 Stefania Nicola1†
Stefania Nicola1† Richard Borrelli1*†
Richard Borrelli1*† Federica Corradi1Luca Lo Sardo1Iuliana Badiu1Alessandra Romito2
Federica Corradi1Luca Lo Sardo1Iuliana Badiu1Alessandra Romito2 Nicolò Rashidy1
Nicolò Rashidy1 Anna Quinternetto1Marina Mazzola1Federico Meli1Elena Saracco1Ilaria Vitali1
Anna Quinternetto1Marina Mazzola1Federico Meli1Elena Saracco1Ilaria Vitali1 Domenico Cosseddu2
Domenico Cosseddu2 Luisa Brussino1
Luisa Brussino1- 1Department of Medical Science, Allergy and Clinical Immunology Unit, Mauriziano Hospital, University of Turin, Turin, Italy
- 2Department of Laboratory Medicine, Mauriziano Hospital, Turin, Italy
Background: Systemic lupus erythematosus (SLE) is a chronic autoimmune disorder characterized by a variety of both signs and symptoms; it mainly affects women of childbearing age, with an estimated prevalence of 24/100,000 people in Europe and North America. SLE is often described as an antibodies-driven disease as its clinical manifestations are usually associated with the presence or the absence of specific antibodies.
Objectives: To evaluate clinical manifestations in patients with SLE and to assess the relationship with the presence of specific antibodies by using real-world data.
Methods: A retrospective study was performed; the 2019 EULAR/ACR Classification Criteria for Systemic Lupus Erythematosus were used to classify patients with SLE. Data concerning serological profiles (which included Antinuclear antibodies – ANA, anti dsDNA, anti-Ro/SS-A, anti-La/SS-B, anti-Smith) were gathered along with medical records of clinical manifestations. Complement levels were also tested for possible clinical correlations. χ² or Fisher’s exact tests were utilized to establish associations between autoantibodies and symptoms. The odds ratios (OR) and their 95% confidence intervals (CI) were computed. No correction was made for multiple testing; only a p-value 0.01 ≤ was considered significant.
Results: One-hundred and twenty-seven patients (n=127, mean age 53.43 ± 14.02) were enrolled in this study. Anti-dsDNA antibodies were found to be statistically significant for both malar rash and proteinuria; anti-Ro/SSA antibodies showed an association with photosensitivity and pericarditis; furthermore, a strong association was found between anti-Ro antibodies and proteinuria, but only if anti-dsDNA antibodies were present as well. Patients who tested positive for anti-La/SSB antibodies correlated with a threefold increase in the risk of developing pericarditis. Lastly, anti-Smith appeared to be associated with NPSLE as well as an increased risk for both autoimmune hemolytic anemia and thrombocytopenia.
Conclusions: In our study, many associations confirmed those found in previous studies; however, new relationships between antibodies and clinical manifestations were found thus indicating the need for additional evaluations to assess these correlations further.
Introduction
Background
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease that causes inflammation and can damage almost any organ and system in the body. It can present with a wide range of symptoms, and the presence of certain antibodies may be related to specific manifestations (1).
To date, the etiology of the disease has not been thoroughly assessed; however, multifactorial participation has been established as it incorporates epigenetic, genetic, ecological, and environmental components (2–4).
Epidemiology
Following the estimates provided by the worldwide epidemiological community, the proportion of females to males is nine to one (F: M 9:1), with the age range of 15 to 44 years old being the highest (5). It has been estimated that the incidence of SLE is 5.14 (1.4; 15.13) per 100 thousand person-years; however, this number can vary greatly depending on the region of interest, ranging from 1.18 (0.16; 3.68) per 100 thousand person-years in central Asia to 13.74 (3.2; 31.82) per 100 thousand person-years in central Europe. Regarding ethnicity, Systemic Lupus Erythematosus appears to be significantly more frequent in African American individuals when compared to Caucasians (6–8).
Pathogenesis and autoantibodies
SLE is a classic example of an autoimmune disease that is caused by the formation of immunocomplexes. An abnormal immune response, along with a change in the process of clearing nucleic acids, leads to the loss of self-tolerance and the production of autoantibodies, which ultimately form pathogenic immunocomplexes. These immune complexes carrying self-DNA and RNA stimulate the production of excessive amounts of type I interferon (IFN) by plasmacytoid dendritic cells via Toll-like receptors seven and nine (TLR7 and TLR9) and are responsible for complement activation leading to damages in the various organs. Type I IFN also affects B-cell activity as it promotes enhanced survival and activation, which includes differentiation and class-switch recombination and can result in the formation of autoantibodies (9–11).
Anti-nuclear antibody (ANA) positivity has gained greater importance in classifying SLE in recent literature. ANA is believed to contribute to disease progression by impacting the immune system and organs such as the brain, kidneys, and skin, and it comprises several autoantibodies, including anti-nucleosome, anti-dsDNA, anti-histone, anti-Smith (Sm), anti-Ribonucleic Protein Antigen (RNP), anti-Ro, and anti-La antibodies, each with specific immunofluorescence pattern (12, 13).
While anti-Sm and anti-dsDNA antibodies are specific to SLE, the others are also found in other autoimmune diseases (14). Moreover, the level of anti-dsDNA antibody is a crucial autoantibody biomarker for the SLE Disease Activity Index (SLEDAI) (15).
Diagnosis and classification
The most recent classification criteria were edited in 2019 by the “European League Against Rheumatism/American College of Rheumatology” (ACR/EULAR) to include patients in an early stage of disease (16); in fact, their sensitivity is 93% (95% CI, 0.83-0.98), which is higher than the 2012 Systemic Lupus International Collaborating Clinics (SLICC) criteria (83%, 95% CI, 0.72- 0.91) (17). However, the newest criteria did not improve specificity, showing a comparable percentage than the previous ones (75%, 95% CI, 0.61-0.85 for the EULAR/ACR VS 73%, 95% CI, 0.59-0.83 for SLICC).
Unlike the previous ones, the presence of an entry criterion (the presence of ANA) is now mandatory for the classification into studies; this element defines a noticeable difference with cohorts from previous studies (14); furthermore, items are now divided into clinical and immunological domains; patients are considered affected if the score is at least 10.
Treatment
The recent update of the recommendations (2023 ACR/EULAR Recommendations on the management of Systemic Lupus Erythematosus) changed the therapeutic approaches for patients with SLE. Hydroxychloroquine (HCQ) is the mainstay of treatment and should be used at a dosage of no more than 5 mg/kg. Prednisone or equivalent is also often required for inducing remission and for chronic maintenance, with a dosage lower than 7.5 mg daily and, wherever feasible, should be stopped if not required. In addition, an immunosuppressant can be considered in individuals who are refractory to HCQ therapy (with or without glucocorticoids or too high dosages). Unlike the previous recommendations, biological therapies like Belimumab (anti-Blys) and Anifrolumab (anti-IFN Receptor 1) can be administered in mild form of disease as they proved to be both safe and effective for patients (18).
Furthermore, Voclosporin, a novel calcineurin inhibitor, was the last medication added to the list of LN in combination with mycophenolate (19). Lastly, in cases of severe disease, like those involving CNS or renal involvement, Cyclophosphamide (CYC) or Rituximab (RTX) should be used (18).
Materials and methods
Study design and population
This retrospective monocentric cohort observational study enrolled outpatients with a confirmed diagnosis of SLE according to the 2019 ACR/EULAR classification criteria with systemic lupus erythematosus (16).
To ensure the quality of the data, patients with inadequate or incomplete medical documentation were excluded from the study. We also applied a range of exclusion criteria, including active neoplasia, diagnosis of primary or secondary immunodeficiency, and substance abuse.
Objectives
The main objective is to assess the correlation between the autoantibody subtypes and the clinical manifestations, in order to verify any possible differences with the previous studies and assist clinicians in predicting possible outcomes of the disease. Possible disease outcomes can be predicted by considering clinical manifestations and serological profiles, which could help establish specific treatment plans for SLE patients.
Data collection
Data concerning age, sex, smoking habits, ongoing and previous treatments, as well as comorbidities were collected.
Serological evaluation
Data on the serological profiles of patients were collected. These data include antinuclear antibodies (ANA, HEp-2 IFA by Euroimmun S.r.L, Italy), anti-double-stranded DNA antibodies (anti-dsDNA, evaluated on fluorescent enzyme immunoassays - FEIAs - by ThermoFisher, Waltham, MA and IFA on Chrithidia luciliae -Euroimmun S.r.L. for positive findings in order to confirm the result), anti-Ro/SS-A antibodies (divided, where available, into 52 kDa and 60 kDa, evaluated on fluorescent enzyme immunoassays - FEIAs by ThermoFisher), anti-La/SS-B and anti-Smith (anti- Sm, FEIAs byThermoFisher) antibodies (20–22).
Complement levels, namely C3 and C4, were also evaluated with blood tests to determine their trend and possible correlation with clinical manifestations.
Systemic and organ involvement
Organ involvement was assessed by using the definitions of 2019 ACR/EULAR for Systemic Lupus Erythematosus (supplementary material, Table 1 of the classification criteria) and the Safety of Estrogen in Lupus National Assessment - Systemic Lupus Erythematosus Disease Activity Index (SELENA-SLEDAI) (23).
The presence of hematological manifestations (namely thrombocytopenia, lymphopenia, and hemolytic anemia) was evaluated with seriated blood tests with a focus on platelets, hemoglobin, WBC, and lymphocytes, haptoglobin, Lactate Dehydrogenase (LDH), direct and indirect bilirubin levels; direct Coombs tests were also performed. Joint manifestations (including arthralgia, Jaccoud’s arthritis, non-deforming non-erosive arthritis, and erosive arthritis) were assessed by the presence of either two or more joints with pain and signs of inflammation (tenderness, swelling or effusion) or ultrasound (US) of the joints with Power Doppler (PWD).
Cutaneous manifestations were defined as acute lupus, discoid lupus alopecia, presence of oral ulcers or malar rash; renal involvement was evaluated by the presence of glomerulonephritis (established with a kidney biopsy) or the presence of proteinuria >0.5 g/L in a 24-hour urine collection.
Neuropsychiatric involvement was assessed in the presence of encephalitis, psychosis, epilepsy, or depression, which could not be related to other plausible causes; pericarditis or pleuritis with or without pericardial or pleural effusion were investigated as per 2019 ACR/EULAR definitions on Systemic Lupus Erythematosus (16, 24, 25).
Statistical analysis
The information that was gathered was analyzed with the help of STATA SE 18.0 (1985-2023 StataCorp LLC, College Station, Texas, United States of America).
For the purpose of establishing connections between autoantibodies and symptoms, either the χ2 or Fisher’s exact tests were applied. Both the odds ratios (OR) and the confidence intervals (CI) for each of them were computed 95% There were no adjustments made to account for multiple testing; as such, the only p value that was considered significant was 0.01 or less.
Ethical approval
All of the subjects gave their consent after being fully informed. All of the procedures were carried out in accordance with the pertinent rules, in accordance with the Declaration of Helsinki from 1964, and in accordance with the regulations that were imposed by the legislative body. This study was approved by the local Ethics Committee (Comitato Etico Territoriale interaziendale AOU Città della Salute e della Scienza di Torino, study #0116953).
Results
One-hundred and twenty-seven patients (n=127) were enrolled in this study as per inclusion criteria; demographics and records can be found in Tables 1, 2a, 2b, 3.
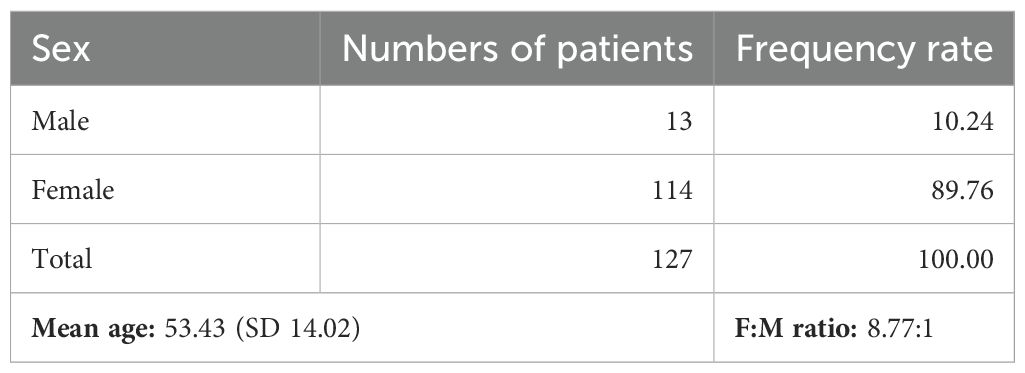
Table 1. Demographic characteristics.
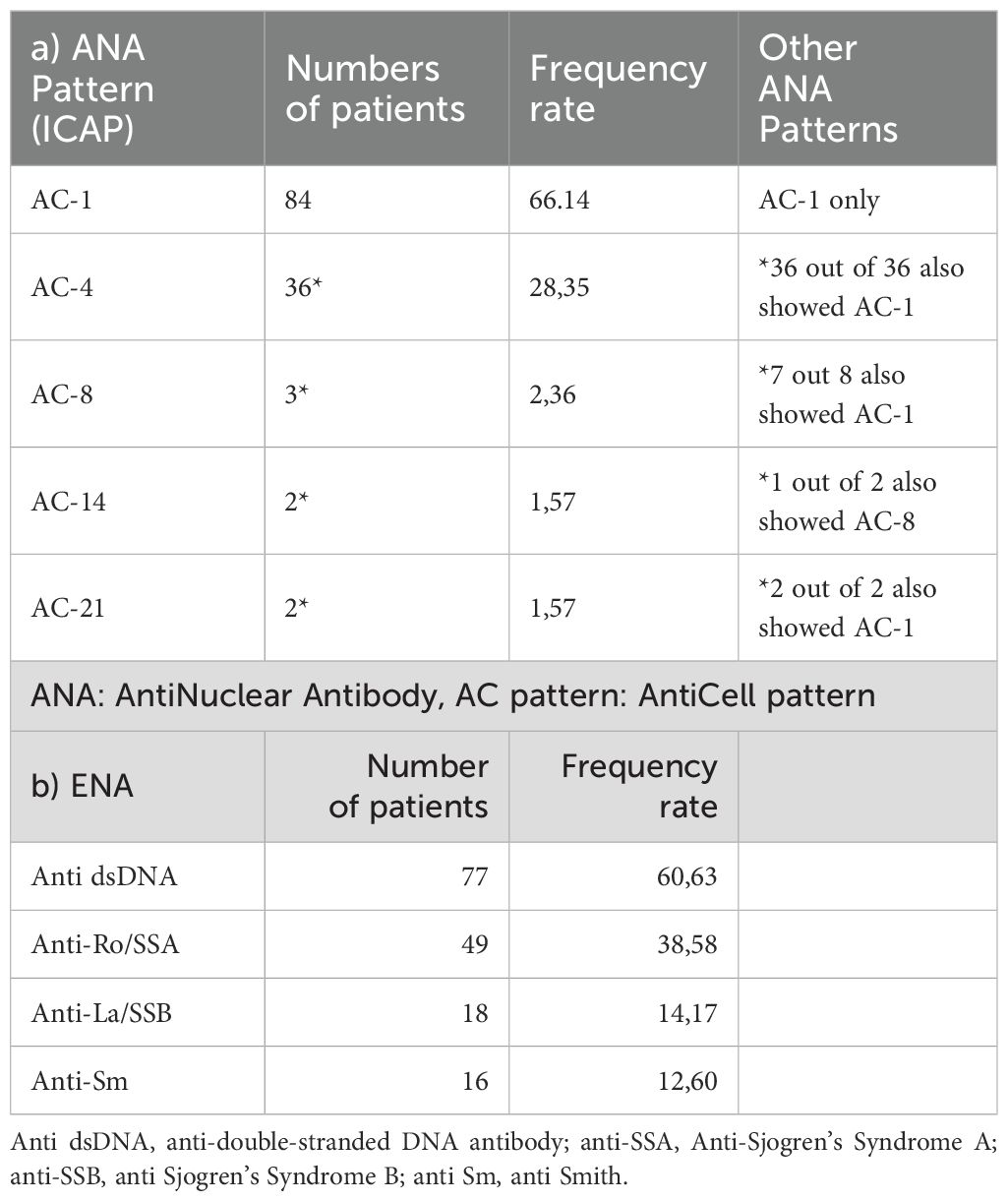
Table 2. Distribution of autoantibodies.
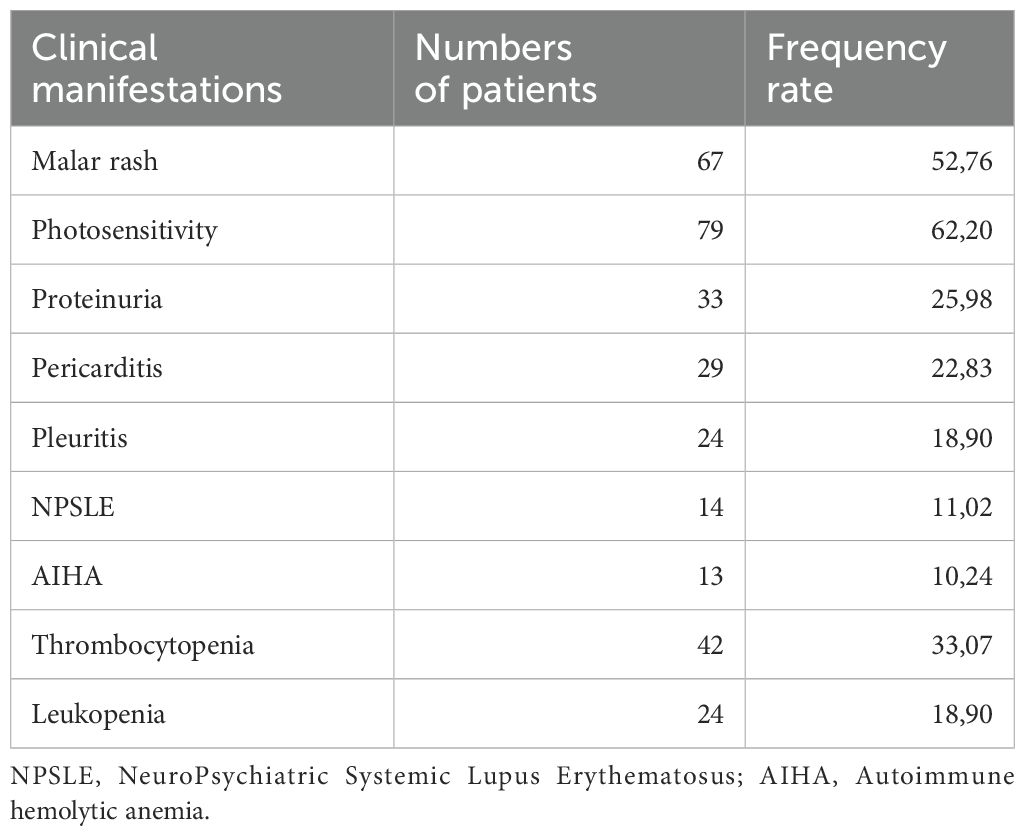
Table 3. Distribution of clinical manifestations.
As shown in the tables, the demographic characteristics of the enrolled patients are comparable to those found in literature.
Alas, different patterns of Antinuclear antibodies (ANA) failed to demonstrate a significant association with specific clinical manifestations As concerns the other types of autoantibodies, the results are summarized and shown in Table 4.
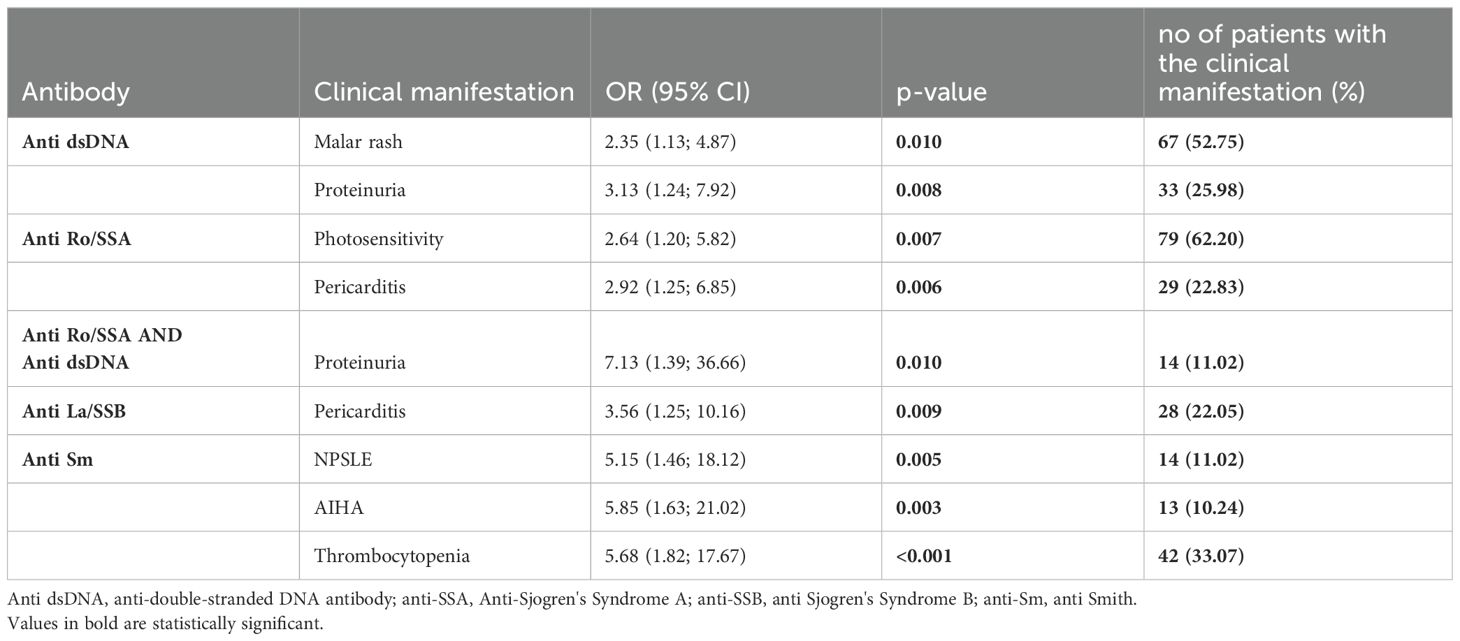
Table 4. Relationship between clinical manifestations and antibodies that reached statistical significance.
Anti dsDNA antibodies were found to be statistically significant for both malar rash (OR 2.35, CI 95% 1.13; 4.87, p=0.01) and proteinuria (OR 3.13, CI 95% 1.24; 7.92, p=0.008).
Anti-Ro/SSA antibodies showed an association with photosensitivity (OR 2.64, CI 95% 1.20; 5.82, p=0.007) and pericarditis (OR 2.92, CI 95% 1.25; 6.85, p=0.006). A strong association was found between anti Ro antibodies and proteinuria, but only in the cohort of patients who also tested positive for anti dsDNA; in fact, this association appeared to be related with a sevenfold increased risk for patients in case of double positivity (OR 7.13, CI 95% 1.39, 36.66, p=0.010).
A different scenario was ascertained in patients who tested positive for anti La/SSB antibodies; in our cohort these antibodies were found to be related with a threefold increase in the risk of pericarditis (OR 3.56, CI 95% 1.25, 10.16, p=0.009). Lastly, anti-Smith antibodies were evaluated; its presence appeared to positively correlate with NPSLE (OR 5.15, CI 95% 1.46, 18.12, p=0.005); as for the hematological manifestations, anti-Smith antibodies increased the risk for both autoimmune hemolytic anemia (OR 5.85, CI 95% 1.63, 21.02, p= 0.003) and thrombocytopenia (OR 5.68, CI 95% 1.82, 17.67, p< 0.001).
Lastly, the relationship between clinical manifestations and complement levels were tested; as showed in Table 5, reduced levels of complement were statistically significant for the development of proteinuria (OR 3.40, CI 95% 1.39, 8.31, p=0.007).

Table 5. Relationship between clinical manifestations and complement levels.
Discussion
SLE is a disease characterized by a combination of clinical manifestations that can widely vary among affected patients; as such, it might be helpful to use real-world data to assess possible correlations between antibodies and clinical manifestations.
The population described in our study is comparable to the cohorts described in the literature for both sex distribution and age (26, 27).
As mentioned in the results, diverse patterns of ANA were not statistically significant for different clinical manifestations among patients with SLE. This result might be explained by the usage of a set of criteria which require ANA to be present as the main inclusion condition; unlike studies from other countries who used ACR criteria (in which differences could be observed due to the heterogeneity of the cohort), our patients were similar and all of them were positive for the presence of ANA. Moreover, the great majority of the patients showed an AC-1 pattern, thus reducing the chance to observe any statistically significant difference.
Patients with anti-dsDNA antibodies saw a statistically significant association with the presence of proteinuria and malar rash, which appear to agree with previous studies (14, 28, 29); however, unlike other evaluations, pleuritis, alopecia and lymphopenia did not reach a significant correlation (30).
Proteinuria was also observed in patients with a double positivity for both anti Ro/SS-A antibodies and anti dsDNA as their copresence appeared to be significant for a sevenfold risk of its development. Additionally, anti-Ro/SSA antibodies correlated with increased photosensitivity for patients who tested positive, which has been assessed in previous studies as well (31); a correlation with pericarditis was also observed in these patients, unlike the results found in other reports as they failed to show a correlation with anti-SSA antibodies (32, 33).
Our work managed to confirm the relationship between anti-La/SSB antibodies and pericarditis, which was observed in previous studies (21, 34) but did not show a significant correlation with renal involvement nor with other manifestations of SLE.
This element might be explained by the difference between the cohorts; in the study of Novak and colleagues, patients only needed to fulfill the American College of Rheumatology (ACR) definition of SLE, which does not require an entry criterion (namely, the presence of ANA); moreover, they needed to have a diagnosis of SLE before 18 years of age. Childhood- onset SLE (cSLE) usually shows, in fact, a more severe combination of constitutional signs and symptoms when compared to patients with a later onset (35).
Lastly, it has already been established that patients from different ethnicities might develop non-identical manifestations of SLE as patients of Latin ethnicity tend to manifest a renal involvement more frequently than Caucasian patients (36).
In our cohort of patients, anti-Smith antibodies were highly associated with hematological pictures, namely lymphopenia and AIHA as well as NPSLE, in agreement with previous reports (37, 38).
Interestingly, we didn’t find any significant association between anti-Smith antibodies and the presence of proteinuria, renal involvement, lymphopenia, or cardiac involvement, which was observed in other studies (36, 39). Similarly to before, this difference might be explained by taking into account the epidemiological elements on which these studies have been conceived.
The main work on this topic comes from the Genetic Profile Predicting the Phenotype study (PROFILE), which is a well-characterized multi-ethnic cohort of SLE patients constituted in 1998; not only was the study based on the 1997 American College of Rheumatology (ACR) revised criteria, but it also enrolled patients who were either Latin-American, Hispanic or African- American. As such, different clinical manifestations are to be expected as this cohort appears to be rather specific and poorly comparable to the one analyzed in this study.
We also checked for possible correlations between low levels of complement and clinical manifestations in our sample; in agreement with previous studies, our work confirmed that patients with reduced C3 and/or C4 levels might develop proteinuria (40, 41).
In conclusion, relationships between clinical manifestations and antibodies have been widely assessed in the past but different definitions of disease and new laboratory methods changed the cohorts of patients in which we can verify such associations. Among these, many relationships have confirmed previous reports, whilst others have diverged or described new possible relationships which might benefit from further investigations.
Limitations
The main limitation of this study is its retrospective design with data collected from medical history and recorded from a single center. Another limitation which might be taken into consideration is the high prevalence of Caucasian patients in our population, unrepresentative of other ethnic groups.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Local Ethics Committee (Comitato Etico Territoriale di Torino). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
SN: Writing – original draft, Writing – review & editing. RB: Conceptualization, Data curation, Formal analysis, Methodology, Software, Validation, Writing – original draft, Writing – review & editing. FC: Conceptualization, Data curation, Formal analysis, Funding acquisition, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. LS: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing. IB: Conceptualization, Investigation, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AR: Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. NR: Conceptualization, Data curation, Formal analysis, Investigation, Visualization, Writing – original draft, Writing – review & editing. AQ: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. MM: Conceptualization, Investigation, Validation, Visualization, Writing – original draft, Writing – review & editing. FM: Conceptualization, Data curation, Investigation, Supervision, Writing – original draft, Writing – review & editing. ES: Data curation, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. IV: Formal analysis, Investigation, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. DC: Formal analysis, Investigation, Visualization, Writing – original draft, Writing – review & editing. LB: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
A special mention to Dr. A. Romito and Dr. D. Cosseddu of the Department of Laboratory Medicine, for the precious support they gave us with the interpretation of ANA patterns as well as with the literature records concerning autoantibodies.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Oku K, Atsumi T. Systemic lupus erythematosus: nothing stale her infinite variety. Mod Rheumatol. (2018) 28:758–65. doi: 10.1080/14397595.2018.1494239
2. Crow MK. Pathogenesis of systemic lupus erythematosus: risks, mechanisms and therapeutic targets. Ann Rheum Dis. (2023) 82:999–1014. doi: 10.1136/ard-2022-223741
3. Catalina MD, Owen KA, Labonte AC, Grammer AC, Lipsky PE. The pathogenesis of systemic lupus erythematosus: Harnessing big data to understand the molecular basis of lupus. J Autoimmun. (2020) 110:102359. doi: 10.1016/j.jaut.2019.102359
4. Kechida M. Influence of age onset in clinical and biological spectrum of systemic lupus erythematosus. Ann Rheumatic Dis. (2017) 76:885 2–885.
5. Ramírez Sepúlveda JI, Bolin K, Mofors J, Leonard D, Svenungsson E, Jönsen A, et al. Sex differences in clinical presentation of systemic lupus erythematosus. Biol Sex Differ. (2019) 10:60. doi: 10.1186/s13293-019-0274-2
6. Tian J. Global epidemiology of systemic lupus erythematosus: a comprehensive systematic analysis and modelling study. Ann Rheum Dis. (2023) 82:351–6. doi: 10.1136/ard-2022-223035
7. EE C. The global burden of SLE: prevalence, health disparities and socioeconomic impact. Nat Rev Rheumatol. (2016) 12:605–20. doi: 10.1038/nrrheum.2016.137
8. F. M. Systemic lupus erythematosus in Latin America: Outcomes and therapeutic challenges. Clin Immunol Commun. (2023) 4:60–4. doi: 10.1016/j.clicom.2023.10.002
9. Satterthwaite AB. TLR7 signaling in lupus B cells: new insights into synergizing factors and downstream signals. Curr Rheumatol Rep. (2021) 23(11):80. doi: 10.1007/s11926-021-01047-1
10. Wang D. TLR9 polymorphisms and systemic lupus erythematosus risk: an update meta-analysis study. Rheumatol Int. (2016) 11(12):3549. doi: 10.1007/s00296-015-3404-0
11. Postal M. Type I interferon in the pathogenesis of systemic lupus erythematosus. Curr Opin Immunol. (2020). 67:87–94. doi: 10.1016/j.coi.2020.10.014
12. Yoshimi R. Clinical and pathological roles of Ro/SSA autoantibody system. Clin Dev Immunol. (2012) 2012:606195. doi: 10.1155/2012/606195
13. Hsieh SC. Anti-SSB/La is one of the antineutrophil autoantibodies responsible for neutropenia and functional impairment of polymorphonuclear neutrophils in patients with systemic lupus erythematosus. Clin Exp Immunol. (2003) 131:506–16. doi: 10.1046/j.1365-2249.2003.02084.x
14. Hoffman IEA, Peene I, Meheus L. Specific antinuclear antibodies are associated with clinical features in systemic lupus erythematosus. Ann Rheumatic Dis. (2004) 63:1155–8. doi: 10.1136/ard.2003.013417
15. Förger F. Clinical significance of anti-dsDNA antibody isotypes: IgG/IgM ratio of anti-dsDNA antibodies as a prognostic marker for lupus nephritis. Lupus. (2004) 13:36–44. doi: 10.1191/0961203304lu485oa
16. Aringer M. European league against rheumatism/american college of rheumatology classification criteria for systemic lupus erythematosus. Arthritis Rheumatol. (2019) 71:1400–12. doi: 10.1002/art.40930
17. Dahlström Ö, Sjöwall C. The diagnostic accuracies of the 2012 SLICC criteria and the proposed EULAR/ACR criteria for systemic lupus erythematosus classification are comparable. Lupus. (2019) 28(6):778–2. doi: 10.1177/096120331984638
18. Fanouriakis A. EULAR recommendations for the management of systemic lupus erythematosus. (2023).
19. Gelder T. Voclosporin: a novel calcineurin inhibitor for the treatment of lupus nephritis. Expert Rev Clin Pharmacol. (2022) 15:515–29. doi: 10.1080/17512433.2022.2092470
20. PE L. Anti-ro/SSA antibodies blocking calcium channels as a potentially reversible cause of atrioventricular block in adults. JACC Clin Electrophysiol. (2023) 9:1631–48. doi: 10.1016/j.jacep.2023.03.007
21. GV N. Anti-RO/SSA and anti-La/SSB antibodies: Association with mild lupus manifestations in 645 childhood-onset systemic lupus erythematosus. Autoimmun Rev. (2017) 16:132–5. doi: 10.1016/j.autrev.2016.12.004
22. Ahn SS, Jung SM, Yoo J, Lee SW, Song JJ, Park YB. Anti-Smith antibody is associated with disease activity in patients with new-onset systemic lupus erythematosus. Rheumatol Int. (2019) 39:1937–44. doi: 10.1007/s00296-019-04445-y
23. Touma Z. Chapter 46 - clinical measures, metrics, and indices, dubois’ Lupus erythematosus and related syndromes. In: Saunders WB, Elsevier (2013).
24. Wang H, Gao Y, Ma Y, Cai F, Huang X, Lan L, et al. Performance of the 2019 EULAR/ACR systemic lupus erythematosus classification criteria in a cohort of patients with biopsy-confirmed lupus nephritis. Lupus Sci Med. (2021) 8:e000458. doi: 10.1136/lupus-2020-000458
25. Tselios K, Urowitz MB. Cardiovascular and pulmonary manifestations of systemic lupus erythematosus. Curr Rheumatol Rev. (2017) 13:206–18. doi: 10.2174/1573397113666170704102444
26. Li YZ, Wu XC. Research progress in systemic lupus erythematosus from 2021 to 2022. Zhongguo Dang Dai Er Ke Za Zhi. (2023) 25:785–90. doi: 10.7499/j.issn.1008-8830.2302150
27. Chung MK, Park JS, Lim H, Lee CH, Lee J. Incidence and prevalence of systemic lupus erythematosus among Korean women in childbearing years: A nationwide population-based study. Lupus. (2021) 30:674–9. doi: 10.1177/0961203320984845
28. Asif S, Khan A, Zahoor S, Lashari N, Haroon M, Khanum A. Correlation between quantitative anti-dsDNA levels with severity of proteinuria in systemic lupus erythematosus patients. Reumatol Clin (Engl Ed). (2022) 18:464–8. doi: 10.1016/j.reuma.2021.06.002
29. Conti F. Systemic lupus erythematosus with and without anti-dsDNA antibodies: analysis from a large monocentric cohort. Mediators Inflammation. (2015) 2015. doi: 10.1155/2015/328078
30. So C. Bilateral pleuritis as the initial symptom of systemic lupus erythematosus: A case series and literature review. Intern Med. (2019) 58(11):1617–20. doi: 10.2169/internalmedicine.1886-18
31. Lu D, Zhu X, Hong T. Serum metabolomics analysis of skin-involved systemic lupus erythematosus: association of anti-SSA antibodies with photosensitivity. J Inflammation Res. (2023) 16:3811–22. doi: 10.2147/JIR.S426337
32. Menendez A. Common and specific associations of anti-SSA/Ro60 and anti- Ro52/TRIM21 antibodies in systemic lupus erythematosus. ScientificWorldJournal. (2013) 2013:832789. doi: 10.1155/2013/832789
33. Mukkera S. Systemic lupus erythematosus-associated serositis managed with intravenous belimumab: A case report. Cureus. (2022) 14(2):e22639. doi: 10.7759/cureus.22639
34. Oshiro AC. Anti-Ro/SS-A and anti-La/SS-B antibodies associated with cardiac involvement in childhood systemic lupus erythematosus. Ann Rheum Dis. (1997) 56:272–4. doi: 10.1136/ard.56.4.272
35. Levy DM, Kamphuis S. Systemic lupus erythematosus in children and adolescents. Pediatr Clin North Am. (2012) 59(2):345–64. doi: 10.1016/j.pcl.2012.03.007
36. Arroyo-Ávila M. Clinical associations of anti-Smith antibodies in PROFILE: a multi- ethnic lupus cohort. Clin Rheumatol. (2015) 34(7):1217–23. doi: 10.1007/s10067-015-2941-y
37. Manson JJ, Isenberg DA. The pathogenesis of systemic lupus erythematosus. Neth J Med. (2003). 61(11):343–6.
38. JY C. Anti-sm antibody, damage index, and corticosteroid use are associated with cardiac involvement in systemic lupus erythematosus: data from a prospective registry study. Korean Med Sci. (2020) 35(21):e139. doi: 10.3346/jkms.2020.35.e139
39. Flechsig A. What is the clinical significance of anti-Sm antibodies in systemic lupus erythematosus? A comparison with anti-dsDNA antibodies and C3. Clin Exp Rheumatol. (2017) 35:598–606.
40. Bao L. Complement in lupus nephritis: new perspectives. Kidney Dis (Basel). (2015) 1(2):91–9. doi: 10.1159/000431278
Keywords: lupus, SLE, autoantibodies, serological profile, immunology
Citation: Nicola S, Borrelli R, Corradi F, Lo Sardo L, Badiu I, Romito A, Rashidy N, Quinternetto A, Mazzola M, Meli F, Saracco E, Vitali I, Cosseddu D and Brussino L (2024) Relationship between clinical manifestations and serological profile in patients affected by Systemic Lupus Erythematosus. Front. Immunol. 15:1390642. doi: 10.3389/fimmu.2024.1390642
Received: 23 February 2024; Accepted: 29 July 2024;
Published: 16 August 2024.
Edited by:
Monica Neagu, Victor Babes National Institute of Pathology (INCDVB), RomaniaReviewed by:
Danieli Castro Oliveira De Andrade, University of São Paulo, BrazilEmanuele Bizzi, ASST Fatebenefratelli Sacco, Italy
Copyright © 2024 Nicola, Borrelli, Corradi, Lo Sardo, Badiu, Romito, Rashidy, Quinternetto, Mazzola, Meli, Saracco, Vitali, Cosseddu and Brussino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Richard Borrelli, cmljaGFyZC5ib3JyZWxsaUB1bml0by5pdA==
†These authors share first authorship