Translating the observed differences in interleukin-6 levels between some antiretroviral regimens into potential long-term risk of serious non-AIDS events: A modeling study
 Sergio Serrano-Villar1,2*†
Sergio Serrano-Villar1,2*† Calvin Cohen3
Calvin Cohen3 Jason V. Baker4,5
Jason V. Baker4,5 Maria João Janeiro6†Filipa Aragão6,7,8†Kathleen Melbourne3Jose Luis Gonzalez9
Maria João Janeiro6†Filipa Aragão6,7,8†Kathleen Melbourne3Jose Luis Gonzalez9 Laura Lara9Connie Kim3
Laura Lara9Connie Kim3 Santiago Moreno1,2,10†
Santiago Moreno1,2,10†- 1Hospital Universitario Ramón y Cajal, Infectious Diseases, Instituto de Investigación Sanitaria Ramón y Cajal (IRYCIS), Madrid, Spain
- 2CIBERInfec, Instituto de Salud Carlos III, Madrid, Spain
- 3HIV Medical Affairs, Gilead Sciences Inc., Foster City, CA, United States
- 4Division of Infectious Diseases, Hennepin Healthcare Research Institute, Minneapolis, MN, United States
- 5Department of Medicine, University of Minnesota, Minneapolis, MN, United States
- 6Maple Health Group, New York, NY, United States
- 7Incremental Action Consulting Lda, Lisbon, Portugal
- 8NOVA National School of Public Health, Public Health Research Centre, Universidade NOVA de Lisboa, Lisbon, Portugal
- 9HIV Medical Affairs, Gilead Sciences Inc., Madrid, Spain
- 10Department of Medicine, Alcalá University, Madrid, Spain
By Serrano-Villar S, Cohen C, Baker JV, Janeiro MJ, Aragão F, Melbourne K, Gonzalez JL, Lara L, Kim C and Moreno S (2022) 13:976564. doi: 10.3389/fimmu.2022.976564
In the published article, there was an error in Tables 2 and 3 and Figures 1 and 2 as published. A formula correction was implemented in the.xlsm file containing the Markov model, leading to changes to the previously reported results. The corrected Tables 2 and 3 and Figures 1 and 2 and their captions appear below.
FIGURE 1
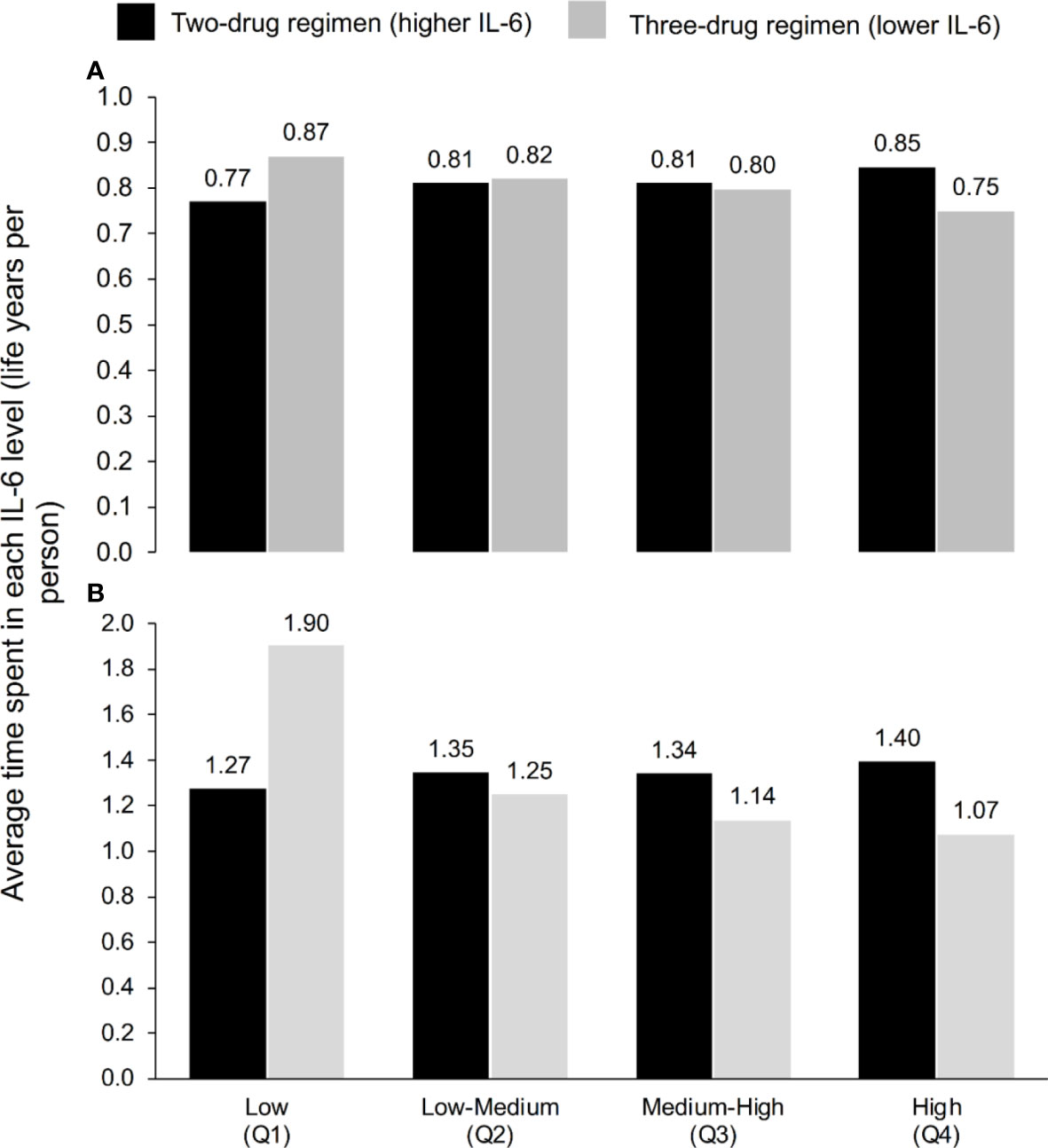
Figure 1 Average time spent in each IL-6 quartile according to ART regimen at (A) 3 years and (B) 5 years, according to the model, which used the IL-6 trajectories seen in TANGO (n=741, up to Week 144) and AIR (n=148, Weeks 144–240).
FIGURE 2
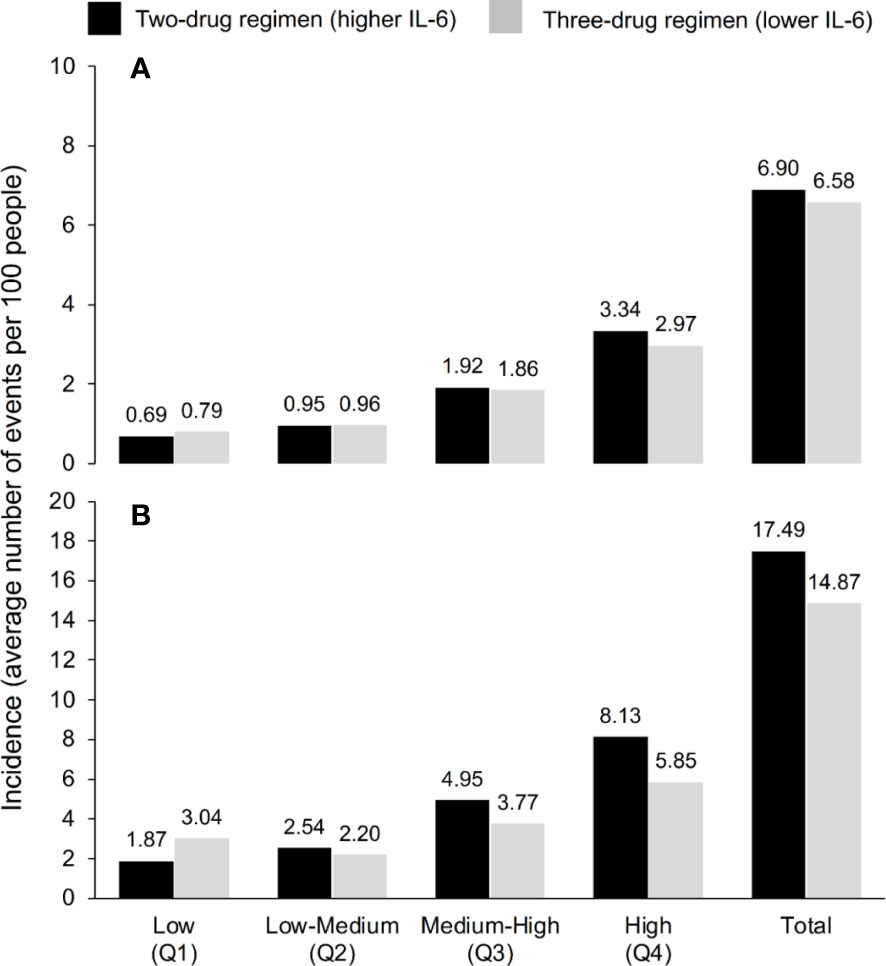
Figure 2 Incidence of serious non-AIDS events (cardiovascular, hepatic or renal event, or malignancy) or all-cause death according to IL-6 quartile and ART regimen over (A) 3 years and (B) 5 years, according to the model, which used the IL-6 trajectories seen in TANGO (n=741, up to Week 144) and AIR (n=148, Weeks 144–240).
TABLE 2
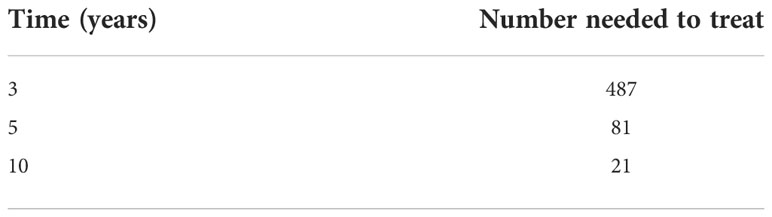
Table 2 Number needed to treat to observe one additional serious non-AIDS event (cardiovascular, hepatic or renal event, or malignancy) or all-cause death, with the two-drug ART regimen versus the three-drug regimen, by time on ART.
TABLE 3
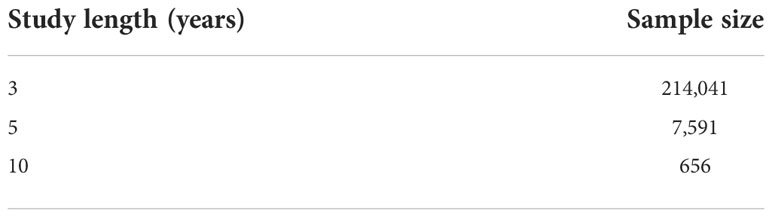
Table 3 Estimated sample size required for a clinical study designed to support or refute the results of the Markov modeling.
Corrections have also been made to the Abstract, Results, Paragraph 1. This paragraph previously stated:
“Over 144 weeks, PWH on one of the three-drug regimens studied were predicted to spend 22% more time in the low IL-6 quartile and 13% less time in the high IL-6 quartile compared with those on one of the two-drug regimens. Over 144 weeks, the predicted mean number of SNAEs/deaths per 100 PWH was 5.6 for a three-drug regimen associated with lower IL-6 levels versus 6.8 for a two-drug regimen associated with higher IL-6 levels. The number needed to treat for one additional SNAE/death among PWH receiving a two-drug versus three-drug regimen for 240 weeks was 43. Approximately 2,900 participants would be required for a 240-week clinical study to evaluate the accuracy of the model.” The corrected paragraph appears below:
“Over 3 years, PWH on one of the three-drug regimens studied were predicted to spend 13% more time in the low IL-6 quartile and 11% less time in the high IL-6 quartile compared with those on one of the two-drug regimens. Over 3 years, the predicted mean number of SNAEs/deaths per 100 PWH was 6.58 for a three-drug regimen associated with lower IL-6 levels versus 6.90 for a two-drug regimen associated with higher IL-6 levels. The number needed to treat for one additional SNAE/death among PWH receiving a two-drug versus three-drug regimen for 3 years was 81. Approximately 7,500 participants would be required for a 5-year clinical study to evaluate the accuracy of the model.”
A correction has been made to the Results, IL-6 trajectories from the Markov model, Paragraph 1. This sentence previously stated: “Within a time horizon of 144 weeks, PWH maintained on the three-drug ART regimens that were associated with lower IL6 levels (‘lower IL-6’ regimen) were predicted to spend 22% more time in the low IL-6 quartile and 13% less time in the high IL-6 quartile than those switching to a two-drug ART regimen associated with higher IL-6 levels (‘higher IL-6’ regimen) (Figure 1A).” The corrected sentence appears below:
“Within a time horizon of 3 years, PWH maintained on the three-drug ART regimens that were associated with lower IL6 levels (‘lower IL-6’ regimen) were predicted to spend 13% more time in the low IL-6 quartile and 11% less time in the high IL-6 quartile than those switching to a two-drug ART regimen associated with higher IL-6 levels (‘higher IL-6’ regimen) (Figure 1A).”
Corrections have been made to the Results, Model-predicted SNAE/death rates and NNT, Paragraph 2.
(1) This sentence previously stated:
“When all four IL-6 quartiles were combined, the predicted mean number of SNAEs/deaths per 100 PWH was 5.6 for continuous treatment with lower IL-6 compared with 6.8 with higher IL-6 (Figure 2).” The corrected sentence appears below:
“When all four IL-6 quartiles were combined, the predicted mean number of SNAEs/deaths per 100 PWH was 6.58 for continuous treatment with lower IL-6 compared with 6.90 with higher IL-6 (Figure 2).”
(2) This sentence previously stated: “Results for the 240-week timeframe based on adding the 148 AIR study participants followed the same pattern, and the predicted mean numbers of SNAEs/deaths per 100 PWH were 11.9 and 15.8 for the three- and two-drug regimens, respectively.” The corrected sentence appears below:
“Results for the 5-year timeframe based on adding the 148 AIR study participants followed the same pattern, and the predicted mean numbers of SNAEs/deaths per 100 PWH were 14.87 and 17.49 for the three- and two-drug regimens, respectively.”
(3) This sentence previously stated: “Based on these results, we calculated that for every 43 PWH treated for 240 weeks after switching to the two-drug regimen, there could be one additional SNAE/death as a consequence of higher IL-6, based on the association of IL-6 values and clinical outcomes from the INSIGHT studies.” The corrected sentence appears below:
“Based on these results, we calculated that for every 81 PWH treated for 5 years after switching to the two-drug regimen, there could be one additional SNAE/death as a consequence of higher IL-6, based on the association of IL-6 values and clinical outcomes from the INSIGHT studies.”
Corrections have been made to the Results, Clinical trial size required to validate model-predicted results, Paragraph 1. (1) This sentence previously stated: “On this basis, 2,906 participants would be required for a study with a 240-week treatment period. Variations in the sample size according to the study duration are shown in Table 3.” The corrected sentence appears below:“On this basis, 7,591 participants would be required for a study with a 5-year treatment period. Variations in the sample size according to the study duration are shown in Table 3." (2) This sentence previously stated: “For example, a total of almost 10,000 patients would be needed for a 240-week study with a three- versus two-drug regimen ratio of 2:1.”The corrected sentence appears below:“For example, a total of almost 8,500 patients would be needed for a 5-year study with a three- versus two-drug regimen ratio of 2:1.”The authors apologize for these errors and state that they do not change the scientific conclusions of the article in any way. The original article has been updated.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Keywords: antiretroviral, HIV, inflammation, interleukin-6, Markov, three-drug regimen, two-drug regimen
Citation: Serrano-Villar S, Cohen C, Baker JV, Janeiro MJ, Aragão F, Melbourne K, Gonzalez JL, Lara L, Kim C and Moreno S (2023) Corrigendum: Translating the observed differences in interleukin-6 levels between some antiretroviral regimens into potential long-term risk of serious non-AIDS events: A modeling study. Front. Immunol. 14:1148980. doi: 10.3389/fimmu.2023.1148980
Received: 20 January 2023; Accepted: 07 February 2023;
Published: 16 February 2023.
Edited and Reviewed by:
Jean-Pierre Routy, McGill University, CanadaCopyright © 2023 Serrano-Villar, Cohen, Baker, Janeiro, Aragão, Melbourne, Gonzalez, Lara, Kim and Moreno. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sergio Serrano-Villar, c2VyZ2lvLnNlcnJhbm9Ac2FsdWQubWFkcmlkLm9yZw==
†ORCID: Sergio Serrano-Villar, orcid.org/0000-0002-5447-3554
Maria João Janeiro, orcid.org/0000-0003-4794-866X
Filipa Aragão, orcid.org/0000-0003-3446-6725
Santiago Moreno, orcid.org/0000-0002-2843-1094