
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Immunol. , 13 May 2024
Sec. Vaccines and Molecular Therapeutics
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1382944
 Eliel Nham1,2
Eliel Nham1,2 Jang Wook Sohn1,2Won Suk Choi1,2Seong-Heon Wie3Jacob Lee4Jin-Soo Lee5Hye Won Jeong6Joong Sik Eom7Yu Jung Choi1,2Hye Seong1,2Jin Gu Yoon1,2Ji Yun Noh1,2
Jang Wook Sohn1,2Won Suk Choi1,2Seong-Heon Wie3Jacob Lee4Jin-Soo Lee5Hye Won Jeong6Joong Sik Eom7Yu Jung Choi1,2Hye Seong1,2Jin Gu Yoon1,2Ji Yun Noh1,2 Joon Young Song1,2
Joon Young Song1,2 Hee Jin Cheong1,2
Hee Jin Cheong1,2 Woo Joo Kim1,2*
Woo Joo Kim1,2*As coronavirus disease-2019 (COVID-19) becomes an endemic disease, the virus continues to evolve and become immunologically distinct from previous strains. Immune imprinting has raised concerns about bivalent mRNA vaccines containing both ancestral virus and Omicron variant. To increase efficacy against the predominant strains as of the second half of 2023, the updated vaccine formulation contained only the mRNA of XBB.1.5 sublineage. We conducted a multicenter, test-negative, case-control study to estimate XBB.1.5 monovalent vaccine effectiveness (VE) and present the results of an interim analysis with data collected in November 2023. Patients who underwent COVID-19 testing at eight university hospitals were included and matched based on age (19-49, 50-64, and ≥65 years) and sex in a 1:1 ratio. VE was calculated using the adjusted odds ratio derived from multivariable logistic regression. Of the 992 patients included, 49 (5.3%) received the XBB.1.5 monovalent vaccine at least 7 days before COVID-19 testing. Patients with COVID-19 (cases) were less likely to have received the XBB.1.5 monovalent vaccine (case 3.5% vs. control 7.2%, p=0.019) and to have a history of COVID-19 within 6 months (2.2% vs. 4.6%, p=0.068). In contrast, patients with COVID-19 were more likely to be healthcare workers (8.2% vs. 3.0%, p=0.001) and to have chronic neurological diseases (16.7% vs. 11.9%, p=0.048). The adjusted VE of the XBB.1.5 monovalent mRNA vaccine was 56.8% (95% confidence interval: 18.7-77.9%). XBB.1.5 monovalent mRNA vaccine provided significant protection against COVID-19 in the first one to two months after vaccination.
Since its first emergence in late 2019, the ever-changing nature of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has made previous immunity acquired through infection or vaccines based on ancestral SARS-CoV-2 less effective. This immune evasion became more apparent with the emergence of the Omicron variant and its sublineages since late 2021 (1–3). To combat this, bivalent vaccines containing the mRNA of both ancestral SARS-CoV-2 and Omicron variant were administered as a booster shot in 2022. However, near-total replacement of the ancestral SARS-CoV-2 by the Omicron variant and the phenomenon of immune imprinting have raised questions about the utility of including the mRNA of the ancestral SARS-CoV-2 in future coronavirus disease 2019 (COVID-19) vaccines (4–8).
In mid-2023, the World Health Organization and the United States (US) Food and Drug Administration advised pharmaceutical companies to only include component of the XBB lineage (“monovalent”) in the updated COVID-19 vaccines for the 2023/2024 season (9, 10). XBB-monovalent vaccines were also recommended by the Advisory Committee on Immunization Practices for the corresponding season, serving as both a booster dose and primary series, for all persons aged six months or older (11).
Similar to influenza vaccines, vaccine efficacy reports are not required for these updated vaccines before authorization. Although it has become essential to monitor the effectiveness of COVID-19 vaccines, studies on this matter are scarce. To fill this knowledge gap, we aimed to investigated COVID-19 XBB.1.5 monovalent mRNA vaccine effectiveness in Korea. This is an interim analysis of data collected through a network of tertiary teaching hospitals created to monitor respiratory infectious diseases since 2011 (12).
This is a retrospective, multicenter, test-negative, case-control study. Patients aged 19 years or older who underwent COVID-19 testing at eight participating hospitals (mostly located in the Seoul Metropolitan Area) were included. Individuals who were tested for COVID-19 as part of pre-admission surveillance (i.e., without clinical or epidemiological risk factors for COVID-19) were excluded. Cases were defined as patients who tested positive for COVID-19 using reverse transcription polymerase chain reaction (RT-PCR) or a lateral flow assay with nasopharyngeal swab samples. Those that tested negative were classified as controls. The limit of detection for the RT-PCR test and RAT we used is 5,000 copies/mL and 2.5×101.8 TCID50/mL, respectively. For SARS-CoV-2, 2.5×101.8 TCID50/mL falls in the range between 5×105–1×106 copies/mL (13). The LOD value of RAT meets the WHO requirement of 100–1,000 TCID50/mL. For this interim analysis, data collected in November 2023 were included.
The case and control groups were matched based on age (19–49, 50–64, and ≥65 years) and sex in a 1:1 ratio. Information on demographics, COVID-19 vaccination history, recent history of COVID-19, comorbidities, symptoms, and clinical outcomes was collected through chart review. The vaccination status was verified using the National Immunization Registry of the Korean Disease Control and Prevention Agency. The vaccine was considered effective if administered at least seven days before the date of COVID-19 testing. In Korea, two mRNA vaccines were available (Comirnaty Omicron XBB.1.5, Spikevax XBB.1.5) since October 19, 2023. Comirnaty and Spikevax are mRNA vaccines manufactured by Pfizer-BioNTech (New York, NY, USA and Mainz, Germany) and Moderna (Cambridge, MA, USA), respectively. Each vaccine contains 30 μg/0.3mL and 50 μg/0.5mL of mRNA encoding the spike protein of SARS-CoV-2 Omicron XBB.1.5 sublineage. Both vaccines were administered intramuscularly.
Categorical variables were compared using the chi-square test or Fisher’s exact test. In addition to receipt of the XBB.1.5 monovalent vaccine, the following variables were included in the multivariable logistic regression: age, sex, comorbidities, receipt of bivalent vaccination in 2022, recent history of COVID-19, and being a healthcare worker. We then removed variables with p values greater than 0.15 from the multivariable model (backward selection). Multicollinearity between variables was defined as a variance inflation factor greater than 10. The goodness of fit of the regression model was examined using the Hosmer–Lemeshow test. Vaccine effectiveness (VE) was calculated using the adjusted odds ratio derived from the multivariable logistic regression (1-adjusted odds ratio). Statistical significance was defined as p < 0.05. Statistical analyses were performed using the R software (version 4.3.1; R Foundation, Vienna, Austria).
This study was reviewed and approved by the Institutional Review Board (IRB) of each participating hospital: Korea University Guro Hospital (approval no. 2022GR0360), Korea University Anam Hospital (2022AN0449), Korea University Ansan Hospital (2022AS0226), St. Vincent’s Hospital (VC22TIDI0150), Kangnam Sacred Heart Hospital (HKS 2022-07-016), Inha University Hospital (2022-07-036), Chungbuk National University Hospital (2022-08-022), and Gil Medical Center (GAIRB2022-306). The requirement for written informed consent was waived because of the retrospective nature of this study.
A total of 992 patients were included in the study. Information on the baseline characteristics and clinical outcomes is summarized in Tables 1 and 2. Among them, 49 (5.3%) received the XBB.1.5 monovalent mRNA vaccine at least seven days before the date of COVID-19 testing. The median time since vaccination to COVID-19 testing was 18 days (range, 7–36 days; interquartile range, 12–27 days). Two hundred and four (22.1%) patients received BA.1 (n=89, 45.1%) or BA.4/5 (n=112, 54.9%) bivalent COVID-19 mRNA vaccine during the 2022/2023 season. Thirty-one patients (3.4%) reported a history of COVID-19 within six months. Those with at least one comorbidity accounted for 58.4% (n=538); diabetes mellitus (n=216, 23.4%), cardiovascular disease (148, 6.1%), and chronic neurologic disease (n=132, 14.3%) were the most common comorbidities. Out of 538, 211 (39%) was younger than 65 years and 327 (61%) was 65 years or older. Four hundred and forty-five (48.3%) patients were hospitalized and 20 (2.2%) died during hospitalization.
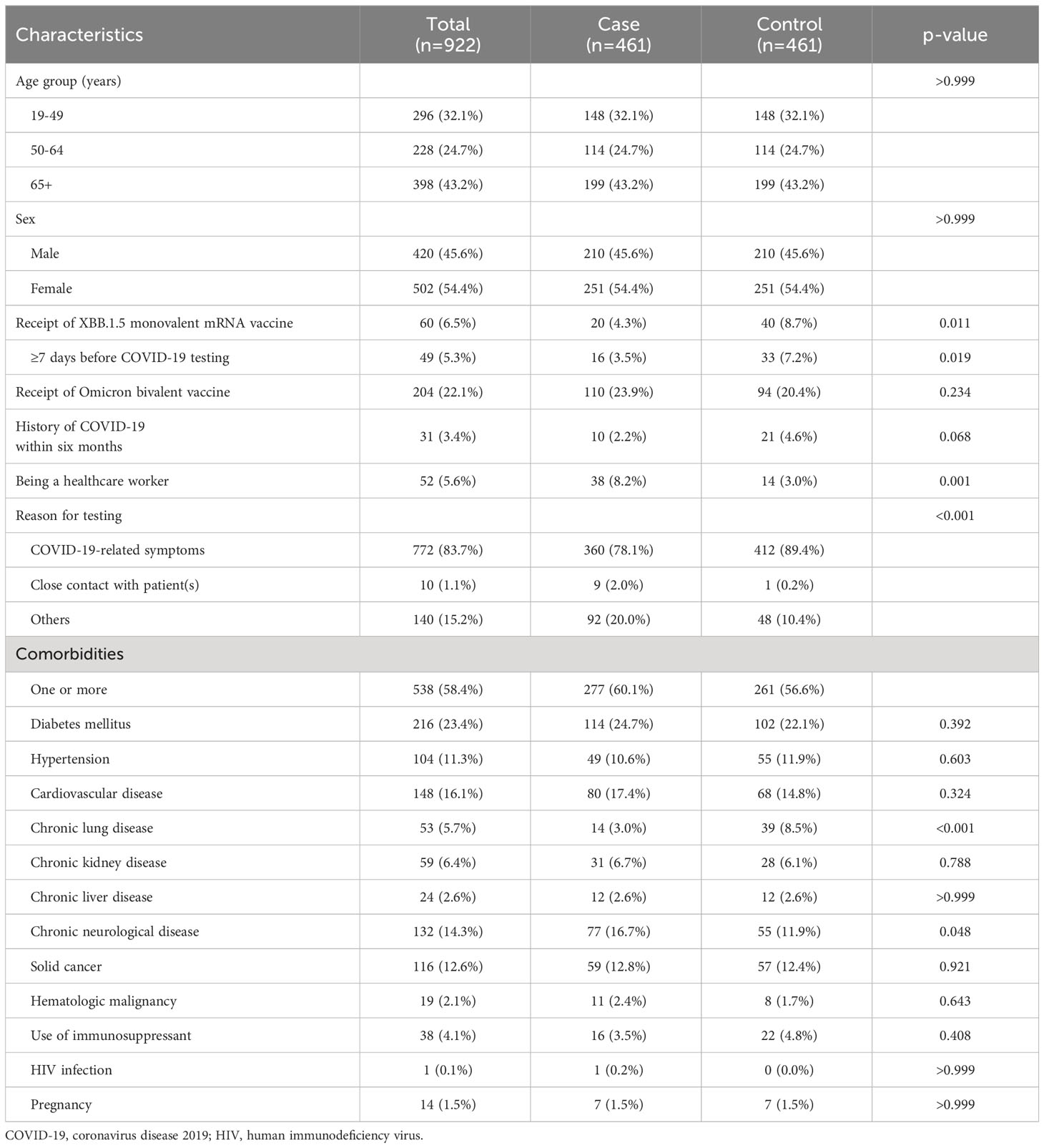
Table 1 Baseline characteristics of study population.
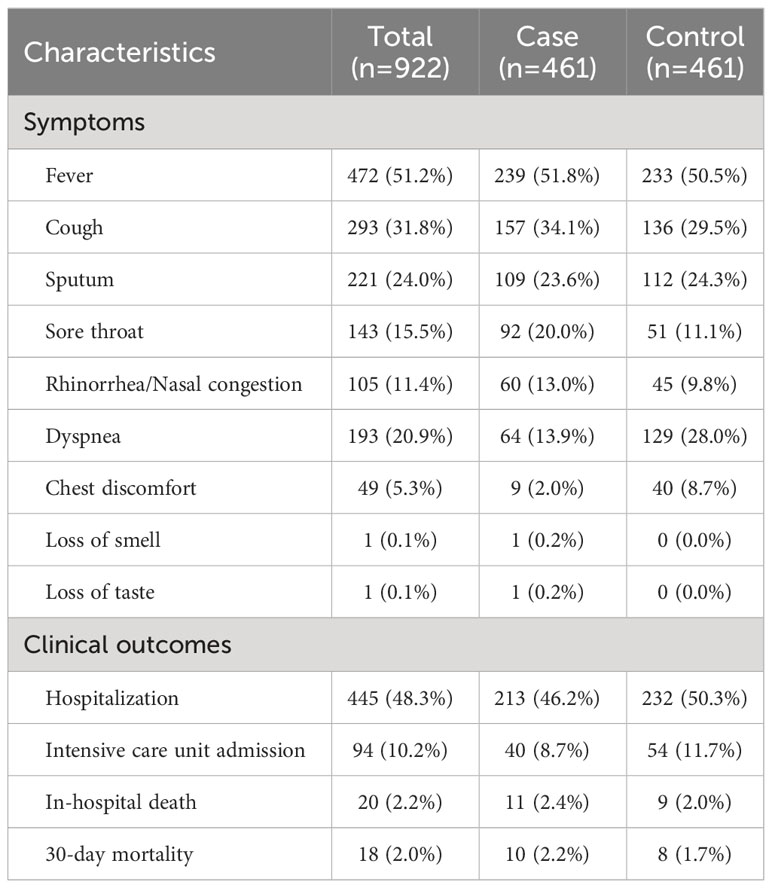
Table 2 Clinical outcomes of study population.
Compared to patients without COVID-19, lesser number of patients with COVID-19 received the XBB.1.5 monovalent vaccine at least seven days before the date of COVID-19 testing (case 3.5% vs. control 7.2%, p=0.019), have a history of COVID-19 within 6 months (2.2% vs. 4.6%, p=0.068), or have chronic pulmonary disease (3.0% vs. 8.5%, p<0.001). In contrast, case patients were more likely to be healthcare workers (8.2% vs. 3.0%, p=0.001) and have chronic neurological disease (16.7% vs. 11.9%, p=0.048). The adjusted VE of the XBB.1.5 monovalent mRNA vaccine was 56.8% (95% confidence interval: 18.7–77.9%, p = 0.011) (Table 3). The Hosmer-Lemeshow test showed that our model provided a good fit to the data (p = 0.988).
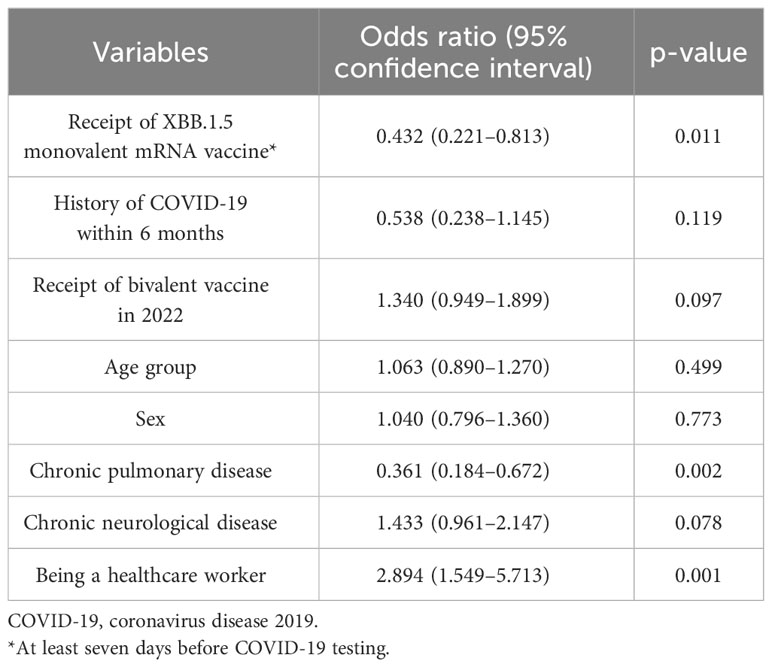
Table 3 Results of multivariable logistic regression analysis.
We found that the XBB.1.5 monovalent mRNA vaccine conferred significant protection against COVID-19 in the first month after vaccination. To the best of our knowledge, this is the first study on XBB.1.5 monovalent VE against symptomatic COVID-19 outside the US as of February 5, 2024, at which this manuscript was submitted for publication. Our results are in line with the most recent US study, which reported 54% of early VE estimate in adults (14).
As it has become clear that COVID-19 is here to stay despite rapid development and distribution of effective vaccines, questions regarding future vaccination strategies have been raised. To improve immunogenicity against the immune-evasive Omicron variant and its sublineages, the first updated “bivalent” vaccine was developed in 2022. However, the bivalent vaccine did not appear to have better immunogenicity against the Omicron variant than the monovalent vaccine based on the ancestral SARS-CoV-2 (7, 15). This has led to the development of XBB-based monovalent vaccines in 2023 to increase the XBB antigen dose and avoid immune imprinting. To date, studies on this novel COVID-19 vaccine are limited. The only study that compared the immunogenicity of XBB.1.5 monovalent and bivalent (XBB.1.5 and BA.4/5) mRNA vaccines found that the monovalent vaccines were not significantly more immunogenic than the bivalent vaccine (16). Because this study was not powered to detect statistical significance, whether a monovalent vaccine would be a better choice in the future remains uncertain.
In addition to the controversy surrounding antigen doses in updated vaccines, there is an ongoing debate regarding the necessity of annual update of the COVID-19 vaccine itself. XBB.1.5 monovalent mRNA vaccines are immunogenic against emerging Omicron sublineages, including EG.5.1, HV.1, and JN.1 (16, 17). Our findings are consistent with this, considering HK.3 and EG.5 accounted for 87% of circulating sublineages during the study period (18). While studies conducted to date, including ours, suggested that XBB.1.5 monovalent vaccines were effective in preventing laboratory-confirmed COVID-19 or COVID-19-related hospitalization, cautious interpretation is needed because all of these studies only included the early post-vaccination period (14, 19, 20). More data from longer observation periods are required to establish future vaccination strategies.
There was a remarkable difference in the number of patients who experienced COVID-19-related symptoms between the case and control group. Symptoms that occurred more frequently in the control group were dyspnea (case 64 [14%] vs. control 129 [28%]) and chest discomfort (case 9 [2%] vs control 40 [9%]). This may be partly explained by the greater number of patients with chronic lung disease in the control group (case 14 [3%] vs. control 39 [9%]). Other respiratory pathogens such as influenza virus, respiratory syncytial virus, adenovirus and Mycoplasma pneumoniae that had been circulating in the community during the study period could have been the cause as well (21).
This study has several limitations. First, owing to the retrospective nature of the study, some confounders may have remained unadjusted. Second, we did not collect data on the exact number of prior COVID-19 vaccinations, which may have been a protective factor. However, this effect is likely to be small because 1) most Korean adults had completed primary series vaccination (96.6% were vaccinated twice and 75.2% three times as of October 28, 2022); 2) 78.6% of the Korean population had acquired natural immunity by contracting COVID-19 (due to any SARS-CoV-2 variant) as of August 31, 2023, which seems to be an undercount; and 3) neutralizing antibody levels after vaccination or infection wane after several months, making remote vaccination or infection less protective, especially less severe ones (22–25). Third, although the control group exclusively comprised symptomatic individuals, the case group included some asymptomatic persons (close contacts with COVID-19 cases), making the two groups less comparable in terms of healthcare-seeking behaviors. Fourth, the use of lateral flow assay, which is less sensitive than RT-PCR, may have overlooked some COVID-19 cases.
In conclusion, the XBB.1.5 monovalent mRNA vaccine provided significant protection against COVID-19 in the first month after vaccination. Full analysis results will be followed.
The datasets presented in this article are not readily available because of the institutional bans on the export of clinical data. Requests to access the datasets should be directed to WK,d2praW1Aa29yZWEuYWMua3I=.
The studies involving humans were approved by Institutional Review Board of: Korea University Guro Hospital, Korea University Anam Hospital, Korea University Ansan Hospital, St. Vincent’s Hospital, Kangnam Sacred Heart Hospital, Inha University Hospital, Chungbuk National University Hospital, and Gil Medical Center. The studies were conducted in accordance with the local legislation and institutional requirements The requirement for written informed consent was waived because of the retrospective nature of this study.
EN: Data curation, Investigation, Formal analysis, Writing – original draft, Writing – review, Supervision. JWS: Data curation, Investigation, Writing – review. WSC: Data curation, Investigation, Writing – review. SHW: Data curation, Investigation, Writing – review. JL: Data curation, Investigation, Writing – review. JSL: Data curation, Investigation, Writing – review. HWJ: Data curation, Investigation, Writing – review. JSE: Data curation, Investigation, Writing – review. YJC: Investigation, Writing – review. HS: Investigation, Writing – review. JGY: Investigation, Writing – review. JYN: Investigation, Writing – review. JYS: Conceptualization, Methodology, Investigation, Writing – original draft, Writing – review, Supervision. HJC: Investigation, Writing – review. WJK: Conceptualization, Investigation, Writing – review, Supervision.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The authors declared that this study received funding from SK Bioscience CO., Ltd. The funder was not involved in the study design, data collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
We appreciate Dr. Soon Young Hwang at the Department of Biostatistics, Korea University College of Medicine, for her advice on statistical analysis.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Dejnirattisai W, Huo J, Zhou D, Zahradník J, Supasa P, Liu C, et al. SARS-CoV-2 Omicron-B.1.1.529 leads to widespread escape from neutralizing antibody responses. Cell. (2022) 185:467–84.e15. doi: 10.1016/j.cell.2021.12.046
2. Wang Q, Iketani S, Li Z, Liu L, Guo Y, Huang Y, et al. Alarming antibody evasion properties of rising SARS-CoV-2 BQ and XBB subvariants. Cell. (2023) 186:279–86.e8. doi: 10.1016/j.cell.2022.12.018
3. Nham E, Kim J, Lee J, Park H, Kim J, Lee S, et al. Low neutralizing activities to the omicron subvariants BN.1 and XBB.1.5 of sera from the individuals vaccinated with a BA.4/5-containing bivalent mRNA vaccine. Immune Netw. (2023) 23:e43. doi: 10.4110/in.2023.23.e43
4. Offit PA. Bivalent covid-19 vaccines — A cautionary tale. N Engl J Med. (2023) 481–83. doi: 10.1056/NEJMp2215780
5. Reynolds CJ, Pade C, Gibbons JM, Otter AD, Lin KM, Muñoz Sandoval D, et al. Immune boosting by B.1.1.529 (Omicron) depends on previous SARS-CoV-2 exposure. Science. (2022) 377:eabq1841. doi: 10.1126/science.abq1841
6. Carreño JM, Singh G, Simon V, Krammer F. Bivalent COVID-19 booster vaccines and the absence of BA.5-specific antibodies. Lancet Microbe. (2023) e569. doi: 10.1016/S2666-5247(23)00118-0
7. Collier AY, Miller J, Hachmann NP, McMahan K, Liu J, Bondzie EA, et al. Immunogenicity of BA.5 bivalent mRNA vaccine boosters. N Engl J Med. (2023) 388:565–7. doi: 10.1056/NEJMc2213948
8. Wang Q, Bowen A, Valdez R, Gherasim C, Gordon A, Liu L, et al. Antibody response to omicron BA.4–BA.5 bivalent booster. N Engl J Med. (2023) 388:567–9. doi: 10.1056/NEJMc2213907
9. World Health Organisation. Statement on the antigen composition of COVID-19 vaccines [updated May 18, 2023. Available at: https://www.who.int/news/item/18-05-2023-statement-on-the-antigen-composition-of-covid-19-vaccines.
10. Food and Drug Administration. Updated COVID-19 Vaccines for Use in the UNITED STATES Beginning in Fall 2023 [updated Jun 16, 2023. Available at: https://www.fda.gov/vaccines-blood-biologics/updated-covid-19-vaccines-use-united-states-beginning-fall-2023?source=email.
11. Regan JJ, Moulia DL, Link-Gelles R, Godfrey M, Mak J, Najdowski M, et al. Use of updated COVID-19 vaccines 2023-2024 formula for persons aged ≥6 months: recommendations of the advisory committee on immunization practices - United States, September 2023. MMWR Morb Mortal Wkly Rep. (2023) 72:1140–6. doi: 10.15585/mmwr.mm7242e1
12. Song JY, Cheong HJ, Choi SH, Baek JH, Han SB, Wie SH, et al. Hospital-based influenza surveillance in Korea: hospital-based influenza morbidity and mortality study group. J Med Virol. (2013) 85:910–7. doi: 10.1002/jmv.23548
13. Liotti FM, Menchinelli G, Lalle E, Palucci I, Marchetti S, Colavita F, et al. Performance of a novel diagnostic assay for rapid SARS-CoV-2 antigen detection in nasopharynx samples. Clin Microbiol Infect. (2021) 27:487–8. doi: 10.1016/j.cmi.2020.09.030
14. Link-Gelles R, Ciesla AA, Mak J, Miller JD, Silk BJ, Lambrou AS, et al. Early estimates of updated 2023–2024 (Monovalent XBB.1.5) COVID-19 vaccine effectiveness against symptomatic SARS-coV-2 infection attributable to co-circulating omicron variants among immunocompetent adults — Increasing community access to testing program, United States, September 2023–January 2024. MMWR Morb Mortal Wkly Rep. (2024) 73:77–83. doi: 10.15585/mmwr.mm7304a2
15. Wang Q, Bowen A, Tam AR, Valdez R, Stoneman E, Mellis IA, et al. SARS-CoV-2 neutralising antibodies after bivalent versus monovalent booster. Lancet Infect Dis. (2023) 23:527–8. doi: 10.1016/S1473-3099(23)00181-0
16. Spyros C, Nichole M, Jordan LW, Brandon E, Adam B, Joanne ET, et al. Interim report of the reactogenicity and immunogenicity of SARS-CoV-2 XBB-containing vaccines. J Infect Dis. (2024) jiae067. doi: 10.1093/infdis/jiae067
17. Qian W, Yicheng G, Anthony B, Ian AM, Riccardo V, Carmen G, et al. XBB.1.5 monovalent mRNA vaccine booster elicits robust neutralizing antibodies against XBB subvariants and JN.1. Cell Host Microbe. (2024) 32(3):315–21.e3. doi: 10.1016/j.chom.2024.01.014
18. Korea Disease Control and Prevention Agency. COVID-19 Weekly Surveillance Report (Nov 26, 2023-Dec 2, 2023) 2023 [updated Dec 8, 2023. Available at: https://ncov.kdca.go.kr/tcmBoardView.do?brdId=3&brdGubun=40&dataGubun=&ncvContSeq=7737&contSeq=7737&board_id=401&gubun=ALL.
19. Hansen CH, Moustsen-Helms IR, Rasmussen M, Søborg B, Ullum H, Valentiner-Branth P. Short-term effectiveness of the XBB.1.5 updated COVID-19 vaccine against hospitalisation in Denmark: a national cohort study. Lancet Infect Dis. (2024) e73–4. doi: 10.1016/S1473-3099(23)00746-6
20. van Werkhoven CH, Valk AW, Smagge B, de Melker HE, Knol MJ, Hahné SJ, et al. Early COVID-19 vaccine effectiveness of XBB.1.5 vaccine against hospitalisation and admission to intensive care, the Netherlands, 9 October to 5 December 2023. Euro Surveill. (2024) 29:2300703. doi: 10.2807/1560-7917.ES.2024.29.1.2300703
21. Korea Disease Control and Prevention Agency. Surveillance Statistics of Infectious Disease for week 1 2024. Available at: https://www.phwr.org/journal/archives_Supple_View.html?eid=U3VwcGxlX251bT01OQ.
22. Korea Disease Control and Prevention Agency. Press release: Oct 28, 2022. Available at: https://www.kdca.go.kr/board/board.es?mid=a20501020000&bid=0015&list_no=720988&cg_code=C01&act=view&nPage=72.
23. Korea Disease Control and Prevention Agency. Domestic COVID-19 case counts (as of August 31, 2023) 2023 [updated Aug 31, 2023. Available at: https://ncov.kdca.go.kr/bdBoardList_Real.do?brdId=1&brdGubun=11&ncvContSeq=&contSeq=&board_id=&gubun.
24. Yang Y, Yang M, Peng Y, Liang Y, Wei J, Xing L, et al. Longitudinal analysis of antibody dynamics in COVID-19 convalescents reveals neutralizing responses up to 16 months after infection. Nat Microbiol. (2022) 7:423–33. doi: 10.1038/s41564-021-01051-2
Keywords: COVID-19, SARS-CoV-2, XBB.1.5, Omicron, vaccine, effectiveness
Citation: Nham E, Sohn JW, Choi WS, Wie S-H, Lee J, Lee J-S, Jeong HW, Eom JS, Choi YJ, Seong H, Yoon JG, Noh JY, Song JY, Cheong HJ and Kim WJ (2024) Effectiveness of COVID-19 XBB.1.5 monovalent mRNA vaccine in Korea: interim analysis. Front. Immunol. 15:1382944. doi: 10.3389/fimmu.2024.1382944
Received: 06 February 2024; Accepted: 10 April 2024;
Published: 13 May 2024.
Edited by:
Mrinmoy Sanyal, Stanford University, United StatesReviewed by:
Yashavanth Shaan Lakshmanappa, University of California, Davis, United StatesCopyright © 2024 Nham, Sohn, Choi, Wie, Lee, Lee, Jeong, Eom, Choi, Seong, Yoon, Noh, Song, Cheong and Kim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Woo Joo Kim, d2praW1Aa29yZWEuYWMua3I=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.