 Geraldo Magela Fernandes1*†
Geraldo Magela Fernandes1*† Lizandra Moura Paravidine Sasaki1,2†
Lizandra Moura Paravidine Sasaki1,2† Gabriela Profírio Jardim-Santos1
Gabriela Profírio Jardim-Santos1 Heidi Luise Schulte1
Heidi Luise Schulte1 Felipe Motta1Ângelo Pereira da Silva2Aleida Oliveira de Carvalho2Yacara Ribeiro Pereira2Caroline de Oliveira Alves3
Felipe Motta1Ângelo Pereira da Silva2Aleida Oliveira de Carvalho2Yacara Ribeiro Pereira2Caroline de Oliveira Alves3 David Alves de Araújo Júnior2Dayde Lane Mendonça-Silva2Karina Nascimento Costa3Maria Eduarda Canellas de Castro1,2Lucas Lauand3Rodrigo de Resende Nery3
David Alves de Araújo Júnior2Dayde Lane Mendonça-Silva2Karina Nascimento Costa3Maria Eduarda Canellas de Castro1,2Lucas Lauand3Rodrigo de Resende Nery3 Rosana Tristão3Patricia Shu Kurizky1,2
Rosana Tristão3Patricia Shu Kurizky1,2 Otávio de Toledo Nóbrega1Laila Salmen Espindola1
Otávio de Toledo Nóbrega1Laila Salmen Espindola1 Luiz Cláudio Gonçalves de Castro1,3Patrícia Nessralla Alpoim4Lara Carvalho Godoi4Luci Maria Sant Ana Dusse4
Luiz Cláudio Gonçalves de Castro1,3Patrícia Nessralla Alpoim4Lara Carvalho Godoi4Luci Maria Sant Ana Dusse4 Jordana Grazziela Alves Coelho-dos-Reis5Laurence Rodrigues do Amaral6Matheus de Souza Gomes6
Jordana Grazziela Alves Coelho-dos-Reis5Laurence Rodrigues do Amaral6Matheus de Souza Gomes6 Pedro Luiz Lima Bertarini6
Pedro Luiz Lima Bertarini6 Joaquim Pedro Brito-de-Sousa7
Joaquim Pedro Brito-de-Sousa7 Ismael Artur da Costa-Rocha7
Ismael Artur da Costa-Rocha7 Ana Carolina Campi-Azevedo7Vanessa Peruhype-Magalhães7Andrea Teixeira-Carvalho7Alberto Moreno Zaconeta3‡
Ana Carolina Campi-Azevedo7Vanessa Peruhype-Magalhães7Andrea Teixeira-Carvalho7Alberto Moreno Zaconeta3‡ Alexandre Anderson de Sousa Munhoz Soares1,3Valéria Valim8,9
Alexandre Anderson de Sousa Munhoz Soares1,3Valéria Valim8,9 Ciro Martins Gomes1,3,10Cleandro Pires de Albuquerque1,2
Ciro Martins Gomes1,3,10Cleandro Pires de Albuquerque1,2 Olindo Assis Martins-Filho7*‡
Olindo Assis Martins-Filho7*‡ Licia Maria Henrique da Mota1,2,10‡
Licia Maria Henrique da Mota1,2,10‡- 1Programa de Pós-Graduação em Ciências Médicas, Universidade de Brasília (UnB), Brasília, Brazil
- 2Hospital Universitário de Brasília, Universidade de Brasília (UnB), Brasília, Brazil
- 3Faculdade de Medicina, Universidade de Brasília (UnB), Brasília, Brazil
- 4Faculdade de Farmácia, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
- 5Laboratório de Virologia Básica e Aplicada, Instituto de Ciências Biológicas, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
- 6Laboratório de Bioinformática e Análises Moleculares, Universidade Federal de Uberlândia, Patos de Minas, Brazil
- 7Instituto René Rachou, Fundação Oswaldo Cruz (FIOCRUZ-Minas), Belo Horizonte, Brazil
- 8Hospital Universitário Cassiano Antônio Moraes, Universidade Federal do Espírito Santo (HUCAM-UFES), Vitória, Brazil
- 9Programa de Pós-Graduação em Saúde Coletiva (PPGSC), Centro de Ciências Médicas, Universidade Federal do Espírito Santo, Vitória, Brazil
- 10Programa de Pós-Graduação em Patologia Molecular, Universidade de Brasília (UnB), Brasília, Brazil
Introduction: SARS-CoV-2 infection during pregnancy can induce changes in the maternal immune response, with effects on pregnancy outcome and offspring. This is a cross-sectional observational study designed to characterize the immunological status of pregnant women with convalescent COVID-19 at distinct pregnancy trimesters. The study focused on providing a clear snapshot of the interplay among serum soluble mediators.
Methods: A sample of 141 pregnant women from all prenatal periods (1st, 2nd and 3rd trimesters) comprised patients with convalescent SARS-CoV-2 infection at 3-20 weeks after symptoms onset (COVID, n=89) and a control group of pre-pandemic non-infected pregnant women (HC, n=52). Chemokine, pro-inflammatory/regulatory cytokine and growth factor levels were quantified by a high-throughput microbeads array.
Results: In the HC group, most serum soluble mediators progressively decreased towards the 2nd and 3rd trimesters of pregnancy, while higher chemokine, cytokine and growth factor levels were observed in the COVID patient group. Serum soluble mediator signatures and heatmap analysis pointed out that the major increase observed in the COVID group related to pro-inflammatory cytokines (IL-6, TNF-α, IL-12, IFN-γ and IL-17). A larger set of biomarkers displayed an increased COVID/HC ratio towards the 2nd (3x increase) and the 3rd (3x to 15x increase) trimesters. Integrative network analysis demonstrated that HC pregnancy evolves with decreasing connectivity between pairs of serum soluble mediators towards the 3rd trimester. Although the COVID group exhibited a similar profile, the number of connections was remarkably lower throughout the pregnancy. Meanwhile, IL-1Ra, IL-10 and GM-CSF presented a preserved number of correlations (≥5 strong correlations in HC and COVID), IL-17, FGF-basic and VEGF lost connectivity throughout the pregnancy. IL-6 and CXCL8 were included in a set of acquired attributes, named COVID-selective (≥5 strong correlations in COVID and <5 in HC) observed at the 3rd pregnancy trimester.
Discussion and conclusion: From an overall perspective, a pronounced increase in serum levels of soluble mediators with decreased network interplay between them demonstrated an imbalanced immune response in convalescent COVID-19 infection during pregnancy that may contribute to the management of, or indeed recovery from, late complications in the post-symptomatic phase of the SARS-CoV-2 infection in pregnant women.
1 Introduction
In March 2020, the World Health Organization (WHO) characterized the outbreak of the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) disease (COVID-19) as a pandemic, having since confirmed more than 655 million COVID-19 cases, 6.6 million of which resulted in death (1). SARS-CoV-2 is transmitted through airborne droplets, respiratory secretions, and direct contact. The clinical symptoms relating to the COVID-19 disease were primarily respiratory, and later reported as multisystemic effects. COVID-19 illness symptoms can be asymptomatic, mild, moderate, severe, or critical (2–4). Fever, cough, dyspnea, and myalgia were the most common mild symptoms. The pathogenesis of COVID-19 has been strongly associated with an unbalanced immune response; however, the pathophysiology of the disease remains under investigation (5–7).
Multiple studies concluded that pregnant women are a high-risk population for the COVID-19 disease. Infectious diseases in pregnancy are regularly considered a critical condition. Physiological changes during pregnancy have significant effects on the immune system, cardiopulmonary system and coagulation, and these changes may result in an altered response to COVID-19 infection (3, 8–11). Cytokine levels during pregnancy could be responsible for metabolic imprinting as cytokines are transferable from maternal to fetal circulation and are capable of modulating placental nutrient transfer. Maternal inflammation may induce metabolic reprogramming at several levels, from the periconceptional period onwards. Such processes and their consequences on the maternal and perinatal periods have not been extensively studied to date. Moreover, the maternal immune activation triggered by COVID-19 can have impacts for the mother, pregnancy outcome and offspring (12, 13). The understanding such phenomena should contribute to the proper management of children born to SARS-CoV-2-infected mothers (14).
The aim of the present study was to conduct a prospective observational study designed to characterize the immunological status of pregnant women with convalescent COVID-19, focusing on an overall snapshot of the interplay between serum soluble mediators.
2 Materials and methods
2.1 Study population
This cross-sectional observational study was conducted between July 2020 and December 2021 during the COVID-19 pandemic in the Federal District of Brazil during circulation of the SARS-CoV-2 B.1.1.28 and B.1.1.33 strains. A total of 141 participants were enrolled as non-probability convenience sampling, including pregnant women with convalescent SARS-CoV-2 infection (COVID, n=89) at 3-20 weeks after symptoms onset during the prenatal period (1st, 2nd and 3rd trimesters), together with a healthy control group composed of age-matched pre-pandemic non-infected pregnant women (HC, n=52).
The COVID-19 pregnant women were recruited at two public hospitals - the University Hospital of Brasília and the Asa Norte Regional Hospital, both public reference centers for COVID-19 in the Federal District of Brazil and participants of a large research project named PROUDEST (15). The COVID group comprised pregnant women aged 18-44 years, with a median age of 31 years. This group was further categorized into subgroups according to the pregnancy trimester, referred to as: 1st (n=7), 2nd (n=34) and 3rd (n=48). COVID-19 diagnosis was confirmed by a documented positive RT-PCR test using a nasopharyngeal swab or rapid test (Biomanguinhos, FIOCRUZ, Brazil) for IgM or IgG, during pregnancy. Most of the COVID-19 group (97%, 86 out of 89) presented the non-severe form of the disease. The most common symptoms were: Anosmia (68%), runny nose and/or nasal congestion (68%), headache (67%), ageusia (63%), myalgia (57%), cough (43%), fever (43%), dyspnea (31%), sore throat (31%), asthenia (22%), diarrhea (17%), nausea and vomiting (11%), joint pain (5%), dizziness (4%) and skin diseases (2%). SARS-CoV-2 infection during pregnancy was associated with important adverse maternal and neonatal outcomes, including gestational diabetes mellitus (37%), Apgar score at first minute ≤ 7 (22%), systemic arterial hypertension (18%), fetal restriction growth (11%), preterm labor (11%), acute fetal distress (8%), Apgar score at fifth minute ≤ 7 (5%) and preeclampsia (3%).
The HC group comprised a selected non-probability convenience sampling from a biorepository maintained at Grupo Integrado de Pesquisas em Biomarcadores, Instituto René Rachou, Fundação Oswaldo Cruz (FIOCRUZ-Minas), Belo Horizonte, Brazil. The HC group comprised pregnant women, aged 18- 42 years, with a median age of 28 years. The healthy control group was composed by primiparous with no previous history or current status of obesity, systemic arterial hypertension, diabetes mellitus and without records of pre-eclampsia. The HC group was further categorized into subgroups according to pregnancy trimester, referred to as: 1st (n=21), 2nd (n=10) and 3rd (n=21).
The Table 1 summarize the major demographic and clinical features of the study population.
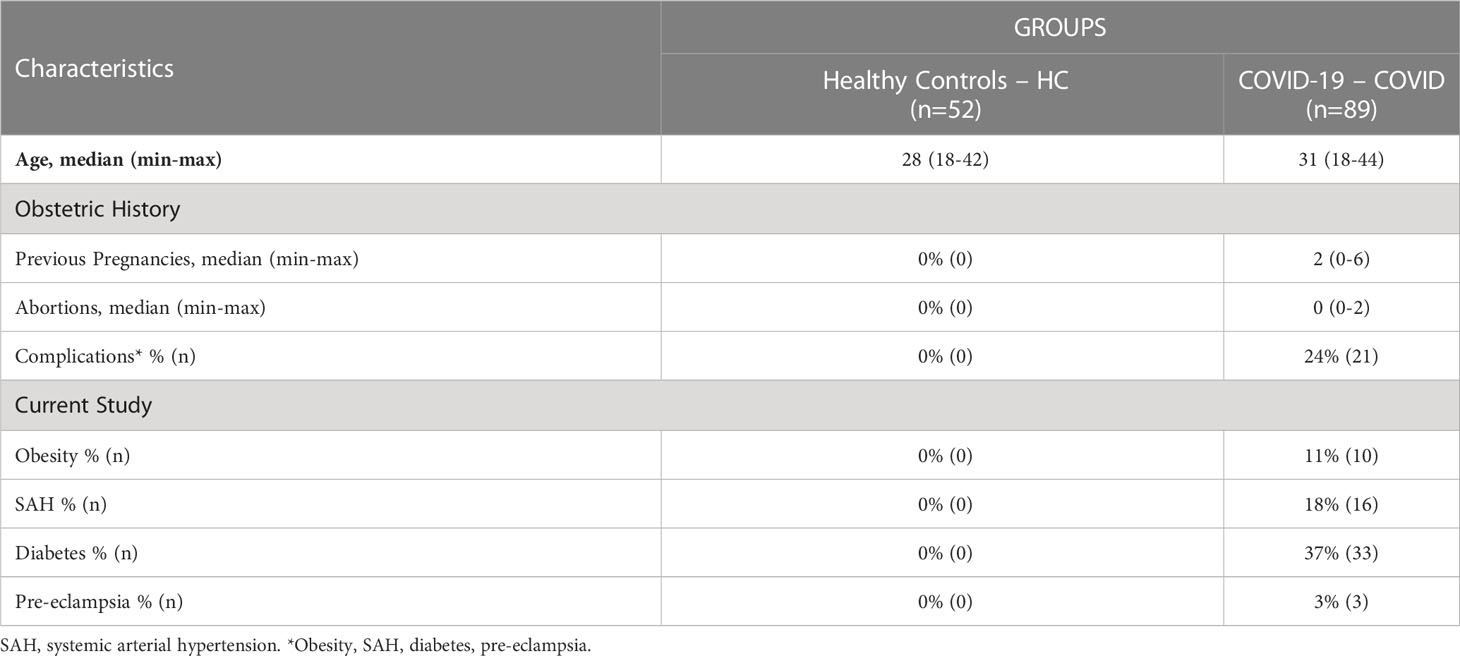
Table 1 Demographic and clinical features of the study population.
All study participants provided written informed consent prior to inclusion in accordance with the Helsinki Declaration and Resolution 466/2012 from the Brazilian National Health Council for research involving human subjects. This study was recorded on the Brazilian Registry of Clinical Trials Platform (ReBEC, RBR-65qxs2) and approved by the National Commission for Ethics in Research in Brazil (CONEP, CAAE 32359620.0.0000.5558). The anonymization strategy to protect the identity of participants was achieved by replacing the direct identifiers by standardized alphanumeric codes (PRAxxxPNy and PRBxxxPNy), where “PR” refer to the PROUDEST project name (15), “A” and “B” refers to the hospital unit, the “xxx” represent the sequential number of patient inclusion, “PN” refer to prenatal period and “y” the trimester of sample collection.
2.2 Biological samples
Whole blood sample (10 mL) were collected from each participant in vacuum tubes without anticoagulant by venipuncture at the first prenatal appointment or upon enrolment in the study. Serum samples were obtained by centrifugation (1400 x g, 10 min, 4°C) of original samples within 6 h after blood collection. The serum specimens were aliquoted and stored at -80°C until quantification of serum soluble mediators.
2.3 Quantification of serum soluble mediators
Serum soluble mediators were quantified by a high-throughput Luminex microbead multiplex assay (Bio-Plex Pro™ Human Cytokine 27-plex Assay, Bio-Rad Laboratories, Hercules, CA, USA). The manufacturer’s instructions were followed to determine the concentrations of chemokines (CXCL8; CCL11; CCL3; CCL4; CCL2; CCL5; CXCL10), pro-inflammatory cytokines (IL-1β; IL-6; TNF-α; IL-12; IFN-γ; IL-15; IL-17), regulatory cytokines (IL-1Ra; IL-4; IL-5; IL-9; IL-10; IL-13) and growth factors (FGF-basic; VEGF; PDGF; G-CSF; GM-CSF; IL-2; IL-7). The assays were conducted in parallel batches by a trained technician at the flow cytometry facility at FIOCRUZ-Minas. The concentrations of serum soluble mediators (pg/mL) were obtained according to a 5-parameter logistic curve fit regression of standard curves.
2.4 Statistical analysis
Descriptive statistics were carried out using the Prism 8.0.2 software (GraphPad Software, San Diego, USA). Data normality was assessed using the Shapiro-Wilk test. Considering the nonparametric distribution of all data sets, multiple comparisons amongst HC and COVID subgroups were carried out using the Kruskal-Wallis followed by Dunn’s post-test. Additionally, comparative analysis between HC and COVID at matching trimesters was performed using the Mann-Whitney test. In all cases, statistical significance was considered at p<0.05.
The serum soluble mediator signatures were calculated as the proportion (%) of pregnant women with serum levels above the reference values (cut-off) defined as the median Z-score of each soluble mediator detected for all HC along the 1st, 2nd and 3rd trimesters (CXCL8=-0.3; CCL11=-0.3; CCL3=-0.3; CCL4=-0.3; CCL2=-0.4; CCL5=-0.2; CXCL10=-0.2; IL-1β=-0.3; IL-6=-0.3; TNF-α=-0.3; IL-12=-0.3; IFN-γ=-0.4; IL-15=-0.5; IL-17=-0.4; IL-1Ra=-0.4; IL-4=-0.3; IL-5=-0.2; IL-9=-0.2; IL-10=-0.2; IL-13=-0.4; FGF-basic=-0.5; PDGF=-0.4; VEGF=-0.4; G-CSF=-0.2; GM-CSF=-0.4; IL-2=-0.4; IL-7=-0.3). Additionally, trimester-matching signatures were assembled, considering the reference values (cut-off) defined as the median Z-score of each soluble mediator detected for HC trimester subgroups at 1st (CXCL8 = 0.2; CCL11 = 0.1; CCL3 = 0; CCL4=-0.6; CCL2 = 0.4; CCL5=-0.2; CXCL10=-0.7; IL-1β=-0.2; IL-6 = 1.6; TNF-α=-0.1; IL-12=-0.2; IFN-γ=0.1; IL-15=-0.5; IL-17 = 0.1; IL-1Ra=0.1; IL-4=-0.5; IL-5=-0.1; IL-9 = 0.5; IL-10=-0.2; IL-13 = 0.2; FGF-basic=0.3; PDGF=0.2; VEGF=0.1; G-CSF=-0.2; GM-CSF=0.1; IL-2=-0.4; IL-7=-0.2), 2nd (CXCL8=-0.3; CCL11=-0.2; CCL3=-0.3; CCL4=-0.2; CCL2=-0.5; CCL5=-0.1; CXCL10=-0.6; IL-1β=-0.3; IL-6=-0.4; TNF-α=-0.3; IL-12=-0.3; IFN-γ=-0.4; IL-15 = 0.2; IL-17=-0.2; IL-1Ra=-0.5; IL-4 = 0.2; IL-5=-0.2; IL-9=-0.6; IL-10=-0.2; IL-13=-0.4; FGF-basic=-0.6; PDGF=-0.6; VEGF=-0.2; G-CSF=-0.1; GM-CSF=-0.6; IL-2=-0.1; IL-7=-0.2) and 3rd trimesters (CXCL8=-0.4; CCL11=-0.4; CCL3=-0.3; CCL4 = 0.3; CCL2=-0.5; CCL5 = 0.1; CXCL10 = 0.6; IL-1β=-0.4; IL-6=-0.3; TNF-α=-0.3; IL-12=-0.3; IFN-γ=-0.4; IL-15=-0.5; IL-17=-0.4; IL-1Ra=-0.6; IL-4=-0.3; IL-5=-0.2; IL-9=-0.8; IL-10=-0.3; IL-13=-0.4; FGF-basic=-0.6; PDGF=-0.7; VEGF=-0.4; G-CSF=-0.2; GM-CSF=-0.7; IL-2=-0.5; IL-7=-0.3). The serum soluble mediators displaying a proportion above 50% in pregnant women were included in the set of biomarkers with increased levels.
Heatmap constructs were assembled using conditional formatting in Microsoft Excel to illustrate the overall profile of serum soluble mediator signatures of the COVID and HC subgroups along the pregnancy trimesters. The ratio between the proportion of pregnant women with serum levels above the reference values in the COVID group in relation to HC (%COVID/%HC) was also assessed by comparative analysis.
Serum-soluble mediator networks were built based on correlation analysis (Pearson and Spearman rank tests) between pairs of serum-soluble mediators. Only significant strong correlations (p<0.05 and “r” scores ≥ |0.67|) were employed to construct the comprehensive networks. The open-source Cytoscape software (available at https://cytoscape.org) was used to create cluster network layouts comprising the 4 categories of serum soluble mediators - chemokines, pro-inflammatory cytokines, regulatory cytokines, and growth factors. Descriptive analysis of serum soluble mediator networks was performed by considering the ascendant number of strong correlations to identify the set of biomarkers with five or more strong correlations (≥ 5). Venn Diagram analysis (available at (http://bioinformatics.psb.ugent.be/webtools/Venn/) was performed to assess the preserved (common), lost or acquired (selective) serum soluble mediators with ≥ 5 strong correlations in COVID subgroups compared to trimester-matching HC.
The MATLAB software was employed for Principal Component Analysis (PCA). The PCA data was assembled to verify the ability of serum soluble mediators to cluster convalescent COVID-19 pregnant women from HC, as well as subgroups of COVID-19 as compared to trimester-matching HC. The PCA analysis enabled data dimensionality reduction.
3 Results
3.1 Levels of serum soluble mediators in convalescent COVID-19 at distinct pregnancy trimesters
The levels of chemokines, pro-inflammatory cytokines, regulatory cytokines and growth factors were measured in serum samples from pregnant women with convalescent COVID-19 at 3-20 weeks after symptoms onset (COVID) and compared with those detected in trimester-matching pre-pandemic non-infected pregnant women as a healthy control (HC). The results are presented in Figures 1 and 2.
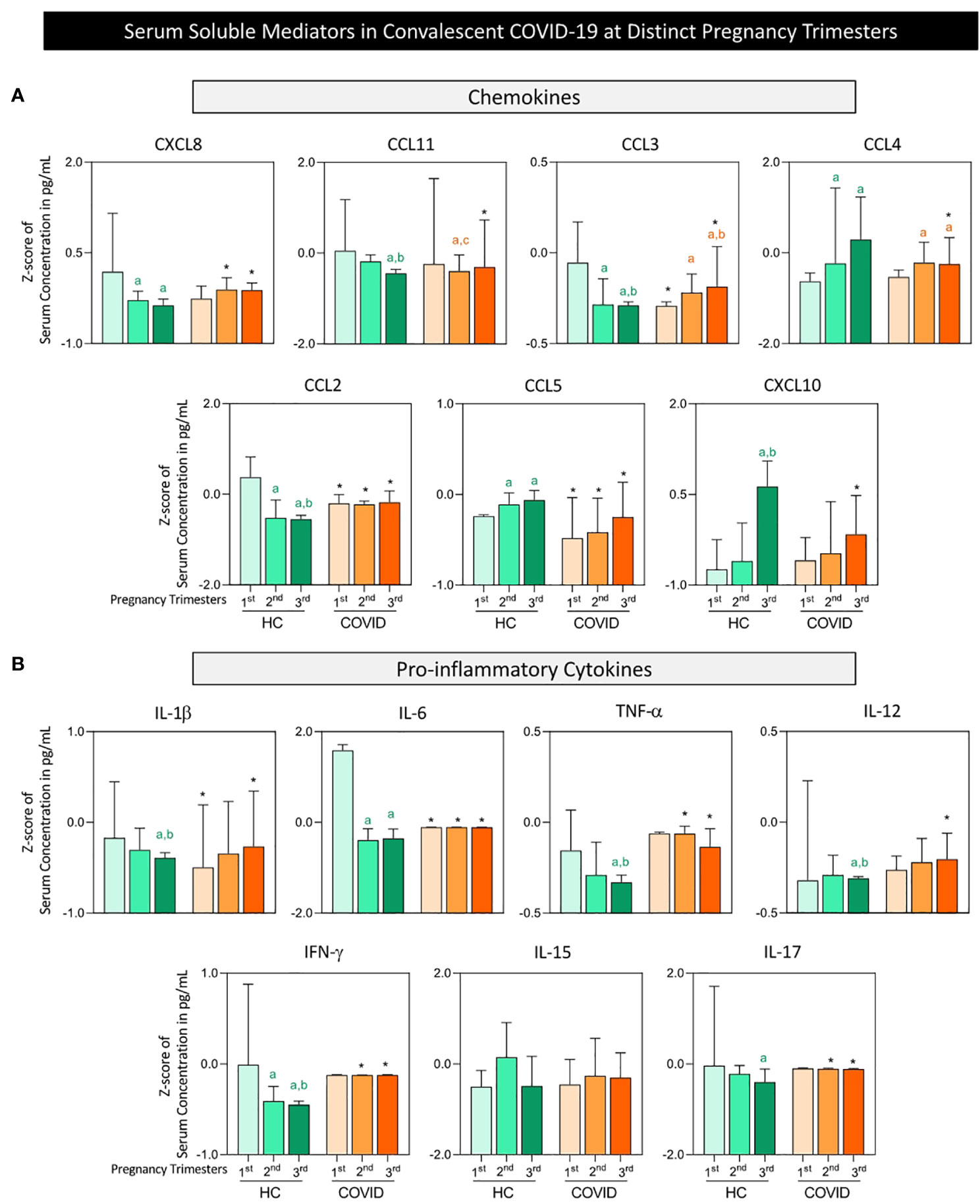
Figure 1 Serum and pro-inflammatory cytokines in convalescent COVID-19 patients at distinct pregnancy trimesters. The levels of: (A) chemokines (CXCL8, CCL11, CCL3, CCL4, CCL2, CCL5, CXCL10), and (B) pro-inflammatory cytokines (IL-1β, IL-6, TNF-α, IL-12, IFN-γ, IL-15, IL -17) were measured in serum samples from pregnant women with convalescent COVID-19 at 3-20 weeks after symptoms onset (COVID, n=89), with pre-pandemic non-infected pregnant women as a Healthy Control (HC, n=52). The HC and COVID-19 groups were further categorized into subgroups according to pregnancy trimester, referred to as: HC 1st ( , n=21), HC 2nd (
, n=21), HC 2nd ( , n=10), HC 3rd (
, n=10), HC 3rd ( , n=21), and COVID 1st (
, n=21), and COVID 1st ( , n=7), COVID 2nd (
, n=7), COVID 2nd ( , n=34), COVID 3rd (
, n=34), COVID 3rd ( , n=48). The measurements were taken by high-throughput multiplex bead array as described in Material and Methods. The results are presented in bar charts of median values and interquartile ranges for Z-score of serum concentration (pg/mL). Multiple comparative analysis was performed by Kruskal-Wallis followed by Dunn’s post-test and comparisons between COVID-19 and HC at matching pregnancy trimesters assessed using the Mann-Whitney test. In all cases, significance was considered at p<0.05. Intragroup differences were underscored by the letters “a”, “b” and “c” for comparisons with the 1st, 2nd and 3rd trimesters, respectively. Inter-group differences at matching pregnancy trimesters were highlighted denoted by an asterisk (*).
, n=48). The measurements were taken by high-throughput multiplex bead array as described in Material and Methods. The results are presented in bar charts of median values and interquartile ranges for Z-score of serum concentration (pg/mL). Multiple comparative analysis was performed by Kruskal-Wallis followed by Dunn’s post-test and comparisons between COVID-19 and HC at matching pregnancy trimesters assessed using the Mann-Whitney test. In all cases, significance was considered at p<0.05. Intragroup differences were underscored by the letters “a”, “b” and “c” for comparisons with the 1st, 2nd and 3rd trimesters, respectively. Inter-group differences at matching pregnancy trimesters were highlighted denoted by an asterisk (*).
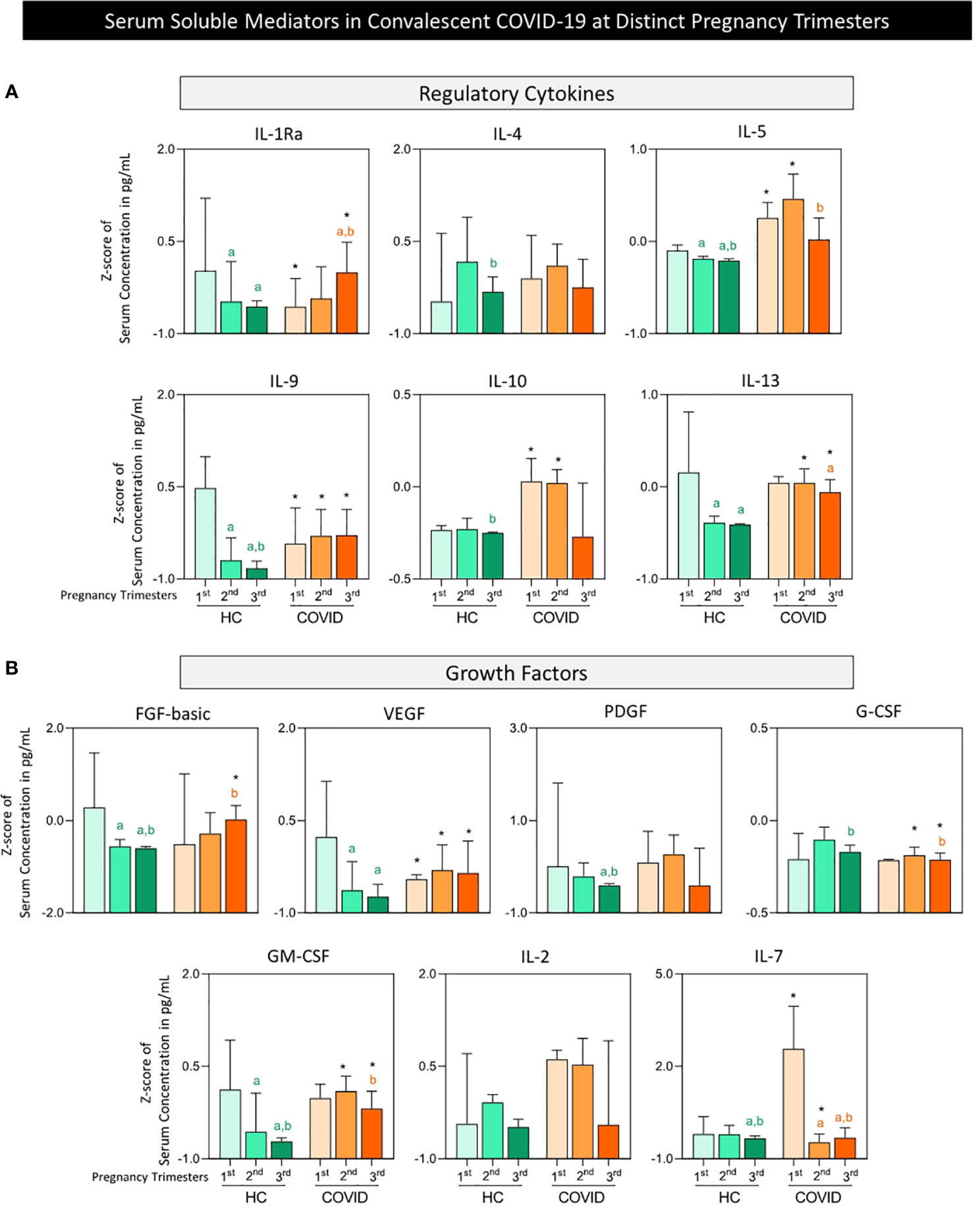
Figure 2 Serum regulatory cytokines and growth factors in convalescent COVID-19 patients at distinct pregnancy trimesters. The levels of: (A) regulatory cytokines (IL-1Ra, IL- 4, IL-5, IL-9, IL-10, IL-13), and (B) growth factors (FGF-basic, PDGF, VEGF, G-CSF, GM- CSF, IL-2, IL-7) were measured in serum samples from pregnant women with convalescent COVID-19 at 3-20 weeks after symptoms onset (COVID, n=89), with pre-pandemic non-infected pregnant women as a Healthy Control (HC, n=52). The HC and COVID-19 groups were further categorized into subgroups according to pregnancy trimester, referred to as: HC 1st (, n=21), HC 2nd (, n=10), HC 3rd (, n=21), and COVID 1st (, n=7), COVID 2nd (, n=34), COVID 3rd (, n=48). The measurements were taken by high-throughput multiplex bead array as described in Material and Methods. The results are presented in bar charts of median values and interquartile ranges for Z-score of serum concentration (pg/mL). Multiple comparative analysis was performed by Kruskal-Wallis followed by Dunn’s post-test, and comparisons between COVID-19 and HC at matching pregnancy trimesters assessed by the Mann-Whitney test. In all cases, significance was considered at p<0.05. Intragroup differences were underscored by the letters “a” and “b” for comparisons with the 1st and 2nd trimesters, respectively. Inter-group differences at matching pregnancy trimesters were denoted by an asterisk (*).
In general, healthy pregnant women presented a progressive decrease in most serum soluble mediators towards the 2nd and 3rd pregnancy trimester, including: chemokines (CXCL8, CCL11, CCL3 and CCL2); pro-inflammatory cytokines (IL-1β, IL-6, TNF-α, IL-12, IFN-γ, and IL-17); regulatory cytokines (IL-1Ra, IL-4, IL-5, IL-9, IL-10 and IL-13), and growth factors (FGF-basic, VEGF, PDGF, GM-CSF and IL-7). Conversely, progressive increases in CCL4, CCL5, CXCL10 and G-CSF were observed in the HC group. No difference was observed in the HC group for IL-15 and IL-2 (Figures 1, 2).
Overall, higher levels of the most soluble mediators were observed in convalescent COVID-19 pregnant women compared to the healthy controls, especially at the 2nd and 3rd trimesters, including higher levels of CXCL8; CCL11; CCL2; CCL3; IL-1β; IL-6; TNF-α; IL-12; IFN-γ; IL-17; IL-1Ra; IL-5; IL-9; IL-10; IL-13; FGF-basic; VEGF, and GM-CSF. Conversely, lower levels of CCL4, CCL5, CXCL10, G-CSF and IL-7 were observed towards the 2nd and 3rd trimesters in the COVID group compared to the HC group (Figures 1, 2).
Additional analysis amongst the COVID subgroups along the pregnancy trimesters demonstrated an inverted profile of CCL3, IL-1Ra and FGF-basic towards higher levels in the 3rd trimester (Figures 1, 2).
Supplementary Figure 1 summarizes the major changes observed in serum soluble mediators along the trimesters of healthy and convalescent COVID-19 pregnancy.
3.2 Serum soluble mediator signatures in convalescent COVID-19 at distinct pregnancy trimesters
Serum soluble mediator signatures were assembled as the percentage of pregnant women with serum levels above the reference values defined as the median Z-score of each soluble mediator detected in all healthy controls along the pregnancy. The results are presented in Figure 3.
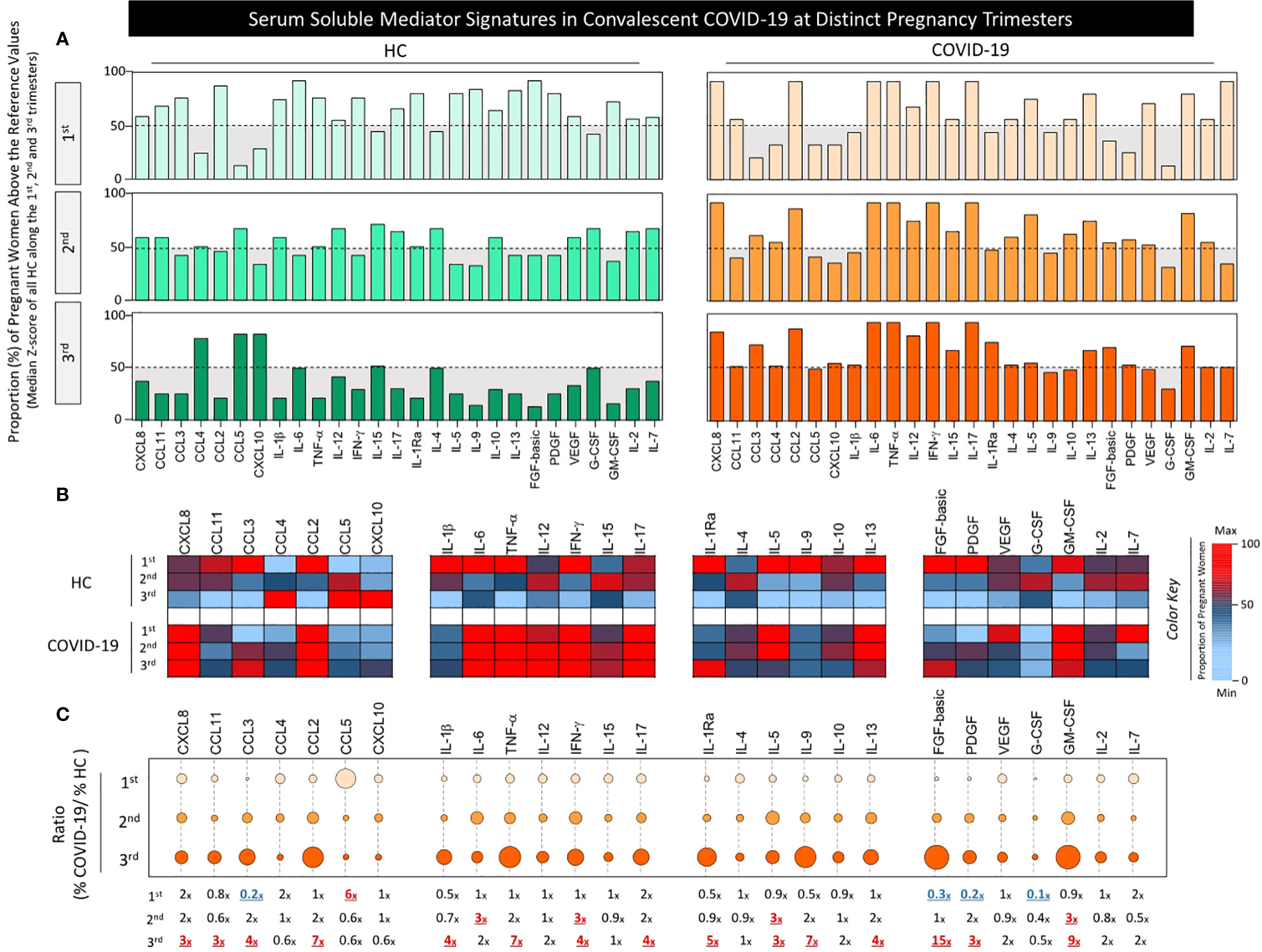
Figure 3 Serum soluble mediator signatures in convalescent COVID-19 patients at distinct pregnancy trimesters. Signatures of: serum chemokines (CXCL8, CCL11, CCL3, CCL4, CCL2, CCL5, and CXCL10), pro-inflammatory cytokines (IL-1β, IL-6, TNF-α, IL-12, IFN-γ, IL-15, and IL-17), regulatory cytokines (IL-1Ra, IL-4, IL-5, IL-9, IL-10, and IL-13), and growth factors (FGF-basic, PDGF, VEGF, G-CSF, GM-CSF, IL-2, and IL-7) were assembled for pregnant women with convalescent COVID-19 at 3-20 weeks after symptoms onset (COVID, n=89) and for pre-pandemic non-infected pregnant women as a Healthy Control (HC, n=52). The HC and COVID-19 groups were further categorized into subgroups according to pregnancy trimester, referred to as: HC 1st (, n=21), HC 2nd (, n=10), HC 3rd (, n=21) and COVID 1st (, n=7), COVID 2nd (, n=34), COVID 3rd (, n=48). The measurements were taken by high-throughput multiplex bead array as described in Material and Methods. (A) The results are presented in bar charts showing the proportion (%) of pregnant women with serum levels above the reference values (cut-off) defined as the median Z-score of each soluble mediator detected for all HC along the 1st, 2nd and 3rd trimesters, as described in Material and Methods. The serum soluble mediators displaying a proportion of pregnant women above 50% (grey zone, dashed line) were included in the set of biomarkers with increased levels. (B) Heatmap constructs were further assembled to illustrate the overall profile of serum soluble mediator signatures of COVID and HC subgroups along the pregnancy trimesters. A color key was used to underscore the serum soluble mediators with decreased (proportion <50%, towards light blue), unaltered (proportion =50%, black) or increased levels (proportion>50%, towards red). (C) The ratio between the proportion of pregnant women with serum levels above the reference values in the COVID group in relation to HC (%COVID/%HC) was further calculated and presented in orbital graphs. The ratios of each serum soluble mediator along the 1st, 2nd and 3rd trimesters are provided in the figure, underscored as decreased (≤0.3x, blue), unaltered (0.4-2x, black) or increased (≥3x, red).
Data analysis demonstrated that the proportion of healthy pregnant women with high levels of serum soluble mediators progressively decreased towards the 2nd and 3rd pregnancy trimesters. These data further corroborated that a healthy pregnancy course has a progressive decrease in most serum soluble mediators towards the 2nd and 3rd trimesters, except for CCL4, CCL5 and CXCL10 (Figure 3A).
On the other hand, the proportion of pregnant women with convalescent COVID-19 presenting high serum soluble mediator levels progressively increased from the 1st to the 3rd pregnancy trimester (Figure 3A). Heatmap constructs further illustrated that the major increase in serum soluble mediators observed in pregnant women with convalescent COVID-19 occurred in pro-inflammatory cytokines, namely IL-6, TNF-α, IL-12, IFN-γ and IL-17 (Figure 3B).
The profile of serum soluble mediators was further characterized as the ratio (%COVID/%HC), assessed by dividing the percentage of pregnant women with soluble mediator levels above the reference values observed in the COVID group by the percentage of trimester-matching HC patients. Using this strategy, the results confirmed that a larger set of biomarkers presented a high ratio (%COVID/%HC) towards the 2nd and 3rd trimester. In the 2nd pregnancy trimester, increased ratios were observed for IL-6, IFN-γ, IL-5 and GM-CSF (3x increase) in the COVID-19 group. A larger set of serum soluble mediators with increased ratios was identified for COVID-19 groups at the 3rd pregnancy trimester, including CXCL8, CCL11, IL-5 and PDGF (3x increase), CCL3, IL-1β, IFN-γ, IL-17 and IL-13 (4x increase), CCL2, TNF-α (7x) along with IL-1Ra, IL-9, GM-CSF and FGF-basic (5x, 9x, 9x, and 15x increase, respectively) (Figure 3C).
The signatures of serum soluble mediators were also assessed considering the reference values of trimester-matching healthy controls. The results are presented in the Supplementary Figure 2. Data reinforce that larger sets of serum soluble mediators with increased ratios were identified for the 2nd and 3rd pregnancy trimesters as compared with trimester-matching controls (Supplementary Figure 2).
3.3 Serum soluble mediator networks in convalescent COVID-19 at distinct pregnancy trimesers
Aimed at assessing a panoramic snapshot of serum soluble mediator interplay in pregnant women with convalescent COVID-19 and healthy controls, integrative networks were constructed based on the overall correlation between pairs of molecules. The results are presented in Figure 4.
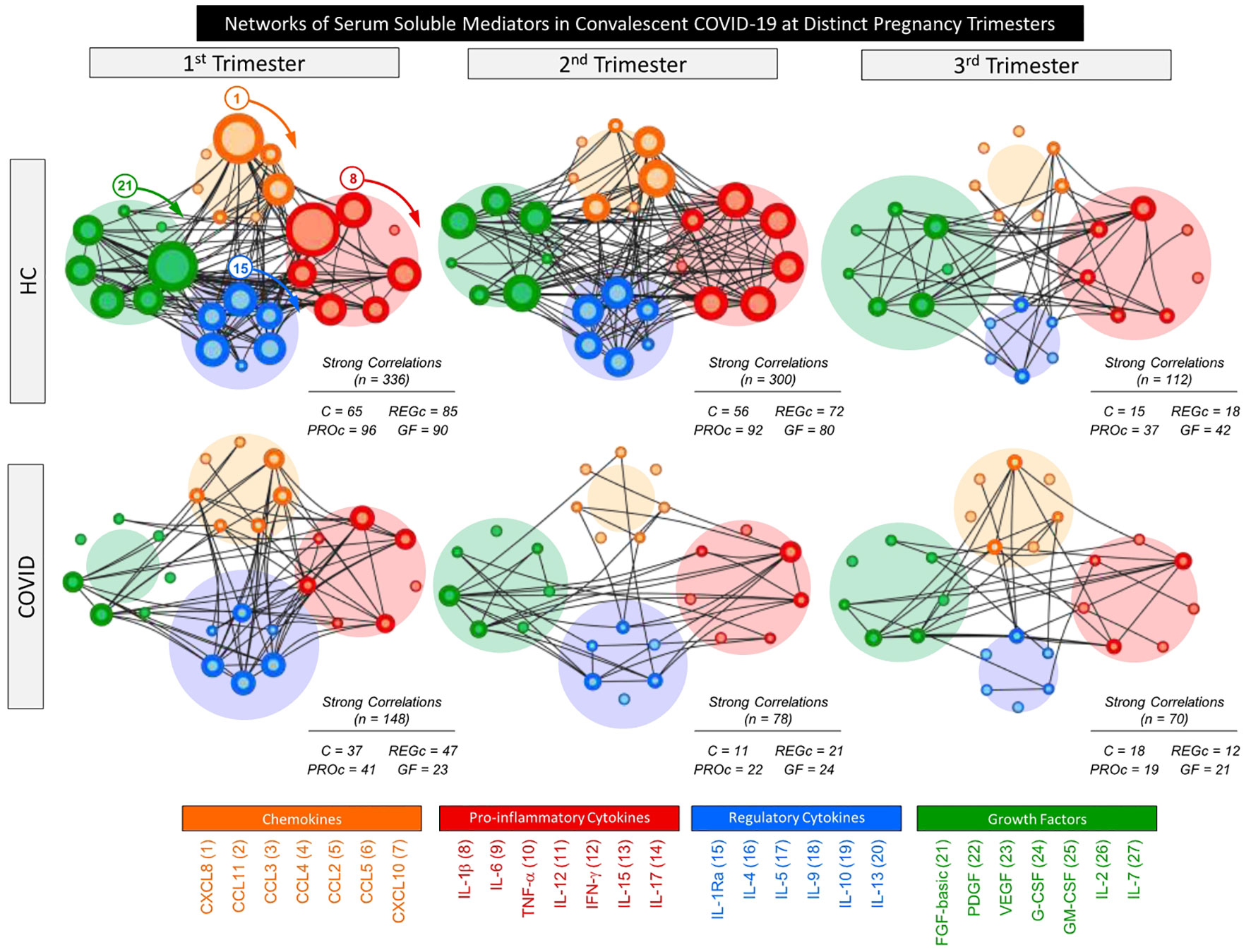
Figure 4 Networks of serum soluble mediators in convalescent COVID-19 patients at distinct pregnancy trimesters. Comprehensive networks were assembled for serum chemokines, pro-inflammatory cytokines, regulatory cytokines, and growth factors observed in pregnant women with convalescent COVID-19 at 3-20 weeks after symptoms onset (COVID, n=89), with pre-pandemic non-infected pregnant women as a Healthy Control (HC, n=52). The HC and COVID-19 groups were further categorized into subgroups according to pregnancy trimester, referred to as: 1st (HC=21 and COVID=7), 2nd (HC=18 and COVID=34) and 3rd (HC=21 and COVID=48). The measurements were taken by high-throughput multiplex bead array as described in Material and Methods. Data analyses were carried out by Pearson and Spearman rank tests with only significant strong correlations (p<0.05 and “r” scores ≥ |0.67|) employed to construct the comprehensive networks. Cluster layout networks were assembled, comprising 4 categories of serum soluble mediators as follows: - Chemokines – C (orange nodes – 1=CXCL8; 2=CCL11; 3=CCL3; 4=CCL4; 5=CCL2, 6=CCL5 and 7=CXCL10); Pro-inflammatory – PROc (red nodes – 8= IL-1β; 9=IL-6; 10= TNF-α; 11=IL-12; 12= IFN-γ; 13=IL-15 and 14=IL-17); Regulatory cytokines – REGc (blue nodes – 15=IL-1Ra; 16=IL-4; 17=IL-5; 18=IL-9; 19=IL-10 and 20=IL-13), and Growth Factors – GF (green nodes – 21=FGF-basic; 22=PDGF; 23=VEGF; 24=GCSF; 25=GM-CSF; 26=IL-2 and 27=IL-7). Node border thickness is proportional to the number of strong correlations. Connecting edges (black lines) are used to link pairs of serum soluble mediators presenting significant correlations. The number of strong correlations (C, PROc, REGc and GF) observed for each network is provided in the figure and used for comparative analysis between COVID and HC, as well as amongst subgroups. The circular background area is proportional to the number of strong correlations of each cluster within the respective network.
Data analysis demonstrated that healthy pregnancy evolves towards the 3rd trimester with an overall decrease in network connectivity (1st = 336; 2nd = 300 and 3rd = 112 strong correlations). Although pregnant women with convalescent COVID-19 exhibited a similar continuous decrease in network connectivity towards the 3rd trimester (1st = 146; 2nd = 78 and 3rd = 70 strong correlations), the number of connections was remarkably lower in the COVID group compared to HC group (Figure 4).
Overall, the analysis of cluster connectivity during healthy pregnancy showed that pro-inflammatory cytokines presented more connections at the 1st and 2nd trimesters (96 and 92 strong correlations, respectively), with growth factor predominance at the 3rd trimester (42 strong correlations). Conversely, the COVID group displayed a predominance of regulatory cytokines in the 1st trimester (47 strong correlations) with growth factor predominance in the 2nd and 3rd trimesters (24 and 21, respectively) (Figure 4).
In general, convalescent COVID-19 infection during pregnancy leads to a loss of network connectivity, with fewer strong correlations and changes in the predominance of connectivity amongst the categories of serum soluble mediators (Figure 4).
3.4 Descriptive analysis of serum soluble mediator networks in convalescent COVID-19 patients at distinct pregnancy trimesters
In order to provide a more comprehensive overview of the network connectivity between serum soluble mediators in pregnant women with convalescent COVID-19 and healthy controls along the pregnancy trimesters, a descriptive Venn diagram analysis was performed to identify the set of biomarkers with preserved (common), lost or acquired (selective) attributes with five or more (≥ 5) strong correlations in COVID subgroups as compared to the trimester-matching HC group. The results are presented in the Figure 5.
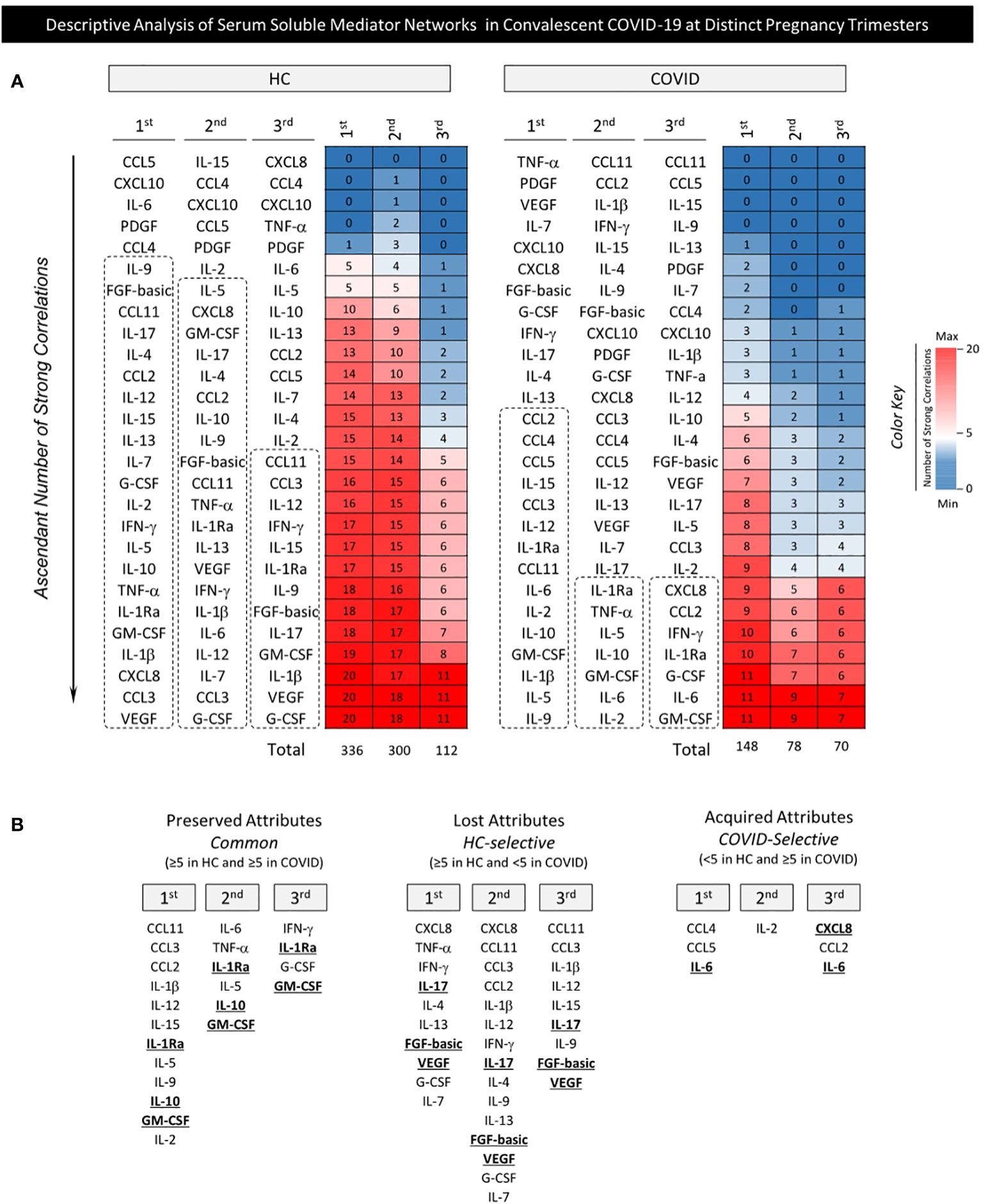
Figure 5 Descriptive analysis of serum soluble mediator networks in convalescent COVID-19 patients at distinct pregnancy trimesters. The overall profile of serum soluble mediator networks was assessed in pregnant women with convalescent COVID-19 at 3-20 weeks after symptoms onset (COVID, n=89) with pre-pandemic non-infected pregnant women as a Healthy Control (HC, n=52). The HC and COVID-19 groups were further categorized into subgroups according to pregnancy trimester, referred to as: 1st (HC=21 and COVID=7), 2nd (HC=10 and COVID=34), and 3rd (HC=21 and COVID=48). (A) The ascendant number of strong correlations was arranged to identify the set of biomarkers with five or more (≥ 5) strong correlations with other molecules at each pregnancy trimester in HC and COVID subgroups. Heatmap constructs were assembled to illustrate the overall profile of serum soluble mediator networks of COVID and HC subgroups along the pregnancy trimesters. A color key was used to underscore the serum soluble mediators with ≥ 5 strong correlations (towards red). (B) A summary of preserved (≥5 in HC and ≥5 in COVID), lost (≥5 in HC and <5 in COVID) or acquired (<5 in HC and ≥5 in COVID) attributes were identified by Venn diagram analysis. Attributes identified along the trimesters are highlighted by bold underline format.
Heatmap constructs were assembled to organize the serum soluble mediators with an ascending order of strong correlations and identify the set of biomarkers with five or more (≥ 5) strong correlations at each pregnancy trimester in the COVID and HC groups (Figure 5A).
Data analysis demonstrated that the number of preserved attributes referred to as common in HC and COVID (≥5 strong correlations in HC and COVID) with five or more correlations progressively decreased from the 1st (n=12) to the 2nd (n=6) and 3rd trimesters (n=4). In detail: 1st: CCL11, CCL3, CCL2, IL-1β, IL-12, IL-15, IL-1Ra, IL-5, IL-9, IL-10, GM-CSF, and IL-2; 2nd: IL-6, TNF-α, IL-1Ra, IL-5, IL-10, GM-CSF and 3rd:IFN-γ, IL-1Ra, G-CSF, and GM-CSF.
The number of lost attributes referred to as HC-selective (≥5 strong correlations in HC and <5 strong correlations in COVID) was higher in the 2nd trimester (n=15) compared to 1st (n=10) and 3rd (n=9). In detail: 1st: CXCL8, TNF-α, IFN-γ, IL-17, IL-4, IL-13, FGF-basic, VEGF, G-CSF, and IL-7; 2nd: CXCL8, CCL11, CCL3, CCL2, IL-1β, IL-12, IFN-γ, IL-17, IL-4, IL-9, IL-13, FGF-basic, VEGF, G-CSF, and IL-7; 3rd: CCL11, CCL3, IL-1β, IL-12, IL-15, IL-17, IL-9, FGF-basic, and VEGF. A set of acquired attributes, named COVID-selective (<5 strong correlations in HC and ≥5 strong correlations in COVID) were identified in each trimester: 1st (n=3): CCL4, CCL5, and IL-6, 2nd: (n=1) IL-2, and 3rd (n=3) CXCL8, CCL2 and IL-6 (Figure 5B).
From an overall perspective, a pronounced decrease in network connectivity between serum soluble mediators was observed in convalescent COVID-19 infection during pregnancy as demonstrated by the fewer number of molecules establishing strong correlations driven by an imbalance between preserved, lost and acquired attributes in the COVID group. While IL-1Ra, IL-10 and GM-CSF presented a preserved number of correlations (≥5 strong correlations in HC and COVID), IL-17, FGF-basic and VEGF lost connectivity throughout pregnancy. IL-6 (at 1st and 3rd trimesters) and CXCL8 (at 3rd trimester) were included in a set of acquired attributes, named COVID-selective (≥5 strong correlations in COVID and <5 in HC) (Figure 5B, bold underline attributes).
3.5 Multivariate analysis of serum soluble mediators in convalescent COVID-19 patients at distinct pregnancy trimesters
Multivariate analysis of chemokines, pro-inflammatory cytokines, regulatory cytokines and growth factors was performed using PCA to verify the ability of serum mediators to cluster convalescent COVID-19 pregnant women apart from trimester-matching pre-pandemic non-infected pregnant women as a healthy control (HC). The results are presented in Figure 6. The PCA coordinates (2nd and 3rd principal components) demonstrated that although convalescent COVID pregnant women could be clustered apart from the HC when considering all trimesters together, the segregation profile was more evident when the COVID and HC subgroups were compared at matching gestational trimesters (Figure 6). Vector analysis conducted in the 1st trimester indicated that CXCL8, CCL3, CCL5, IL-1β, TNF-α, IL-12, IL-15, IL-1Ra, IL-10, and G-CSF were associated with convalescent COVID-19 in pregnant women. Data from the 2nd trimester showed that most soluble mediators were vectors associated with differential distribution of convalescent COVID-19 in pregnant women, except for GM-CSF. Additionally, the PCA coordinates obtained from the 3rd trimester demonstrated that several soluble mediators were vectors related to convalescent COVID-19 in pregnant women, except for CXCL10, IL-1β, TNF-α, IFN-γ, PDGF and GM-CSF (Figure 6).
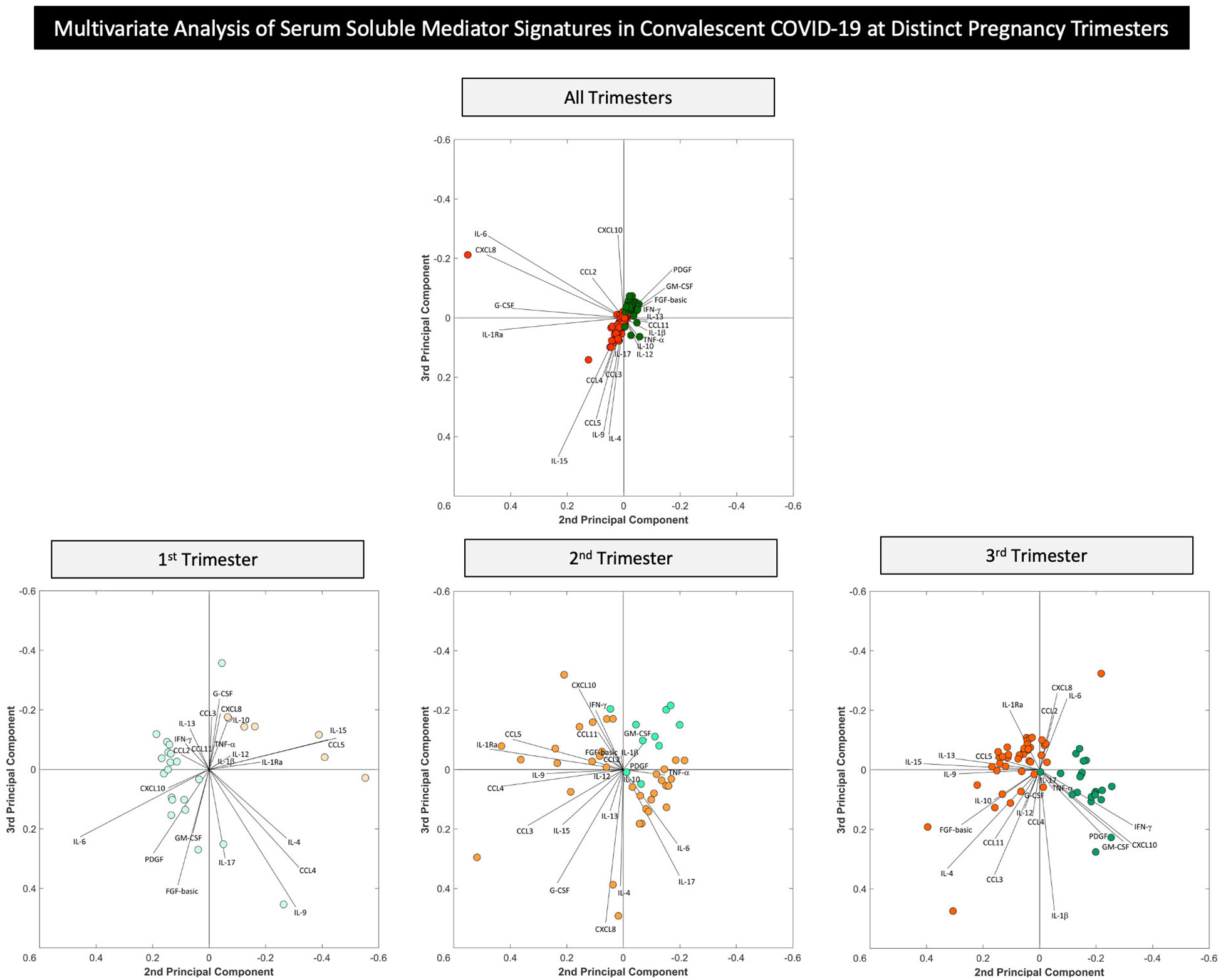
Figure 6 Multivariate analysis of serum soluble mediator networks in convalescent COVID-19 patients at distinct pregnancy trimesters. Multivariate analysis of serum chemokines, pro-inflammatory cytokines, regulatory cytokines and growth factors were performed to verify the ability of soluble mediators to cluster convalescent COVID-19 pregnant women at 3-20 weeks after symptoms onset (COVID, n=89), with pre-pandemic non-infected pregnant women as a Healthy Control (HC, n=52) as well as subgroups of COVID-19 and HC categorized according to pregnancy trimester, referred to as: HC 1st ( , n=21), HC 2nd (
, n=21), HC 2nd ( , n=10), HC 3rd (
, n=10), HC 3rd ( , n=21) and COVID 1st (
, n=21) and COVID 1st ( , n=7), COVID 2nd (
, n=7), COVID 2nd ( , n=34), COVID 3rd (
, n=34), COVID 3rd ( , n=48). The measurements were taken by high-throughput multiplex bead array as described in Material and Methods. Principal Component Analysis (PCA) was carried out by MATLAB software as described in Material and Methods. PCA coordinates (2nd and 3rd principal components) were used to compare and visualize the grouping of convalescent COVID-19 vs HC and subgroups according to pregnancy trimesters.
, n=48). The measurements were taken by high-throughput multiplex bead array as described in Material and Methods. Principal Component Analysis (PCA) was carried out by MATLAB software as described in Material and Methods. PCA coordinates (2nd and 3rd principal components) were used to compare and visualize the grouping of convalescent COVID-19 vs HC and subgroups according to pregnancy trimesters.
4 Discussion
Pregnancy triggers a unique immunological status, aiming to protect the fetus from maternal rejection and guarantee fetal development until birth. Several studies have reported that the immune system plays a balancing role during pregnancy with constant changes according to maternal and fetal demands (16, 17). Physiological changes in immune status during pregnancy are often characterized by alterations in cell-mediated immunity and humoral responses, from the 1st to 3rd pregnancy trimesters. Previous studies have demonstrated that successful implantation is associated with a transient increase in systemic proinflammatory profile followed by a switch toward an anti-inflammatory profile after blastocyst transfer when pregnancy is confirmed (18). Pregnant women are particularly susceptible to COVID-19 due to physiological changes in the immune system, which may result in an altered response to SARS-CoV-2 infection in pregnancy. Furthermore, SARS-CoV-2 infection during pregnancy can disrupt the immune response homeostasis, impacting the maternal immune activation, with effects on pregnancy outcome and offspring (12, 13, 19, 20). It has already been reported that the adverse impacts of the COVID-19 pandemic on maternal health are not limited to morbidity and mortality caused by the disease itself, but are also associated with adverse pregnancy outcomes, including preeclampsia, preterm birth and stillbirth (19).
Most of the information on the impact of SARS-CoV-2 infection in pregnancy has been derived from reports concerning acute symptomatic infection (21). However, little data is available regarding the long-term impact of SARS-CoV-2 infection on pregnancy during the convalescent phase of the disease. In view of this, we designed this study as a pioneer exploratory investigation to perform descriptive and panoramic analysis of serum soluble mediator interplay in pregnant women during the convalescent phase of SARS-CoV-2 infection throughout prenatal care. This study comprises an innovative investigation of the long-lasting impact of SARS-CoV-2 infection during pregnancy focusing on the analysis of the immune response during the convalescent phase comprising 3-20 weeks after symptoms onset.
Our results demonstrate that, in general, serum soluble mediators have different trajectories during healthy pregnancy and are disturbed in pregnant women with convalescent SARS-CoV-2 infection. Herein, healthy pregnant women presented a progressive decrease in most serum soluble mediators towards the 2nd and 3rd pregnancy trimester, including chemokines, pro-inflammatory and regulatory cytokines, in addition to growth factors. Previous studies corroborate our findings in healthy pregnancies. The levels of chemokines and pro-inflammatory cytokines usually peak in the first trimester of pregnancy and decline in the 2nd and 3rd trimesters, while regulatory cytokines and growth factors have diverse trajectories (22, 23). Our findings highlighted that higher levels of most soluble mediators were observed in the COVID group compared to HC control group. The major increase occurred in pro-inflammatory cytokines, including IL-6, TNF-α and IFN-γ, a larger set of biomarkers with elevated COVID/HC ratios observed towards the 2nd (3x increase) and 3rd (3-15x increase) pregnancy trimesters. Studies of immune mediators in SARS-CoV-2 infection during pregnancy remain scarce. It has been proposed that the immunomodulation observed during pregnancy may protect pregnant COVID-19 patients from suffering from a cytokine storm (15, 24). However, no studies focusing on comparative analysis of immunological profiles of COVID-19 and healthy pregnant women at matching pregnancy trimesters have been reported. It is noteworthy that due to physiological changes in the immune response during pregnancy, the inclusion of trimester-matching healthy controls is essential to enable conclusive analysis. Therefore, our study is pioneering in terms of providing a detailed profile of long-lasting changes during convalescent COVID-19 infection in pregnancy as it made direct comparison to trimester-matching healthy controls. Our findings did not support that an immunomodulatory profile is triggered by SARS-CoV-2 infection during pregnancy. In fact, the lower levels of soluble mediators previously reported in convalescent COVID-19 pregnant women were compared with those observed in non-pregnant women and did not consider the physiological changes triggered by pregnancy or alterations in soluble mediators inherent in trimesters (24). Moreover, other studies proposing the immunomodulatory state for acute COVID-19 infection during pregnancy in comparison to healthy pregnant women did not consider stratification by gestational trimesters (15). According to our findings, higher levels of serum soluble mediators were observed for convalescent COVID-19 infection during pregnancy, especially IL-6, TNF-α and IFN-γ in comparison to healthy pregnant women at matching pregnancy trimesters.
Successful pregnancy requires finely coordinated communication between the maternal and fetal microenvironments. Cytokine signaling pathways participate as mediators of these communications to guarantee healthy pregnancy. From the existing data available, there is no consensus trend for the changes observed for IL-6, TNF-α and IFN-γ during pregnancy (16). Several studies have demonstrated that IL-6, TNF-α and IFN-γ concentrations significantly increased between the 1st, 2nd and 3rd trimesters of healthy pregnancy (25–30). However, corroborating our findings, other authors detected significant reductions in IL-6, TNF-α and IFN-γ in maternal serum concentrations between the 1st and 3rd trimesters (31–33).
Infections or inflammatory conditions, such as COVID-19 during pregnancy, can have a detrimental impact on fetal development and also contribute to pregnancy-associated pathological conditions (34). Despite the conflicting data regarding the overall profile of IL-6, TNF-α and IFN-γ during healthy pregnancy, there is a consensus that the establishment of a pro-inflammatory microenvironment is associated with the risk of developing pregnancy-associated pathological conditions, including pregnancy loss, preeclampsia, and gestational diabetes mellitus (35). In this sense, the upregulation of pro-inflammatory cytokines in pregnant women with convalescent COVID-19 may suggest that these patients are more vulnerable to developing adverse pregnancy outcomes.
Integrative network analysis demonstrated that both HC and convalescent COVID-19 pregnancies evolve with decreasing connectivity between serum soluble mediators towards the 3rd trimester. However, the COVID group exhibited a remarkably lower number of connections. Overall, IL-1Ra, IL-10 and GM-CSF presented a preserved number of correlations throughout the pregnancy.
Further research is warranted to determine the precise IL-10 profile during healthy pregnancy (14). A few studies have reported that IL-10 significantly increases from the 1st to the 2nd and 3rd trimesters in healthy pregnancy (30, 36). However, corroborating our findings, other studies have detected that IL-10 decreases between the 1st and 3rd trimesters (31, 37). Considering the critical role of IL-10 as a chief anti-inflammatory cytokine, the preserved IL-10 connectivity axis observed during the 1st and 2nd trimesters may represent a mechanism to protect the fetus from maternal pro-inflammatory rejection and guarantee fetal development until birth.
Our data demonstrated that IL-1Ra decreased in convalescent COVID-19 pregnant women in the 1st trimester but increased in the 3rd trimester. Previous studies reported that IL-1Ra levels increased during the inflammatory response to control acute inflammation and prevent immunopathological events (38). The IL-1 receptor antagonist (IL-1Ra) is an anti-inflammatory cytokine that blocks IL-1α and IL-1β functions and modulates their biological effects (39). It has been previously demonstrated in experimental models that high IL-1Ra levels at the beginning of pregnancy may lead to miscarriage due to impaired embryonic adhesion (40), and data from human studies showed that higher levels of circulating IL-1Ra have been reported in adverse pregnancy outcomes, including preeclampsia (41). Regarding the changes in IL-1Ra levels observed in convalescent COVID-19 along the pregnancy trimesters, our findings of preserved correlation profile between IL-1Ra and other soluble mediators throughout the pregnancy may suggest that an intricate microenvironment of soluble mediators is relevant to guarantee fetal development until birth.
Our data also demonstrated that GM-CSF presented preserved correlation with other soluble mediators throughout pregnancy. It was previously reported that after embryo implantation, GM-CSF participates in a network of cytokines and growth factors that regulate morphological and functional development of the placenta (42).
Conversely, despite increases in IL-17, FGF-basic and VEGF, loss of connectivity was observed throughout pregnancy. IL-17 up-regulates the expression of a variety of biological molecules with angiogenic properties including VEGF (43–47). VEGF plays a central role in vasculogenesis and angiogenesis, which augments vascular endothelial cell proliferation, migration, and survival. Moreover, data from previous studies have shown that IL-17 can induce placental oxidative stress and vascular dysfunction, resulting in hypertension and increased risk of preeclampsia (48). The loss of network connection of IL-17 and VEGF with other soluble mediators throughout the pregnancy may lead to intrinsic vascular dysfunction that results in impaired neonatal development. Post-natal follow-up studies may contribute to identifying impaired new-born growth and development related to altered angiogenesis.
Our data also demonstrated that IL-6 and CXCL8 were included in the set of attributes acquiring strong correlation in the 3rd pregnancy trimester, named COVID-selective correlations. Implications of IL-6 and CXCL8 in pregnancy-associated pathological conditions, such as pregnancy loss, preeclampsia, gestational diabetes mellitus, and infection/inflammation have been reported (35). These two soluble mediators are abundantly produced at the feto-maternal interface throughout pregnancy and have been shown to participate in several pregnancy-related events. Unbalanced expression/secretion of IL-6 and CXCL8 at the feto-maternal interface has been indicated in unexplained pregnancy loss (35). A study of the dynamic connections of the soluble mediator network in pre-eclampsia identified positive correlation between IL-6 and CXCL8, suggesting that these molecules are implicated in the pathophysiology of this pregnancy-associated disease (35, 49). Moreover, a meta-analysis and systematic review suggested a role of CXCL8 in shaping the immune microenvironment in gestational diabetes mellitus (50).
The present study has some limitations. The low number of pregnant women enrolled in each pregnancy trimester re-enforce the need to further validate our findings. This work was performed during circulation of the B.1.1.28 and B.1.1.33 SARS-CoV-2 strains and therefore, the impact of other variants on the immunological profiles remains to be addressed. Despite the pioneering approach of this exploratory investigation, the observational design with multiple comparisons without corrections for co-morbidities or other confounding variables also constitutes a study limitation that may interfere in the levels of systemic soluble mediators. Moreover, regardless the relevance of nutritional aspects ant the dietary inflammatory indices interfering in the immune response during pregnancy (51), we did not have the opportunity to address this issue in the present investigation.
In conclusion, the main finding of this study, a pronounced increase in serum levels of soluble mediators with decreased network interplay between them, portrayed an imbalanced immune response in convalescent COVID-19 infection during pregnancy that may contribute to the prevention or management of clinical course pregnancy complications.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving human participants were reviewed and approved by National Commission for Ethics in Research in Brazil (CONEP, CAAE 32359620.0.0000.5558). The patients/participants provided their written informed consent to participate in this study.
Author contributions
Study design: GF, LS, FM, CA, KC, MC, RT, ON, AS, CPA, AZ and LM. Advisory committee: CG, DM-S, PK, ON, LC, COA, and AZ. Funding acquisition: LE, OM-F and LM. Sample collection, experimental procedures, and data acquisition: ÂS, AC, YP, DA, LL, RN, PA, LG, LD, and JCdR. Data analysis: GF, LS, GJ-S, HS, LA, MG, PB, JBdS, IC-R, AC-A, VP-M, AC, and OM-F. Writing and reviewing the manuscript: GF, LS, GJ-S, HS, OM-F and LM. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the Conselho Nacional de Desenvolvimento Tecnológico (CNPq), Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG) and the University of Brasilia (Grant # 7155, “Fundo COVID-19 UnB em Ação: Ações emergenciais para combate à COVID-19 e mitigação das consequências da pandemia”, “Eficácia de um protocolo de testagem RT-PCR para SARS-CoV-2 sobre a preservação da força de trabalho em saúde durante a pandemia COVID-19 no Brasil: ensaio clínico randomizado” and Grant # 7110, “Amamentar em tempos de pandemia de COVID-19: um protocolo para avaliação do impacto do SARS-COV-2 no sucesso do aleitamento materno”).
Acknowledgments
This study was performed by students and professors enrolled in Postgraduate Programs: Programa de Pós-graduação em Ciências Médicas da Universidade de Brasília (UnB), supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES). The authors thank the Program for Technological Development in Tools for Health-RPT-FIOCRUZ for use of the flow cytometry facilities. The authors also express their gratitude to Dayane Andriotti Otta for technical support. ON, MG, JCdR, LA, AC and OM-F received PQ fellowships from CNPq. AC and OM-F are research fellows from FAPEAM (PVN-II, PRÓ-ESTADO Program #005/2019).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1176898/full#supplementary-material
References
1. World Health Organization. WHO coronavirus (COVID-19) dashboard data (2022). Available at: https://covid19.who.int/ (Accessed January 25, 2022).
2. Brandt JS, Hill J, Reddy A, Schuster M, Patrick HS, Rosen T, et al. Epidemiology of coronavirus disease 2019 in pregnancy: risk factors and associations with adverse maternal and neonatal outcomes. Am J Obstet Gynecol (2021) 224(4):e1–9. doi: 10.1016/j.ajog.2020.09.043
3. Khoury R, Bernstein PS, Debolt C, Stone J, Sutton DM, Simpson LL, et al. Characteristics and outcomes of 241 births to women with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection at five new York city medical centers. Obstetrics Gynecol (2020) 136(2):273–82. doi: 10.1097/AOG.0000000000004025
4. Metz TD, Clifton RG, Hughes BL, Sandoval G, Saade GR, Grobman WA, et al. Disease severity and perinatal outcomes of pregnant patients with coronavirus disease 2019 (COVID-19). Obstetrics Gynecol (2021) 137(4):571–80. doi: 10.1097/AOG.0000000000004339
5. Darif D, Hammi I, Kihel A, Idrissi Saik I, Guessous F, Akarid K. The pro-inflammatory cytokines in COVID-19 pathogenesis: What goes wrong? Microb Pathog (2021) 153:104799. doi: 10.1016/j.micpath.2021.104799
6. Asakura H, Ogawa H. COVID-19-associated coagulopathy and disseminated intravascular coagulation. Int J Hematol (2021) 113(1):45–57. doi: 10.1007/s12185-020-03029-y
7. Chen R, Lan Z, Ye J, Pang L, Liu Y, Wu W, et al. Cytokine storm: The primary determinant for the pathophysiological evolution of COVID-19 deterioration. Front Immunol (2021) 12. doi: 10.3389/fimmu.2021.589095
8. Allotey J, Fernandez S, Bonet M, Stallings E, Yap M, Kew T, et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta-analysis. BMJ (2020), 370:m3320. doi: 10.1136/bmj.m3320
9. Villar J, Ariff S, Gunier RB, Thiruvengadam R, Rauch S, Kholin A, et al. Maternal and neonatal morbidity and mortality among pregnant women with and without COVID-19 infection. JAMA Pediatr (2021) 175(8):817. doi: 10.1001/jamapediatrics.2021.1050
10. Huntley BJF, Huntley ES, di Mascio D, Chen T, Berghella V, Chauhan SP. Rates of maternal and perinatal mortality and vertical transmission in pregnancies complicated by severe acute respiratory syndrome coronavirus 2 (SARS-Co-V-2) infection. Obstetrics Gynecol (2020) 136(2):303–12. doi: 10.1097/AOG.0000000000004010
11. Savasi VM, Parisi F, Patanè L, Ferrazzi E, Frigerio L, Pellegrino A, et al. Clinical findings and disease severity in hospitalized pregnant women with coronavirus disease 2019 (COVID-19). Obstetrics Gynecol (2020) 136(2):252–8. doi: 10.1097/AOG.0000000000003979
12. Cavalcante MB, Cavalcante CTMB, Sarno M, Barini R, Kwak-Kim J. Maternal immune responses and obstetrical outcomes of pregnant women with COVID-19 and possible health risks of offspring. J Reprod Immunol (2021) 143:103250. doi: 10.1016/j.jri.2020.103250
13. Cavalcante MB, de Melo Bezerra Cavalcante CT, Cavalcante ANM, Sarno M, Barini R, Kwak-Kim J. COVID-19 and miscarriage: From immunopathological mechanisms to actual clinical evidence. J Reprod Immunol (2021) 148:103382. doi: 10.1016/j.jri.2021.103382
14. Parisi F, Milazzo R, Savasi VM, Cetin I. Maternal low-grade chronic inflammation and intrauterine programming of health and disease. Int J Mol Sci (2021) 22(4):1732. doi: 10.3390/ijms22041732
15. Fernandes GM, Motta F, Sasaki LMP, da Silva ÂP, Miranda AM, de Carvalho AO, et al. Pregnancy outcomes and child development effects of SARS-CoV-2 infection (PROUDEST trial): Protocol for a multicenter, prospective cohort study. JMIR Res Protoc (2021) 10(4):e26477. doi: 10.2196/26477
16. Spence T, Allsopp PJ, Yeates AJ, Mulhern MS, Strain JJ, McSorley EM. Maternal serum cytokine concentrations in healthy pregnancy and preeclampsia. J Pregnancy (2021) 2021:1–33. doi: 10.1155/2021/6649608
17. Chen G, Liao Q, Ai J, Yang B, Bai H, Chen J, et al. Immune response to COVID-19 during pregnancy. Front Immunol (2021) 12. doi: 10.3389/fimmu.2021.675476
18. Zhao Y, Zhang T, Guo X, Wong CK, Chen X, Chan YL, et al. Successful implantation is associated with a transient increase in serum pro-inflammatory cytokine profile followed by a switch to anti-inflammatory cytokine profile prior to confirmation of pregnancy. Fertile Sterile (2021) 115(4):1044–53. doi: 10.1016/j.fertnstert.2020.10.031
19. Wei SQ, Bilodeau-Bertrand M, Liu S, Auger N. The impact of COVID-19 on pregnancy outcomes: a systematic review and meta-analysis. Can Med Assoc J (2021) 193(16):E540–8. doi: 10.1503/cmaj.202604
20. Chen G, Zhang Y, Zhang Y, Ai J, Yang B, Cui M, et al. Differential immune responses in pregnant patients recovered from COVID-19. Signal Transduct Target Ther (2021) 6(1):289. doi: 10.1038/s41392-021-00703-3
21. Mullins E, Perry A, Banerjee J, Townson J, Grozeva D, Milton R, et al. Pregnancy and neonatal outcomes of COVID-19: The PAN-COVID study. Eur J Obstetrics Gynecol Reprod Biol (2022) 276:161–7. doi: 10.1016/j.ejogrb.2022.07.010
22. Jarmund AH, Giskeødegård GF, Ryssdal M, Steinkjer B, Stokkeland LMT, Madssen TS, et al. Cytokine patterns in maternal serum from first trimester to term and beyond. Front Immunol (2021) 12. doi: 10.3389/fimmu.2021.752660
23. Azizieh F, Dingle K, Raghupathy R, Johnson K, VanderPlas J, Ansari A. Multivariate analysis of cytokine profiles in pregnancy complications. Am J Reprod Immunol (2018) 79(3):e12818. doi: 10.1111/aji.12818
24. Tartaglia E, Bordoni V, Oliva A, Vergori A, Girardi E, Antinori A, et al. T Helper profile in pregnant women recovered from COVID-19. J Reprod Immunol (2022) 153:103661. doi: 10.1016/j.jri.2022.103661
25. Subha M, Pal P, Pal GK, Habeebullah S, Adithan C, Sridhar MG. Decreased baroreflex sensitivity is linked to sympathovagal imbalance, low-grade inflammation, and oxidative stress in pregnancy-induced hypertension. Clin Exp Hypertens (2016) 38(8):666–72. doi: 10.1080/10641963.2016.1200596
26. Blackmore ER, Moynihan JA, Rubinow DR, Pressman EK, Gilchrist M, O’Connor TG. Psychiatric symptoms and proinflammatory cytokines in pregnancy. Psychosom Med (2011) 73(8):656–63. doi: 10.1097/PSY.0b013e31822fc277
27. Simavli S, Derbent AU, Uysal S, Turhan NÖ. Hepcidin, iron status, and inflammation variables among healthy pregnant women in the Turkish population. J Maternal-Fetal Neonatal Med (2014) 27(1):75–9. doi: 10.3109/14767058.2013.804054
28. Björkander S, Bremme K, Persson JO, van Vollenhoven RF, Sverremark-Ekström E, Holmlund U. Pregnancy-associated inflammatory markers are elevated in pregnant women with systemic lupus erythematosus. Cytokine (2012) 59(2):392–9. doi: 10.1016/j.cyto.2012.04.046
29. Lindsay K, Buss C, Wadhwa P, Entringer S. Maternal stress potentiates the effect of an inflammatory diet in pregnancy on maternal concentrations of tumor necrosis factor alpha. Nutrients (2018) 10(9):1252. doi: 10.3390/nu10091252
30. Olimpia SS, Magdalena P, Tomasz P, Piotr W, Elzbieta RW. Changes in the concentration of sHLA-I and selected cytokines in pregnancy complicated by antiphospholipid syndrome. Ginekol Pol (2011) 82(5):354–8. doi: 10.3390/nu10091252
31. Stokkeland LMT, Giskeødegård GF, Stridsklev S, Ryan L, Steinkjer B, Tangerås LH, et al. Serum cytokine patterns in first half of pregnancy. Cytokine (2019) 119:188–96. doi: 10.1016/j.cyto.2019.03.013
32. Doria A, Cutolo M, Ghirardello A, Zen M, Villalta D, Tincani A, et al. Effect of pregnancy on serum cytokines in SLE patients. Arthritis Res Ther (2012) 14(2):R66. doi: 10.1186/ar3782
33. Iaccarino L, Ghirardello A, Zen M, Villalta D, Tincani A, Punzi L, et al. Polarization of TH2 response is decreased during pregnancy in systemic lupus erythematosus. Reumatismo (2012) 64(5):314–20. doi: 10.4081/reumatismo.2012.314
34. Yockey LJ, Iwasaki A. Interferons and proinflammatory cytokines in pregnancy and fetal development. Immunity (2018) 49(3):397–412. doi: 10.1016/j.immuni.2018.07.017
35. Vilotić A, Nacka-Aleksić M, Pirković A, Bojić-Trbojević Ž, Dekanski D, Jovanović Krivokuća M. IL-6 and IL-8: An overview of their roles in healthy and pathological pregnancies. Int J Mol Sci (2022) 23(23):14574. doi: 10.3390/ijms232314574
36. Nayak M, Peinhaupt M, Heinemann A, Eekhoff MEW, van Mechelen W, Desoye G, et al. Sedentary behavior in obese pregnant women is associated with inflammatory markers and lipid profile but not with glucose metabolism. Cytokine (2016) 88:91–8. doi: 10.1016/j.cyto.2016.08.031
37. Ross KM, Miller G, Culhane J, Grobman W, Simhan HN, Wadhwa PD, et al. Patterns of peripheral cytokine expression during pregnancy in two cohorts and associations with inflammatory markers in cord blood. Am J Reprod Immunol (2016) 76(5):406–14. doi: 10.1111/aji.12563
38. Witkin SS, Gerber S, Ledger WJ. Influence of interleukin-1 receptor antagonist gene polymorphism on disease. Clin Infect Diseases (2002) 34(2):204–9. doi: 10.1086/338261
39. Steinkasserer A, Spurr NK, Cox S, Jeggo P, Sim RB. The human IL-1 receptor antagonist gene (IL1RN) maps to chromosome 2q14-q21, in the region of the IL-1 alpha and IL-1 beta loci. Genomics (1992) 13(3):654–7. doi: 10.1016/0888-7543(92)90137-H
40. Simón C, Valbuena D, Krüssel J, Bernal A, Murphy CR, Shaw T, et al. Interleukin-1 receptor antagonist prevents embryonic implantation by a direct effect on the endometrial epithelium. Fertil Steril (1998) 70(5):896–906. doi: 10.1016/S0015-0282(98)00275-1
41. Kimya Y, Akdiş C, Cengiz C, Ozan H, Tatlikazan S, Uncu G, et al. Plasma interleukin-1alpha, interleukin-1beta and interleukin-1 receptor antagonist levels in pre-eclampsia. Eur J Obstet Gynecol Reprod Biol (1997) 73(1):17–21. doi: 10.1016/S0301-2115(97)02698-5
42. Bowen JM, Chamley L, Mitchell MD, Keelan JA. Cytokines of the placenta and extra-placental membranes: biosynthesis, secretion and roles in establishment of pregnancy in women. Placenta (2002) 23(4):239–56. doi: 10.1053/plac.2001.0781
43. Numasaki M, Lotze MT, Sasaki H. Interleukin-17 augments tumor necrosis factor-alpha-induced elaboration of proangiogenic factors from fibroblasts. Immunol Lett (2004) 93(1):39–43. doi: 10.1016/j.imlet.2004.01.014
44. Numasaki M, Takahashi H, Tomioka Y, Sasaki H. Regulatory roles of IL-17 and IL-17F in G-CSF production by lung microvascular endothelial cells stimulated with IL-1beta and/or TNF-alpha. Immunol Lett (2004) 95(1):97–104. doi: 10.1016/j.imlet.2004.06.010
45. Numasaki M. Interleukin-17 promotes angiogenesis and tumor growth. Blood (2003) 101(7):2620–7. doi: 10.1182/blood-2002-05-1461
46. Takahashi H, Numasaki M, Lotze MT, Sasaki H. Interleukin-17 enhances bFGF-, HGF- and VEGF-induced growth of vascular endothelial cells. Immunol Lett (2005) 98(2):189–93. doi: 10.1016/j.imlet.2004.11.012
47. Numasaki M, Watanabe M, Suzuki T, Takahashi H, Nakamura A, McAllister F, et al. IL-17 enhances the net angiogenic activity and In vivo growth of human non-small cell lung cancer in SCID mice through promoting CXCR-2-Dependent angiogenesis. J Immunol (2005) 175(9):6177–89. doi: 10.4049/jimmunol.175.9.6177
48. Cornelius DC, Lamarca B. TH17- and IL-17- mediated autoantibodies and placental oxidative stress play a role in the pathophysiology of pre-eclampsia. Minerva Ginecol (2014) 66(3):243–9. doi: 10.4049/jimmunol.175.9.6177
49. Pinheiro MB, Martins-Filho OA, Mota APL, Alpoim PN, Godoi LC, Silveira ACO, et al. Severe preeclampsia goes along with a cytokine network disturbance towards a systemic inflammatory state. Cytokine (2013) 62(1):165–73. doi: 10.1016/j.cyto.2013.02.027
50. Liu H, Liu A, Kaminga AC, McDonald J, Wen SW, Pan X. Chemokines in gestational diabetes mellitus. Front Immunol (2022) 13. doi: 10.3389/fimmu.2022.705852
Keywords: chemokines, cytokines, growth factors, COVID-19, pregnancy
Citation: Fernandes GM, Sasaki LMP, Jardim-Santos GP, Schulte HL, Motta F, da Silva ÂP, de Carvalho AO, Pereira YR, Alves CdO, de Araújo Júnior DA, Mendonça-Silva DL, Costa KN, de Castro MEC, Lauand L, Nery RdR, Tristão R, Kurizky PS, Nóbrega OdT, Espindola LS, de Castro LCG, Alpoim PN, Godoi LC, Dusse LMSA, Coelho-dos-Reis JGA, Amaral LRd, Gomes MdS, Bertarini PLL, Brito-de-Sousa JP, Costa-Rocha IAd, Campi-Azevedo AC, Peruhype-Magalhães V, Teixeira-Carvalho A, Zaconeta AM, Soares AAdSM, Valim V, Gomes CM, de Albuquerque CP, Martins-Filho OA and da Mota LMH (2023) Panoramic snapshot of serum soluble mediator interplay in pregnant women with convalescent COVID-19: an exploratory study. Front. Immunol. 14:1176898. doi: 10.3389/fimmu.2023.1176898
Received: 01 March 2023; Accepted: 30 March 2023;
Published: 12 April 2023.
Edited by:
Diana Boraschi, Chinese Academy of Science (CAS), ChinaReviewed by:
Olukemi Amodu, University of Ibadan, NigeriaMarcelo Cavalcante, University of Fortaleza, Brazil
Copyright © 2023 Fernandes, Sasaki, Jardim-Santos, Schulte, Motta, da Silva, de Carvalho, Pereira, Alves, de Araújo Júnior, Mendonça-Silva, Costa, de Castro, Lauand, Nery, Tristão, Kurizky, Nóbrega, Espindola, de Castro, Alpoim, Godoi, Dusse, Coelho-dos-Reis, Amaral, Gomes, Bertarini, Brito-de-Sousa, Costa-Rocha, Campi-Azevedo, Peruhype-Magalhães, Teixeira-Carvalho, Zaconeta, Soares, Valim, Gomes, de Albuquerque, Martins-Filho and da Mota. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Geraldo Magela Fernandes, Z2VyYWxkb21hZmVyQGdtYWlsLmNvbQ==; Olindo Assis Martins-Filho, b2xpbmRvLmZpbGhvQGZpb2NydXouYnI=
†These authors have contributed equally to this work
‡These authors share senior authorship