
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol., 22 June 2023
Sec. Alloimmunity and Transplantation
Volume 14 - 2023 | https://doi.org/10.3389/fimmu.2023.1178546
This article is part of the Research TopicRegulatory immune cells in organ transplantationView all 9 articles
 Adil Ahmed Ali1
Adil Ahmed Ali1 Khalid Eltahir Khalid1,2*
Khalid Eltahir Khalid1,2* Somaya Elhaj Mohammed3
Somaya Elhaj Mohammed3 Mohammed Salman Akhtar2*Osman Khalafalla Saeed4
Mohammed Salman Akhtar2*Osman Khalafalla Saeed4The aim of this study was to determine the Human Leukocyte Antigen (HLA) class II (DRB1 and DQB1) alleles and haplotype frequency in Rheumatoid Arthritis (RA) in the Sudanese population. The frequency of HLA-DRB1 and -DQB1 alleles and DRB1-DQB1 haplotypes were determined in 122 RA patients and 100 controls. HLA alleles were genotyped by the polymerase chain reaction-sequence specific primers (PCR-SSP) method. In RA patients, HLA-DRB1*04 and *10 alleles were high in frequency (9.6% vs 14.2%, P = 0.038 and P = 0.042, respectively), and dependently on anti-citrullinated protein antibodies (ACPAs) seropositivity (P = 0.044 and P = 0.027, respectively). In contrast, the frequency of the HLA-DRB1*07 allele was significantly low in patients than in controls (11.7% vs 5.0%, P = 0.010). Moreover, the HLA-DQB1*03 allele was strongly associated with RA risk (42.2%, P = 2.2x10-8), whereas, HLA-DQB1*02 and *06 showed protective effects against RA (23.1% and 42.2%, P = 0.024 and P = 2.2x10-6, respectively). Five different HLA haplotypes, DRB1*03-DQB1*03 (P = 0.00003), DRB1*04-DQB1*03 (P = 0.00014), DRB1*08-DQB1*03 (P = 0.027), DRB1*13-DQB1*02 (P = 0.004), and DRB1*13-DQB1*03 (P = 3.79x10-8) were significantly associated with RA risk, while 3 protective haplotypes, DRB1*03-DQB1*02 (Pc = 0.008), DRB1*07-DQB1*02 (Pc = 0.004), and DRB1*13-DQB1*06 (Pc = 0.02) were identified. This is the first study determining the association between HLA class II alleles and haplotypes and RA risk in our population.
Rheumatoid arthritis (RA) is a systemic chronic inflammatory disease of unknown etiology, characterized by multifactorial etiology and complex genetic background, particularly with Human Leukocyte Antigen (HLA) (1). The exact etiology of RA is unknown, although the pathogenesis is critically influenced by genetic and environmental factors. The genetic components, particularly for HLA-DR/DQ genotypes were extensively studied worldwide and proved to contribute to RA risk (2). Their rate of contribution to RA is varied in different studies and between different populations. In general, RA patients who carried certain HLA-DR/DQ alleles are subjected to a high risk of developing the disease in different populations (3–5), including sub-Saharan African populations (6, 7). There is extensive evidence that some HLA-DRB1 alleles, including HLA-DRB1*01, HLA-DRB1*04, HLA-DRB1*09, HLA-DRB1*10, and HLA-DRB1*14 implicated with RA susceptibility in different populations (7–11).
The serological anti-citrullinated protein antibodies (ACPA) and the rheumatoid factor (RF) have been extensively studied and reported as important diagnostic and prognostic biomarkers for RA and were also found to be associated with more aggressive and erosive disease. ACPA was found more specific and sensitive for RA diagnosis and a better predictor of poor prognostic features such as progressive joint destruction and has been strongly associated with HLA class 11 molecules, like HLA-DRB1 (8, 12).
Sudan is a large country of high effective population size and traditional societies that have diverse linguistic, ethnic, social, cultural, and religious characteristics. The manifestation of the impact of culture in disease burden with regard to consanguinity has been associated with genetic disorders, particularly those of autosomal recessive nature such as sickle cell mutation (HbS) among the ‘Baggara’, and with lactase persistence (LP) mutations among the ‘Beja’ and ‘Fulani’ of western Sudan (9, 10). In our population, with regard to different ethnicities and consanguineous marriages, no study relating RA and genetic associations has been yet conducted and no data on RA prevalence, especially with RF or anti-CCP positivity, are available. Therefore, this study was conducted for the first time to investigate the frequency of HLA-DRB/DQ alleles and haplotypes and their association with RA, as this might emphasize the nature, susceptibility, and prognosis of the disease in our population.
This is a cross-sectional study, comprising 122 RA patients (mean age, 44.95±14.03 yrs; 106 female, 16 male) diagnosed in the rheumatology clinics at Ibrahim Malik & The Academy Teaching Hospitals, in Khartoum state-Sudan. Sudan’s Khartoum state, in which the study was conducted, is the capital, fulminated by different ethnic groups that equally share easy access to health facilities that are provided via primary and tertiary health care. The quality of life in the state is quite high as to other regions, where the highest abundance of health facilities exists.
All patients were clinically examined by two rheumatologists and were assessed based on the American College of Rheumatology Criteria (ACR) Board of Directors and the European League Against Rheumatism (EULAR) Executive Committee (13). The demographic, clinical information, and laboratory profiles were indicated in the clinical interview form as shown in Table 1. The control group included 100 non-related healthy volunteers (mean age, 43.06±10.51 years; 89 female, 11 male), with no apparent disease, no family history of RA or other autoimmune diseases, and were from the same hospitals, departments, and geographical areas. All participants were notified of the study purposes and objectives, and written consent was obtained before the inclusion applied, directly from adults or guardians of children under 18 years of age. The study protocol was approved by the University of Gezira Ethical Committee and performed according to the ethical guidelines of the Helsinki Declaration.
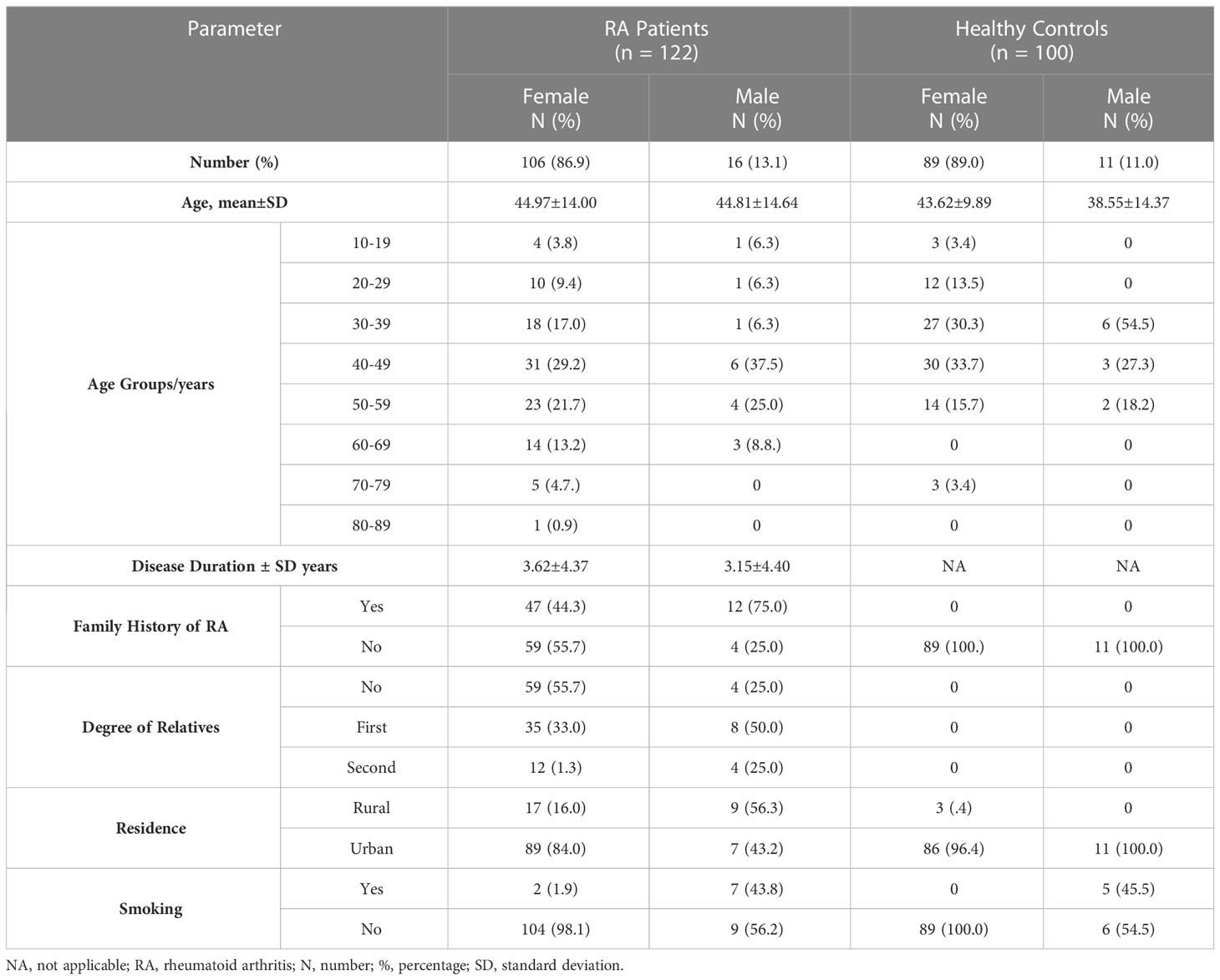
Table 1 Baseline characteristics in RA patients and healthy controls.
Genomic DNA was extracted from peripheral venous blood using QIA amp® DNA mini kit (Qiagen CA, USA) according to the manufacturer’s instructions.
HLA class II DRB1-DQB1 genotyping was carried out by polymerase chain reaction (PCR) with sequence-specific primers (SSP) using low-resolution kits (Rose, HLA-SSP Typing Kits, Germany). The PCR amplification of DNA was performed using Applied Biosystem 9700 thermo-cycler (Thermo Fisher, UK), and the procedure was carried out according to the manufacturer’s instructions. The obtained DNA fragments were photographed, edited, and documented on 2% agarose gel with 0.5μg/ml ethidium bromide added, using a gel documentation system, and the typing genotypes were obtained using HLA software provided by Rose Company (R.O.S.E. Europe GmbH).
Serum ACPA was measured using anti-CCP IgG antibodies, detected by Immunoscan CCPlus® ELISA kits (Euro Diagnostic, AB-Malmo, Sweden), as per the manufacturer’s instructions. ACPA concentration >25 U/ml was considered positive. Serum IgM rheumatoid factor (RF) and c-reactive protein (CRP) were assessed using an automated chemistry analyzer (Cobas Mira Plus, Roche, Basel, Switzerland) and rapid latex agglutination test (NS Bio-Tec, Egypt), respectively. CRP level <10 mg/L (0-9.9 mg/L) was considered normal, while the presence of RF agglutination indicates a positive test.
The statistical analysis was conducted by using SPSS software, version 23 (SPSS Inc., Chicago, IL, USA). Categorical variables were presented as counts and percentages. The independent sample t-test was used to compare the mean differences of quantitative variables between patients and controls. The significant differences in allele frequencies (AF) of DRB1 and DQB1 were compared between patients and controls by using a chi-square test or Fisher’s exact test for discrete data. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated as indicated. Two-locus associations and haplotype frequencies (HF) were determined by direct counting of samples with a particular combination of alleles, and the significance of these associations was determined by a chi-square test with Yates’ correction. Bonferroni correction was used for alleles and haplotypes with frequencies >5% and applied when the P-value is significant. Corrected probability values (Pc) were calculated by multiplying individual P-values by the number of comparisons made at the allele or haplotype levels: 8 for HLA-DRB1 alleles and 3 for DRB1-DQB1 haplotypes. In our data analysis, a P-value less than 0.05 was considered significant.
The demographic data and the clinical features of 122 patients diagnosed with RA are presented in Table 1. Mainly females are predominant in the study subjects. A high frequency of RA patients was found in the age group between 40-59 years. Almost half of the patients (48.4%) were having a family history of RA, out of them 72.9% as first-degree relatives. The RA clinical picture indicates that the majority (68.0%) suffered from morning stiffness, and half of the patients were positive for ACPA (52.5%) and CRP (45.9%). Joint pain was mostly in the wrist, fingers, knee & hands. Ulnar deviation is the most frequent deformity (26.2%), followed by Boutonniere deformity (14.8%) (Table 2).
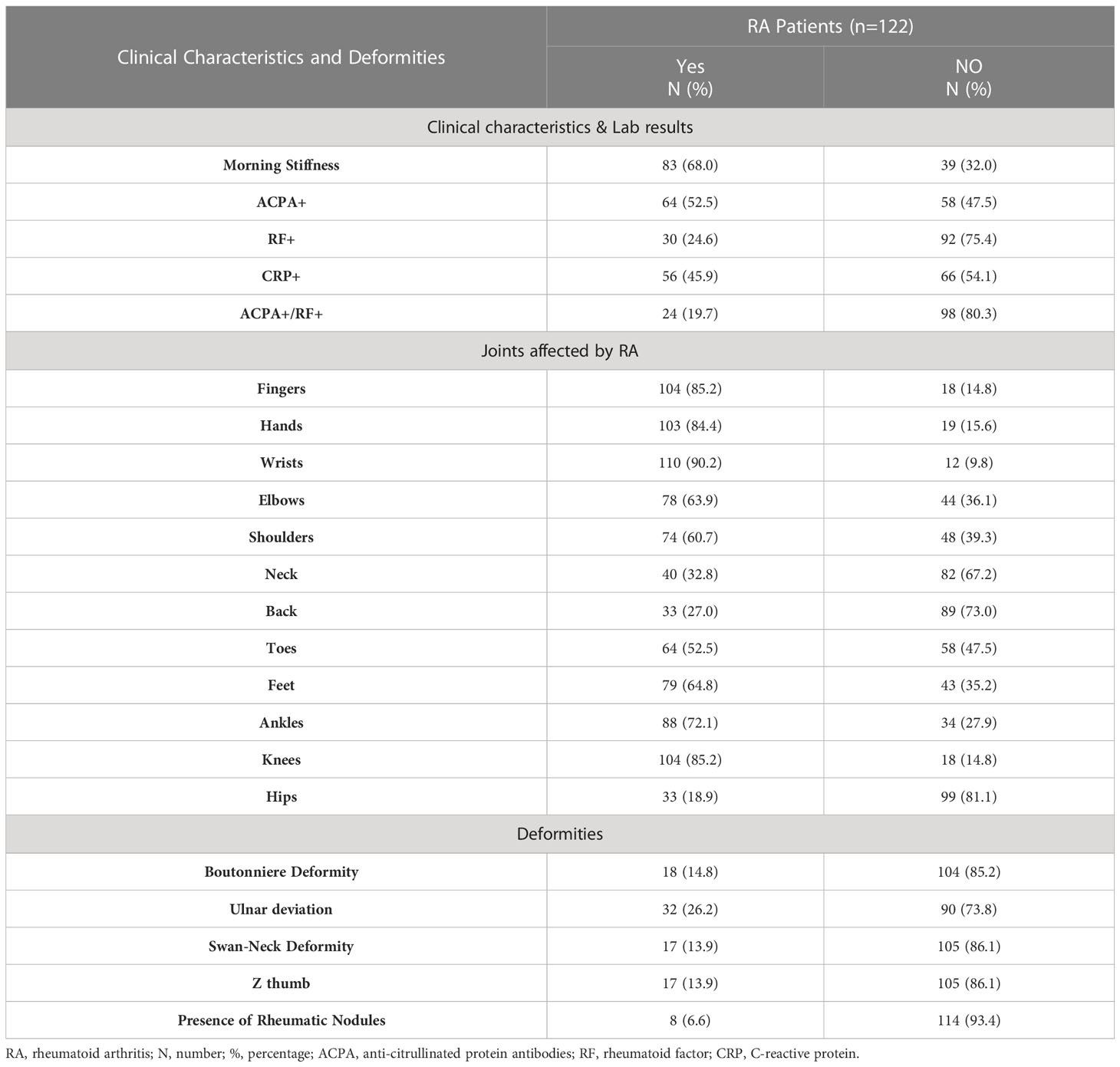
Table 2 RA Clinical characteristics and deformities.
The distribution of HLA-DRB1 and HLA-DQB1 alleles in our study subjects is shown in Table 3. In patients, the most frequent HLA-DRB1 alleles were *13 (20.4%), *10 (14.2%), and *15 (12.5%), while HLA-DRB1*13 (23.5%), *11 (22.2%), and *07 (11.7%) were in controls. HLA-DRB1*04 and *10 frequency were significantly higher in patients than in controls [9.6% vs 5.1%, P = 0.038, OR (95% CI) = 0.47 (0.32-0.54) and 14.2% vs 8.2%, P = 0.042, OR (95% CI) = 1.86 (0.99-3.48)], and was associated with ACPA positivity [22.2% vs 8.8%, P = 0.044, OR (95% CI) = 2.97 (1.00-8.87) and 23.8% vs 8.8%, P = 0.027, OR (95% CI) = 3.25 (1.10-9.62), respectively] (Table 4). In contrast, the HLA-DRB1*07 allele was significantly lower (P = 0.010) in patients (5.0%) than in controls (11.7%).

Table 3 HLA-DRB1 and DQB1 allele frequencies in RA patients and healthy controlsa.
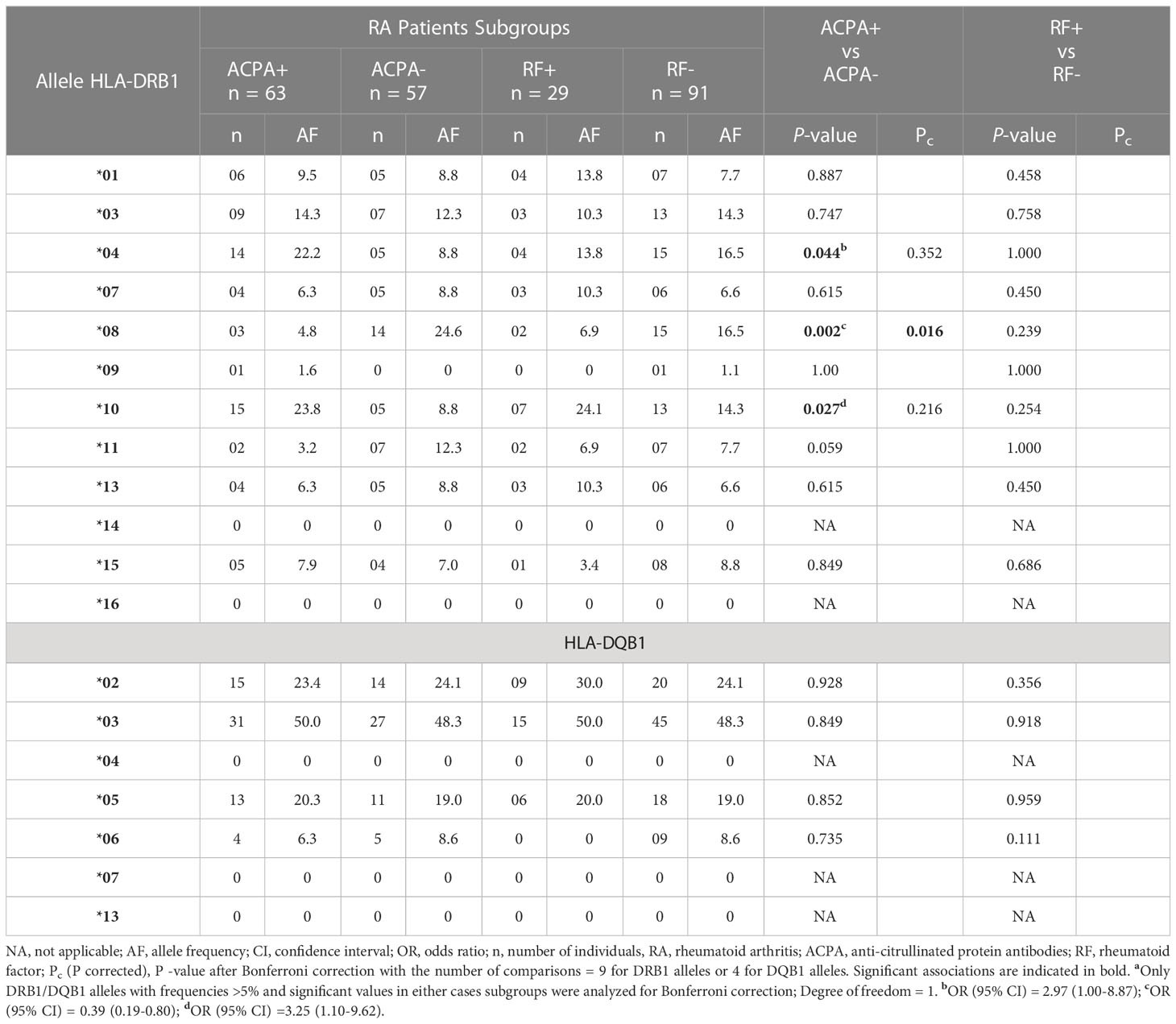
Table 4 HLA-DRB1 and DQB1 allele frequencies in ACPA/RF+ and ACPA/RF- RA patientsa.
Among ACPA seronegative patients, HLA-DRB1*08 frequency was significantly higher than in ACPA seropositive counterpart [24.6% vs 4.8%, P = 0.002, OR (95% CI) = 0.40 (0.19-0.82)], which remained significant after Bonferroni correction (Pc = 0.016).
No associations were found between RF antibody and HLA-DRB1 and HLA-DQB1 alleles and haplotypes (Table 4).
The most frequent HLA-DQB1 alleles in patients were HLA-DQB1*03 (42.2%) and *06 (23.4%), while in controls, were HLA-DQB1*06 (42.2%) and *02 (23.1%). HLA-DQB1*03 allele was significantly higher in frequency and associated with RA risk [42.2% vs 17.6%, P = 2.2x10-8; OR (95% CI) = 3.43 (2.19-5.34)], this association persisted after multiple comparisons (Pc = 6.6x10-8). In contrast, HLA-DQB1*02 and *06 were significantly higher in frequency in controls and may confer protection [23.1% vs 14.8%, P = 0.024, OR (95% CI) = 0.58 (0.34-9.30); 42.2% vs 23.4%, P = 2.2x10-6, OR (95% CI) = 0.42 (0.28-0.63), respectively] (Table 3). HLA-DQB1*06 significance remained following Bonferroni correction (Pc = 6.6x10-6).
As shown in Table 5, 13 HLA-DRB1 and HLA-DQB1 haplotypes were identified in our study subjects. In patients as compared with controls, HLA-DRB1*03-DQB1*03 [2.8% vs -%, P = 0.00003, OR (95% CI) = 2.54 (2.20-2.93)], HLA-DRB1*04-DQB1*03 [3.2% vs 0.5%, P = 0.00014, OR (95% CI) = 10.85 (2.42-48.65)], HLA-DRB1*13-DQB1*02 [1.4% vs -%, P = 0.004, OR (95% CI) = 2.46 (2.14-2.83)], and HLA-DRB1*13-DQB1*03 [5.6% vs 0.2%, P = 3.79x10-8, OR (95% CI) = 41.11 (5.48-308.46)] were associated with RA risk, each of which remained significant after correction of multiple comparisons (Pc = 0.0003, Pc = 0.0001, Pc = 0.032, and Pc = 3.3x10-9, respectively). On the other hand, HLA-DRB1*03-DQB1*02 [0.7% vs 4.6%, P = 0.004, OR (95% CI) = 0.19 (0.06-0.65), HLA-DRB1*07-DQB1*02 [1.3% vs 5.1%, P = 0.002, OR (95% CI) = 0.17 (0.05-0.58)], and HLA-DRB1*13-DQB1*06 [3.9% vs 10.4%, P = 0.010, OR (95% CI) = 0.45 (0.24-0.83)] haplotypes were significantly low in patients than in controls and remained significant when Bonferroni correction applied (Pc = 0.008, Pc = 0.004 and Pc = 0.02 respectively) (Table 5).
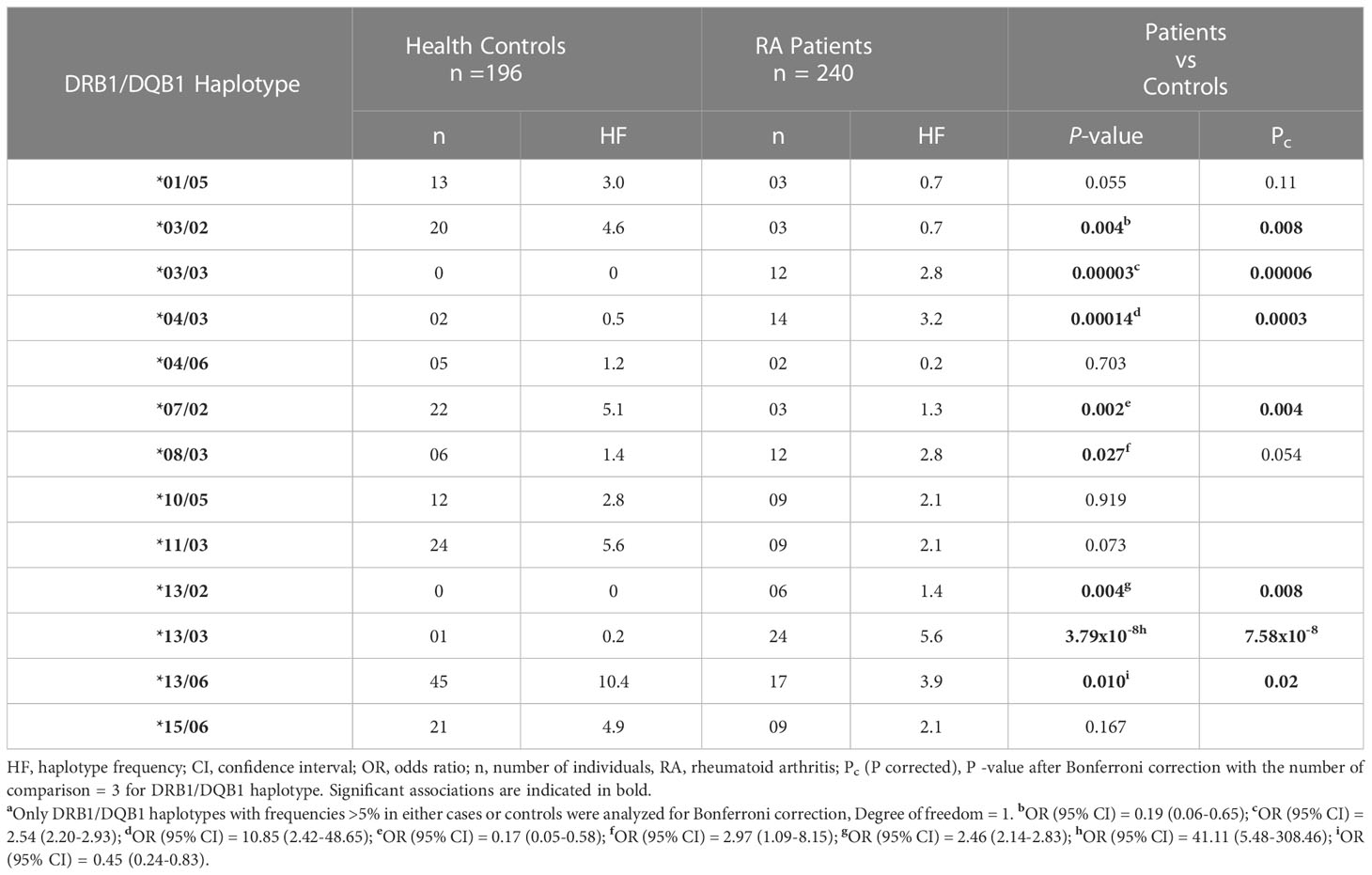
Table 5 HLA-DRB1/DQB1 haplotype frequencies in RA patients and healthy controlsa.
Furthermore, HLA-DRB1*08-DQB1*03 frequency was significantly high in patients [2.8% vs 1.4%, P = 0.027, (95% CI) = 2.97 (1.09-8.15)] and was found to be associated with ACPA seronegativity [OR (95% CI) = 0.09 (0.01-0.70), P = 0.006, Pc = 0.012] (Table 6). No association was found between HLA-DRB1/DQB1 haplotypes and RF antibodies (Table 6).
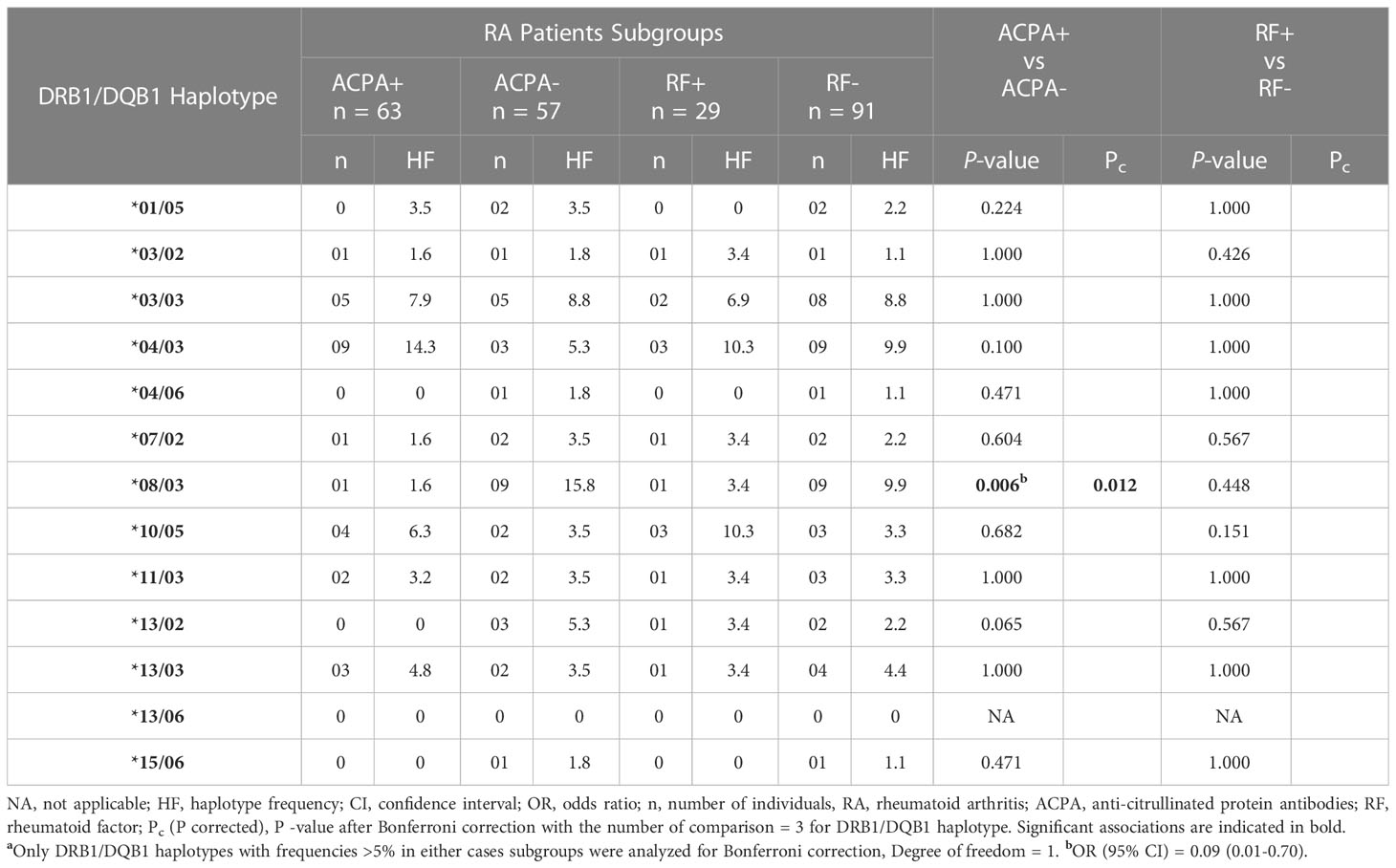
Table 6 HLA-DRB1/DQB1 haplotype frequencies in ACPA/RF+ and ACPA/RF- RA patientsa.
The most important genetic factors associated with RA are the Human Leukocyte Antigen (HLA) linked genes, accounting for approximately 30% of the total genetic contribution for RA susceptibility (14). The HLA-DRB1 locus is highly polymorphic and confers more risk for RA than any other locus (15). Susceptibility for developing rheumatoid arthritis (RA) is associated with particular HLA-DRB1 alleles like HLA- DRB1*04, HLA-DRB1*01, and HLA-DRB1*10 (16).
In our study cases, HLA-DRB1*04 and *10 were the most frequent alleles, which is consistent with studies in populations with different ethnicity (11, 17–23). Two small genetic studies have been performed in West/Middle Africa, showing the risk of developing RA was associated with HLA-DRB1*10 but not *04 (6, 24). Compared to people of European descent, African Americans are thought to have a lower prevalence of RA, lower frequency of the highest risk HLA-DRB1 classical alleles (e.g. *04:01, *04:04), and lower effect size of high-risk alleles with RA (15).
We also found that both alleles were statistically associated with ACPA seropositivity, which is consistent with studies in populations with different ethnicity (7, 25–28). Furthermore, strong evidence suggests that some HLA-DRB1 alleles, including HLA-DRB1*01, *04, and *10, were associated with the structural severity of RA, and were likely related to the production of ACPA by influencing the antigen presentation (29, 30).
In contrast, the HLA-DRB1*07 allele was found significantly increased in controls as compared with RA patients. This finding was consistent with studies from Algeria (27), Tunis (31, 32), Turkey (33), Finland (34), and Slovakia (35), suggesting that DRB1*07 confers a protective effect against RA development. On the contrary, the HLA-DRB1*07 allele was found common in both cases and controls in Bangladeshi (17) and Pakistani (36) populations.
On the other hand, our data showed that the significant frequent alleles of HLA-DQB1 identified in RA patients were HLA-DQB1*03 (P = 0.000, OR = 3.43), whereas in controls, was HLA-DRQB1*02 (P = 0.02, OR = 0.58) and *06 (P = 0.00, OR = 0.42).
HLA-DRQ1*02 and *06 were found protective against RA in the Albanian population (28), while in the Kurdi population, these alleles showed a susceptible effect to RA (37). Other studies in the Turkish population failed to prove any association (33).
In this study, HLA-DRB1*03/DRB1*03, HLA-DRB1*04/DRB1*03, HLA-DRB1*08/DRB1*3, HLA-DRB1*13/DRB1*02, and HLA-DRB1*13/DRB1*03 haplotypes, were associated with RA risk. A previous study on females with RA found that HLA-DRB1*03/DRB1*03 was associated with the development of RA, while HLA-DRB1*13/DRB1*03 represents a protective effect (38), other studies found that the haplotype HLA-DQB1*3 was linked to HLA-DRB1*09:01 or *04 and the haplotype HLA-DQB*05 linked to HLA-DRB1*01:01, *01:02, *01:03, and *10:01, and they were positively associated with RA in Caucasians (34). Collectively, the controversial results in HLA genotyping are strongly associated with the genetic makeup, owing to the differences in ethnicity between populations.
In this study, the level of biochemical markers such as ACPA, CRP, and ESR was found significantly high in RA patients as compared with the controls, which was consistent with other studies (39–42), and may indicate that the maintenance of process activity in RA patients as a result of acute phase reactants, the acceleration of sedimentation, and high CRP (41). Nevertheless, compared to anti-CCP, our data showed no significant association was found between HLA genotypes and RF. This finding is similar to the studies conducted in Turkish and Saudi populations, where the association was found with positive anti-CCP and not with RF (43, 44). This is not surprising as anti-CCP is more specific than RF, and seemed to play a pivotal role in the pathogenesis of RA.
Our data showed that HLA-DRB1*03/DRB1*02, HLA-DRB1*07/DRB1*02, and HLA-DRB1*13/DRB1*06 haplotypes confer a protective effect against RA. The protective effect of the HLA-DRB1*07/DRB1*02 haplotype was stated earlier in a population from Pakistan, who reported a negative association with RA (36). In parallel, a Moroccan study reported that the frequency of DRB1*07-DQB1*02 and DRB1*13-DQB1*06 haplotypes was decreased in RF-positive patients compared to controls (45). The HLA-DRB1*03/DRB1*02 protective effect has been observed in multiple autoimmune disorders, such as celiac disease (46) and type 1 diabetes (47), but not in RA.
The present study highlighted and reported for the first time the association of HLA class II (DRB1 and DQB1) alleles and haplotypes and the risk of developing RA in our population. HLA-DRB1*04, *10, and HLA-DQB1*03 were found associated with RA risk, while HLA-DRB1*07, HLA-DQB1*02, and *06 showed protection against RA. On the other hand, HLA-DRB1*03-DQB1*03, HLA-DRB1*04-DQB1*03, HLA-DRB1*08-DQB1*03, and HLA-DRB1*13-DQB1*02 haplotypes were associated with RA risk, whereas HLA-DRB1*03-DQB1*02, DRB1*07-DQB1*02, and HLA-DRB1*13- DQB1*06 confers protection.
We could not run the high-resolution genotyping due to cost constraints. Furthermore, the study sample size makes the degree of significance to determine the genetic risk relatively weak. More hands-on studies with large sample sizes and the use of high-resolution genotyping are needed to verify our findings.
The original contributions presented in the study are included in the article/supplementary materials. Further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by University of Gezira Ethical Committee. The patients/participants provided their written informed consent to participate in this study.
All authors contributed to the study perception and design; AA collected and analyzed the data with input from KK; AA, KK, and SM wrote the initial draft of the manuscript; KK, SM, MA, and OS revised and approved the final draft. All authors contributed to the article and approved the submitted version.
The authors would like to thank the hospital staff for their kind cooperation and the patients for their participation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Coenen MJ, Gregersen PK. Rheumatoid arthritis: a view of the current genetic landscape. Genes Immun (2009) 10(2):101–11. doi: 10.1038/gene.2008.77
2. Imboden JB. The immunopathogenesis of rheumatoid arthritis. Annu Rev Pathol (2009) 4:417–34. doi: 10.1146/annurev.pathol.4.110807.092254
3. Citera G, Padulo LA, Fernandez G, Lazaro MA, Rosemffet MG, Maldonado Cocco JA. Influence of HLA-DR alleles on rheumatoid arthritis: susceptibility and severity in Argentine patients. J Rheumatol (2001) 28(7):1486–91.
4. Bridges SL Jr, Kelley JM, Hughes LB. The HLA-DRB1 shared epitope in caucasians with rheumatoid arthritis: a lesson learned from tic-tactoe. Arthritis Rheum (2008) 58(5):1211–5. doi: 10.1002/art.23433
5. Delgado-Vega AM, Anaya JM. Meta-analysis of HLA DRB1 polymorphism in Latin American patients with rheumatoid arthritis. Autoimmun Rev (2007) 6(6):402–8. doi: 10.1016/j.autrev.2006.11.004
6. Dieye A, Diallo S, Diatta M. Identification of HLA-DR alleles for susceptibility to rheumatoid polyarthritis in Senegal. Dakar Méd (1997) 42(2):111–3.
7. Konda Mohan V, Ganesan N, Gopalakrishnan R, Venkatesan V. HLA-DRB1 shared epitope alleles in patients with rheumatoid arthritis: relation to autoantibodies and disease severity in a south Indian population. Int J Rheum Dis (2017) 20(10):1492–8. doi: 10.1111/1756-185X.12948
8. Bos WH, van de Stadt LA, Sohrabian A, Rönnelid J, van Schaardenburg D. Development of anti-citrullinated protein antibody and rheumatoid factor isotypes prior to the onset of rheumatoid arthritis. Arthritis Res Ther (2014) 16(2):405–6. doi: 10.1186/ar4511
9. Bereir RE, Hassan HY, Salih NA, Underhill PA, Cavalli-Sforza LL, Hussain AA, et al. Co-Introgression of y-chromosome haplogroups and the sickle cell gene across africa's sahel. Eur J Hum Genet (2007) 15(11):1183–5. doi: 10.1038/sj.ejhg.5201892
10. Priehodová E, Austerlitz F, Čížková M, Nováčková J, Ricaut FX, Hofmanová Z, et al. Sahelian pastoralism from the perspective of variants associated with lactase persistence. Am J Phys Anthropol (2020) 173(3):423–36. doi: 10.1002/ajpa.24116
11. Naqi N, Ahmed TA, Malik JM, Ahmed M, Bashir MM. HLA DRβ1 alleles in Pakistani patients with rheumatoid arthritis. J Coll Physicians Surg Pak (2011) 21(12):727–30.
12. Szodoray P, Szabó Z, Kapitány A, Gyetvai A, Lakos G, Szántó S, et al. Anti-citrullinated protein/peptide autoantibodies in association with genetic and environmental factors as indicators of disease outcome in rheumatoid arthritis. Autoimmun Rev (2010) 9(3):140–3. doi: 10.1016/j.autrev.2009.04.006
13. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO 3rd, et al. 2010 rheumatoid arthritis classification criteria: an American college of Rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheum (2010) 62(9):2569–81. doi: 10.1002/art.27584
14. Liu X, Guo J, Jia Y, Zhao Y, Liu X, Cheng F, et al. HLA-DRB1 shared epitope-dependent DR-DQ haplotypes are associated with both anti-CCP-positive and -negative rheumatoid arthritis in Chinese han. PloS One (2013) 8(8):e71373. doi: 10.1371/journal.pone.0071373
15. Reynolds RJ, Ahmed AF, Danila MI, Hughes LB, Consortium for the Longitudinal Evaluation of African Americans with Early Rheumatoid Arthritis Investigators, Gregersen PK, et al. HLA-DRB1-associated rheumatoid arthritis risk at multiple levels in African americans: hierarchical classification systems, amino acid positions, and residues. Arthritis Rheumatol (2014) 66(12):3274–82. doi: 10.1002/art.38855
16. Balandraud N, Picard C, Reviron D, Landais C, Toussirot E, Lambert N, et al. HLA-DRB1 genotypes and the risk of developing anti citrullinated protein antibody (ACPA) positive rheumatoid arthritis. PloS One (2013) 8(5):e64108. doi: 10.1371/journal.pone.0064108
17. Begum M, Sattar H, Haq SA, Islam MN, Saha SK, Hassan MM, et al. Study on association of human leukocyte antigen-DRB1 alleles amongst Bangladeshi patients with rheumatoid arthritis. Int J Rheum Dis (2018) 21(8):1543–7. doi: 10.1111/1756-185X.13291
18. Sandoughi M, Fazaeli A, Bardestani G, Hashemi M. Frequency of HLA-DRB1 alleles in rheumatoid arthritis patients in zahedan, southeast Iran. Ann Saudi Med (2011) 31(2):171–3. doi: 10.4103/0256-4947.78205
19. Mourad J, Monem F. HLA-DRB1 allele association with rheumatoid arthritis susceptibility and severity in Syria. Rev Bras Reumatol (2013) 53(1):47–56. doi: 10.1016/S2255-5021(13)70005-1
20. Al-Swailem R, Al-Rayes H, Sobki S, Arfin M, Tariq M. HLA-DRB1 association in Saudi rheumatoid arthritis patients. Rheumatol Int (2006) 26(11):1019–24. doi: 10.1007/s00296-006-0119-2
21. Louzada-Júnior P, Freitas MV, Oliveira RD, Deghaide NH, Conde RA, Bertolo MB, et al. A majority of Brazilian patients with rheumatoid arthritis HLA-DRB1 alleles carry both the HLA-DRB1 shared epitope and anti-citrullinated peptide antibodies. Braz J Med Biol Res (2008) 41(6):493–9. doi: 10.1590/s0100-879x2008005000021
22. Hughes LB, Morrison D, Kelley JM, Padilla MA, Vaughan LK, Westfall AO, et al. The HLADRB1 shared epitope is associated with susceptibility to rheumatoid arthritis in African americans through European genetic admixture. Arthritis Rheum (2008) 58(2):349–58. doi: 10.1002/art.23166
23. Liu SC, Chang TY, Lee YJ, Chu CC, Lin M, Chen ZX, et al. Influence of HLADRB1 genes and the shared epitope on genetic susceptibility to rheumatoid arthritis in Taiwanese. J Rheumatol (2007) 34(4):674–80.
24. Singwe-Ngandeu M, Finckh A, Bas S, Tiercy JM, Gabay C. Diagnostic value of anti-cyclic citrullinated peptides and association with HLA-DRB1 shared epitope alleles in African rheumatoid arthritis patients. Arthritis Res Ther (2010) 12(2):R36. doi: 10.1186/ar2945
25. Soliman AF, Egaila SE, Ali AI, Azab NI, Al-Gohary HH. HLA-DRB1 alleles in Egyptian rheumatoid arthritis patients: relations to anti-cyclic citrullinated peptide antibodies, disease activity and severity. Egyptian Rheumatologist (2016) 38(4):269–27. doi: 10.1016/j.ejr.2016.03.0007
26. Snir O, Widhe M, von Spee C, Lindberg J, Padyukov L, Lundberg K, et al. Multiple antibody reactivities to citrullinated antigens in sera from patients with rheumatoid arthritis: association with HLADRB1 alleles. Ann Rheum Dis (2009) 68(5):736–43. doi: 10.1136/ard.2008.091355
27. Djidjik R, Allam I, Douaoui S, Meddour Y, Cherguelaîne K, Tahiat A, et al. Association study of human leukocyte antigen-DRB1 alleles with rheumatoid arthritis in Algerian patients. Int J Rheum Dis (2017) 20(12):1993–7. doi: 10.1111/1756-185X.12272
28. Prifti-Kurti M, Nunes JM, Shyti E, Ylli Z, Sanchez-Mazas A, Sulcebe G. HLA-DRB1 and HLA-DQB1 allele associations in an Albanian patient population with rheumatoid arthritis: correlations with the specific autoantibody markers and inter-population DRB1 allele frequency variability. Rheumatol Int (2014) 34(8):1065–71. doi: 10.1007/s00296-013-2932-8
29. de Vries R. Genetics of rheumatoid arthritis: time for a change. Curr Opin Rheumatol (2011) 23(3):227–32. doi: 10.1097/BOR.0b013e3283457524
30. Bax M, van Heemst J, Huizinga TW, Toes RE. Genetics of rheumatoid arthritis: what have we learned? Immunogenetics (2011) 63(8):459–66. doi: 10.1007/s00251-011-0528-6
31. Dhaouadi T, Sfar I, Abdelmoula L, Bardi R, Jendoubi-Ayed S, Makhlouf M, et al. Association of specific amino acid sequence (QRRAA) of HLA-DRB1*0405 with rheumatoid arthritis in a Tunisian population. Arch Inst Pasteur Tunis (2010) 87(1-2):53–9.
32. Ben Hamad M, Mahfoudh N, Marzouk S, Kammoun A, Gaddour L, Hakim F, et al. Association study of human leukocyte antigen-DRB1 alleles with rheumatoid arthritis in south Tunisian patients. Clin Rheumatol (2012) 31(6):937–42. doi: 10.1007/s10067-012-1954-z
33. Uçar F, Karkucak M, Alemdaroğlu E, Capkin E, Yücel B, Sönmez M, et al. HLADRB1 allele distribution and its relation to rheumatoid arthritis in eastern black Sea Turkish population. Rheumatol Int (2011) 32(4):1003–7. doi: 10.1007/s00296-010-1792-8
34. Laivoranta-Nyman S, Möttönen T, Hermann R, Tuokko J, Luukkainen R, Hakala M, et al. HLA-DR-DQ haplotypes and genotypes in Finnish patients with rheumatoid arthritis. Ann Rheum Dis (2004) 63(11):1406–12. doi: 10.1136/ard.2003.009969
35. Stark K, Rovenský J, Blazicková S, Grosse-Wilde H, Ferencik S, Hengstenberg C, et al. Association of common polymorphisms in known susceptibility genes with rheumatoid arthritis in a Slovak population using osteoarthritis patients as controls. Arthritis Res Ther (2009) 11(3):R70. doi: 10.1186/ar2699
36. Muazzam AG, Mansoor A, Ali L, Siddiqi S, Hameed A, Ajmal M, et al. Association of HLA-DRB1 and -DQB1 alleles and haplotypes with rheumatoid arthritis in a Pakistani population. Arthritis Res Ther (2013) 15(4):R95. doi: 10.1186/ar4275
37. Al-Timimi DJ, Rasool MT, Sulaiman DM. HLA-DR/DQ genotypes in Kurd patients with rheumatoid arthritis: relation to disease activity. J Clin Diagn Res (2014) 8(5):CC01–4. doi: 10.7860/JCDR/2014/8112.4349
38. Klimenta B, Nefic H, Prodanovic N, Jadric R, Hukic F. Association of biomarkers of inflammation and HLA-DRB1 gene locus with risk of developing rheumatoid arthritis in females. Rheumatol Int (2019) 39(12):2147–57. doi: 10.1007/s00296-019-04429-y
39. Xue L, Tao L, Sun H, Wang Y, Zhang Y, Lei N, et al. Association between blood PLT and RBC related indices and disease activity in patients with rheumatoid arthritis. Int J Gen Med (2022) 15:573–81. doi: 10.2147/IJGM.S351505
40. Dechanuwong P, Phuan-Udom R. Hematological parameters as a predictor of disease remission in patients with rheumatoid arthritis. Ann Med Surg (Lond) (2021) 72:103085. doi: 10.1016/j.amsu.2021.103085
41. Klimenta B, Nefic H, Prodanovic N, Hukic F, Mesic A. Hematological parameters in patients with rheumatoid arthritis and gene variants HLA-DRB1*04 and HLA-DRB1*03. Genet Appl (2020) 4(1):1–8. doi: 10.31383/ga.vol4iss1pp30-37
42. Mykola V, Ganna S, Gennadiy T. Hematological abnormalities in Ukrainian patients with rheumatoid arthritis. J Arthritis (2015) 4(1):1000146. doi: 10.4172/2167-7921.1000146
43. Dayan İ, Tıkız C, Taneli F, Ulman C, Ulutaş G, Tüzün Ç. Relationship between cyclic citrullinated peptide antibodies positivity and HLADRB1 shared epitope alleles in patients with rheumatoid arthritis in Turkey. Turk J Rheumatol (2010) 25:12–8. doi: 10.5152/TJR.2010.02
44. Alrogy A, Dirar A, Alrogy W, Fakhoury H, Hajeer A. Association of human leukocyte antigen DRB1 with anti-cyclic citrullinated peptide autoantibodies in Saudi patients with rheumatoid arthritis. Ann Saudi Med (2017) 37(1):38–41. doi: 10.5144/0256-4947.2017.38
45. Atouf O, Benbouazza K, Brick C, Bzami F, Bennani N, Amine B, et al. HLA polymorphism and early rheumatoid arthritis in the Moroccan population. Joint Bone Spine (2008) 75(5):554–8. doi: 10.1016/j.jbspin.2008.01.027
46. Rubio-Tapia A, Abdulkarim AS, Wiesner RH, Moore SB, Krause PK, Murray JA. Celiac disease autoantibodies in severe autoimmune liver disease and the effect of liver transplantation. Liver Int (2008) 28(4):467–76. doi: 10.1111/j.1478-3231.2008.01681.x
Keywords: rheumatoid arthritis, HLA-DRB1, HLA-DQB1, anti-CCP, rheumatoid factor
Citation: Ali AA, Khalid KE, Mohammed SE, Akhtar MS and Saeed OK (2023) Association of Human Leukocyte Antigen (HLA) class II (DRB1 and DQB1) alleles and haplotypes with Rheumatoid Arthritis in Sudanese patients. Front. Immunol. 14:1178546. doi: 10.3389/fimmu.2023.1178546
Received: 02 March 2023; Accepted: 05 June 2023;
Published: 22 June 2023.
Edited by:
Bin Yang, University of Leicester, United KingdomReviewed by:
Luiza Guilherme, University of São Paulo, BrazilCopyright © 2023 Ali, Khalid, Mohammed, Akhtar and Saeed. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Khalid Eltahir Khalid, a2hhdGFoaXIxMkBnbWFpbC5jb20=; Mohammed Salman Akhtar, bWRzYWxtYW5ha2h0YXJAeWFob28uY29t; bWlseWFzQGJ1LmVkdS5zYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.