 Patrick-Pascal Strunz1*†‡
Patrick-Pascal Strunz1*†‡ Linus Maximilian Risser2†‡
Linus Maximilian Risser2†‡ Matthias Englbrecht3‡
Matthias Englbrecht3‡ Torsten Witte2‡Matthias Froehlich1‡
Torsten Witte2‡Matthias Froehlich1‡ Marc Schmalzing1‡
Marc Schmalzing1‡ Michael Gernert1‡
Michael Gernert1‡ Sebastian Hueper4‡Peter Bartz-Bazzanella5,6,7‡Cay von der Decken5,6,7,8‡Kirsten Karberg7,9‡Georg Gauler7,10‡
Sebastian Hueper4‡Peter Bartz-Bazzanella5,6,7‡Cay von der Decken5,6,7,8‡Kirsten Karberg7,9‡Georg Gauler7,10‡ Susanna Späthling-Mestekemper7,11‡Christoph Kuhn7,12‡Wolfgang Vorbrüggen7,8‡Martin Welcker7,13‡
Susanna Späthling-Mestekemper7,11‡Christoph Kuhn7,12‡Wolfgang Vorbrüggen7,8‡Martin Welcker7,13‡ Stefan Kleinert1,7,14‡
Stefan Kleinert1,7,14‡- 1University Hospital of Würzburg, Department of Medicine II, Rheumatology/Clinical Immunology, Würzburg, Germany
- 2Medical School Hannover, Department of Rheumatology and Immunology, Hannover, Germany
- 3Freelance Healthcare Data Scientist, Greven, Germany
- 4Praxis für Rheumatologie und Osteologie, Hildesheim, Germany
- 5Klinik für Internistische Rheumatologie, Rhein-Maas-Klinikum, Würselen, Germany
- 6Medizinisches Versorgungszentrum, Stolberg, Germany
- 7RHADAR – RheumaDatenRheport GbR, Planegg, Germany
- 8Verein zur Förderung der Rheumatologie e.V., Würselen, Germany
- 9Rheumatologisches Versorgungszentrum Steglitz, Berlin, Germany
- 10Rheumatology Practice, Osnabrück, Germany
- 11Rheumapraxis München, Munich, Germany
- 12Praxis für Rheumatologie, Karlsruhe, Germany
- 13Medizinisches Versorgungszentrum für Rheumatologie Dr. M. Welcker GmbH, Planegg, Germany
- 14Praxisgemeinschaft Rheumatologie-Nephrologie, Erlangen, Germany
Background: Safety recommendations for Janus kinase inhibitors (JAKi) issued by the European Medical Agency (EMA) in 2023 could potentially influence treatment patterns for rheumatoid arthritis (RA) drugs, but little is known about the impact of these recommendations in routine clinical care.
Methods: We retrospectively analyzed the German RHADAR rheumatology database for adult patients with RA and documentation of a new therapy with a JAKi, tumor necrosis factor inhibitor (TNFi), or interleukin-6 receptor inhibitor (IL-6Ri). Data were grouped into half-yearly intervals from quarter (Q)2/2020 to Q3/2023. The period from Q4/2022 to Q1/2023 immediately followed the initial EMA endorsement of Pharmacovigilance Risk Assessment Committee (PRAC) recommendations and Q2/2023-Q3/2023 immediately followed the direct healthcare provider communication (DHPC) containing the new safety JAKi recommendations.
Results: Between April 1, 2020 and September 23, 2023, 3008 newly initiated therapies for TNFi (1499 [49.8%]), JAKi (1126 [37.4%]), and IL-6Ri (383 [12.7%]) were documented by the treating physicians. JAKi were increasingly used in the first two half-year periods (from 29.7% of these therapies in Q2/2020-Q3/2020 to 46.7% in Q2/2021-Q3/2021; odds ratio [OR] 2.08; p<0.001). The proportion of initiated JAKi therapies decreased significantly after the PRAC recommendations (32.9%; OR vs peak 0.56; p=0.001) and the DHPC letter (26.1%; OR vs peak 0.40; p<0.001). JAKi were more likely to be used as >3rd-line therapy in later time periods.
Conclusions: This exploratory study suggests that EMA safety recommendations for JAKi influenced treatment patterns of RA patients who received JAKi in Germany. Additional studies will be needed to confirm these findings.
1 Introduction
Janus kinase inhibitors (JAKi) play a key role in the management of chronic immune-mediated disorders. Tofacitinib was approved by the European Medicines Agency (EMA) in 2017 for rheumatoid arthritis (RA) and was soon joined by other drugs in this class, including baricitinib, upadacitinib, and filgotinib. Although these agents all affect the JAK/STAT pathway, they vary in their selectivity for different kinases and cell types (1).
The manufacturers of tofacitinib were required to conduct a post-approval safety trial. The resulting ORAL Surveillance Study, which was published in January 2022, found that tofacitinib was associated with significantly higher rates of major adverse cardiovascular events, cancers, and opportunistic infections compared with tumor necrosis factor inhibitors (TNFi) in RA patients ≥50 years with ≥1 cardiovascular risk factor (2). Based on these data, regulatory agencies strengthened safety recommendations for all JAKi. On November 11, 2022, the EMA endorsed recommendations from the Pharmacovigilance Risk Assessment Committee (PRAC) stating that JAKi should only be used if no suitable treatment alternatives are available in patients 65 years or older, at increased risk of major cardiovascular problems or cancer, or current or long-term past smokers, and should be used with caution in patients at risk for venous thromboembolism (3). A direct healthcare professional communication (DHPC) with this information was sent to clinicians in Europe on March 30, 2023 (4).
The effect of these regulatory changes on rheumatology treatment practices has not been well studied. We used the German RHADAR rheumatology database (5) to assess the proportions of patients initiating therapy with JAKi, TNFi, or an interleukin-6 receptor inhibitor (IL-6Ri) across time periods spanning before and immediately after the regulatory changes.
2 Methods
2.1 Study design
This exploratory study was a non-interventional, retrospective analysis of pseudonymized data collected during routine clinical care from adult patients (≥18 years) in the RheumaDatenRhePort (RHADAR) GbR (A Network of Rheumatologists) database, which includes patients seen at German clinical rheumatology sites (5).
Data were evaluated in half-year intervals (two quarters ([Q]; Q2–Q3=April 1 to September 30; Q4–Q1=October 1 to March 31) over the following time periods:
● Before PRAC recommendations: Q2/2020–Q3/2020; Q4/2020–Q1/2021; Q2/2021–Q3/2021; Q4/2021–Q1/2022; Q2/2022–Q3/2022
● After PRAC recommendations: Q4/2022–Q1/2023
● After DHPC: Q2/2023–Q3/2023 (ending September 23, 2023)
All patients gave prior written informed consent for evaluation within the RHADAR database. Included patients had a diagnosis of RA and documentation of the initiation of treatment with a JAKi, TNFi, or IL-6Ri between April 1, 2020 and September 23, 2023; no other selection criteria were applied. Data on patient characteristics and therapies were collected as part of routine care.
A draft of the study was submitted to the Ethics Committee of the Hannover Medical School (Application 11291_BO_K_2024), which advised that the retrospective analysis of anonymized clinical data did not require ethical approval according to German law.
2.2 Outcomes
We evaluated patient characteristics, initiation of specified new treatments, and line of therapy as included in patient documentation during routine clinical care. Relevant comorbidities related to the PRAC/EMA safety recommendations (cardiovascular risk factors and malignancy) were based on ICD-10 codes and included comorbidities recorded in the database at any point in time.
2.3 Statistical analysis
A study size calculation was not performed due to the retrospective nature of the study. Sample size was determined by all available prescriptions in the registry during the observational period.
We analyzed descriptive data for patients with reported data; missing data were not imputed. For sample characterization, we used absolute and relative frequencies and means with standard deviation (SD). To evaluate changes in the proportion of JAKi therapies over time, we used odds ratios (OR) and 95% confidence intervals (CIs) with adjusted p values derived by the Benjamini-Hochberg method (6). Statistical significance was set at p ≤ 0.05. Statistical analyses were performed using R software (version 4.3.0), RStudio (version 1.1.453), and Prism Version 5.
3 Results
3.1 Initiation of new therapies and patient characteristics
Between April 1, 2020 and September 23, 2023, 3008 new therapies with a JAKi, TNFi, or IL6-Ri were documented in the RHADAR database. The TNFi drug class was initiated most frequently (1499 [49.8%]) followed by JAKi (1126 [37.4%]) and IL-6Ri (383 [12.7%]). Baseline characteristics and comorbidity profiles by drug class were generally similar (Table 1). Patients receiving treatment with TNFi were slightly younger (mean of 56.6 years) than those receiving treatment with JAKi (60.4 years) or IL-6Ri (61.8 years) and had a shorter disease duration (mean of 11.7 years) than those treated with JAKi (13.7 years).
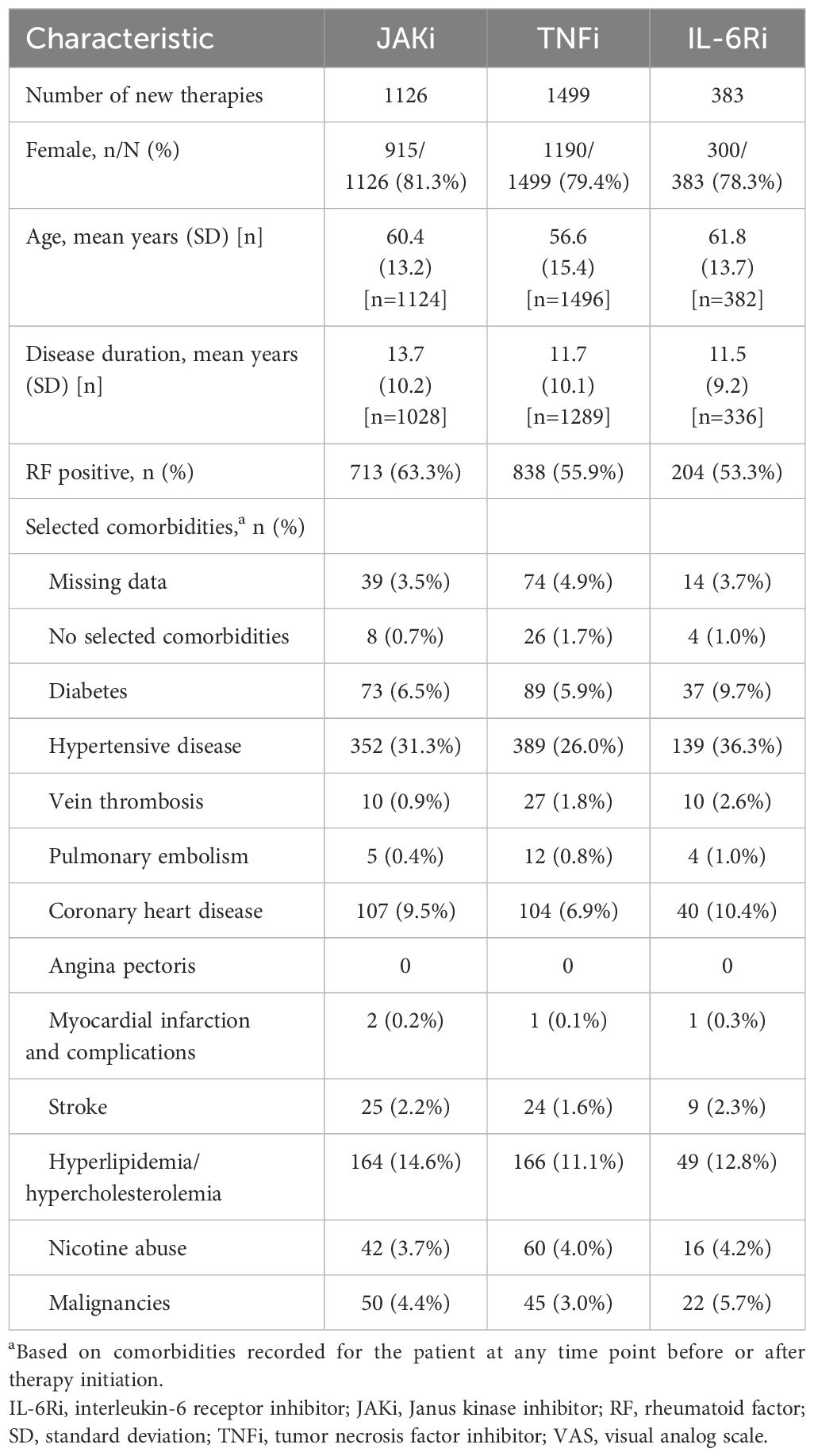
Table 1. Patient characteristics at time of therapy initiation.
3.2 Changes in treatment patterns over time
The proportion of patients initiating therapy with JAKi significantly increased from 29.7% in the earliest period (Q2/2020-Q3/2020) to a peak of 46.7% one year later (Q2/2021/Q3/2021; OR 2.08 [95% CI 1.62, 2.68]; p<0.001) and then decreased, particularly in the post-PRAC (32.9%; Q4/2022-Q1/2023; OR vs peak 0.56 [95% CI 0.41, 0.75]; p<0.001) and post-DHPC (26.1%; Q2/2023-Q3/2023; OR vs peak 0.40 [95% CI 0.29, 0.57]; p<0.001) periods (Figure 1). The proportion of newly initiated TNFi therapies showed the opposite pattern (decreases followed by increases). The proportions of new treatments with IL-6Ri showed modest variability over the observation period (Figure 1).
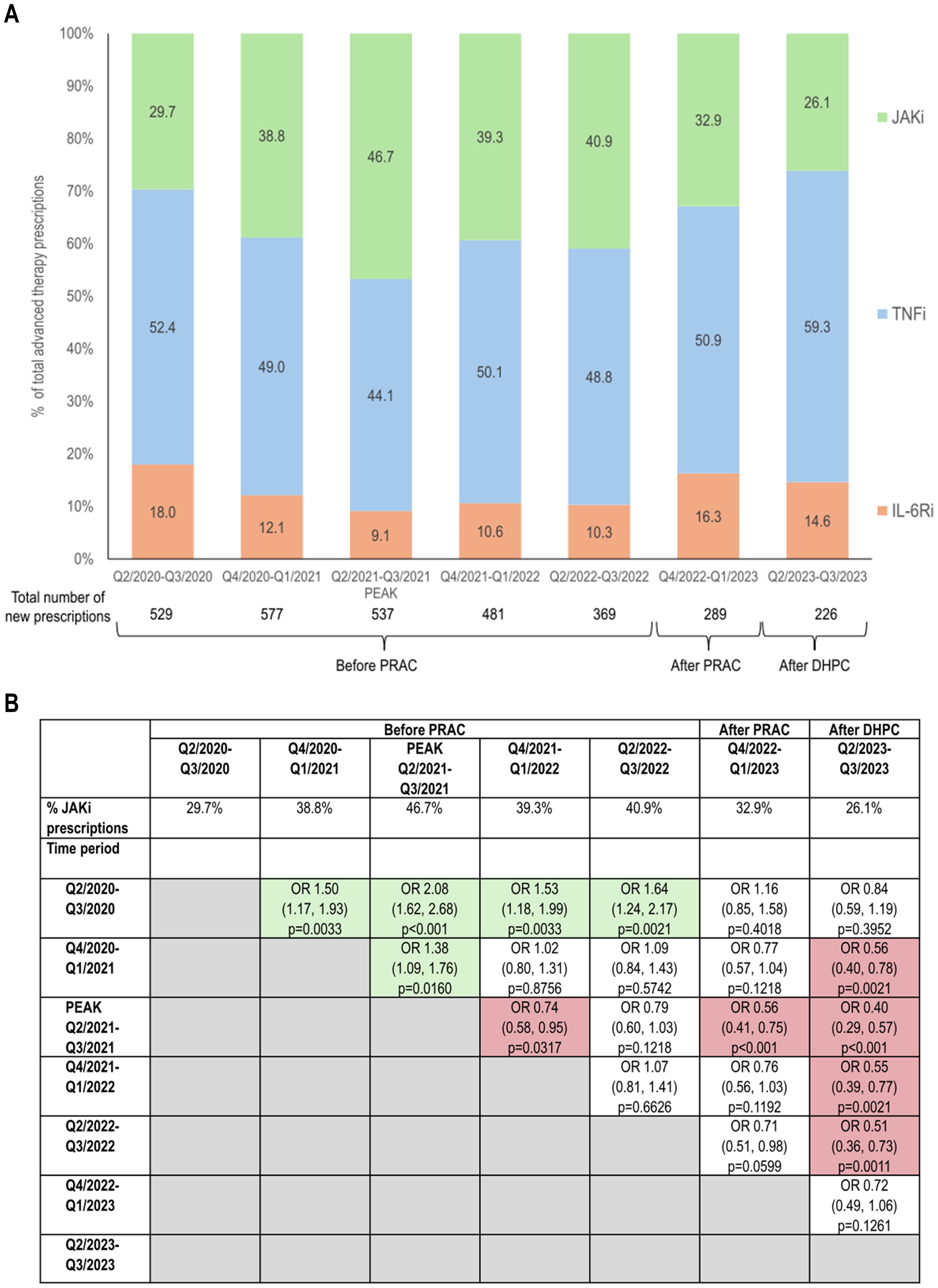
Figure 1. Changes in initiation of JAKi therapy in the time periods before and after JAKi EMA safety recommendations. (A) Proportion of new therapies initiated with JAKi, TNFi, or IL-6Ri; (B) Odds ratios (95% CI) and statistical significance of changes in proportions of newly initiated JAKi treatment over time. Green shading indicates significant increases in the proportion of JAKi therapies and red shading indicates significant decreases in the proportion of JAKi therapies. P values were calculated using the Benjamini-Hochberg adjustment. CI, confidence interval; DHPC, direct healthcare provider communication; EMA, European Medical Agency; IL-6Ri, interleukin-6 receptor inhibitor; JAKi, Janus kinase inhibitor; PRAC, Pharmacovigilance Risk Assessment Committee recommendations; Q, quarter; TNFi, tumor necrosis factor inhibitor.
Numerically, the Q4/2020-Q1/2021 time period had the most newly initiated therapies for these three drug classes (total of 577) and numbers of new therapies fell throughout the remaining periods (Figure 1).
New JAKi usage as 1st-line therapy generally decreased over time, although there was variability across time periods (Figure 2). Use as 2nd-line therapy decreased markedly (from 48.0% Q2/2020-Q3/2020 to 17.2% Q2/2023-Q3/2023), and this was accompanied by large increases in use as >3rd-line therapy (from 12.4% to 48.3%).
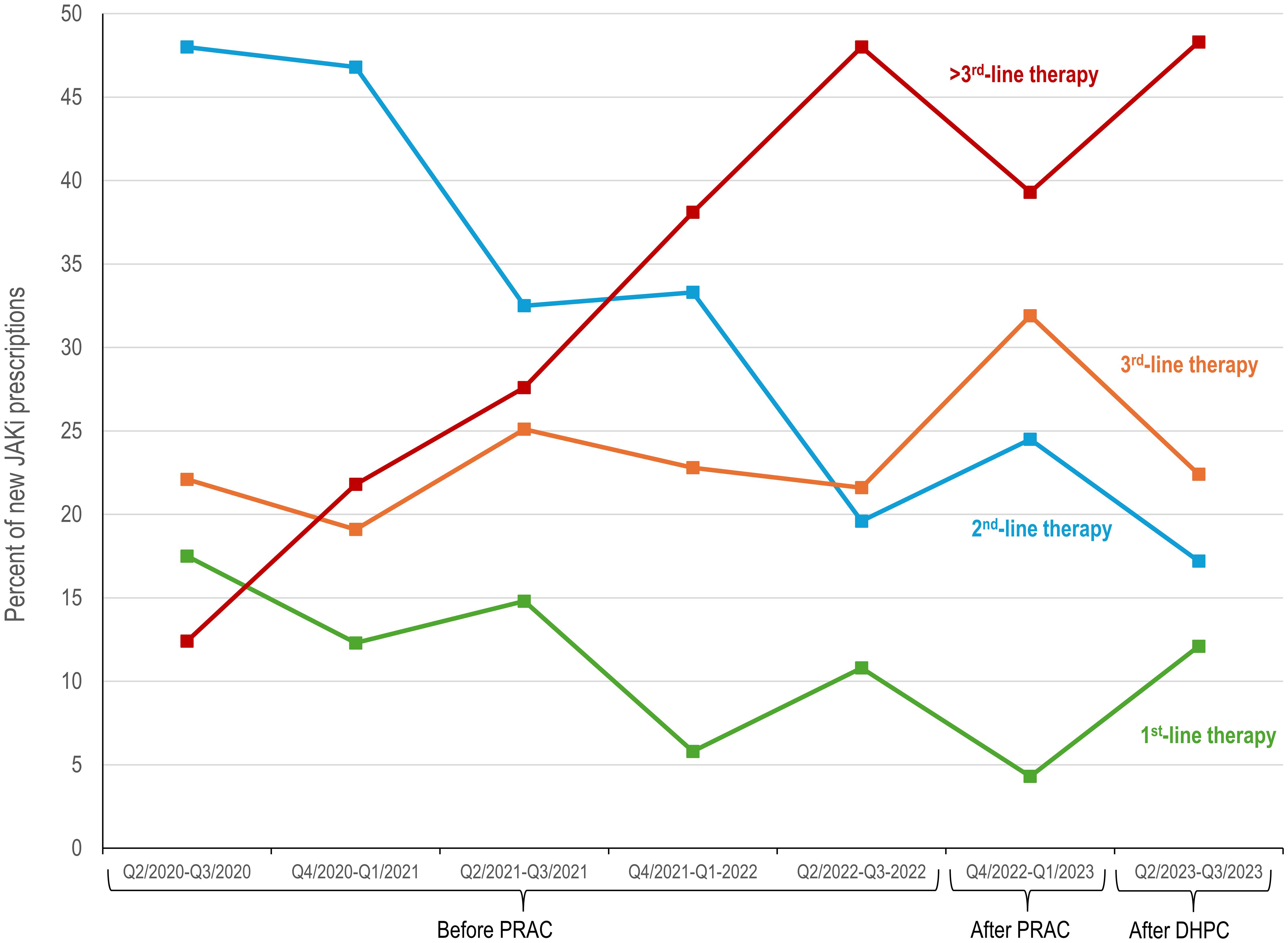
Figure 2. Changes in line of therapy in patients initiating JAKi treatment before and after JAKi EMA safety recommendations. DHPC, direct healthcare provider communication; EMA, European Medical Agency; JAKi, Janus kinase inhibitor; PRAC, Pharmacovigilance Risk Assessment Committee recommendations.
4 Discussion
The data from this exploratory analysis provide insights into changes in treatment practices in RA patients following the issuance of new safety recommendations for JAKi. Compared with earlier time periods, there was a significant decrease in the proportions of patients receiving new JAKi treatment in the time periods following the safety recommendations, and JAKi therapies initiated later in the study were more likely to be used as >3rd-line therapy.
In our study, the proportion of new JAKi therapies peaked during the Q2/2021-Q3/2021 time period. The decreases observed in the two following half-year periods, which were prior to the PRAC and DHPC time points, suggest that professionals may have begun to consider the implications of JAKi safety data on patient selection prior to the EMA recommendations; preliminary data were released by the manufacturer in January 2021 (7) and subsequently presented at a November 2021 conference (8). The proportions of new TNFi therapies showed an inverse pattern to JAKi. Our findings are consistent with a US study of RA prescriptions, which found significant decreases in JAKi prescriptions after the January 2021 release of preliminary ORAL Surveillance data and an association between decreases in new JAKi prescriptions and increases in TNFi use (9).
In addition to rheumatologic conditions, the EMA safety recommendations apply to all other JAKi indications as well. In particular, JAKi are frequently used for dermatologic conditions, including psoriasis and atopic dermatitis. Increased rates of malignancy and thromboembolic events have been observed in dermatologic patients treated with systemic JAKi drugs (10), particularly older patients (11), who are more likely to have multiple risk factors (12). It would therefore be of interest to also evaluate JAKi prescription patterns in these populations.
To the best of our knowledge, the change in the line of therapy for JAKi drugs over time has not been reported elsewhere and does not seem to have a clear alternative explanation. This change in treatment patterns is likely explained by the fact that a large proportion of RA patients have characteristics or comorbidities specified in the JAKi safety recommendations, including age of 65 years or older (13, 14), and therefore would not be considered good candidates for 1st-line JAKi therapy based on EMA guidance.
An unavoidable confounding factor is that the earlier study time periods were likely affected by changes in treatment patterns and IL-6Ri shortages during the COVID-19 pandemic (15, 16). Somewhat surprisingly, we observed higher numbers of new advanced therapies during the pandemic period compared with later timepoints. The reasons for this remain unclear, but may relate to the specific drug classes evaluated in this study and pandemic-related changes in prescribing practices. In particular, rituximab and methotrexate showed decreases in drug initiation during the pandemic (17), likely due to concerns about poor COVID outcomes and reduced vaccination responses (18–20). It is possible that as treatment patterns normalized during post-pandemic years, some patients on the therapies evaluated here (JAKi, TNFi, and IL-6Ri) returned to treatment with drugs not included in our analyses. In addition, the delayed documentation frequently observed in EHR data may have artificially decreased numbers of documented therapies during later time periods. However, it is unlikely that the lower numbers of therapies in the last two time periods affected the proportions of drug usage observed in our study.
Study limitations include those inherent to retrospective database analyses, including the inability to verify treatment adherence. Some data, such as smoking status, were not routinely reported. Reasons for treatment discontinuation and comorbidity start dates were not available in our database. Other studies have noted decreases in JAKi-treated patients with cardiovascular risk factors and other relevant comorbidities (21–23). Our study was focused on a subset of advanced therapies, and inclusion of additional agents may have affected the treatment patterns observed here. In addition, our analyses were limited to patients with RA and did not include other rheumatology and non-rheumatology indications for JAKi, such as psoriatic arthritis or axial spondyloarthritis (24, 25).
In conclusion, our data suggest that the updated EMA safety recommendations for JAKi were associated with changes in treatment practices for patients with RA in Germany. Future studies will be required to see if these changes represent a temporary shift or more long-lasting usage patterns.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Hannover Medical School (Application 11291_BO_K_2024). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
P-PS: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. LR: Conceptualization, Investigation, Writing – original draft, Writing – review & editing, Data curation, Formal Analysis, Methodology. ME: Data curation, Formal Analysis, Writing – original draft, Writing – review & editing. TW: Investigation, Writing – original draft, Writing – review & editing. MF: Investigation, Writing – original draft, Writing – review & editing. MS: Investigation, Writing – original draft, Writing – review & editing. MG: Investigation, Writing – original draft, Writing – review & editing. SH: Investigation, Writing – original draft, Writing – review & editing. PB-B: Investigation, Writing – original draft, Writing – review & editing. CV: Investigation, Writing – original draft, Writing – review & editing. KK: Investigation, Writing – original draft, Writing – review & editing. GG: Investigation, Writing – original draft, Writing – review & editing. SS-M: Investigation, Writing – original draft, Writing – review & editing. CK: Investigation, Writing – original draft, Writing – review & editing. WV: Investigation, Writing – original draft, Writing – review & editing. MW: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. SK: Conceptualization, Data curation, Formal Analysis, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by RHADAR GbR, Bahnhofstr. 32, 82152 Planegg, Germany. The authors declare that this study received funding from AbbVie Deutschland GmbH & Co. KG. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Acknowledgments
We thank the rheumatologists, patients, and medical staff who participated in this study and Sharon L. Cross, PhD, who provided medical writing support under the direction of the authors with funding from RheumaDatenRhePort (RHADAR) GbR (A Network of Rheumatologists).
Conflict of interest
P-PS received research funding from Chugai and speaker’s fees or travel grants from AbbVie, Boehringer/Ingelheim, Eli Lilly, Galapagos, and Janssen-Cilag. LR received travel/meeting support from AbbVie and Biocon Biologics Germany. ME received funding for the present study for data analysis from RHADAR GbR and also received consulting fees from AbbVie and RHADAR, speaker’s fees from AbbVie, Janssen-Cilag, Sanofi, and Swedish Orphan Biovitrum, and is on the advisory board of Chugai Pharma Germany. TW received consulting and/or speaker’s fees from AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, Chugai, Fresenius Kabi, Galapagos, GSK, Janssen, Lilly, Medac, Nordic, Novartis, Sanofi, and UCB and travel/meeting support from AbbVie, Janssen, Lilly, and UCB. MF received consulting fees or travel/meeting support from AbbVie, Amgen, AstraZeneca, Eli Lilly, Novartis, Janssen, Hexal, Pfizer, Takeda, and UCB. MS received research grants from Chugai and Novartis, consulting and/or speaker’s fees from AbbVie, Alfasigma/Galapagos/Gilead, Amgen, AstraZeneca, BMS, Boehringer/Ingelheim, Chugai/Roche, EUSA-Pharma, Hexal/Sandoz, Janssen-Cilag, Lilly, Novartis, onkowissen.de, and UCB, travel/meeting support from Alfasigma/Galapagos, Boehringer/Ingelheim, Celgene, Chugai/Roche, Medac, Mylan, and UCB, participates on advisory boards for AbbVie, Alfasigma/Galapagos/Gilead, Amgen, AstraZeneca, Boehringer/Ingelheim, Chugai/Roche, EUSA-Pharma, Hexal/Sandoz, Janssen-Cilag, Lilly, Novartis, onkowissen.de, and UCB, and has a leadership role in the Deutsches Netzwerk Systemische Sklerodermie DNSS. MG receive grants from AbbVie, Eli Lilly, and Pfizer, consulting fees from Amgen, AstraZeneca, Novartis, and Takeda, speaker’s fees from AbbVie, Eli Lilly, Janssen, and Novartis, and travel/meeting support from AbbVie, Eli Lilly, Pfizer, and UCB. SH received speaker’s fees from AbbVie and travel/meeting support from Janssen-Cilag and UCB. PB-B received speaker’s fees from AbbVie, Boehringer Ingelheim, Chugai/Roche, Janssen-Cilag, Novartis, Pfizer, and UCB and travel/meeting support from AbbVie. CV received travel/meeting support from AbbVie and Galapagos/Alpha sigma. KK received speaker’s fees from AbbVie, Galapagos, Novartis, Rheumakademie, and UCB and travel/meeting support from UCB. GG received speaker’s fees from AbbVie, Galapagos, and Novartis and travel/meeting support from AbbVie and Novartis. SS-M received speakers fees from AbbVie, Boehringer Ingelheim, Eli Lilly, GSK, Janssen-Cilag, Novartis, and UCB. WV received travel support from Bundesverband Managed Care. MW received consulting and/or speaker’s fees from AbbVie, Fresenius, Galapagos, Lilly, and UCB and travel/meeting support from AbbVie, Galapagos, GSK, Lilly, and UCB. SK received grants from AbbVie, Novartis, and Sparrow, and consulting and/or speaker’s fees from AbbVie, Celgene, Chugai, Galapagos, Novartis, and Siemens Healthineers. PB-B, CvdD, KK, GG, SS-M, CK, WV, MW, and SK are members of RheumaDatenRhePort RHADAR GbR.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Taylor PC, Choy E, Baraliakos X, Szekanecz Z, Xavier RM, Isaacs JS, et al. Differential properties of Janus kinase inhibitors in the treatment of immune-mediated inflammatory diseases. Rheumatol (Oxford). (2024) 63:298–308. doi: 10.1093/rheumatology/kead448
2. Ytterberg SR, Bhatt DL, Mikuls TR, Koch GG, Fleischmann R, Rivas JL, et al. Cardiovascular and cancer risk with tofacitinib in rheumatoid arthritis. N Engl J Med. (2022) 386:316–26. doi: 10.1056/NEJMoa2109927
3. European Medicines Agency. EMA confirms measures to minimize risk of serious side effects with Janus kinase inhibitors for chronic inflammatory disorders (2022). Available online at: https://www.ema.europa.eu/en/news/ema-confirms-measures-minimise-risk-serious-side-effects-janus-kinase-inhibitors-chronic-inflammatory-disorders#:~:text=EMA's%20human%20medicines%20committee%20(CHMP,treat%20several%20chronic%20inflammatory%20disorders (Accessed 8 April 2024).
4. European Medicines Agency. Cibinqo (abrocitinib), Jyseleca (filgotinib), Olumiant (baricitinib), Rinvoq (Upadacitinib) and Xeljanz (tofacitinb) — Updated recommendations to minimize the risks of Malignancy, major adverse cardiovascular events, serious infections, venous thromboembolism and mortality with use of Janus kinase inhibitors (JAKi) (2023). Available online at: https://www.ema.europa.eu/en/documents/dhpc/direct-healthcare-professional-communication-dhpc-updated-recommendations-minimise-risks-malignancy-major-adverse-cardiovascular-events-serious-infections-venous-thromboembolism-and-mortality-use_en.pdf (Accessed 8 April 2024).
5. Kleinert S, Bartz-Bazzanella P, von der Decken C, Knitza J, Witte T, Fekete SP, et al. A real-world rheumatology registry and research consortium: the German RheumaDatenRhePort (RHADAR) Registry. J Med Internet Res. (2021) 23:e28164. doi: 10.2196/28164
6. Benjamani Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Society: Ser B (Methodological). (1995) 57:289–300. doi: 10.1111/j.2517-6161.1995.tb02031.x
7. Pfizer shares co-primary endpoint results from post-marketing required safety study of Xeljanz® (tofacitinib) in subjects with rheumatoid arthritis (RA) (2021). Available online at: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-shares-co-primary-endpoint-results-post-marketing (Accessed 16 April 2024).
8. Ytterberg SR, Bhatt DL, Mikuls TR, Koch GG, Rivas JL, Germino R, et al. Safety and efficacy of tofacitinib vs TNF inhibitors in RA patients aged 50 years or older with one or more cardiovascular risks: results form a phase 3b/4 randomized safety trial [abstract 0831]. Arthritis Rheumatol. (2021) 73. https://acrabstracts.org/abstract/safety-and-efficacy-of-tofacitinib-vs-tnf-inhibitors-in-ra-patients-aged-50-years-or-older-with-one-or-more-cardiovascular-risks-results-from-a-phase-3b-4-randomized-safety-trial/.
9. Jeong S, George MD, Mikuls TR, England BR, Sauer B, Cannon GW, et al. Changes in patterns of use of advanced therapies following emerging data about adverse events in patients with rheumatoid arthritis from the Veterans Affairs Health System. ACR Open Rheumatol. (2023) 5:563–7. doi: 10.1002/acr2.11602
10. Samuel C, Cornman H, Kambala A, Kwatra SG. A review on the safety of using JAK inhibitors in dermatology: Clinical and laboratory Monitoring. Dermatol Ther (Heidelb). (2023) 13:729–49. doi: 10.1007/s13555-023-00892-5
11. Simpson EL, Silverberg JI, Nosbaum A, Winthrop K, Guttman-Yassky E, Hoffmeister KM, et al. Integrated safety update of abrocitinib in 3802 patients with moderate-to-severe atopic dermatitis: Data from more than 5200 patient-years with up to 4 years of exposure. Am J Clin Dermatol. (2024) 25:639–54. doi: 10.1007/s40257-024-00869-w
12. Vittrup I, Thein D, Thomsen SF, Egeberg A, Thyssen JP. Risk factors that impact treatment with oral Janus kinase inhibitors among adult patients with atopic dermatitis: A nationwide registry study. Acta Derm Venereol. (2024) 104:adv18638. doi: 10.2340/actadv.v104.18638
13. GBD 2021 Rheumatoid Arthritis Collaborators, Black RJ, Cross M, Haile LM, Culbreth GT, Steinmetz JD, et al. Global, regional, and national burden of rheumatoid arthritis, 1990-2020, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021 Lancet Rheumatol. (2023) 5(10):e594–e610. doi: 10.1016/S2665-9913(23)00211-4
14. Grellmann C, Dombrowsky W, Fabricius V, Suruki R, Sheahan A, Joeres L. Epidemiology and treatment of patients with rheumatoid arthritis, psoriatic arthritis and psoriasis in Germany: A real-world evidence study. Adv Ther. (2021) 38:366–85. doi: 10.1007/s12325-020-01522-8
15. MaChado PM, Verschueren P, Grainger R, Jones H, Piercy J, van Beneden K, et al. Impact of COVID-19 pandemic on the management of patients with RA: a survey of rheumatologists in six European countries. Rheumatol Adv Pract. (2022) 7:rkac108. doi: 10.1093/rap/rkac108
16. Iacobucci G. Shortages of rheumatoid arthritis drugs hit Europe after demand surges for treating covid. BMJ. (2021) 374:n2384. doi: 10.1136/bmj.n2384
17. Peasah SK, Swart ECS, Huang Y, Kane-Gill SL, Seybert AL, Patel U, et al. Disease-modifying medications in patients with rheumatoid arthritis in the USA: Trends from 2016 to 2021. Drugs Real World Outcomes. (2024) 11:241–9. doi: 10.1007/s40801-024-00416-3
18. Fagni F, Simon D, Tascilar K, Schoenau V, Sticherling M, Neurath MF, et al. COVID-19 and immune-mediated inflammatory diseases: effect of disease and treatment on COVID-19 outcomes and vaccine responses. Lancet Rheumatol. (2021) 3:e724–36. doi: 10.1016/S2665-9913(21)00247-2
19. Haberman RH, Herati R, Simon D, Samanovic M, Blank RB, Tuen M, et al. Methotrexate hampers immunogenicity to BNT162b2 mRNA COVID-19 vaccine in immune-mediated inflammatory disease. Ann Rheum Dis. (2021) 80:1339–44. doi: 10.1136/annrheumdis-2021-220597
20. Koehm M, Klippstein M, Dauth S, Hallmann K, Kohmer N, Burkhardt H, et al. Impact of different classes of immune-modulating treatments on B cell-related and T cell-related immune response before and after COVID-19 booster vaccination in patients with immune-mediated diseases and primary immunodeficiency: a cohort study. RMD Open. (2023) 9:e003094. doi: 10.1136/rmdopen-2023-003094
21. Huschek D, Herzer P, Zink A, Feuchtenberger M, Strangfeld A. Initiation of a Janus kinase inhibitor before and after safety warnings: changes in characteristics of patients with rheumatoid arthritis (abstract POS1085). Ann Rheum Dis. (2023) 82:865–6. doi: 10.1136/annrheumdis-2023-eular.4643
22. Philippoteaux C, Deprez V, Nottez A, Cailliau E, Houvenagel E, Deprez X, et al. Characteristics of patients treated with JAK inhibitors in rheumatoid arthritis before versus after VTE risk warnings. J Clin Med. (2022) 12:207. doi: 10.3390/jcm12010207
23. Song S, England BR, Sauer B, George MD, Riley TR, Wallace B, et al. Changes in characteristics of patients initiating and discontinuing advanced therapies for rheumatoid arthritis following the release of safety data. Arthritis Care Res (Hoboken). (2024) 76:463–9. doi: 10.1002/acr.25268
24. Strunz P-P, Englbrecht M, Risser LM, Witte T, Froehlich M, Schmalzing M, et al. Drug survival superiority of tumor necrosis factor inhibitors and interleukin-17 inhibitors over Janus kinase inhibitors and interleukin-12/23 inhibitors in German psoriatic arthritis outpatients: retrospective analysis of the RHADAR database. Front Immunol. (2024) 15:1395968. doi: 10.3389/fimmu.2024.1395968
25. Strunz P-P, Englbrecht M, Risser LM, Witte T, Froehlich M, Schmalzing M, et al. Analysis of the shorter drug survival times for Janus kinase inhibitors and interleukin-17 inhibitors compared with tumor necrosis factor inhibitors in a real-world cohort of axial spondyloarthritis patients - a retrospective analysis from the RHADAR network. Rheumatol Int. (2024). doi: 10.1007/s00296-024-05671-9
Keywords: rheumatoid arthritis, cancer, treatment, tumor necrosis factor inhibitors, interleukin-6 receptor inhibitors, oral surveillance, major adverse cardiac event, venous thromboembolism
Citation: Strunz P-P, Risser LM, Englbrecht M, Witte T, Froehlich M, Schmalzing M, Gernert M, Hueper S, Bartz-Bazzanella P, von der Decken C, Karberg K, Gauler G, Späthling-Mestekemper S, Kuhn C, Vorbrüggen W, Welcker M and Kleinert S (2024) Use of Janus kinase inhibitors before and after European Medicines Agency safety recommendations: a retrospective study. Front. Immunol. 15:1445680. doi: 10.3389/fimmu.2024.1445680
Received: 07 June 2024; Accepted: 02 August 2024;
Published: 22 August 2024.
Edited by:
Lazaros Ignatios Sakkas, University of Thessaly, GreeceReviewed by:
Silvia Scriffignano, University of Molise, ItalyElias Toubi, Technion Israel Institute of Technology, Israel
Copyright © 2024 Strunz, Risser, Englbrecht, Witte, Froehlich, Schmalzing, Gernert, Hueper, Bartz-Bazzanella, von der Decken, Karberg, Gauler, Späthling-Mestekemper, Kuhn, Vorbrüggen, Welcker and Kleinert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Patrick-Pascal Strunz, U3RydW56X1BAdWt3LmRl
†These authors have contributed equally to this work and share first authorship
‡ORCID: Patrick-Pascal Strunz, orcid.org/0000-0002-3168-7074
Linus Maximilian Risser, orcid.org/0009-0005-4105-6064
Matthias Englbrecht, orcid.org/0000-0003-0228-7183
Torsten Witte, orcid.org/0000-0003-4531-0267
Matthias Froehlich, orcid.org/0000-0001-7745-3903
Marc Schmalzing, orcid.org/0000-0002-3289-2299
Michael Gernert, orcid.org/0000-0003-0074-4459
Sebastian Hueper, orcid.org/0000-0002-3771-4635
Peter Bartz-Bazzanella, orcid.org/0000-0001-8084-4497
Cay von der Decken, orcid.org/0000-0001-9780-7174
Kirsten Karberg, orcid.org/0000-0002-1362-7326
Georg Gauler, orcid.org/000-0002-2132-8369
Susanna Späthling-Mestekemper, orcid.org/0009-0008-8124-2111
Christoph Kuhn, orcid.org/0000-0002-0538-1717
Wolfgang Vorbrüggen, orcid.org/0000-0003-1076-5560
Martin Welcker, orcid.org/0000-0002-1856-3085
Stefan Kleinert, orcid.org/0000-0002-2588-7547