 Maria Jose Gallardo-Nelson1*
Maria Jose Gallardo-Nelson1* Marcos Cruces2Yolanda M. Gómez3*Constanza Fuenzalida2Javiera Silva1Laura Aravena-Traipi1Eduardo Nuñez1
Marcos Cruces2Yolanda M. Gómez3*Constanza Fuenzalida2Javiera Silva1Laura Aravena-Traipi1Eduardo Nuñez1 Aracelly Gaete-Angel4,5
Aracelly Gaete-Angel4,5 Elizabeth Rivas-Yañez1
Elizabeth Rivas-Yañez1 Alexis M. Kalergis5,6,7
Alexis M. Kalergis5,6,7 Ricardo Soto-Rifo4,5
Ricardo Soto-Rifo4,5 Fernando Valiente-Echeverria4,5
Fernando Valiente-Echeverria4,5- 1Departamento de Medicina, Facultad de Medicina, Universidad de Atacama, Copiapó, Chile
- 2Policlínico Reumatología e Inmunología, Hospital Regional de Copiapó, Copiapó, Chile
- 3Departamento de Estadística, Facultad de Ciencias, Universidad del Bío-Bío, Concepción, Chile
- 4Laboratory of Molecular and Cellular Virology, Virology Program, Institute of Biomedical Sciences, Faculty of Medicine, Universidad de Chile, Santiago, Chile
- 5Millennium Institute on Immunology and Immunotherapy, Santiago, Chile
- 6Facultad de Ciencias Biológicas, Pontificia Universidad Católica de Chile, Santiago, Chile
- 7Departamento de Endocrinología, Facultad de Medicina, Escuela de Medicina, Pontificia Universidad Católica de Chile, Santiago, Chile
Objective: to evaluate the immune response to the SARS-CoV-2 vaccines in adults with immune-mediated rheumatic diseases (IMRDs) in comparison to healthy individuals, observed 1-20 weeks following the fourth vaccine dose. Additionally, to evaluate the impact of immunosuppressive therapies, vaccination schedules, the time interval between vaccination and sample collection on the vaccine’s immune response.
Methods: We designed a longitudinal observational study conducted at the rheumatology department of Hospital de Copiapó. Neutralizing antibodies (Nabs) titers against the Wuhan and Omicron variant were analyzed between 1-20 weeks after administration of the fourth dose of the SARS-CoV-2 vaccine to 341 participants (218 IMRD patients and 123 healthy controls). 218 IMRD patients with rheumatoid arthritis (RA), psoriatic arthritis (PsA), ankylosing spondylitis (AS), systemic lupus erythematosus (SLE), systemic vasculitis (VS) and systemic scleroderma (SS) were analyzed.
Results: Performing a comparison between the variants, Wuhan vs Omicron, we noticed that there were significant differences (p<0.05) in the level of the ID50, both for healthy controls and for patients with IMRDs. The humoral response of patients with IMRDs is significantly lower compared to healthy controls for the Omicron variant of SARS-CoV-2 (p = 0.0015). The humoral response of patients with IMRDs decreases significantly when the time interval between vaccination and sample collection is greater than 35 days. This difference was observed in the response, both for the Wuhan variant and for the Omicron variant.
Conclusion: The IMRDs patients, the humoral response variation in the SARS-CoV-2 vaccine depends on doses and type of vaccine administered, the humoral response times and the treatment that these patients are receiving.
Introduction
The worldwide pandemic of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has resulted in over 6 million fatalities (1). In Chile, until December 25, 2022, there were 5,366,630 cases of COVID-19 (2). It was critically important to prevent the spread of the COVID-19 pandemic. An increasing variety of SARS-CoV-2 vaccines are being utilized globally, encompassing mRNA-based, adenoviral vector, protein subunit, and inactivated virus vaccines (3). The immunogenicity of the SARS-CoV-2 vaccine can be quantified through the measurement of humoral IgG to the spike protein or cellular T-cell reactivity through interferon (IFN)-γ response towards SARS-CoV-2 peptides. The antibody responses are commonly recorded as ‘seroconversion’ (freshly positive anti-spike protein IgG), or via post-immunization antibody levels (4). In Chile, the effectiveness of booster shots against symptomatic COVID-19 was measured, with 56-80% for CoronaVac (Sinovac Biotech), 56-90% for BNT162b2 (Pfizer-BioNTech) and 56-93% for ChAdOx1-S (AstraZeneca-Oxford). The effectiveness against hospitalization 14 days after the booster shot was 84-88%, 84-87% and 84-96% respectively (5).
The Omicron variant (B.1.1.529 lineage) was the most frequent variant in the Chilean population during January 2022, representing 71.8% (6). Patients with immune-mediated rheumatic diseases (IMRDs) are at increased risk of serious infections because of the subyacent dysregulation of their immune system and the common use of immunosuppressors and antirheumatic biological therapies (7). Decreased reactions to traditional vaccines are linked with advanced age, high-dose steroid use, elevated inflammatory activity index, and immunosuppressive treatments (8). Findings indicate that in patients with rheumatic diseases, the responses to the SARS-CoV-2 vaccine are compromised by rituximab, glucocorticoids (GC), methotrexate, abatacept, mycophenolate mofetil, and JAK inhibitors (9–12). In Chile, diverse immunocompromising conditions markedly reduce the humoral response to the CoronaVac vaccine (13). The present study aimed to evaluate the immune response induced by 4th dose of different SARS-CoV-2 vaccines, measuring levels of neutralizing antibodies (NAbs) in adult patients with IMRDs and comparing them with healthy controls.
Methodology
This longitudinal observational study was carried out in the rheumatology department of the Regional Hospital of Copiapó (Atacama, Chile) between March and July 2022. The primary objective was to assess the immunogenicity of SARS-CoV-2 vaccines in adult patients with IMRD compared to healthy controls, measured between 1 and 20 weeks after the fourth vaccine dose. Additionally, other secondary objectives were analyzed, such as the immunogenic effect of the original Wuhan strain and its Omicron variant in healthy controls and patients, the SARS-CoV-2 vaccination schedules implemented in the country, the kinetics of the humoral response to SARS-CoV-2 vaccination, and the effect of immunosuppressive pharmacological treatments and specific pathologies (RA, PsA, AS, VS, and SS) on the immunogenicity of the vaccine in patients with IMRD.
Study population
A non-probabilistic convenience sampling was carried out in the population with IMRDs population over 18 years from the rheumatology outpatient clinic at Hospital de Copiapó. Patients with 4th dose SARS-CoV-2 vaccine were included. Selected diseases were rheumatoid arthritis (RA), psoriatic arthritis (PsA), ankylosing spondylitis (AS), systemic lupus erythematosus (SLE), systemic vasculitis (VS) and systemic scleroderma (SS). Patients continued with their usual medication during the vaccination period, in certain cases, patients using rituximab were instructed to delay treatment after vaccination at the doctor’s discretion.
Participants without immunosuppression vaccinated with 4th dose against SARS-CoV2 during the same timeframe, were chosen for the control group. The control group consisted predominantly of health care professionals, providing a representative sample of the broader population (Figure 1).
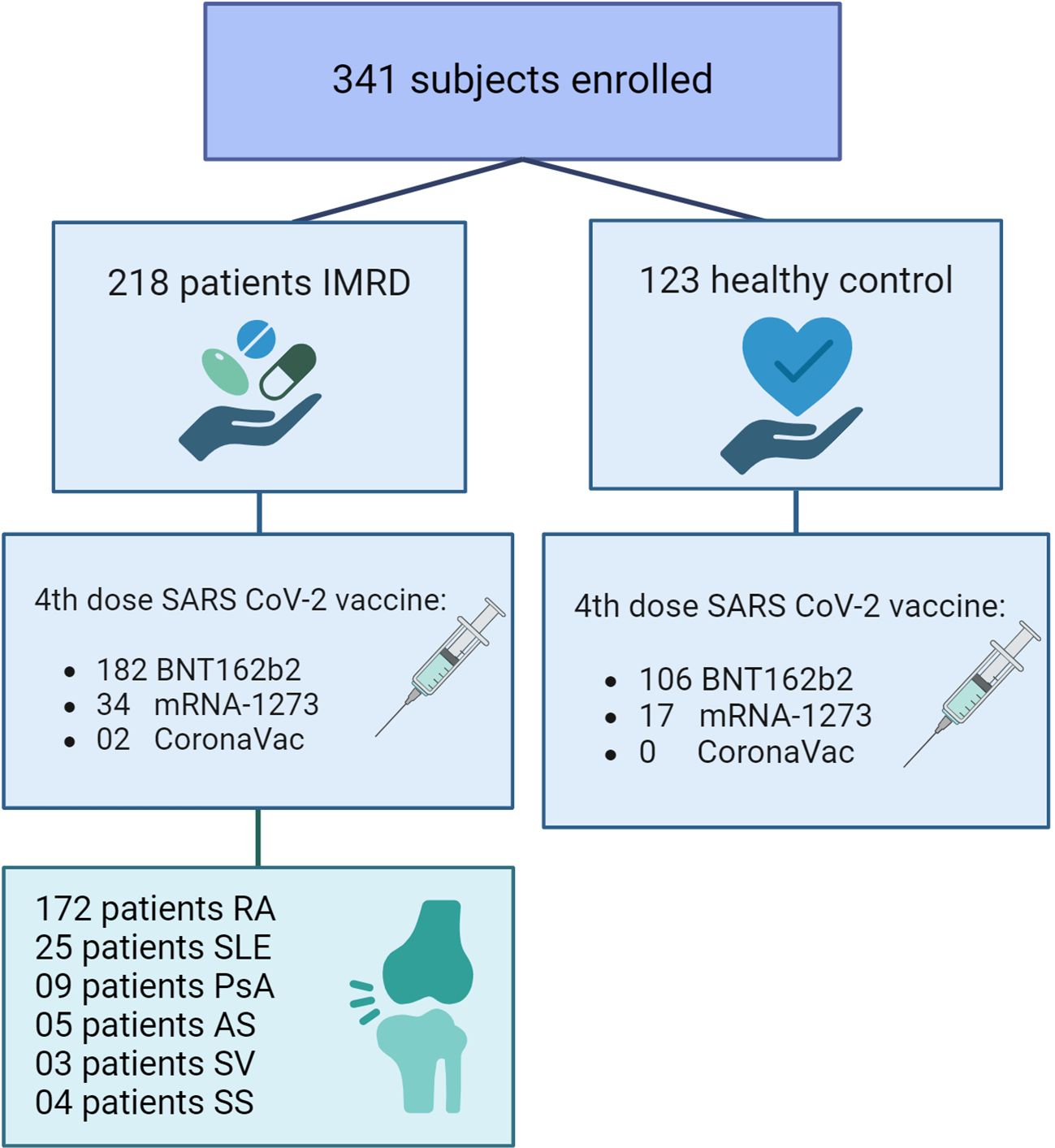
Figure 1 Flow diagram of the population participating in the study. IMRDs, immune-mediated rheumatic diseases. RA, Rheumatoid arthritis; SLE, Systemic lupus erythematosus; PsA, Psoriatic arthritis; AS, Ankylosing spondylitis; SV, Systemic Vasculitis; SS, Systemic scleroderma.
General exclusion criteria were previous serologically or PCR-confirmed COVID-19, and in the control group, a history of IMRDs and immunosuppressive treatment.
The subsequent factors were documented: age, sex, type of rheumatic disease, a brand of vaccine administered, time since diagnosis, current treatment with synthetic disease-modifying antirheumatic drugs (DMARDs), biological disease-modifying antirheumatic drugs (bDMARDs) and or JAK inhibitors, glucocorticoid dose (prednisone equivalent), time since last infusion in rituximab or cyclophosphamide treated patients, safety of vaccination and comorbidities.
Vaccination procedure
All patients and controls received a 4th dose of the SARS-CoV-2 vaccine with BNT162b2, CoronaVac or mRNA-1273 vaccines (6). Samples for measured immunogenicity were taken 1–20 weeks after vaccination.
Determination of Nabs against SARS-CoV-2
We conducted an analysis of the neutralizing antibody levels against SARSCoV-2 D614G (B.1 lineage) and Omicron (BA.1 lineage) by utilizing an HIV-1–SΔ19 pseudotype (SARS-CoV-HIV-luciferase). This method facilitates large-scale detection and quantification of the existence of neutralizing antibodies (Nabs) (14). Serum samples that were inactivated underwent a 3-fold serial dilution, ranging from 1:5 to 1:10935, in DMEM that was supplemented with 10% FBS. These samples were then incubated with 3 ng of p24 HIV-1-based SARS-CoV-2 variant pseudotyped virus hailing from either the Wuhan (B.1 lineage) or Omicron (BA.1 lineage)), for a period of 1 hour at a temperature of 37°C. Following this, 1 × 104 HEK-ACE2 cells were introduced into each well. As a negative control, HEK293T cells were incubated with the pseudotyped virus. After 48 hours, cells were broken down, and the firefly luciferase activity was assessed using the Luciferase Assay Reagent (Promega) in a Glomax 96 Microplate luminometer (Promega). The average relative luminescence units (RLUs) of HEK293T cells infected with the equivalent pseudovirus were assumed as 100% neutralization, while RLUs recorded at each sample’s highest dilution were set as 0% neutralization. Consequently, the neutralization percentage of each of the eight dilutions of a sample was determined as the complement of the division between the related RLUs and the RLUs achieved at the higher dilution after subtracting the background (HEK293T + pseudovirus). This calculation was performed individually for each technical replicate and for each spike variant. The Relative pseudotyped Virus Neutralization Titer 50 (ID50) is a term used to describe the sample dilution required to decrease firefly luciferase activity by 50% when compared to both positive and negative controls. The negative control is the HEK293T without the pseudovirus and the positive control is the highest sample dilution. The calculation of the ID50 was performed using GraphPad Prism v9.1.2, a software-based in La Jolla, California, USA, by applying a four-parameter non-linear regression model with a variable slope. This model curbs the highest values at 100 and the lowest at 0. If a sample displayed a pVNT50 value that was lower than the first dilution (1:10), it was noted as 10 (15, 16). Figure 1 of the Supplementary Material is a graphical explanation of the method to explain neutralizing antibodies determination.
Statistical analysis
Variables in categories were presented in percentage form, while continuous variables were depicted as median and Interquartile Range (IQR) values. The Mann-Whitney U test was employed to evaluate the distinctions between groupings. Comparison of categorical variables was achieved using contingency tables, and p values were determined with either χ2 or Fisher’s exact tests, as the situation required. P values of ≤0.05 were considered statistically significant. All the given p values are two-tailed. These data were entered and administered using the REDCap database tool housed at the Faculty of Medicine, University of Chile (17), statistical analyses were performed using the R software version 4.3.1 (18) and GraphPad Prism version 8.4.3.
Ethics
The study was carried out following the principles of the Declaration of Helsinki and was approved by the ethics committee of the Faculty of Medicine of the University of Chile (Project N° 161-2021). All participants signed informed consent before inclusion in the study.
Results
Demographic characteristics of the study population
A total of 341 participants were enrolled, of which 218 were patients with IMRDs and 123 healthy controls. The demographic characteristics of the group finally analyzed are given in Table 1.
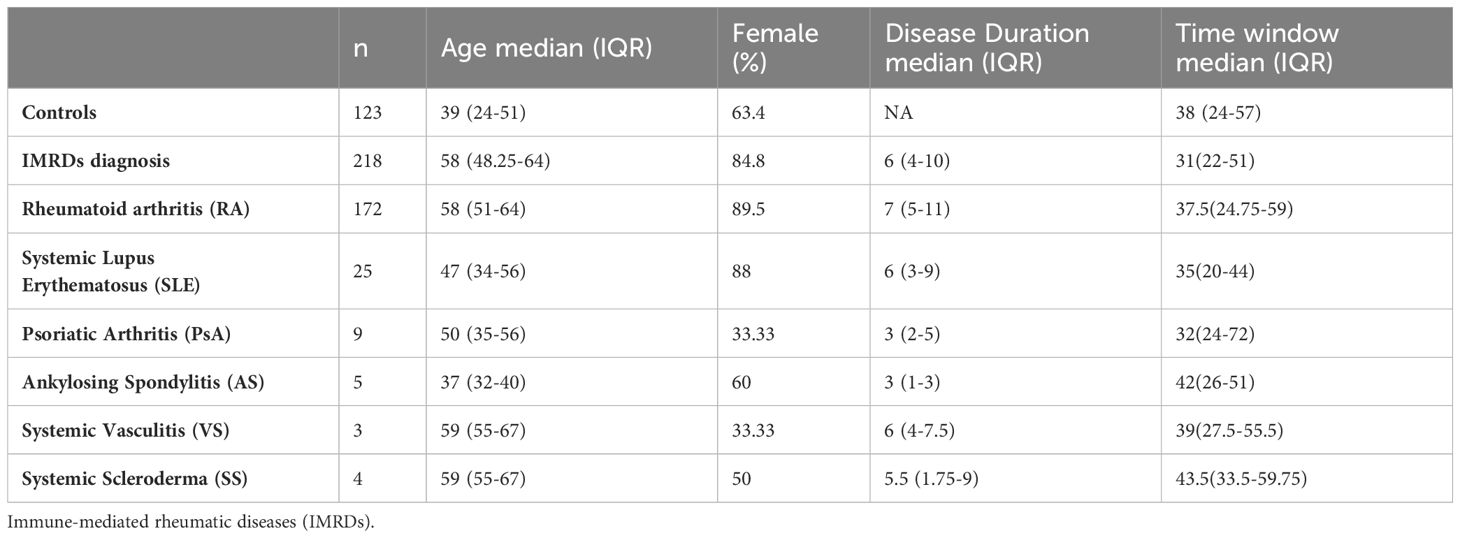
Table 1 Demographic characteristics of patients with IMRDs and controls.
The median age of healthy controls was 39 years, while for IMRDs patients was 58 years. Regarding gender distribution, 63.4% of healthy controls were women, while IMRDs patients were 84.8%. RA was the most common disease among participants (n=172), followed by SLE (n=25). The median duration of the rheumatic disease in patients was 6 years. Samples are measured 1-20 weeks after vaccination, the median of the time window is 35 days.
Immunogenicity of vaccination against SARS-CoV-2
The fourth dose of SARS-CoV-2 vaccination was mostly administered with BNT162b2, both for healthy controls and IMRDs patients. The NAbs titer against SARS-CoV-2 was determined for the original Wuhan strain and Omicron variant, using the methodology for the detection of antibodies with neutralizing capacity described in the work by Beltrán-Pavez et al. (2021) (14). The presence of NAbs against protein S of the Wuhan strain was 100% for healthy controls and 99.5% for rheumatic patients. For the Omicron variant, it was 100% for healthy controls and 99% for rheumatic patients.
The NAbs titer in patients and healthy controls presented a higher titer for the original Wuhan strain than for the Omicron variant (Figures 2A, B). The median ID50 for the Wuhan strain was 6030 ± 7285.5 versus 3533 ± 6912.3 for the Omicron variant (p=0.0003) for healthy controls (Figure 3A). In IMRDs patients the median ID50 was 5298 ± 7514.3 for the Wuhan strain compared to 2144.5 ± 6354.8 for the Omicron variant (p < 0.001) (Figure 3B). The humoral response of IMRDs patients is significantly lower compared to healthy controls for the Omicron variant of SARS-CoV-2 (p=0.0015) (Figure 2D), but not in the NAbs titer for the Wuhan strain (Figure 3C).
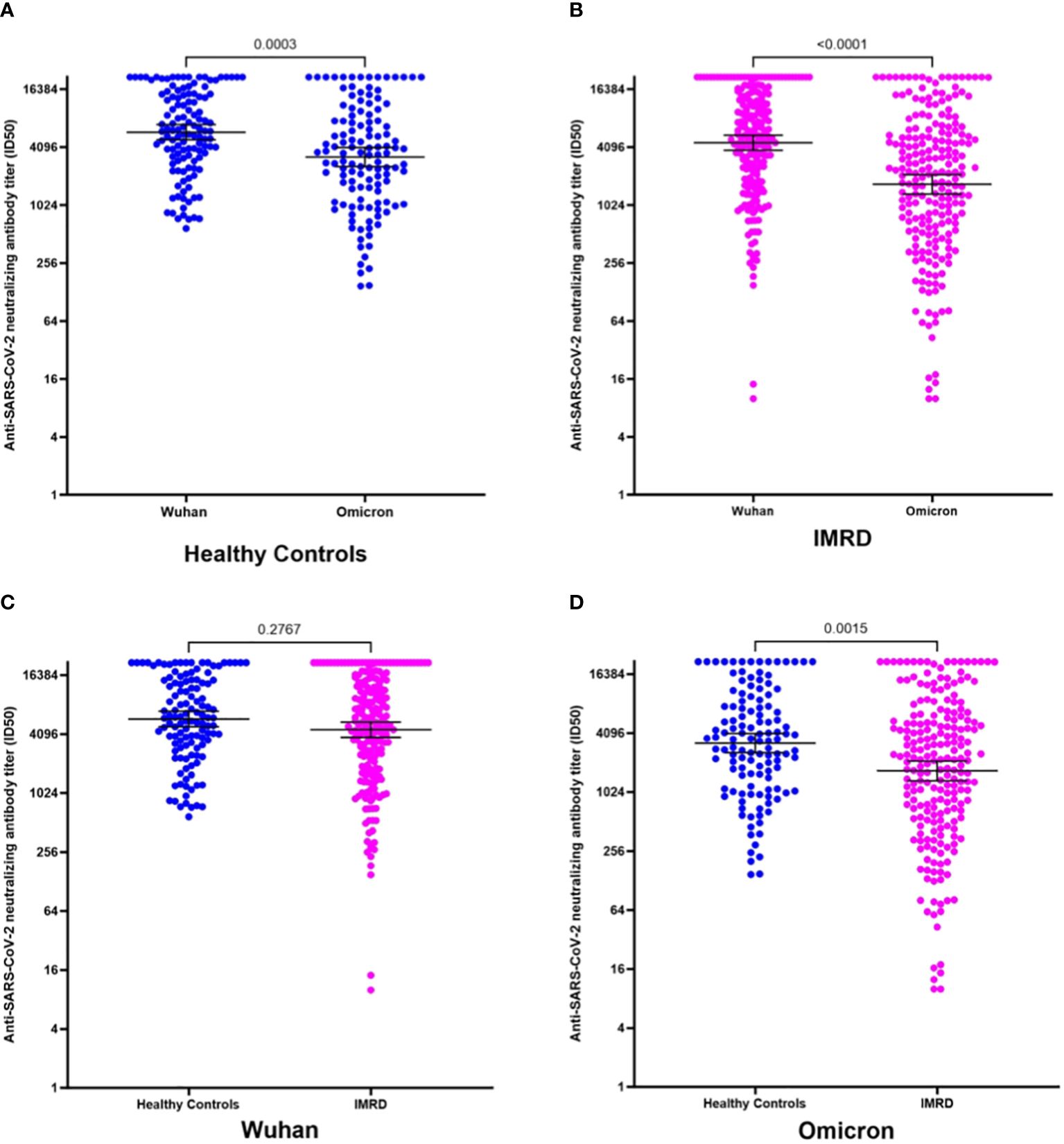
Figure 2 NAbs titer against SARS-CoV-2 for the Wuhan strain and Omicron variant, according to the time interval between vaccination and sample collection. (A) ID50 neutralizing antibodies of healthy controls according to the post-vaccination time, for the Wuhan strain. (B) ID50 of NAbs from IMDRs patients according to time post-vaccination for the Wuhan strain. (C) ID50 of NAbs from healthy controls according to time post-vaccination for the Omicron variant. (D) ID50 of NAbs from IMDRs patients according to time post vaccination for the Omicron variant.

Figure 3 NAbs titer against SARS-CoV-2 for the original Wuhan strain and the omicron variant, in the serum of rheumatic patients and healthy controls after the fourth dose of vaccination against SARS-CoV-2. (A) ID50 for the original Wuhan strain and the omicron variant in the serum of healthy controls. (B) ID50 for the original Wuhan strain and the omicron variant in the serum of IMRDs patients. (C) ID50 of NAbs in healthy controls and IMRDs patients for the original Wuhan strain. (D) ID50 of NAbs in healthy controls and IMRDs patients for the Omicron variant.
The measurement of NAbs was performed between 1 and 20 weeks after vaccination of the fourth dose. This allows us to observe the humoral response in the time interval between the administration of the vaccine and the sample collection, the median of the time window is 35 days, we choose this endpoint of 35 days to ensure 50% of the samples were in each group. Besides in this case there is no significant difference (p-value>0.05), therefore we have no differences between the times since vaccination and sampling between patients and healthy controls.
The NAbs titer of patients with IMRDs decreases significantly when the time interval between vaccination and sample collection is greater than 35 days (Figure 2). This difference is observed in the response, both for the original strain from Wuhan (Figure 2B) and for the Omicron variant (Figure 2D). In contrast, in healthy controls, the humoral response is maintained over time, both for intervals less than or equal to 35 days and for intervals of more than 35 days (Figures 2A–C), in response to both strains.
Immunogenicity according to the vaccination scheme used against SARS-CoV-2
Study participants have different vaccination schedules against SARS-CoV-2. Homologous schemes are defined as those that use the BNT162b2 and mRNA-1273 vaccines since they present the same vaccination strategy through mRNA. Heterologous schemes are defined as mixed schemes, where CoronaVac vaccines were used for the first 2 doses and then different combinations with vaccines such as BNT162b2, ChAdOx1-S or mRNA-1273. Healthy controls with homologous schemes represent 54% and with heterologous schemes 46%. In IMRDs patients the heterologous scheme was the majority with 68% of the patients and 32% with a homologous scheme.
In homologous vaccination schemes, no differences in their NAbs titers against SARS-CoV-2 were observed between healthy controls and IMRDs patients (Figures 4A–C). In contrast, in heterologous schemes, the NAbs titer against SARS-CoV-2 was lower in IMRDs patients than in healthy controls, in response to the Omicron variant (p =0.0149) (Figure 4C), which is not observed in response to the Wuhan strain (Figure 4A).
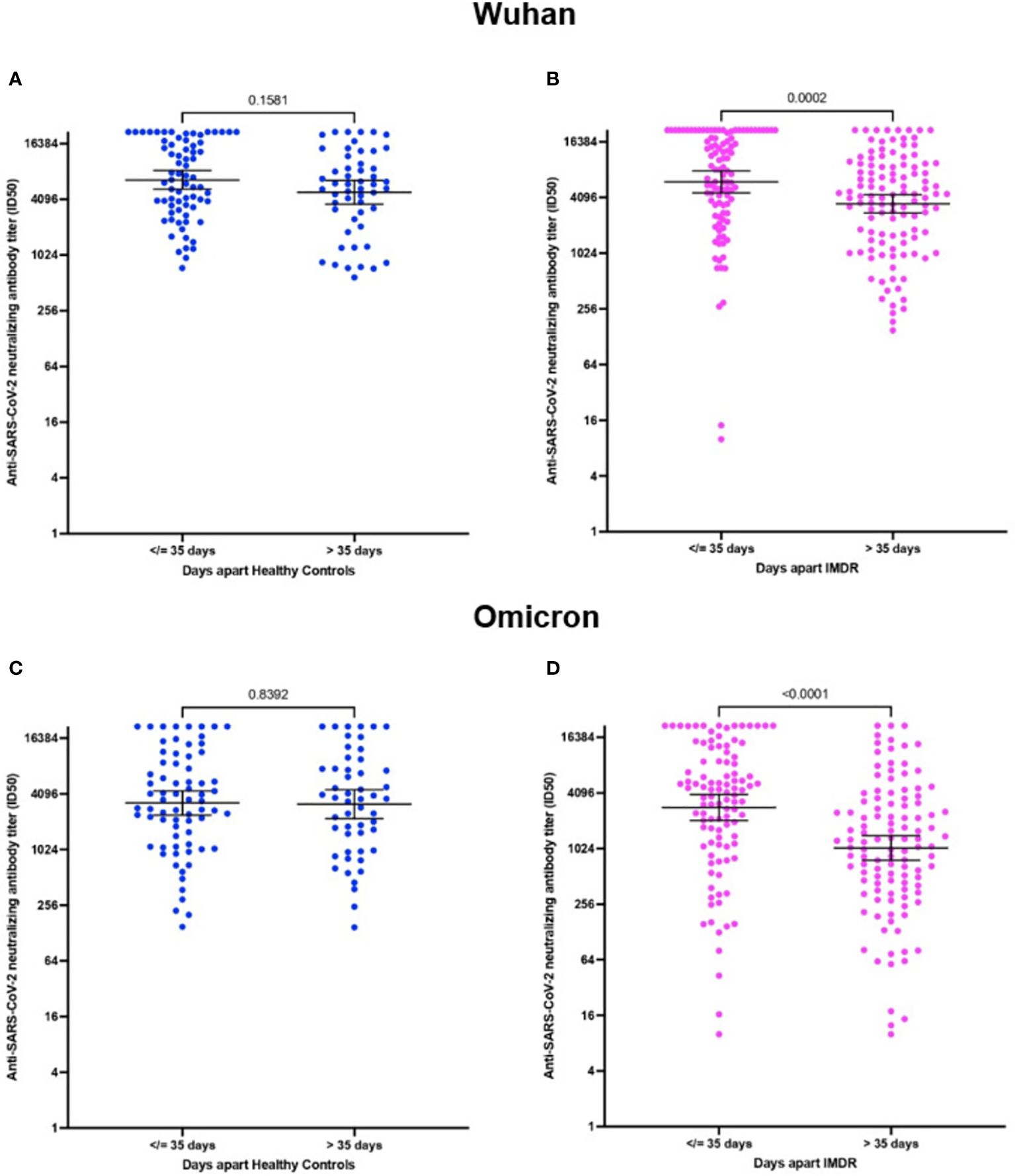
Figure 4 NAbs titer against SARS-CoV-2 in the serum of rheumatic patients and healthy controls according to the vaccination scheme used against SARS-CoV-2. (A) ID50 of NAbs against SARS-CoV-2 between IMDRs patients and healthy controls for the Wuhan strain. (B) ID50 of NAbs against SARS-CoV-2 according to the vaccination scheme for the Wuhan strain. (C) ID50 of NAbs against SARS-CoV-2 between IMDRs patients and healthy controls for the Omicron variant. (D) ID50 of NAbs against SARS-CoV-2 according to the vaccination schedule for the Omicron variant.
The NAbs titer against SARS-CoV-2 in the serum of patients who followed a heterologous regimen is significantly lower than that of patients who followed a homologous regimen. Results were observed for the original Wuhan strain (p =0.0186) (Figure 4B) and for the Omicron variant (p = 0.0014) (Figure 4D). In healthy controls, the NAbs titers against SARS-CoV-2 do not show differences between the different vaccination schemes.
Immunogenicity according to IMRDs
In our patients with IMRDs, the main disease represented is RA. The humoral response of RA patients against the parental Wuhan strain did not show differences compared to healthy controls (Figure 5A). Instead, when analyzing the response of these patients against the Omicron variant, a significant decrease in the NAbs titers was observed compared to healthy controls (Figure 5D). When analyzing the response to the antibody titer of SLE patients compared to healthy controls, no significant differences were observed, neither for the Wuhan strain nor for the Omicron (Figures 5B–E). The other IMRDs included in our study are PsA, AS, SV and SS. These diseases were analyzed together due to their small sample size, without observing significant differences in the titer of NAbs against the Wuhan strain or Omicron variant compared to healthy controls (Figures 5C–F).
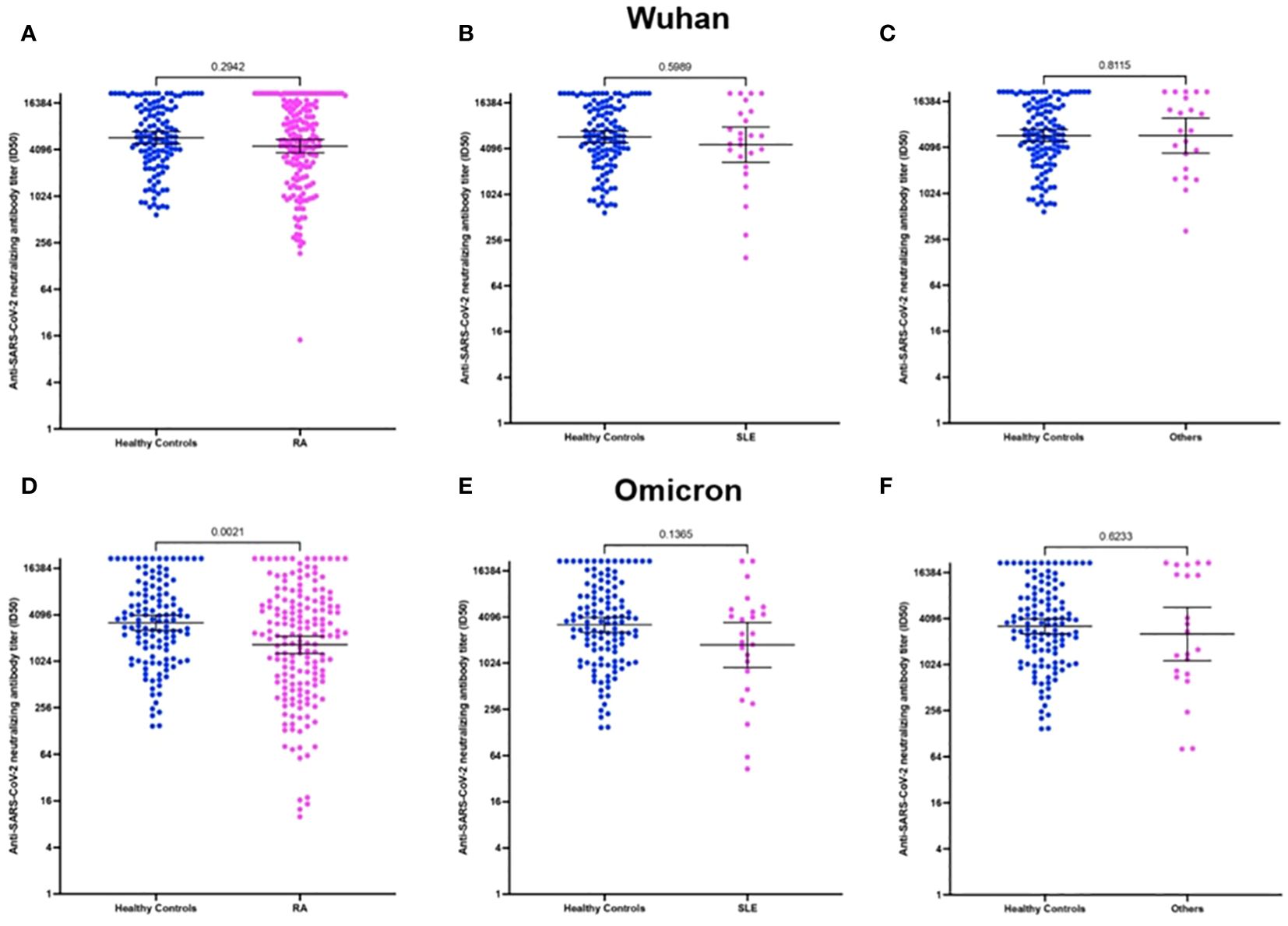
Figure 5 NAbs titer against SARS-CoV-2 in the serum of patients with rheumatoid arthritis (RA), Systemic lupus erythematosus (SLE) and other rheumatic diseases included in the study. (A) ID50 of neutralizing antibodies against SARS-CoV-2 from RA patients against the Wuhan strain. (B) ID50 of NAbs against SARS-CoV-2 from SLE patients against the Wuhan strain. (C) ID50 of NAbs against SARS-CoV-2 from patients with other rheumatic diseases against the Wuhan strain. (D) ID50 of NAbs against SARS-CoV-2 from RA patients against the Omicron variant. (E) ID50 of NAbs against SARS-CoV-2 from SLE patients against the Omicron variant. (F) ID50 of NAbs against SARS-CoV-2 from patients with other rheumatic diseases against the Omicron variant.
Effect of pharmacological treatments on the immune response
In participating IMRDs patients, 72% are treated with GC (approximately 5 mg/day) (Table 2). We can observe that these patients present a significant decrease in the titer of NAbs for SARS-CoV-2 in response to vaccination, both for the original Wuhan strain and for the Omicron variant.
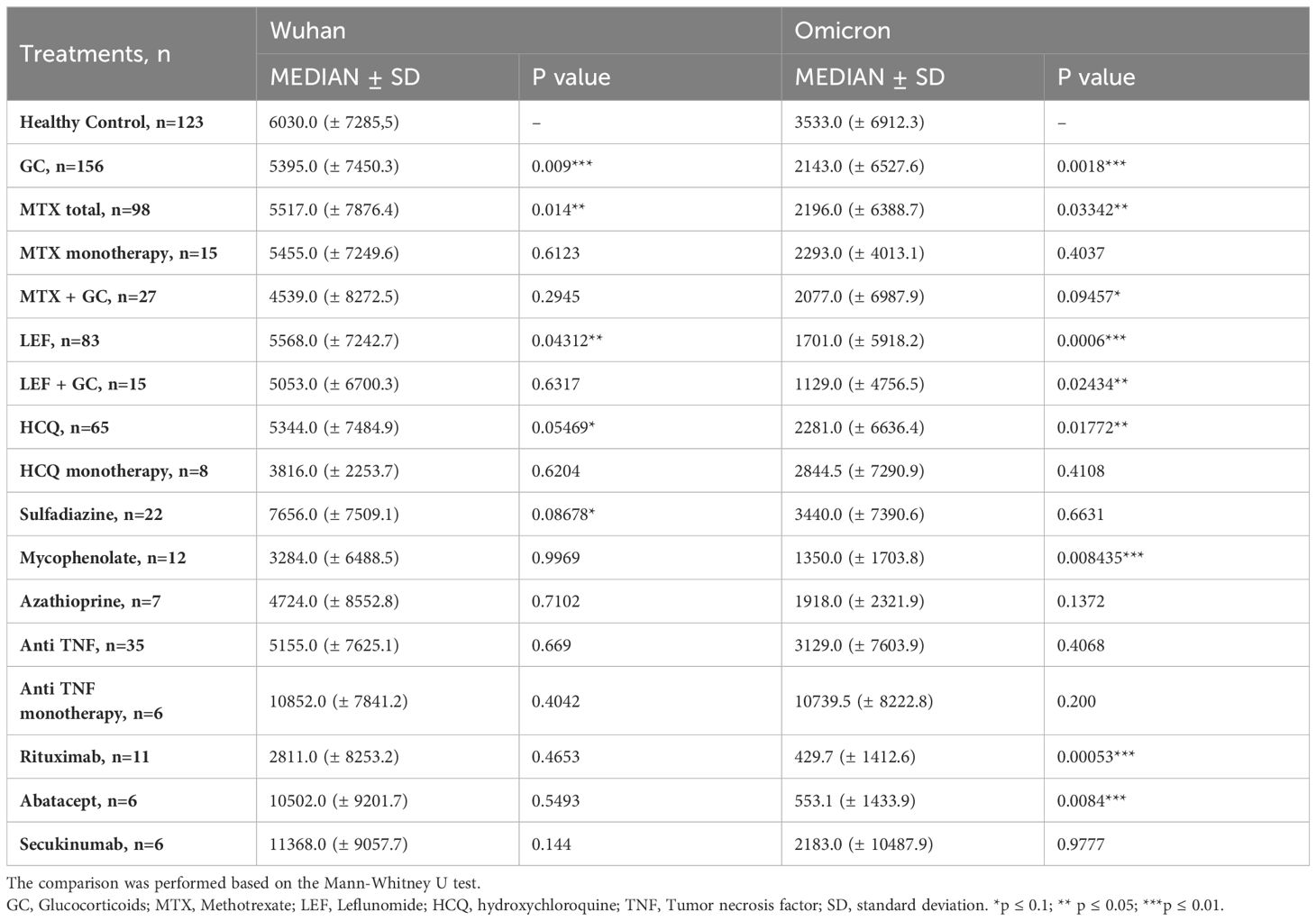
Table 2 Immunogenicity of vaccination against SARS-CoV-2 according to the treatments used by IMRDs patients compared to healthy controls.
Likewise, methotrexate (MTX) and leflunomide (LEF) treatment is widely used by IMRDs patients (mainly in RA patients), either as monotherapy or in combination with other treatments. The titer of NAbs against SARS-CoV-2 of patients treated with MTX or LEF in combination with other treatments significantly decreased compared to healthy controls both for the original Wuhan strain and for the Omicron variant. Treatments such as Hydroxychloroquine (in combination), mycophenolate, rituximab and abatacept also show a decrease in NAbs titer against SARS-CoV-2, but only in response to the Omicron variant (Table 2).
Discussion
Our data reveal that both healthy controls and IMRDs patients have high seropositivity and high NAbs titer against the original SARS-CoV-2 Wuhan strain and the Omicron variant. This could be attributed to the extensive vaccination campaign carried out by the Chilean Ministry of Health, which contemplated four vaccination doses until the development of this study, intending to maintain high antibody titers against SARS-CoV-2 and to control the infection of the Omicron variant strain in 2022 (6, 19–21). These data are consistent with recent studies carried out in a population vaccinated against SARS-CoV-2, plus one or two booster doses, where it was observed that 98.2% of people had NAbs against the Wuhan variant, while 65.5% had NAbs against the Omicron variant (22).
The Omicron variant was the most frequent in the Chilean population during January 2022 (6). This variant presents 36 mutations in the S (spike) protein, which is the immunological target against NAbs (23, 24). The most relevant mutations are found within the receptor-binding domain which allows the escape of NAbs induced by the vaccine (24, 25). The immune evasive potential of the Omicron variant to escape the humoral immunity generated by the vaccination schemes led to the implementation of a fourth immunization (6, 23). Our data reveal a higher immune response for the original Wuhan strain than for the Omicron variant, but even so, there is a high response to Omicron after the fourth dose, which demonstrates the effectiveness of increasing the humoral response of the booster of the SARS-CoV-2 vaccine. However, in IMRDs patients a lower response to Omicron was observed, which may be due to the pharmacological treatments used to control rheumatic disease.
Knowing the duration of humoral immunity is crucial for the control of SARS-CoV-2 infection and, therefore, for making public health decisions regarding vaccination programs. Various studies analyze the permanence of total and NAbs against SARS-CoV-2 in healthy controls (26–29). In scientific studies carried out in IMRDs patients, such as RA, a difference in the kinetics of the humoral response has been observed, where patients required 2 doses of the vaccination to reach higher levels of antibodies (30). Other articles show that patients with RA have a high seropositivity of 97% but with significantly lower total antibody levels than healthy controls (31). This information is consistent with our data since we have also observed a high antibody titer for the original Wuhan strain and the Omicron variant. According to our data, seropositivity in rheumatic patients was 99.5% for the Wuhan variant and 99% for the Omicron variant, while in controls it was 100% for both strains. However, further analysis revealed that after 35 days from vaccine administration, IMRDs patients experienced a decrease in NAbs to SARS-CoV-2. This could be due to the initial state of the immune system of IMRDs patients, who are under Immunosuppressive treatments. Therefore, the response to vaccination is not maintained over time, as is the case with healthy controls. The rapid decline in NAbs leads to reduced protection and increased risk of infection (32), which reinforces the idea to consider booster doses (30–34).
In response to the pandemic, the Chilean Ministry of Health implemented different vaccination schemes against SARS-CoV-2. After two doses of vaccines, reinforcements were made with the BNT162b2, CoronaVac or mRNA-1273 vaccines (6, 20, 35). Recent studies carried out by health workers reveal that homologous vaccination presents better results than heterologous schemes (36). Due to the increased risk of contracting severe COVID-19 by the population using immunosuppressive treatments, such as IMDRs patients, it is necessary to analyze the efficacy of vaccination against SARS-CoV-2 in this population. Studies carried out with the CoronaVac (37) and BNT162b2 (11) vaccines show good immunogenicity for IMDRs patients. However, metadata analysis studies suggest that IMDRs patients may obtain better results if they are inoculated with a homologous vaccination scheme (38). This is consistent with our results, where a homologous vaccination system showed a higher neutralizing antibody titer against SARS-CoV-2.
The humoral response of each IMRDs was evaluated, but it has limitations due to the small sample size of some diseases included, such as PsA, AS, SV and SS. The humoral response of RA patients against the parental Wuhan strain did not show differences compared to healthy controls, but against the Omicron variant, a significant decrease in the NAbs titers was observed compared to healthy controls. The other diseases included did not show differences in humoral response. The high humoral response achieved in these diseases demonstrates the effectiveness of the 4th dose of vaccine against SARS-CoV-2. The decreased response against the Omicron variant in RA patients may be secondary to immunosuppressive treatment. In a study of two-dose regimen of the BNT162b2 vaccine in patients with PsA, axial spondylarthritis, SLE and Large vessel vasculitis, the seropositive rate was above 90%. In patients with RA, the seropositive rate was 82.1%, whereas the lowest seropositive rate (<40%) was observed in patients with ANCA-associated vasculitis and idiopathic inflammatory myositis (11) Our study provides information on the impact of pharmacological treatments on the immunogenicity induced by vaccination. GC are commonly used in combination with other drugs, making it difficult to assess their effect in monotherapy. A reduction in immunity from SARS-CoV-2 vaccines has been reported in patients receiving GC therapies (11, 39). Likewise, our data reveal that the use of GC in combination with other therapies decreases the titer of NAbs against SARS-CoV-2.
The impact of MTX treatment on the immunogenic response to vaccination has been analyzed in various scientific papers, showing an adverse effect on the humoral and cellular immune response to mRNA vaccines (11, 12). Due to this, the possibility of suspending MTX two weeks before vaccination to favour the immunogenicity of the vaccine against SARS-CoV-2 has been discussed (40, 41). However, other authors point out that this suspension does not improve the response to the vaccine or could cause flares of the disease in patients who are not stable (42, 43). Our data indicates that the combined use of methotrexate with other drugs reduces the humoral immune response, but the analysis of the individual impact of the drug does not show statistical differences, although a median similar to the combined treatment is observed. Our data also reveal that other DMARDs, such as LEF and mycophenolate, are associated with decreased immunogenic response to vaccination, as has been observed in other studies (11, 44). HCQ, in combination, also decreased the humoral response in this study, but HCQ is frequently combined with MTX, so this could be an effect of MTX.
In addition to the limitations mentioned above, we can indicate the sample size of the control group, which was smaller than the group of rheumatological patients. Besides the sample size of the control group, it can be mentioned that the age of the control group was significantly lower. This was due to the vaccination process that occurred in Chile and how certain groups of the population were prioritized for the fourth dose, which meant that the vaccination times of the rheumatological group coincided with the health personnel, who on average are younger than the patients. It is important to take this bias into consideration when interpreting the results; in any case, the necessary statistical analyzes were carried out.
Biological treatments used to control rheumatic diseases and whose objective is to inhibit cytokines do not seem to interfere with the production of antibodies induced by vaccination (11). Drugs such as golimumab, etanercept, and adalimumab, which are TNF inhibitors, and secukinumab, an interleukin 17 inhibitor, are used by the patients in our study, and no significant decrease in the production of antibodies in response to vaccination against SARS-CoV-2 was observed.
In this study, treatment with rituximab and abatacept demonstrated a significant decrease in the humoral response against the Omicron variant. Following what has been reported in other studies, patients treated with rituximab and abatacept present a decrease in the immunogenic response to vaccination (11, 45–48). The lapse of time between the administration of rituximab and vaccination is a relevant factor in the immunogenic response of IMRDs patients, showing an improvement in the serological response when there is a longer interval between both administrations (11, 47).
Conclusions
Our study provides information on the humoral response to SARS-CoV-2 vaccines in patients with IMRDs. Factors such as the different vaccination schedules, humoral response times, diagnosis, and different pharmacological treatments of IMRDs patients were considered. In IMRDs patients, the humoral response variation in the SARS-CoV-2 vaccine depends on doses and type of vaccine administered, the humoral response times and the treatment that these patients are receiving. In light of our results, it is highly relevant to carry out studies on the response to vaccination in immunosuppressed populations, since their response to vaccination differs from the general population.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Proyecto: No 161-2021 Archivo acta: N° 109. UNIVERSIDAD DE CHILE - FACULTAD DE MEDICINA COMITÉ DE ÉTICA DE INVESTIGACIÓN EN SERES HUMANOS. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
MG: Conceptualization, Investigation, Writing – original draft, Writing – review & editing, Data curation, Funding acquisition, Methodology, Project administration, Supervision. MC: Writing – original draft, Writing – review & editing, Investigation, Methodology. YG: Formal analysis, Investigation, Software, Supervision, Validation, Writing – original draft, Writing – review & editing, Data curation. CF: Methodology, Writing – review & editing. JS: Investigation, Writing – review & editing. LA: Data curation, Investigation, Writing – review & editing. EN: Investigation, Writing – review & editing. AG: Formal analysis, Investigation, Writing – review & editing. ER: Investigation, Writing – review & editing. AK: Resources, Writing – review & editing. RS: Investigation, Resources, Writing – review & editing. FV: Conceptualization, Funding acquisition, Investigation, Methodology, Resources, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. ANID Chile supports the authors through FONIS grant number SA21I0078 (MG and FV); FONDECYT grants numbers 1190156 (RS), 1211547 (FV) and through the ICM grant number ICN2021_045 (FV, AK and RS). Anillo-ANID ATE220034.
Acknowledgments
The authors wish to thank all the patients and healthy volunteers who participated in this study. Authors also thank to Joseline Catrileo, Dina Silva (Universidad de Chile).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1427501/full#supplementary-material
References
1. Curtis JR, Johnson SR, Anthony DD, Arasaratnam RJ, Baden LR, Bass AR, et al. American college of rheumatology guidance for covid-19 vaccination in patients with rheumatic and musculoskeletal diseases – version 5. Arthritis Rheumatol. (2022). doi: 10.1002/art.42372
2. Chilean Ministry of Health. INFORME EPIDEMIOLÓGICO No218 ENFERMEDAD POR SARS-CoV-2 (COVID-19) (2022). Available online at: https://www.minsal.cl/wp-content/uploads/2023/01/Informe_Epidemiolo%CC%81gico-218.pdf.
3. Creech CB, Walker SC, Samuels RJ. SARS-CoV-2 vaccines. JAMA - J Am Med Assoc. (2021) 325:1318–20. doi: 10.1001/jama.2021.3199
4. Friedman MA, Curtis JR, Winthrop KL. Impact of disease-modifying antirheumatic drugs on vaccine immunogenicity in patients with inflammatory rheumatic and musculoskeletal diseases. Ann rheumatic diseases. NLM (Medline);. (2021) 80:1255–65. doi: 10.1136/annrheumdis-2021-221244
5. Chilean Ministry of Health. Immunization Campaign against SARS-CoV-2 Early estimates of the effectiveness of booster shots in Chile. Ministry of Health of Chile specifically the SARS-CoV-2 vaccine study group MINSAL (2021).
6. Chilean Ministry of Health. Cuarta dosis de vacuna contra SARS-CoV-2 población general desde los 18 años (2022). Available online at: https://www.minsal.cl/wp-content/uploads/2022/01/Informe-Epidemiol.
7. Landewé RBM, Landewé RBM, MacHado PM, Kroon F, Bijlsma HWJ, Burmester GR, et al. EULAR provisional recommendations for the management of rheumatic and musculoskeletal diseases in the context of SARS-CoV-2. Ann Rheum Dis. (2020) 79:851–8. doi: 10.1136/annrheumdis-2020-217877
8. Lopez A, Mariette X, Bachelez H, Belot A, Bonnotte B, Hachulla E, et al. Vaccination recommendations for the adult immunosuppressed patient: A systematic review and comprehensive field synopsis. J Autoimmun. (2017) 80:10–27. doi: 10.1016/j.jaut.2017.03.011
9. Deepak P, Kim W, Paley MA, Yang M, Carvidi AB, El-Qunni AA, et al. Effect of immunosuppression on the immunogenicity of mRNA vaccines to SARS-CoV-2 : a prospective cohort study. Ann Intern Med. (2021) 174:1572–85. doi: 10.7326/M21-1757
10. Boyarsky BJ, Ruddy JA, Connolly CM, Ou MT, Werbel WA, Garonzik-Wang JM, et al. Antibody response to a single dose of SARS-CoV-2 mRNA vaccine in patients with rheumatic and musculoskeletal diseases. Ann Rheumatic Dis. (2021) 80:1098–9. doi: 10.1136/annrheumdis-2021-220289
11. Furer V, Eviatar T, Zisman D, Peleg H, Paran D, Levartovsky D, et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: A multicentre study. Ann Rheum Dis. (2021) 80:1330–8. doi: 10.1136/annrheumdis-2021-220647
12. Haberman RH, Herati RS, Simon D, Samanovic M, Blank RB, Tuen M, et al. Methotrexate hampers immunogenicity to BNT162B2 mRNA COVID-19 vaccine in immune-mediated inflammatory disease. Ann Rheum Dis. (2021) 80:1339–44. doi: 10.1101/2021.05.11.21256917
13. Balcells ME, Le Corre N, Durán J, Ceballos ME, Vizcaya C, Mondaca S, et al. Reduced immune response to inactivated severe acute respiratory syndrome coronavirus 2 vaccine in a cohort of immunocompromised patients in Chile. Clin Infect Diseases. (2022) 75:E594–602. doi: 10.1093/cid/ciac167
14. Beltrán-Pavez C, Riquelme-Barrios S, Oyarzún-Arrau A, Gaete-Argel A, González-Stegmaier R, Cereceda-Solis K, et al. Insights into neutralizing antibody responses in individuals exposed to SARS-CoV-2 in Chile. Sci Adv. (2021) 7:eabe6855. doi: 10.1126/sciadv.abe6855
15. Escobar A, Reyes-López FE, Acevedo ML, Alonso-Palomares L, Valiente-Echeverría F, Soto-Rifo R, et al. Evaluation of the immune response induced by coronaVac 28-day schedule vaccination in a healthy population group. Front Immunol. (2022) 12:766278. doi: 10.3389/fimmu.2021.766278
16. Gaete-Argel A, Saavedra-Alarcón V, Sauré D, Alonso-Palomares L, Acevedo ML, Alarcón M, et al. Impact of homologous and heterologous boosters in neutralizing antibodies titers against SARS-CoV-2 Omicron in solid-organ transplant recipients. Front Immunol. (2023) 14:1135478. doi: 10.3389/fimmu.2023.1135478
17. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. J BioMed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
18. R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2022).
19. Chilean Ministry of Health. Planificación: Vacunación contra SARS-COV-2 . Available online at: https://vacunas.minsal.cl/wp-content/uploads/2020/12/CAVEI-Subpriorizacion-personal-salud_15Dic2020.pdf.
20. Chilean Ministry of Health. DOSIS DE REFUERZO EN LA CAMPAÑA DE VACUNACIÓN CONTRA SARS-COV-2 EN CHILE FASE 2. Santiago, Chile: Elsevier B.V (2021) p. 1–9.
21. Chilean Ministry of Health. DOSIS DE REFUERZO EN LA CAMPAÑA DE VACUNACIÓN CONTRA SARS-COV-2 EN CHILE (2021). Available online at: https://www.minsal.cl/wp-.
22. Hormazábal J, Nuñez-Franz L, Rubilar P, Apablaza M, Vial C, Cortés LJ, et al. Factors influencing neutralizing antibody response to the original SARS-CoV-2 virus and the Omicron variant in a high vaccination coverage country, a population-based study. Vaccine X. (2023) 15:100372. doi: 10.1016/j.jvacx.2023.100372
23. Garcia-Beltran WF, St. Denis KJ, Hoelzemer A, Lam EC, Nitido AD, Sheehan ML, et al. mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS-CoV-2 Omicron variant. Cell. (2022) 185:457–66. doi: 10.1016/j.cell.2021.12.033
24. Garcia-Beltran WF, Lam EC, St. Denis K, Nitido AD, Garcia ZH, Hauser BM, et al. Multiple SARS-CoV-2 variants escape neutralization by vaccine-induced humoral immunity. Cell. (2021) 184:2523. doi: 10.1016/j.cell.2021.04.006
25. Cele S, Gazy I, Jackson L, Hwa SH, Tegally H, Lustig G, et al. Escape of SARS-CoV-2 501Y.V2 from neutralization by convalescent plasma. Nature. (2021) 593:142–6. doi: 10.1038/s41586-021-03471-w
26. Bayart JL, Douxfils J, Gillot C, David C, Mullier F, Elsen M, et al. Waning of igg, total and neutralizing antibodies 6 months post-vaccination with bnt162b2 in healthcare workers. Vaccines (Basel). (2021) 9:1092. doi: 10.21203/rs.3.rs-862966/v1
27. Midorikawa R, Nakama M, Furukawa H, Oka S, Higuchi T, Nagai H, et al. Detection of SARS-coV-2 nucleocapsid, spike, and neutralizing antibodies in vaccinated Japanese. Viruses. (2022) 14:965. doi: 10.3390/v14050965
28. Terpos E, Karalis V, Ntanasis-Stathopoulos I, Apostolakou F, Gumeni S, Gavriatopoulou M, et al. Sustained but Declining Humoral Immunity against SARS-CoV-2 at 9 Months Postvaccination with BNT162b2: A Prospective Evaluation in 309 Healthy Individuals. Hemasphere. (2022) 6:E677. doi: 10.1097/HS9.0000000000000677
29. Campo F, Venuti A, Pimpinelli F, Abril E, Blandino G, Conti L, et al. Antibody persistence 6 months post-vaccination with bnt162b2 among health care workers. Vaccines (Basel). (2021) 9:1125. doi: 10.3390/vaccines9101125
30. Rubbert-Roth A, Vuilleumier N, Ludewig B, Schmiedeberg K, Haller C, von Kempis J. Anti-SARS-CoV-2 mRNA vaccine in patients with rheumatoid arthritis. Lancet Rheumatol. (2021) 37:e470–2. doi: 10.1016/S2665-9913(21)00186-7
31. Furukawa H, Oka S, Higuchi T, Nakama M, Nagai N, Tohma S. Anti-SARS-coV-2 spike antibody titers and neutralizing antibodies in vaccinated rheumatoid arthritis patients. Vaccines (Basel). (2022) 10:1365. doi: 10.3390/vaccines10081365
32. Qi H, Liu B, Wang X, Zhang L. The humoral response and antibodies against SARS-CoV-2 infection. Nat Immunol. (2022) 23:1008–20. doi: 10.1038/s41590-022-01248-5
33. Dayam R, Law J, Goetgebuer R, Chao G, Abe K, Sutton M, et al. Accelerated waning of immunity to SARS-CoV-2 mRNA vaccines in patients with immune-mediated inflammatory diseases. JCI Insight. (2022) 77:e159721. doi: :10.1172/jci.insight.159721
34. Farroni C, Aiello A, Picchianti-Diamanti A, Laganà B, Petruccioli E, Agrati C, et al. Booster dose of SARS-CoV-2 messenger RNA vaccines strengthens the specific immune response of patients with rheumatoid arthritis: A prospective multicenter longitudinal study. Int J Infect Diseases. (2022) 125:195–208. doi: 10.1016/j.ijid.2022.10.035
35. Borobia AM, Carcas AJ, Pérez-Olmeda M, Castaño L, Bertran MJ, García-Pérez J, et al. Immunogenicity and reactogenicity of BNT162b2 booster in ChAdOx1-S-primed participants (CombiVacS): a multicentre, open-label, randomised, controlled, phase 2 trial. Lancet. (2021) 398:121–30. doi: 10.1016/S0140-6736(21)01420-3
36. Çiçek K, Özkaya Y, Eser E, Buran ZC, Öztürk Arıkan ZÖ, Akçalı S, et al. Efficacy of homologous and heterologous vaccine applications on SARS-coV-2 omicron variant: cohort of manisa celal bayar university healthcare workers. Mikrobiyol Bul. (2023) 57:238–51. doi: 10.5578/mb.20239918
37. Seyahi E, Bakhdiyarli G, Oztas M, Kuskucu MA, Tok Y, Sut N, et al. Antibody response to inactivated COVID-19 vaccine (CoronaVac) in immune-mediated diseases: a controlled study among hospital workers and elderly. Rheumatol Int. (2021) 41:1429–40. doi: 10.1007/s00296-021-04910-7
38. Tang KT, Hsu BC, Chen DY. Immunogenicity, effectiveness, and safety of COVID-19 vaccines in rheumatic patients: an updated systematic review and meta-analysis. Biomedicines. (2022) 10:834. doi: 10.3390/biomedicines10040834
39. Geisen UM, Berner DK, Tran F, Sümbül M, Vullriede L, Ciripoi M, et al. Immunogenicity and safety of anti-SARS-CoV-2 mRNA vaccines in patients with chronic inflammatory conditions and immunosuppressive therapy in a monocentric cohort. Ann Rheum Dis. (2021) 80:1306–11. doi: 10.1136/annrheumdis-2021-220272
40. Coates LC, Abhishek A. Suspending methotrexate for 2 weeks after COVID-19 vaccination. Vol. 4 Lancet Rheumatol Elsevier Ltd;. (2022) p:e740–1. doi: 10.1016/S2665-9913(22)00265-X
41. Park JK, Lee YJ, Shin K, Ha YJ, Lee EY, Song YW, et al. Impact of temporary methotrexate discontinuation for 2 weeks on immunogenicity of seasonal influenza vaccination in patients with rheumatoid arthritis: A randomised clinical trial. Ann Rheum Dis. (2018) 77:898–904. doi: 10.1136/annrheumdis-2018-213222
42. Xie Y, Liu Y, Liu Y. The flare of rheumatic disease after SARS-coV-2 vaccination: A review. Front Immunol. (2022) 13:919979. doi: 10.3389/fimmu.2022.919979
43. Durez P, Combe B. Should we stop methotrexate or not for vaccination? RMD Open. (2023) 9:e002798. doi: 10.1136/rmdopen-2022-002798
44. van Sleen Y, van der Geest KSM, Huckriede ALW, van Baarle D, Brouwer E. Effect of DMARDs on the immunogenicity of vaccines. Nat Rev Rheumatol. (2023) 19:560–75. doi: 10.1038/s41584-023-00992-8
45. Sieiro Santos C, Calleja Antolin S, Moriano Morales C, Garcia Herrero J, Diez Alvarez E, Ramos Ortega F, et al. Immune responses to mRNA vaccines against SARS-CoV-2 in patients with immune-mediated inflammatory rheumatic diseases. RMD Open. (2022) 8:e001898. doi: 10.1136/rmdopen-2021-001898
46. Spiera R, Jinich S, Jannat-Khah D. Rituximab, but not other antirheumatic therapies, is associated with impaired serological response to SARS- CoV-2 vaccination in patients with rheumatic diseases. Ann Rheumatic Diseases. (2021) 80:1357–9. doi: 10.1136/annrheumdis-2021-220604
47. Schultz K, Jannat-Khah D, Spiera R. B cell reconstitution is associated with COVID-19 booster vaccine responsiveness in patients previously seronegative treated with rituximab. J Rheumatol. (2023) 50:420–5. doi: 10.3899/jrheum.22047
48. Auroux M, Laurent B, Coste B, Massy E, Mercier A, Durieu I, et al. Serological response to SARS-CoV-2 vaccination in patients with inflammatory rheumatic disease treated with disease modifying anti-rheumatic drugs: A cohort study and a meta-analysis. Joint Bone Spine. (2022) 89:105380. doi: 10.1016/j.jbspin.2022.105380
Keywords: SARS-CoV-2, COVID-19 vaccines, autoimmune rheumatic diseases, humoral IgG, immunosuppressive therapies
Citation: Gallardo-Nelson MJ, Cruces M, Gómez YM, Fuenzalida C, Silva J, Aravena-Traipi L, Nuñez E, Gaete-Angel A, Rivas-Yañez E, Kalergis AM, Soto-Rifo R and Valiente-Echeverria F (2024) 4th booster-dose SARS-CoV-2 heterologous and homologous vaccination in rheumatological patients. Front. Immunol. 15:1427501. doi: 10.3389/fimmu.2024.1427501
Received: 13 May 2024; Accepted: 08 July 2024;
Published: 26 July 2024.
Edited by:
Ritthideach Yorsaeng, Chulalongkorn University, ThailandCopyright © 2024 Gallardo-Nelson, Cruces, Gómez, Fuenzalida, Silva, Aravena-Traipi, Nuñez, Gaete-Angel, Rivas-Yañez, Kalergis, Soto-Rifo and Valiente-Echeverria. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Jose Gallardo-Nelson, bWFyaWFqb3NlLmdhbGxhcmRvQHVkYS5jbA==; Yolanda M. Gómez, eWdvbWV6QHViaW9iaW8uY2w=