 José Carlos Jaime-Pérez*
José Carlos Jaime-Pérez* Jorge Valdespino-Valdes‡
Jorge Valdespino-Valdes‡ Andrés Gómez-De LeónRenata Valeria Barragán-Longoria‡
Andrés Gómez-De LeónRenata Valeria Barragán-Longoria‡ Adriana Dominguez-VillanuevaOlga Graciela Cantú-Rodríguez‡
Adriana Dominguez-VillanuevaOlga Graciela Cantú-Rodríguez‡ César Homero Gutiérrez-Aguirre
César Homero Gutiérrez-Aguirre David Gómez-Almaguer
David Gómez-Almaguer- Hematology Department, Internal Medicine Division, Dr. José E. González University Hospital, School of Medicine, Universidad Autónoma de Nuevo León, Monterrey, Mexico
Background: Hematopoietic cell transplantation (HCT) increases survival for acute leukemia. Outpatient allogeneic HCT reduces costs and increases transplant rates in developing countries. We report outcomes of outpatient HLA-identical and haploidentical HCT in acute leukemia.
Methods: This single-center retrospective cohort study analyzed 121 adult patients with acute myeloblastic (AML) and acute lymphoblastic leukemia (ALL) receiving an outpatient allogeneic HCT with peripheral blood allografts after reduced-intensity conditioning (RIC) from 2012-2022.
Results: There were 81 (67%) haploidentical and 40 (33%) HLA-identical transplants. Complete chimerism (CC) at day +100 was not different in HLA-identical compared to haploidentical HCT (32.5% and 38.2%, P=0.054). Post-HCT complications, including neutropenic fever (59.3% vs. 40%), acute graft-versus-host-disease (aGVHD) (46.9% vs. 25%), cytokine release syndrome (CRS) (18.5% vs. 2.5%), and hospitalization (71.6% vs 42.5%) were significantly more frequent in haploidentical HCT. Two-year overall survival (OS) was 60.6% vs. 46.9%, (P=0.464) for HLA-identical and haplo-HCT, respectively. There was no difference in the 2-year disease-free-survival (DFS) (33.3% vs. 35%, P=0.924) between transplant types. In multivariate analysis, positive measurable residual disease (MRD) at 30 days (HR 8.8, P=0.018) and 100 days (HR 28.5, P=0.022) was associated with lower OS, but not with non-relapse mortality (NRM) (P=0.252 and P=0.123, univariate). In univariate analysis, both 30-day and 100-day MRD were associated with lower DFS rates (P=0.026 and P=0.006), but only day 30 MRD was significant in multivariate analysis (P=0.050). In the case of relapse, only MRD at day 100 was associated with increased risk in the univariate and multivariate analyses (HR 4.48, P=0.003 and HR 4.67, P=0.008). Chronic graft-versus-host-disease (cGVHD) was protective for NRM (HR 0.38, P=0.015). There was no difference in cumulative incidence of relapse (CIR) between transplant types (P=0.126). Forty-four (36.4%) patients died, with no difference between HCT type (P=0.307). Septic shock was the most frequent cause of death with 17 cases, with no difference between transplant types
Conclusions: Outpatient peripheral blood allogenic HCT after RIC is a valid and effective alternative for adult patients suffering acute myeloblastic or lymphoblastic leukemia in low-income populations.
1 Introduction
Allogeneic hematopoietic cell transplantation (allo-HCT) is a potentially curative option for patients with acute leukemia with previous failed treatments (1). Improved criteria for selection and better transplant strategies have balanced outcomes between HLA-identical and haploidentical allografting (2). With haploidentical transplantation, virtually all patients have a potential donor (3). Reduced-intensity conditioning (RIC) and improved GVHD prophylaxis are associated with fewer toxic-related complications, allowing for an outpatient setting (4). This scenario considerably reduces costs and is highly relevant for low-middle income countries (LMIC) lacking optimally funded health systems, a well-established donor network, and fully equipped and staffed transplant units (5).
An outpatient setting broadens HCT, providing access to many uninsured patients who would otherwise die from disease progression; its efficacy in a LMIC has been described (6). In this situation, acute myeloid leukemia (AML) and acute lymphoblastic leukemia (ALL) have been reported to be more prevalent in Latin American populations compared to developed countries (7, 8). Few studies report outcomes after an outpatient allo-HCT strategy employing a RIC scheme in LMIC as treatment for acute leukemia (6). This information is needed to allow physicians to identify the benefits, risks, and limitations of employing this transplant modality.
This study assessed the efficacy and safety of outpatient allo-HCT with a RIC regimen performed in a LMIC in patients with ALL or AML. We report patients’ clinical characteristics, most frequent post-HCT complications, clinical evolution, survival and relapse rates, and risk factors associated with mortality and relapse between donor types.
2 Materials and methods
2.1 Study design and patients
This single-center retrospective cohort study included patients ≥ 18 years diagnosed with AML or ALL who underwent an outpatient allo-HCT after RIC at the Hematology Department of the Dr. José E. González University Hospital of the School of Medicine of the Autonomous University of Nuevo León, in Monterrey, Mexico, from 2012 to 2022. Patients who had complete information on the clinical file and electronic database, and who received the conditioning regimen, central venous catheter insertion, and hematoprogenitors graft infusion in the ambulatory setting were included. Eligibility involved a Karnofsky score ≥70%, creatinine <2 mg/dL, ECOG ≤2, HCT-specific comorbidity index ≤2, and round-the-clock availability of a caregiver for the first month after HCT. The stem cell source was non-T-cell depleted peripheral blood; the selection of HLA-identical or haplo-HCT depended on the availability of the corresponding sibling donor. Our center cares for an open population, mainly low-income uninsured patients from the country’s northeast region. This study received approval by the institutional ethics and research committees (HE21-00033), and the principles of the Helsinki Declaration were observed. All patients provided written informed consent before transplantation.
2.2 Donors mobilization, collection, and stem cell source
Granulocyte colony-stimulating factor at 10 μg/kg/day was administered subcutaneously to donors for 4 days. Peripheral blood hematopoietic stem cells were collected through peripheral veins, or a central venous catheter placed in the outpatient clinic on the 5th day. Single large volume leukapheresis processing was 3 to 5 times the estimated donor’s total blood volume to obtain at least 4x106/kg viable CD34+ cells. The peripheral blood T-cell repleted graft was refrigerated and infused unmanipulated the same day of its collection.
2.3 Outpatient allo-HCT procedure and criteria for hospital admission
A detailed description of the outpatient HCT methods and transplant unit functioning has been previously described (9). All transplants were performed in an outpatient setting, including conditioning regimen administration, central catheter placement, stem cell infusion, and posttransplant cyclophosphamide (PTCY) administration. Patients who experienced regimen-related toxicity, grade III-IV hemorrhagic cystitis, severe mucositis, oral intolerance, diarrhea, severe neutropenic fever, hemodynamic instability or cardiovascular complications, severe cytokine release syndrome (CRS), or severe infection were hospitalized.
2.4 Outpatient supportive care
After graft infusion in the outpatient hematology clinic, patients went home under the supervision of their caregivers who had been instructed regarding specific needs; the nursing staff provided instructions on hygiene measures for the patient and caregiver. The treating physician explained the required medications, their presentation, dose, and schedule, and detection and course of action in case of untoward reactions, untoward effects, changes in psychological well-being, and signs of emergency events requiring immediate attention. Round-the-clock contact numbers were provided to seek urgent attention at any time and day. Staying at home following strict hygiene measures and diet indications was required during the first four post-transplant weeks. Patients had daily outpatient follow-up visits at the hematology day clinic from day +1 to +4, then every 48 hours until hematological recovery was observed. Subsequent visits were scheduled weekly until day +90, and then every month, or as frequently as required by the posttransplant clinical evolution. (10) Long-term follow-up for outstate recipients consisted of appointments at the hematology clinic every 2-3 months for two years, with monthly interim visits to the patient´s local physician.
2.5 Conditioning regimens and graft-versus-host disease prophylaxis
HLA-identical recipients received intravenous cyclophosphamide (CY) 350 mg/m2 and fludarabine (Flu) 25 mg/m2 from day -7 to -5, followed by oral busulphan (Bu) 4 mg/kg on days -4 to -2, or melphalan 140-200 mg/m2 i.v. on day -1. For graft-versus-host disease (GVHD) prophylaxis, oral cyclosporine (CsA) 5 mg/kg was employed on day -1, and intravenous methotrexate (5mg/m2) on days +1, +3, and +5. Oral CsA was continued through day +120-180 and then individualized, adjusting for a target level of 150-250 ng/mL and tapered over 30-60 days. If GvHD was suspected, oral CsA was tapered for a longer period.
Conditioning for haploidentical recipients included CY (350 mg/m2) and Flu (25 mg/m2), which were administered from days -4 to -2, and melphalan (MEL) (140-200 mg/m2) on day -1 with or without 2 Gy of total body irradiation. GvHD prophylaxis consisted of PT-CY (50 mg/kg/day) administered on days +3 and +4, mycophenolic acid (2 g/day) from day +5 to day +30, and oral CsA with the same dosing scheme described for the HLA-identical group. The stem cell source was unmanipulated peripheral blood and was infused on day 0.
Acute GVHD (aGVHD) was graded according to the Glucksberg criteria, and chronic (cGVHD) according to the National Institutes of Health criteria (11, 12).
2.6 Chimerism and measurable residual disease
Chimerism was determined by PCR analyses of short tandem repeats or variable number tandem repeats. In the case of sex mismatch between donor and recipient, chimerism was assessed by fluorescence in situ hybridization. The analysis was performed on days 30, 100, and 365 post-HCT. Complete chimerism required a ≥95% identical result between donor and patient in variable number tandem repeats, short tandem repeats, or fluorescence in situ hybridization analysis.
2.7 Antimicrobial prophylaxis
Anti-infectious prophylaxis initiated on day 0 with an oral quinolone (Levofloxacin 500 mg/day), oral itraconazole (100 mg/day PO BID), or voriconazole 200 mg twice a day, and daily low-dose oral acyclovir (800 mg/day) until engraftment. Subsequently, trimethoprim-sulfamethoxazole 160/800 mg/day 3 days per week and daily low-dose oral acyclovir (800 mg/day) were administered until immunosuppressive therapy was halted. Meropenem i.v., 1 gram every 8 hours, was administered empirically for neutropenic fever, unless resistant bacteria were documented; in that case targeted antibiotic combinations were employed. Cytomegalovirus (CMV) viral load was determined at days 14 and 30 post-transplant for all patients and further evaluated on a clinical basis according to their risk factors, such as GVHD development, corticosteroid use, prior reactivation, or when suspected by the treating physician. CMV infection treatment consisted of valganciclovir (450 mg BID) at a ≥500 IU/mL threshold. A different donor was chosen in the case of second transplants; the conditioning regimen was the same as in the first procedure.
2.8 Definitions
The transplant was considered ambulatory if the conditioning regimen and stem cell infusion were performed completely in the outpatient clinic, regardless of whether the patient required post-transplant hospitalization. Overall survival (OS) was defined as the time from the allo-HCT to death or last follow-up. Disease-free survival (DFS) was defined as the time from the allo-HCT to GF, disease progression, relapse, death, or last follow-up, whichever occurred first. Non-relapse mortality (NRM) was defined as death from any cause without relapse. Transplant-related mortality (TRM) was defined as death due to any transplant-related cause other than disease relapse or progression. Transplant-related hospitalization was any transplant-related event requiring inpatient care within day +1 to day +100 in the post-HSCT period. Neutrophil engraftment was defined as an absolute neutrophil count (ANC) of >0.5 x 109/L for at least three consecutive days unsupported by granulocyte colony-stimulating factor. Platelet engraftment was when platelets reached >20 x 109/L for at least 7 consecutive days without transfusion support. Primary graft failure (GF) was defined as neutrophil engraftment failure by day +28 and secondary GF was defined as a drop in ANC <0.5 x 109/L after initial engraftment with loss of donor chimerism. Complete chimerism was assumed if ≥95% of hematopoietic cells were from donor origin; mixed chimerism was defined as 5 to 95% donor cells and the absence of chimerism as <5% donor cells (13). In the case of second transplants, only the last procedure was included, and it was assessed the same way as the first transplants.
2.9 Statistical analysis
SPSS version 25 (IBM Corp., Armonk, NY) was used for all data analysis, except cumulative incidence analyses that were estimated using R (Murray Hill, NJ, USA). A descriptive analysis used medians (range) for continuous variables and proportions for categorical variables. Univariate comparison of basal characteristics and HCT complications was conducted between donor types using the chi-square test for categorical variables or the Mann-Whitney test for continuous variables. Overall survival and DFS were estimated with Kaplan-Meier curves and compared between groups with the log-rank test. Cox proportional hazard regression analysis was performed to identify OS, DFS, NRM and relapse risk factors in univariate and multivariate analysis. For the multivariate analysis, stepwise analysis was used with a variable entry criterion of p <.1. Cox analyses were reported as the hazard ratio (HR), 95% confidence interval (CI) for the HR, and the corresponding p-value. The cumulative incidence of relapse was estimated from the time of allo-HCT to relapse/progression. The cumulative incidence of NRM was estimated from the time of allo-HCT to death or last follow-up without relapse/disease progression. As a secondary analysis, patients were analyzed stratified according to type of acute leukemia, lymphoblastic vs. myeloblastic. A p-value ≤.05 was considered statistically significant.
3 Results
3.1 Patient, donor, and allo-HCT characteristics
One hundred twenty-one outpatient allo-HCTs were performed during our study period; 81 (66.9%) were haploidentical, and 40 (33.1%) were HLA-identical. Diagnoses were ALL in 64 (52.9%) and AML in 57 (47.1%) patients. Nine (7.4%) patients underwent their second allo-HCT. Median CD34+ infused cells were 10x106/kg for haploidentical and 8x106/kg for HLA-identical recipients (P=0.006). Myeloid engraftment was achieved in a median of 14 days for both groups; platelet engraftment median time was 16 days for haploidentical and 14 days for HLA-identical recipients (P=0.013). 69.1% vs. 72.5% patients had reactive IgG anti-CMV in the haploidentical and HLA-identical HCT group, respectively (P=0.047). The median follow-up for the cohort was 31 months (10–98). Other demographic and clinical characteristics, including CMV status in recipient/donor pairs, are summarized in Table 1.
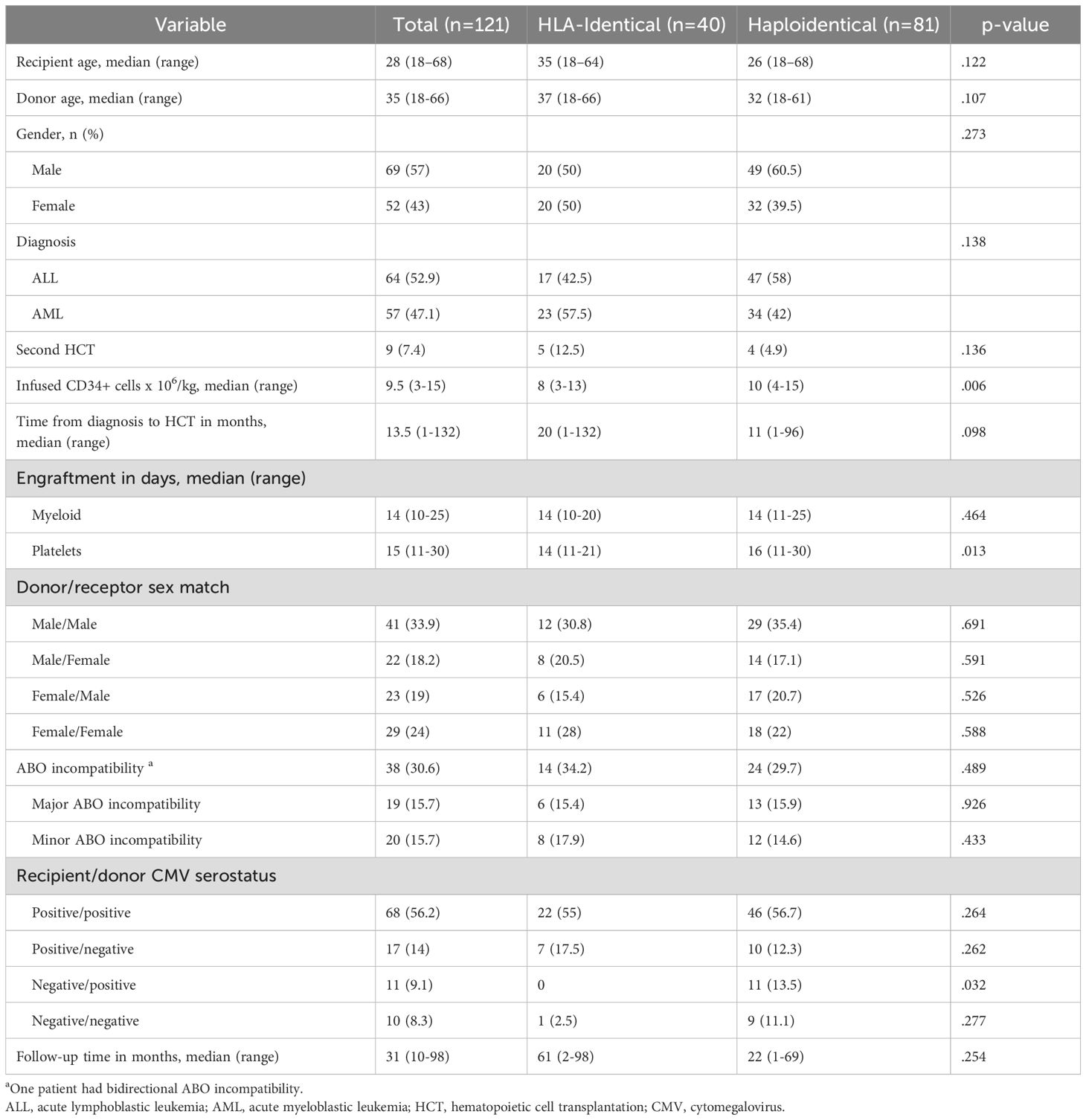
Table 1. Baseline characteristics of 121 adults with acute leukemia who underwent an outpatient allogeneic hematopoietic cell transplantation with a reduced intensity conditioning.
The salient characteristics of patients in the cohort according to type of acute leukemia are shown in Table 2. Patients were younger in the ALL group, median age of 19 vs. 38 years in the AML group (P=0.001), median time from diagnosis to transplant was considerably longer in ALL patients, 15 vs. 8 months in AML patients (P=0.001); also, median CD34+ cell dose infused was higher for ALL recipients, 10x106/kg of body weight vs. 8.8x106/kg in AML cases (P=0.024). Regarding clinical features, only cytokine release syndrome (CRS) incidence was higher in ALL patients, 20.3% vs. 5.3% (P=0.015) in AML patients. Mortality rate according to leukemia type was, for the ALL group, 34.4% vs. 38.6% for AML patients, (P=0.630), while 50% vs. 57.9% (P=0.385), suffered relapse, progression, or graft failure, respectively.
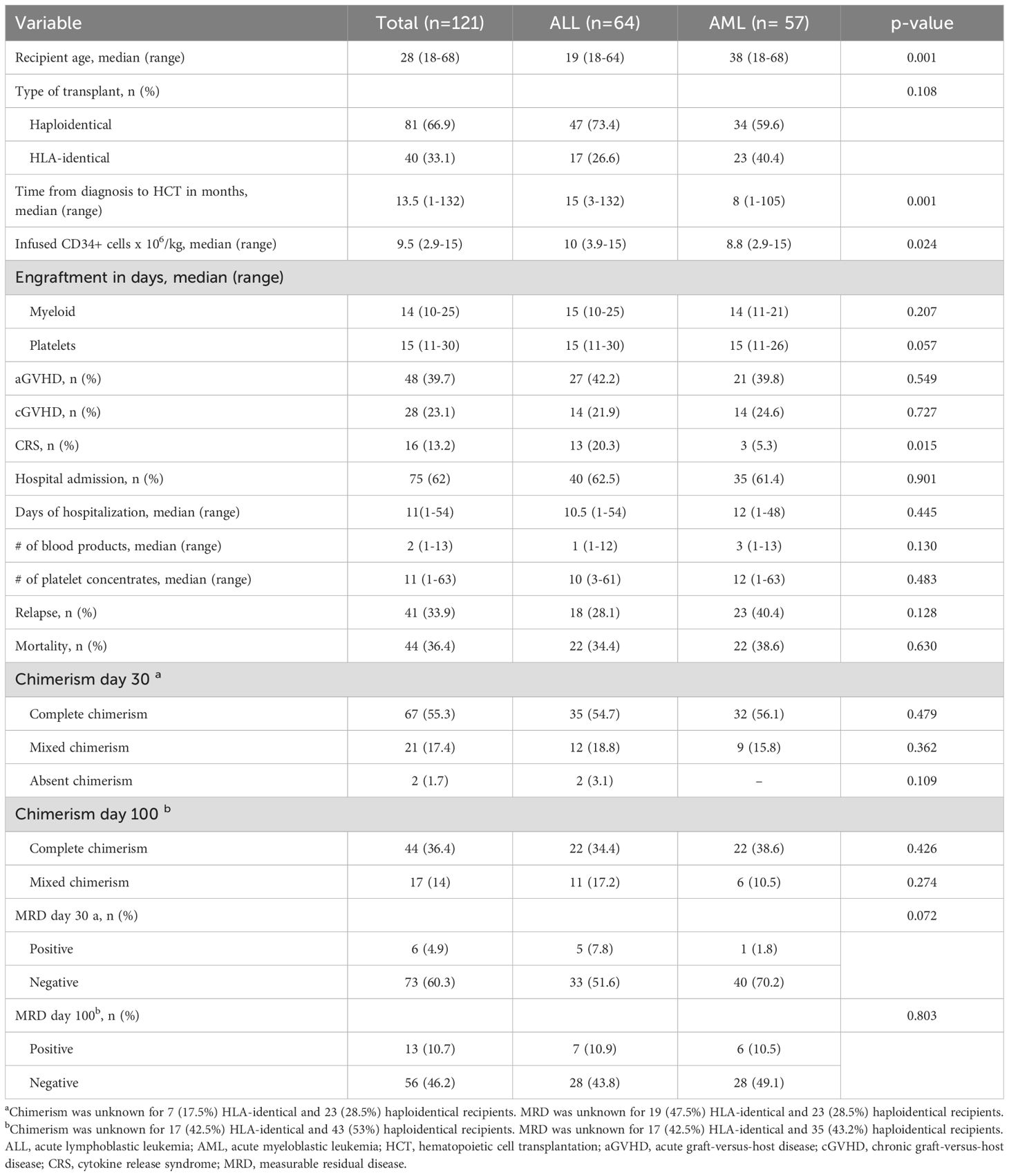
Table 2. Comparison of salient characteristics and main outcomes between 64 patients with ALL and 57 with AML who underwent an outpatient hematopoietic cell transplantation with a reduced intensity conditioning.
3.2 Allo-HCT outcomes and complications
Forty-eight (59.3%) and 16 (40%) patients had neutropenic fever in haploidentical and HLA-identical HCT, respectively (P=0.027). Infections occurred in 53 (43.8%) patients, bacteria being the most frequent cause in 30 (56.6%), E. coli being the most frequent agent in 27% of the cases. aGVHD incidence was lower in HLA-identical (25%) than haplo-HCT (46.9%), P=0.016. On the other hand, cGVHD was not different between haploidentical and HLA-identical HCT, 25.9% and 17.5%, respectively (P=0.251). Cytokine release syndrome was present in 18.5% of haploidentical and 2.5% of HLA-identical recipients (P=0.020). Cytokine release syndrome grade was similar between groups (P=0.108).
All transplants were outpatient, yet 58 (71.6%) haploidentical recipients were hospitalized compared to 17 (42.5%) HLA-identical recipients (P=0.002). The most common cause of hospitalization was neutropenic fever (58.6%), with no difference observed between groups. Seventeen (14%) patients required more than 1 hospitalization, with no difference between HCT type. There was a difference in days of hospital stay between HLA-identical and haploidentical recipients, 8 (1–23) vs. 12 (1–54) days respectively (P=0.024). No difference was observed at 30 and 100-day chimerism between HCT types. MRD screening at 30 and 100 days was similar between groups. A detailed description of the allo-HCT outcomes and complications is shown in Table 3.
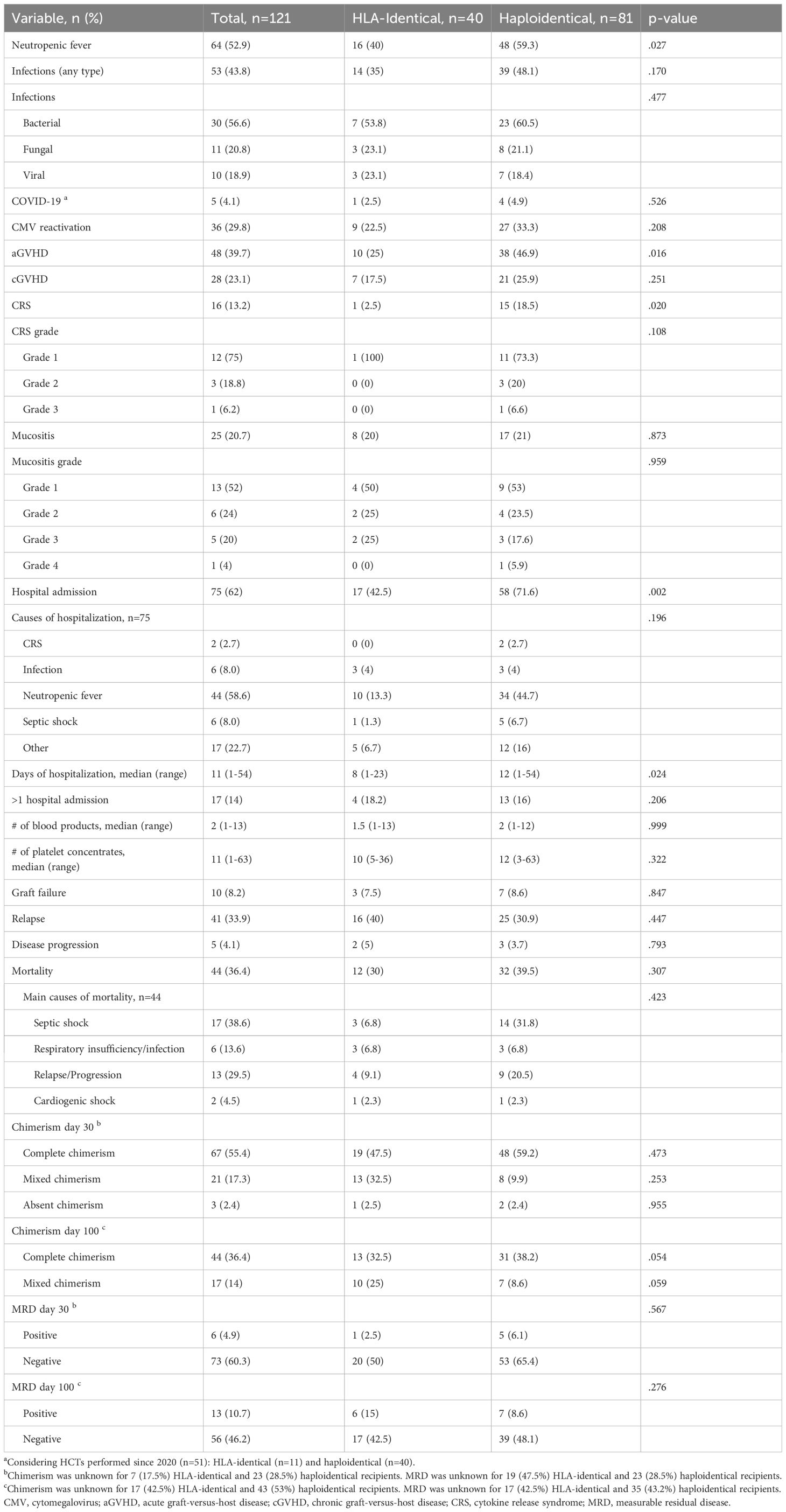
Table 3. Outcomes after outpatient allogeneic hematopoietic cell transplant (HCT) in 121 adults with acute leukemia.
3.3 Survival outcomes
At 31 months 50% of the cohort was alive, median OS for HLA-identical recipients was 61 (2–98) months, while for haplo-HCT it was 22 (1–69) months (P=0.283). The 2-year OS was 60.6% and 46.9% for HLA-identical and haploidentical HCT, respectively (P=0.464), OS for the whole cohort is shown in Figure 1A. Forty-four (36.4%) patients died in a median time of 6 (1–61) months, with no difference between HCT type (P=0.307). The main causes of death were septic shock (n=17, 38.6%), relapse or progression (n=13, 29.5%), and respiratory insufficiency or infection (n=6, 13.6%). Five-year OS for the patients diagnosed with ALL was 49.4%, while in the AML group it was 46.2% (P=0.508). Univariate and multivariate Cox regression analyses for OS were estimated (Table 4). In univariate and multivariate analysis, positive MRD at 30 days (HR 4.18, P=0.011 and HR 8.8, P=0.018) and 100 days (HR 4.72, P=0.003 and HR 28.5, P=0.022) was associated with lower OS, while in the univariate analysis, patients with infections of any type had an increased risk for an event in the OS (HR 3.28, P=0.001); bacterial infections were of most risk (HR 2.41, P=0.005). These findings are illustrated in Figure 2. Median OS for patients with 30-day positive MRD was 12 months, versus 61 months for those negative (P=0.005).
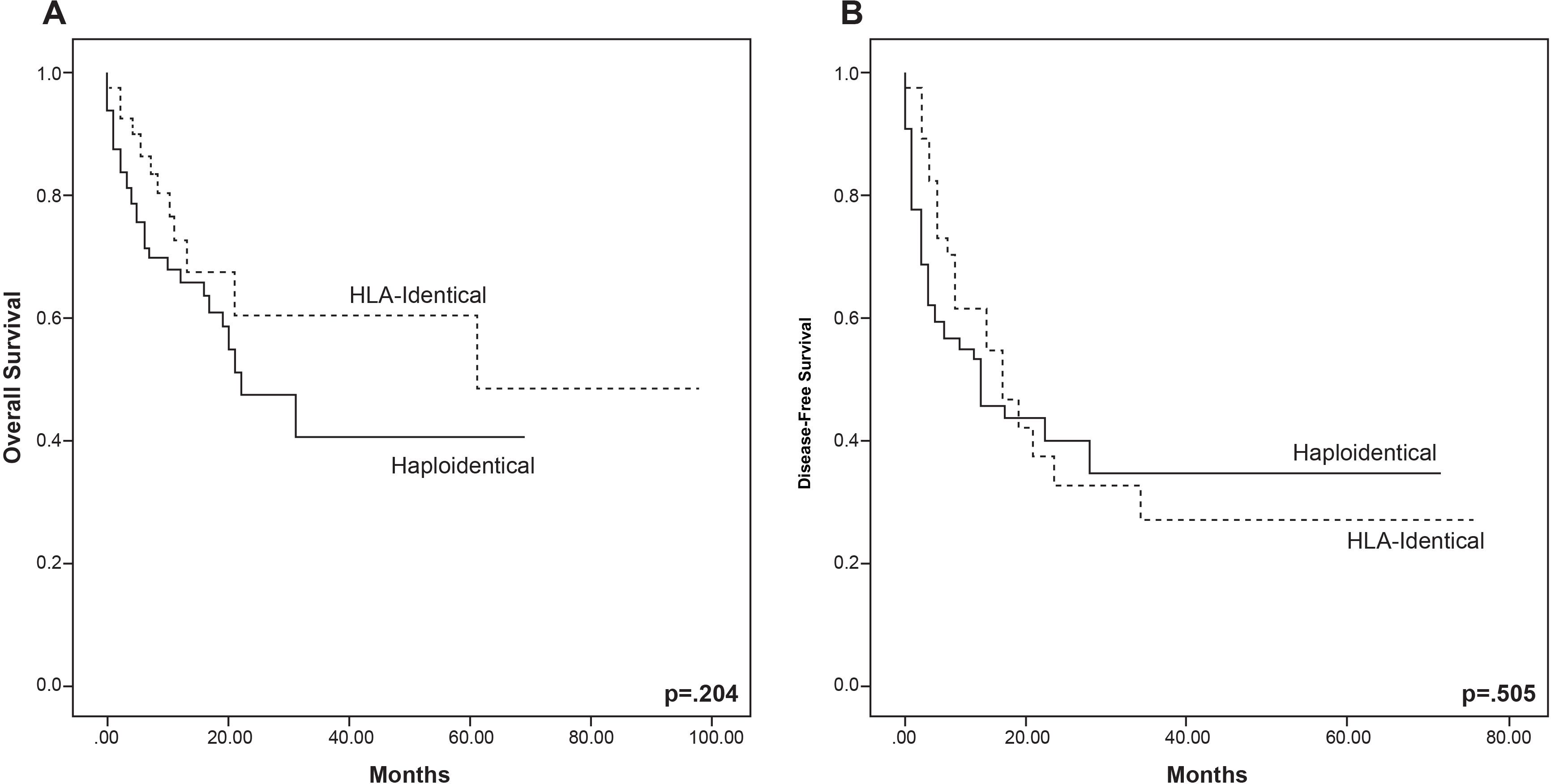
Figure 1. Overall survival (A) and disease-free survival (B) by allogeneic hematopoietic cell transplant types of 121 patients with acute leukemia in a completely outpatient setting and with reduced intensity conditioning. P-values represent overall comparisons without reference to specific time points.
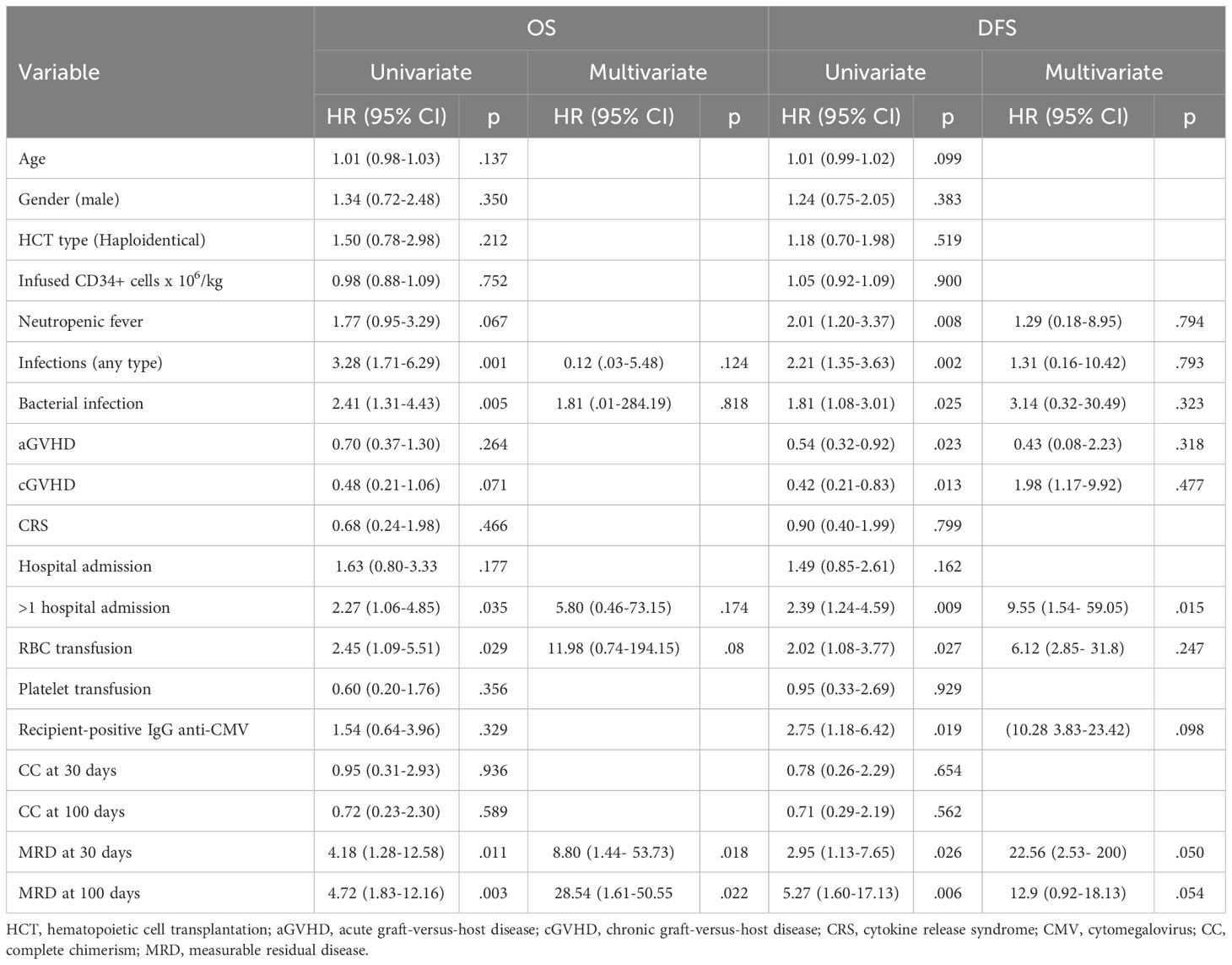
Table 4. Univariate and multivariate analyses of risk factors for Overall Survival and Disease-Free Survival in acute leukemia after an outpatient allogeneic hematopoietic cell transplant with a reduced intensity regimen.
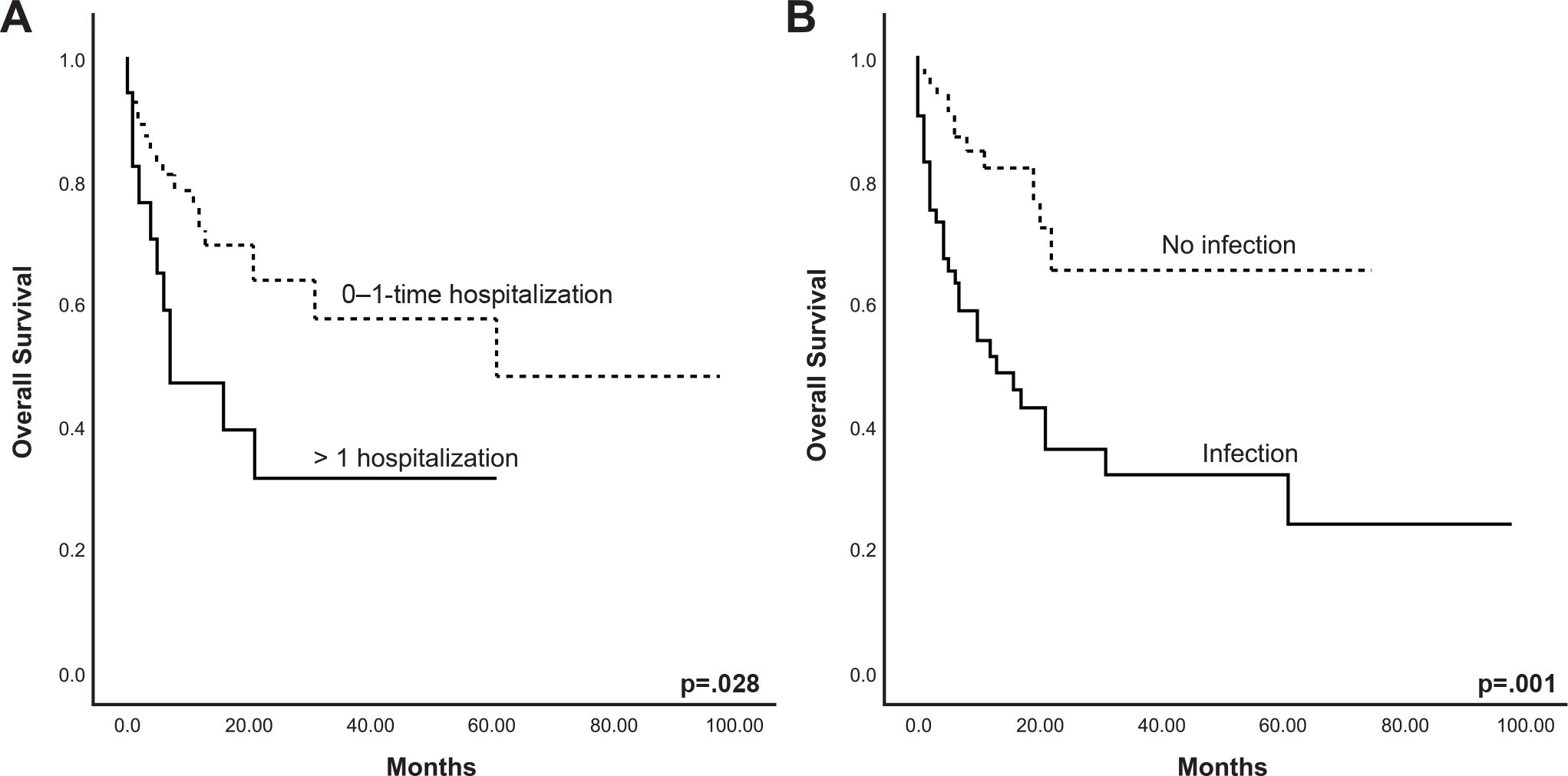
Figure 2. Overall survival of 121 patients with acute leukemia considering those who presented post-hematopoietic cell transplant complications: (A) >1 hospitalization, (B) infection. P-values represent overall comparisons without reference to specific time points.
Although hospital admissions per se had no risk for mortality, patients with more than 1 hospitalization were at greater risk (HR 2.27, P=0.035). Patients who received red blood cell transfusions (HR 2.45, P=0.029) had an increased mortality risk in univariate analysis. Platelet transfusions did not increase this risk, Table 4.
3.4 Disease-free survival
The median DFS for the total cohort was 6 (1–75) months, 9 (1–75) months for HLA-identical, and 5 (1–69) for haplo-HCT (P=0.067). The two-year DFS was 33.3% and 35% for HLA-identical and haplo-HCT, respectively (P=0.924), Figure 1B. Forty-one (33.9%) patients relapsed, 5 (4.1%) had disease progression, and 10 (8.2%) had GF after allo-HCT, with no difference between HCT types for any of these events (Table 3). Cox regression analyses for DFS are shown in Table 4. In the univariate analysis, post-HCT complications, such as neutropenic fever (HR 2.01, P=0.008), infections of any type (HR 2.21, P=0.002), bacterial infections (HR 1.81, P=0.025), more than 1 hospitalization (HR 2.39, P=0.009), and RBC transfusions (HR 2.02, P=0.027), were all associated with increased risk of lower DFS. Both aGVHD (HR 0.540, P=0.023) and cGVHD (HR 0.42, P=0.013) conferred a lower risk for an event in DFS in the univariate analysis, this was confirmed in Kaplan-Meier analysis, with a higher DFS in the presence of aGVHD (P=0.017) and cGVHD (P=0.012), Figure 3A, B. Recipient IgG reactive to CMV was a risk factor for lower DFS (HR 2.75, P=0.019). In univariate analysis, positive MRD at 30 (HR 2.95, P=0.026) and 100 days (HR 5.27, P=0.006) was associated with lower DFS. In the multivariate analysis, having >1 hospital admission (HR 9.55, P=0.015) and positive MRD on day 30 (HR 22.56, P=0.50) were associated with an increased risk for lower DFS. In the Kaplan-Meier analyses, >1 hospitalization, infection, red blood cell transfusion, and receiving a second transplant were all statistically significant for lower DFS, shown in Figures 3C–F. In multivariate analysis, only patients who had >1 hospital admission had lower DFS (HR 9.55, P=0.015).
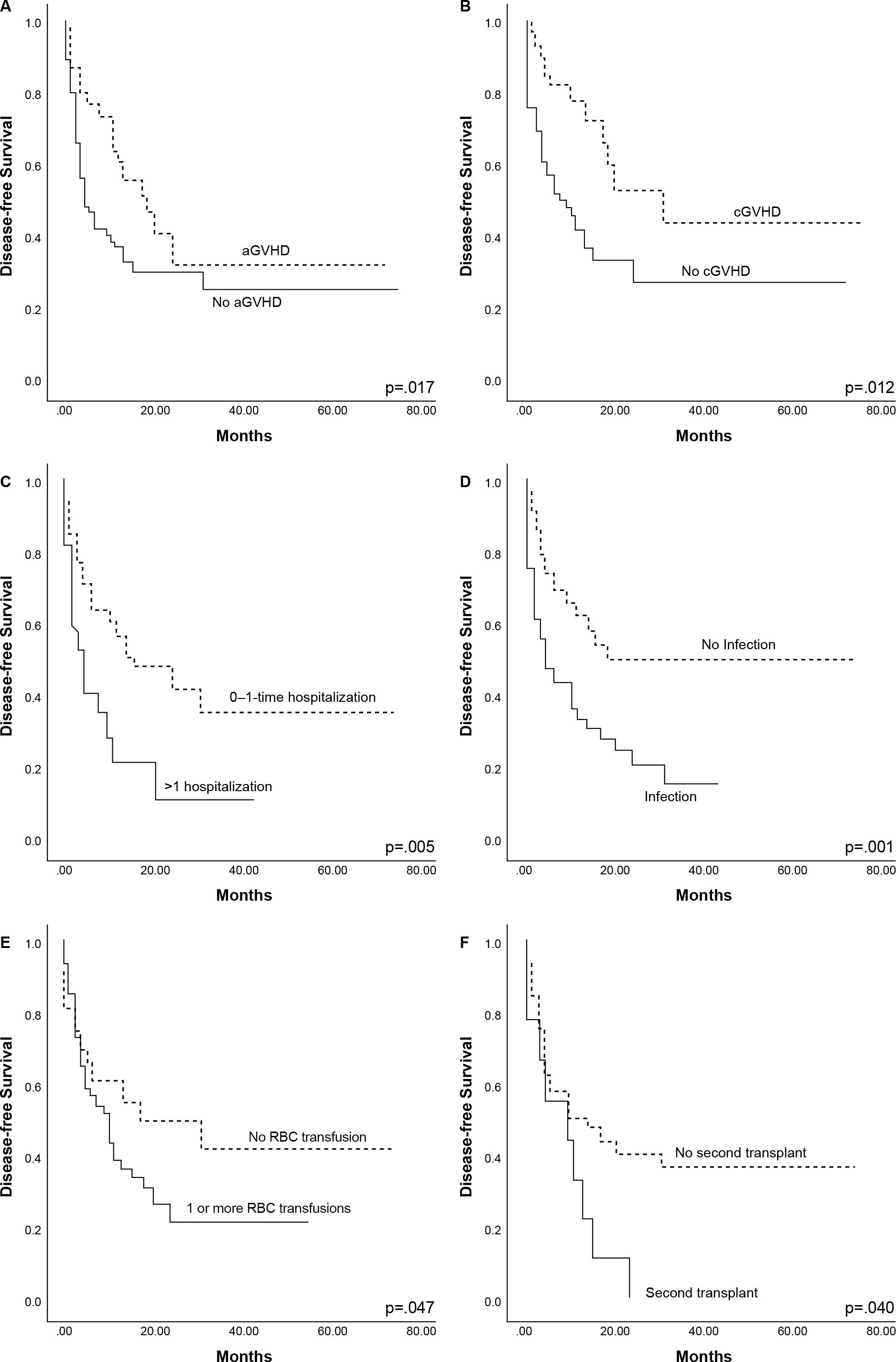
Figure 3. Complications affecting disease-free survival of 121 patients with acute leukemia: (A) acute graft-versus-host-disease (aGVHD), (B) chronic graft-versus-host-disease (cGVHD), (C) >1 hospitalization, (D) infection, (E) transfusion, (F) second transplant. P-values represent overall comparisons without reference to specific time points.
3.5 Relapse and non-relapse mortality
The cumulative incidence of relapse (CIR) for the whole cohort was 44% at 2 years (95% CI 32-55%). No significant difference was observed between transplant types (P=0.800). The cumulative incidence of NRM was 20% at 2 years (95% CI 13-28%) for the entire cohort, with no statistical difference between transplant types (P=0.500). Patients with positive 30-day MRD showed no difference in the 6-month CIR compared to those with negative 30-day MRD, 60% versus 38% (P=0.500), Figure 4A; yet a significant difference was observed in the 6-month CIR between positive and negative 100-day MRD, 60% versus 12% (P=0.003), Figure 4B. A significant difference was observed in the cumulative incidence of 6-month NRM between positive and negative MRD patients at day 30, 20% versus 6.3% (P=0.023), Figure 4C; this finding was not significant between the 100-day MRD groups (P=0.900), Figure 4D.
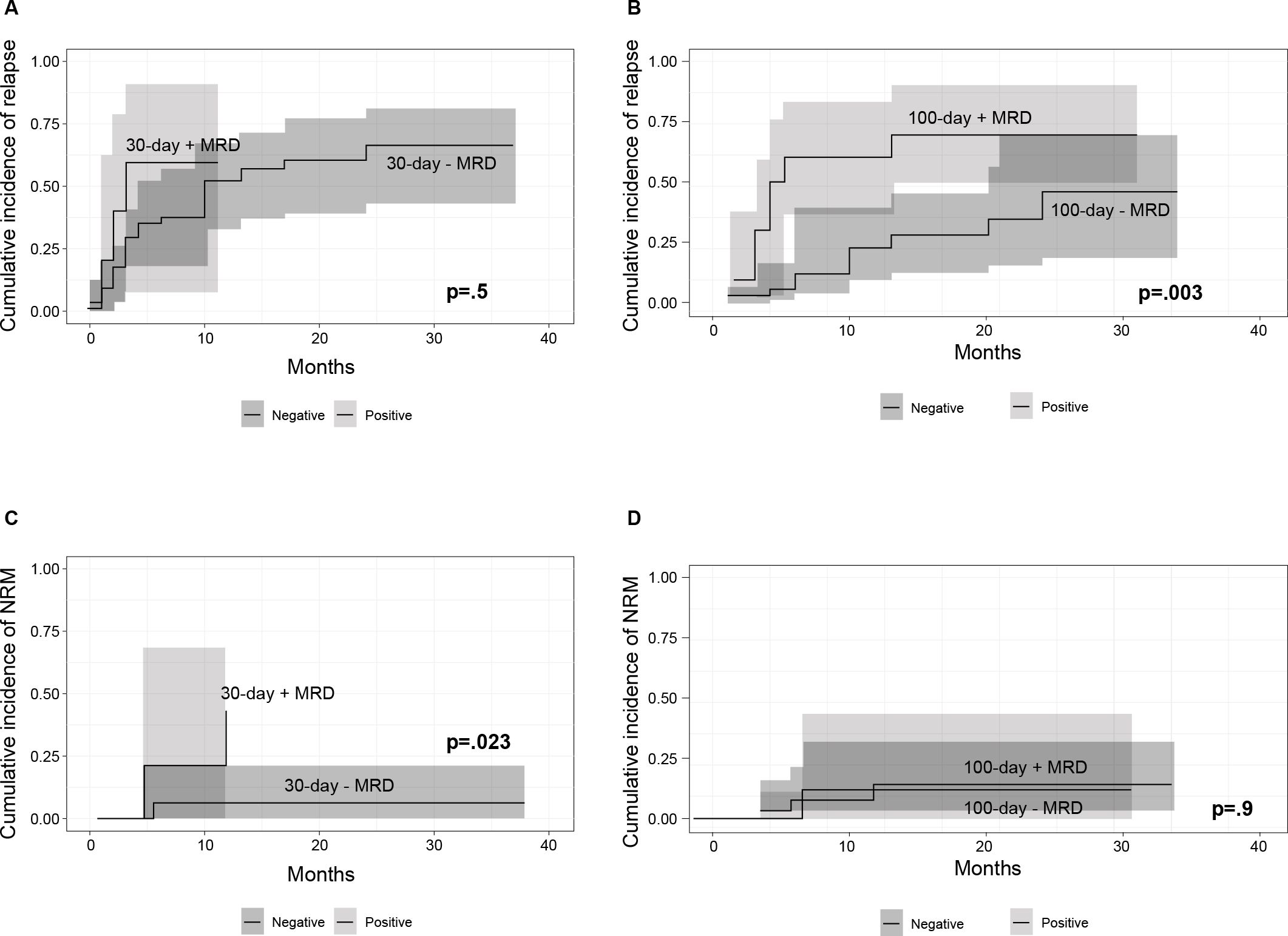
Figure 4. (A) Cumulative incidence of relapse (CIR) in patients with 30-day positive and negative minimal-residual disease (MRD) (B) CIR in patients with 100-day positive and negative MRD (C) CI of non-relapse mortality (NRM) in patients with 30-day positive and negative MRD (D) CI of NRM in patients with 100-day positive and negative MRD. P values refer to 6-month cumulative incidence of relapse and non-relapse mortality.
In the univariate analysis, an increase in age (HR 1.03, P=0.009) and patients with major ABO incompatibility (HR 2, P=0.040) had an increased risk for NRM. CGVHD was associated with decreased NRM in the univariate (HR 0.37, P=0.009) and multivariate analysis (HR 0.38, P=0.015). Positive MRD at 100 days increased relapse risk (HR 4.48, P=0.003) in the univariate and multivariate analyses (HR 4.67, P=0.008), as shown in Table 5.
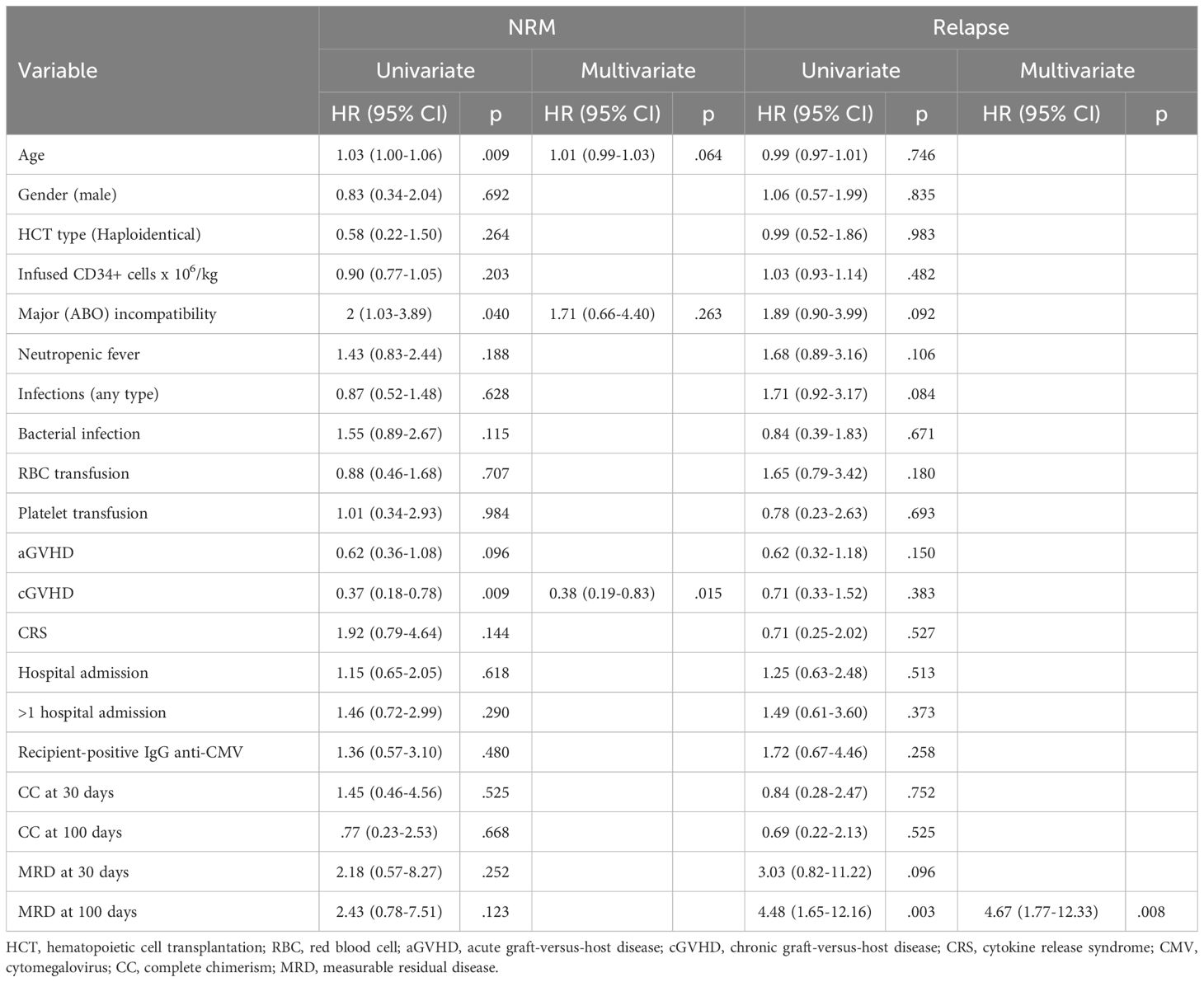
Table 5. Univariate and multivariate analyses of risk factors for non-relapse mortality (NRM) and relapse in acute leukemia after an outpatient allogeneic hematopoietic cell transplant with a reduced intensity regimen.
4 Discussion
The introduction of RIC regimens and alternative stem cell sources has made HCT more available to treat acute leukemia when considered appropriate, such as in high-risk disease or after relapse. Two major advances in hematopoietic cell transplantation derived from Luznik and cols.’ pioneering work, namely, the use of high-dose post-transplant cyclophosphamide for GVHD prophylaxis and HLA-haploidentical allografting (14–16), benefited our cohort.
The two main causes of death in acute leukemia after an HCT are transplant-related complications or disease relapse. We found that our outpatient peripheral blood allogeneic HCT program with a RIC regimen for AML achieved a 2-year OS of 46.2%, DFS of 28.8%, and NRM of 27.5%, in comparison to 58.5%, 53.2%, and 33% at 3 years in AML patients, respectively, in one report (17); for our allografted adults with ALL the corresponding 2-year rates were OS 55.5%, DFS 39.6%, and NRM 17.8%, while in a comparable group, 3-year rates for OS were 66%, for DFS 72.4%, and for NRM 20.3% (18). In a study including 331 AML patients allografted using RIC, 2-year OS was 66%, and NRM 22.5% (19). Thus, our findings are important due to the limited data on post-HCT clinical outcomes for acute leukemia reported by transplant centers in low-middle income countries (LMIC). Several factors could help explain the lower DFS observed in our cohort in comparison to other reports, including a positive MRD at the time of transplant, a second transplant, the use of RIC in AML, the presence of undetected Ph+ cases in ALL patients, a low incidence of GVHD, and the administration of sequential conditioning regimens in chemo-resistant leukemias employing a toxic scheme. Since only RIC was used, HCT performed in our center was conducted in an outpatient setting, making of it a cost-effective method, with an estimated cost of $ 11,053 ± 2,817 USD for ALL, and 10,251 ± 1,538 USD for AML, as previously reported (5); these costs are considerably lower than those documented for RIC HSCT in a study carried out at two centers in the USA, ranging from 96,000 (74–152,000) to 129,000 (84–171,000) USD; no differences in costs were found between centers (20); lower mean costs are reported from other countries, including Spain, 76.112 USD (21). Importantly, the previous comparisons are made with studies using outpatient (USA) and home care (Spain) models, not hospitalization.
Additionally, most uninsured patients belonging to the open population cannot afford an inpatient HCT. Most of the HCTs performed in this study were haploidentical, partly favored by our country’s lack of a well-established donor network, a limitation shared with many other LMICs. As observed, most haploidentical HCTs received a higher CD34+ cell infusion and had slower platelet engraftment, in line with other reports comparing HLA-identical recipients (22, 23). A higher infusion dose of CD34+ cells is associated with earlier engraftment and increased survival in patients with acute leukemia (24, 25), although in our study no association between the infused dose and survival was observed. In this respect, it is worth mentioning that the establishment of a CD34+ cell dose threshold for improving HCT outcomes is controversial. Since the infusion dose can be controlled before employing the HCT, this association should be clarified in future studies.
Haploidentical HCT has been associated with poor immune recovery and infections that lead to higher mortality and relapse rates (26–28). In addition, in previous reports comparing outcomes for an HLA-identical sibling vs. HLA-haploidentical HCT, the haploidentical group had significantly higher NRM, lower progression-free and overall survival, and higher risk of viral and fungal infections, as well as other complications (29, 30).
In the present study, haploidentical HCTs had more neutropenic fever cases than HLA-identical transplants, yet it did not increase the mortality risk and was not associated either in the univariate or multivariate analyses with OS. Additionally, it is known that a serious and frequent complication of infection is neutropenic fever; infection has been shown to increase the risk for decreased OS (28). Our results show that the incidence of infections in HLA-identical and haploidentical HCT was similar, 35% and 48%, P=0.170. These findings show that the infection incidence is lower than that reported with myeloablative inpatient allogeneic HCT (31, 32). HCT with RIC produces less myelosuppression and mucosal toxicity, which are implicated in a higher infection risk due to microbiota imbalance (31). In our study, patients with infections had a significantly lower OS rate. Yet, no difference in OS was observed between HCT types, confirming that haplo-HCT represents a safe transplant alternative to HLA-identical allografting. Additionally, a RIC regimen allows transplantation to be conducted in an outpatient setting, which exposes the patient to fewer nosocomial infections and, thus, reduces the risk for increased morbidity.
Close to 45% of the patients in our series had a documented infection and almost 20% of the total suffered infection related mortality (IRM); in addition, in univariate analysis, OS and DFS were significantly lower in patients who suffered infection compared to those who did not. Thus, infections were the principal cause of death in our transplant patients, confirming a previous report from our center (28), and similar reports in allo-HCT recipients (33–36). Most (41%) deaths due to infections occurred in the first one-hundred days following HCT, probably related to neutropenia and poor immune function (37). No differences in IRM were observed based on HCT type, a finding also observed in other cohorts (35, 38). Other studies documented an increased IRM in haplo-HCT recipients, proposing that delayed reconstitution of the immune system after PT-Cy could lead to increased IRM (36, 39).
Cytokine release syndrome (CRS) occurs in approximately 15% of outpatient procedures compared to 70% of inpatient HCT (9). Our results are comparable to the former at a rate of 18.5% in the haplo-HCT recipients, while for the HLA-identical group it was 2.5%. CRS was more common in our haploidentical patients, which has been previously reported as a frequent complication observed in 25-90% of unmanipulated peripheral blood HCT performed in haploidentical recipients treated with PTCy for GvHD prophylaxis, although its association with increased mortality has not been demonstrated in all studies (40–43). CRS did not increase the risk for a lower OS and DFS in our cohort. Since haploidentical HCT employment is increasing, especially in LMIC, measures to prevent and treat CRS effectively should be emphasized in these settings to reduce patient morbidity. Future studies employing outpatient HCTs with RIC should report risk factors that could predict CRS occurrence and severity and help prevent its development.
The most common cause for hospitalization was neutropenic fever in both haploidentical and HLA-identical HCT, although it was more common in the former. A recent review reported that 50-80% of patients were hospitalized after an outpatient allogeneic HCT with RIC, where neutropenic fever, infections, and regimen-related complications were the most common causes (44). Hospital admission was not associated with increased mortality, yet patients with more than one hospitalization had an increased risk for lower OS and DFS. Interestingly, limited information is available comparing hospitalization rates and causes between the different transplant types. This information should be reported in additional studies due to its important association with mortality. Identifying the most frequent causes can help transplant centers using RIC to improve outcomes through better prophylactic measures, especially in LMIC, where outpatient HCT is frequently performed.
Chimerism analyses are an important tool for clinicians to predict relapse. Its use is more frequent in HTCs using non-myeloablative conditionings due to its higher risk for disease relapse (45). There is limited information on chimerism between donor types. Other studies report findings similar to ours, yet they involve patients with aplastic anemia and non-malignant diseases with different graft sources and conditionings (46–49).
It has been reported that complete chimerism (CC) at 30 days post-transplant is associated with longer relapse-free survival (50). Our study found no association with OS, DFS, NRM, and relapse in patients with CC at 30- and 100-days post-transplant. Similarly, a previous report found no association of OS and DFS with mixed chimerism (MC) at 30- and 60-days post-transplant (51). In contrast, other studies have suggested that chimerism was significantly associated with survival (52, 53). Differences between studies demonstrating significant findings were that chimerism was analyzed as a continuous variable (53), and no specific time points were described. There is no universal consensus on the ideal regimen of post-HSCT chimerism follow-up. Intervals ranging from weekly to monthly analysis have been used, and for RIC regimens, measuring chimerism at 1, 2, 3, 6, and 12 months has been proposed (54, 55). This should be further addressed as it is highly relevant for LMIC, where measuring chimerism is a significant economic burden for most patients who pay out-of-pocket for these studies and should be performed in justified time points.
Measurable residual disease (MRD) detection predicts survival and relapse in acute leukemia (54, 55). However, its association with OS, DFS, and relapse after an outpatient transplant and its pertinent time points remains inconclusive (56). Our results confirm that early positive MRD at day 30 post-HCT increases the risk for lower OS. A similar study demonstrates the clinical relevance of 30-day MRD post-transplant with survival outcomes (57). Although we did not find a higher NRM in the presence of 30-day MRD+, an increased risk for NRM in MRD+ patients has been reported (58). In our cohort, MRD positivity at day 100, but not at day 30, increased the patient’s risk for relapse at 6 months, probably reflecting the time-dependent nature of this complication. Also, the number of MRD-positive recipients at 100 days was greater than those at 30 days; thus, there were more patients at risk in the group who relapsed significantly more at 6 months. Thus, there was a correlation between MRD+ and relapse, and the discrepancies observed with the CIR in the 30-day MRD+ group will probably be solved in a larger series that include more patients at risk on day 30. These results support that MRD is more relevant for predicting relapse than chimerism, as reported in recent studies (59, 60).
It is noteworthy that no difference in most of the principal transplant characteristics, complications and outcomes, including OS, DFS, relapse, and GVHD, were found when allografted patients were compared according to type of leukemia, ALL vs. AML. This suggests that despite their known biological features and differences in clinical behavior, HSCT can give an equivalent survival probability to both types of leukemia.
In our center the graft is infused the same day it is obtained; although there were no delays in the reported cohort, it is important to consider that, due to the short viability period of hematoprogenitors, there is limited time to solve complications forcing a delay in the infusion day. These can include, for example, a receptor experiencing fever before or on day 0, or a donor not mobilizing enough cells on the transplant day; thus, a protocol to deal with events delaying or preventing the graft infusion on the scheduled day should be in place at each center.
Among the several limitations in this report, due to budgetary restrictions in the health system over the study period, partial data for MRD and chimerism are to be noted; the main reason for this is that our retrospective study spans over 10 years, and routine performance of these two laboratory measures was adopted at our center five years ago. In addition, Ph chromosome status was not available for most patients in the cohort; also, since most of our patients come from outstate and are allowed to continue their vigilance with their local hematologists after returning home to limit their out-of-pocket travel expenses, there was a relatively short follow-up. Finally, a low number of events for 30-day MRD univariate analysis could have contributed to the lack of statistical significance in Cox regression, yet this number was sufficient to yield a significant cumulative incidence for NRM.
In conclusion, outpatient HLA-identical and haploidentical transplants after reduced-intensity conditioning in adult patients with AML and ALL from a low-income population demonstrated high efficacy, achieving survival rates comparable to those reported from developed countries with inpatient procedures employing myeloablative conditioning. An acceptable safety profile was documented, although improved efforts to decrease the elevated rate of infection-related mortality are needed, which requires statistically powered collaborative efforts for defining the best strategy to deal with this potentially fatal complication.
Data availability statement
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving humans were approved by Ethics and Research Committee of the School of Medicine and Dr. José Eleuterio González University Hospital, Universidad Autónoma de Nuevo León. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
JJ-P: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. JV-V: Data curation, Formal analysis, Investigation, Software, Validation, Writing – review & editing. AG-L: Methodology, Resources, Validation, Writing – review & editing. RB-L: Data curation, Formal analysis, Software, Visualization, Writing – review & editing. AD-V: Writing – review & editing, Formal analysis. OC-R: Investigation, Software, Validation, Writing – review & editing, Methodology, Project administration, Resources. CG-A: Investigation, Validation, Writing – review & editing, Data curation, Software. DG-A: Writing – review & editing, Investigation, Methodology, Project administration, Resources, Supervision, Validation.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors thank Sergio Lozano-Rodríguez, MD, for his critical manuscript review.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Lozano Cerrada S, Altaf SY, Olavarria E. Allogeneic stem cell transplantation from unrelated donors in acute leukaemia. Curr Opin Oncol. (2018) 30:418–24. doi: 10.1097/CCO.0000000000000485
2. Bailén R, Pascual-Cascón MJ, Guerreiro M, López-Corral L, Chinea A, Bermúdez A, et al. Post-transplantation cyclophosphamide after HLA identical compared to haploidentical donor transplant in acute myeloid leukemia: A study on behalf of GETH-TC. Transplant Cell Ther. (2022) 28:204.e1–10. doi: 10.1016/j.jtct.2022.01.020
3. Fuchs EJ. Haploidentical transplantation for hematologic Malignancies: where do we stand? Hematol Am Soc Hematol Educ Program. (2012), 230–6. doi: 10.1182/asheducation-2012.1.230
4. Subirà M, Sureda A, Ancín I, Martino R, Altés A, Brunet S, et al. Allogeneic stem cell transplantation with reduced-intensity conditioning is potentially feasible as an outpatient procedure. Bone Marrow Transplant. (2003) 32:869–72. doi: 10.1038/sj.bmt.1704254
5. Jaime-Pérez JC, Heredia-Salazar AC, Cantú-Rodríguez OG, Gutiérrez-Aguirre H, Villarreal-Villarreal CD, Mancías-Guerra C, et al. Cost structure and clinical outcome of a stem cell transplantation program in a developing country: the experience in northeast Mexico. Oncologist. (2015) 20:386–92. doi: 10.1634/theoncologist.2014-0218
6. Jaime-Pérez JC, Salazar-Cavazos L, Aguilar-Calderón P, Herrera-Garza JL, Gutiérrez-Aguirre CH, Gómez-Almaguer D. Assessing the efficacy of an ambulatory peripheral blood hematopoietic stem cell transplant program using reduced intensity conditioning in a low-middle-income country. Bone Marrow Transplant. (2019) 54:828–38. doi: 10.1038/s41409-018-0338-7
7. Douer D, Santillana S, Ramezani L, Samanez C, Slovak ML, Lee MS, et al. Acute promyelocytic leukaemia in patients originating in Latin America is associated with an increased frequency of the bcr1 subtype of the PML/RARα fusion gene. Br J Haematol. (2003) 122:563–70. doi: 10.1046/j.1365-2141.2003.04480.x
8. Switzer GE, Bruce JG, Myaskovsky L, Dimartini A, Shellmer D, Confer DL, et al. Race and ethnicity in decisions about unrelated hematopoietic stem cell donation. Blood. (2013) 121:1469–76. doi: 10.1182/blood-2012-06-437343
9. Colunga-Pedraza PR, Gómez-De León A, Rodríguez-Roque CS, Morcos-Sandino M, Colunga-Pedraza JE, Cantú-Rodriguez OG, et al. Outpatient haploidentical stem cell transplantation using post-transplant cyclophosphamide is safe and feasible. Transplant Cell Ther. (2021) 27:259. doi: 10.1016/j.jtct.2020.12.006
10. Jaime-Pérez JC, Hernández-Coronado M, Picón-Galindo E, Salazar-Cavazos L, Gutiérrez-Aguirre CH, Gómez-Almaguer D. Results of a completely outpatient autologous stem cell transplant program for lymphoma patients receiving reduced-intensity conditioning. Leuk Lymphoma. (2021) 62:1619–28. doi: 10.1080/10428194.2021.1876870
11. Glucksberg H, Storb R, Fefer A, Buckner CD, Neiman PE, Clift RA, et al. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HLA-matched sibling donors. Transplantation. (1974) 18:295–304. doi: 10.1097/00007890-197410000-00001
12. Jagasia MH, Greinix HT, Arora M, Williams KM, Wolff D, Cowen EW, et al. National institutes of health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. The 2014 diagnosis and staging working group report. Biol Blood Marrow Transplant. (2015) 21:389–401.e1. doi: 10.1016/j.bbmt.2014.12.001
13. Kharfan-Dabaja MA, Kumar A, Ayala E, Aljurf M, Nishihori T, Marsh R, et al. Standardizing definitions of hematopoietic recovery, graft rejection, graft failure, poor graft function, and donor chimerism in allogeneic hematopoietic cell transplantation: A report on behalf of the american society for transplantation and cellular therapy. Transplant Cell Ther. (2021) 27:642–649. doi: 10.1016/j.jtct.2021.04.007
14. Luznik L, Jalla S, Engstrom LW, Iannone R, Fuchs EJ. Durable engraftment of major histocompatibility complex-incompatible cells after nonmyeloablative conditioning with fludarabine, low-dose total body irradiation, and posttransplantation cyclophosphamide. Blood. (2001) 98:3456–64. doi: 10.1182/blood.v98.12.3456
15. Luznik L, O’Donnell PV, Fuchs EJ. Post-transplantation cyclophosphamide for tolerance induction in HLA-haploidentical bone marrow transplantation. Semin Oncol. (2012) 39:683–93. doi: 10.1053/j.seminoncol.2012.09.005
16. Rimando J, McCurdy SR, Luznik L. How I prevent GVHD in high-risk patients: posttransplant cyclophosphamide and beyond. Blood. (2023) 141:49–59. doi: 10.1182/blood.2021015129
17. Sharma SK, Choudhary D, Doval D, Khandelwal V, Patel A, Setia R, et al. Myeloablative versus reduced intensity conditioning regimens for allogeneic hematopoietic stem cell transplant for acute myeloid leukemia and myelodysplastic syndrome: A retrospective analysis. Indian J Hematol Blood Transfus. (2021) 37:472–8. doi: 10.1007/s12288-020-01386-6
18. Oliveira Fernandes Junior I, Arcuri LJ. Myeloablative or reduced-intensity/non myeloablative hematopoietic cell transplantation for Philadelphia-positive acute lymphoblastic leukemia in adults older than 40 years old - a secondary analysis of a CIBMTR database. Ann Hematol. (2024) 103:603–7. doi: 10.1007/s00277-023-0
19. Alfaro Moya T, Mattsson J, Remberger M, Lipton JH, Kim DD, Viswabandya A, et al. Influence of conditioning regimen intensity on outcomes post-allogeneic hematopoietic cell transplantation for acute myeloid leukemia in complete morphological remission. Eur J Haematol. (2023) 111:553–61. doi: 10.1111/ejh.14041
20. Khera N, Emmert A, Storer BE, Sandmaier BM, Alyea EP, Lee SJ. Costs of allogeneic hematopoietic cell transplantation using reduced intensity conditioning regimens. Oncologist. (2014) 19:639–44. doi: 10.1634/theoncologist.2013-0406
21. Gutiérrez-García G, Rovira M, Arab N, Gallego C, Sánchez J, Ángeles Álvarez M, et al. A reproducible and safe at-home allogeneic haematopoietic cell transplant program: first experience in Central and Southern Europe. Bone Marrow Transplant. (2020) 55:965–73. doi: 10.1038/s41409-019-0768-x
22. Atsuta Y, Sugita J, Nakamae H, Maruyama Y, Ishiyama K, Shiratori S, et al. Comparable survival outcomes with haploidentical stem cell transplantation and unrelated bone marrow transplantation. Bone Marrow Transplant. (2022) 57:1781–7. doi: 10.1038/s41409-022-01822-3
23. Yamazaki R, Kuwana M, Mori T, Okazaki Y, Kawakami Y, Ikeda Y, et al. Prolonged thrombocytopenia after allogeneic hematopoietic stem cell transplantation: Associations with impaired platelet production and increased platelet turnover. Bone Marrow Transplant. (2006) 38:377–84. doi: 10.1038/sj.bmt.1705444
24. Aversa F, Prezioso L, Manfra I, Galaverna F, Spolzino A, Monti A. Immunity to infections after haploidentical hematopoietic stem cell transplantation. Mediterr J Hematol Infect Dis. (2016) 8:e2016057. doi: 10.4084/MJHID.2016.057
25. Klingebiel T, Cornish J, Labopin M, Locatelli F, Darbyshire P, Handgretinger R, et al. Results and factors influencing outcome after fully haploidentical hematopoietic stem cell transplantation in children with very high-risk acute lymphoblastic leukemia: Impact of center size: An analysis on behalf of the Acute Leukemia and Pediatric Disease Working Parties of the European Blood and Marrow Transplant group. Blood. (2010) 115:3437–46. doi: 10.1182/blood-2009-03-207001
26. Pei X, Zhao X, Wang Y, Xu L, Zhang X, Liu K, et al. Comparison of reference values for immune recovery between event-free patients receiving haploidentical allografts and those receiving human leukocyte antigen-matched sibling donor allografts. Front Med. (2018) 12:153–63. doi: 10.1007/s11684-017-0548-1
27. Liu J, Yan C, Zhang C, Xu L, Liu Y, Huang X. Late-onset Epstein-Barr virus-related disease in acute leukemia patients after haploidentical hematopoietic stem cell transplantation is associated with impaired early recovery of T and B lymphocytes. Clin Transplant. (2015) 29:904–10. doi: 10.1111/ctr.12593
28. Jaime-Pérez JC, Meléndez-Flores JD, Ramos-Dávila EM, Gutiérrez-Aguirre CH, Cantú-Rodríguez OG, Marfil-Rivera LJ, et al. Infection-related mortality after HLA-identical and haploidentical hematopoietic cell transplantation using reduced-intensity conditioning in an outpatient setting. Clin Transplant. (2023) 37:e14972. doi: 10.1111/ctr.14972
29. Mehta RS, Saliba RM, Ghanem S, Alousi AM, Rondon G, Anderlini P, et al. Haploidentical versus Matched Unrelated versus Matched Sibling Donor Hematopoietic Cell Transplantation with Post-Transplantation Cyclophosphamide. Transplant Cell Ther. (2022) 28:395. doi: 10.1016/j.jtct.2022.04.020
30. Battipaglia G, Boumendil A, Labopin M, Ciceri F, Tischer J, Stelljes M, et al. Unmanipulated haploidentical versus HLA-matched sibling allogeneic hematopoietic stem cell transplantation in relapsed/refractory acute myeloid leukemia: a retrospective study on behalf of the ALWP of the EBMT. Bone Marrow Transplant. (2019) 54:1499–510. doi: 10.1038/s41409-019-0459-7
31. Junghanss C, Marr KA, Carter RA, Sandmaier BM, Maris MB, Maloney DG, et al. Incidence and outcome of bacterial and fungal infections following nonmyeloablative compared with myeloablative allogeneic hematopoietic stem cell transplantation: A matched control study. Biol Blood Marrow Transplant. (2002) 8:512–20. doi: 10.1053/bbmt.2002.v8.pm12374456
32. Ustun C, Young JAH, Papanicolaou GA, Kim S, Ahn KW, Chen M, et al. Bacterial blood stream infections (BSIs), particularly post-engraftment BSIs, are associated with increased mortality after allogeneic hematopoietic cell transplantation. Bone Marrow Transplant. (2019) 54:1254–65. doi: 10.1038/s41409-018-0401-4
33. Lindsay J, Kerridge I, Wilcox L, Tran S, O'Brien TA, Greenwood M, et al. Infection-related mortality in adults and children undergoing allogeneic hematopoietic cell transplantation: an Australian registry report. Transplant Cell Ther. (2021) 27:798. doi: 10.1016/j.jtct.2021.05.028
34. Esquirol A, Pascual MJ, Kwon M, Pérez A, Parody R, Ferra C, et al. Severe infections and infection-related mortality in a large series of haploidentical hematopoietic stem cell transplantation with post-transplant cyclophosphamide. Bone Marrow Transplant. (2021) 56:2432–44. doi: 10.1038/s41409-021-01328-4
35. Irene G-C, Albert E, Anna B-V, Rahinatu A, Silvana N, Silvana S, et al. Patterns of infection and infectious-related mortality in patients receiving post-transplant high dose cyclophosphamide as graft-versus-host-disease prophylaxis: impact of HLA donor matching. Bone Marrow Transplant. (2021) 56:818–27. doi: 10.1038/s41409-020-01092-x
36. Chang J, Hsiao M, Blodget E, Akhtari M. Increased risk of 100-day and 1-year infection-related mortality and complications in haploidentical stem cell transplantation. J Blood Med. (2019) 10:135–43. doi: 10.2147/JBM.S201073
37. Centers for Disease Control and Prevention, Infectious Diseases Society of America, American Society of Blood and Marrow Transplantation. Guidelines for preventing opportunistic infections among hematopoietic stem cell transplant recipients. Cytotherapy. (2001) 3:41–54. doi: 10.1080/146532401753156403
38. Oltolini C, Greco R, Galli L, Clerici D, Lorentino F, Xue E, et al. Infections after allogenic transplant with post-transplant cyclophosphamide: impact of donor HLA matching. Biol Blood Marrow Transplant. (2020) 26:1179–88. doi: 10.1016/j.bbmt.2020.01.013
39. Bashey A, Zhang X, Jackson K, Jackson K, Morris LE, Holland HK, et al. Comparison of outcomes of hematopoietic cell transplants from T-replete haploidentical donors using post-transplantation cyclophosphamide with 10 of 10 HLA-A, -B, -C, -DRB1, and -DQB1 allele-matched unrelated donors and HLA-identical sibling donors: a mul. Biol Blood Marrow Transplant. (2016) 22:125–33. doi: 10.1016/j.bbmt.2015.09.002
40. Raj RV, Hamadani M, Szabo A, Pasquini MC, Shah NN, Drobyski WR, et al. Peripheral blood grafts for T cell–replete haploidentical transplantation increase the incidence and severity of cytokine release syndrome. Biol Blood Marrow Transplant. (2018) 24:1664–70. doi: 10.1016/j.bbmt.2018.04.010
41. Imus PH, Blackford AL, Bettinotti M, Luznik L, Fuchs EJ, Huff CA, et al. Severe cytokine release syndrome after haploidentical peripheral blood stem cell transplantation. Biol Blood Marrow Transplant. (2019) 25:2431–7. doi: 10.1016/j.bbmt.2019.07.027
42. Abboud R, Wan F, Mariotti J, Arango M, Castagna L, Romee R, et al. Cytokine release syndrome after haploidentical hematopoietic cell transplantation: an international multicenter analysis. Bone Marrow Transplant. (2021) 56:2763–70. doi: 10.1038/s41409-021-01403-w
43. Tang J, Jensen R, Bryan B, Hoda D, Hunter B. Reduced incidence of cytokine release syndrome and improved outcomes with earlier initiation of immunosuppressive therapy in haploidentical stem cell transplant. Blood. (2022) 140:10528–9. doi: 10.1182/blood-2022-163853
44. Gómez-Almaguer D, Gómez-De León A, Colunga-Pedraza PR, Cantú-Rodríguez OG, Gutierrez-Aguirre CH, Ruíz-Arguelles G. Outpatient allogeneic hematopoietic stem-cell transplantation: a review. Ther Adv Hematol. (2022) 13:20406207221080739. doi: 10.1177/20406207221080739
45. Blouin AG, Ye F, Williams J, Askar M. A practical guide to chimerism analysis: Review of the literature and testing practices worldwide. Hum Immunol. (2021) 82:838–49. doi: 10.1016/j.humimm.2021.07.013
46. Xu Z-L, Xu L-P, Wu D-P, Wang S-Q, Zhang X, Xi R, et al. Comparable long-term outcomes between upfront haploidentical and identical sibling donor transplant in aplastic anemia: a national registry-based study. Haematologica. (2022) 107:2918–27. doi: 10.3324/haematol.2022.280758
47. Zhang Y, Li Y, Wu L, Zhou M, Wang C, Mo W, et al. Mixed chimerism after allogeneic hematopoietic stem cell transplantation for severe aplastic anemia. Hematol (United Kingdom). (2021) 26:435–43. doi: 10.1080/16078454.2021.1938422
48. Xu ZL, Cheng YF, Zhang YY, Mo XD, Han TT, Wang FR, et al. The incidence, clinical outcome, and protective factors of mixed chimerism following hematopoietic stem cell transplantation for severe aplastic anemia. Clin Transplant. (2021) 35:e14160. doi: 10.1111/ctr.14160
49. Tan W, He Y, Feng X, Wu X, Li C, Liao J, et al. Mixed chimerism after allogeneic hematopoietic stem cell transplantation in patients with β Thalassemia: impact on outcome and risk factors. Blood. (2020) 136:48–9. doi: 10.1182/blood-2020-134448
50. Chen CT, Gau JP, Liu JH, Chiou TJ, Hsiao LT, Liu YC. Early achievement of full donor chimerism after allogeneic hematopoietic stem cell transplantation predicts lower relapse risk in patients with acute lymphoblastic leukemia. J Chin Med Assoc. (2018) 81:1038–43. doi: 10.1016/j.jcma.2018.06.005
51. Mountjoy L, Palmer J, Kunze KL, Khera N, Sproat LZ, Leis JF, et al. Does early chimerism testing predict outcomes after allogeneic hematopoietic stem cell transplantation? Leuk Lymphoma. (2021) 62:252–4. doi: 10.1080/10428194.2020.1827249
52. Jain T, Kunze KL, Mountjoy L, Partain DK, Kosiorek H, Khera N, et al. Early post-transplantation factors predict survival outcomes in patients undergoing allogeneic hematopoietic cell transplantation for myelofibrosis. Blood Cancer J. (2020) 10:36. doi: 10.1038/s41408-020-0302-9
53. Reshef R, Hexner EO, Loren AW, Frey NV, Stadtmauer EA, Luger SM, et al. Early donor chimerism levels predict relapse and survival after allogeneic stem cell transplantation with reduced-intensity conditioning. Biol Blood Marrow Transplant. (2014) 20:1758–66. doi: 10.1016/j.bbmt.2014.07.003
54. Wethmar K, Matern S, Eßeling E, Angenendt L, Pfeifer H, Brüggemann M, et al. Monitoring minimal residual/relapsing disease after allogeneic haematopoietic stem cell transplantation in adult patients with acute lymphoblastic leukaemia. Bone Marrow Transplant. (2020) 55:1410–20. doi: 10.1038/s41409-020-0801-0
55. Ivey A, Hills RK, Simpson MA, Jovanovic JV, Gilkes A, Grech A, et al. Assessment of minimal residual disease in standard-risk AML. New Engl J Med. (2016) 374:422–33. doi: 10.1056/nejmoa1507471
56. Waterhouse M, Pennisi S, Pfeifer D, Scherer F, Zeiser R, Duyster J, et al. Monitoring of measurable residual disease using circulating DNA after allogeneic hematopoietic cell transplantation. Cancers (Basel). (2022) 14:3307. doi: 10.3390/cancers14143307
57. Kim HJ, Kim Y, Kang D, Kim HS, Lee JM, Kim M, et al. Prognostic value of measurable residual disease monitoring by next-generation sequencing before and after allogeneic hematopoietic cell transplantation in acute myeloid leukemia. Blood Cancer J. (2021) 11:109. doi: 10.1038/s41408-021-00500-9
58. Shen X, Pan J, Qi C, Feng Y, Wu H, Qian S, et al. Impact of pre-transplantation minimal residual disease (MRD) on the outcome of Allogeneic hematopoietic stem cell transplantation for acute leukemia. Hematology. (2021) 26:295–300. doi: 10.1080/16078454.2021.1889162
59. Klyuchnikov E, Badbaran A, Massoud R, Fritzsche-Friedland U, Freiberger P, Ayuk F, et al. Post-transplantation day +100 minimal residual disease detection rather than mixed chimerism predicts relapses after allogeneic stem cell transplantation for intermediate-risk acute myelogenous leukemia patients undergoing transplantation in complete remission. Transplant Cell Ther. (2022) 28:374.e1–9. doi: 10.1016/j.jtct.2022.04.009
60. Devine SM, Owzar K, Blum W, Mulkey F, Stone RM, Hsu JW, et al. Phase II study of allogeneic transplantation for older patients with acute myeloid leukemia in first complete remission using a reduced-intensity conditioning regimen: Results from Cancer and Leukemia Group B 100103 (Alliance for Clinical Trials in Oncology)/Blood and Marrow Transplant Clinical Trial Network 0502. J Clin Oncol. (2015) 33:4167–75. doi: 10.1200/JCO.2015.62.7273
Keywords: hematopoietic cell transplant, outpatient transplantation, acute lymphoblastic leukemia, acute myeloblastic leukemia, reduced-intensity conditioning, peripheral blood transplant, Latin America
Citation: Jaime-Pérez JC, Valdespino-Valdes J, Gómez-De León A, Barragán-Longoria RV, Dominguez-Villanueva A, Cantú-Rodríguez OG, Gutiérrez-Aguirre CH and Gómez-Almaguer D (2024) A comparison of haploidentical versus HLA-identical sibling outpatient hematopoietic cell transplantation using reduced intensity conditioning in patients with acute leukemia. Front. Immunol. 15:1400610. doi: 10.3389/fimmu.2024.1400610
Received: 13 March 2024; Accepted: 12 September 2024;
Published: 04 October 2024.
Edited by:
Marta Garcia-Recio, Hospital Clinic of Barcelona, SpainReviewed by:
Olle Thor,Hans Ringdén, Karolinska Institutet (KI), SwedenBarry Paul, Levine Cancer Institute, United States
Copyright © 2024 Jaime-Pérez, Valdespino-Valdes, Gómez-De León, Barragán-Longoria, Dominguez-Villanueva, Cantú-Rodríguez, Gutiérrez-Aguirre and Gómez-Almaguer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Carlos Jaime-Pérez, Y2FyamFpbWU3QGdtYWlsLmNvbQ==
‡ORCID: Jorge Valdespino-Valdes, orcid.org/0000-0002-7889-8426
Renata Valeria Barragán-Longoria, orcid.org/0009-0004-0807-7405
Olga Graciela Cantú -Rodríguez, orcid.org/0000-0003-2134-3734