 Shuhan Zheng1†
Shuhan Zheng1† Yang Wang
Yang Wang Jiaming Geng
Jiaming Geng Liang Huo
Liang Huo
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Immunol. , 02 February 2024
Sec. Multiple Sclerosis and Neuroimmunology
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1278867
Objective: The purpose of this study was to investigate the current research status, focus areas, and developmental trends in the field of Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) through an analysis of scientific literature.
Methods: The relevant research articles on MOGAD published from 1947 to 2022 were retrieved from the Web of Science database. The quantitative output of MOGAD related research articles, their distribution by country/region, data on collaborative publishing, influential authors, high-yield institutions, keywords, hotspots, and development trends were analyzed. Additionally, visual knowledge maps were generated using VOSviewer and Citespace.
Results: There has been a steady increase in the number of MOGAD related publications indicating that the subject has garnered increasing interest among researchers globally. The United States has been the leading contributor with 496 papers (19.25%), followed by China (244, 9.63%), Japan (183, 7.10%), the United Kingdom (154, 5.98%), and Germany (149, 5.78%). Among these countries, the United Kingdom boasts the highest citation frequency at the rate of 46.49 times per paper. Furthermore, active collaboration in MOGAD related research is observed primarily between the United States and countries such as Canada, Germany, Australia, Italy, the United Kingdom and Japan. Mayo Clinic ranks first in total articles published (109) and frequency of citations per article (77.79). Takahashi Toshiyuki from Tohoku University is the most prolific author, while Multiple Sclerosis and Related Disorders is the most widely read journal in this field. “Disease Phenotype”, “Treatment”, “Novel Coronavirus Infection and Vaccination”, “Immunopathological Mechanisms”, “Clinical characteristics of children” and “Prognosis” are the primary keywords clusters in this field. “Novel Coronavirus Infection and Vaccination” and “Immunopathological Mechanisms” are research hotspots and have great development potential.
Conclusion: The past three decades have witnessed a significant expansion of research on MOGAD. The pathogenetic mechanism of MOGAD is poised to be the prominent research focus in this field in the foreseeable future.
Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) is a newly-defined demyelinating disorder of the central nervous system (CNS) with antibodies against myelin oligodendrocyte glycoprotein (MOG) that are expressed on the surface of oligodendrocytes and myelin sheath in the central nervous system (1–6). The clinical phenotype of this demyelinating disease is distinct from that of aquaporin-4 (AQP4) IgG-positive neuromyelitis optica Spectrum disorders (NMOSD) and multiple sclerosis (MS) (7–9) The pathogenesis of MOGAD is believed to be related to the demyelination process mediated by antibody/complement, but the specific pathogeneticmechanism is yet to be elucidated (3, 10). The epidemiological data of MOGAD based on geographic region and ethnicity is limited. The female-to-male ratio is about 1:1, and the estimated annual incidence is 1.6 per million person-years. There are differences between children and adults regarding the incidence, clinical phenotype, treatment, recurrence, and prognosis (7, 11–13).The most common clinical manifestations of MOGAD are optic neuritis (ON), myelitis, and acute disseminated encephalomyelitis (ADEM) which most frequently occurs in children (12, 14). The severity of MOGAD varies, with about 3% of severe patients requiring mechanical ventilation support during the acute phase of the disease (15).Approximately 40%-50% of M (16)OGAD patients maintain a monophasic course while 50-60% of cases experience disease relapses (17–19).The risk of recurrence may be related to the persistence of MOG-IgG seropositivity after the first attack. Moreover, the utility of routine magnetic resonance imaging (MRI) to monitor disease activity was limited by the course of MOGAD with no disease activity between episodes (16, 20, 21). High-dose corticosteroids are effective in treating MOGAD, but early treatment with intravenous gamma globulin or plasmapheresis is recommended for patients with severe disease or high potential for disability (5, 22). Most patients with MOGAD have a good prognosis (23–25).The possibility of legacy nervous system dysfunction is significantly higher in children (11, 24, 26).The international consensus diagnostic criteria for MOGAD are currently being developed. Due to the lack of prospective randomized controlled trials, there are many unresolved questions about the pathogenesis, clinical features, and treatment of MOGAD.
Bibliometrics is an important approach for quantitative measurement of research in a particular field. It entails the use of statistical methods for analysis of factors such as the temporal trend of technological development, future trends, and global scientific and technological competitiveness in a specific field based on published data including papers and patents (27). In recent years, bibliometric analysis has been widely adopted for analysis of massive scientific research data and identification of developing trends (28). Bibliometric analysis methods in this study are necessary and valuable. First, bibliometric analysis method can analyze the current situation and development trend of the discipline from an objective perspective, without individual subjective judgment. So, the data results are more objective. Secondly, compared to the other disciplines, researchers in the medical field tend to choose journal papers as the form of publication. So medical paper data can better reflect the current development status, research hotspots, and future trends. It is necessary and appropriate to use medical data as the research object of the discipline trend. Finally, some researchers in the medical field have used bibliometric methods for review and analysis, and the research results have also been recognized by peers (29–36). Therefore, bibliometric methods to study MOGAD is feasible. To the best of our knowledge, this is the first study that applied bibliometric visualization methods into systematic investigation about the year of publication, countries/regions, organizations, active authors, journals, references, keywords and hotspots involved in MOGAD research. We combined the quantitative and qualitative comprehensive analysis to evaluate the progress and evolution of MOGAD by using the VOSViewer and Citespace software. We considered that this study performed visualization analysis from 1947 to 2022 to identify cooperation networks, track research trends and highlight current hotspots. It can not only help researchers identify its significant features and predict future research directions, but also provide them with meaningful guidance in the selection of frontier topics.
The data in this study were obtained from Web of Science core collection (WoSCC) by Clarivate Analytics. This database is the earliest citation index database in the world and contains>150million highly recognized and authoritative social science and science citations. The database offers full functionality for literature search, citation analysis, and data export to facilitate data processing. In this study, keywords related to MOGAD were selected with the search formula: TS=((“MOG antibody associated” or “MOG associated” or “Myelin Oligodendrocyte Glycoprotein antibody associated” or “Myelin Oligodendrocyte Glycoprotein associated” or “MOG INDUCE*” or “Myelin Oligodendrocyte Glycoprotein INDUCE*” or “MOG antibody” or “Myelin Oligodendrocyte Glycoprotein” or myelitis or medullitis or acutemyelitis or rachiomyelitis or rhachiomyelitis or “optic neuromyelitis” or “neuromyelitisoptica” or “ophthalmoneuromyelitis” or “neurooptic myelitis” or “neuromyelitis optical” or “Optic neuritis” or neuropapillitis or “neuritis optica” or “optic neuvitis” or “acute disseminated encephalomyelitis” or “multiphasic acute disseminated encephalomyelitis” or “ADEM” or “multiphasic ADEM”) and (demyelinat* or myelinolysis)) not TS=(marmoset* or mice or mouse or rat or murine or animal* or macaque* or mammalian). The reference period for the literature search was from 1900 to 2022. The language type was set to English, and the article type was set to article and review. After removing articles unrelated to MOGAD, 2574 publications were obtained. The export type of publication was plain text file and the content included full record and cited references. The retrieval framework is shown in Figure 1.
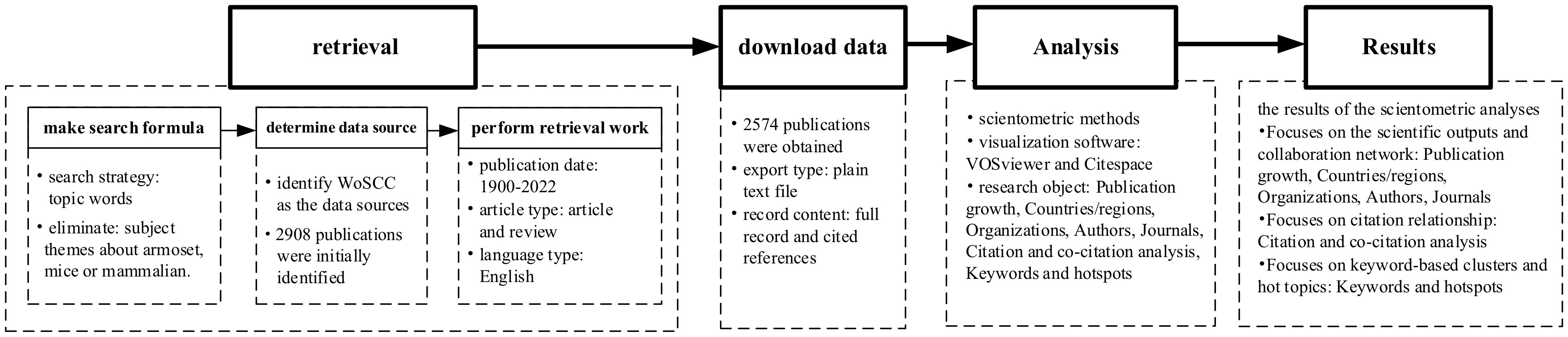
Figure 1 Research process applied in this study.
Bibliometrics refers to the study of bodies of interrelated documents. It is a methodology for the analysis and visualization of the connections among research topics, researchers, affiliations, or journals. In this study, WOS-based literature analysis was conducted to understand the distribution of year of publication, journals, organizations, authors, and research fields. The Standard Competition Ranking method was used to determine the ranking order. Subsequently, the VOSviewer and Citespace software tool were used to map collaborations (co-authorships), topics (term co-occurrence), and citation patterns (bibliographic coupling). The results of the scientometric analyses focuse on 3 themes, which is the scientific outputs and collaboration network, the citation relationship and keyword-based clusters and hot topics. Specifically, the sections of Publication growth, Countries/regions, Organizations, Authors, Journals focuse on the scientific outputs and collaboration network. The section of Citation and co-citation analysis focuses on citation relationship, while the section of Keywords and hotspots focuses on keyword-based clusters and hot topics.
The chronological distribution of published articles is shown in Figure 2A. The data showed a steady increase in the publications related to MOGAD. Research articles related to MOGAD were published as early as the 1940s. However, before the 1990s, the annual output of relevant research articles was less than 5. Since the 1990s, there was a rapid increase in the output of MOGAD research articles to over 10 articles per year. In 2011, the number exceeded 100 for the first time, reaching 108, which shows a rapid upward trend. In the past few years, there has been a gradual increase in the number of published studies, peaking at 171 in 2021.Theincreasing trend in the number of published articles suggests that MOGAD will continue to be a research hotspot in the foreseeable future.
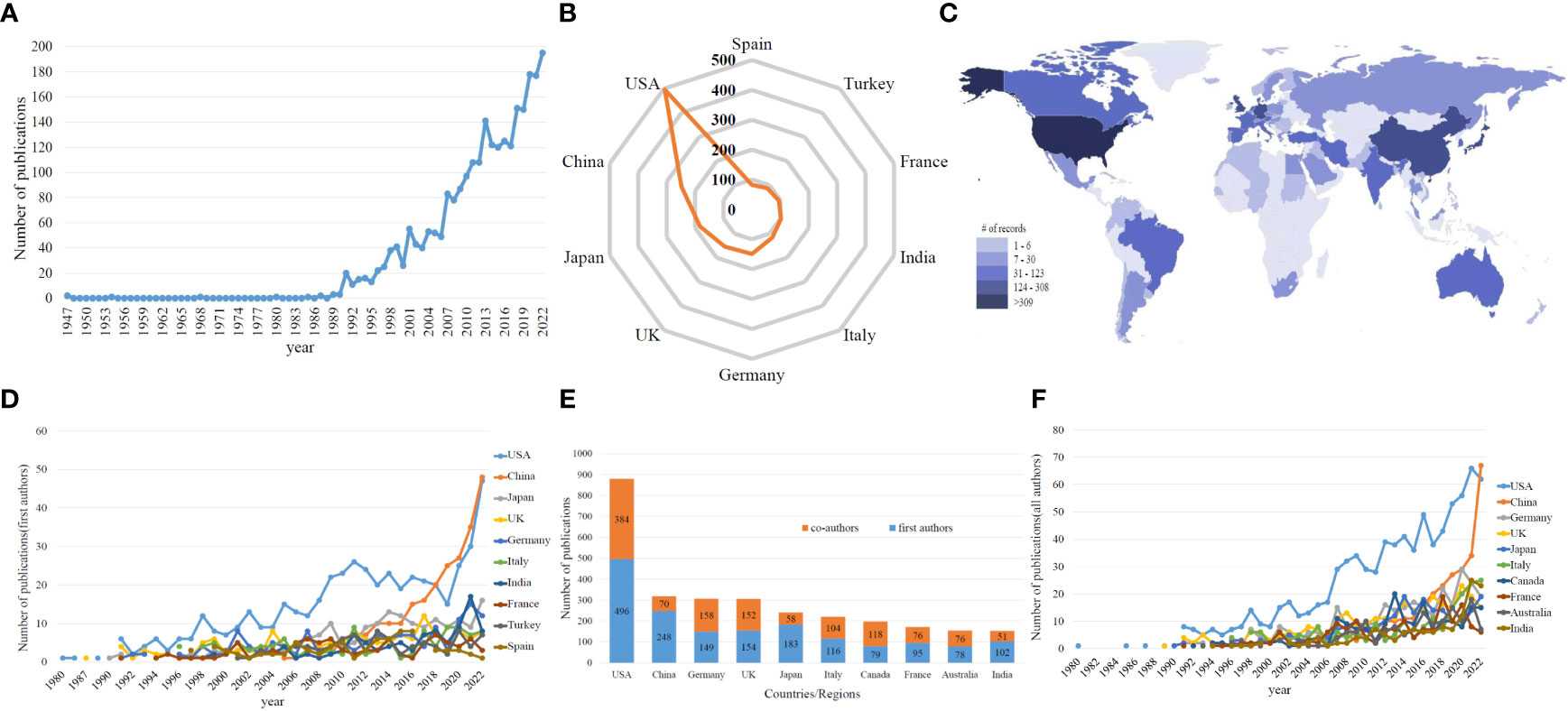
Figure 2 (A) The global number of publications related to MOG research. (B) The sum of publications related to MOGAD research from the top 10 countries/regions based on the first authors. (C) Distribution of MOGAD research in world map based on first authors. (D) The annual number of publications in the top 10 most productive countries based on the first authors from 1980 to 2022. (E) The sum of publications related to MOGAD research from the top 10 countries/regions based on the first and co-authors. (F) The annual number of publications in the top 10 most productive countries based on the first and co-authors from 1980 to 2022.
Figure 2B shows the country/region statistics of the institution where the first author is located. Seventy-two countries/regions have contributed to the literature in this field. The output of top 10 countries accounts for nearly 70% of the total number of papers. The United States (USA) has published the most papers (496, 19.25%), followed by China (244, 9.63%), Japan (183, 7.10%), the United Kingdom (UK) (154, 5.98%) and Germany (149, 5.78%). Figure 2C shows that East Asia, North America, and West Europe were the regions making the top contributions to the number of publications. As shown in Figure 2D, the number of papers published annually by the top 10 countries/regions increased from 1 in 1980 to 158 in 2022, accounting for 81.03% of the total global publications in 2022. The United States ranked first with 496 articles, far exceeding other countries/regions in terms of quantity. China and Japan ranked second and third with 244 and 183 articles published, respectively. These results indicate that MOGAD has attracted increasing attention from researchers and has reached a stage of rapid development. Statistical analysis of the first author country can demonstrate the dominant position of MOGAD, while statistical analysis of each author country can reflect the international cooperation status. As shown in Figure 2E, the number of articles participated by American researchers is the highest, with a total of 880 articles, followed by 318 articles from China and 307 articles from Germany. The proportion of co-authors articles in most countries/regions is around 50%. Especially in the United States, the number of co-authors articles has grown rapidly since 2012, and co-authors from other countries led to USA consistently maintaining the highest number of articles every year (Figure 2F).
The frequency of citations can reflect the quality of the paper to a certain extent. The higher the frequency of citations, the greater is the attention and recognition of researchers in the same field. Figure 3A shows the top 10 countries ranked according to the frequency of citations. On comparing the number of papers, total citation frequency, and average citation frequency, it can be seen that the USA, the UK, and Germany rank among the top three in terms of total citation frequency. The UK has a higher citation frequency, reaching 46.49 times per paper. China ranks second in terms of output of MOGAD-related research papers, but the citation frequency of Chinese publications is 9.16 times per article.

Figure 3 (A) The total cites (blue bars) and average cited frequency per paper (red curve) of publications related to MOGAD research from the top 10 countries. (B) Cooperation network of country/regions.
The cooperation network of the publications can visually display the status of scientific and technological cooperation among countries/regions. In this network map, two countries/regions collaborating to publish papers are connected by line segments. The thicker the line segments, the closer is the degree of cooperation and the colors are the same. As shown in Figure 3B, USA has the most active cooperation in the field of MOGAD, with frequent cooperation with countries such as Canada, Germany, Australia, Italy, the UK, and Japan. In addition, Australia has shown close cooperation with Germany. China has also actively participated in international cooperation, with most notable cooperation with Australia, the USA, the UK, Canada, Germany, France, and Italy.
Table 1 shows the status of the institutions in the field of MOGAD research. United States accounts for the largest share among the top 10 institutions. Mayo Clinic ranks first with a total of 109 articles published, and the frequency of citations per article is as high as 77.79. Mayo Clinic is a nonprofit organization committed to clinical practice, education, and research with a history of over a hundred years. It is now the leading institution in the world in terms of MOGAD related research articles. University College London ranked second with 85 articles. In addition, Medical University of Vienna in Austria has published 49 articles about MOGAD, and the frequency of citations per article is as high as 81, which to some extent reflects the high quality of its articles.

Table 1 Top 10 institutions in the field of MOGAD related research.
Figure 4 shows the cooperative network relationships of the institutions. It shows frequent collaboration between institutions from different countries/regions, such as Mayo Clinic in the USA, Medical University of Vienna in Austria (correlation degree=0.50), and University of Gottingen in Germany (correlation degree=0.60); Spain’s Autonomous University of collaborates closely with the UK’s UCL (correlation degree=0.58) and Austria’s Medical University of Innsbruck (correlation degree=0.83). University of California, USA collaborates more frequently with Johns Hopkins University (correlation degree=0.82), University of Oxford and Great Ormond Street Hospital in the UK (correlation degree=0.79), and University of British Columbia and University of Toronto in Canada (correlation degree=0.68) with strong connections.
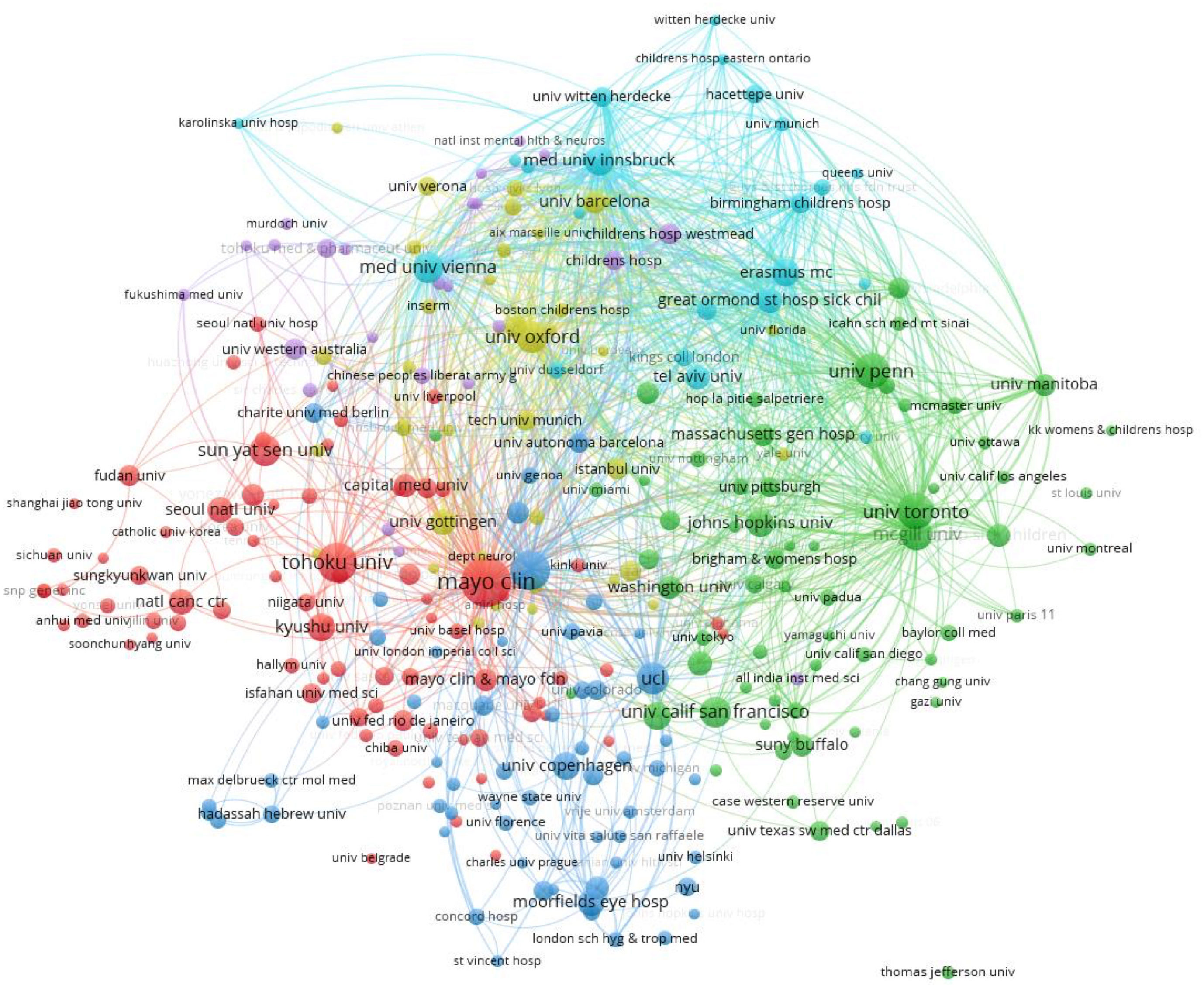
Figure 4 Cooperation network of institutions.
In order to demonstrate the influence of important authors comprehensively, the indicators of the publication counts and citation weight are chosen to represent. Table 2 shows the influential authors of publication counts and citations weight. Takahashi Toshiyuki from Tohoku University has the highest number of publications (37 publications). The second ranked researchers are Reindl Markus from Medical University of Innsbruck, Banwell Brenda from University of Pennsylvania, and Pittock Sean J from Mayo Clinic, all of whom have published 31 papers each. Dale Russell C of University of Sydney has published 29 papers, ranking third. The citations weights of Lucchinetti, Claudia F (citations weight=110.39) and Pittock, Sean J (citations weight=102.90) from Mayo Clin are over 100. And the citation weight ranks of Lassmann, Hans (citations weight=94.49), Vincent, Angela (citations weight=67.94), Flanagan, Eoin P. (citations weight=67.54), Jacqueline, Palace (citations weight=62.00), Jacob, Anu (citations weight=58.01) are in the TOP10.
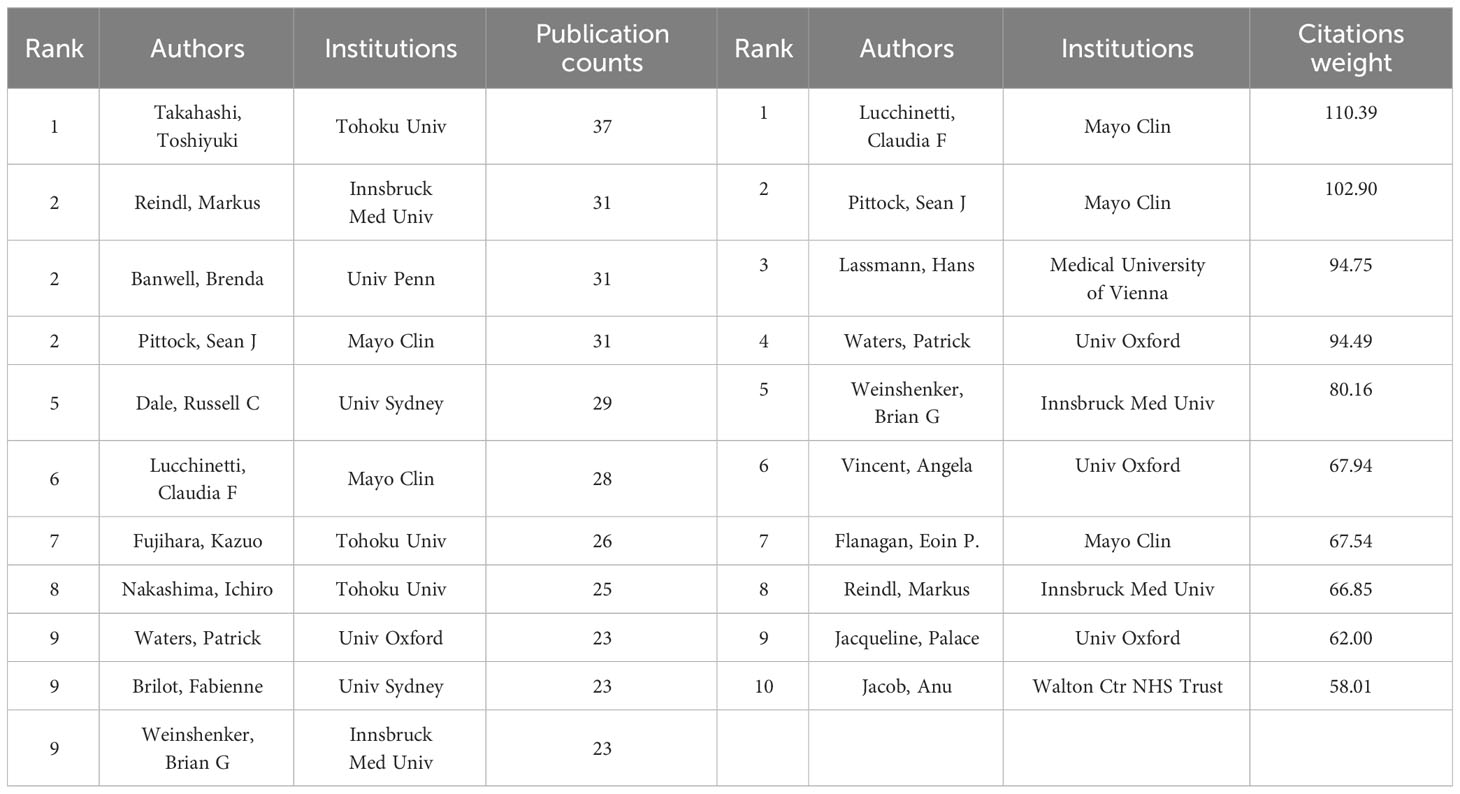
Table 2 Influential authors in the field of MOGAD related research.
Figure 5 shows the author’s collaborative network relationship. The network reflects strong connections between authors from different countries. A total of 871 authors with a minimum of 5 documents were analyzed using VOSviewer. The top 5 authors with largest total link strength were as follows: Rostasy Kevin (total link strength =1975 times), WatersPatrick (total link strength = 1738 times), Reindl Markus (total link strength =1722 times), Lucchinetti Claudia F. (total link strength = 1373 times), and Wassmer Evangeline (total link strength = 1346 times).
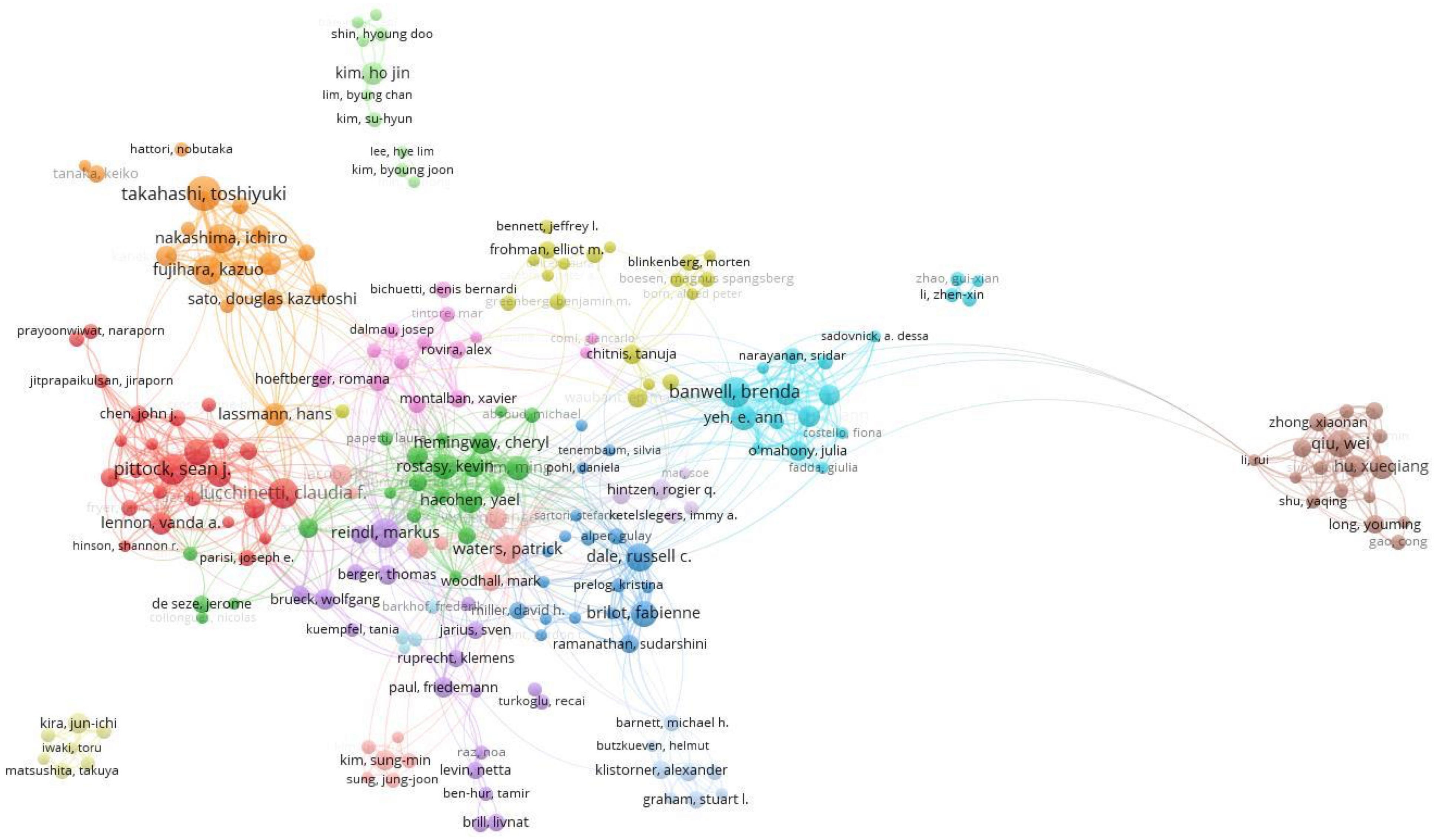
Figure 5 Cooperation network of authors.
Table 3 lists the top 10 productive journals in terms of MOGAD related publications and their respective Journal Impact Factor (JIF). Multiple Sclerosis and Related Disorders (JIF=4.0, 2022) has the highest number of publications (144). There were 138 publications in Multiple Sclerosis Journal (IF =5.8, 2022), 95 publications in Neurology (IF=9.9, 2022), 83 publications in Journal of Neuroimmunology (IF=3.3, 2022), and 74 articles in Journal of the Neurological Sciences (IF= 4.4, 2022).
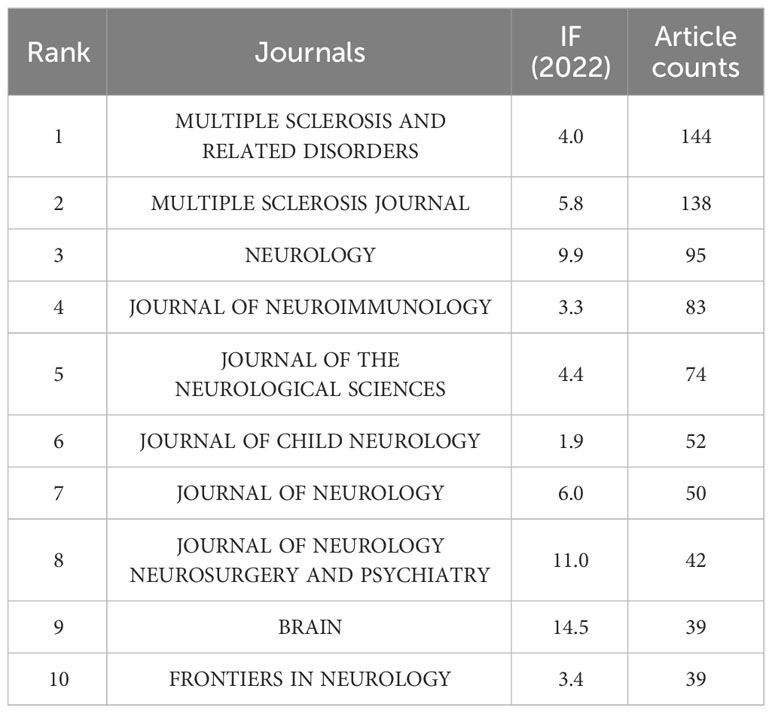
Table 3 Top 10 journals in the field of MOGAD related research.
Figure 6 plots 98 journals in terms of the total link strength. The top 5 journals with best total link strength were as follows: Neurology (total link strength =1832 times), Multiple Sclerosis Journal (total link strength =1222 times), Brain (total link strength = 833 times), Multiple Sclerosis and Related Disorders (total link strength = 762 times), and Journal of Neurology, Neurosurgery, and Psychiatry (total link strength = 539 times).
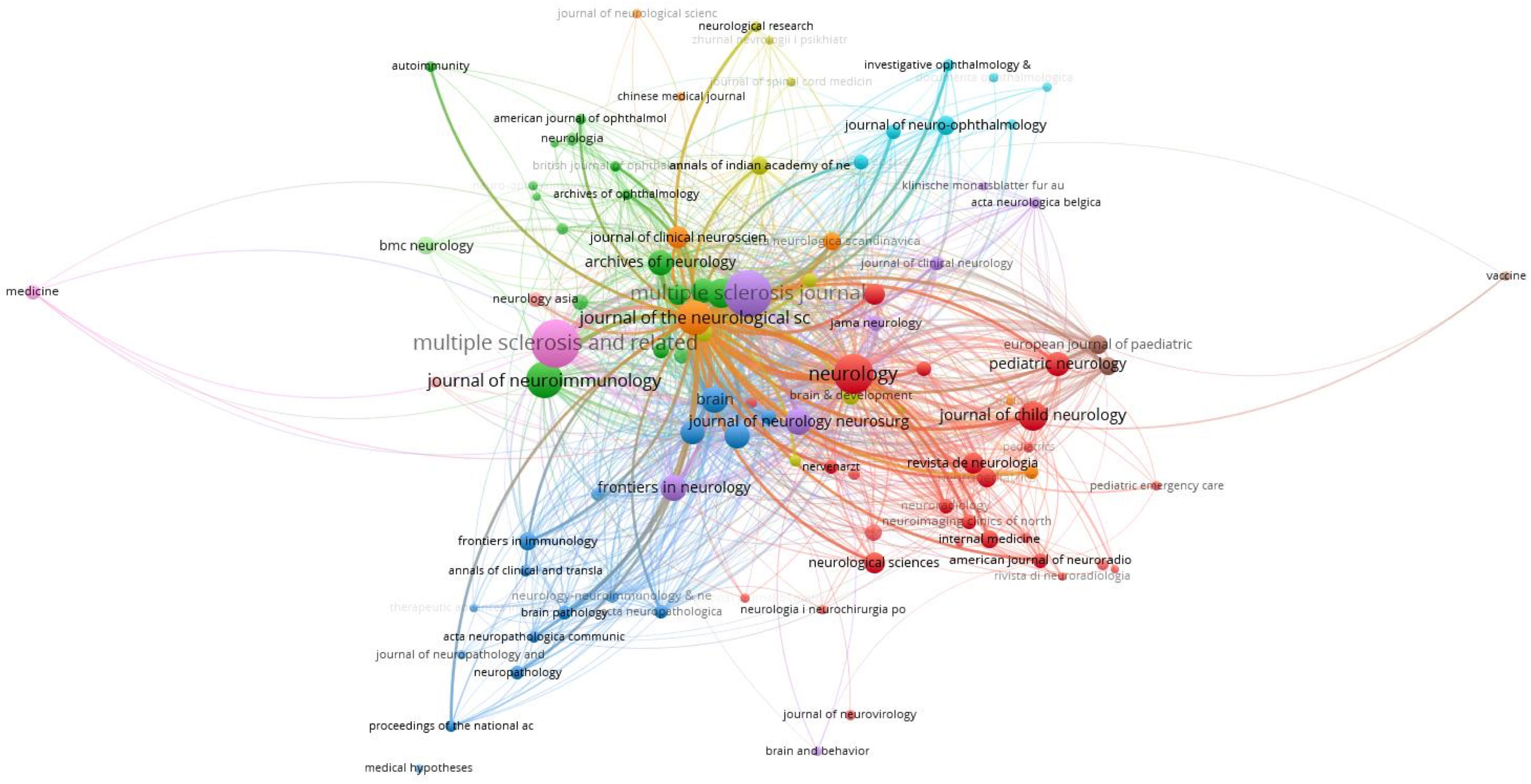
Figure 6 Co-occurrence network of journals.
The Journal Overlay Maps (Figure 7) is composed of a journal citing map (left) and a journal cited map (right) based on the clustering of discipline field. The co-citation links connecting the two maps shows the flow of disciplines. The horizontal axis of the ellipse represents the number of articles, and the vertical axis represents the number of authors. In the discipline field of Psychology, Education, Social, the number of authors and articles are more than others. There are 3 clusters (Medicine, Medical, Clinical/Molecular, Biology, Immunology/Neurology, Sports, Ophthalmology) in the journal citing map. And the discipline field has gradually developed to 3 clusters (Molecular, Biology, Genetics/Health, Nursing, Medicine/Psychology, Education, Social) shown in the journal cited map.
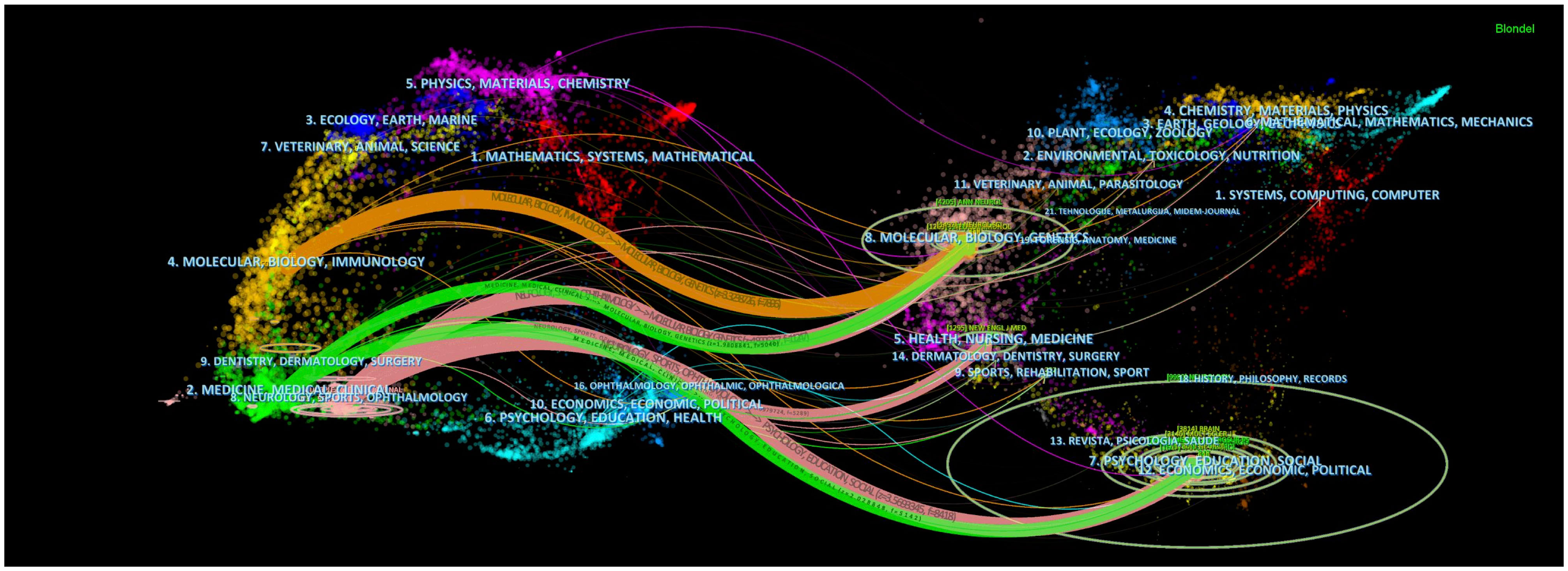
Figure 7 Journal overlay map related to MOGAD research.
A total of 841 articles in this field have more than 20 citations (Figure 8). The top 10 most cited documents are shown in Table 4. There were 2763 citations for “Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria”, followed by 1146 citations for “Intramuscular interferon beta-1a therapy initiated during a first demyelinating event in multiple sclerosis”. The third most frequently cited article was “A role for humoral mechanisms in the pathogenesis of Devic’s neuromyelitisoptica” with 873 citations.
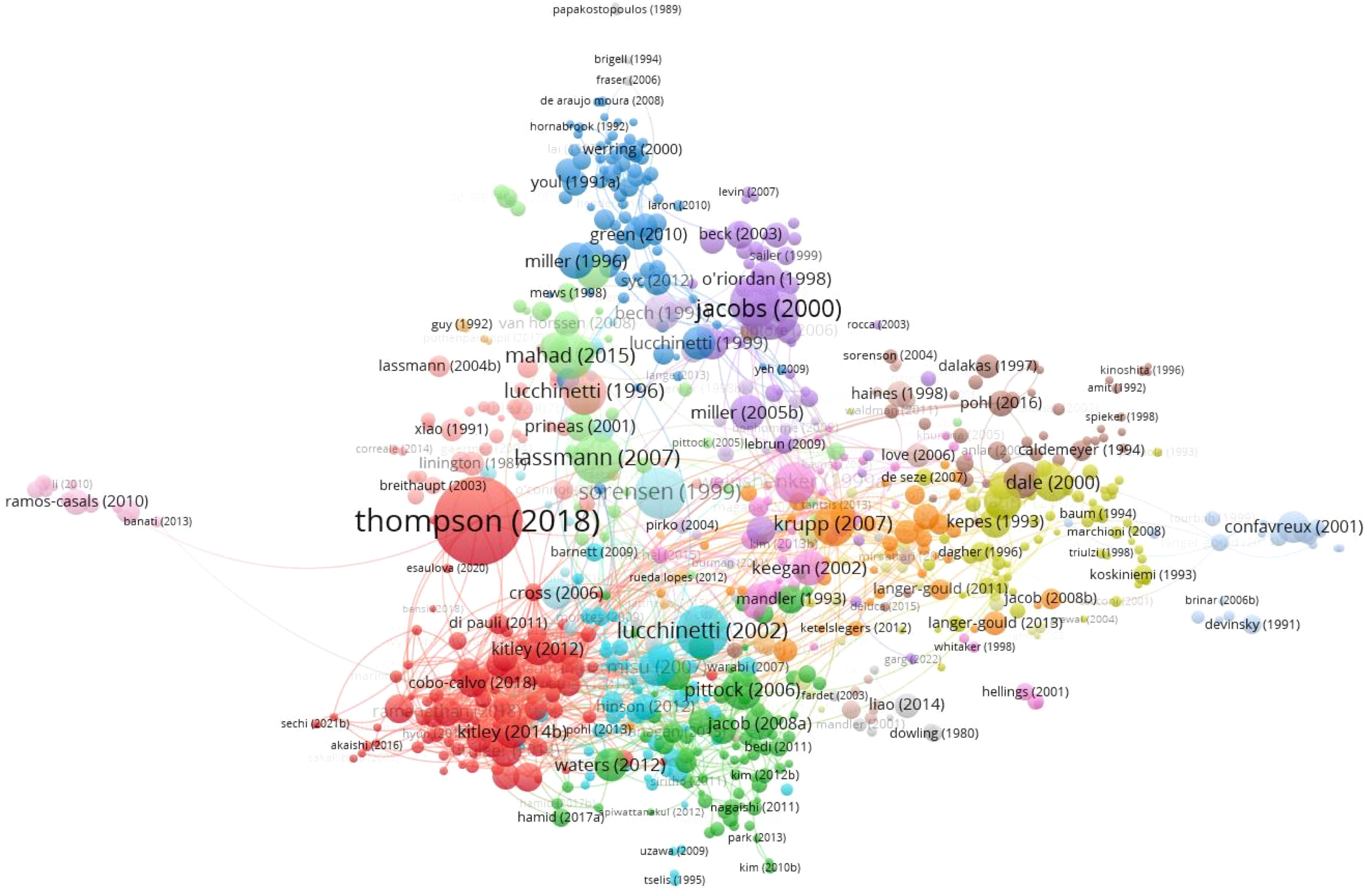
Figure 8 Citation network of articles related to MOGAD research.
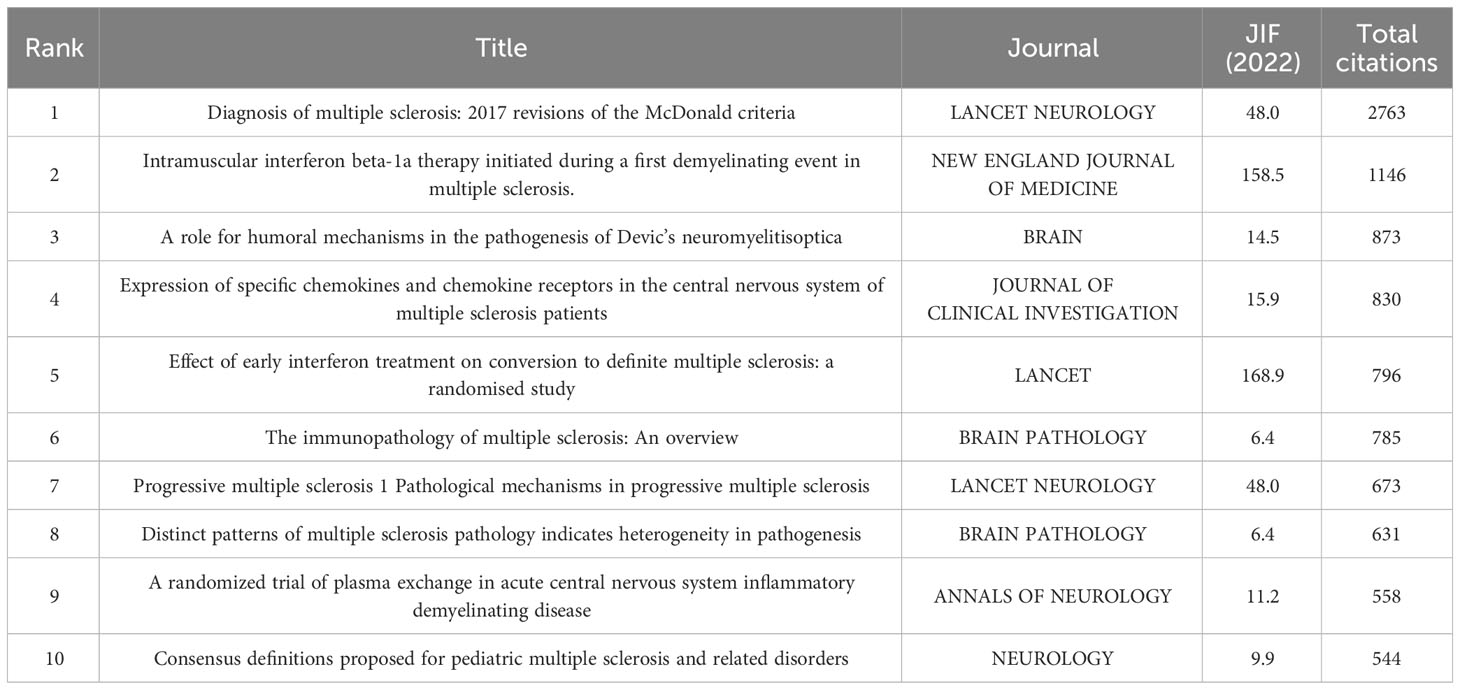
Table 4 Top 10 documents with the most citations in the field of MOGAD related research.
Table 5 shows the top 10 most average cited documents per year. Compared to the total citations, the annual average citation index can better reflect the attention paid to articles, as the annual average citation takes into account the factor of publication time. This will avoid the issue of the popularity of articles published in recent years being overlooked because low total citations. There were 577 citations for “Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria”, followed by 93 citations for “The spectrum of neuromyelitis optica”. The third most frequently cited article was “Progressive multiple sclerosis 1 Pathological mechanisms in progressive multiple sclerosis” with 82 citations.
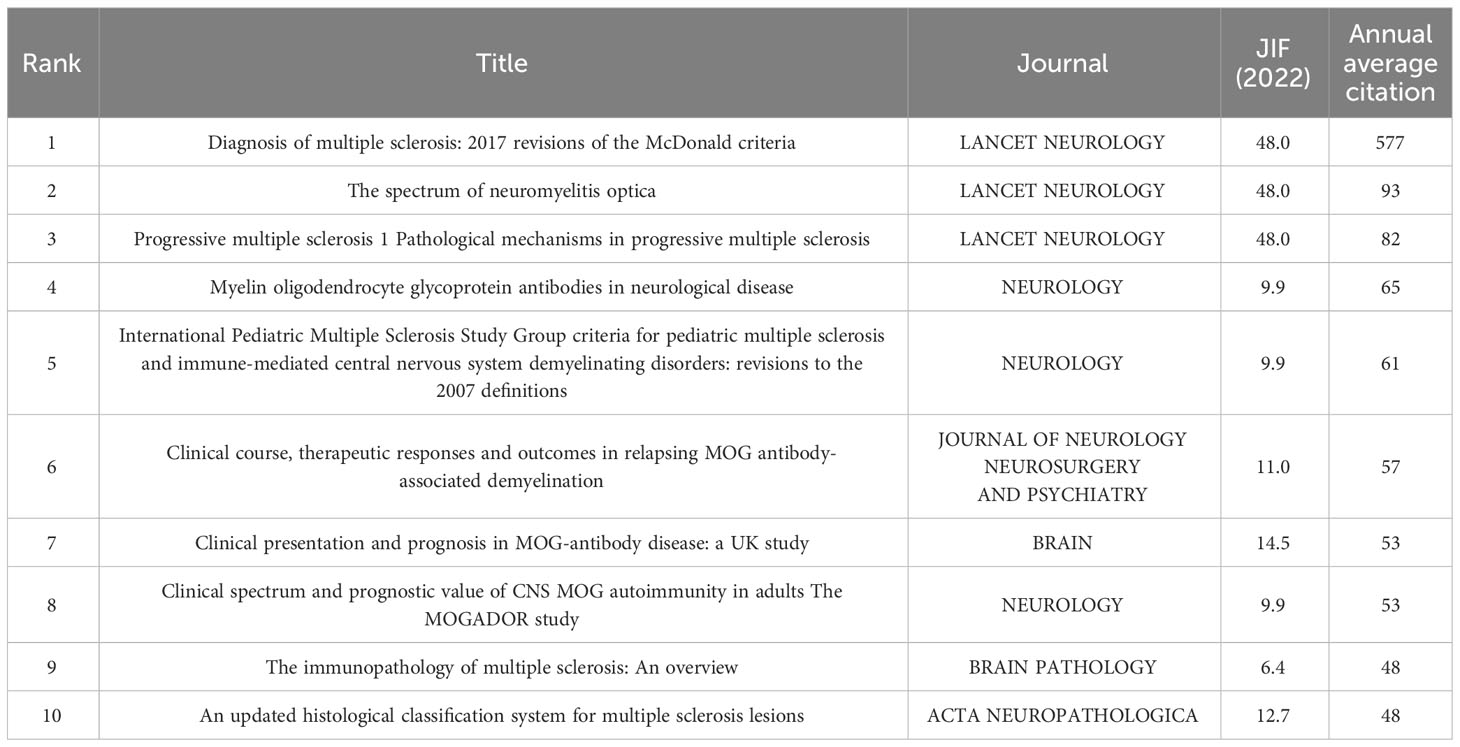
Table 5 Top 10 documents with the most annual average citation in the field of MOGAD related research.
In the co-occurrence analysis, a keyword was defined as the word that was used more than 5 times in titles or abstracts in all papers. 3295 keywords were extracted, of which 233 terms appeared more than 5 times. The top 10 keywords with the highest frequency in the field of MOGAD research are displayed in Table 6. “Multiple sclerosis” was the most frequent and strongest Link strength keyword. In addition, “neuromyelitis optica”, “optic neuritis”, “demyelination” and “acute disseminated encephalomyelitis” have stronger links among the keywords.
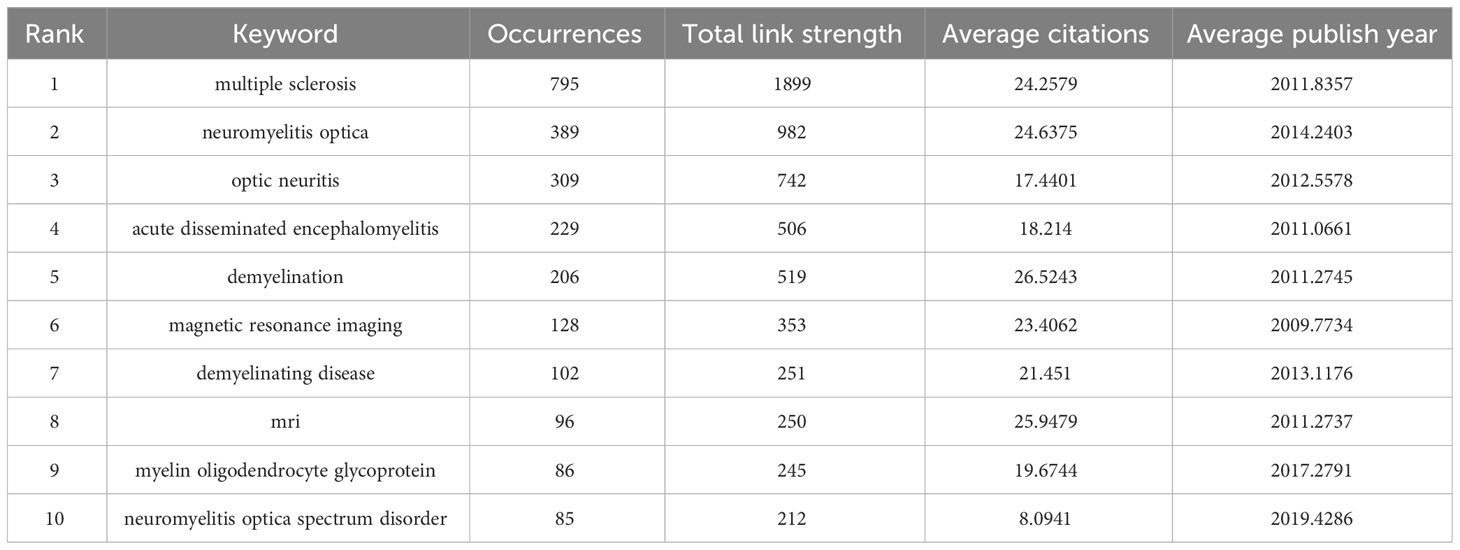
Table 6 Top 10 keywords with the highest frequency in the field of MOGAD related research.
In the co-occurrence analysis, a keyword was defined as the word that was used more than 5 times in titles or abstracts in all papers. The selected keywords were analyzed via VOSviewer. Figure 9A shows six clusters classified from 233 identified keywords. Cluster 1: Disease Phenotype (yellow); Cluster 2: Treatment (green); Cluster 3: Novel Coronavirus Infection and Vaccination (dark blue); Cluster 4: Immunopathological Mechanisms (Purple); Cluster 5: Clinical characteristics of children (orange); Cluster 6: Prognosis (red). In the “Disease Phenotype”cluster, the frequently used keywords were demyelination, ADEM, and NOMSD. In the “Treatment” cluster, the primary keywords were rituximab, corticosteroids, and immunoadsorption. In the “Novel Coronavirus Infection and Vaccination” cluster, the frequently used keywords werecovid-19, sars-cov-2, and vaccine. In the “Immunopathological Mechanisms” cluster, the dominantly used keywords were aquaporin 4, auto-antibodies, and autoimmunity. In the “Clinical characteristics of children” cluster, the main keywords used were children, acute disseminated encephalomyelitis, and epidemiology. Prognosis, outcome, acute transverse myelitis were the most commonly used keywords in the “Prognosis” cluster. The results exhibited the six most prominent directions of MOGAD-related research.
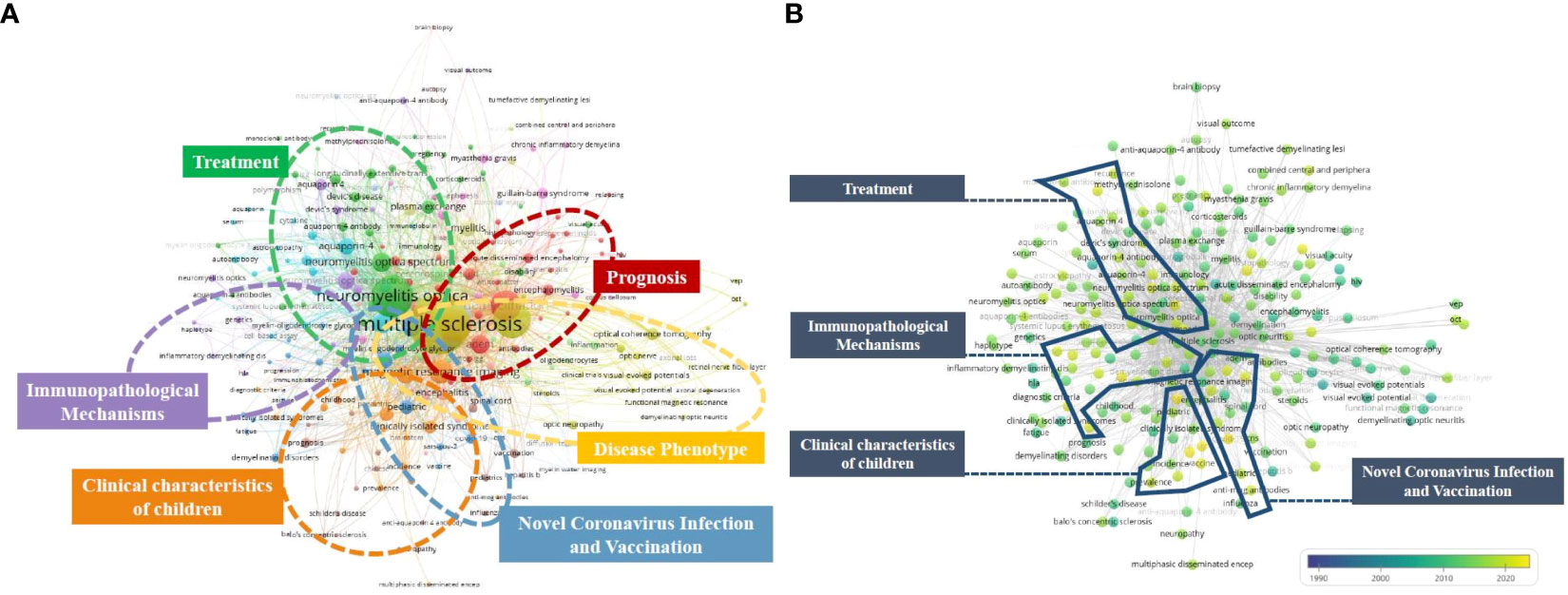
Figure 9 (A) Keyword co-occurrence network diagram of MOGAD. (B) Keyword co-occurrence average years network diagram of MOGAD.
In Figure 9B, the VOSviewer colored all keywords based on the average publication year they appeared in the MOGAD papers. Specifically, the yellow color indicates a more recent appearance (new words), while blue color indicates that the keywords appeared relatively early (old words).
The research trends of most studies in the six clusters are related to the novel coronavirus and vaccine (cluster 3), immunopathological mechanism (cluster 4), clinical characteristics of children (cluster 5), and treatment (cluster 2), suggesting that future research hotspots may be related to the novel coronavirus, pathogenesis, and special population.
Recent decade shave witnessed significant research on MOGAD, resulting in noteworthy advances in the understanding of disease phenotypes and their classification. However, there is a lack of international consensus regarding the diagnostic criteria for MOGAD. Moreover, there are several gaps in our understanding of the pathogenesis, treatment, and prognosis of MOGAD. At present, there is no bibliometric analysis on MOGAD. Therefore, the present study provides useful reference for relevant researchers to identify new research ideas and directions. This study provides an overview of the trends in the emergence of MOGAD. Notably, there has been a substantial rise in the annual publication count, particularly after 1991. Furthermore, the relative research interest (RRI) has exhibited a slight upward trajectory in recent years, signifying a growing popularity of this research domain. Approximately 72 countries have published research papers pertaining to MOGAD. Notably, the largest number of articles was published in the United States. Our study shows that the United States has high research quality and great academic influence in the field of MOGAD research, and has made the greatest contribution to publications. It also reflects that the United States has the most outstanding researchers and institutions in the world, and is a highly productive and leading country in the field of MOGAD. We found that while the Netherlands only ranks 15th in the number of publications, it has made significant progress in the average frequency of citations per article, ranking third. At the opposite end of the spectrum is China, which, although ranked second in terms of total number of publications, performs relatively poorly in terms of total and average number of citations. Therefore, China needs to investigate and resolve the contradiction between the quantity and quality of research published by Chinese researchers in order to further improve the quality of MOGAD related research. The Mayo Clinic USA, University College London, and the University of Sydney have made significant contributions to MOGAD related research. Notably, approximately 60% of research institutions are located in the top five countries by volume, indicating that leading research institutions play a pivotal role in enhancing a country’s academic research ranking. Our study shows that future research on MOGAD needs to be conducted through further cooperation and exchanges with leading countries to guide researchers to publish higher quality papers.
The Japanese authors with the highest ranking and most publications hold a critical position in the field of MOGAD, indicating Japan’s significant contribution. These early participants have likely pioneered new advancements in the field of MOGAD. Additionally, based on collaborative analysis, the research relationships between authors from different countries appear to be relatively dispersed, indicating a lack of academic connections and communication among them. Therefore, it is imperative for authors from diverse countries and institutions to enhance collaboration in order to collectively advance research on MOGAD. Almost all the studies related to MOGAD have been published in journals in the field of neurology. The top 5 journals with the highest combined link strength are Neurology, Journal of Multiple Sclerosis, Brain, Multiple Sclerosis and Related Disorders, and Journal of Neurology Neurosurgery and Psychiatry, which will be the journals of choice for researchers to publish high-quality research in the future. According to the results of co-citation and total citation analysis, Lancet Neurology has made significant contributions in the field of MOGAD research. Although the number of publications is small, the quality of publications in the fields of molecular biology, immunology and pharmacology is prioritized.
The co-occurrence analysis of keywords and bursts provides insights into the development trends and hotspots of MOGAD related research. “Multiple sclerosis” was the most frequently cited burst keyword, indicating its significance in the early stages of research on MOGAD. For instance, in the 1990s, Xiao BG et al. identified MOG as a potential target for antibody-mediated immune attack in experimental autoimmune encephalomyelitis (EAE), which has been extensively used as the model of MS. This demonstrated the significance of anti-MOG antibodies in MS CSF. The cluster analysis performed in our study not only reflects the primary research trends in MOGAD but also provide insights into future research directions.
The last 15 years have witnessed a significant shift in the global concept of inflammatory demyelinating disorders of the CNS, with the identification of distinct autoantibody-associated disorders such as aquaporin 4-IgG-positive neuromyelitisoptica spectrum disorder and MOGAD, which are distinct from MS (5, 37–39). MOGAD is a newly identified autoimmune disorder manifesting as CNS demyelination in both adults and children. It can present with various clinical phenotypes, including ON, myelitis, encephalitis, ADEM, NMOSD, or any combination of these entities. The frequency of MOGAD varies depending on the phenotype in both adults and children. In a single-center retrospective study, serum anti-MOG antibodies were detected in 60% (12 out of 20) of adult patients with acute disseminated encephalomyelitis (ADEM) either at onset or during follow-up (17). In a population-based Danish study, anti-MOG antibodies were detected in 4% (2/51) of adults with initial ON (26). Additionally, in two retrospective studies of individuals with anti-APQ4 antibody seronegative longitudinal extensive TM, 16-23% of cases tested positive for anti-MOG antibodies (40, 41). MOG antibodies are detectable in up to 64% of children with ADEM and in nearly all children who relapse after acute disseminated myelitis (including multistage ADEM or acute NMOSD) (13, 42, 43). However, MOG antibodies were detected in 33-43% of pediatric patients with ON and only in 3 (6%) out of 50 children with myelitis (22). As the understanding of MOGAD continues to evolve, there is a constant update on its clinical phenotype, which has become a research hotspot.
In 1999, a groundbreaking randomized controlled double-blind trial demonstrated the effectiveness of plasma exchange in patients with severe demyelinating episodes who did not respond to intravenous glucocorticoids (44). Observational studies have shown that a brief course of intravenous steroids can achieve significant symptom relief in MOGAD (18, 19, 45, 46). In patients who do not respond to intravenous glucocorticoids or those with severe disease, plasma exchange, immunoadsorption therapy, intravenous immune globulin, or a combination of plasma exchange followed by intravenous immune globulin may be necessary (47). Patients with a monophasic course of MOGAD account for 40-50% of cases, and the majority exhibit a favorable prognosis. Consequently, there is no clear consensus on the need for long-term immunosuppressive therapy. In general, preventative immunotherapy should be considered for patients who experience two or more relapses or severe functional disability following their initial episode (11, 48, 49).The majority of current literature is based on real-world clinical data from MOGAD patients, and there is a dearth of clinical trials pertaining to MOGAD treatment as well as related studies examining the risk factors for recurrence and predictors of long-term efficacy. These areas are poised to emerge as key areas of focus in future MOGAD research.
Following the emergence of the 2019 novel coronavirus, there has been a surge in literature pertaining to COVID-19, SARS-CoV-2, and vaccines. In 2021, Japanese scholar Kenji Kashiwagi reported the first case of acute ON associated with MOG antibody potentially induced by COVID-19 in adults (50). With the increasing number of case reports, large-scale studies, and reviews on COVID-19 in patients with NMOSD and MOGAD, there has been a gradual increase in knowledge regarding this topic (51–54). Aksel Siva et al. (2022) conducted a retrospective study of 63 COVID-19 patients with NMOSD and MOGAD from 25 centers. They found that advanced age, high disability rate, and comorbidities were risk factors for severe COVID-19 in NMOSD and MOGAD patients (55).Studies have shown that approximately 20% of MOGAD cases manifest initially following COVID-19 infection or vaccination (6, 56–58). The literature provides a comprehensive review of the epidemiological, clinical, imaging, electrophysiological, and laboratory characteristics as well as treatment outcomes for patients with SARS-CoV-2 and COVID-19 vaccine-associated MOGAD. Such patients exhibit severe symptoms at onset and typically require escalated immunotherapy while maintaining long-term persistence of MOG-IgG (59). Previous studies have indicated that approximately 30% of patients with MOGAD exhibit a prodromal history of infection or vaccination (60). However, the overall risk for developing MOGAD or experiencing a relapse after SARS-CoV-2 infection/vaccination appears to be exceedingly low (61). These findings suggest that certain novel environments associated with an elevated risk for neuroautoimmune disease development may also be linked to the emergence of MOGAD.
The trigger for the production of anti-MOG antibodies remains unknown, but is likely attributable to the induction of autoimmunity in the peripheral immune system. Although infection-induced autoimmunity may serve as a trigger, disease-specific pathogens have yet to be identified. Potential mechanisms of post-infection autoimmunity include molecular mimicry, bystander activation, epitope spreading, B-cell receptor-mediated antigen co-capture, and polyclonal activation of B cells (62–64). The presence of anti-MOG antibodies and plasma cells can also augment the activation of cognate MOG-specific CD4+ T cells or myelin basic protein-specific T effector cells and macrophages in the CNS (65). Kaneko K et al. found elevated levels of proinflammatory cytokines (IL-6, IL-17, G-CSF, and TNFα), as well as B-cell cytokines and chemokines (BAFF, APRIL, CXCL13, and CCL19) in the CSF of patients with MOGAD compared to that in healthy controls (62). It has been proposed that anti-MOG antibodies can directly trigger the classical pathway of the complement cascade, leading to demyelination. Both children and adults with MOGAD exhibit a significant increase in proteins indicating systemic activation of the classical and alternative complement pathways, which may result in CNS damage caused by activated complement proteins (66). Due to the gaps in our understanding of the pathogenesis of MOGAD, research on immunopathological mechanisms is currently a key research focus.
The seropositivity rate of MOG-IgG in pediatric patients is higher than that in adults (7), with approximately 34% of children diagnosed with acquired demyelinating diseases testing positive for MOG antibodies. There is no significant seasonal variation observed in the onset or recurrence of MOG-IgG related disorders (8).No significant sex-based differences have been noted (male-to-female ratio 1:1.3) (9). MOGAD is characterized by age-dependent phenotypic expression (67), seizure severity, and recovery outcomes (60).The primary clinical phenotypes observed in children with MOGAD are ADEM (53%), ON (40%), and TM (18%) (2). Children with ADEM typically exhibit multifocal and asymmetric white matter abnormalities on MRI, while those with leukodystrophy tend to present with fused, bilateral, and essentially symmetric white matter abnormalities on MRI. These abnormalities are more prevalent in young children (mean onset age: 3.7 years), and their prognosis is worse than that of other patients, possibly due to the immaturity of CNS development (68). Older children are more prone to present with ON and/or TM as well as brainstem symptoms (22, 68). The coexistence of MOGAD and other autoantibodies has been reported, with double-positive patients exhibiting greater overlap in clinical manifestations with NMDAR encephalitis and greater similarity in MRI changes with MOGAD (69, 70). While children have a relatively low risk of recurrence, the majority of other patients experience a monophasic course (22).Less than10% of relapsing children (typically very young) exhibit a leukodystrophic phenotype characterized by large confluent hyper-enhancing lesions on MRI and progressive brain atrophy leading to permanent cognitive and motor disability (68).
Despite favorable clinical outcomes in the majority of MOGAD patients, recurrence rates remain high and a subset of patients may experience residual disabilities including visual impairment, motor dysfunction, cognitive deficits, sensory disturbances, bladder dysfunction, and epilepsy (19). Patients with the TM phenotype are more likely to experience physical dysfunction, whereas those with the ON phenotype tend to exhibit less disability (19, 71). Relapse is defined as the onset of new symptoms at least three months after disease onset, with or without steroid treatment (24, 25). Numerous studies have reported that patients exhibiting certain factors are more prone to experiencing a recurrent course, including clinical phenotype of ON, persistent high levels of MOG antibodies, MRI manifestations of cortical encephalitis and leukodystrophy, as well as concomitant presence of other autoantibodies such as anti-NMDAR antibody (63, 68, 69). A study revealed decreased brain volume in adults with MOGAD compared to healthy individuals (72). Furthermore, patients with recurrent episodes exhibited significant reductions in total brain volume, deep gray matter, cerebellum, and hippocampus when compared to those with a monophasic course (72). Several studies have suggested that the neutrophil-to-lymphocyte ratio can serve as a potential biomarker for predicting recurrence in MOGAD. This ratio only increases during the clinical onset of MOGAD and remains stable during remission, indicating its correlation with disease activity. These findings may aid in more accurate recurrence prediction and facilitate improved treatment decisions (73).
The aforementioned analysis provides insights on the likely future trends and potential impacts of diseases related to MOG antibodies. According to a review published in Nature Reviews in 2018, future studies will focus on the mechanisms of MOGAD tolerance and age-dependent mechanisms of disease recurrence, and the genetic factors associated with MOGAD need to be identified. A review published in The Lancet in 2021 stated that future research should be more important to understand the mechanism behind the development of MOG autoimmune response, and there is an urgent need to identify disease-specific biomarkers of outcome and treatment response, which may pave the way for antigen-specific immunotherapy (5, 6). Similar to our research trend, with the advancement of medicine, the focus of research has shifted from clinical phenotype/characteristics to special populations, biomarkers, and molecular biological mechanisms. This shift will have a significant impact on future research. The patients exhibiting diverse phenotypes and possessing anti-MOG antibodies may harbor distinct underlying pathobiology driving their disease. In the future, advancements in in-vivo and in-vitro models, such as human-derived oligodendrocyte cultures, rodent models expressing humanized MOG, or animal models featuring MOG proteins with a higher homology to human MOG than rodents, will offer an enhanced foundation for investigating the pathogenic mechanisms. The identification of markers indicating disease outcome holds paramount significance for clinicians to propose optimal therapy and management strategies at disease onset. For future research, the formulation of a sophisticated analytical approach is crucial, particularly considering that only antibodies capable of recognizing properly folded MOG protein exhibit pathogenicity. The identification of new biomarkers may prove instrumental in monitoring disease activity in MOGAD. It is imperative to establish treatment protocols for MOGAD in the coming years. Investigating antigen-specific CD4+ T-cells and B-cells will be pivotal in gaining a deeper understanding of the mechanisms underlying autoimmune responses to MOG and will pave the way for antigen-specific immune therapies. Conducting multicenter international studies will not only expand our current knowledge but also enable us to evaluate initial therapy options as well as intensified therapeutic approaches.
The significant advantage of our study lies in the extensive analysis of global publications on MOGAD from the perspective of scientific literature. Bibliometric analysis methods in this study are necessary and valuable, which can quantitatively reflect research status and practical applications simultaneously. It is important to be aware of the limitations of the work. The first issue concerns the search strategy. We use the database of Web of Science Core Collection (WoSCC) for analysis, which it is the most commonly used bibliometric analysis database. Because the format of literature data in WoSCC is very standardized and has a very complete citation network relationship. Moreover, the existing knowledge map software support the extraction and meta-analysis of multi-database records from WoSCC very much. The realistic dilemma is that the document included in one database may not be comprehensive. Using the other citation databases such as Scopus or SciFinder somewhat different results may be found. The second issue concerns the bibliometrics, which has been debated by some researchers. In our study, quantitative metrics such as the number of publications and the number of citations (Total citations and Annual average citation) were used to reflect the co-authorship, co-occurrence, and co-citation. Some researchers like Garfield (74) and Lynch (75) think these metrics above should not be understood as quality measures or endorsements of the research outputs, and high citation rate does not imply correctness or impact beyond the academic context. So, developing more objective quantitative metrics is one of the important goals in the future. In addition, since the research included in this paper is not comprehensive enough on the research about the identification of markers of the disease status and outcome and the establishment of in vivo and in vitro models of MOGAD. Finally, prospective randomized controlled trials with large sample sizes should be conducted to establish the most optimal way of care and treatment strategy.
In conclusion, this study represents the first comprehensive bibliometric analysis of global research related to MOGAD since 1947. The systematic summary of global publishing trends identifies the leading authors, institutions, and journals in the field. Furthermore, the utilization of key words and co-citation cluster analysis identifies the main research avenues, primarily encompassing “phenotypes”, “treatment”, “COVID-19 and vaccination”, “immunopathological mechanism”, “The clinical characteristics of the pediatric population” and “prognosis”. It is anticipated that future collaborations among authors, institutions, and countries will expedite advancements in the study of MOGAD.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
SZ: Conceptualization, Data curation, Writing – original draft. YW: Conceptualization, Data curation, Writing – original draft. JG: Methodology, Software, Writing – review & editing. XL: Formal analysis, Methodology, Writing – review & editing. LH: Formal analysis, Funding acquisition, Supervision, Visualization, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by 2023 China Medical University High-quality Development Fund (2023JH2/20200119), CAAE Epilepsy Research Fund (CX-B-2021-02), Henan Pediatric Disease Clinical Medical Research Center Foundation (YJZX202207), Medical Education Research Project of Liaoning Province (2022-N004-09).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Satukijchai C, Mariano R, Messina S, Sa M, Woodhall MR, Robertson NP, et al. Factors associated with relapse and treatment of myelin oligodendrocyte glycoprotein antibody-associated disease in the United Kingdom. JAMA Netw Open (2022) 5(1):e2142780. doi: 10.1001/jamanetworkopen.2021.42780
2. Bruijstens AL, Lechner C, Flet-Berliac L, Deiva K, Neuteboom RF, Hemingway C, et al. E.U. paediatric MOG consortium consensus: Part 1 - Classification of clinical phenotypes of paediatric myelin oligodendrocyte glycoprotein antibody-associated disorders. Eur J Paediatr Neurol (2020) 29:2–13. doi: 10.1016/j.ejpn.2020.10.006
3. Ramanathan S, Dale RC, Brilot F. Anti-MOG antibody: The history, clinical phenotype, and pathogenicity of a serum biomarker for demyelination. Autoimmun Rev (2016) 15(4):307–24. doi: 10.1016/j.autrev.2015.12.004
4. Johns TG, Bernard CC. The structure and function of myelin oligodendrocyte glycoprotein. J Neurochem (1999) 72(1):1–9. doi: 10.1046/j.1471-4159.1999.0720001.x
5. Reindl M, Waters P. Myelin oligodendrocyte glycoprotein antibodies in neurological disease. Nat Rev Neurol (2019) 15(2):89–102. doi: 10.1038/s41582-018-0112-x
6. Marignier R, Hacohen Y, Cobo-Calvo A, Pröbstel AK, Aktas O, Alexopoulos H, et al. Myelin-oligodendrocyte glycoprotein antibody-associated disease. Lancet Neurol (2021) 20(9):762–72. doi: 10.1016/S1474-4422(21)00218-0
7. de Mol CL, Wong Y, van Pelt ED, Wokke B, Siepman T, Neuteboom RF, et al. The clinical spectrum and incidence of anti-MOG-associated acquired demyelinating syndromes in children and adults. Mult Scler (2020) 26(7):806–14. doi: 10.1177/1352458519845112
8. Dos Passos GR, Elsone L, Luppe S, Kitley J, Messina S, Rodríguez Cruz PM, et al. Seasonal distribution of attacks in aquaporin-4 antibody disease and myelin-oligodendrocyte antibody disease. J Neurol Sci (2020) 415:116881. doi: 10.1016/j.jns.2020.116881
9. Jarius S, Lechner C, Wendel EM, Baumann M, Breu M, Schimmel M, et al. Cerebrospinal fluid findings in patients with myelin oligodendrocyte glycoprotein (MOG) antibodies. Part 2: Results from 108 lumbar punctures in 80 pediatric patients. J Neuroinflamm (2020) 17(1):262. doi: 10.1186/s12974-020-01825-1
10. Asseyer S, Hamblin J, Messina S, Mariano R, Siebert N, Everett R, et al. Prodromal headache in MOG-antibody positive optic neuritis. Mult Scler Relat Disord (2020) 40:101965. doi: 10.1016/j.msard.2020.101965
11. Zhou J, Lu X, Zhang Y, Ji T, Jin Y, Xu M, et al. Follow-up study on Chinese children with relapsing MOG-IgG-associated central nervous system demyelination. Mult Scler Relat Disord (2019) 28:4–10. doi: 10.1016/j.msard.2018.12.001
12. Song H, Zhou H, Yang M, Tan S, Wang J, Xu Q, et al. Clinical characteristics and prognosis of myelin oligodendrocyte glycoprotein antibody-seropositive paediatric optic neuritis in China. Br J Ophthalmol (2019) 103(6):831–6. doi: 10.1136/bjophthalmol-2018-312399
13. Duignan S, Wright S, Rossor T, Cazabon J, Gilmour K, Ciccarelli O, et al. Myelin oligodendrocyte glycoprotein and aquaporin-4 antibodies are highly specific in children with acquired demyelinating syndromes. Dev Med Child Neurol (2018) 60(9):958–62. doi: 10.1111/dmcn.13703
14. Krupp LB, Tardieu M, Amato MP, Banwell B, Chitnis T, Dale RC, et al. International Pediatric Multiple Sclerosis Study Group criteria for pediatric multiple sclerosis and immune-mediated central nervous system demyelinating disorders: revisions to the 2007 definitions. Mult Scler (2013) 19(10):1261–7. doi: 10.1177/1352458513484547
15. Zhao-Fleming HH, Valencia Sanchez C, Sechi E, Inbarasu J, Wijdicks EF, Pittock SJ, et al. CNS demyelinating attacks requiring ventilatory support with myelin oligodendrocyte glycoprotein or aquaporin-4 antibodies. Neurology (2021) 97(13):e1351–1351e1358. doi: 10.1212/WNL.0000000000012599
16. Camera V, Holm-Mercer L, Ali A, Messina S, Horvat T, Kuker W, et al. Frequency of new silent MRI lesions in myelin oligodendrocyte glycoprotein antibody disease and aquaporin-4 antibody neuromyelitis optica spectrum disorder. JAMA Netw Open (2021) 4(12):e2137833. doi: 10.1001/jamanetworkopen.2021.37833
17. López-Chiriboga AS, Majed M, Fryer J, Dubey D, McKeon A, Flanagan EP, et al. Association of MOG-igG serostatus with relapse after acute disseminated encephalomyelitis and proposed diagnostic criteria for MOG-igG-associated disorders. JAMA Neurol (2018) 75(11):1355–63. doi: 10.1001/jamaneurol.2018.1814
18. Jurynczyk M, Messina S, Woodhall MR, Raza N, Everett R, Roca-Fernandez A, et al. Clinical presentation and prognosis in MOG-antibody disease: a UK study. Brain (2017) 140(12):3128–38. doi: 10.1093/brain/awx276
19. Ramanathan S, Mohammad S, Tantsis E, Nguyen TK, Merheb V, Fung V, et al. Clinical course, therapeutic responses and outcomes in relapsing MOG antibody-associated demyelination. J Neurol Neurosurg Psychiatry (2018) 89(2):127–37. doi: 10.1136/jnnp-2017-316880
20. Jarius S, Paul F, Aktas O, Asgari N, Dale RC, de Seze J, et al. MOG encephalomyelitis: international recommendations on diagnosis and antibody testing. J Neuroinflamm (2018) 15(1):134. doi: 10.1186/s12974-018-1144-2
21. Fadda G, Banwell B, Waters P, Marrie RA, Yeh EA, O'Mahony J, et al. Silent new brain MRI lesions in children with MOG-antibody associated disease. Ann Neurol (2021) 89(2):408–13. doi: 10.1002/ana.25957
22. Waters P, Fadda G, Woodhall M, O'Mahony J, Brown RA, Castro DA, et al. Serial anti-myelin oligodendrocyte glycoprotein antibody analyses and outcomes in children with demyelinating syndromes. JAMA Neurol (2020) 77(1):82–93. doi: 10.1001/jamaneurol.2019.2940
23. Ketelslegers IA, Visser IE, Neuteboom RF, Boon M, Catsman-Berrevoets CE, Hintzen RQ. Disease course and outcome of acute disseminated encephalomyelitis is more severe in adults than in children. Mult Scler (2011) 17(4):441–8. doi: 10.1177/1352458510390068
24. Hacohen Y, Wong YY, Lechner C, Jurynczyk M, Wright S, Konuskan B, et al. Disease course and treatment responses in children with relapsing myelin oligodendrocyte glycoprotein antibody-associated disease. JAMA Neurol (2018) 75(4):478–87. doi: 10.1001/jamaneurol.2017.4601
25. Baumann M, Sahin K, Lechner C, Hennes EM, Schanda K, Mader S, et al. Clinical and neuroradiological differences of paediatric acute disseminating encephalomyelitis with and without antibodies to the myelin oligodendrocyte glycoprotein. J Neurol Neurosurg Psychiatry (2015) 86(3):265–72. doi: 10.1136/jnnp-2014-308346
26. Soelberg K, Jarius S, Skejoe H, Engberg H, Mehlsen JJ, Nilsson AC, et al. A population-based prospective study of optic neuritis. Mult Scler (2017) 23(14):1893–901. doi: 10.1177/1352458517734070
27. Yang Z, Lin J, Li H, He Z, Wang K, Lei L, et al. Bibliometric and visualization analysis of macrophages associated with osteoarthritis from 1991 to 2021. Front Immunol (2022) 13:1013498. doi: 10.3389/fimmu.2022.1013498
28. Wu K, Liu Y, Liu L, Peng Y, Pang H, Sun X, et al. Emerging trends and research foci in tumor microenvironment of pancreatic cancer: A bibliometric and visualized study. Front Oncol (2022) 12:810774. doi: 10.3389/fonc.2022.810774
29. Chen Y, You Y, Wang Y, Wang Y, Dai T. Global insights into rural health workers' Job satisfaction: A scientometric perspective. Front Public Health (2022) 10:895659. doi: 10.3389/fpubh.2022.895659
30. You Y, Min L, Tang M, Chen Y, Ma X. Bibliometric evaluation of global tai chi research from 1980-2020. Int J Environ Res Public Health (2021) 18(11):6150. doi: 10.3390/ijerph18116150
31. Zhang L, Yu K, Zhu B, Mei S, Huo J, Zhao Z. Trends in research related to vaccine and cancer prevention from 1992 to 2022: A 30-years bibliometric analysis. Hum Vaccin Immunother (2023) 19(1):2207441. doi: 10.1080/21645515.2023.2207441
32. You Y, Wang D, Liu J, Chen Y, Ma X, Li W. Physical exercise in the context of air pollution: an emerging research topic. Front Physiol (2022) 13:784705. doi: 10.3389/fphys.2022.784705
33. Robert C, Wilson CS. Thirty-year survey of bibliometrics used in the research literature of pain: Analysis, evolution, and pitfalls. Front Pain Res (Lausanne) (2023) 4:1071453. doi: 10.3389/fpain.2023.1071453
34. Gunashekar S, Wooding S, Guthrie S. How do NIHR peer review panels use bibliometric information to support their decisions. Scientometrics (2017) 112(3):1813–35. doi: 10.1007/s11192-017-2417-8
35. Cascajares M, Alcayde A, Salmerón-Manzano E, Manzano-Agugliaro F. The bibliometric literature on scopus and woS: the medicine and environmental sciences categories as case of study. Int J Environ Res Public Health (2021) 18(11):5851. doi: 10.3390/ijerph18115851
36. Ullah R, Asghar I, Griffiths MG. An integrated methodology for bibliometric analysis: A case study of internet of things in healthcare applications. Sensors (Basel) (2022) 23(1):67. doi: 10.3390/s23010067
37. Lennon VA, Wingerchuk DM, Kryzer TJ, Pittock SJ, Lucchinetti CF, Fujihara K, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet (2004) 364(9451):2106–12. doi: 10.1016/S0140-6736(04)17551-X
38. O'Connor KC, McLaughlin KA, De Jager PL, Chitnis T, Bettelli E, Xu C, et al. Self-antigen tetramers discriminate between myelin autoantibodies to native or denatured protein. Nat Med (2007) 13(2):211–7. doi: 10.1038/nm1488
39. Flanagan EP. Neuromyelitis optica spectrum disorder and other non-multiple sclerosis central nervous system inflammatory diseases. Continuum (Minneap Minn) (2019) 25(3):815–44. doi: 10.1212/CON.0000000000000742
40. Cobo-Calvo Á, Sepúlveda M, Bernard-Valnet R, Ruiz A, Brassat D, Martínez-Yélamos S, et al. Antibodies to myelin oligodendrocyte glycoprotein in aquaporin 4 antibody seronegative longitudinally extensive transverse myelitis: Clinical and prognostic implications. Mult Scler (2016) 22(3):312–9. doi: 10.1177/1352458515591071
41. Jitprapaikulsan J, Chen JJ, Flanagan EP, Tobin WO, Fryer JP, Weinshenker BG, et al. Aquaporin-4 and myelin oligodendrocyte glycoprotein autoantibody status predict outcome of recurrent optic neuritis. Ophthalmology (2018) 125(10):1628–37. doi: 10.1016/j.ophtha.2018.03.041
42. Baumann M, Hennes EM, Schanda K, Karenfort M, Kornek B, Seidl R, et al. Children with multiphasic disseminated encephalomyelitis and antibodies to the myelin oligodendrocyte glycoprotein (MOG): Extending the spectrum of MOG antibody positive diseases. Mult Scler (2016) 22(14):1821–9. doi: 10.1177/1352458516631038
43. Rostásy K, Mader S, Hennes EM, Schanda K, Gredler V, Guenther A, et al. Persisting myelin oligodendrocyte glycoprotein antibodies in aquaporin-4 antibody negative pediatric neuromyelitis optica. Mult Scler (2013) 19(8):1052–9. doi: 10.1177/1352458512470310
44. Weinshenker BG, O'Brien PC, Petterson TM, Noseworthy JH, Lucchinetti CF, Dodick DW, et al. A randomized trial of plasma exchange in acute central nervous system inflammatory demyelinating disease. Ann Neurol (1999) 46(6):878–86. doi: 10.1002/1531-8249(199912)46:6<878::aid-ana10>3.0.co;2-q
45. Wong Y, Hacohen Y, Armangue T, Wassmer E, Verhelst H, Hemingway C, et al. Paediatric acute disseminated encephalomyelitis followed by optic neuritis: disease course, treatment response and outcome. Eur J Neurol (2018) 25(5):782–6. doi: 10.1111/ene.13602
46. Baumann M, Bartels F, Finke C, Adamsbaum C, Hacohen Y, Rostásy K, et al. E.U. paediatric MOG consortium consensus: Part 2 - Neuroimaging features of paediatric myelin oligodendrocyte glycoprotein antibody-associated disorders. Eur J Paediatr Neurol (2020) 29:14–21. doi: 10.1016/j.ejpn.2020.10.002
47. Hacohen Y, Banwell B. Treatment approaches for MOG-ab-associated demyelination in children. Curr Treat Options Neurol (2019) 21(1):2. doi: 10.1007/s11940-019-0541-x
48. Cobo-Calvo A, Sepúlveda M, Rollot F, Armangué T, Ruiz A, Maillart E, et al. Evaluation of treatment response in adults with relapsing MOG-Ab-associated disease. J Neuroinflamm (2019) 16(1):134. doi: 10.1186/s12974-019-1525-1
49. Chen JJ, Flanagan EP, Bhatti MT, Jitprapaikulsan J, Dubey D, Lopez Chiriboga A, et al. Steroid-sparing maintenance immunotherapy for MOG-IgG associated disorder. Neurology (2020) 95(2):e111–111e120. doi: 10.1212/WNL.0000000000009758
50. Kogure C, Kikushima W, Fukuda Y, Hasebe Y, Takahashi T, Shibuya T, et al. Myelin oligodendrocyte glycoprotein antibody-associated optic neuritis in a COVID-19 patient: A case report. Med (Baltimore) (2021) 100(19):e25865. doi: 10.1097/MD.0000000000025865
51. Durovic E, Bien C, Bien CG, Isenmann S. MOG antibody-associated encephalitis secondary to Covid-19: case report. BMC Neurol (2021) 21(1):414. doi: 10.1186/s12883-021-02449-5
52. Dias da Costa M, Leal Rato M, Cruz D, Valadas A, Antunes AP, Albuquerque L. Longitudinally extensive transverse myelitis with anti-myelin oligodendrocyte glycoprotein antibodies following SARS-CoV-2 infection. J Neuroimmunol (2021) 361:577739. doi: 10.1016/j.jneuroim.2021.577739
53. Sinha R, Wander A, Kapoor A, Yadav R, Kumar A, Gulati S. Acute demyelinating syndrome (MOG antibody positive) associated with COVID-19 infection: A widening spectrum. Clin Pediatr (Phila) (2021) 60(13):501–3. doi: 10.1177/00099228211037210
54. Feizi P, Sharma K, Pasham SR, Nirwan L, Joseph J, Jaiswal S, et al. Central nervous system (CNS) inflammatory demyelinating diseases (IDDs) associated with COVID-19: A case series and review. J Neuroimmunol (2022) 371:577939. doi: 10.1016/j.jneuroim.2022.577939
55. Sen S, Tuncer A, Ozakbas S, Uzunkopru C, Baba C, Demir S, et al. The Turkish experience of COVID-19 infection in people with NMOSD and MOGAD: A milder course. Mult Scler Relat Disord (2022) 58:103399. doi: 10.1016/j.msard.2021.103399
56. Netravathi M, Dhamija K, Gupta M, Tamborska A, Nalini A, Holla VV, et al. COVID-19 vaccine associated demyelination & its association with MOG antibody. Mult Scler Relat Disord (2022) 60:103739. doi: 10.1016/j.msard.2022.103739
57. Pandit L, Sudhir A, Malli C, D'Cunha A. COVID-19 infection and vaccination against COVID-19: Impact on managing demyelinating CNS disorders in Southern India- experience from a demyelinating disease registry. Mult Scler Relat Disord (2022) 66:104033. doi: 10.1016/j.msard.2022.104033
58. Gernert JA, Zimmermann H, Oswald E, Christmann T, Kümpfel T, Havla J. Clinical onset of CNS demyelinating disease after COVID-19 vaccination: denovo disease. Mult Scler Relat Disord (2022) 67:104175. doi: 10.1016/j.msard.2022.104175
59. Jarius S, Bieber N, Haas J, Wildemann B. MOG encephalomyelitis after vaccination against severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2): case report and comprehensive review of the literature. J Neurol (2022) 269(10):5198–212. doi: 10.1007/s00415-022-11194-9
60. Cobo-Calvo A, Ruiz A, Rollot F, Arrambide G, Deschamps R, Maillart E, et al. Clinical features and risk of relapse in children and adults with myelin oligodendrocyte glycoprotein antibody-associated disease. Ann Neurol (2021) 89(1):30–41. doi: 10.1002/ana.25909
61. Dinoto A, Sechi E, Ferrari S, Gajofatto A, Orlandi R, Solla P, et al. Risk of disease relapse following COVID-19 vaccination in patients with AQP4-IgG-positive NMOSD and MOGAD. Mult Scler Relat Disord (2022) 58:103424. doi: 10.1016/j.msard.2021.103424
62. Kaneko K, Sato DK, Nakashima I, Ogawa R, Akaishi T, Takai Y, et al. CSF cytokine profile in MOG-IgG+ neurological disease is similar to AQP4-IgG+ NMOSD but distinct from MS: a cross-sectional study and potential therapeutic implications. J Neurol Neurosurg Psychiatry (2018) 89(9):927–36. doi: 10.1136/jnnp-2018-317969
63. Spadaro M, Winklmeier S, Beltrán E, Macrini C, Höftberger R, Schuh E, et al. Pathogenicity of human antibodies against myelin oligodendrocyte glycoprotein. Ann Neurol (2018) 84(2):315–28. doi: 10.1002/ana.25291
64. Winklmeier S, Schlüter M, Spadaro M, Thaler FS, Vural A, Gerhards R, et al. Identification of circulating MOG-specific B cells in patients with MOG antibodies. Neurol Neuroimmunol Neuroinflamm (2019) 6(6):625. doi: 10.1212/NXI.0000000000000625
65. Spadaro M, Gerdes LA, Krumbholz M, Ertl-Wagner B, Thaler FS, Schuh E, et al. Autoantibodies to MOG in a distinct subgroup of adult multiple sclerosis. Neurol Neuroimmunol Neuroinflamm (2016) 3(5):e257. doi: 10.1212/NXI.0000000000000257
66. Keller CW, Lopez JA, Wendel EM, Ramanathan S, Gross CC, Klotz L, et al. Complement activation is a prominent feature of MOGAD. Ann Neurol (2021) 90(6):976–82. doi: 10.1002/ana.26226
67. Hennes EM, Baumann M, Schanda K, Anlar B, Bajer-Kornek B, Blaschek A, et al. Prognostic relevance of MOG antibodies in children with an acquired demyelinating syndrome. Neurology (2017) 89(9):900–8. doi: 10.1212/WNL.0000000000004312
68. Hacohen Y, Rossor T, Mankad K, Chong W, Lux A, Wassmer E, et al. 'Leukodystrophy-like' phenotype in children with myelin oligodendrocyte glycoprotein antibody-associated disease. Dev Med Child Neurol (2018) 60(4):417–23. doi: 10.1111/dmcn.13649
69. Weihua Z, Shuai G, Changhong R, Xiaotun R, Fang. Pediatric anti-N-methyl-D-aspartate receptor encephalitis with MOG-Ab co-existence: Relapse propensity and treatability. Mult Scler Relat Disord (2022) 58:103447. doi: 10.1016/j.msard.2021.103447
70. Hou C, Wu W, Tian Y, Zhang Y, Zhu H, Zeng Y, et al. Clinical analysis of anti-NMDAR encephalitis combined with MOG antibody in children. Mult Scler Relat Disord (2020) 42:102018. doi: 10.1016/j.msard.2020.102018
71. Lechner C, Baumann M, Hennes EM, Schanda K, Marquard K, Karenfort M, et al. Antibodies to MOG and AQP4 in children with neuromyelitis optica and limited forms of the disease. J Neurol Neurosurg Psychiatry (2016) 87(8):897–905. doi: 10.1136/jnnp-2015-311743
72. Rechtman A, Brill L, Zveik O, Uliel B, Haham N, Bick AS, et al. Volumetric brain loss correlates with a relapsing MOGAD disease course. Front Neurol (2022) 13:867190. doi: 10.3389/fneur.2022.867190
73. Benetou C, Berti F, Hemingway C, Hacohen Y, Lim M. Neutrophil-to-lymphocyte ratio correlates with disease activity in myelin oligodendrocyte glycoprotein antibody associated disease (MOGAD) in children. Mult Scler Relat Disord (2020) 45:102345. doi: 10.1016/j.msard.2020.102345
74. Garfield E. Is citation analysis a legitimate evaluation tool? Scientometrics (1979) 1:359–75. doi: 10.1007/BF02019306
Keywords: global trends, MOG antibody associated disease, bibliometric, visualization analysis, VOSviewer, Citespace
Citation: Zheng S, Wang Y, Geng J, Liu X and Huo L (2024) Global trends in research on MOG antibody-associated disease: bibliometrics and visualization analysis. Front. Immunol. 15:1278867. doi: 10.3389/fimmu.2024.1278867
Received: 17 August 2023; Accepted: 17 January 2024;
Published: 02 February 2024.
Edited by:
Fumitaka Shimizu, Yamaguchi University, JapanReviewed by:
Yuquan Chen, Chinese Academy of Medical Sciences and Peking Union Medical College, ChinaCopyright © 2024 Zheng, Wang, Geng, Liu and Huo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Liang Huo, aHVvbEBzai1ob3NwaXRhbC5vcmc=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.