
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol., 29 April 2024
Sec. Nutritional Immunology
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1396589
This article is part of the Research TopicGluten-Related Disorders: Pathogenesis, Diagnosis, and TreatmentView all 10 articles
 Ana Luísa Falcomer1,2*
Ana Luísa Falcomer1,2* Bernardo Romão de Lima1,2
Bernardo Romão de Lima1,2 Priscila Farage3
Priscila Farage3 Samantha Fabris1Ruth Ritter1
Samantha Fabris1Ruth Ritter1 António Raposo4*
António Raposo4* Edite Teixeira-Lemos5
Edite Teixeira-Lemos5 Cláudia Chaves6
Cláudia Chaves6 Renata Puppin Zandonadi1
Renata Puppin Zandonadi1Celiac disease (CD) is an autoimmune chronic enteropathy provoked by gluten ingestion in genetically predisposed individuals. Considering it´s only safe treatment is a lifelong gluten-free diet, the burden of living with the disease becomes evident, as well as the need to assess CD health-related quality of life (HRQOL). This review aims to identify and analyze the instruments used to evaluate the HRQOL of adults with CD. This integrative review using a systematic approach was designed to achieve high scientific standards. Accordingly, the search strategy was developed and executed as recommended by the guideline of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. Detailed individual searches were developed to Pubmed, Science Direct, Scopus, Web of Science, and Google Scholar. After careful analysis of the papers, 43 studies were included, in which seven instruments were identified: Celiac Disease Questionnaire (CDQ) (n=21), Celiac Disease Specific Quality of Life Instrument (CD-QOL) (n=17), Celiac Disease Assessment Questionnaire (CDAQ) (n=4), CeliacQ-7 (n=1), CeliacQ-27 (n=1), Black and Orfila´s self-developed instrument (n=1) and the Coeliac Disease Quality of Life Questionnaire (CDQL) (n=1). The CDQ and CD-QOL were the two most applied instruments. Since the first focuses on the physical and mental symptoms related to the disease and the second focuses on the emotional repercussions of adhering to the GFD treatment for life (dysphoria), the CDQ application is an interesting option for countries that struggle with public policies for CD patients and patients with active CD. The CD-QOL could be used for countries with strict regulations for CD and gluten-free products and populations in remission. When comparing results among different populations, it is preferable to utilize culturally validated instruments, which have been applied across multiple countries, providing greater comparability between study findings.
Celiac disease (CD) is an autoimmune chronic enteropathy by the ingestion of gluten in genetically predisposed individuals. It affects approximately 1% of the world´s population (1). As CD is linked to small bowel mucosa damage, its classic form main feature includes gastrointestinal malabsorption syndrome. Its clinical picture usually includes chronic diarrhea, abdominal distention and pain, weight loss, and failure to grow in infants (2, 3).
However, patients also usually face a wide range of extraintestinal symptoms and disorders that might include chronic fatigue, depression, anxiety, osteoporosis, compromised fertility, and libido, especially in women (4, 5). Although CD ordinarily combines a vast number of symptoms, some individuals are asymptomatic, even in cases in which mucosal damage is present (6). Those patients have a heightened risk of complications since they do not recognize the clinical aggravation of CD and tend to be more resistant to the treatment (7, 8).
Until now, the only safe and effective treatment for CD is the adoption of a gluten-free diet (GFD), characterized by the exclusion of cereal grains (wheat, rye, barley, and, in some cases, oats) and all their derivatives from the diet (9). When following a strict GFD, most patients experience remission of the disease’s physical manifestations and normalization of small bowel mucosa (10, 11). Nonetheless, compliance with the GFD is challenging since it requires changes in lifelong dietary habits, which are accompanied by the lack of information and guidance for the preparation of healthy gluten-free meals among the general population, the high cost of gluten-free products, the risk of gluten cross-contamination, and even social exclusion (12). The combination of the physical, emotional, and social burdens and worries related to the GFD experienced by celiac patients is directly related to how they perceive their quality of life (4, 9).
Quality of life (QOL) is a multidimensional concept that includes subjective evaluations of both positive and negative aspects of life regarding individuals’ goals, expectations, standards, and concerns (13). In the past years, worries about QOL in CD have increased and many questionnaires have been developed, adapted to different cultures, and validated to explore patients’ perception of well-being (9, 14, 15).
However, instruments used to measure the QOL of celiac individuals must be carefully elaborated to comprise the specificities of CD, from its clinical manifestations to the overall difficulties faced regarding compliance with the GFD (16, 17). Thus, it is important to highlight that questionnaires whose domains do not address these particularities may present limitations (18, 19). Therefore, CD population-specific validated questionnaires are the most reliable ones since they include the patients’ struggles and CD specificities (20, 21).
To our knowledge, no studies compare the existing instruments that measure celiac individuals’ QOL, nor the main domains used to evaluate it. In this sense, this review aimed to identify and analyze the instruments used to evaluate the health-related quality of life of adults with celiac disease. The findings of this study may guide researchers in studies related to QOL and assist the development of public policies for celiac individuals, reducing the impact on health assistance and the costs of treatment of CD and its consequences.
This integrative review using a systematic approach was designed to achieve high scientific standards. Accordingly, the search strategy was developed and executed as recommended by the guideline of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (22).
This review included quantitative studies that developed; translated and culturally adapted; or validated questionnaires to measure the QOL of adults with CD. Studies that evaluated QOL in the population mentioned using instruments designed for people with CD were also included.
All studies that analyzed the QOL of celiac patients using instruments designed for the general population were excluded. Additionally, qualitative studies, studies in which the population evaluated was under eighteen years old, reviews, letters, conference summaries, case reports, short communications, and books were excluded.
Detailed individual search strategies were developed for the following databases: Pubmed, Science Direct, Scopus, and Web of Science. Partial gray literature research was conducted using Google Scholar. The final search in all databases was performed on September 7th, 2023. Additionally, a manual examination of the reference lists of the full-text studies included was performed to ensure that possible relevant studies that could have been lost during the electronic search of databases were identified.
The literature search was conducted in English using the following terms, their mesh terms, and synonyms: “quality of life” AND (“celiac disease” OR “coeliac disease”) AND (“questionnaire” OR “instrument”) AND “adults”. The appropriate combinations of truncation and words were selected and adapted to the search specificities of each database (Supplementary Table S1 - Supplementary File). No limitations of language or date of publication were applied; therefore, all studies published until the final search were included.
All references were managed by Endnote Web. After removing duplicate hits, the references were transferred to Rayyan, where the authors performed the selection of titles and abstracts.
Calibration exercises were conducted before starting the review to ensure consistency among reviewers. The selection was conducted in two phases. In phase 1, two reviewers (SF, RR) independently reviewed the titles and abstracts of all references identified from databases. Articles that did not meet the eligibility criteria were discarded. In phase 2, the same reviewers (SF, RR) applied the eligibility criteria to the full texts of the selected articles. In cases of disagreement, the two reviewers discussed until a consensus was obtained. A third reviewer (ALF) made the final decision when there was no consensus. These data were synthesized by the three reviewers (SR, RR, ALF) using a standardized table. The final selection was always based on the complete text of the publication. The list of references from the selected studies was critically evaluated by the BRL examiner. Additional studies were added by the experts (PF and RPZ). Figure 1 demonstrates the search and study selection processes through a flow diagram.
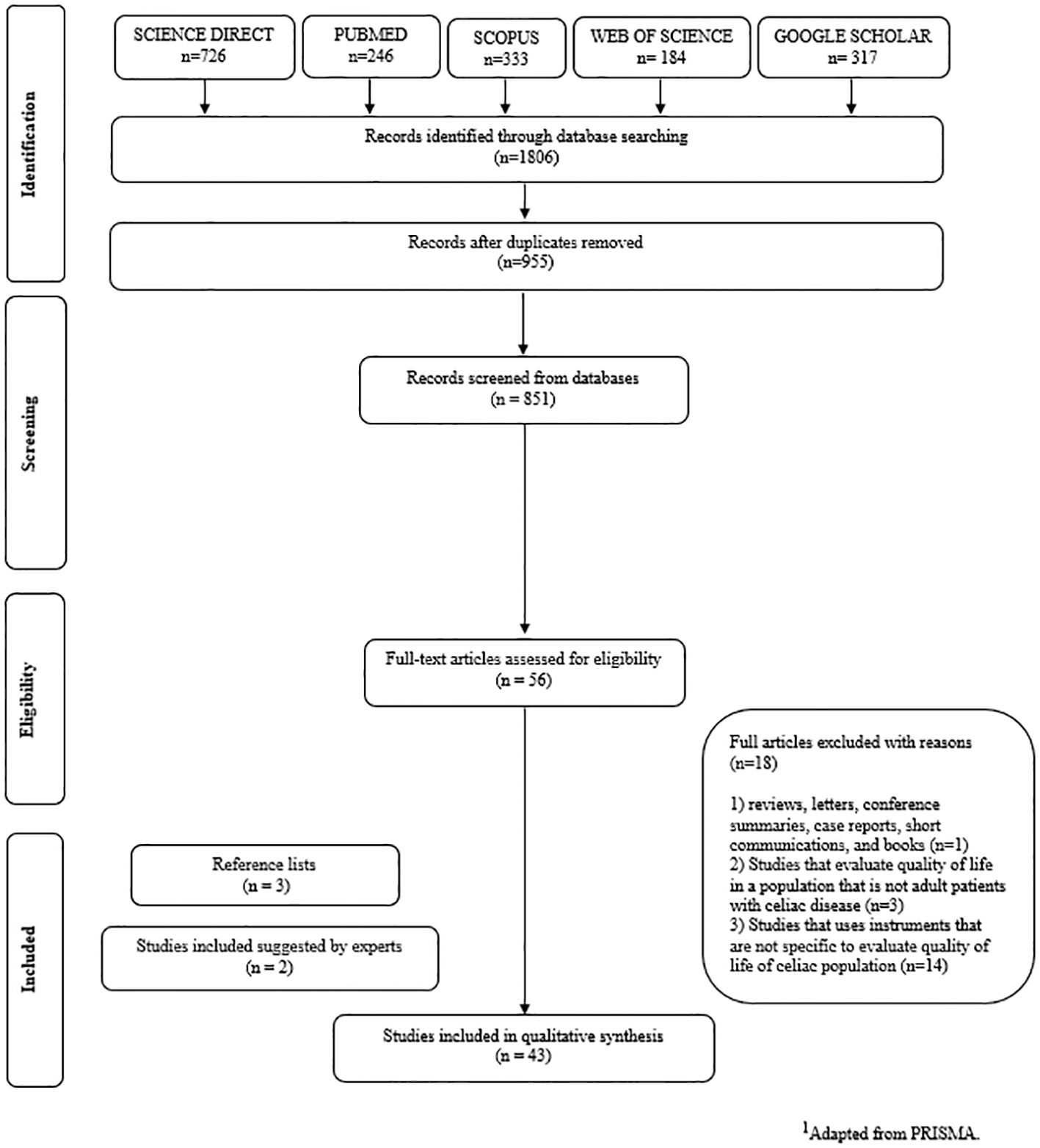
Figure 1 Flow Diagram of Literature Search and Selection Criteria.1
The following characteristics were collected from the selected articles and synthesized using a standardized table containing authors and year of publication, the country where the research was conducted, the aim of the study, methods, participants and sample size, instrument(s) used to measure the quality of life, and main findings. The complete table with collected results is available in Table 1.

Table 1 Summary of descriptive characteristics and instruments included in the studies.
After a systematic literature search and subsequent peer analysis, 43 studies, published between 2006 and 2023, were included in this review. Table 1 presents the studies’ general characteristics.
The 43 included studies were conducted in a total of 21 countries. Spain had the highest number of studies with 16.28% (n=7), followed by the United Kingdom (UK) (13.95%, n=6), the United States of America (USA), and Italy (9.3% each, n=4). In South America, Brazil accounted for 6.98% (n=3) of the studies, while Argentina, Chile, and Paraguay each contributed one study (2.33%). Iran, Portugal, France, and Germany each had two studies (4.65%, n=2 per country). Additionally, Canada, Hungary, Netherlands, Poland, Morocco, Australia, and Turkey contributed one study each (2.33% each). A collaboration between Denmark and Ireland resulted in a joint research contribution (2.33%, n=1). A choropleth map regarding the distribution of the frequencies of included studies by different countries is available in Figure 2.

Figure 2 Chroropleth map generated from the number of studies according to their origin. Higher frequencies are represented with darker tones of green.
This article comprises information on studies published in a 17-year period, with the majority (53.33%, n=24) published in the last six years (2018-present). As evidenced in Figure 3, the first instrument developed to measure celiac QOL, the CDQ, was developed in 2006 (17) and set an important precedent for researchers in the field, since then, it became evident that the assessment of celiac QOL should be performed using tools designed to the celiac population specificities.
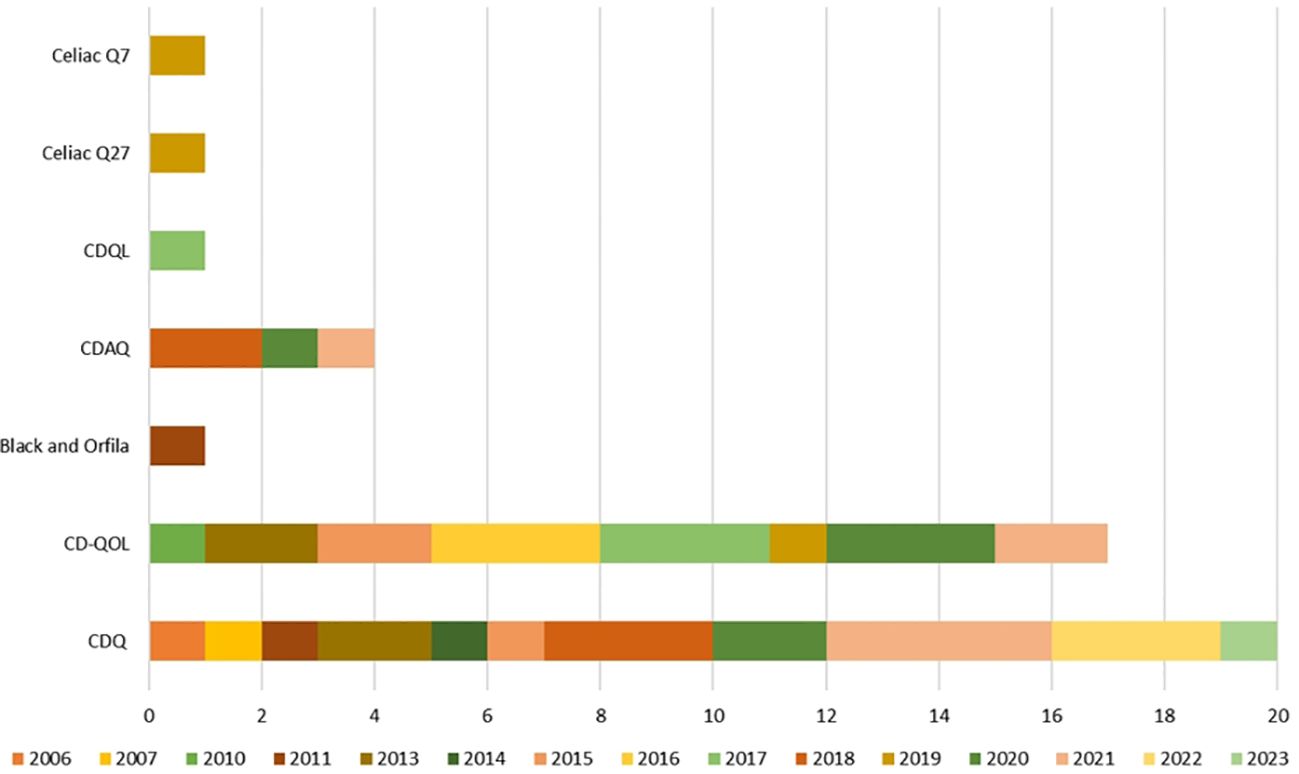
Figure 3 Use of specific questionnaires to measure celiac patients’ quality of life throughout time.
Among the studies that applied validated methods and questionnaires for analyzing QOL of CD patients, following instruments were identified: (i) Celiac Disease Questionnaire (CDQ) (n=21) (ii) Celiac Disease Specific Quality of Life Questionnaire (CD-QoL) (n=17); (iii) Celiac Q27 (n=1); (iv) Celiac Q7(n=1); (v) Coeliac Disease Assessment Questionnaire (CDAQ) (n=4); and (vi) Celiac Disease Quality of Life Questionnaire (CDQL) (n=1). It is imperative to emphasize the importance of cultural adaptation when using validated instruments like the ones mentioned in this review in different sociocultural backgrounds since the experiences and challenges faced by individuals with celiac disease can vary across different countries and cultural backgrounds. Studies carried out without cultural adaptation may fail to accurately capture the unique factors influencing the quality of life for celiac patients in the countries´ specific contexts.
Concerning the domains in the included instruments, a total of fifteen domains were observed when all instruments were analyzed together Clique ou toque aqui para inserir o texto (14, 17, 21, 27, 32, 34, 52). Figure 4 graphically represents the domains of the seven instruments included, it also represents intersections between domains with similar nomenclatures/subjects in different questionnaires.
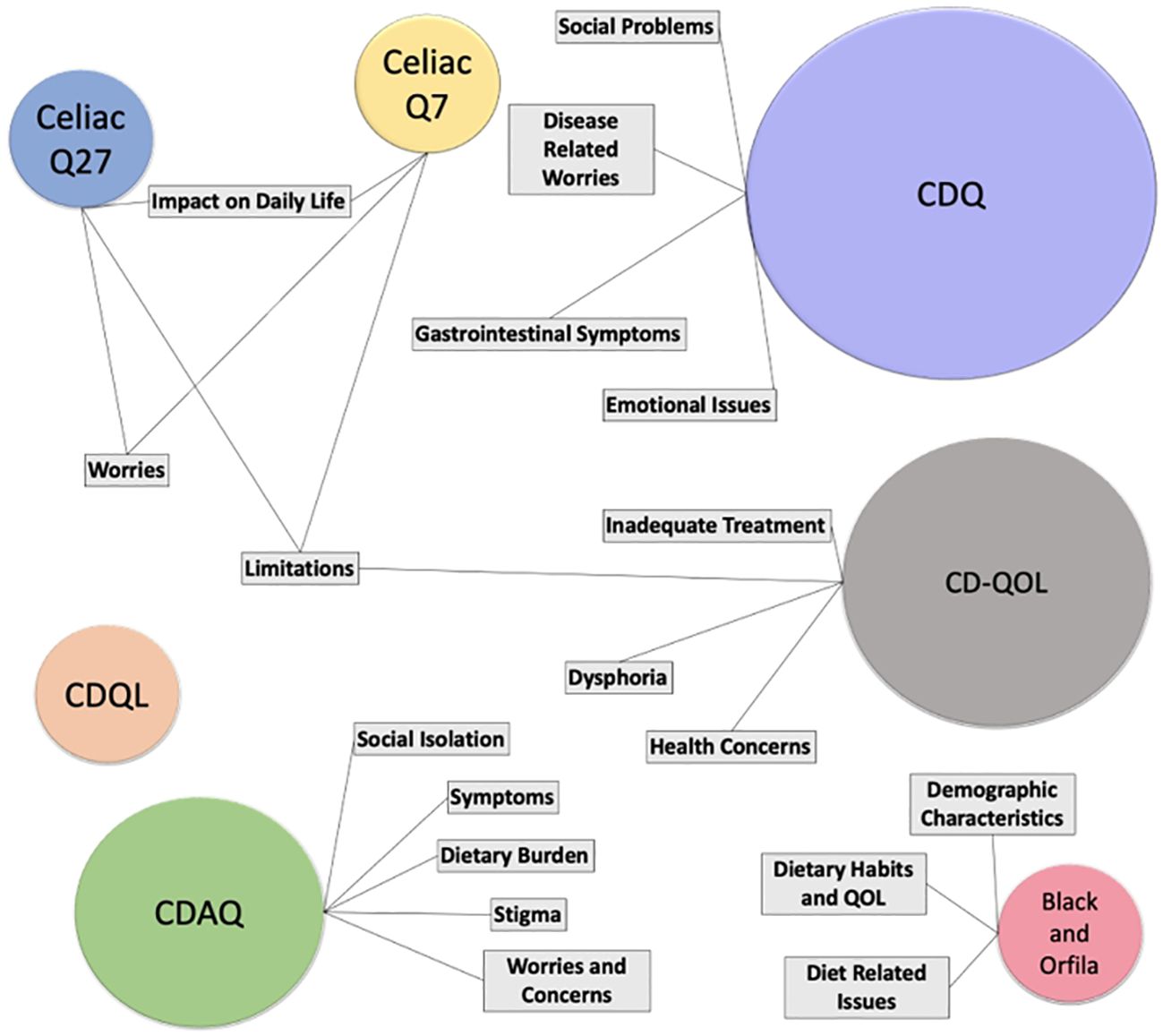
Figure 4 Graphical representation of the present domains in the included instruments and their respective intersections. Most utilized instruments are represented with proportional bigger circles.
It is important to note that similar denominations of the domains present in different questionnaires can evaluate different constructs depending on the questionnaire. Also, domains with different nomenclatures evaluate similar constructs.
As displayed in Figure 2, the countries that have executed more research on the topic are Spain, followed by the UK, Italy, and the USA. It can be inferred that developed countries tend to have more preoccupation regarding health-related quality of life (HRQOL), more access to CD diagnoses and deal with less misdirection from CD diagnosis due to infectious diseases, which represents a struggle to control acute gastrointestinal cases, and the fact that there used to be a misconceived association of CD with populations exclusively of Caucasian origin (54, 55). This may explain the range of countries where studies regarding the quality of life of celiac patients were conducted.
In addition, it is essential to emphasize the importance of investigating celiacs´ health dimensions in nations that have not yet done so, even though CD has been reported in them, such as India and Russia, both of which rank among the world’s ten most populous countries, along with several others (54, 56). The recent increase in studies reflects a growing awareness about how celiac disease impacts patients’ quality of life. This heightened focus may stem from either an escalating prevalence of CD over time or an increased recognition of its importance as a global public health issue in the past two decades (54, 55).
The CDQ was designed in Germany in 2007 through the prism of patients, experts in the CD field and scientific literature to evaluate celiac individuals’ HRQOL, being a pioneer in the subject (17, 18). It is a quantitative 10-minute self-administered questionnaire composed of four subscales: emotional issues, social problems, disease-related worries, and gastrointestinal symptoms. Each subscale has seven sub-items each, resulting in a total of 28 questions (18, 30).
The CDQ domains consider the patient´s feelings and perceptions concerning the challenges the disease and the GFD impose in their lives (29).The subcategories comprehend the dimensions of HRQOL, which are physical, emotional and social, and were related to domains of other disease-specific instruments like the Chronic Liver Disease Questionnaire (57) and the Inflammatory Bowel Disease Questionnaire (58).
The participants’ answers are evaluated using a 7-point Likert scale that varies in crescent punctuation, from always, most of the time, often, now and then, rarely, almost never, and never (18). The CDQ final evaluation score is a result of the addition of each question´s points, and therefore ranges from a total of 0 to 196 points; the score varies from 0 to 49 in all domains (18, 30). Lower scores indicate reduced HRQOL, hence higher values indicate high HRQOL (18). Although the CDQ score does not have a cut-off point, its development included a group of people who do not present CD-related disease as a comparison (18).
Throughout various studies conducted in different countries, the CDQ was used for measuring HRQOL in its original version, developed and validated in Germany (17), and has also been translated, culturally adapted, and validated to a diverse range of populations. The adapted versions were applied to populations in Italy (25, 26, 46), Portugal (28, 53), France (29, 51), Turkey, Brazil (21, 45), Poland (9), Iran (38), Argentina (43), Morocco (52), and Spain (50). Furthermore, the original CDQ was employed in studies conducted in Germany (17), Italy (23), Poland (9), Australia (40), Hungary (47), UK (8). Overall, the CDQ has been applied across 21 different studies (48.4%) spanning 15 countries, corresponding to 71,42% of the nations that investigated the thematic and are contemplated in this review.
In the original paper, the total score of QOL indicated that in Germany, people with CD presented lower QOL (143.1) than people without CD-associated disease (157.6), suggesting that celiac does negatively impact patients’ well-being (18). As the CDQ was developed for the German population, performing cultural adaptation as well as translation and validation of the tool to other countries is strongly recommended to minimize bias in QOL assessment and, consequently, data interpretation. In addition, since the original version of CQD is designed for on-paper applications, adapting to a web-based version is interesting for online applications.
The CD populations that presented the highest and lowest CDQ scores were Italian (159 score) (26) and Portuguese (103 score) (53). As the instrument has been applied only once in Portugal, it is not possible to compare the QOL scores over time. However, as the data was collected during COVID-19 pandemic, it could have negatively interfered with the score, especially over the social domain punctuation (53). However, as discussed by the Portuguese study, isolation can have a positive effect on GFD adherence, and it can be analyzed in Brazilian scores (53).
Brazil´s first assessment of celiac QOL was in 2018 and obtained a 119.79 (21) and the second CDQ application took place during COVID-19 and found a 125.26 score (45). Authors associate the improvement in celiac well-being in the pandemic period to the reduced social interactions involving gluten-containing food, which have negative repercussions in social and emotional domains, as well as the increase of home meal preparation that is a protective factor to GFD adherence, impacting positively in the emotional, social, worries and symptoms scales 383838.
Regarding the psychometric quality and quantitative parameters, the Cronbach’s alpha for the CDQ domains ranged from 0.80 to 0.91, as instruments are viable when Cronbach’s alpha is higher than 0.7 (18). All adaptations of the questionnaire presented over 0.7 values of Cronbach’s alpha. Therefore, the CDQ is a valid instrument to measure QOL of celiac patients that contemplates HRQOL dimensions.
The CD-QOL is a quantitative, self-administered questionnaire of 20 items distributed across four subscales: limitations, dysphoria, health concerns, and inadequate treatment (19). Researchers sought to capture in the instrument how patients perceive changes in their daily lives after diagnosis by consulting a celiac support group for input during the focus group stage (19). The answers to each item are allocated into a 5-point Likert Scale response, ranging from “not at all” to “a great deal”.
Each subscale is associated with factors that can negatively impact the QOL of individuals with CD. The first factor is called limitations and refers to the feeling of facing difficulties in belonging to or being part of routine events, such as eating with coworkers, not being able to eat conventional foods on important occasions (e.g., birthday cake) or struggling to take long trips due to CD and GFD (19). The second factor is dysphoria and is associated with a feeling of emotional dissatisfaction or discomfort due to the CD, the items in this category question if the participant feels depressed, frightened, or overwhelmed about having CD; it also inquires If the person believes not to have enough knowledge about CD (19). The third subscale, health concerns, is based on items of concern of increased risk of stigma due to the disease (19). The last category is inadequate treatment and it´s items inquire if patients feel like the GFD is sufficient treatment for CD (19).
It is noticeable that the CD-QOL approach focuses more on the individuals’ perceptions of external elements and challenges related to adhering to a gluten-free lifestyle rather than on gastrointestinal or extra gastrointestinal symptoms affecting the quality of life, from an urge to use the bathroom to sexual activities. The main difference between the CDQ and the CD-QOL instruments is that the first focuses on repercussions of the CD in physiological repercussions, psychological symptoms, and impact in daily activities (e.g., work, leisure, etc.); whereas the second targets attitudes and perceptions of the celiac population in routine events such as socializing. The CD-QOL does not include any item to measure the physical impact of CD since the individuals in its population, which included American celiac support group members, did not emphasize symptoms as a struggle, which could be a characteristic of the USA population or public policies. That highlights the need to perform a cultural adaptation and validation of the questionnaire when assessing the QOL of people with CD. The questionnaire was applied in 17 papers (39,53%) of 9 countries and applied in 8 nations (38.09% of all countries included in this review).
The original version of CD-QOL was utilized in the USA (19, 31, 33, 34), Canada (35), Brazil (5). Cultural adaptation and validation were conducted in Italy (25), Spain (20, 27, 32, 41, 42, 59), and Iran (49); the CD-QOL was also adapted to the Netherlands (39), but it was not applied to the population, it was used to develop new questionnaires. The Spanish version of the instrument (27) was applied to the Spanish-speaking countries of Paraguay (60) and Chile (48); however, it was not adapted to South American specificities. It´s possible to suggest that all four subscales of the CD-QOL are susceptible to changes due to regional influences in the exposome and public policies such as regulations for specialized health service support to people with CD, therefore the cultural adaptation is recommended even for countries with same mother language (55).
The CeliacQ-27 and CeliacQ-7 aim to evaluate CD HRQOL. It was developed and validated in Dutch, considering the cross-cultural adaptation of the CD-QOL to the Netherlands (19, 39). These questionnaires offer a unique approach by comparing different phases of CD, including active/clinical remission periods as well as instances where individuals may deviate from their gluten-free diet.
The CeliacQ-27 consists of 27 questions categorized into three domains: limitations (11 items), worries (10 items), and impact on daily life (6 items) (39). The limitations domain is related to patients’ perceptions of daily life restrictions because of the CD or GFD. The worries domain questions about mental and general challenges associated with CD (39). The third domain, impact on daily life, comprises questions about the social influences of the CD and GFD (39). Higher scores in de CeliacQ27 equal better QOL. The internal consistency of the questionnaire domains ranged from Chronbach´s α of 0.87 and 0.92, demonstrating good to excellent reliability (39).
Its shorter version contained only seven questions (CeliacQ-7) and was created by excluding all items with loads <0.70 Chronbach´s α in the Dutch version of the CD-QOL (39). The final version obtained a 0.88 Chronbach´s α and a high correlation with the CeliacQ-27 (39).
Since the CeliacQ-27 and the CeliacQ-7 are both derived from the Danish version of the CD-QOL, the two do not include questions to assess the repercussions of the physical symptoms associated with CD in patients’ well-being (39). However, introducing a condensed questionnaire could increase participation rates in surveys and be an interesting tool for ambulatory assistance and follow-ups, especially for patients who have been following a GFD.
The Coeliac Disease Assessment Questionnaire (CDAQ) was developed in two stages in 2018 (36, 37). The premise for developing this instrument was that the questionnaires available at the time were constructed without considering patient-reported outcome measures (PROM), which consider patients’ point of view, not necessarily measured by biological markers or associated with clinical outcomes (61).
In the first phase of development, qualitative interviews were conducted and analyzed through a data framework, which revealed six common themes reported by the participants: symptoms, gluten-free diet, emotional health, impact on activities, relationships, and financial issues (36). In the first phase, 64 items were present in the instrument (36). The subsequent phase was centered on the item reduction of the first version of the instrument; in this sense, items were refined through item appraisal, expert review, cognitive interviews and translatability assessment (37).
The resultant instrument comprises 32 items in five domains: stigma, dietary burden, symptoms, social isolation and worries, and concerns (37). Concerning its psychometric quality and quantitative parameters, this instrument presented Cronbach’s alpha between 0.82 and 0.88 for all domains. These values demonstrate the viability of the instrument, since an instrument of this type is considered viable when its Cronbach’s alpha is higher than 0.7 (62). Another highlight regarding CDAQ’s quantitative parameters is related to its strong intraclass correlation (0.86) with SF-36’s domains, the Short Form Health Survey developed by the World Health Organization (WHO) (37).
Regarding its application, the questionnaire is structured on a five-point Likert scale (never, rarely, sometimes, often and always), which is later converted into a scale of 0-100, with 100 being the highest quality of life (QOL) (37). Two studies (4.65%) included in this review used this instrument, one being the pilot study developed by Crocker et al. (2018) (36) in the United Kingdom and another carried out through a telephone survey in the same region in 2020 (44).
In a study of 276 people (166; 61.9% women and 110; 38.1% men), the results revealed an average quality of life score of 53.6 on the instrument´s proposed 0-100 scale (37). Significant differences (p <0.05) were found between the two groups, with male participants showing a higher overall quality of life (60.91) compared to women (49.18). However, potential reasons for this difference were not explored by the authors (37).
The other study that used the CDAQ as an instrument to assess the QOL with CD evaluated the effectiveness of telephone monitoring in improving the QOL of this population, evaluating, in addition to the quality of life, adherence to a GFD (44). The results demonstrated that although the intervention was effective in improving adherence to the gluten-free diet, quality of life parameters did not differ significantly between the treated and control groups, with emphasis on assessments in the “dietary burden” domain, which assesses the difficulty of diet be followed (44).
Based on its quantitative parameters, the CDAQ is an appropriate instrument for assessing the QOL in patients with CD. However, the low application of this questionnaire in studies outside the UK stands out, in addition to the fact that, to date, studies regarding the translation of this instrument into other languages have not been carried out. A possible hypothesis is that the instrument is relatively new (2018) compared to other instruments already developed and applied in different countries, such as the CDQ, which was developed in 2006 (15, 37).
The CDQL consists of a 44-item questionnaire developed in 2017 for CD patients of all ages and applied in one of the studies contemplated in this review (n=1, 2,32%) (11). It was designed in Ireland and Denmark and occurred in three phases: focus groups to collect celiacs’ insights and important aspects of QOL that should be in the final questionnaire; CD patients responded to the pilot version of the CDQL; refinement of the final version of the CDQL and application to Danish participants (11).
The final version of the instrument was web-based and estimated to take 5-10 minutes to complete (11). It included twelve items about background information, covering demographic characteristics and diagnosis data; two generic QOL questions; and 30 CD specific questions attributed to ten scales, the first two being general and followed by eight CD specific categories (11). The CDQL evaluates specific CD scales including: worries-about-symptoms (1 general item with thirteen alternatives); symptoms (1 general item with thirteen alternatives); contacting health care (3 items); having coeliac disease and following a gluten-free diet (7 items); communicating about coeliac disease and gluten-free diet (4 items); others´ handling my coeliac disease (3 items); confronting gluten-containing food (4 items); knowing about coeliac disease and gluten-free food (3 items); gluten-free food supply (3 items); evaluating having coeliac disease in overall (3 items) (11).
For scoring procedures, items are evaluated through a 5-point Likert scale, alternating among ´very unwell´, ´unwell´, ´neutral´, ´well´ or ´very well´. All response choices were followed by a smiley communicating the analogous emotion (11). The final score was calculated using the average score of each scale, higher results on the Likert scale indicate better QOL (11).
Though the CDQL was developed for children, adolescents and adults, the focus group step included only a few adults, which poses a limiting factor despite the items being formulated in a non-age-restricted way (11). On the other hand, this instrument presents the opportunity to evaluate patient reported HRQOL across different ages using a unique questionnaire (11). As far as we know, the CDQL has not been reapplied or translated/adapted culturally to any other country. Further studies are necessary to corroborate the pilot study results and their applicability to all age segments.
One of the studies included in this review (2.32%) aimed to analyze the quality of life of participants in an observational cohort conducted in 2011 with 146 CD patients who were members of the Coeliac UK Charity (24). However, in addition to the fact that this study did not use an instrument created and validated by other authors, it also included a food frequency questionnaire, seeking to relate the quality of life with the participants’ dietary habits (24).
In this sense, the authors developed a questionnaire composed of 32 questions, of which 10 are related to demographic variables, 10 to dietary habits (including availability of gluten-free foods and accidental ingestion of gluten due to cross-contamination) and 12 questions related to quality of life (24). It is important to highlight that although the questionnaire developed by the authors is not validated, such questions were derived from previously validated questionnaires, such as the Canadian Celiac Health Survey and the EPIC-norfolk food frequency questionnaire (63, 64).
It´s structured on a Likert scale, with five points: all of the time, most of the time, some of the time and never (24). Furthermore, the results were interpreted based only on the frequencies of answers on each point, with no corresponding scale to assess the quality of life (24).
As a main result, the cohort study demonstrated that CD impacts participants’ daily habits; however, most participants reported good physical health (24). Also, 97% of the participants reported good dietary compliance, with results supported by the food frequency questionnaire (24). Regarding the critical situations that affect the quality of life of these people, anxiety and depression related to social isolation resulting from dietary restriction and pain resulting from both intentional and unintentional gluten ingestion have been reported (24).
As the main limitation of this instrument, it is important to highlight that given the fact that it has not been validated or culturally adapted, the results from this study cannot be extrapolated to other populations with celiac disease. Also, no statistical assessment of the psychometric constructs of the items and sections was performed.
As presented in Figure 4, CD symptoms are explicitly described only in the domains of the CDQ (17) and CDAQ (37). However, while the CDQ domain related to symptoms only presents questions regarding bowel movements, diarrhea, gas, bloating and abdominal cramps, CDAQ includes symptoms related to mental health, such as tiredness, exhaustion, limitation of daily activities and general pain (36, 37).
Yet, issues regarding the same symptoms are also assessed in the instrument developed by Black and Orfila (24); however, under both domains of Dietary Habits and QOL and Diet-related issues. In the CDQ (17) instrument, such constructs are assessed under the “emotional issues” domain and in Celiac Q27 and Celiac Q7 in the Impact of Daily Life domain (39).
The “worries” domain is present in the CDQ (17), Celiac Q7 and Q27, CD-QOL (19) and CDAQ (36, 37) instruments. However, different scales relate to which spheres of life such worries refer. While in Celiac Q7 and 27 (39) such worries include conditions that relate to problems such as food availability outside the household, social interactions, and unpredictable bowel movements, in other questionnaires such as the CDAQ (36, 37), CDQ (17), and CD-QOL (19) such conditions are better stratified into other specific domains such as “Dietary Burden”, and “Social Problems”. In the CDAQ instrument, the concern regarding the availability of safe gluten-free food is measured in questions from the “dietary burden” domain (36, 37).
The domain entitled “Limitations” is found in the Celiac Q27 575757, Celiac Q7 (39) and CD-QOL (19) instruments. In both CeliacQ27 and Celiac Q7, questions assigned under this domain regard quotidian challenges present in patients’ lives, such as persistent symptoms, changes in the composition of foods previously labeled as “gluten-free” and situations regarding social acceptance while coexisting with celiac disease (39). In the context of CD-QOL (19), similar questions are present in the limitations´ domain, thus showing similarities between those three instruments.
However, questions regarding similar situations before addressed in the “Limitations” domain in CD-QOL (19), Celiac Q27 and Celiac Q7 (39) are also present in other instruments, for example, in “Dietary Related Issues” domain in the instrument created by Black and Orfila (24), “Disease related worries” (CDQ (17)) and “Social isolation” (CDAQ (36, 37),.
It is important to highlight that evaluating domains is challenging, given the semantic obstacles related to the proposed construct to be evaluated by different instruments (65). Furthermore, given the context that most instruments undergo translation and cultural validation, possible changes in the meaning of the constructs may occur (66, 67). Such differences make it difficult to compare the effectiveness of different instruments which, despite being individually statistically validated, may not be possible to be applied together given the differences between the literal meanings of the domains present (65–67).
The assessment of QOL in individuals with CD plays a crucial role in gaining insight into the well-being and impact of the disease. To effectively measure QoL, researchers have developed and validated various questionnaires that consider the unique experiences and management strategies associated with CD. Notably, two questionnaires stood out, the CDQ and the CD-QOL. Since the first focuses on the physical and mental symptoms related to the disease and the second focuses on the emotional repercussions of adhering to the GFD treatment for life (dysphoria), the CDQ application is an interesting option for countries that struggle with public policies for CD patients and patients with active CD; whereas the CD-QOL could be used for countries that have GF and CD regulations and populations in remission. When comparing results among different populations, it is preferable to utilize culturally validated instruments, which have been applied across multiple countries, providing greater comparability between study findings.
AF: Conceptualization, Formal Analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. BdL: Formal Analysis, Investigation, Visualization, Writing – original draft, Writing – review & editing. PF: Formal Analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. SF: Investigation, Visualization, Writing – review & editing. RR: Investigation, Visualization, Writing – review & editing. AR: Funding acquisition, Resources, Supervision, Writing – review & editing. ET-L: Funding acquisition, Writing – review & editing. CC: Funding acquisition, Writing – review & editing. RZ: Conceptualization, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was partially supported by FAPDF N° 539/2022 and the Brazilian National Council for Scientific and Technological Development (CNPq - N° 302602/2021-6). This work was also funded by National Funds through the FCT-Foundation for Science and Technology, I.P., within the scope of the projects Refa UIDB/05507/2020 and UIDB/00681/202.
The authors acknowledge the University of Brasília, Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Fundação de Apoio à Pesquisa do Distrito Federal (FAP-DF) and the Brazilian National Council for Scientific and Technological Development (CNPq) for their scientific support. This work was supported by the FCT—Foundation for Science and Technology, Portugal. Furthermore, we would like to thank the Centre for Studies in Education and Innovation (CI&DEI), Centre for Natural Resources, Environment and Society (CERNAS) and the Institute Polytechnic of Viseu for their support.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1396589/full#supplementary-material
1. Biagi F, Corazza GR. Mortality in celiac disease. Nat Rev Gastroenterol Hepatol. (2010) 7:158–62. doi: 10.1038/nrgastro.2010.2
2. Rodrigues M, Yonaminez GH, Satiro CA. Rate and determinants of non-adherence to a gluten-free diet and nutritional status assessment in children and adolescents with celiac disease in a tertiary Brazilian referral center: A cross-sectional and retrospective study. BMC Gastroenterol. (2018) 18:1–8. doi: 10.1186/s12876-018-0740-z
3. Queiroz MS, Nery M, Cançado EL, Gianella-Neto D, Liberman B. Prevalence of celiac disease in Brazilian children of short stature. Braz J Med Biol Res. (2004) 37:55–60. doi: 10.1590/S0100-879X2004000100008
4. Casellas F, Rodrigo L, López Vivancos J, Riestra S, Pantiga C, Baudet JS, et al. Factors that impact health-related quality of life in adults with celiac disease: A multicenter study. World J Gastroenterol. (2008) 14:46–52. doi: 10.3748/wjg.14.46
5. Castilhos AC, Gonçalves BC, Macedo e Silva M, Lanzoni LA, Metzger LR, Kotze LMS, et al. Quality of life evaluation in celiac patients from southern Brazil. Arq Gastroenterol. (2015) 52:171–5. doi: 10.1590/S0004-28032015000300003
6. Itzlinger A, Branchi F, Elli L, Schumann M, Itzlinger A, Branchi F, et al. Gluten-free diet in celiac disease—Forever and for all? Nutrients. (2018) 10:1796. doi: 10.3390/nu10111796
7. Aspasia S, Emmanuela-Kalliopi K, NikoLaos T, Eirini S, Ioannis S, Anastasia M. The gluten-free diet challenge in adults with coeliac disease: the hellenic survey. PEC Innovation. (2022) 1:1–5. doi: 10.1016/j.pecinn.2022.100037
8. Dimidi E, Kabir B, Singh J, Ageridou A, Foster C, Ciclitira P, et al. Predictors of adherence to a gluten-free diet in celiac disease: do knowledge, attitudes, experiences, symptoms, and quality of life play a role? Nutrition. (2021) 90:1–9. doi: 10.1016/j.nut.2021.111249
9. Zysk W, Głąbska D, Guzek D. Social and emotional fears and worries influencing the quality of life of female celiac disease patients following a gluten-free diet. Nutrients. (2018) 10:1414. doi: 10.3390/NU10101414
10. Fasano A, Catassi C. Current approaches to diagnosis and treatment of celiac disease: an evolving spectrum. Gastroenterology. (2001) 120:636–51. doi: 10.1053/gast.2001.22123
11. Skjerning H, Hourihane J, Husby S, DunnGalvin AA. Comprehensive questionnaire for the assessment of health-related quality of life in coeliac disease (CDQL). Qual Life Res. (2017) 26:2831–50. doi: 10.1007/s11136-017-1632-3
12. Farage P, Zandonadi RP, Austin J. Sci the gluten-free diet: difficulties celiac disease patients have to face daily. Austin J Nutri Food Sci. (2014) 2:1027–5.
14. Abreu Paiva LM, Gandolfi L, Pratesi R, Harumi Uenishi R, Puppin Zandonadi R, Nakano EY, et al. Measuring quality of life in parents or caregivers of children and adolescents with celiac disease: development and content validation of the questionnaire. Nutrients. (2019) 11:2302. doi: 10.3390/nu11102302
15. Häuser W, Stallmach A, Caspary WF, Stein J. Predictors of reduced health-related quality of life in adults with coeliac disease. Aliment Pharmacol Ther. (2007) 25:569–78. doi: 10.1111/j.1365-2036.2006.03227.x
16. Paarlahti P, Kurppa K, Ukkola A, Collin P, Huhtala H, Mäki M, et al. Predictors of persistent symptoms and reduced quality of life in treated coeliac disease patients: A large cross-sectional study. BMC Gastroenterol. (2013) 13:1–8. doi: 10.1186/1471-230X-13-75
17. Häuser W, Gold J, Stein J, Caspary WF, Stallmach A. Health-related quality of life in adult coeliac disease in Germany: results of a national survey. Eur J Gastroenterol Hepatol. (2006) 18:747–53. doi: 10.1097/01.meg.0000221855.19201.e8
18. Hauser W, Gold J, Stallmach A, Caspary WF, Stein J. Development and validation of the celiac disease quality of life measure for adult patients with celiac disease. Jornal Clin Gastroenterol. (2007) 41:157–66. doi: 10.1097/01.mcg.0000225516.05666.4e
19. Dorn SD, Hernandez L, Minaya MT, Morris CB, Hu Y, Leserman J, et al. The development and validation of a new coeliac disease quality of life survey (CD-QOL). Aliment Pharmacol Ther. (2010) 31:666–75. doi: 10.1111/j.1365-2036.2009.04220.x
20. Casellas F, Rodrigo L, Lucendo AJ, Fernández-Bañares F, Molina-Infante J, Vivas S, et al. Benefit on health-related quality of life of adherence to gluten-free diet in adult patients with celiac disease. Spanish J Gastroenterol. (2015) 107:196–201.
21. Pratesi CB, Häuser W, Uenishi RH, Selleski N, Nakano EY, Gandolfi L, et al. Quality of life of celiac patients in Brazil: questionnaire translation, cultural adaptation and validation. Nutrients. (2018) 10:1167. doi: 10.3390/nu10091167
22. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:1–9. doi: 10.1136/bmj.n71
23. Zampieron A, Daicampi C, Martin A, Buja A. Quality of life in adult celiac disease in a mountain area of northeast Italy. Gastroenterol Nurs. (2011) 34:313–9. doi: 10.1097/SGA.0b013e3182248a73
24. Black JL, Orfila C. Impact of coeliac disease on dietary habits and quality of life. J Hum Nutr Dietetics. (2011) 24:582–7. doi: 10.1111/j.1365-277X.2011.01170.x
25. Zingone F, Iavarone A, Tortora R, Imperatore N, Pellegrini L, Russo T, et al. The Italian translation of the celiac disease-specific quality of life scale in celiac patients on gluten free diet. Digestive Liver Dis. (2013) 45:115–8. doi: 10.1016/j.dld.2012.10.018
26. Marchese A, Klersy C, Biagi F, Balduzzi D, Bianchi PI, Trotta L, et al. Quality of life in coeliac patients: Italian validation of a coeliac questionnaire. Eur J Intern Med. (2013) 24:87–91. doi: 10.1016/j.ejim.2012.09.015
27. Casellas F, Rodrigo L, Molina-Infante J, Vivas S, Lucendo AJ, Rosinach M, et al. Transcultural adaptation and validation of the celiac disease quality of life transcultural adaptation and validation of the celiac disease quality of life (CD-QOL) survey, a specific questionnaire to measure quality of life in patients with celiac dis. Rev Espanõla Enfermedades Digestivas. (2013) 105:585–93. doi: 10.4321/S1130-01082013001000003
28. Lobão C, Gonçalves R, Baltazar RM. Desenvolvimento da versão portuguesa do celiac disease questionnaire. Rev Internacional Cienc Sociales. (2013) 2:1–8. doi: 10.37467/gka-revsocial.v2.1229
29. Pouchot J, Despujol C, Malamut G, Ecosse E, Coste J, Cellier C. Validation of a french version of the quality of life “Celiac disease questionnaire”. PloS One. (2014) 9:1–9. doi: 10.1371/journal.pone.0096346
30. Aksan AAA, Mercanligil SM, Häuser W, Karaismailo E, Mercanlıgil SM, Häuser W, et al. Validation of the turkish version of the celiac disease questionnaire (CDQ). Health Qual Life Outcomes. (2015) 13:1–7. doi: 10.1186/s12955-015-0272-y
31. Lee AR, Wolf R, Contento I, Verdeli H, Green PHR. Coeliac disease: the association between quality of life and social support network participation. J Hum Nutr Dietetics. (2016) 29:383–90. doi: 10.1111/jhn.12319
32. Rodríguez-Almagro J, Hernández-Martínez A, Lucendo AJ, Casellas F, Solano-Ruiz MC, Siles-González J, et al. Health-related quality of life and determinant factors in celiac disease. A population-based analysis of adult patients in Spain. Spanish J Gastroenterol. (2016) 108:181–189. doi: 10.17235/reed.2016.4094/2015
33. Mahadev S, Gardner R, Lewis SK, Lebwohl B, Green PH. Quality of life in screen-detected celiac disease patients in the United States. J Clin Gastroenterol. (2016) 50:393–7. doi: 10.1097/MCG.0000000000000433
34. Lee J, Clarke K. Effect of clinical and laboratory parameters on quality of life in celiac patients using celiac disease-specific quality of life scores. Scand J Gastroenterol. (2017) 52:1235–9. doi: 10.1080/00365521.2017.1350283
35. Dowd AJ, Jung ME. Self-compassion directly and indirectly predicts dietary adherence and quality of life among adults with celiac disease. Appetite. (2017) 113:293–300. doi: 10.1016/j.appet.2017.02.023
36. Crocker H, Jenkinson C, Peters M. Quality of life in coeliac disease: qualitative interviews to develop candidate items for the coeliac disease assessment questionnaire. Patient Relat Outcome Meas. (2018) 9:211–20. doi: 10.2147/prom.s149238
37. Crocker H, Jenkinson C, Peters M. Quality of life in coeliac disease: item reduction, scale development and psychometric evaluation of the coeliac disease assessment questionnaire (CDAQ). Aliment Pharmacol Ther. (2018) 48:852–62. doi: 10.1111/apt.14942
38. Barzegar F, Pourhoseingholi MA, Rostami-nejad M, Gholizadeh S, Malekpour MR, Sadeghi A, et al. Transcultural adaptation and validation of Persian version of celiac disease questionnaire (CDQ); A specific questionnaire to measure quality of life of Iranian patients. Galen Med J. (2018) e1106:1–7. doi: 10.22086/gmj.v0i0.1106
39. Burger JPW, Van Middendorp H, Drenth JPH, Wahab PJ, Evers AWM. How to best measure quality of life in coeliac disease? A validation and comparison of disease-specific and generic quality of life measures. Eur J Gastroenterol Hepatol. (2019) 31:941–7. doi: 10.1097/MEG.0000000000001432
40. Harnett JE, Myers SP. Quality of life in people with ongoing symptoms of coeliac disease despite adherence to a strict gluten-free diet. Sci Rep. (2020) 10:7–11. doi: 10.1038/s41598-020-58236-8
41. Fueyo-Díaz R, Montoro M, Magallóon-Botaya R, Gáscon-Santos S, Asensio-Martínez Á., Palacios-Navarro G, et al. Influence of compliance to diet and self-efficacy expectation on quality of life in patients with celiac disease in Spain. Nutrients. (2020) 12:1–15. doi: 10.3390/nu12092672
42. Casellas F, Argüelles F, Burgos R, van der Hofstadt Rovira M. National survey on the experiences of people with celiac disease in Spain. The CELIAC-SPAIN project. Rev Espanola Enfermedades Digestivas. (2020) 112:343–54. doi: 10.17235/reed.2020.6929/2020
43. Selleski N, Zandonadi RP, Milde LB, Gandolfi L, Pratesi R, Häuser W, et al. Evaluation of quality of life of adult patients with celiac disease in Argentina: from questionnaire validation to assessment. Int J Environ Res Public Health. (2020) 17:7051. doi: 10.3390/ijerph17197051
44. Muhammad H, Reeves S, Ishaq S, Mayberry JF, Jeanes YM. Telephone clinic improves gluten-free dietary adherence in adults with coeliac disease: sustained at 6 months. Frontline Gastroenterol. (2021) 12:586–92. doi: 10.1136/flgastro-2020-101643
45. Falcomer AL, Farage P, Pratesi CB, Pratesi R, Gandolfi L, Nakano EY, et al. Health-related quality of life and experiences of Brazilian celiac individuals over the course of the sars-cov-2 pandemic. Nutrients. (2021) 13:1582. doi: 10.3390/NU13051582
46. Schiepatti A, Maimaris S, De Queiros C, Archela M, Rusca G, Costa S, et al. Long-Term adherence to a gluten-Free diet and quality of life of celiac patients after transition to an adult referral center. Dig Dis Sci. (2021) 67:1–9. doi: 10.1007/s10620-021-07231-8
47. Szőcs H, Horváth Z, Vizin G. The mediating role of shame in the relationship between stigma and quality of life in patients with celiac disease. Orv Hetil. (2021) 162:1968–76. doi: 10.1556/650.2021.32258
48. Parada A, Méndez C, Espino A, Reyes Á., Santibáñez H. Adherence to a gluten-free diet and quality of life in Chilean celiac patients. Rev Espanola Enfermedades Digestivas. (2021) 113:429–31. doi: 10.17235/reed.2020.7293/2020
49. Nikniaz Z, Asghari Jafarabadi M, Ghaffarifar S, Ravand Z, Akbari Namvar Z, Shirmohammadi M. The persian translation and validation of the celiac disease quality of life questionnaire (CDQOL). Health Qual Life Outcomes. (2021) 19:1–7. doi: 10.1186/s12955-021-01694-z
50. de Lourdes Moreno M, Sánchez-Muñoz D, Sousa C. Quality of life in teenagers and adults with coeliac disease: from newly Spanish coeliac disease questionnaire validation to assessment in a population-based study. Front Nutr. (2022) 9:887573. doi: 10.3389/fnut.2022.887573
51. Enaud R, Tetard C, Dupuis R, Laharie D, Lamireau T, Zerbib F, et al. Compliance with gluten free diet is associated with better quality of life in celiac disease. Nutrients. (2022) 14:1–10. doi: 10.3390/nu14061210
52. Guennouni M, Admou B, Elkhoudri N, Bouchrit S, Ait Rami A, Bourrahouat A, et al. Quality of life of moroccan patients with celiac disease: arabic translation, cross-cultural adaptation, and validation of the celiac disease questionnaire. Arab J Gastroenterol. (2022) 23:246–52. doi: 10.1016/J.AJG.2022.06.009
53. Chaves C, Raposo A, Zandonadi RP, Nakano EY, Ramos F, Teixeira-Lemos E. Quality of life perception among Portuguese celiac patients: A cross-sectional study using the celiac disease questionnaire (CDQ). Nutrients. (2023) 15:1–12. doi: 10.3390/nu15092051
54. Singh P, Arora A, Strand TA, Leffler DA, Catassi C, Green PH, et al. Global prevalence of celiac disease: systematic review and meta-analysis. Clin Gastroenterol Hepatol. (2018) 16:823–36. doi: 10.1016/j.cgh.2017.06.037
55. Falcomer AL, Luchine BA, Gadelha HR, Szelmenczi JR, Nakano EY, Farage P, et al. Worldwide public policies for celiac disease: are patients well assisted? No prelo. (2020) 65:937–45. doi: 10.1007/s00038-020-01451-x
56. Catassi C, Gatti S, Lionetti E. World perspective and celiac disease epidemiology. Digestive Dis. (2015) 33:141–6. doi: 10.1159/000369518
57. Jacoby A, Rannard A, Buck D, Bhala N, Newton JL, James OFW, et al. Development, validation, and evaluation of the PBC-40, a disease specific health related quality of life measure for primary biliary cirrhosis. Gut. (2005) 54:1622–9. doi: 10.1136/gut.2005.065862
58. Guyatt G, Mitchell A, Irvine EJ, Singer J, Williams N, Goodacre R, et al. New measure of health status for clinical trials in inflammatory bowel disease. Gastroenterology. (1989) 96:804–10. doi: 10.1016/S0016-5085(89)80080-0
59. Fueyo-díaz R, Magallón-botaya R, Gascón-santos S, Palacios-navarro G, Sebastián-domingo JJ, Fueyo-d R, et al. The effect of self-efficacy expectations in the adherence to a gluten free diet in celiac disease. Psychol Health. (2019) 0:1–16. doi: 10.1080/08870446.2019.1675658
60. Real-Delor RE, Centurión-Medina IC. Quality of life in Paraguayan adults with celiac disease. Duazary: Rev Internacional Cienc la Salud. (2018) 15:61–70. doi: 10.21676/2389783X.2026
61. Makhni EC, Meadows M, Hamamoto JT, Higgins JD, Romeo AA, Verma NN. Patient reported outcomes measurement information system (PROMIS) in the upper extremity: the future of outcomes reporting? J Shoulder Elbow Surg. (2017) 26:352–7. doi: 10.1016/J.JSE.2016.09.054
62. Pesudovs K, Burr JM, Harley C, Elliott DB. The development, assessment, and selection of questionnaires. Optometry Vision Sci. (2007) 84:663–74. doi: 10.1097/OPX.0B013E318141FE75
63. Welch AA, Luben R, Khaw KT, Bingham SA. The CAFE computer program for nutritional analysis of the EPIC-norfolk food frequency questionnaire and identification of extreme nutrient values. J Hum Nutr Diet. (2005) 18:99–116. doi: 10.1111/j.1365-277X.2005.00593.x
64. Cranney A, Zarkadas M, Graham ID, Butzner JD, Rashid M, Warren R, et al. The Canadian celiac health survey. Dig Dis Sci. (2007) 52:1087–95. doi: 10.1007/S10620-006-9258-2
65. Dean DL, Hender JM, Rodgers TL, Santanen EL. Identifying quality, novel, and creative ideas: constructs and scales for idea evaluation 1. J Assoc Inf Syst. (2006) 7:646. doi: 10.17705/1jais
66. Yu DSF, Lee DTF, Woo J. Issues and challenges of instrument translation. Western J Nursing Res. (2004) 26:307–20. doi: 10.1177/0193945903260554
Keywords: Celiac disease, gluten-free, quality of life, questionnaire, systematic review
Citation: Falcomer AL, de Lima BR, Farage P, Fabris S, Ritter R, Raposo A, Teixeira-Lemos E, Chaves C and Zandonadi RP (2024) Enhancing life with celiac disease: unveiling effective tools for assessing health-related quality of life. Front. Immunol. 15:1396589. doi: 10.3389/fimmu.2024.1396589
Received: 05 March 2024; Accepted: 15 April 2024;
Published: 29 April 2024.
Edited by:
Ángela Ruiz-Carnicer, Sevilla University, SpainReviewed by:
Ezequiel Pinto, University of Algarve, PortugalCopyright © 2024 Falcomer, de Lima, Farage, Fabris, Ritter, Raposo, Teixeira-Lemos, Chaves and Zandonadi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Luísa Falcomer, YW5hLmZhbGNvbWVyQGFsdW5vLnVuYi5icg==; António Raposo, YW50b25pby5yYXBvc29AdWx1c29mb25hLnB0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.