 Sophie Servais1*
Sophie Servais1* Frédéric Baron1
Frédéric Baron1 Chantal Lechanteur2
Chantal Lechanteur2 Laurence Seidel3
Laurence Seidel3 Etienne Baudoux2Alexandra Briquet2Dominik Selleslag4Johan Maertens5Xavier Poire6Wilfried Schroyens7
Etienne Baudoux2Alexandra Briquet2Dominik Selleslag4Johan Maertens5Xavier Poire6Wilfried Schroyens7 Carlos Graux8
Carlos Graux8 Ann De Becker9Pierre Zachee10Aurélie Ory11Julie Herman11
Ann De Becker9Pierre Zachee10Aurélie Ory11Julie Herman11 Tessa Kerre12Yves Beguin1
Tessa Kerre12Yves Beguin1- 1Department of Clinical Hematology, University Hospital Center and University of Liège, Liège, Belgium
- 2Laboratory of Cell and Gene Therapy, University Hospital Center and University of Liège, Liège, Belgium
- 3Department of Biostatistics, SIMÉ, University Hospital Center and University of Liège, Liège, Belgium
- 4Department of Clinical Hematology, AZ Sint-Jan Brugge-Oostende AV, Bruges, Belgium
- 5Department of Clinical Hematology, University Hospital Leuven, Leuven, Belgium
- 6Department of Clinical Hematology, Cliniques Universitaires Saint-Luc, Brussels, Belgium
- 7Department of Clinical Hematology, Antwerp University Hospital, Edegem, Belgium
- 8Department of Clinical Hematology, Université Catholique de Louvain, University Hospital Center Namur (Godinne), Yvoir, Belgium
- 9Department of Clinical Hematology, Vrije Universiteit Brussel, Universitair Ziekenuis Brussel, Brussels, Belgium
- 10Department of Clinical Hematology, ZNA Stuivenberg, Antwerp, Belgium
- 11Belgian Hematology Society, Brussels, Belgium
- 12Department of Clinical Hematology, Ghent University Hospital, Ghent, Belgium
Introduction: Poor graft function (PGF) is a rare but serious complication of allogeneic hematopoietic cell transplantation (alloHCT). Due to their hematopoietic supporting properties and immune regulatory effects, multipotent mesenchymal stromal cells (MSC) could be considered a good candidate to help to restore bone marrow (BM) niches homeostasis and facilitate hematopoiesis after alloHCT.
Methods: We prospectively assessed the efficacy and safety of ex-vivo expanded BM-derived MSC from third-party donor in a series of 30 patients with prolonged severe cytopenia and PGF after alloHCT. This multicenter trial was registered at www.clinicaltrials.gov (#NTC00603330).
Results: Within 90 days post-MSC infusion, 53% (95% CI, 35 – 71%) of patients improved at least one cytopenia (overall response, OR) and 37% (95% CI, 19 - 54%) achieved a complete hematological response (CR: absolute neutrophil count, ANC >0.5 x 109/L, Hb > 80g/L and platelet count > 20 x 109/L with transfusion independence). Corresponding response rates increased to 67% (95% CI, 50 - 84%) OR and 53% (95% CI, 35 - 71%) CR within 180 days after MSC infusion. A significant decrease in red blood cells and platelets transfusion requirement was observed after MSC (median of 30-days transfusion requirement of 0.5 and 0 from d90-120 post-MSC versus 5 and 6.5 before MSC, respectively, p ≤0.001). An increase in ANC was also noted by day +90 and +180, with 3/5 patients with severe neutropenia having recovered an ANC > 1 x 109/L within the 90-120 days after MSC infusion. Overall survival at 1 year post-MSC was 70% (95% CI, 55.4 – 88.5), with all but one of the patients who achieved CR being alive. A single infusion of third-party MSC appeared to be safe, with the exception of one deep vein thrombotic event possibly related to the intervention.
Discussion: In conclusion, a single i.v. infusion of BM-derived MSC from third party donor seemed to improve hematological function after alloHCT, although spontaneous amelioration cannot be excluded. Comparative studies are warranted to confirm these encouraging results.
1. Introduction
Allogeneic hematopoietic cell transplantation (alloHCT) offers potential curative treatment for a number of hematological disorders (1). Besides graft rejection and graft failure, there are rare conditions after alloHCT where donor cells engraft but have low hematopoietic functions, resulting in prolonged cytopenias. These situations are referred to as poor graft function (PGF). Multiple definitions have been proposed in the literature for PGF (2–6). Recently, a panel of experts defined PGF as a condition with frequent dependence on red blood cell (RBC) and/or platelet transfusions and/or growth factor support despite donor cell engraftment and in the absence of disease relapse or any other cause (7).
Although rare, PGF is a serious complication after alloHCT and coping with this condition remains a challenge for patients as they may be at increased risk of infections, bleeding events or complications related to iron overload and must undergo an increased number of hospital visits for transfusion support (2, 4, 5, 8). Currently, there is no consensus on how to manage this condition. Most commonly used treatment options include growth factors such as thrombopoietin receptor agonists (TPO-RA), infusion of a donor-derived stem cell boost and second alloHCT (4, 5, 9, 10). However, these options are not always feasible and could be associated with variable efficacity and toxicity. Therefore, there is still room for improvement and development of new therapies to deal with this rare complication.
In transplanted patients, the microenvironment of the bone marrow (BM) hematopoietic stem cell niches can be altered, as a result of damages induced by the hematological malignancy, the conditioning regimen and/or immune mediated graft-versus-host reactions (11, 12). A dysfunctional BM microenvironment may compromise the hematopoietic functions of transplanted stem cells and contribute to the pathogenesis of PGF (4, 5, 13). Mesenchymal stromal cells (MSC) are multipotent progenitor cells that are a major constituent of BM hematopoietic stem cell niches. Compared to patients with good hematopoietic function after alloHCT, it has been shown that BM MSC from patients with PGF exhibited increased intracellular reactive oxygen species, higher levels of apoptosis, accelerated senescence and reduced hematopoietic supportive properties in vitro (14). Some studies indicated that MSC play a vital role in supporting HSC self-renewal, differentiation and functions by secreting an array of growth factors and cytokines (15). MSCs can also exert modulatory effects on immune reactions (16).
Co-infusion of MSC with the stem cell graft has been reported to accelerate neutrophil and platelet engraftment after alloHCT (17–21). However, their ability to restore hematopoietic functions when administered after alloHCT in patients with prolonged post-transplant cytopenia has been little explored. Here, we prospectively assessed the safety and efficacy of a single intravenous (i.v.) infusion of ex-vivo expanded BM-derived MSCs from third party donor in patients with PGF after alloHCT.
2. Patients and methods
2.1. Patient selection
Patients were eligible for this study if they had at least one severe cytopenia (absolute neutrophil count, ANC < 0.5 x 109/L, platelet count < 20 x 109/L, and/or hemoglobin level (Hb) < 80 g/L and reticulocytes < 1%) and/or were dependent on transfusions. Cytopenia(s) had to be present for more than 2 consecutive weeks beyond day + 42 after alloHCT (beyond day +60 in case of cord blood transplantation). Primary PGF was defined as incomplete reconstitution of blood counts since transplantation while secondary PGF was defined as cytopenia appearing after a period of hematological recovery after alloHCT. Patients had to be screened for full-donor chimerism, absence of disease relapse or any other identifiable cause of cytopenia (such as infection, severe acute GVHD, drug-induced myelotoxicity, peripheral destruction) at inclusion. Patients could have received a prior CD34+-selected stem cell boost for PGF before study entry, if they were deemed non-responders to this prior treatment by the investigator. Exclusion criteria consisted of HIV seropositivity and active uncontrolled infection.
Eight Belgian centers participated in this study between January 2008 and October 2014. All patients (or their legal guardians) provided written informed consent to enroll in the study. The protocol was approved by the respective ethics review boards of all participating centers and the study was conducted in accordance with the Declaration of Helsinki. This clinical trial was registered at www.clinicaltrials.gov (#NCT00603330).
2.2. Mesenchymal stromal cell production and administration
For this study, MSCs were collected from the BM (50 ± 10mL) of 13 third-party healthy volunteer donors (11 men and 2 women) at the CHU of Liège (Liège, Belgium) between 2007 and 2012. Median age of MSC donors was 26 years (range, 20 - 36). Written informed consent was obtained from each donor and the MSC harvest protocol was approved by the institutional ethics review board. MSCs were expanded, cryopreserved and stored in the clinical-grade cell production facility of the Laboratory of Cell and Gene Therapy, CHU and University of Liège (Liège, Belgium). The whole process for donor screening, BM collection, mononuclear cell isolation, MSC expansion, harvesting, cryopreservation, batch selection and thawing procedure, as well as quality control criteria has been described in details elsewhere (22–24). Briefly, MSC were cultured in fetal bovine serum (FBS)-supplemented medium in a normoxic and humidified atmosphere, harvested after 3 passages and cryopreserved in a 10% dimethyl sulfoxide (DMSO)-containing solution.
MSC were administered as a single i.v. infusion at a dose of 1-2 million(s) cells/kg body weight, through a central venous catheter and within 1 hour of thawing. Patients were premedicated with 2 mg/kg methylprednisolone and an anti-histaminic drug.
2.3. Hematological response assessment
ANC as well as the numbers of transfused RBC and/or platelet concentrates over 30-day periods were prospectively recorded at day 0 (baseline), +30, +60, +90, +120, +150 and day +180 after MSC infusion.
The primary endpoint was the best hematological response within 90 days after MSC administration (d0-90). Lineage specific response was defined as (1) ANC ≥ 1 x 109/L for neutropenia and (2) Hb > 80g/L and platelet count > 20 x 109/L with no need for transfusion over a 30-day period for anemia and thrombocytopenia respectively. A complete response (CR) was defined as trilineage response, a partial response (PR) as response in at least 1 lineage but with persistence of 1 or 2 cytopenia(s) and nonresponse (NoR) as no improvement of any of the cytopenias. For patients with monolineage cytopenia, only CR and NoR were applicable. Patients were considered to achieve an overall response (OR) if they obtained either CR or PR. In case of death, relapse of the hematological disease or a second transplant before day + 90 after MSC, OR was recorded as the best hematological response before the event (data censored afterwards).
The best hematological responses within 60 days and 180 days after MSC infusion (d0-180) were also analysed.
2.4. Other clinical outcomes
Other clinical outcomes included overall survival (OS) and disease relapse within 1 year of MSC infusion. Primary cause of death was defined according to the Copelan hierarchical algorithm (25). Acute and chronic GVHD were monitored and graded according to established criteria at study initiation (26, 27). Serious infectious events (28) were registered within 1 year of MSC infusion. Safety was also carefully monitored.
2.5. Statistical analysis
For descriptive statistics, results were expressed as numbers and proportions (%) for qualitative variables and response rates and as medians and ranges for quantitative variables. For univariate analyses, variables were analysed using Wilcoxon rank sum test or logistic regression. Graft CD34+ cell dose and time between alloHCT and MSC infusion were log-transformed to normalize their distributions. A multivariate logistic regression with stepwise selection was applied to identify baseline variables associated with ORd0-90 and CRd0-90. Overall survival (OS) was estimated by Kaplan-Meier curve. The cumulative incidence of relapse was estimated with death and second alloHCT as competing risks and the cumulative incidence of first serious infection with death, second alloHCT and relapse as competing risks. Comparisons of survival between subgroups were performed by the log-rank test. Landmark analyses at day + 90 were performed to compare survival between responders (ORd0-90 or CRd0-90) and non-responders to MSC therapy. Statistical analyses were performed using GraphPad Prism (GraphPad Software, San Diego, CA) and SAS version 9.4 (SAS Institute, Cary, NC, USA). Statistical significance was set at a level of p < 0.05.
3. Results
3.1. Patients
Thirty patients met eligibility criteria for this study. Patient characteristics are summarized in Table 1. The median age at MSC infusion was 51 years (range 11-70; 1 child and 29 adults). All patients had been transplanted for hematological malignancies, the majority of them after a reduced intensity conditioning regimen and with a peripheral blood stem cell graft. The median dose of transfused CD34+ stem cells had been 5.5 x 106/kg recipient’s weight. Seven patients had received a graft from HLA-haploidentical donor and 6 from HLA-mismatched unrelated donor. Recipient/donor ABO major or bidirectional incompatibility was present in 6 cases. Six patients had experienced acute graft-versus-host disease and 6 CMV infection after alloHCT and prior to study entry (all these complications were resolved at the time of inclusion).

Table 1 Patients characteristics (n= 30).
Three patients (10%) were treated for tri-, 17 (57%) for bi- and 10 (33%) for monolineage cytopenia(s). The majority of patients had severe anemia and/or thrombocytopenia. Only 5 patients had severe isolated or combined neutropenia. Overall, 22 patients had primary PGF and 8 secondary PGF. The median delay between alloHCT and MSC infusion was 159 days (range 42-595). Four patients had received a prior CD34+ stem cell boost (median dose 4.53 million CD34+ cells/kg) for PGF before study entry, with a median delay between boost and MSC infusion of 104 days (42-393). No patient had received or were on treatment with thrombopoietin receptor agonists before or after MSC therapy.
3.2. Hematological recovery
Within 90 days after MSC therapy, 16 patients (53%, 95% CI: 35 – 71%) achieved OR and 11 patients (37%, 95% CI, 19 - 54%) achieved CR (Figure 1A). Among the 4 patients who had been pre-treated with a CD34+ stem cell boost, 1 of them responded to MSC therapy and achieved CRd0-90 (the 3 others had NoRd0-90).
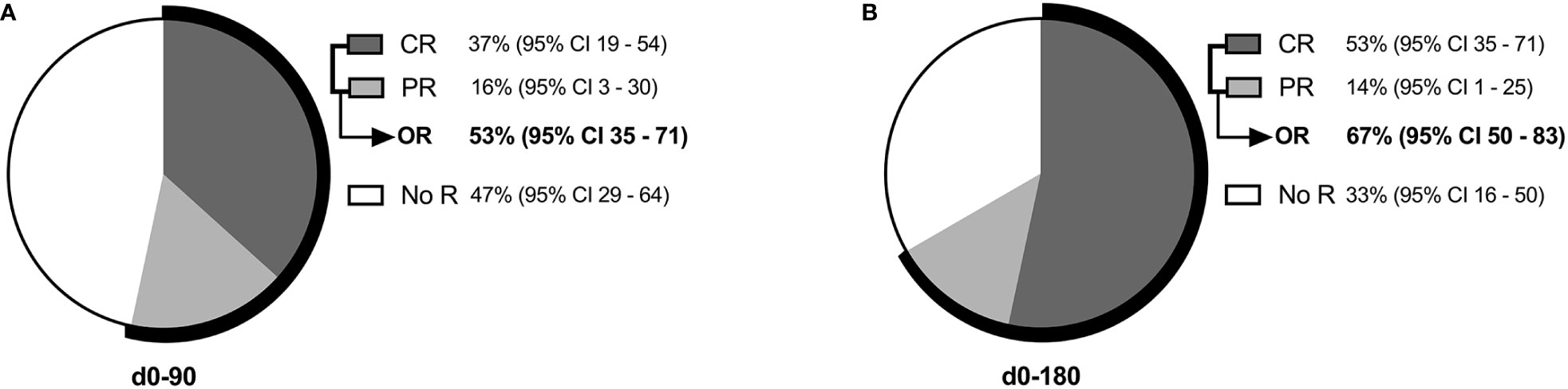
Figure 1 Hematological response (A) within 90 days (d0-90) and (B) within 180 days (d0-180) of MSC therapy. CR refers to complete response; NoR, no response; OR, overall response (CR + PR); PR, partial response.
Response rate increased to 67% (20 patients, 95% CI, 50 - 84%) OR and 53% (16 patients, 95% CI, 35 - 71%) CR within 180 days after MSC infusion (Figure 1B). All patients who achieved CRd0-90 maintained satisfactory hematological function within the next 3 months (CRd0-180). Two patients with PRd0-90 and 3 with NoRd0-90 converted to CRd0-180.
Considering earlier time-point, eight patients achieved OR (27%, 95% CI: 14-44%) and 3 achieved CR (10%, 95% CI: 3-26%) within 60 days after MSC (Supplemental Figure S1).
Lineage-specific recovery over time after MSC infusion is depicted in Figure 2. Twenty-six and 22 patients suffered from severe anemia and thrombocytopenia, respectively, and were transfusion-dependent before MSC therapy. The median number of transfusions in a 30-day period significantly decreased from d30-60 post-MSC for RBC and from d60-90 for platelet transfusions, and dropped to 0.5 and 0 from d90-120 post-MSC (versus 5 and 6.5 before MSC, respectively, p ≤0.001) (Figures 2A, B). An increase in ANC was also observed after MSC therapy in comparison with baseline, which was statistically significant by days + 90 and +180 (Figure 2C). Among the 5 patients who had severe neutropenia by the time of MSC therapy, 3 recovered an ANC > 1 x 10exp9/L within 90-120 days after MSC infusion.
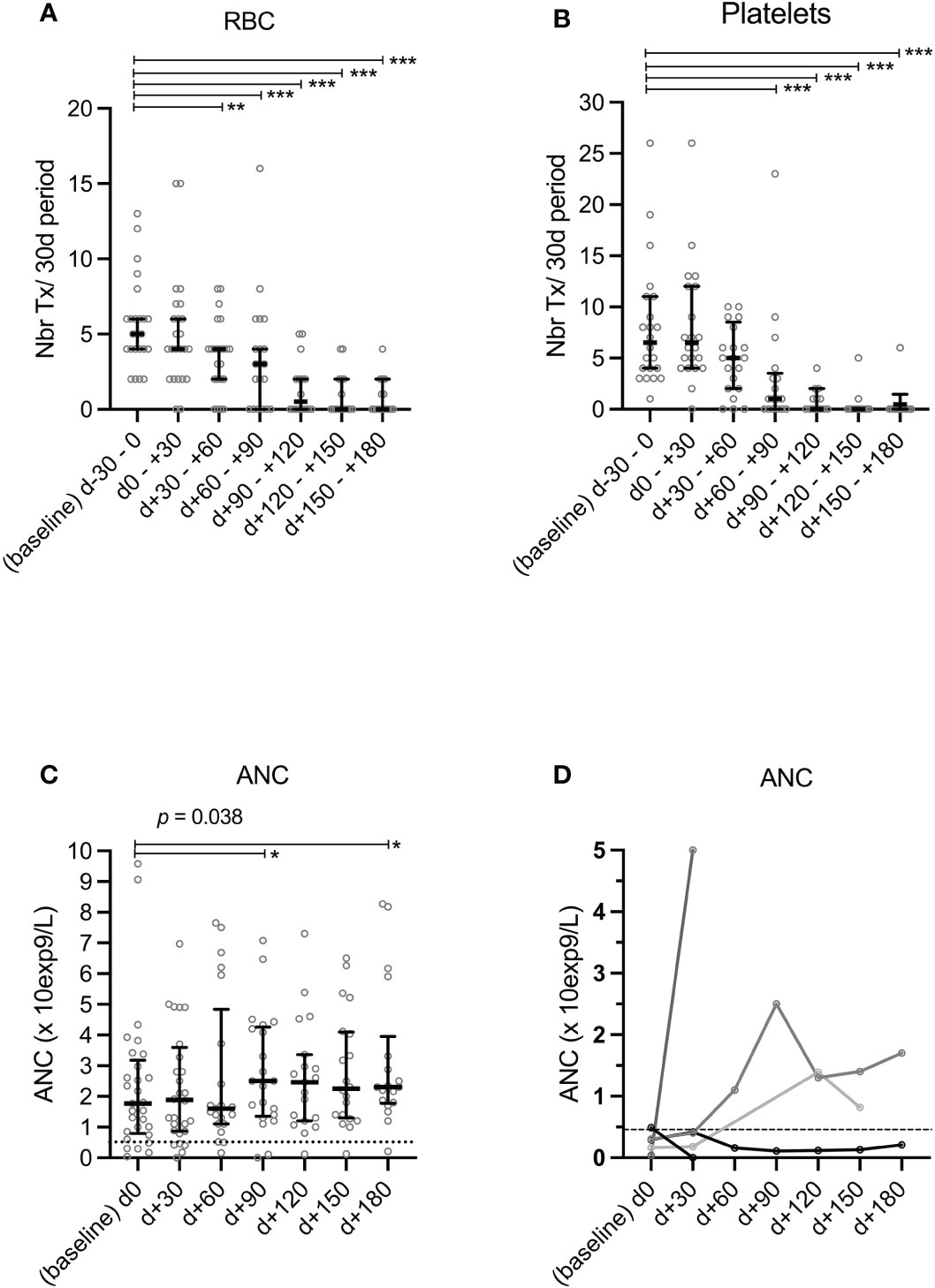
Figure 2 Prospective monitoring of transfusion requirements and ANC after MSC therapy. Numbers of transfused red blood cell (RBC) (A) and platelet (B) concentrates over 30-day periods and circulating absolute neutrophil counts (ANC) (C, D) were prospectively recorded from baseline and up to 180 days after MSC infusion. Data were censored at relapse of hematological malignancy or second transplantation. Among the 5 patients who had severe neutropenia by the time of MSC therapy (D), 1 received a second alloHCT on d+33 after MSC for persistent PGF (NoR at d+30); 1 recovered an ANC > 1x109/L at d+30 then relapsed from the malignant hematological pathology, 2 recovered an ANC > 1x109/L at d90-120 and 1 retained persistent severe neutropenia. *p<0.05, **p<0.01, ***p<0.001 (Wilcoxon rank sum test). ANC refers to absolute neutrophil counts; Nbr Tx, number of transfusions; RBC, red blood cells.
We further analyzed associations between several baseline parameters (patient and transplant-related characteristics, history of prior aGVHD and CMV infection, number of cytopenias, primary vs. secondary PGF, prior stem cell boost and delay between alloHCT and MSC infusion) and response to MSC therapy, as assessed by ORd0-90 and CRd0-90, but we did not identify any significant association in multivariate analyses (results of the univariate analyses are illustrated in Supplemental Table S1).
3.3. Survival
The 1-year OS after MSC therapy was 70% (95% CI, 55.4 – 88.5) (Figure 3). Relapse of the hematological malignancy and infections were the leading causes of deaths (Table 2). No difference in survival was observed when comparing responders and non-responders to MSC therapy, as assessed by ORd0-90 and CRd0-90 (landmark analysis at day + 90, p= 0.88 and p= 0,61, respectively) (Supplemental Figure S2). Of note, 10 of the 11 patients who achieved CRd0-90 were alive at 1 year (1 died because of relapse of hematological malignancy).
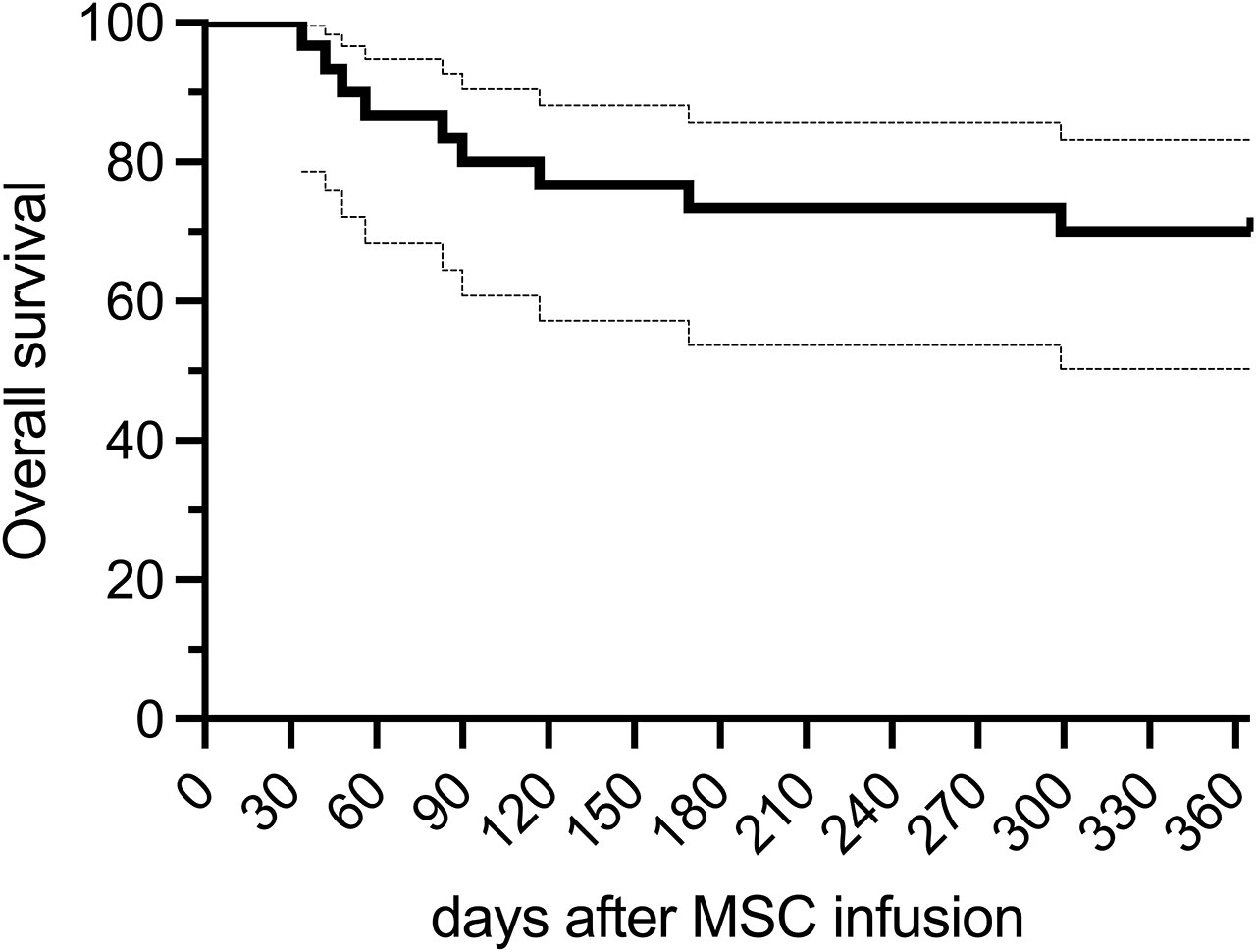
Figure 3 Overall survival (OS) after MSC therapy.
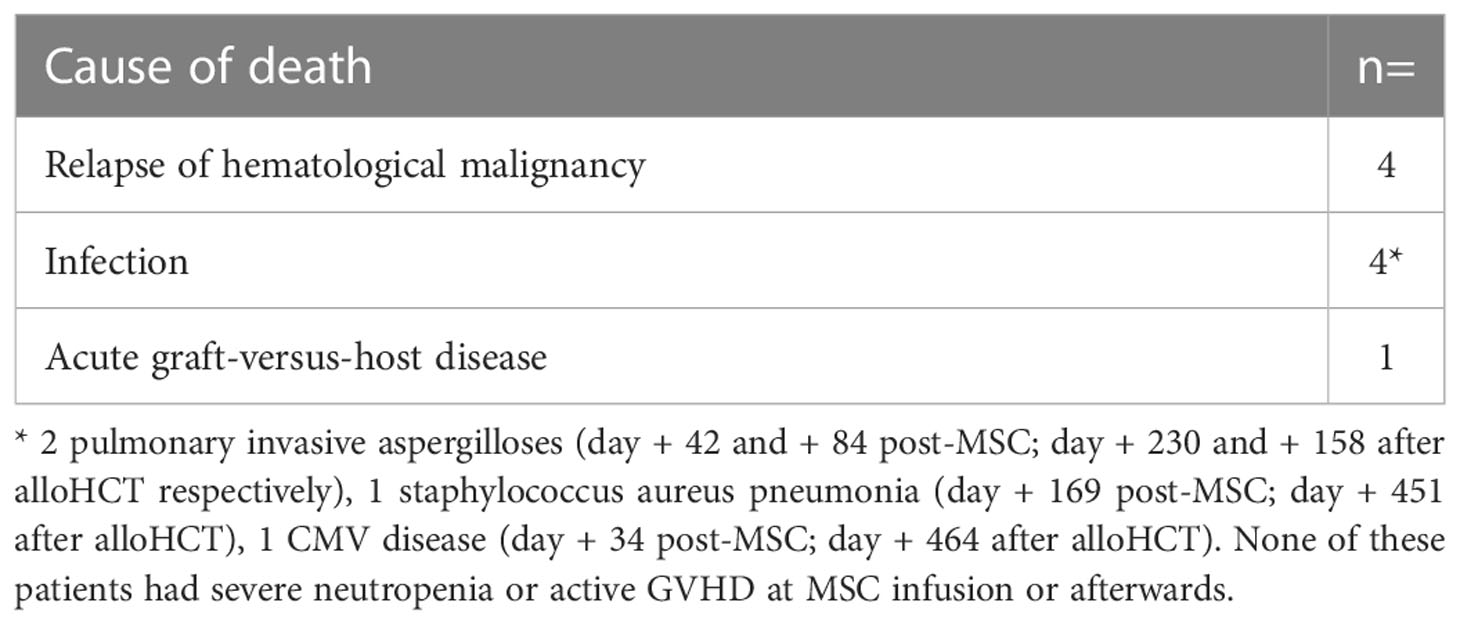
Table 2 Primary cause of death within 1 year after MSC infusion.
3.4. Safety data and other clinical outcomes
No immediate reaction to MSC perfusion was reported. Two deep vein thrombotic (DVT) events were reported as serious adverse events following MSC therapy. The first patient developed seizure due to cerebral sinus thrombosis on day + 8 after MSC infusion (day + 191 after alloHCT for B-cell acute lymphoblastic leukemia). No signs of leukemic relapse, active infection or GVHD were present at the time of thrombosis. The relationship with MSC therapy could not be excluded. The second patient developed deep vein thrombosis of the left arm at day + 199 after MSC therapy. Due to a predisposing factor (central venous implantable device on this side) and the delay after MSC therapy, this event was deemed unrelated to MSC therapy by the investigators. None of these episodes was fatal.
The cumulative incidence of relapse of the hematological malignancy at 1 year after MSC infusion was 20% (95% CI: 7.9–35.9%) (Supplemental Figure S3). Median time from MSC infusion to relapse was 92 days (range 28-280 days). No patient developed clinically significant (grade II-IV) acute GVHD or (moderate/severe) chronic GVHD within 1 year after MSC infusion. A total of 30 serious infections (15 of bacterial, 10 of viral and 5 of fungal origin) was recorded during the 1-year follow-up period after MSC therapy. The 1-year cumulative incidence of a first serious infection after initiation of MSC therapy was 60% (95% CI: 39.7-75.4%) and most of them occurred during the first 90 days after MSC therapy (Supplemental Figure S3). Four infections were fatal (Table 2). No secondary malignancy was observed during the first year after MSC therapy, with the exception of one case of basocellular skin carcinoma (at day + 231 after MSC).
4. Discussion
In this multicenter prospective study, we assessed efficacy and safety of a single i.v. infusion of 1-2 millions/kg BM-derived MSCs from third party donors in 30 patients with PGF after alloHCT. MSCs were expanded ex vivo in FBS-supplemented medium in normoxic atmosphere, early passaged and cryopreserved in the setting of an academic clinical-grade cell production facility, thereby ensuring a homogeneous manufacturing process (22, 24). In these conditions, more than half of the patients improved at least one cytopenia and more than one third achieved a complete hematological response to MSC therapy within the 90 days after their infusion. Interestingly, all patients who achieved CRd0-90 maintained a satisfactory hematological function within the next 3 months and all but one of them were alive at 1 year.
These results are consistent with results from previous smaller reports having evaluated BM-derived MSC from third party donors for PGF (29–32). Among them, Liu et al. reported even more encouraging results, with 17 of 20 patients with primary or secondary PGF experiencing hematological response (defined as ANC > 0.5 × 109/L and platelets > 20 × 109/L for 3 consecutive days) to MSC therapy (31). In that study, MSC could be administered for 1 – 3 consecutive courses (at 28-days intervals), based on response to a prior infusion. Whether repeated infusions of MSC may improve the response rate to MSC-based therapy for PGF is unknown. Unfortunately, a direct comparison of our results with this previous study is not possible due to differences in inclusion criteria, definition and timing of response assessment.
Transplantation of donor-derived CD34+-selected stem cell boost and pharmacological therapy with TPO-RA are under investigation as other options for managing prolonged thrombocytopenia and PGF after alloHCT. Two recent systematic reviews have summarized current available evidence utilizing these approaches, respectively (9, 10). They have reported encouraging results in terms of efficacy (with overall responses ranging from 70% to 80%) and acceptable toxicity profile for both of these options, but with the limitations that most of the current evidence is derived from retrospective real-world analyses and case-series, with a potential publication bias toward successful treatment outcomes. Here also, a direct comparison of our results with these studies is difficult due to heterogeneity in inclusion criteria as well as definition of PGF and criteria and timing of response assessment. Future prospective trials, ideally comparative, are needed to determine the efficacy and safety of each of these three options in the management of PGF after alloHCT. Standardization of the definition and timing of evaluation of the hematological response criteria should be recommended in order to homogenize these future clinical trials.
Nevertheless, current evidence of treatment with a stem cell boost or TPO-RA revealed that some patients are refractory to these therapies. Moreover, the option of a stem cell boost could be limited by logistic challenges of donor availability and concerns about risks of GVHD. Whether MSC therapy represents an alternative option for those patients with PGF for whom a CD34+-stem cell boost is not feasible or for those who were unresponsive to it and/or to treatment with TPO-RA is an open question. Our cohort included 4 patients with refractory cytopenia after prior therapy with a CD34+ stem cell boost. Among them, one achieved complete hematological recovery within 90 days after MSC therapy. None of our patients had received TPO-RA before or after MSC therapy.
Whether the combination of several approaches (CD34-stem cell boost, TPO-RA, MSC) can lead to beneficial effects in terms of efficacy and toxicity of the procedures needs to be explored in the future. To the best of our knowledge, co-administration of MSC with a CD34+-stem cell boost for PGF has never been explored yet. Recently, Zhu et al. reported their experience of 16 patients with prolonged thrombocytopenia after alloHCT treated with 4-6 weekly administrations of umbilical cord MSC (1×106 cells/kg) in combination with avatrombopag (a second generation TPO-RA) (32). Thirteen of these patients improved their platelet count above 50 x 109/L after a median of 32 days of combined therapy. However, safety and efficacy of this combined approach has to be confirmed in further prospective studies.
The way data was collected and analyzed (over a 30-day period) in our study did not allow us to determine the precise timing of response to MSC therapy. The response rate observed within d0-60 after MSC infusion was approximately two times lower than that observed within d0-90. Does this mean that the hematopoietic supporting effects of MSCs mainly appear during the second month after MSC infusion and carry over to d60-90 or is it the manifestation of a spontaneous hematopoietic recovery over time? It’s impossible to conclude in the absence of a control group. Some other studies reported that neutrophiles and/or platelet recovery after hematopoietic supportive therapies with either MSC or TPO-RA for PGF was indeed generally observed during the second month of treatment (31, 33, 34).
In our study, we could not identify any baseline predictive factor of hematological response to MSC therapy. Our small cohort of patients indicated that MSC appeared to be equally effective for primary and secondary PGF, patients with single and multiple lineage cytopenia(s) and regardless of prior transplantation modalities and prior history of acute GVHD or CMV infection. Nevertheless, our results have to be interpreted with caution, regarding the small number of patients.
Our cohort included 10 patients with monolineage severe cytopenia, and therefore was not strictly limited to patients with at least bilineage cytopenia, as suggested to be the definition of PGF by the European Society of Blood and Marrow Transplantation (EBMT) and some other experts or investigators of recent studies (2–4, 8, 35, 36). However, in our analysis, mono- versus multiple lineage cytopenia did not appear as a factor influencing response to MSC in univariate and multivariate analyses, therefore precluding that this subgroup of patients could have influence the response rate of the overall cohort. Moreover, prolonged severe monolineage cytopenia (i.e. isolated neutropenia or thrombocytopenia) has also been reported to be associated with adverse outcomes after alloHCT (37, 38), could be a challenge to improve and therefore could still represent a real clinical concern. Recently, a panel of experts of the American Society for Transplantation and Cellular Therapy proposed a broader definition for PGF as a situation of frequent dependence on transfusions of RBC and/or platelets and/or growth factor support, without precising the number of cytopenia required to fit the definition (7). Unfortunately, only 5 patients in our cohort had isolated or combined severe neutropenia, thus precluding the possibility to assess the effects of MSC on ANC recovery.
We observed a 1-year OS of 70% after MSC infusion in our cohort, without difference between responders and non-responders to the therapy. This survival rate contrasts with some prior retrospective reports showing very dismal outcome in patients without hematological recovery, with survival as low as 25% and 6% of at 1 and 2 years (2, 8). However, heterogenous outcomes are reported in the literature for patients with PGF (2, 8, 39, 40). Variability in PGF definitions between studies might possibly account for this heterogeneity. The presence or absence of severe neutropenia could likely be a factor influencing the outcomes, with increased nonrelapse mortality being expected in PGF without neutrophil recovery because of the risk of infectious complications. The few numbers of patients with severe neutropenia included in our study might have accounted for the favorable OS of our cohort.
Regarding acute toxicity, MSC i.v. infusion appeared to be safe in our study, with the exception of one deep vein thrombotic event occurring a few days after MSC administration whose relationship to the intervention is not clear. Based on our previously published clinical experience with i.v. infusions of BM-derived MSCs from third-party donors (produced and administered in the same manner as described here), no other deep vein thrombotic event has been observed in more than 200 treated patients for a range of conditions other than PGF (including GVHD after alloHCT, solid organ transplantation, coronavirus disease [COVID-19]) (22–24, 41–45). A recent meta-analysis of prospective randomized controlled trials (RTC) that compared intravascular administration of MSC to controls in various indications in adult patients (55 studies, 2696 patients) did not suggest either an association between MSC treatment and thrombotic/embolic events (46). However, in vitro procoagulant effects of MSC on human blood and plasma have been described, although MSC procoagulant phenotype seem to be influenced by multiple factors including the MSC source and manufacturing (passage number, cryopreservation,…) but also patient-related factors (pre-existing inflammation) (47–49). Therefore, although no significant association between MSC and thrombotic events has been detected so far in humans, it is still possible that these events are rare and we encourage researchers to continue to monitor and report them in future MSC studies to confirm the absence of safety signals.
More than half of our patients experienced at least one serious infection within the first year after MSC therapy and four of them died because of infection as primary cause of death. Similarly, Liu et al. reported a high number of infectious events in their cohort of patients with PGF treated with MSC (31). Infections are frequent complications and a leading cause of mortality after alloHCT (50). Susceptibility to infections can also be higher in patients with PGF (as a consequence of neutropenia, iron overload, increased hospitalizations and hospital visits). Whether MSC with immunosuppressive properties could confer an increased risk of serious or fatal infections in this fragile population could not be established from our and Liu’s studies, since there was no comparative control group. Reassuringly, several meta-analyses of RCTs with MSC administered in various clinical settings (not limited to alloHCT) have reported no association between MSC therapy and an increased risk of infections (46, 48).
Limits of our study stem in the small number of patients, inclusion of patients with mono- versus multilineage cytopenia(s), the small numbers of patients with severe neutropenia, and the absence of a control group that could not allow us to apprehend the potential contribution of spontaneous recovery of the hematopoietic function over time.
In conclusion, our study provides encouraging results on the efficacy and safety of MSC-based therapy for PGF and prolonged severe cytopenia after alloHCT. Future studies, ideally comparative, are warranted to confirm them.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the respective ethics review boards of all participating centers and by the Comité d’Éthique Hospitalo-Facultaire Universitaire deLiège, Liège, Belgium (central commitee).
Author contributions
Conception and design: FB, YB; Provision of study material or patients: All authors; Collection and assembly of data: SS, FB, AO, YB; Data analysis and interpretation: SS, LS, YB; Manuscript writing: SS, YB. All authors contributed to the article and approved the submitted version.
Funding
YB and FB are Senior Research Associate at the FNRS. SS is Postdoctoral Researcher at the Belgian Foundation against Cancer (FBC). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgments
The authors would like to thank the patients, the medical staffs of participating centers for competent care given to the patients, as well as the staff of the Laboratory of Cell and Gene Therapy (LTCG), ULiege for MSC production.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1106464/full#supplementary-material
References
1. Snowden JA, Sánchez-Ortega I, Corbacioglu S, Basak GW, Chabannon C, de la Camara R, et al. Indications for haematopoietic cell transplantation for haematological diseases, solid tumours and immune disorders: current practice in Europe, 2022. Bone Marrow Transplant. (2022) 57(8):1217–39. doi: 10.1038/s41409-022-01691-w
2. Zhao Y, Gao F, Shi J, Luo Y, Tan Y, Lai X, et al. Incidence, risk factors, and outcomes of primary poor graft function after allogeneic hematopoietic stem cell transplantation. Biol Blood marrow Transplant J Am Soc Blood Marrow Transplant. (2019) 25(9):1898–907. doi: 10.1016/j.bbmt.2019.05.036
3. Sun YQ, He GL, Chang YJ, Xu LP, Zhang XH, Han W, et al. The incidence, risk factors, and outcomes of primary poor graft function after unmanipulated haploidentical stem cell transplantation. Ann Hematol (2015) 94(10):1699–705. doi: 10.1007/s00277-015-2440-x
4. Man Y, Lu Z, Yao X, Gong Y, Yang T, Wang Y. Recent advancements in poor graft function following hematopoietic stem cell transplantation. Front Immunol (2022) 13:911174. doi: 10.3389/fimmu.2022.911174
5. Prabahran A, Koldej R, Chee L, Ritchie D. Clinical features, pathophysiology, and therapy of poor graft function post-allogeneic stem cell transplantation. Blood Adv (2022) 6(6):1947–59. doi: 10.1182/bloodadvances.2021004537
6. Cuadrado MM, Szydlo RM, Watts M, Patel N, Renshaw H, Dorman J, et al. Predictors of recovery following allogeneic CD34+-selected cell infusion without conditioning to correct poor graft function. Haematologica (2020) 105(11):2639–46.
7. Kharfan-Dabaja MA, Kumar A, Ayala E, Aljurf M, Nishihori T, Marsh R, et al. Standardizing definitions of hematopoietic recovery, graft rejection, graft failure, poor graft function, and donor chimerism in allogeneic hematopoietic cell transplantation: A report on behalf of the American society for transplantation and cellular Th. In: Transplantation and cellular therapy, vol. 27. . United States (2021). p. 642–9.
8. Prabahran A, Koldej R, Chee L, Wong E, Ritchie D. Evaluation of risk factors for and subsequent mortality from poor graft function (PGF) post allogeneic stem cell transplantation. Leuk Lymphoma. (2021) 62(6):1482–9. doi: 10.1080/10428194.2021.1872072
9. Mahat U, Rotz SJ, Hanna R. Use of thrombopoietin receptor agonists in prolonged thrombocytopenia after hematopoietic stem cell transplantation. Biol Blood marrow Transplant J Am Soc Blood Marrow Transplant. (2020) 26(3):e65–73. doi: 10.1016/j.bbmt.2019.12.003
10. Shahzad M, Siddiqui RS, Anwar I, Chaudhary SG, Ali T, Naseem M, et al. Outcomes with CD34-selected stem cell boost for poor graft function after allogeneic hematopoietic stem cell transplantation: A systematic review and meta-analysis. Transplant Cell Ther (2021) 27(10):877.e1–8. doi: 10.1016/j.jtct.2021.07.012
11. Kong Y, Wang YT, Hu Y, Han W, Chang YJ, Zhang XH, et al. The bone marrow microenvironment is similarly impaired in allogeneic hematopoietic stem cell transplantation patients with early and late poor graft function. Bone Marrow Transplant. (2016) 51(2):249–55. doi: 10.1038/bmt.2015.229
12. Kong Y, Chang YJ, Wang YZ, Chen YH, Han W, Wang Y, et al. Association of an impaired bone marrow microenvironment with secondary poor graft function after allogeneic hematopoietic stem cell transplantation. Biol Blood marrow Transplant J Am Soc Blood Marrow Transplant. (2013) 19(10):1465–73. doi: 10.1016/j.bbmt.2013.07.014
13. Kong Y. Poor graft function after allogeneic hematopoietic stem cell transplantation-an old complication with new insights(☆). Semin Hematol (2019) 56(3):215–20. doi: 10.1053/j.seminhematol.2018.08.004
14. Song Y, Zhao HY, Lyu ZS, Cao XN, Shi MM, Wen Q, et al. Dysfunctional bone marrow mesenchymal stem cells in patients with poor graft function after allogeneic hematopoietic stem cell transplantation. Biol Blood marrow Transplant J Am Soc Blood Marrow Transplant. (2018) 24(10):1981–9. doi: 10.1016/j.bbmt.2018.06.021
15. Crippa S, Santi L, Berti M, De Ponti G, Bernardo ME. Role of ex vivo expanded mesenchymal stromal cells in determining hematopoietic stem cell transplantation outcome. Front Cell Dev Biol (2021) 9:663316. doi: 10.3389/fcell.2021.663316
16. Song N, Scholtemeijer M, Shah K. Mesenchymal stem cell immunomodulation: Mechanisms and therapeutic potential. Trends Pharmacol Sci (2020) 41(9):653–64. doi: 10.1016/j.tips.2020.06.009
17. Ball LM, Bernardo ME, Roelofs H, Lankester A, Cometa A, Egeler RM, et al. Cotransplantation of ex vivo expanded mesenchymal stem cells accelerates lymphocyte recovery and may reduce the risk of graft failure in haploidentical hematopoietic stem-cell transplantation. Blood (2007) 110(7):2764–7. doi: 10.1182/blood-2007-04-087056
18. Li T, Luo C, Zhang J, Wei L, Sun W, Xie Q, et al. Efficacy and safety of mesenchymal stem cells co-infusion in allogeneic hematopoietic stem cell transplantation: a systematic review and meta-analysis. Stem Cell Res Ther (2021) 12(1):246. doi: 10.1186/s13287-020-02064-0
19. Carrancio S, Romo C, Ramos T, Lopez-Holgado N, Muntion S, Prins HJ, et al. Effects of MSC coadministration and route of delivery on cord blood hematopoietic stem cell engraftment. Cell Transplant. (2013) 22(7):1171–83. doi: 10.3727/096368912X657431
20. Preciado S, Muntión S, Sánchez-Guijo F. Improving hematopoietic engraftment: Potential role of mesenchymal stromal cell-derived extracellular vesicles. Stem Cells (2021) 39(1):26–32. doi: 10.1002/stem.3278
21. Preciado S, Sirerol-Piquer MS, Muntión S, Osugui L, Martí-Chillón GJ, Navarro-Bailón A, et al. Co-Administration of human MSC overexpressing HIF-1α increases human CD34(+) cell engraftment in vivo. Stem Cell Res Ther (2021) 12(1):601.
22. Lechanteur C, Briquet A, Giet O, Delloye O, Baudoux E, Beguin Y. Clinical-scale expansion of mesenchymal stromal cells: a large banking experience. J Transl Med [Internet]. (2016) 14(1):145. doi: 10.1186/s12967-016-0892-y
23. Servais S, Baron F, Lechanteur C, Seidel L, Selleslag D, Maertens J, et al. Infusion of bone marrow derived multipotent mesenchymal stromal cells for the treatment of steroid-refractory acute graftversus- host disease: A multicenter prospective study. Oncotarget (2018) 9(29). doi: 10.18632/oncotarget.25020
24. Lechanteur C, Briquet A, Bettonville V, Baudoux E, Beguin Y. MSC manufacturing for academic clinical trials: From a clinical-grade to a full GMP-compliant process. Cells (2021) 10(6). doi: 10.3390/cells10061320
25. Copelan E, Casper JT, Carter SL, van Burik JAH, Hurd D, Mendizabal AM, et al. A scheme for defining cause of death and its application in the T cell depletion trial. Biol Blood marrow Transplant J Am Soc Blood Marrow Transplant. (2007) 13(12):1469–76. doi: 10.1016/j.bbmt.2007.08.047
26. Filipovich AH, Weisdorf D, Pavletic S, Socie G, Wingard JR, Lee SJ, et al. National institutes of health consensus development project on criteria for clinical trials in chronic graft-versus-Host disease: I. diagnosis and staging working group report. Biol Blood Marrow Transplant [Internet]. (2005) 11(12):945–56. Available at: https://linkinghub.elsevier.com/retrieve/pii/S1083879105006312.
27. Przepiorka D, Weisdorf D, Martin P, Klingemann HG, Beatty P, Hows J, et al. Bone marrow transplant [Internet], vol. 15. (19941995). p. 825–8.
28. Servais S, Lengline E, Porcher R, Carmagnat M, Peffault de Latour R, Robin M, et al. Long-term immune reconstitution and infection burden after mismatched hematopoietic stem cell transplantation. Biol Blood Marrow Transplant [Internet] (2014) 20(4):507–17. Available at: http://linkinghub.elsevier.com/retrieve/pii/S1083879114000020.
29. Meuleman N, Tondreau T, Ahmad I, Kwan J, Crokaert F, Delforge A, et al. Infusion of mesenchymal stromal cells can aid hematopoietic recovery following allogeneic hematopoietic stem cell myeloablative transplant: a pilot study. Stem Cells Dev (2009) 18(9):1247–52. doi: 10.1089/scd.2009.0029
30. Sánchez-Guijo FM, López-Villar O, López-Anglada L, Villarón EM, Muntión S, Díez-Campelo M, et al. Allogeneic mesenchymal stem cell therapy for refractory cytopenias after hematopoietic stem cell transplantation. Transfusion (2012) 52(5):1086–91. doi: 10.1111/j.1537-2995.2011.03400.x
31. Liu X, Wu M, Peng Y, Chen X, Sun J, Huang F, et al. Improvement in poor graft function after allogeneic hematopoietic stem cell transplantation upon administration of mesenchymal stem cells from third-party donors: A pilot prospective study. Cell Transplant. (2014) 23(9):1087–98. doi: 10.3727/096368912X661319
32. Zhu L, Liu J, Kong P, Gao S, Wang L, Liu H, et al. Analysis of the efficacy and safety of avatrombopag combined with MSCs for the treatment of thrombocytopenia after allogeneic hematopoietic stem cell transplantation. Front Immunol (2022) 13:910893. doi: 10.3389/fimmu.2022.910893
33. Uria-Oficialdegui ML, Alonso L, Benitez-Carabante MI, Renedo B, Oliveras M, Diaz-de-Heredia C. Use of eltrombopag for the treatment of poor graft function after hematopoietic stem cell transplantation in children. Pediatr Transplant. (2021) 25(4):e14010. doi: 10.1111/petr.14010
34. Peffault de Latour R, Chevret S, Ruggeri AL, Suarez F, Souchet L, Michonneau D, et al. Romiplostim in patients undergoing hematopoietic stem cell transplantation: results of a phase 1/2 multicenter trial. Vol. 135 Blood. United States; (2020) p:227–9.
35. Carreras E, Dufour C, Mohty M, Kröger N. The EBMT handbook: Hematopoietic stem cell transplantation and cellular therapies. Cham, Switzerland: Springer N (2019).
36. McLornan DP, Hernandez-Boluda JC, Czerw T, Cross N, Joachim Deeg H, Ditschkowski M, et al. Allogeneic haematopoietic cell transplantation for myelofibrosis: proposed definitions and management strategies for graft failure, poor graft function and relapse: best practice recommendations of the EBMT chronic malignancies working party. Leukemia (2021) 35(9):2445–59. doi: 10.1038/s41375-021-01294-2
37. Yamazaki R, Kuwana M, Mori T, Okazaki Y, Kawakami Y, Ikeda Y, et al. Prolonged thrombocytopenia after allogeneic hematopoietic stem cell transplantation: Associations with impaired platelet production and increased platelet turnover. Bone Marrow Transplant. (2006) 38(5):377–84. doi: 10.1038/sj.bmt.1705444
38. Bolwell B, Pohlman B, Sobecks R, Andresen S, Brown S, Rybicki L, et al. Prognostic importance of the platelet count 100 days post allogeneic bone marrow transplant. Bone Marrow Transplant. (2004) 33(4):419–23. doi: 10.1038/sj.bmt.1704330
39. Alchalby H, Yunus DR, Zabelina T, Ayuk F, Kröger N. Incidence and risk factors of poor graft function after allogeneic stem cell transplantation for myelofibrosis. Bone Marrow Transplant. (2016) 51(9):1223–7. doi: 10.1038/bmt.2016.98
40. Reich-Slotky R, Al-Mulla N, Hafez R, Segovia-Gomez J, Goel R, Mayer S, et al. Poor graft function after T cell-depleted allogeneic hematopoietic stem cell transplant. Leuk Lymphoma. (2020) 61(12):2894–9. doi: 10.1080/10428194.2020.1789622
41. Baron F, Lechanteur C, Willems E, Bruck F, Baudoux E, Seidel L, et al. Cotransplantation of mesenchymal stem cells might prevent death from graft-versus-host disease (GVHD) without abrogating graft-versus-tumor effects after HLA-mismatched allogeneic transplantation following nonmyeloablative conditioning. Biol Blood marrow Transplant J Am Soc Blood Marrow Transplant. (2010) 16(6):838–47. doi: 10.1016/j.bbmt.2010.01.011
42. Grégoire C, Layios N, Lambermont B, Lechanteur C, Briquet A, Bettonville V, et al. Bone marrow-derived mesenchymal stromal cell therapy in severe COVID-19: Preliminary results of a phase I/II clinical trial. Front Immunol (2022) 13:932360. doi: 10.3389/fimmu.2022.932360
43. Moermans C, Lechanteur C, Baudoux E, Giet O, Henket M, Seidel L, et al. Impact of cotransplantation of mesenchymal stem cells on lung function after unrelated allogeneic hematopoietic stem cell transplantation following non-myeloablative conditioning. Transplant [Internet] (2014) 98(3):348–53. Available at: http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00007890-201408150-00020.
44. Detry O, Vandermeulen M, Delbouille MH, Somja J, Bletard N, Briquet A, et al. Infusion of mesenchymal stromal cells after deceased liver transplantation: A phase I-II, open-label, clinical study. J Hepatol (2017) 67(1):47–55. doi: 10.1016/j.jhep.2017.03.001
45. Vandermeulen M, Mohamed-Wais M, Erpicum P, Delbouille MH, Lechanteur C, Briquet A, et al. Infusion of allogeneic mesenchymal stromal cells after liver transplantation: A 5-year follow-up. Liver Transplant Off Publ Am Assoc Study Liver Dis Int Liver Transplant Soc (2022) 28(4):636–46. doi: 10.1002/lt.26323
46. Thompson M, Mei SHJ, Wolfe D, Champagne J, Fergusson D, Stewart DJ, et al. Cell therapy with intravascular administration of mesenchymal stromal cells continues to appear safe: An updated systematic review and meta-analysis. EClinicalMedicine (2020) 19:100249. doi: 10.1016/j.eclinm.2019.100249
47. Grégoire C, Ritacco C, Hannon M, Seidel L, Delens L, Belle L, et al. Comparison of mesenchymal stromal cells from different origins for the treatment of graft-vs.-Host-Disease in a humanized mouse model. Front Immunol (2019) 10:619. doi: 10.3389/fimmu.2019.00619
48. Lalu MM, McIntyre L, Pugliese C, Fergusson D, Winston BW, Marshall JC, et al. Safety of cell therapy with mesenchymal stromal cells (SafeCell): A systematic review and meta-analysis of clinical trials. In: Beltrami AP, editor. PLoS one [Internet], vol. 7 (2012). Available at: http://dx.plos.org/10.1371/journal.pone.0047559.
49. Ringdén O, Moll G, Gustafsson B, Sadeghi B. Mesenchymal stromal cells for enhancing hematopoietic engraftment and treatment of graft-Versus-Host disease, hemorrhages and acute respiratory distress syndrome. In: Fron Immunol (Switzerland) (2022) 13:839844.
Keywords: poor graft function, cytopenia, thrombocytopenia, mesenchymal stromal cells, allogeneic stem cell transplantation
Citation: Servais S, Baron F, Lechanteur C, Seidel L, Baudoux E, Briquet A, Selleslag D, Maertens J, Poire X, Schroyens W, Graux C, De Becker A, Zachee P, Ory A, Herman J, Kerre T and Beguin Y (2023) Multipotent mesenchymal stromal cells as treatment for poor graft function after allogeneic hematopoietic cell transplantation: A multicenter prospective analysis. Front. Immunol. 14:1106464. doi: 10.3389/fimmu.2023.1106464
Received: 23 November 2022; Accepted: 13 January 2023;
Published: 01 February 2023.
Edited by:
Selim Kuci, University Hospital Frankfurt, GermanyReviewed by:
Olle Thor, Hans Ringden, Karolinska Institutet (KI), SwedenFermin Sanchez-Guijo, University of Salamanca, Spain
Copyright © 2023 Servais, Baron, Lechanteur, Seidel, Baudoux, Briquet, Selleslag, Maertens, Poire, Schroyens, Graux, De Becker, Zachee, Ory, Herman, Kerre and Beguin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sophie Servais, cy5zZXJ2YWlzQGNodWxpZWdlLmJl