
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Immunol. , 13 November 2024
Sec. Primary Immunodeficiencies
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1472957
 Renan Cesar Sbruzzi1,2
Renan Cesar Sbruzzi1,2 Mayara Jorgens Prado1Bibiana Fam1,2
Mayara Jorgens Prado1Bibiana Fam1,2 Helena Ashton Prolla1,3
Helena Ashton Prolla1,3 Alessandra Hellwig4
Alessandra Hellwig4 Grazielle Motta Rodrigues4Fernanda de-Paris4Mariana Jobim5Osvaldo Artigalás6,7Yoann Seeleuthner8
Grazielle Motta Rodrigues4Fernanda de-Paris4Mariana Jobim5Osvaldo Artigalás6,7Yoann Seeleuthner8 Jean-Laurent Casanova8,9,10,11
Jean-Laurent Casanova8,9,10,11 Jacinta Bustamante8,9,12
Jacinta Bustamante8,9,12 Fernanda Sales Luiz Vianna1,2,13,14,15*
Fernanda Sales Luiz Vianna1,2,13,14,15*Inborn errors of immunity (IEI) encompass a broad range of disorders with heterogeneous clinical presentations, often leading to challenges in early diagnosis. This study presents a case of a Brazilian patient with a T-B+NK- severe combined immunodeficiency (SCID) diagnosed at the age of 6 months when was admitted to the hospital due to multiple infectious diseases. Despite undergoing hematopoietic stem cell transplantation (HSCT), the patient had recurrent infections, requiring constant hospital care, including IgG infusions and several antibiotic treatments for the following months. One year after HSCT, presenting mixed chimerism, the patient tested positive for SARS-CoV-2 in nasopharyngeal, duodenum, and intestine samples, with persistent positive tests over a six-month period. Whole exome sequencing identified a private homozygous missense variant (c.1202T>C; p.Leu401Pro) in the Janus Kinase 3 (JAK3) gene. This substitution is located in a highly conserved position, and different bioinformatic variant effect predictors classified the variant as damaging. In silico structural analysis suggested that the variant led to increased structural instability, disrupting the hydrophobic interactions within the SH2 domain, thereby influencing the neighboring residues and potentially altering the interaction between JAK3 and gamma chain (γc) intracellular receptors. This study provides evidence for the novel pathogenicity classification of the variant and highlights the importance of the JAK3 and SH2 domain modulating protein function and their contribution to the SCID pathogenesis.
Severe combined immunodeficiencies (SCIDs) are a group of Inborn Errors of Immunity (IEI) characterized by abnormalities in development and function of the adaptive immune system. Patients with SCID present thymopoiesis defects that results in both numeric and functional impairment of T cells and, depending on the genetic variants responsible for the condition, defects in B and natural killer (NK) cells might also be found (1). The T-B+NK- phenotype SCID has been associated with cytokine signaling abnormalities, caused by either deficiency in the gamma chain (γc) subunit, encoded by the interleukin 2 receptor subunit gamma (IL2RG), or Janus Kinase 3 (JAK3) deficiency (1, 2). SCID patients generally present no symptoms on their first days of life, but soon they develop severe opportunistic infections and present higher susceptibility to attenuated-pathogen vaccine-associated infections (1). Unless proper treatment is early administered, usually immunoglobulin reposition and hematopoietic stem cell transplantation (HSCT), affected individuals have a significant risk of mortality within the first year of life (2, 3). SCID patients as well as patients with other IEIs, are susceptible to severe COVID-19 (4) and to persistent SARS-CoV-2 infection (5). The delayed viral clearance in those patients leads to prolonged periods of viral replication and chronic infection, increasing the risk of viral transmission and prompting medical care for longer periods (5, 6). In addition to patient management challenges, prolonged SARS-CoV-2 infection may also present an epidemiological risk, as the immune status of the host can create different selective pressures that may allow the emergence of new variants of concern (7). In this study, we report a patient with a T-B+NK- SCID associated with several pulmonary infections, BCG-itis and a six-months long SARS-CoV-2 infection, who presented a new homozygous missense variant in JAK3 gene.
A 6-month-old Brazilian boy of a first-cousin consanguineous couple, with no gestational complications or history of immunodeficiency, was admitted at the hospital’s Intensive Care Unit (ICU) in March 2020, presenting sibilant breathing, severe respiratory dysfunction, and cyanosis (Figures 1A–C). As newborn screening for T and B cell deficiencies isn’t fully implemented in Brazil, the boy received all vaccines following the Brazilian National Calendar of Vaccination (8), including Bacillus Calmette-Guérin (BCG) at 4 months of age, which later caused BCG-itis. He was treated using rifampicin (18 mg/kg/day), isoniazid (14.5 mg/kg/day), and ethambutol (24 mg/kg/day) intermittently in the next following months. The chest X-Ray showed signs of bronchopneumopathy (Figure 1A) and Pneumocystis jirovecii, Pneumococcus and Bordetella were detected on bronchoalveolar aspirate. Pneumocystosis was treated with oral trimethoprim (TMP)- sulfamethoxazole (SMZ) (4 mg of TMP and 20 mg of SMZ/kg/day) for approximately two months, in addition of courses of fluconazole (6 mg/kg/day) and prednisolone (0.47 mg/kg/day) to manage and prevent other infections. Pneumococcus and Bordetella infections were managed with courses of amoxicillin (70 mg/kg/day) and azithromycin (10 mg/kg/day). First immunological screening found low immunoglobulin G (IgG <108 mg/dL, with reference values for this age around 203 mg/dL) and the absence of T cells (CD3/CD4 and CD4-/CD8-) as well as NK cells (CD53+/CD16+/CD3-), and low counts (0.1%) of T CD3 and CD3/CD8 cells. The patient also presented 99% of his lymphocyte population composed of CD19 and CD19/20 B cells. The immunophenotypic analysis allowed the classification of SCID as T-B+NK- phenotype and he was referred to HSCT. Molecular diagnosis for SCID was not performed at assistance care. Forty days after admission the patient received ICU discharge.
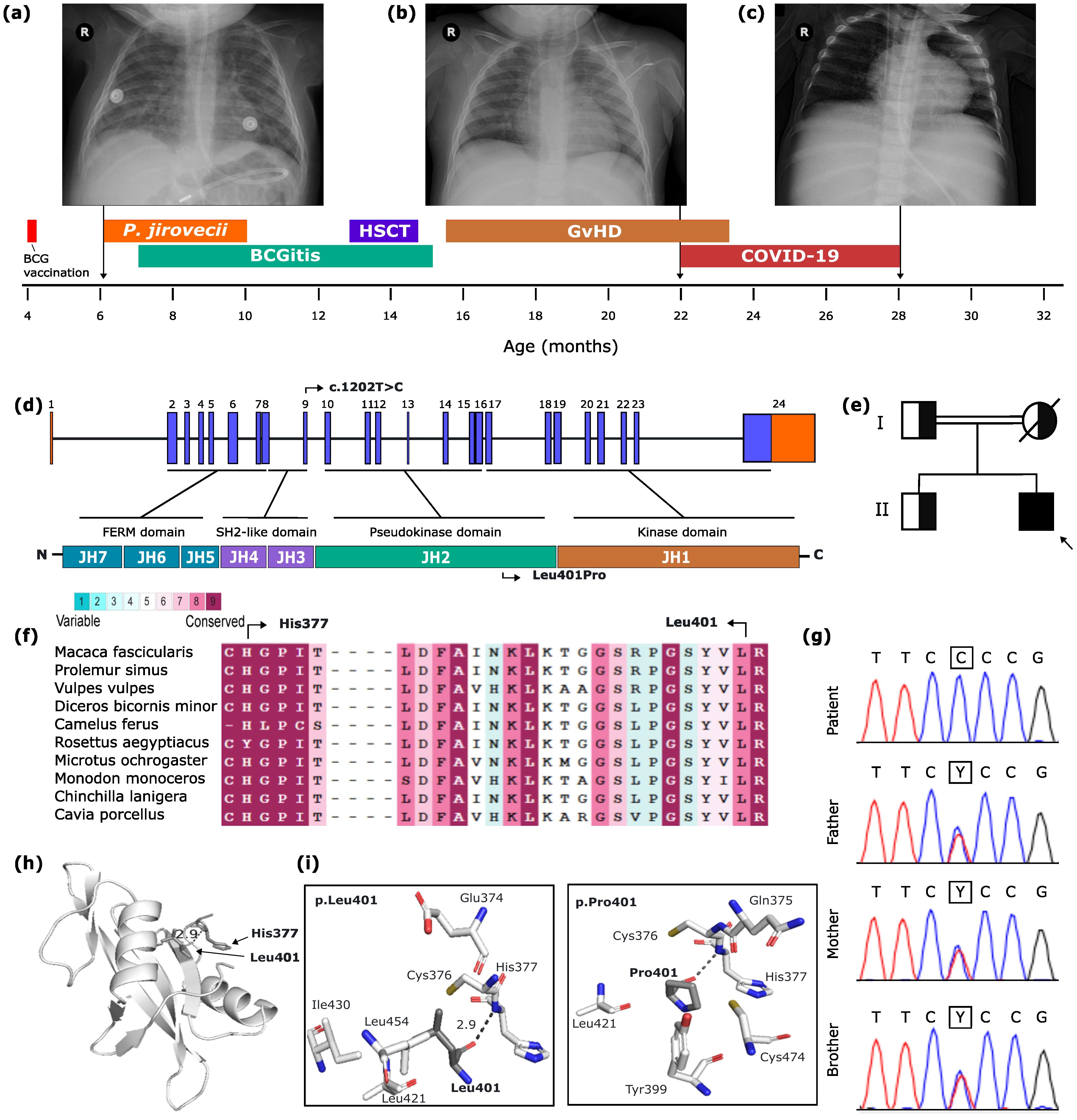
Figure 1. Brazilian patient with SCID due to JAK3 deficiency. SCID case report findings, patient’s timeline describing relevance events, and related X-ray findings. In (A) Lung hyperinflation signs. Peribronchovascular bundles, especially in the central lung areas, along with faint heterogeneous opacities, primarily in the lower parts of the left lung and upper parts of the right lung. (B) Mild infiltration in the medullary region of the left lung, with no other evidence of pleuropulmonary alteration. (C) Mild thickening of bronchial walls and apparent splenomegaly can be seen. (D) JAK3 gene and protein. JAK3 gene comprises 24 exons (23 coding) that code seven Janus kinase homology domains (JH1-JH7) highlighting JH3 and JH4 together constitute the SH2-like domain, and JH4 domains constitute the FERM domain. (E) Family pedigree. (F) Multisequence alignment colored according to conservation scores, highlighting p.His377 and p.Leu401. (G) Electropherogram showing the variant’s segregation pattern on the kindred (Y= C+T). (H) 3D structure of JAK3 SH2 domain. (I) 3D stick structure of residues under a distance of 4 angstroms of p.Leu401 (left) and p.Pro401 (right).
At 13 months old, conditioned HSCT was conducted using stem cells from his father (Table 1). The patient continued presenting hypogammaglobulinemia and was treated with periodic intravenous immunoglobulin infusions. One month after HSCT, the patient presented ulceration on BCG scar and fever, followed by erythematous skin rashes disseminated throughout the whole body. Soon after BCG-itis treatment, the patient was diagnosed with cutaneous manifestation of graft versus host disease (GvHD). As this was a case of steroid-refractory GvHD, the patient did not respond to treatment with methylprednisolone, basiliximab, needing the application of five mesenchymal cells infusion to halt disease progression (Figure 1B). One year after the HSCT, the patient had an ICU admission due to respiratory symptoms and radiological findings indicating extensive lung damage (Figure 1C). A PCR test was conducted and SARS-CoV-2 was detected. The patient suffered from an episode of bronchospasm, which was managed with noninvasive ventilation and salbutamol, and was discharged after 10 days. In the following months, the patient had constant hospital admissions related to both skin lesions due to GvHD and opportunistic infections, such as urinary tract infection by Enterobacter kobei, catheter-associated infection by E. faecium, and infection by Clostridium difficile. The patient was again tested for SARS-CoV-2 in November and December 2021, presenting persistently positive results and viable viral particles throughout this period, as well as increased viral load over time (9). In addition, he presented persistence of respiratory and gastrointestinal symptoms. SARS-CoV-2 was tested and detected in duodenum and intestine, but not in stomach samples. Six months after the first positive result for SARS-CoV-2 infection, the patient obtained his first negative test result for SARS-CoV-2 from nasopharyngeal samples. Currently, the patient is undergoing regular follow-up and, despite HSCT in 2020 and of the recovery of T and NK cell populations, he still presents mixed donor chimerism, close to 40% (Table 2).
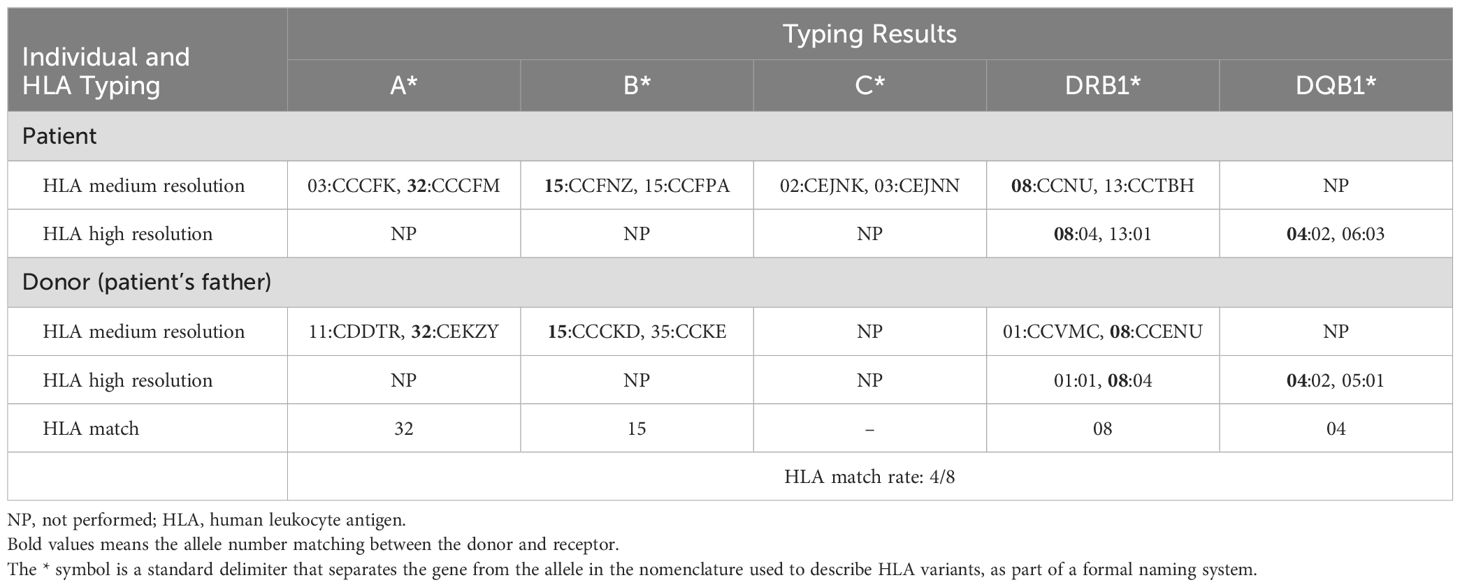
Table 1. Summary of HLA typing results using different resolutions methods.
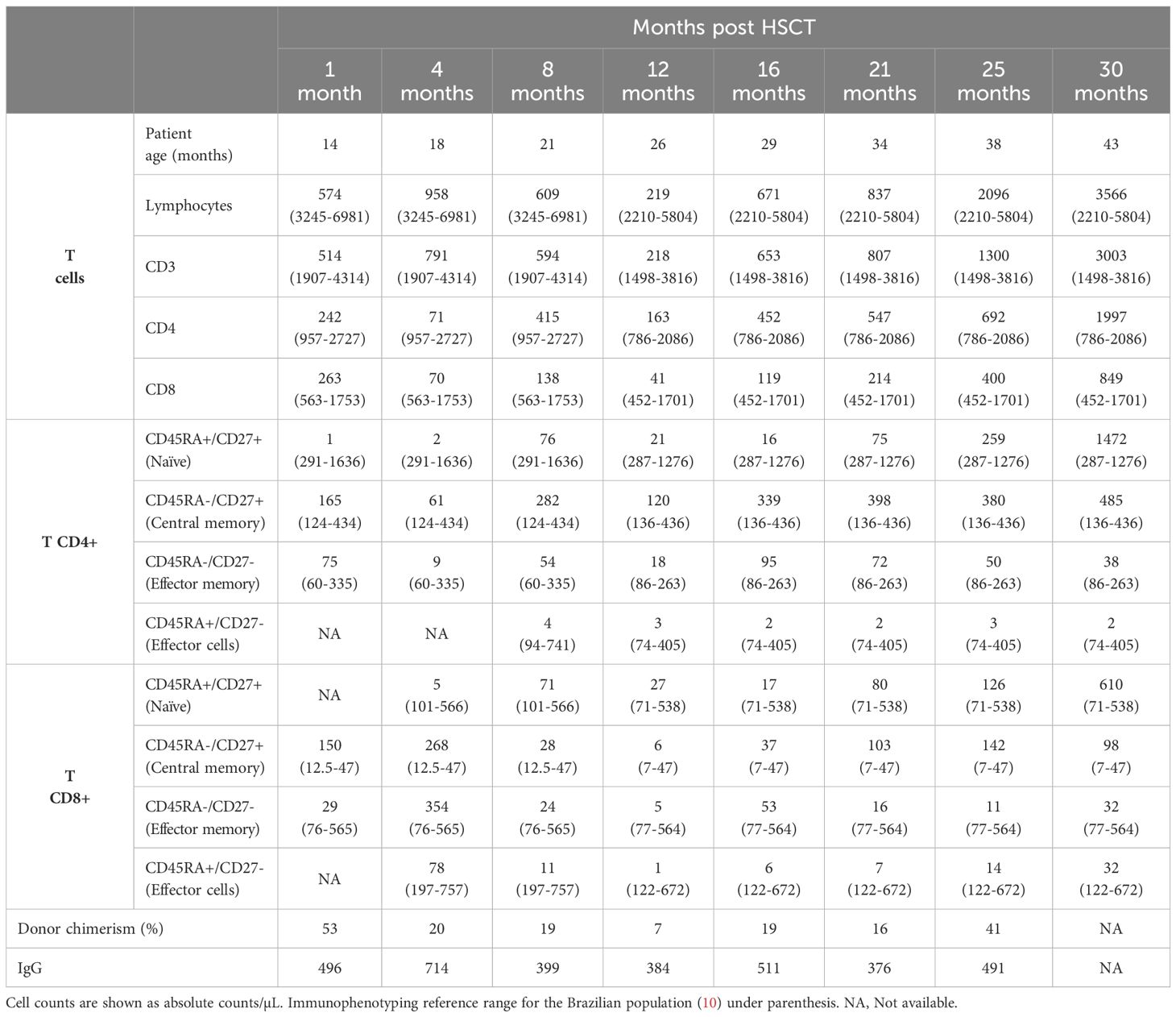
Table 2. Patient’s immunophenotyping findings post HSCT.
Molecular investigation was performed through whole exome sequencing (WES) using DNA isolated from the patient’ whole blood, taken before HSCT. WES revealed a high homozygosity rate (3.8%), consistent with the parental consanguinity. Homozygous nonsense, missense, indel or splice site variants were prioritized. We further filtered variants with global low frequency (MAF <0.01) in public databases, and with a combined annotation dependent depletion (CADD) score higher than the gene’s mutational significance cutoff (MSC) (11), particularly in IL2RG and JAK3 genes which are involved in T-B+NK- SCID (1). A novel homozygous missense variant was identified in the JAK3 (NM_000215.4) gene, c.1202T>C, leading to the p.Leu401Pro substitution (Figure 1D). This private variant is classified as a variant of unknown significance (VUS) by the American College of Medical Genetics (ACMG) criteria (12). Sanger sequencing confirmed the variant to be in homozygosity in the patient, and in heterozygosity in his parents and brother (Figures 1E, G). The variant obtained a damaging score across most of the tested prediction tools (including CADD, AlphaMissense, SIFT, PolyPhen2, MAPP, MutationTaster, and MutPred2). The p.Leu401 residue, as analyzed with the ConSurf server (13), is at a high conservation level across different species, suggesting the functional importance of the residue position (Figure 1F). The p.Leu401 residue is located within the Src homology 2 (SH2) domain, an essential region for the protein signalization through interaction with the γc intracellular receptors. Furthermore, this residue forms a hydrogen bridge with a highly conserved residue, p.His377, located at the terminus of the FERM domain (Figures 1H, I). In addition, the novel variant led to increased structural instability, evidenced by chance in free energy (ΔΔG 0.15), as analyzed with STRUM (14) and cause a disruption in the hydrophobic interactions within the SH2 domain, thereby influencing the neighboring residues (Figures 1H, I).
In this study we describe a six-months-old Brazilian patient carrying a private JAK3 variant c.1202T>C, leading to the p.Leu401Pro substitution, in homozygosity causing T-B+NK- phenotype of SCID who suffered from a prolonged SARS-CoV-2 infection. Brazil is a continental dimension country with economic constraints, making newborn screening nationwide implementation challenging. Studies have demonstrated the newborn screening’s (NBS) feasibility and benefits of this strategy in Brazil (16, 17), and they were fundamental to drive the approval of this strategy in Brazil. However, NBS still remains in an implementation stage nationwide, though a few states are currently testing all newborns TRECs and KRECs (15, 18). Thus, SCID was belatedly diagnosed and, as BCG vaccination is mandatory in Brazil and recommended at birth, the patient received the vaccine at four months of age, which led to BCG-itis requiring treatment. One year after the patient’s HSCT, SARS-CoV-2 was detected in nasopharyngeal samples, in addition to duodenum and intestine samples, with persistently positive results throughout a period of six months. Despite the overall low donor chimerism following HSCT, the non-critical SARS-CoV-2 infection, along with successful management of various bacterial infections, can be attributed to the residual functional JAK3 activity derived from the transplanted cells of the patient’s father. The patient’s compromised immune response, however, was not effective enough to promote timely viral clearance, leading to the 6-month-long SARS-CoV-2 infection as well as several ICU admissions due to other bacterial infections. The patient was infected with the Gamma lineage, and samples collected and tested during the hospitalization presented the same lineage (9), strongly suggesting that the persistently positive results in SARS-CoV-2 detection tests was due to chronic persistent infection rather than any reinfection events.
JAK3 is a member of the JAK family of tyrosine kinase proteins involved in cytokine receptor-mediated intracellular signal transduction through the JAK/STAT signaling pathway. Due to the essential role of JAK3- γc receptor interaction and signaling, functional variants in both JAK3 and IL2RG genes can lead to autosomal recessive and X-linked recessive T-B+NK- SCID, respectively, as result of the impairment on signalization of cytokines involved in the development of B cells (IL-2, IL-4 and IL-9) and differentiation and activation of T and NK cells (IL-7, IL-15 and IL-21) (2, 19, 20). Protein structure and mutation modeling of JAK3 indicated that the p.Leu401Pro substitution increases structural instability of the protein region, changing both the distances and the pattern of interaction with neighbor residues. The Leu401 residue is located in a highly conserved position within the SH2 domain on different species, a region that, together with the four-point-one, ezrin, radixin, moesin (FERM) domain, form a single receptor binding module known to mediate JAK association with different cytokine receptors containing the common γc. The JAK interaction with common γc receptors is mediated by a membrane-proximal site in the intracellular portion of the receptor, a region composed by the proline-rich “Box1” and the downstream hydrophobic “Box2” regions, separated by an “interbox” segment (19, 21). Substitutions in residues of both the receptor binding module and in the Box1 or Box2 regions of the intracellular portion of the γc receptor, may disrupt the JAK interaction with the cytokine receptor γc and therefore impair the cytokine signaling pathway, leading to SCID. One study evaluating EBV-transformed B (EBV-B) cells from a SCID patient observed that the p.Tyr100Cys substitution, located in the hydrophobic core of JAK3 FERM domain, was found to disrupt the protein’s interaction with γc receptor chain, as tested by co-immunoprecipitation, and to cause constitutive JAK3 phosphorylation (22).
Other missense variants in JAK3 were reported affecting the same domain, such as p.Arg402His and p.Arg403Cys variants, associated with SCID (23, 24). A different study identified the p.Phe292Val variant, also in the FERM domain, that leads to an impairment of JAK3 expression in the patient’s EBV-B cells and causes SCID in an Italian patient (25). Taken together, this evidence indicates the importance of the amino terminal FERM-SH2 region in the JAK3 interaction with the γc receptor and point towards the pathogenic effect of different variants found in this region causing SCID. We therefore hypothesize that the variant identified in this current report patient (p.Leu401Pro) leads to greater flexibility of the SH2 domain, potentially compromising the interaction between JAK3 FERM-SH2 region and the intracellular portion of common γc receptors, finally leading to the observed SCID phenotype. Although we were unable to perform in vitro functional validation of the variant, we provided compelling evidence for the reclassification of pathogenicity of the identified variant using up-to-date ACMG-AMP criteria for germline sequence variant classification (12). Two lines of pathogenic supporting evidence (PP3+ PP4+) and one line of pathogenic moderate evidence (PM2_sup), are related to the computational analysis pointing towards a deleterious effect of the variant, the fact that the patient’s phenotype is highly specific to the JAK3 gene, and due to the absence of the identified variant in population databases, respectively. The possible fourth evidence for pathogenicity classification, also moderate, refers to PM1_sup (non-truncating non-synonymous variant located in a mutational hot spot and/or critical and well-established functional domain), as the relevance of FERM and SH2 domains to JAK3 interaction with the intracellular tail of the γc receptors and hence downstream pathway signaling was already evidenced in previous studies. Other limitations in our study include the absence of evaluation in terms of JAK3 expression or STAT5 phosphorylation data before and after the HSCT, as the hospital does not perform such analysis in health care assistance. We only used already stored samples for this report.
This report described a novel JAK3 missense variant (c.1202T>C) causing p.Leu401Pro substitution in the protein’s SH2 domain leading to T-B+NK- SCID in a six-months-old boy, who suffered from different infectious diseases, including BCG-itis, P. jirovecii pneumonia, and a prolonged SARS-CoV-2 infection, lasting for six months. This study highlights the critical importance of the implementation of newborn screening programs in order to detect SCID as well as other T and B cell deficiencies, especially in children from families with no history of immunodeficiency, avoiding the inoculation of live-attenuated vaccines, in particular in the numerous countries where vaccines like BCG are mandatory in infancy. The early detection of the disease through newborn screening also prompts the timely HSCT deployment before infections onset. In addition, performing SCID molecular diagnosis and identifying the causal genetic variant can drive donor selection strategies, factors that ultimately improve overall survival and prognosis after HSCT, besides to allow better characterization of causal mutations and genes in IEIs phenotypes and aiding the understanding of the function of non-well functionally characterized protein domains. This study provided evidence for the reclassification of pathogenicity for the novel variant identified, currently a variant of unknown significance by the ACMG criteria. Further investigations are required to better understand the molecular mechanisms of the interaction between the FERM-SH2 region of JAK3 protein with cytokine receptor’s γc, as well as the impact of the p.Leu401Pro and other similar substitutions on its function, receptor binding, and relation to SCID pathogenesis.
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author/s.
The studies involving humans were approved by Hospital de Clínicas de Porto Alegre Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin. Written informed consent was obtained from the individual(s), and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article. Written informed consent was obtained from the participant/patient(s) for the publication of this case report.
RS: Writing – review & editing, Writing – original draft, Visualization, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. MP: Writing – review & editing, Writing – original draft, Visualization, Investigation, Formal analysis, Data curation, Conceptualization. BF: Writing – review & editing, Writing – original draft, Formal analysis, Data curation. HP: Writing – review & editing, Writing – original draft, Visualization, Investigation. AH: Investigation, Writing – review & editing, Writing – original draft. GR: Investigation, Writing – review & editing, Writing – original draft. Fd: Investigation, Writing – review & editing, Writing – original draft. MJ: Investigation, Writing – review & editing, Writing – original draft. OA: Writing – review & editing, Writing – original draft, Formal analysis, Conceptualization. YS: Visualization, Formal analysis, Writing – review & editing, Writing – original draft. JC: Investigation, Writing – review & editing, Supervision. JB: Writing – review & editing, Writing – original draft, Supervision, Methodology, Conceptualization. FV: Writing – review & editing, Writing – original draft, Visualization, Supervision, Project administration, Methodology, Investigation, Funding acquisition, Conceptualization.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study received funding from Financiamento e Incentivo à Pesquisa (FIPE/HCPA), Hospital de Clı́nicas de Porto Alegre (grant: 2022-0378), and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001. F.S.L.V. is the recipient of a CNPq scholarship 312960/2021-2, and R.C.S is the recipient of a CNPq scholarship 937823/2024-00.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Aranda CS, Gouveia-Pereira MP, Da Silva CJM, Rizzo MCFV, Ishizuka E, De Oliveira EB, et al. Severe combined immunodeficiency diagnosis and genetic defects. Immunol Rev. (2024) 322:138–47. doi: 10.1111/imr.13310
2. Casanova J-L, Holland SM, Notarangelo LD. Inborn errors of human JAKs and STATs. Immunity. (2012) 36:515–28. doi: 10.1016/j.immuni.2012.03.016
3. Rivers L, Gaspar HB. Severe combined immunodeficiency: Recent developments and guidance on clinical management. Arch Dis Child. (2015) 100:667–72. doi: 10.1136/archdischild-2014-306425
4. Meyts I, Bucciol G, Quinti I, Neven B, Fischer A, Seoane E, et al. Coronavirus disease 2019 in patients with inborn errors of immunity: An international study. J Allergy Clin Immunol. (2021) 147:520–31. doi: 10.1016/j.jaci.2020.09.010
5. Avanzato VA, Matson MJ, Seifert SN, Pryce R, Williamson BN, Anzick SL, et al. Case study: prolonged infectious SARS-CoV-2 shedding from an asymptomatic immunocompromised individual with cancer. Cell. (2020) 183:1901–1912.e9. doi: 10.1016/j.cell.2020.10.049
6. Dolan SA, Mulcahy Levy J, Moss A, Pearce K, Butler M, Jung S, et al. SARS-CoV-2 persistence in immunocompromised children. Pediatr Blood Cancer. (2021) 68:e29277. doi: 10.1002/pbc.29277
7. Hettle D, Hutchings S, Muir P, Moran E. Persistent SARS-CoV-2 infection in immunocompromised patients facilitates rapid viral evolution: Retrospective cohort study and literature review. Clin Infect Pract. (2022) 16:100210. doi: 10.1016/j.clinpr.2022.100210
8. BRASIL. Programa Nacional de Imunizações: Calendário Nacional de Vacinação/2020/PNI/MS (2020). Brasília: Ministério da Saúde. Available online at: https://www.gov.br/saude/pt-br/vacinacao/calendario-tecnico/calendario-tecnico-nacional-de-vacinacao-da-crianca (Accessed June 05, 2024).
9. Filippi M, Ribeiro Amorim M, Soares Da Silva M, Schons Gularte J, Demoliner M, Girardi V, et al. Prolonged SARS-CoV-2 infection and intra-patient viral evolution in an immunodeficient child. Pediatr Infect Dis J. (2023) 42:212–7. doi: 10.1097/INF.0000000000003782
10. Moraes-Pinto MID, Ono E, Santos-Valente EC, Almeida LC, Andrade PRD, Dinelli MIS, et al. Lymphocyte subsets in human immunodeficiency virus-unexposed Brazilian individuals from birth to adulthood. Mem Inst Oswaldo Cruz. (2014) 109:989–98. doi: 10.1590/0074-0276140182
11. Itan Y, Shang L, Boisson B, Ciancanelli MJ, Markle JG, Martinez-Barricarte R, et al. The mutation significance cutoff: gene-level thresholds for variant predictions. Nat Methods. (2016) 13:109–10. doi: 10.1038/nmeth.3739
12. Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. (2015) 17:405–24. doi: 10.1038/gim.2015.30
13. Ashkenazy H, Abadi S, Martz E, Chay O, Mayrose I, Pupko T, et al. ConSurf 2016: an improved methodology to estimate and visualize evolutionary conservation in macromolecules. Nucleic Acids Res. (2016) 44:W344–50. doi: 10.1093/nar/gkw408
14. Quan L, Lv Q, Zhang Y. STRUM: structure-based prediction of protein stability changes upon single-point mutation. Bioinformatics. (2016) 32:2936–46. doi: 10.1093/bioinformatics/btw361
15. Chong-Neto HJ, Radwan N, Condino-Neto A, Rosário Filho NA, Ortega-Martell JA, El-Sayed ZA. Newborn screening for inborn errors of immunity: The status worldwide. World Allergy Organ J. (2024) 17:100920. doi: 10.1016/j.waojou.2024.100920
16. Kanegae MPP, Barreiros LA, Mazzucchelli JTL, Hadachi SM, De Figueiredo Ferreira Guilhoto LM, Acquesta AL, et al. Neonatal screening for severe combined immunodeficiency in Brazil. Jornal Pediatria. (2016) 92:374–80. doi: 10.1016/j.jped.2015.10.006
17. Kanegae MPP, Barreiros LA, Sousa JL, Brito MAS, Oliveira Junior EBD, Soares LP, et al. Triagem neonatal de imunodeficiências graves combinadas por meio de TRECs e KRECs: segundo estudo piloto no brasil. Rev paul Pediatr. (2017) 35:25–32. doi: 10.1590/1984-0462/;2017;35;1;00013
18. Meehan CA, Bonfim C, Dasso JF, Costa-Carvalho BT, Condino-Neto A, Walter JE. IN TIME: Importância e implicações globais da triagem neonatal para a imunodeficiência grave combinada. Rev paul Pediatr. (2018) 36:388–97. doi: 10.1590/1984-0462/;2018;36;4;00020
19. Hu X, li J, Fu M, Zhao X, Wang W. The JAK/STAT signaling pathway: from bench to clinic. Signal Transduct Target Ther. (2021) 6:402. doi: 10.1038/s41392-021-00791-1
20. Notarangelo LD, Giliani S, Mella P, Schumacher RF, Mazza C, Savoldi G, et al. Combined immunodeficiencies due to defects in signal transduction: defects of the γc-JAK3 signaling pathway as a model. Immunobiology. (2000) 202:106–19. doi: 10.1016/S0171-2985(00)80058-3
21. Ferrão R, Lupardus PJ. The Janus kinase (JAK) FERM and SH2 domains: bringing specificity to JAK–receptor interactions. Front Endocrinol (Lausanne). (2017) 8:71. doi: 10.3389/fendo.2017.00071
22. Cacalano NA. Autosomal SCID caused by a point mutation in the N-terminus of Jak3: mapping of the Jak3-receptor interaction domain. EMBO J. (1999) 18:1549–58. doi: 10.1093/emboj/18.6.1549
23. Qamar F, Junejo S, Qureshi S, Seleman M, Bainter W, Massaad M, et al. A novel mutation in the JH4 domain of JAK3 causing severe combined immunodeficiency complicated by vertebral osteomyelitis. Clin Immunol. (2017) 183:198–200. doi: 10.1016/j.clim.2017.09.007
24. El Hawary R, Meshaal S, Mauracher AA, Opitz L, Abd Elaziz D, Lotfy S, et al. Whole-exome sequencing of T-B+ severe combined immunodeficiency in Egyptian infants, JAK3 predominance and novel variants. Clin Exp Immunol. (2021) 203:448–57. doi: 10.1111/cei.13536
Keywords: SCID, case report, JAK3, whole exome sequencing, prolonged SARS-CoV-2, inborn errors of immunity
Citation: Sbruzzi RC, Prado MJ, Fam B, Prolla HA, Hellwig A, Motta Rodrigues G, de-Paris F, Jobim M, Artigalás O, Seeleuthner Y, Casanova J-L, Bustamante J and Vianna FSL (2024) Case report: A novel JAK3 homozygous variant in a patient with severe combined immunodeficiency and persistent COVID-19. Front. Immunol. 15:1472957. doi: 10.3389/fimmu.2024.1472957
Received: 30 July 2024; Accepted: 10 September 2024;
Published: 13 November 2024.
Edited by:
Francesca Pala, National Institute of Allergy and Infectious Diseases (NIH), United StatesReviewed by:
Safa Baris, Marmara University, TürkiyeCopyright © 2024 Sbruzzi, Prado, Fam, Prolla, Hellwig, Motta Rodrigues, de-Paris, Jobim, Artigalás, Seeleuthner, Casanova, Bustamante and Vianna. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fernanda Sales Luiz Vianna, ZnNsdmlhbm5hQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.