 Yan-hao Wei†
Yan-hao Wei† Yan-mei Qiu
Yan-mei Qiu Chun-lin Zhang
Chun-lin Zhang Ya-nan Li
Ya-nan Li Bo Hu
Bo Hu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol. , 02 June 2023
Sec. Multiple Sclerosis and Neuroimmunology
Volume 14 - 2023 | https://doi.org/10.3389/fimmu.2023.1141387
This article is part of the Research Topic The Immune Microenvironment Landscape in Cerebrovascular Diseases View all 7 articles
Ischemic stroke is a highly complex systemic disease characterized by intricate interactions between the brain and gastrointestinal tract. While our current understanding of these interactions primarily stems from experimental models, their relevance to human stroke outcomes is of considerable interest. After stroke, bidirectional communication between the brain and gastrointestinal tract initiates changes in the gastrointestinal microenvironment. These changes involve the activation of gastrointestinal immunity, disruption of the gastrointestinal barrier, and alterations in gastrointestinal microbiota. Importantly, experimental evidence suggests that these alterations facilitate the migration of gastrointestinal immune cells and cytokines across the damaged blood-brain barrier, ultimately infiltrating the ischemic brain. Although the characterization of these phenomena in humans is still limited, recognizing the significance of the brain-gastrointestinal crosstalk after stroke offers potential avenues for therapeutic intervention. By targeting the mutually reinforcing processes between the brain and gastrointestinal tract, it may be possible to improve the prognosis of ischemic stroke. Further investigation is warranted to elucidate the clinical relevance and translational potential of these findings.
Stroke represents a significant global burden in terms of mortality and disability. It is currently ranked as the second leading cause of death and the third leading cause of disability worldwide (1). Stroke can be categorized into two major types: ischemic stroke (IS) and hemorrhagic stroke. IS occurs when cerebrovascular diseases disrupt blood supply to the brain, leading to ischemic hypoxic necrosis in brain tissues. Consequently, a cascade of inflammatory reactions occurs, causing damage to the brain and the blood-brain barrier (BBB) during the early stages of IS. This process establishes major channels of communication between the brain and the gastrointestinal tract (GT), initiating frequent interactions and contributing to a poor prognosis of stroke.
In clinical practice, current treatments for ischemic stroke primarily involve thrombolysis and embolectomy. However, each treatment modality comes with its own specific requirements. Intravenous thrombolysis necessitates the administration of recombinant tissue plasminogen activator (rtPA) within a strict time window of 4.5 hours from the onset of stroke symptoms. On the other hand, mechanical thrombectomy is indicated for patients with large artery occlusion who can undergo the procedure within 6 hours of symptom onset (2). However, some patients experience poor treatment outcomes and prognoses (3, 4). Therefore, there is an urgent need to explore novel therapeutic strategies.
In recent years, there has been a growing interest in understanding the bidirectional communication and interaction between the brain and GT following ischemic stroke, leading to the emergence of the concept known as the gut-brain-microbiota axis (GBMA). Multiple animal experiments and clinical evidence now suggest that there is mutual communication and interaction between the post-stroke brain and GT (5–10).
Stroke can lead to complications such as impaired intestinal barrier function, microbiota translocation, and post-stroke infections, while cellular debris and brain-derived antigens activate the intestinal immune system (5, 11). The activated immune cells and cytokines then infiltrate the ischemic brain, exacerbating stroke injury and perpetuating a vicious cycle that culminates in a significant deterioration of stroke prognosis (5, 11).
Therefore, closely monitoring the post-stroke crosstalk between the brain and GT is crucial for identifying potential therapeutic strategies that can terminate this vicious cycle, ultimately leading to improved stroke prognosis. This review aims to provide a comprehensive overview of the crosstalk between the brain and GT following ischemic stroke, elucidate the underlying mechanisms by which the brain and GT interact to worsen stroke outcomes, and discuss potential therapeutic strategies that may enhance stroke prognosis.
After a stroke, brain tissues experience ischemia and hypoxia, leading to cellular edema and neuronal dysfunction. If blood supply is not promptly restored, brain cells will undergo irreversible damage, resulting in the death of brain tissues. Even when blood supply is quickly restored, an increase in reactive oxygen species (ROS) and free radicals during reperfusion can over-activate the inflammatory response, causing secondary brain injury and further activation of local immune cells, which leads to inflammation in the brain tissues (12). The occurrence and progression of local inflammation in the ischemic brain then contribute to the expansion of the infarct and the recruitment of central microglia and peripheral immune cells, resulting in a more robust inflammatory response (13–15).
The GBMA, proposed in recent years, refers to a bidirectional regulatory axis comprising the brain, GT, and gastrointestinal microbiota (GM). Numerous studies have demonstrated the significant impact of GBMA on the pathophysiological processes of IS (16). For example, research suggests that stroke can rapidly induce dysbiosis in the gastrointestinal microbiota, which, in turn, exacerbates brain infarction. This bidirectional relationship between gut dysbiosis and stroke highlights the intricate interplay between the gut and the brain (11).
The script of GBMA after stroke encompasses three main subjects:
The brain as the main subject: On the one hand, ischemic brain tissues after stroke produce local neuroinflammation (12). The activation of matrix metalloproteinases (MMPs) and the increase in ROS lead to the disruption of the BBB, facilitating the outward migration of damage-associated molecular patterns (DAMPs), injured brain-secreted antigens, exosomes, and the inward migration of peripheral immune cells (17). On the other hand, the brain receives various signals after stroke onset, which affect the homeostasis of the gastrointestinal microenvironment. These effects include increased gastrointestinal permeability and alterations in the composition and translocation of gastrointestinal microbiota, mediated by neurotransmission (18), neuroendocrine (19), and other mechanisms.
The gastrointestinal immune system as the main subject: On the one hand, the GT serves as a vital immune organ, housing a significant number of immune cells that account for more than 70% of the entire immune system. Therefore, it acts as a crucial source of recruited immune cells in the ischemic brain tissue (20).
Immune cells in the GT, activated by DAMPs, injured brain-secreted antigens, and exosomes, release a plethora of cytokines. Subsequently, these immune cells and cytokines migrate through the damaged BBB and infiltrate the ischemic brain tissues, facilitated by chemokines, exacerbating neuroinflammation (21). On the other hand, the activation of gastrointestinal immunity can also affect the homeostasis of the gastrointestinal microenvironment (22).
The gut microbiota as the main subject: On the one hand, the translocation of gastrointestinal microbiota intensifies the degree of systemic inflammation, thereby significantly worsening patient prognosis (23, 24). Furthermore, the composition of gastrointestinal microbiota is closely linked to risk factors for stroke (5). On the other hand, the presence of gastrointestinal microbiota has specific effects on gastrointestinal immune cells (25).
In conclusion, the interaction among these three subjects initiates after ischemic stroke, involving a complex interplay of various pathophysiological events (Figure 1). While certain processes can contribute to a detrimental cycle, such as the activation of inflammatory cascades, it’s also important to note that protective immune subpopulations play a role in promoting tissue recovery after the injury. Therefore, the overall impact of these interactions on stroke outcomes is multifaceted and involves both detrimental and protective elements. Understanding and modulating these interconnected processes may hold the key to improving the prognosis associated with ischemic stroke.
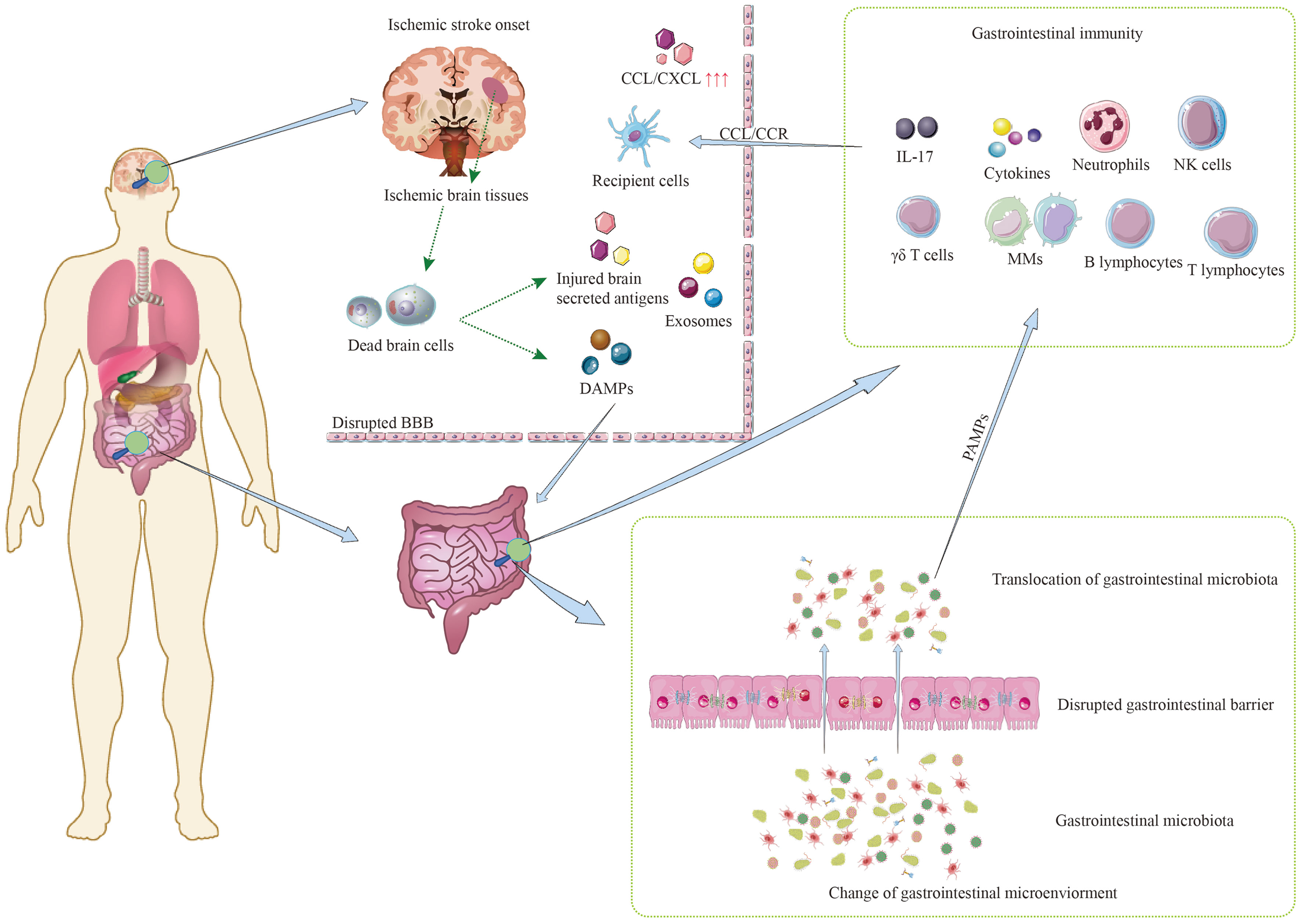
Figure 1 Mutual communication among three main subjects after ischemic stroke.
GBMA is a bidirectional communication system composed of the brain, GT, and GM. Three components of the bidirectional communication system interact and participate in the occurrence, development, and prognosis of IS. The mechanisms of interaction between the brain and GT are as follows (Figure 2).

Figure 2 The mechanisms of interaction between the brain and gastrointestinal tract.
The neurotransmission within the GBMA is primarily mediated by the enteric nervous system (ENS), the autonomic nervous system (ANS), and the vagus nerve (VN). The central nervous system (CNS) integrates information from the brain and spinal cord and transmits signals to the ENS and various gastrointestinal cells, including smooth muscle cells, blood vessels, and gland cells, through the ANS or neuroendocrine pathways. These inputs of signals modulate gastrointestinal motility, permeability, innate immune cell activation, secretion of the GT, and composition of the gastrointestinal microbiota (26). For example, brain injury after stroke causes sympathetic stimulation of the cecum to release norepinephrine, which is accompanied by a decrease in mucin secretion (27). Changes in sympathetic nerve activity can also lead to changes in cecal bacterial communities, and the degree of changes is correlated with the severity of brain injury (27). In the post-stroke mice, the total neuron and nerve fiber numbers were not unchanged compared with the sham group, but the ratio of adrenergic neurons to cholinergic neurons was elevated after IS, suggesting a misbalance between adrenergic and cholinergic signaling within the submucosal plexus in the GT following IS (18). In addition, the elevated levels of catecholamines in the GT after IS are associated with damage of the gastrointestinal mucosal barrier (18). These findings suggest that post-stroke alterations in adrenergic and cholinergic signals received by the ENS, resulting in the damage of gastrointestinal microenvironment.
Moreover, the ENS interacts with both the GT endocrine and immune systems and plays a critical role in nutrient absorption and guaranteeing the integrity of the mucosal barrier (18). Additionally, the ENS includes the myenteric plexus and submucosal plexus, which integrate and process various gastrointestinal signals and directly transmit the information to the CNS via the VN (28). Furthermore, some studies show that the VN is also the primary way for the gastrointestinal microbiota to affect the function and metabolism of CNS.
The activation of the hypothalamic-pituitary-adrenal (HPA) axis, a critical neuroendocrine system, occurs in response to vagal afferent fibers during stroke, triggering the release of cortisol from the adrenal cortex (19). Currently, there is insufficient evidence to substantiate the hypothesis that elevated cortisol levels directly cause an ecological imbalance in the gastrointestinal tract in the context of stroke. However, stress can enhance intestinal permeability through mast cell activation mediated by corticotropin-releasing hormone (CRH) (29). Additionally, the HPA axis, via stimulation of β-adrenergic receptors of sympathetic nervous system (SNS), increases gastrointestinal permeability, promotes the generation of Th17 cells in the GT and bring about alterations in the gastrointestinal microbiota composition in the context of stressful stimuli (30, 31). These changes in gastrointestinal permeability and microbiota composition trigger the release of inflammatory mediators, including pro-inflammatory cytokines, microbial antigens, and prostaglandins, capable of crossing the BBB and activating the HPA axis (32). These findings suggest that the HPA axis offers bidirectional communication in the GBMA. However, further research is needed to validate the association between HPA axis activation and gastrointestinal ecological imbalance following stroke. Moreover, it remains to be elucidated whether stroke acts as a stressor that initiates a stress response, subsequently leading to HPA axis activation, or if stroke directly triggers HPA axis activation.
Enterochromaffin cells (ECs), specialized cells found in the gastrointestinal tract, play a crucial role in the secretion of 5-hydroxytryptamine (5-HT), a multifunctional molecule (33). Acting upon G protein-coupled receptors (GPCRs) of gastrointestinal cells, 5-HT influences various aspects such as gastrointestinal secretion, motility, permeability, and inflammation (33). Although 5-HT cannot directly penetrate the BBB to exert an impact on the brain, it modulates the VN and contributes to gastrointestinal inflammation (34). Additionally, a few specialized bacterial and gastrointestinal metabolites, such as γ-aminobutyric acid, deoxycholic acid, and tyramine, have been found to induce the synthesis and secretion of 5-HT by stimulating GPCR5 of ECs (35).
Ischemic brain tissues release DAMPs, injured brain-secreted antigens, and exosomes, which activate microglia, leading to increased production of pro-inflammatory cytokines and chemokines, as well as recruitment and infiltration of immune cells into the ischemic brain (36). These DAMPs, antigens, exosomes, and pro-inflammatory cytokines cross the disrupted BBB and enter the peripheral circulation. Then elevated levels of DAMPs and pro-inflammatory cytokines in circulation contribute to increased gastrointestinal permeability, leading to the translocation of gastrointestinal microbiota and the development of gastrointestinal dysbiosis (26, 37). Furthermore, DAMPs, injured brain-secreted antigens (38, 39), and exosomes (40, 41) activate the immune cells in the GT, triggering peripheral immune reactions. Moreover, gastrointestinal innate immune cells, such as neutrophils, monocyte macrophages (MMs), natural killer (NK) cells, and γ-δ T cells, respond rapidly and utilize the CCR-CCL pathways to cross the BBB and infiltrate ischemic brain tissues within hours (42, 43).Then these immune cells cause local and systemic inflammatory and immune reactions (37, 44). The activated immune cells produce inflammatory mediators that recruit additional immune cells, further exacerbating neuroinflammation (21). The progression of neuroinflammation leads to worsened brain tissue damage and increased release of DAMPs, injured brain-secreted antigens, and exosomes into the peripheral circulation, thereby exacerbating the deterioration of the gastrointestinal microenvironment.
Additionally, the translocation of gastrointestinal microbiota into the circulation generates pathogen−associated molecular patterns (PAMPs), which activate pattern−recognition receptors (PRRs) and trigger bacterial inflammation and immune reactions (45, 46). In an animal experiment, all mice with middle cerebral artery occlusion (MCAO) developed spontaneous bacterial infection after three days, with > 95% of the cultured bacteria identified as E. coli, while no signs of pneumonia were observed in the sham-operated group, ruling out surgical stress as a trigger (47). Another study detected lipopolysaccharide (LPS) in ischemic brain tissue following stroke (48). These findings suggest that PAMPs begin to mediate bidirectional communication of GBMA during the non-acute phase after stroke. Therefore, it can be concluded that prior to gastrointestinal dysbiosis and GM translocation, inflammatory and immune reactions are solely mediated by DAMPs. Initial inflammatory activation caused by DAMPs is acute and first to occur during brain damage. However, following GM translocation, both DAMPs and PAMPs contribute to the inflammatory and immune reactions (45, 46). Furthermore, as a protective mechanism for the brain, systemic immunosuppression (SIS) occurs quickly and involves the SNS, VN, and HPA axis. However, the protective mechanism also facilitates the exacerbation of inflammatory responses after GM translocation.
Gastrointestinal bacterial metabolites influence GBMA by binding to gastrointestinal receptors and parenteral receptors as well as intervening in the three pathways mentioned above.
Short-chain fatty acids (SCFAs) are a class of crucial gastrointestinal bacterial metabolites that significantly impact stroke pathophysiology by modulating systemic and intracerebral immune cells. Multiple studies have confirmed that SCFAs readily cross the BBB and exerts effects on post-stroke recovery by influencing immune cells within the brain and the entire body (49–51). SCFAs may exert their effects through the following mechanisms: (1) SCFAs, a kind of inhibitor of histone deacetylases, act on the immune cells by blocking histone deacetylation to influence gene expression (52, 53). For example, HDAC inhibition with SCFAs downregulated IL-17 expression and increased the production of Foxp3+, CD4+, and CD25+, which induced the proliferation of CD4+ and Tregs and promoted neuroprotection after IS (54–56). (2) SCFAs work as signaling molecules binding to the GPCR of immune cells’ surface to activate immune cells. Binding of SCFAs to the GPR41/43 of ECs and phagocytes in the GT leads to the rapid production of cytokines and chemokines, mediating systemic inflammation (57). Additionally, SCFAs decrease IL-6 and IL-8 production by activating endothelial cells through acting on the GPR41/43, exerting anti-inflammatory effects of activated (58). (3) SCFAs contribute to strengthening the gastrointestinal mucosal barrier by regulating mucus secretion from gastrointestinal epithelial cells and repairing injured intestinal mucosa through increased expression of tight junction proteins, thereby decreasing the GM translocation (59, 60). (4) SCFAs activate the SNS by binding to GPR41 of sympathetic neurons, crossing the BBB and affecting the neural signaling and neurotransmitter production (49, 61). (5) SCFAs promote the expression of the tryptophan hydroxylase 1 (TPH1) gene in ECs, leading to increased secretion of 5-HT, which impacts gastrointestinal motility, permeability, and inflammation (33, 62). These findings highlight the critical role of SCFAs in the immunomodulation, post-stroke pathophysiology, and recovery.
LPS, a primary component of the gram-negative bacterial outer membranes, is an inflammatory stimulus that triggers immune responses through toll-like receptors (TLR) activation, thereby contributing to gastrointestinal dysbiosis (48). There is study have shown the presence of LPS in ischemic brain tissues, neurons, and microglia following stroke, with the higher levels of TLR4 (LPS receptor) and inflammatory cytokines in the ischemic brain tissues compared to control groups (63). Therefore, LPS may enter the blood circulation and ischemic brain tissues by crossing the disrupted gastrointestinal barrier and BBB after stroke. Furthermore, LPS induced endotoxemia exacerbates post-stroke neuroinflammation by increasing pro-inflammatory cytokines levels in the blood circulation (63). Animal experiments have indicated that TLR4 knockout may confer neuroprotective effects in mice with ischemic brain injury (64). Additionally, LPS directly activates the HPA axis by binding to TLR4 on human adrenal cells, stimulating cortisol secretion (65). Moreover, Clinical studies have shown elevated LPS levels in circulation after ischemic stroke, with high levels associated with poor short-term prognosis in stroke patients (66). Another clinical study suggests that dysbiosis of gut microbiota and elevated LPS levels increase the risk of poor functional outcomes in acute ischemic stroke patients, highlighting their potential as prognostic markers and therapeutic targets (67). These findings underscore the importance of LPS as a mediator in the interaction between GT and brain after stroke. Therefore, regulating the level of LPS may be a useful therapy for treating IS.
Aryl hydrocarbon ligands (AHLs) are another active metabolite derived from tryptophan. Intestinal epithelial cells (IECs) express the aryl hydrocarbon receptor (AHR), and AHLs activate the AHR of IECs, contributing to the renewal of gastrointestinal barrier epithelial cells, thus ensuring their integrity and normal function (68). For example, the AHR agonist FICZ reduces the damage to gastrointestinal mucosal barrier function (69). Moreover, AHLs maintains the expression and distribution of tight junction protein ZO-1 to improve the increase of intestinal permeability induced by hypoxia (69). AHLs also regulate the immune functions of gastrointestinal immune cells by acting on AHR. Microbiota-derived indoles, a type of tryptophan metabolite, act on the AHR of immune cells in the GT, inducing the production of IL-22, which is beneficial for the maintenance of gastrointestinal homeostasis (70). AHR also modulates neutrophil function and promotes the secretion of IL-17 and IL-22 (71). Tryptophan metabolites drive neuroprotection by activating the AHR of astrocytes (72). Gastrointestinal macrophages are also involved in AHR mediated maintenance of gastrointestinal epithelial integrity (73). In addition to acting locally in the GT, AHLs can also cross BBB, exerting effects on the CNS. For example, AHR expression in microglia is upregulated after IS and contributes to the development of neuroinflammation and subsequent brain parenchymal edema (74). And the use of the AHR antagonist CH223191 reduces the severity of neurological impairment (74). Although AHLs and AHR have been extensively studied in the context of gastrointestinal diseases, their role in stroke is relatively understudied, and further mechanistic research is needed.
Vitamin B12 (VB12) can be obtained from animal derived foods or can be provided by certain gastrointestinal microbiota (75). Some studies have demonstrated that exogenous VB12 supplementation stimulates the production of SCFAs by GM, indirectly involved in the effect of SCFAs on the GBMA (76). VB12 is essential for the synthesis of methionine and nucleotides. VB12 deficiency leads to the accumulation of homocysteine, promoting atherogenesis and the risk of ischemic stroke. Homocysteine accumulation alters immune homeostasis, promoting inflammation, inducing MCP-1 and IL-8 secretion, and enhances endotoxin-induced activation monocytes by activating nuclear factor κ B (77, 78). Additionally, VB12 deficiency hinders the recovery of neurological function after ischemic stroke due to the decrease nucleotide synthesis (79).
Besides the aforementioned microbial metabolites, various other gastrointestinal microbiota-derived metabolites, such as γ-aminobutyric acid, norepinephrine, tyramine, and dopamine, participate in the communication between the brain and GT by acting directly on brain cells or indirectly through interactions with vagal afferent fibers. In conclusion, gastrointestinal bacterial metabolites play a crucial regulatory role in the post-stroke immune system. A deeper understanding of the gastrointestinal microbiota and their metabolites is required to develop a novel therapeutic strategy for stroke treatment.
Dysbiosis occurs in the GT following ischemic stroke due to various mechanisms mentioned previously, including increased gastrointestinal permeability resulting from disruption of the gastrointestinal barrier, translocation and alteration of the gastrointestinal microbiota, post-stroke infections, and other GT complications.
The GT encompasses three key entities: the gastrointestinal barrier, gastrointestinal microbiota, and the mucosal immune system. The gastrointestinal barrier and the mucosal immune system consist of many immune cells and lymphoid tissues, which protect the normal tissues of GT from pathogenic microorganisms (80). The gastrointestinal barrier has the critical physiological function that separates normal gastrointestinal tissues from toxic luminal contents (81). Among the components influencing the permeability of the gastrointestinal barrier, intercellular junctional complexes play a significant role. These complexes tightly connect intestinal epithelial and endothelial cells and are highly dynamic regions. Various external and intracellular stimuli, bacterial toxins, cytokines, hormones, and drugs, can impact the permeability of intercellular junctional complexes (82, 83).
Numerous studies have reported that activating the SNS and HPA axis increases gastrointestinal permeability after IS (5, 27, 84). Both young and old mice subjected MCAO exhibited a significant increase in gastrointestinal vascular and epithelial permeability from 90 minutes to 24 hours post-stroke, with aged mice demonstrating more pronounced intestinal leakage (23). This could be associated with the decreased distribution of ZO-1, a tight junction protein in the GT. For example, the research carried out by Stanley et al. revealed a quantitative decrease in ZO-1 expression in the stroke group compared to the sham group, indicating damage to the gastrointestinal barrier and the increase in gastrointestinal permeability (18). However, it is unclear whether stroke will affect other intestinal tight junctions, such as occludin, vascular endothelial cadherin, β-catenin, and junctional adhesion molecule-A (85). Additionally, certain gastrointestinal bacterial metabolites as mentioned earlier, also influence in the gastrointestinal barrier. For example, bacterial-derived indole enhances epithelial tight junction integrity and reduces inflammation (86). Moreover, stroke affects the composition and metabolic activity of the gastrointestinal microbiota, potentially compromising the function of gastrointestinal epithelial cells, thereby influencing their structure and function and increasing gastrointestinal permeability and translocation of GM (87). For example, the reduction of intestinal goblet cells, crucial for intestinal homeostasis, may impair the formation of the intestinal mucus barrier and promote the translocation of intestinal microbiota (88).
In conclusion, stroke disrupts the function of the gastrointestinal barrier, allowing harmful substances to cross the gastrointestinal mucosa, enter the bloodstream, and eventually reach the brain through the damaged BBB, thereby exacerbating stroke prognosis. Therefore, protecting gastrointestinal barrier function following stroke might represent a potential target for improving stroke prognosis.
The gastrointestinal tract harbors a complex community of over 1000 species of commensal microbiota (89). After the gastrointestinal barrier is damaged, the gastrointestinal microbiota and toxic luminal contents cross the damaged gastrointestinal barrier into the circulation, potentially serving as the source of systemic inflammation or systemic inflammatory response syndrome (90). Moreover, increasing evidence from experimental and clinical studies suggest that IS can induce alterations in the composition of gastrointestinal microbiota (Table 1). Various clinical studies and animal experiments have observed a decrease in the abundance of bacteria responsible for SCFAs production in the intestine to varying degrees (5, 8, 93, 94). For example, the occurrence of dysbiosis in the gastrointestinal microbiota following stroke has been well-documented. It involves a disruption in the balance of microbial populations, characterized by decreased beneficial bacteria and an overgrowth of potentially harmful bacteria (11). However, the precise molecular mechanisms underlying the changes in intestinal microbial composition have yet to be elucidated.
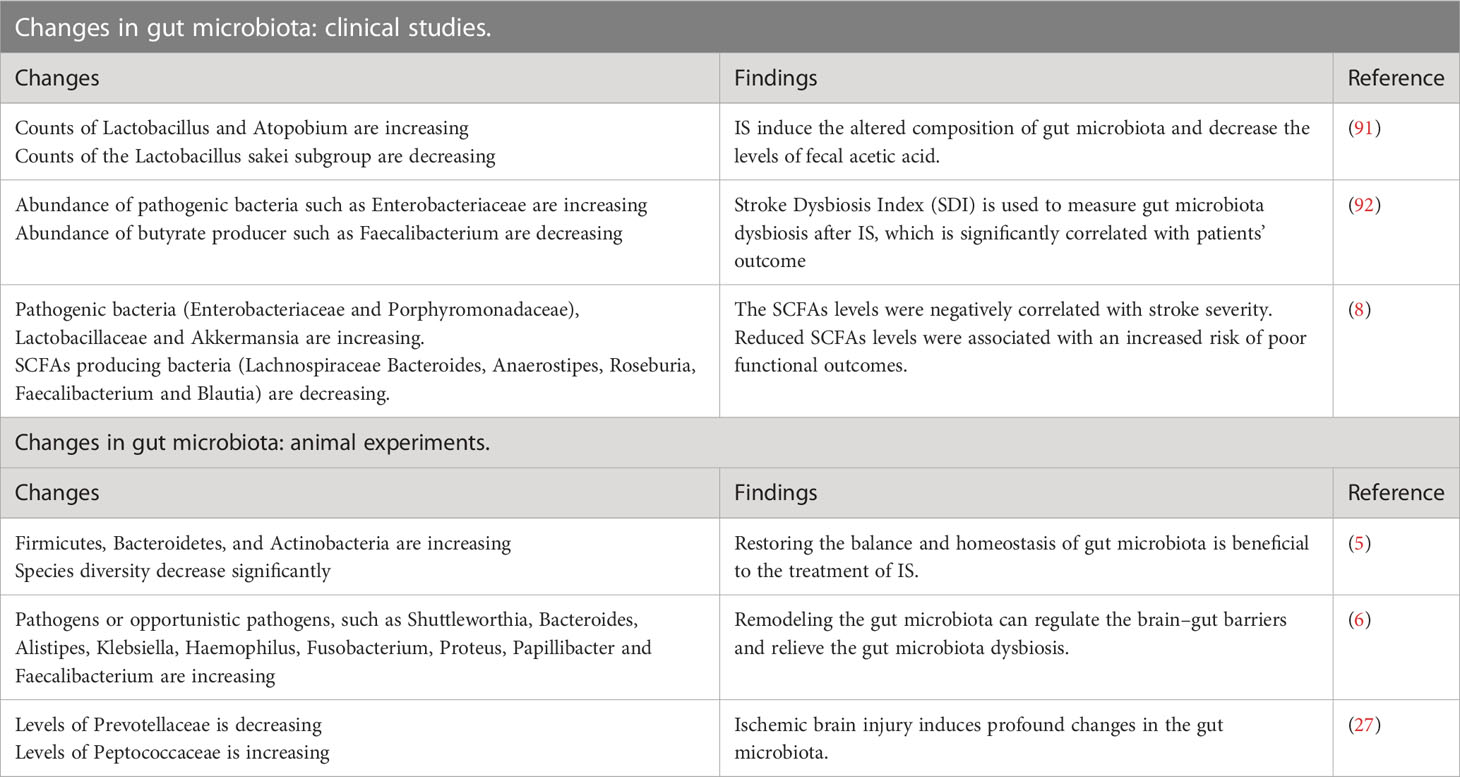
Table 1 Changes of gastrointestinal microbiota in the clinical studies and animal experiments.
Gastrointestinal bacteria translocate into the blood circulation following disruption of the gastrointestinal barrier. Subsequently, these bacteria have the potential to invade normal sterile tissues and internal organs via the bloodstream, giving rise to gut-derived sepsis and infections at various sites (24, 95). Moreover, individuals who have experienced ischemic stroke are more susceptible to post-stroke infections, which can be attributed to the systemic immunosuppressed state (96). The systemic immunosuppression (SIS) manifests approximately 24 hours after stroke onset and characterized by decreased levels of lymphocytes and NK cells, and increased levels of anti-inflammatory cytokines in the peripheral circulation (97). The underlying mechanisms of SIS are thought to involve complex pathways, including the SNS, VN, and HPA axis, through which CNS communicates with the peripheral immune system (97, 98). The occurrence of SIS at 24 hours post-stroke, accompanied by a significant reduction in circulating lymphocyte count, may contribute to an increased risk of infections (99). Indeed, post-stroke infectious complications are frequently observed in stroke cases, with pneumonia and urinary tract infections being the most common, and pneumonia has been shown to significantly contribute to mortality after stroke (18, 100). Notably, many of the detected common infecting microbes following stroke are gastrointestinal commensal bacteria, indicating that the translocation of gastrointestinal microbiota after stroke may play a role in post-stroke infections (Figure 3) (18). In addition to the abovementioned complications, many other gastrointestinal complications may occur, such as dysphagia, incontinence, constipation, gastrointestinal bleeding, and deep vein thrombosis (101–104).
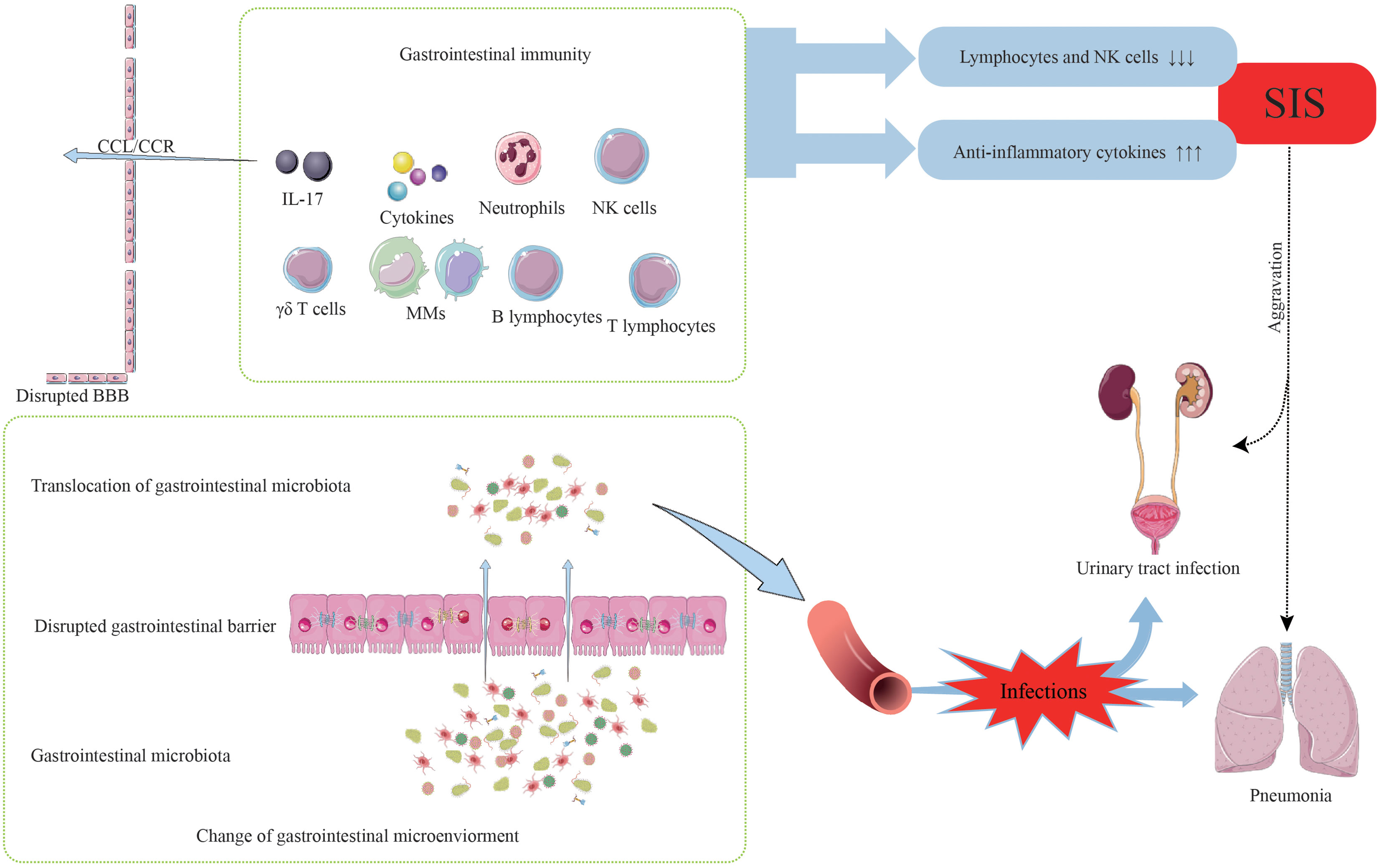
Figure 3 The occurrence of post-stroke infections.
In summary, stroke disrupts the original balance between the CNS and the gastrointestinal immune system, thereby resulting in the occurrence and development of post-stroke infection. The mechanisms underlying post-stroke infections require further investigation. Protecting the gastrointestinal barrier function from damage, promoting its recovery following stroke, and impeding the migration of harmful microbiota across the damaged barrier are important directions for future efforts.
After stroke, there is evidence suggesting the disruption of the gastrointestinal barrier, translocation of gastrointestinal microbiota (GM), and activation of the gastrointestinal immune system, which may simultaneously impact the pathophysiological development of ischemic stroke and related risk factors. It is important to note that the supporting evidence primarily stems from experimental studies, and while some studies have provided corroborative results, there may be variability among the findings. Therefore, a critical examination of the existing evidence and its implications is warranted. Next, the effect of the GT on IS will be discussed from three aspects.
Ischemic brain tissues release DAMPs, often resulting in altered gastrointestinal immune homeostasis. Altered gastrointestinal immune homeostasis regulate the neuroinflammatory response via the communication between CNS and gastrointestinal immune cells as well as cytokines (105).
DAMPs take the lead to activate the innate immune response in the early stage of IS, followed by the release of brain-derived antigens, leading to adaptive immunity. Immune cells such as neutrophils, monocytes/macrophages (MMs), natural killer (NK) cells, and lymphocytes are recruited from the gastrointestinal tract to the ischemic brain tissues after IS, where they become activated and participate in post-stroke inflammation. Neutrophils, the earliest responders, enter the brain rapidly within hours post-stroke. In the AIS patients, neutrophils were recruited to ischemic regions within twenty-four hours (106). Neutrophil infiltration into the ischemic hemisphere is followed by the release of MMP, NO, and ROS, which exacerbates disruption of BBB and leads to secondary brain injury, resulting in more immune cell infiltration (106–108). Neutrophils’ depletion with antibodies reduces the cerebral infarct volume, alleviates brain edema, and improves neurological function in the experimental IS models (109, 110). MMs migrate and infiltrate the brain via the CCL2-CCR2 axis, which also promotes secondary brain injury and neuroinflammation after IS (111). MMs in the ischemic brain tissues increase from the first day. Then they reach peaks on the third day (112). In mice, the Ly6Chigh monocyte subset is recruited into the ischemic brain by CCL2 and becomes the typically activated M1 macrophages. In contrast, the Ly6Clow monocyte subset expresses CX3CR1 and lacks CCR2 expression. This anti-inflammatory Ly6Clow monocyte subset is recruited into the ischemic brain by CX3CL1 and develops into M2 macrophages (113, 114). However, the mechanisms that regulate subsets and the timing of migrating into the ischemic brain are currently unknown. Furthermore, administration of clodronate liposomes decreases the migration of MMs into the brain, reduces the cerebral infarct volume, and promotes neurological function recovery (115). NK cells with cytotoxic functions enter the ischemic brain tissues from the GT in response to chemokines released by necrotic neurons and subsequently cause brain damage via cytotoxic effects and secreting several pro-inflammatory cytokines, such as IFN-γ and IL-17 (17, 116, 117). CD8+ T cells, cytotoxic cells which mediate many cytotoxic responses, are found in the ischemic brain tissues within three hours post-stroke (118). Subsequently, antigen-specific cells, such as CD4+ T cells and B cells, participate in the pathophysiology after stroke much later after activation by brain-derived antigens and antigen-presenting cells (APCs) (14, 119). Many studies show that T cells play a deleterious role in secondary brain damage after stroke (120–122). However, there are also other studies showing that Th2 cells exert neuroprotective effects by secreting IL-4 or brain-derived neurotrophic molecules to promote stroke recovery (123, 124). So, there is the potential to move stroke towards the good direction by switching the Th1 cell phenotype to the Th2 cell phenotype. Additionally, recent studies have shown that regulatory T cells (Tregs), a class of anti-inflammatory immune cells, are elevated following IS. Tregs account for more than 30% of colonic lamina propria CD4 T+ cells and 20% of small gastrointestinal CD4 T+ cells (125). Tregs have neuroprotective effects and improve the prognosis of IS by producing anti-inflammatory factors (126–128). For example, Tregs maintain the integrity of gastrointestinal barrier by promoting intestinal stem cells differentiation into intestinal epithelial components via secreting IL-10. On the contrary, Tregs deficiency often leads to a decreased proportion of differentiated intestinal epithelial cells (129).Next, we would like to discuss the role of one type of innate lymphocyte mainly distributed in the GT, γ-δ T cells, in stroke in detail.
γ-δ T cells make up 30% of all T cells in the GT (130). Following IS, γ-δ T cells infiltrate ischemic brain tissues and meninges and are involved in the neuroinflammation and immune responses to cerebral ischemic injury (5, 131, 132). Notably, in one study, γ-δ T cells only accumulated in the meninges, but not in regions of ischemic brain tissue, after stroke (131). However, two other studies suggested that γ-δ T cells infiltrated ischemic brain tissues. The factors responsible for this variability remain unclear (133, 134). In the experimental IS models, γ-δ T cells exacerbate the pro-inflammatory responses and contribute to poor prognosis through IL-17 production (133). Additionally, the migration of γ-δ T cells is dependent on the presence of CCR6. Genetic defects in CCR6 result in significantly reduced migration of γ-δ T cells to the ischemic brain and leptomeninges, along with improved neurological outcomes (134). Nonetheless, the precise mechanisms underlying γ-δ T cell migration require further investigation. Furthermore, γ-δ T cells exert critical effects on the brain tissue injury after IS not by themselves, but by producing all kinds of cytokines, with IL-17 being the most notable.
Small amounts of IL-17 were produced by Th17 cells, but large amounts of IL-17 are generated during acute infection by γ-δ T cells, which rapidly induces inflammation (135). IL-17 is a cytokine family that consists of six members, from IL-17A to IL-17F. IL-17A, one of the members of the IL-17 cytokine family, has been extensively studied in recent years. IL-17A starts to increase from the first day, reaches its peak on the third day, and then then gradually decrease in the experimental IS models (136). IL-17A brain endothelial cells and glial cells to secret a large amount of secretion of CXCL1 and CCL2 by binding to IL-17R up-regulated after experimental IS, thereby promoting the recruitment of immune cells (137). In addition, IL-17A aggravates neuronal ischemic brain injury by mediating excessive autophagy via the Src-PP2B-mTOR pathway (138). These findings show that IL-17A plays a pro-inflammatory effect. Interestingly, IL-17A increases again and reaches a second peak at 28 days post-stroke, mainly produced by astrocytes, and exerts beneficial effects. The effects of IL-17A may be that maintain the survival of neural precursor cells, and enhance neuronal differentiation and synapse formation, which are beneficial for functional recovery after IS (139). Consequently, further studies are required to elucidate the effects of IL-17A in IS patients and the underlying mechanisms that could be targeted for effective clinical therapies. However, it is important to note that most of the supporting evidence originates from experimental studies, and there are discrepancies and unconfirmed phenomena in human stroke. Thus, future research should focus on better clinical translation and the application of experimental findings in clinical practice.
Besides abundant immune cells, GT harbors also a complex community of commensal microbiota (89). Severe ischemic stroke disrupts the balance of the GT microbiota, leading to gastrointestinal dysbiosis. This dysbiosis triggers bacterial inflammation and immune responses in the gastrointestinal tract due to the translocation of microbiota and PAMPs into the bloodstream (11). The term “bacterial inflammation” refers to the immune system’s activation in response to the presence of gastrointestinal microbiota and their metabolites in the bloodstream, which occurs as a result of increased intestinal permeability (140). Then dysbiosis-induced inflammation and immune activation can lead to the release of pro-inflammatory cytokines and oxidative stress, further exacerbating brain injury (11). Additionally, the bacterial inflammation disrupts the gastrointestinal immune homeostasis and further leads to gastrointestinal dysbiosis and more ectopic bacteria. Consequently, ectopic gastrointestinal bacteria and many immune cells enter ischemic brain tissues through the damaged BBB, exacerbating ischemic brain injury (141). Moreover, IS-induced gastrointestinal dysbiosis increase the infiltration of γ-δ T cells from GT into the meninges and ischemic brain (131, 142). The accumulation of γ-δ T cells leads to secret more IL-17, further inducing ischemic brain tissues injury (142). Animal experiments involving the transplantation of fecal matter from ischemic stroke mice into sterile mice have shown that the transplanted feces lead to greater immune cell infiltration, increased cytokine expression in the ischemic brain tissues, and larger cerebral infarction size compared to sterile mice not receiving fecal transplantation (5, 143). This suggests that immune system activation triggered by post-stroke microbiota translocation may result in excessive immune cell activation and subsequent migration to ischemic brain tissue. In addition, gastrointestinal bacteria translocate into the blood circulation following disruption of the gastrointestinal barrier. Subsequently, intestinal bacteria will invade normal sterile tissues and internal organs along with the blood stream, potentially causing gut-derived sepsis and infections at various sites (24, 95). Severe infections occurring either early or late after ischemic stroke are associated with an increased risk of death and poorer prognosis, independent of treatment and baseline characteristics (144). Therefore, it is crucial to actively repair the damaged gastrointestinal barrier after stroke to prevent further deterioration of the gastrointestinal microenvironment, halt the mutually reinforcing processes, decrease the incidence of post-stroke infections, and improve stroke prognosis. Meanwhile, close monitoring the blood composition in stroke patient is also important to prevent post-stroke infectious complications. For example, in a clinical study, researchers found that the red cell distribution width-albumin (RA) ratio predicted stroke-related infections and mortality in stroke patients (145). Moreover, although prophylactic antibiotics don’t improve functional outcomes versus mortality, they significantly reduce the overall risk of infections, particularly urinary tract infections (94, 146).
The development of risk factors for ischemic stroke (IS) is influenced by various complex factors, including the gut microbiota (GM). In particular, GM has been found to impact several key risk factors associated with IS.
GM and hypertension: Hypertension, a common risk factor of IS, has a critical induction effect on IS and is closely related to the prognosis of IS (147, 148). Studies have revealed that GM metabolites regulate blood pressure (BP) levels. SCFAs modulate vasodilation of intestinal vessels to affect BP by binding with GPR41 (57, 149). Conversely, hypertension affects the composition of GM, leading to significant alterations and imbalances. The abundance of gastrointestinal microbiota decreased significantly and was unbalanced in the animals and humans with hypertension (149, 150). Additionally, hypertension is associated with decreased levels of tight junction proteins in the gastrointestinal tract, resulting in the increased permeability of the gastrointestinal barrier (151). Trimethylamine oxide (TMAO), a metabolite of gut microbiota, affects BP by prolonging the duration of angiotensin II action and increasing water reabsorption via the TMAO-AVP-AQP-2 signaling pathway (152, 153). Increased TMAO levels in the patient’s circulation are closely correlated with the elevated levels of CD14 + and CD16 + pro-inflammatory monocyte, which may contribute to an increased risk of cardiovascular events (154).
GM and hyperlipidemia: Hyperlipidemia are associated with increased occurrence of cardiovascular events and poor stroke prognosis. The interplay between GM and cholesterol levels has been observed, with specific GM taxa such as Erysipelotrichaceae, Bacteroides, Alistipes, and Pasteurella positively correlating with plasma cholesterol levels (155). Hyperlipidemia also influences peripheral inflammatory and immune responses. Hyperlipidemia increases the generation of hematopoietic progenitors from the bone marrow, leading to an increase in the population of MMs and neutrophils in the peripheral circulation (156). Ly6Chigh proinflammatory monocytes are observed in hyperlipidemic mice (157). Moreover, hyperlipidemia regulates lymphocyte functions. For example, LDL uptake by APCs stimulates naive T cells to differentiate into Th1 cells while reducing the activity of anti-inflammatory Th2 cells (158). In addition to affecting inflammation and immune responses, hyperlipidemia affects tissue repair and remodeling processes by influencing the clearance of pathogens and injured tissues (158).
GM and atherosclerosis: Recent studies have shown that elevated levels of TMAO have been associated with the probability and severity of cardiovascular events (159, 160). Moreover, the level of TMAO is also related to the size of atherosclerotic plaque (161). This shows that microorganisms, TMAO and atherosclerosis have a certain relationship, but at present, little is known about the specific molecular mechanism of how TMAO mediates atherosclerosis. Some studies have found that DNA of bacteria is found in atherosclerotic plaque. The bacteria also exist in gastrointestinal microorganisms, suggesting a potential role of gut microorganisms in the development of atherosclerosis (162). Recent clinical trials have demonstrated significant changes in the composition of GM after stroke, particularly an increase in the proportion of harmful opportunistic pathogens in individuals with atherosclerosis (9).
GM and diabetes: Patients with diabetes have a high incidence of stroke and a generally poor prognosis (163). Altered GM composition contributes to changes in insulin levels and insulin resistance by interfering with the insulin signaling pathway (164). Animal experimental studies suggested that acetate might reduce the frequency of autoreactive T cells in lymphoid tissues of diabetic mice. In contrast, butyrate increases the number and promotes the function of Tregs by inhibiting HDAC9 and increasing the key gene transcription of Tregs (165). Dietary interventions involving butyrate and acetate have shown beneficial effects on GM integrity, Treg numbers, and cytokine levels (165). Moreover, diabetes disrupts the balance of T cell differentiation, leading to an increased proportion of pro-inflammatory Th1 and Th17 cells, while reducing the proportion of anti-inflammatory Th2 cells and Tregs (166, 167).
GM and aging: Aging is an inevitable risk factor for stroke, and elderly individuals have a higher mortality rate following stroke, regardless of the extent of brain damage (168). Compared with healthy young adults, the gastrointestinal microbiota of the elderly is significantly changed (169). The gastrointestinal microbiota of the elderly significantly differs from that of healthy young adults, with a decline in diversity, decreased abundance of commensal bacteria, and an increase in potentially harmful pathogens. These changes may contribute to gastrointestinal inflammation and disruption of immune homeostasis (170, 171). Moreover, recent study has provided evidence indicating that in elderly individuals, the deterioration of intestinal barrier function contributes to the increased translocation of bacteria from the gut, thereby heightening the risk of bacterial infection following stroke (172). Additionally, aging downregulates innate and adaptive immunity upon CNS injury. Aging reduces phagocytic activities of MMs, chemotaxis of neutrophils, and cytotoxicity of NK cells (23, 173–175). T and B lymphocytes also undergo alterations in the number and function, and the differentiation of memory B cells into plasma cells is impaired in older individuals (176, 177).
GM and micronutrient deficiencies: Micronutrient supplementation for stroke prevention has been extensively studied, but the results have been inconclusive in terms of safety and efficacy (178–181). Some studies have suggested a potential reduction in the risk of ischemic stroke with certain vitamin supplementation. However, the underlying mechanisms by which vitamins exert their protective effects against stroke risk remain uncertain (182).
In conclusion, the interplay between GBMA and these risk factors has a significant impact on the occurrence and development of stroke. Therefore, active secondary prevention strategies should be implemented following stroke to halt further deterioration, improve prognosis, and reduce the likelihood of recurrence. It is equally important to consider the influence of GBMA on stroke risk factors, not only focusing on post-stroke changes in the gastrointestinal microenvironment, but also monitoring and managing alterations in gastrointestinal microbiota and function before a stroke occurs. Further exploration of pre-stroke gastrointestinal management and interventions is necessary to better understand and proactively address changes in the gastrointestinal microenvironment prior to stroke onset.
In recent years, the role of the brain gut axis after stroke has become a research hotspot, therefore, clinical evidence of the crosstalk between the post-stroke brain and the GM and gastrointestinal immune system has gradually increased (Table 2). After stroke, the probability of intestinal dysfunction in patients increased sevenfold (186). Some fecal samples from acute ischemic stroke patients all suggest that opportunistic pathogens from the patient’s gut show a variable degree of enrichment and decrease in the abundance of SCFA producing bacteria (8, 9, 93, 185). These alterations appear to increase the risk of adverse functional outcomes.
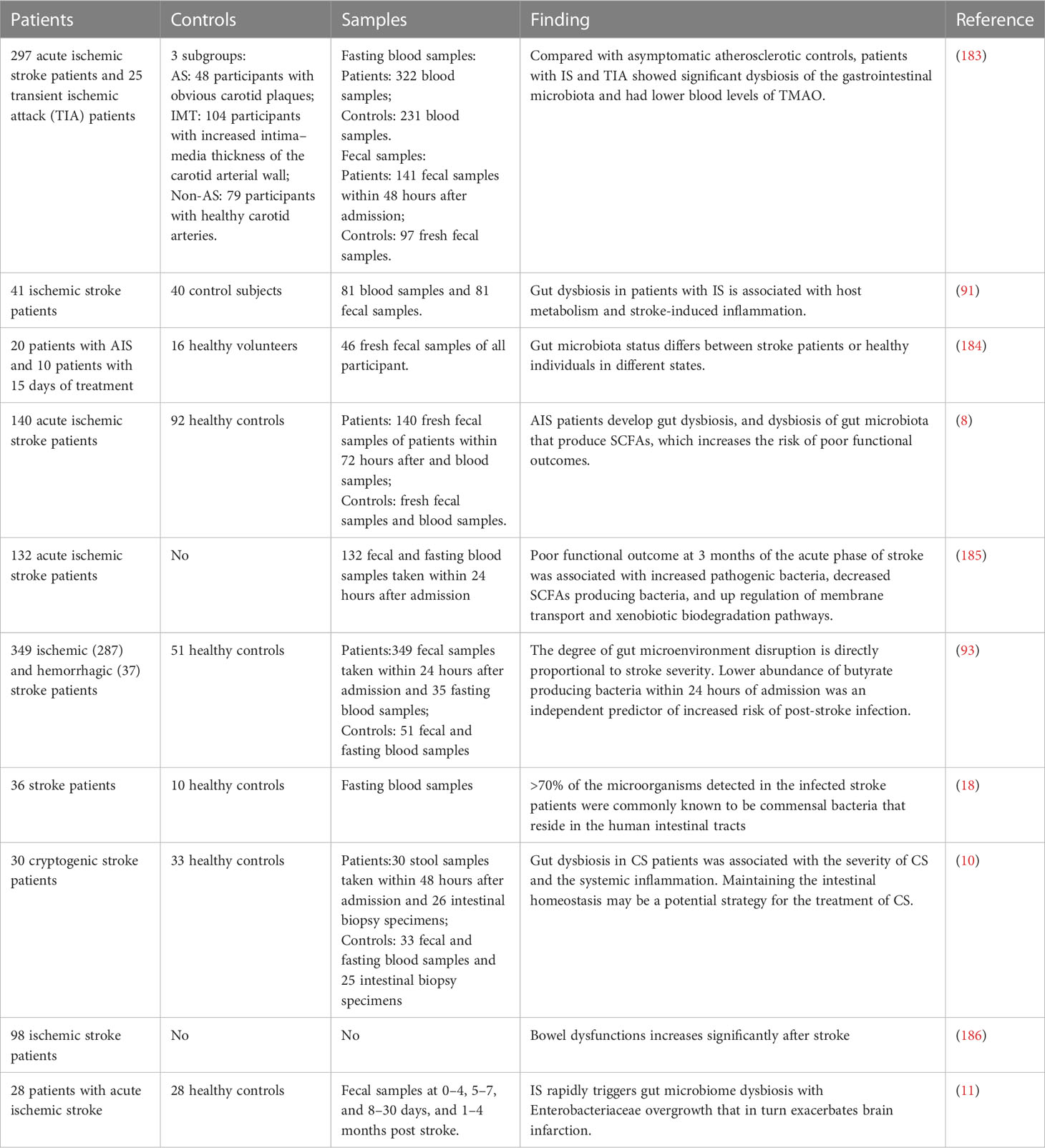
Table 2 Summary of clinical evidence about brain and GT interactions after stroke.
In a clinical study, it was observed that stroke patients generally exhibit increased levels of plasma c-reactive protein (CRP), lipopolysaccharide (LPS), LPS-binding protein, and white blood cell counts. These findings suggest the presence of a systemic inflammatory response in stroke patients. Additionally, the prevalence of gastrointestinal disorders, gastrointestinal inflammation, and gastrointestinal permeability was found to be higher in a group of 26 stroke patients compared to the control group of 25 healthy individuals. These results indicate a close association between gastrointestinal disorder in stroke patients, stroke severity, and systemic inflammation. However, it is important to note that this clinical study had limitations due to the small number of subjects included (10).
Another clinical study indicates that a higher abundance of opportunistic pathogens and a lower abundance of butyrate producing bacteria are observed in the GM of individuals at high risk of stroke relative to low-risk healthy individuals (187). In another clinical study, researchers separately collected data on the GM of 16 healthy people, 20 patients with stroke, and 10 patients treated for 15 days after acute cerebral infarction, hoping to reach the goal of diagnosing ischemic stroke by identifying the characteristics of the microbiota (184). When considering these two clinical studies together, it suggests that the microbiota of individuals at high risk of stroke may be undergoing insidious changes slowly compared to healthy individuals. The onset of stroke acts as a triggering point that rapidly amplifies this gradual process, leading to a significant alteration in the gastrointestinal microenvironment. This amplification process occurs through a positive feedback mechanism of crosstalk between the brain and the GT, wherein the three components mutually reinforce each other, thereby exacerbating the prognosis of stroke. Of course, this at the same time provides novel therapeutic strategies based GBMA, where we can stop the aggravation of IS by interrupting the positive feedback effect among three components.
After IS, communication between CNS and the GT occurs through various pathways, including SNS, PNS, ENS, and HPA axis. Certain drugs can be used to modulate this crosstalk by targeting proteins and receptors involved in the brain-gut communication and inhibiting nerve conduction.
Following IS, there is an imbalance between gastrointestinal adrenergic signaling and cholinergic signaling, with a shift towards increased adrenergic signaling and reduced cholinergic signaling (18). Adrenergic signaling has been associated with systemic immunosuppression after stroke, which increases the risk of post-stroke infections (188, 189). On the other hand, reduced cholinergic signaling promotes proinflammatory immune responses (189, 190). Therefore, the application of drugs blocking adrenergic receptors or stimulating cholinergic receptors may be a viable approach to prevent the formation of positive feedback. For example, the use of β-adrenergic receptor blockers has been shown to significantly decrease bacterial presence in the lungs, liver, and spleen of stroke mice (18). However, the effects of post-stroke β-adrenergic receptor blocker therapy on stroke treatment outcomes have shown variability (Table 3). Therefore, in the clinical application of β-blockers for stroke treatment, careful consideration of the timing of administration is necessary to counteract the systemic immunosuppressive effects induced by SNS activation and enhance the immune response to prevent post-stroke infections.
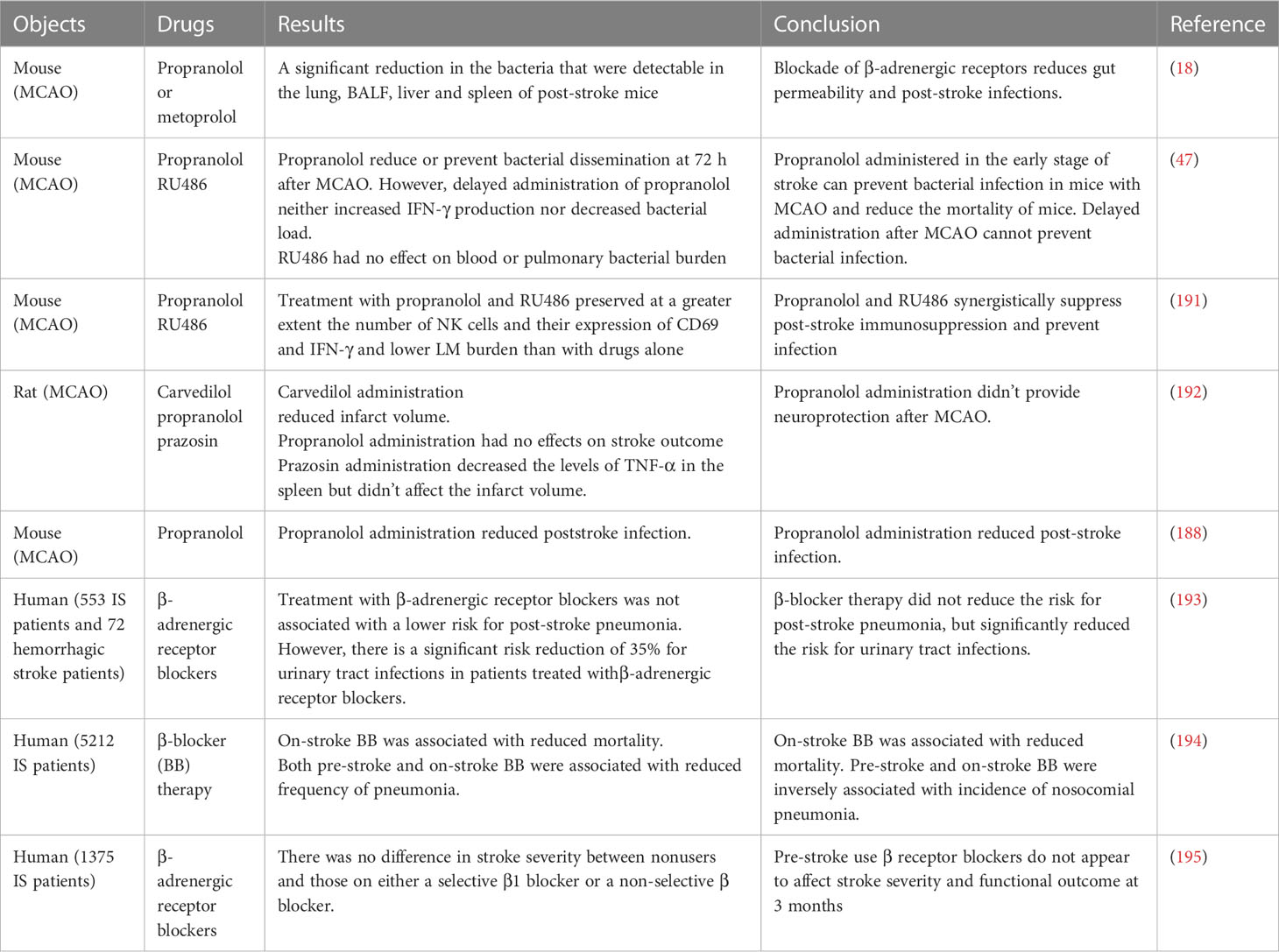
Table 3 Some relevant researches on the application of receptor blockers after stroke.
In the context of traumatic brain injury, enhancement of cholinergic signaling prevents increases in gastrointestinal and cerebrovascular permeability (196, 197). The mechanism has not been demonstrated in the ischemic stroke. However, a study suggests that targeted vagus nerve stimulation can have complex effects in reducing neuroinflammation (198). Moreover, the release of acetylcholine (Ach) is enhanced by electrical stimulation of the VN, which acts on α7 nicotinic acetylcholine receptors of macrophages to inhibit the release of proinflammatory cytokine, such as TNF and attenuate the serum TNF response induce by LPS after stroke-induced GM translocation (199). CNI-1493, an anti-inflammatory agent, causes deactivation of macrophages and inhibits the synthesis of pro-inflammatory mediators. Intracerebroventricular injection of CNI-1493 after IS inhibits TNF synthesis in the brain. However, the inhibitory effect of CNI-1493 on LPS induced TNF synthesis was counteracted when VN conduction was disrupted through surgery or the application of atropine (200, 201). When considering the translation of research findings to clinical applications, the process of using drugs to interrupt positive feedback might be feasible in the course of future clinical studies. However, it is crucial to focus on the development of more precise receptor blockers or agonists and to carefully consider the timing of drug administration. Additionally, completely cutting off nerve conduction is not a feasible approach, but these findings have important implications for the potential treatment of stroke and warrant further investigation in clinical settings.
The gastrointestinal microbiota, immune cells, and cytokines are interconnected components within the complex network of post-stroke inflammation. Dysbiosis of the gastrointestinal microbiota following stroke can initiate immune cell activation and subsequent release of pro-inflammatory cytokines, exacerbating neuroinflammation. Numerous animal experiments have highlighted the potential therapeutic strategy of targeting immune cells and cytokines to modulate the inflammatory response and mitigate neuroinflammation in stroke. Antibody-mediated neutrophil depletion has shown promising effects in experimental ischemic stroke, including reductions in cerebral infarct volume, alleviation of brain edema, and improvement in neurological function (109, 110). Likewise, the use of clodronate liposomes, which effectively reduce monocyte-derived macrophages (MMs) by 80%, has resulted in decreased migration of MMs into the brain, decreased cerebral infarct volume, and facilitated recovery of neurological function (115). Blockade of T cell infiltration through the use of immunosuppressants such as FTY720 or the targeted elimination of γ-δ T cells and IL-17 T lymphocytes in the brain using TCRγδ during the subacute stage of cerebral infarction has shown improved outcomes in ischemia-reperfusion injury (133). However, it is important to consider the potential impact of targeting immune cells on the overall immune function of the post-stroke organism, as this can affect the occurrence and development of post-stroke infection. For example, reducing blood neutrophils may increase the risk of post-stroke infection due to the presence of post-stroke systemic inflammatory response syndrome (SIS). Clinical studies have found that impaired neutrophil function is associated with the development of post-stroke infection, but further research is needed to determine whether neutropenia influences the development of post-stroke infection in the context of post-stroke immunosuppression (202). Therefore, additional studies are required to investigate the feasibility of targeting immune cells for post-stroke therapy and to support risk assessment of post-stroke infection in clinical practice.
Following immune system activation triggered by stroke, certain immune cells play a neuroprotective role. Regulatory T cells (Tregs) contribute to neuroprotection by maintaining immune homeostasis and balancing the release of anti-inflammatory and pro-inflammatory factors. Modulating the number and functions of Tregs has been identified as a potential therapeutic approach. For instance, pretreatment with resveratrol has been shown to increase Treg production and accumulation before stroke onset, offering partial protection to ischemic brain tissues (203). Furthermore, modulating the gastrointestinal microbiota presents a promising approach to influence immune cell activation after stroke. Achieving gastrointestinal microecological homeostasis through fecal microbiota transplantation (FMT) increases the number of Tregs, which primes a protective immune response after stroke (143). Another group of immune cells, known as regulatory B cells (Bregs), also exhibit neuroprotective effects by suppressing inflammatory responses and modulating immunity. Pretreatment with lipopolysaccharide (LPS) increases Bregs populations in post-stroke mice, leading to the attenuation of inflammatory response and neurological damage. Specifically, the expansion of marginal zone B cells and follicular B cells in mice is associated with these neuroprotective effects (204). In addition to the aforementioned experiments, various other immune cells and cytokines can serve as potential therapeutic targets, as detailed in Table 4. While the precise mechanisms and optimal therapeutic targets are still being elucidated, targeting immune cells and cytokines holds promise as a therapeutic approach for attenuating neuroinflammation and promoting post-stroke recovery. It is important to note that there is still a considerable gap between experimental research and clinical translation, requiring further investigation and validation.
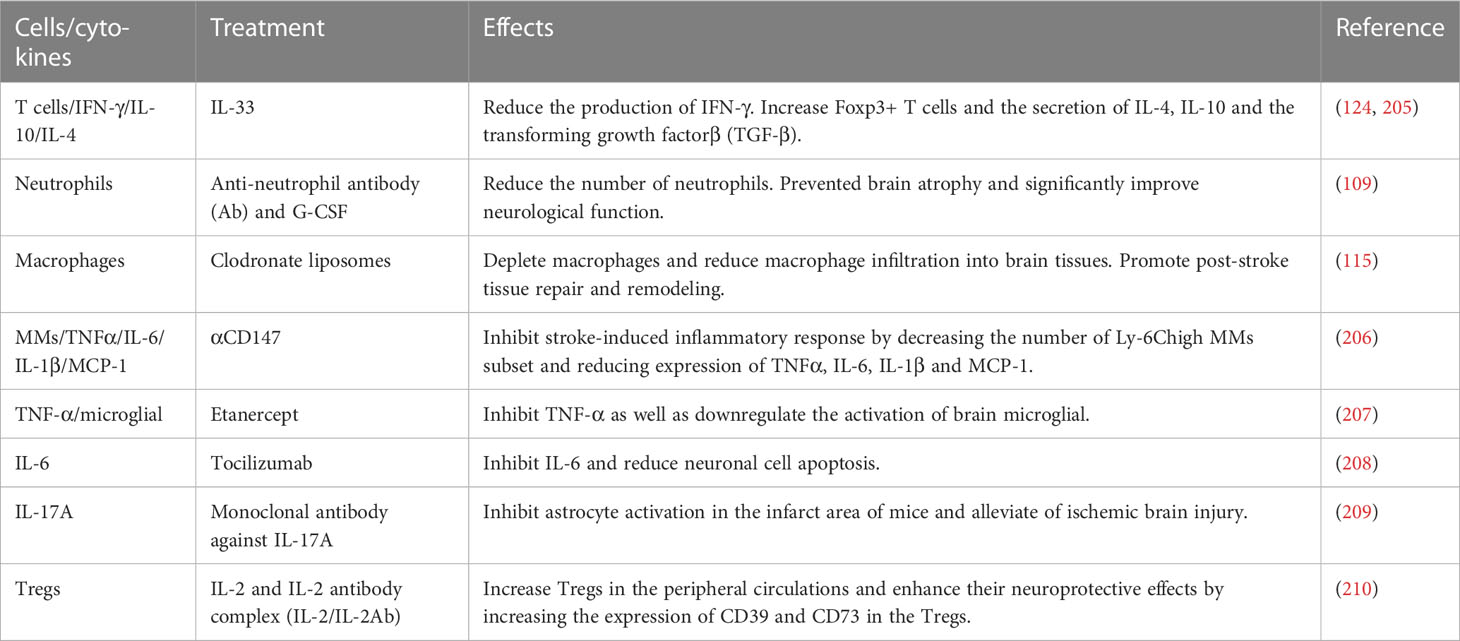
Table 4 Treatment of ischemic stroke with immune cells or cytokines as targets.
After IS, gastrointestinal dysbiosis occurs, leading to the translocation and alteration of the gastrointestinal microbiota, which can significantly influence the severity of brain damage. Therefore, correcting dysbiosis in acute ischemic stroke (AIS) patients through fecal microbiota transplantation (FMT) appears to be a feasible strategy to restore gastrointestinal (GT) homeostasis (211, 212). Notably, FMT enriched with SCFAs has shown positive effects on cerebral ischemia in experimental IS models by remodeling the gastrointestinal microbiota, enhancing the abundance of beneficial Lactobacillus species, and improving the gastrointestinal microenvironment (213). In severe stroke patients, the gastrointestinal microbiota undergoes significant changes following stroke, contributing to immune homeostasis disturbances. FMT has demonstrated considerable improvements in outcomes and survival rates among these severe IS patient (5). It is important to acknowledge that, like any medical intervention, FMT carries potential adverse effects such as nausea, vomiting, abdominal discomfort, low-grade fever, flatus, and alterations in bowel habits, which are generally self-limiting in nature (214). The underlying mechanisms through which FMT improves the outcome of IS remain largely unknown, although it is generally believed that restoration of intestinal homeostasis plays a pivotal role. Further research is necessary to elucidate the specific mechanisms involved. Additionally, individualized characteristics of the gastrointestinal microbiota should be taken into consideration. It is plausible that there may be differential alterations in the gastrointestinal microbiota among individuals after stroke, necessitating tailored treatment regimens based on individual differences at the time of intervention. Furthermore, given that the gastrointestinal microbiota may also contribute to disease, careful selection of appropriate healthy FMT donors is of utmost importance.
Probiotics are live microorganisms that, when administered in adequate doses, confer health benefits on the host. Prebiotics’ definition is selectively used substrates by host microorganisms, which are beneficial to the host’s health (215). In Section 2.4, we discussed the crucial roles of short-chain fatty acids (SCFAs) and acyl-homoserine lactones (AHLs) in the gut-brain-microbiota axis (GBMA). Numerous animal experiments and clinical studies have demonstrated that probiotic and prebiotic treatments can enhance the production of SCFAs and AHLs, indirectly influencing the prognosis of stroke. Probiotics derived from food sources, when introduced into the gastrointestinal tract (GT), increase the abundance of SCFA-producing microorganisms and promote SCFA production (216). Furthermore, probiotics have been shown to improve post-stroke gastrointestinal complications such as constipation, abdominal distension, and diarrhea (217). Daily oral administration of probiotics also rebalances the Th1/Th2 immune response and improve neuronal function in patients with severe traumatic brain injury (218). Prebiotics, specifically carbohydrates, can influence the production of SCFAs and mucin, as well as modulate the local inflammatory response of the gut-associated lymphoid tissue (GALT) (219). High amylose maize starches are used as a substrate for bacterial fermentation, which increases the production of SCFAs and fecal concentrations of acetate and butyrate (220). Supplementation with lactulose, a common prebiotic, has been shown to repair gut barrier damage, mitigate gut microbiota dysregulation, and partially improve functional outcomes after stroke e (221). Additionally, a clinical study demonstrated that the use of functional barley as a prebiotic increased the abundance of butyric acid-producing bacteria, consequently elevating butyric acid levels in the GT (222). Moreover, the combination of probiotics and prebiotics can harness the synergistic effect between the two. In an animal study, co-administration of inulin and SCFA-producing bacteria increased SCFA production and improved neurological deficit scores and behavioral outcomes in post-stroke mice compared to the administration of SCFA-producing bacteria alone (6). Another animal experiment showed that the combination of Li01 and resveratrol improved microbiota composition and metabolism, increased SCFA and AHL production, and enhanced the prognosis of colitis (223). Based on these findings, it can be hypothesized that probiotics and prebiotics may improve the prognosis of ischemic stroke patients by influencing the production of SCFAs and AHLs. In summary, probiotics and prebiotics have the potential to improve the composition of the microbiota and gastrointestinal function, thereby positively impacting the prognosis of stroke patients. While probiotic and prebiotic therapies are already being used in clinical practice for stroke treatment and secondary prevention, prospective clinical intervention trials are still needed to establish their effectiveness.
Diet plays an essential role in influencing the composition of gastrointestinal microbiota. Consuming high amounts of phosphatidylcholine and L-carnitine in the diet increases the production of trimethylamine N-oxide (TMAO), potentially raising the risk of cardiovascular event (224). Antibiotic treatment has been shown to reduce TMAO production by altering the composition of the gut microbiota, while controls without antibiotics exhibited elevated TMAO levels (154). The specific mechanisms through which ketogenic diets modulate the gastrointestinal microbiota to improve outcomes in ischemic stroke (IS) are not yet fully understood. However, several studies provide valuable insights for further exploration of the relationship between ketogenic diets, microbiota modulation, and stroke outcomes. Ketogenic diets significantly increase GABA levels in the hippocampus, which is related to the regulatory effects of gastrointestinal microbiota (225). Early intervention with ketogenic diets improves the gastrointestinal microbiota, enhances cerebrovascular function, improves metabolism, and promotes the elimination of β-amyloid, thus reducing the risk for Alzheimer’s disease (226).
There is a growing interest in understanding the impact of dietary fiber on the composition of the GM. Dietary fiber is primarily digested by Firmicutes upon entering the gastrointestinal tract, leading to increased production of SCFA (227). Animal experiments have demonstrated that adding butyric acid to the diet is effective for treating IS (228). Moreover, clinical studies have shown that short-term vegetarian diets increase the abundance of Roseburia, Ruminococcus, and butyrate-producing bacteria in the gut microbiota (229). The impact of SCFAs on post-stroke development and recovery is reviewed in detail above. Therefore, supplementing SCFAs and precursors of SCFAs in the diet may be an excellent therapeutic strategy (51). Taken together, diet therapy improves microbiota composition and intestinal function and then the prognosis of stroke patients.
The advancing research in the field has gradually unveiled the intricate crosstalk between the brain and gastrointestinal tract (GT). As previously discussed, the involvement of the gut-brain-microbiota axis (GBMA) in stroke onset and progression emphasizes the interconnectedness of these systems following a stroke. In this section, we delve deeper into the mutual crosstalk among the three components of GBMA and explore how the formation of a vicious circle contributes to a poor prognosis in stroke. However, while our understanding of the role of GBMA in stroke has expanded, the precise cellular, signaling, and molecular mechanisms underlying its influence remain to be fully elucidated. Further research is required to unravel these intricate mechanisms.
One of the unresolved aspects is the differential effects exerted by GBMA at different stages of ischemic stroke, particularly when various immune cells infiltrate the ischemic brain tissue. The specific molecular mechanisms that govern these differential effects are not yet clear. Consequently, there is an urgent need to intensify preclinical studies focusing on developing new therapies for the prevention and treatment of ischemic stroke. Additionally, the combination of potential therapeutic strategies with rtPA thrombolytic therapy has been proposed as a means to minimize post-stroke injury. However, translating the findings from animal experiments and clinical studies into clinical practice poses several challenges.
Although numerous reports have shed light on the alterations in gastrointestinal microbiota after stroke and the bidirectional communication between GBMA components, many specific molecular mechanisms remain poorly understood. For instance, while stroke leads to increased gastrointestinal permeability, it is not yet elucidated whether stroke alters the expression of critical tight junction proteins associated with gastrointestinal permeability. Furthermore, although the impact of stroke on the gastrointestinal microbiota is well-documented, the precise mechanisms underlying these alterations are still largely unexplained. We have yet to determine the molecular mechanisms through which certain bacterial metabolites affect the development and prognosis of stroke. Addressing these gaps in knowledge will require further investigations at the molecular level.
Moreover, the ultimate goal of future research is to translate the findings from basic experiments into clinical practice. The conclusions drawn from these experiments need to be applied in a clinical setting to have practical significance. However, there are numerous challenges associated with this process of clinical translation. These challenges stem from various factors, such as the complexity of the human body, the heterogeneity of stroke patients, and the limitations in conducting large-scale clinical trials. Overcoming these hurdles is crucial for successfully integrating the knowledge gained from basic research into clinical applications
In this review, we have summarized potential therapeutic strategies based on the exacerbation cycle of GBMA. However, it is important to note that translating the results of animal experiments and clinical studies into clinical practice presents its own set of difficulties. These therapeutic strategies require further validation through long-term clinical studies to determine their feasibility and efficacy. The process of discovering these intricate details and effectively translating them into clinical practice is expected to be an arduous and time-consuming endeavor.
In conclusion, the investigation of the crosstalk between the brain and gastrointestinal microbiota following stroke has provided valuable insights into the pathophysiology of stroke and potential therapeutic approaches. However, there are still many unanswered questions regarding the specific molecular mechanisms and clinical implications of GBMA in stroke. Future research efforts should focus on elucidating these mechanisms and overcoming the challenges associated with clinical translation. By doing so, we can pave the way for the development of novel therapies and interventions that have a meaningful impact on stroke prevention, treatment, and patient outcomes.
Y-HW and R-TB wrote this manuscript. BH and Y-NL designed the review and edited the manuscript. C-LZ, Y-MQ, and J-ZL provided some suggestions. All authors contributed to the article and approved the submitted version.
This work was supported by National Natural Science Foundation of China (no. 82071336 to Y-NL, no. 82090044 to BH, no. 81820108010 to BH), Natural Science Foundation of Hubei Province (no. 2020CF763 to Y-NL) and National Key R&D Program of China (no. 2018YFC1312200).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
IS, ischemic stroke; BBB, blood-brain barrier; GT, gastrointestinal tract; GBMA, gut-brain-microbiota axis; ROS, reactive oxygen species; GM, gastrointestinal microbiota; MMPs, matrix metalloproteinases; DAMPs, damage associated molecular patterns; ENS, enteric nervous system; ANS, autonomic nervous system; VN, vagus nerve; CNS, central nervous system; HPA, hypothalamic-pituitary-adrenal; SNS, sympathetic nervous system; ECs, enterochromaffin cells; 5-HT, 5-hydroxytryptamine; GPCR, G protein-coupled receptors; MMs, monocyte macrophages; PAMPs, pathogen−associated molecular patterns; PRRs, pattern−recognition receptors; SCFAs, short-chain fatty acids; TPH1, tryptophan hydroxylase 1; LPS, lipopolysaccharide; TLR, toll-like receptors; AHLs, aryl hydrocarbon ligands; IECs, intestinal epithelial cells; AHR, aryl hydrocarbon receptor; VB12, vitamin B12; MCAO, middle cerebral artery occlusion; SDI, stroke dysbiosis index; SIS, systemic immunosuppression; BP, blood pressure; TMAO, trimethylamine oxide; CS, cryptogenic stroke; TIA, transient ischemic attack; CRP, c-reactive protein; Ach, acetylcholine; FMT, fecal microbiota transplantation.
1. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet (2020) 396(10258):1204–22. doi: 10.1016/S0140-6736(20)30925-9
2. Rabinstein AA. Update on treatment of acute ischemic stroke. Continuum (Minneap Minn) (2020) 26(2):268–86. doi: 10.1212/CON.0000000000000840
3. Roaldsen MB, Jusufovic M, Berge E, Lindekleiv H. Endovascular thrombectomy and intra-arterial interventions for acute ischaemic stroke. Cochrane Database Syst Rev (2021) 6:CD007574. doi: 10.1002/14651858.CD007574.pub3
4. Gottlieb M, Meissner H, Kalina M. What is the efficacy and safety of intravenous thrombolysis and thrombectomy among patients with a wake-up stroke? Ann Emerg Med (2022) 80(2):165–7. doi: 10.1016/j.annemergmed.2022.02.013
5. Singh V, Roth S, Llovera G, Sadler R, Garzetti D, Stecher B, et al. Microbiota dysbiosis controls the neuroinflammatory response after stroke. J Neurosci (2016) 36(28):7428–40. doi: 10.1523/JNEUROSCI.1114-16.2016
6. Chen R, Wu P, Cai Z, Fang Y, Zhou H, Lasanajak Y, et al. Puerariae lobatae radix with chuanxiong rhizoma for treatment of cerebral ischemic stroke by remodeling gut microbiota to regulate the brain-gut barriers. J Nutr Biochem (2019) 65:101–14. doi: 10.1016/j.jnutbio.2018.12.004
7. Lee J, d’Aigle J, Atadja L, Quaicoe V, Honarpisheh P, Ganesh BP, et al. Gut microbiota-derived short-chain fatty acids promote poststroke recovery in aged mice. Circ Res (2020) 127(4):453–65. doi: 10.1161/CIRCRESAHA.119.316448
8. Tan C, Wu Q, Wang H, Gao X, Xu R, Cui Z, et al. Dysbiosis of gut microbiota and short-chain fatty acids in acute ischemic stroke and the subsequent risk for poor functional outcomes. JPEN J Parenter Enteral Nutr (2021) 45(3):518–29. doi: 10.1002/jpen.1861
9. Xu DJ, Wang KC, Yuan LB, Li HF, Xu YY, Wei LY, et al. Compositional and functional alterations of gut microbiota in patients with stroke. Nutr Metab Cardiovasc Dis (2021) 31(12):3434–48. doi: 10.1016/j.numecd.2021.08.045
10. Zheng Q, Chen Y, Zhai Y, Meng L, Liu H, Tian H, et al. Gut dysbiosis is associated with the severity of cryptogenic stroke and enhanced systemic inflammatory response. Front Immunol (2022) 13:836820. doi: 10.3389/fimmu.2022.836820
11. Xu K, Gao X, Xia G, Chen M, Zeng N, Wang S, et al. Rapid gut dysbiosis induced by stroke exacerbates brain infarction in turn. Gut (2021) 70:1486–94. doi: 10.1136/gutjnl-2020-323263
12. Bayraktutan U. Endothelial progenitor cells: potential novel therapeutics for ischaemic stroke. Pharmacol Res (2019) 144:181–91. doi: 10.1016/j.phrs.2019.04.017
13. Venkat P, Chen J, Chopp M. Exosome-mediated amplification of endogenous brain repair mechanisms and brain and systemic organ interaction in modulating neurological outcome after stroke. J Cereb Blood Flow Metab (2018) 38(12):2165–78. doi: 10.1177/0271678X18782789
14. Anrather J, Iadecola C. Inflammation and stroke: an overview. Neurotherapeutics (2016) 13(4):661–70. doi: 10.1007/s13311-016-0483-x
15. Rayasam A, Hsu M, Kijak JA, Kissel L, Hernandez G, Sandor M, et al. Immune responses in stroke: how the immune system contributes to damage and healing after stroke and how this knowledge could be translated to better cures? Immunology (2018) 154(3):363–76. doi: 10.1111/imm.12918
16. Zhao L, Xiong Q, Stary CM, Mahgoub OK, Ye Y, Gu L, et al. Bidirectional gut-brain-microbiota axis as a potential link between inflammatory bowel disease and ischemic stroke. J Neuroinflamm (2018) 15(1):339. doi: 10.1186/s12974-018-1382-3
17. Petrovic-Djergovic D, Goonewardena SN, Pinsky DJ. Inflammatory disequilibrium in stroke. Circ Res (2016) 119(1):142–58. doi: 10.1161/CIRCRESAHA.116.308022
18. Stanley D, Mason LJ, Mackin KE, Srikhanta YN, Lyras D, Prakash MD, et al. Translocation and dissemination of commensal bacteria in post-stroke infection. Nat Med (2016) 22(11):1277–84. doi: 10.1038/nm.4194
19. Bonaz B, Sinniger V, Pellissier S. Anti-inflammatory properties of the vagus nerve: potential therapeutic implications of vagus nerve stimulation. J Physiol (2016) 594(20):5781–90. doi: 10.1113/JP271539
20. Zheng D, Liwinski T, Elinav E. Interaction between microbiota and immunity in health and disease. Cell Res (2020) 30(6):492–506. doi: 10.1038/s41422-020-0332-7
21. Jian Z, Liu R, Zhu X, Smerin D, Zhong Y, Gu L, et al. The involvement and therapy target of immune cells after ischemic stroke. Front Immunol (2019) 10:2167. doi: 10.3389/fimmu.2019.02167
22. Yang Z, Wei F, Zhang B, Luo Y, Xing X, Wang M, et al. Cellular immune signal exchange from ischemic stroke to intestinal lesions through brain-gut axis. Front Immunol (2022) 13:688619. doi: 10.3389/fimmu.2022.688619
23. Crapser J, Ritzel R, Verma R, Venna VR, Liu F, Chauhan A, et al. Ischemic stroke induces gut permeability and enhances bacterial translocation leading to sepsis in aged mice. Aging (Albany NY) (2016) 8(5):1049–63. doi: 10.18632/aging.100952
24. Vaishnavi C. Translocation of gut flora and its role in sepsis. Indian J Med Microbiol (2013) 31:334–42. doi: 10.4103/0255-0857.118870
25. Huang Q, Xia J. Influence of the gut microbiome on inflammatory and immune response after stroke. Neurol Sci (2021) 42(12):4937–51. doi: 10.1007/s10072-021-05603-6
26. Carabotti M, Scirocco A, Maselli MA, Severi C. The gut-brain axis: interactions between enteric microbiota, central and enteric nervous systems. Ann Gastroenterol (2015) 28(2):203–9.
27. Houlden A, Goldrick M, Brough D, Vizi ES, Lénárt N, Martinecz B, et al. Brain injury induces specific changes in the caecal microbiota of mice via altered autonomic activity and mucoprotein production. Brain Behav Immun (2016) 57:10–20. doi: 10.1016/j.bbi.2016.04.003
28. Schroeder BO, Backhed F. Signals from the gut microbiota to distant organs in physiology and disease. Nat Med (2016) 22(10):1079–89. doi: 10.1038/nm.4185
29. Vanuytsel T, van Wanrooy S, Vanheel H, Vanormelingen C, Verschueren S, Houben E, et al. Psychological stress and corticotropin-releasing hormone increase intestinal permeability in humans by a mast cell-dependent mechanism. Gut (2014) 63(8):1293–9. doi: 10.1136/gutjnl-2013-305690
30. de Punder K, Pruimboom L. Stress induces endotoxemia and low-grade inflammation by increasing barrier permeability. Front Immunol (2015) 6:223. doi: 10.3389/fimmu.2015.00223
31. Kelly JR, Kennedy PJ, Cryan JF, Dinan TG, Clarke and N.P. Hyland G. Breaking down the barriers: the gut microbiome, intestinal permeability and stress-related psychiatric disorders. Front Cell Neurosci (2015) 9:392. doi: 10.3389/fncel.2015.00392
32. Misiak B, Loniewski I, Marlicz W, Frydecka D, Szulc A, Rudzki L, et al. The HPA axis dysregulation in severe mental illness: can we shift the blame to gut microbiota? Prog Neuropsychopharmacol Biol Psychiatry (2020) 102:109951. doi: 10.1016/j.pnpbp.2020.109951
33. Gao J, Xu K, Liu H, Liu G, Bai M, Peng C, et al. Impact of the gut microbiota on intestinal immunity mediated by tryptophan metabolism. Front Cell Infect Microbiol (2018) 8:13. doi: 10.3389/fcimb.2018.00013
34. Kaelberer MM, Buchanan KL, Klein ME, Barth BB, Montoya MM, Shen X, et al. A gut-brain neural circuit for nutrient sensory transduction. Science (2018) 361(6408):5236–43. doi: 10.1126/science.aat5236
35. Yano JM, Yu K, Donaldson GP, Shastri GG, Ann P, Ma L, et al. Indigenous bacteria from the gut microbiota regulate host serotonin biosynthesis. Cell (2015) 161(2):264–76. doi: 10.1016/j.cell.2015.02.047
36. Yamaguchi A, Jitsuishi T, Hozumi T, Iwanami J, Kitajo K, Yamaguchi H, et al. Temporal expression profiling of DAMPs-related genes revealed the biphasic post-ischemic inflammation in the experimental stroke model. Mol Brain (2020) 13(1):57. doi: 10.1186/s13041-020-00598-1
37. Wang HX, Wang YP. Gut microbiota-brain axis. Chin Med J (Engl) (2016) 129(19):2373–80. doi: 10.4103/0366-6999.190667
38. Ortega SB, Noorbhai I, Poinsatte K, Kong X, Anderson A, Monson NL, et al. Stroke induces a rapid adaptive autoimmune response to novel neuronal antigens. Discovery Med (2015) 19(106):381–92.
39. Planas AM, Gómez-Choco M, Urra X, Gorina R, Caballero M, Chamorro Á. Brain-derived antigens in lymphoid tissue of patients with acute stroke. J Immunol (2012) 188(5):2156–63. doi: 10.4049/jimmunol.1102289
40. Raposo G, Nijman HW, Stoorvogel W, Liejendekker R, Harding CV, Melief CJ, et al. B lymphocytes secrete antigen-presenting vesicles. J Exp Med (1996) 183(3):1161–72. doi: 10.1084/jem.183.3.1161
41. Montecalvo A, Shufesky WJ, Stolz DB, Sullivan MG, Wang Z, Divito SJ, et al. Exosomes as a short-range mechanism to spread alloantigen between dendritic cells during T cell allorecognition. J Immunol (2008) 180(5):3081–90. doi: 10.4049/jimmunol.180.5.3081
42. Zaremba J, Ilkowski J, Losy J. Serial measurements of levels of the chemokines CCL2, CCL3 and CCL5 in serum of patients with acute ischaemic stroke. Folia Neuropathol (2006) 44(4):282–9.
43. Shi J, Li W, Zhang F, Park JH, An H, Guo S, et al. CCL2 (C-c motif chemokine ligand 2) biomarker responses in central versus peripheral compartments after focal cerebral ischemia. Stroke (2021) 52(11):3670–9. doi: 10.1161/STROKEAHA.120.032782
44. Arya AK, Hu B. Brain-gut axis after stroke. Brain Circ (2018) 4(4):165–73. doi: 10.4103/bc.bc_32_18
45. Neher MD, Weckbach S, Flierl MA, Huber-Lang MS, Stahel PF. Molecular mechanisms of inflammation and tissue injury after major trauma–is complement the “bad guy”? J BioMed Sci (2011) 18:90. doi: 10.1186/1423-0127-18-90
46. Vourc’h M, Roquilly A, Asehnoune K. Trauma-induced damage-associated molecular patterns-mediated remote organ injury and immunosuppression in the acutely ill patient. Front Immunol (2018) 9:1330. doi: 10.3389/fimmu.2018.01330
47. Prass K, Meisel C, Höflich C, Braun J, Halle E, Wolf T, et al. Stroke-induced immunodeficiency promotes spontaneous bacterial infections and is mediated by sympathetic activation reversal by poststroke T helper cell type 1-like immunostimulation. J Exp Med (2003) 198(5):725–36. doi: 10.1084/jem.20021098
48. Kawai T, Akira S. The role of pattern-recognition receptors in innate immunity: update on toll-like receptors. Nat Immunol (2010) 11(5):373–84. doi: 10.1038/ni.1863
49. Frost G, Sleeth ML, Sahuri-Arisoylu M, Lizarbe B, Cerdan S, Brody L, et al. The short-chain fatty acid acetate reduces appetite via a central homeostatic mechanism. Nat Commun (2014) 5:3611. doi: 10.1038/ncomms4611
50. Morrison DJ, Preston T. Formation of short chain fatty acids by the gut microbiota and their impact on human metabolism. Gut Microbes (2016) 7(3):189–200. doi: 10.1080/19490976.2015.1134082
51. Sadler R, Cramer JV, Heindl S, Kostidis S, Betz D, Zuurbier KR, et al. Short-chain fatty acids improve poststroke recovery via immunological mechanisms. J Neurosci (2020) 40(5):1162–73. doi: 10.1523/JNEUROSCI.1359-19.2019
52. Park J, Kim M, Kang SG, Jannasch AH, Cooper B, Patterson J, et al. Short-chain fatty acids induce both effector and regulatory T cells by suppression of histone deacetylases and regulation of the mTOR-S6K pathway. Mucosal Immunol (2015) 8(1):80–93. doi: 10.1038/mi.2014.44
53. Schilderink R, Verseijden C, de Jonge WJ. Dietary inhibitors of histone deacetylases in intestinal immunity and homeostasis. Front Immunol (2013) 4:226. doi: 10.3389/fimmu.2013.00226
54. Arpaia N, Campbell C, Fan X, Dikiy S, van der Veeken J, deRoos P, et al. Metabolites produced by commensal bacteria promote peripheral regulatory T-cell generation. Nature (2013) 504(7480):451–5. doi: 10.1038/nature12726
55. Liesz A, Zhou W, Na SY, Hämmerling GJ, Garbi N, Karcher S, et al. Boosting regulatory T cells limits neuroinflammation in permanent cortical stroke. J Neurosci (2013) 33(44):17350–62. doi: 10.1523/JNEUROSCI.4901-12.2013
56. Smith PM, Howitt MR, Panikov N, Michaud M, Gallini CA, Bohlooly YM, et al. The microbial metabolites, short-chain fatty acids, regulate colonic treg cell homeostasis. Science (2013) 341(6145):569–73. doi: 10.1126/science.1241165
57. Kim MH, Kang SG, Park JH, Yanagisawa M, Kim CH. Short-chain fatty acids activate GPR41 and GPR43 on intestinal epithelial cells to promote inflammatory responses in mice. Gastroenterology (2013) 145(2):396–406.e1-10. doi: 10.1053/j.gastro.2013.04.056
58. Li M, van Esch B, Henricks PAJ, Folkerts G, Garssen J. The anti-inflammatory effects of short chain fatty acids on lipopolysaccharide- or tumor necrosis factor alpha-stimulated endothelial cells via activation of GPR41/43 and inhibition of HDACs. Front Pharmacol (2018) 9:533. doi: 10.3389/fphar.2018.00533
59. Willemsen LEM, Koetsier MA, van Deventer SJH, van Tol EAF. Short chain fatty acids stimulate epithelial mucin 2 expression through differential effects on prostaglandin E1 and E2 production by intestinal myofibroblasts. Gut (2003) 52(10):1442–7. doi: 10.1136/gut.52.10.1442
60. Wang HB, Wang PY, Wang X, Wan YL, Liu YC. Butyrate enhances intestinal epithelial barrier function via up-regulation of tight junction protein claudin-1 transcription. Dig Dis Sci (2012) 57(12):3126–35. doi: 10.1007/s10620-012-2259-4
61. Kimura I, Inoue D, Maeda T, Hara T, Ichimura A, Miyauchi S, et al. Short-chain fatty acids and ketones directly regulate sympathetic nervous system via G protein-coupled receptor 41 (GPR41). Proc Natl Acad Sci U.S.A. (2011) 108(19):8030–5. doi: 10.1073/pnas.1016088108
62. Reigstad CS, Salmonson CE, Rainey JF 3rd, Szurszewski JH, Linden DR, Sonnenburg JL, et al. Gut microbes promote colonic serotonin production through an effect of short-chain fatty acids on enterochromaffin cells. FASEB J (2015) 29(4):1395–403. doi: 10.1096/fj.14-259598
63. Kurita N, Yamashiro K, Kuroki T, Tanaka R, Urabe T, Ueno Y, et al. Metabolic endotoxemia promotes neuroinflammation after focal cerebral ischemia. J Cereb Blood Flow Metab (2020) 40(12):2505–20. doi: 10.1177/0271678X19899577
64. Hyakkoku K, Hamanaka J, Tsuruma K, Shimazawa M, Tanaka H, Uematsu S, et al. Toll-like receptor 4 (TLR4), but not TLR3 or TLR9, knock-out mice have neuroprotective effects against focal cerebral ischemia. Neuroscience (2010) 171(1):258–67. doi: 10.1016/j.neuroscience.2010.08.054
65. Vakharia K, Hinson JP. Lipopolysaccharide directly stimulates cortisol secretion by human adrenal cells by a cyclooxygenase-dependent mechanism. Endocrinology (2005) 146(3):1398–402. doi: 10.1210/en.2004-0882
66. Klimiec E, Pera J, Chrzanowska-Wasko J, Golenia A, Slowik A, Dziedzic T. Plasma endotoxin activity rises during ischemic stroke and is associated with worse short-term outcome. J Neuroimmunol (2016) 297:76–80. doi: 10.1016/j.jneuroim.2016.05.006
67. Jiang Z, Li L, Liu L, Ding B, Yang Y, He F, et al. Ischemic stroke and dysbiosis of gut microbiota: changes to LPS levels and effects on functional outcomes. Altern Ther Health Med (2023).
68. Stockinger B, Di Meglio P, Gialitakis M, Duarte JH. The aryl hydrocarbon receptor: multitasking in the immune system. Annu Rev Immunol (2014) 32:403–32. doi: 10.1146/annurev-immunol-032713-120245
69. Han B, Sheng B, Zhang Z, Pu A, Yin J, Wang Q, et al. Aryl hydrocarbon receptor activation in intestinal obstruction ameliorates intestinal barrier dysfunction via suppression of MLCK-MLC phosphorylation pathway. Shock (2016) 46(3):319–28. doi: 10.1097/SHK.0000000000000594
70. Zelante T, Iannitti RG, Cunha C, De Luca A, Giovannini G, Pieraccini G, et al. Tryptophan catabolites from microbiota engage aryl hydrocarbon receptor and balance mucosal reactivity via interleukin-22. Immunity (2013) 39(2):372–85. doi: 10.1016/j.immuni.2013.08.003
71. Chen F, Cao A, Yao S, Evans-Marin HL, Liu H, Wu W, et al. mTOR mediates IL-23 induction of neutrophil IL-17 and IL-22 production. J Immunol (2016) 196(10):4390–9. doi: 10.4049/jimmunol.1501541
72. Rothhammer V, Mascanfroni ID, Bunse L, Takenaka MC, Kenison JE, Mayo L, et al. Type I interferons and microbial metabolites of tryptophan modulate astrocyte activity and central nervous system inflammation via the aryl hydrocarbon receptor. Nat Med (2016) 22(6):586–97. doi: 10.1038/nm.4106
73. Chng SH, Kundu P, Dominguez-Brauer C, Teo WL, Kawajiri K, Fujii-Kuriyama Y, et al. Ablating the aryl hydrocarbon receptor (AhR) in CD11c+ cells perturbs intestinal epithelium development and intestinal immunity. Sci Rep (2016) 6:23820. doi: 10.1038/srep23820
74. Tanaka M, Fujikawa M, Oguro A, Itoh K, Vogel CFA, Ishihara Y. Involvement of the microglial aryl hydrocarbon receptor in neuroinflammation and vasogenic edema after ischemic stroke. Cells (2021) 10(4):718. doi: 10.3390/cells10040718
75. O’Leary F, Samman S. Vitamin B12 in health and disease. Nutrients (2010) 2(3):299–316. doi: 10.3390/nu2030299
76. Xu Y, Xiang S, Ye K, Zheng Y, Feng X, Zhu X, et al. Cobalamin (Vitamin B12) induced a shift in microbial composition and metabolic activity in an in vitro colon simulation. Front Microbiol (2018) 9:2780. doi: 10.3389/fmicb.2018.02780
77. Hofmann MA, Lalla E, Lu Y, Gleason MR, Wolf BM, Tanji N, et al. Hyperhomocysteinemia enhances vascular inflammation and accelerates atherosclerosis in a murine model. J Clin Invest (2001) 107(6):675–83. doi: 10.1172/JCI10588
78. Chang L, Zhang Z, Li W, Dai J, Guan Y, Wang X. Liver-x-receptor activator prevents homocysteine-induced production of IgG antibodies from murine b lymphocytes via the ROS-NF-kappaB pathway. Biochem Biophys Res Commun (2007) 357(3):772–8. doi: 10.1016/j.bbrc.2007.04.016
79. B vitamins in patients with recent transient ischaemic attack or stroke in the VITAmins TO prevent stroke (VITATOPS) trial: a randomised, double-blind, parallel, placebo-controlled trial. Lancet Neurol (2010) 9(9):855–65. doi: 10.1016/S1474-4422(10)70187-3
80. Ahluwalia B, Magnusson MK, Öhman L. Mucosal immune system of the gastrointestinal tract: maintaining balance between the good and the bad. Scand J Gastroenterol (2017) 52(11):1185–93. doi: 10.1080/00365521.2017.1349173
81. Tomasello E, Bedoui S. Intestinal innate immune cells in gut homeostasis and immunosurveillance. Immunol Cell Biol (2013) 91(3):201–3. doi: 10.1038/icb.2012.85
82. Ulluwishewa D, Anderson RC, McNabb WC, Moughan PJ, Wells JM, Roy NC. Regulation of tight junction permeability by intestinal bacteria and dietary components. J Nutr (2011) 141(5):769–76. doi: 10.3945/jn.110.135657
83. Gasbarrini G, Montalto M. Structure and function of tight junctions. role in intestinal barrier. Ital J Gastroenterol Hepatol (1999) 31(6):481–8.
84. Wen SW, Wong CHY. An unexplored brain-gut microbiota axis in stroke. Gut Microbes (2017) 8(6):601–6. doi: 10.1080/19490976.2017.1344809
85. Spadoni I, Zagato E, Bertocchi A, Paolinelli R, Hot E, Di Sabatino A, et al. A gut-vascular barrier controls the systemic dissemination of bacteria. Science (2015) 350(6262):830–4. doi: 10.1126/science.aad0135
86. Bansal T, Alaniz RC, Wood TK, Jayaraman A. The bacterial signal indole increases epithelial-cell tight-junction resistance and attenuates indicators of inflammation. Proc Natl Acad Sci U.S.A. (2010) 107(1):228–33. doi: 10.1073/pnas.0906112107
87. Ye D, Hu Y, Zhu N, Gu W, Long G, Tao E, et al. Exploratory investigation of intestinal structure and function after stroke in mice. Mediators Inflammation (2021) 2021:1315797. doi: 10.1155/2021/1315797
88. Hii HP, Lo WZ, Fu YH, Chen MH, Shih CC, Tsao CM, et al. Improvement in heat stress-induced multiple organ dysfunction and intestinal damage through protection of intestinal goblet cells from prostaglandin E1 analogue misoprostol. Life Sci (2022) 310:121039. doi: 10.1016/j.lfs.2022.121039
89. Qin J, Li R, Raes J, Arumugam M, Burgdorf KS, Manichanh C, et al. A human gut microbial gene catalogue established by metagenomic sequencing. Nature (2010) 464(7285):59–65. doi: 10.1038/nature08821
90. de Jong PR, González-Navajas JM, Jansen NJ. The digestive tract as the origin of systemic inflammation. Crit Care (2016) 20(1):279. doi: 10.1186/s13054-016-1458-3
91. Yamashiro K, Tanaka R, Urabe T, Ueno Y, Yamashiro Y, Nomoto K, et al. Correction: gut dysbiosis is associated with metabolism and systemic inflammation in patients with ischemic stroke. PloS One (2017) 12(4):e0176062. doi: 10.1371/journal.pone.0176062
92. Xia GH, You C, Gao XX, Zeng XL, Zhu JJ, Xu KY, et al. Stroke dysbiosis index (SDI) in gut microbiome are associated with brain injury and prognosis of stroke. Front Neurol (2019) 10:397. doi: 10.3389/fneur.2019.00397
93. Haak BW, Westendorp WF, van Engelen TSR, Brands X, Brouwer MC, Vermeij JD, et al. Disruptions of anaerobic gut bacteria are associated with stroke and post-stroke infection: a prospective case-control study. Transl Stroke Res (2021) 12(4):581–92. doi: 10.1007/s12975-020-00863-4
94. Wang Q, Wu ZY, Tang HL, Yi ZM, Zhai SD. The efficacy and safety of prophylactic antibiotics for post-acute stroke infection: a systematic review and meta-analysis. Br J Clin Pharmacol (2022) 89(3):946–955. doi: 10.22541/au.166541231.17172152/v1
95. Sun J, Zhang J, Wang X, Ji F, Ronco C, Tian J, et al. Gut-liver crosstalk in sepsis-induced liver injury. Crit Care (2020) 24(1):614. doi: 10.1186/s13054-020-03327-1
96. Westendorp WF, Nederkoorn PJ, Vermeij JD, Dijkgraaf MG, van de Beek D. Post-stroke infection: a systematic review and meta-analysis. BMC Neurol (2011) 11:110. doi: 10.1186/1471-2377-11-110
97. Faura J, Bustamante A, Miró-Mur F, Montaner J. Stroke-induced immunosuppression: implications for the prevention and prediction of post-stroke infections. J Neuroinflamm (2021) 18(1):127. doi: 10.1186/s12974-021-02177-0
98. Brambilla R, Couch Y, Lambertsen KL. The effect of stroke on immune function. Mol Cell Neurosci (2013) 53:26–33. doi: 10.1016/j.mcn.2012.08.011
99. Corey S, Abraham DI, Kaneko Y, Lee JY, Borlongan CV. Selective endovascular cooling for stroke entails brain-derived neurotrophic factor and splenic IL-10 modulation. Brain Res (2019) 1722:146380. doi: 10.1016/j.brainres.2019.146380
100. Miller CM, Behrouz R. Impact of infection on stroke morbidity and outcomes. Curr Neurol Neurosci Rep (2016) 16(9):83. doi: 10.1007/s11910-016-0679-9
101. Camara-Lemarroy CR, Ibarra-Yruegas BE, Gongora-Rivera F. Gastrointestinal complications after ischemic stroke. J Neurol Sci (2014) 346(1-2):20–5. doi: 10.1016/j.jns.2014.08.027
102. Su Y, Zhang X, Zeng J, Pei Z, Cheung RT, Zhou QP, et al. New-onset constipation at acute stage after first stroke: incidence, risk factors, and impact on the stroke outcome. Stroke (2009) 40(4):1304–9. doi: 10.1161/STROKEAHA.108.534776
103. Muir KW, Watt A, Baxter G, Grosset DG, Lees KR. Randomized trial of graded compression stockings for prevention of deep-vein thrombosis after acute stroke. Qjm (2000) 93(6):359–64. doi: 10.1093/qjmed/93.6.359
104. Wijdicks EF, Fulgham JR, Batts KP. Gastrointestinal bleeding in stroke. Stroke (1994) 25(11):2146–8. doi: 10.1161/01.STR.25.11.2146
105. Rahman Z, Dandekar MP. Crosstalk between gut microbiome and immunology in the management of ischemic brain injury. J Neuroimmunol (2021) 353:577498. doi: 10.1016/j.jneuroim.2021.577498
106. Price CJ, Menon DK, Peters AM, Ballinger JR, Barber RW, Balan KK, et al. Cerebral neutrophil recruitment, histology, and outcome in acute ischemic stroke: an imaging-based study. Stroke (2004) 35(7):1659–64. doi: 10.1161/01.STR.0000130592.71028.92
107. Amantea D, Nappi G, Bernardi G, Bagetta G, Corasaniti MT. Post-ischemic brain damage: pathophysiology and role of inflammatory mediators. FEBS J (2009) 276(1):13–26. doi: 10.1111/j.1742-4658.2008.06766.x
108. Kim J, Song TJ, Park JH, Lee HS, Nam CM, Nam HS, et al. Different prognostic value of white blood cell subtypes in patients with acute cerebral infarction. Atherosclerosis (2012) 222(2):464–7. doi: 10.1016/j.atherosclerosis.2012.02.042
109. Doycheva DM, Hadley T, Li L, Applegate RL II, Zhang JH, Tang J. Anti-neutrophil antibody enhances the neuroprotective effects of G-CSF by decreasing number of neutrophils in hypoxic ischemic neonatal rat model. Neurobiol Dis (2014) 69:192–9. doi: 10.1016/j.nbd.2014.05.024
110. Shiga Y, Onodera H, Kogure K, Yamasaki Y, Yashima Y, Syozuhara H, et al. Neutrophil as a mediator of ischemic edema formation in the brain. Neurosci Lett (1991) 125(2):110–2. doi: 10.1016/0304-3940(91)90003-C
111. Pedragosa J, Miró-Mur F, Otxoa-de-Amezaga A, Justicia C, Ruíz-Jaén F, Ponsaerts P, et al. CCR2 deficiency in monocytes impairs angiogenesis and functional recovery after ischemic stroke in mice. J Cereb Blood Flow Metab (2020) 40(1_suppl):S98–s116. doi: 10.1177/0271678X20909055
112. Kim E, Yang J, Beltran CD, Cho S. Role of spleen-derived monocytes/macrophages in acute ischemic brain injury. J Cereb Blood Flow Metab (2014) 34(8):1411–9. doi: 10.1038/jcbfm.2014.101
113. Auffray C, Fogg D, Garfa M, Elain G, Join-Lambert O, Kayal S, et al. Monitoring of blood vessels and tissues by a population of monocytes with patrolling behavior. Science (2007) 317(5838):666–70. doi: 10.1126/science.1142883
114. Nahrendorf M, Swirski FK, Aikawa E, Stangenberg L, Wurdinger T, Figueiredo JL, et al. The healing myocardium sequentially mobilizes two monocyte subsets with divergent and complementary functions. J Exp Med (2007) 204(12):3037–47. doi: 10.1084/jem.20070885
115. Ma Y, Li Y, Jiang L, Wang L, Jiang Z, Wang Y, et al. Macrophage depletion reduced brain injury following middle cerebral artery occlusion in mice. J Neuroinflamm (2016) 13:38. doi: 10.1186/s12974-016-0504-z
116. Gan Y, Liu Q, Wu W, Yin JX, Bai XF, Shen R, et al. Ischemic neurons recruit natural killer cells that accelerate brain infarction. Proc Natl Acad Sci U.S.A. (2014) 111(7):2704–9. doi: 10.1073/pnas.1315943111
117. Wang ZK, Xue L, Wang T, Wang XJ, Su ZQ. Infiltration of invariant natural killer T cells occur and accelerate brain infarction in permanent ischemic stroke in mice. Neurosci Lett (2016) 633:62–8. doi: 10.1016/j.neulet.2016.09.010
118. Iadecola C, Anrather J. The immunology of stroke: from mechanisms to translation. Nat Med (2011) 17(7):796–808. doi: 10.1038/nm.2399
119. Selvaraj UM, Poinsatte K, Torres V, Ortega SB, Stowe AM. Heterogeneity of b cell functions in stroke-related risk, prevention, injury, and repair. Neurotherapeutics (2016) 13(4):729–47. doi: 10.1007/s13311-016-0460-4
120. Gu L, Xiong X, Zhang H, Xu B, Steinberg GK, Zhao H. Distinctive effects of T cell subsets in neuronal injury induced by cocultured splenocytes in vitro and by in vivo stroke in mice. Stroke (2012) 43(7):1941–6. doi: 10.1161/STROKEAHA.112.656611
121. Hurn PD, Subramanian S, Parker SM, Afentoulis ME, Kaler LJ, Vandenbark AA, et al. T- and b-cell-deficient mice with experimental stroke have reduced lesion size and inflammation. J Cereb Blood Flow Metab (2007) 27(11):1798–805. doi: 10.1038/sj.jcbfm.9600482
122. Yilmaz G, Arumugam TV, Stokes KY, Granger DN. Role of T lymphocytes and interferon-gamma in ischemic stroke. Circulation (2006) 113(17):2105–12. doi: 10.1161/CIRCULATIONAHA.105.593046
123. Filiano AJ, Gadani SP, Kipnis J. How and why do T cells and their derived cytokines affect the injured and healthy brain? Nat Rev Neurosci (2017) 18(6):375–84. doi: 10.1038/nrn.2017.39
124. Luo Y, Zhou Y, Xiao W, Liang Z, Dai J, Weng X, et al. Interleukin-33 ameliorates ischemic brain injury in experimental stroke through promoting Th2 response and suppressing Th17 response. Brain Res (2015) 1597:86–94. doi: 10.1016/j.brainres.2014.12.005
125. Tanoue T, Atarashi K, Honda K. Development and maintenance of intestinal regulatory T cells. Nat Rev Immunol (2016) 16(5):295–309. doi: 10.1038/nri.2016.36
126. Offner H, Subramanian S, Parker SM, Wang C, Afentoulis ME, Lewis A, et al. Splenic atrophy in experimental stroke is accompanied by increased regulatory T cells and circulating macrophages. J Immunol (2006) 176(11):6523–31. doi: 10.4049/jimmunol.176.11.6523
127. Liesz A, Suri-Payer E, Veltkamp C, Doerr H, Sommer C, Rivest S, et al. Regulatory T cells are key cerebroprotective immunomodulators in acute experimental stroke. Nat Med (2009) 15(2):192–9. doi: 10.1038/nm.1927
128. Li P, Gan Y, Sun BL, Zhang F, Lu B, Gao Y, et al. Adoptive regulatory T-cell therapy protects against cerebral ischemia. Ann Neurol (2013) 74(3):458–71. doi: 10.1002/ana.23815
129. Biton M, Haber AL, Rogel N, Burgin G, Beyaz S, Schnell A, et al. T Helper cell cytokines modulate intestinal stem cell renewal and differentiation. Cell (2018) 175(5):1307–1320.e22. doi: 10.1016/j.cell.2018.10.008
130. Mayassi T, Jabri B. Human intraepithelial lymphocytes. Mucosal Immunol (2018) 11(5):1281–9. doi: 10.1038/s41385-018-0016-5
131. Benakis C, Brea D, Caballero S, Faraco G, Moore J, Murphy M, et al. Commensal microbiota affects ischemic stroke outcome by regulating intestinal γδ T cells. Nat Med (2016) 22(5):516–23. doi: 10.1038/nm.4068
132. Wo J, Zhang F, Li Z, Sun C, Zhang W, Sun G. The role of gamma-delta T cells in diseases of the central nervous system. Front Immunol (2020) 11:580304. doi: 10.3389/fimmu.2020.580304
133. Shichita T, Sugiyama Y, Ooboshi H, Sugimori H, Nakagawa R, Takada I, et al. Pivotal role of cerebral interleukin-17-producing gammadeltaT cells in the delayed phase of ischemic brain injury. Nat Med (2009) 15(8):946–50. doi: 10.1038/nm.1999
134. Arunachalam P, Ludewig P, Melich P, Arumugam TV, Gerloff C, Prinz I, et al. CCR6 (CC chemokine receptor 6) is essential for the migration of detrimental natural interleukin-17-Producing γδ T cells in stroke. Stroke (2017) 48(7):1957–65. doi: 10.1161/STROKEAHA.117.016753
135. Weaver CT, Hatton RD, Mangan PR, Harrington LE. IL-17 family cytokines and the expanding diversity of effector T cell lineages. Annu Rev Immunol (2007) 25:821–52. doi: 10.1146/annurev.immunol.25.022106.141557
136. Zhang Q, Liao Y, Liu Z, Dai Y, Li Y, Li Y, et al. Interleukin-17 and ischaemic stroke. Immunology (2021) 162(2):179–93. doi: 10.1111/imm.13265
137. Wojkowska DW, Szpakowski P, Glabinski A. Interleukin 17A promotes lymphocytes adhesion and induces CCL2 and CXCL1 release from brain endothelial cells. Int J Mol Sci (2017) 18(5). doi: 10.3390/ijms18051000
138. Liu T, Han S, Dai Q, Zheng J, Liu C, Li S, et al. IL-17A-Mediated excessive autophagy aggravated neuronal ischemic injuries via src-PP2B-mTOR pathway. Front Immunol (2019) 10:2952. doi: 10.3389/fimmu.2019.02952
139. Lin Y, Zhang JC, Yao CY, Wu Y, Abdelgawad AF, Yao SL, et al. Critical role of astrocytic interleukin-17 A in post-stroke survival and neuronal differentiation of neural precursor cells in adult mice. Cell Death Dis (2016) 7(6):e2273. doi: 10.1038/cddis.2015.284
140. Brandsma E, Kloosterhuis NJ, Koster M, Dekker DC, Gijbels MJJ, van der Velden S, et al. A proinflammatory gut microbiota increases systemic inflammation and accelerates atherosclerosis. Circ Res (2019) 124(1):94–100. doi: 10.1161/CIRCRESAHA.118.313234
141. Hu W, Kong X, Wang H, Li and Y. Luo Y. Ischemic stroke and intestinal flora: an insight into brain-gut axis. Eur J Med Res (2022) 27(1):73. doi: 10.1186/s40001-022-00691-2
142. Gelderblom M, Weymar A, Bernreuther C, Velden J, Arunachalam P, Steinbach K, et al. Neutralization of the IL-17 axis diminishes neutrophil invasion and protects from ischemic stroke. Blood (2012) 120(18):3793–802. doi: 10.1182/blood-2012-02-412726
143. Singh V, Sadler R, Heindl S, Llovera G, Roth S, Benakis C, et al. The gut microbiome primes a cerebroprotective immune response after stroke. J Cereb Blood Flow Metab (2018) 38(8):1293–8. doi: 10.1177/0271678X18780130
144. Learoyd AE, Woodhouse L, Shaw L, Sprigg N, Bereczki D, Berge E, et al. Infections up to 76 days after stroke increase disability and death. Transl Stroke Res (2017) 8(6):541–8. doi: 10.1007/s12975-017-0553-3
145. Zhao N, Hu W, Wu Z, Wu X, Li W, Wang Y, et al. The red blood cell distribution width-albumin ratio: a promising predictor of mortality in stroke patients. Int J Gen Med (2021) 14:3737–47. doi: 10.2147/IJGM.S322441
146. Vermeij JD, Westendorp WF, Dippel DW, van de Beek D, Nederkoorn PJ. Antibiotic therapy for preventing infections in people with acute stroke. Cochrane Database Syst Rev (2018) 1(1):Cd008530. doi: 10.1002/14651858.CD008530.pub3
147. Powers WJ, Clarke WR, Grubb RL, Videen TO, Adams HP, Derdeyn CP. Lower stroke risk with lower blood pressure in hemodynamic cerebral ischemia. Neurology (2014) 82(12):1027–32. doi: 10.1212/WNL.0000000000000238
148. Boehme AK, Esenwa C, Elkind MS. Stroke risk factors, genetics, and prevention. Circ Res (2017) 120(3):472–95. doi: 10.1161/CIRCRESAHA.116.308398
149. Yang T, Santisteban MM, Rodriguez V, Li E, Ahmari N, Carvajal JM, et al. Gut dysbiosis is linked to hypertension. Hypertension (2015) 65(6):1331–40. doi: 10.1161/HYPERTENSIONAHA.115.05315
150. Li J, Zhao F, Wang Y, Chen J, Tao J, Tian G, et al. Gut microbiota dysbiosis contributes to the development of hypertension. Microbiome (2017) 5(1):14. doi: 10.1186/s40168-016-0222-x
151. Santisteban MM, Qi Y, Zubcevic J, Kim S, Yang T, Shenoy V, et al. Hypertension-linked pathophysiological alterations in the gut. Circ Res (2017) 120(2):312–23. doi: 10.1161/CIRCRESAHA.116.309006
152. Ufnal M, Jazwiec R, Dadlez M, Drapala A, Sikora and J. Skrzypecki M. Trimethylamine-n-oxide: a carnitine-derived metabolite that prolongs the hypertensive effect of angiotensin II in rats. Can J Cardiol (2014) 30(12):1700–5. doi: 10.1016/j.cjca.2014.09.010
153. Liu M, Han Q, Yang J. Trimethylamine-n-oxide (TMAO) increased aquaporin-2 expression in spontaneously hypertensive rats. Clin Exp Hypertens (2019) 41(4):312–22. doi: 10.1080/10641963.2018.1481420
154. Haghikia A, Li XS, Liman TG, Bledau N, Schmidt D, Zimmermann F, et al. Gut microbiota-dependent trimethylamine n-oxide predicts risk of cardiovascular events in patients with stroke and is related to proinflammatory monocytes. Arterioscler Thromb Vasc Biol (2018) 38(9):2225–35. doi: 10.1161/ATVBAHA.118.311023
155. Le Roy T, Lecuyer E, Chassaing B, Rhimi M, Lhomme M, Boudebbouze S, et al. The intestinal microbiota regulates host cholesterol homeostasis. BMC Biol (2019) 17(1):94. doi: 10.1186/s12915-019-0715-8
156. Seijkens T, Hoeksema MA, Beckers L, Smeets E, Meiler S, Levels J, et al. Hypercholesterolemia-induced priming of hematopoietic stem and progenitor cells aggravates atherosclerosis. FASEB J (2014) 28(5):2202–13. doi: 10.1096/fj.13-243105
157. Swirski FK, Libby P, Aikawa E, Alcaide P, Luscinskas FW, Weissleder R, et al. Ly-6Chi monocytes dominate hypercholesterolemia-associated monocytosis and give rise to macrophages in atheromata. J Clin Invest (2007) 117(1):195–205. doi: 10.1172/JCI29950
158. Newton AH, Benedict SH. Low density lipoprotein promotes human naive T cell differentiation to Th1 cells. Hum Immunol (2014) 75(7):621–8. doi: 10.1016/j.humimm.2014.04.017
159. Fernández-Ruiz I. Acute coronary syndromes: microbial-dependent TMAO as a prognostic marker in ACS. Nat Rev Cardiol (2017) 14(3):128–9. doi: 10.1038/nrcardio.2017.10
160. Organ CL, Otsuka H, Bhushan S, Wang Z, Bradley J, Trivedi R, et al. Choline diet and its gut microbe-derived metabolite, trimethylamine n-oxide, exacerbate pressure overload-induced heart failure. Circ Heart Fail (2016) 9(1):e002314. doi: 10.1161/CIRCHEARTFAILURE.115.002314
161. Wang Z, Klipfell E, Bennett BJ, Koeth R, Levison BS, Dugar B, et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature (2011) 472(7341):57–63. doi: 10.1038/nature09922
162. Koren O, Spor A, Felin J, Fåk F, Stombaugh J, Tremaroli V, et al. Human oral, gut, and plaque microbiota in patients with atherosclerosis. Proc Natl Acad Sci U.S.A. (2011) 108 Suppl 1(Suppl 1):4592–8. doi: 10.1073/pnas.1011383107
163. Lau LH, Lew J, Borschmann K, Thijs V, Ekinci EI. Prevalence of diabetes and its effects on stroke outcomes: a meta-analysis and literature review. J Diabetes Investig (2019) 10(3):780–92. doi: 10.1111/jdi.12932
164. Saad MJ, Santos A, Prada PO. Linking gut microbiota and inflammation to obesity and insulin resistance. Physiol (Bethesda) (2016) 31(4):283–93. doi: 10.1152/physiol.00041.2015
165. Marino E, Richards JL, McLeod KH, Stanley D, Yap YA, Knight J, et al. Gut microbial metabolites limit the frequency of autoimmune T cells and protect against type 1 diabetes. Nat Immunol (2017) 18(5):552–62. doi: 10.1038/ni.3713
166. Cortez-Espinosa N, Cortés-Garcia JD, Martínez-Leija E, Rodríguez-Rivera JG, Barajas-López C, González-Amaro R, et al. CD39 expression on treg and Th17 cells is associated with metabolic factors in patients with type 2 diabetes. Hum Immunol (2015) 76(9):622–30. doi: 10.1016/j.humimm.2015.09.007
167. Nekoua MP, Fachinan R, Atchamou AK, Nouatin O, Amoussou-Guenou D, Amoussou-Guenou MK, et al. Modulation of immune cells and Th1/Th2 cytokines in insulin-treated type 2 diabetes mellitus. Afr Health Sci (2016) 16(3):712–24. doi: 10.4314/ahs.v16i3.11
168. Ritzel RM, Lai YJ, Crapser JD, Patel AR, Schrecengost A, Grenier JM, et al. Aging alters the immunological response to ischemic stroke. Acta Neuropathol (2018) 136(1):89–110. doi: 10.1007/s00401-018-1859-2
169. O’Toole PW, Jeffery IB. Gut microbiota and aging. Science (2015) 350(6265):1214–5. doi: 10.1126/science.aac8469
170. Odamaki T, Kato K, Sugahara H, Hashikura N, Takahashi S, Xiao JZ, et al. Age-related changes in gut microbiota composition from newborn to centenarian: a cross-sectional study. BMC Microbiol (2016) 16:90. doi: 10.1186/s12866-016-0708-5
171. Pamer EG. Immune responses to commensal and environmental microbes. Nat Immunol (2007) 8(11):1173–8. doi: 10.1038/ni1526
172. Wen SW, Shim R, Ho L, Wanrooy BJ, Srikhanta YN, Prame Kumar K, et al. Advanced age promotes colonic dysfunction and gut-derived lung infection after stroke. Aging Cell (2019) 18(5):e12980. doi: 10.1111/acel.12980
173. Liang S, Domon H, Hosur KB, Wang M, Hajishengallis G. Age-related alterations in innate immune receptor expression and ability of macrophages to respond to pathogen challenge in vitro. Mech Ageing Dev (2009) 130(8):538–46. doi: 10.1016/j.mad.2009.06.006
174. Beli E, Clinthorne JF, Duriancik DM, Hwang I, Kim S, Gardner EM. Natural killer cell function is altered during the primary response of aged mice to influenza infection. Mech Ageing Dev (2011) 132(10):503–10. doi: 10.1016/j.mad.2011.08.005
175. Brubaker AL, Rendon JL, Ramirez L, Choudhry MA, Kovacs EJ. Reduced neutrophil chemotaxis and infiltration contributes to delayed resolution of cutaneous wound infection with advanced age. J Immunol (2013) 190(4):1746–57. doi: 10.4049/jimmunol.1201213
176. Wertheimer AM, Bennett MS, Park B, Uhrlaub JL, Martinez C, Pulko V, et al. Aging and cytomegalovirus infection differentially and jointly affect distinct circulating T cell subsets in humans. J Immunol (2014) 192(5):2143–55. doi: 10.4049/jimmunol.1301721
177. Frasca D, Diaz A, Romero M, Blomberg BB. The generation of memory b cells is maintained, but the antibody response is not, in the elderly after repeated influenza immunizations. Vaccine (2016) 34(25):2834–40. doi: 10.1016/j.vaccine.2016.04.023
178. Huo Y, Li J, Qin X, Huang Y, Wang X, Gottesman RF, et al. Efficacy of folic acid therapy in primary prevention of stroke among adults with hypertension in China: the CSPPT randomized clinical trial. Jama (2015) 313(13):1325–35. doi: 10.1001/jama.2015.2274
179. Kullo IJ. HOPE 2: can supplementation with folic acid and b vitamins reduce cardiovascular risk? Nat Clin Pract Cardiovasc Med (2006) 3(8):414–5. doi: 10.1038/ncpcardio0611
180. Bønaa KH, Njølstad I, Ueland PM, Schirmer H, Tverdal A, Steigen T, et al. Homocysteine lowering and cardiovascular events after acute myocardial infarction. N Engl J Med (2006) 354(15):1578–88. doi: 10.1056/NEJMoa055227
181. Spence JD, Yi Q, Hankey GJ. B vitamins in stroke prevention: time to reconsider. Lancet Neurol (2017) 16(9):750–60. doi: 10.1016/S1474-4422(17)30180-1
182. Roth W, Mohamadzadeh M. Vitamin B12 and gut-brain homeostasis in the pathophysiology of ischemic stroke. EBioMedicine (2021) 73:103676. doi: 10.1016/j.ebiom.2021.103676
183. Yin J, Liao SX, He Y, Wang S, Xia GH, Liu FT, et al. Dysbiosis of gut microbiota with reduced trimethylamine-N-Oxide level in patients with Large-artery atherosclerotic stroke or transient ischemic attack. J Am Heart Assoc (2015) 4(11):e002699. doi: 10.1161/JAHA.115.002699
184. Xiang L, Lou Y, Liu L, Liu Y, Zhang W, Deng J, et al. Gut microbiotic features aiding the diagnosis of acute ischemic stroke. Front Cell Infect Microbiol (2020) 10:587284. doi: 10.3389/fcimb.2020.587284
185. Sun H, Gu M, Li Z, Chen and J. Zhou X. Gut microbiota dysbiosis in acute ischemic stroke associated with 3-month unfavorable outcome. Front Neurol (2021) 12:799222. doi: 10.3389/fneur.2021.799222
186. Engler TM, Dourado CC, Amâncio TG, Farage L, de Mello PA, Padula MP. Stroke: bowel dysfunction in patients admitted for rehabilitation. Open Nurs J (2014) 8:43–7. doi: 10.2174/1874434601408010043
187. Zeng X, Gao X, Peng Y, Wu Q, Zhu J, Tan C, et al. Higher risk of stroke is correlated with increased opportunistic pathogen load and reduced levels of butyrate-producing bacteria in the gut. Front Cell Infect Microbiol (2019) 9:4. doi: 10.3389/fcimb.2019.00004
188. Wong CH, Jenne CN, Lee WY, Léger C, Kubes P. Functional innervation of hepatic iNKT cells is immunosuppressive following stroke. Science (2011) 334(6052):101–5. doi: 10.1126/science.1210301
189. Elenkov IJ, Wilder RL, Chrousos GP, Vizi ES. The sympathetic nerve–an integrative interface between two supersystems: the brain and the immune system. Pharmacol Rev (2000) 52(4):595–638.
190. Pavlov VA, Wang H, Czura CJ, Friedman SG, Tracey KJ. The cholinergic anti-inflammatory pathway: a missing link in neuroimmunomodulation. Mol Med (2003) 9(5-8):125–34. doi: 10.1007/BF03402177
191. Liu Q, Jin WN, Liu Y, Shi K, Sun H, Zhang F, et al. Brain ischemia suppresses immunity in the periphery and brain via different neurogenic innervations. Immunity (2017) 46(3):474–87. doi: 10.1016/j.immuni.2017.02.015
192. Ajmo CT Jr., Collier LA, Leonardo CC, Hall AA, Green SM, Womble TA, et al. Blockade of adrenoreceptors inhibits the splenic response to stroke. Exp Neurol (2009) 218(1):47–55. doi: 10.1016/j.expneurol.2009.03.044
193. Maier IL, Karch A, Mikolajczyk R, Bähr M, Liman J. Effect of beta-blocker therapy on the risk of infections and death after acute stroke–a historical cohort study. PloS One (2015) 10(2):e0116836. doi: 10.1371/journal.pone.0116836
194. Sykora M, Siarnik P, Diedler J. β-blockers, pneumonia, and outcome after ischemic stroke: evidence from virtual international stroke trials archive. Stroke (2015) 46(5):1269–74. doi: 10.1161/STROKEAHA.114.008260
195. De Raedt S, Haentjens P, De Smedt A, Brouns R, Uyttenboogaart M, Luijckx GJ, et al. Pre-stroke use of beta-blockers does not affect ischaemic stroke severity and outcome. Eur J Neurol (2012) 19(2):234–40. doi: 10.1111/j.1468-1331.2011.03475.x
196. Bansal V, Costantini T, Ryu SY, Peterson C, Loomis W, Putnam J, et al. Stimulating the central nervous system to prevent intestinal dysfunction after traumatic brain injury. J Trauma (2010) 68(5):1059–64. doi: 10.1097/TA.0b013e3181d87373
197. Lopez NE, Krzyzaniak MJ, Costantini TW, Putnam J, Hageny A-M, Eliceiri B, et al. Vagal nerve stimulation decreases blood-brain barrier disruption after traumatic brain injury. J Trauma Acute Care Surg (2012) 72(6):1562–6. doi: 10.1097/TA.0b013e3182569875
198. Duris K, Lipkova J, Jurajda M. Cholinergic anti-inflammatory pathway and stroke. Curr Drug Delivery (2017) 14(4):449–57. doi: 10.2174/1567201814666170201150015
199. Borovikova LV, Ivanova S, Zhang M, Yang H, Botchkina GI, Watkins LR, et al. Vagus nerve stimulation attenuates the systemic inflammatory response to endotoxin. Nature (2000) 405(6785):458–62. doi: 10.1038/35013070
200. Bernik TR, Friedman SG, Ochani M, DiRaimo R, Ulloa L, Yang H, et al. Pharmacological stimulation of the cholinergic antiinflammatory pathway. J Exp Med (2002) 195(6):781–8. doi: 10.1084/jem.20011714
201. Borovikova LV, Ivanova S, Nardi D, Zhang M, Yang H, Ombrellino M, et al. Role of vagus nerve signaling in CNI-1493-mediated suppression of acute inflammation. Auton Neurosci (2000) 85(1-3):141–7. doi: 10.1016/S1566-0702(00)00233-2
202. van Gemmeren T, Schuppner R, Grosse GM, Fering J, Gabriel MM, Huber R, et al. Early post-stroke infections are associated with an impaired function of neutrophil granulocytes. J Clin Med (2020) 9(3):872. doi: 10.3390/jcm9030872
203. Yang H, Zhang A, Zhang Y, Ma S, Wang C. Resveratrol pretreatment protected against cerebral Ischemia/Reperfusion injury in rats via expansion of T regulatory cells. J Stroke Cerebrovasc Dis (2016) 25(8):1914–21. doi: 10.1016/j.jstrokecerebrovasdis.2016.04.014
204. Wang Z, Zhou Y, Yu Y, He K, Cheng LM. Lipopolysaccharide preconditioning increased the level of regulatory b cells in the spleen after acute ischaemia/reperfusion in mice. Brain Res (2018) 1701:46–57. doi: 10.1016/j.brainres.2018.05.036
205. Xiao W, Guo S, Chen and Y. Luo L. The role of interleukin-33 in the modulation of splenic T-cell immune responses after experimental ischemic stroke. J Neuroimmunol (2019) 333:576970. doi: 10.1016/j.jneuroim.2019.576970
206. Jin R, Zhong W, Liu S, Li G. CD147 as a key mediator of the spleen inflammatory response in mice after focal cerebral ischemia. J Neuroinflamm (2019) 16(1):198. doi: 10.1186/s12974-019-1609-y
207. Wu MH, Huang CC, Chio CC, Tsai KJ, Chang CP, Lin NK, et al. Inhibition of peripheral TNF-alpha and downregulation of microglial activation by alpha-lipoic acid and etanercept protect rat brain against ischemic stroke. Mol Neurobiol (2016) 53(7):4961–71. doi: 10.1007/s12035-015-9418-5
208. Wang S, Zhou J, Kang W, Dong and H. Wang Z. Tocilizumab inhibits neuronal cell apoptosis and activates STAT3 in cerebral infarction rat model. Bosn J Basic Med Sci (2016) 16(2):145–50. doi: 10.17305/bjbms.2016.853
209. Dai Q, Li S, Liu T, Zheng J, Han S, Qu A, et al. Interleukin-17A-mediated alleviation of cortical astrocyte ischemic injuries affected the neurological outcome of mice with ischemic stroke. J Cell Biochem (2019) 120(7):11498–509. doi: 10.1002/jcb.28429
210. Zhang H, Xia Y, Ye Q, Yu F, Zhu W, Li P, et al. In vivo expansion of regulatory T cells with IL-2/IL-2 antibody complex protects against transient ischemic stroke. J Neurosci (2018) 38(47):10168–79. doi: 10.1523/JNEUROSCI.3411-17.2018
211. Kim KO, Gluck M. Fecal microbiota transplantation: an update on clinical practice. Clin Endosc (2019) 52(2):137–43. doi: 10.5946/ce.2019.009
212. Evrensel A, Ceylan ME. Fecal microbiota transplantation and its usage in neuropsychiatric disorders. Clin Psychopharmacol Neurosci (2016) 14(3):231–7. doi: 10.9758/cpn.2016.14.3.231
213. Chen R, Xu Y, Wu P, Zhou H, Lasanajak Y, Fang Y, et al. Transplantation of fecal microbiota rich in short chain fatty acids and butyric acid treat cerebral ischemic stroke by regulating gut microbiota. Pharmacol Res (2019) 148:104403. doi: 10.1016/j.phrs.2019.104403
214. Gupta A, Khanna S. Fecal microbiota transplantation. JAMA (2017) 318(1):102–2. doi: 10.1001/jama.2017.6466
215. Hill C, Guarner F, Reid G, Gibson GR, Merenstein DJ, Pot B, et al. Expert consensus document. the international scientific association for probiotics and prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol (2014) 11(8):506–14. doi: 10.1038/nrgastro.2014.66
216. Muralitharan RR, Jama HA, Xie L, Peh A, Snelson M, Marques FZ. Microbial peer pressure: the role of the gut microbiota in hypertension and its complications. Hypertension (2020) 76(6):1674–87. doi: 10.1161/HYPERTENSIONAHA.120.14473
217. Liu Y, Kong C, Gong L, Zhang X, Zhu Y, Wang H, et al. The association of post-stroke cognitive impairment and gut microbiota and its corresponding metabolites. J Alzheimers Dis (2020) 73(4):1455–66. doi: 10.3233/JAD-191066
218. Tan M, Zhu JC, Du J, Zhang LM, Yin HH. Effects of probiotics on serum levels of Th1/Th2 cytokine and clinical outcomes in severe traumatic brain-injured patients: a prospective randomized pilot study. Crit Care (2011) 15(6):R290. doi: 10.1186/cc10579
219. Markowiak P, Slizewska K. Effects of probiotics, prebiotics, and synbiotics on human health. Nutrients (2017) 9(9):1021. doi: 10.3390/nu9091021
220. Le Leu RK, Hu Y, Brown and G.P. Young IL. Effect of high amylose maize starches on colonic fermentation and apoptotic response to DNA-damage in the colon of rats. Nutr Metab (2009) 6(1):11. doi: 10.1186/1743-7075-6-11
221. Yuan Q, Xin L, Han S, Su Y, Wu R, Liu X, et al. Lactulose improves neurological outcomes by repressing harmful bacteria and regulating inflammatory reactions in mice after stroke. Front Cell Infect Microbiol (2021) 11:644448. doi: 10.3389/fcimb.2021.644448
222. Akagawa S, Akagawa Y, Nakai Y, Yamagishi M, Yamanouchi S, Kimata T, et al. Fiber-rich barley increases butyric acid-producing bacteria in the human gut microbiota. Metabolites (2021) 11(8):559. doi: 10.3390/metabo11080559
223. Fei Y, Zhang S, Han S, Qiu B, Lu Y, Huang W, et al. The role of dihydroresveratrol in enhancing the synergistic effect of ligilactobacillus salivarius Li01 and resveratrol in ameliorating colitis in mice. Res (Wash D C) (2022) 2022:9863845. doi: 10.34133/2022/9863845
224. Ferguson JF, Allayee H, Gerszten RE, Ideraabdullah F, Kris-Etherton PM, Ordovas JM, et al. Nutrigenomics, the microbiome, and gene-environment interactions: new directions in cardiovascular disease research, prevention, and treatment: a scientific statement from the American heart association. Circ Cardiovasc Genet (2016) 9(3):291–313. doi: 10.1161/HCG.0000000000000030
225. Olson CA, Vuong HE, Yano JM, Liang QY, Nusbaum and E.Y. Hsiao DJ. The gut microbiota mediates the anti-seizure effects of the ketogenic diet. Cell (2018) 174(2):497. doi: 10.1016/j.cell.2018.06.051
226. Ma D, Wang AC, Parikh I, Green SJ, Hoffman JD, Chlipala G, et al. Ketogenic diet enhances neurovascular function with altered gut microbiome in young healthy mice. Sci Rep (2018) 8(1):6670. doi: 10.1038/s41598-018-25190-5
227. Parada Venegas D, de la Fuente MK, Landskron G, Gonzalez MJ, Quera R, Dijkstra G, et al. Short chain fatty acids (SCFAs)-mediated gut epithelial and immune regulation and its relevance for inflammatory bowel diseases. Front Immunol (2019) 10:277. doi: 10.3389/fimmu.2019.00277
228. Chen H, Nwe PK, Yang Y, Rosen CE, Bielecka AA, Kuchroo M, et al. A forward chemical genetic screen reveals gut microbiota metabolites that modulate host physiology. Cell (2019) 177(5):1217–1231.e18. doi: 10.1016/j.cell.2019.03.036
Keywords: ischemic stroke, brain, inflammation, gastrointestinal tract, gastrointestinal microbiota
Citation: Wei Y-h, Bi R-t, Qiu Y-m, Zhang C-l, Li J-z, Li Y-n and Hu B (2023) The gastrointestinal-brain-microbiota axis: a promising therapeutic target for ischemic stroke. Front. Immunol. 14:1141387. doi: 10.3389/fimmu.2023.1141387
Received: 10 January 2023; Accepted: 22 May 2023;
Published: 02 June 2023.
Edited by:
Xiao-Yi Xiong, Chengdu University of Traditional Chinese Medicine, ChinaReviewed by:
Yong Ge, The University of Texas Health Science Center at San Antonio, United StatesCopyright © 2023 Wei, Bi, Qiu, Zhang, Li, Li and Hu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ya-nan Li, bHluLmh1c3RAcXEuY29t; Bo Hu, aHVib0BodXN0LmVkdS5jbg==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.