 Mahtab Zamani1,2*
Mahtab Zamani1,2* Karolina Skagen1,2
Karolina Skagen1,2 Beate Lindberg3Vigdis Bjerkeli4
Beate Lindberg3Vigdis Bjerkeli4 Pål Aukrust2,4,5
Pål Aukrust2,4,5 Bente Halvorsen2,4
Bente Halvorsen2,4 Mona Skjelland1,2
Mona Skjelland1,2- 1Department of Neurology, Oslo University Hospital, Oslo, Norway
- 2Institute of Clinical Medicine, University of Oslo, Oslo, Norway
- 3Department of Cardiothoracic Surgery, Oslo University Hospital, Oslo, Norway
- 4Research Institute of Internal Medicine (RIIM), Oslo University Hospital, Oslo, Norway
- 5Section of Clinical Immunology and Infectious Diseases, Oslo University Hospital, Oslo, Norway
Background: Unstable atherosclerotic carotid plaques with intraplaque neovascularization (IPN) carry a substantial risk for ischemic stroke. Conventional ultrasound methods fall short in detecting IPN, where superb microvascular imaging (SMI) has emerged as a promising tool for both visualizing and quantification. High levels of fibroblast growth factor 23 (FGF-23) have, in observational studies, been suggested as related to cardiovascular morbidity and mortality. The association of FGF-23 to atherosclerotic carotid plaque instability remains relatively unexplored.
Methods: A cohort of twenty-nine patients with ≥50% atherosclerotic carotid stenosis underwent conventional carotid ultrasound, SMI, and blood tests, including measurement of FGF-23 in plasma. Nineteen patients were characterized as symptomatic and ten as asymptomatic.
Results: Our major findings were: i) Higher FGF-23 levels were strongly correlated with increased SMI-assessed IPN. ii) Neo-vessel count recorded by quantitative SMI was positively correlated to increased FGF-23 levels, but not with basic FGF levels. (iii) In contrast, traditional risk factors for plaque instability exhibited no noteworthy associations with SMI-assessed IPN or with FGF-23 levels.
Conclusion: This pilot study suggest the potential of FGF-23 as a valuable marker for neovascularization and atherosclerotic carotid plaque instability as a risk factor for ischemic stroke. Further research involving larger cohorts and prospective data is necessary to understand FGF-23’s role in this context comprehensively.
Introduction
Ischemic stroke due to thromboembolism from an unstable atherosclerotic carotid plaque accounts for 15-25% of all ischemic strokes (1). Intraplaque neovascularization (IPN) is a feature of plaque vulnerability associated with an increased risk of lesion rupture and subsequent ischemic stroke (2). Therefore, identifying carotid plaques with IPN is crucial in treatment alternatives targeting stroke prevention. Pathological IPN is the sprouting of newly formed immature and leaky blood vessels from pre-existing vasa vasorum vasculature, extending throughout the entire arterial wall and towards the plaque core (3). This neovascularization is thought to occur in response to increased oxygen and nutrition demands due to inflammation and increased metabolic activity in a chronic atherosclerotic lesion (4). Still, the mechanisms leading to IPN are not fully understood, and detecting of these micro-vessels with small blood flow signals using standard Doppler ultrasound methods is challenging.
In our recent study, we introduced a novel ultrasound method, Superb Microvascular Imaging (SMI), which utilizes an algorithm that effectively overcomes the challenges faced by standard ultrasound in the visualization and quantification of IPN. We demonstrated SMI to be comparable to contrast-enhanced ultrasound for the assessment of IPN (5).
Fibroblast growth factor (FGF)-23 is a bone-secreted hormone, involved in phosphate homeostasis in the kidney and vitamin D metabolism (6). FGF-23 regulates the expression of its co-receptor, Klotho; together as a collective unit, they assemble into a trimeric signaling complex alongside FGF-receptors (FGFRs) within target tissues, facilitating the execution of FGF-23’s physiological as well pathophysiological functions. Klotho is highly expressed in renal tubules, where it downregulates sodium-phosphate cotransporters (7). Elevated FGF-23 is an independent risk factor for end-stage renal disease in patients with relatively preserved kidney function and for mortality across the spectrum of chronic kidney disease (CKD) (8). However, serum levels of FGF-23 have also been associated with a higher risk of cardiovascular disease (CVD), such as myocardial infarction, ischemic stroke, and heart failure, and these associations were not restricted to patients with impaired kidney function (9, 10). Indeed, in a population-based study, individuals with increased FGF-23 levels had a more significant burden of carotid atherosclerosis independent of CKD (11).
While increased plasma levels of FGF-23 have previously been associated with increased intima-media thickness in the common carotid artery, data on FGF-23 concerning carotid plaque instability are scarce or lacking (7). Based on its role in atherosclerosis, we hypothesized that plasma levels of FGF-23 are associated with the presence of IPN and plaque instability, as measured by SMI assessments. In this pilot study we tested this hypothesis in 29 patients with carotid atherosclerosis previously included in our SMI study cohort who had available plasma for growth factor analysis.
Materials and methods
Study population
We included 29 consecutive patients attending the Department of Neurology, Oslo University Hospital. Sixteen patients with available plasma from our SMI cohort study up to January 2019 were included and 13 new patients were included from January to April 2019. All patients had carotid artery plaque with stenosis ≥ 50% and underwent conventional Doppler ultrasound and SMI ultrasound of the carotid arteries before carotid endarterectomy (CEA) or at a routine outpatient control for the asymptomatic patients. Nineteen included patients were symptomatic, i.e., the patients had undergone ipsilateral cerebral ischemia (minor ischemic strokes, transitory ischemic attacks, or amaurosis fugax) within 30 days prior to study inclusion. Exclusion criteria were ongoing infection, cancer, or autoimmune disease.
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki. The study was approved by the Norwegian Regional Committee for Medical and Health Research Ethics (ID REC 2014/1468), and written informed consent was obtained from all patients before study inclusion.
Ultrasonographic investigation
Ultrasonography Imaging was performed with a Canon ultrasound system Aplio 500 (Canon Medical Systems, Otawara, Japan) using a 7.5 MHz linear probe on both carotid arteries for standard Doppler ultrasound and SMI ultrasound. Common carotid artery, carotid bifurcation, and internal carotid arteries were examined in longitudinal and transverse planes in standard ultrasound. The degree of carotid artery stenosis was determined based on peak-systolic and end-diastolic velocities according to consensus criteria of the Society of Radiologists in ultrasound (12). Plaque echogenicity was classified visually in high-resolution B-mode gray-scale pictures according to the modified version of the classification proposed by Gray-Weale classification as follows: (1) uniformly or predominantly hypoechoic (hypoechoic or hypoechoic with small hyperechoic regions), (2) uniformly or predominantly hyperechoic (hyperechoic or hyperechoic with small hypoechoic regions) (13).
Superb microvascular imaging
Following the standard ultrasound examination, the monochrome-SMI mode was turned on, twin-view display of the plaque in B-mode and monochrome-SMI side by side was enabled. Details on optimized SMI settings and configurations for the assessment of IPN is previously published (5). Plaques were first observed in the transverse plane and then in the longitudinal plane for 2 minutes, and the video images were stored in the ultrasound scanner’s hard drive. Static enhancements were excluded, and moving enhancements were classified as intraplaque microvascular flow (IMVF). IMVF signals were first categorized into three groups on a visual scale as follows: No IPN (no IMVF within the plaque or IMVF confined to the adjacent adventitia), moderate IPN (moving IMVF confined to the adventitial side or moving IMVF at the plaque shoulder), and extensive IPN (IMVF moving to the plaque core or expanded IMVF throughout plaque). Second, a visual assessment of IMVF signals involved tallying the number of neovessels observed within a 2-minute SMI video clip, providing a quantitative evaluation of IPN when assessed using SMI (5).
Biochemical investigation
Blood samples were analyzed by routine methods at the Department of Clinical Biochemistry, Oslo University Hospital. They included Low-Density Lipoprotein (LDL) cholesterol, High-Density Lipoprotein (HDL) cholesterol, Triglycerides (TG), Total cholesterol, fasting glucose, glycosylated Hemoglobin (HbA1c), estimated Glomerular filtration rate (eGFR), high-sensitivity C-reactive protein (CRP), Leukocyte and platelets count, sedimentation rate (ESR) and electrolytes. In addition, EDTA plasma was collected and kept on melting ice for 30 minutes until centrifuged at 2000g for 20 minutes to obtain platelet-poor plasma. Plasma was stored at -80°C until FGF-23, basic (b)-FGF, Interleukin-6 (IL-6) and Tumor Necrosis Factor alpha (TNF-α) were analyzed by U-Plex Metabolic Group 1 (human) assay (Meso Scale Diagnostics, Rockville, MD, USA).
Statistical methods
SPSS for Windows statistical software (version 28.0) was used for data analyses. Categorical variables were compared with Kruskal Wallis and post hoc pairwise comparison tests were used to perform the statistical analysis. Coefficients of correlation were calculated by the Spearman ρ correlation for scale variables. The factors found significant were included in the linear multiple regression model. All statistical results were considered significant when p<0.05.
Results
Twenty-nine patients participated in this study, 18 [70 ± 6 years] men and 11 women [77 ± 6 years] (Table 1). Plaque characteristics assessed by conventional ultrasound and advanced ultrasound assessment of IPN are presented in Table 2. Eleven (38%) uniformly or predominantly hypoechoic and 18 (62%) uniformly or predominantly hyperechoic plaques were examined with B-mode ultrasound. SMI revealed IMVF signal representing IPN in 23 of the 29 plaques assessed visually and quantitatively. Of the 23 patients exhibiting IPN on SMI, nine patients (31%) exhibited moderate IPN, and 14 patients (48%) displayed extensive IPN on the visual scale.
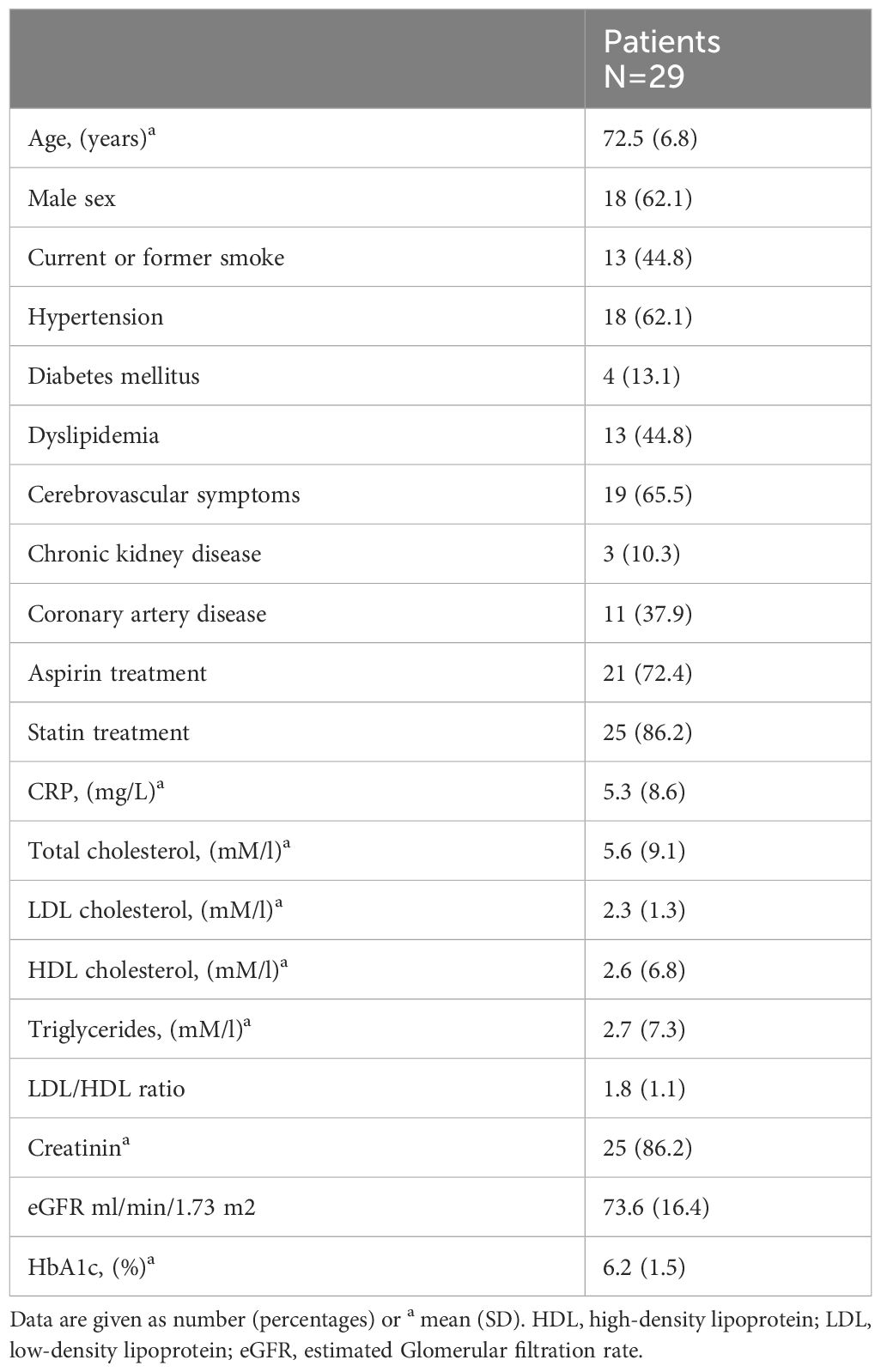
Table 1 Baseline variables of the study population.
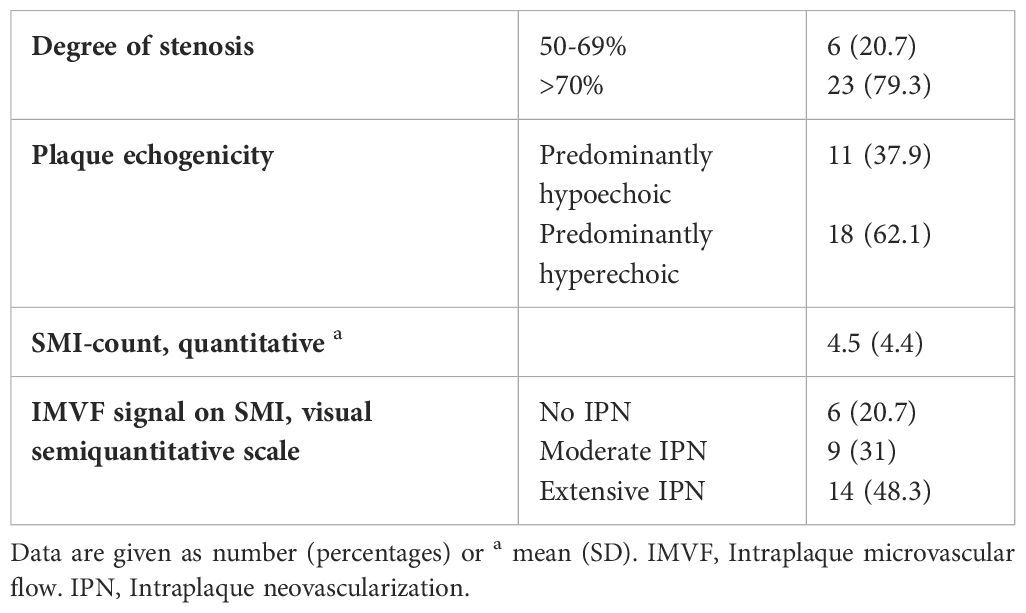
Table 2 Plaque characteristics using standard Doppler ultrasound, IPN assessment using SMI (N=29).
Correlation between plasma level FGF-23 and IPN
Interestingly, plaques with higher grades of IMVF signal on the semi-quantitative-SMI visual scale had significantly higher values of circulating FGF-23 levels (p=0.011, r=0.466) (Figure 1). Neo-vessel count recorded by quantitative SMI was also positively correlated to higher circulatory FGF-23 levels (p=0.007, r= 0.491) (Figure 2). Patients with lower eGFR had statistically higher plasma level FGF-23 (p=0.030, r= -0.347) and higher neo-vessel counts on SMI (p= 0.030, r=-0.403). Including FGF-23 and eGFR, regression analyses indicated that the model explained 30% of the variance and was a significant predictor of intraplaque neo-vessel count assessed by SMI, F (2.26) = 5.5, p< 0.001. While plasma level of FGF-23 alone significantly predicted SMI-assessed intraplaque neo-vessel count (β= 0.389, p= 0.04), eGFR did not (β= -0.256, p=0.163).
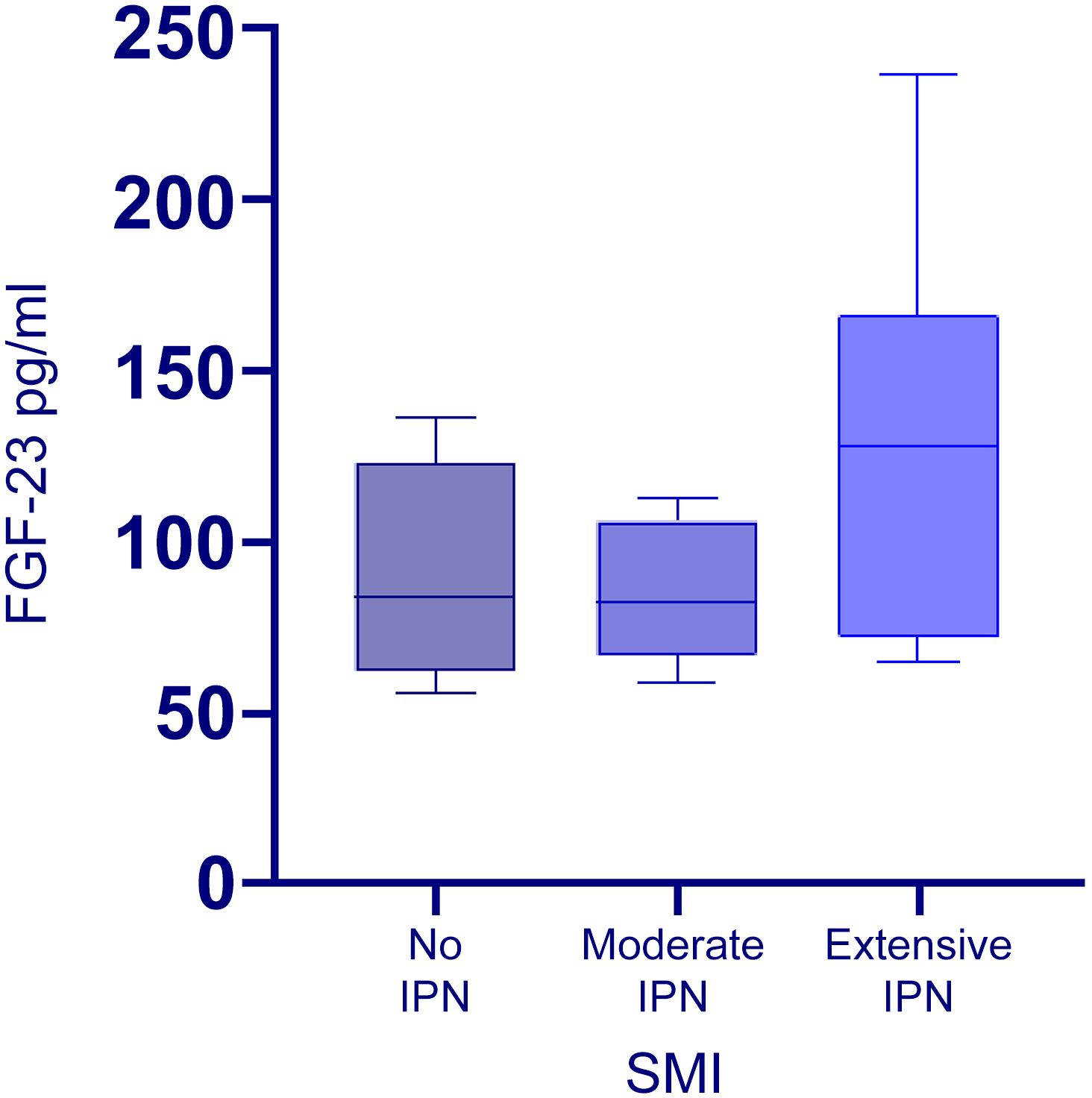
Figure 1 Box plot showing median serum level FGF-23 distribution in patients with no IPN, moderate IPN, and extensive IPN on SMI. Horizontal lines in boxes represent the median levels (second quartile), and the whiskers are the range limits. The median plasma level FGF-23 was respectively 84.2 (range 55.8-136.2), 78.1 (range 58.5-112.7) and 132.8 (range 64.9-236.5).
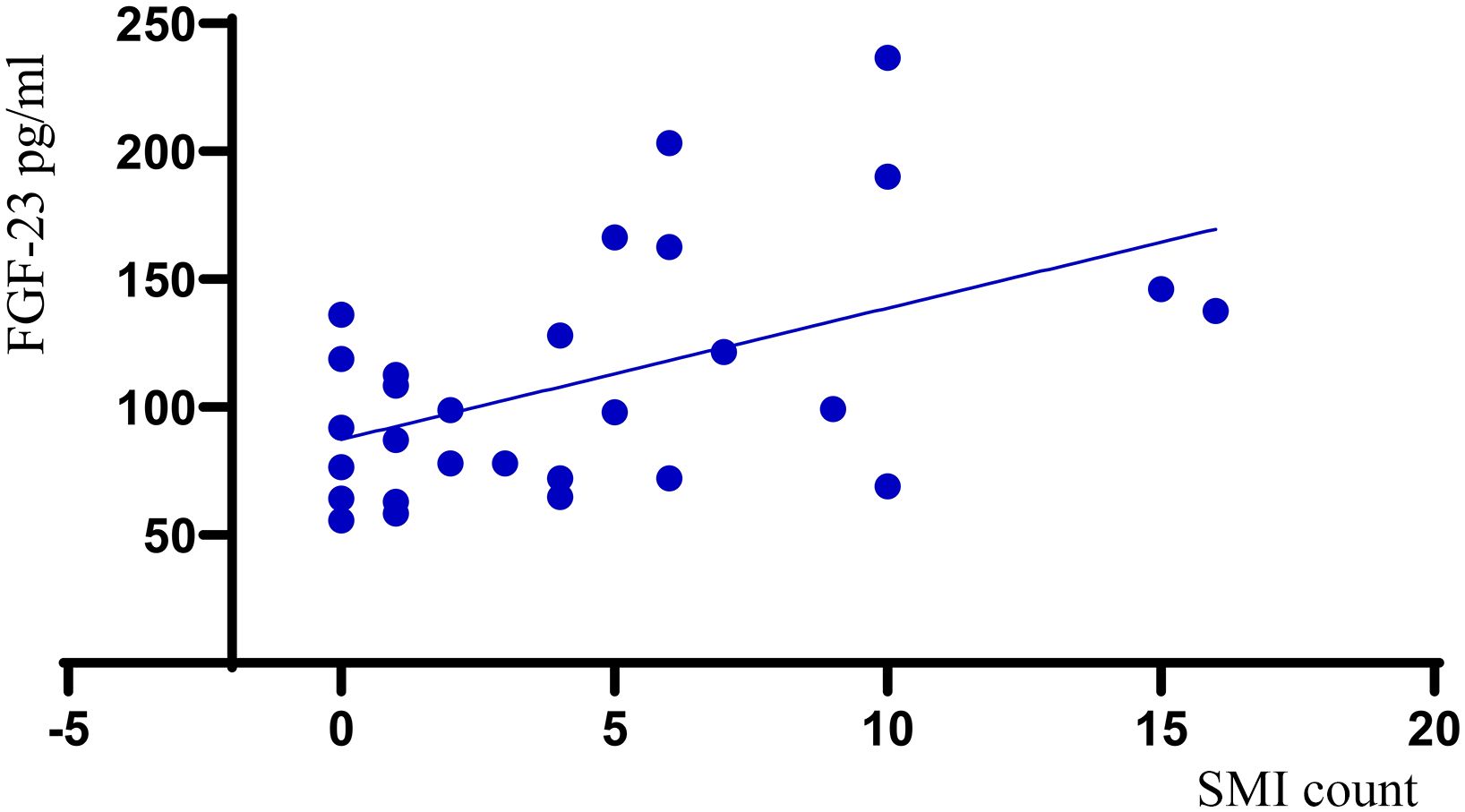
Figure 2 Scatter plot demonstrating the relationship between FGF-23 values and quantitative SMI (SMI count).
We next employed the Kruskal-Wallis test to assess whether there are significant differences in FGF-23 values across the three visual SMI classification groups. Whereas the Kruskal-Wallis test yielded a significant result (H=7.23, df = 2, p= 0.027), the post hoc pairwise comparison revealed significant differences in FGF-23 values between patients with moderate IPN and those with extensive IPN (p= 0.016) and trend for significant differences between no IPN and extensive IPN groups (p=0.052). These results further support higher values of FGF-23 among patients with extensive IPN assessed with SMI compared to the other groups. There was no differences in baseline variables in the three SMI IPN groups (Supplementary Table S1).
In contrast to FGF-23, there was no significant relation between b-FGF and quantitative and semi-quantitative SMI-assessed IPN (p=0.598, r=0.106 and p=0.577, r=-0.084, respectively).
To further analyze if the associations of FGF-23 and IPN merely reflect activation of inflammatory pathway, we analyzed the levels of IL-6 and TNF-α, two prototypical inflammatory cytokines. However, in contrast to FGF-23, plasma levels of these cytokines showed no correlation with quantitative and semi-quantitative SMI-assessed IPN (p=0,482, r=-0.136, p=0.370, r=-0.173 and p=0,723, r=0.069, p= 0.765, r=0.058, respectively).
No correlation between plasma FGF-23 and traditional cardiovascular risk factors
No statistically significant relationship was found between plasma level FGF-23 and traditional risk factors for CVD (hypertension, hypercholesterolemia, diabetes mellitus, and smoking) or plasma levels of total cholesterol, HDL/LDL ratio, Triglycerides, CRP. (Supplementary Table S2). Moreover, in contrast to FGF-23 these risk factors were not associated with quantitative and semi-quantitative SMI-assessed IPN (Supplementary Table S2).
Discussion
In this pilot study we investigated the association between plasma level FGF-23 and atherosclerotic carotid plaque IPN assessed by SMI both semi-quantitatively and quantitatively. Our main and novel findings were: i) plaques with higher grades of IMVF signal on semi-quantitative SMI visual scale assessment of IPN, had significantly increased levels of circulating FGF-23 levels, ii) patients in Extensive-IPN group assessed with semi-quantitative SMI had increased plasma levels of FGF-23 compared to the other patient groups (No-IPN group and Moderate-IPN group) iii) Neo-vessel count recorded by quantitative SMI was positively correlated to increased plasma level FGF-23 levels and this association remained significant after adjusting for eGFR iv) FGF-23 did not correlate with traditional risk factors for CVD, and in contrast to FGF-23, these risk factors did not correlate with SMI-assessed IPN.
An association between circulatory FGF-23 and unstable carotid plaque has previously been reported by Biscetti et al. in patients with type two diabetes mellitus, using histological assessment of plaque after endarterectomy (14). To the best of our knowledge, the current report is the first to demonstrate increased plasma level FGF-23 to be independently associated with increased SMI-assessed IPN, an essential sign of plaque instability in a population with carotid atherosclerosis. Importantly, in the current cohort, only 13.8% had diabetes, and 10.3% had CKD. The association of FGF-23 with SMI-assessed IPN was also seen after adjusting for eGFR. In contrast, other risk markers for plaque instability, such as an unfavorable risk profile and systemic inflammation—as assessed by CRP and prototypical cytokines TNF-α and IL-6—were not associated with SMI-assessed IPN.
Previous studies have shown that FGF-23 is an independent predictor of cardiovascular events in the community (11, 15, 16), and even in a population at high risk of CVD with intact phosphate-FGF-23-calcitriol system (10) raising the question of whether circulating FGF-23 may reflect novel and important aspects of cardiovascular risk yet to be unraveled and may possibly be involved in vascular pathology. Nirav et al. showed a clear relationship between FGF-23 and the presence of atherosclerotic plaque and size, studying 1512 stroke-free participants with FGF-23 serum levels and 2D carotid ultrasound data available (11). There were, however, no records of the degree of stenosis or hemodynamic effect of plaques nor any assessment of plaque morphology. In another study, Rodríguez-Ortiz et al. showed that increased vessel wall intima-media thickness (IMT) was significantly associated with higher median serum level FGF-23 (10); however, IMT measurements were done at common carotid arteries. It is well known that the most prevalent site for pre-cranial carotid artery atherosclerosis is at the carotid artery bifurcation alongside the proximal internal carotid artery (17). To our knowledge, the present study is the first to show higher levels of plasma FGF-23 in patients with higher SMI neo-vessel count and IPN visual grades as a sign of plaque instability, more clearly linking FGF-23 levels to plaque destabilization of carotid atherosclerosis.
Pathophysiology of atherosclerosis is a complex interaction of cellular elements (e.g., platelets, monocytes/macrophages, lymphocytes, endothelial cells, and smooth muscle cells) acting locally and systemically involving a bidirectional interaction between lipids and inflammation. Whereas most previous studies on FGF-23 are performed on subclinical carotid plaques or without complete ultrasonographic examination, the present study suggests that FGF-23 could be one of the contributing factors to plaque progression and induction of plaque instability. Notably, we found no association between basic FGF (b-FGF) and SMI-assessed IPN, suggesting that this property is more specific for FGF-23.
The mechanisms by which FGF-23 may induce plaque instability are not clear. However, Klotho, the FGF-23 obligate co-receptor, is expressed in human vascular tissue (18), and both Klotho and FGF-23 regulate vascular tone (19). Moreover, although FGF-23 displays the highest expression in bone, it can also be detected in other organs, including the brain, heart, intestine, and skeletal muscle (20), and notably, the FGF receptors, FGFR1 and FGFR4 are expressed in tunica media of several arteries and veins including heart microvessels (21). Moreover, Del Porto et al. detected FGF-23 inside the atherosclerotic plaque after endarterectomy and plaque immunohistochemistry (22).
The main limitation of this study is the sample size, which is too small to make any firm conclusion. Moreover, although the association of FGF-23 and IPN was not seen for CRP a reliable marker of general inflammation and prototypical cytokines IL-6 and TNF-α, we cannot exclude that other molecules related to inflammation and fibrogenesis could be of more importance than FGF-23. Forthcoming studies should therefor include the analyses of other potential markers that could be related to IPN as well as analyses within the plaques. The strengths are the well-clinically defined group, including the advanced and accurate carotid ultrasound examinations.
Conclusion
This pilot study adds knowledge on the association between plasma FGF-23 levels and atherosclerotic carotid plaque neovascularization, underscoring the potential of FGF-23 as a valuable marker for neovascularization and atherosclerotic carotid plaque instability and a risk factor for ischemic stroke. Further research, including larger validation cohorts and prospective data about clinical outcomes, is needed to clarify the role of FGF-23 as a marker and potentially also a mediator and novel therapeutic target in carotid atherosclerosis.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Norwegian Regional Committee for Medical and Health Research Ethics (ID REC 2014/1468). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MZ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. KS: Conceptualization, Formal analysis, Methodology, Supervision, Validation, Writing – review & editing. BL: Investigation, Writing – review & editing. VB: Formal analysis, Resources, Writing – review & editing. PA: Conceptualization, Methodology, Supervision, Validation, Visualization, Writing – review & editing. BH: Conceptualization, Formal analysis, Resources, Visualization, Writing – review & editing. MS: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study is funded by South-Eastern Norway Regional Health Authority (ID 2010011).
Acknowledgments
This paper is dedicated to the memory of our dear colleague, Professor David Russell, who sadly passed away on April 20, 2022. He was a driving force behind the idea and plan for this study, and his groundbreaking contributions have cemented his legacy as a true pioneer in stroke research. Also, we would like to thank Ellen Sagen for laboratory assistance.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1385377/full#supplementary-material
References
1. Johnson CO, Nguyen M, Roth GA, Nichols E, Alam T, Abate D, et al. Global, regional, and national burden of stroke, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. (2019) 18:439–58. doi: 10.1016/S1474-4422(19)30034-1
2. Moreno PR, Purushothaman KR, Fuster V, Echeverri D, Truszczynska H, Sharma SK, et al. Plaque neovascularization is increased in ruptured atherosclerotic lesions of human aorta: implications for plaque vulnerability. Circulation. (2004) 110:2032–8. doi: 10.1161/01.CIR.0000143233.87854.23
3. Van der Veken B, De Meyer GR, Martinet W. Intraplaque neovascularization as a novel therapeutic target in advanced atherosclerosis. Expert Opin Ther Targets. (2016) 20:1247–57. doi: 10.1080/14728222.2016.1186650
4. Michel J-B, Martin-Ventura JL, Nicoletti A, Ho-Tin-Noé B. Pathology of human plaque vulnerability: mechanisms and consequences of intraplaque haemorrhages. Atherosclerosis. (2014) 234:311–9. doi: 10.1016/j.atherosclerosis.2014.03.020
5. Zamani M, Skagen K, Scott H, Lindberg B, Russell D, Skjelland M. Carotid plaque neovascularization detected with superb microvascular imaging ultrasound without using contrast media. Stroke. (2019) 50:3121–7. doi: 10.1161/STROKEAHA.119.025496
6. Shimada T, Hasegawa H, Yamazaki Y, Muto T, Hino R, Takeuchi Y, et al. FGF-23 is a potent regulator of vitamin D metabolism and phosphate homeostasis. J Bone mineral Res. (2004) 19:429–35. doi: 10.1359/JBMR.0301264
7. Shalhoub V, Ward S, Sun B, Stevens J, Renshaw L, Hawkins N, et al. Fibroblast growth factor 23 (FGF23) and alpha-klotho stimulate osteoblastic MC3T3. E1 cell proliferation and inhibit mineralization. Calcified Tissue Int. (2011) 89:140–50. doi: 10.1007/s00223-011-9501-5
8. Isakova T, Xie H, Yang W, Xie D, Anderson AH, Scialla J, et al. Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. Jama. (2011) 305:2432–9. doi: 10.1001/jama.2011.826
9. Marthi A, Donovan K, Haynes R, Wheeler DC, Baigent C, Rooney CM, et al. Fibroblast growth factor-23 and risks of cardiovascular and noncardiovascular diseases: a meta-analysis. J Am Soc Nephrol. (2018) 29:2015–27. doi: 10.1681/ASN.2017121334
10. Rodríguez-Ortiz ME, Alcalá-Díaz JF, Canalejo A, Torres-Peña JD, Gómez-Delgado F, Muñoz-Castañeda JR, et al. Fibroblast growth factor 23 predicts carotid atherosclerosis in individuals without kidney disease. The CORDIOPREV study. Eur J Internal Med. (2020) 74:79–85. doi: 10.1016/j.ejim.2019.12.008
11. Shah NH, Dong C, Elkind MS, Sacco RL, Mendez AJ, Hudson BI, et al. Fibroblast growth factor 23 is associated with carotid plaque presence and area: the Northern Manhattan Study. Arteriosclerosis thrombosis Vasc Biol. (2015) 35:2048–53. doi: 10.1161/ATVBAHA.115.305945
12. Grant EG, Benson CB, Moneta GL, Alexandrov AV, Baker JD, Bluth EI, et al. Carotid artery stenosis: gray-scale and Doppler US diagnosis—Society of Radiologists in Ultrasound Consensus Conference. Radiology. (2003) 229:340–6. doi: 10.1148/radiol.2292030516
13. Gray-Weale A, Graham J, Burnett J, Byrne K, Lusby R. Carotid artery atheroma: comparison of preoperative B-mode ultrasound appearance with carotid endarterectomy specimen pathology. J Cardiovasc Surg. (1988) 29:676–81.
14. Biscetti F, Straface G, Porreca CF, Bertoletti G, Vincenzoni C, Snider F, et al. Increased FGF23 serum level is associated with unstable carotid plaque in type 2 diabetic subjects with internal carotid stenosis. Cardiovasc Diabetol. (2015) 14:1–7. doi: 10.1186/s12933-015-0301-5
15. Ärnlöv J, Carlsson AC, Sundström J, Ingelsson E, Larsson A, Lind L, et al. Serum FGF23 and risk of cardiovascular events in relation to mineral metabolism and cardiovascular pathology. Clin J Am Soc Nephrology: CJASN. (2013) 8:781. doi: 10.2215/CJN.09570912
16. Hu X, Ma X, Luo Y, Xu Y, Xiong Q, Pan X, et al. Contribution of fibroblast growth factor 23 to Framingham risk score for identifying subclinical atherosclerosis in Chinese men. Nutrition Metab Cardiovasc Dis. (2017) 27:147–53. doi: 10.1016/j.numecd.2016.11.009
17. Prasad K. Pathophysiology and medical treatment of carotid artery stenosis. Int J Angiology. (2015) 24:158–72. doi: 10.1055/s-00000167
18. Lim K, Lu T-S, Molostvov G, Lee C, Lam F, Zehnder D, et al. Vascular Klotho deficiency potentiates the development of human artery calcification and mediates resistance to fibroblast growth factor 23. Circulation. (2012) 125:2243–55. doi: 10.1161/CIRCULATIONAHA.111.053405
19. Mirza MA, Larsson A, Lind L, Larsson TE. Circulating fibroblast growth factor-23 is associated with vascular dysfunction in the community. Atherosclerosis. (2009) 205:385–90. doi: 10.1016/j.atherosclerosis.2009.01.001
20. Quarles LD. FGF-23 and α-Klotho co-dependent and independent functions. Curr Opin Nephrol hypertension. (2019) 28:16. doi: 10.1097/MNH.0000000000000467
21. Hughes SE. Differential expression of the fibroblast growth factor receptor (FGFR) multigene family in normal human adult tissues. J Histochem Cytochem. (1997) 45:1005–19. doi: 10.1177/002215549704500710
Keywords: atherosclerosis, unstable carotid artery plaque, intraplaque neovascularization (IPN), superb microvascular imaging (SMI), fibroblast growth factor-23, ischemic stroke, intraplaque hemmorhage
Citation: Zamani M, Skagen K, Lindberg B, Bjerkeli V, Aukrust P, Halvorsen B and Skjelland M (2024) Relationship between fibroblast growth factor in plasma and carotid plaque neovascularization: a pilot study. Front. Immunol. 15:1385377. doi: 10.3389/fimmu.2024.1385377
Received: 12 February 2024; Accepted: 08 April 2024;
Published: 22 April 2024.
Edited by:
Chao Li, China Medical University, ChinaReviewed by:
Hiroya Ohta, Hokkaido University of Science, JapanIvana Kawikova, University of Hartford, United States
Copyright © 2024 Zamani, Skagen, Lindberg, Bjerkeli, Aukrust, Halvorsen and Skjelland. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mahtab Zamani, TWF0emFtQG91cy1oZi5ubw==