
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 08 October 2024
Sec. Viral Immunology
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1422349
This article is part of the Research Topic Immunogenetics in times of COVID-19 pandemic View all 20 articles
 Ingrid Marins de Almeida1
Ingrid Marins de Almeida1 Bruna Ramos Tosta1
Bruna Ramos Tosta1 Laiane da Cruz Pena1Hatilla dos Santos Silva1Fabiane S. Reis-Goes2Nívia N. Silva2João Victor Andrade Cruz1Mailane dos Anjos Silva1Jéssica Francisco de Araújo1
Laiane da Cruz Pena1Hatilla dos Santos Silva1Fabiane S. Reis-Goes2Nívia N. Silva2João Victor Andrade Cruz1Mailane dos Anjos Silva1Jéssica Francisco de Araújo1 Juliana Lopes Rodrigues1Gabriella Oliveira3
Juliana Lopes Rodrigues1Gabriella Oliveira3 Ricardo Gassmann Figueiredo4
Ricardo Gassmann Figueiredo4 Sara Nunes Vaz5
Sara Nunes Vaz5 Iris Montaño-Castellón5Daniele Santana5Alex Torres2
Iris Montaño-Castellón5Daniele Santana5Alex Torres2 Fabyan Esberard de Lima Beltrão6
Fabyan Esberard de Lima Beltrão6 Valdirene Leão Carneiro7
Valdirene Leão Carneiro7 Gubio Soares Campos8
Gubio Soares Campos8 Carlos Brites5
Carlos Brites5 Vitor Fortuna2
Vitor Fortuna2 Camila Alexandrina Figueiredo1
Camila Alexandrina Figueiredo1 Soraya Castro Trindade2,4
Soraya Castro Trindade2,4 Helton Estrela Ramos9
Helton Estrela Ramos9 Ryan dos Santos Costa1*
Ryan dos Santos Costa1*Introduction: The COVID-19, triggered by the SARS-CoV-2 virus, has varied clinical manifestations, ranging from mild cases to severe forms such as fatal pneumonia and acute respiratory distress syndrome (ARDS). Disease severity is influenced by an exacerbated immune response, characterized by high pro-inflammatory cytokine levels. Inhibition of AKT can potentially suppress pathological inflammation, cytokine storm and platelet activation associated with COVID-19. In this study, we aimed to investigate the rs2494746 and rs1130214 variants in the AKT1 gene associated with severe COVID-19 outcomes.
Methods: Peripheral blood samples and sociodemographic data from 508 individuals with COVID-19, measuring plasma cytokine concentrations using ELISA and genotyped the AKT1 variants.
Results: The rs2494746-C allele was associated with severity, ICU admission, and death from COVID-19. The C allele at rs1130214 was linked to increased TNF and D-dimer levels. Moreover, both variants exhibited an increased cumulative risk of disease severity, ICU admission, and mortality caused by COVID-19. In the predictive analysis, the rs2494746 obtained an accuracy of 71%, suggesting a high probability of the test determining the severity of the disease.
Discussion: Our findings contribute to understanding the influence of the AKT1 gene variants on the immunological damage in individuals infected with SARS-CoV-2.
COVID-19, caused by the SARS-CoV-2 virus, has emerged as a worldwide crisis. Transmitted mainly through the respiratory route, the virus infiltrates the host by binding to angiotensin-converting enzyme 2 (ACE2) receptors, found extensively in tissues and immune cells. This invasion can give rise to diverse clinical manifestations, ranging from mild cases to severe or critical forms that can lead to fatal outcomes (1).
Several studies have reported that immunopathological damage caused by highly elevated levels of pro-inflammatory cytokines produced by immune and epithelial cells can lead to fatal pneumonia and acute respiratory distress syndrome (ARDS) (2). As accumulating evidence indicates that severe COVID-19 is a multifaceted inflammatory disease affecting multiple systems, it’s also worth noting that comorbidities like hypertension, heart failure, cardiac arrhythmia, diabetes, kidney failure, and chronic lung disease, as well as factors such as older age and male gender, are linked to unfavorable clinical outcomes (3).
Host genetics may also be important in the severity of COVID-19. AKT, a serine/threonine protein kinase that has 3 isoforms (AKT1, AKT2, and AKT3), is part of the PI3K/AKT/mTOR pathway, a crucial cellular signaling pathway that regulates various cellular functions (4). A proteomics and transcriptomics study demonstrated that cells infected with SARS-CoV-2 showed increased AKT/mTOR pathway signaling. Inhibiting this pathway can significantly reduce virus production (5). The PI3K/AKT pathway regulates the generation and function of regulatory T cells (Tregs) (6). This suggests that increasing the population of regulatory T cells (Tregs) might promote lung recovery in patients diagnosed with acute respiratory distress syndrome (7).
Although hyperactivation of various immune system cellular components has been observed in patients with severe COVID-19, the host genetic factors determining susceptibility to disease severity are not entirely understood (8). Previous studies have shown that variants of the AKT1 gene may be associated with other diseases (9–12).
Our studies previously indicated a possible implication of the AKT/mTOR pathway in severe manifestations of COVID-19. The association of the rs1057079 variant of the MTOR gene with severe and critical outcomes suggests a direct influence of this pathway on disease severity. Furthermore, the association between the rs2536 variant and elevated levels of IL-6 and mortality from COVID-19 suggests a possible role for this pathway in regulating the exacerbated inflammatory response characteristic of the cytokine storm observed in severe cases of the disease (13). These findings provide important insights into the potential impact of the AKT/mTOR pathway on the pathophysiology of COVID-19. Therefore, this study aimed to investigate the association between variants in the AKT1 gene and worse outcomes of COVID-19.
Five hundred-eight individuals with COVID-19, 216 mild cases and 292 severe cases, were recruited from April 2020 to April 2021, prior to the national vaccination period. Severe cases were recruited at Hospital Metropolitano Dom José Maria Pires (Paraíba, Brazil), Hospital EMEC (Empreendimentos Médico Cirúrgicos Ltda), and Hospital Couto Maia (Bahia, Brazil). Among the severe cases, 103 patients were admitted to the Intensive Care Unit (ICU), and 53 died. A non-probabilistic sample of mild subjects was recruited at the Primary Care Unit of the Professor Edgard Santos University Hospital - HUPES (Bahia, Brazil) and in the community.
Recruitment was conducted through three studies previously approved by the Human Research Ethics Committee of the Lauro Wanderley University Hospital (Paraíba, Brazil) under n°. 31562720.9.0000.5183, by the Research Ethics Committee of the State University of Feira de Santana (Bahia, Brazil) under n°. 30764720.1.0000.0053, and the Research Ethics Committee of HUPES (Bahia, Brazil) under no. 31748320.3.1001.5543.
Confirmation of infection was performed by quantitative reverse transcription polymerase chain reaction (RT-qPCR) testing for SARS-CoV-2 with samples from the respiratory tract (nasopharyngeal swab, airway aspiration, or sputum induction) or in cases of negative RT-qPCR, clinical, radiological diagnosis (ground-glass opacities, with or without consolidation, located close to visceral pleural surfaces and bilateral distribution - CO-RADS 5) and positive serological test (IgG for SARS-CoV-2) were used (14).
The definition of severity within 48 hours after patient admission was established using two scoring systems: 1) the “Quick Sequential Organ Failure Assessment (qSOFA)” score, 2) the “National Early Warning Score 2 (NEW2)”, analyzing CT scans and application of the severity score (15) or accessing parameters such as pulse oxygen saturation less than 94%, respiratory rate persistently above 24 breaths per minute, or indication for hospital admission.
Intensive care unit (ICU) admission data and mortality were used for secondary analyses. The severe group was divided into critical patients - individuals admitted to the ICU, and non-critical patients – individuals not admitted to the ICU. Blood samples were collected before interventions or therapies that could interfere with cytokine results. We considered the mild form of the disease to be all individuals with SARS-CoV-2 infection and the absence of the aforementioned risk factors.
DNA extraction was performed from whole blood and buffy coat samples according to the standard protocol with the FlexiGene® DNA kit (Qiagen GmbH, Hilden, Germany). DNA concentration and purity were estimated by spectrophotometry with the “NanoDrop™ Lite Spectrophotometer” (Thermo Fisher Scientific, Wilmington, DE, USA). We standardized at a 5 ng/μL concentration using nuclease-free water in a 96-well molecular biology plate and stored in a freezer at -20°C for later use.
The SNPs rs1130214 and rs2494746 were selected for genotyping based on specific criteria. These criteria included minor allele frequency (MAF) between 0.05 and 0.5, functional impact on the gene assessed by RegulomeDb (http://regulomedb.org/), and previous associations with clinical conditions related to AKT1 gene expression and an unfavorable COVID-19 prognosis, such as cancer, lung, viral, heart, and mental diseases, as indicated by Ensembl (http://www.ensembl.org/index.html) and the National Center for Biotechnology Information (NCBI) (http://www.ncbi.nlm.nih.gov/). Additionally, linkage disequilibrium with other variants was also considered, as assessed by HaploReg V4.1 (http://compbio.mit.edu/HaploReg).
The genotyping assay was performed with the GoTaq Probe qPCR Master Mix kit (Promega, WI) and the TaqMan® SNP Genotyping Assays probe (Thermo Fisher Scientific, Waltham, MA, USA). RT-qPCR was performed on the QuantStudio ™ 12K Flex Real-Time PCR System (Applied Biosystems, Life Technologies, Carlsbad USA).
Plasma concentrations of cytokines were measured using the Human TNF alpha Uncoated ELISA, Human IL-6 Uncoated ELISA, and Human CCL2 (MCP-1) Uncoated ELISA (Invitrogen; Thermo Fisher Scientific, Waltham, MA, USA) according to the manufacturer’s protocol. We used the Multiskan GO Spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA) to read the absorbance at 450 nm. The kit’s detection limit was 4–500 pg/mL for TNF, 2–200 pg/mL for IL-6, and 7-1000 pg/mL for CCL2. A standard curve was generated with the optical density (OD) values, and to perform the comparative analysis, only samples with concentrations ≥ the lowest point of the curve of each cytokine kit were used.
According to the manufacturer’s protocol, D-dimer plasma concentrations were assessed using chemiluminescence immunoassay (MAGLUMI-2000-PLUS, Shenzhen New Industries Biomedical Engineering Co., Shenzhen, China).
Descriptive statistical analyses were performed on comparative groups, such as the chi-square test, Fisher’s exact test, and Mann-Whitney U test, using IBM® SPSS® Statistics 25 software (SPSS Inc., Illinois, USA). For quality control of genotyping data, the following filters were applied: genotyping rate < 0.90 and minor allele frequency (MAF) < 0.05. Association analyses for categorical variables were conducted using logistic regression with three genetic models of inheritance (additive, dominant, and recessive) in PLINK 1.9 software.
To estimate the cumulative contribution of risk alleles to outcomes, individuals were categorized into groups with no risk allele or with one risk allele (≤1, GG+AA; GG+AC; AA+CG), two alleles (GG+CC; CC+AA; CG+AC), three risk alleles (CG+CC; CC+AC), and four risk alleles (CC+CC). Logistic regression analyses for severity and critical outcomes were performed using R Statistical Software packages (v 4.1.1; R Core Team 2022). Both analyses were adjusted for defined covariate values, such as age, sex, hypertension, diabetes, and heart disease for the severity variable; age, sex, diabetes, and heart disease for the critical condition variable; and age and sex for the death variable.
For cytokine and D-dimer analyses, normality was initially assessed using the Kolmogorov-Smirnov test. Considering the non-parametric distribution of the data, an unpaired two-tailed Mann-Whitney U test was employed for comparisons between groups, and the data were presented as median and interquartile range. Survival analysis was conducted using the Kaplan-Meier method to plot survival curves for a subsample of severe cases, the log-rank test (Mantel-Cox) to compare the two survival curves, and the Hazard Ratio (Mantel-Haenszel) to measure the time at which individuals died. GraphPad Prism 8 statistical software (GraphPad Inc., San Diego, CA) was utilized for both analyses.
The prediction analysis involved conducting Cohen’s Kappa Test to assess the agreement between the variable of interest (disease severity) and the genotypes of the rs2494746 and rs1130214 variants, using IBM® SPSS® Statistics 25 software (SPSS Inc., Illinois, USA). After obtaining the test results, the following performance metrics were calculated: Accuracy (A/(A+B+C+D)), Sensitivity (A/(A+C)), Specificity (D/(B+D)), Positive Predictive Value (PPV) (A/(A+B)), and Negative Predictive Value (NPV) (D/(C+D)). The values A, B, C, and D, representing true positives, false negatives, false positives, and true negatives, respectively, were used in the calculations of the mentioned metrics.
Values of p < 0.05 were considered statistically significant.
In the descriptive table, it is possible to observe the significant prevalence (p<0.05) of elderly individuals, male and with comorbidities such as hypertension (60.3%), diabetes mellitus (42.2%), and cardiopathy (18.3%) in the severe group compared with the mild group (Table 1).
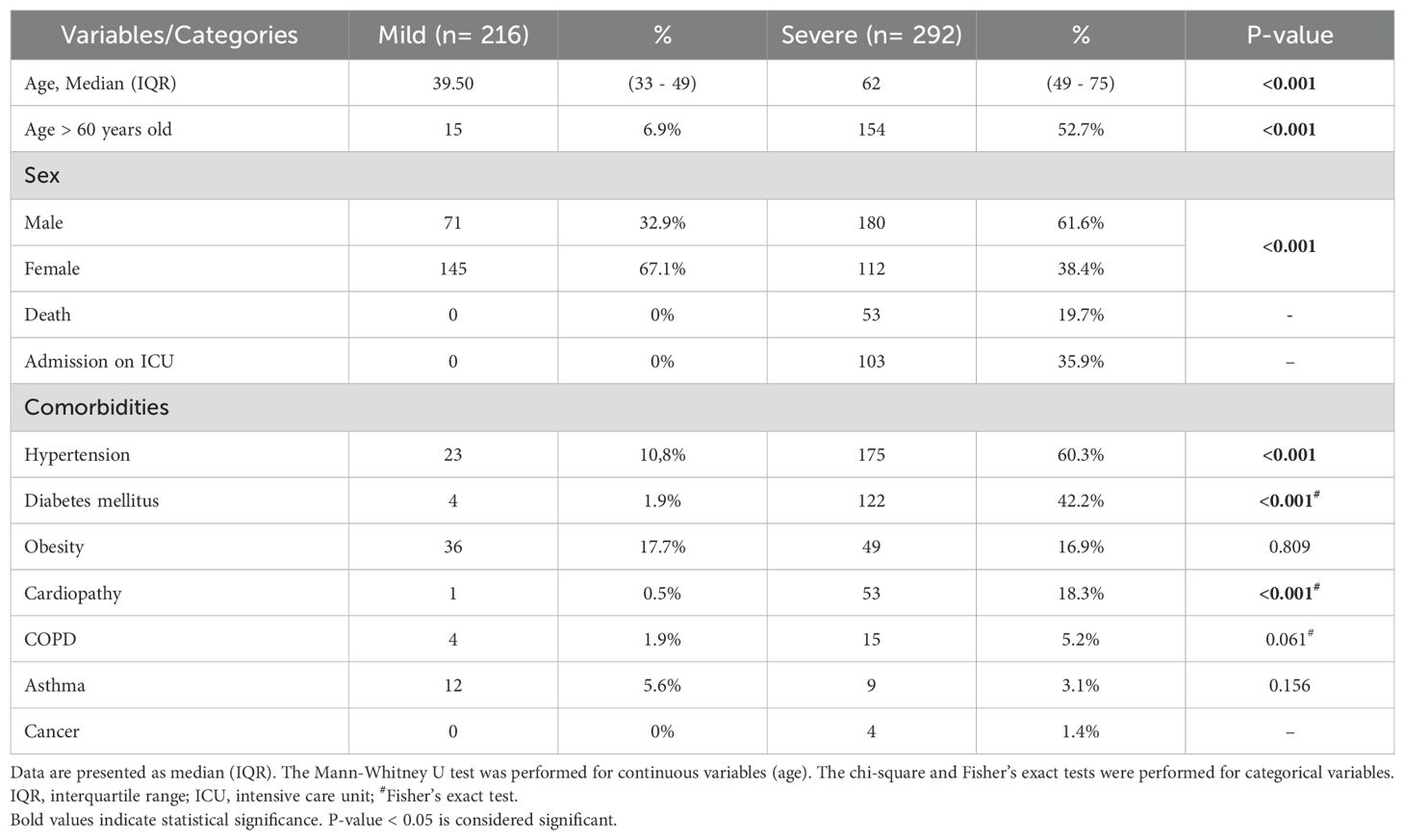
Table 1. Characteristics of the population according to the COVID-19 severity and variables included in this study.
Two single nucleotide polymorphisms (SNPs) of the AKT1 gene, rs2494746, and rs1130214, located on chromosome 14, were selected. The rs2494746 is an intronic variant found at position 104791382 (GRCh38.p14; NC_000014.9) that presents a polymorphic G allele with a minor allele frequency (MAF) of 39% in this population. While the rs1130214 variant is located in the 5’ UTR position of the gene, the messenger RNA (mRNA) region that is directly upstream of the initiation codon, with the polymorphic allele A having a MAF of 31% (Supplementary Table S1).
A significant association was found between the C risk allele of the SNP rs2494746 and the greater chance of the individual presenting the most severe form of the disease after infection with SARS-CoV-2 in the additive model (OR: 1.79; 95%CI: 1.28-2.50) and dominant model (OR: 7.81; 95%CI: 3.74-16.31). The rs1130214 association did not reach statistical significance (Table 2).
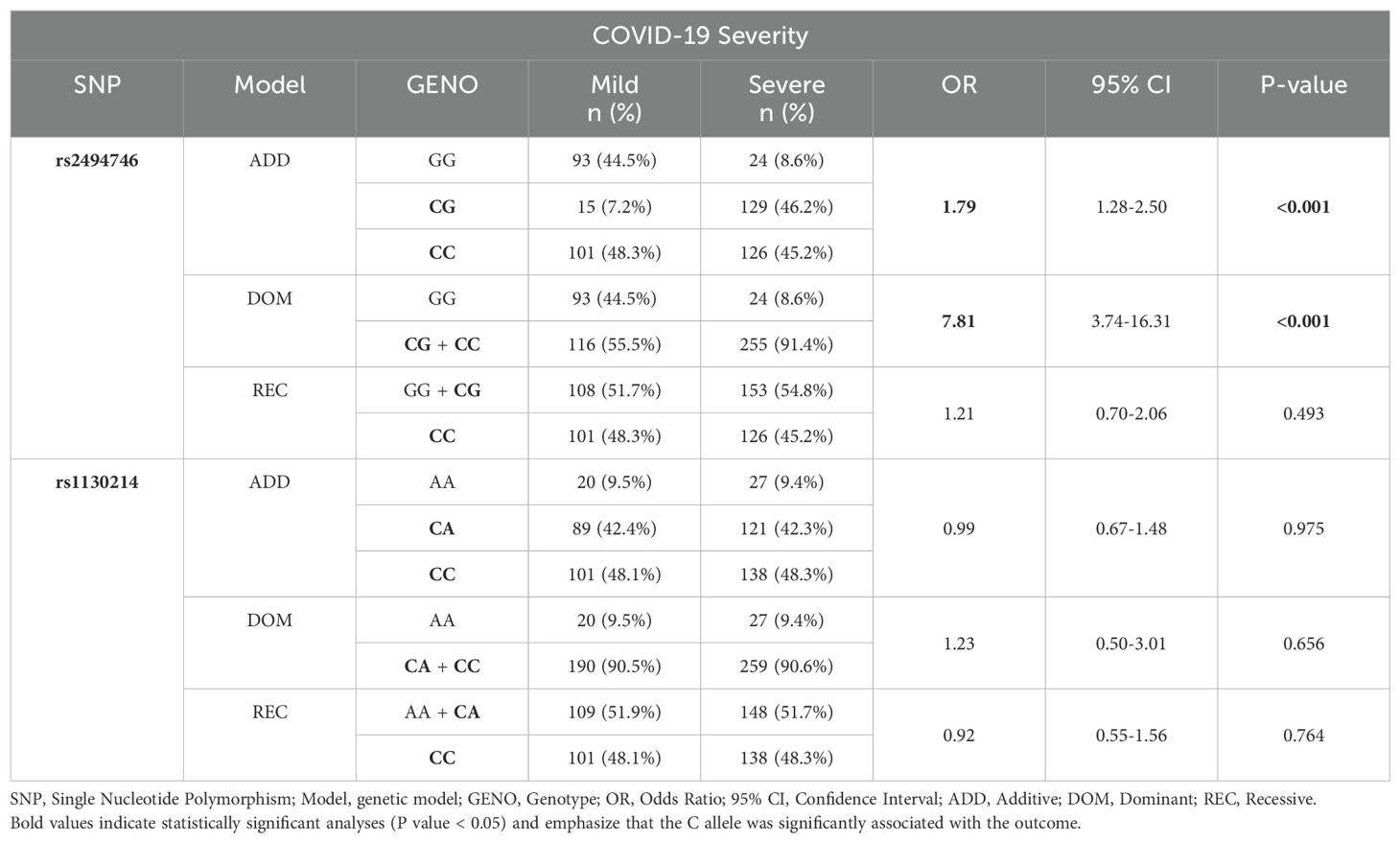
Table 2. A significant association between SNP on AKT1 gene and severity of COVID-19 by logistic regression adjusted for age, sex, hypertension, diabetes, and cardiopathy.
Individuals with severe COVID-19 carrying at least one C allele of the SNP rs2494746 (genotypes CG and CC) exhibited a high frequency of ICU admission. These genotypes were associated with a significantly higher risk of ICU admission, with an OR of 4.026 (95% CI: 1.15-13.98) and a p-value of 0.028, compared to those with the GG genotype (Table 3).
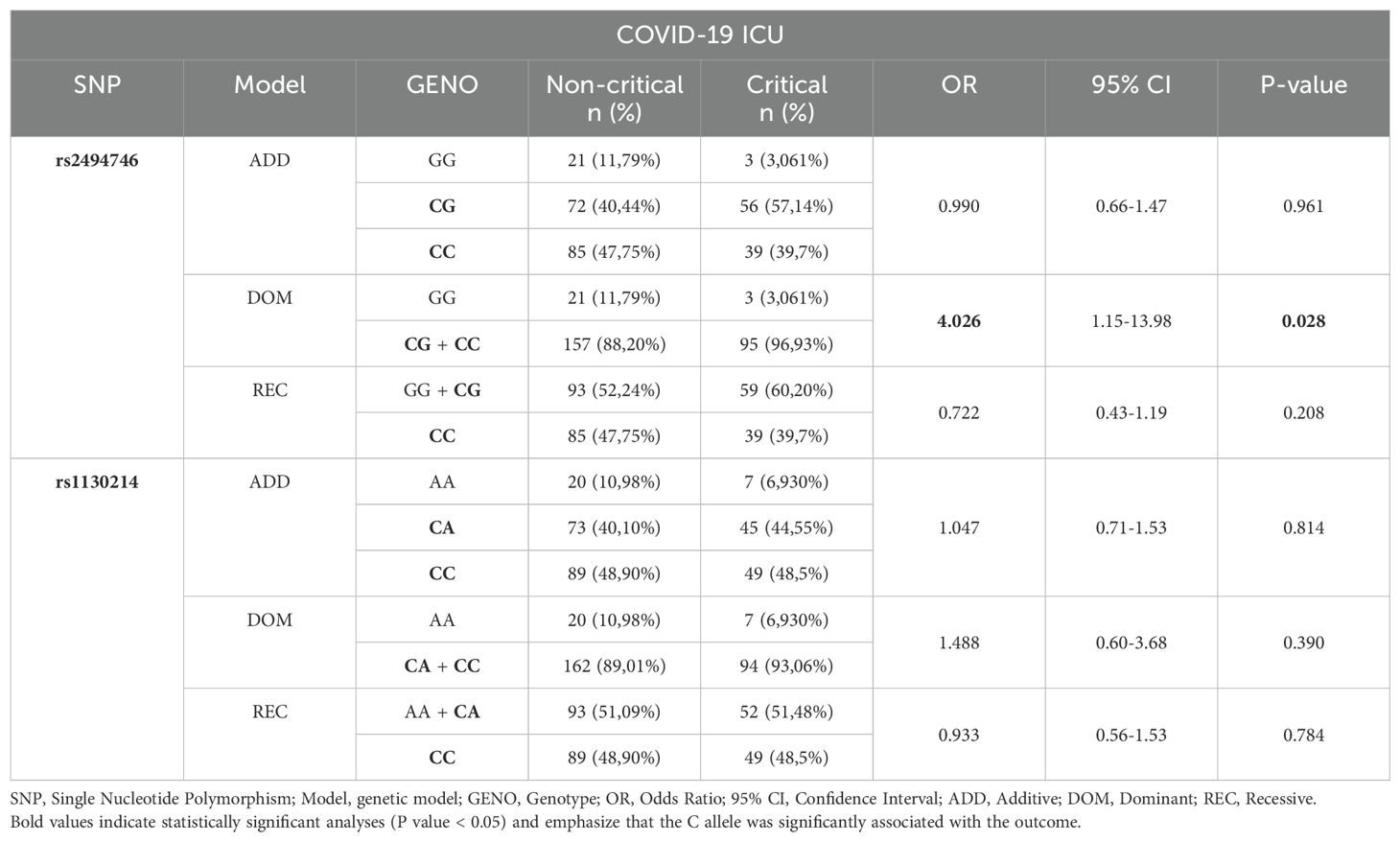
Table 3. A significant association between SNP in the AKT1 gene and patients admitted to the ICU with severe COVID-19 by logistic regression adjusted for age, sex, diabetes, and cardiopathy.
Among all individuals with COVID-19, those carrying at least one C allele of rs2494746 presented more than 7-fold higher chance of being admitted to the ICU compared with patients without this allele-specific expression in the dominant model (OR: 7.81; 95%CI: 3.74-16.31, Supplementary Table S2). The rs1130214 was not associated with hospitalization (Supplementary Table S2).
The genotype risk score of the SNPs rs2494746 and rs1130214 was analyzed. The individuals were divided into groups without any risk allele or with one risk allele (≤1, GG+AA; GG+AC; AA+CG), with two risk alleles (GG+CC; CC+AA; CG+AC), three risk alleles (CG+CC; CC+AC), and four risk alleles (CC+CC). Individuals with 2 and 3 risk alleles were four times more likely to develop severe COVID-19 (OR:4.04; CI:1.73-9.40; p=0.001 and OR:4.71; IC:2.03-10.97 p<0.001). Meanwhile, individuals with four risk alleles were twice as likely to develop the severity of the disease (OR:2.61; CI:1.21-5.64; p=0.015) (Table 4).
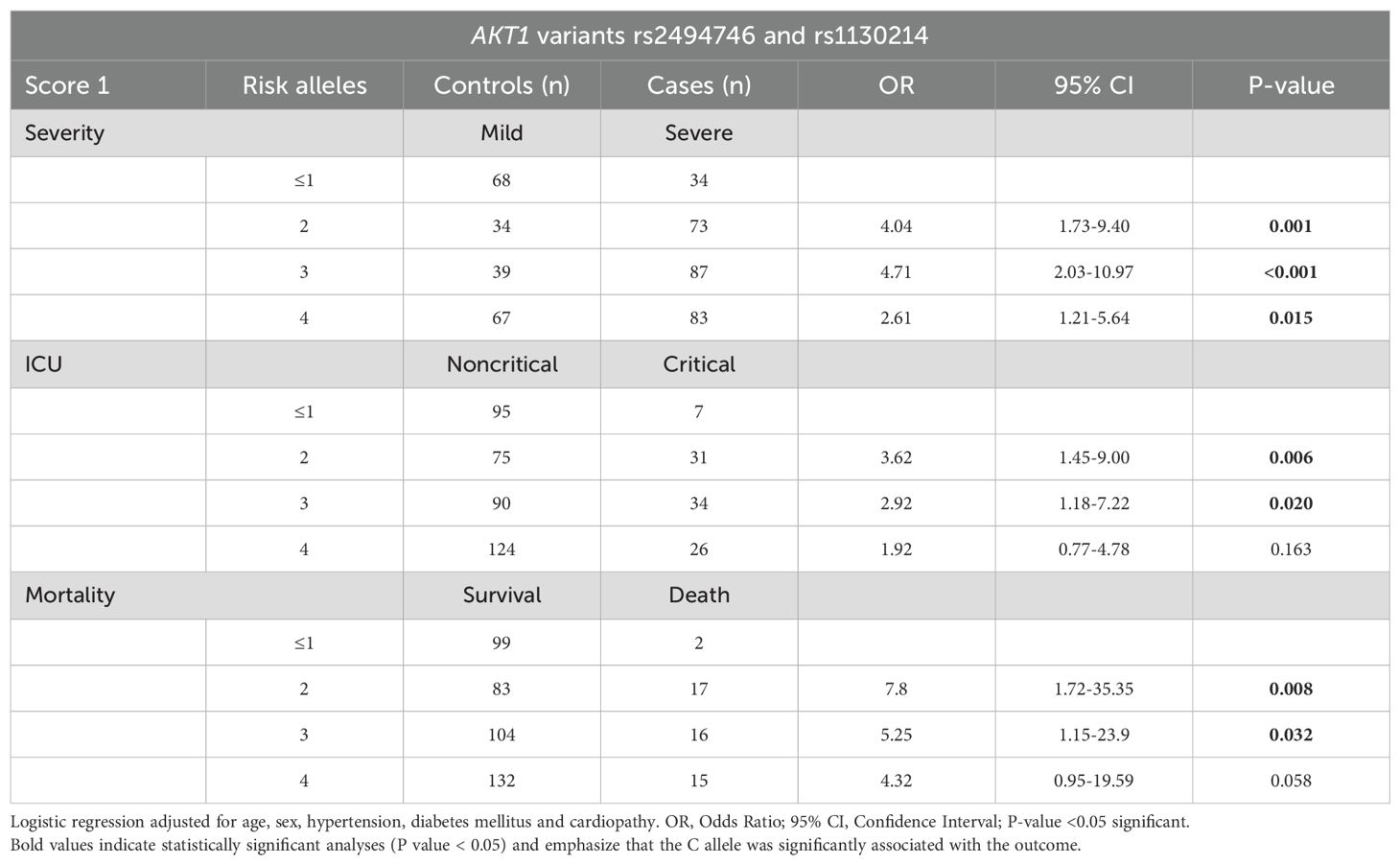
Table 4. Genotyping risk score analysis for severity, ICU and mortality with rs2494746 and rs1130214 AKT1 variants.
The analysis of disease criticality and mortality demonstrated that individuals with two or three risk alleles were associated with approximately three times greater chance of having the critical condition (OR:3.62; CI:1.45-9.00; p=0.006 and OR:2.92; CI:1.18-7.22; p=0.020) and seven times more chance of dying (OR:7.8; CI:1.72-35.35; p=0.008 and OR:5.25; CI:1.15-23.9; p=0.032) (Table 4).
Individuals homozygous AA of rs1130214 had low concentrations of TNF when compared with individuals who carried the allele C (AC/CC) (p =0.0063, Figure 1B). We did not find statistical significance when analyzing the association between TNF levels and rs2494746 genotypes (Figure 1A). No difference was found in IL-6 and CCL2 levels between the genotypes of both SNPs (Supplementary Figure S1).
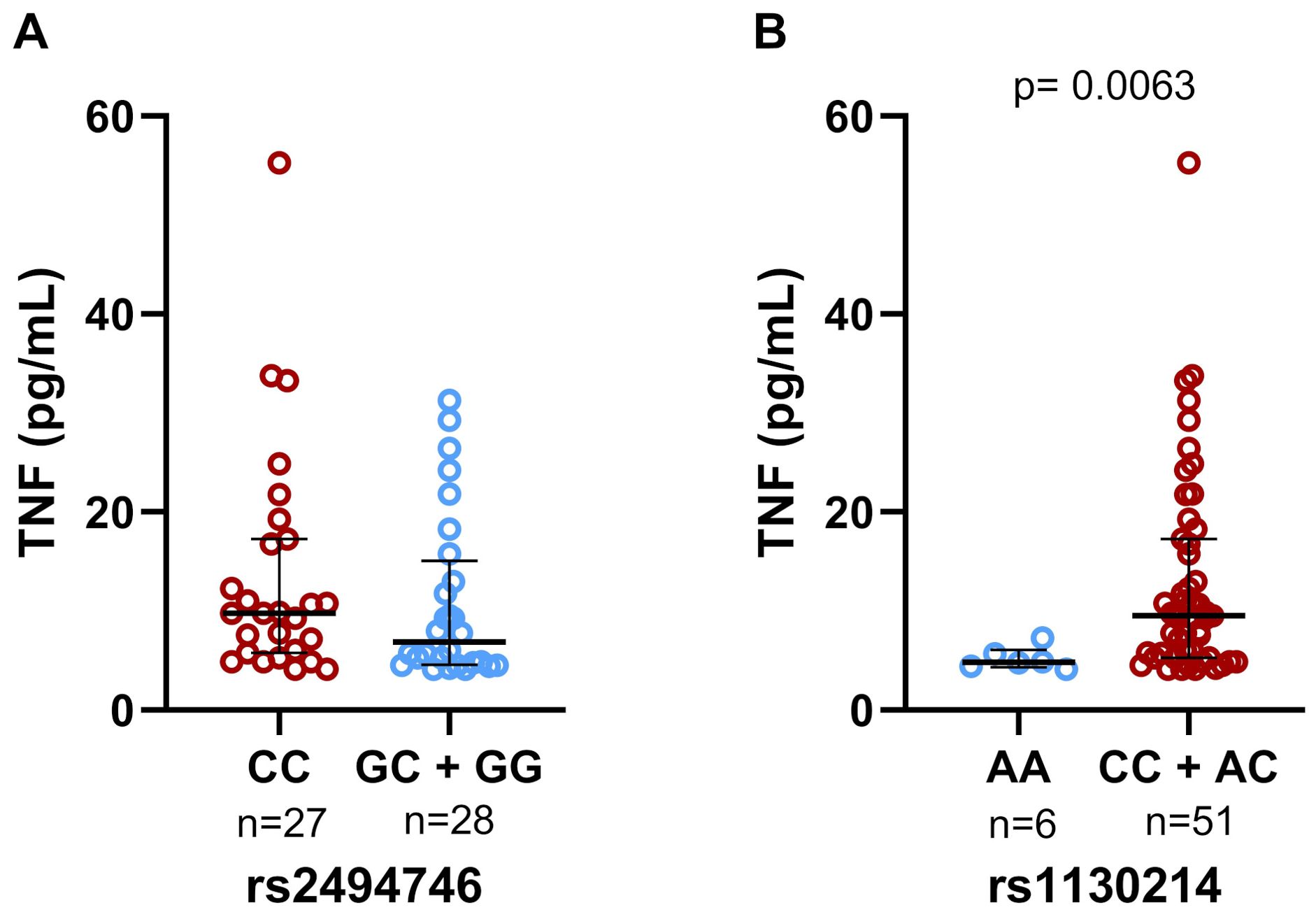
Figure 1. Genotypic association of the rs2494746 and rs1130214 variants with cytokine levels. (A) There was no statistical significance in the plasma levels of TNF between the genotypes of the rs2494746; (B) The risk allele C (rs1130214) was significantly associated with increased levels of TNF. Data are presented as median and interquartile ranges for non-parametric distribution. The unpaired two-tailed Mann-Whitney U test was used for comparisons between groups (p= 0.0063).
Analyzing the cytokine levels and the genetic profiles of individuals afflicted with severe COVID-19, we noted findings consistent with our prior study. Notably, individuals carrying the rs1130214 risk allele (C) exhibited elevated concentrations of TNF. (p=0.0014, Supplementary Figure 2B).
When analyzing D-dimer levels and genotypes among patients with COVID-19 admitted to the ICU, we observed that rs1130214 homozygous CC individuals had high concentrations of D-dimer when compared to individuals with the A allele (AA/AC) (p<0.0001, Figure 2B). This difference was not observed in rs2494746 (Figure 2A).
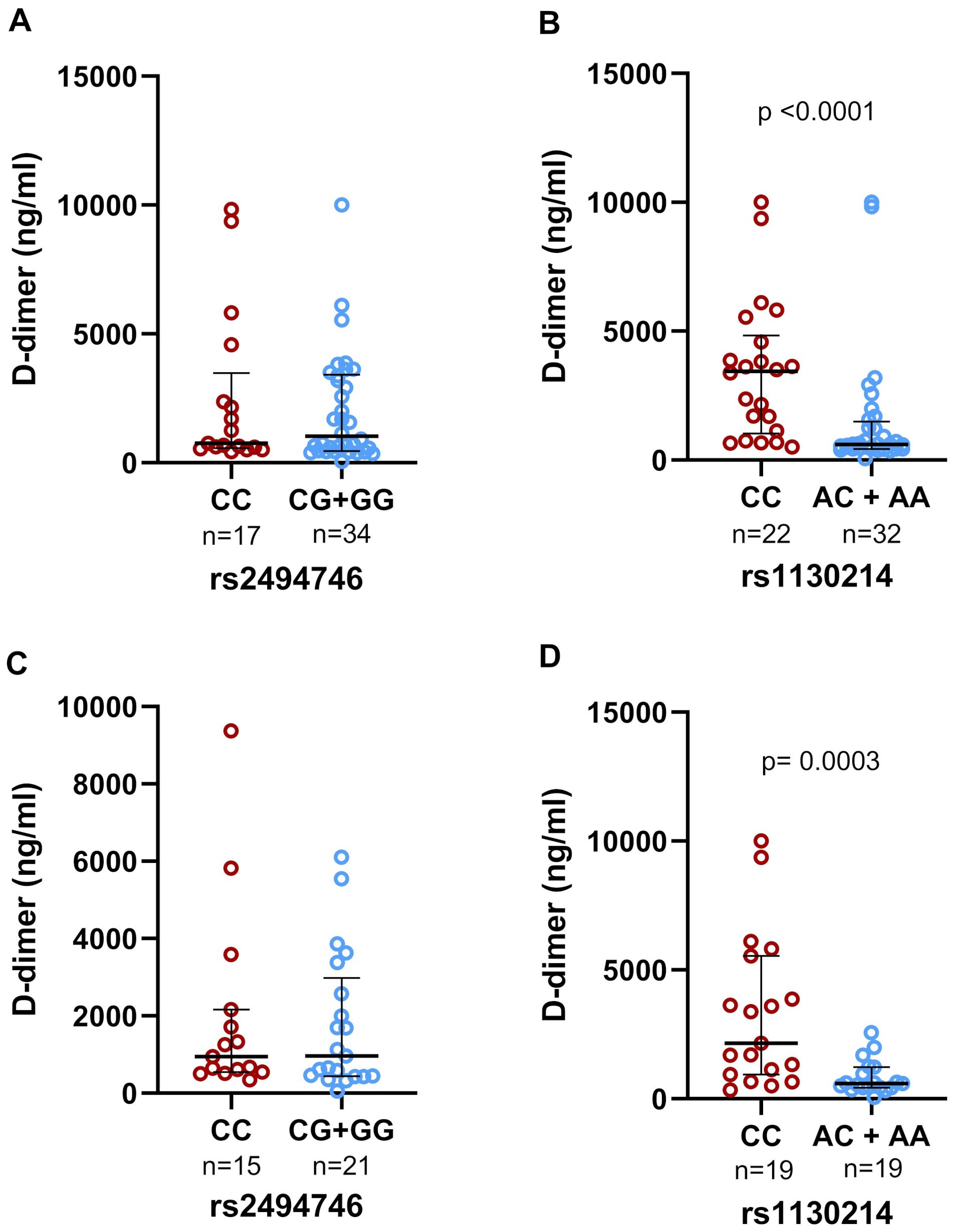
Figure 2. Genotypic association of the rs2494746 and rs1130214 variants with d-dimer levels in the plasma of individuals with COVID-19 in severe cases of Paraíba. There was no statistical difference between the rs2494746 genotypes in (A) individuals admitted to the ICU and (C) individuals who died. Homozygotes for the C risk allele (rs1130214) were significantly associated with increased d-dimer levels compared to individuals carrying the AC or AA genotype in (B) individuals admitted to the ICU and (D) individuals who died. Data are presented as median and interquartile ranges for non-parametric distribution. The unpaired two-tailed Mann-Whitney U test was used for comparisons between groups (p<0.0001 – p=0.0003).
Furthermore, when analyzing the D-dimer concentration in patients who died, individuals with genotype CC of rs1130214 had higher concentrations than AA/AC individuals (p=0.0003, Figure 2D). The rs2494746 variant showed no significant difference (Figure 2C).
The Kaplan-Meier graph showed no significant difference in the survival of individuals infected with SARS-CoV-2 based on different genotypes of the studied variants. However, patients with at least one C allele of AKT1 variants exhibited a prolonged hospital stay compared to homozygote individuals (Figures 3A, B). This suggests that the presence of the C allele may be associated with an extended duration of hospitalization and an increased risk of mortality from COVID-19.
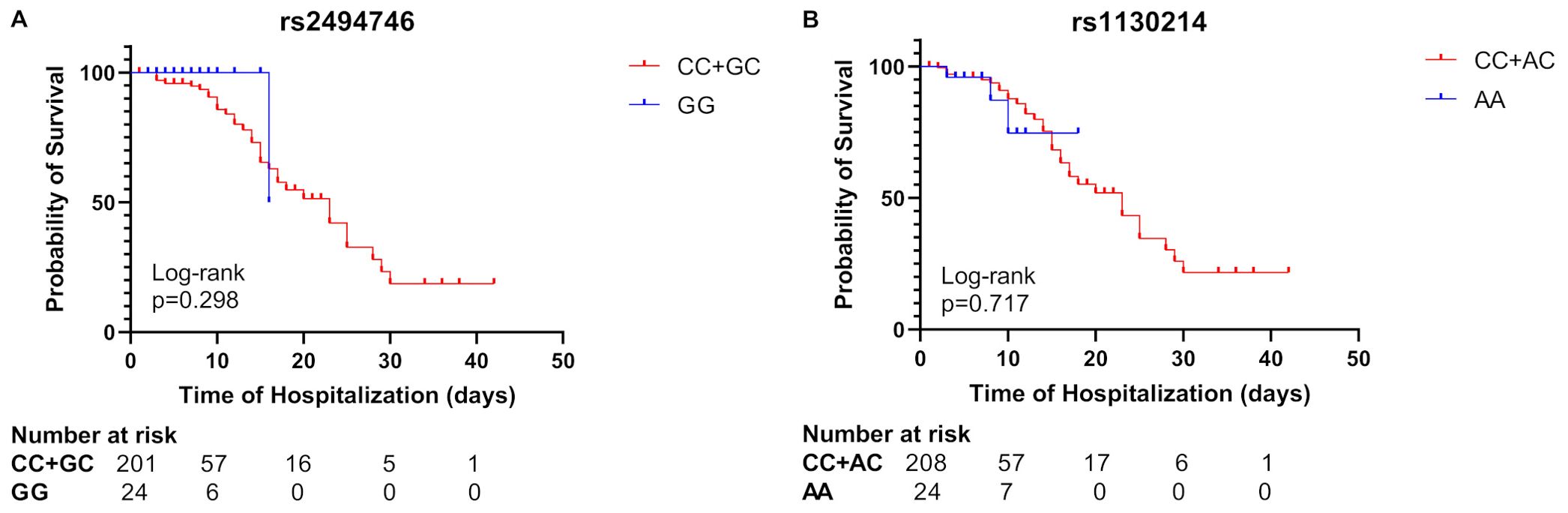
Figure 3. Kaplan–Meier survival curves of severe COVID-19 patients for genotype of rs2494746 and rs1130214 AKT1 variants. The recessive models showed no statistically significant difference between individuals with at least one C allele compared to homozygote individuals in the rs2494746 variant (A) or the rs1130214 (B).
Regarding the relationship between rs2494746-C allele and mortality, we observed 12.86-fold increased COVID-19 mortality compared with subjects without C allele at rs2494746 in the dominant model (p=0.013, Supplementary Table S3). No significant association with mortality was found for rs1130214 (Supplementary Table S3).
In the predictive analysis for rs2494746, with 494 individuals, we obtained a sensitivity of 91% and specificity of 45%, a positive predictive value of 69% and a negative predictive value of 80% (Kappa concordance index= 0.384, accuracy=71% and p<0.001). The rs1130214, with 502 individuals, had a sensitivity of 90% and specificity of 10%, a positive predictive value of 58% and a negative predictive value of 43% (Kappa concordance index= 0.002). In addition, it presents an accuracy of 56% and p>0.05, demonstrating that it is not statistically significant or accurate (Table 5).
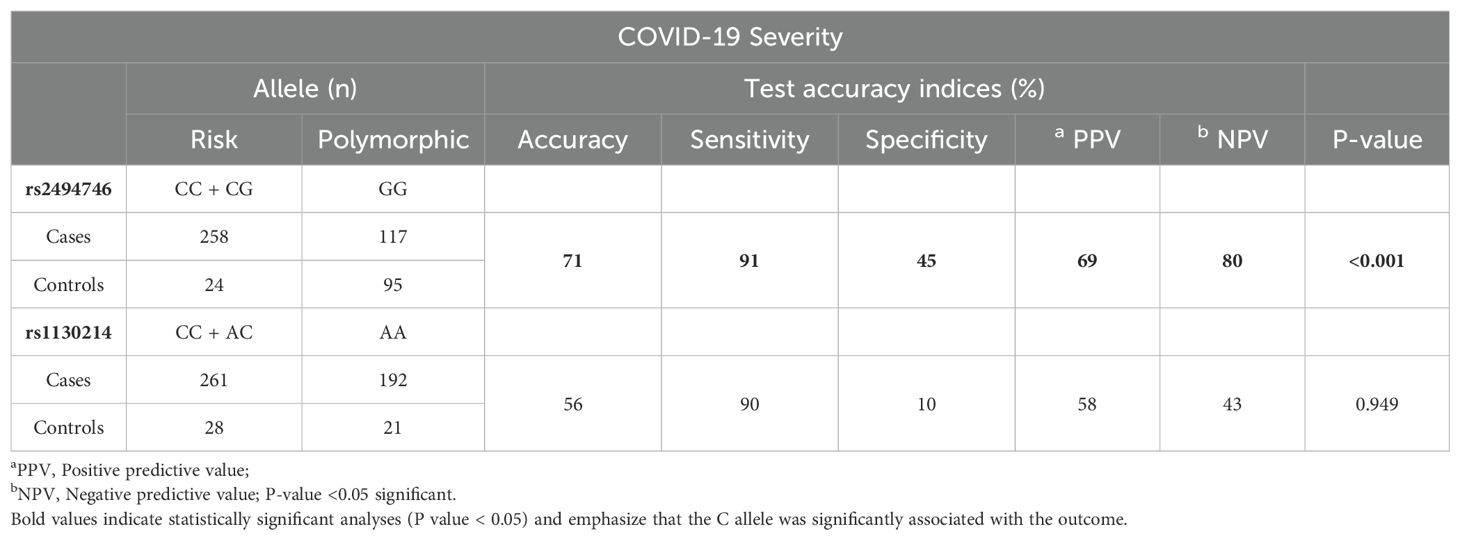
Table 5. Prediction analysis for severity with rs2494746 and rs1130214 AKT1 variants.
The study analyzed the association between the rs1130214 and rs2494746 variants of the AKT1 gene with the severity of COVID-19. We found that individuals who presented the C allele of rs2494746 are eight times more likely to develop severe COVID-19 and require ICU support.
This is the first study that correlates variants on the AKT1 gene with COVID-19. A previous study associated rs2494746 with an increased risk of developing type 2 diabetes mellitus (11). COVID-19 has also been associated with an increased risk of developing new-onset diabetes after infection (16, 17), suggesting that COVID-19 and diabetes share a mechanism of genetic predisposition.
In silico functional analysis from Regulome Db 2.2 uses two distinct metrics, ranking and scoring, to assess the relevance and reliability of genetic variants in genomic studies. The rs2494746 variant received a rank of 1f, indicating strong evidence of a functional effect, possibly related to gene regulation or other biological functions. The score assigned to the variant (0.22271) reflects the confidence in the classification, based on several functional characteristics (Supplementary Table S1). In summary, the results suggest that the rs2494746 variant plays a significant biological role, with strong evidence for a functional effect, possibly involved in gene regulation or other relevant biological processes. Furthermore, in the lungs, this variant is associated with strong transcriptional activity and acts as an enhancer of gene expression in genetic regulatory elements, potentially influencing lung function and playing a crucial role in the immune response to respiratory infections.
SARS-Cov-2 binds to the ACE2 receptor and activates many signaling pathways promoting the production of inflammatory cytokines, including TNF, IL-17, IL-6, IL-8, and IL-1β. These cytokines are secreted by numerous cells, such as epithelial cells, macrophages, T lymphocytes, neutrophils, and Th17 cells, and exacerbate SARS-CoV-2 infection. Excessive release of cytokines has consequences such as acute respiratory distress syndrome (ARDS) (2).
The PI3K/AKT pathway plays a crucial role in regulating various cellular functions such as proliferation, survival, cell cycle, apoptosis, glycogen metabolism, and inflammation. It can modulate the synthesis of pro-inflammatory cytokines (IL-1β, IL-6, and IL-8) induced by TNF (18), trigger TGF-β1 activation and protein phosphorylation, leading to excessive proliferation and differentiation of fibroblasts in the lungs (19). Therefore, genetic variants on AKT can play a key role in the production of cytokines (20) and may be related to an exacerbated immune response to COVID-19.
According to the HaploReg v4.2 platform, the rs1130214 variant, located in the 5’-UTR region of the AKT1 gene, is associated with regulatory elements such as protein binding sites and altered transcription motifs in various cells and tissues, including T cells, B cells and peripheral blood mononuclear cells. The presence of these regulatory elements suggests that the variant can influence gene activity in cells involved in regulating the inflammatory response and the production of cytokines, such as TNF. Furthermore, the presence of binding sites for known transcription factors, such as CTCF and RAD21, indicates that the variant may be involved in chromatin organization and transcription regulation (21, 22). This information highlights the importance of the rs1130214 variant in regulating gene expression and modulating biological processes associated with the AKT1 gene.
We also observed an association between the CC genotype of the rs1130214 variant and higher D-dimer levels compared to AA/AC. As a coagulation marker, increased D-dimer reflects hypercoagulability and thrombotic burden. Higher D-dimer levels have been reported to provide useful prognostic information regarding COVID-19 progression and mortality (23). It is known that AKT phosphorylation is involved in thrombus formation through the PI3K/AKT signaling pathway that activates platelets, and the use of PI3K or AKT inhibitors potently abolishes the increased binding of platelet fibrinogen induced by incubation with patient sera with COVID-19 admitted to the ICU (24). This suggests a possible contribution of this variant to thrombotic events in COVID-19.
Here, individuals with the risk allele (C) of the rs1130214 were associated with increased TNF production compared to the AA genotype. Furthermore, the CC genotype of rs1130214 was associated with higher levels of D-dimer. These results suggest a contribution of this variant in the cytokine storm and blood clotting. The rs1130214 has been associated with persistently high CD4+ T cell glycolytic activity in HIV-positive individuals (10), increased risk of having congenital heart disease (12), glucose homeostasis and metabolic syndrome (9), among other conditions.
Genotype risk score analysis revealed a cumulative effect of the risk alleles of the rs1130214 and rs2494746 variants with a greater chance of severity, criticality, and mortality of COVID-19. This finding supports the hypothesis that the co-inheritance of these variants may heighten an individual’s susceptibility to severe COVID-19. However, the specific molecular mechanisms underlying this phenomenon remain unclear.
The predictive power evaluation of rs2494746 revealed an accuracy of 71%, suggesting that such variant may be a valuable marker to assist in the early detection of individuals who will develop severe COVID-19 following SARS-CoV-2 infection. Other studies demonstrated that serum levels of IL-6 and TNF remained independent and significant predictors of disease severity and death (25), identified a panel of laboratory indicators of severe disease, such as creatinine levels, neutrophil count, C-reactive protein (CRP) and D-dimer (26). In addition to biomarkers to assess the risk of thrombosis in these patients, including markers of platelet activation, platelet aggregation, activation or injury of endothelial cells, coagulation, and fibrinolysis (27). Although a panel of laboratory indicators of severe disease has been identified, these values represent relatively nonspecific markers of an increased inflammatory state and organ dysfunction. Consequently, this variant has the potential to be integrated into the existing set of clinical markers, enhancing the precision of disease prognosis.
Nonetheless, it is essential to acknowledge certain limitations inherent to this study. First, the GG genotype of the rs2494746 variant was detected in a relatively small proportion of ICU patients who ultimately died, and this observation may have had an impact on our findings. Second, this study was unpowered to demonstrate whether the variants alter gene expression, and the predictive values may not be confirmed in the current population. Despite these restrictions, this sample is made up of unvaccinated people. This has a positive point, which is the original response to the virus, thus improving the understanding of pathogenic mechanisms. This study is pioneering in highlighting the impact of genetic variants of the AKT1 gene on the more unfavorable prognosis of COVID-19.
In conclusion, the rs2494746 variant was associated with risk of severity and critical outcome, as well as death from COVID-19. Meanwhile, rs1130214 was related to increased levels of TNF and D-dimer. These variants presented cumulative risk when inherited together. Furthermore, the predictive analysis demonstrated a moderate probability of the individual with the risk allele of the rs2494746 variant developing the severity of the disease. Therefore, the present study contributes to understanding the influence of the AKT1 gene and its variants on the immunological damage in individuals infected with SARS-CoV-2. This could be useful in the future to assist in predicting a worse outcome of COVID-19.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://www.ncbi.nlm.nih.gov/snp/, rs2494746; https://www.ncbi.nlm.nih.gov/snp/, rs1130214.
The studies involving humans were approved by Human Research Ethics Committee of the Lauro Wanderley University Hospital (Paraíba, Brazil) under n°. 31562720.9.0000.5183, by the Research Ethics Committee of the State University of Feira de Santana (Bahia, Brazil) under n°. 30764720.1.0000.0053, and the Research Ethics Committee of HUPES (Bahia, Brazil) under no. 31748320.3.1001.5543. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
IA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. BT: Data curation, Formal analysis, Methodology, Visualization, Writing – review & editing. LP: Formal analysis, Methodology, Writing – review & editing. HS: Formal analysis, Methodology, Writing – review & editing. FG: Methodology, Writing – review & editing. NS: Methodology, Writing – review & editing. JC: Methodology, Writing – review & editing. MS: Methodology, Writing – review & editing. JA: Methodology, Writing – review & editing. JR: Methodology, Writing – review & editing. GO: Methodology, Writing – review & editing. RF: Methodology, Writing – review & editing. SV: Methodology, Writing – review & editing. IM-C: Methodology, Writing – review & editing. DS: Methodology, Writing – review & editing. AT: Methodology, Writing – review & editing. FB: Methodology, Writing – review & editing. VC: Methodology, Writing – review & editing. GC: Methodology, Writing – review & editing. CB: Methodology, Writing – review & editing. VF: Methodology, Writing – review & editing. CF: Methodology, Writing – review & editing. ST: Methodology, Writing – review & editing. HR: Methodology, Writing – review & editing. RC: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior -Brasil (CAPES) -Finance Code 001 to IA; and the Foundation for Research Support of the State of Bahia (FAPESB) -Programa Pesquisa para o SUS: gestão compartilhada em saúde -PPSUS/FAPESB 02/2020 to RC.
The authors would like to acknowledge all the lab members and contributors for their support during the preparation of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1422349/full#supplementary-material
1. Hu B, Guo H, Zhou P, Shi Z-L. Characteristics of SARS-coV-2 and COVID-19. Nat Rev Microbiol. (2021) 19:141–54. doi: 10.1038/s41579-020-00459-7
2. Darif D, Hammi I, Kihel A, El Idrissi Saik I, Guessous F, Akarid K. The pro-inflammatory cytokines in COVID-19 pathogenesis: What goes wrong? Microb Pathog. (2021) 153:104799. doi: 10.1016/j.micpath.2021.104799
3. Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature. (2020) 584:430–6. doi: 10.1038/s41586-020-2521-4
4. Ersahin T, Tuncbag N, Cetin-Atalay R. The PI3K/AKT/mTOR interactive pathway. Mol Biosyst. (2015) 11:1946–54. doi: 10.1039/C5MB00101C
5. Appelberg S, Gupta S, Svensson Akusjärvi S, Ambikan AT, Mikaeloff F, Saccon E, et al. Dysregulation in Akt/mTOR/HIF-1 signaling identified by proteo-transcriptomics of SARS-CoV-2 infected cells. Emerg Microbes Infect. (2020) 9:1748–60. doi: 10.1080/22221751.2020.1799723
6. Pompura SL, Dominguez-Villar M. The PI3K/AKT signaling pathway in regulatory T-cell development, stability, and function. J Leukoc Biol. (2018) 103:1065–76. doi: 10.1002/JLB.2MIR0817-349R
7. Lin S, Wu H, Wang C, Xiao Z, Xu F. Regulatory T cells and acute lung injury: cytokines, uncontrolled inflammation, and therapeutic implications. Front Immunol. (2018) 9:1545. doi: 10.3389/fimmu.2018.01545
8. Schmiedel BJ, Rocha J, Gonzalez-Colin C, Bhattacharyya S, Madrigal A, Ottensmeier CH, et al. COVID-19 genetic risk variants are associated with expression of multiple genes in diverse immune cell types. Nat Commun. (2021) 12:6760. doi: 10.1038/s41467-021-26888-3
9. Harmon BT, Devaney SA, Gordish-Dressman H, Reeves EK, Zhao P, Devaney JM, et al. Functional characterization of a haplotype in the AKT1 gene associated with glucose homeostasis and metabolic syndrome. Hum Genet. (2010) 128:635–45. doi: 10.1007/S00439-010-0891-7
10. Masson JJR, Cherry CL, Murphy NM, Sada-Ovalle I, Hussain T, Palchaudhuri R, et al. Polymorphism rs1385129 within glut1 gene SLC2A1 is linked to poor CD4+ T cell recovery in antiretroviral-treated HIV+ Individuals. Front Immunol. (2018) 9:900. doi: 10.3389/FIMMU.2018.00900
11. Yin X, Xu Z, Zhang Z, Li L, Pan Q, Zheng F, et al. Association of PI3K/AKT/mTOR pathway genetic variants with type 2 diabetes mellitus in Chinese. Diabetes Res Clin Pract. (2017) 128:127–35. doi: 10.1016/J.DIABRES.2017.04.002
12. Zhao J, Zeng Z. Combined effects of AKT serine/threonine kinase 1 polymorphisms and environment on congenital heart disease risk: A case-control study. Medicine. (2020) 99:e20400–0. doi: 10.1097/MD.0000000000020400
13. Tosta BR, de Almeida IM, da Cruz Pena L, dos Santos Silva H, Reis-Goes FS, Silva NN, et al. MTOR gene variants are associated with severe COVID-19 outcomes: A multicenter study. Int Immunopharmacol. (2023) 125:111155. doi: 10.1016/J.INTIMP.2023.111155
14. Penha D, Pinto EG, Matos F, Hochhegger B, Monaghan C, Taborda-Barata L, et al. CO-RADS: coronavirus classification review. J Clin Imaging Sci. (2021) 11:9. doi: 10.25259/JCIS_192_2020
15. Pan F, Ye T, Sun P, Gui S, Liang B, Li L, et al. Time course of lung changes on chest CT during recovery from 2019 novel coronavirus (COVID-19) pneumonia. Radiology. (2020) 295:715–21. doi: 10.1148/RADIOL.2020200370
16. Groß R, Kleger A. COVID-19 and diabetes — where are we now? Nat Metab. (2022) 4:1611–3. doi: 10.1038/s42255-022-00691-w
17. Ssentongo P, Zhang Y, Witmer L, Chinchilli VM, Ba DM. Association of COVID-19 with diabetes: a systematic review and meta-analysis. Sci Rep. (2022) 12:1–8. doi: 10.1038/s41598-022-24185-7
18. Xu H, He Y, Yang X, Liang L, Zhan Z, Ye Y, et al. Anti-malarial agent artesunate inhibits TNF-α-induced production of proinflammatory cytokines via inhibition of NF-κB and PI3 kinase/Akt signal pathway in human rheumatoid arthritis fibroblast-like synoviocytes. Rheumatology. (2007) 46:920–6. doi: 10.1093/RHEUMATOLOGY/KEM014
19. Vaz de Paula CB, Nagashima S, Liberalesso V, Collete M, da Silva FPG, Oricil AGG, et al. COVID-19: immunohistochemical analysis of TGF-β Signaling pathways in pulmonary fibrosis. Int J Mol Sci. (2021) 23:168. doi: 10.3390/IJMS23010168/S1
20. Jin JO, Yu Q. Fucoidan delays apoptosis and induces pro-inflammatory cytokine production in human neutrophils. Int J Biol Macromol. (2015) 73:65–71. doi: 10.1016/J.IJBIOMAC.2014.10.059
21. Kim S, Yu NK, Kaang BK. CTCF as a multifunctional protein in genome regulation and gene expression. Exp Mol Med. (2015) 47:e166–6. doi: 10.1038/emm.2015.33
22. Sun Y, Xu X, Zhao W, Zhang Y, Chen K, Li Y, et al. RAD21 is the core subunit of the cohesin complex involved in directing genome organization. Genome Biol. (2023) 24:255. doi: 10.1186/S13059-023-02982-1
23. Varikasuvu SR, Varshney S, Dutt N, Munikumar M, Asfahan S, Kulkarni PP, et al. D-dimer, disease severity, and deaths (3D-study) in patients with COVID-19: a systematic review and meta-analysis of 100 studies. Sci Rep. (2021) 11:1–11. doi: 10.1038/s41598-021-01462-5
24. Pelzl L, Singh A, Funk J, Witzemann A, Marini I, Zlamal J, et al. Antibody-mediated procoagulant platelet formation in COVID-19 is AKT dependent. J Thromb Haemostasis. (2022) 20:387. doi: 10.1111/JTH.15587
25. Del Valle DM, Kim-Schulze S, Huang HH, Beckmann ND, Nirenberg S, Wang B, et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat Med 2020 26:10. (2020) 26:1636–43. doi: 10.1038/s41591-020-1051-9
26. Hufnagel K, Fathi A, Stroh N, Klein M, Skwirblies F, Girgis R, et al. Discovery and systematic assessment of early biomarkers that predict progression to severe COVID-19 disease. Commun Med. (2023) 3:1–13. doi: 10.1038/s43856-023-00283-z
Keywords: AKT1, COVID-19, severity, polymorphism, immunogenetics
Citation: de Almeida IM, Tosta BR, Pena LdC, Silva HdS, Reis-Goes FS, Silva NN, Cruz JVA, Silva MdA, de Araújo JF, Rodrigues JL, Oliveira G, Figueiredo RG, Vaz SN, Montaño-Castellón I, Santana D, Torres A, Beltrão FEdL, Carneiro VL, Campos GS, Brites C, Fortuna V, Figueiredo CA, Trindade SC, Ramos HE and Costa RdS (2024) Genetic signatures of AKT1 variants associated with worse COVID-19 outcomes – a multicentric observational study. Front. Immunol. 15:1422349. doi: 10.3389/fimmu.2024.1422349
Received: 23 April 2024; Accepted: 18 September 2024;
Published: 08 October 2024.
Edited by:
Gabriela Angélica Martínez-Nava, National Institute of Rehabilitation Luis Guillermo Ibarra Ibarra, MexicoReviewed by:
Stelvio Tonello, University of Eastern Piedmont, ItalyCopyright © 2024 de Almeida, Tosta, Pena, Silva, Reis-Goes, Silva, Cruz, Silva, de Araújo, Rodrigues, Oliveira, Figueiredo, Vaz, Montaño-Castellón, Santana, Torres, Beltrão, Carneiro, Campos, Brites, Fortuna, Figueiredo, Trindade, Ramos and Costa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ryan dos Santos Costa, cnlhbnNjb3N0YUB5YWhvby5jb20uYnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.