
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol., 11 November 2024
Sec. Primary Immunodeficiencies
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1468823
This article is part of the Research TopicAdvancing Research, Clinical Recognition, and Targeted Therapies for WHIM SyndromeView all 4 articles
 Lilian Roland1,2†
Lilian Roland1,2† Chi Huu Nguyen3†
Chi Huu Nguyen3† Katarina Zmajkovicova3
Katarina Zmajkovicova3 Mélanie Khamyath1,2
Mélanie Khamyath1,2 Maria Kalogeraki1,2
Maria Kalogeraki1,2 Bérénice Schell1,2
Bérénice Schell1,2 Vanessa Gourhand1,2Vincent Rondeau1,2
Vanessa Gourhand1,2Vincent Rondeau1,2 Zeina Abou Nader1,2
Zeina Abou Nader1,2 Halenya Monticelli3
Halenya Monticelli3 Barbara Maierhofer3
Barbara Maierhofer3 Robert Johnson4Arthur Taveras4
Robert Johnson4Arthur Taveras4 Marion Espéli1,2*‡
Marion Espéli1,2*‡ Karl Balabanian1,2*‡
Karl Balabanian1,2*‡Background: WHIM (Warts, Hypogammaglobulinemia, Infections, and Myelokathexis) syndrome is an ultra-rare, combined primary immunodeficiency and chronic neutropenic disorder characterized by a range of clinical presentations, including peripheral neutropenia, lymphopenia, and recurrent infections. WHIM syndrome is most often caused by gain-of-function mutations in the gene encoding C-X-C chemokine receptor 4 (CXCR4). As such, inhibition of CXCR4 with XOLREMDI® (mavorixafor), an orally bioavailable CXCR4 antagonist, demonstrated clinically meaningful increases in absolute neutrophil and lymphocyte counts and concomitant reduction in infections in patients with WHIM syndrome, resulting in its recent U.S. Food and Drug Administration approval. The impact of CXCR4 antagonism on other aspects of the pathobiology in WHIM syndrome, such as lymphopoiesis and leukocyte trafficking between primary and secondary lymphoid organs, is less understood.
Methods: In the current study, the effects of CXCR4 antagonism on leukocyte trafficking and distribution in primary and secondary lymphoid organs were investigated in a mouse model of WHIM syndrome carrying the heterozygous Cxcr41013 mutation. Cxcr4+/1013 and Cxcr4 wild-type mice received the orally bioavailable CXCR4 antagonist X4-185. Blood, spleen and bone marrow samples were collected for numeration, flow cytometry, and functional studies.
Results: Cxcr4+/1013 mice exhibited profound peripheral blood leukopenia as seen in patients with WHIM syndrome. CXCR4 antagonism corrected circulating leukopenia and mobilized functional neutrophils without disrupting granulopoiesis in the bone marrow of Cxcr4+/1013 mice. Furthermore, Cxcr4+/1013 displayed aberrant splenic T and B-cell counts and frequency. Treatment with X4-185 normalized splenic T-cell abnormalities, correcting the reduced CD8+ T-cell numbers, restoring the CD4/CD8 T-cell ratio, and ameliorating peripheral blood T-cell lymphopenia. In addition, CXCR4 antagonism was able to correct the abnormal frequencies and numbers of splenic marginal zone and follicular B cells in Cxcr4+/1013 mice, and ultimately normalize B-cell lymphopenia in the peripheral circulation.
Conclusions: Our study provides comprehensive evidence that oral dosing with a CXCR4 antagonist can effectively correct WHIM-associated neutrophil and lymphocyte abnormalities in a mouse model of WHIM syndrome. These findings extend our understanding of how targeting the dysregulated CXCR4 signaling pathway can ameliorate the pathogenesis of WHIM syndrome.
WHIM syndrome is an ultra-rare, combined, primary immunodeficiency and chronic neutropenic disorder characterized by the presence of any of four key diagnostic features: Warts, Hypogammaglobulinemia, Infections, and Myelokathexis (1–4). Patients may have diverse clinical presentations, including peripheral blood neutropenia and lymphocytopenia, recurrent and sometimes severe bacterial infections, variable hypogammaglobulinemia, increased susceptibility to human papillomavirus (HPV) and Epstein-Barr virus (EBV) infections, and increased risk of malignancy (2, 3, 5, 6). WHIM syndrome is most often caused by gain-of-function (GOF) mutations in the gene encoding C-X-C chemokine receptor 4 (CXCR4) (3, 7–10), a master regulator of immune cell trafficking, homeostasis, and organogenesis (11, 12). GOF mutations cause impaired CXCR4 receptor internalization and desensitization, prolonged downstream signaling, and enhanced chemotaxis in response to its ligand, C-X-C chemokine ligand 12 (2, 3, 13). These altered responses lead to abnormal retention of neutrophils in the bone marrow (BM) and reduce their egress to peripheral blood (2, 10). Moreover, CXCR4 GOF mutations not only affect neutrophils but also B- and T-cell lymphopoiesis and their peripheral trafficking and localization, resulting in B and T-cell lymphopenia (2, 3, 14–18).
As CXCR4 GOF mutations play a central role in the pathogenesis of WHIM syndrome, correction of aberrant CXCR4 signaling using CXCR4 antagonists including plerixafor and mavorixafor has been explored as a potential therapeutic approach for the treatment of WHIM syndrome (19–24). In a placebo-controlled, double-blind Phase 3 study (NCT03995108), mavorixafor demonstrated clinically meaningful increases in absolute neutrophil and lymphocyte counts in patients with WHIM syndrome, resulting in the recent U.S. Food and Drug Administration (FDA) approval of XOLREMDI® (mavorixafor). In addition, treatment with mavorixafor resulted in a reduction of the annualized infection rate in patients with WHIM syndrome (24). Characterizing the pathobiology in tissue compartments of patients with WHIM syndrome (such as B- and T-cell lymphopoiesis and leukocyte trafficking between primary and secondary lymphoid organs) remains a challenge due to the invasiveness of these procedures. Alternatively, preclinical studies in animal models of WHIM syndrome may be used to provide insights into potential WHIM pathogenesis in tissues and the impact of CXCR4 antagonism on these processes.
In previously reported preclinical studies, acute inhibition of CXCR4 was associated with transient increases in neutrophils, and B- and T-cell counts in the peripheral blood of mice harboring the heterozygous Cxcr41013 mutation (15, 18). However, whether prolonged CXCR4 antagonism could correct leukocyte trafficking and distribution defects in primary and secondary lymphoid organs in this WHIM mouse model remained unclear. In a separate knock-in WHIM mouse model harboring the Cxcr41000 mutation, chronic CXCR4 inhibition by the orally bioavailable CXCR4 antagonist X4-185 was shown to normalize B cell alteration in BM and B-cell counts in circulation and in secondary lymphoid organs (17). The impact of chronic CXCR4 inhibition on splenic B-cell compartmentalization, as well as granulopoiesis and neutrophil trafficking in this second WHIM mouse model, however, was not described. In addition, whether neutrophil function is impaired and whether CXCR4 antagonist treatment can restore normal neutrophil function in these WHIM mouse models have not been investigated. The current study aimed to comprehensively investigate the effects of chronic dosing with an orally bioavailable CXCR4 antagonist on the WHIM-associated leukocyte dysfunctions in primary and secondary lymphoid organs exhibited by mice carrying the heterozygous Cxcr41013 mutation.
Mice harboring the heterozygous Cxcr4+/1013 mutation were generated as previously described (15, 16, 25). This mouse model was selected because it bears a point mutation in the second exon of Cxcr4, which is frequently observed in patients with WHIM syndrome, and was inserted using a knock-in strategy. Littermate wild type (WT) mice were used as controls in all experiments. All mice were 8 -16 weeks old. Daily observation was performed to ensure that no animal was left in a state of pain or suffering during experimentation.
All in vivo mouse experiments were conducted at Université Paris Cité, Institut de Recherche Saint-Louis (Paris, France) from March 2022 to May 2023. Studies were conducted in compliance with the European Union guide for the care and use of laboratory animals, which have been reviewed and approved by an institutional review committee (Comité d’éthique Paris-Nord N°121, France).
Cxcr4+/1013 and Cxcr4WT mice received CXCR4 antagonist X4-185 at 10 mg/kg/day (X4 Pharmaceuticals) (17, 26) or vehicle daily for 7 or 28 days in a row (5 days on/2 days off). Vehicle only was given as control in all experiments (H20-NaCl-0.4% pH4 or phosphate-buffered saline [PBS]). X4-185 is an orally bioavailable, small molecule CXCR4 antagonist of molecular weight ~400 g/mol. In internal control experiments, mice were injected intraperitoneally with plerixafor (AMD3100) (5 mg/kg/day) (Sigma-Aldrich, Darmstadt, Germany) for 21 days (15, 25, 27). Mice were bled 7 days before the start of the experiments, 3 hours after the first dose, then every 7 days 3 hours after the dose. Euthanasia was performed by increasing gradient of CO2. At sacrifice, BM, spleens, and blood were harvested and processed for numeration on an MS9-5 counter (Melet Schloesing, Laboratoires, Osny, France), and flow cytometry. BM cells were extracted by centrifugation from intact femurs, tibia, and hips to separate marrow and bone fractions. Spleens were manually isolated. Cell collection was performed in PBS supplemented with 2% fetal bovine serum and filtered through a 70-μm nylon strainer to remove debris and fat. The peripheral blood was collected by submandibular puncture. Red blood cell lysis was performed using an ammonium-chloride-potassium buffer.
Single cell suspensions were stained with appropriate antibodies in PBS supplemented with 2% bovine serum albumin and 2 mM ethylenediaminetetraacetic acid for cell surface staining. The list of antibodies used in the study is shown in Supplementary Table S1. Analyses were carried out on an LSRII Fortessa flow cytometer (BD Biosciences, Franklin Lakes, NJ, USA), and data were analyzed with the FlowJo software (TreeStar, Ashland, OR, USA).
To determine Reactive Oxygen Species (ROS) levels, whole blood was loaded with 0.5 µg/mL Dihydrorodamine 123 (cat#D1054, Sigma-Aldrich) and incubated for 15 minutes at 37°C. Subsequently, 200 nM phorbol 12-myristate 13-acetate was added, and the samples were incubated for an additional 45 minutes at 37°C to induce the ROS production. For unstimulated samples, incubation with PBS was performed. Then, 2 mL of red blood cell lysis buffer was added, and the mixture was incubated at room temperature. After 10 minutes, the reaction was halted by adding 4 mL of PBS, and samples were centrifuged at 200 g for 5 minutes. The red blood cell lysis procedure was repeated a second time. The fluorescence levels were measured using flow cytometry (BD FACSCanto™ II, BD Biosciences). The gating strategy of granulocytes was based on forward and side scatter plots of the lysed whole blood.
To quantify phagocytic activity, pHrodo™ BioParticles™ Conjugates for Phagocytosis (Cat# P35367, Thermo Fisher Scientific, Waltham, MA, USA) was used. Whole blood was incubated with pHrodo BioParticles for 15 minutes at 37°C. Negative controls were incubated for 15 minutes on ice. Then, all the samples were placed on ice to stop the uptake process. Subsequently, 2 mL of red blood cell lysis buffer was added, and the mixture was incubated on ice for 15 minutes. The reaction was halted by adding 4 mL of PBS and samples were centrifuged at 200 g for 5 minutes. The fluorescence levels were measured using flow cytometry (BD FACSCanto™ II). The gating strategy of granulocytes was based on forward and side scatter plots of the lysed whole blood.
The data were presented as mean ± standard error of the mean (SEM) and the number of mice per experiments was indicated in the figure legends. All statistical analyses were conducted using Prism software (GraphPad Software, Boston, MA, USA). The significance of differences between two independent groups was calculated using Mann-Whitney test. P values <0.05 were considered statistically significant.
It was shown that transient inhibition of CXCR4 signaling reversed circulating leukopenia in Cxcr4+/1013 mice (15). However, whether CXCR4 antagonism durably corrects leukopenia in Cxcr4+/1013 mice following chronic administration has not been investigated. To this end, Cxcr4+/1013 and littermate WT mice were treated with vehicle or the orally bioavailable CXCR4 antagonist X4-185 by daily gavage at 10 mg/kg/day for 7 days, and blood cell counts were measured 3 hours after the last dose (Figure 1A). Cxcr4+/1013 mice exhibited profound circulating panleukopenia, with lymphocytes being the most impacted leukocyte subtype. Specifically, Cxcr4+/1013 mice had 75%, 80%, 56% and 66% fewer leukocytes, lymphocytes, granulocytes, and monocytes, respectively, than their WT littermates (Figures 1B–E). Membrane expression levels of CXCR4 on neutrophils, B cells, CD4+-T cells and CD8+-T cells from peripheral blood and BM were similar between Cxcr4+/1013 and WT mice (Supplementary Figures S1A, B), in line with our previous reports (15). This finding suggests that peripheral blood leukopenia observed in Cxcr4+/1013 mice is likely due to CXCR4 GOF rather than changes in CXCR4 expression. CXCR4 antagonism led to a significant increase in absolute number of all these subsets in Cxcr4+/1013 mice (Figures 1B–E; Table 1). While CXCR4 antagonism corrected peripheral blood leukopenia in Cxcr4+/1013 mice (Figures 1B–E), it did not appear to affect the count of red blood cells or platelets in both Cxcr4+/1013 and WT mice (Supplementary Figures S2A, B).
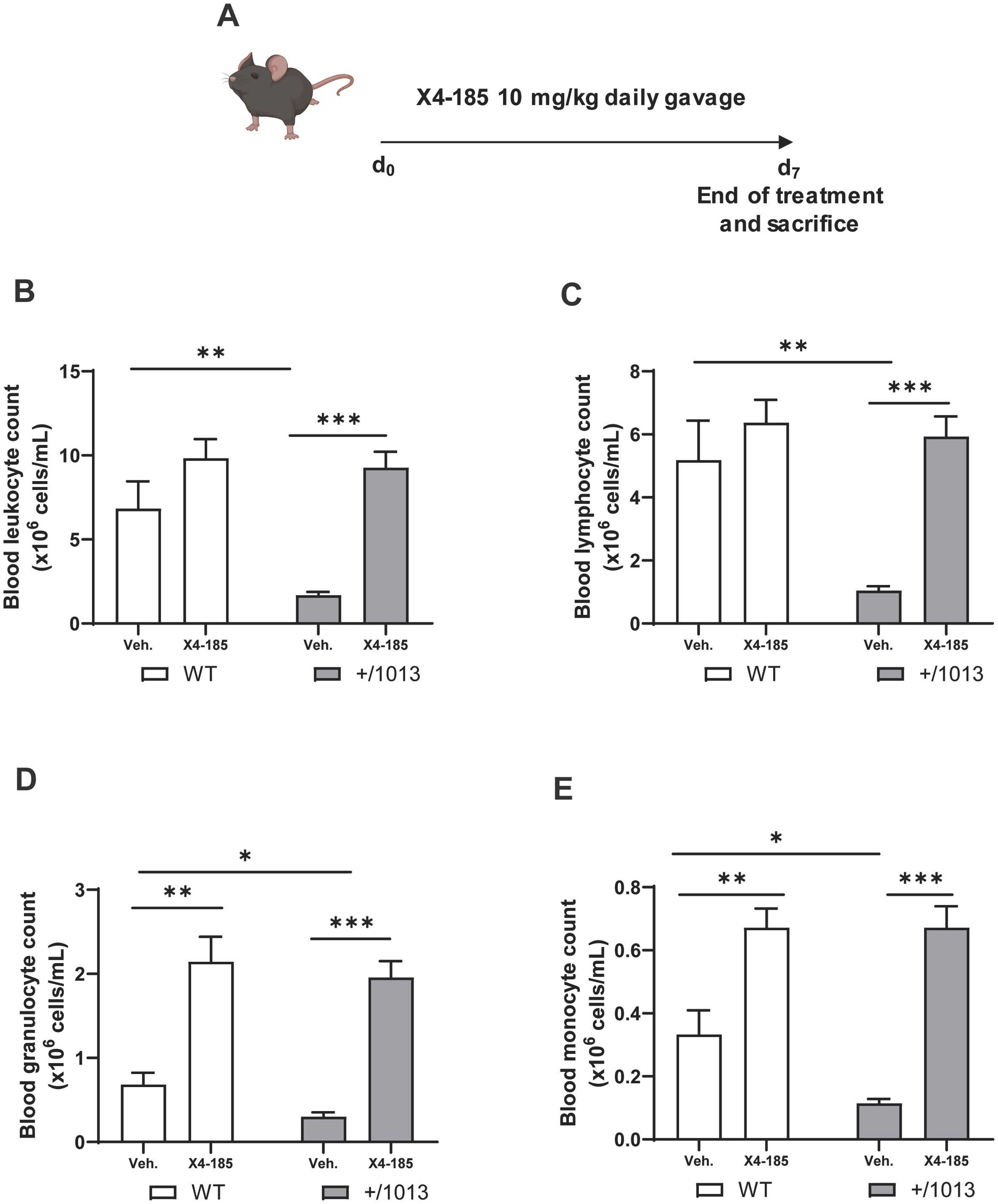
Figure 1. CXCR4 antagonism corrects the peripheral panleukopenia in Cxcr4+/1013 mice. (A) Experimental design for CXCR4 signaling inhibition by CXCR4 antagonist X4-185 in WT and Cxcr4+/1013 mice. Absolute (B) leucocyte, (C) lymphocyte, (D) granulocyte, and (E) monocyte counts were determined in the blood of WT and Cxcr4+/1013 mice 3 hours after the last dose on day 7. Data (mean + SEM) were from two independent experiments with 6–10 mice per group. Statistics were calculated using the nonparametric Mann-Whitney test, two-sided. *p < 0.05, **p < 0.01, ***p < 0.0001. CXCR4, C-X-C chemokine receptor 4; d, day; SEM, standard error of the mean; Veh., vehicle; WT, wild-type.

Table 1. Effects of CXCR4 antagonist X4-185 on blood cell counts in WT and Cxcr4+/1013 mice.
Altogether, these results indicate that CXCR4 antagonism corrected the peripheral blood leukopenia in Cxcr4+/1013 mice.
Next, we explored the effect of CXCR4 antagonism on granulopoiesis and neutrophil function. Cxcr4+/1013 mice were neutropenic, displaying 61% less circulating mature neutrophils than WT mice (Figure 2A). The observed neutropenia in Cxcr4+/1013 mice was not associated with defective granulocyte maturation nor accumulation of mature neutrophils in the BM (Figure 2B). Treatment with CXCR4 antagonist significantly increased the number of mature neutrophils in the blood of Cxcr4+/1013 mice (Figure 2A; Table 1) while, in parallel, decreased the number of mature neutrophils in BM (Figure 2B). A similar tendency was observed in WT mice. These findings support BM as an important reservoir for CXCR4 antagonist-mobilized neutrophils, in line with other reports (27, 28). It is worth noting that treatment with CXCR4 antagonist did not affect granulocyte subset cell counts (promyelocytes, myelocytes and metamyelocytes) in BM of both Cxcr4+/1013 and WT mice, indicating that neutrophil differentiation and maturation remained intact during treatment (Figure 2B).
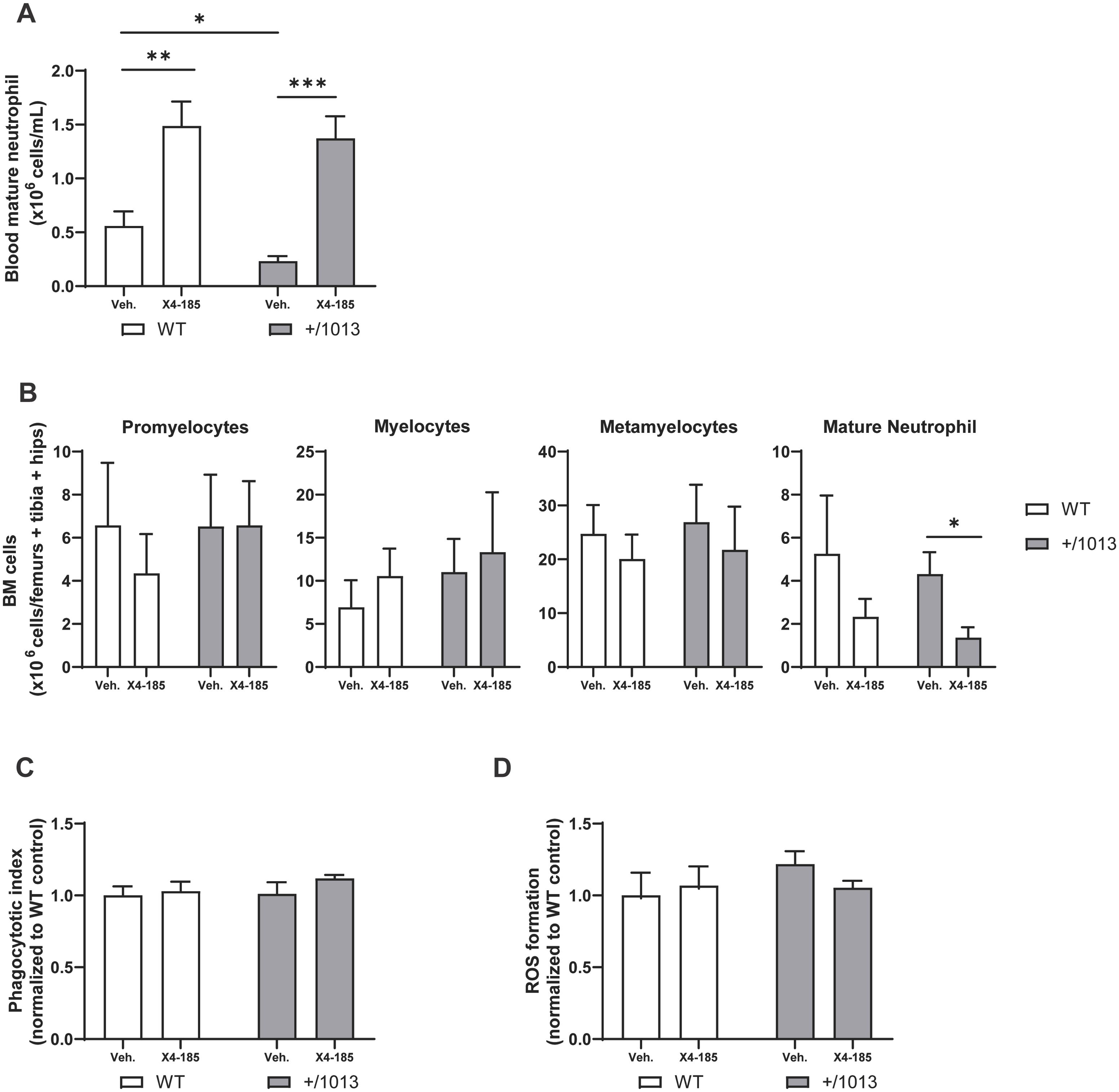
Figure 2. CXCR4 antagonism mobilizes neutrophils in the peripheral blood and preserves their function. (A) Absolute counts of mature neutrophils in the blood and (B) granulocyte subset cell counts in BM were determined 3 hours after the last dose on day 7. (C) Blood neutrophils were harvested 3 hours after the last dose on day 7, incubated with pHrodo BioParticles, and phagocytotic uptake was measured. (D) Blood neutrophils were harvested at 3 hours after the last dose on day 7, stimulated with phorbol 12-myristate 13-acetate, and ROS formation was measured. Data (mean + SEM) were from two independent experiments with 6–10 mice per group (A, B) and from one experiment with three to four mice per group (C, D). Statistics were calculated using the nonparametric Mann-Whitney test, two-sided. *p < 0.05, **p < 0.01, *** p < 0.001. BM, bone marrow; CXCR4, C-X-C chemokine receptor 4; ROS, reactive oxygen species; SEM, standard error of the mean; Veh., vehicle; WT, wild-type.
At the functional level, blood Cxcr4+/1013 neutrophils exhibited similar capacities to conduct phagocytosis of S. aureus BioParticles or to produce ROS compared to their WT counterparts, and these functions were not altered with CXCR4 antagonist treatment (Figures 2C, D). These findings support the notion that the enhanced risk of recurrent infections due to pathogenic bacteria in patients with WHIM syndrome is driven by their low leukocyte counts in peripheral blood rather than reduction of phagocytic or ROS neutrophil functions.
Altogether, these results show that CXCR4 antagonism corrected peripheral blood neutropenia and mobilized functional neutrophils, likely from the BM, without impairing BM granulopoiesis in Cxcr4+/1013 mice.
CXCR4 GOF mutations are associated with T-cell lymphopenia in mice, which may result from alteration in T-cell trafficking through secondary lymphoid organs and/or accumulation of T cells in primary lymphoid organs (15–18). It has been shown that transient blockade of CXCR4 signaling resulted in a reversion of circulating T-cell lymphopenia in Cxcr4+/1013 mice (15, 18). However, the impact of CXCR4 antagonism on T cell abnormalities within the secondary lymphoid organs of this WHIM mouse model has not been thoroughly investigated. In the current study, we focused on investigating whether chronic administration of CXCR4 antagonist could modulate T-cell abnormalities in the spleen and peripheral blood of Cxcr4+/1013 mice. In agreement with a recent report (18), Cxcr4+/1013 mice exhibited severe T-cell lymphopenia that affected more CD8+ than CD4+ T cells, which were reduced by 82% and 55%, respectively, compared with WT mice (Figures 3A, B; Supplementary Figures S3A, B). Accordingly, circulating CD4/CD8 T-cell ratios were increased by ~3-fold in Cxcr4+/1013 mice compared to WT mice (Figure 3C; Supplementary Figure S3C). CXCR4 antagonism corrected peripheral blood CD4+ and CD8+ T-cell lymphopenia in these mice and even restored the circulating CD4/CD8 T-cell ratios to WT levels after 7 days (Supplementary Figures S3A–C; Table 1) and 28 days of treatment (Figures 3A–C).
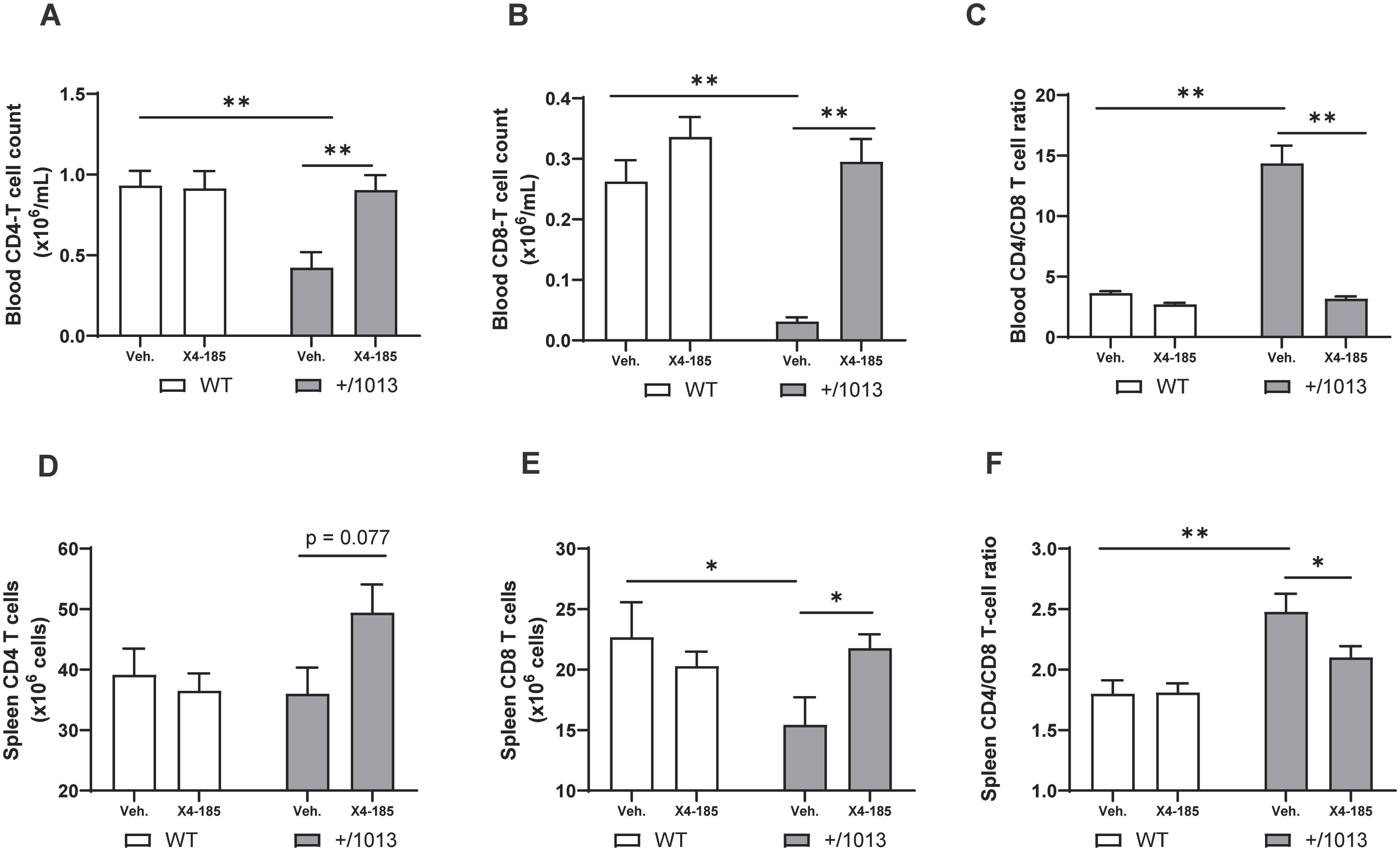
Figure 3. CXCR4 antagonism normalizes the splenic T-cell compartment in Cxcr4+/1013 mice. Absolute (A) CD4+ T-cell counts, (B) CD8+ T-cell counts, and (C) CD4/CD8 T-cell ratio were determined in the blood 3 hours after the last dose on day 28. Total (D) CD4 T-cell numbers, (E) CD8 T-cell numbers, and (F) CD4/CD8 T-cell ratio were determined in the spleen of WT and Cxcr4+/1013 mice after 28 days of X4-185 treatment. Data (mean + SEM) were from two independent experiments with 6–10 mice per group. Statistics were calculated using the nonparametric Mann-Whitney test, two-sided. *p < 0.05, **p < 0.01. CXCR4, C-X-C chemokine receptor 4; SEM, standard error of the mean; Veh., vehicle; WT, wild-type.
Next, we quantified CD4+ and CD8+ T cells in the spleen of WT and Cxcr4+/1013 mice. Cxcr4+/1013 mice had lower CD8+ T-cell numbers in the spleen, while CD4+ T-cell numbers remained unchanged (Figures 3D, E; Supplementary Figures S3D, E). Splenic CD4/CD8 T-cell ratios were also increased by ~1.4-fold compared with WT mice (Figure 3F; Supplementary Figure S3F). Treatment with CXCR4 antagonist for 7 days did not appear to modulate splenic T cell abnormalities (Supplementary Figures S3D, E). However, prolonged CXCR4 antagonism for 28 days normalized splenic CD8-T cell numbers in Cxcr4+/1013 mice and restored splenic CD4/CD8 T-cell ratios to WT levels (Figures 3E, F). In contrast, this prolonged treatment had no impact on splenic T-cell composition in WT mice (Figures 3D–F).
Our data thus indicate that prolonged CXCR4 antagonism can correct splenic T-cell abnormalities and normalize T-cell lymphopenia in peripheral blood in Cxcr4+/1013 mice.
CXCR4 GOF mutations alter B-cell development and trafficking resulting in B-cell lymphopenia in mice (15–17). Consistent with these observations, we found that Cxcr4+/1013 mice had severe B-cell lymphopenia in peripheral blood (Figure 4A). Treatment with a CXCR4 antagonist for 7 days resulted in an increased B-cell count in Cxcr4+/1013 mice that reached levels seen in WT mice (Figure 4A; Table 1). Consistent with a previous report (15), IgM levels were slightly higher in Cxcr4+/1013 mice compared to WT mice, while IgG1 levels were comparable to those in WT mice. Chronic treatment with CXCR4 antagonist had no significant impact on IgM and IgG1 levels (Supplementary Figures S4A, B).
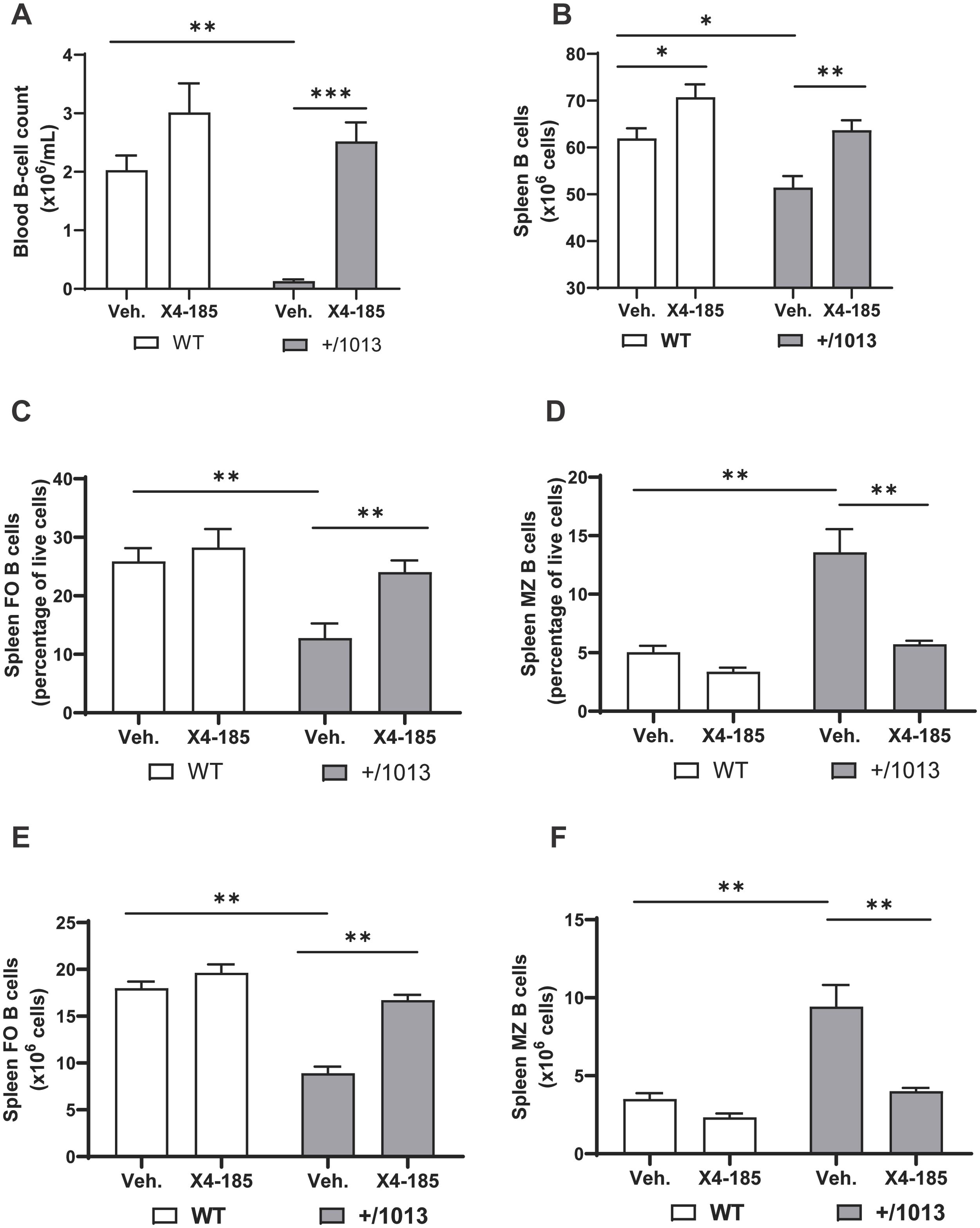
Figure 4. CXCR4 antagonism normalizes the splenic B-cell compartment in Cxcr4+/1013 mice. (A) Absolute B-cell counts were determined in the blood of WT and Cxcr4+/1013 mice 3 hours after the last dose on day 7. (B) Total splenic B-cell number in WT and Cxcr4+/1013 mice after 28 days of X4-185 treatment. The frequency of (C) FO or (D) MZ B cells and the total numbers of (E) FO or (F) MZ B cells were determined in the spleen of WT and Cxcr4+/1013 mice after 28 days of X4-185 treatment. Data (mean + SEM) were from two independent experiments with 6–10 mice per group. Statistics were calculated using the nonparametric Mann-Whitney test, two-sided. *p < 0.05, **p < 0.01, ***p < 0.001. CXCR4, C-X-C chemokine receptor 4; FO, follicular; MZ, marginal zone; SEM, standard error of the mean; Veh., vehicle; WT, wild-type.
The observed normalization of circulating B-cell count following CXCR4 antagonist treatment may result from correction of defective B-cell development and/or redistribution of B cells from primary and secondary lymphoid organs. An analysis of spleens from Cxcr4+/1013 mice revealed multiple defects, including decreased spleen weight (~42%), cellularity (39%) and total B cell count (17%) compared with WT mice (Supplementary Figures S5A, B; Figure 4B) (15). Chronic dosing with CXCR4 antagonist (28-days of treatment) rescued total splenic B -cell number in Cxcr4+/1013 mice to levels observed in WT mice (Figure 4B).
It is well established that immature B cells migrating from the BM emerge in the spleen as transitional B cells and further develop into mature marginal zone (MZ) and follicular (FO) B cells (15). We questioned whether this process and distribution of B-cells were defective in Cxcr4+/1013 mice and whether CXCR4 antagonism could correct any related defects observed. As previously reported (15), the frequency and number of FO B cells in Cxcr4+/1013 mice were reduced by >50% compared with WT mice (Figures 4C, E). In contrast, the frequency and number of MZ B cells in Cxcr4+/1013 mice were significantly increased compared with WT mice (Figures 4D, F). Chronic treatment with the oral CXCR4 antagonist X4-185 for 28 days resulted in correction of both frequency and absolute number of FO and MZ B cells to levels seen in WT mice (Figures 4C–F). Reminiscent of previous works (17, 27), no changes in the frequency and counts of splenic FO and MZ B cell were observed in the spleen of WT mice. Interestingly, chronic treatment with plerixafor (AMD3100), an injectable CXCR4 antagonist that has a shorter receptor occupancy time and more limited tissue distribution (as measured by volume of distribution) compared with the orally bioavailable CXCR4 antagonist X4-185 (Supplementary Table S2; Supplementary Figure S6), was unable to correct splenic FO and MZ B-cell defects observed in Cxcr4+/1013 mice over a 21-day treatment period (Supplementary Figures S7A–D).
These data demonstrate that prolonged treatment with CXCR4 antagonist X4-185 corrected splenic B-cell abnormalities in Cxcr4+/1013 mice, while normalizing B-cell lymphopenia in the peripheral blood.
In the present study, we have investigated the impact of chronic dosing of the orally bioavailable CXCR4 antagonist X4-185 on leukocyte trafficking and distribution in primary and secondary lymphoid organs in a mouse model of WHIM syndrome harboring the heterozygous Cxcr41013 mutation, which is frequently observed in patients with WHIM syndrome. We provide evidence that CXCR4 antagonism corrected peripheral blood leukopenia and mobilized functional neutrophils without affecting BM granulopoiesis in Cxcr4+/1013 mice. In addition, CXCR4 antagonism restored splenic T and B cell abnormalities in Cxcr4+/1013 mice. These findings provide a more comprehensive understanding of how targeting the dysregulated CXCR4 signaling pathway can mitigate the pathogenesis of WHIM syndrome.
WHIM syndrome is predominantly caused by GOF mutations in the gene coding the CXCR4 receptor that leads to severe peripheral leukopenia (2, 3, 29). A recent phase 3 trial has shown that blockade of CXCR4 with mavorixafor, an orally bioavailable and selective CXCR4 antagonist, demonstrated clinically meaningful increases in absolute neutrophil and lymphocyte counts in patients with WHIM syndrome, leading to the recent FDA approval of XOLREMDI® (mavorixafor). Moreover, treatment with mavorixafor was shown to reduce the annualized infection rate in patients with WHIM syndrome (24). In agreement with these observations in patients with WHIM syndrome, we found that CXCR4 antagonism efficiently corrected the quantitative defects of circulating leukocyte counts in Cxcr4+/1013 mice. It is worth noting that CXCR4 antagonism had a more pronounced effect on leukocyte mobilization in Cxcr4+/1013 than in WT mice (Table 1). This observation raises several hypotheses that are not mutually exclusive: (1) Cxcr4+/1013 mice may have a greater leukocyte reservoir than WT mice due to sequestration of leukocytes in different tissues; (2) CXCR4 antagonism may mobilize cells from different and/or multiple tissue compartments in Cxcr4+/1013 mice compared with WT mice. Additional studies are required to fully address these questions.
In patients with WHIM syndrome, CXCR4 GOF mutations cause increased retention of neutrophils in the BM, and this process is thought to contribute to circulating neutropenia (2, 10). Cxcr4+/1013 mice exhibited moderate neutropenia; however, this happened in the context of normal neutrophil maturation and was associated with neither accumulation of neutrophils nor increased apoptosis in the BM (15). This observation suggests that in Cxcr4+/1013 mice, neutrophils may preferentially accumulate in other tissues, rather than in BM, or that the clearance of neutrophils by tissue-resident macrophages could be differentially regulated in mice versus humans in this WHIM mouse model. Nonetheless, we observed that chronic treatment with a CXCR4 antagonist led to an increased mature neutrophil count in the blood, which correlated with a decreased mature neutrophil count in the BM of Cxcr4+/1013 and WT mice. Our data implicate the BM as a critical source of CXCR4 antagonist-mobilized neutrophils, which is consistent with previous reports (27, 28, 30). Whether CXCR4 antagonism also leads to a redistribution of neutrophils from different sources other than BM warrants further investigations. Notably, we also observed that continuous dosing with a CXCR4 antagonist did not appear to hinder the differentiation and maturation of neutrophils within the BM of both Cxcr4+/1013 and WT mice, thereby effectively facilitating the mobilization of neutrophils into peripheral blood without disrupting their production and maturation in BM.
Increased risk of infection in patients with WHIM syndrome is thought to be associated with the reduced levels of circulating neutrophils and/or defects in neutrophil function. Surprisingly, little is known about neutrophil function in the context of WHIM syndrome. Here, we found that blood Cxcr4+/1013 neutrophils were able to produce similar ROS levels and to phagocytose S. aureus BioParticles as efficiently as their WT counterparts, thus suggesting that Cxcr4+/1013 neutrophil function remained intact. Congruent with this, neutrophil function in most WHIM patients with reported functional studies showed normal levels of phagocytosis, bacterial killing activity, and ROS production in response to PMA or bacterial-derived polysaccharide complexes (3, 23, 31). Moreover, we showed that CXCR4 antagonist treatment increased neutrophil counts in blood, while preserving their effector functions. Our findings suggest that the susceptibility of patients with WHIM syndrome to infection may be more a consequence of neutropenia rather than a defect in neutrophil function. Our data provide additional evidence to support the notion that CXCR4 antagonist treatment effectively mobilizes more functional neutrophils, that may, in turn, help patients with WHIM syndrome to overcome the recurrent infections commonly observed.
It was recently reported that CXCR4 GOF mutations lead to a more severe depression of circulating CD8+ T-cell counts compared with CD4+ T cells in patients with WHIM syndrome and in a WHIM mouse model (18). In the phase 3 trial in patients with WHIM syndrome, treatment with CXCR4 antagonist mavorixafor increased and corrected peripheral blood CD4+ and CD8+ T-cell lymphopenia (32, 33). The current data presented here with Cxcr4+/1013 mice corroborated these previous observations in patients with WHIM syndrome. Specifically, we found that Cxcr4+/1013 mice exhibited reduced T-cell counts in peripheral blood and spleen compared with WT mice, with CD8+ T cells being more affected. CXCR4 antagonism reversed peripheral T-cell lymphopenia and restored the CD4/CD8 T-cell ratio in Cxcr4+/1013 mice. Importantly, we uncovered that chronic treatment with a CXCR4 antagonist was able to normalize splenic CD8+ T-cell counts and splenic CD4/CD8 T-cell ratio in Cxcr4+/1013 mice. T-cell lymphopenia in Cxcr4+/1013 and Cxcr4+/1000 mice was attributed to sequestration of T cells in primary lymphoid organs, or defects in T-cell trafficking between bloodstream and secondary lymphoid organs (15, 17, 18). Correction of splenic T-cell counts and distribution abnormalities by CXCR4 antagonism may be facilitated by the release of sequestered T cells from primary lymphoid organs and renewed migration to peripheral lymphoid organs. However, we cannot exclude that CXCR4 antagonist treatment may have a direct impact on the survival of splenic T cells in Cxcr4+/1013 mice. Further work will be required to address this point.
In addition to correcting T-cell lymphopenia, we also observed that CXCR4 antagonist treatment normalized peripheral blood B-cell counts in Cxcr4+/1013 mice. Moreover, we uncovered that chronic treatment with a CXCR4 antagonist X4-185 for four weeks corrected splenic B-cell alterations in Cxcr4+/1013 mice. In line with our data, chronic treatment with the CXCR4 antagonist X4-185 for three weeks was reported to increase and normalize B-cell numbers in blood and spleen in an independent WHIM mouse model harboring the Cxcr41000 mutation (17). Our findings are thus consistent with the recent phase 3 trial results in patients, in which mavorixafor treatment resulted in correction of circulating B-cell lymphopenia (32, 33). Interestingly, we further showed that CXCR4 antagonist X4-185 normalized the frequencies and numbers of splenic MZ and FO B cells in Cxcr4+/1013 mice. The precise mechanisms by which CXCR4 antagonism corrected the splenic B-cell abnormalities in this WHIM mouse model remain unclear. However, it is possible that the CXCR4 antagonist may act directly or indirectly on the splenic stromal cell compartment, favoring the proper trafficking, compartmentalization, and/or maturation of B cells within the spleen. CXCR4 antagonism may also normalize B-cell development and subsequently correct peripheral B-cell count in Cxcr4+/1013 mice, as was recently shown in the Cxcr4+/1000 model (17). Interestingly, we observed that chronic treatment with a CXCR4 antagonist does not alter antibody production in WT and Cxcr4+/1013 mice, suggesting that while the distribution of cells from the B lineage is corrected, their functionality remains unchanged. The ability of CXCR4 antagonists to normalize the abnormalities observed in the splenic B-cell populations may be compound specific and related to the unique tissue distribution properties and residence time of each compound bound to the CXCR4 receptor, as well as the duration of treatment of the antagonist. Supporting these hypotheses, we found that chronic treatment with plerixafor (AMD3100) was unable to correct splenic FO and MZ B-cell defects observed in Cxcr4+/1013 mice. This is in contrast to the effects observed with the orally bioavailable CXCR4 antagonist X4-185.
In summary, this study provides more comprehensive evidence that CXCR4 antagonism can effectively correct WHIM-associated neutrophil and lymphocyte abnormalities in primary and secondary lymphoid organs in a mouse model of WHIM syndrome. Specifically, CXCR4 antagonism normalized peripheral blood leukopenia and restored abnormal splenic B- and T-cell counts and distribution in Cxcr4+/1013 mice. CXCR4 antagonism mobilized functional neutrophils from BM without disrupting normal granulopoiesis. These findings significantly advance our understanding of how targeting the dysregulated CXCR4 signaling pathway can ameliorate the leukocyte pathogenesis of WHIM syndrome.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
The animal studies were approved by Comité d’éthique Paris-Nord N°121, France. The studies were conducted in accordance with the local legislation and institutional requirements.
LR: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. CN: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. KZ: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. MeK: Investigation, Writing – review & editing. MaK: Investigation, Writing – review & editing. BS: Investigation, Writing – review & editing. VG: Investigation, Writing – review & editing. VR: Investigation, Writing – review & editing. ZAN: Investigation, Writing – review & editing. HM: Methodology, Writing – review & editing. BM: Methodology, Writing – review & editing. RJ: Conceptualization, Writing – review & editing. AT: Conceptualization, Writing – original draft, Writing – review & editing. ME: Conceptualization, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing, Resources, Validation. KB: Conceptualization, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing, Resources, Validation.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was supported by an ANR JCJC grant (ANR-19-CE15-0019-01) to ME and an ANR PRC grant (ANR-17-CE14-0019) and the FRM (Programme Equipe FRM 2022, EQU202203014627) to KB. ME and KB received a grant from X4 Pharmaceuticals in the frame of a research agreement. MKh was fellowship recipient from the French Ministry and then supported by La Ligue Contre le Cancer. MKa is fellowship recipient from the French Ministry. BS is fellowship recipient from Poste d’Accueil Inserm. VR was supported by the FRM, La Ligue contre le Cancer and la Société Française d’Hématologie. ZAN was fellowship recipient from the French Ministry and then supported by the FRM.
We thank Drs. C. Doliger, N. Setterblad and V. Parietti-Montcuquet (UMS Saint-Louis US53/UAR2030), and Sabine Maier (X4 Pharmaceuticals (Austria) GmbH, Vienna, Austria) for their technical assistance.
CN, KZ, HM, BM, RJ, and AT are employees and shareholders of X4 Pharmaceuticals. LR, MKh, MKa, BS, VG, VR, ZA, ME and KB had a research agreement with X4 Pharmaceuticals.
The handling editor TT declared a past collaboration with the authors KZ and AT.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1468823/full#supplementary-material
1. Balabanian K, Lagane B, Pablos JL, Laurent L, Planchenault T, Verola O, et al. WHIM syndromes with different genetic anomalies are accounted for by impaired CXCR4 desensitization to CXCL12. Blood. (2005) 105:2449–57. doi: 10.1182/blood-2004-06-2289
2. Geier CB, Ellison M, Cruz R, Pawar S, Leiss-Piller A, Zmajkovicova K, et al. Disease progression of WHIM syndrome in an international cohort of 66 pediatric and adult patients. J Clin Immunol. (2022) 42:1748–65. doi: 10.1007/s10875-022-01312-7
3. Heusinkveld LE, Majumdar S, Gao JL, McDermott DH, Murphy PM. WHIM syndrome: from pathogenesis towards personalized medicine and cure. J Clin Immunol. (2019) 39:532–56. doi: 10.1007/s10875-019-00665-w
4. Wetzler M, Talpaz M, Kleinerman ES, King A, Huh YO, Gutterman JU, et al. A new familial immunodeficiency disorder characterized by severe neutropenia, a defective marrow release mechanism, and hypogammaglobulinemia. Am J Med. (1990) 89:663–72. doi: 10.1016/0002-9343(90)90187-i
5. Kawai T, Malech HL. WHIM syndrome: congenital immune deficiency disease. Curr Opin Hematol. (2009) 16:20–6. doi: 10.1097/MOH.0b013e32831ac557
6. Moulin C, Beaupain B, Suarez F, Bertrand Y, Beaussant SC, Fischer A, et al. CXCR4 WHIM syndrome is a cancer predisposition condition for virus-induced Malignancies. Br J Haematol. (2024) 204(4):1383–92. doi: 10.1111/bjh.19373
7. Liu Q, Chen H, Ojode T, Gao X, Anaya-O’Brien S, Turner NA, et al. WHIM syndrome caused by a single amino acid substitution in the carboxy-tail of chemokine receptor CXCR4. Blood. (2012) 120:181–9. doi: 10.1182/blood-2011-12-395608
8. Liu Q, Pan C, Lopez L, Gao J, Velez D, Anaya-O’Brien S, et al. WHIM syndrome caused by waldenstrom’s macroglobulinemia-associated mutation CXCR4 (L329fs). J Clin Immunol. (2016) 36:397–405. doi: 10.1007/s10875-016-0276-3
9. Hernandez PA, Gorlin RJ, Lukens JN, Taniuchi S, Bohinjec J, Francois F, et al. Mutations in the chemokine receptor gene CXCR4 are associated with WHIM syndrome, a combined immunodeficiency disease. Nat Genet. (2003) 34:70–4. doi: 10.1038/ng1149
10. Beaussant Cohen S, Fenneteau O, Plouvier E, Rohrlich PS, Daltroff G, Plantier I, et al. Description and outcome of a cohort of 8 patients with WHIM syndrome from the French Severe Chronic Neutropenia Registry. Orphanet J Rare Dis. (2012) 7:71. doi: 10.1186/1750-1172-7-71
11. Pozzobon T, Goldoni G, Viola A, Molon B. CXCR4 signaling in health and disease. Immunol Lett. (2016) 177:6–15. doi: 10.1016/j.imlet.2016.06.006
12. De Filippo K, Rankin SM. CXCR4, the master regulator of neutrophil trafficking in homeostasis and disease. Eur J Clin Invest. (2018) 48 Suppl 2:e12949. doi: 10.1111/eci.12949
13. Zmajkovicova K, Pawar S, Maier-Munsa S, Maierhofer B, Wiest I, Skerlj R, et al. Genotype-phenotype correlations in WHIM syndrome: a systematic characterization of CXCR4(WHIM) variants. Genes Immun. (2022) 23:196–204. doi: 10.1038/s41435-022-00181-9
14. Majumdar S, Murphy PM. Adaptive immunodeficiency in WHIM syndrome. Int J Mol Sci. (2018) 20(1):3. doi: 10.3390/ijms20010003
15. Balabanian K, Brotin E, Biajoux V, Bouchet-Delbos L, Lainey E, Fenneteau O, et al. Proper desensitization of CXCR4 is required for lymphocyte development and peripheral compartmentalization in mice. Blood. (2012) 119:5722–30. doi: 10.1182/blood-2012-01-403378
16. Freitas C, Wittner M, Nguyen J, Rondeau V, Biajoux V, Aknin ML, et al. Lymphoid differentiation of hematopoietic stem cells requires efficient Cxcr4 desensitization. J Exp Med. (2017) 214:2023–40. doi: 10.1084/jem.20160806
17. Zehentmeier S, Lim VY, Ma Y, Fossati J, Ito T, Jiang Y, et al. Dysregulated stem cell niches and altered lymphocyte recirculation cause B and T cell lymphopenia in WHIM syndrome. Sci Immunol. (2022) 7:eabo3170. doi: 10.1126/sciimmunol.abo3170
18. Majumdar S, Pontejo SM, Jaiswal H, Gao JL, Salancy A, Stassenko E, et al. Severe CD8+ T lymphopenia in WHIM syndrome caused by selective sequestration in primary immune organs. J Immunol. (2023) 210:1913–24. doi: 10.4049/jimmunol.2200871
19. McDermott DH, Liu Q, Velez D, Lopez L, Anaya-O’Brien S, Ulrick J, et al. A phase 1 clinical trial of long-term, low-dose treatment of WHIM syndrome with the CXCR4 antagonist plerixafor. Blood. (2014) 123:2308–16. doi: 10.1182/blood-2013-09-527226
20. McDermott DH, Pastrana DV, Calvo KR, Pittaluga S, Velez D, Cho E, et al. Plerixafor for the treatment of WHIM syndrome. N Engl J Med. (2019) 380:163–70. doi: 10.1056/NEJMoa1808575
21. McDermott DH, Velez D, Cho E, Cowen EW, DiGiovanna JJ, Pastrana DV, et al. A phase III randomized crossover trial of plerixafor versus G-CSF for treatment of WHIM syndrome. J Clin Invest. (2023) 133(19):e164918. doi: 10.1172/JCI164918
22. Dale DC, Firkin F, Bolyard AA, Kelley M, Makaryan V, Gorelick KJ, et al. Results of a phase 2 trial of an oral CXCR4 antagonist, mavorixafor, for treatment of WHIM syndrome. Blood. (2020) 136:2994–3003. doi: 10.1182/blood.2020007197
23. McDermott DH, Liu Q, Ulrick J, Kwatemaa N, Anaya-O’Brien S, Penzak SR, et al. The CXCR4 antagonist plerixafor corrects panleukopenia in patients with WHIM syndrome. Blood. (2011) 118:4957–62. doi: 10.1182/blood-2011-07-368084
24. Badolato R, Alsina L, Azar A, Bertrand Y, Bolyard AA, Dale D, et al. A phase 3 randomized trial of mavorixafor, a CXCR4 antagonist, for WHIM syndrome. Blood. (2024) 144(1):35–45. doi: 10.1182/blood.2023022658
25. Anginot A, Nguyen J, Abou Nader Z, Rondeau V, Bonaud A, Kalogeraki M, et al. WHIM Syndrome-linked CXCR4 mutations drive osteoporosis. Nat Commun. (2023) 14:2058. doi: 10.1038/s41467-023-37791-4
26. Feng X, Sun R, Lee M, Chen X, Guo S, Geng H, et al. Cell circuits between leukemic cells and mesenchymal stem cells block lymphopoiesis by activating lymphotoxin beta receptor signaling. Elife. (2023) 12:e83533. doi: 10.7554/eLife.83533
27. Liu Q, Li Z, Gao JL, Wan W, Ganesan S, McDermott DH, et al. CXCR4 antagonist AMD3100 redistributes leukocytes from primary immune organs to secondary immune organs, lung, and blood in mice. Eur J Immunol. (2015) 45:1855–67. doi: 10.1002/eji.201445245
28. Jorgensen AS, Daugvilaite V, De Filippo K, Berg C, Mavri M, Benned-Jensen T, et al. Biased action of the CXCR4-targeting drug plerixafor is essential for its superior hematopoietic stem cell mobilization. Commun Biol. (2021) 4:569. doi: 10.1038/s42003-021-02070-9
29. McDermott DH, Murphy PM. WHIM syndrome: Immunopathogenesis, treatment and cure strategies. Immunol Rev. (2019) 287:91–102. doi: 10.1111/imr.12719
30. Martin C, Burdon PC, Bridger G, Gutierrez-Ramos JC, Williams TJ, Rankin SM. Chemokines acting via CXCR2 and CXCR4 control the release of neutrophils from the bone marrow and their return following senescence. Immunity. (2003) 19:583–93. doi: 10.1016/s1074-7613(03)00263-2
31. Hord JD, Whitlock JA, Gay JC, Lukens JN. Clinical features of myelokathexis and treatment with hematopoietic cytokines: a case report of two patients and review of the literature. J Pediatr Hematol Oncol. (1997) 19:443–8. doi: 10.1097/00043426-199709000-00007
32. Badolato R, Group WS, Hu Y, Karlsson L, Monticelli H, Nguyen C, et al. Assessment of lymphocyte subpopulations in blood: results of a phase 3 trial in WHIM syndrome. In: Presented at American Society of Pediatric Hematology and Oncology (ASPHO) Conference; April 3-6; Seattle, Washington, USA. Seattle, Washington, USA.
33. Results of a Phase 3 Trial of an Oral CXCR4 Antagonist, Mavorixafor, for the Treatment of Participants With WHIM Syndrome: Investigational Assessment of Lymphocyte Subpopulations in Peripheral Blood (2024). Washington, DC, USA: American Academy of Allergy Asthma and Immunology (AAAAI 2024 (Accessed February 23-26, 2024).
Keywords: WHIM syndrome, primary immunodeficiency, chronic neutropenia, CXCR4 antagonism, preclinical study, neutrophil function
Citation: Roland L, Nguyen CH, Zmajkovicova K, Khamyath M, Kalogeraki M, Schell B, Gourhand V, Rondeau V, Abou Nader Z, Monticelli H, Maierhofer B, Johnson R, Taveras A, Espéli M and Balabanian K (2024) CXCR4 antagonism ameliorates leukocyte abnormalities in a preclinical model of WHIM syndrome. Front. Immunol. 15:1468823. doi: 10.3389/fimmu.2024.1468823
Received: 22 July 2024; Accepted: 22 October 2024;
Published: 11 November 2024.
Edited by:
Teresa Kathleen Tarrant, Duke University, United StatesReviewed by:
Artem Kalinichenko, St. Anna Children’s Cancer Research Institute (CCRI), AustriaCopyright © 2024 Roland, Nguyen, Zmajkovicova, Khamyath, Kalogeraki, Schell, Gourhand, Rondeau, Abou Nader, Monticelli, Maierhofer, Johnson, Taveras, Espéli and Balabanian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marion Espéli, bWFyaW9uLmVzcGVsaUBpbnNlcm0uZnI=; Karl Balabanian, a2FybC5iYWxhYmFuaWFuQGluc2VybS5mcg==
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.