
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 16 February 2023
Sec. Cancer Immunity and Immunotherapy
Volume 14 - 2023 | https://doi.org/10.3389/fimmu.2023.1115291
This article is part of the Research Topic Mechanism and Application of Synergistic Effect of Radiotherapy and Immunotherapy View all 7 articles
 Chaoyuan Liu1†
Chaoyuan Liu1† Wei Zhao2,3†
Wei Zhao2,3† Junpeng Xie1
Junpeng Xie1 Huashan Lin4
Huashan Lin4 Xingsheng Hu1Chang Li2Youlan Shang2Yapeng Wang1Yingjia Jiang2
Xingsheng Hu1Chang Li2Youlan Shang2Yapeng Wang1Yingjia Jiang2 Mengge Ding1
Mengge Ding1 Muyun Peng5Tian Xu1Ao’ran Hu1Yuda Huang6
Muyun Peng5Tian Xu1Ao’ran Hu1Yuda Huang6 Yuan Gao7Xianling Liu1*
Yuan Gao7Xianling Liu1* Jun Liu2,3,8*
Jun Liu2,3,8* Fang Ma1*
Fang Ma1*Introduction: The treatment response to neoadjuvant immunochemotherapy varies among patients with potentially resectable non-small cell lung cancers (NSCLC) and may have severe immune-related adverse effects. We are currently unable to accurately predict therapeutic response. We aimed to develop a radiomics-based nomogram to predict a major pathological response (MPR) of potentially resectable NSCLC to neoadjuvant immunochemotherapy using pretreatment computed tomography (CT) images and clinical characteristics.
Methods: A total of 89 eligible participants were included and randomly divided into training (N=64) and validation (N=25) sets. Radiomic features were extracted from tumor volumes of interest in pretreatment CT images. Following data dimension reduction, feature selection, and radiomic signature building, a radiomics-clinical combined nomogram was developed using logistic regression analysis.
Results: The radiomics-clinical combined model achieved excellent discriminative performance, with AUCs of 0.84 (95% CI, 0.74-0.93) and 0.81(95% CI, 0.63-0.98) and accuracies of 80% and 80% in the training and validation sets, respectively. Decision curves analysis (DCA) indicated that the radiomics-clinical combined nomogram was clinically valuable.
Discussion: The constructed nomogram was able to predict MPR to neoadjuvant immunochemotherapy with a high degree of accuracy and robustness, suggesting that it is a convenient tool for assisting with the individualized management of patients with potentially resectable NSCLC.
Non-small cell lung cancer (NSCLC) accounts for 80-85% of all lung cancers and is the leading cause of cancer death worldwide (1). About 20-25% of NSCLCs are resectable at the time of diagnosis, including most stage I–IIIa and a small proportion of stage IIIb tumors (2, 3). The 5-year overall survival (OS) rates of resectable lung cancer patients are unsatisfactory (4). Pathological response to neoadjuvant treatment is a potential surrogate for an early clinical endpoint for long-term survival (5–7). Only about 4% of NSCLC patients achieve a pathological complete response (PCR) after neoadjuvant chemotherapy alone (5), which is far from satisfactory. It is well known that no major advances have been made in neoadjuvant treatments for NSCLC over the 25 years prior to the emergence of immunotherapeutic drugs (5). Checkmate 816, the first stage 3 randomized neoadjuvant immunotherapy-based combination study, confirmed that neoadjuvant immunotherapy in combination with chemotherapy is significantly more efficacious than neoadjuvant chemotherapy alone for resectable NSCLC (8). The neoadjuvant immunochemotherapy group was superior to the neoadjuvant chemotherapy group in both MPR (36.9% vs. 8.9%) and median event-free survival (EFS) (31.6 months vs. 20.8 months) (9, 10). Minimally invasive surgery was more common, there were minimal delays in surgery and minimal differences in treatment-related adverse events. Based on the promising results of this trial, combination treatment with neoadjuvant chemotherapy and nivolumab was formally approved by the FDA in March 2022 (10).
Though neoadjuvant immunochemotherapy has greatly succeeded at treating NSCLC, the MPR% of immunochemotherapy is still approximately 36%, which is relatively low (10). Some patients, especially those with stage IIIA/B NSCLC, had a poor response that required timely changes to their treatment regimen. Immunochemotherapy can also lead to severe immune-related adverse effects (irAEs, such as pneumonitis) in some patients. Given this, finding a reliable approach for predicting MPR before administering neoadjuvant immunochemotherapy is critical to maximizing patient benefit, minimizing risks, and recommending personalized perioperative treatment for patients with potentially operable NSCLC. There is presently no reliable parameter or biomarker that can predict the response to neoadjuvant immunochemotherapy. Tumor PD-L1 expression could predict the efficacy of immunotherapy to some extent, but its predictive value is not as good with combination immunochemotherapy vs. mono-immunotherapy (9). Previous studies have shown that patients who achieve PCR have a distinctive peripheral blood immune status (11), and pretreatment tissue TCR repertoire evenness is also associated with PCR (12). Other reports have shown that baseline neutrophil-to-lymphocyte ratio (NLR) can independently predict the pathological response to neoadjuvant immunochemotherapy (13). However, these serological biomarkers are either too expensive or susceptible to various factors such as inflammation or infection and have not been prospectively validated. They are not presently applied clinically. Alternative predictive biomarkers are needed urgently, especially those that can be detected using a non-invasive method.
Medical imaging, such as computed tomography (CT), plays a vital role in the diagnosis, evaluation, and treatment monitoring of NSCLC (14). Medical images possess a significant amount data that cannot be observed intuitively (15). Data mining of medical images to assist with clinical decision-making has emerged as a hot spot in medical research. Radiomics, first proposed by Philippe (16), refers to an emerging data-driven strategy that can extract either a set of predefined engineered features that describe radiographic aspects of shape, intensity, and texture, or alternatively high-level features (i.e. valvelet). Radiomics have been widely studied to aid in disease diagnosis, prognostication, and the prediction of treatment response to facilitate personalized medicine (17). Several previous studies also used radiomics to predict gene mutation status and the response to chemoradiotherapy for various tumors, with promising results (18, 19). However, to the best of our knowledge, no previous studies have evaluated the potential value of radiomics to predict MPR after neoadjuvant immunochemotherapy in NSCLC.
The present study aimed to develop and validate a radiomics-based model that can efficiently predict MPR for potentially resectable NSCLC treated with neoadjuvant immunochemotherapy. We also explored the integration of CT-based radiomics and clinical data into a multidimensional nomogram to predict MPR.
The patient selection and distribution flowchart is shown in Figure 1A, and the model construction and assessment flowchart is shown in Figure 1B.
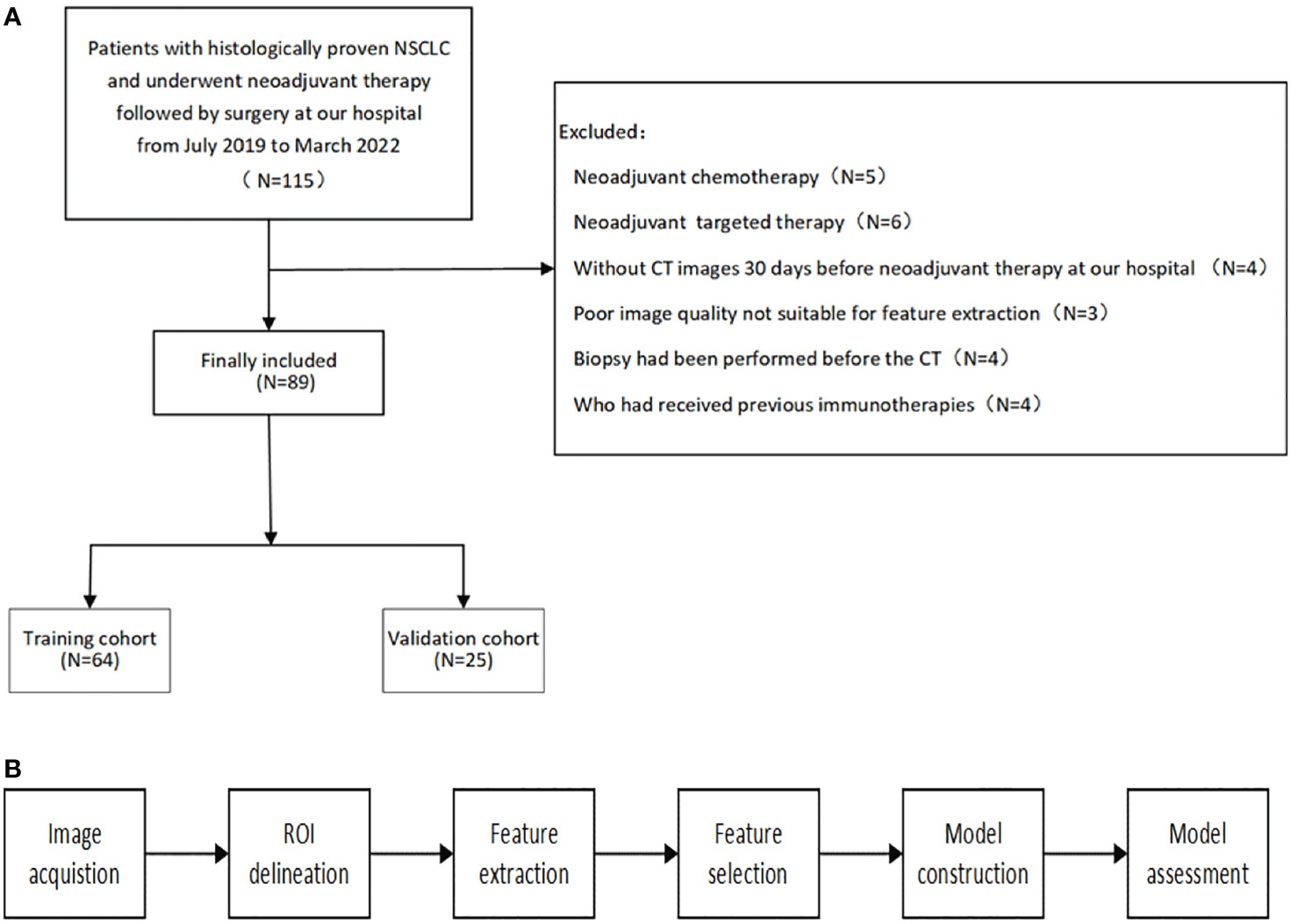
Figure 1 (A) patient selection and distribution flowchart. (B) model construction and assessment flowchart.
We collected data retrospectively from July 2019 to March 2022. We included all NSCLC patients at our hospital who were: (1) age 18 years or older, (2) pathologically confirmed, (3) clinical stage IB–IIIC, and (4) underwent neoadjuvant immunochemotherapy followed by surgery. The exclusion criteria were as follows: (1) previous immunotherapy, (2) no available pretreatment CT scans, (3) non-measurable lesions per the Response Evaluation Criteria in Solid Tumors (RECIST) 1.1, (4) poor image quality that was not suitable for feature extraction, and (5) a biopsy was performed prior to the available CT. Patient clinicopathological information, including age, sex, stage, PD-L1 expression (Dako 22C3), and details about their neoadjuvant treatment, including agents and course of treatment, were collected from the electronic database. MPR was defined as 0-10% of viable tumor cells remaining in the residual tumor.
All patients underwent a standard preoperative staging workup that included a pretreatment tumor biopsy, a contrast-enhanced CT scan of the chest and abdomen, contrast-enhanced brain magnetic resonance imaging, and a 99mTc-labeled methylene diphosphonate (99mTc-MDP) whole-body bone scan. Tumors were staged according to the 8th edition of the American Joint Committee on Cancer criteria. The surgeon evaluated all patients to determine whether they were appropriate for surgical intervention or should continue neoadjuvant therapy after two to four cycles of neoadjuvant immunochemotherapy. All pathologic information, including MPR or non-MPR (N-MPR) status, was reconfirmed by a senior pathologist. Patients who achieved MPR or PCR were assigned to the MPR group, and all others were assigned to the N-MPR group.
CT scans obtained within 30 days of the treatment start date were analyzed. If there was more than one CT scan, the closest CT scan before the biopsy was used. The included patients underwent CT scans with the following four scanners: Somatom Definition Flash, Siemens, Germany; uCT780, United Imaging, Shanghai, China; Somatom Perspective 128, Siemens, Germany; and Somatom Definition Force, Siemens, Germany. Scanning protocols were as follows: 120 kVp, 100–200 mAs, and pitch 0.75–1.5. Plain CT images with 5-mm thickness cuts were retrieved from the Picture Archiving and Communication System (PACS) for further analysis. CT images were acquired in the supine position at full inspiration for all patients.
All targeted tumors were manually delineated slice by slice by one author with 5 years of experience with chest CT interpretation using the medical image processing and navigation software 3D Slicer (version 4.10.1, Brigham and Women’s Hospital). Patients with multiple lesions on their CT scan had the lesion with the largest diameter selected. Volumes of interests (VOIs) were then confirmed by another radiologist with 10 years of experience with chest CT interpretation. Images and VOIs were exported in the NII format for further analysis. Prior to radiomic feature extraction, the voxel size of the VOI was resampled to 1*1*1 mm3 via cubic interpolation to reduce feature value variability due to different voxel sizes. A total of 1746 radiomic features were extracted, including First order, Shape3D, GLCM, GLSZM, GLRLM, NGTDM, GLDM, and high order features.
Given concerns about the reproducibility of radiomic features, we performed an intra-observer reproducibility analysis. One author segmented 50 randomly chosen images at two-time points with an interval time of one month, producing two VOIs of each selected patient. Agreement between feature extractions was assessed using intra-class correlation coefficients (ICCs). An ICC value greater than 0.8 indicated good agreement. To eliminate redundant radiomic features, we performed a two-step feature selection strategy. MRMR was initially used to select the 20 most valuable features. The LASSO method, which is suitable for the regression of high-dimensional data (18, 20), was then used to select the most useful predictive features. A radiomics score (Rad-score) was calculated for each patient via the linear combination of selected features weighted by their respective coefficients.
We randomly divided the dataset into training and validation sets with a ratio of 7:3. We then constructed the radiomics model, clinical model, and radiomics-clinical combined model. Optimal radiomic features were determined through dimension reduction by MRMR and LASSO. Clinical variables were selected via univariate and multivariable logistic regression analysis, which began with the following clinical candidate predictors: age, gender, site, smoking, differentiation, pathological type, cT-stage, cN-stage, immuno-therapy regimen, neoadjuvant cycles, PD-L1 expression, Ki67, and NLR. The retained optimal radiomic features and clinical variables whose P-values were <0.05 were used to develop logistic regression analysis model. AUC, accuracy, sensitivity, specificity, PPV, and NPV were used to evaluate model performance. The DeLong test was used to evaluate differences in the ROCs of various models. Calibration of the training set and validation set of each model was measured using a calibration curve. The Hosmer-Lemeshow test was performed to assess the goodness-of-fit of these models. DCA was also performed on the training set of the three models by calculating the net benefits over a range of threshold probabilities.
Statistical analysis was performed using R software (version 3.4.3; http://www.Rproject.org) and IBM SPSS Statistics (version 24; IBM, New York, USA). Quantitative data was compared using Student’s t-test or the Wilcoxon test. Categorical data was compared using the χ2 test. Predictive performance was evaluated with the AUC of the receiver operator characteristic (ROC). The Lasso algorithm was executed using the “glmnet” package, and multivariate binary logistic regression, nomograms, and calibration plots were executed with the “rms” package. Internal validation was performed using the “rms” package. DCA was performed using the “rmda” package. Univariate and multivariate logistic regression analyses were used to select clinical variables with p<0.05 for model construction. A two-sided P value <0.05 was considered statistically significant.
Eighty-nine eligible patients were included in this retrospective study. The entire cohort was randomly divided into a training set (n = 64) and a validation set (n = 25) at a ratio of 7:3. The demographics and clinicopathological characteristics of the patients in the training and validation cohorts are shown in Table 1. The majority of the participants were male smokers aged ≤60 who had squamous cell carcinoma and a PD-L1 expression >1%. Eighty-one patients were male (91.01%) and 8 were female (8.99%). Fifty-four (60.67%) had a smoking history. The majority of the tumor histologies included squamous cell carcinoma (SCC) and adenocarcinoma (ADC). Of these, 41 (64.1%) cases were SCC and 20 (31.2%) were ADC in the training cohort, while 18 (72%) were SCC and 6 (24%) were ADC in the validation cohort. There were no significant differences between the training and the validation sets in terms of clinical characteristics, proving that they could be used as training and validation sets (Table 1). MPR was achieved by 62.5% (40/89) of the training cohort and 64% (16/25) of the validation cohort (Table 1). No statistical differences in baseline characteristics were identified between patients with and without MPR except for ki-67 (p=0.046) and NLR (p=0.022) in the validation cohort.
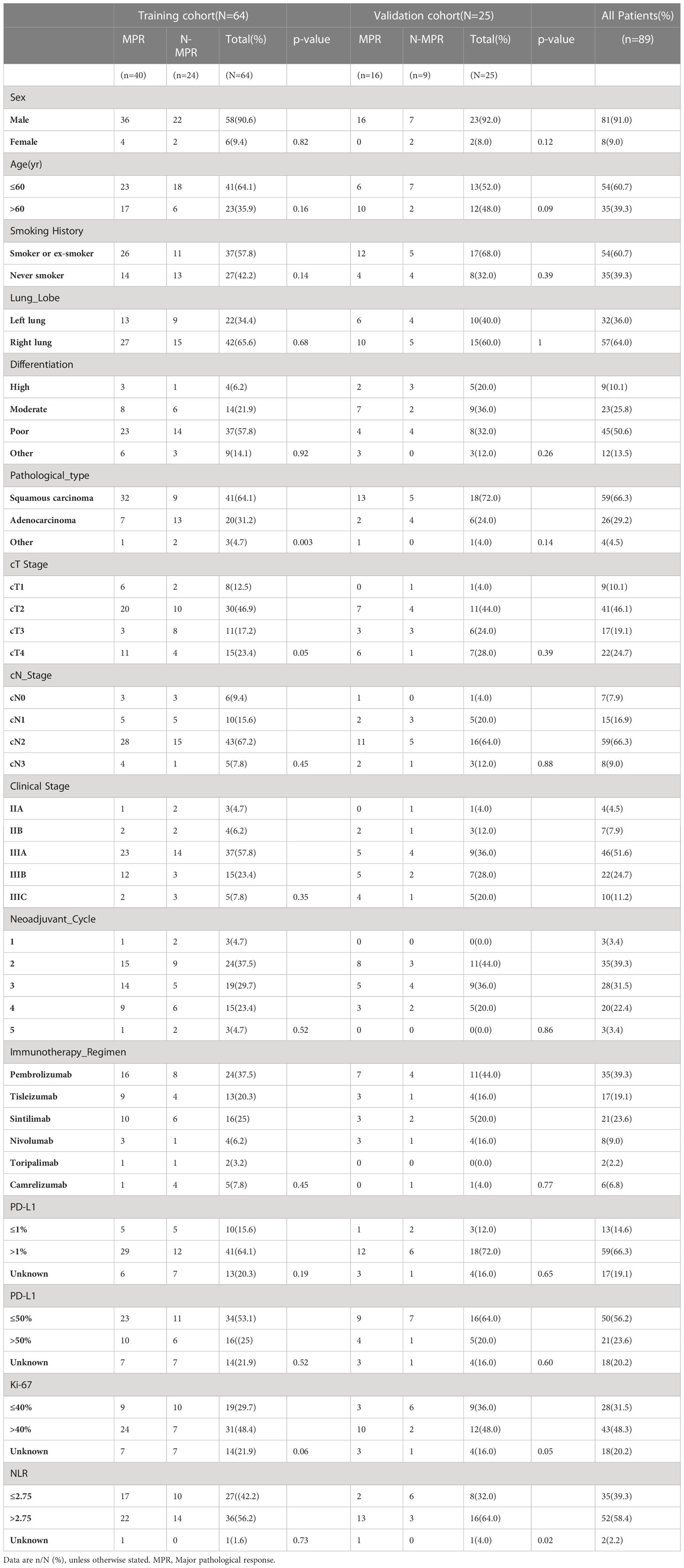
Table 1 Clinicopathological characteristics of the dataset.
A total of 1746 radiomics features were extracted, of which 1251 (71.65%) had an intra-class correlation coefficient of 0.8 or more in the reproducibility analysis. These were chosen for subsequent analysis. After dimension reduction with MRMR, the 20 best features were selected. The Lasso algorithm was used for further dimension reduction (Figures 2A, B). Seven optimal radiomics features were chosen to construct the models (Supplement). There was a significant difference in Rad-score between MPR and N-MPR patients in the training (P<0.001) and validation cohorts (P = 0.037) (Figure 2C).
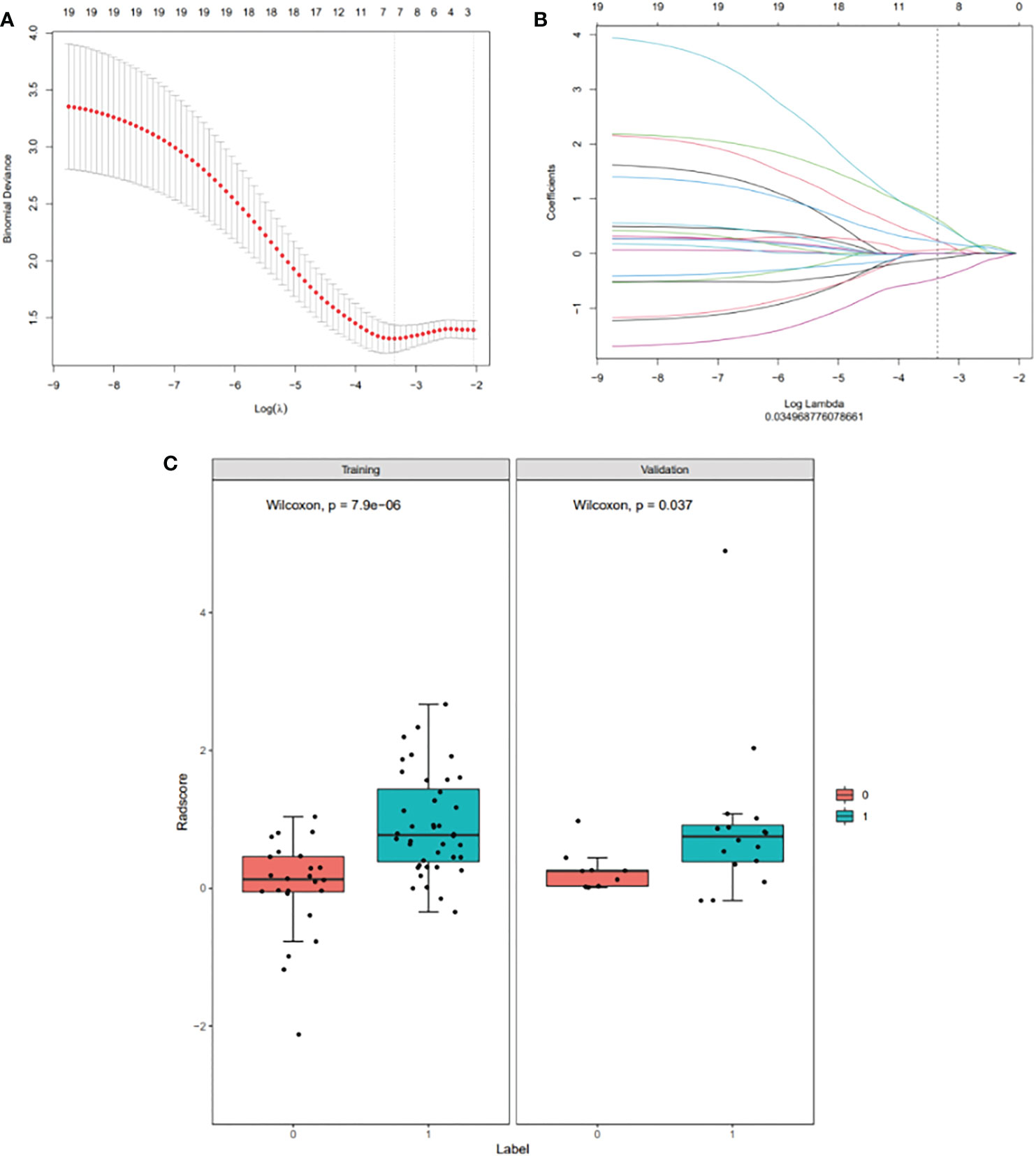
Figure 2 Radiomic feature selection using a least absolute shrinkage and selection operator (LASSO) binary logistic regression model (A, B), with a comparison of the Rad-scores of the MPR and N-MPR groups (C): Red represents the N-MPR group and blue represents the MPR group. There was a significant difference in Rad-score between MPR and N-MPR patients in the training (P<0.001) and validation cohorts (P = 0.037). (A) Selection of the tuning parameter (λ) for the LASSO model via 10-fold cross-validation based on minimum criteria. The y-axis indicates binomial deviance. The lower x-axis indicates the log (λ). Numbers along the upper x-axis represent the average number of predictors. The optimal λ value of 0.035 with log (λ)= - 3.353 was selected. (B) LASSO coefficient profiles (y-axis) of the 20 texture features. The upper and lower x-axis has the same meaning as in Fig. 2A. A black vertical line was drawn at the value selected using 10-fold cross-validation in Fig. 2A. The 7 resulting features with non-zero coefficients are shown in the plot. (C) Comparison of Rad-scores between the MPR and N-MPR groups. Red represents the N-MPR group and blue represents the MPR group. There was a significant difference in the Rad-scores of MPR and N-MPR patients in both the training (P<0.001) and validation cohorts (P = 0.037).
After univariate and multivariate logistic regression analysis, only pathologic type was identified as an independent predictive value and used to build further models (Table 2). Three models were built based on selected radiomics features (Rad-score), pathological-type, or their combination (radiomics-only, clinical-only, and radiomics-clinical combined model). The ROC curves of the three models were compared in the training set (Figure 3A) and the validation set (Figure 3B) for predicting MPR. The AUCs in the training set were 0.82 (95% CI, 0.72-0.93) and 0.68 (95% CI, 0.57-0.80) for the radiomics-only and clinical-only models, respectively. After development in the training cohort, both radiomics-only and clinical-only models accurately predicted MPR in the validation cohort, with AUCs of 0.76 (95% CI, 0.55-0.97) and 0.66(95% CI, 0.47-0.85), respectively. The radiomics-clinical combined model had the best performance, with an AUC of 0.84 (95% CI, 0.74-0.93) and 0.81 (95% CI, 0.63-0.98) in the training and validation sets, respectively.

Table 2 Univariate and multivariate analysis of clinical data.
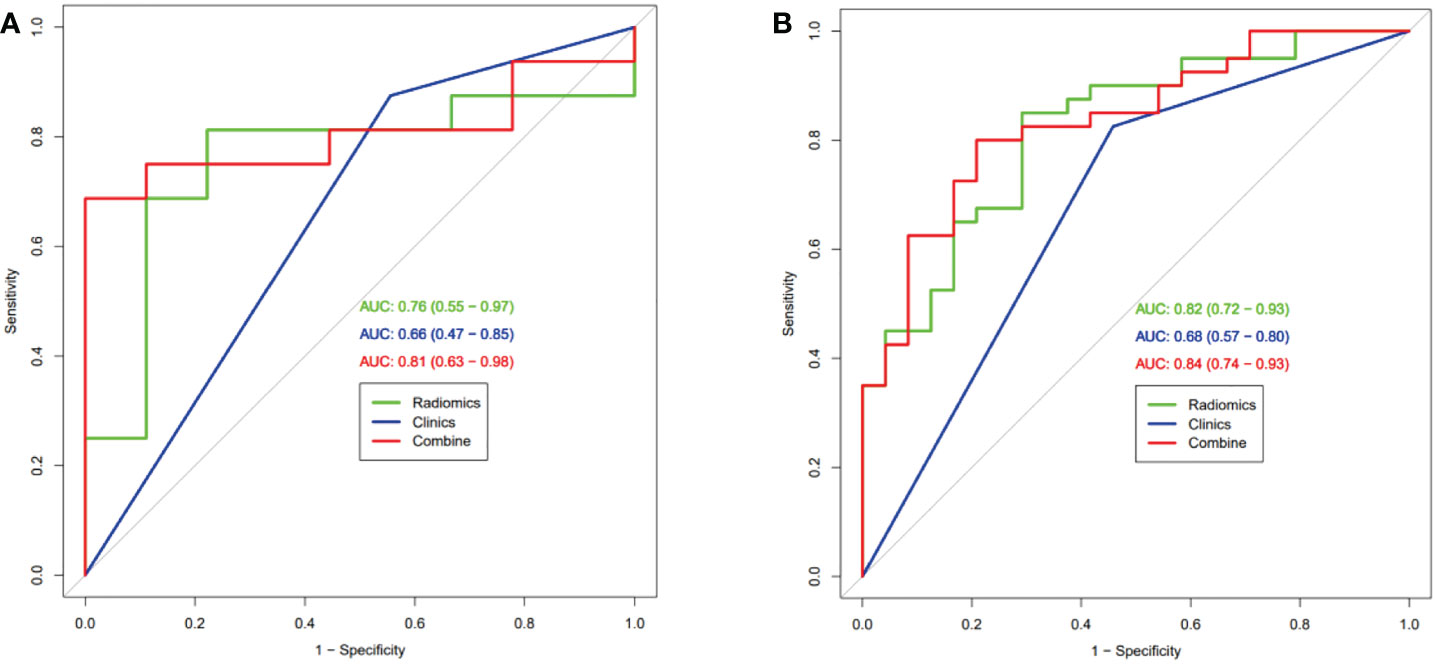
Figure 3 Receiver operating characteristic curve analysis of three models in the training set (A) and the validation set (B) for predicting Major Pathological Response.
The accuracy, sensitivity, specificity, PPV, and NPV of the radiomics-only, clinical-only, and radiomics-clinical combined models in the training and validation cohorts were compared and illustrated in Table 3. These quantitative evaluation metrics were balanced between their respective training and validation set in all three models. They were superior in the radiomics-only model compared with the clinical-only model but performed best in the radiomics-clinical combined model. ACC was 79%, 72%, and 80%, sensitivity 85%, 83%, and 80%, specificity 71%, 54%, and 79%, PPV 83%, 75%, and 86%, and NPV 74%, 65%, and 70% for the radiomics-only, clinical-only and combined models in the training set, respectively (Table 3). ACC was 80%, 72%, and 80%, sensitivity 81%, 87%, and 75%, specificity 78%, 44%, and 89%, PPV 87%, 74%, and 92%, and NPV 70%, 67%, and 67% for the radiomics-only, clinical-only, and combined models, respectively.
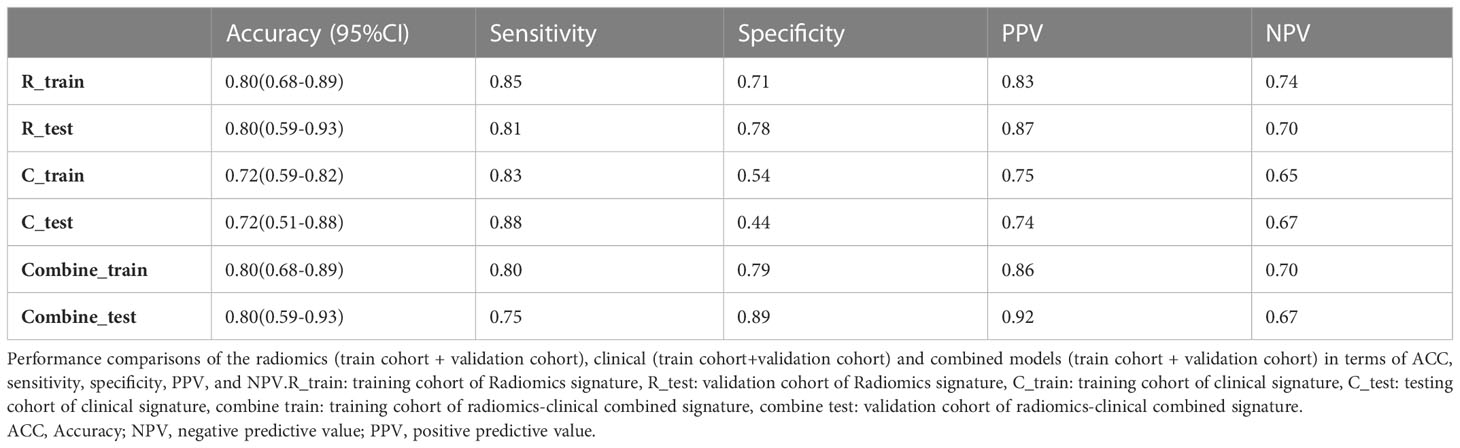
Table 3 Model predictive performance.
The radiomics-clinical combined model, which incorporated Rad-score and pathologic type, was developed and presented as a nomogram to predict MPR to neoadjuvant immunochemotherapy (Figure 4A).

Figure 4 Nomogram, Calibration curve and Decision curve analysis. (A) Nomogram and (B) Calibration curve for Major Pathological Response in the training and validation groups. (C) Decision curve analysis for each model (clinical (Clinics) model, radiomics (Radiomics) model, and integrated (combined) model).
The calibration curve of the nomogram for the probability of MPR demonstrated good agreement between prediction and observation in the training and validation cohorts of the combined model (Figure 4B). The Hosmer-Lemeshow test with a calibration curve had P-values of more than 0.05 (P=0.433, P=0.683 respectively) in the training and test cohorts, suggesting that the nomogram model fit well with the data.
The decision curve analysis (DCA) for the nomogram is presented in Figure 4C. The decision curve showed that if the threshold probability of the patient is between 0.3 and 0.95, using both the radiomics model and combined model in the current study to predict MPR added more benefit than a treat-all-patients or treat-none scheme. However, the net benefit of the clinical model was worse than that of the radiomics and combined models.
Accurate treatment response prediction is critical to stratifying and selecting patients who can benefit most from neoadjuvant immunochemotherapy and avoiding ir-sAEs. The present study developed and validated an accurate radiomics-clinical combined model to predict a major pathologic response to neoadjuvant immunochemotherapy in patients with potentially resectable NSCLC, with a favorable AUC (0.84) and a high sensitivity (80%) and specificity (79%), outperforming radiomics-only and clinical-only models.
Pre-treatment CT images show intratumor spatial variation. Previous studies have shown that pre-treatment CT radiomics could reflect tumor CD8 cell infiltration and objective response to immune checkpoint blockade (ICB) monotherapy (21). The combination of immunotherapy and chemotherapy could have a synergistic effect. Several studies have reported on the promising predictive performance of radiomics models in patients with advanced NSCLC receiving immunotherapy or immunochemotherapy. However, this is the first study to the best of our knowledge to predict MPR after neoadjuvant immune-chemotherapy in potentially resectable NSCLC using a radiomics-clinical combined method.
Due to the multiple mechanisms of immunotherapy, atypical patterns of response produced by immunotherapy (e.g., pseudo-progression, delayed responses, and hyper-progression) cannot be correctly assessed using traditional response criteria, making it difficult to judge the benefits of immunotherapy. The pathological test remains the gold standard. MPR is an early surrogate of long-term survival. The nomogram constructed in the present study only contains Rad-score and pathological type, which can be obtained with a routine CT scan and biopsy. The present model can also apply to advanced NSCLC patients to some extent, patients with higher score according to the nomogram are likely to respond better to immunochemotherapy.
Pathological type was the only chosen clinical variable to build the nomogram through univariate and multivariate logistic regression analyses in the present work. Some phase 3 randomized trials, such as Keynote 024 (22), CheckMate 026 (23), CheckMate 227 (24), and CheckMate 017 (25), have already illustrated that squamous NSCLC benefits more from immune checkpoint inhibitors (ICIs) than adenocarcinoma NSCLC. There are two reasons for this: first, both PD-L1 expression and TMB, the two major biomarkers for immunotherapy, are significantly higher in lung squamous carcinoma than lung adenocarcinoma; second, previous studies reported the majority of genomic alterations are distinct between squamous and adenocarcinoma NSCLC since they have different origins (26, 27). The difference in tumor infiltrating lymphocytes (TILs) between the two subtypes may also contribute to ICI clinical outcomes (28). In our study, 66.3% of the patients had squamous carcinoma, which is higher than in CheckMate 816 (50.8%). Our total MPR% (62.9%) thus far exceeded that of CheckMate 816 (36.9%). In addition, the MPR% of both the training and validation sets in the lung squamous carcinoma subgroup was more than 2-fold higher than the lung adenocarcinoma subgroup (Table 1).
PD-L1 failed to predict MPR in our study and was not chosen for model construction. Several neoadjuvant immunochemotherapy clinical trials, such as NADIM, LCMC3, and NEOSTAR, have already confirmed that PD-L1 is not an ideal biomarker for predicting MPR (7, 10, 29). In these studies, although a high expression of tumor PD-L1 was associated with MPR, it was not sensitive enough since a substantial fraction of patients with low PD-L1 expression also achieved MPR/PCR. Neither univariate nor multivariate logistic regression analyses in our study showed that PD-L1 is a potential predictor, which is consistent with these findings.
NLR also failed to predict MPR in NSCLC patients receiving neoadjuvant immunochemotherapy in the present work, which is inconsistent with a previous study on the topic (13). In that study, a high baseline NLR level correlated with a poor pathological response. The reasons for this may be as follows: first, the sample sizes in that study (79 patients) and ours (89 patients) were small; second, both studies were retrospective, making bias inevitable; Last but not least, NLR is an inflammatory indicator and is susceptible to various factors, such as bacterial infection, that are common in lung cancer patients. Extensive cohort studies are needed to confirm the value of NLR.
Our nomogram, which was constructed based on Rad-score and pathological type, performed exceptionally well on calibration curve and decision curve analysis, which means that the nomogram fitted well with our data and was useful clinically.
Despite its promising results, our study has several limitations. First, this is a retrospective study, making bias inevitable. A prospective study is needed to further verify our proposed model. Second, our sample size was small and imbalanced. As neoadjuvant immunochemotherapy was recently approved by the FDA in March 2022, the study period was short. Moreover, most participants were male smokers, had squamous carcinoma, and had PD-L1 levels >1%. Third, only pretreatment CT images were able to predict neoadjuvant immunochemotherapy response. Dynamic changes in radiomics (delta radiomics) and other potentially useful clinic-pathological factors, such as tumor infiltrating lymphocyte, gene-mutation profile, PET images, or serum densities of specific subgroups of immune cells has not yet been investigated. Fourth, only the targeted thoracic tumors were delineated manually and analyzed. Accurate automatic segmentation methods should be explored and developed in the future. The radiomics of lymph nodes may also provide valuable information for predicting the response to neoadjuvant immunochemotherapy. Although our current results proved that this model was useful, further confirmation in a larger cohort is mandatory before it can be applied to routine clinical practice.
A constructed easy-to-use nomogram that incorporates radiomics and clinical feature was able to predict a major pathological response to neoadjuvant immunochemotherapy with high levels of accuracy and robustness. Such a nomogram makes it a convenient tool for assisting with the individualized management of potentially resectable NSCLC.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
This study was performed in accordance with the ethical standards of the Declaration of Helsinki and was approved by the institutional review board of our institution (Approved Number: 2022-032), which waived the requirement for informed consent for this retrospective study.
Conceptualization: XL, JL, FM. Methodology: CyL, WZ, HL. Software: CL, YJ, YS. Validation: JX, XH. Formal analysis: HL, JX. Investigation: MP, MD. Resources: TX, YH, and AH. Writing - original draft preparation: CyL, WZ. Writing review and editing: YW, MD, YG. Supervision: XL, JL and FM. All authors contributed to the article and approved the submitted version.
This study was supported by the National Natural Science Foundation of China (82102157), the Hunan Provincial Natural Science Foundation for Excellent Young Scholars (2022JJ20089), the Hunan Provincial Natural Science Foundation of China (2021JJ40895, 2022JJ70053), the Research Project of Postgraduate Education and Teaching Reform of Central South University (2021JGB147, 2022JGB117), the Scientific Research Launch Project for new employees of the Second Xiangya Hospital of Central South University, the Clinical Research Center For Medical Imaging In Hunan Province (2020SK4001), and the Science and Technology Innovation Program of Hunan Province (2021RC4016).
Author HL was employed by the company GE Healthcare.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1115291/full#supplementary-material
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. Liang Y, Wakelee HA. Adjuvant chemotherapy of completely resected early stage non-small cell lung cancer (Nsclc). Transl Lung Cancer Res (2013) 2(5):403–10. doi: 10.3978/j.issn.2218-6751.2013.07.01
3. Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WE, et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol (2016) 11(1):39–51. doi: 10.1016/j.jtho.2015.09.009
4. Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WE, et al. The iaslc lung cancer staging project: Proposals for revision of the tnm stage groupings in the forthcoming (Eighth) edition of the tnm classification for lung cancer. J Thorac Oncol (2016) 11(1):39–51. doi: 10.1016/j.jtho.2015.09.009
5. Hellmann MD, Chaft JE, William WN, Rusch V, Pisters KMW, Kalhor N, et al. Pathological response after neoadjuvant chemotherapy in resectable non-Small-Cell lung cancers: Proposal for the use of major pathological response as a surrogate endpoint. Lancet Oncol (2014) 15(1):e42–50. doi: 10.1016/s1470-2045(13)70334-6
6. Pataer A, Kalhor N, Correa AM, Raso MG, Erasmus JJ, Kim ES, et al. Histopathologic response criteria predict survival of patients with resected lung cancer after neoadjuvant chemotherapy. J Thorac Oncol (2012) 7(5):825–32. doi: 10.1097/JTO.0b013e318247504a
7. Provencio M, Nadal E, Insa A, García-Campelo MR, Casal-Rubio J, Dómine M, et al. Neoadjuvant chemotherapy and nivolumab in resectable non-Small-Cell lung cancer (Nadim): An open-label, multicentre, single-arm, phase 2 trial. Lancet Oncol (2020) 21(11):1413–22. doi: 10.1016/s1470-2045(20)30453-8
8. Herbst RS, Wang M, Chen L. When immunotherapy meets surgery in non-small cell lung cancer. Cancer Cell (2022) 40(6):603–5. doi: 10.1016/j.ccell.2022.05.010
9. Soh J, Hamada A, Fujino T, Mitsudomi T. Perioperative therapy for non-small cell lung cancer with immune checkpoint inhibitors. Cancers (Basel) (2021) 13(16):4035. doi: 10.3390/cancers13164035
10. Forde PM, Spicer J, Lu S, Provencio M, Mitsudomi T, Awad MM, et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N Engl J Med (2022) 386(21):1973–85. doi: 10.1056/NEJMoa2202170
11. Laza-Briviesca R, Cruz-Bermudez A, Nadal E, Insa A, Garcia-Campelo MDR, Huidobro G, et al. Blood biomarkers associated to complete pathological response on nsclc patients treated with neoadjuvant chemoimmunotherapy included in nadim clinical trial. Clin Transl Med (2021) 11(7):e491. doi: 10.1002/ctm2.491
12. Casarrubios M, Cruz-Bermudez A, Nadal E, Insa A, Garcia Campelo MDR, Lazaro M, et al. Pretreatment tissue tcr repertoire evenness is associated with complete pathologic response in patients with nsclc receiving neoadjuvant chemoimmunotherapy. Clin Cancer Res (2021) 27(21):5878–90. doi: 10.1158/1078-0432.CCR-21-1200
13. Sun X, Feng Y, Zhang B, Huang W, Zhao X, Zhang H, et al. The role of neutrophil-to-Lymphocyte ratio in predicting pathological response for resectable nsclc treated with neoadjuvant chemotherapy combined with pd-1 checkpoint inhibitors. Cancer Res Treat (2021) 54(4):1017–29. doi: 10.4143/crt.2021.1007
14. Gridelli C, Rossi A, Carbone DP, Guarize J, Karachaliou N, Mok T, et al. Non-Small-Cell lung cancer. Nat Rev Dis Primers (2015) 1:15009. doi: 10.1038/nrdp.2015.9
15. Gillies RJ, Kinahan PE, Hricak H. Radiomics: Images are more than pictures, they are data. Radiology (2016) 278(2):563–77. doi: 10.1148/radiol.2015151169
16. Lambin P, Rios-Velazquez E, Leijenaar R, Carvalho S, van Stiphout RG, Granton P, et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur J Cancer (2012) 48(4):441–6. doi: 10.1016/j.ejca.2011.11.036
17. Chetan MR, Gleeson FV. Radiomics in predicting treatment response in non-Small-Cell lung cancer: Current status, challenges and future perspectives. Eur Radiol (2021) 31(2):1049–58. doi: 10.1007/s00330-020-07141-9
18. Zhao W, Wu Y, Xu Y, Sun Y, Gao P, Tan M, et al. The potential of radiomics nomogram in non-invasively prediction of epidermal growth factor receptor mutation status and subtypes in lung adenocarcinoma. Front Oncol (2019) 9:1485. doi: 10.3389/fonc.2019.01485
19. Zhang N, Liang R, Gensheimer MF, Guo M, Zhu H, Yu J, et al. Early response evaluation using primary tumor and nodal imaging features to predict progression-free survival of locally advanced non-small cell lung cancer. Theranostics (2020) 10(25):11707–18. doi: 10.7150/thno.50565
20. Zhao W, Xu Y, Yang Z, Sun Y, Li C, Jin L, et al. Development and validation of a radiomics nomogram for identifying invasiveness of pulmonary adenocarcinomas appearing as subcentimeter ground-glass opacity nodules. Eur J Radiol (2019) 112:161–8. doi: 10.1016/j.ejrad.2019.01.021
21. Sun R, Limkin EJ, Vakalopoulou M, Dercle L, Champiat S, Han SR, et al. A radiomics approach to assess tumour-infiltrating Cd8 cells and response to anti-Pd-1 or anti-Pd-L1 immunotherapy: An imaging biomarker, retrospective multicohort study. Lancet Oncol (2018) 19(9):1180–91. doi: 10.1016/s1470-2045(18)30413-3
22. Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med (2016) 375(19):1823–33. doi: 10.1056/NEJMoa1606774
23. Carbone DP, Reck M, Paz-Ares L, Creelan B, Horn L, Steins M, et al. First-Line Nivolumab in Stage IV or Recurrent Non-Small-Cell Lung Cancer. N Engl J Med (2017) 376(25):2415–26. doi: 10.1056/NEJMoa1613493
24. Hellmann MA-O, Paz-Ares L, Bernabe Caro R, Zurawski B, Kim SW, Carcereny Costa E, et al. Nivolumab plus ipilimumab in advanced non-Small-Cell lung cancer N Engl J Med (2019) 381(21):202–31. doi: 10.1056/NEJMoa1910231
25. Brahmer J, Reckamp KL, Baas P, Crinò L, Eberhardt WE, Poddubskaya E, et al. Nivolumab versus docetaxel in advanced squamous-cell non-Small-Cell lung cancer. N Engl J Med (2015) 373(2):123–35. doi: 10.1056/NEJMoa1504627
26. Swanton C, Govindan R. Clinical implications of genomic discoveries in lung cancer. N Engl J Med (2016) 374(19):1864–73. doi: 10.1056/NEJMra1504688
27. Cheung WK, Nguyen DX. Lineage factors and differentiation states in lung cancer progression. Oncogene (2015) 34(47):5771–80. doi: 10.1038/onc.2015.85.
28. Tian Y, Zhai X, Yan W, Zhu H, Yu J. Clinical outcomes of immune checkpoint blockades and the underlying immune escape mechanisms in squamous and adenocarcinoma nsclc. Cancer Med (2021) 10(1):3–14. doi: 10.1002/cam4.3590
Keywords: radiomics, nomogram, major pathological response, NSCLC, neoadjuvant immunochemotherapy
Citation: Liu C, Zhao W, Xie J, Lin H, Hu X, Li C, Shang Y, Wang Y, Jiang Y, Ding M, Peng M, Xu T, Hu A’r, Huang Y, Gao Y, Liu X, Liu J and Ma F (2023) Development and validation of a radiomics-based nomogram for predicting a major pathological response to neoadjuvant immunochemotherapy for patients with potentially resectable non-small cell lung cancer. Front. Immunol. 14:1115291. doi: 10.3389/fimmu.2023.1115291
Received: 03 December 2022; Accepted: 02 February 2023;
Published: 16 February 2023.
Edited by:
Bin Duan, University of Nebraska Medical Center, United StatesReviewed by:
Chunxia Su, Shanghai Pulmonary Hospital, ChinaCopyright © 2023 Liu, Zhao, Xie, Lin, Hu, Li, Shang, Wang, Jiang, Ding, Peng, Xu, Hu, Huang, Gao, Liu, Liu and Ma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xianling Liu, bGl1eGlhbmxpbmdAY3N1LmVkdS5jbg==; Jun Liu, anVubGl1MTIzQGNzdS5lZHUuY24=; Fang Ma, ZmFuZ21hQGNzdS5lZHUuY24=
†These authors contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.