 Marcos Adriano Garcia Campos1
Marcos Adriano Garcia Campos1 Tiago de Oliveira Valois2
Tiago de Oliveira Valois2 Luís Eduardo Magalhães1
Luís Eduardo Magalhães1 Lucas Fernandes Vasques3Rafael Goulart de Medeiros3
Lucas Fernandes Vasques3Rafael Goulart de Medeiros3 Denise Maria do Nascimento Costa4,5
Denise Maria do Nascimento Costa4,5 Natalino Salgado Filho1Raquel Moraes da Rocha Nogueira6
Natalino Salgado Filho1Raquel Moraes da Rocha Nogueira6 Precil Diego Miranda de Menezes Neves7
Precil Diego Miranda de Menezes Neves7 Gyl Eanes Barros Silva1,8*
Gyl Eanes Barros Silva1,8*- 1Clinical Hospital of State University Júlio de Mesquita Filho, State University of São Paulo, Botucatu, São Paulo, Brazil
- 2Divison of Nephrology, University Hospital of the Federal University of Maranhão, São Luís, Maranhão, Brazil
- 3Faculty of Medicine, University of Taubate, Taubaté, São Paulo, Brazil
- 4Divison of Nephrology, Hospital das Clínicas, Federal University of Pernambuco, Recife, Pernambuco, Brazil
- 5Recife Medical School, Federal University of Pernambuco, Recife, Pernambuco, Brazil
- 6Faculty of Medicine, CEUMA University, São Luís, Maranhão, Brazil
- 7Divison of Nephrology and Molecular Medicine, University of São Paulo, São Paulo, São Paulo, Brazil
- 8Department of Pathology and Legal Medicine, Ribeirão Preto Medical School, University of São Paulo, Ribeirão Preto, São Paulo, Brazil
With the coverage of COVID-19 vaccination, it has been possible to observe the potential side effects of SARS-CoV-2 vaccines, with the most common ones being fever, myalgia, headache, and fatigue. However, an association has been observed between new and recurrent kidney injuries, mainly glomerulonephritis and lupus nephritis associated with ANCA, with the Pfizer-BioNTech, Moderna, Sinovac, and AstraZeneca vaccines, although the relationship between them is not clear. We report a case of ANCA-related vasculitis and lupus glomerulonephritis after the second dose of the AstraZeneca vaccine. The elderly patient presented significant worsening of kidney function after immunosuppression and complications after a new onset COVID-19 infection that led to death. We provide a literature review about kidney damage related to ANCA vasculitis after COVID-19 vaccine, aiming for a better understanding of the pathophysiological mechanism of kidney injury, its presentation, and treatment.
1 Introduction
The most common side effects of the 2019 coronavirus vaccine (COVID-19) are fever, myalgia, headache, fatigue, local pain, and, rarely, anaphylactic reaction. However, case reports have demonstrated the occurrence of new and relapses cases of renal injury associated with SARS-CoV-2 immunization, including IgA nephropathy, membranous nephropathy, minimal change disease, anti-glomerular basement membrane disease, antineutrophil cytoplasmic antibody-associated vasculitis (ANCA), IgG4-related disease, lupus nephritis, scleroderma renal crisis, and thrombotic microangiopathy (1, 2). In these cases, such diseases had a temporal link with vaccination and a positive COVID-IgG response to SARS-CoV-2 (3).
Herein, we report a case from the Brazilian Consortium for the Study of COVID-19-Associated Renal Disease, which collects kidney biopsies from patients with kidney damage secondary to COVID-19 and its vaccine in 42 private and public hospitals (4, 5). This is a case report of ANCA-associated glomerulonephritis and lupus nephritis following COVID-19 vaccination, and a review of kidney manifestations related to this vaccine.
2 Case report
A 75-year-old woman presented to the emergency department with fever for 15 days, headache, adynamia, progressive dyspnea, polyarthralgia, macroscopic hematuria, foamy urine with no changes in urine volume. She had a previous diagnosis of hypothyroidism, hypertension and normal kidney function. She had been immunized against COVID-19 with the second dose AstraZeneca vaccine 15 days prior to admission. On physical examination, she was febrile (37.8 °C), normal blood pressure (130/80 mmHg), pulse rate 110 beats per minute, eupneic, and had an oxygen saturation of 98% in ambient air. The complementary physical examination was normal.
Three sequential RT-PCR tests for COVID-19 were negative, repeated every 2 days, and computed tomography (CT) of the chest showed no alterations. Laboratory tests on admission showed normocytic normochromic anemia, with hemoglobin (Hb) 10.4 g/dL and hematocrit (Ht): 30.1% and leukocytes: 10,810/mm3 with neutrophilia (9,015/mm3). Other laboratory tests were creatinine 2.9 mg/dL, sodium (Na): 128 mEq/L; potassium (K): 3.5 mEq/L, pH: 7.26, arterial partial oxygen pressure (PaO2): 81 mmHg; partial pressure of arterial carbon dioxide (PaCO2): 49 mmHg; bicarbonate: 20 mmol/L. Her urinalysis showed proteinuria, leukocyturia and hematuria, raising the hypothesis of nephritic syndrome. Her urine/protein/creatinine ratio was 2.5 mg/mg.
Although the RT-PCR test for COVID-19 was negative, the patient was admitted to the bed unit for COVID-19 cases for observation. Seven days after admission, her general condition worsened and her kidney function was compromised, with signs of hypervolemia such as peripheral edema, pulmonary congestion and dyspnea, requiring renal replacement therapy. At that time, laboratory tests showed Hb 7.5 g/dL; Ht 23.1%; platelets 104,000/mm3; D-dimer 3,250 ng/ml; ferritin 6,406 ng/ml; direct bilirubin 2.9 mg/dl; C-reactive protein 18.6 mg/dl; AST 230.6 U/L; ALT 139.4 U/L; urea: 105 mg/dl; Cr 2.7 mg/dl; procalcitonin: 0.98 ng/dl. Her c-ANCA serology was negative, with positive antinuclear antibody (ANA) (1:640) in a fine speckled pattern, as was p-ANCA (1:80). Considering the hypothesis of rapidly progressive glomerulonephritis, a kidney biopsy was performed five days after worsening (about 20 days after hospitalization). Laboratory findings at admission and seven days later are organized in Table 1.
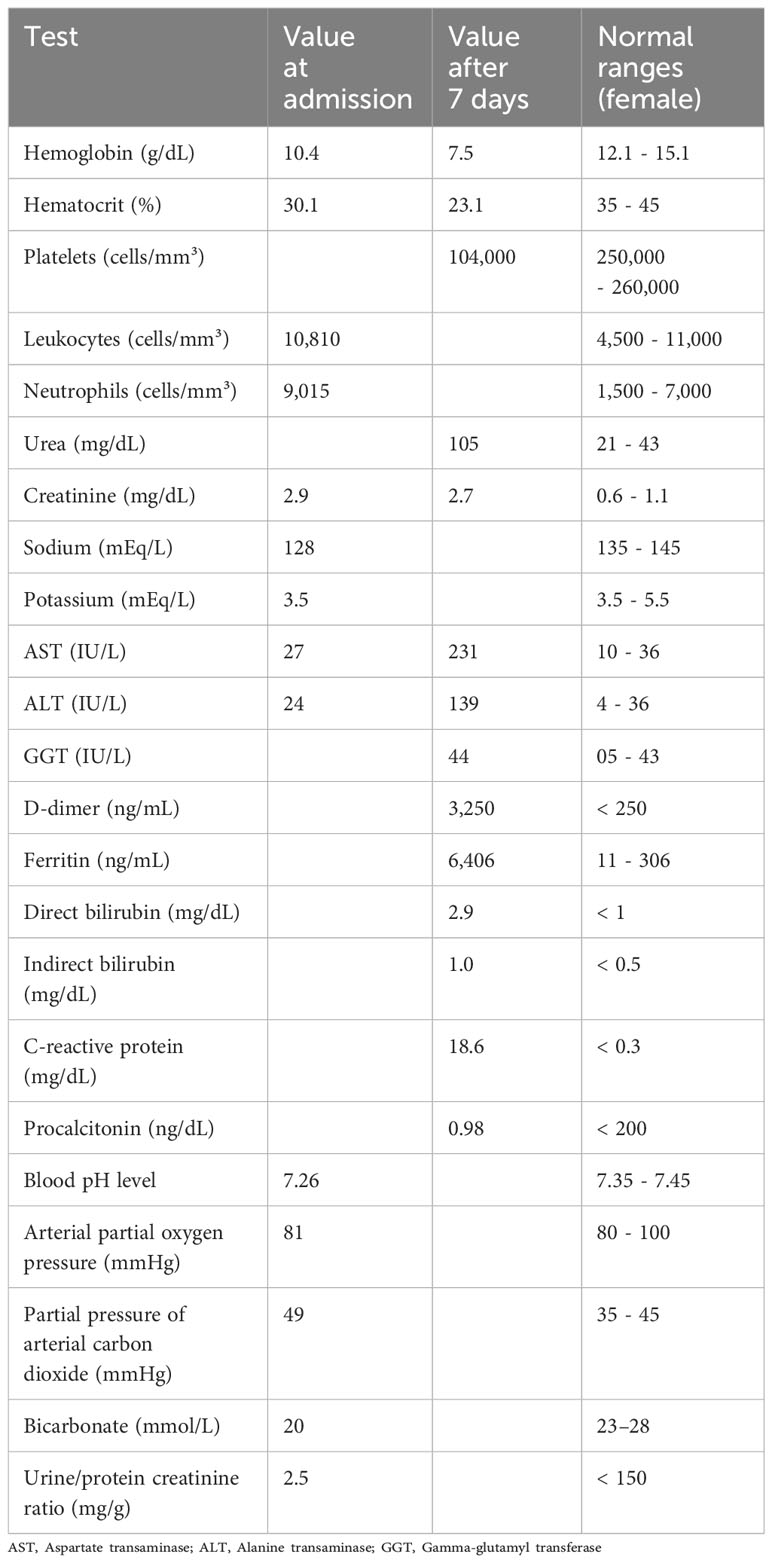
Table 1 Laboratory findings on admission and seven days after admission.
A renal biopsy revealed a proliferative and necrotizing glomerulonephritis with a full house immunofluorescence pattern, leading to the suspicion of lupus nephritis (Figure 1). There was mild interstitial fibrosis, tubular atrophy and degeneration of the tubular epithelium. The blood vessels showed no significant changes. Because of the presence of diffuse crescents and the necrotizing appearance of the lesion, the histological hypothesis of lupus glomerulonephritis associated with ANCA-related vasculitis was confirmed.
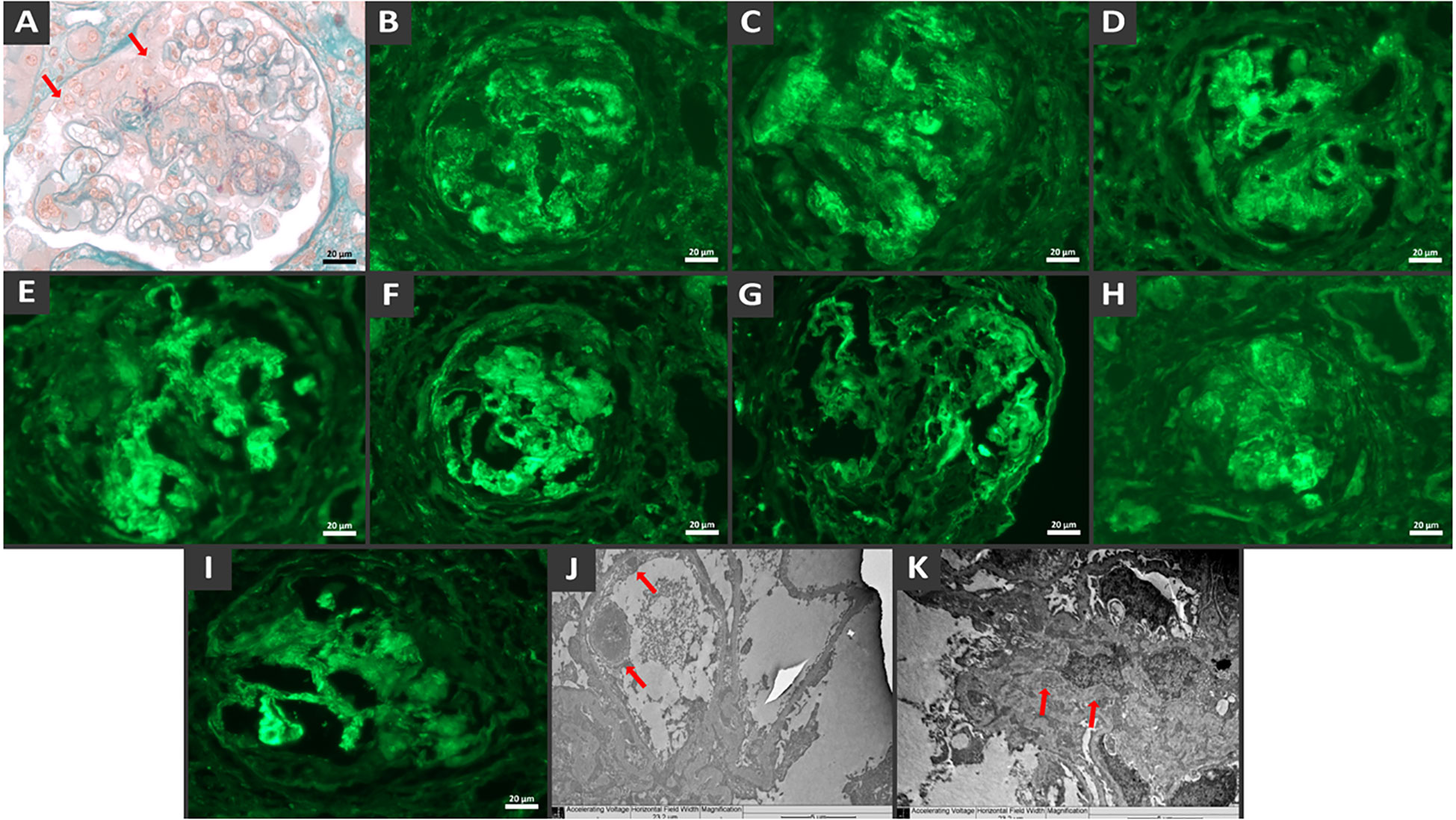
Figure 1 Histological findings show diffuse crescentic necrotizing glomerulonephritis with endocapillary proliferation and full-house immune complex deposition. Glomerulus with cellular crescent (arrow), endocapillary crescent and fibrinoid necrosis by light microscopy, Masson’s trichrome stain (A). Direct immunofluorescence demonstrates granular mesangial and capillary wall staining deposits of IgG (B), IgM (C), IgA (D), C3 (E), C1q (F), Fibrinogen (G), Kappa (H) e Lambda (I). Note the crescent surrounding the vascular tuft. Electron microscopy from paraffin embedded tissue reveals electron-dense deposits in the subendothelial (J) and mesangial (K) regions.
The patient was treated methylprednisolone 500mg for 3 days, followed by prednisone 1 mg/kg/day, and administered one dose of cyclophosphamide 1 g. After 30 days of the first symptoms, the RT-PCR test for COVID-19 was positive, possibly due to intra-hospital contamination. The imunossupression drugs were stopped. Immunoglobulin, plasmapheresis or remdesivir was not performed. Her general condition worsened rapidly, requiring intensive care due to dyspnea. Chest CT showed a extensive bilateral pleural effusion extensive with laminar consolidations, adjacent atelectasis, diffuse bilateral ground-glass opacities involving 75% of the parenchym, and signs of parapseptal and centrilobular emphysema. Unfortunately, the patient presented clinical worsening, with refractory hemodynamic instability, respiratory acidosis, and hypoxia, and evolved to death. The timeline of the patient’s evolution is shown in Figure 2.
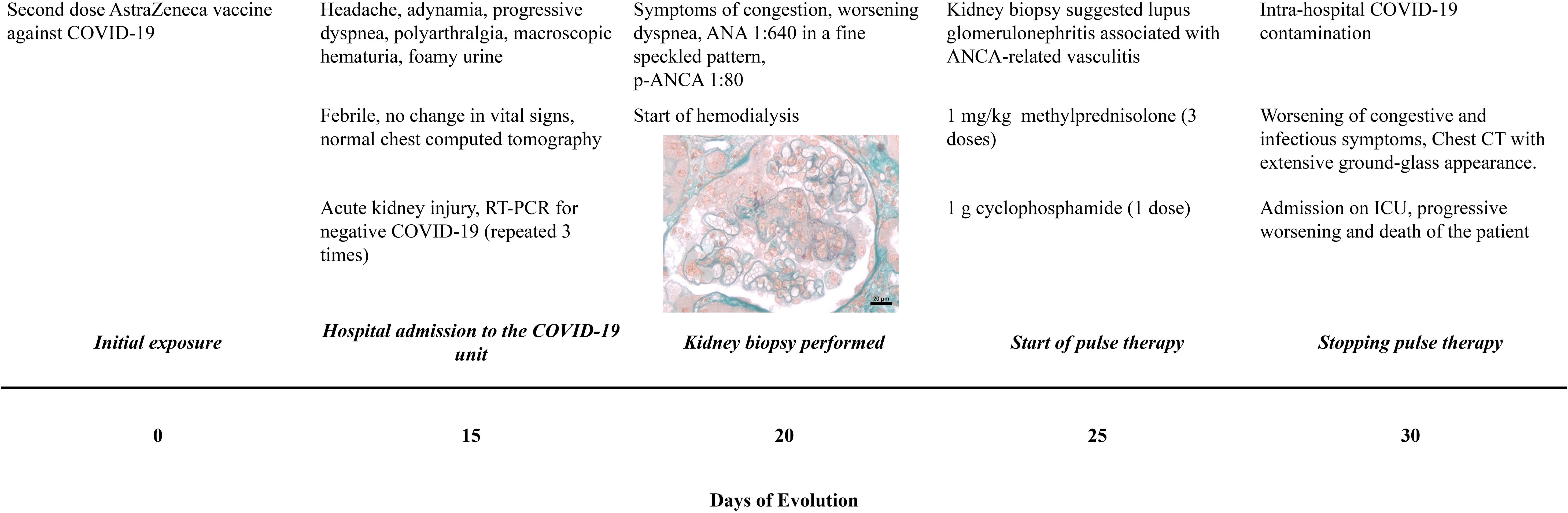
Figure 2 Timeline of clinical evolution. The time and initial symptoms are specified from COVID-19 vaccination, investigation, treatment and patient outcome.
3 Discussion
The remarkable increase in the coverage of immunization against COVID-19 worldwide allows us to learn about the possible adverse effects of the vaccine, including those involving the renal system. Some vaccines have been previously linked to kidney injury. The influenza vaccine has been associated with nephrotic syndrome secondary to minimal change disease (6, 7), membranous nephropathy (8), vasculitis with pauci-immune glomerulonephritis (9), microscopic polyangiitis (10), ANCA-associated glomerulonephritis (9), rhabdomyolysis with acute kidney injury (11), vasculitis (12) and Henoch-Schonlein purpura (13, 14). The hepatitis B vaccine has been associated with nephrotic syndrome secondary to minimal change disease (15) and lupus nephritis (16). The pneumococcal vaccine was associated with glomerulonephritis (related to anti-glomerular basement membrane antibody) (17), the polio-diphtheria-tetanus vaccine with nephrotic syndrome (secondary to minimal change disease) (18), the varicella vaccine with nephrotic syndrome (19), and the measles vaccine with minimal change disease (20). The rabies vaccine was associated with possible relapse of nephrotic syndrome (21). The Bacillus Calmette-Guerin (BCG) vaccine used as intravesical immunotherapy to treat bladder cancer and not for immunization was associated with membranous nephropathy, interstitial nephritis, and formation of asymptomatic renal granulomas (22).
Several COVID-19 vaccines and their different mechanisms of action have been reported to have some renal injury side effects (4) (Table 2). Lipid-based nanoparticle-mRNA vaccines cause a stimulatory response to CD4+ and CD8+ T lymphocytes and an increased production of B lymphocytes in germinal centers, resulting in the secretion of interferons (mainly gamma) and interleukin-2. DNA-adenovirus vaccines stimulate CD4+ and CD8+ cytotoxic T lymphocytes, in addition to increasing antibody production by B lymphocytes, mainly IgG1-IgG3 and to a lesser extent IGg2-IgG4 (2). Both vaccine classes have the same antigenic target, the viral spike protein, and have been associated with glomerular injury.
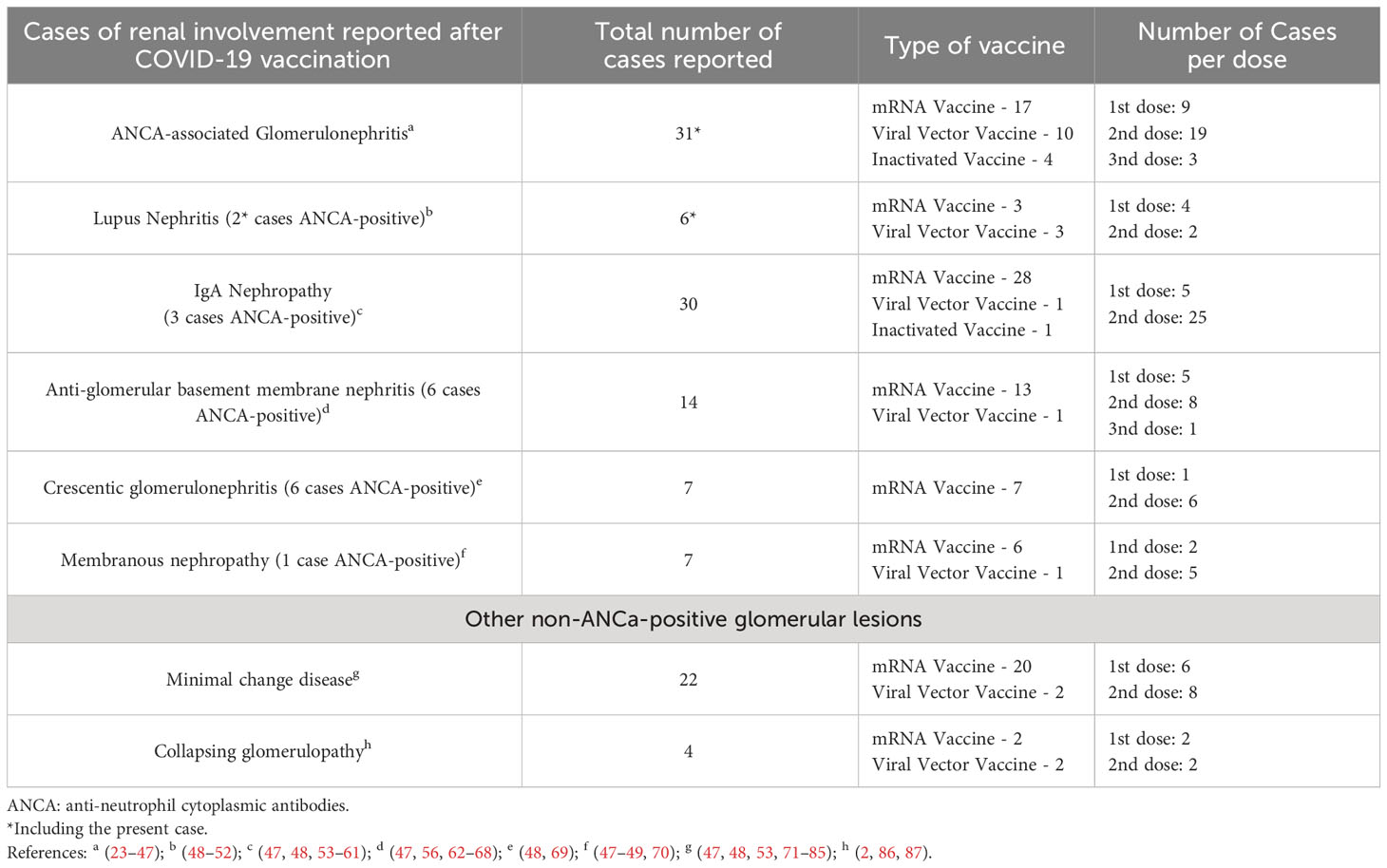
Table 2 New onset and relapses cases of ANCA-associated glomerulonephritis and other glomerular lesions with ANCA-positive association reported after COVID-19 vaccination.
The pathophysiological mechanism of post-vaccine glomerulonephritis remains unknown. However, the likely cause is mimicry of the remade viral proteins with the host’s proteins, thereby causing a type of “second wave infection” and subsequent renal damage (1). Infection by SARS-CoV-2 has been recognized as a trigger for the onset of several diseases and autoimmune reactions (48). The viral RNA is recognized by host receptors, binding to them and stimulating the production of type I interferon and inflammatory cytokines. In turn, type I interferon stimulates antibodies production, which are strictly associated with autoimmune diseases (1, 2).
The SARS-CoV-2 vaccine seems to be related to some cases of ANCA-associated glomerulonephritis and lupus nephritis, majority related after Pfizer-BioNTech, Moderna, Sinovac and AstraZeneca (23). The relationship between the vaccine and autoimmune diseases is still unclear. The mRNA vaccines can induce, for example, double-positive anti–glomerular basement membrane antibody and myeloperoxidase ANCA (62), subsequently nephritis and vasculitis. Proinflammatory status mediated by the vaccine containing lipid-based nanoparticles can lead to a subsequent loss of tolerance to self-antigens due to autoreactivity and immune system hyperactivation (88). It is suggested that the vaccines’ antigenic target, the viral spicule protein, stimulates antibody production.
The overlap of ANCA-associated glomerulonephritis and lupus nephritis is not uncommon (89). Although these diseases are easy to differentiate from each other by autoantibody profile and histopathological findings, some patients have shown an overlap of such findings (90). Crescentic glomerulonephritis is not rare in lupus nephritis, and the presence of ANCA antibodies is also well established in the literature (90, 91). ANCA antibodies are present more markedly in crescentic lupus nephritis than in lupus nephritis without crescents; such a finding favors the role of ANCA antibodies in renal crescent formation. Similarly, although associated p-ANCA glomerulonephritis is defined as pauci-immune on immunofluorescence, the presence of immune-complexes described in the present case is explained by the full house pattern of overlapping lupus nephritis (90, 91).
We present Supplementary Material with a detailed review of the literature on ANCA-related glomerulonephritis and other renal lesions in which ANCA positivity occurred after COVID-19 vaccination. The main conditions were ANCA glomerulonephritis (14%), IgA nephropathy (12.3%), anti-glomerular basement membrane glomerulonephritis (10.5%), crescentic glomerulonephritis (10.5%). In this review, 55.17% were women, 81.03% were vaccinated with the mRNA vaccine. The symptoms were nonspecific and started on average 18 days after the vaccine. Most patients used high doses of glucocorticoids and some type of immunosuppressant, and 18.96% required hemodialysis. In general, clinically significant chronic kidney disease may persist in more than 75% of ANCA-associated vasculitis in those with kidney impairment (24). The proportion of normal glomeruli appears to be associated with dialysis discontinuation, although some treatments such as plasmapheresis did not show significance with dialysis discontinuation (25).
4 Conclusion
The study of adverse effects, including renal involvement, of the COVID-19 vaccine, gives us the opportunity for early diagnosis and provision of assistance to patients with complications after autoimmune activation by the vaccine or direct contact with the SARS-CoV-2 virus.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The requirement of ethical approval was waived by Comitê de Ética e Pesquisa do HUUFMA for the studies involving humans because Comitê de Ética e Pesquisa do HUUFMA. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
MC: Conceptualization, Writing – original draft. TV: Data curation, Investigation, Writing – original draft. LM: Data curation, Investigation, Writing – original draft. LF: Data curation, Investigation, Writing – original draft. RM: Data curation, Investigation, Writing – original draft. DC: Writing – review & editing. NS: Resources, Writing – review & editing. RN: Conceptualization, Investigation, Writing – original draft. PN: Writing – review & editing. GS: Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
National Council for Scientific and Technological Development (CNPq in the Portuguese acronym) and the Foundation for the Support of Research and Scientific and Technological Development of Maranhão (FAPEMA in the Portuguese acronym).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1298622/full#supplementary-material
References
1. Hassanzadeh S, Djamali A, Mostafavi L, Pezeshgi A. Kidney complications following COVID-19 vaccination; a review of the literature. J Nephropharmacol (2021) 11:e1–1. doi: 10.34172/npj.2022.01
2. Li NL, Coates PT, Rovin BH. COVID-19 vaccination followed by activation of glomerular diseases: does association equal causation? Kidney Int (2021) 100:959–65. doi: 10.1016/j.kint.2021.09.002
3. Carr EJ, Kronbichler A, Graham-Brown M, Abra G, Argyropoulos C, Harper L, et al. Review of early immune response to SARS-CoV-2 vaccination among patients with CKD. Kidney Int Rep (2021) 6:2292–304. doi: 10.1016/j.ekir.2021.06.027
4. Pacheco ICR, Costa DM do N, Sousa DS, Salgado Filho N, Silva GEB, Neves PDM de M. Kidney injury associated with COVID-19 infection and vaccine: A narrative review. Front Med (2022) 9:956158. doi: 10.3389/fmed.2022.956158
5. Teixeira Júnior AAL, Neves PDM de M, Lages JS, Cunha K de A, Muniz MPR, Brito DJ de A, et al. Brazilian consortium for the study on renal diseases associated with COVID-19: A multicentric effort to understand SARS-CoV-2-related nephropathy. Front Med (2020) 7:584235. doi: 10.3389/fmed.2020.584235
6. Patel C, Shah HH. Vaccine-associated kidney diseases: A narrative review of the literature. Saudi J Kidney Dis Transplant (2019) 30:1002–9. doi: 10.4103/1319-2442.270254
7. Kielstein JT, Termühlen L, Sohn J, Kliem V. Minimal change nephrotic syndrome in a 65-year-old patient following influenza vaccination. Clin Nephrol (2000) 54:246–8.
8. Kutlucan A, Gonen I, Yildizhan E, Aydin Y, Sav T, Yildirim U. Can influenza H1N1 vaccination lead to the membranous glomerulonephritis? Indian J Pathol Microbiol (2012) 55:239–41. doi: 10.4103/0377-4929.97893
9. Orbach H, Agmon-Levin N, Zandman-Goddard G. Vaccines and autoimmune diseases of the adult. Discovery Med (2010) 9:90–7.
10. Uji M, Matsushita H, Iwata S. Microscopic polyangiitis after influenza vaccination. Intern Med Tokyo Jpn (2005) 44:892–6. doi: 10.2169/internalmedicine.44.892
11. Plotkin E, Bernheim J, Ben-Chetrit S, Mor A, Korzets Z. Influenza vaccine–a possible trigger of rhabdomyolysis induced acute renal failure due to the combined use of cerivastatin and bezafibrate. Nephrol Dial Transplant (2000) 15:740–1. doi: 10.1093/ndt/15.5.740
12. Hyla-Klekot L, Kucharska G, Cieslak W. [Necrotizing glomerulonephritis in decursu vasculitis after vaccination against influenza]. Pol Merkur Lek Organ Pol Tow Lek (2005) 19:75–7.
13. Liu J-Y, Wu Q, Liu M, Wang L, Gao Y, Li S. HENOCH-SCHÖNLEIN PURPURA NEPHRITIS FOLLOWING INFLUENZA VACCINATION: A CASE REPORT AND REVIEW OF THE LITERATURE. Southeast Asian J Trop Med Public Health (2016) 47:945–50.
14. Damjanov J, Amato JA. Progression of renal disease in Henoch-Schönlein purpura after influenza vaccination. JAMA (1979) 242:2555–6. doi: 10.1001/jama.242.23.2555
15. Macário F, Freitas L, Correia J, Campos M, Marques A. Nephrotic syndrome after recombinant hepatitis B vaccine. Clin Nephrol (1995) 43:349.
16. Santoro D, Stella M, Montalto G, Castellino S. Lupus nephritis after hepatitis B vaccination: an uncommon complication. Clin Nephrol (2007) 67:61–3. doi: 10.5414/cnp67061
17. Tan SY, Cumming AD. Vaccine related glomerulonephritis. BMJ (1993) 306:248. doi: 10.1136/bmj.306.6872.248-b
18. Clajus C, Spiegel J, Bröcker V, Chatzikyrkou C, Kielstein JT. Minimal change nephrotic syndrome in an 82 year old patient following a tetanus-diphteria-poliomyelitis-vaccination. BMC Nephrol (2009) 10:21. doi: 10.1186/1471-2369-10-21
19. Angeletti A, Lugani F, La Porta E, Verrina E, Caridi G, Ghiggeri GM. Vaccines and nephrotic syndrome: efficacy and safety. Pediatr Nephrol Berl Ger (2022) 38(9):2915–28. doi: 10.1007/s00467-022-05835-4
20. Kuzemko JA. Measles vaccination and the nephrotic syndrome. Br Med J (1972) 4:665–6. doi: 10.1136/bmj.4.5841.665-a
21. Singhal PC, Gupta VK, Nampoory MR, Lazar AI, Chugh KS. Case report: glomerulonephritis after immunization with antirabies vaccine. Ann Allergy (1981) 46:98–9.
22. Mohammed A, Arastu Z. Emerging concepts and spectrum of renal injury following Intravesical BCG for non-muscle invasive bladder cancer. BMC Urol (2017) 17:114. doi: 10.1186/s12894-017-0304-5
23. Thammathiwat T, Banjongjit A, Iampenkhae K, Townamchai N, Kanjanabuch T. ANCA associated glomerulonephritis following SARS-CoV-2 vaccination: A case series and systematic review. Vaccines (2023) 11:983. doi: 10.3390/vaccines11050983
24. Hanberg JS, Cook C, Fu X, Choi HK, Zhang Y, Wallace ZS. Longitudinal patterns of renal function in antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Care Res (2023) 75:2190–8. doi: 10.1002/acr.25100
25. Lee Y-J, Ahn S-M, Oh J-S, Kim Y-G, Lee C-K, Yoo B, et al. Recovery and long-term renal outcome of patients with anti-neutrophil cytoplasmic antibody-associated vasculitis who are on dialysis at presentation. J Rheum Dis (2023) 30:251–9. doi: 10.4078/jrd.2023.0031
26. Anderegg MA, Liu M, Saganas C, Montani M, Vogt B, Huynh-Do U, et al. De novo vasculitis after mRNA-1273 (Moderna) vaccination. Kidney Int (2021) 100:474–6. doi: 10.1016/j.kint.2021.05.016
27. Sekar A, Campbell R, Tabbara J, Rastogi P. ANCA glomerulonephritis after the Moderna COVID-19 vaccination. Kidney Int (2021) 100:473–4. doi: 10.1016/j.kint.2021.05.017
28. Dube GK, Benvenuto LJ, Batal I. Antineutrophil cytoplasmic autoantibody-associated glomerulonephritis following the Pfizer-BioNTech COVID-19 vaccine. Kidney Int Rep (2021) 6:3087–9. doi: 10.1016/j.ekir.2021.08.012
29. Chen C-C, Chen H-Y, Lu C-C, Lin S-H. Case report: anti-neutrophil cytoplasmic antibody-associated vasculitis with acute renal failure and pulmonary hemorrhage may occur after COVID-19 vaccination. Front Med (2021) 8:765447. doi: 10.3389/fmed.2021.765447
30. Davidovic T, Schimpf J, Sprenger-Mähr H, Abbassi-Nik A, Soleiman A, Zitt E, et al. De Novo and Relapsing Glomerulonephritis following SARS-CoV-2 mRNA Vaccination in Microscopic Polyangiitis. Case Rep Nephrol (2021) 2021:8400842. doi: 10.1155/2021/8400842
31. Feghali EJ, Zafar M, Abid S, Santoriello D, Mehta S. De-novo antineutrophil cytoplasmic antibody-associated vasculitis following the mRNA-1273 (Moderna) vaccine for COVID-19. Cureus (2021) 13:e19616. doi: 10.7759/cureus.19616
32. Hakroush S, Tampe B. Case report: ANCA-associated vasculitis presenting with rhabdomyolysis and pauci-immune crescentic glomerulonephritis after Pfizer-BioNTech COVID-19 mRNA vaccination. Front Immunol (2021) 12:762006. doi: 10.3389/fimmu.2021.762006
33. Schaubschlager T, Rajora N, Diep S, Kirtek T, Cai Q, Hendricks AR, et al. De novo or recurrent glomerulonephritis and acute tubulointerstitial nephritis after COVID-19 vaccination: A report of six cases from a single center. Clin Nephrol (2022) 97:289–97. doi: 10.5414/CN110794
34. Shakoor MT, Birkenbach MP, Lynch M. ANCA-associated vasculitis following Pfizer-BioNTech COVID-19 vaccine. Am J Kidney Dis (2021) 78:611–3. doi: 10.1053/j.ajkd.2021.06.016
35. Villa M, Díaz-Crespo F, Pérez de José A, Verdalles Ú, Verde E, Almeida Ruiz F, et al. A case of ANCA-associated vasculitis after AZD1222 (Oxford-AstraZeneca) SARS-CoV-2 vaccination: casualty or causality? Kidney Int (2021) 100:937–8. doi: 10.1016/j.kint.2021.07.026
36. David R, Hanna P, Lee K, Ritchie A. Relapsed ANCA associated vasculitis following Oxford AstraZeneca ChAdOx1-S COVID-19 vaccination: A case series of two patients. Nephrol Carlton Vic (2022) 27:109–10. doi: 10.1111/nep.13993
37. Garcia DS, Martins C, da Fonseca EO, de Carvalho VCP, de Rezende RPV. Clinical Images: Severe proteinase 3 antineutrophil cytoplasmic antibody glomerulonephritis temporally associated with Sinovac Biotech’s inactivated SARS-CoV-2 vaccine. ACR Open Rheumatol (2022) 4:277–8. doi: 10.1002/acr2.11397
38. El Hasbani G, Uthman I. ANCA-associated vasculitis following the first dose of Pfizer-BioNTech COVID-19 vaccine. Nephron (2023) 147:103–7. doi: 10.1159/000525562
39. Kim BC, Kim HS, Han KH, Han SY, Jo HA. A case report of MPO-ANCA-associated vasculitis following heterologous mRNA1273 COVID-19 booster vaccination. J Korean Med Sci (2022) 37:e204. doi: 10.3346/jkms.2022.37.e204
40. Noel E, Rashid U, Rabbani R, Khan WA, Benjamin YS, Lee I. Antineutrophil cytoplasmic autoantibody-associated glomerulonephritis as a possible side effect of COVID-19 vaccination. Cureus (2022) 14:e30565. doi: 10.7759/cureus.30565
41. Obata S, Hidaka S, Yamano M, Yanai M, Ishioka K, Kobayashi S. MPO-ANCA-associated vasculitis after the Pfizer/BioNTech SARS-CoV-2 vaccination. Clin Kidney J (2021) 15:357–9. doi: 10.1093/ckj/sfab181
42. Prabhahar A, Naidu GSRSNK, Chauhan P, Sekar A, Sharma A, Sharma A, et al. ANCA-associated vasculitis following ChAdOx1 nCoV19 vaccination: case-based review. Rheumatol Int (2022) 42:749–58. doi: 10.1007/s00296-021-05069-x
43. Ramezanzade E, Ghanbari R, Yazdanipour T. Antineutrophil cytoplasmic antibody (ANCA)-associated glomerulonephritis in a 15-year-old patient after receiving the second dose of the BBIBP-CorV (Sinopharm) COVID-19 vaccine: A case report. Nephro-Urol Mon (2022) 14:e127124. doi: 10.5812/numonthly-127124
44. So D, Min K-W, Jung WY, Han S-W, Yu M-Y. Microscopic polyangiitis following mRNA COVID-19 vaccination: A case report. J Korean Med Sci (2022) 37:e154. doi: 10.3346/jkms.2022.37.e154
45. Suzuki M, Sekiguchi Y, Sasaki M, Inaba S, Oyama S, Inoue Y, et al. Antineutrophil cytoplasmic antibody-associated vasculitis after COVID-19 vaccination with Pfizer-BioNTech. Intern Med Tokyo Jpn (2022) 61:2925–9. doi: 10.2169/internalmedicine.9807-22
46. Yadav R, Shah S, Chhetri S. ANCA-associated vasculitis following Johnson and Johnson COVID-19 vaccine. Ann Med Surg (2022) 79:104123. doi: 10.1016/j.amsu.2022.104123
47. Zamoner W, Scardini JB, De Dio BJ, Marques A de M, Silva VDS, Garcia AL, et al. ANCA-associated vasculitis following Oxford-AstraZeneca COVID-19 vaccine in Brazil: Is there a causal relationship? A case report. Front Med (2022) 9:1003332. doi: 10.3389/fmed.2022.1003332
48. Caza TN, Cassol CA, Messias N, Hannoudi A, Haun RS, Walker PD, et al. Glomerular disease in temporal association with SARS-CoV-2 vaccination: A series of 29 cases. Kidney360 (2021) 2:1770–80. doi: 10.34067/KID.0005372021
49. Bansal SB, Rana AS, Manhas N, Rana A. Post COVID vaccination (COVAXINTM -BB152 V) pauci-immune crescentic glomerulonephritis. Indian J Nephrol (2022) 32:495–7. doi: 10.4103/ijn.ijn_352_21
50. Klomjit N, Alexander MP, Fervenza FC, Zoghby Z, Garg A, Hogan MC, et al. COVID-19 vaccination and glomerulonephritis. Kidney Int Rep (2021) 6:2969–78. doi: 10.1016/j.ekir.2021.09.008
51. Tuschen K, Bräsen JH, Schmitz J, Vischedyk M, Weidemann A. Relapse of class V lupus nephritis after vaccination with COVID-19 mRNA vaccine. Kidney Int (2021) 100:941–4. doi: 10.1016/j.kint.2021.07.019
52. Sekar A. Lupus nephritis flare post Moderna mRNA-1273 coronavirus vaccine. QJM Mon J Assoc Physicians (2022) 114:882–3. doi: 10.1093/qjmed/hcab284
53. Zavala-Miranda MF, González-Ibarra SG, Pérez-Arias AA, Uribe-Uribe NO, Mejia-Vilet JM. New-onset systemic lupus erythematosus beginning as class V lupus nephritis after COVID-19 vaccination. Kidney Int (2021) 100:1340–1. doi: 10.1016/j.kint.2021.09.009
54. Kim HJ, Jung M, Lim BJ, Han SH. New-onset class III lupus nephritis with multi-organ involvement after COVID-19 vaccination. Kidney Int (2022) 101:826–8. doi: 10.1016/j.kint.2022.01.013
55. Baskaran K, Cohen AWS, Weerasinghe N, Vilayur E. Report of two cases of minimal change disease following vaccination for COVID -19. Nephrol Carlton Vic (2022) 27:111–2. doi: 10.1111/nep.13995
56. Fernández P, Alaye ML, Chiple MEG, Arteaga JD, Douthat W, Fuente JDL, et al. Glomerulopathies after vaccination against COVID-19. Four cases with three different vaccines in Argentina. Nefrol Publicacion Of Soc Espanola Nefrol (2021) 43(5):655–7. doi: 10.1016/j.nefro.2021.09.003
57. Hanna C, Herrera Hernandez LP, Bu L, Kizilbash S, Najera L, Rheault MN, et al. IgA nephropathy presenting as macroscopic hematuria in 2 pediatric patients after receiving the Pfizer COVID-19 vaccine. Kidney Int (2021) 100:705–6. doi: 10.1016/j.kint.2021.06.032
58. Izzedine H, Bonilla M, Jhaveri KD. Nephrotic syndrome and vasculitis following SARS-CoV-2 vaccine: true association or circumstantial? Nephrol Dial Transplant (2021) 36:1565–9. doi: 10.1093/ndt/gfab215
59. Kudose S, Friedmann P, Albajrami O, D’Agati VD. Histologic correlates of gross hematuria following Moderna COVID-19 vaccine in patients with IgA nephropathy. Kidney Int (2021) 100:468–9. doi: 10.1016/j.kint.2021.06.011
60. Lo WK, Chan KW. Gross haematuria after mRNA COVID-19 vaccination in two patients with histological and clinical diagnosis of IgA nephropathy. Nephrol Carlton Vic (2022) 27:110–1. doi: 10.1111/nep.13992
61. Nakatani S, Mori K, Morioka F, Hirata C, Tsuda A, Uedono H, et al. New-onset kidney biopsy-proven IgA vasculitis after receiving mRNA-1273 COVID-19 vaccine: case report. CEN Case Rep (2022) 11:358–62. doi: 10.1007/s13730-021-00677-9
62. Ting JA, Barbir E-B, McRae SA, Schachter M, De Luca L, Riazy M, et al. Double-Positive Anti–Glomerular Basement Membrane Antibody and Myeloperoxidase Antineutrophil Cytoplasmic Autoantibody–Associated Glomerulonephritis Post COVID-19 mRNA vaccine: A Case Series of 4 Patients. Can J Kidney Health Dis (2023) 10:20543581231153217. doi: 10.1177/20543581231153217
63. Sugita K, Kaneko S, Hisada R, Harano M, Anno E, Hagiwara S, et al. Development of IgA vasculitis with severe glomerulonephritis after COVID-19 vaccination: a case report and literature review. CEN Case Rep (2022) 11:436–41. doi: 10.1007/s13730-022-00695-1
64. Tan HZ, Tan RY, Choo JCJ, Lim CC, Tan CS, Loh AHL, et al. Is COVID-19 vaccination unmasking glomerulonephritis? Kidney Int (2021) 100:469–71. doi: 10.1016/j.kint.2021.05.009
65. Coorey CP, Phua E, Chou A, Shen Y, Mather A. Anti-GBM Disease after Oxford-AstraZeneca ChAdOx1 nCoV-19 Vaccination: A Report of Two Cases. Case Rep Nephrol Dial (2022) 12:234–7. doi: 10.1159/000525737
66. Terakawa K, Niikura T, Katagiri D, Sugita A, Kikuchi T, Hayashi A, et al. A case of rapidly progressive glomerulonephritis with double-positive anti-GBM antibody and MPO-ANCA after SARS-CoV-2 vaccination and relapse during 1 year follow-up. CEN Case Rep (2023) 27:1–7. doi: 10.1007/s13730-023-00792-9
67. Sacker A, Kung V, Andeen N. Anti-GBM nephritis with mesangial IgA deposits after SARS-CoV-2 mRNA vaccination. Kidney Int (2021) 100:471–2. doi: 10.1016/j.kint.2021.06.006
68. Gupta RK, Ellis BK. Concurrent antiglomerular basement membrane nephritis and antineutrophil cytoplasmic autoantibody-mediated glomerulonephritis after second dose of SARS-CoV-2 mRNA vaccination. Kidney Int Rep (2022) 7:127–8. doi: 10.1016/j.ekir.2021.10.020
69. Hoi S, Ogawa M, Munemura C, Takata T, Isomoto H. Atypical anti-glomerular basement membrane nephritis after the first dose of the severe acute respiratory syndrome coronavirus 2 mRNA vaccine. Yonago Acta Med (2023) 66:300–5. doi: 10.33160/yam.2023.05.008
70. Aydın MF, Yıldız A, Oruç A, Sezen M, Dilek K, Güllülü M, et al. Relapse of primary membranous nephropathy after inactivated SARS-CoV-2 virus vaccination. Kidney Int (2021) 100:464–5. doi: 10.1016/j.kint.2021.05.001
71. Nagai K, Iwase M, Ueda A. A case of anti-GBM nephritis following centipede bites and COVID-19 vaccination. CEN Case Rep (2022) 11:166–70. doi: 10.1007/s13730-021-00646-2
72. Kim S, Jung J, Cho H, Lee J, Go H, Lee JH. A child with crescentic glomerulonephritis following SARS-CoV-2 mRNA (Pfizer-BioNTech) vaccination. Pediatr Nephrol Berl Ger (2023) 38:299–302. doi: 10.1007/s00467-022-05681-4
73. Lebedev L, Sapojnikov M, Wechsler A, Varadi-Levi R, Zamir D, Tobar A, et al. Minimal change disease following the Pfizer-BioNTech COVID-19 vaccine. Am J Kidney Dis (2021) 78:142–5. doi: 10.1053/j.ajkd.2021.03.010
74. Talotta R. Do COVID-19 RNA-based vaccines put at risk of immune-mediated diseases? In reply to “potential antigenic cross-reactivity between SARS-CoV-2 and human tissue with a possible link to an increase in autoimmune diseases”. Clin Immunol Orlando Fla (2021) 224:108665. doi: 10.1016/j.clim.2021.108665
75. Al-Rasbi S, Al-Maqbali JS, Al-Farsi R, Al Shukaili MA, Al-Riyami MH, Al Falahi Z, et al. Myocarditis, pulmonary hemorrhage, and extensive myositis with rhabdomyolysis 12 days after first dose of Pfizer-BioNTech BNT162b2 mRNA COVID-19 vaccine: A case report. Am J Case Rep (2022) 23:e934399. doi: 10.12659/AJCR.934399
76. Gambella A, Barreca A, Biancone L, Roccatello D, Peruzzi L, Besso L, et al. Spectrum of kidney injury following COVID-19 disease: renal biopsy findings in a single Italian pathology service. Biomolecules (2022) 12:298. doi: 10.3390/biom12020298
77. Psyllaki A, Stavrakaki I, Androvitsanea A, Gakiopoulou H, Petrakis I, Stylianou K. Two cases of glomerular involvement after vaccination against COVID-19: epiphenomenon or causality? Clin Kidney J (2022) 15:574–5. doi: 10.1093/ckj/sfab252
78. Park HJ, An WS, Rha SH, Kim SE, Lee SM. Minimal change glomerulonephritis following the second dose of the Moderna COVID-19 vaccine. QJM Mon J Assoc Physicians (2022) 115:490–1. doi: 10.1093/qjmed/hcac094
79. Annicchiarico Petruzzelli L, Minale B, Serio V, De Luca A, Marino Marsilia G, Campione S, et al. Pediatric Minimal Change Disease and AKI following the Pfizer-BioNTech COVID-19 Vaccine: causal or incidental correlation? G Ital Nefrol Organo Uff Della Soc Ital Nefrol (2022) 39:2022–vol6.
80. D’Agati VD, Kudose S, Bomback AS, Adamidis A, Tartini A. Minimal change disease and acute kidney injury following the Pfizer-BioNTech COVID-19 vaccine. Kidney Int (2021) 100:461–3. doi: 10.1016/j.kint.2021.04.035
81. Maas RJ, Gianotten S, van der Meijden WAG. An additional case of minimal change disease following the Pfizer-BioNTech COVID-19 vaccine. Am J Kidney Dis Off J Natl Kidney Found (2021) 78:312. doi: 10.1053/j.ajkd.2021.05.003
82. Weijers J, Alvarez C, Hermans MMH. Post-vaccinal minimal change disease. Kidney Int (2021) 100:459–61. doi: 10.1016/j.kint.2021.06.004
83. Kervella D, Jacquemont L, Chapelet-Debout A, Deltombe C, Ville S. Minimal change disease relapse following SARS-CoV-2 mRNA vaccine. Kidney Int (2021) 100:457–8. doi: 10.1016/j.kint.2021.04.033
84. Komaba H, Wada T, Fukagawa M. Relapse of minimal change disease following the Pfizer-BioNTech COVID-19 vaccine. Am J Kidney Dis (2021) 78:469–70. doi: 10.1053/j.ajkd.2021.05.006
85. Morlidge C, El-Kateb S, Jeevaratnam P, Thompson B. Relapse of minimal change disease following the AstraZeneca COVID-19 vaccine. Kidney Int (2021) 100:459. doi: 10.1016/j.kint.2021.06.005
86. Holzworth A, Couchot P, Cruz-Knight W, Brucculeri M. Minimal change disease following the Moderna mRNA-1273 SARS-CoV-2 vaccine. Kidney Int (2021) 100:463–4. doi: 10.1016/j.kint.2021.05.007
87. Neves PD, Caires RA, Guimarães MP, Costalonga EC, Cavalcante LB, Costa E Silva VT, et al. Collapsing glomerulopathy following SARS-CoV-2 adenovirus-vector-based vaccine: report of 2 cases. Kidney Int (2022) 101:637–9. doi: 10.1016/j.kint.2021.12.016
88. Ndeupen S, Qin Z, Jacobsen S, Bouteau A, Estanbouli H, Igyártó BZ. The mRNA-LNP platform’s lipid nanoparticle component used in preclinical vaccine studies is highly inflammatory. iScience (2021) 24:103479. doi: 10.1016/j.isci.2021.103479
89. Turner-Stokes T, Wilson HR, Morreale M, Nunes A, Cairns T, Cook HT, et al. Positive antineutrophil cytoplasmic antibody serology in patients with lupus nephritis is associated with distinct histopathologic features on renal biopsy. Kidney Int (2017) 92:1223–31. doi: 10.1016/j.kint.2017.04.029
90. Nasr SH, D’Agati VD, Park H-R, Sterman PL, Goyzueta JD, Dressler RM, et al. Necrotizing and crescentic lupus nephritis with antineutrophil cytoplasmic antibody seropositivity. Clin J Am Soc Nephrol CJASN (2008) 3:682–90. doi: 10.2215/CJN.04391007
Keywords: ANCA, glomerulonephritis, lupus nephritis, COVID-19, vaccine
Citation: Campos MAG, Valois TO, Magalhães LE, Vasques LF, de Medeiros RG, Costa DMN, Salgado Filho N, Nogueira RMR, Neves PDMM and Silva GEB (2024) ANCA-associated glomerulonephritis and lupus nephritis following COVID-19 vaccination: a case report and literature review. Front. Immunol. 14:1298622. doi: 10.3389/fimmu.2023.1298622
Received: 22 September 2023; Accepted: 13 December 2023;
Published: 08 January 2024.
Edited by:
Elmostafa Bahraoui, INSERM U1043 Centre de Physiopathologie de Toulouse Purpan, FranceReviewed by:
Emanuele Bizzi, ASST Fatebenefratelli Sacco, ItalyTsuneaki Kenzaka, Kobe University, Japan
Copyright © 2024 Campos, Valois, Magalhães, Vasques, de Medeiros, Costa, Salgado Filho, Nogueira, Neves and Silva. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gyl Eanes Barros Silva, Z3lsZWFuZXNAYWx1bW5pLnVzcC5icg==