and sample collection to hospitalization was 4 days (IQR 3 to 5).
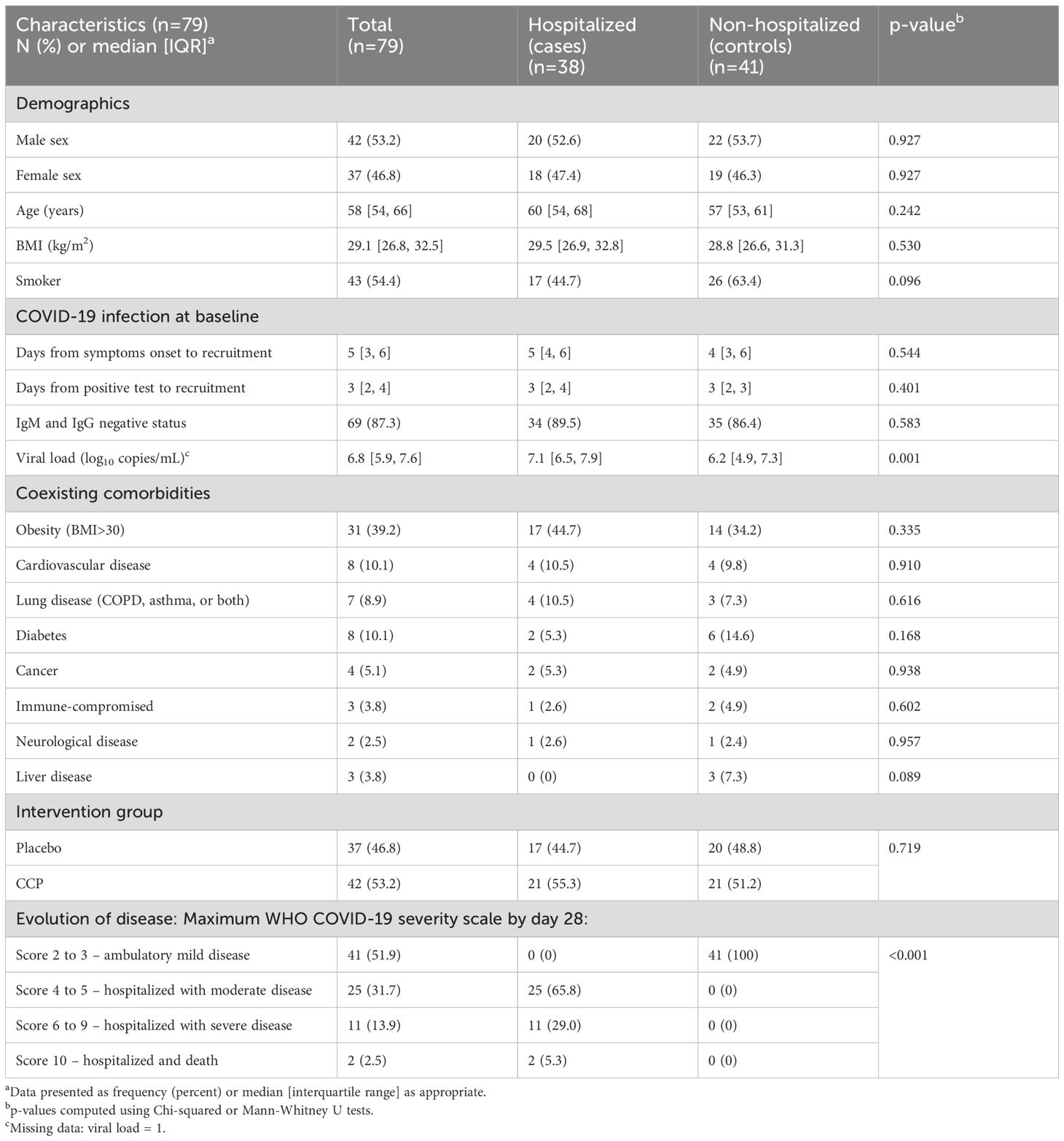
Table 1. Analysis population characteristics.
Selection of best discriminatory biomarkers for further exploration
Of the 39 biomarkers of interest, 11 biomarkers showed an overall significant difference in median baseline biomarker levels based on hospitalization and COVID-19 severity up to day 28, including CRP, ferritin, IFNα, IL6, IL8, IL1RA, IP10, MCP1, RANTES, suPAR, and lymphocytes (Figure 1). Lymphocytes were excluded as levels were not changing sequentially with severity, and the remaining 10 biomarkers were selected for further exploration. Prognostic markers previously highlighted in the literature such as Angpt2, sTREM1, and PCT didn’t show significant differences overall when considering these three groups. Interestingly, our findings showed that while hospitalized participants had lower lymphocyte levels compared to controls (median 1.2x109 cells/L, IQR 1.0 to 1.6), those hospitalized with moderate disease exhibited lower lymphocyte levels than those hospitalized with severe disease (median 0.9x109 cells/L, IQR 0.8 to 1.2 vs median 1.1x109 cells/L, IQR 0.8 to 1.2).

Figure 1. Heatmap: selection of best discriminatory biomarkers. Legend: Heatmap of median levels of the 39 biomarkers of interest with severity of disease achieved within 28 days: (i) non-hospitalized, (ii) hospitalized with moderate COVID-19 disease (WHO Clinical Progression Scale score 4 to 5), (iii) hospitalized with severe COVID-19 disease (WHO Clinical Progression Scale score 6 to 10). P-values were calculated using Krustal-Wallis test. Statistically significant differences are indicated with asterisk (*).
Biomarkers as indicators of hospitalization and severe COVID-19
We observed a significant increased odds of hospitalization within 28 days from enrolment for every two-fold increased level of the biomarkers CRP, IL6, IP10, ferritin, IFNα, IL8, IL1RA, MCP1, and a decrease of RANTES (Table 2). Results were similar after adjustment for age, sex, and BMI. When adjusting for viral load, IFNα, IL8, IL1RA, and MCP1 lost significance, whereas suPAR gained significance. We also observed a significant increased odds of severe COVID-19 (WHO Clinical Progression Scale score 6 to 10) for increased concentration of CRP, IL6, IP10, IL8, IL1RA, and suPAR (Table 2). After adjustment for age, sex, and BMI, ferritin showed a significant increase, suPAR lost significance, and the rest of biomarkers’ associations remained unchanged. After adjusting for viral load, IL1RA was no longer significant. Adjustment for viral load was conducted as baseline viral load showed an independent association with both hospitalization and severe COVID-19, with an odds ratio of 1.71 for every ten-fold increase (95% CI 1.20 to 2.45; p=0.03 for both outcomes).
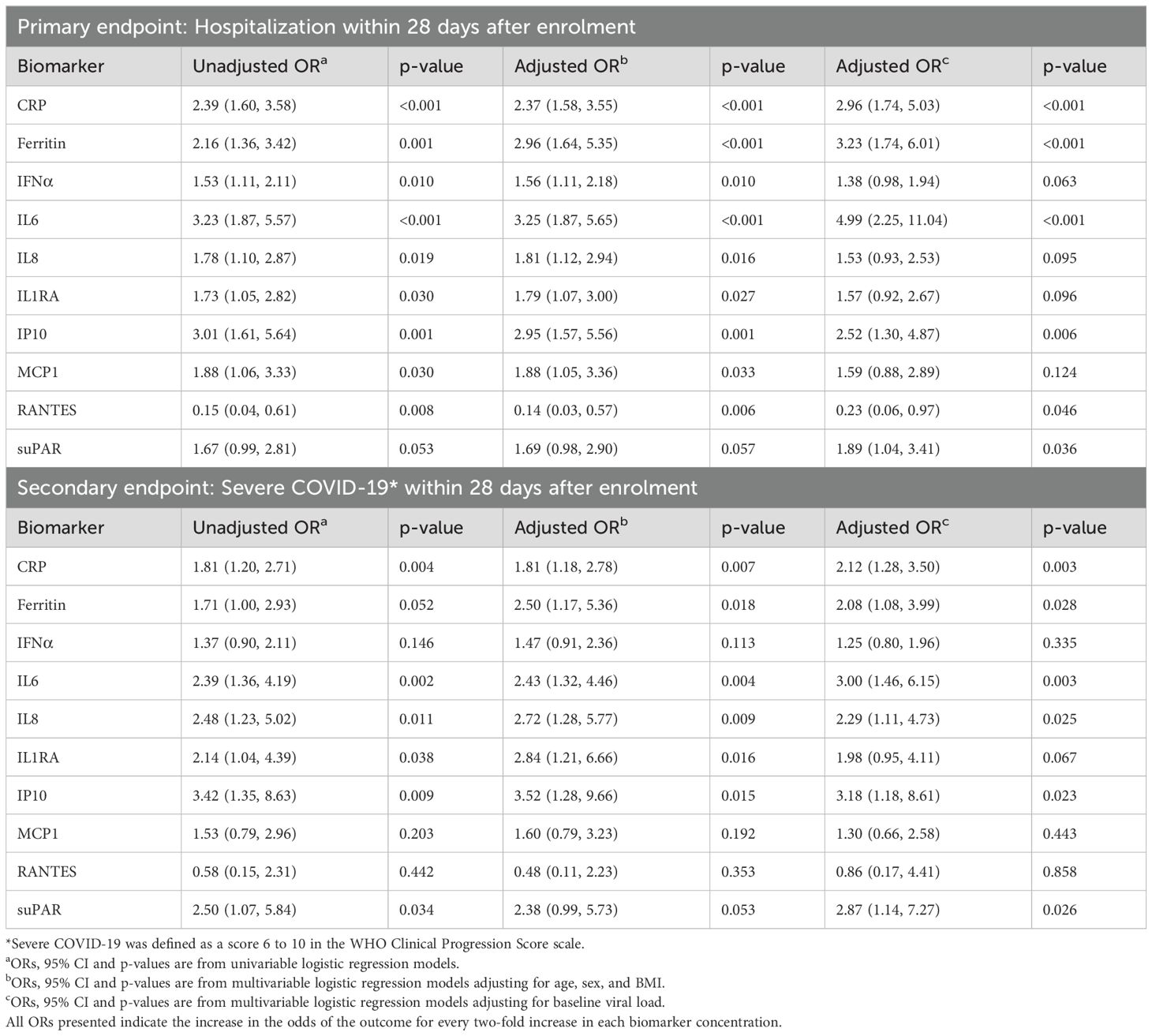
Table 2. Associations between biomarker levels and endpoints in the analysis population.
The biomarkers with the best discrimination capacity for hospitalization were CRP and IL6 (AUROC of 0.83 95% CI: 0.74 to 0.92; and 0.83 95% CI: 0.74 to 0.92, respectively), followed by RANTES, IP10, ferritin, MCP1, IFNα (AUROCs of 0.76 95% CI 0.65 to 0.87; 0.76 95% CI: 0.65 to 0.87; 0.73 95% CI: 0.62 to 0.84; 0.69 95% CI: 0.57 to 0.81; and 0.68 95% CI 0.55 to 0.80), which were not significantly different predictors (Figure 2A). The biomarker with the best discrimination capacity for severe COVID-19 was IL6, with an AUROC of 0.79 (95%CI: 0.66 to 0.93), closely followed by IP10 and CRP (AUROCs of 0.78, 95% CI 0.68 to 0.89; and 0.78, 95% CI 0.67 to 0.89). However, these three markers did not show higher discriminatory capacity for severity compared to IL8, suPAR, IL1RA, ferritin, MCP1, IFNα, and RANTES (Figure 2B).
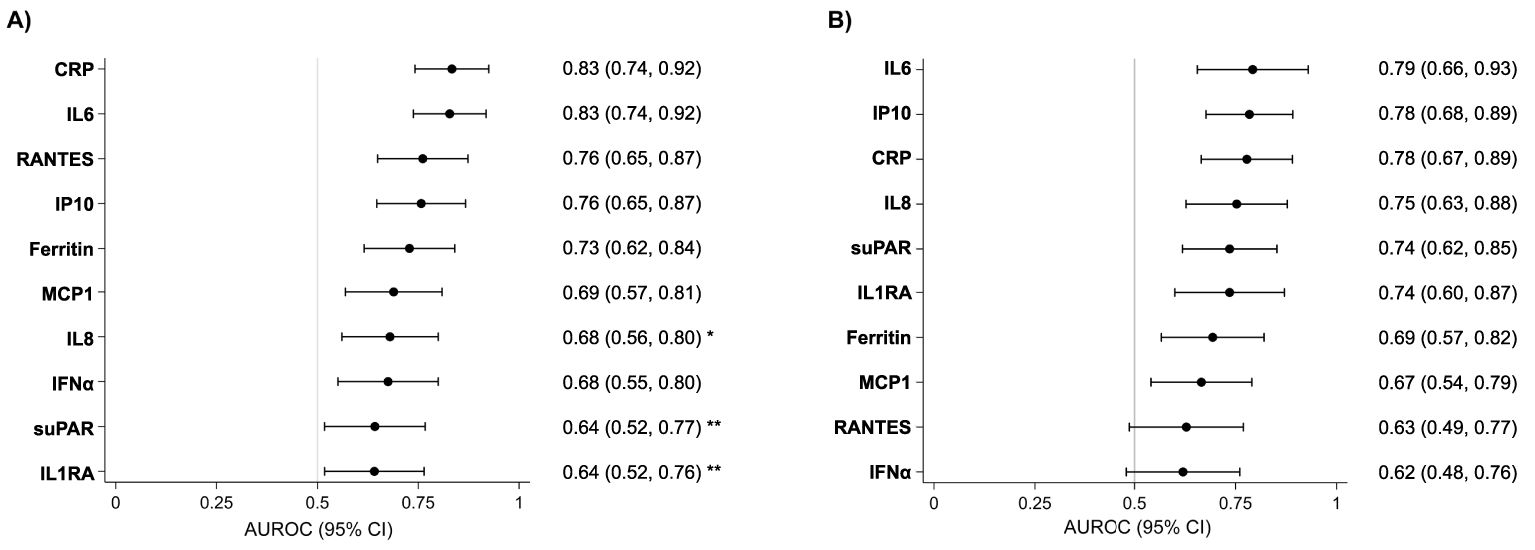
Figure 2. AUROC of each biomarker for hospitalization and severe COVID-19 within 28 days. Legend: Forest plot showing AUROC for hospitalization (A) and for severe COVID-19 (B) within 28 days after enrolment of the 10 selected biomarkers. Dots show AUROC with lines indicating 95% CI. Differences in AUROC between the top-ranking biomarker and other biomarkers were tested using methods recommended by DeLong et al., with an asterisk (*) indicating the AUROC is significantly different to the best one (*p<0.05, **<0.01, ***p<0.001).
We calculated the sensitivity and specificity of CRP and IL6, using the established laboratory reference ranges or cut-off values, to predict hospitalization and severe COVID-19, respectively, in our study cohort (Supplementary Table S1). We obtained high sensitivities of 90% and 92%, respectively. However, while specificity was relatively high for CRP with hospitalization (63%), IL6 showed low specificity to predict severity (44%). We also explored the cut-off values within our cohort that maximize sensitivity and specificity (Supplementary Table S1).
Finally, viral load showed no significant correlation with the selected biomarkers, except for IFNα, IP10, MCP1 and RANTES, with IP10 demonstrating the strongest correlation (Supplementary Figure S2).
Biomarker levels and kinetics by day 7
Distribution of biomarker levels at baseline according to hospitalization status and COVID-19 severity within 28 days is shown in Figure 3. Participants hospitalized with moderate disease (WHO Clinical Progression Scale score 4 to 5), compared to controls, showed significantly higher baseline median levels of CRP, IL6, IP10, ferritin, and MCP1; but not IL8, IL1RA, IFNα, and suPAR, and significantly lower levels of RANTES. Participants hospitalized with severe COVID-19 (WHO Clinical Progression Scale score 6 to 10), showed significantly higher baseline median levels of all selected biomarkers, except for IFNα, and significantly lower levels of RANTES, compared to controls.

Figure 3. Distribution of levels of immune and endothelial activation biomarkers according to hospitalization status and COVID-19 severity within 28 days. Legend: Violin plots showing the distribution of levels of 10 biomarkers of immune and endothelial activation according to hospitalization status and COVID-19 severity within 28 days. Dots indicate median values, with lines indicating IQR. Groups: 0=Non hospitalized (controls), 1=Hospitalized with moderate disease (WHO Clinical Progression Scale score 4 to 5), 2=Hospitalized with severe disease (WHO Clinical Progression Scale score 6 to 10). P-values were calculated using Pairwise Dunn’s test and adjusted by Holm method. Statistically significant differences are indicated with asterisk (*p<0.05, **<0.01, ***p<0.001, ns, non significant).
Biomarker kinetics were explored by determining the mean change in levels of each biomarker (in log10 scale) from baseline to day 7 after enrolment and administration of investigational product. This was done only in a subset of individuals with available sample on day 7 for biomarker’s assessment. We compared biomarkers dynamics between three groups, according to hospitalization status and length of hospitalization as a proxy of severity/recovery: (1) patients non-hospitalized up to day 28 (controls), (2) patients hospitalized but already discharged at day 7 (cases with shorter hospitalization), and (3) patients still hospitalized at day 7 (cases with longer hospitalization) (Figure 4; Supplementary Table S2). Most biomarkers’ levels showed a decrease between baseline and day 7 in non-hospitalized participants, in line with lack of progress towards severity. However, a trend in increasing levels of CRP and ferritin was observed in participants who required hospitalization within 28 days, regardless of hospitalization status at day 7, which showed statistical significance only for ferritin. Moreover, a trend in higher mean levels of IL6, IP10, IL8, IL1RA, and suPAR was observed only in participants still hospitalized at day 7, compared to those already discharged at day 7 and controls. We did not observe significant differences in kinetics for any of the selected biomarkers according to the interventional treatment received at baseline (convalescent plasma or placebo), except for IL1RA (Supplementary Table S3).
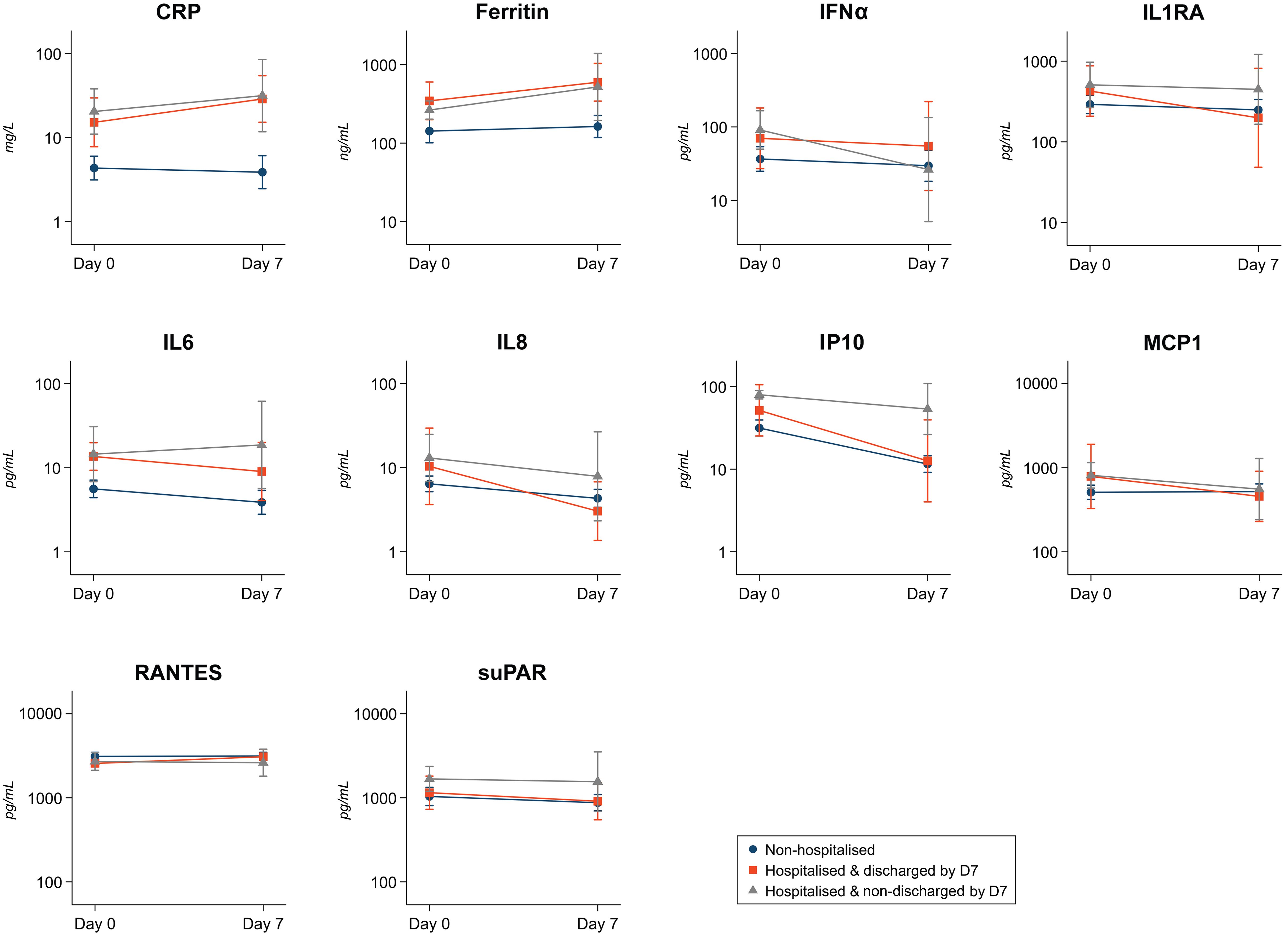
Figure 4. Biomarkers kinetics between baseline and day 7. Legend: Figure shows the kinetics of the 10 selected biomarkers from baseline to day 7 after enrolment in a subset of individuals with available biomarker data on day 7 in three severity groups: (i) non-hospitalized up to day 28 (controls) in blue color; (ii) hospitalized but already discharged at day 7 (cases with shorter hospitalization) in orange; (iii) still hospitalized at day 7 (cases with longer hospitalization) in grey. Figure shows mean (dots) in log10 biomarker levels and 95% CI (vertical lines), and lines connect mean levels between baseline (day 0) and day 7. The mean difference of each biomarker level and the number of participants with available biomarker data on day 7 for each severity group is shown in Supplementary Table S1.
Discussion
In this nested case-control study in mild-to-moderate COVID-19 outpatients, the concentration of the biomarkers CRP, IL6, IP10, ferritin, IFNα, IL8, IL1RA, MCP1, and RANTES determined within 7 days of symptoms onset showed good individual prognostic performance for progression towards hospitalization due to COVID-19 within 28 days. The biomarkers CRP, IL6, IP10, IL8, IL1RA, and suPAR showed also a good performance in identifying those participants at risk of developing severe COVID-19, defined as patients who required oxygen by non-invasive ventilation or high flow, intubation and mechanical ventilation, or who died. These results are in line with large body of evidence showing that several immune activation and inflammatory biomarkers are associated with progression to severe COVID-19. Importantly, we confirmed their prognostic potential when assessed early in the course of disease, prior to the development of clinically noticeable severe manifestations and hospitalization requirement.
Interestingly, CRP, IL6 and IP10 had the most robust association with hospitalization and severe COVID-19, with CRP having the highest discriminatory capacity for hospitalization, and IL6 for severe COVID-19. These results confirm the early prognostic capacity of IL6 to predict oxygen requirement, as observed in two prospective studies of patients presenting with COVID-19 to emergency services (15, 16), given that severity in our study participants was primarily associated with oxygen needs rather than mortality. Unlike our study, these prospective studies found limited prognostic value of CRP levels, especially to discriminate hospital requirement. Although CRP has been largely associated to poor COVID-19 outcomes, also independently of age (23), it is known to be affected by sex, age, and comorbidities (24, 25). This may explain the stronger prognostic performance of CRP in our study, as our population was restricted to older patients with comorbidities. On the other hand, IP10 was linked to severe COVID-19 in early clinical reports of hospitalized patients (26), and has been described as a proxy of viral load for other viral infections, particularly HIV (27–29). While findings regarding the direct relationship between viral load and COVID-19 severity have been inconsistent, our results show higher viral loads in hospitalized patients, confirming viral load is a risk factor in this study population. Additionally, we observed a significant correlation between viral load and IP10 levels, indicating that IP10 may serve as a surrogate marker for disease severity related to viral load in our cohort.
CRP and IL6 levels are widely used in emergency departments in high-income settings as markers of inflammation and disease severity, primarily measured through laboratory assays like ELISA. Interestingly, when applying current reference cut-off values in our cohort, we obtained high sensitivity for both CRP and IL6 to predict hospitalization and severity, respectively. This aligns with the goal of achieving a high negative predictive value to ensure that no patient at risk is overlooked. Notably, novel point-of-care assays for rapid measurement of CRP, IL6, and IP10 are now available or in development, which can enable assessment of these biomarkers in primary health care and resource-limited settings. CRP, IL6, and IP10 could support clinical decision making, particularly the need of referral or admission, by identifying high-risk COVID-19 patients in an outpatient setting or emergency service. They could also inform the need of close follow-up of patients discharged home. Such risk stratification strategies could facilitate timely intervention and treatment, help reduce disease progression and risk of sequelae, while also optimizing resource allocation. To avoid unnecessary hospitalizations, cut-off values resulting in low specificity could be reviewed or combined with other risk factors to refine such risk stratification strategies.
Our results also suggest that some biomarkers, including suPAR, IL8, and IL1RA might have a better prognostic performance at identifying more severe COVID-19 in comparison to overall hospitalization, which included patients without oxygen requirement and no other truly severe manifestations. However, the frequency of more severe endpoints in our cohort was relatively low (only 5 patients required mechanical ventilation, 2 of whom died), limiting statistical power to draw strong conclusions. Indeed, we could not measure the association of biomarkers’ levels with the highest severity scores related to intubation and mortality, due to the low frequency of these events. In accordance, levels of sTREM1, which typically have been found to predict mortality in many life-threatening infections including COVID-19 (30–35), were not associated with hospitalization and severity in our study. Interestingly, lymphocyte levels in our study did not follow the expected trend with increasing severity, contrasting with most existing evidence (primarily from hospitalized patients), which identifies lymphopenia as a strong predictor of COVID-19 severity and mortality (36, 37). As lymphocyte levels typically decline over time as severity increases (38), lymphopenia may be a reliable late indicator of severe disease, but not an effective early predictor.
Of note, we examined biomarker kinetics from baseline to day 7 according to disease progression in a subset of participants with available biomarkers’ data at day 7, which has been largely unexplored. We observed a trend of increasing levels of ferritin and CRP in participants that required hospitalization within 28 days, regardless of their hospitalization status at day 7, compared to controls. Additionally, IL6 and IP10 showed a trend in faster normalization in participants discharged by day 7, compared to those still hospitalized. This secondary analysis was restricted to participants with available sample on day 7, in the context of challenging sample collection particularly in severe cases. While results may be impacted by the small sample size, these findings are relevant for monitoring disease progression and suggest that IL6 and IP10 may serve as timely indicators of recovery, warranting further investigation.
A main strength of our study is the use of a nested case-control design from a multicenter randomized clinical trial with consistent data collection and standardized outcome definitions and laboratory assays. Moreover, we compared a large panel of inflammatory, immune, and endothelial activation markers, including most of the key prognostic markers proposed in the literature, which allowed to draw strong conclusions on their early prognostic performance in mild-to-moderate COVID-19.
Our study has some limitations. First, the low incidence of mechanical ventilation and death in our study cohort limited our ability to assess the association between biomarkers and the most severe endpoints, including mortality risk. Second, the study was conducted during the first and second years of the COVID-19 pandemic and involved unvaccinated patients aged 50 or older, most of whom were immunocompetent. This limits the generalizability of our findings to the current population at highest risk of severe outcomes, mainly immunocompromised individuals with prior infections and full vaccination. Third, our nested case-control design did not involve matching to minimize confounding bias, given the highly homogeneous characteristics of the original cohort. Instead, we adjusted for relevant covariates in the statistical analysis. Finally, we did not evaluate the prognostic performance of biomarkers combinations or their integration with clinical severity indicators in risk prediction models.
In conclusion, higher levels of the biomarkers CRP, IL6, IP10, ferritin, IFNα, IL8, IL1RA, MCP1, and lower levels of RANTES measured within 7 days of symptoms onset were associated with increased risk of hospitalization due to COVID-19 progression. CRP and IL6 were the biomarkers with the highest discriminatory capacity for hospitalization, and severe COVID-19, respectively. These findings could guide management decisions in the context of new COVID-19 outbreaks to help guide triage and management decisions, including admission versus discharge and prioritization of early treatment, especially in those patients with risk factors or unvaccinated.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee at Hospital Germans Trials i Pujol (number PI 20-313). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AA: Conceptualization, Data curation, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. NB: Conceptualization, Data curation, Formal analysis, Investigation, Writing – review & editing. PM-M: Conceptualization, Investigation, Methodology, Writing – review & editing. DO: Formal analysis, Writing – review & editing. MC-M: Investigation, Writing – review & editing. CM-I: Investigation, Methodology, Writing – review & editing. GFR: Investigation, Methodology, Writing – review & editing. IB: Investigation, Methodology, Writing – review & editing. OM: Funding acquisition, Writing – review & editing. RA: Investigation, Methodology, Writing – review & editing. CD: Investigation, Methodology, Writing – review & editing, Funding acquisition, Conceptualization. QB: Conceptualization, Funding acquisition, Writing – review & editing. GM: Investigation, Methodology, Supervision, Writing – review & editing. BB: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The COnV-ert trial was sponsored by the Fight Infectious Diseases Foundation (Badalona, Spain) with funding from the pharmaceutical company, Grifols Worldwide Operations (Dublin, Ireland), and the Crowdfunding campaign, YoMeCorono. The study received support from the Hospital Universitari Germans Trias i Pujol, the Fundació Privada Daniel Bravo Andreu, and Banc de Sang i Teixits de Catalunya. ISGlobal acknowledges support from the grant CEX2023-0001290-S funded by MCIN/AEI/10.13039/501100011033, and support from the Generalitat de Catalunya through the CERCA Program. CM-I is supported by the Government of Mozambique and the Spanish Agency for International Development (AECID). NB is supported by an FPU predoctoral fellowship from the Spanish Ministry of Universities (FPU18/04260). BB is a Beatriu de Pinos postdoctoral fellow granted by the Government of Catalonia’s Secretariat for Universities and Research, and by Marie Sklodowska-Curie Actions COFUND Program (BP3, 801370). GM is supported by RYC 2020-029886-I/AEI/10.13039/501100011033, cofunded by European Social Fund (ESF). Funding bodies played no role in study design; collection, analysis or interpretation of the data; writing of the report, or in submission of this article for publication.
Acknowledgments
We thank all the participants who volunteered for the COnV-ert trial; all the investigational site members involved in the trial (listed in the Supplementary Data Sheet S1) and the personnel from the Fight Aids and Infectious Diseases Foundation, Germans Trias i Pujol University Hospital, and Barcelona Institute for Global Health for their support and contributions.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1501872/full#supplementary-material
References
1. Cascella M, Rajnik M, Aleem A, Dulebohn SC, Di Napoli R. Features, Evaluation, and Treatment of Coronavirus (COVID-19). Treasure Island (FL: StatPearls (2024). Available at: https://www.ncbi.nlm.nih.gov/books/NBK554776/.
2. COVID-ICU Group on behalf of the REVA Network and the COVID-ICU Investigators. Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: a prospective cohort study. Intensive Care Med. (2021) 47:60–73. doi: 10.1007/s00134-020-06294-x
3. Li J, Huang DQ, Zou B, Yang H, Hui WZ, Rui F, et al. Epidemiology of COVID-19: A systematic review and meta-analysis of clinical characteristics, risk factors, and outcomes. J Med Virol. (2021) 93:1449–58. doi: 10.1002/jmv.26424
4. Chaudhary R, Garg J, Houghton DE, Murad MH, Kondur A, Chaudhary R, et al. Thromboinflammatory biomarkers in COVID-19: systematic review and meta-analysis of 17,052 patients. Mayo Clinic Proceedings: Innovations Qual Outcomes. (2021) 5:388–402. doi: 10.1016/j.mayocpiqo.2021.01.009
5. Iwamura APD, Tavares Da Silva MR, Hümmelgen AL, Soeiro Pereira PV, Falcai A, Grumach AS, et al. Immunity and inflammatory biomarkers in COVID-19: A systematic review. Rev Med Virol. (2021) 31(4):e2199. doi: 10.1002/rmv.v31.4
6. Mohebbi A, Haybar H, Nakhaei Moghaddam F, Rasti Z, Vahid MA, Saki N. Biomarkers of endothelial dysfunction are associated with poor outcome in COVID-19 patients: A systematic review and meta-analysis. Rev Med Virol. (2023) 33(4):e2442. doi: 10.1002/rmv.v33.4
7. Lampsas S, Tsaplaris P, Pantelidis P, Oikonomou E, Marinos G, Charalambous G, et al. The role of endothelial related circulating biomarkers in COVID-19. A systematic review and meta-analysis. Curr Medicinal Chem. (2022) 29:3790–805. doi: 10.2174/0929867328666211026124033
8. Semiz S. COVID19 biomarkers: What did we learn from systematic reviews? Front Cell Infection Microbiol. (2022) 12. doi: 10.3389/fcimb.2022.1038908
9. De Bruin S, Bos LD, Van Roon MA, Tuip-De Boer AM, Schuurman AR, Koel-Simmelinck MJA, et al. Clinical features and prognostic factors in Covid-19: A prospective cohort study. EBioMedicine. (2021) 67:103378. doi: 10.1016/j.ebiom.2021.103378
10. Enocsson H, Idoff C, Gustafsson A, Govender M, Hopkins F, Larsson M, et al. Soluble urokinase plasminogen activator receptor (suPAR) independently predicts severity and length of hospitalisation in patients with COVID-19. Front Med. (2021) 8. doi: 10.3389/fmed.2021.791716
11. Da Silva-Neto PV, De Carvalho JCS, Pimentel VE, Pérez MM, Toro DM, Fraga-Silva TFC, et al. sTREM-1 predicts disease severity and mortality in COVID-19 patients: involvement of peripheral blood leukocytes and MMP-8 activity. Viruses. (2021) 13:2521. doi: 10.3390/v13122521
12. Pons MJ, Ymaña B, Mayanga-Herrera A, Sáenz Y, Alvarez-Erviti L, Tapia-Rojas S, et al. Cytokine profiles associated with worse prognosis in a hospitalized Peruvian COVID-19 cohort. Front Immunol. (2021) 12. doi: 10.3389/fimmu.2021.700921
13. Del Valle DM, Kim-Schulze S, Huang H-H, Beckmann ND, Nirenberg S, Wang B, et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat Med. (2020) 26:1636–43. doi: 10.1038/s41591-020-1051-9
14. Arnold DT, Attwood M, Barratt S, Morley A, Elvers KT, McKernon J, et al. Predicting outcomes of COVID-19 from admission biomarkers: a prospective UK cohort study. Emergency Med J. (2021) 38:543–8. doi: 10.1136/emermed-2020-210380
15. Van Singer M, Brahier T, Ngai M, Wright J, Weckman AM, Erice C, et al. COVID-19 risk stratification algorithms based on sTREM-1 and IL-6 in emergency department. J Allergy Clin Immunol. (2021) 147:99–106.e4. doi: 10.1016/j.jaci.2020.10.001
16. Chandna A, Mahajan R, Gautam P, Mwandigha L, Gunasekaran K, Bhusan D, et al. Facilitating safe discharge through predicting disease progression in moderate COVID-19: a prospective cohort study to develop and validate a clinical prediction model in resource-limited settings. Clin Infect Dis. (2022) 75:e368–e79. doi: 10.1093/cid/ciac224
17. Alemany A, Millat-Martinez P, Corbacho-Monné M, Malchair P, Ouchi D, Ruiz-Comellas A, et al. High-titre methylene blue-treated convalescent plasma as an early treatment for outpatients with COVID-19: a randomised, placebo-controlled trial. Lancet Respir Med. (2022) 10:278–88. doi: 10.1016/S2213-2600(21)00545-2
18. Characterisation WWGotC, Covid-infection Mo. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect Dis. (2020) 20:e192–e7. doi: 10.1016/S1473-3099(20)30483-7
19. Aguilar R, Campo JJ, Chicuecue S, Cisteró P, Català A, Luis L, et al. Changing plasma cytokine, chemokine and growth factor profiles upon differing malaria transmission intensities. Malaria J. (2019) 18:406. doi: 10.1186/s12936-019-3038-x
20. Ballart C, Torrico MC, Vidal G, Torrico F, Lozano D, Gállego M, et al. Clinical and immunological characteristics of tegumentary leishmaniasis cases in Bolivia. PloS Negl Trop Diseases. (2021) 15:e0009223. doi: 10.1371/journal.pntd.0009223
21. Natama HM, Moncunill G, Rovira-Vallbona E, Sanz H, Sorgho H, Aguilar R, et al. Modulation of innate immune responses at birth by prenatal malaria exposure and association with malaria risk during the first year of life. BMC Med. (2018) 16:198. doi: 10.1186/s12916-018-1187-3
22. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. (1988) 44:837–45. doi: 10.2307/2531595
23. Bannaga AS, Tabuso M, Farrugia A, Chandrapalan S, Somal K, Lim VK, et al. C-reactive protein and albumin association with mortality of hospitalised SARS-CoV-2 patients: A tertiary hospital experience. Clin Med. (2020) 20:463–7. doi: 10.7861/clinmed.2020-0424
24. Avihai B, Sundel EP, Lee E, Greenberg PJ, Cook BP, Altomare NJ, et al. CRP monitoring in early hospitalization: implications for predicting outcomes in patients with COVID-19. Pathogens. (2023) 12:1315. doi: 10.3390/pathogens12111315
25. Landry A, Docherty P, Ouellette S, Cartier LJ. Causes and outcomes of markedly elevated C-reactive protein levels. Can Fam Physician. (2017) 63:e316–e23.
26. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
27. Papan C, Argentiero A, Adams O, Porwoll M, Hakim U, Farinelli E, et al. Association of viral load with TRAIL, IP-10, CRP biomarker signature and disease severity in children with respiratory tract infection or fever without source: A prospective, multicentre cohort study. J Med Virol. (2023) 95:e28113. doi: 10.1002/jmv.28113
28. Pastor L, Casellas A, Carrillo J, Alonso S, Parker E, Fuente-Soro L, et al. IP-10 levels as an accurate screening tool to detect acute HIV infection in resource-limited settings. Sci Rep. (2017) 7:8104. doi: 10.1038/s41598-017-08218-0
29. Pastor L, Casellas A, Rupérez M, Carrillo J, Maculuve S, Jairoce C, et al. Interferon-γ–inducible protein 10 (IP-10) as a screening tool to optimize human immunodeficiency virus RNA monitoring in resource-limited settings. Clin Infect Dis. (2017) 65:1670–5. doi: 10.1093/cid/cix600
30. Erdman LK, Dhabangi A, Musoke C, Conroy AL, Hawkes M, Higgins S, et al. Combinations of host biomarkers predict mortality among Ugandan children with severe malaria: A retrospective case-control study. PloS One. (2011) 6:e17440. doi: 10.1371/journal.pone.0017440
31. Richard-Greenblatt M, Boillat-Blanco N, Zhong K, Mbarack Z, Samaka J, Mlaganile T, et al. Prognostic accuracy of soluble triggering receptor expressed on myeloid cells (sTREM-1)-based algorithms in febrile adults presenting to Tanzanian outpatient clinics. Clin Infect Dis. (2020) 70:1304–12. doi: 10.1093/cid/ciz419
32. Gibot S. Clinical review: role of triggering receptor expressed on myeloid cells-1 during sepsis. Crit Care. (2005) 9:485–9. doi: 10.1186/cc3732
33. Wright SW, Lovelace-Macon L, Hantrakun V, Rudd KE, Teparrukkul P, Kosamo S, et al. sTREM-1 predicts mortality in hospitalized patients with infection in a tropical, middle-income country. BMC Med. (2020) 18:159. doi: 10.1186/s12916-020-01627-5
34. de Nooijer A, Grondman I, Lambden S, Kooistra EJ, Janssen NAF, Kox M, et al. Increased sTREM-1 plasma concentrations are associated with poor clinical outcomes in patients with COVID-19. Bioscience Rep. (2021) 41:BSR20210940. doi: 10.1042/BSR20210940
35. Balanza N, Erice C, Ngai M, McDonald CR, Weckman AM, Wright J, et al. Prognostic accuracy of biomarkers of immune and endothelial activation in Mozambican children hospitalized with pneumonia. PloS Glob Public Health. (2023) 3:e0001553. doi: 10.1371/journal.pgph.0001553
36. Lai K-L, Hu F-C, Wen F-Y, Chen J-J. Lymphocyte count is a universal predictor of health outcomes in COVID-19 patients before mass vaccination: A meta-analytical study. J Global Health. (2022) 12:05041. doi: 10.7189/jogh.12.05041
37. Huang I, Pranata R. Lymphopenia in severe coronavirus disease-2019 (COVID-19): systematic review and meta-analysis. J Intensive Care. (2020) 8:36. doi: 10.1186/s40560-020-00453-4
Keywords: biomarkers, host response, COVID-19, SARS-CoV-2, outpatients
Citation: Alemany A, Balanza N, Millat-Martinez P, Ouchi D, Corbacho-Monné M, Morales-Indiano C, Fernández Rivas G, Blanco I, Mitjà O, Aguilar R, Dobaño C, Bassat Q, Moncunill G, Baro B and COnV-ert BMK STUDY GROUP (2024) Prognostic performance of early immune and endothelial activation markers in mild-to-moderate COVID-19 outpatients: a nested case-control study. Front. Immunol. 15:1501872. doi: 10.3389/fimmu.2024.1501872
Received: 25 September 2024; Accepted: 06 November 2024;
Published: 27 November 2024.
Edited by:
Qian Chen, Boston Children’s Hospital and Harvard Medical School, United StatesReviewed by:
Kautilya Kumar K. Jena, Boston Children’s Hospital and Harvard Medical School, United StatesYing Luo, Shenzhen Children’s Hospital, China
Copyright © 2024 Alemany, Balanza, Millat-Martinez, Ouchi, Corbacho-Monné, Morales-Indiano, Fernández Rivas, Blanco, Mitjà, Aguilar, Dobaño, Bassat, Moncunill, Baro and COnV-ert BMK STUDY GROUP. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bàrbara Baro, YmFyYmFyYS5iYXJvQGlzZ2xvYmFsLm9yZw==