 Jelle Praet1*†
Jelle Praet1*† Lina Anderhalten2†
Lina Anderhalten2† Giancarlo Comi3,4
Giancarlo Comi3,4 Dana Horakova5
Dana Horakova5 Tjalf Ziemssen6
Tjalf Ziemssen6 Patrick Vermersch7
Patrick Vermersch7 Carsten Lukas8
Carsten Lukas8 Koen van Leemput9,10,11
Koen van Leemput9,10,11 Marjan Steppe12
Marjan Steppe12 Cristina Aguilera13
Cristina Aguilera13 Ella Maria Kadas14Alexis Bertrand15Jean van Rampelbergh16Erik de Boer17Vera Zingler18
Ella Maria Kadas14Alexis Bertrand15Jean van Rampelbergh16Erik de Boer17Vera Zingler18 Dirk Smeets1
Dirk Smeets1 Annemie Ribbens1†
Annemie Ribbens1† Friedemann Paul2,19,20,21,22† on behalf of CLAIMS consortium
Friedemann Paul2,19,20,21,22† on behalf of CLAIMS consortium- 1icometrix NV, Leuven, Belgium
- 2Experimental and Clinical Research Center (ECRC), A Cooperation Between the Max Delbrück Center for Molecular Medicine in the Helmholtz Association and Charité - Universitätsmedizin Berlin, Berlin, Germany
- 3Department of Neurorehabilitative Sciences, Casa di Cura Igea, Italy
- 4Department of Neurology, Vita-Salute San Raffaele University-Ospedale San Raffaele, Milan, Italy
- 5Department of Neurology and Center of Clinical Neuroscience, First Faculty of Medicine, Charles University and General University Hospital, Prague, Czechia
- 6Center of Clinical Neuroscience, Department of Neurology, University Clinic Carl Gustav Carus, TU Dresden, Dresden, Germany
- 7Univ. Lille, InsermU1172 LilNCog, CHU Lille, FHU Precise, Lille, France
- 8Institute of Neuroradiology, St. Josef Hospital, Ruhr-University Bochum, Bochum, Germany
- 9Athinoula A. Martinos Center, Department of Radiology, Massachusetts General Hospital, Charlestown, MA, United States
- 10Department of Neuroscience and Biomedical Engineering, Aalto University, Espoo, Finland
- 11Department of Computer Science, Aalto University, Espoo, Finland
- 12European Charcot Foundation, Brussels, Belgium
- 13SYNAPSE Research Management Partners, Madrid, Spain
- 14Nocturne GmbH, Berlin, Germany
- 15AB Science, Clinical Development, Paris, France
- 16Imcyse SA, Liège, Belgium
- 17Bristol-Myers Squibb Company Corp, Princeton, NJ, United States
- 18F. Hoffmann-La Roche Ltd., Product Development Medical Affairs, Neuroscience, Basel, Switzerland
- 19Experimental and Clinical Research Center (ECRC), Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
- 20Max Delbrück Center for Molecular Medicine in the Helmholtz Association (MDC), Berlin, Germany
- 21Neuroscience Clinical Research Center (NCRC), Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
- 22Department of Neurology with Experimental Neurology, Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
Multiple sclerosis (MS) is a devastating immune-mediated disorder of the central nervous system resulting in progressive disability accumulation. As there is no cure available yet for MS, the primary therapeutic objective is to reduce relapses and to slow down disability progression as early as possible during the disease to maintain and/or improve health-related quality of life. However, optimizing treatment for people with MS (pwMS) is complex and challenging due to the many factors involved and in particular, the high degree of clinical and sub-clinical heterogeneity in disease progression among pwMS. In this paper, we discuss these many different challenges complicating treatment optimization for pwMS as well as how a shift towards a more pro-active, data-driven and personalized medicine approach could potentially improve patient outcomes for pwMS. We describe how the ‘Clinical Impact through AI-assisted MS Care’ (CLAIMS) project serves as a recent example of how to realize such a shift towards personalized treatment optimization for pwMS through the development of a platform that offers a holistic view of all relevant patient data and biomarkers, and then using this data to enable AI-supported prognostic modelling.
1 The heterogeneous disease course of multiple sclerosis
Multiple sclerosis (MS) is a devastating immune-mediated disorder of the central nervous system (CNS) resulting in progressive disability accumulation in most individuals affected (1, 2). MS imposes a significant burden on patients, affecting all aspects of their life, and additionally, it poses a significant challenge to society as with growing disability, indirect expenses (productivity losses associated with sick absence, inability to work, and early retirement) and care costs rise substantially (3).
The classical view on MS describes different clinical subtypes, with relapsing-remitting MS (RRMS) being the most common form, occurring in 85% of patients (National MS Society). Patients with RRMS experience neurological exacerbation (relapses) as well as intermittent periods of remission in which they remain clinically stable. Relapses can either recover completely or leave persistent clinical disability, referred to as Relapse Associated Worsening (RAW). Among these patients, approximately two-thirds progress to secondary-progressive MS (SPMS) (4). In contrast to RRMS, the disease course of patients with SPMS or primary-progressive MS (PPMS, 15% of MS patients) is mainly driven by a gradual worsening of disability in the absence of relapse activity (5).
Recent research has challenged this classical view of distinct MS subtypes, as they may not sufficiently account for the large spectrum of multifaceted clinical phenotypes and disease courses as well as sub-clinical disease variability (6). This disease heterogeneity is further complicated by a high prevalence of comorbidities and multi-pharmacy in MS. Data from the NARCOMS registry suggested that, at the time of MS diagnosis, 35% of MS patients suffer physical comorbidities while 18% reported a psychiatric comorbidity (7, 8). Additionally, accumulation of clinical disability independent of acute inflammatory relapses - commonly referred to as Progression Independent of Relapse Activity (PIRA) (9) - was found to occur in any of the classical MS subtypes, including RRMS, and at any stage of the disease (10, 11). Most importantly, in a substantial proportion of people with MS (pwMS), PIRA occurs already very early on, and this is associated with worse long-term outcomes (2). Recent studies have also shown that PIRA gradually becomes the dominant driver of disability worsening as the disease progresses (9).
While new insights into PIRA continue to be unraveled, exact criteria of how to define, assess, and monitor PIRA are still lacking. Several definitions have been put forward, but these focus mainly only on measuring disability worsening by means of the Expanded Disability Status Scale (EDSS) and Confirmed Disability Worsening (CDW) (2). Relying solely on EDSS or CDW to describe PIRA, however, seems to be insufficient as (i) there are heterogeneous symptoms and disease aspects contributing to disability worsening and MS severity, and (ii) this omits sub-clinical processes such as compartmentalized inflammation, chronically active (smouldering) lesions, diffuse normal-appearing matter damage (12, 13), as well as brain (14) and spinal cord atrophy (15, 16). Such processes seem to represent relevant substrates of (silent/smouldering) disease progression even during early stages and to contribute to enhanced long-term disability worsening in pwMS (17). In this regard, the topographical disease model proposed by Krieger et al. may facilitate the interpretation of the clinical course revision, providing a unified visualization across phenotypes, while providing insights in the interplay between the distinct processes of relapse activity and progression, and accounting for latent variables such as relapse localization, frequency, severity, recovery and progression rate (18). Additionally, this model was recently validated in terms of brain MRI markers (19). Aligning with this model, individuals deemed neurologically normal in early MS (e.g., with an EDSS score of 0) demonstrated subtle deficits in high-challenging motor tasks (20) and often have fatigue (21) and cognitive impairments (22). The former was also shown to correlate with imaging markers of disease burden and brain reserve, challenging traditional severity definitions and underscoring the importance of looking beyond standard clinical measures such as the EDSS (20).
2 A changing landscape in treatment strategies
The heterogeneity in disease progression among individuals with MS (both clinically and sub-clinically) contributes to a high diversity in treatment responses across pwMS (23). As there is no cure available yet for MS, the primary therapeutic objective is to slow down disability progression and to reduce relapses as early as possible during the disease to maintain and/or improve the health-related quality of life (24).
To this end, all regulatory-approved disease-modifying treatments (DMT) have shown their worth in preventing relapses during the few years of the clinical trial in which their efficacy was evaluated. However, the impact on the long-term accumulation of disability and chronic subtle disease processes was often limited as even the most effective DMTs available were only able to mitigate the short-term risk of disability progression by 30-42% (25). A recent review from Gasperini et al. emphasizes how dire the situation really is, indicating that only 30- 40% of patients receiving a DMT remain stable over a period of 5 to 7 years, and only up to 10% over a period of 7 to 10 years after initiating DMT (26).
Despite the approval of ±20 different DMTs by the European Medicines Agency (EMA) and the US Food and Drug Administration (FDA) (27, 28), concerns about side effects and efficacy might discourage many pwMS from initiating a high-efficacy DMT therapy (29, 30), an issue further aggravated by therapeutic inertia (31). Additionally, those who do receive a DMT usually start with one of the less effective but well-established therapies due to their minimal side effects (32). Traditionally, it’s only when these well-established DMTs fail to prevent relapses and disability progression, that the treatment is escalated to a higher-efficacy treatment, which usually is more expensive, might have more pronounced side effects, and is potentially more challenging to administer (oral and injectables versus infusions) (33). However, multiple studies support the observation that reducing the accrual of neurological damage in the initial stages of the disease potentially improves overall clinical outcomes throughout the patient’s lifespan when employing early intervention with higher efficacy DMT (34–38). Additionally, DMTs were shown to be more efficacious, and side effects less likely to occur in younger patients (39). Taken together, these studies question the traditional treatment escalation paradigm which is therefore nowadays considered outdated by most physicians. Instead, current thinking emphasizes the potential advantages of early initiation of high-efficacy DMTs, indicating the need for and the significance of an early MS diagnosis, proactive monitoring to detect disease activity early, and shared decision-making as crucial elements in patient care (32, 40).
Additionally, given the shortcomings of current DMTs to halt long-term disability accumulation, a next generation of DMTs might focus more on the silent progression of the disease. A first novel category of DMTs in this regard are potentially the Bruton tyrosine kinase inhibitors. This new class of drugs might become the first to target both acute inflammatory relapses as well chronic inflammatory processes in the CNS thought to drive disability accumulation (41). In this context, especially the early recognition of individuals prone to developing PIRA will be essential. A better understanding of PIRA and RAW as well as their interplay, combined with data-driven prognosis, will enhance the selection of current and future DMTs and allow to treat patients beyond just relapse activity. Nevertheless, certain variables pose challenges to the trajectory of precision medicine and treatment optimization on an individual level. While there are guidelines on the use of DMTs in MS (24), these are all based on expert judgment and differ across countries, even within the EU (28, 37). This variance extends to therapy selection post-diagnosis or during follow-ups, driven by perceived levels of clinical and subclinical disease activity and progression.
3 Precision medicine enables treatment optimization
Accumulating evidence suggests that the reactive treatment of lesion activity is insufficient, negatively impacting long-term patient outcomes (42). In the complex landscape of MS treatment, an increasing acknowledgment of disease heterogeneity and underlying disease mechanisms underscores the imperative for a paradigm shift toward proactive, data-driven precision medicine (43). However, despite its promise, such data-driven approaches come hand in hand with substantial challenges.
The understanding of the complex and heterogeneous underlying neuropathology of MS is still limited. The adoption of precision medicine in MS is further complicated by the chronic nature of the disease, exhibiting variable courses over time. Consequently, given the longitudinal disease aspect, one must account for the fact that data might be incomplete at times, particularly in routine practice. In addition, the influence of comorbidities adds another layer of complexity (44). Various biomarkers are deemed relevant for their role in identifying diverse MS aspects and patterns of progression in MS, aiding diagnosis, prognosis, and treatment selection (45). However, they might not capture the full complexity of MS and their interpretation requires a nuanced understanding of the disease context. Moreover, the heterogeneous nature of MS challenges the development of universally applicable biomarkers and complicates the tracking of different treatment effects on an individual basis (46).
Notably, with a variety of treatment options being available (27, 28), emerging biomarkers, including liquid and imaging markers, have shown potential in monitoring treatment efficacy (45, 47). However, the validation, availability, and implementation of biomarker assessments in real-world clinical practice is often still missing as this differs significantly from their application in clinical trials. Moreover, biomarkers that demonstrate both sensitivity and specificity in the context of progressive MS are still lacking (47). While early diagnosis and prognosis modelling are pivotal for timely and effective treatment initiation, the ability to clearly define and disentangle disability accumulation attributed to RAW or PIRA will be key to optimizing individual treatment over the course of the disease.
Advancements in artificial intelligence (AI) can offer enhanced and data-driven support by considering longitudinal data on multiple biomarkers simultaneously and subtyping patients more accurately. In particular, this can include biomarkers more related to PIRA such as motor dysfunction beyond EDSS (2, 48), optical coherence tomography (49–51), magnetic resonance imaging markers predictive of disability worsening such as brain atrophy (14), slowly expanding lesions and paramagnetic rim lesions (52–54) and cognitive impairment (55–57), as well as subjective markers [i.e. patient-reported outcomes (PROs) such as quality of live (58, 59)]. We believe that a holistic overview of the patient will be crucial to avoid overlooking relevant information, including both existing and new biomarkers as our disease understanding evolves further (Figure 1).
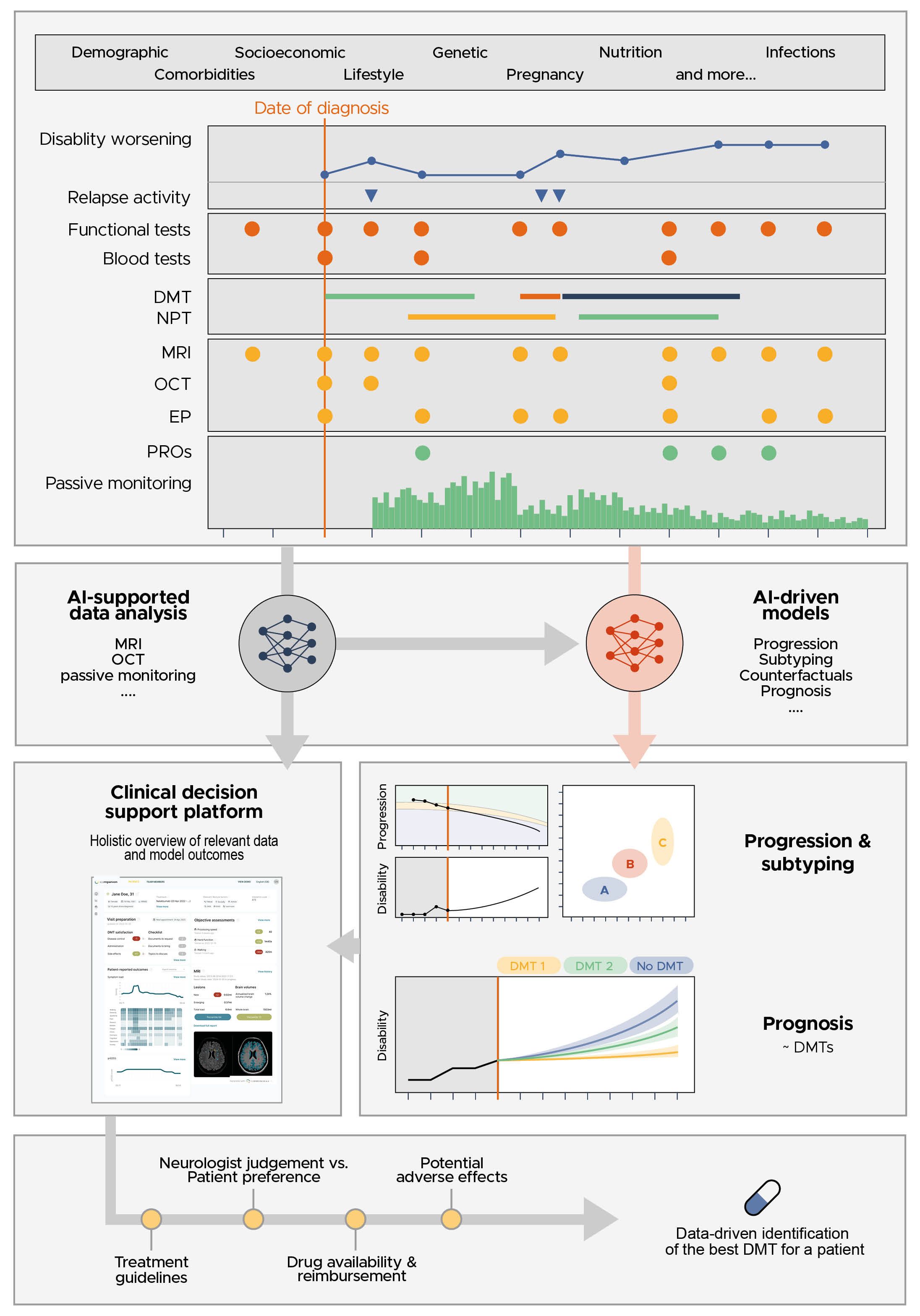
Figure 1. A clinical decision support tool should be capable of visualizing the very heterogenous MS patient data, the AI-supported analysis of this data and the outcome of prognostic models using this data, enabling a data-driven discussion between the neurologist and patient to identify the best DMT for the patient.
Such transformative approaches hold the potential to significantly enhance treatment strategies and extend the adjusted quality of life years for individuals with MS. Nevertheless, the current landscape is still fragmented, often focusing on singular aspects or biomarkers rather than adopting a more holistic and comprehensive approach. Data strategies to reduce the level of heterogeneity, particularly improving data harmonization by means of a common data model, are wishful to guarantee standardization in clinical decision making (60). However, the implementation of such initiatives is still in the early stages. Care pathways for pwMS are also not commonly standardized and while some diagnostic and treatment guidelines and recommendations are available (1, 61, 62), the assessment of relevant outcomes may not always be sufficiently covered and integrated into the routine clinical workflow (63). A modular-integrative framework of digital patient pathways for MS management and treatment is needed, which should incorporate AI, data harmonization and review relevant research concerning the use of pathways in healthcare (64, 65). Although initial evidence of acting upon AI-driven MRI biomarkers has indicated to improve patient outcome (66), the evaluation of impact in real-world practice and evidence on whether acting upon data-driven models and biomarkers truly improves the quality of life for patients with MS are crucial components that demand more attention in the pursuit of effective precision medicine strategies for MS.
4 Clinical impact through AI-assisted MS care
A data-driven and personalized clinical decision support tool is urgently needed for MS, to prevent and slow down disease progression more efficiently via optimizing treatment. The EU-funded ‘Clinical Impact through AI-assisted MS Care’ (CLAIMS, www.claims.ms) project aims to address this need. The project will develop, validate and seek regulatory approval for an AI-driven clinical decision-support platform, which offers the MS care team a holistic view of the patient through the visualization of all relevant patient data and the prognosis on the expected disease trajectories under different treatment regimens.
Initially, the project focusses on the development and optimization of these prognostic models via the use of retrospectively collected clinical routine data in combination with clinical trial data. A detailed description of this retrospective multi-center observational study (called RECLAIM) is accessible via ClincialTrials.gov. This study aims to collect and harmonize both clinical and subclinical data and store it in a central database on a secure cloud environment. Data harmonization will be following the common data model proposed in Parciak et al. (67), but kept to the minimum necessary as we aim to stay as close as possible to the real-world clinical setting and to ensure the clinical relevance.
The combination of real-world with clinical trial data is an important aspect of the study. Clinical trial data is very homogeneous and highly curated, making it an ideal dataset to develop AI-driven prognostic models. For instance, MRI scans obtained in clinical trials adhere to a standardized protocol, include all necessary sequences, and ensure follow-up scans within a specific timeframe. In contrast, MRI scans acquired in a real-world setting frequently don’t meet these requirements (68, 69). As the CLAIMS project aims to create AI-based prediction models applicable in real-world clinical settings, it is crucial to also incorporate routine care data in the development and validation phases. By combining both types of data, we aim to achieve an extensive dataset that leverages the strengths of both types of data ensuring applicability in a routine clinical care setting where confounding factors (e.g., comorbidities), low quality data and missing data are common (70, 71).
The focus will be on modelling disease progression. Disease progression models often have strong assumptions about the monotonicity of disease progression processes, the missingness model and associated completeness of the data, the longitudinal regularity of the observations, and homoscedastic noise characteristics of the measurements. Due to the different MS subtypes, and relapse and recurrence events, many of these assumptions do not hold in a MS setting. Furthermore, when using clinical observational data, data points are missing-not-at-random, both because patients often miss their appointments, but also because certain examinations (clinical assessments, MRI, etc) are performed as a function of patient presentation. Tackling this requires us to explore applicability of advanced and appropriate models of data imputation, and from generative models that explicitly model the causal relationships of the observations.
Contrary to clinical research trials where patients are assigned to a treatment or placebo arm at random, in an observational setting, DMTs are given to patients according to guideline recommendations and patient presentation. Observational data is thus biased by these guidelines, and appropriate measures are needed to control for this bias. Causal inference mechanisms via counterfactuals allows one to model such observational data and predict what the potential outcome would have been under a counterfactual treatment. By disentangling causes and effects, one gains a clearer understanding of the underlying biological or pathological markers that are predictive of the observed effect and outcome. This enables a more grounded clustering of patients (e.g., what are the patient characteristics that predict drug efficacy), providing an explanation of the optimal therapeutic inference (e.g., what is the biological reason why a certain drug is optimal for a specific patient). While some of these challenges have been addressed in highly controlled randomized clinical research environments, solving them using an observational experimental setup would allow one to exploit large amounts of data while ensuring the models remain accurate when deployed in a real-world environment where the aforementioned problems exist. Observational studies using real-world data allow for more heterogeneous and comprehensive cohorts, thereby elevating external validity and supplying valuable insights to guide treatment approaches (69).
At the time of writing this paper, the first version of the CLAIMS platform was already available, building upon a regulatory cleared AI solution for brain MRI quantification, a patient app for pwMS and a regulatory cleared AI solution for optical coherence tomography (OCT) quantification (72–75), but without the prognostic models (Figure 2). The complete clinical decision support platform, including the prognostic models, will be included in prospective clinical trial (called PROCLAIM), designed to obtain regulatory approval, and bringing it to the market as soon as possible. Meanwhile, the platform will be iteratively improved as new biomarker data becomes available and models are further refined. This iterative approach ensures that the CLAIMS project achieves true clinical impact for patients sooner rather than later.
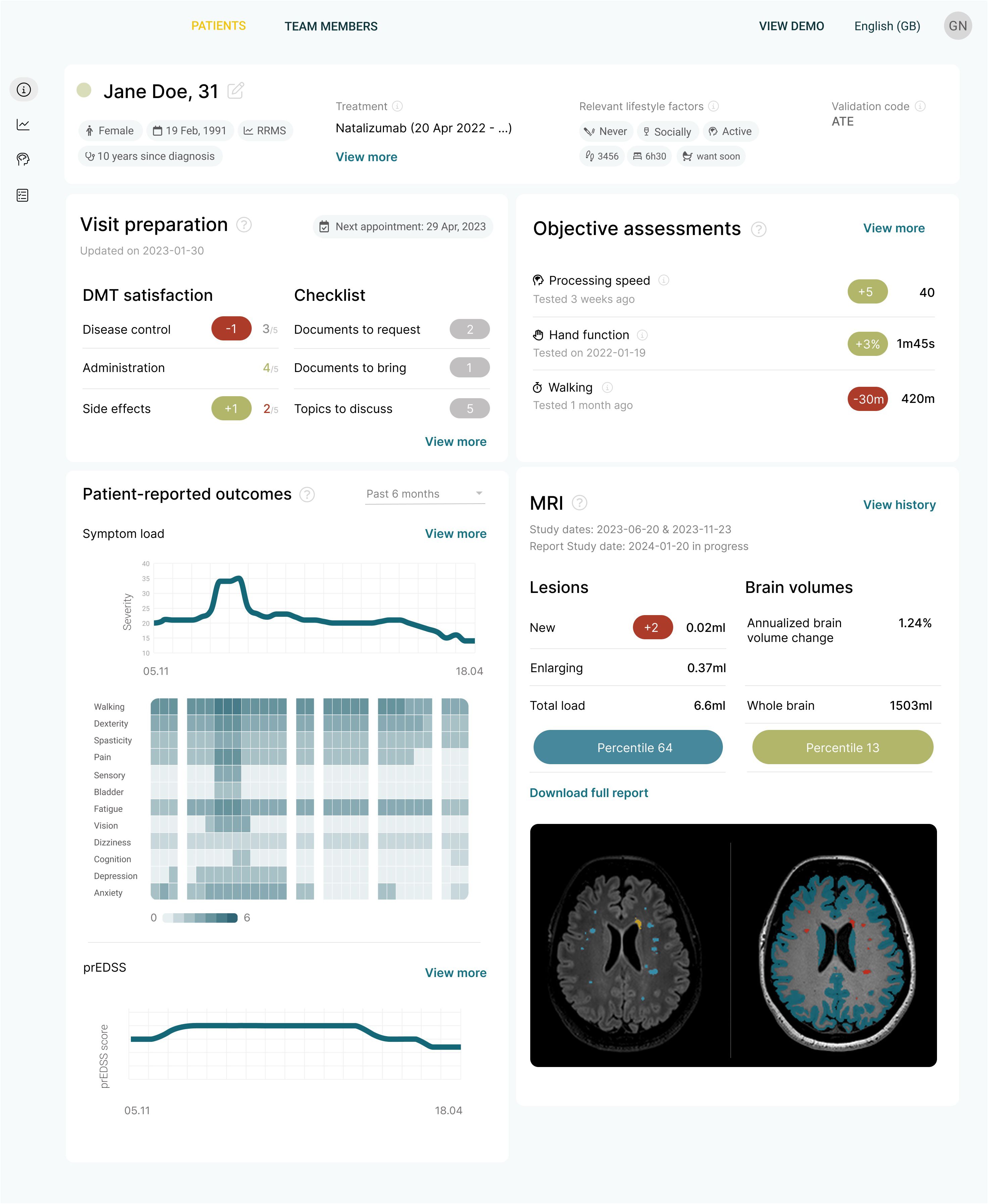
Figure 2. The first iteration of the clinical decision support platform being developed in the CLAIMS project. It offers a concise overview of the most important data for making a clinical decision.
5 Digital health and how this support prognosis
The CLAIMS project is exploring an additional avenue for the identification of promising markers of disease progression by capturing digital biomarkers using digital health tools. A first set of digital health tools includes AI solutions tailored for the quantification of brain MRI scans (74, 75). Notable advancement of these tools’ accuracy, in combination with rigorous technological, workflow, clinical and even initial health economic validation makes that this solution steadily gains recognition as standard of care. In the United States, this trend towards embracing AI-based brain MRI quantification is further exemplified by the recent provision of two new Current Procedural Terminology (CPT) codes. Evidence has shown that by using such a solution, disease activity can be detected up to 3 years earlier with a potentially significant impact on treatment decisions (66).
Patient apps, another major trend in the digital health tools, could enhance the early detection of disease progression in pwMS and allow monitoring disease progression in between visits with their treating physician. This can be achieved by monitoring symptoms and disability progression through capturing patient-reported outcomes (PROs), through passive monitoring of various markers (activity, sleep, vital signs, …) or through the digital administration of tests assessing for example cognition, vision, mobility, etc. (76, 77). In addition, these tools can play an important role in increasing and monitoring medication adherence, improving a patient’s lifestyle through creating awareness, and to educate and empower patients in managing their disease better. As such, disease monitoring via digital health tools provides a dynamic, more continuous, and more nuanced understanding of disease progression.
Development of such tools poses a socio-technical challenge. Any tool which aims to obtain regulatory clearance for use in a clinical setting will need to obtain sufficient technical and clinical evidence, which is often a long and laborious process. A bigger challenge, however, is patient adoption and thereafter adherence in using the tools. Concerns on data security and privacy need to be adequately addressed and simultaneously, it needs to be very clear to patients that they will benefit from enhanced care and personalized interventions driven by a more holistic understanding and monitoring of their health status and disease progression. CLAIMS aims to address this by empowering and educating patients on the need to better monitor their disease. In this light, the patient app used in CLAIMS is positioned as a companion app, available to support the patient as needed, focusing on topics of interest to the patient, rather than mandating the app usage. Actively involving patients and capturing their feedback on the app utilization, whether via real-world usage or within a clinical study setting, will contribute valuable insights, allowing to further refine the tools and ultimately, the clinical decision support platform.
Besides patient adherence, integration into routine clinical workflows poses another challenge. To address this, the clinical decision support platform in CLAIMS aims to keep the steps of platform adoption to a bare minimum. It aggregates all of a patient’s data, including data from the patient app, from the AI-driven MRI analysis and from the AI-driven OCT-analysis. While the full datasets and analyses will be available via this platform, the main dashboard focusses on providing a holistic overview of all clinically actionable measures and markers. While this is rather straightforward for subjective and episodic data such as with questionnaires or simple tests captured via the patient app, this will be harder to achieve for data from passive monitoring. The latter is known to generate large longitudinal datasets where AI algorithms are needed to identify subtle patterns and disease subtypes, and to predict trajectories.
Patient-reported outcomes (PROs) represent a unique occasion to involve patients using digital health tools and measure the impact of health care on outcomes that hold utmost significance to pwMS. However, the variety of PRO measures available and the absence of standards across different healthcare centers and countries present a considerable challenge (58). The recently established initiative ‘Patient-Reported Outcomes for Multiple Sclerosis’ (PROMS), consisting of an interdisciplinary, international network of different stakeholders, addresses the challenge of creating PRO measures that meet the diverse needs of all parties involved to enhance the influence of both scientific research and patient perspectives on the lives of pwMS (59). In this context, digital health tools enable meaningful assessments, but patient satisfaction can influence assessment compliance and indirectly affect outcome measures. To assess patient satisfaction with digital tools, patient-reported and expert-reported experience measures (PREM) should be collected in parallel (78).
6 The road ahead
As our understanding of MS increases, it becomes evident that we should go beyond making treatment decisions solely based on relapses, EDSS progression and lesion activity and move towards proactively treating pwMS for the best possible prognostic outcome. A focus on maintaining/improving health-related quality of life and slowing down disease progression and disability worsening - also independent of relapse activity - has sprouted a clear need for data-driven and personalized clinical decision support tools in MS. Such tools are crucial to administer the right drug to the right patient at the right time to preserve long-term neurological function while minimizing side effects. However, such solutions require well validated biomarkers and models that clearly link to the specificity of the disease course and outcome at individual patient level and can be easily implemented along the clinical care path of the patient.
The CLAIMS project aims to develop such a data-driven and personalized clinical decision support tool while addressing the posed challenges. Biomarker validation and model building will be performed in the retrospective RECLAIM study using both real world data and data from clinical trials. Subsequently, the prospective PROCLAIM study will evaluate the envisioned platform in daily clinical routine, evaluating feasibility and impact on patient care pathways and patient outcome. As such the project will generate a platform for daily clinical routine that provides a holistic view of each patient including existing and novel biomarker assessments to better monitor relapse related disability worsening and progression independent of relapse activity. Driven by deep-learning-based disease subtyping and progression models, the platform will allow the estimation of individual disease trajectories and as such contribute to the urgent need of a more pro-active and data-driven precision medicine in MS care.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author contributions
JP: Conceptualization, Funding acquisition, Project administration, Visualization, Writing – original draft, Writing – review & editing. LA: Conceptualization, Project administration, Writing – original draft, Writing – review & editing. GC: Conceptualization, Writing – review & editing. DH: Conceptualization, Writing – review & editing. TZ: Conceptualization, Writing – review & editing. PV: Conceptualization, Writing – review & editing. CL: Conceptualization, Writing – review & editing. KV: Conceptualization, Writing – review & editing. MS: Conceptualization, Writing – review & editing. CA: Conceptualization, Funding acquisition, Project administration, Writing – review & editing. EK: Conceptualization, Writing – review & editing. AB: Conceptualization, Writing – review & editing. JV: Conceptualization, Writing – review & editing. ED: Conceptualization, Writing – review & editing. VZ: Conceptualization, Writing – review & editing. DS: Conceptualization, Funding acquisition, Writing – review & editing. AR: Conceptualization, Funding acquisition, Project administration, Visualization, Writing – original draft, Writing – review & editing. FP: Conceptualization, Funding acquisition, Project administration, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The CLAIMS project is supported by the Innovative Health Initiative Joint Undertaking (JU) under grant agreement No 101112153. The JU receives support from the European Union’s Horizon Europe research and innovation program and COCIR, EFPIA, EuropaBio, MedTech Europe, Vaccines Europe, AB Science SA and Icometrix NV. This work was partially supported by an ITEA grant (20030 HeKDisco, HBC.2021.0500) from Flanders Innovation and Entrepreneurship. DH has received support from the Charles University Cooperation Program in Neuroscience, from the National Institute for Neurological Research (Program EXCELES, ID Project No. LX22NPO5107), from the European Union –Next Generation EU, and from the General University Hospital in Prague (project MH CZ-RVO-VFN64165).
Conflict of interest
JP is a shareholder of icometrix NV. AR is a shareholder of icometrix NV. DS is a shareholder of icometrix NV. MS has no relevant or material financial interests that relate to the research described in this paper. However, she is employed as Operational Director of The European Charcot Foundation. TZ reports scientific advisory board and/or consulting for Biogen, Roche, Novartis, Celgene, and Merck; compensation for serving on speaker’s bureaus for Roche, Novartis, Merck, Sanofi, Celgene, and Biogen; and research support from Biogen, Novartis, Merck, and Sanofi. VZ is a shareholder of F. Hoffmann-La Roche Ltd PV reports honorarium, contributions to meeting from Biogen, Sanofi-Genzyme, Novartis, Teva, Merck, Roche, Imcyse, AB Science, Janssen, Ad Scientiam and BMS-Celgene. Research support from Novartis, Sanofi-Genzyme and Merck. EK is a shareholder of Nocturne GmbH. DH received compensation for travel, speaker honoraria and consultant fees from Biogen Idec, Novartis, Merck, Bayer, Sanofi Genzyme, Roche, and Teva, as well as support for research activities from Biogen Idec. JR is a shareholder of Imcyse SA. GC has received consulting and speaking fees from Novartis, Sanofi, Janssen, Bristol Myers Squibb, Roche and Rewind. FP provided research support to Neurosciences Clinical Research Center, German Ministry for Education and Research (BMBF), Deutsche Forschungsgemeinschaft (DFG), Einstein Foundation, Guthy Jackson Charitable Foundation, EU FP7 Framework Program, Biogen, Genzyme, Merck Serono, Novartis, Bayer, Roche, Parexel and Almirall, received honoraria for lectures, presentations, speakers from Guthy Jackson Foundation, Bayer, Biogen, Merck Serono, Sanofi Genzyme, Novartis, Viela Bio, Roche, UCB, Mitsubishi Tanabe and Celgene, in addition, received compensation for serving on a scientific advisory board of Celgene, Roche, UCB and Merck, and is an Academic Editor of PLos One and Associate Editor of Neurology® Neuroimmunology & Neuroinflammation, all unrelated to this work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. (2018) 17:162–73. doi: 10.1016/s1474-4422(17)30470-2
2. Tur C, Carbonell-Mirabent P, Cobo-Calvo A, Otero-Romero S, Arrambide G, Midaglia L, et al. Association of early progression independent of relapse activity with long-term disability after a first demyelinating event in multiple sclerosis. JAMA Neurol. (2023) 80:151. doi: 10.1001/jamaneurol.2022.4655
3. Kobelt G, Berg J, Lindgren P, Jönsson B. Costs and quality of life in multiple sclerosis in Europe: method of assessment and analysis. Eur J Health Econ. (2006) 7:5–13. doi: 10.1007/s10198-006-0365-y
4. Tutuncu M, Tang J, Zeid NA, Kale N, Crusan DJ, Atkinson EJ, et al. Onset of progressive phase is an age-dependent clinical milestone in multiple sclerosis. Multiple Sclerosis. (2013) 19:188–98. doi: 10.1177/1352458512451510
5. Lublin FD, Reingold SC, Cohen JA, Cutter GR, Sørensen PS, Thompson AJ, et al. Defining the clinical course of multiple sclerosis. Neurology. (2014) 83:278–86. doi: 10.1212/wnl.0000000000000560
6. Kuhlmann T, Moccia M, Coetzee T, Cohen JA, Correale J, Graves J, et al. Multiple sclerosis progression: time for a new mechanism-driven framework. Lancet Neurol. (2023) 22:78–88. doi: 10.1016/s1474-4422(22)00289-7
7. Marrie RA, Horwitz RI, Cutter G, Tyry T, Vollmer T. Association between comorbidity and clinical characteristics of MS. Acta Neurol Scand. (2011) 124:135–41. doi: 10.1111/j.1600-0404.2010.01436.x
8. Marrie RA, Cohen JA, Stuve O, Trojano M, Sørensen PS, Reingold S, et al. A systematic review of the incidence and prevalence of comorbidity in multiple sclerosis: Overview. Multiple Sclerosis. (2015) 21:263–81. doi: 10.1177/1352458514564491
9. Lublin FD, Häring DA, Ganjgahi H, Ocampo A, Hatami F, Čuklina E, et al. How patients with multiple sclerosis acquire disability. Brain. (2022) 145:3147–61. doi: 10.1093/brain/awac016
10. Kappos L, Wolinsky JS, Giovannoni G, Arnold DL, Wang Q, Bernasconi C, et al. Contribution of relapse-independent progression vs relapse-associated worsening to overall confirmed disability accumulation in typical relapsing multiple sclerosis in a pooled analysis of 2 randomized clinical trials. JAMA Neurol. (2020) 77:1132. doi: 10.1001/jamaneurol.2020.1568
11. Portaccio E, Bellinvia A, Fonderico M, Pastò L, Razzolini L, Totaro R, et al. Progression is independent of relapse activity in early multiple sclerosis: a real-life cohort study. Brain. (2022) 145:2796–805. doi: 10.1093/brain/awac111
12. Lassmann H. Targets of therapy in progressive MS. Multiple Sclerosis. (2017) 23:1593–9. doi: 10.1177/1352458517729455
13. Lassmann H. Pathogenic mechanisms associated with different clinical courses of multiple sclerosis. Front Immunol. (2019) 9:3116. doi: 10.3389/fimmu.2018.03116
14. Cagol A, Schaedelin S, Barakovic M, Benkert P, Todea RA, Rahmanzadeh R, et al. Association of brain atrophy with disease progression independent of relapse activity in patients with relapsing multiple sclerosis. JAMA Neurol. (2022) 79:682. doi: 10.1001/jamaneurol.2022.1025
15. Bischof A, Papinutto N, Keshavan A, Rajesh A, Kirkish G, Zhang X, et al. Spinal cord atrophy predicts progressive disease in relapsing multiple sclerosis. Ann Neurol. (2022) 91:268–81. doi: 10.1002/ana.26281
16. Cagol A, Benkert P, Melie-Garcia L, Schaedelin SA, Leber S, Tsagkas C, et al. Association of spinal cord atrophy and brain paramagnetic rim lesions with progression independent of relapse activity in people with MS. Neurology. (2024) 102:e207768. doi: 10.1212/wnl.0000000000207768
17. UCA San Francisco MS-EPIC Team, Bruce ACC, Hollenbach JA, Bove R, Kirkish G, Sacco S, et al. Silent progression in disease activity–free relapsing multiple sclerosis. Ann Neurol. (2019) 85:653–66. doi: 10.1002/ana.25463
18. Krieger SC, Cook K, De Nino S, Fletcher M. The topographical model of multiple sclerosis. Neurology® Neuroimmunol Neuroinflamm. (2016) 3:e279. doi: 10.1212/nxi.0000000000000279
19. Krieger SC, Billiet T, Maes C, Barros N, Ribbens A, Wang C, et al. MSMilan2023 – paper poster - session 1' (2023). Multiple Sclerosis. (2023) 29:137–393. doi: 10.1177/13524585231196192
20. Krieger SC, Antoine A, Sumowski JF. EDSS 0 is not normal: Multiple sclerosis disease burden below the clinical threshold. Multiple Sclerosis. (2022) 28:2299–303. doi: 10.1177/13524585221108297
21. Runia TF, Jafari N, Siepman DAM, Hintzen RQ. Fatigue at time of CIS is an independent predictor of a subsequent diagnosis of multiple sclerosis. J Neurol Neurosurg Psychiatry. (2015) 86:543–6. doi: 10.1136/jnnp-2014-308374
22. Paul F. Pathology and MRI: exploring cognitive impairment in MS. Acta Neurol Scand. (2016) 134:24–33. doi: 10.1111/ane.12649
23. Kalincik T, Manouchehrinia A, Sobisek L, Jokubaitis V, Spelman T, Horakova D, et al. Towards personalized therapy for multiple sclerosis: prediction of individual treatment response. Brain. (2017) 140:2426–43. doi: 10.1093/brain/awx185
24. Montalban X, Gold R, Thompson AJ, Otero-Romero S, Amato MP, Chandraratna D, et al. ECTRIMS/EAN Guideline on the pharmacological treatment of people with multiple sclerosis. Multiple Sclerosis J. (2018) 24:96–120. doi: 10.1177/1352458517751049
25. Wingerchuk DM, Carter JL. Multiple sclerosis: current and emerging disease-modifying therapies and treatment strategies. Mayo Clin Proc. (2014) 89:225–40. doi: 10.1016/j.mayocp.2013.11.002
26. Gasperini C, Prosperini L, Tintoré M, Sormani MP, Filippi M, Rio J, et al. Unraveling treatment response in multiple sclerosis. Neurology. (2019) 92:180–92. doi: 10.1212/wnl.0000000000006810
27. Amin M, Hersh CM. Updates and advances in multiple sclerosis neurotherapeutics. Neurodegenerative Dis Manage. (2023) 13:47–70. doi: 10.2217/nmt-2021-0058
28. Bayas A, Christ M, Faissner S, Klehmet J, Pul R, Skripuletz T, et al. Disease-modifying therapies for relapsing/active secondary progressive multiple sclerosis – a review of population-specific evidence from randomized clinical trials. Ther Adv Neurol Disord. (2023) 16:175628642211468. doi: 10.1177/17562864221146836
29. Visser LH, Van Der Zande A. Reasons patients give to use or not to use immunomodulating agents for multiple sclerosis. Eur J Neurol. (2011) 18:1343–9. doi: 10.1111/j.1468-1331.2011.03411.x
30. Jokubaitis VG, Spelman T, Lechner-Scott J, Barnett M, Shaw C, Vucic S, et al. The Australian Multiple Sclerosis (MS) Immunotherapy Study: A prospective, multicentre study of drug utilisation using the MSBase platform. PloS One. (2013) 8:e59694. doi: 10.1371/journal.pone.0059694
31. Saposnik G, Andhavarapu S, de la Maza SS, Castillo-Triviño T, Borges M, Barón BP, et al. Delayed cognitive processing and treatment status quo bias in early-stage multiple sclerosis. Multiple Sclerosis Related Disord. (2022) 68:104138. doi: 10.1016/j.msard.2022.104138
32. Giovannoni G, Butzkueven H, Dhib-Jalbut S, Hobart J, Kobelt G, Pepper G, et al. Brain health: time matters in multiple sclerosis. Multiple Sclerosis Related Disord. (2016) 9:S5–S48. doi: 10.1016/j.msard.2016.07.003
33. Inojosa H, Proschmann U, Akgün K, Ziemssen T. The need for a strategic therapeutic approach: multiple sclerosis in check. Ther Adv Chronic Dis. (2022) 13:204062232110630. doi: 10.1177/20406223211063032
34. Harding K, Williams O, Willis M, Hrastelj J, Rimmer A, Joseph F, et al. Clinical outcomes of escalation vs early intensive disease-modifying therapy in patients with multiple sclerosis. JAMA Neurol. (2019) 76:536. doi: 10.1001/jamaneurol.2018.4905
35. Buron MD, Chalmer TA, Sellebjerg F, Barzinji I, Bech D, Christensen JR, et al. Initial high-efficacy disease-modifying therapy in multiple sclerosis. Neurology. (2020) 95:e1041–51. doi: 10.1212/wnl.0000000000010135
36. Simpson A, Mowry EM, Newsome SD. Early aggressive treatment approaches for multiple sclerosis. Curr Treat Options Neurol. (2021) 23:19. doi: 10.1007/s11940-021-00677-1
37. Spelman T, Magyari M, Piehl F, Svenningsson A, Rasmussen PV, Kant M, et al. Treatment escalation vs immediate initiation of highly effective treatment for patients with relapsing-remitting multiple sclerosis. JAMA Neurol. (2021) 78:1197. doi: 10.1001/jamaneurol.2021.2738
38. Freeman L, Longbrake EE, Coyle PK, Hendin B, Vollmer T. High-efficacy therapies for treatment-naïve individuals with relapsing–remitting multiple sclerosis. CNS Drugs. (2022) 36:1285–99. doi: 10.1007/s40263-022-00965-7
39. Weideman AM, Tapia-Maltos MA, Johnson K, Greenwood M, Bielekova B. Meta-analysis of the age-dependent efficacy of multiple sclerosis treatments. Front Neurol. (2017) 8:577. doi: 10.3389/fneur.2017.00577
40. He A, Merkel B, Brown JWL, Ryerson LZ, Kister I, Malpas CB, et al. Timing of high-efficacy therapy for multiple sclerosis: a retrospective observational cohort study. Lancet Neurol. (2020) 19:307–16. doi: 10.1016/s1474-4422(20)30067-3
41. Krämer J, Bar-Or A, Turner TJ, Wiendl H. Bruton tyrosine kinase inhibitors for multiple sclerosis. Nat Rev Neurol. (2023) 19:289–304. doi: 10.1038/s41582-023-00800-7
42. Hult KJ. Measuring the potential health impact of personalized medicine: evidence from multiple sclerosis treatments. In: Economic Dimensions of Personalized and Precision Medicine (2019) (Chicago, USA: University of Chicago Press). p. 185–216. doi: 10.7208/chicago/9780226611235.003.0008
43. Van Wijmeersch B, Hartung HP, Vermersch P, Pugliatti M, Pozzilli C, Grigoriadis N, et al. Using personalized prognosis in the treatment of relapsing multiple sclerosis: A practical guide. Front Immunol. (2022) 13:991291. doi: 10.3389/fimmu.2022.991291
44. Marrie RA, Fisk JD, Fitzgerald K, Kowalec K, Maxwell C, Rotstein D, et al. Etiology, effects and management of comorbidities in multiple sclerosis: recent advances. Front Immunol. (2023) 14:1197195. doi: 10.3389/fimmu.2023.1197195
45. Yang J, Hamade M, Wu Q, Wang Q, Axtell R, Giri S, et al. Current and future biomarkers in multiple sclerosis. Int J Mol Sci. (2022) 23:5877. doi: 10.3390/ijms23115877
46. Voigt I, Inojosa H, Wenk J, Akgün K, Ziemssen T. Building a monitoring matrix for the management of multiple sclerosis. Autoimmun Rev. (2023) 22:103358. doi: 10.1016/j.autrev.2023.103358
47. Gill AJ, Schorr EM, Gadani SP, Calabresi PA. Emerging imaging and liquid biomarkers in multiple sclerosis. Eur J Immunol. (2023) 53:2250228. doi: 10.1002/eji.202250228
48. Trentzsch K, Schumann P, Śliwiński G, Bartscht P, Haase R, Schriefer D, et al. Using machine learning algorithms for identifying gait parameters suitable to evaluate subtle changes in gait in people with multiple sclerosis. Brain Sci. (2021) 11:1049. doi: 10.3390/brainsci11081049
49. Guerrieri S, Comi G, Leocani L. Optical coherence tomography and visual evoked potentials as prognostic and monitoring tools in progressive multiple sclerosis. Front Neurosci. (2021) 15:692599. doi: 10.3389/fnins.2021.692599
50. Paul F, Calabresi PA, Barkhof F, Green AJ, Kardon R, Sastre-Garriga J, et al. Optical coherence tomography in multiple sclerosis: A 3-year prospective multicenter study. Ann Clin Trans Neurol. (2021) 8:2235–51. doi: 10.1002/acn3.51473
51. Graves JS. Identifying multiple sclerosis activity. Neurology. (2022) 99:269–70. doi: 10.1212/wnl.0000000000200903
52. Absinta M, Sati P, Masuzzo F, Nair G, Sethi V, Kolb H, et al. Association of chronic active multiple sclerosis lesions with disability in vivo. JAMA Neurol. (2019) 76:1474. doi: 10.1001/jamaneurol.2019.2399
53. Blindenbacher N, Brunner E, Asseyer S, Scheel M, Siebert N, Rasche L, et al. Evaluation of the ‘ring sign’ and the ‘core sign’ as a magnetic resonance imaging marker of disease activity and progression in clinically isolated syndrome and early multiple sclerosis. Multiple Sclerosis J - Exp Trans Clin. (2020) 6:205521732091548. doi: 10.1177/2055217320915480
54. Preziosa P, Pagani E, Meani A, Moiola L, Rodegher M, Filippi M, et al. Slowly expanding lesions predict 9-Year multiple sclerosis disease progression. Neurology® Neuroimmunol Neuroinflamm. (2022) 9:e1139. doi: 10.1212/nxi.0000000000001139
55. Oreja-Guevara C, Blanco TA, Ruiz LB, Pérez MAH, Meca-Lallana V, Ramió-Torrentà L. Cognitive dysfunctions and assessments in multiple sclerosis. Front Neurol. (2019) 10:581. doi: 10.3389/fneur.2019.00581
56. Podda J, Ponzio M, Pedullà L, Bragadin MM, Battaglia MA, Zaratin P, et al. Predominant cognitive phenotypes in multiple sclerosis: Insights from patient-centered outcomes. Multiple Sclerosis Related Disord. (2021) 51:102919. doi: 10.1016/j.msard.2021.102919
57. Carotenuto A, Costabile T, Pontillo G, Moccia M, Falco F, Petracca M, et al. Cognitive trajectories in multiple sclerosis: a long-term follow-up study. Neurol Sci. (2021) 43:1215–22. doi: 10.1007/s10072-021-05356-2
58. Brichetto G, Zaratin P. Measuring outcomes that matter most to people with multiple sclerosis: the role of patient-reported outcomes. ' Curr Opin Neurol. (2020) 33:295–9. doi: 10.1097/wco.0000000000000821
59. Zaratin P, Vermersch P, Amato MP, Brichetto G, Coetzee T, Cutter G, et al. The agenda of the global patient reported outcomes for multiple sclerosis (PROMS) initiative: Progresses and open questions. Multiple Sclerosis Related Disord. (2022) 61:103757. doi: 10.1016/j.msard.2022.103757
60. Peeters LM, Parciak T, Kalra D, Moreau Y, Kasilingam E, van Galen P, et al. Multiple Sclerosis Data Alliance – A global multi-stakeholder collaboration to scale-up real world data research. Multiple Sclerosis Related Disord. (2021) 47:102634. doi: 10.1016/j.msard.2020.102634
61. Yamout B, Sahraian M, Bohlega S, Al-Jumah M, Goueider R, Dahdaleh M, et al. Consensus recommendations for the diagnosis and treatment of multiple sclerosis: 2019 revisions to the MENACTRIMS guidelines. Multiple Sclerosis Related Disord. (2020) 37:101459. doi: 10.1016/j.msard.2019.101459
62. Wattjes MP, Ciccarelli O, Reich DS, Banwell B, de Stefano N, Enzinger C, et al. 2021 MAGNIMS–CMSC–NAIMS consensus recommendations on the use of MRI in patients with multiple sclerosis. Lancet Neurol. (2021) 20:653–70. doi: 10.1016/s1474-4422(21)00095-8
63. Tur C, Moccia M, Barkhof F, Chataway J, Sastre-Garriga J, Thompson AJ, et al. Assessing treatment outcomes in multiple sclerosis trials and in the clinical setting. Nat Rev Neurol. (2018) 14:75–93. doi: 10.1038/nrneurol.2017.171
64. Voigt I, Benedict M, Susky M, Scheplitz T, Frankowitz S, Kern R, et al. A digital patient portal for patients with multiple sclerosis. Front Neurol. (2020) 11:400. doi: 10.3389/fneur.2020.00400
65. Wenk J, Voigt I, Inojosa H, Schlieter H, Ziemssen T. Building digital patient pathways for the management and treatment of multiple sclerosis. Front Immunol. (2024) 15:1356436. doi: 10.3389/fimmu.2024.1356436
66. Sima DM, Esposito G, Van Hecke W, Ribbens A, Nagels G, Smeets D. Health economic impact of software-assisted brain MRI on therapeutic decision-making and outcomes of relapsing-remitting multiple sclerosis patients—A microsimulation study. Brain Sci. (2021) 11:1570. doi: 10.3390/brainsci11121570
67. Parciak T, Geys L, Helme A, van der Mei I, Hillert J, Schmidt H, et al. Introducing a core dataset for real-world data in multiple sclerosis registries and cohorts: Recommendations from a global task force. Multiple Sclerosis. (2023) 30:396–418. doi: 10.1177/13524585231216004
68. Sastre-Garriga J, Pareto D, Battaglini M, Rocca MA, Ciccarelli O, Enzinger C, et al. MAGNIMS consensus recommendations on the use of brain and spinal cord atrophy measures in clinical practice. Nat Rev Neurol. (2020) 16:171–82. doi: 10.1038/s41582-020-0314-x
69. Aboseif A, Roos I, Krieger SC, Kalincik T, Hersh CM. Leveraging Real-World evidence and observational studies in treating multiple sclerosis. Neurol Clinics. (2024) 42:203–27. doi: 10.1016/j.ncl.2023.06.003
70. Katkade VB, Sanders KN, Zou KH. Real world data: an opportunity to supplement existing evidence for the use of long-established medicines in health care decision making. J Multidiscip Healthcare. (2018) 11:295–304. doi: 10.2147/jmdh.s160029
71. Vercruyssen S, Brys A, Verheijen M, Steach B, Van Vlierberge E, Sima DM, et al. Abstracts from the 34th annual meeting of the consortium of multiple sclerosis centers. Int J MS Care. (2020) 22:1–116. doi: 10.7224/1537-2073-22.s2.1
72. Yadav SK, Motamedi S, Oberwahrenbrock T, Oertel FC, Polthier K, Paul F, et al. CuBe: parametric modeling of 3D foveal shape using cubic Bézier. Biomed Optics Express. (2017) 8:4181. doi: 10.1364/boe.8.004181
73. Yadav SK, Kadas EM. Optic nerve head three-dimensional shape analysis. J Biomed Optics. (2018) 23:1. doi: 10.1117/1.jbo.23.10.106004
74. Rakić M, Vercruyssen S, Van Eyndhoven S, de la Rosa E, Jain S, Van Huffel S, et al. 'icobrain ms 5.1: Combining unsupervised and supervised approaches for improving the detection of multiple sclerosis lesions. NeuroImage Clin. (2021) 31:102707. doi: 10.1016/j.nicl.2021.102707
75. Van Hecke W, Costers L, Descamps A, Ribbens A, Nagels G, Smeets D, et al. A novel digital care management platform to monitor clinical and subclinical disease activity in multiple sclerosis. Brain Sci. (2021) 11:1171. doi: 10.3390/brainsci11091171
76. Dillenseger A, Weidemann ML, Trentzsch K, Inojosa H, Haase R, Schriefer D, et al. Digital biomarkers in multiple sclerosis. Brain Sci. (2021) 11:1519. doi: 10.3390/brainsci11111519
77. Voigt I, Inojosa H, Dillenseger A, Haase R, Akgün K, Ziemssen T. Digital twins for multiple sclerosis. Front Immunol. (2021) 12:669811. doi: 10.3389/fimmu.2021.669811
Keywords: multiple sclerosis, personalized medicine, disease progression, prognosis, diagnosis, AI, data
Citation: Praet J, Anderhalten L, Comi G, Horakova D, Ziemssen T, Vermersch P, Lukas C, van Leemput K, Steppe M, Aguilera C, Kadas EM, Bertrand A, van Rampelbergh J, de Boer E, Zingler V, Smeets D, Ribbens A and Paul F (2024) A future of AI-driven personalized care for people with multiple sclerosis. Front. Immunol. 15:1446748. doi: 10.3389/fimmu.2024.1446748
Received: 10 June 2024; Accepted: 11 July 2024;
Published: 19 August 2024.
Edited by:
Yolanda Aladro, European University of Madrid, SpainReviewed by:
Giulia Sancesario, Santa Lucia Foundation (IRCCS), ItalyCopyright © 2024 Praet, Anderhalten, Comi, Horakova, Ziemssen, Vermersch, Lukas, van Leemput, Steppe, Aguilera, Kadas, Bertrand, van Rampelbergh, de Boer, Zingler, Smeets, Ribbens and Paul. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jelle Praet, amVsbGUucHJhZXRAaWNvbWV0cml4LmNvbQ==
†These authors have contributed equally to this work