 Paula Muñiz1,2
Paula Muñiz1,2 María Martínez-García2,3
María Martínez-García2,3 Rebeca Bailén1,2María Chicano1,2Gillen Oarbeascoa1,2
Rebeca Bailén1,2María Chicano1,2Gillen Oarbeascoa1,2 Juan Carlos Triviño4
Juan Carlos Triviño4 Ismael de la Iglesia-San Sebastian1,2
Ismael de la Iglesia-San Sebastian1,2 Sara Fernández de Córdoba1,2Javier Anguita1,2
Sara Fernández de Córdoba1,2Javier Anguita1,2 Mi Kwon1,2José Luis Díez-Martín1,2,5Pablo M. Olmos2,3
Mi Kwon1,2José Luis Díez-Martín1,2,5Pablo M. Olmos2,3 Carolina Martínez-Laperche1,2*†
Carolina Martínez-Laperche1,2*† Ismael Buño1,2,6,7*†
Ismael Buño1,2,6,7*†- 1Department of Hematology, Gregorio Marañón General University Hospital, Madrid, Spain
- 2Signal Theory and Communications Department, School of Engineering, Carlos III University, Leganés, Madrid, Spain
- 3Department of Signal Theory and Communications, University Carlos III of Madrid, Madrid, Spain
- 4Bioinformatic Department, Sistemas Genómicos, Valencia, Spain
- 5Department of Medicine, School of Medicine, Complutense University of Madrid, Madrid, Spain
- 6Genomics Unit, Gregorio Marañón General University Hospital, IiSGM, Madrid, Spain
- 7Department of Cell Biology, School of Medicine, Complutense University of Madrid, Madrid, Spain
Backgrounds: Although allogeneic hematopoietic stem cell transplantation (allo-HSCT) is a potentially curative therapy for hematological malignancies, it can be associated with relevant post-transplant complications. Several reports have shown that polymorphisms in immune system genes are correlated with the development of post-transplant complications. Within this context, this work focuses on identifying novel polymorphisms in cytokine genes and developing predictive models to anticipate the risk of developing graft-versus-host disease (GVHD), transplantation-related mortality (TRM), relapse and overall survival (OS).
Methods: Our group developed a 132-cytokine gene panel which was tested in 90 patients who underwent an HLA-identical sibling-donor allo-HSCT. Bayesian logistic regression (BLR) models were used to select the most relevant variables. Based on the cut-off points selected for each model, patients were classified as being at high or low-risk for each of the post-transplant complications (aGVHD II-IV, aGVHD III-IV, cGVHD, mod-sev cGVHD, TRM, relapse and OS).
Results: A total of 737 polymorphisms were selected from the custom panel genes. Of these, 41 polymorphisms were included in the predictive models in 30 cytokine genes were selected (17 interleukins and 13 chemokines). Of these polymorphisms, 5 (12.2%) were located in coding regions, and 36 (87.8%) in non-coding regions. All models had a statistical significance of p<0.0001.
Conclusion: Overall, genomic polymorphisms in cytokine genes make it possible to anticipate the development all complications studied following allo-HSCT and, consequently, to optimize the clinical management of patients.
1 Introduction
Although allogeneic hematopoietic stem-cell transplantation (allo-HSCT) is a curative therapeutic approach for patients with hematologic malignancies, procedure-related morbidity and mortality may increase in the months or years following the procedure. In addition to the risk of malignancy relapse (30–40%), multiple factors such as drug-induced organ toxicity, infections and graft-versus-host disease (GVHD) compromise the full curative potential of allo-HSCT. Despite complications and mortality associated with transplantation have decreased in recent years, transplantation-related mortality (TRM) continues to be a major barrier to allo-HSCT. Several studies have found that 60–80% of TRM occurs within 100 days of transplantation. The increased use of reduced-intensity conditioning regimens and improvements in supportive care have reduced TRM.
Donor T cells promote hematopoietic engraftment, reconstitute T-cell immunity and mediate a potent beneficial antitumor effect known as graft-versus-leukemia (GVL) (1). Unfortunately, donor T cells also cause GVHD. GVHD occurs when the donor T cells within the graft identify the patient’s (host) healthy cells from various tissues as foreign, and attack and damage them (2). GVHD remains one of the major causes of morbidity following allo-HSCT, leading to prolonged use of immunosuppressive agents, organ dysfunction, increased risk of infection, and ultimately increased mortality (3). The manifestations and severity of GVHD are highly variable and are influenced by the proportions of naive cells maturing along regulatory T-cell, Th1, Th2, or Th17 phenotypes. This maturation is largely influenced by local cytokines, which, in turn, activate transcription factors and drive development toward a dominant phenotype. In addition, proinflammatory cytokines exert direct effects on GVHD target tissues. Genetic differences in non-HLA genes between recipients and donors are important, and the role of polymorphisms in cytokines and other immune related genes must be taken into account (4).
Although there are several studies that associate the presence of polymorphisms in cytokine genes with the development of different complications, no single nucleotide polymorphism (SNP) genotyping in non-HLA genes is currently used for decision making in routine clinical practice. Many of these polymorphisms have been associated with GVHD or other complications (5, 6), however, the identification of a unique polymorphism of a single gene does not have the sensitivity and specificity required for a reliable prediction of these post-transplant complications. The ideal approach would then be the combined use of several of them, along with clinical variables, to construct a predictive model. Predictive models are designed to anticipate a response variable and have become useful tools in improving the diagnostic and prognostic use of biomarkers. In this context, in recent years several groups have developed different predictive models, including clinical and genetic variables. Kim et al. built a risk model incorporating polymorphisms and clinical markers, which allowed for improved risk stratification for acute GVHD (aGVHD), TRM, overall survival (OS) and relapse-free survival (7, 8). Paczesny et al. developed a protein panel of four cytokines measured in plasma for the diagnosis of aGVHD, and another panel for patient stratification based on the risk of chronic GVHD (cGVHD) (9). Our group developed several clinical-genetic predictive models for GVHD applying a complex estimation method, the least absolute shrinkage and selection operator (LASSO) procedure (10).
In order to further gain knowledge on new genetic variants not previously described and improve our previously published predictive models, we designed a 132-gene next generation sequencing (NGS) panel (including coding and non-coding regions) to identify new polymorphisms in genes related to the immune response, specifically cytokines, which may be associated with the development of post-transplant complications.
2 Materials and methods
2.1 Study design
We consecutively selected all patients who had received an HLA-identical sibling-donor allo-HSCT in our center between 2000 and 2015 and for whom we had DNA samples available for NGS analysis. GVHD prophylaxis included cyclosporine A and methotrexate for all patients.
Those patients who died or relapsed without having developed GVHD before day +100 for aGVHD (n=2) or day +180 for cGVHD (n=28) were censored. Those patients who died due to causes not related to transplant toxicity were also censored (n=20), and in our analysis of relapse, patients who died during the first year after transplantation, without having relapsed, were also excluded (n=13).
Clinical variables considered were donor and recipient sex, donor and recipient age, underlying disease, stem-cell source, conditioning regimen, prior radiation therapy and previous HSCT (Table 1).
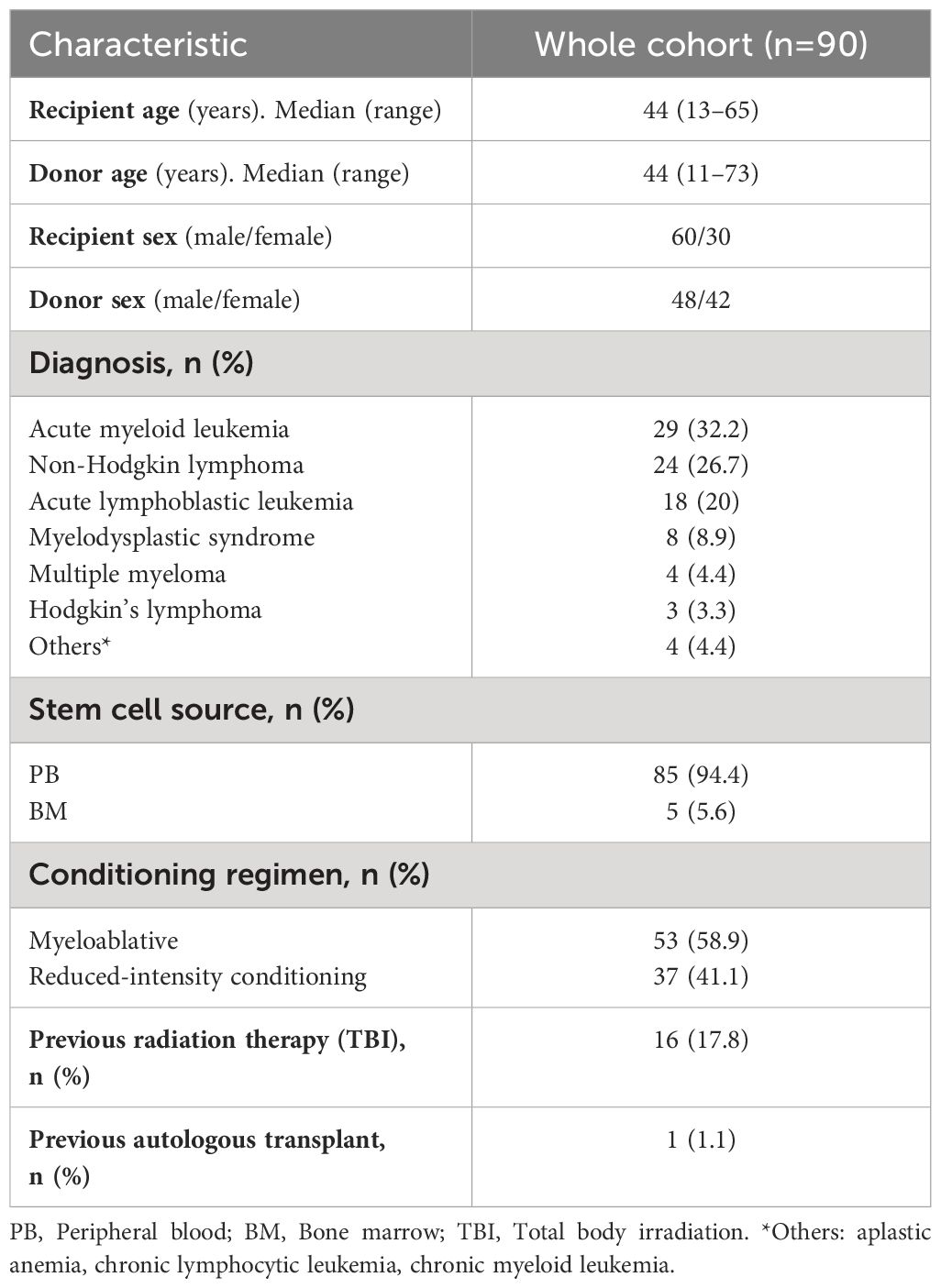
Table 1. Patient and donor characteristics.
The local ethics committee approved the study, and all recipients and donors provided written informed consent in accordance with the Declaration of Helsinki.
2.2 Posttransplant evaluation
Post-transplant complications analyzed were grade II-IV aGVHD, III-IV aGVHD, cGVHD, moderate-severe cGVHD, TRM, relapse and OS.
GVHD classification and clinical data collection were performed at the moment of GVHD diagnosis by the attending physician following the 1994 Consensus Conference on aGVHD grading and the National Institutes of Health criteria for diagnosis and staging of cGVHD.
In the case of TRM, we have considered TRM every death that occurs while the patient is in remission, any death not attributable to relapse.
2.3 Genotyping
Pre-transplant samples were selected, mostly peripheral blood. The selected samples were in complete remission as the objective was to identify germline variants (polymorphism). Subsequently, genomic DNA was purified automatically (Maxwell® 16 Blood DNA Purification Kit; Promega, Madison, Wisconsin) following manufacturer instructions. The DNA extracted was frozen at -80°C in our biobank (ISCIII N°C.0000915).
We designed a custom panel of 132 cytokine genes that included 73 interleukin and 59 chemokine genes (Supplementary Table 1). The probes were designed to detect coding and non-coding regions, namely untranslated regions (UTR), splicing (± 1,2 base pairs), and upstream and downstream regions (± 200 base pairs).
Libraries were prepared using a capture gene panel according to the manufacturer’s protocol (Agilent, Santa Clara, California). Paired-end sequencing (2×101 bp) was performed using the Illumina HiSeq platform (Illumina, San Diego, California). FASTQ files were aligned against the human reference genome (GRCh38/hg38 version) using the Burrows Wheeler Alignment tool v0.7.15-r1140. Variant calling and indel-realignment were performed using a combination of two different algorithms: GATK and VarScan. GeneSystems software (Sistemas Genómicos, Valencia, Spain) was used for variant annotation in order to provide the infrastructure and interface for bioinformatic analysis. Identified variants were annotated using the Ensembl database, population databases (the Exome Aggregation Consortium and 1000 Genomes), and specific variant databases (ClinVar, Catalogue of Somatic Mutations in Cancer (COSMIC). The population bases GenomAD and 1000 Genomes were used to determine population frequency (Minor Allele Frequency, MAF).
All polymorphisms located in coding sequences, splicing (± 1,2 base pairs), UTR and upstream and downstream regions (± 200 base pairs) were analyzed. Non-synonymous variants with ≥30X depth in the canonical isoform, a variant allele frequency (VAF) greater than 40%, a MAF ≥1% and representing at least 5% of our cohort were selected. From the total number of polymorphisms (genetic variants) analyzed, we selected those in which the presence of the minor variant (allele) is associated with the development of a complication.
2.4 Statistical analysis
Given the high dimensionality of the data and the limited sample size, conventional methods were not flexible enough to find discriminative features. To address this, we proposed Bayesian probabilistic methods to manage uncertainty while performing dimensionality reduction.
Data analysis consisted of two main steps: feature selection and classification or prediction. To address the first step, we developed a novel probabilistic variant of the Logistic Regressor, incorporating L1 regularization, referred to as the Bayesian Logistic Regression (BLR) model. The proposed BLR model follows a Variational Autoencoder (VAE) approach, in which the weight vector is approximated through a multivariate Gaussian distribution. Additional details of the BLR model and VAE approach can be found in the Supplementary Material.
In the classification step, we wanted to account for the potential non-linear relationships between the selected input variables and the complications. As the BLR is limited in its ability to capture non-linear relationships, it was only utilized for the feature selection stage. As an alternative, a probabilistic non-parametric kernel model, specifically a Gaussian Process (GP) classifier, was used to generate predictions. Additional details can be found in the Supplementary Material.
2.5 Predictive models
Taking into account the number of variables, BLR models were used to select the most important variables involved in each complication. Initially, the 15 most relevant genetic/clinical variables were selected. The strategy implemented was to select those predictive models that obtained the highest area under the curve (AUC), i.e. the greatest predictive power, with the lowest number of variables (Supplementary Table 3). Depending on the presence of the variables selected for each model, a score was calculated for each patient. Subsequently, taking into account sensitivity, specificity, false positives, and false negatives (in both cases setting the limit at 15%), the best cutoff point was selected for the subsequent stratification of patients into high or low risk according to the model selected for each post-transplant complication (Supplementary Table 4).
The selected variants were represented in Tables 2–8, in these tables display the following characteristics:
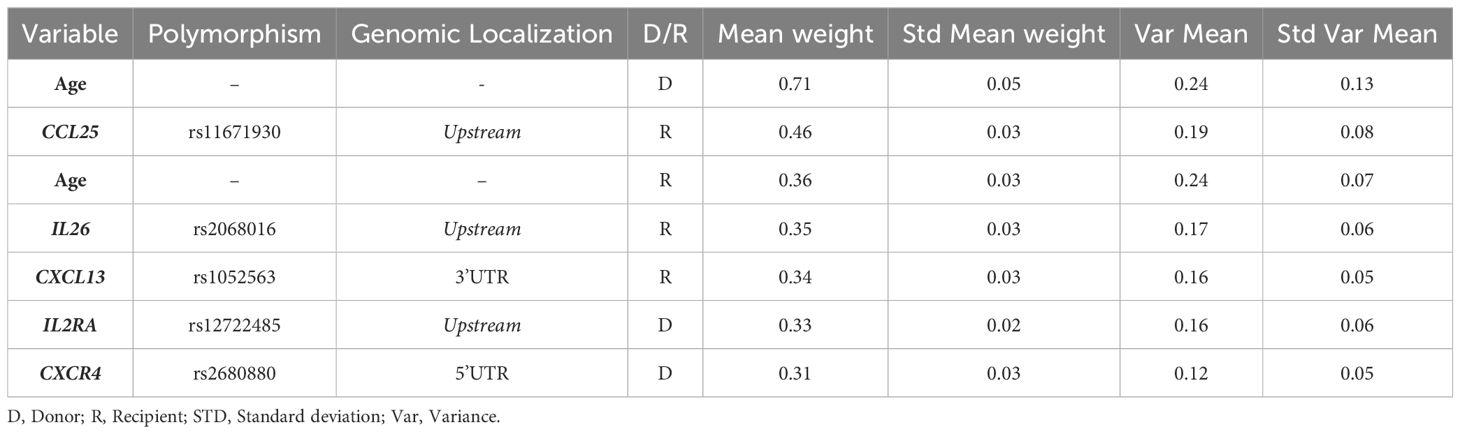
Table 2. Genetic risk score for aGVHD II-IV.
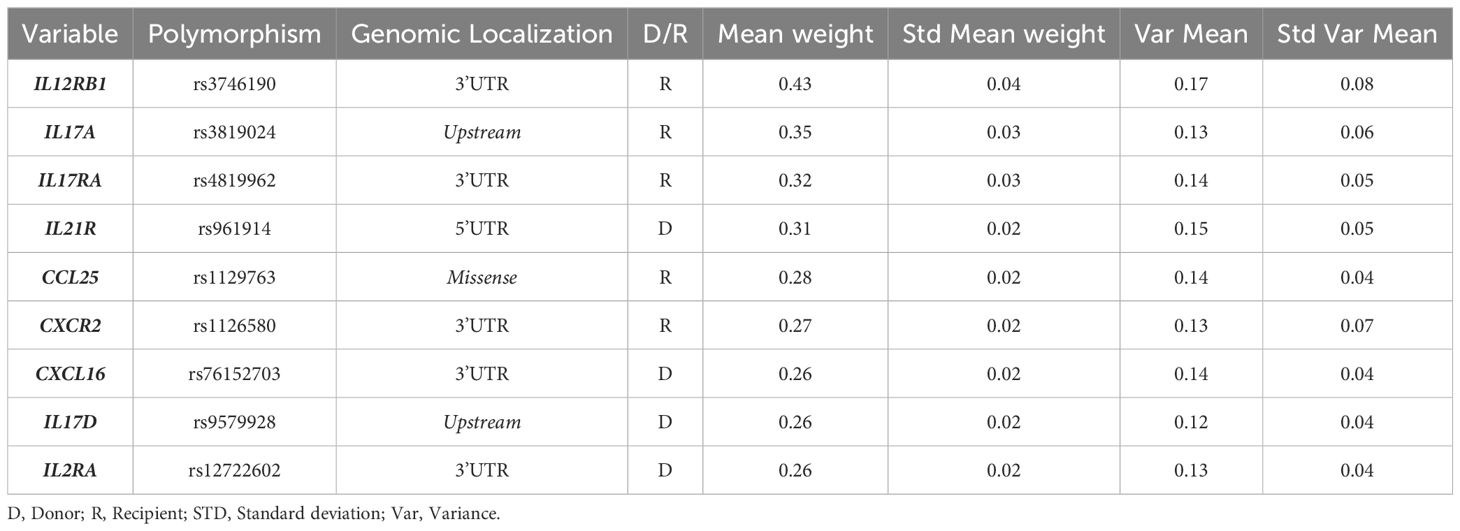
Table 3. Genetic risk score for aGVHD III-IV.

Table 4. Genetic risk score for cGVHD.
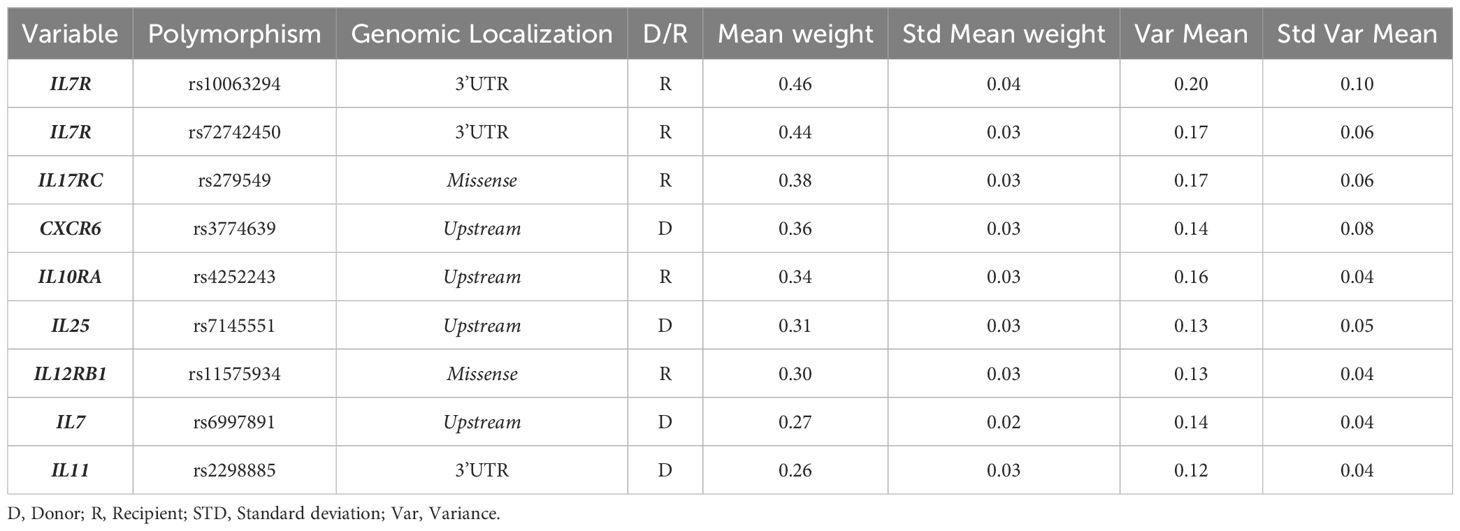
Table 5. Genetic risk score for moderate-severe cGVHD.
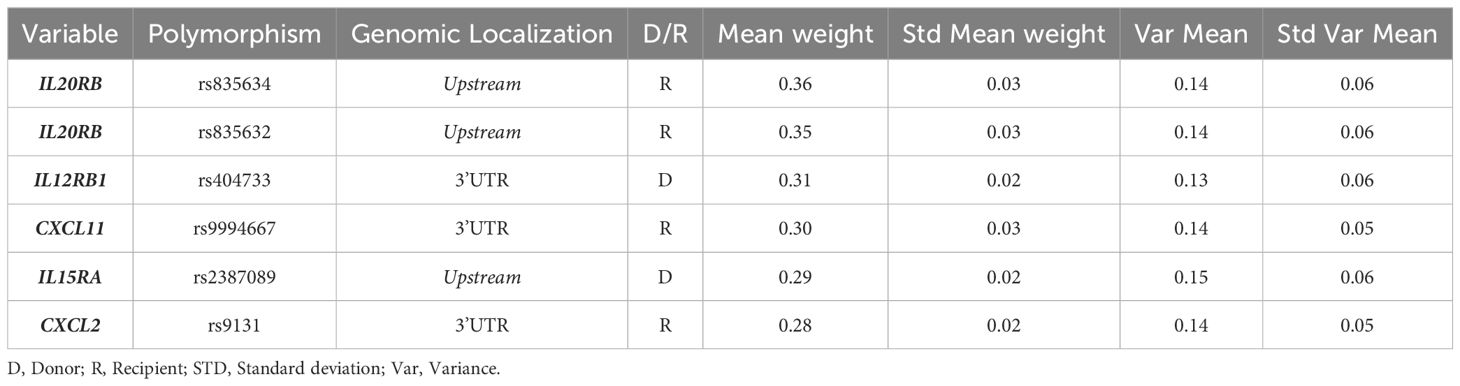
Table 6. Genetic risk score for TRM.
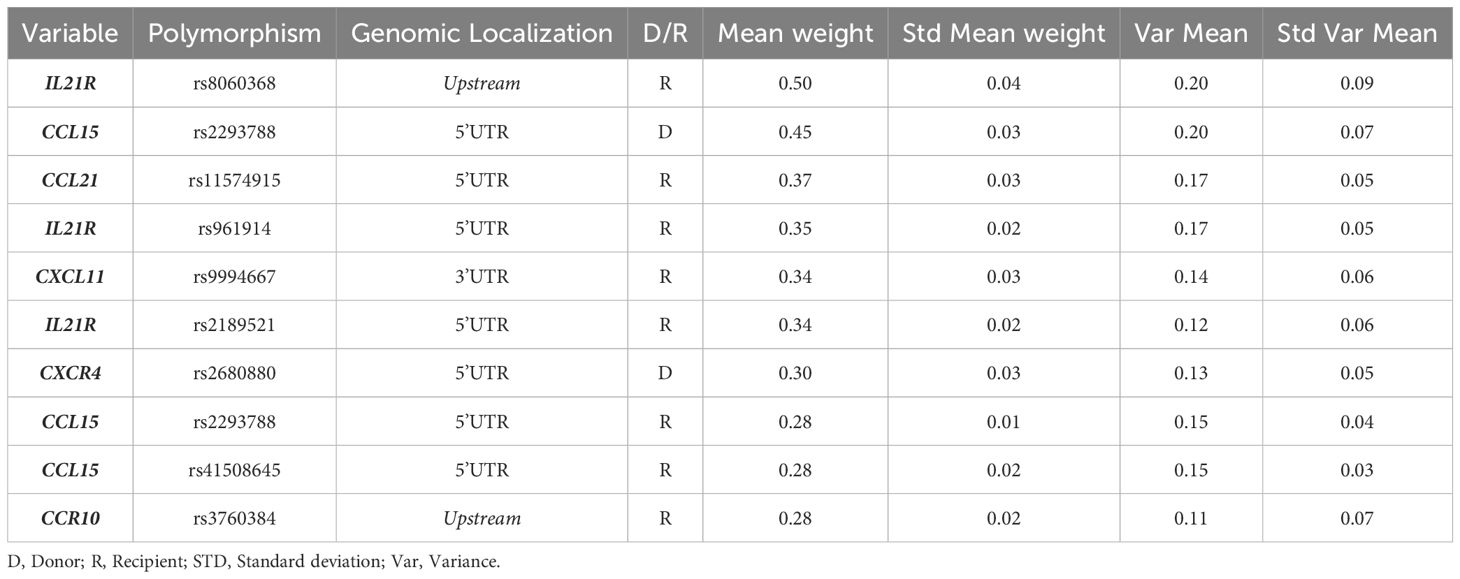
Table 7. Genetic risk score for relapse.
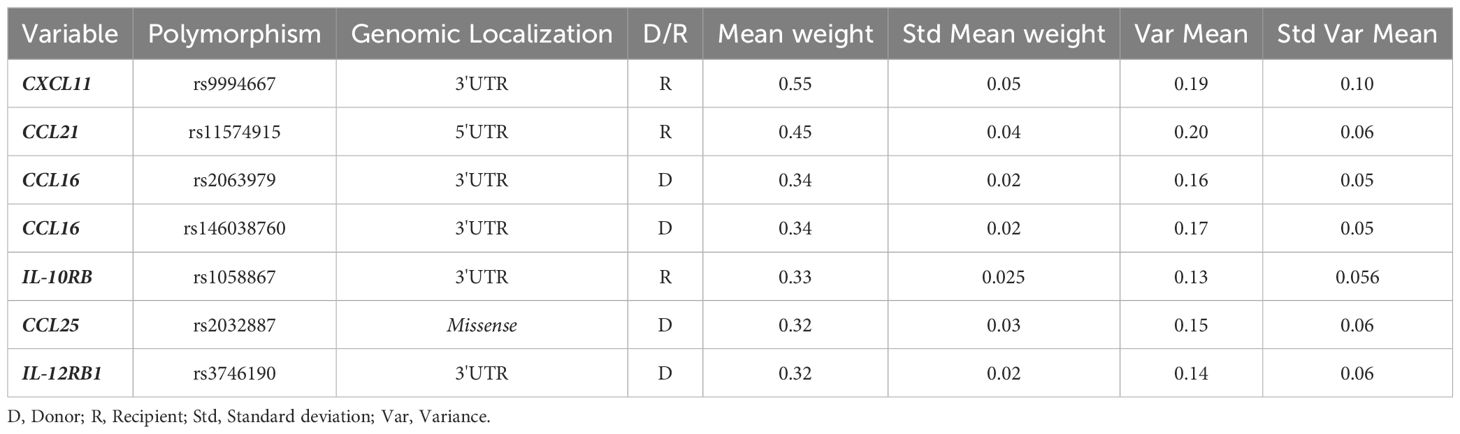
Table 8. Genetic risk score for OS.
Mean weight: Mean over partitions of the inferred mean in absolute value.
Std Mean weight: Standard deviation over partitions of the inferred mean.
Var Mean: Mean over partitions of the inferred variance.
Std Var Mean: Standard deviation over partitions of the inferred variance.
2.6 Functional analysis of the genes included in the selected predictive models
An enrichment analysis of the genes included in the models ultimately selected was conducted using the Enrichr web-based software application in order to establish common functions and establish a functional relationship between them.
3 Results
3.1 Clinical data
Of the global cohort, 51/88 (58%) of patients presented grade II-IV and 27/88 (30.6%) III-IV aGVHD. Additionally, 39/63 (62%) and 25/61 (41%) developed cGVHD and moderate-severe GVHD respectively. Regarding TRM, 22/70 (31,4%) patients presented. Finally, 17/81 (23%) and 44/90 (49%) patients relapse or died respectively.
The cumulative incidence (CI) of grade II-IV and III-IV aGVHD at 100 days post-transplant was 56.7% and 23.3%, respectively. Cumulative incidence of cGVHD and moderate-severe cGVHD (mod-sev cGVHD) at three years post-transplant was 43.3% and 27.8%, respectively. Three-year CI for TRM was 24.4%, and 2-year OS was 60%.
The median times and the survival plot of each complication are shown in Supplementary Figure 1:
3.2 Variant data
Using the filters previously defined in Material and Methods, 737 polymorphisms in the 119 genes were detected in 90 donor-recipient pairs (Supplementary Table 2, Figure 1). Of these polymorphisms, 93 (12.6%) were located in coding regions, and 644 (87.4%) in non-coding regions: 3’ and 5’ UTR, splicing, upstream and downstream regions.
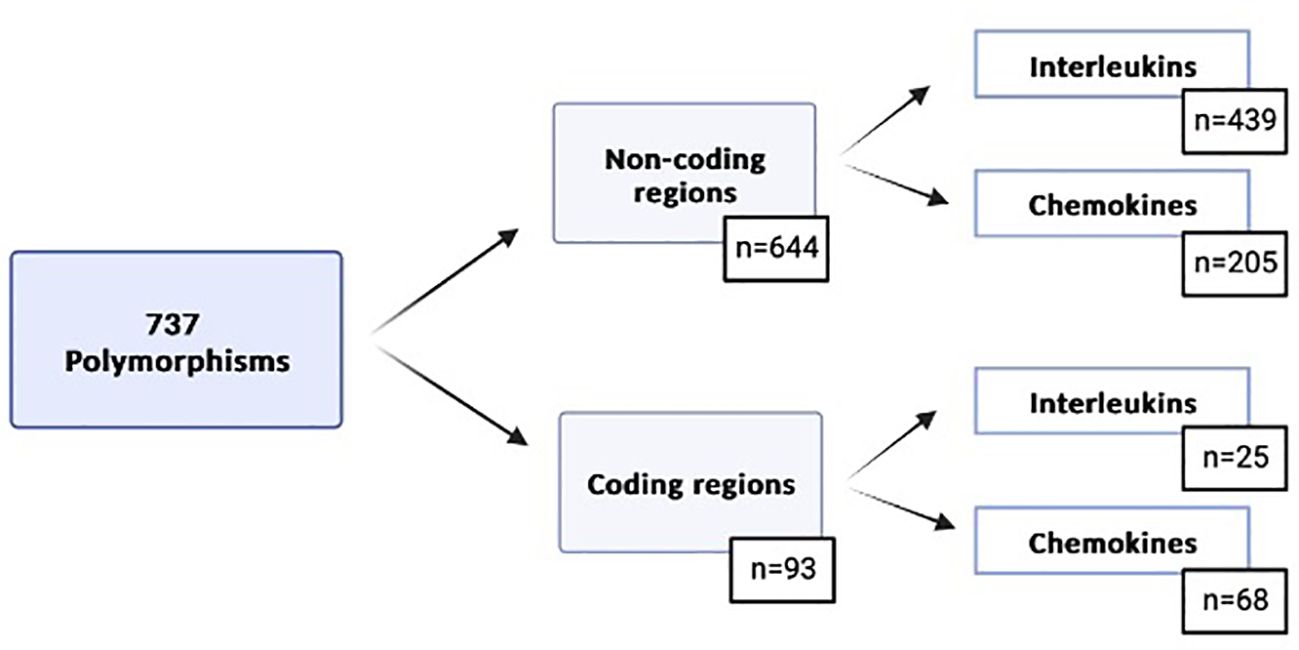
Figure 1. Genetic variables selected based on the previously defined filters.
3.3 Predictive models for post-transplant complications
Different predictive models, including clinical variables and 737 genetic variants, were built to anticipate the development of post-transplant complications such as GVHD, TRM, relapse and OS following allo-HSCT.
Initially, the 15 most relevant genetic/clinical variables were selected to reduce the dimensionality of the data (Supplementary Table 3). Of these initial 15 variables, the final variables for predictive models were selected taking into account the AUC and the number of variables. The models ultimately obtained for each of the post-transplant complications (aGVHD II-IV, aGVHD III-IV, cGVHD, mod-sev cGVHD, TRM, relapse and OS) are shown in Tables 2–8. Finally, 41 polymorphisms in 30 cytokine genes were selected (17 interleukins and 13 chemokines). Of these polymorphisms, 5 (12.2%) were located in coding regions, and 36 (87.8%) in non-coding regions.
Based on the sensitivity and specificity data, as well as the ratio of false positives and false negatives (a limit of 15% was established), cut-off points were selected to classify the patients at high or low-risk for the development of each post-transplant complication (Supplementary Table 4). Finally, the cumulative incidence of each complication according to patient risk stratification (Figure 2).
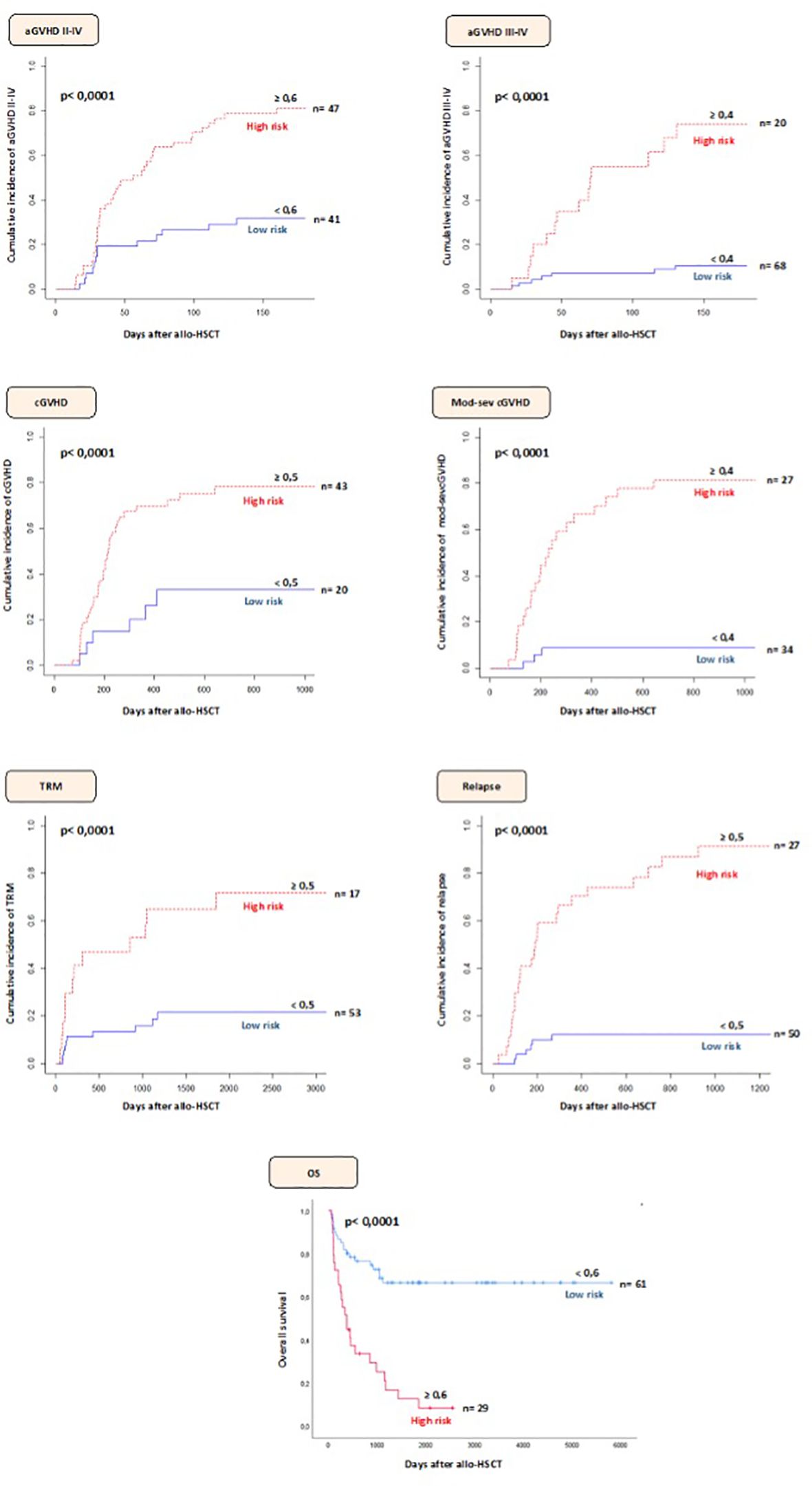
Figure 2. Stratification of patients at high/low-risk of developing complications after allo-HSCT according to the selected predictive model and cut-off point.
3.3.1 GVHD
3.3.1.1 aGVHD
3.3.1.1.1 Grade II-IV aGVHD
The predictive model selected consisted of seven variables in 5 genes (CCL25, IL-26, CXCL13, IL-2RA, CXCR4) (Table 2) and achieved AUC: 0.81, sensitivity: 74.77% and specificity: 73.53%. The only clinical variables selected were donor and recipient age. We calculated the II-IV aGVHD risk score for each patient to test the usefulness of the model in identifying patients at a high-riskof experiencing an II-IV aGVHD following allo-HSCT. At 180 days after allo-HSCT, 80.8% of patients with a high-risk score experienced II-IV aGVHD compared to 31.7% of those with a low-risk score (Figure 2).
3.3.1.1.2 Grade III-IV aGVHD
A model (with AUC: 0.81; sensitivity: 65.29% and specificity: 91.09%) consisting of nine genetic variables (IL-12RB1, IL-17A, IL-17RA, IL-12R, CCL25, CXCR2, CXCL16, IL-17D, IL-2RA) was selected (Table 3). According to this model, we observed that 70% of the patients classified as high-risk developed this complication while only 10.3% of patients classified as low-risk showed III-IV aGVHD at 180 days post-transplant (Figure 2).
3.3.1.2 cGVHD
3.3.1.2.1 cGVHD
The model developed (AUC: 0.73; sensitivity: 83.28% and specificity: 58.99%) consisted of four genetic variables (IL-2RA, IL-7R, XCR1, IL-3RA) (Table 4). Based on the selected model, 76.7% of the patients with a high-risk score developed cGVHD at two years post-transplant. However, 30% of patients classified as low-risk also developed cGVHD (Figure 2).
3.3.1.2.2 Moderate-severe cGVHD
Based on the number of variables and their associated weight, a genetic model (AUC: 0.88; sensitivity: 87.88% and specificity: 84.34%) composed of nine polymorphisms in 8 genes (IL-7R, IL-17RC, CXCR6, IL-10RA, IL-25, IL-12RB1, IL-7, IL-11) was selected (Table 5). We calculated the moderate-severe cGVHD risk score for each patient. Of the participants, 81.4% with a high-risk score experienced moderate-severe cGVHD compared to 14.8% of those with a low-risk score at two years after allo-HSCT (Figure 2).
3.3.2 TRM
The model selected for TRM (AUC: 0.74; sensitivity: 54.79% and specificity: 88.93%) was composed of six polymorphisms in 5 genes (IL-20RB, IL-12RB1, CXCL11, IL-15RA, CXCL2) (Table 6). Based on the stratification of patients into high or low-risk based on the cutoff point it was observed that the CI of TRM in patients classified as high-risk was 47.1% at two years post-transplant. In contrast, the CI of low-risk patients was 13.2% (Figure 2).
3.3.3 Relapse
This predictive model (AUC: 0.93; sensitivity: 79.06% and specificity: 90.61%) included ten polymorphisms in 6 genes (IL-21R, CCL15, CCL21, CXCL11, CXCR4, CCR10) (Table 7). Based on the selected model, 81.5% of high-risk patients had relapsed at two years post-transplant. In contrast, 12% of low-risk patients relapsed at two years after allo-HSCT (Figure 2).
3.3.4 Overall survival
Finally, seven genetic variables in 6 genes (CXCL11, CCL21, CCL16, IL-10RB, CCL25, IL-12RB1) were selected for this model (AUC: 0.78; sensitivity: 57.39% and specificity: 86.81%; Table 8). When the model selected was applied, it was observed that at five years post-transplant 17.3% of the patients classified as high-risk were still alive compared to 68.6% of the low-risk patients (Figure 2).
3.4 Enrichment analysis
Considering the genes included in the predictive models for post-transplant complications, 41 polymorphisms in 30 cytokines. Four signaling pathways functionally associated with the genes were obtained by enrichment analysis using web-based Enrichr software (Table 9) with a p-value of 2.5*10-56, 1.48*10-27, 4.04*10-18 and 4.97*10-9, respectively.
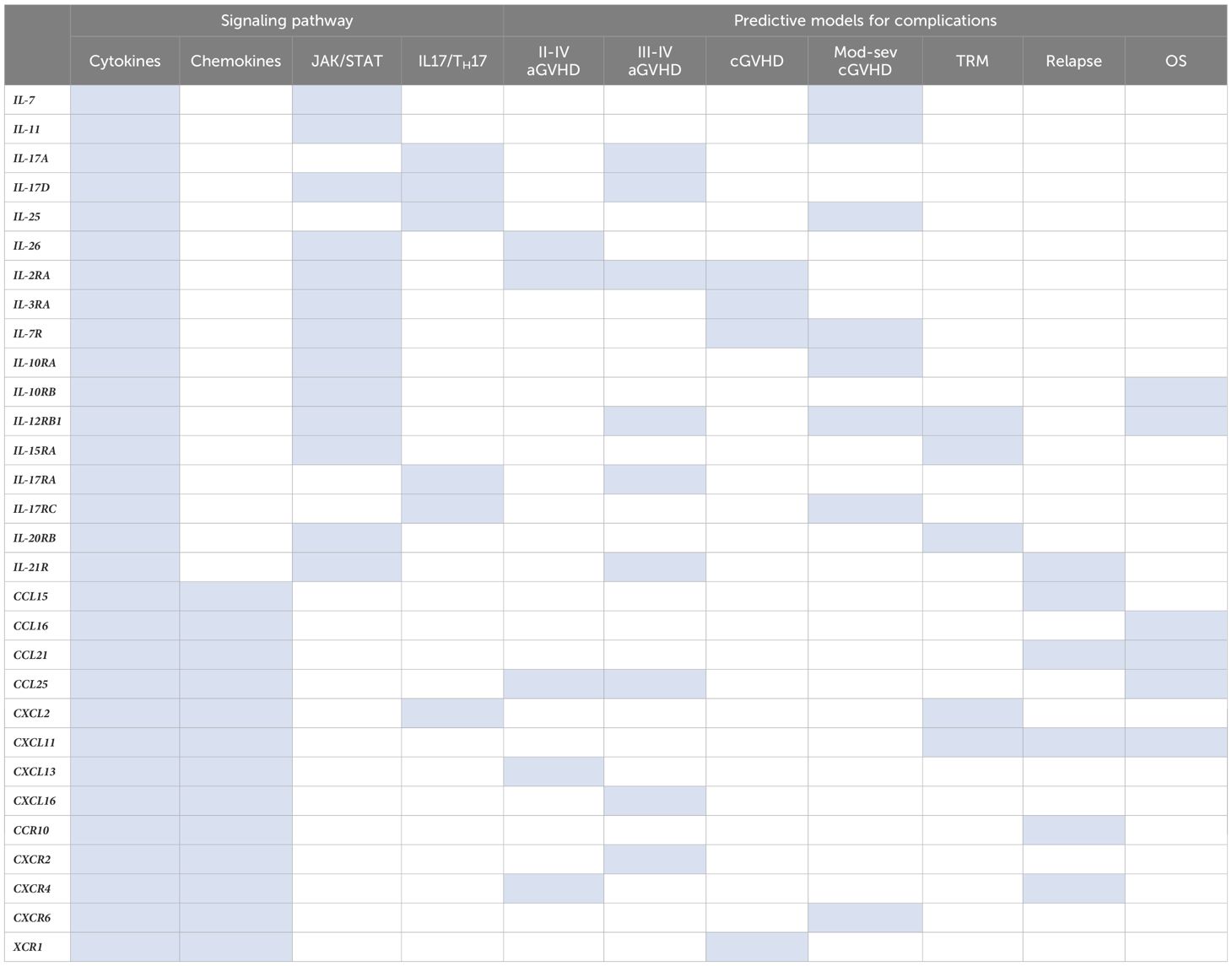
Table 9. Functional relationship between the genes selected for each post-transplant complication and the signaling pathway in which they participate as well as predictive models of the complications in which each gene has been selected.
All genes selected were included in the cytokine signaling pathway. Another signaling pathway selected by Enrichr was JAK/STAT, in which 13/30 cytokines, specifically interleukins (43.3%), were included. Finally, the IL-17/TH17 signaling pathway consisted of 6/30 cytokines (20%), including five interleukins and one chemokine.
4 Discussion
Allo-HSCT may be a successful curative treatment for hematological malignancies mainly due to GVL. Despite current knowledge on the pathophysiology of allo-HSCT, it continues to be a complex procedure in which a large number of patients experience related complications, including disease relapse, which represents the leading cause of treatment failure, and GVHD. Approximately 40% of patients develop GVHD; consequently, GVHD and associated infectious complications contribute to transplant-related morbidity and mortality (11).
There are several known risk factors that have an impact on the results of allo-HSCT, including HLA histocompatibility, the hematopoietic stem cell source, sex/age disparity between donor and recipient, conditioning regimen, underlying disease, etc. (12). However, the use of these clinical variables is not enough to accurately identify those patients who are at higher risk of developing post-transplant complications.
Recently, it has been shown that genetic variability (polymorphisms) in non-HLA genes also affects the outcome of allo-HSCT (13). In this context, there is evidence that polymorphisms in cytokine genes, which usually alter the expression or function of these proteins, impact the immune response that occurs in GVHD and could therefore be used as biomarkers to anticipate the risk of developing these complications (8, 9, 14–16). Therefore, it is important to build risk models in which several polymorphisms and clinical variables are included in order to anticipate these complications more accurately. In order to extend our knowledge to new genetic variants not previously described, we designed an NGS panel of 132 genes (including coding and non-coding sequences) to identify new polymorphisms in genes related to the immune response, specifically cytokines, which could be related to the development of post-transplant complications.
A total of 737 polymorphisms were selected from the custom panel genes. Of these, 41 polymorphisms were included in the predictive models, of which 87.8% were located in non-coding regions (UTR, upstream and downstream). It is interesting to note that most of the selected genetic variables had not been previously reported. Supplementary Table 5 provides a brief summary of the biological function of each of the selected genes, as described in the literature. Although it is not yet possible to specify the exact effect of the polymorphisms on the function of each gene, it is important to provide context for the function of each of these genes in the immune system.
Therefore, the non-coding regions could be of significant importance as these are usually related to increased or decreased protein expression. Although functional studies are not yet available, the selected variables could be related to increased expression of the proinflammatory protein, as occurs with many of the polymorphisms described, or decreased expression of an anti-inflammatory protein for which they encode and therefore influence the risk of developing different post-transplant complications.
4.1 GVHD models
GVHD models Interleukins related to the activation, proliferation and differentiation of immune system cells involved in the development of GVHD were included in acute and chronic GVHD models. In addition, different chemokines responsible for driving these cells to the sites of inflammation were included (Figure 3A). IL-12RB1 is a CD4+ T cell receptor that, depending on the binding of the IL-12 or IL-23 ligand, leads to a differentiation to a Th1 or Th17 phenotype (17), characteristic of aGVHD and cGVHD, respectively, that was selected for the aGVHD and cGVHD models. The IL-2RA receptor, which is responsible for the proliferation of T cells involved in GVHD and which in soluble form has been reported to be increased in stages of immune activation (18), was also included in these models. Specifically, the aGVHD model included interleukins such as IL-17A, IL-17RA and IL-26 related to the synthesis of proinflammatory cytokines (19, 20), which may be involved in the development of this complication. CCL25, although described in inflammatory diseases, is also associated with the proliferation of regulatory T cells (Tregs) that inhibit GVHD (21, 22). IL-21R has been reported as responsible for the proliferation and differentiation of lymphoid cells, but there are already studies that demonstrate that blocking IL-21/IL-21R in the gut increases Tregs, thereby inhibiting GVHD (23). Regarding cGVHD, it is worth noting that the chemokines selected in the predictive models have already been described in the literature as related to the development of GVHD. The interleukins IL-7/IL-7R, related to survival, proliferation and activity of T and B cells (24); as well as IL-25, which is related to TH2 activation but inhibits TH17 (25), T cells related to cGVHD, were also included (Figure 3B).
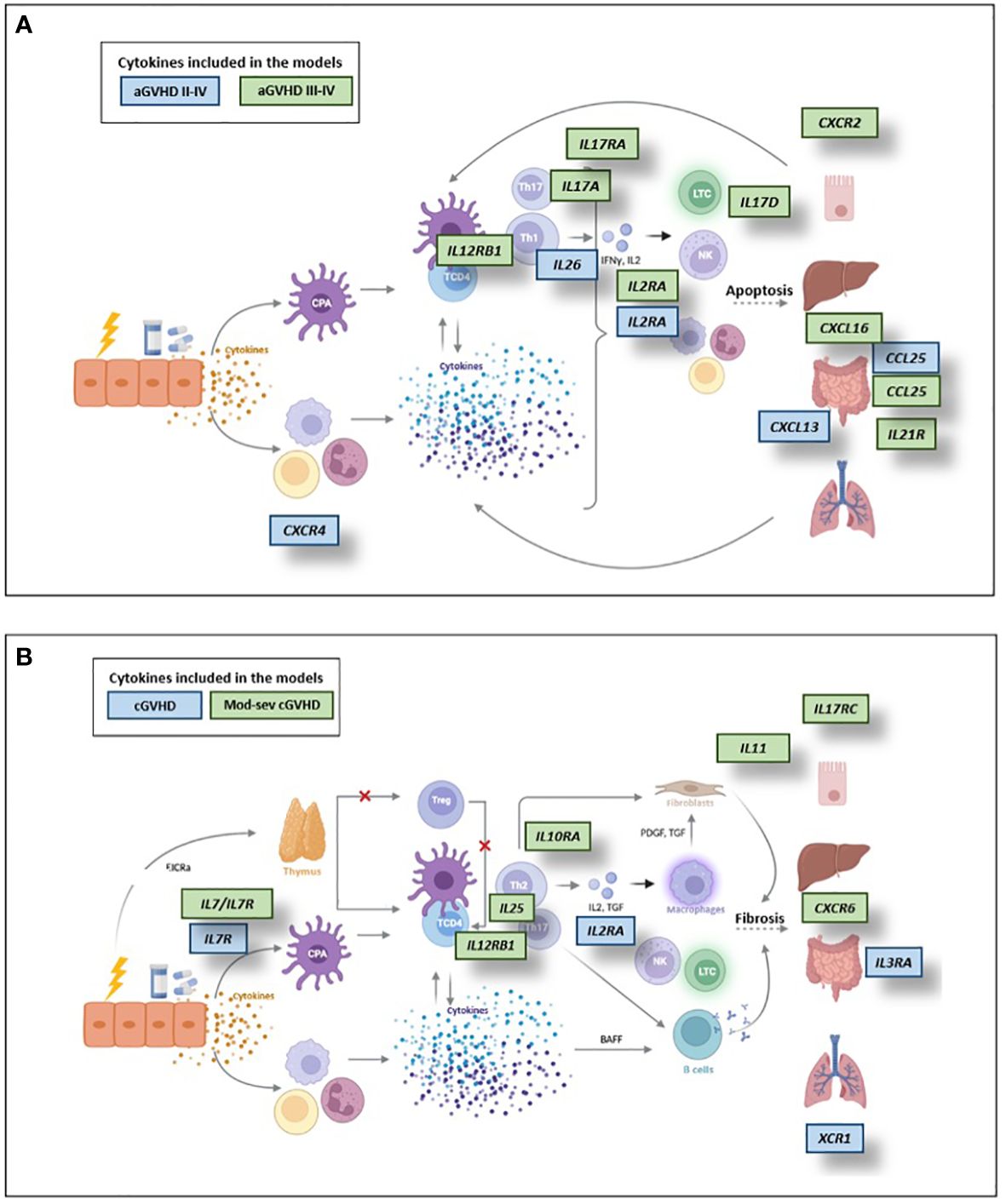
Figure 3. Cytokines included in the predictive models of aGVHD (A) and cGVHD (B). APC, Antigen-presenting cells; TCD4, CD4 T cells; BAFF, B-cell activating factor of the tumor necrosis factor family. Created with Biorender.com.
Notably, a greater number of genes were selected in the more severe GVHD models. This may be explained by the fact these could be expected to involve a more inflammatory context affecting various organs and thus producing a greater severity of GVHD. This is consistent with the selected models for severe GVHD obtained in a previous study (8).
Regarding the genetic model for TRM, all interleukins selected signaled through the JAK/STAT pathway, leading to the synthesis of proinflammatory cytokines. These cytokines could lead to an inflammatory environment that can affect TRM due to tissue damage. This is further enhanced by the chemokines selected for this model, which are related to the migration of immune system cells to inflammatory sites.
For the relapse model, three polymorphisms were selected in a single interleukin, IL-21R, which through its signaling leads to the proliferation and differentiation of lymphoid cells (26, 27). Thus, it could positively or negatively regulate immune responses. It worth noting that mainly chemokines were selected in this model (7/10). This could be explained as proposed in a study of pediatric patients diagnosed with acute lymphoblastic leukemia where the expression of chemokines and their receptors is increased in relapsed patients. In this study the authors propose that the cells secrete chemokines that recruit those leukocytes that express the specific receptor. Thus, tumor cells that secrete and/or respond to chemokines would have a selective advantage and may show resistance to chemokine therapy (28).
Finally, regarding the OS model, IL-10RB signaling exerts anti-inflammatory functions (29); hence we must identify the effect of the polymorphism selected on the expression of this gene. In turn, signaling of the other interleukin included, IL-12RB1, leads to the synthesis of IFN-γ, which may have an antitumor role in the activation of effector T cells, which will destroy tumor cells. However, it may also have a protumor role, involving proliferative and antiapoptotic signals (30). The chemokines selected are related to the migration and differentiation processes of different cells in the immune system. It is likely that these chemokines are able to recruit different types of immune cells in the tumor which, in turn, can modulate tumor growth and metastasis, as has been demonstrated in the literature (31).
An analysis of enrichment with the Enrichr application (32) found that in addition to the cytokine and chemokine signaling pathway, as expected, two signaling pathways represented in the inflammatory context were also selected: the IL17/TH17 and JAK/STAT signaling pathways. TH17 cells are CD4+ T cells that produce proinflammatory cytokines such as IL-17A, IL-17F, IL-21, IL-22, TNF-α, G-CSF and some chemokines. IL-17 is related to innate immunity and inflammation and relates T cell activation to neutrophil mobilization and activation (33). Several studies provide evidence of the role of IL-17 in GVHD, demonstrating that activated TH1 and TH17 lymphocytes secrete proinflammatory cytokines that lead to apoptosis of cells in target tissues in GVHD, primarily in the intestine, liver and skin (34, 35). The JAK/STAT signaling pathway regulates the activation of immune cells related to GVHD, including APCs, T cells, neutrophils and B cells (36, 37). It is therefore involved in regulating cell activation, proliferation, migration and cytokine production, increasing the severity of GVHD. In this context, drugs such as ruxolitinib that inhibit this signaling pathway are already available and used for the treatment of GVHD (38).
Based on the results obtained, it should be taken into account that most of the genetic variables selected for the predictive models of each of the post-transplant complications were located in non-coding regions, and that most of these polymorphisms identified for their clinical relevance (association with post-transplant complications) are not described in the literature. Therefore, it will be important in the future to conduct functional studies to determine whether these genetic variables produce changes in protein expression. In addition, these models should be validated with a larger sample size and in other HSCT regimens.
In conclusion, the incorporation of these predictive models in the management of transplanted patients may contribute to optimize the treatment and improve the outcomes of these patients in the context of a personalized precision medicine.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material. The datasets analyzed for this study can be found in the repositorio institucional de la consejería de sanidad de la comunidad de madrid: https://repositoriosaludmadrid.es//handle/20.500.12530/87923.
Ethics statement
The studies involving humans were approved by Drug Research Ethics Committee (CEIm) of Gregorio Marañón General University Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
PM: Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft. MM-G: Formal analysis, Methodology, Validation, Writing – review & editing. RB: Formal analysis, Methodology, Writing – review & editing. MC: Writing – review & editing. GO: Writing – review & editing. JT: Data curation, Methodology, Writing – review & editing. Id: Writing – review & editing. SF: Writing – review & editing. JA: Writing – review & editing. MK: Formal analysis, Writing – review & editing. JD-M: Funding acquisition, Writing – review & editing. PO: Writing – review & editing, Formal analysis, Methodology. CM-L: Formal analysis, Writing – review & editing, Conceptualization, Funding acquisition, Supervision, Writing – original draft. IB: Conceptualization, Formal analysis, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing, Investigation, Project administration, Resources, Validation, Visualization.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was partially supported by the Ministry of Economy and Competitiveness ISCIII-FIS Grants PI14/01731 and PI17/01880, PI20-00521, PID2021-123182OB-I00, and co-financed by the European Regional Development Fund from the European Commission, the “A way of making Europe” initiative, as well as grants from Asociación Madrileña de Hematología y Hemoterapia (AMHH) and Sociedad Española de Hematología y Hemoterapia (SEHH). The work by P. M. and M.M.G. has been supported by MCIN/AEI/10.13039/501100011033/FEDER, UE, under grant PID2021-123182OB-I00, and by Comunidad de Madrid under grants IND2022/TIC-23550 and ELLIS Unit Madrid. M.M.G was the recipient of pre-doctoral contract from Gregorio Marañón Health Research Institute (IiSGM) (2021-II-PREDOC-03).
Acknowledgments
The authors would also like to acknowledge the patients who participated in this study, as well as the staff of the Hematology Department, Gregorio Marañón General University Hospital (Madrid, Spain), who made the study possible.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1396284/full#supplementary-material
Supplementary Table 1 | Genes included in the designed NGS panel, corresponding to interleukins and chemokines.
Supplementary Table 2 | Genetic variables obtained after application of the filters described in the Patients and Methods section for the analysis of the designed NGS panel. Cr: Chromosome; Ref: Most frequent allele; Var: Minority variant allele; EUR MAF: Minority allele frequency in Europeans.
Supplementary Table 3 | AUC of the 15 most relevant variables included in the selected predictive models for post-transplant complications. D: Donor; R: Recipient; STD: standard deviation; GVHD: graft-versus-host disease; aGVHD: acute graft-versus-host disease; cGVHD: chronic graft-versus-host disease; mod-sev cGVHD: moderate-severe cGVHD; TRM: transplant-related mortality; OS: overall survival.
Supplementary Table 4 | Relationship of the characteristics of the different cut-off points for the stratification of patients for each of the post-transplant complications. aGVHD: acute graft-versus-host disease; cGVHD: chronic graft-versus-host disease; mod-sev cGVHD: moderate-severe cGVHD; TRM: transplant-related mortality; OS: overall survival; STD: standard deviation; S: sensitivity; E: specificity. The cut-off points selected for stratification of patients at high/low-risk of developing each complication according to the selected model are identified in bold.
Supplementary Table 5 | Function and polymorphisms associated with each post-transplant complication of the genes selected in the present study. GVHD: Graft-versus-host disease; aGVHD: acute graft-versus-host disease; cGVHD: chronic graft-versus-host disease; mod-sev cGVHD: moderate-severe cGVHD; TRM: Transplant-related mortality; OS: Overall survival; IL: Interleukin; TH: T-helper T lymphocyte. Proinflammatory cytokines are identified in yellow, and chemokines included in the GVHD models are identified in orange.
Abbreviations
aGVHD, Acute GVHD; Allo-HSCT, Allogeneic hematopoietic stem-cell transplantation; AUC, Area under the curve; BLR, Bayesian Logistic Regression; cGVHD, Chronic GVHD; CI, Cumulative incidence; GP, Gaussian Process; GVHD, Graft versus host disease; GVL, Graft versus leukemia; Mod-sev cGVHD, Moderate-severe cGVHD; OS, Overall survival; Treg, Regulatory T cells; TRM, Transplantation-related mortality; VAE, Variational Autoencoder.
References
1. Copelan EA. Hematopoietic stem-cell transplantation. N Engl J Med. (2006) 354:1813–26. doi: 10.1056/NEJMra052638
2. Ferrara JL, Levine JE, Reddy P, Holler E. Graft-versus-host disease. Lancet. (2009) 373:1550–61. doi: 10.1016/S0140-6736(09)60237-3
3. Horwitz ME, Sullivan KM. Chronic graft-versus-host disease. Blood Rev. (2006) 20:15–27. doi: 10.1016/j.blre.2005.01.007
4. Henden AS, Hill GR. Cytokines in graft-versus-host disease. J Immunol. (2015) 194:4604–12. doi: 10.4049/jimmunol.1500117
5. Dickinson AM, Charron D. Non-HLA immunogenetics in hematopoietic stem cell transplantation. Curr Opin Immunol. (2005) 17:517–25. doi: 10.1016/j.coi.2005.07.017
6. Gorbacheva R, Chukhlovin AB. Beyond HLA system: non-HLA gene alleles of donor origin may influence risk of immune allo-HSCT complications. CTT. (2017) 6:36–51. doi: 10.18620/ctt-1866-8836
7. Kim DD, Yun J, Won HH, Cheng L, Su J, Xu W, et al. Multiple single-nucleotide polymorphism-based risk model for clinical outcomes after allogeneic stem-cell transplantation, especially for acute graft-versus-host disease. Transplantation. (2012) 94(12):1250–7. doi: 10.1097/TP.0b013e3182708e7c
8. Kim D, Won HH, Su S, Cheng L, Xu W, Hamad N, et al. Risk stratification of organ-specific GVHD can be improved by single-nucleotide polymorphism-based risk models. Bone Marrow Transplant. (2014) 49(5):649–56. doi: 10.1038/bmt.2014.20
9. Paczesny S, Krijanovski OI, Braun TM, Choi SW, Clouthier SG, Kuick R, et al. A biomarker panel for acute graft-versus-host disease. Blood. (2009) 113(2):273–8. doi: 10.1182/blood-2008-07-167098
10. Martínez-Laperche C, Buces E, Aguilera-Morillo MC, Picornell A, González-Rivera M, Lillo R, et al. A novel predictive approach for GVHD after allogeneic SCT based on clinical variables and cytokine gene polymorphisms. Blood Adv. (2018) 2(14):1719–37. doi: 10.1182/bloodadvances.2017011502
11. Mohty B, Mohty M. Long-term complications and side effects after allogeneic hematopoietic stem cell transplantation: an update. Blood Cancer J. (2011) 1:e16. doi: 10.1038/bcj.2011.14
12. Giralt S, Bishop MR. Principles and overview of allogeneic hematopoietic stem cell transplantation. Cancer Treat Res. (2009) 144:1–21. doi: 10.1007/978–0-387–78580-6_1
13. Warren EH, Zhang XC, Li S, Fan W, Storer BE, Chien JW, et al. Effect of MHC and non-MHC donor/recipient genetic disparity on the outcome of allogeneic HCT. Blood. (2012) 120(14):2796–806. doi: 10.1182/blood-2012-04-347286
14. Kumar S, Mohammadpour H, Cao X. Targeting cytokines in GVHD therapy. J Immunol Res Ther. (2017) 2:90–9. doi: 10.1002/eji.201040793
15. Dickinson AM. Non-HLA genetics and predicting outcome in HSCT. Int J Immunogenet. (2008) 35:375–80. doi: 10.1111/j.1744-313X.2008.00790.x
16. Martin PJ, Fan W, Storer BE, Levine DM, Zhao LP, Warren EH, et al. Replication of associations between genetic polymorphisms and chronic graft-versus-host disease. Blood. (2016) 128(20):2450–6. doi: 10.1182/blood-2016-07-728063
17. Teng MW, Bowman EP, McElwee JJ, Smyth MJ, Casanova JL, Cooper AM, et al. IL-12 and IL-23 cytokines: from discovery to targeted therapies for immune-mediated inflammatory diseases. Nat Med. (2015) 21(7):719–29. doi: 10.1038/nm.3895
18. Mathias C, Mick R, Grupp S, Duffy K, Harris F, Laport G, et al. Soluble interleukin-2 receptor concentration as a biochemical indicator for acute graft-versus-host disease after allogeneic bone marrow transplantation. J Hematother Stem Cell Res. (2000) 9(3):393–400. doi: 10.1089/15258160050079506
19. Chang SH, Dong C. Signaling of interleukin-17 family cytokines in immunity and inflammation. Cell Signal. (2011) 23:1069–75. doi: 10.1016/j.cellsig.2010.11.022
20. Stephen-Victor E, Fickenscher H, Bayry J. IL-26: an emerging proinflammatory member of the IL-10 cytokine family with multifaceted actions in antiviral, antimicrobial, and autoimmune responses. PloS Pathog. (2016) 12:e1005624. doi: 10.1371/journal.ppat.1005624
21. Hadeiba H, Sato T, Habtezion A, Oderup C, Pan J, Butcher EC. CCR9 expression defines tolerogenic plasmacytoid dendritic cells able to suppress acute graft-versus-host disease. Nat Immunol. (2008) 9:1253–60. doi: 10.1038/ni.1658
22. Wu X, Sun M, Yang Z, Lu C, Wang Q, Wang H, et al. The roles of CCR9/CCL25 in inflammation and inflammation-associated diseases. Front Cell Dev Biol. (2021) 9:686548. doi: 10.3389/fcell.2021.686548
23. Bucher C, Koch L, Vogtenhuber C, Goren E, Munger M, Panoskaltsis-Mortari A, et al. IL-21 blockade reduces graft-versus-host disease mortality by supporting inducible T regulatory cell generation. Blood. (2009) 114(26):5375–84. doi: 10.1182/blood-2009-05-221135
24. Chen D, Tang TX, Deng H, Yang XP, Tang ZH. Interleukin-7 biology and its effects on immune cells: mediator of generation, differentiation, survival, and homeostasis. Front Immunol. (2021) 12:747324. doi: 10.3389/fimmu.2021.747324
25. Deng C, Peng N, Tang Y, Yu N, Wang C, Cai X, et al. Roles of IL-25 in type 2 inflammation and autoimmune pathogenesis. Front Immunol. (2021) 12:691559. doi: 10.3389/fimmu.2021.691559
26. Spolski R, Leonard WJ. Interleukin-21: a double-edged sword with therapeutic potential. Nat Rev Drug Discovery. (2014) 13:379–95. doi: 10.1038/nrd4296
27. Davis MR, Zhu Z, Hansen DM, Bai Q, Fang Y. The role of IL-21 in immunity and cancer. Cancer Lett. (2015) 358:107–14. doi: 10.1016/j.canlet.2014.12.047
28. Gómez AM, Martínez C, González M, Luque A, Melen GJ, Martínez J, et al. Chemokines and relapses in childhood acute lymphoblastic leukemia: A role in migration and in resistance to antileukemic drugs. Blood Cells Mol Dis. (2015) 55(3):220–7. doi: 10.1016/j.bcmd.2015.07.001
29. Lobo-Silva D, Carriche GM, Castro AG, Roque S, Saraiva M. Balancing the immune response in the brain: IL-10 and its regulation. J Neuroinflammation. (2016) 13:297. doi: 10.1186/s12974-016-0763-8
30. Castro F, Cardoso AP, Gonçalves RM, Serre K, Oliveira MJ. Interferon-gamma at the crossroads of tumor immune surveillance or evasion. Front Immunol. (2018) 9:847. doi: 10.3389/fimmu.2018.00847
31. Vilgelm AE, Richmond A. Chemokines modulate immune surveillance in tumorigenesis, metastasis, and response to immunotherapy. Front Immunol. (2019) 10:333. doi: 10.3389/fimmu.2019.00333
32. Kuleshov MV, Jones MR, Rouillard AD, Fernandez NF, Duan Q, Wang Z, et al. Enrichr: a comprehensive gene set enrichment analysis web server 2016 update. Nucleic Acids Res. (2016) 44(W1):W90–7. doi: 10.1093/nar/gkw377
33. Piper C, Drobyski WR. Role of TH17 cells and interleukin 17 in graft versus host disease and graft versus leukemia reactivity. In: Immune Biology of Allogeneic Hematopoietic Stem Cell Transplantation. Elsevier (2019). p. 231–49. doi: 10.1016/b978-0-12-812630-1.00014-1
34. Zhao XY, Xu LL, Lu SY, Huang XJ. IL-17-producing T cells contribute to acute graft-versus-host disease in patients undergoing unmanipulated blood and marrow transplantation. Eur J Immunol. (2011) 41:514–26. doi: 10.1002/eji.201040793
35. Carlson MJ, West ML, Coghill JM, Panoskaltsis-Mortari A, Blazar BR, Serody JS. In vitro-differentiated TH17 cells mediate lethal acute graft-versus-host disease with severe cutaneous and pulmonary pathologic manifestations. Blood. (2009) 113:1365–74. doi: 10.1182/blood-2008-06-162420
36. Schroeder MA, Choi J, Staser K, DiPersio JF. The role of janus kinase signaling in graft-versus-host disease and graft versus leukemia. Biol Blood Marrow Transplant. (2018) 24:1125–34. doi: 10.1016/j.bbmt.2017.12.797
37. Braun LM, Zeiser R. Kinase inhibition as treatment for acute and chronic graft-versus-host disease. Front Immunol. (2021) 12:760199. doi: 10.3389/fimmu.2021.760199
Keywords: polymorphisms, graft-versus-host-disease, predictive models, cytokines, allogeneic transplantation
Citation: Muñiz P, Martínez-García M, Bailén R, Chicano M, Oarbeascoa G, Triviño JC, de la Iglesia-San Sebastian I, Fernández de Córdoba S, Anguita J, Kwon M, Díez-Martín JL, Olmos PM, Martínez-Laperche C and Buño I (2024) Identification of predictive models including polymorphisms in cytokines genes and clinical variables associated with post-transplant complications after identical HLA-allogeneic stem cell transplantation. Front. Immunol. 15:1396284. doi: 10.3389/fimmu.2024.1396284
Received: 05 March 2024; Accepted: 08 July 2024;
Published: 23 August 2024.
Edited by:
Jukka Partanen, Finnish Red Cross Blood Service, FinlandReviewed by:
Albert Rosenberger, University Medical Center Goettingen, GermanyKatarzyna Bogunia-Kubik, Polish Academy of Sciences, Poland
Copyright © 2024 Muñiz, Martínez-García, Bailén, Chicano, Oarbeascoa, Triviño, de la Iglesia-San Sebastian, Fernández de Córdoba, Anguita, Kwon, Díez-Martín, Olmos, Martínez-Laperche and Buño. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carolina Martínez-Laperche, Y21sYXBlcmNoZWhndWdtQGdtYWlsLmNvbQ==; Ismael Buño, aXNtYWVsYnVub0BpaXNnbS5lcw==
†These authors have contributed equally to this work