 Yangming Tang
Yangming Tang Yue Li
Yue Li Turun Song
Turun Song
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol. , 04 April 2023
Sec. Alloimmunity and Transplantation
Volume 14 - 2023 | https://doi.org/10.3389/fimmu.2023.1150341
The coronavirus disease 2019 (COVID-19) pandemic has caused a significant burden of morbidity and mortality worldwide, with solid organ transplant recipients (SOTRs) being particularly vulnerable. Nirmatrelvir and ritonavir have demonstrated the potential for reducing the risk of hospitalization and death in patients with mild-to-moderate COVID-19. However, ritonavir has a strong drug–drug interaction with CYP3A-dependent drugs such as calcineurin inhibitors, potentially leading to rapid increases in blood concentration. As SOTRs are commonly prescribed immunosuppressants, co-administration with nirmatrelvir/ritonavir requires careful consideration. To address this issue, we conducted a literature review to evaluate the use and adverse effects of nirmatrelvir/ritonavir in SOTRs and explore feasible immunosuppressant adjustment regimens. Our findings suggest that nirmatrelvir/ritonavir could be a feasible treatment option for COVID-19 in SOTRs, provided that appropriate immunosuppressive drug management is in place during co-administration. Although prescribing the novel anti-SARS-CoV-2 drug to transplant recipients poses challenges, potential strategies to overcome these issues are discussed. Further studies are needed to determine the optimal dosing strategies of nirmatrelvir/ritonavir, immunosuppressant adjustment, and monitoring in this patient population.
The coronavirus disease 2019 (COVID-19) pandemic has persisted for nearly 3 years, resulting in significant morbidity and mortality worldwide (1). Despite global efforts, combating severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has remained challenging. The emergence of the Omicron variant in November 2021 has further complicated the situation, leading to rapid global spread and becoming the predominant variant in circulation (2). Recent in vitro studies have shown that many therapeutic monoclonal antibodies have lower neutralizing activity against the Omicron variant compared to earlier strains (3). As a result, there is an urgent need for the development of effective drugs to treat COVID-19.
Paxlovid™ (Pfizer, New York City, NY, USA) is a novel oral antiviral drug from Pfizer that contains nirmatrelvir and ritonavir (NR). In a phase II–III clinical trial, NR demonstrated an 89% reduction in the risk of hospitalization or death within 28 days compared to a placebo in 2,246 unvaccinated patients with mild COVID-19 (4). On 22 December 2021, the US Food and Drug Administration (FDA) approved an emergency use authorization (EUA) for Paxlovid, approving it for outpatient treatment of mild-to-moderate COVID-19 patients who are at risk for progression (≥ 12 years of age and weighing ≥ 40 kg) within 5 days of symptom onset (5). Since then, NR has emerged as a promising treatment option for patients infected with SARS-CoV-2 during the Omicron surge, demonstrating inspiring results against the Omicron variant (6).
Nirmatrelvir is an oral protease inhibitor with in vitro pan-human coronavirus antiviral activity. It targets MPRO, a viral protease that plays a crucial role in viral replication and exhibits excellent off-target selectivity and in vivo safety profiles (7). Ritonavir is another component of NR and acts as an HIV-1 protease inhibitor and a cytochrome P450 3A (CYP3A) inhibitor, which is necessary to achieve adequate concentrations of nirmatrelvir. However, the interaction between ritonavir and CYP3A-dependent drugs can result in a rapid and substantial increase in blood concentrations of the latter drugs (8).
Immunosuppressive drugs (ISDs) such as calcineurin inhibitors (CNIs) (e.g., tacrolimus and cyclosporine) and mammalian target of rapamycin (mTOR) inhibitors rely heavily on CYP3A metabolism (9), which can lead to drug interactions and potentially harmful increases in blood concentrations if co-administered with NR. It is therefore recommended to adjust the dose of the ISDs and monitor concentrations and immunosuppressant-associated adverse reactions if co-administered with NR (10). Patients with transplants are particularly vulnerable to COVID-19 morbidity and mortality due to immunosuppression, comorbidities, and suboptimal response to vaccination (11). Given the current surge of SARS-CoV-2 and the Omicron variant, it is likely that transplanted patients will be prescribed Paxlovid more frequently. However, there is currently a paucity of clinical data available regarding the use of Paxlovid in solid organ transplant recipients (SOTRs), and no consensus exists regarding the adjustment of CNIs used in these patients. Therefore, there is an urgent need to gather available data on this subject. In this paper, we conducted a literature review to summarize the adverse reactions associated with Paxlovid administration in SOTRs and explore feasible protocols for adjusting ISDs dosages.
We conducted a comprehensive literature search from 1 December 2021 to 15 November 2022, using the Medline and Embase databases. The search strategy included the following keywords: Paxlovid, nirmatrelvir or PF-07321332, ritonavir, COVID-19, solid organ transplant (SOT), kidney transplantation, liver transplantation, heart transplantation, lung transplantation, pancreas transplantation, and kidney–pancreas transplantation. We included all types of studies, including case reports, case series, and case-control studies that reported on SOT recipients who received CNIs as maintenance immunosuppressants and nirmatrelvir/ritonavir as a treatment for COVID-19.
Table 1 summarizes the characteristics of the study populations. A total of 13 articles, involving 84 SOT cases treated with NR, were included. Patient ages ranged from 14 to 79 years, with 50% (42/84) being men. The transplant types included 35 kidney transplants (41.6%), 22 heart transplants (26.2%), 21 lung transplants (25%), five liver transplants (6%), and one pancreas–kidney transplant (1.2%). Of the reported patients, 67 (79.8%) had been vaccinated, with 47 (70%) having received three doses or more. The time from transplant to COVID-19 ranged from 2 to 27.7 years.
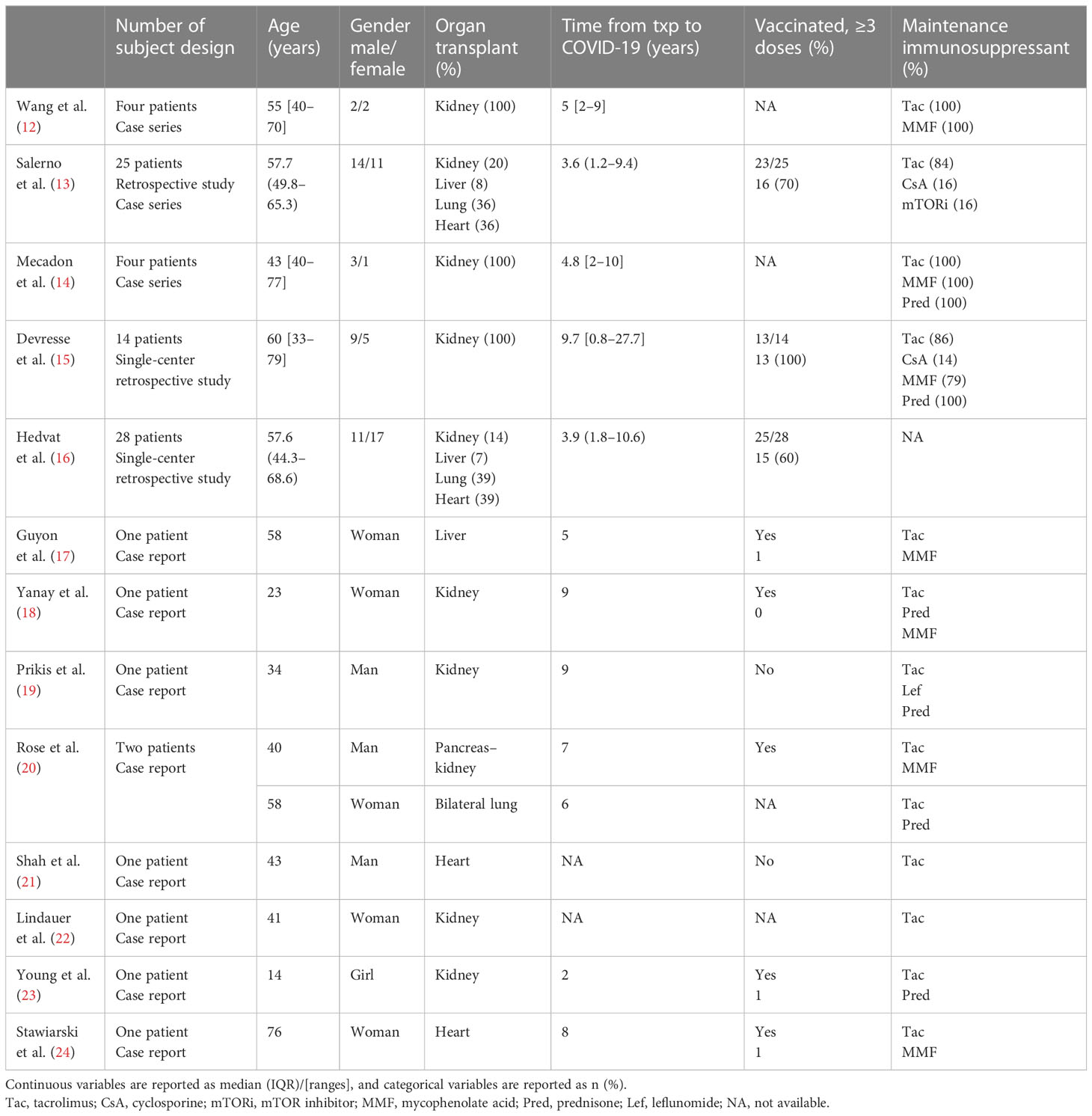
Table 1 Study characteristics.
All studies reported the incidence of hospital admission or mortality as well as immunosuppressant drug levels and dose adjustments after NR treatment. Notably, the majority of patients received tacrolimus-based immunosuppressive therapy, which can affect NR administration and the clinical manifestations of SOTRs. Therefore, we focused on the use and monitoring of tacrolimus during NR therapy.
A total of 75 cases (65 tacrolimus, six cyclosporines, three everolimus, and one sirolimus) from six studies were included in this analysis. Similar adjustment strategies were utilized for SOT patients receiving outpatient care, and all completed 5 days of nirmatrelvir/ritonavir treatment with slight variations in the timing of tacrolimus discontinuation and resumption of dose. Table 2 summarizes the main findings.
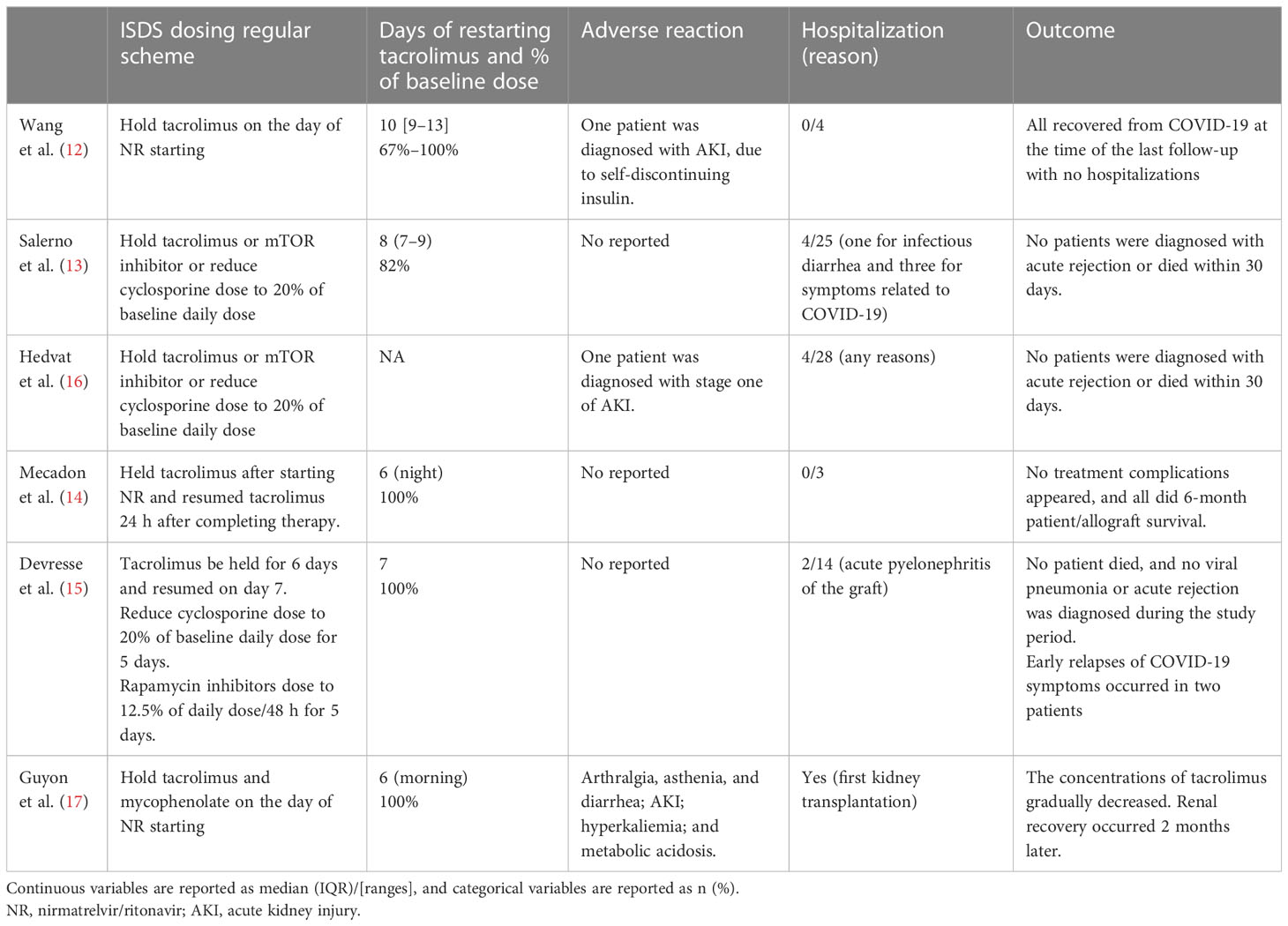
Table 2 Studies of holding CNIs/mTOR inhibitors.
In the study by Wang et al. (12), four kidney transplant recipients (KTRs) held tacrolimus on the day of NR initiation and resumed at 66%–100% of their baseline dose on days 9–13 (day 1 being the day of NR initiation). Mecadon et al. (14) described four KTRs who received NR for COVID-19; three of them held tacrolimus after starting NR and resumed tacrolimus 24 h after completing therapy. Similarly, Salerno et al. (13), Hedvat et al. (16), and Devresse et al. (15) adopted a similar dosing guideline: holding tacrolimus/mTOR inhibitors or reducing cyclosporine dose to 20% of the baseline daily dose on the day of NR initiation. In one liver transplant recipient who had recently undergone kidney transplantation, Guyon et al. (17) discontinued all immunosuppressants. Patients resumed taking tacrolimus either 12 h after the last dose of NR at 100% of the baseline dose (17), on day 7 (day 1 being the day of NR initiation) at 100% (15), or 3 days (2–5 days) after the completion of NR at 82% (interquartile range (IQR), 71–100) of their baseline dose (13).
In 85.3% (64/75) of patients, satisfactory trough concentrations of CNI were observed at the end of NR treatment; however, individual variability was high (12–14). Wang et al. (12) reported low or undetectable tacrolimus levels in two patients (2.7%, 2/75) on days 8–9 (day 1 being the day of NR initiation), while Salerno et al. (13) reported undetectable everolimus trough concentrations in two patients (2.7%, 2/75) on days 7 and 9. After resuming tacrolimus or cyclosporine for 3–4 days, the first assessment revealed a significant increase in CNI trough levels in 12% (9/75) of patients. Salerno et al. (13) reported one patient with a tacrolimus trough concentration of 24.6 ng/ml. Devresse et al. (15) reported a > 10-ng/ml increase in tacrolimus trough concentration for three patients and a > 350-ng/ml increase in cyclosporine for one patient. Mecadon et al. (14) reported that three patients experienced supratherapeutic levels (> 20 ng/ml), and Guyon et al. (17) reported a patient with a tacrolimus trough level of > 111 ng/ml.
During ISDs adjustment periods, most patients had a stable renal function. Two out of 75 patients (3%) experienced acute kidney injury (AKI), and one case was induced by tacrolimus nephrotoxicity (12, 17). No acute rejection or patient death occurred during the follow-up period of approximately 30 days. Out of the 75 patients, 13.3% (10/75) required hospitalization, with one case of infectious diarrhea, three cases related to COVID-19 symptoms (13), two cases of acute pyelonephritis (15), one case of general condition deterioration (17), and four cases of unknown reasons (16). Two patients experienced relapses of early SARS-CoV-2 infection, which may have been caused by infection with new variants, but both patients rapidly recovered within a few days of follow-up (15).
Notably, Hedvat et al. (16) reported that patients who received NR (n = 28) had a lower rate of 30-day hospitalization or death due to COVID-19 compared to those who received no specific treatment (n = 75) (10.7% vs. 30.7%, p = 0.043). Interestingly, there was no difference in the rate of hospitalization or death at 30 days among patients who received NR, regardless of whether they completed the COVID-19 vaccination series (≥ 3 doses) or not (0% vs. 25%, p = 0.113).
Nine cases have been reported in which patients were prescribed NR as outpatients without holding tacrolimus but later required hospitalization due to serious adverse reactions or a surge in tacrolimus concentrations (14, 18–24). The clinical manifestations and course of treatment for these cases are presented in Table 3.
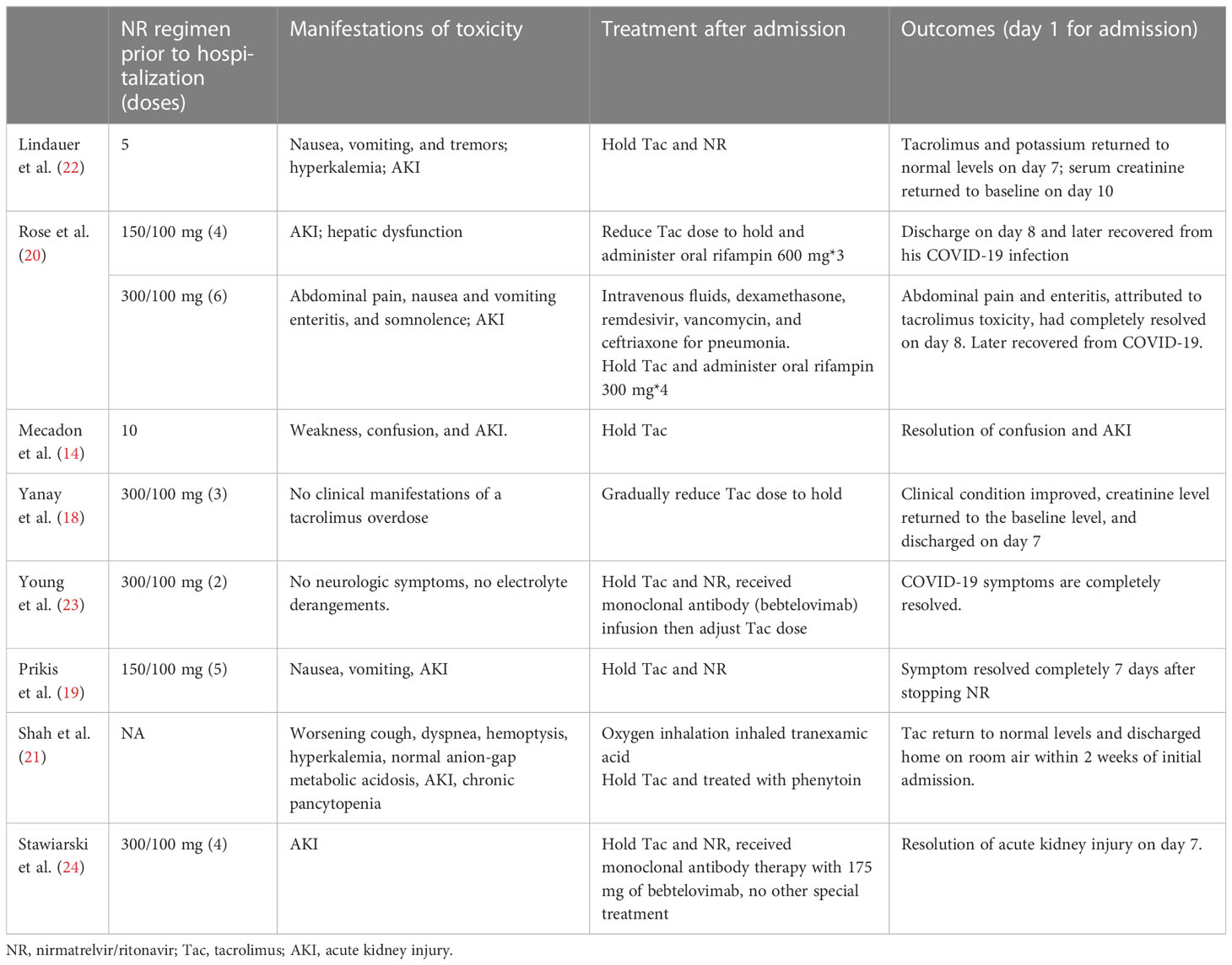
Table 3 Manifestations and outcomes of cases of keeping tacrolimus.
Among these cases, only one patient (11.1%) completed the full NR treatment course, while the others either were admitted to the hospital for adverse reactions or notified their transplant care team and were promptly instructed to stop the medication while monitoring tacrolimus concentrations. All the cases reported supratherapeutic tacrolimus levels (> 30 ng/ml), and only two cases showed no significant clinical manifestations. Common adverse reactions reported during treatment with NR included AKI (78%, 7/9); gastrointestinal symptoms such as nausea, vomiting, and abdominal pain (33%, 3/9); neurologic symptoms such as tremors, confusion, and somnolence (33%, 3/9); and electrolyte disturbances (33%, 3/9). Other adverse events, such as hepatic dysfunction and pancytopenia, were less common. Most of these adverse reactions were likely due to tacrolimus toxicity. The median time for the tacrolimus concentration to return to baseline levels after holding NR was 8 (IQR, 7–12) days. Notably, in two case reports (20, 21), rifampin and phenytoin were used to accelerate tacrolimus metabolism, resulting in a rapid decline in therapeutic levels.
As to the concurrent management of steroids and antimetabolite drugs, Devresse et al. (15) kept the steroid dose constant; Yanay et al. (18) doubled the prednisone dose while maintaining mycophenolic acid; and Rose et al. (20) also maintained mycophenolic acid. There was no report on the effect of this adjustment.
In this study, we conducted a thorough review of all available evidence regarding SOTRs who have been infected by SARS-CoV-2 and have received nirmatrelvir/ritonavir in conjunction with immunosuppressants. Our focus was on the potential drug interactions and the adjustment of immunosuppressant dosages during treatment.
Due to their dependence on CYP3A metabolism and P-glycoprotein-mediated transport, CNIs pose a significant risk for drug interactions when co-administered with ritonavir, a well-known irreversible potent inhibitor of CYP3A (25). Ritonavir has been shown to significantly increase the exposure of tacrolimus by up to 40-fold (26). To reduce or avoid this drug interaction, two key phases must be considered: the initiation of NR and empirical adjustments to baseline CNI dosing, and the reintroduction or dose adjustment of CNIs following the completion of NR treatment.
We compared patients who stopped taking tacrolimus during NR treatment with those who continued or reduced their dosage. As expected, the former group had better clinical outcomes, with lower rates of hospitalization (13.3% vs. 89.9%) and tacrolimus toxicity (4% vs. 78%) during the follow-up period. Although some patients in the tacrolimus-holding group had low or undetectable tacrolimus concentrations during the 5-day treatment period, no cases of acute rejection were reported, and tacrolimus concentrations remained relatively stable. Therefore, holding tacrolimus at the start of NR treatment appears to be a simple and safe strategy to avoid overexposure. A study has suggested reducing tacrolimus dosage by approximately 0.5 mg once weekly to prevent toxicity when co-administered with ritonavir-boosted antiretroviral therapy (27), and another research also considered a tacrolimus dose of less than 1 mg/week may be sufficient to maintain adequate blood tacrolimus concentrations in patients on Kaletra (lopinavir and ritonavir) (28), which were worth considering. Additionally, for patients with high immunologic risk factors, such as those in the early posttransplant period or with a high risk of rejection, one study recommended administering a single 1/8 of the daily tacrolimus dosage on the first day of NR treatment and then no further doses for the rest of the treatment period. This approach can maintain comparable total exposure during the 5-day antiviral treatment while limiting overexposure and preventing rejection (29).
According to our analysis of the included studies, there was no consensus on the optimal timing and dosing of tacrolimus re-initiation. Some studies, such as those by Salerno et al. (13) and Wang et al. (12), implemented an individualized resumption strategy for their patients, administering the adjusted tacrolimus dose based on monitoring levels, with satisfactory results. We also observed that in some cases, supratherapeutic levels of tacrolimus persisted for up to 10 days after partial or full dose resumption, despite low tacrolimus concentrations, due to a longer CYP3A4 inhibition induced by NR administration (13). A simulation study of lopinavir/ritonavir treatment cessation showed a gradual decrease in drug transport and CYP3A inhibition, with 50% recovery of metabolism after 24 hours and 75% after 48 hours (30). Therefore, Lemaitre et al. proposed reintroducing tacrolimus at 50% of the daily dose on Day 6 (Day 1 for the initiation of NR) and increasing it to 75% on day 7 before resuming the usual daily dose on day 8 (29). Along with monitoring whole blood tacrolimus concentrations, qualified institutions can measure nirmatrelvir and ritonavir plasma concentrations to better determine metabolic status and the appropriate timing of tacrolimus administration. A recent study has reported a simple and rapid UPLC-MS/MS method for the quantitative determination of NR in human plasma, which may improve drug guidance (17).
Our literature search yielded limited evidence to support specific adjustment schemes for other ISDs. Table 4 provides a summary of the available guidance and published recommendations on the adjustment strategy of immunosuppressive drugs when co-administered with nirmatrelvir/ritonavir (9, 10, 26, 31, 32). Based on current experience, cyclosporine should be reduced to 20% of the baseline daily dose (DD) upon initiation of NR and gradually reintroduced from day 6, following a similar approach to tacrolimus resumption. As for mTOR inhibitors, it is recommended that they be stopped during the administration of NR or administered at 1/8 of the usual DD on days 1, 3, and 5, and the usual DD be reintroduced on day 7. Our included studies have reported little evidence about mycophenolic acid and steroid management. Current guidelines suggest that mycophenolic acid and steroid doses may remain unchanged, as a weak interaction is expected (26, 32). These recommendations are primarily theoretical, and individualized drug concentration monitoring is necessary due to the inhibitory effect of ritonavir on various immunosuppressive agents. Further clinical studies are needed to explore the most appropriate strategy for these drugs with NR in transplant patients.
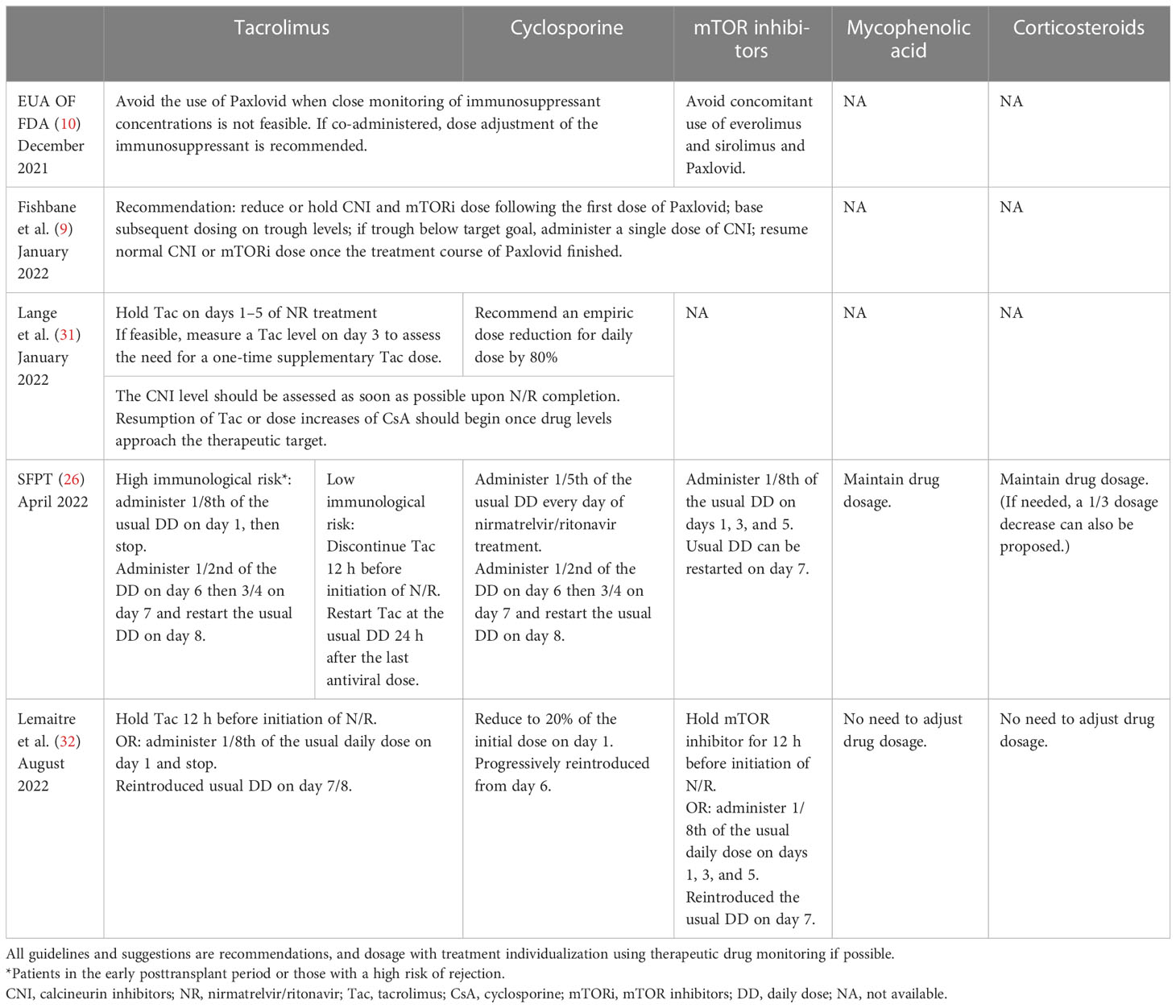
Table 4 A summary of adjustment strategies of immunosuppressive drugs.
However, there are special circumstances where transplant patients may first seek medical attention from primary care providers who may not be aware of the potential drug interactions between ritonavir and CNIs or mTOR inhibitors during the COVID-19 pandemic. In SOT patients who took Paxlovid without adjusting their CNIs, especially tacrolimus, most experienced a significant increase in tacrolimus levels and severe complications such as AKI, neurotoxicity, and gastrointestinal symptoms. Fortunately, most transplant patients recovered after prompt drug withdrawal and hospital care. Notably, two studies have reported that phenytoin and rifampicin can be used to accelerate tacrolimus metabolism and excretion, resulting in a significant reduction in tacrolimus concentration (20, 21). Phenytoin and rifampin are potent inducers of CYP3A4 and P-glycoprotein, which can quickly reduce tacrolimus levels as antidotes (33, 34). Therefore, clinicians should consider these medications when transplant patients require hospitalization due to a severe increase in tacrolimus concentration caused by Paxlovid administration.
Similar to the findings in the general population, NR has been shown to be effective in preventing COVID-19-related hospitalization and death in SOTRs, as demonstrated by Hedvat et al. (16). Evidence has suggested that the BA.2 subvariant of Omicron is substantially more infectious than previous Omicron variants. A case series conducted by Devresse et al. (15) demonstrated the effectiveness of NR in SOTRs infected with the Omicron BA.2 variant. None of the patients required hospitalization for viral pneumonia, and the viral load of all patients had decreased substantially by day 7. These findings suggest that during the pandemic of Omicron variants, NR could be an effective treatment option for COVID-19 in SOTRs, provided that immunosuppressive regimens are properly managed.
Moreover, it is important to note that the inhibition of CYP3A by nirmatrelvir/ritonavir can also lead to potential drug interactions with other medications commonly prescribed to transplant recipients for different comorbidities. These medications include HMG-CoA reductase inhibitors (statins), azole antifungals, calcium channel blockers, and anticoagulants like warfarin, which may need to be either held or adjusted during the administration of nirmatrelvir/ritonavir therapy (26).
It is also worth mentioning that molnupiravir is an oral ribonucleoside antiviral agent that is authorized for emergency use in the outpatient treatment of mild-to-moderate COVID-19 patients within five days of symptom onset and that it does not exhibit the drug interactions observed with NR. But the MOVeOUT phase 3 trial has demonstrated a roughly 30% relative risk reduction of hospitalization or death at day 29 for patients who received molnupiravir versus placebo (35), which indicates that NR is more effective than molnupiravir. Transplant patients may experience rapid disease changes, and guidelines recommend Molnupinavir as a second-line agent (36). Therefore, most transplant physicians choose NR as their first choice.
This review has several limitations. Firstly, all studies included in this review were either case reports or case series, with only one study having a control group. Additionally, the sample sizes of the studies were limited. Secondly, most of the studies were retrospective, and the follow-up period was less than 30 days. Therefore, it is not possible to conclude that withholding CNIs is safe in terms of immunological risk and the occurrence of rejection. Thirdly, most patients in the studies received tacrolimus, with a few cases receiving cyclosporine and mTOR inhibitors. Therefore, it is difficult to draw an informative conclusion regarding the most appropriate strategy for these drugs when used with NR in transplant patients. Further clinical studies are needed to better understand the optimal use of NR in this population.
In conclusion, our analysis indicates that nirmatrelvir/ritonavir can be a promising therapeutic option for SOT recipients with COVID-19. However, careful drug adjustments and monitoring are necessary to minimize the risk of adverse effects and harm to the allograft. It is, therefore, crucial to actively monitor drug concentration levels to prevent toxicity and adjust immunosuppressive agents accordingly. Collaborative management of COVID-19 in transplant patients involving primary care providers, pharmacists, and transplant teams is essential for optimizing patient outcomes.
YT made the literature search and wrote the manuscript; YL collected the data; TS designed the study and revised the manuscript. All authors reviewed the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Worobey M, Pekar J, Larsen BB, Nelson MI, Hill V, Joy JB, et al. The emergence of SARS-CoV-2 in Europe and north America. Science (2020) 370:564–70. doi: 10.1126/science.abc8169
2. Karim SSA, Karim QA. Omicron SARS-CoV-2 variant: A new chapter in the COVID-19 pandemic. Lancet (2021) 398:2126–8. doi: 10.1016/S0140-6736(21)02758-6
3. Takashita E, Kinoshita N, Yamayoshi S, Sakai-Tagawa Y, Fujisaki S, Ito M, et al. Efficacy of antiviral agents against the SARS-CoV-2 omicron subvariant BA.2. N Engl J Med (2022) 386:1475–7. doi: 10.1056/NEJMc2201933
4. Mahase E. Covid-19: Pfizer’s paxlovid is 89% effective in patients at risk of serious illness, company reports. BMJ (2021) 375:n2713. doi: 10.1136/bmj.n2713
5. Commissioner O of the. Coronavirus. (COVID-19) update: FDA authorizes first oral antiviral for treatment of COVID-19 (2021). FDA. Available at: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-first-oral-antiviral-treatment-covid-19 (Accessed October 30, 2022).
6. Vangeel L, Chiu W, De Jonghe S, Maes P, Slechten B, Raymenants J, et al. Remdesivir, molnupiravir and nirmatrelvir remain active against SARS-CoV-2 omicron and other variants of concern. Antiviral Res (2022) 198:105252. doi: 10.1016/j.antiviral.2022.105252
7. Owen DR, Allerton CMN, Anderson AS, Aschenbrenner L, Avery M, Berritt S, et al. An oral SARS-CoV-2 mpro inhibitor clinical candidate for the treatment of COVID-19. Science (2021) 374:1586–93. doi: 10.1126/science.abl4784
8. Marzolini C, Kuritzkes DR, Marra F, Boyle A, Gibbons S, Flexner C, et al. Recommendations for the management of drug–drug interactions between the COVID-19 antiviral Nirmatrelvir/Ritonavir (Paxlovid) and comedications. Clin Pharmacol Ther (2022) 112:1191–200. doi: 10.1002/cpt.2646
9. Fishbane S, Hirsch JS, Nair V. Special considerations for paxlovid treatment among transplant recipients with SARS-CoV-2 infection. Am J Kidney Dis (2022) 79:480–2. doi: 10.1053/j.ajkd.2022.01.001
10. EMERGENCY USE AUTHORIZATION FOR PAXLOVID. Available at: https://www.fda.gov/media/155050/download (Accessed October 23, 2022).
11. Nair V, Jandovitz N, Hirsch JS, Nair G, Abate M, Bhaskaran M, et al. COVID-19 in kidney transplant recipients. Am J Transplant (2020) 20:1819–25. doi: 10.1111/ajt.15967
12. Wang AX, Koff A, Hao D, Tuznik NM, Huang Y. Effect of nirmatrelvir/ritonavir on calcineurin inhibitor levels: Early experience in four SARS-CoV-2 infected kidney transplant recipients. Am J Transplant (2022) 22:2117–9. doi: 10.1111/ajt.16997
13. Salerno DM, Jennings DL, Lange NW, Kovac DB, Shertel T, Chen JK, et al. Early clinical experience with nirmatrelvir/ritonavir for the treatment of COVID-19 in solid organ transplant recipients. Am J Transplant (2022) 22:2083–8. doi: 10.1111/ajt.17027
14. Mecadon K, Arvanitis P, Farmakiotis D, Rogers R. Single-center experience with nirmatrelvir/ritonavir in kidney transplant recipients on tacrolimus maintenance immunosuppression. Clin Transplant (2022) 36:e14752. doi: 10.1111/ctr.14752
15. Devresse A, Briol S, De Greef J, Lemaitre F, Boland L, Haufroid V, et al. Safety, efficacy, and relapse of nirmatrelvir-ritonavir in kidney transplant recipients infected with SARS-CoV-2. Kidney Int Rep (2022) 7:2356–63. doi: 10.1016/j.ekir.2022.08.026
16. Hedvat J, Lange NW, Salerno DM, DeFilippis EM, Kovac D, Corbo H, et al. COVID-19 therapeutics and outcomes among solid organ transplant recipients during the omicron BA.1 era. Am J Transplant (2022) 22:2682–8. doi: 10.1111/ajt.17140
17. Guyon J, Novion M, Fulda V, Ducint D, Molimard M, Couzi L, et al. A UPLC-MS/MS method for plasma biological monitoring of nirmatrelvir and ritonavir in the context of SARS-CoV-2 infection and application to a case. J Am Soc Mass Spectrom (2022) 33:1975–81. doi: 10.1021/jasms.2c00204
18. Berar Yanay N, Bogner I, Saker K, Tannous E. Paxlovid-tacrolimus drug-drug interaction in a 23-Year-Old female kidney transplant patient with COVID-19. Clin Drug Investig (2022) 42:693–5. doi: 10.1007/s40261-022-01180-4
19. Prikis M, Cameron A. Paxlovid (Nirmatelvir/Ritonavir) and tacrolimus drug-drug interaction in a kidney transplant patient with SARS-2-CoV infection: A case report. Transplant Proc (2022) 54:1557–60. doi: 10.1016/j.transproceed.2022.04.015
20. Rose DT, Gandhi SM, Bedard RA, Mondy KE, Chu AL, Gamble KC, et al. Supratherapeutic tacrolimus concentrations with Nirmatrelvir/Ritonavir in solid organ transplant recipients requiring hospitalization: A case series using rifampin for reversal. Open Forum Infect Dis (2022) 9:ofac238. doi: 10.1093/ofid/ofac238
21. Shah A, Nasrullah A, Butt MA, Young M. Paxlovid with caution: Novel case of paxlovid-induced tacrolimus toxicity in a cardiac transplant patient. Eur J Case Rep Intern Med (2022) 9:3528. doi: 10.12890/2022_003528
22. Lindauer KE, Hamel AG. Case report: Nirmatrelvir/Ritonavir and tacrolimus in a kidney transplant recipient with COVID-19. Am Fam Physician (2022) 105:569–70.
23. Young C, Papiro T, Greenberg JH. Elevated tacrolimus levels after treatment with nirmatrelvir/ritonavir (Paxlovid) for COVID-19 infection in a child with a kidney transplant. Pediatr Nephrol (2022). Pediatr Nephrol 38, 1387–8 doi: 10.1007/s00467-022-05712-0
24. Stawiarski K, Avery R, Strout S, Umapathi P. Risks of paxlovid in a heart transplant recipient. J Heart Lung Transplant (2022) S1053-2498(22):02106–4. doi: 10.1016/j.healun.2022.08.029
25. Mertz D, Battegay M, Marzolini C, Mayr M. Drug-drug interaction in a kidney transplant recipient receiving HIV salvage therapy and tacrolimus. Am J Kidney Dis (2009) 54:e1–4. doi: 10.1053/j.ajkd.2009.01.268
26. Lemaitre F, Grégoire M, Monchaud C, Bouchet S, Saint-Salvi B, Polard E, et al. Management of drug-drug interactions with nirmatrelvir/ritonavir in patients treated for covid-19: Guidelines from the French society of pharmacology and therapeutics (SFPT). Therapies (2022) 77:509–21. doi: 10.1016/j.therap.2022.03.005
27. Naccarato M, Kwee F, Zaltzman J, Fong IW. Ritonavir-boosted antiretroviral therapy precipitating tacrolimus toxicity in a renal transplant patient: Is it time for a priori tacrolimus dosage reduction? AIDS (2021) 35:2065–8. doi: 10.1097/QAD.0000000000003002
28. Jain AB, Venkataramanan R, Eghtesad B, Marcos A, Ragni M, Shapiro R, et al. Effect of coadministered lopinavir and ritonavir (Kaletra) on tacrolimus blood concentration in liver transplantation patients. Liver Transpl (2003) 9:954–60. doi: 10.1053/jlts.2003.50171
29. Lemaitre F. Yes we can (Use Nirmatrelvir/Ritonavir even in high immunological risk patients treated with immunosuppressive drugs)! Clin Pharmacokinet (2022) 61:1071–3. doi: 10.1007/s40262-022-01158-7
30. Stader F, Khoo S, Stoeckle M, Back D, Hirsch HH, Battegay M, et al. Stopping lopinavir/ritonavir in COVID-19 patients: duration of the drug interacting effect. J Antimicrob Chemother (2020) 75:3084–6. doi: 10.1093/jac/dkaa253
31. Lange NW, Salerno DM, Jennings DL, Choe J, Hedvat J, Kovac D, et al. Nirmatrelvir/ritonavir use: Managing clinically significant drug-drug interactions with transplant immunosuppressants. Am J Transplant (2022) 22:1925–6. doi: 10.1111/ajt.16955
32. Lemaitre F, Budde K, Van Gelder T, Bergan S, Lawson R, Noceti O, et al. Therapeutic drug monitoring and dosage adjustments of immunosuppressive drugs when combined with nirmatrelvir/ritonavir in patients with COVID-19. Ther Drug Monit (2022). Therapeutic Drug Monitoring 45(2), 191–9 doi: 10.1097/FTD.0000000000001014
33. Sharma A, Wahby KA, Inany M, Lee SJ. Use of phenytoin for treatment of tacrolimus toxicity with superimposed sepsis. BMJ Case Rep (2020) 13:e234839. doi: 10.1136/bcr-2020-234839
34. Hebert MF, Fisher RM, Marsh CL, Dressler D, Bekersky I. Effects of rifampin on tacrolimus pharmacokinetics in healthy volunteers. J Clin Pharmacol (1999) 39:91–6. doi: 10.1177/00912709922007499
35. Jayk Bernal A, Gomes da Silva MM, Musungaie DB, Kovalchuk E, Gonzalez A, Delos Reyes V, et al. Molnupiravir for oral treatment of covid-19 in nonhospitalized patients. N Engl J Med (2022) 386:509–20. doi: 10.1056/NEJMoa2116044
36. Molnupiravir. COVID-19 treatment guidelines . Available at: https://www.covid19treatmentguidelines.nih.gov/therapies/antivirals-including-antibody-products/molnupiravir/ (Accessed February 26, 2023).
Keywords: COVID-19/SARS-CoV-2, drug interaction, immunosuppressant, nirmatrelvir and ritonavir/Paxlovid, pharmacology, solid organ transplantation
Citation: Tang Y, Li Y and Song T (2023) Optimizing the use of nirmatrelvir/ritonavir in solid organ transplant recipients with COVID-19: A review of immunosuppressant adjustment strategies. Front. Immunol. 14:1150341. doi: 10.3389/fimmu.2023.1150341
Received: 24 January 2023; Accepted: 24 March 2023;
Published: 04 April 2023.
Edited by:
Mohammad Hossein Karimi, Shiraz University of Medical Sciences, IranReviewed by:
Ernesto Paoletti, San Martino Hospital (IRCCS), ItalyCopyright © 2023 Tang, Li and Song. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Turun Song, c29uZ3R1cnVuMTk4NkBzY3UuZWR1LmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.