 Anna Grenda1*
Anna Grenda1* Barbara Kuźnar-Kamińska2
Barbara Kuźnar-Kamińska2 Ewa Kalinka3*
Ewa Kalinka3* Paweł Krawczyk1
Paweł Krawczyk1 Marek Sawicki4Agata Filip5
Marek Sawicki4Agata Filip5 Izabela Chmielewska1
Izabela Chmielewska1 Małgorzata Frąk1Natalia Krzyżanowska1Janusz Milanowski1
Małgorzata Frąk1Natalia Krzyżanowska1Janusz Milanowski1- 1Department of Pneumonology, Oncology and Allergology, Medical University of Lublin, Lublin, Poland
- 2Department of Pulmonology, Allergology and Pulmonary Oncology, Poznan University of Medical Sciences, Poznań, Poland
- 3Department of Oncology, Polish Mother’s Memorial Hospital Research Institute, Łódź, Poland
- 4Department of Thoracic Surgery, Medical University of Lublin, Lublin, Poland
- 5Department of Cancer Genetics with Department of Cancer Genetics with Cytogenetics Laboratory, Medical University in Lublin, Lublin, Poland
Introduction: Expression of PD-L1 on cancer cells is the only validated predictive factor for immunotherapy in NSCLC (Non-Small Cell Lung Cancer) patients. However, on this basis, it is difficult to predict the occurrence of resistance to immune checkpoint inhibitors (ICIs). MicroRNAs are widely studied as biomarkers of cancers. Our study was designed to determine whether microRNAs can be sensitive predictive factors in the qualification of NSCLC patients to first-line immunotherapy or chemoimmunotherapy.
Material and methods: The two-stage research on validation group (n=20) and study group (n=35) of patients with advanced NSCLC was conducted. Analysis of microRNAs expression by qPCR in plasma collected prior to the start of immunotherapy (pembrolizumab) or chemoimmunotherapy (combination of pembrolizumab with chemotherapy) was made. Broad-spectrum analysis of microRNAs expression was used in the studied group. Three microRNAs selected in that group as important for the effectiveness of ICIs were then examined in the validation group.
Results: In the studied group, significantly higher expression of miRNA-126-3p, miR-144-3p and miR-146-5p was observed in patients with long PFS compared to those with short PFS. In the validation group, low miRNA-126 expression indicated lower median progression-free survival and overall survival (2.3 vs. 5.0 months and 5.2 vs 11.2, respectively). These patients had a significantly higher risk of progression (HR= 2.92, 95% CI: 1.01 to 8.40, p=0.04) and death (HR=3.64, 95% CI: 1.22 to 10.84, p=0.02).
Conclusion: Our study showed that the expression of miR-126 in blood plasma may be a predictive factor for the effectiveness of first-line immunotherapy or chemoimmunotherapy in advanced NSCLC patients.
Introduction
The percentage of tumor cells (TC) with PD-L1 (Programmed Cell Death Ligand 1) expression is determined during the qualification of patients with advanced non-small cell lung cancer (NSCLC) to therapy with immune checkpoint inhibitors (ICIs) in monotherapy or combination with chemotherapy. Atezolizumab, pembrolizumab or cemiplimab can be used in first-line monotherapy when PD-L1 expression is observed on ≥50% of TC. Immunotherapy combined with chemotherapy can be considered for first-line therapy if PD-L1 expression is found on less than 50% of tumor cells. For advanced NSCLC patients with PD-L1 expression on less than 1% of TC or regardless of this expression, pembrolizumab or nivolumab or atezolizumab could be used in second-line therapy in patients who have not previously received immunotherapy (1–14).
PD-L1 is the only validated predictor of immunotherapy efficacy, but it is not perfect. The probability of disease progression and resistance to ICIs therapy cannot be accurately determined based on PD-L1 expression. Approximately 40% of patients with high PD-L1 expression have primary resistance to immunotherapy and show disease progression. Another 30% of patients achieve disease stabilization with a short progression-free survival (PFS) of approximately 6 months. These patients develop an acquired resistance to immunotherapy. However, in the remaining patients, the response to immunotherapy is long-lasting (11–13). Moreover, immunotherapy may be highly beneficial in patients with low or no expression of PD-L1 protein on TCs. The mechanism of resistance to immunotherapies is not fully understood (1, 14). Resistance to immunotherapy may be influenced by intrinsic factors of the cancer cell, such as epigenetic factors and disruption in gene expression, as well as mutations that compose the molecular landscape of the cancer cells (15–17). The action of immunosuppressive cytokines or growth factors, neoangiogenesis associated with the formation of abnormal blood vessels, expression of molecules on T cells that send signals to silence the immune system, tumor-infiltrating lymphocyte (TIL) status, or the composition of the gut microbiome belong to the external factors, independent of the tumor cells (17, 18).
Our attention was drawn to epigenetic factors which are microRNA molecules. They are short in length (~21nt), stable, and present in plasma/serum, which ensures easy availability of material for testing, without the need for invasive methods. MicroRNAs affect almost all cellular processes, by regulating gene expression at the post-transcriptional level. Expression of microRNAs changes under pathological conditions, including cancer development. Thus, they may be related to all molecular and immunological mechanisms of resistance to immunotherapy. MicroRNAs are widely studied as precise biomarkers in the context of early cancer diagnosis. Our present study was designed to determine whether they can be sensitive predictive factors for the effectiveness of immunotherapy or chemoimmunotherapy in patients with advanced NSCLC.
Materials and methods
Patients characteristic
The study consisted of two stages. The first involved the selection of microRNAs from a panel of miRCURY LNA Human Serum/Plasma Focus PCR Panels (Qiagen, Venlo, Netherlands) and was conducted on a group of 20 NSCLC patients (in stage IV) treated with immunotherapy (10 patients with PD-L1 expression on ≥50% of TC) or chemoimmunotherapy (10 patients with PD-L1 expression on <50% of TC).
Patients were divided based on the length of progression-free survival. Ten patients were characterized by short disease stabilization or disease progression with a PFS of less than 6 months and 10 patients had a PFS longer than 6 months. There were 6 (30%) women and 14 (70%) men. 13 (65%) patients were over 65 years of age and 7 (35%) patients were under 65 years of age. All patients were in stage IV according to 8th TNM classification. There were 7 patients diagnosed with squamous cell carcinoma and 13 patients with adenocarcinoma.
In the second stage, we performed assays on an independent, validation group of patients with selected micoRNAs (from the first stage of the study) that were classified as potential predictors of immunotherapy or chemoimmunotherapy efficacy. The group consisted of 35 patients. Thirty-four patients were in stage IV and one patient in stage IIIB of the disease. EGFR mutations (Epidermal Growth Factor Receptor), ALK (Anaplastic Lymphoma Kinase Tyrosine Kinase Receptor) and ROS1 (ROS Proto-Oncogene 1, Tyrosine Kinase Receptor) rearrangement were excluded in all patients. Responses to immunotherapy, progression-free survival, and overall survival were calculated from the start of therapy in all 35 patients.
Demographic and clinical characteristics of the entire study group are presented in Table 1.
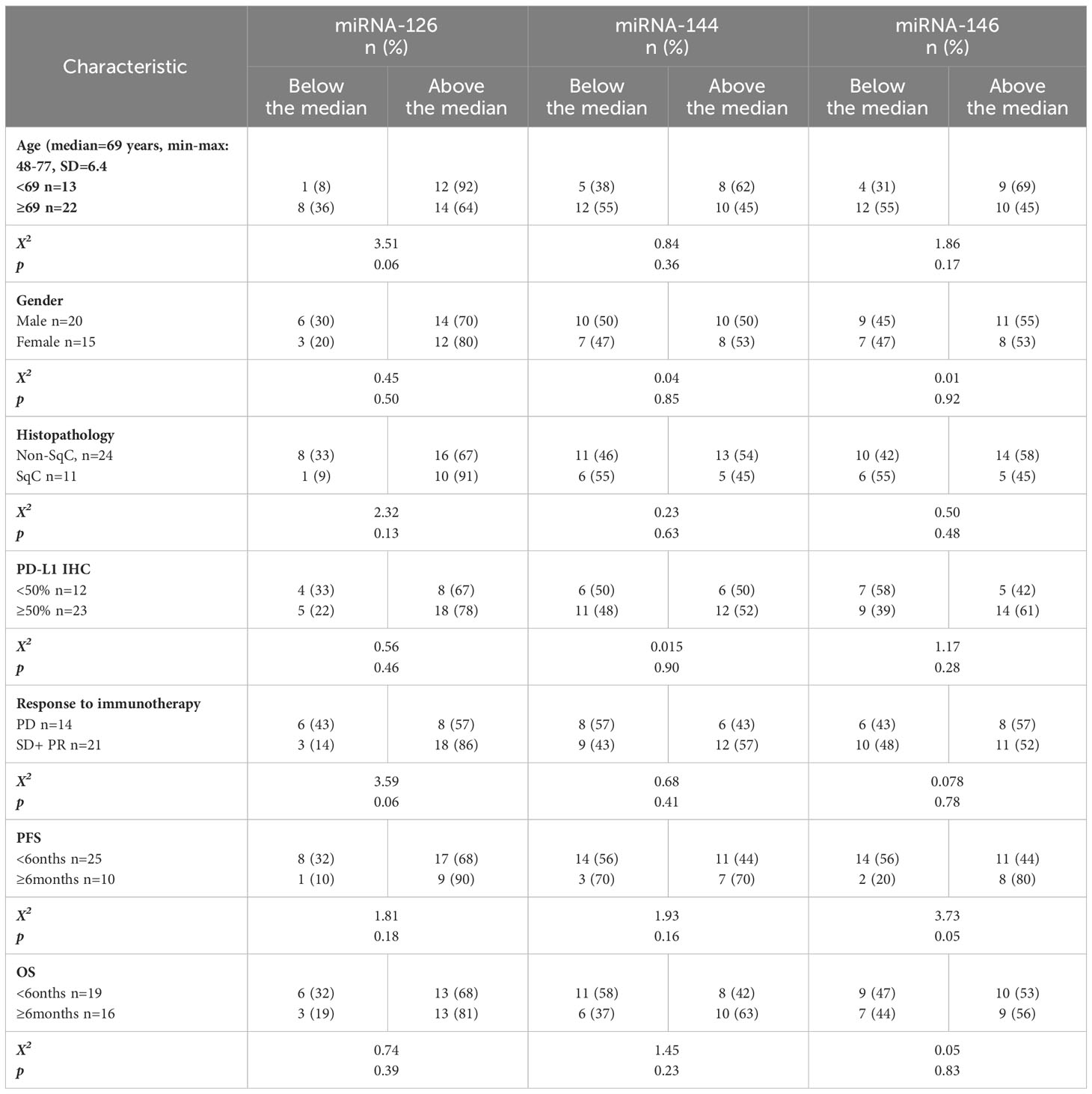
Table 1 Clinical and demographic characteristics of patients in the validation group (n=35).
The research was approved by the bioethics committee at the Medical University of Lublin (KE-0254/95/2018). Informed consent was obtained from all patients.
Sample collection
The material for the study consisted of plasma samples taken from patients before the treatment. The blood was collected in EDTA (ethylenediaminetetraacetic acid) tubes and centrifuged for 10 min at 2000 x g. The plasma was pipetted in equal amounts into eppendorf tubes. Plasma samples were stored at -80°C until isolation of RNA was carried out.
MicroRNA expression testing in the experimental group
Isolation of free-circulating microRNAs was performed using the miRNeasy Serum/Plasma Kit (Qiagen, Venlo, Netherlands). The isolated RNA was stored at -80°C until the reverse transcription reaction was performed. Reverse transcription reactions were performed using miRCURY® LNA® RT Kit (Qiagen, Venlo, Netherlands) according to the manufacturer’s instructions on the T Personal instrument (Analitik Jena, Jena, Germany). MicroRNAs expression was evaluated by qPCR in 20 patients from the experimental group using the miRCURY LNA Human Serum/Plasma Focus PCR Panels (Qiagen, Venlo, Netherlands) kit on the Applied Biosystems 7500 Fast Real-Time PCR System (Applied Biosystems, Waltham, USA). The 10-microliter reaction was prepared according to the manufacturer’s instructions. qPCR was performed according to the following time and temperature conditions: PCR initial heat activation: 2 min, 95°C, and next 40 cycles: denaturation 10 s, 95°C, annealing/extension 60 s, 56°C. A melting curve analysis was attached to each run. The obtained Ct values were used for calculations using the method 2-ΔCt. MiRNA-484 and cel-miR-39-3p spike-in were used as controls.
MicroRNA expression testing in the validation group
Isolation of free-circulating miRNAs was performed using miRNeasy Serum/Plasma Kit (Qiagen, Venlo, Netherlands). The isolated RNA was stored at -80°C until the reverse transcription reaction was performed. For cDNA synthesis TaqMan™ Advanced miRNA cDNA Synthesis Kit (ThermoFisher Scientific, Waltham, Massachusetts, USA) was used.
Three microRNAs were selected for further validation analyses among the microRNAs tested in the experimental group. These microRNAs showed significantly different expression in patients with short and long PFS in the experimental group. The tests were performed using TaqMan probes. Expression of miRNA-126-3p (cat. A25576 477887_mir), miR-144-3p (cat. A25576 477913_mir), miR-146a-5p (cat. A25576 478399_mir) were examined. Expression of miRNA-484 (A25576 478308_mir) and cel-miR-39-3p (cat. A25576 478293_mir) spike-in were used as controls. Reactions were performed on the illumina Eco Real-Time PCR system. The 20 microliter reaction contained: 10 μl TaqMan™ Fast Advanced Master Mix (ThermoFisher Scientific, Waltham, Massachusetts, USA), 1 μl TaqMan® Advanced miRNA Assay, 4 μl nuclease free water and 5 µL of the diluted cDNA (1:10) template. Temperature conditions were used as follows: enzyme activation 95°C by 20 seconds and then 40 cycles: denature 95°C by 3 seconds and anneal/extend 62°C by 30 seconds. The obtained Ct values were used for calculations using the 2-ΔCt method.
Statistical analysis
Statistical analysis was performed using Statistica 13.3 (TIBCO Software Inc, Palo Alto, USA) and MedCalc (MedCalc Software Ltd, Ostend Belgium) software. The U-Mann–Whitney test was used to assess differences in miRNA expression between groups of patients. Kaplan-Meier survival analysis were used for the calculation of PFS and OS. The results are presented as medians and maximum and minimum values (min-max). A p-value below 0.05 was considered statistically significant.
Results
The median PFS in the experimental group was 1.9 months (95%CI: 1.5 to 11.6, min-max: 1.0-23.6). The median overall survival calculated from the start of immunotherapy was 6.6 months (95%CI: 1.7 to 13.8, min-max: 1.0-23.6).
Based on the analysis of microRNAs expression in experimental group, significantly higher expression of miRNA-126-3p (p=0.007), miR-144-3p (p=0.04) and miR-146-5p (p=0.03) was observed in patients with long PFS compared to those with short PFS (Figures 1A–C respectively).
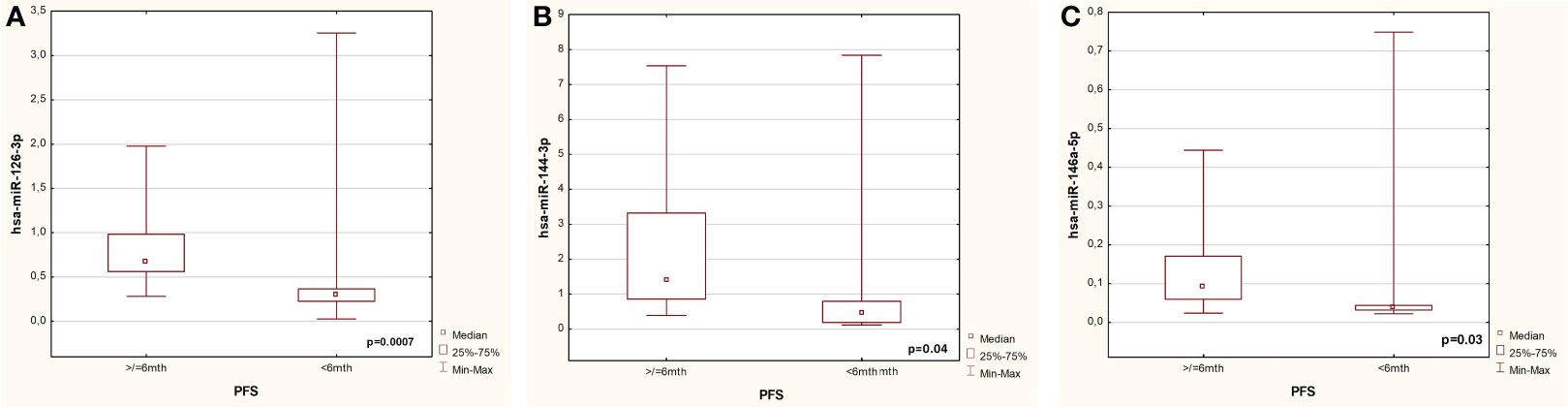
Figure 1 Differences in expression of miRNA-126 (A), miR-144 (B), miR-146 (C) in patients with short and long PFS from the experimental group.
Therefore, further studies in the validation group focused on these three microRNA molecules. In an independent validation group, miRNA-126 expression was non-significantly higher in patients with PFS over 6 months (p=0.07, Figure 2A) in comparison to patients with shorter PFS. Significantly higher expression of miRNA-146 (p=0.04, Figure 2B) was found in patients with long PFS than in patients with short PFS. No such differences were observed during analysis of the miRNA-144 expression in these groups (p=0.5).
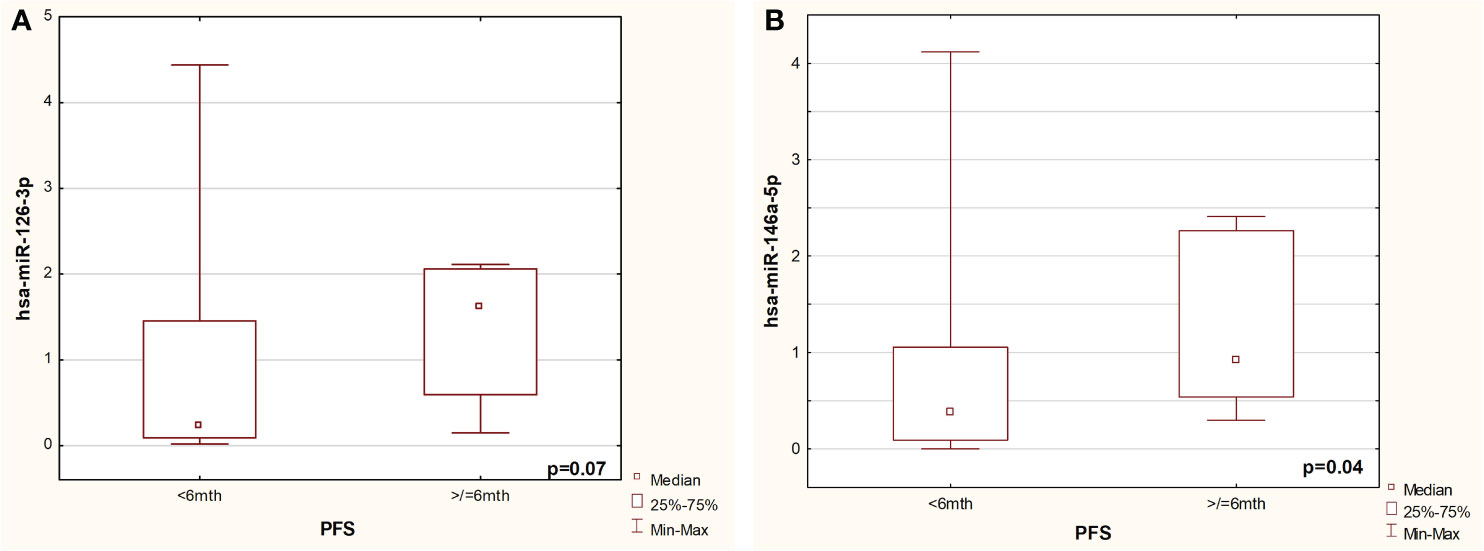
Figure 2 Comparison of expression of miRNA-126-3p (A) and miR-146-5p (B) in patients with short and long PFS from validated group.
Kaplan-Meier analysis showed that the median PFS was lower in patients with low expression of miRNA-126 compared to patients with high expression of this molecule (2.3 vs. 5.0 months). The risk of progression was almost three times higher in the group of patients with low expression of the tested microRNA compared to patients with high expression of this molecule (HR= 2.92, 95% CI: 1.01 to 8.40, p=0.04, Figure 3A). Moreover, median OS was lower in patients with lower miRNA-126 expression than in patients with higher miRNA-126 expression (5.2 vs. 11.2 months). Lower expression of miRNA-126 indicated almost four times higher risk of OS shortening (HR=3.64, 95% CI: 1.22 to 10.84, p=0.02, Figure 3B).
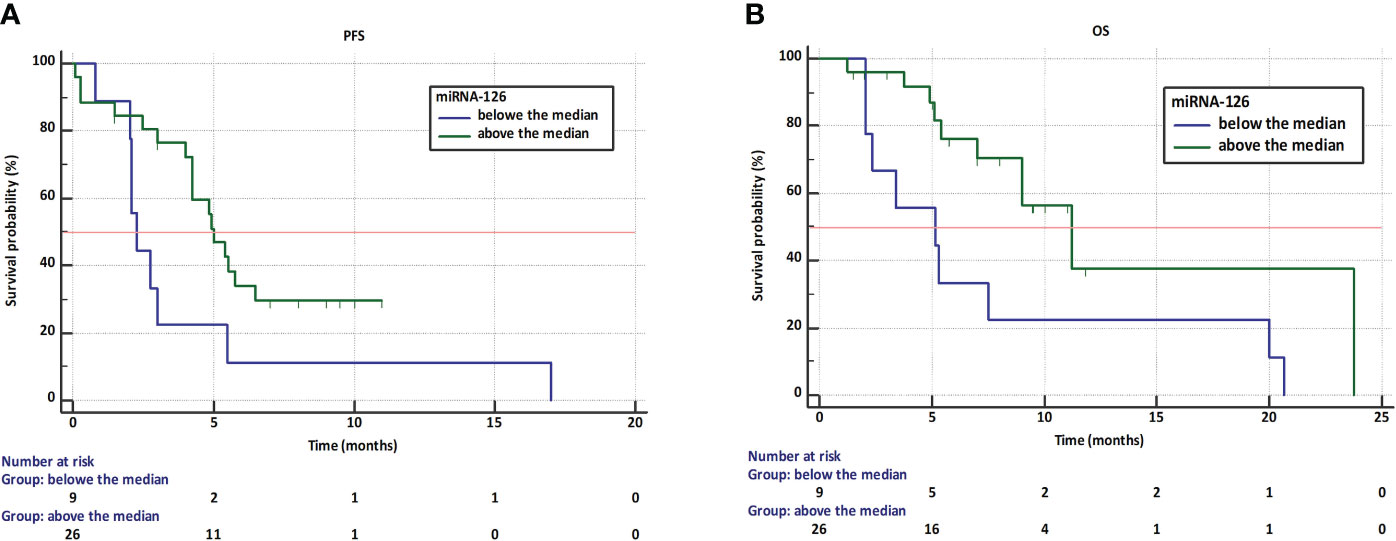
Figure 3 Kaplan-Meier curves showing progression-free survival (A) and overall survival (B) in NSCLC patients treated with first-line immunotherapy or chemoimmunotherapy with different expression of miRNA-126-3p.
Discussion
We selected three microRNAs which expression could be a predictive factor for the efficacy of immunotherapy with anti-PD-1 antibodies. For this purpose, we used an analysis of a broad panel of miRNA molecules in the plasma of NSCLC patients treated with first-line immunotherapy or chemoimmunotherapy. Expression of miRNA-126-3p, miRNA-144-3p and miRNA-146a-5p have been indicated as potentially useful factors in the qualification for immunotherapy. In further studies in an independent validation group, we found that high miRNA-126-3p expression could be a predictive factor for first-line immunotherapy efficacy in non-small cell lung cancer patients. It should be mentioned that the expression of miRNAs, including miRNA-126, may be influenced by chemotherapy or other method of treatment. Our goal was to evaluate whether any miRNA molecules expression could be a universal biomarker of response to immune checkpoints inhibitors used alone or in combination with chemotherapy in advanced NSCLC patients. Therefore, we analyzed these potential predictive factors before starting treatment.
Other authors’ research indicated that miRNA-126 expression is significantly reduced in adenocarcinoma of the lung compared to the normal tissue. Therefore, reduction of miRNA-126 expression is associated with the development of lung adenocarcinoma (LUAD) (19). Moreover, lower expression of miRNA-126-3p and miRNA126-5p promotes vascular invasion, and lymph node metastasis, and occurs in higher stages (III-IV) of adenocarcinoma patients.
The target transcripts for miRNA-126 activity were identified: IGF2BP1 (Insulin Like Growth Factor 2 MRNA Binding Protein 1), TRPM8 (Transient Receptor Potential Cation Channel Subfamily M Member 8), DUSP4 (Dual Specificity Phosphatase 4), SOX11 (SRY-Box Transcription Factor 11), PLOD2 (Procollagen-Lysine,2-Oxoglutarate 5-Dioxygenase 2), LIN28A (Lin-28 Homolog A), LIN28B (Lin-28 Homolog B), SLC7A11 (Solute Carrier Family 7 Member 11), mTOR (Mechanistic Target Of Rapamycin Kinase), PIK3R2 (Phosphoinositide-3-Kinase Regulatory Subunit 2) (19–21). MiRNA-126 has tumor suppressor properties. MiRNA-126 has an inhibitory effect on NSCLC cell invasion by silencing oncogenes: VEGFA (Vascular Endothelial Growth Factor A), AKT1 (AKT Serine/Threonine Kinase 1) and KRAS (Kirsten Rat Sarcoma Virus Proto-Oncogene, GTPase) (22). Moreover, it has been found that miR-126-3p inhibits the growth, migration, and invasion of NSCLC by targeting CCR1 (C-C Motif Chemokine Receptor 1) in NSCLC cells (23). However, it was demonstrated that the over-expression of CCR1 molecule rescued the inhibitory effects of miR-126-3p on NSCLC cell growth, migration and invasion. Further, the knocked-down of CCR1 was able to mimic the inhibitory effects of miR-126-3p on the progression of NSCLC cells (23).
Di Paolo et al. identified in a group of 38 NSCLC patients that the expression of miR-126-3p and miR-221-3p was significantly changed in tumor tissue compared to healthy tissue (24). They found that concomitant miR-126-3p activation and miR-221-3p inhibition reduced lung cancer cell viability by inhibiting AKT, PIK3R2 and PTEN (Phosphatase And Tensin Homolog) signaling pathways (24). PIK3R2 was a target for the action of miR-126-3p and PTEN for miR-221-3p. Researchers proved that the simultaneous interaction of these molecules reduced metastatic dissemination of lung cancer cells both in vitro and in vivo through CXCR4 (C-X-C Motif Chemokine Receptor 4) inhibition. Further, Ichikawa et al. showed miR−126−3p could inhibit cell migration and invasion and induce apoptosis by regulating the PI3K/PDK1/AKT pathway in HeLa cells (25). A meta-analysis of Sun et al. showed that generally high expression of miR-126 is associated with better prognosis in NSCLC patients (26). In research by Yang et al., expression of miRNA-126 was decreased in NSCLC lines and tumor tissues. The patients with low expression of miRNA-126 had significantly poorer overall survival than those with high miRNA-126 expression (means OS reached 24.4 vs. 29.3 months, respectively) (27).
It has also been shown that miRNA-126-3p down-regulation contributes to dabrafenib-acquired resistance in melanoma patients by up-regulating ADAM9 (ADAM Metallopeptidase Domain 9) and VEGFA (28). This is consistent with the observation that decreased ADAM9 mRNA expression correlated with a better response to nivolumab therapy in hepatocellular cancer (29). Liu et al. reported that miR-126 suppressed esophageal cancer cell proliferation and migration by interacting with ADAM9 mRNA 3′UTR (Untranslated Region) (30). They indicated that expression of miR-126 was reduced in esophageal cancer tissues, which was correlated with shorter overall survival of patients, implying their potential function as a prognostic factor (30). In contrast, in colorectal cancer, high expression of miR-126 in tumor and stroma was associated with increased overall survival. In multivariate analyses, high miR-126 expression in tumor remained a significant independent predictor of improved survival (31). The authors postulate that this factor may help in the qualification of patients for adjuvant chemotherapy (31).
In turn, Schmittnaegel et al. postulated that the blockade of Ang2 (angiopoietin-2) and VEGFA induces antitumor immunity enhanced by PD-1 checkpoint blockade (32). These are indications that the expression of the miRNA-126-3p molecule is a beneficial factor for NSCLC patients receiving immunotherapy. Researchers indicated that the miR-126 molecule is associated with the functioning of T lymphocytes, especially Treg cells. Chen et al. postulated that investigation of the role of miR-126 in lung cancer development and progression, including in activation of the immune response, may be valuable for the estimation of immunotherapy efficacy (22).
The previous considerations and our results indicate that higher miR-126 expression may be a favorable predictive factor for immunotherapy. Qin et al. found that miRNA-126 was expressed in mouse and human Treg cells (33). It has been shown that miRNA-126 regulates the activity of the PI3K-AKT signaling pathway, crucial for Foxp3 (Forkhead Box P3) expression, and limited activation of PI3K/AKT pathway was necessary for Tregs development and function. Researchers in further studies showed that silencing of miRNA-126 using antisense oligonucleotides (ASO) could significantly reduce the induction of Treg cells in vitro. Furthermore, miR-126 silencing could reduce the expression of Foxp3 on Treg cells, which was accompanied by decreased expression of CTLA-4 (Cytotoxic T-Lymphocyte Associated Protein 4) and GITR (TNF Receptor Superfamily Member 18), as well as IL-10 and TGF-β production. Therefore, high expression of miRNA-126 in lymphocytes may be associated with the activation, differentiation and suppressive activity of Treg cells. Moreover, Fortunato et al. found that high level of miRNA-126-3p in plasma may be related to the induction and activation of Treg cells, which enhance the metabolism and secretion of exosomes containing microRNAs, including miRNA-126-3p (34). In turn, high activity of Treg cells in the tumor microenvironment and lymph nodes is associated with immunosuppression and poorer effectiveness of immunotherapy. However, the function of Treg lymphocytes is only one of many immunological factors influencing the efficacy of immunotherapy. One of them may be the function of monocytes on the spreading of cancer. Zhang et al. indicated that miRNA-126 independently suppress the sequential recruitment of mesenchymal stem cells and inflammatory monocytes into the tumor stroma. The lack of these cells in the microenvironment may be favorable for metastases development in the breast cancer mouse xenograft model (35).
Conclusion
Our study shows that miR-126 may be a predictive factor of the effectiveness of first-line immunotherapy or chemoimmunotherapy in NSCLC patients. We are aware that our study groups were not very large. We postulate that further research should be carried out in a larger group and in patients treated with second-line immunotherapy to investigate whether the expression of this molecule has predictive properties in these patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Bioethics Committee at the Medical University of Lublin. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AG: Conceptualization, Formal analysis, Methodology, Project administration, Writing – original draft. BK: Conceptualization, Formal analysis, Investigation, Resources, Writing – original draft. EK: Data curation, Formal analysis, Methodology, Writing – review & editing. PK: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. MS: Data curation, Investigation, Supervision, Writing – review & editing. AF: Software, Supervision, Writing – review & editing. IC: Data curation, Formal analysis, Investigation, Resources, Visualization, Writing – original draft. MF: Data curation, Formal analysis, Writing – original draft. NK: Data curation, Writing – review & editing. JM: Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Vokes EE, Ready N, Felip E, Horn L, Burgio MA, Antonia SJ, et al. Nivolumab versus docetaxel in previously treated advanced non-small-cell lung cancer (CheckMate 017 and CheckMate 057): 3-year update and outcomes in patients with liver metastases. Ann Oncol Off J Eur Soc Med Oncol. (2018) 29:959–65. doi: 10.1093/annonc/mdy041
2. Siciliano MA, Caridà G, Ciliberto D, d’Apolito M, Pelaia C, Caracciolo D, et al. Efficacy and safety of first-line checkpoint inhibitors-based treatments for non-oncogene-addicted non-small-cell lung cancer: a systematic review and meta-analysis. ESMO Open. (2022) 7:100465. doi: 10.1016/j.esmoop.2022.100465
3. Rittmeyer A, Barlesi F, Waterkamp D, Park K, Ciardiello F, von Pawel J, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet Lond Engl. (2017) 389:255–65. doi: 10.1016/S0140-6736(16)32517-X
4. Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Five-year outcomes with pembrolizumab versus chemotherapy for metastatic non-small-cell lung cancer with PD-L1 tumor proportion score ≥ 50. J Clin Oncol Off J Am Soc Clin Oncol. (2021) 39:2339–49. doi: 10.1200/JCO.21.00174
5. Jassem J, de Marinis F, Giaccone G, Vergnenegre A, Barrios CH, Morise M, et al. Updated overall survival analysis from IMpower110: Atezolizumab versus platinum-based chemotherapy in treatment-naive programmed death-ligand 1-selected NSCLC. J Thorac Oncol Off Publ Int Assoc Study Lung Cancer. (2021) 16:1872–82. doi: 10.1016/j.jtho.2021.06.019
6. Özgüroğlu M, Kilickap S, Sezer A, Gümüş M, Bondarenko I, Gogishvili M, et al. First-line cemiplimab monotherapy and continued cemiplimab beyond progression plus chemotherapy for advanced non-small-cell lung cancer with PD-L1 50% or more (EMPOWER-Lung 1): 35-month follow-up from a mutlicentre, open-label, randomised, phase 3 trial. Lancet Oncol. (2023) 24:989–1001. doi: 10.1016/S1470-2045(23)00329-7
7. Denault M-H, Melosky B. Immunotherapy in the first-line setting in wild-type NSCLC. Curr Oncol. (2021) 28:4457–70. doi: 10.3390/curroncol28060378
8. Novello S, Kowalski DM, Luft A, Gümüş M, Vicente D, Mazières J, et al. Pembrolizumab plus chemotherapy in squamous non-small-cell lung cancer: 5-year update of the phase III KEYNOTE-407 study. J Clin Oncol Off J Am Soc Clin Oncol. (2023) 41:1999–2006. doi: 10.1200/JCO.22.01990
9. Addeo A, Banna GL, Metro G, Di Maio M. Chemotherapy in combination with immune checkpoint inhibitors for the first-line treatment of patients with advanced non-small cell lung cancer: A systematic review and literature-based meta-analysis. Front Oncol. (2019) 9:264. doi: 10.3389/fonc.2019.00264
10. Garassino MC, Gadgeel S, Speranza G, Felip E, Esteban E, Dómine M, et al. Pembrolizumab plus pemetrexed and platinum in nonsquamous non–small-cell lung cancer: 5-year outcomes from the phase 3 KEYNOTE-189 study. J Clin Oncol. (2023) 41:1992–8. doi: 10.1200/JCO.22.01989
11. Gandhi L, Rodríguez-Abreu D, Gadgeel S, Esteban E, Felip E, De Angelis F, et al. Pembrolizumab plus chemotherapy in metastatic non–small-cell lung cancer. N Engl J Med. (2018) 378:2078–92. doi: 10.1056/NEJMoa1801005
12. West H, McCleod M, Hussein M, Morabito A, Rittmeyer A, Conter HJ, et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. (2019) 20:924–37. doi: 10.1016/S1470-2045(19)30167-6
13. Topalian SL, Hodi FS, Brahmer JR, Gettinger SN, Smith DC, McDermott DF, et al. Five-year survival and correlates among patients with advanced melanoma, renal cell carcinoma, or non-small cell lung cancer treated with nivolumab. JAMA Oncol. (2019) 5:1411–20. doi: 10.1001/jamaoncol.2019.2187
14. Pacheco JM, Gao D, Camidge DR. Extended follow-up on KEYNOTE-024 suggests significant survival benefit for pembrolizumab in patients with PD-L1 ≥50%, but unanswered questions remain. Ann Transl Med. (2019) 7:S127. doi: 10.21037/atm.2019.05.72
15. Kovács SA, Győrffy B. Transcriptomic datasets of cancer patients treated with immune-checkpoint inhibitors: a systematic review. J Transl Med. (2022) 20:249. doi: 10.1186/s12967-022-03409-4
16. Liu Z, Ren Y, Weng S, Xu H, Li L, Han X. A new trend in cancer treatment: the combination of epigenetics and immunotherapy. Front Immunol. (2022) 13:809761. doi: 10.3389/fimmu.2022.809761
17. Vu SH, Vetrivel P, Kim J, Lee M-S. Cancer resistance to immunotherapy: molecular mechanisms and tackling strategies. Int J Mol Sci. (2022) 23:10906. doi: 10.3390/ijms231810906
18. Frisone D, Friedlaender A, Addeo A, Tsantoulis P. The landscape of immunotherapy resistance in NSCLC. Front Oncol. (2022) 12:817548. doi: 10.3389/fonc.2022.817548
19. Chen P, Gu Y-Y, Ma F-C, He R-Q, Li Z-Y, Zhai G-Q, et al. Expression levels and co−targets of miRNA−126−3p and miRNA−126−5p in lung adenocarcinoma tissues: An exploration with RT−qPCR, microarray and bioinformatic analyses. Oncol Rep. (2019) 41:939–53. doi: 10.3892/or.2018.6901
20. Wei L, Chen Z, Cheng N, Li X, Chen J, Wu D, et al. MicroRNA-126 inhibit viability of colorectal cancer cell by repressing mTOR induced apoptosis and autophagy. OncoTargets Ther. (2020) 13:2459–68. doi: 10.2147/OTT.S238348
21. Song L, Li D, Gu Y, Wen Z-M, Jie J, Zhao D, et al. MicroRNA-126 targeting PIK3R2 inhibits NSCLC A549 cell proliferation, migration, and invasion by regulation of PTEN/PI3K/AKT pathway. Clin Lung Cancer. (2016) 17:e65–75. doi: 10.1016/j.cllc.2016.03.012
22. Chen Q, Chen S, Zhao J, Zhou Y, Xu L. MicroRNA-126: A new and promising player in lung cancer. Oncol Lett. (2021) 21:35. doi: 10.3892/ol.2020.12296
23. Liu R, Zhang Y-S, Zhang S, Cheng Z-M, Yu J-L, Zhou S, et al. MiR-126-3p suppresses the growth, migration and invasion of NSCLC via targeting CCR1. Eur Rev Med Pharmacol Sci. (2019) 23:679–89. doi: 10.26355/eurrev_201901_16881
24. Di Paolo D, Pontis F, Moro M, Centonze G, Bertolini G, Milione M, et al. Cotargeting of miR-126-3p and miR-221-3p inhibits PIK3R2 and PTEN, reducing lung cancer growth and metastasis by blocking AKT and CXCR4 signalling. Mol Oncol. (2021) 15:2969–88. doi: 10.1002/1878-0261.13036
25. Ichikawa R, Kawasaki R, Iwata A, Otani S, Nishio E, Nomura H, et al. MicroRNA−126−3p suppresses HeLa cell proliferation, migration and invasion, and increases apoptosis via the PI3K/PDK1/AKT pathway. Oncol Rep. (2020) 43:1300–8. doi: 10.3892/or.2020.7512
26. Sun L, Zhou H, Yang Y, Chen J, Wang Y, She M, et al. Meta-analysis of diagnostic and prognostic value of miR-126 in non-small cell lung cancer. Biosci Rep. (2020) 40:BSR20200349. doi: 10.1042/BSR20200349
27. Yang J, Lan H, Huang X, Liu B, Tong Y. MicroRNA-126 inhibits tumor cell growth and its expression level correlates with poor survival in non-small cell lung cancer patients. PloS One. (2012) 7:e42978. doi: 10.1371/journal.pone.0042978
28. Caporali S, Amaro A, Levati L, Alvino E, Lacal PM, Mastroeni S, et al. miR-126-3p down-regulation contributes to dabrafenib acquired resistance in melanoma by up-regulating ADAM9 and VEGF-A. J Exp Clin Cancer Res CR. (2019) 38:272. doi: 10.1186/s13046-019-1238-4
29. Oh S, Park Y, Lee H-J, Lee J, Lee S-H, Baek Y-S, et al. A disintegrin and metalloproteinase 9 (ADAM9) in advanced hepatocellular carcinoma and their role as a biomarker during hepatocellular carcinoma immunotherapy. Cancers. (2020) 12:745. doi: 10.3390/cancers12030745
30. Liu X, Jiang X, Liu R, Wang L, Qian T, Zheng Y, et al. B cells expressing CD11b effectively inhibit CD4+ T-cell responses and ameliorate experimental autoimmune hepatitis in mice. Hepatol Baltim Md. (2015) 62:1563–75. doi: 10.1002/hep.28001
31. Selven H, Busund L-TR, Andersen S, Bremnes RM, Kilvær TK. High expression of microRNA-126 relates to favorable prognosis for colon cancer patients. Sci Rep. (2021) 11:9592. doi: 10.1038/s41598-021-87985-3
32. Schmittnaegel M, Rigamonti N, Kadioglu E, Cassará A, Wyser Rmili C, Kiialainen A, et al. Dual angiopoietin-2 and VEGFA inhibition elicits antitumor immunity that is enhanced by PD-1 checkpoint blockade. Sci Transl Med. (2017) 9:eaak9670. doi: 10.1126/scitranslmed.aak9670
33. Qin A, Wen Z, Zhou Y, Li Y, Li Y, Luo J, et al. MicroRNA-126 regulates the induction and function of CD4+ Foxp3+ regulatory T cells through PI3K/AKT pathway. J Cell Mol Med. (2013) 17:252–64. doi: 10.1111/jcmm.12003
34. Fortunato O, Gasparini P, Boeri M, Sozzi G. Exo-miRNAs as a new tool for liquid biopsy in lung cancer. Cancers. (2019) 11:888. doi: 10.3390/cancers11060888
Keywords: microRNA, immunotherapy, anti-PD-1, NSCLC, miRNA
Citation: Grenda A, Kuźnar-Kamińska B, Kalinka E, Krawczyk P, Sawicki M, Filip A, Chmielewska I, Frąk M, Krzyżanowska N and Milanowski J (2024) MicroRNA-126 selected with broad-spectrum analysis of microRNAs – a new predictive factor for the effectiveness of immunotherapy or chemoimmunotherapy in advanced NSCLC patients? Front. Immunol. 15:1344858. doi: 10.3389/fimmu.2024.1344858
Received: 26 November 2023; Accepted: 07 February 2024;
Published: 26 February 2024.
Edited by:
Ziheng Wang, University of Macau, ChinaReviewed by:
Ming Yi, Zhejiang University, ChinaEsmaeil Mortaz, Shahid Beheshti University of Medical Sciences, Iran
Copyright © 2024 Grenda, Kuźnar-Kamińska, Kalinka, Krawczyk, Sawicki, Filip, Chmielewska, Frąk, Krzyżanowska and Milanowski. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ewa Kalinka, ZXdha2FsaW5rYUB3cC5wbA==; Anna Grenda, YW5ubmEuZ3JlbmRhQHVtbHViLnBs