 Mário Sousa-Pimenta1,2,3*
Mário Sousa-Pimenta1,2,3* Pedro Berraondo
Pedro Berraondo
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Immunol. , 23 November 2023
Sec. Cancer Immunity and Immunotherapy
Volume 14 - 2023 | https://doi.org/10.3389/fimmu.2023.1295293
Introduction and aims: Richter syndrome (RS) represents the clonal evolution of chronic lymphocytic leukemia with histological transformation into a high-grade B cell lymphoma (diffuse large B cell lymphoma - DLBCL) or Hodgkin lymphoma. Considering that RS is an uncommon condition with poor prognosis, few high-quality evidence is available. To overcome this unmet need, this meta-analysis aimed to pool efficacy of early clinical trials in Richter syndrome (DLBCL subtype).
Methods: MEDLINE, Scopus and Web of Science were searched up to May of 2023 to identify clinical trials decoying efficacy. The pooled complete response, objective response and intension-to-treat failure rates were calculated by pharmacological categories (classical chemotherapy, immunochemotherapy, immunotherapy, Bruton-tyrosine kinase inhibitors, targeted approaches, cell-based therapies and combinatorial regimens) using the Der-Simonian and Laird random-effects model. The Freeman-Tukey double arcsine method was used to estimate variance and confidence intervals. Heterogeneity was assessed using the I2 method.
Results: Overall, from 1242 studies identified, 30 were included, pooling data from 509 patients. The higher efficacy rates when, cell-based therapies were excluded, were achieved by immunochemotherapeutic regimens followed by combinatorial regimens, with complete response rates of 21.54% (IC95%14.93-28.87) and 23.77% (IC95% 8.70-42.19), respectively. Bispecific antibodies (alone or coupled with a chemotherapy debulking strategy) overtook Bruton tyrosine kinase inhibitors response rates. The latter, although achieving objective response rates above average, presented scarce complete response rates. Checkpoint inhibitors alone usually do not lead to complete responses, but their effectiveness may improve when combined with other agents, unveiling the importance of immune microenvironmental modulation.
Conclusion: This is the first meta-analysis of early clinical trials assessing the impact of different therapeutics in RS. By analyzing the pooled efficacy estimates, our work suggests the role of a tailor-made bridging therapy for young patients with RS eligible for allogeneic hematopoietic stem cell transplantation (alloSCT), formally the only curative strategy.
Richter syndrome affects 2 to 10% of patients diagnosed with chronic lymphocytic leukemia (1), being regarded as the phenotypic transdifferentiating phenomenon that occurs in a minority of chronic lymphocytic leukemia patients who develop a diffuse large B-cell lymphoma (DLBCL) or, less commonly, Hodgkin’s lymphoma (2). If clonally related to chronic lymphocytic leukemia, RS has a worse prognosis in comparison with clonally unrelated clones (3, 4). Indeed, while its etiopathogenesis involves a gradual accumulation of genomic and microenvironmental changes resulting in clonal divergence, the debate surrounding the presence or absence of clonality in relation to CLL vividly underscores the uncertainties regarding the cell of origin in RS. It remains unclear whether RS originates from CLL cells with stem-like properties or from dormant circulating CLL pools that, through successive damage, achieve competitive edge and become predominant (5). The median overall survival of patients diagnosed with RS rounds 12 months; however, this expectancy decreases with the presence of other risk factors or previous exposure to treatment regimens (6). Several risk factors have been associated with RS burden, including unmutated immunoglobulin heavy-chain status, TP53 pathological variants, BCR stereotype subset #8, del(17p) or complex karyotype, NOTCH1 and MYC mutations, as well as CDKN2A/B tumour suppressor gene loss (5).
Concerning the immunological fitness unbalance in CLL, which preceeds overt RS burden, there is an inhibitory effect in NK cells cytotoxicity, decreased function of γδ T cells, increased T cell exhaustion and higher circulating T regulatory (Treg) lymphocytes (7). Impaired immune effector functions and increased immune tolerance may jeopardize the immunosurveillance, creating a substrate for disease progression. Beyond immunological overall fitness, nodal tissue analysis revealed a higher PD-L1 expression in histiocytes and dendritic cells of RS patients in comparison to those with CLL, analogously to increased infiltration by FOXP3+ T cells and CD163-positive macrophages (8). These results not only endorse the idea of maintaining an immune microenvironment that nurtures malignancy but also underscore the prerequisites for the implementation of immunotherapeutic approaches with checkpoint inhibitors.
The efficient treatment of RS comprises a deep understanding of the disease biology and patient characteristics (namely immunological fitness status, highly dependent upon previous therapeutic incursions for CLL and/or RS), as well as a strategical therapeutic sequencing that maximizes the potential to bridge young and fit patients to allogeneic hematopoietic stem cells transplantation. Beyond R-CHOP (rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone) as a frontline approach to RS-DLBCL subtype and the use of platinum-based regimens as rescue therapy (1), there is no established consensus regarding the therapeutic sequencing.
This systematic review and meta-analysis delves into the treatment approaches for RS (DLBCL-subtype) that were the focus of clinical trials, aiming to assess their efficacy (complete response and objective response rates). By comparing the outcomes of early trials and analyzing the characteristics of enrolled patients, we intend to suggest a tailor-made therapeutic sequencing.
This study was conducted according to the Cochrane collaboration guidelines for systematic reviews. The search was performed in MEDLINE (https://pubmed.ncbi.nlm.nih.gov), Web of Science (https://www.webofknowledge.com) and SCOPUS (https://www.scopus.com). All data, without language or publication dates restriction imposed, was collected from inception up to 7th May of 2023 using the following keywords or medical subject heading terms: “Richter” AND (“syndrome” OR “transformation”) AND (“treatment” OR “therapy”).
We aimed to identify all relevant publications focusing clinical trials assessing the efficacy of treatment strategies in the context of Richter syndrome. Only scientific publications that fulfill the inclusion criteria were analyzed, namely: 1) clinical trials addressing therapeutic approaches to Richter syndrome (classical chemotherapeutic agents, targeted drugs, immunomodulatory agents and/or cell-based therapies); 2) all patients should have active disease upon study enrollment and 3) studies had to report at least complete response and/or partial response rates; 4) studies should provide efficacy results of patient treated with doses below the toxicity threshold.
The exclusion criteria were: being case reports, observational studies, narrative reviews, in vitro assays and animal studies, as well as guidelines, editorial, correspondences, consensus statements and cost-effectiveness studies, which were withdrawn from analysis.
Two authors (MSP and AM) independently reviewed the titles and abstracts of the studies identified in the search and excluded those that clearly did not meet the eligibility criteria. The full text of the remaining manuscripts was evaluated to determine their inclusion or exclusion. The lists of studies selected for inclusion independently by each author were compared, and disagreements were resolved jointly through discussion until consensus was reached; when necessary, a third author was also involved in the discussion. The following information was abstracted from each study into a data extraction form: complete response rate, objective response rate (the sum of complete and partial response rates), prevalence of the most frequent and severe (grade ≥ 3) adverse effects. Differences in data extraction were settled by consensus.
The methodology of studies and the reporting quality were assessed independently by two authors using the Critical Appraisal Skills Programme (CASP) checklist for Clinical Trials, adapted considering the inclusion of early clinical trials that preclude randomization. Furthermore, an analysis of potential bias across the studies was performed by examining funnel plots to identify any signs of asymmetry.
The endpoints analyzed were: i) objective clinical response, ii) complete response rates, and iii) treatment failure in intension-to-treat analysis (patients not achieving at least a partial response, maintaining a stable disease or progressing) of the patients with Richter syndrome submitted to pharmacological therapies. The proportions achieved at each outcome were retrieved from each study and the pooled metrics were obtained using the Der-Simonian and Laird random-effects model, which considers both between-study and within-study variation (9, 10). The Freeman–Tukey double arcsine method was used to retrieve the variance, as previously reported (11). Furthermore, subgroup analysis was performed, dividing studies by the most common therapeutic strategies (classical chemotherapy regimens; chemoimmunotherapy [monoclonal antibodies and/or immunomodulators and/or bispecific antibodies coupled with classic chemotherapy backbones]; immunotherapy [bispecific antibodies or immune-checkpoint inhibitors]; Bruton-tyrosine kinase inhibitors [iBTK]; other targeted therapies excluding iBTK and cell-based therapies, comprising CAR-T cells). The evaluation of heterogeneity among the studies was conducted through I2 statistics along with corresponding 95% confidence intervals. Lastly, Egger’s statistical tests followed by the funnel plot visual assessment were used to recognize publication bias. All statistical analyses were performed using the meta package (12) for R, version 3.5.3 (R Foundation for Statistical Computing, Vienna, Austria). A p-value less than 0.05 was considered statistically significant.
Our query identified 2095 records, of which 853 were duplicates. The remaining 1242 articles were evaluated considering the titles and abstracts, and 1204 records that did not fulfill the inclusion criteria were eliminated. Then, 38 potentially relevant records were retrieved and underwent full evaluation. Finally, 30 studies were included in our meta-analysis (Figure 1).
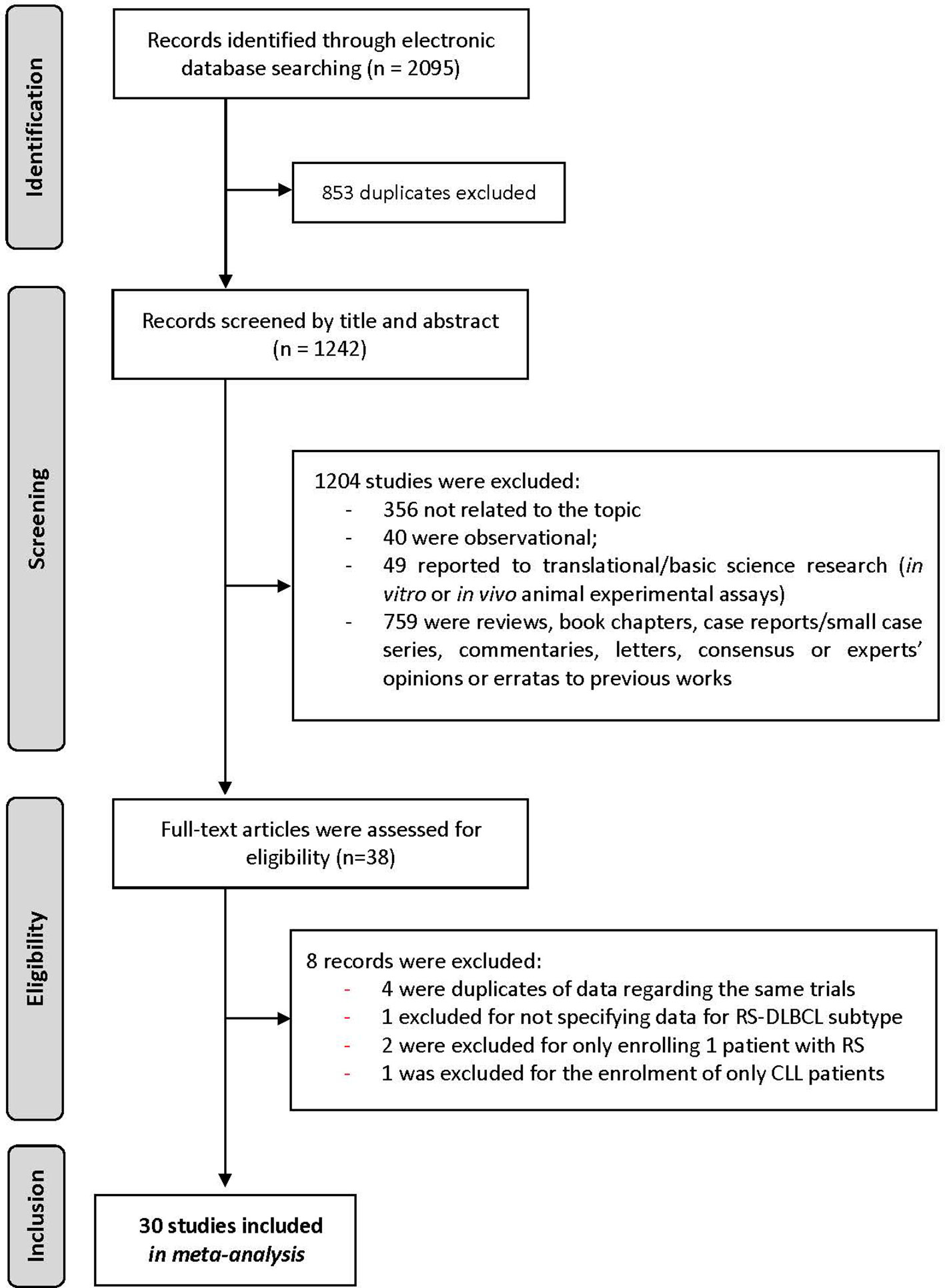
Figure 1 Flowchart representing the selection of studies.
The analysis of studies was performed following the Comprehensive Assessment of Study Protocols (CASP) for clinical trials. Overall studies’ quality was classified as moderate (Figure 1, Supplementary Materials). The analysis of the funnel plots along with the results of the Egger test (p>0.05) suggested low potential for publication bias (Figure 2, Supplementary Materials).
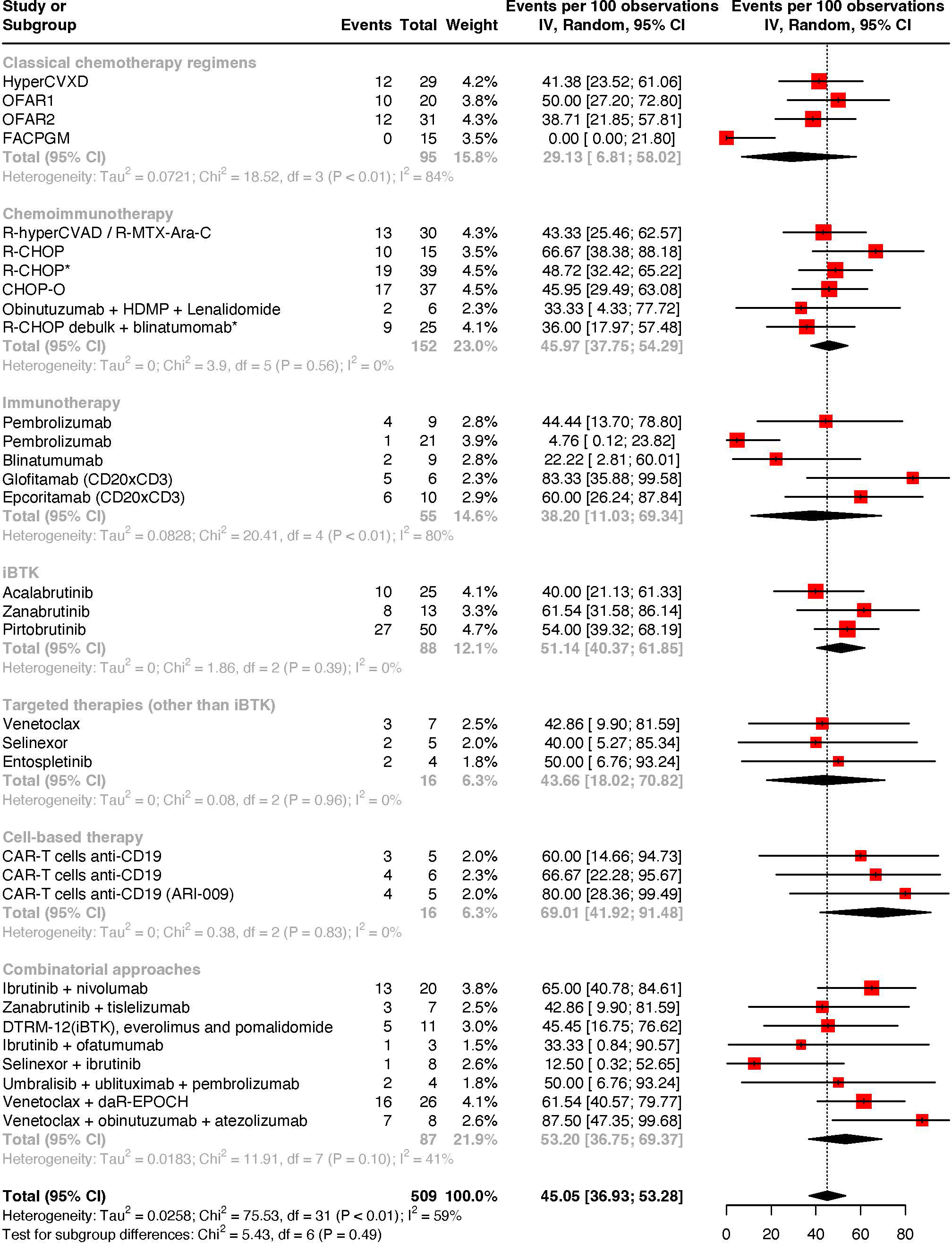
Figure 2 Meta-analysis of objective response rates by treatment strategies.
Characteristics of studies are summarized in Table 1. Thirty studies were included, comprising early phase clinical trials (phase I and II) assessing response’ efficacy of therapeutic approaches in Richter syndrome, DLBCL-subtype. From these, four assessed the outcomes with classical chemotherapy regimens, five explored immunochemotherapy regimens, five focused on immunotherapy as a standalone approach, three dissected regimens encompassing Bruton-tyrosine kinase inhibitors and three studies analyzed other targeted therapies beyond iBTK, eight studies assessed combinatorial approaches and three analyzed the outcomes of CAR-T cells. Globally, the studies enrolled 509 patients, the majority of whom had previous therapeutic incursions exposition, either to chronic lymphocytic leukemia and/or to Richter syndrome.
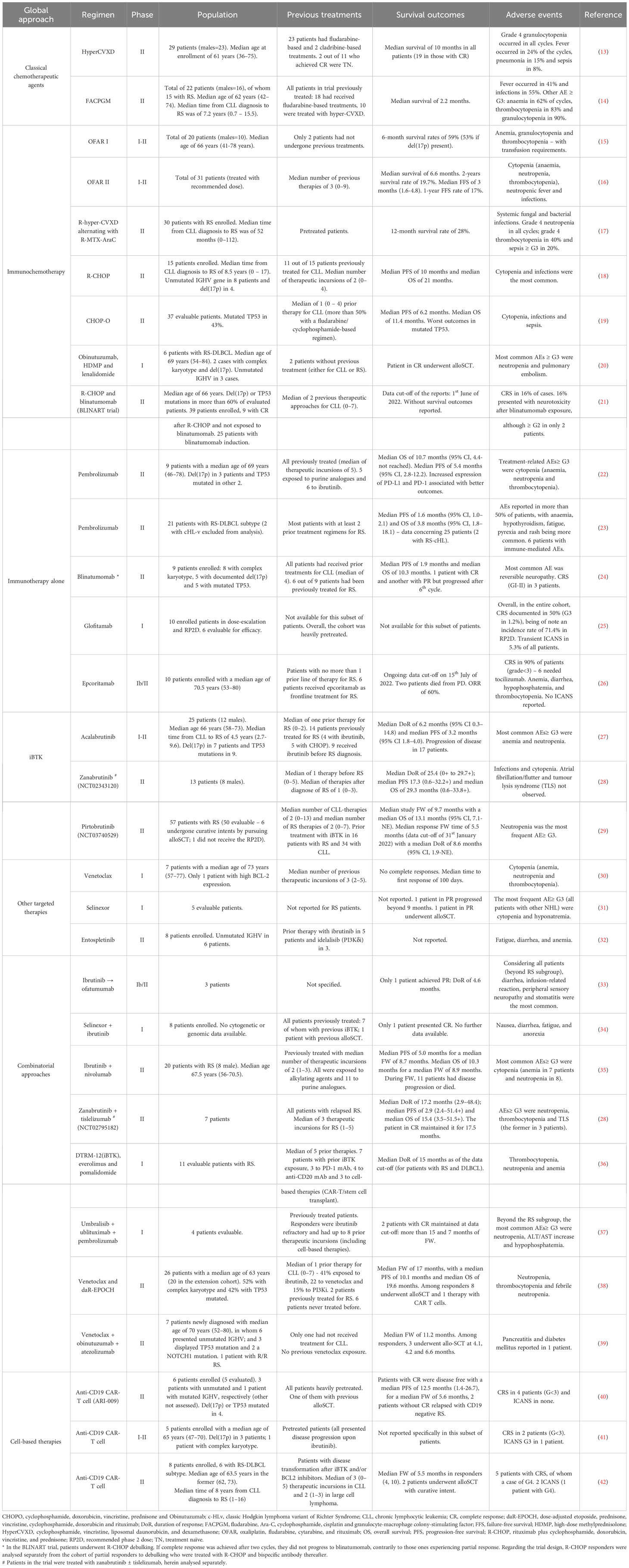
Table 1 Richter syndrome treatment approaches in early clinical trials.
Considering the studies reporting objective response rates in patients with RS, the pooled estimate rate was 45.05% (95% CI: 36.93–53.28%; I2 = 59% - Figure 2). The subgroup analysis revealed higher overall response rates upon chemoimmunotherapy, iBTK-based and combination treatment approaches (iBTK ± immune checkpoint inhibitor ± PI3K inhibitor ± immunochemotherapy backbones ± other target agents). In fact, overall response rates were 45.97% (95% CI: 37.75–54.29%; I2 = 0%) for chemoimmunotherapy, 51.14% (95% CI: 40.37–61.85%; I2 = 0%) for iBTK-based approaches and 53.20% (95% CI: 36.75–69.37%; I2 = 41%) for combination therapy. Chemoimmunotherapeutic approaches outlasted classical chemotherapeutic regimens, which presented modest objective response rates of 29.13% (95% CI: 6.81–58.02%; I2 = 84%). Other targeted therapies beyond iBTK achieved objective responses in 43.66% of patients (95% CI: 18.02-70.82; I2 = 0%), yet these agents were unable to produce complete responses.
Regarding complete response rates, pooled estimates were 17.99% (95% CI: 11.95–24.75%; I2 = 59% - Figure 3). Chemoimmunotherapy regimens achieve higher scores with an overall complete response rate of 21.54% (95% CI: 14.93–28.87%; I2 = 0%). Immunotherapy-based strategies achieved a complete response rate of 17.90% (95% CI: 0.84–44.90%; I2 = 77%), yet at the expense of a non-negligible heterogeneity.
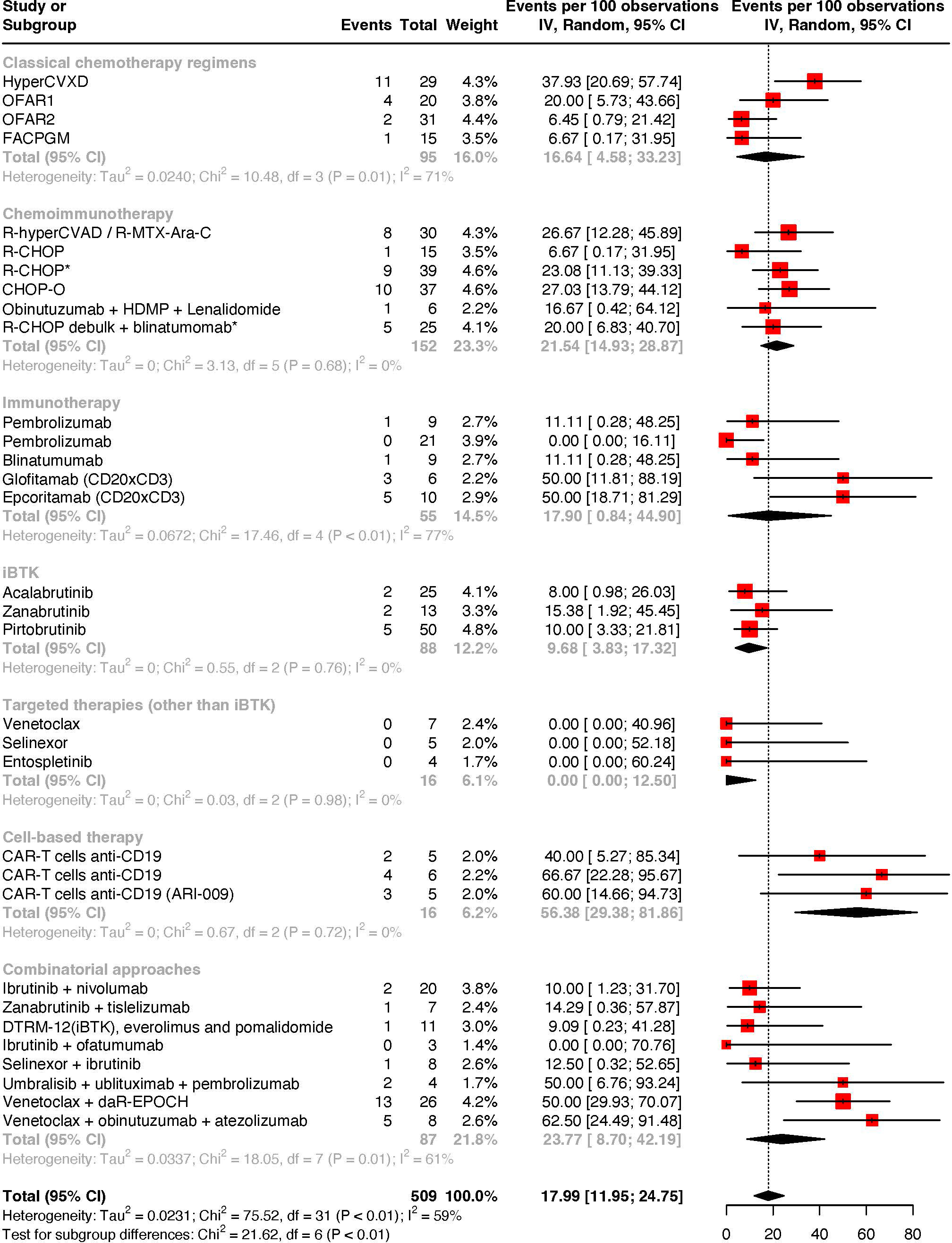
Figure 3 Meta-analysis of complete response rates by treatment strategies.
Cell-based therapies with CD19-directed CAR-T cells achieved the highest pooled scores with a complete response rate of 56.38% (95% CI: 29.38-81.86; I2 = 0%), and an overall response rate of 69.01% (95% CI: 41.92 - 91.48; I2 = 0%).
Among all the patients with Richter syndrome enrolled in early-phase clinical trials, 54.95% (95% CI: 46.72-63.07) failed to achieve at least a partial response (Supplementary Figure 3).
Considering the low prevalence of Richter syndrome, its biological heterogeneity, and its typical stringent clinical urgency demanding a prompt therapeutic approach, the conceptualization and operationalization of randomized clinical trials is a challenge. Despite early trials lacking randomization and the potential for a theoretical selection bias (including patients with milder forms of the disease who can adhere to a feasible treatment timeline, as opposed to heavily pretreated individuals with limited treatment avenues beyond clinical trials), our review acknowledges the valuable insights already present within the analyzed studies, summarizes the evidence and proposes a new conceptual sequential framework of treatment regimens in this cohort of patients.
The sole application of classical chemotherapeutic backbones is outdated, given the burst and continuous expansion of immunotherapeutic and targeted approaches that were able to improve therapeutic outcomes while simultaneously sparing undesirable toxicities. Notwithstanding, the initial trials with classic chemotherapeutic agents were essential for the refinement of modern therapeutic armamentariums. The OFAR 1 and 2 (oxaliplatin, fludarabine, cytarabine, and rituximab) trials explored the role of platinum agents (15); or fludarabine and cytarabine (16), respectively, by means of progressively scaling up the cumulative doses of those agents until undesirable toxicities. Interestingly, OFAR1 achieved higher rates of complete responses that rounded 20% in comparison with 6% in OFAR2. The potential role of platinum agents in RS rendered the substratum to R-DHAP recommendation (rituximab, dexamethasone, cytarabine, cisplatin) as a potential salvage strategy in RS refractory to R-CHOP (1). Besides this proposal regarding R-DHAP as a potential salvage regimen, no specific trials were performed, nor retrospective observational studies are available to reinforce these recommendations. HyperCVXD, although paradoxically associated with the higher rate of complete responses in the classical strategy cohort, was associated with lower rates of objective responses per comparison with other strategies (13). These findings may potentially illustrate the role of a dose-dense cyclophosphamide protocol in a disease with complex biology and heterogeneous behavior. As a matter of fact, we can speculate that although in a subset of patients, this protocol is able to eradicate disease, in other ones, the immune-pauperization induced by cyclophosphamide with a decrease in the counts of immune effector cells may promote the maintenance of disease by sustaining a nurturing microenvironment. Up to date, apart from palliative metronomic chemotherapy protocols, no trials have explored the role of low doses of cyclophosphamide, now acknowledged for paradoxically boosting immune effector functions (43). Herein, cyclophosphamide is a double-edged sword in treating lymphoid malignancies, without a direct relationship between dose and the achieved effect: its use should be titrated in contexts where there is a probable need to manipulate the immune system for cancer treatment.
Concerning R-CHOP, results are different between trials, potentially reflecting different subsets of patients enrolled. Langerbeins et al. demonstrated a reduced response to the abovementioned strategy, although only 15 patients were enrolled, of whom at least 8 displayed adverse prognostic genetic features (18). On the other hand, a subgroup analysis of the BLINART cohort, in whom patients were treated with R-CHOP and only if a partial response was achieved after two cycles, subsequently underwent therapy with blinatumomab (bispecific antibody targeting CD19 in neoplastic cells and CD3+ in T cells); initial debulking strategy displayed an objective response rate of 48.7% and a complete response rate rounding 23.0%, considering the 39 patients firstly enrolled (21). Anthracycline-based chemotherapy backbones are particularly interesting given the immunogenic cell death induced in neoplastic tissues, which contrasts with the general state of immunosuppression classically induced by other chemotherapeutic drugs (44).
R-CHOP results as a standalone are not statistically different from those produced by the combination of a CHOP backbone with obinutuzumab, followed by a maintenance strategy with the anti-CD20 antibody after chemotherapy each 8 weeks (19).
Considering the use of bispecific antibodies as a standalone strategy or coupled with a sequential debulking strategy first, the last option seems to produce better results. Indeed, considering the R-CHOP debulking followed by blinatumomab immunotherapy, complete response and objective response rounded 20% and 36%, respectively (21); per comparison with blinatumomab alone where more modest response rates of 11% and 22%, respectively (24), were achieved.
In our meta-analysis, besides the reduced number of included patients, when considering the immunotherapeutic strategies as a standalone, patients treated with bispecific antibodies achieved better outcomes per comparison with those treated singly with anti-PD1 (programmed-death 1) antibodies. Bispecific antibodies targeting CD20 in malignant cells produced higher rates of responses (25, 26) per comparison with blinatumomab. Unfortunately, disease relapse after bispecific antibody treatment was biologically characterized not infrequently by the trogocytosis of the targeted differentiation-cluster in the neoplastic entity (24).
Bruton-tyrosine kinase inhibitors achieve only modest response rates. Namely, the higher response rates are achieved by zanabrutinib, followed by pirtobrutinib. These results may reflect intrinsic characteristics of the disease, given that the majority of RS enrolled patients was pretreated (for CLL and/or RS), and herein potentially exposed to iBTK and prone to acquire resistances to this targeted therapy or even develop gain of function mutations in downstream signaling mediators. Indeed, patients with CLL who exhibit early refractoriness to iBTK appear to have a higher likelihood of histologic transformation, regardless of acquired resistance to this group of agents. Conversely, those who progress later during therapy often exhibit a higher incidence of variants in the BTK at residue C481 or downstream signaler phospholipase C gamma 2 (PLCγ2) within its autoinhibitory domain, which confers resistance to ibrutinib (45). Besides the BTK variant affecting the activity of iBTK covalent inhibitors (ibrutinib, acalabrutinib and zanabrutinib); noncovalent inhibitors as pirtobrutinib also have variants in BTK kinase domain able to confer resistance (V416L, A428D, M437R, T474I, and L528W), that once again, may be coupled with gain of function variants in PLCγ2 (46). BTK kinase domain variants are documented to appear up to nine months before overt clinical resistance and their search may allow the reshape of the treatment strategy. Moreover, gain-of-function variants of PLCγ2 are dependent on SYK and LYN signaling, with in vitro studies showing that the inhibition of the former kinases may counter-regulate the resistance induced by PLCγ2 (47). Metabolic reprogramming with increased oxidative phosphorylation and increased independence upon BTK downstream signaling may further explain iBTK resistance in the setting of RS pathobiology (48).
The administration of iBTK in individuals whose immune function is impaired either by disease progression or by successive cycles of chemotherapy-induced immunosuppression followed by immune-reconstitution phenomena and increased immune-tolerance arousal renders another pathway that might potentially explain the below-average results in this subset of patients. Although previous studies in relapsed or refractory CLL have shown that ibrutinib exposure led to a decrease in pathological B cells, regulatory T cells and myeloid-derived suppressor cells, while preserving naive T cells and NK cells and boosting its activity (49), this parallel immune outcome may become compromised if there is an impairment of the basic physiological immune reserve imposed by overt disease burden and bone marrow involvement.
Overall, the second generation iBTKs, by means of a higher potency and lower off-target effects, coupled with a better pharmacokinetic profile, may explain a mild increase in the efficacy results observed. For instance, zanabrutinib, the drug achieving better results, was shown to display a low affinity to glycoprotein-P, herein displaying lower pharmacokinetic variability (50).
iBTK treatment coupled with anti-PD1 or anti-PD-L1 (programmed-death ligand 1) antibodies seemed to not significantly improve outcomes in treatment response. Once again, heavily pretreated individuals and immune exhaustion may explain the results.
Beyond iBTKs, none of the other targeted agents included in early phase trials (venetoclax – BCL-2 inhibitor; entospletinib – spleen tyrosine kinase inhibitor; and selinexor - selective inhibitor of nuclear export) were able to induce complete responses. The rising trend of treating CLL patients upfront with venetoclax-based regimens may partially account for the results. This is due to the propensity for the development of variants that reduce venetoclax’s affinity towards BCL-2, as well as the upregulation of the anti-apoptotic members BCL-xL and MCL1, with the former being correlated with the overexpression of NOTCH2. In in vitro experiments, it was demonstrated that MCL1 inhibitors partially overcame venetoclax resistance when used in combination (47).
Among combinatorial approaches, higher response rates are achieved with venetoclax associated with obinutuzumab and atezolizumab, where complete response rounds 62.50% and objective response 87.50%, despite the small number of patients (whose majority was pretreated) enrolled in the early trial (39). Contrarily to CLL cells and non-clonally related DLBCL, PD-1 expression seems to be increased in RS cells. Although more infrequently, PD-L1 may also become expressed in RS and microenvironmental immune players as histocytes and dendritic cells (51). Perhaps, the divergence between the objective response rates of PD-1 monoclonal antibodies (pembrolizumab) as a standalone therapeutic approach and the respective complete response rates act as a reflection of neoplastic heterogeneity within the treated patients, herein imposing a further need in the characterization of the neoplasia before treatment. Assessing the expression levels of PD-1 and PD-L1 in RS may become of surmount importance when defining salvage regimens that may take into consideration the resource to checkpoint inhibitors.
The trial addressing the combinatory regimen with umbralisib (PI3K-δ inhibitor), ublituximab (anti-CD20 mAb) and pembrolizumab enrolled only four patients with RS and produced an ORR and CR of 50%. Umbralisib, beyond PI3K-δ inhibition, downregulates CK-1ε (casein kinase-1 epsilon), allowing a simultaneous sparing the circulatory T regulatory cells (expected to antagonize immune adverse effects mediated by PI3K inhibition) (52).
Lastly, venetoclax associated with daR-EPOCH is another combinatorial regimen producing above-average results in our meta-analysis. Although the majority of patients was previously exposed to venetoclax before enrolment in the trial (38), daEPOCH backbone differs from the CHOP standard by means of a modified drug dosage associated with the addition of etoposide. Beyond topoisomerase II inhibition, etoposide-quinone (metabolite of the drug) is known to impair the activity of CREBBP (acetyltransferase enzyme also with tumour suppressor functions) (53) herein potentially increasing the risk of additional molecular anomalies that increase even further the neoplastic phenotypic aggressiveness. Although the inclusion of etoposide in metronomic palliative regimens is acceptable, the switch of frontline R-CHOP regimens to daEPOCH backbones, may induce more harm than good by increasing the genomic anomalies within tumours with higher cellular turnover, ultimately rendering further chemoresistance.
Zilovertamab-vedotin is an antibody-drug conjugate that by targeting the receptor tyrosine kinase-like orphan receptor 1 (ROR1) in the cellular membrane of neoplastic cells and acting as a cargo for monomethyl auristatin E (antimicrotubule cytotoxic agent), is currently being explored in the context of RS. Although early results have prompted objective responses in four out of seven patients enrolled (54), the inclusion of RS patients both with DLBCL and cHL-variants without a subgroup analysis in preliminary results led to the withdrawal of this agent from our meta-analysis.
Richter syndrome detrimental prognosis demands a steady hand in disease management and therapeutic sequencing as an attempt to bridge young and fit patients to alloSCT, the only approach up-to-date documented as conveying a curative intent.
After prompt disease immune and molecular characterization, as well as staging, frontline immunochemotherapy with R-CHOP is recommended. In refractory patients or in those who relapse before alloSCT, the therapeutic sequencing should take into consideration the patient and disease characteristics, as well as the previous therapeutic exposures. For instance, fludarabine-based protocols are known to induce immunological dysfunction. For patients with chronic lymphocytic leukemia and treated with RFC (rituximab, fludarabine and cyclophosphamide), a profound depletion of all T-cell populations is documented. Indeed, a median time of 24 months is needed to reach counts of CD4+ T levels above 400/μL; while CD8+ T cells needed a median time of 12 months to achieve counts within the normal range (55). Analogously, bendamustine is also responsible for inducing a severe T cell depletion, with CD4+ T cell counts remaining lower than 200 cells/μL for more than 9 months after treatment completion (56). Given the immune off-target effects produced by these classical chemotherapeutic agents widely used in the treatment of CLL, previous exposition to any of them, especially if recently, should be taken into consideration when defining the therapeutic strategy to RS.
Indeed, in those recently exposed to lymphodepleting chemotherapeutic agents, such as fludarabine or bendamustine, iBTK approaches should be prioritized, particularly in previously naïve patients. Whenever possible, molecular characterization of the neoplasm should be conducted to identify C481 variants of BTK (which confer resistance to covalent inhibitors) or V416L, A428D, M437R, T474I, and L528W (which confer resistance to noncovalent inhibitors). Additionally, a search for pathological variants with gain-of-function mutations in PLCγ2 (which promote disease progression independently of BTK inhibition) should be done. The discovery of any genetic variant impairing the pharmacological inhibition of the Bruton tyrosine kinase pathway should prompt a reconsideration of this strategy. Refractoriness or relapse after iBTK in this setting should trigger the switch of the strategy to an immunotherapeutic approach with bispecific antibodies (bulky disease, higher tumour burden with hyperleukocytosis, or impaired immunological fitness may withdraw this strategy) or a combinatorial approach encompassing venetoclax associated with obinutuzumab and an immune checkpoint inhibitor (dependent on the relative expression of PD1 or PD-L1).
In patients with Richter syndrome arising from a CLL being treated with iBTK, therapy should start with R-CHOP. If the transformation happens early after iBTK incursion, its burden is potentially independent of the BTK resistance-conferring variants, being likely the result of downstream signaler variants with gain of function and subsequent neoplastic cells metabolic reprogramming. In this subset of patients, in case of refractoriness or relapse after R-CHOP, platinum-based protocols (R-DHAP) or a switch to bispecific antibodies can be done and posteriorly, if necessary, an off-label salvage regimen with venetoclax associated with obinutuzumab and an immune checkpoint inhibitor initiated.
In patients with newly diagnosed RS and treatment naïve (either for CLL and RS), following R-CHOP, therapeutic incursions can be performed sequentially with platinum-based protocols (R-DHAP), iBTK, bispecific antibodies and lastly, as an off-label salvage regimen, with a combinatorial strategy encompassing venetoclax associated with obinutuzumab and an immune checkpoint inhibitor.
CAR-T cells produced interesting results, although a small number of patients was assessed by this new cell-based therapeutic approach. Moreover, there is a shortage of extended follow-up data concerning this group of treated patients. However, it is anticipated that as advancements continue in this biotechnological method, modified CAR-T cells might eventually eliminate the need for some patients to undergo alloSCT with curative intent.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
MS-P: conceptualization, data curation, formal analysis, investigation, methodology, project administration, software, visualization, writing – original draft, writing – review & editing. ÂM: conceptualization, writing – review & editing, data curation. JM: writing – review & editing. PB: conceptualization, project administration, supervision, writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Instituto de Salud Carlos III (PI22/00147) co-financed by Fondos Feder and Gobierno de Navarra Proyecto ARNMUNE Ref.: 0011–1411-2023.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
PB declared that he was an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1295293/full#supplementary-material
1. Parikh SA, Kay NE, Shanafelt TD. How we treat Richter syndrome. Blood (2014) 123(11):1647–57. doi: 10.1182/blood-2013-11-516229
2. Rossi D, Spina V, Gaidano G. Biology and treatment of Richter syndrome. Blood (2018) 131(25):2761–72. doi: 10.1182/blood-2018-01-791376
3. Rossi D, Spina V, Deambrogi C, Rasi S, Laurenti L, Stamatopoulos K, et al. The genetics of Richter syndrome reveals disease heterogeneity and predicts survival after transformation. Blood (2011) 117(12):3391–401. doi: 10.1182/blood-2010-09-302174
4. Mao Z, Quintanilla-Martinez L, Raffeld M, Richter M, Krugmann J, Burek C, et al. IgVH mutational status and clonality analysis of Richter’s transformation: diffuse large B-cell lymphoma and Hodgkin lymphoma in association with B-cell chronic lymphocytic leukemia (B-CLL) represent 2 different pathways of disease evolution. Am J Surg Pathol (2007) 31(10):1605–14. doi: 10.1097/PAS.0b013e31804bdaf8
5. Parry EM, Ten Hacken E, Wu CJ. Richter syndrome: Novel insights into the biology of transformation. Blood (2023) 142(1):11–2. doi: 10.1182/blood.2022016502
6. Wang Y, Tschautscher MA, Rabe KG, Call TG, Leis JF, Kenderian SS, et al. Clinical characteristics and outcomes of Richter transformation: experience of 204 patients from a single center. Haematologica (2020) 105(3):765–73. doi: 10.3324/haematol.2019.224121
7. Mahmoud AM, Gaidano G, Mouhssine S. Immunological aspects of richter syndrome: from immune dysfunction to immunotherapy. Cancers (Basel). (2023) 15(4):1015. doi: 10.3390/cancers15041015
8. Wang Y, Sinha S, Wellik LE, Secreto CR, Rech KL, Call TG, et al. Distinct immune signatures in chronic lymphocytic leukemia and Richter syndrome. Blood Cancer J (2021) 11(5):86. doi: 10.1038/s41408-021-00477-5
9. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. (1986) 7(3):177–88. doi: 10.1016/0197-2456(86)90046-2
10. DerSimonian R, Laird N. Meta-analysis in clinical trials revisited. Contemp Clin Trials. (2015) 45:139–45. doi: 10.1016/j.cct.2015.09.002
11. Barendregt JJ, Doi SA, Lee YY, Norman RE, Vos T. Meta-analysis of prevalence. J Epidemiol Community Health (2013) 67(11):974–8. doi: 10.1136/jech-2013-203104
12. Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Software (2010) 36(3):1–48. doi: 10.18637/jss.v036.i03
13. Dabaja BS, O’Brien SM, Kantarjian HM, Cortes JE, Thomas DA, Albitar M, et al. Fractionated cyclophosphamide, vincristine, liposomal daunorubicin (daunoxome), and dexamethasone (hyperCVXD) regimen in Richter’s syndrome. Leuk Lymphoma. (2001) 42(3):329–37. doi: 10.3109/10428190109064589
14. Tsimberidou AM, O’Brien SM, Cortes JE, Faderl S, Andreeff M, Kantarjian HM, et al. Phase II study of fludarabine, cytarabine (ara-C), cyclophosphamide, cisplatin and GM-CSF (FACPGM) in patients with Richter’s syndrome or refractory lymphoproliferative disorders. Leuk Lymphoma. (2002) 43(4):767–72. doi: 10.1080/10428190290016872
15. Tsimberidou AM, Wierda WG, Plunkett W, Kurzrock R, O’Brien S, Wen S, et al. Phase I-II study of oxaliplatin, fludarabine, cytarabine, and rituximab combination therapy in patients with Richter’s syndrome or fludarabine- refractory chronic lymphocytic leukemia. J Clin Oncol (2008) 26(2):196–203. doi: 10.1200/JCO.2007.11.8513
16. Tsimberidou AWGW, Wen S, Plunkett W, O’Brien S, Kipps TJ, Jones JA, et al. Phase I-II clinical trial of oxaliplatin, fludarabine, cytarabine, and rituximab therapy in aggressive relapsed/refractory chronic lymphocytic leukemia or Richter syndrome. Clin lymphoma myeloma leukemia (2013) 13:568–74. doi: 10.1016/j.clml.2013.03.012
17. Tsimberidou AM, Kantarjian HM, Cortes J, Thomas DA, Faderl S, Garcia-Manero G, et al. Fractionated cyclophosphamide, vincristine, liposomal daunorubicin, and dexamethasone plus rituximab and granulocyte-macrophage-colony stimulating factor (GM-CSF) alternating with methotrexate and cytarabine plus rituximab and GM-CSF in patients with Rich. Cancer (2003) 97(7):1711–20. doi: 10.1002/cncr.11238
18. Langerbeins P, Busch R, Anheier N, Dürig J, Bergmann M, Goebeler ME, et al. Poor efficacy and tolerability of R-CHOP in relapsed/refractory chronic lymphocytic leukemia and Richter transformation. Am J Hematol (2014) 89:E239–43. doi: 10.1002/ajh.23841
19. Eyre TA, Clifford R, Bloor A, Boyle L, Roberts C, Cabes M, et al. NCRI phase II study of CHOP in combination with ofatumumab in induction and maintenance in newly diagnosed Richter syndrome. Br J haematology (2016) 175:43–54. doi: 10.1111/bjh.14177
20. Heyman BM, Choi MY, Kipps TJ. Obinutuzumab, high-dose methylprednisolone (HDMP), and lenalidomide for the treatment of patients with Richter’s syndrome. Cancers (Basel). (2022) 14(24):6035. doi: 10.3390/cancers14246035
21. Guieze R, Ysebaert L, Roos-Weil D, Fornecker L-M, Ferrant E, Molina L, et al. Blinatumomab for patients with richter syndrome: final results of the phase 2 blinart trial from the filo group. Blood (2022) 140(Supplement 1):6631–2. doi: 10.1182/blood-2022-159695
22. Ding W, LaPlant BR, Call TG, Parikh SA, Leis JF, He R, et al. Pembrolizumab in patients with CLL and Richter transformation or with relapsed CLL. Blood (2017) 129(26):3419–27. doi: 10.1182/blood-2017-02-765685
23. Armand P, Murawski N, Molin D, Zain J, Eichhorst B, Gulbas Z, et al. Pembrolizumab in relapsed or refractory Richter syndrome. . Vol. 190 Br J haematology. England; (2020) p:e117–20. doi: 10.1111/bjh.16762
24. Thompson PA, Jiang X, Banerjee P, Basar R, Garg N, Chen K, et al. A phase two study of high dose blinatumomab in Richter’s syndrome. Leukemia (2022) 36:2228–32. doi: 10.1038/s41375-022-01649-3
25. Hutchings M, Morschhauser F, Iacoboni G, Carlo-Stella C, Offner FC, Sureda A, et al. Glofitamab, a novel, bivalent CD20-targeting T-cell-engaging bispecific antibody, induces durable complete remissions in relapsed or refractory B-cell lymphoma: A phase I trial. J Clin Oncol Off J Am Soc Clin Oncol (2021) 39(18):1959–70. doi: 10.1200/JCO.20.03175
26. Kater AP, Ye JC, Sandoval-Sus J, Bellido M, Christensen JH, Mato AR, et al. Subcutaneous epcoritamab in patients with richter’s syndrome: early results from phase 1b/2 trial (EPCORE CLL-1). Blood (2022) 140(Supplement 1):850–1. doi: 10.1182/blood-2022-158298
27. Eyre TA, Schuh A, Wierda WG, Brown JR, Ghia P, Pagel JM, et al. Acalabrutinib monotherapy for treatment of chronic lymphocytic leukaemia (ACE-CL-001): analysis of the Richter transformation cohort of an open-label, single-arm, phase 1-2 study. Lancet Haematology (2021) 8:e912–21. doi: 10.1016/S2352-3026(21)00305-7
28. Tam C, Munoz J, Cull G, Opat S, Allewelt H, Zhang X, et al. Zanubrutinib, alone and in combination with tislelizumab, for the treatment of Richter transformation of chronic lymphocytic leukemia. HemaSphere (2023) 7(4):e870. doi: 10.1097/HS9.0000000000000870
29. Wierda WG, Lewis DJ, Ghia P, Shah NN, Coombs CC, Cheah CY, et al. Efficacy of pirtobrutinib, a highly selective, non-covalent (Reversible) BTK inhibitor in richter transformation: results from the phase 1/2 BRUIN study. Blood (2022) 140(Supplement 1):846–9. doi: 10.1182/blood-2022-157058
30. Davids MS, Roberts AW, Seymour JF, Pagel JM, Kahl BS, Wierda WG, et al. Phase i first-in-human study of venetoclax in patients with relapsed or refractory non-hodgkin lymphoma. J Clin Oncol (2017) 35(8):826–33. doi: 10.1200/JCO.2016.70.4320
31. Kuruvilla J, Savona M, Baz R, Mau-Sorensen PM, Gabrail N, Garzon R, et al. Selective inhibition of nuclear export with selinexor in patients with non-Hodgkin lymphoma. Blood (2017) 129:3175–83. doi: 10.1182/blood-2016-11-750174
32. Awan FT, Thirman MJ, Patel-Donnelly D, Assouline SAVR, Ye W, Hill B, et al. Entospletinib monotherapy in patients with relapsed or refractory chronic lymphocytic leukemia previously treated with B-cell receptor inhibitors: results of a phase 2 study. Leukemia lymphoma (2019) 60:1972–7. doi: 10.1080/10428194.2018.1562180
33. Jaglowski SM, Jones JA, Nagar V, Flynn JM, Andritsos LA, Maddocks KJ, et al. Safety and activity of BTK inhibitor ibrutinib combined with ofatumumab in chronic lymphocytic leukemia: A phase 1b/2 study. Blood (2015) 126(7):842–50. doi: 10.1182/blood-2014-12-617522
34. Stephens DM, Huang Y, Ruppert AS, Walker JS, Cempre CB, Fu Q, et al. Selinexor combined with ibrutinib demonstrates tolerability and safety in advanced B-cell Malignancies: A phase I study. Clin Cancer Res (2022) 28(15):3242–7. doi: 10.1158/1078-0432.CCR-21-3867
35. Younes A, Brody J, Carpio C, Lopez-Guillermo A, Ben-Yehuda D, Ferhanoglu B, et al. Safety and activity of ibrutinib in combination with nivolumab in patients with relapsed non-Hodgkin lymphoma or chronic lymphocytic leukaemia: a phase 1/2a study. Lancet Haematol (2019) 6(2):e67–78. doi: 10.1016/S2352-3026(18)30217-5
36. Mato AR, Schuster SJ, Foss FM, Isufi I, Kothari SK, Ding W, et al. A once daily, oral, triple combination of BTK inhibitor, mTOR inhibitor and IMiD for treatment of relapsed/refractory Richter’s transformation and de novo diffuse large B-cell lymphoma. Blood (2020) 136(Supplement 1):21–2. doi: 10.1182/blood-2020-138896
37. Mato A, Svoboda J, Luning-Prak E, Schuster S, Tsao P, Dorsey C, et al. Phase I/II Study of Umbralisib (TGR-1202) in Combination with Ublituximab (TG-1101) and Pembrolizumab in Patients with Relapsed/Refractory CLL and Richter's Transformation. Blood (2018) 132(Supplement 1):297. doi: 10.1182/blood-2018-99-117526
38. Davids MS, Rogers KA, Tyekucheva S, Wang Z, Pazienza SSKR, Renner SK, et al. Venetoclax plus dose-adjusted R-EPOCH for Richter syndrome. Blood (2022) 139:686–9. doi: 10.1182/blood.2021011386
39. Jain N, Ferrajoli A, Thompson PA, Konopleva M, Green MR, Sampath D, et al. Venetoclax, obinutuzumab and atezolizumab (PD-L1 checkpoint inhibitor) for treatment for patients with richter transformation. Blood (2021) 138(Supplement 1):1550. doi: 10.1182/blood-2021-154279
40. Ortiz-Maldonado V, Frigola G, Español-Rego M, Balagué O, Martínez-Cibrián N, Magnano L, et al. Results of ARI-0001 CART19 cells in patients with chronic lymphocytic leukemia and Richter’s transformation. Front Oncol (2022) 12:828471. doi: 10.3389/fonc.2022.828471
41. Turtle CJ, Hay KA, Hanafi L-A, Li D, Cherian S, Chen X, et al. Durable molecular remissions in chronic lymphocytic leukemia treated with CD19-specific chimeric antigen receptor-modified T cells after failure of ibrutinib. J Clin Oncol Off J Am Soc Clin Oncol (2017) 35(26):3010–20. doi: 10.1200/JCO.2017.72.8519
42. Benjamini O, Shimoni A, Besser M, Shem-Tov N, Danylesko I, Yerushalmi R, et al. Safety and efficacy of CD19-CAR T cells in richter’s transformation after targeted therapy for chronic lymphocytic leukemia. Blood (2020) 136(Supplement 1):40. doi: 10.1182/blood-2020-138904
43. Hughes E, Scurr M, Campbell E, Jones E, Godkin A, Gallimore A. T-cell modulation by cyclophosphamide for tumour therapy. Immunology (2018) 154(1):62–8. doi: 10.1111/imm.12913
44. Casares N, Pequignot MO, Tesniere A, Ghiringhelli F, Roux S, Chaput N, et al. Caspase-dependent immunogenicity of doxorubicin-induced tumour cell death. J Exp Med (2005) 202(12):1691–701. doi: 10.1084/jem.20050915
45. Ahn IE, Underbayev C, Albitar A, Herman SEM, Tian X, Maric I, et al. Clonal evolution leading to ibrutinib resistance in chronic lymphocytic leukemia. Blood (2017) 129(11):1469–79. doi: 10.1182/blood-2016-06-719294
46. Wang E, Mi X, Thompson MC, Montoya S, Notti RQ, Afaghani J, et al. Mechanisms of resistance to noncovalent bruton’s tyrosine kinase inhibitors. N Engl J Med (2022) 386(8):735–43. doi: 10.1056/NEJMoa2114110
47. Maher N, Mouhssine S, Matti BF, Alwan AF, Gaidano G. Treatment refractoriness in chronic lymphocytic leukemia: old and new molecular biomarkers. Int J Mol Sci (2023) 24(12):10374. doi: 10.3390/ijms241210374
48. Mouhssine S, Gaidano G. Richter syndrome: from molecular pathogenesis to druggable targets. Cancers (Basel). (2022) 14(19):4644. doi: 10.3390/cancers14194644
49. Solman IG, Blum LK, Hoh HY, Kipps TJ, Burger JA, Barrientos JC, et al. Ibrutinib restores immune cell numbers and function in first-line and relapsed/refractory chronic lymphocytic leukemia. Leuk Res (2020) 97:106432. doi: 10.1016/j.leukres.2020.106432
50. Tam CS, Ou YC, Trotman J, Opat S. Clinical pharmacology and PK/PD translation of the second-generation Bruton’s tyrosine kinase inhibitor, zanubrutinib. Expert Rev Clin Pharmacol (2021) 14(11):1329–44. doi: 10.1080/17512433.2021.1978288
51. He R, Ding WDSV, Chen D, Shi M, Van Dyke D, Tian S, et al. PD-1 expression in chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and large B-cell richter transformation (DLBCL-RT): A characteristic feature of DLBCL-RT and potential surrogate marker for clonal relatedness. Am J Surg Pathol (2018) 42(7):843–54. doi: 10.1097/PAS.0000000000001077
52. Maharaj K, Powers JJ, Achille A, Mediavilla-Varela M, Gamal W, Burger KL, et al. The dual PI3Kδ/CK1ε inhibitor umbralisib exhibits unique immunomodulatory effects on CLL T cells. Blood Adv (2020) 4(13):3072–84. doi: 10.1182/bloodadvances.2020001800
53. Zhang W, Berthelet J, Michail C, Bui L-C, Gou P, Liu R, et al. Human CREBBP acetyltransferase is impaired by etoposide quinone, an oxidative and leukemogenic metabolite of the anticancer drug etoposide through modification of redox-sensitive zinc-finger cysteine residues. Free Radic Biol Med (2021) 162:27–37. doi: 10.1016/j.freeradbiomed.2020.11.027
54. Spurgeon SE, Mei M, Barr PM, Barrientos JC, de Vos S, Furman RR, et al. Waveline-001: updated results from a phase 1 dose escalation and cohort expansion study of zilovertamab vedotin (MK-2140) in non-hodgkin lymphoma. Blood (2022) 140(Supplement 1):6640–1. doi: 10.1182/blood-2022-163509
55. Ysebaert L, Gross E, Kühlein E, Blanc A, Corre J, Fournié JJ, et al. Immune recovery after fludarabine-cyclophosphamide-rituximab treatment in B-chronic lymphocytic leukemia: implication for maintenance immunotherapy. Leukemia (2010) 24(7):1310–6. doi: 10.1038/leu.2010.89
56. García Muñoz R, Izquierdo-Gil A, Muñoz A, Roldan-Galiacho V, Rabasa P, Panizo C. Lymphocyte recovery is impaired in patients with chronic lymphocytic leukemia and indolent non-Hodgkin lymphomas treated with bendamustine plus rituximab. Ann Hematol (2014) 93(11):1879–87. doi: 10.1007/s00277-014-2135-8
Keywords: Richter syndrome, immunotherapy, targeted-therapy, cell-based therapy, meta-analysis
Citation: Sousa-Pimenta M, Martins Â, Mariz JM and Berraondo P (2023) Response to therapy in Richter syndrome: a systematic review with meta-analysis of early clinical trials. Front. Immunol. 14:1295293. doi: 10.3389/fimmu.2023.1295293
Received: 15 September 2023; Accepted: 09 November 2023;
Published: 23 November 2023.
Edited by:
Maria Teresa Sabrina Bertilaccio, University of Texas MD Anderson Cancer Center, United StatesReviewed by:
Patrick Kevin Reville, University of Texas MD Anderson Cancer Center, United StatesCopyright © 2023 Sousa-Pimenta, Martins, Mariz and Berraondo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mário Sousa-Pimenta, bXNvdXNhcGltZW50YUBpcG9wb3J0by5taW4tc2F1ZGUucHQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.