
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol., 05 January 2023
Sec. Inflammation
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.959141
This article is part of the Research TopicOrgan Cross Talk and its Impact on the Clinical Course in Multiple Trauma and Critical IllnessView all 18 articles
 Tazio Maleitzke1,2,3
Tazio Maleitzke1,2,3 Sijia Zhou2
Sijia Zhou2 Dario Zocholl4Florian Nima Fleckenstein5
Dario Zocholl4Florian Nima Fleckenstein5 David Alexander Back1,6Julius Maximilian Plewe7
David Alexander Back1,6Julius Maximilian Plewe7 Jérôme Weber1,2
Jérôme Weber1,2 Tobias Winkler1,2,8Ulrich Stöckle1
Tobias Winkler1,2,8Ulrich Stöckle1 Serafeim Tsitsilonis1,2Sven Märdian1*
Serafeim Tsitsilonis1,2Sven Märdian1*Background: Knife crime has increased considerably in recent years in Northern Europe. Affected patients often require immediate surgical care due to traumatic organ injury. Yet, little is known about clinically relevant routine laboratory parameters in stab injury patients and how these are associated with intensive care unit (ICU) admission, hospitalization and number of surgeries.
Methods: We retrospectively analyzed 258 stab injury cases between July 2015 and December 2021 at an urban Level I Trauma Center. Annual and seasonal incidences, injury site, injury mechanism, Injury Severity Score (ISS), and surgical management were evaluated. First, correlations between routine laboratory parameters for hematology, coagulation, and serum biochemistry (peak, and Δ (change from admission to peak within 3 days following admission)) and length of hospital stay, ICU stay, and number of surgeries were assessed using Spearman’s rank correlation coefficients. Second, multivariable Least Absolute Shrinkage and Selection Operator (LASSO) regression analyses were conducted to identify parameters predictive of clinical outcomes. Third, longitudinal developments of routine laboratory parameters were assessed during hospital admission.
Results: In 2021, significantly more stab injuries were recorded compared with previous years and occurred less during winter compared with other seasons. Mean ISS was 8.3 ± 7.3, and ISS was positively correlated with length of hospital and ICU stay (r = 0.5–0.8, p < 0.001). Aspartate transaminase (AST) (Δ) (r = 0.690), peak C-reactive protein (CrP) (r = 0.573), and erythrocyte count (Δ) (r = 0.526) showed the strongest positive correlations for length of ICU stay for penetrating, thoracoabdominal, and organ injuries, respectively. No correlations were observed between routine laboratory parameters and number of surgeries. For patients with penetrating injuries, LASSO-selected predictors of ICU admission included ISS, pH and lactate at admission, and Δ values for activated partial thromboplastin time (aPTT), K+, and erythrocyte count. CrP levels on day 3 were significantly higher in patients with penetrating (p = 0.005), thoracoabdominal (p = 0.041), and organ injuries (p < 0.001) compared with those without.
Conclusion: Our data demonstrate an increase in stab injury cases in 2021 and an important link between changes in routine laboratory parameters and ICU admission and hospitalization. Monitoring ISS and changes in AST, CrP, erythrocyte count, pH, lactate, aPTT, and K+ may be useful to identify patients at risk and adjust surgical and ICU algorithms early on.
Stab injuries are primarily observed in urban environments and predominantly affect young men between 20 and 30 years of age (1, 2). In a recent retrospective analysis of ~240,000 severely injured patients enrolled in the German Trauma Registry (TraumaRegister DGU®), 4,333 stab injuries (1.8%) were recorded between 2009 and 2018 (3).
While overall patient volumes declined in emergency departments (EDs) during the COVID-19 pandemic, incidences of stabbing trauma increased in both Europe (4, 5) and the United States (6–9). Although most stab injuries are not fatal, thoracoabdominal injuries often require surgery and are associated with postsurgical complications and hospital readmissions (10).
Stab injuries result in the disruption of macro (skin) and micro (cell membranes) barriers, causing the release of damage-associated molecular patterns (DAMPs) into the bloodstream, which leads to an activation of the innate immune system (11). Pathogen-associated molecular patterns (PAMPs) from bacteria, viruses, or fungi are also commonly present at the injury site following penetrating trauma. Both DAMPs and PAMPs cause a rapid immune response, including activation of coagulation and complement cascades and reprioritizing of leukocytes (12). In addition, endothelial damage and platelet activation cause a pro-inflammatory cytokine release, which facilitates neutrophil activation and subsequent tissue damage (13). Therefore, stab injuries are likely to affect multiple-organ systems, both primarily though the injury and secondarily through the concomitant cellular and molecular response.
Various serum laboratory parameters are regularly acquired upon arrival of stab injury patients in the ED to monitor health status and organ functions. Blood tests commonly include hematology, coagulation, and serum biochemistry profiles and may be repeated during later stages of admission depending on the patient’s clinical development. How stab injuries alter routine laboratory parameters has not yet been investigated in detail. Knowledge about relevant laboratory parameters to monitor in stab injury patients may however improve assessment and prediction of the clinical course and outcomes early on.
Therefore, this study aimed to describe (i) clinical characteristics of stab injury cases according to the Injury Severity Score (ISS); (ii) explore annual and seasonal differences in monthly stab injury incidences; (iii) evaluate whether peak and Δ (change from admission to peak within 3 days following admission) values of routinely acquired laboratory parameters correlate with clinical outcomes, including length of hospital and ICU stay and number of surgeries performed during admission; and (iv) assess the predictive strength of routinely acquired laboratory parameters for clinical outcomes employing a multivariable regression analysis approach; and (v) compare the longitudinal course of routine laboratory parameters between patients with different injury characteristics over time.
All patients admitted to the ED of a Level I Trauma Center (Berlin, Germany) who sustained one or more stab injuries between July 2015 and December 2021 were included and retrospectively reviewed (retrospective chart review employing a convenience sampling approach (14)). All patients were directly admitted to our center (no transfers from other hospitals).
For all patients, the following parameters were extracted: Injury Severity Score (ISS) ((based on injury patterns present at admission); gender; age; time of admission; health insurance status; mental health condition; alcohol consumption; body temperature at admission; injury mechanism; number of stabs; injured body regions; type of injury, X-ray, ultrasonography, and computed tomography (CT) scan reports (acute pathological findings were quantified); trauma team activation (initiated if patients met Grade of Recommendation B-criteria (GoR-B) defined by DGU® (e.g., penetrating injuries) (15)); performed surgeries (including all acute and elective “in house” surgeries and chest drain insertions via mini-thoracotomy, whereas simple superficial wound closures in the ED were not included); massive transfusion of blood products (defined as transfusion of ≥10 red blood cell units within 24 h or more than four red blood cell units within 1 h (16)); red blood cell (RBC); fresh frozen plasma (FFP); and platelet units; length of hospital and ICU stay.
As the study population comprised mono- and polytrauma patients, Table 1 categorizes patients based on ISS at admission: minor injuries (ISS of 1–8), moderate injuries (ISS of 9–15), severe injuries (ISS of 16–24), and very severe injuries (ISS ≥25) (17).
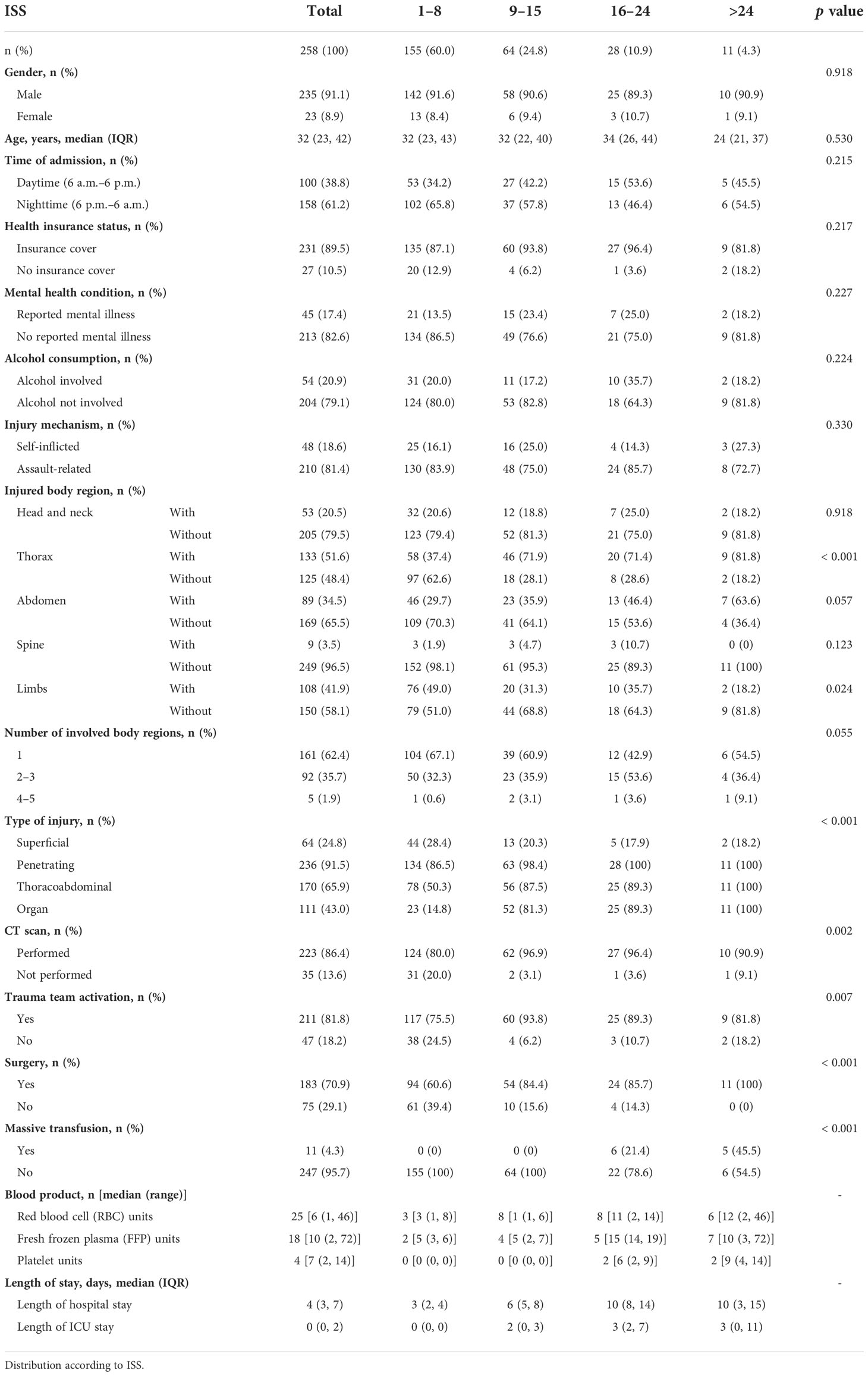
Table 1 Characteristics of patients who suffered stab injuries between July 2015 and December 2021 at a Level I Trauma Center in Berlin, Germany.
According to admission dates, differences in monthly stab injuries between years (2015–2021) and seasons (spring: March–May; summer: June–August; autumn: September–November; winter: December–February) were recorded. As the data set for 2015 only included data for July–December, it was excluded for the assessment of seasonal differences.
Next to demographic data, laboratory values for hematology, coagulation, serum biochemistry, and venous blood gas were recorded. These included hemoglobin, erythrocyte count, leukocyte count, platelet count (all hematology), international normalized ratio (INR), activated partial thromboplastin time (aPTT), fibrinogen (all coagulation), creatinine, urea, total bilirubin, myoglobin, alanine transferase (ALT), aspartate transferase (AST), alkaline phosphatase (ALP), creatine kinase (CK), potassium (K+), C-reactive protein (CrP) (all serum biochemistry), and pH and lactate at admission (both venous blood gas).
To explore clinically relevant changes in routine laboratory parameters in stab injury patients, Δ and peak values were calculated. Δ values express the difference between admission and peak levels within 3 days of admission (Δ = peak level until day 3-admission level) (18).
To test for relationships between groups of different injury severities (according to ISS), chi-square test and Fisher’s exact test were employed to analyze variables in contingency Table 1.
The non-parametric Mann–Whitney U test was used to compare continuous or ordinal variables. Due to the asymmetric distribution of laboratory values, the median was reported.
Associations between included laboratory parameters and length of hospital and ICU stay and number of surgeries were evaluated by Spearman’s rank correlation coefficients. Following Mukak’s guide to the appropriate use of correlation coefficients in medical research, correlation coefficients were categorized as negligible (r = 0–0.3), weak (r = 0.3–0.5), moderate (r = 0.5–0.7), high (r = 0.7–0.9), and very high (r = 0.9–1) (19). Correlation analyses were conducted for patient cohorts with (i) penetrating (all injuries where the visceral or deep fascia was perforated), (ii) thoracoabdominal, and (iii) organ injuries.
To further identify clinically meaningful relationships from the multivariate data set (20), a multivariable selection method was employed to identify potentially predictive sets of variables: LASSO [Least Absolute Shrinkage and Selection Operator (21)] analyses were conducted for each patient cohort of (i) penetrating, (ii) thoracoabdominal, and (iii) organ injuries and each outcome of interest. LASSO models have been commonly used for high-dimensional model selection problems, i.e., if there are numerous predictive factors for a limited sample size. LASSO applies a shrinkage parameter lambda, which shrinks some coefficients of a regression model to zero, thus selecting only those variables that are useful for prediction. The specific value of lambda determines how many non-zero coefficients are considered. Due to this shrinkage, coefficient estimates are biased by design and p-values or confidence intervals do not have reliable statistical properties (22). Therefore, we report trace plots, showing coefficients of each variable for different lambda values. To identify a single model, a suitable value for lambda was determined via cross-validation. The identified model was then used to predict admission to ICU, and sensitivity, specificity, and total accuracy of this prediction were assessed as well as the area under the receiver operating characteristic curve (AUC). Since multivariable regression methods require non-missing data on all variables, a subset of patients with most complete data (n = 66) was used and only variables with less than 120 missing values were considered for variable selection.
It should be noted that the models were purely explorative and should be used to identify potentially predictive factors for future research rather than serve as a final predictive model.
Additionally, longitudinal changes of CrP, hemoglobin, erythrocyte, leukocyte, and platelet counts, total bilirubin, ALT, AST, creatinine, urea, CK, INR, and aPTT were recorded for 21 days following admission and the day of discharge.
To compare daily CrP values between patients with different injury characteristics, patient cohorts were compared according to (i) penetrating injuries, (ii) thoracoabdominal injuries, and (iii) organ injuries to those without, as well as in (iv) patients who were admitted to ICU to those who were not. Where less than four data points were available per group, no statistical tests were conducted.
For Spearman correlation, LASSO regression, and longitudinal laboratory parameter analyses, 26 patients were excluded. These included 18 patients who left the hospital against medical advice, five patients who died in hospital due to their injuries, and three patients who were initially transferred to specialized medical departments for further treatment.
A two-tailed p-value <0.05 was considered statistically significant. Data analyses were conducted using SPSS 26.0 (IBM, Chicago, USA) and Prism V.9.0 (GraphPad, California, USA) and R version 4.1.2 [for LASSO analysis: package glmnet (23)].
Prior to study initiation, ethical approval (EA1/082/20) was obtained from the local ethics committee, Ethikkommission Charité – Universitätsmedizin Berlin.
Between July 2015 and December 2021, 258 stab injuries were identified (23 women, 235 men) with a median age of 32 years (interquartile range (IQR) 23; 42). Most stab injuries occurred between 6 p.m. and 6 a.m. (61.2%) and were due to interpersonal conflicts (81.4%), whereas 18.6% were self-inflicted. In 17.4% of sustained stab injuries, mental illness was recorded, and in 20.9% elevated blood alcohol levels or obvious alcohol intoxication were present.
The trauma team was activated in 81.8% of cases, and 70.9% of patients underwent surgery. More than half of the patients (51.6%) sustained a thorax injury, whereas the limbs and abdomen were affected in 41.9% and 34.5% of cases, respectively. Most patients presented with penetrating injuries (91.5%), and 43.0% sustained organ injuries (Figure 1A; Table 1). The detailed distribution of cases according to ISS is provided in Table 1.
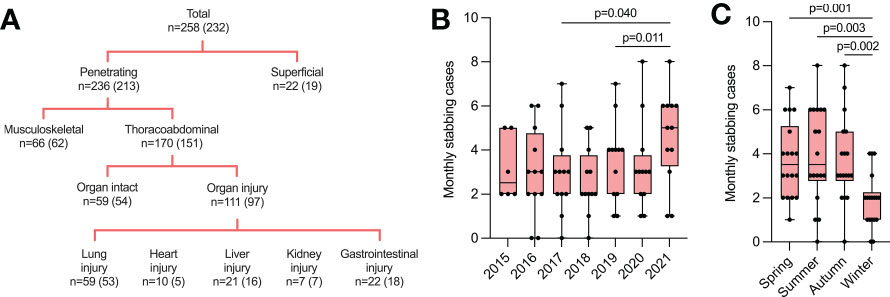
Figure 1 Annual and seasonal differences in monthly stab injuries. (A) Characteristics of included stab injuries divided by penetrating vs. superficial, thoracoabdominal vs. musculoskeletal, and organ injuries vs. non-organ injuries. Numbers in brackets show the number of cases included in statistical analysis (for details, please see Materials and Methods). (B) Monthly stab injury cases between 2015 and 2021. Individual data points represent the number of stabbing cases per month for indicated years. (C) Monthly stab injury cases between 2016 and 2021 divided by seasons. Individual data points represent the number of stabbing cases per month for indicated seasons. Data are presented as median box plots with interquartile range and whiskers from minimum to maximum.
We recorded significantly more monthly stab injuries in 2021 compared to 2017 (p = 0.040) and 2018 (p = 0.011) (Figure 1B). Most stabbings occurred during spring, summer, and autumn, whereas significantly fewer cases were seen during winter (spring vs. winter, p = 0.001; summer vs. winter, p = 0.003; autumn vs. winter, p = 0.002) (Figure 1C).
We next analyzed how injury severity and routine laboratory parameters correlated with length of hospital and ICU stay and number of surgeries in patients with penetrating stab injuries (n = 213). The median time from admission to first blood samples was 35 min (IQR 28–41 min) for blood hematology, biochemistry, and coagulation samples and 10 min (IQR 10–18 min) for venous blood gas samples.
Number of organ injuries, number of pathological CT findings, number of pathological findings in all imaging modalities combined, and ISS were all moderately to highly positively correlated with length of hospital and ICU stay (r = 0.513–0.805, p < 0.001 for all) (Figure 2A).
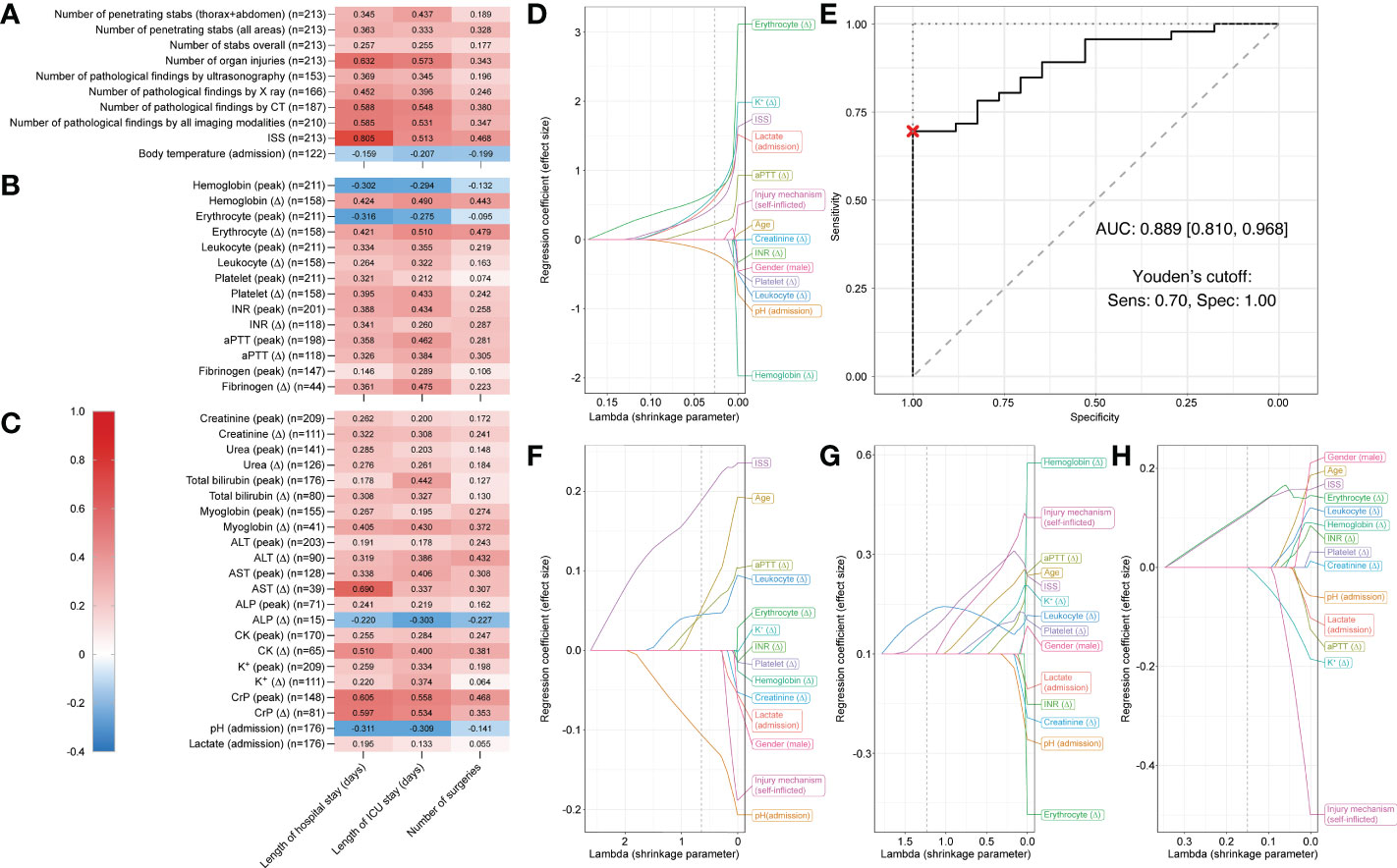
Figure 2 Correlation matrix showing Spearman’s rank correlation coefficients and Least Absolute Shrinkage and Selection Operator (LASSO) plots showing regression coefficients for patients who suffered penetrating stab injuries. Correlation strength is indicated by color scale on the left. Correlations between three different outcome parameters (length of hospital stay, length of ICU stay, and number of surgeries) and (A) injury specifics, (B) routine hematology and coagulation, and (C) serum biochemistry and venous blood gas laboratory parameters for penetrating injuries (n = 213). Multivariable LASSO trace plots indicate potentially predictive sets of variables for (D) ICU admission (yes/no). (E) Receiver operating characteristic (ROC) curve for the LASSO model of ICU admission (yes/no). Youden’s cutoff indicates the optimal cutoff based on sensitivity (Sens.) and specificity (Spec). (F) Further LASSO trace plots for length of hospital stay, (G) length of ICU stay, and (H) number surgeries. Grey dotted line displays optimal lambda value calculated via cross-validation. AUC, area under the curve.
Further, AST (Δ), CK (Δ), peak CrP, and CrP (Δ) (Figure 2C) were all moderately positively correlated with length of hospital stay (r = 0.510–0.690) and erythrocyte count (Δ) (Figure 2B), peak CrP, and CrP (Δ) (Figure 2C) were also moderately positively correlated with length of ICU stay (r = 0.510–0.558).
The strongest positive correlations were observed between ISS and hospital stay (r = 0.805) and AST (Δ) and ICU stay (r = 0.690). For all reported r-values >0.3, p-values were <0.01. Negligible to weak correlations were observed between all assessed parameters and number of surgeries.
For admission to ICU (yes/no), LASSO regression analyses selected the following predictive variables when shrinkage parameter lambda was set to 0.027 (determined via cross-validation): pH (admission) (coefficient = -0.213), aPTT (Δ) (coefficient = 0.219), ISS (coefficient = 0.479), lactate (admission) (coefficient = 0.594), K+ (Δ) (coefficient = 0.657), and erythrocyte count (Δ) (coefficient = 0.696) (Figure 2D).
With these predictive variables, a binary logistic regression model predicting ICU admission had a sensitivity of 73.9% (95% confidence interval [58.7%, 95.7%]), a specificity of 100% [76.5%, 100.0%], and a total accuracy of 81% [69.8%, 92.1%]. The AUC was 0.889 [0.810, 0968] (Figure 2E). Thus, prediction by this model was statistically significantly better than random. In the trace plot, it can be seen that other parameters became dominant with smaller values of lambda. For instance, hemoglobin (Δ) was the largest negative coefficient for lambda values close to zero (Figure 2D).
For length of hospital stay the variable ISS, for length of ICU stay hemoglobin (Δ), and for number of surgeries male gender were the largest coefficients for lambda values close to zero (Figures 2F–H). Details on LASSO-selected variables and their coefficients can be found in Table 2.
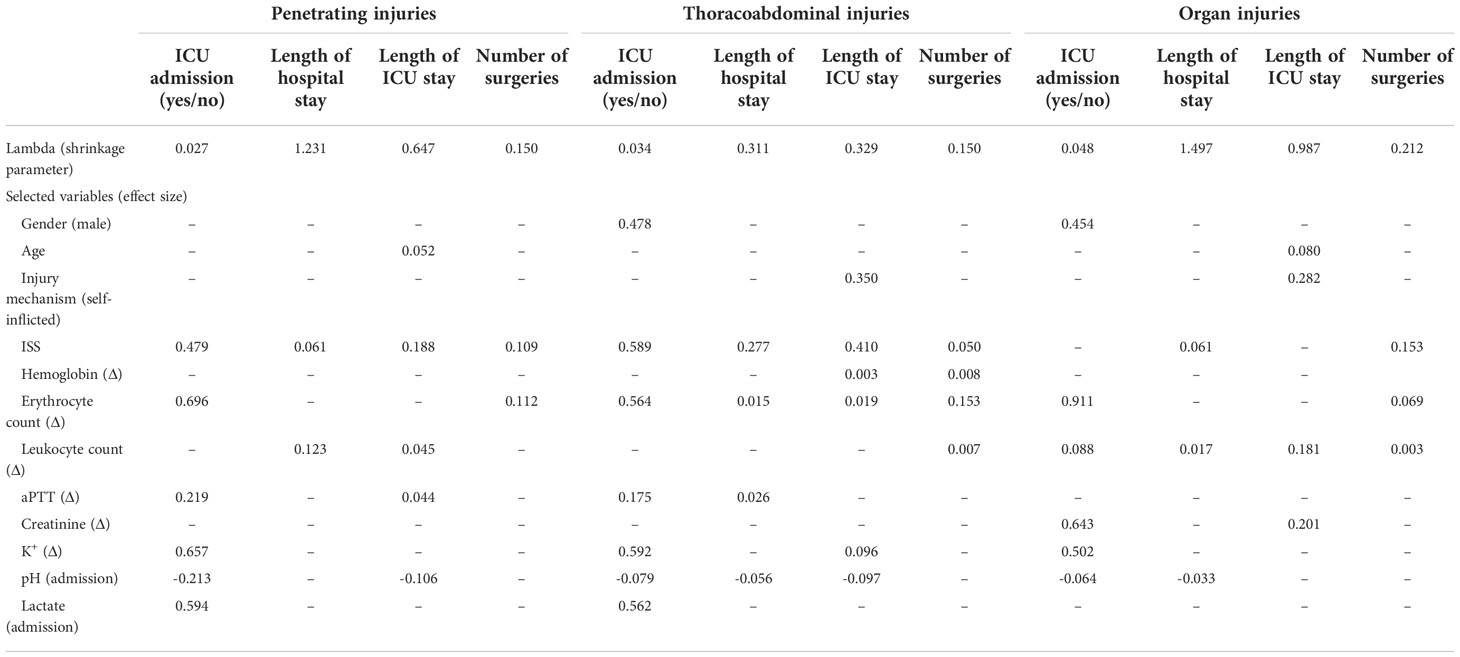
Table 2 LASSO-selected predictive variables with corresponding coefficients (n = 66).
Next, we assessed patients who suffered penetrating injuries that affected thoracoabdominal cavities (n = 151).
Number of organ injuries, number of pathological X-ray findings, number of pathological CT findings, and number of pathological findings in all imaging modalities combined, ISS (Figure 3A), AST (Δ), peak CrP, and CrP (Δ) (Figure 3C) were moderately to highly positively correlated with length of hospital stay (r = 0.529–0.821). Similarly, number of organ injuries, number of pathological CT findings, and number of pathological findings in all imaging modalities combined, ISS (Figure 3A), hemoglobin (Δ), erythrocyte count (Δ) (Figure 3B), peak CrP, and CrP (Δ) (Figure 3C) showed moderate to high positive correlations with length of ICU stay (r = 0.520–0.821). The strongest positive correlations were again observed between ISS and hospital stay (r = 0.821) and between peak CrP and ICU stay (r = 0.573). For all reported r-values > 0.3, p-values were <0.01 and only negligible to weak correlations were observed between all assessed parameters and number of surgeries.
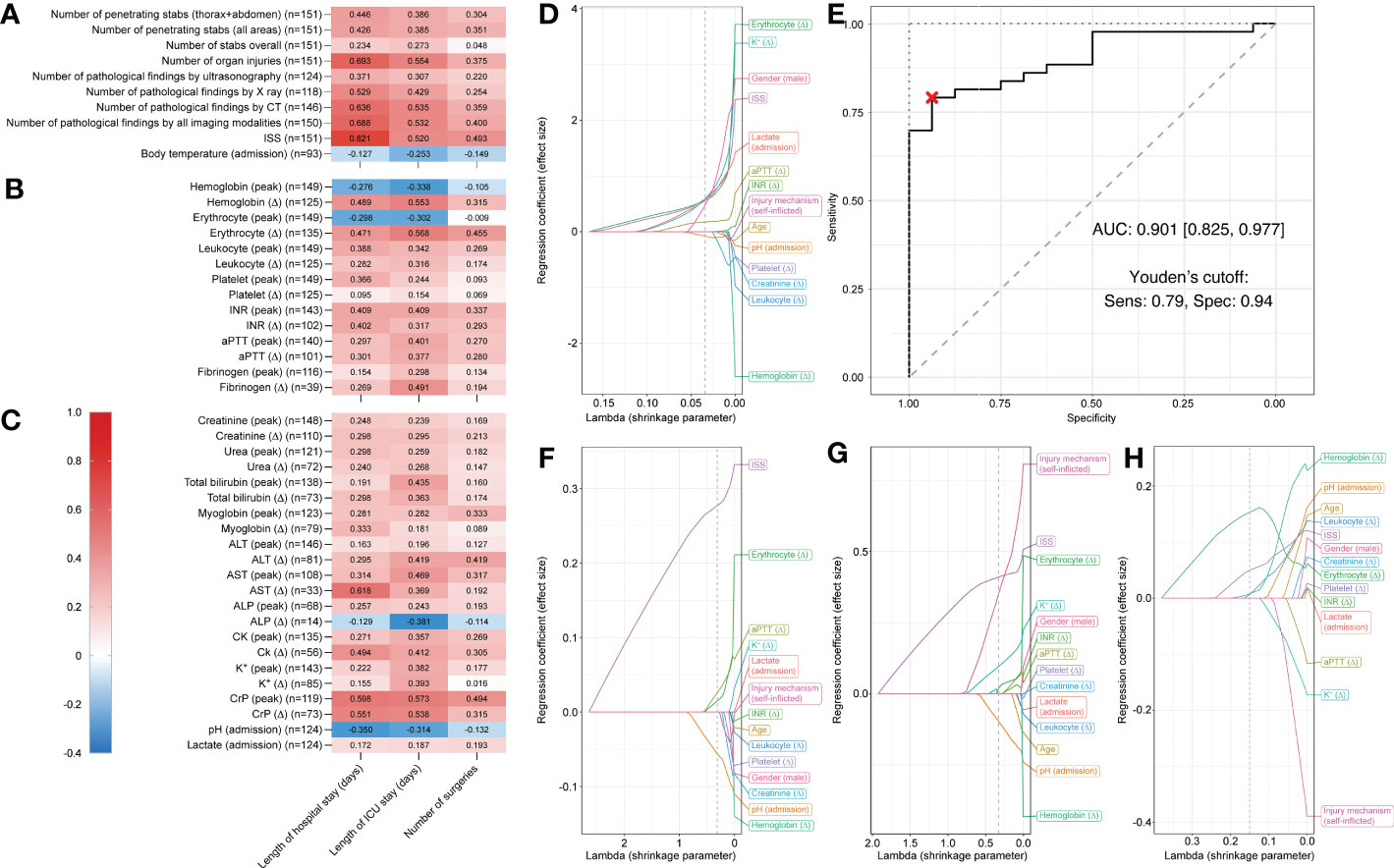
Figure 3 Correlation matrix showing Spearman’s rank correlation coefficients and Least Absolute Shrinkage and Selection Operator (LASSO) plots showing regression coefficients for patients who suffered thoracoabdominal stab injuries. Correlation strength is indicated by color scale on the left. Correlations between three different outcome parameters (length of hospital stay, length of ICU stay, and number of surgeries) and (A) injury specifics, (B) routine hematology and coagulation, and (C) serum biochemistry and venous blood gas laboratory parameters for penetrating injuries (n = 151). Multivariable LASSO trace plots indicate potentially predictive sets of variables for (D) ICU admission (yes/no). (E) Receiver operating characteristic (ROC) curve for the LASSO model of ICU admission (yes/no). Youden’s cutoff indicates the optimal cutoff based on sensitivity (Sens.) and specificity (Spec). (F) Further LASSO trace plots for length of hospital stay, (G) length of ICU stay, and (H) number surgeries. Grey dotted line displays optimal lambda value calculated via cross-validation. AUC, area under the curve.
For admission to ICU (yes/no), LASSO regression analyses selected variables pH (admission) (coefficient = -0.079), aPPT (Δ) (coefficient 0.175), male gender (coefficient = 0.478), lactate (coefficient = 0.562), erythrocyte count (Δ) (coefficient = 0.564), ISS (coefficient = 0.589), and K+ (Δ) (coefficient = 0.592) when shrinkage parameter lambda was set to 0.034 (determined via cross-validation) (Figure 3D).
The binary logistic regression model predicting ICU admission had a sensitivity of 79.1% (95% confidence interval [62.8%, 93%]), a specificity of 100% [81.2%, 100.0%], and a total accuracy of 84.7% [72.9%, 93.2%]. The AUC was 0.901 [0.825, 0.977] (Figure 3E). Thus, prediction by this model was statistically significantly better than random (Figure 3D).
For length of hospital stay the variable ISS, for length of ICU stay self-inflicted injuries, and for number of surgeries hemoglobin (Δ) were the largest coefficients for lambda values close to zero (Figures 3F–H). Details on LASSO-selected variables and their coefficients can be found in Table 2.
When only analyzing patients who suffered organ injuries (n = 97), length of hospital and ICU stay showed moderate positive correlations with ISS (Figure 4A), hemoglobin (Δ), erythrocyte count (Δ), peak platelet count, platelet count (Δ) (Figure 4B), myoglobin (Δ), AST (Δ), and peak CrP (r = 0.505–0.644) (Figure 4C). The strongest positive correlation was again observed between ISS and hospital stay (r = 0.644) and between erythrocyte count (Δ) and ICU stay (r = 0.526). For all reported r-values > 0.3, p-values were <0.01. Again, only negligible to weak correlations were observed between all assessed parameters and number of surgeries.
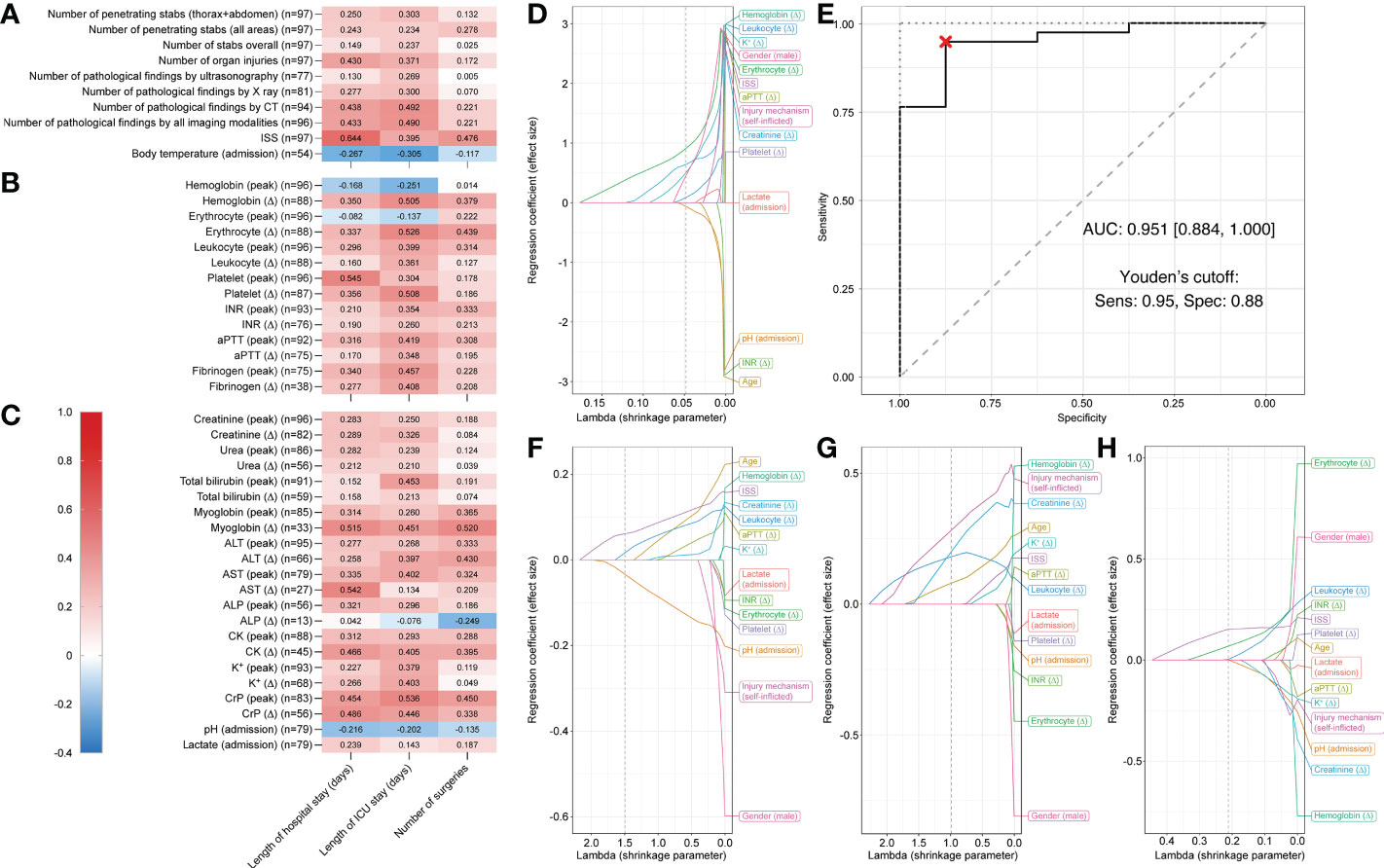
Figure 4 Correlation matrix showing Spearman’s rank correlation coefficients and Least Absolute Shrinkage and Selection Operator (LASSO) plots showing regression coefficients for patients who suffered organ injuries. Correlations between three different outcome parameters (length of hospital stay, length of ICU stay, and number of surgeries) and (A) injury specifics, (B) routine hematology and coagulation, and (C) serum biochemistry and venous blood gas laboratory parameters for penetrating injuries (n = 97). Multivariable LASSO trace plots indicate potentially predictive sets of variables for (D) ICU admission (yes/no). (E) Receiver operating characteristic (ROC) curve for the LASSO model of ICU admission (yes/no). Youden’s cutoff indicates the optimal cutoff based on sensitivity (Sens.) and specificity (Spec). (F) Further LASSO trace plots for length of hospital stay, (G) length of ICU stay, and (H) number surgeries. Gray dotted line displays optimal lambda value calculated via cross-validation. AUC, area under the curve.
For admission to ICU (yes/no), LASSO regression analyses selected variables pH (admission) (coefficient = -0.064), leukocyte count (Δ) (coefficient = 0.088), male gender (coefficient = 0.454), K+ (Δ) (coefficient = 0.502), creatinine (Δ) (coefficient = 0.643), and erythrocyte count (Δ) (coefficient = 0.911), when shrinkage parameter lambda was set to 0.048 (determined via cross-validation) (Figure 4D).
The binary logistic regression model predicting ICU admission showed a sensitivity of 92.1% (95% confidence interval [71.1%, 100%]), a specificity of 100% [75.01%, 100.0%], and a total accuracy of 93.5% [76.1%, 100%]. The AUC was 0.941 [0.884, 1.000] (Figure 4E). Thus, prediction by this model was statistically significantly better than random. In the trace plot, it can be seen that other parameters became dominant with smaller values of lambda. For instance, hemoglobin (Δ) was the largest coefficient for lambda values close to zero (Figure 4D).
For length of hospital stay age, for length of ICU stay hemoglobin (Δ), and for number of surgeries erythrocyte count (Δ) were the largest coefficients for lambda values close to zero (Figures 4F–H). Details on LASSO-selected variables and their coefficients can be found in Table 2.
As a next step, we assessed the longitudinal development of CrP values following stab injuries over time in different patient cohorts.
When assessing all patients (superficial and penetrating injuries combined; patients excluded for correlation and LASSO regression analyses were also excluded here), an increase in CrP levels was observed between admission and day 4. Values then peaked between days 4 and 6 before slowly decreasing again (Figures 5A, B).
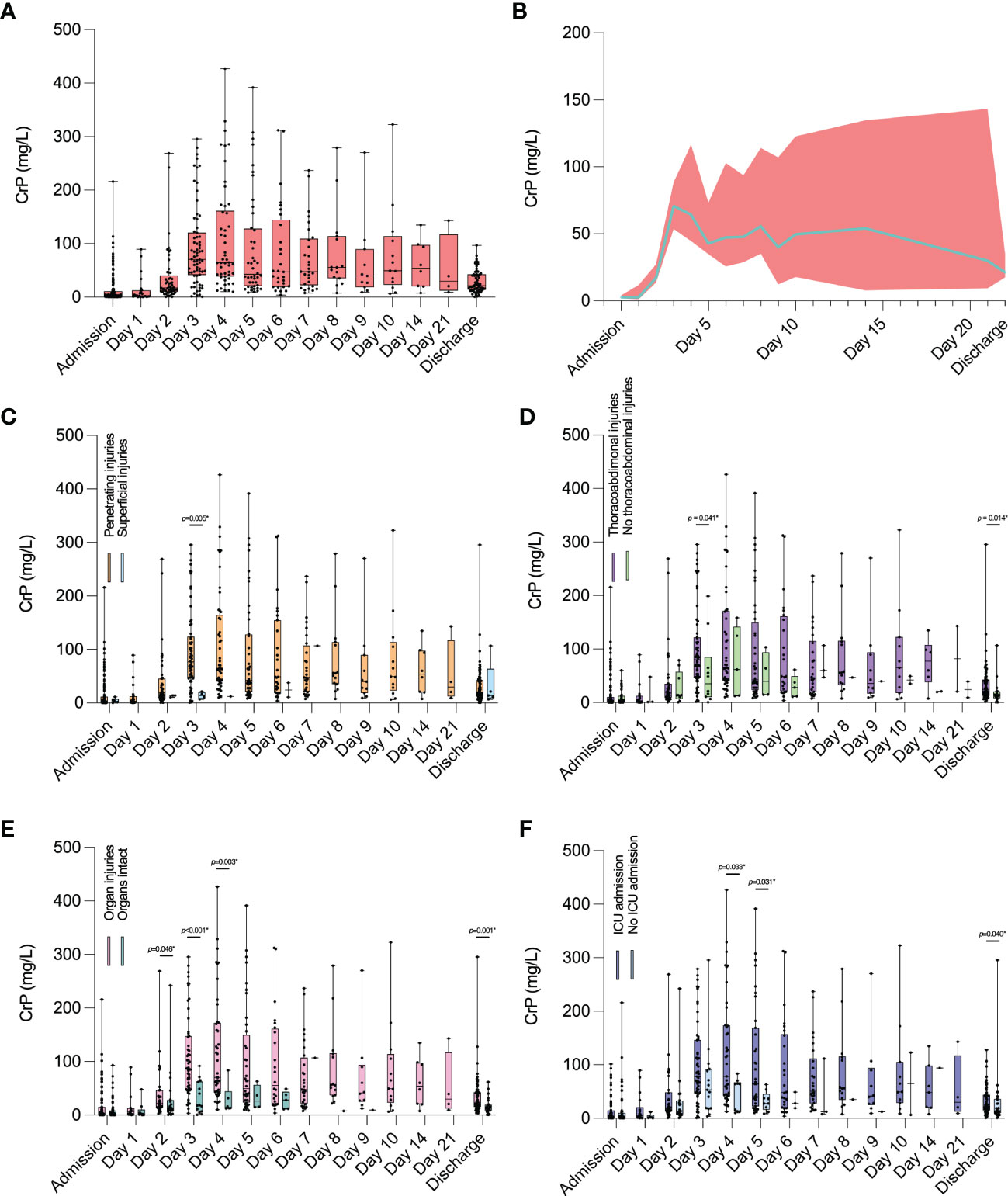
Figure 5 Longitudinal development of daily CrP levels in patients who suffered stab injuries. (A, B) Values for all patients who suffered stab injuries. (C) Comparison of CrP values between penetrating and superficial injuries during hospitalization. (D) Comparison of CrP values between patients with and without thoracoabdominal injuries, (E) between patients with and without organ injuries, and (F) between patients who were admitted to ICU and those who were not. Physiological CrP concentration: <5 mg/l. Data are presented as median box plots with interquartile range and whiskers from minimum to maximum and in (B) as median line with 95% confidence intervals displayed as error bands. CrP, C-reactive peptide.
When comparing patients with penetrating injuries to those with superficial injuries, CrP levels were significantly higher in the penetrating group on day 3 following admission (p = 0.005) (Figure 5C).
Comparing patients with thoracoabdominal injuries to those without, CrP levels were again significantly higher on day 3 following admission (p = 0.041) and on the day of discharge (p = 0.014) (Figure 5D).
CrP values were also significantly higher on days 2 (p = 0.046), 3 (p < 0.001), and 4 (p = 0.003) following admission, as well as on the day of discharge (p = 0.001) in patients with organ injuries compared to those without (Figure 5E).
Finally, in patients admitted to ICU, CrP levels were significantly higher on days 4 (p = 0.033) and 5 (p=0.031) following admission and on the day of discharge (p = 0.040) compared to patients who were not admitted to ICU (Figure 5F).
To illustrate the longitudinal development of routine laboratory parameters in stab injury patients, we provided an overview for the most relevant parameters, obtained from all patients (superficial and penetrating injuries combined; patients excluded for correlation and LASSO regression analyses were also excluded here).
The longitudinal development of hemoglobin and erythrocyte count over time followed a reversed hockey stick pattern, with physiologically high values at admission, followed by a marked decrease on days 1 and 2 and a stable plateau phase until day 21 (Supplementary Figure S1A). Both hemoglobin and erythrocyte count levels were lower on the day of discharge compared to admission.
Leukocyte and platelet counts followed an S-curve over time (Supplementary Figure S1B). Compared to admission, leukocyte levels increased on day 1, then decreased until day 5, and increased again until day 10, before decreasing again until day 21. Platelet levels decreased on day 1 compared to admission but followed a similar pattern to leukocyte counts over time (Supplementary Figure S1B).
Longitudinal development plots for total bilirubin, ALT, AST, creatinine, urea, CK, K+, hemoglobin, erythrocyte, leukocyte and platelet counts, INR, and aPTT can be found in Supplementary Figures S1C–F.
In this retrospective study, annual and seasonal differences in stab injury incidences were assessed at an urban Level I Trauma Center. We further investigated how routine laboratory parameters in stab injury patients correlated with and predicted ICU admission, length of hospital and ICU stay, and number of surgeries performed during admission.
We found that number of organ injuries, the number of acute pathological findings in several imaging modalities, ISS, and Δ values for AST, CK, and CrP correlated moderately to highly with hospitalization length. Only negligible to weak correlations were observed between assessed parameters and number of surgeries. Further, we identified ISS, pH, and lactate at admission, and Δ values for aPPT, K+, and erythrocyte count as predictors for ICU admission in patients suffering penetrating stab injuries.
ISS and new ISS (NISS) are widely used to predict mortality and morbidity in patients suffering multiple trauma, and both scores correlate with length of hospital stay (24) and can predict ICU admission (25). In this study, we confirmed that ISS may also predict ICU admission and length of hospital stay in patients suffering stab injuries as a higher ISS was associated with longer hospitalization.
The study period in the present study covered more than 20 months during the COVID-19 pandemic (2020/2021), a period that was, to our knowledge, previously not evaluated regarding stab injuries.
Several studies assessed stab injury incidences during the COVID-19 pandemic, and most found a rise in penetrating injuries during the first months of 2020 (4–9), but not all (26, 27). Conversely, it was reported that during the first months of the COVID-19 pandemic, crime rates, including assault, decreased globally (28).
We found that stab injuries significantly increased in 2021, i.e., in the later phase of the pandemic and after most COVID-19-related measures had been lifted in Germany. This is congruent with studies demonstrating that several psychological effects occurring after crises (posttraumatic stress disorder, anxiety, fear, and anger) may only be observed with a certain delay (29, 30). A study from Mexico showed that assault and battery numbers decreased in the beginning of the COVID-19 pandemic but increased again when national lockdowns were lifted (31). Congruently, data from the UK showed a return of penetrating injury numbers to pre-pandemic levels, following an initial decline during the first months of the COVID-19 pandemic (27). In line with our findings, observations from natural catastrophes showed a link between length of exposure to natural disasters and increased violence (32, 33), which may explain why significantly more stab injuries were seen during the later phases of the COVID-19 pandemic, in 2021.
We further found that stab injuries occurred less often during winter than during other seasons. This is concordant with data from Ho et al., who reported a positive association between warm weather and penetrating trauma (34). A study from the UK demonstrated that stabbings in young adults mainly occurred after midnight (35). In accordance, we showed that over 60% of stab injury patients were admitted between 6 p.m. and 6 a.m.
From a clinical and surgical perspective, changes in blood composition are of particular interest in patients suffering penetrating organ injuries. Platelet dysfunction following trauma has previously been linked to increased mortality (36, 37), however, to the best of our knowledge, stab injury-associated thrombocytopenia has not yet been investigated.
In the current study, we found Δ platelet values, which take admission values into account, to be positively correlated with length of ICU stay for patients who suffered organ injuries.
Due to blood loss and dilution following intravenous fluid administration, platelet counts may be reduced in patients suffering stab injuries. In severely injured patients, early administration of platelets is therefore advised, as it was shown to improve hemostasis and reduce mortality (38).
For patients with penetrating and thoracoabdominal injuries, aPTT (Δ) was identified as a predictor for ICU admission. While previous research showed that among other coagulation parameters, aPTT increased significantly during the first hours following trauma (39, 40), we could show that increased aPTT (Δ) values may also predict ICU admission in stab injury patients.
These data underline the importance of monitoring changes in platelet levels and coagulation parameters at and during admission to initiate and adjust early interventions and to avoid prolonged hospitalization.
The acute-phase protein CrP rises in response to trauma and tissue injury. Both penetrating injuries and surgeries disrupt skin barriers and cause an instant and delayed immune response (12). While admission CrP values were generally within the physiological range, we saw that peak CrP values correlated with length of hospital (r = 0.605) and ICU stay (r = 0.558) in patients suffering penetrating stab injuries. Correlations were similar for Δ values.
In penetrating trauma, prophylactic antibiotic treatment is commonly employed to prevent and treat infectious complications, and strong evidence exists for prophylactic antibiotic treatment for chest wounds that require tube thoracostomy (41).
During the first days of admission, we observed that patients with penetrating stab injuries showed higher CrP values than those without. This also applied to patients with thoracoabdominal injuries, organ injuries, and patients who were admitted to ICU. Similarly, CrP values at discharge were still significantly higher in patients with thoracoabdominal injuries, organ injuries, and ICU admission than in those without.
High CrP concentrations (values higher than 75 mg/l at ICU discharge (42–44) and hospital discharge (45)) were reported as predictors of poor clinical outcomes and increased readmission rates in critically ill patients including multiple trauma, burns, and open heart surgery patients. However, conflicting evidence suggests that CrP values at ICU discharge are unrelated to readmission rates or death (46, 47). Therefore, determining the right time point to discharge a patient requires thorough and repeated clinical assessments in addition to CrP monitoring and must be decided individually.
However, if stab injury patients fall into one of the aforementioned categories (penetrating, thoracoabdominal, organ injuries, or ICU admission), inflammation and sepsis markers including CrP and procalcitonin shall be monitored in addition to the patient’s clinical state (48, 49). Further, early admission of prophylactic antibiotics should be considered to potentially reduce hospitalization time.
Tissue damage or hemorrhagic shock commonly cause hyperkalemia in trauma patients (50, 51). Importantly, hyperkalemia is associated with acute kidney injury following severe trauma (52). In our study population, we were able to identify K+ (Δ) as a predictor of ICU admission in all assessed patient groups (penetrating, thoracoabdominal, and organ injuries).
Hemorrhagic shock and infectious complications can further trigger and exacerbate trauma-related acute kidney injury (53), and elevated CK levels, mainly due to muscle injury, compromise kidney function additionally (54). In line with these findings, we identified creatinine (Δ) as a predictor of ICU admission in patients suffering organ injuries and CK (Δ) correlated with length of hospital stay in patients suffering penetrating stab injuries.
Data from the ongoing UK-based Activation of Coagulation and Inflammation in Trauma (ACIT) study showed that trauma-induced acute kidney injury occurred in more than 10% of multiple trauma patients (n = 1,410) (55). Therefore, monitoring and treating acute kidney injury by avoiding fluid volume deficit, nephrotoxic agents and by facilitating blood pressure support may decrease the risk of complications and mortality (53, 56). Fluid overload, which may worsen acute kidney injury, shall be avoided simultaneously (57, 58).
Prehospital lactate levels were previously shown to predict resuscitative care in trauma patients and may be used to aid triage of normotensive trauma patients (59). High lactate and low pH additionally predicted 72 h mortality in multiple trauma patients (60). Coherently, we identified increased lactate and low pH levels at admission as predictors of ICU admission in penetrating and thoracoabdominal injury patients following stabbing trauma.
Last, we identified Δ values of AST to positively correlate with length of hospital stay in patients with penetrating, thoracoabdominal and organ injuries. Previously, liver transaminase levels were shown to predict liver injury following blunt and penetrating trauma (61, 62).
Our data indicate that even in the absence of organ injuries, monitoring liver and kidney function and adjusting treatment algorithms early on may help to avoid prolonged hospitalization in stab injury patients.
This study has several limitations. First, this is a retrospective single-center study conducted at an urban Level I Trauma Center, which only allows limited generalization of the findings, especially regarding other geographical regions and countries. These results may also not translate to rural or remote areas where transfers to Level I Trauma Centers commonly cause delayed admissions. These findings should thus be corroborated by further prospective studies from different regions.
Second, the presence of non-medical factors that may have affected ICU admission and discharge could not be taken into consideration in this study (e.g., bed availability due to COVID-19 patients).
Third, due to the observational character of this study, we identified correlations and predictors but can only speculate about causality. Due to the exploratory nature of this study, confounding factors were not included in the analyses and study design.
In summary, we provide solid evidence that routine laboratory parameters have a predictive strength for outcome parameters in patients who suffer stab injuries. Monitoring specific laboratory parameters in stab injury patients may help to identify risk groups and adjust treatment algorithms early on.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Ethikkommission Charité – Universitätsmedizin Berlin. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
TM and SM designed and conceived the study. SZ, DZ, TM, FNF, JMP, and JW provided, selected, assembled, analyzed, and interpreted data. Data curation and project administration by DAB, TW, US, and ST. SM provided project supervision and resources. TM drafted the original manuscript. All authors critically reviewed and edited the final manuscript, agreed to be accountable for all aspects of the work and have read and confirmed that they meet ICMJE criteria for authorship.
TM is a participant in the BIH Charité Clinician Scientist Program funded by the Charité – Universitätsmedizin Berlin and the Berlin Institute of Health at Charité (BIH).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.959141/full#supplementary-material
Supplementary Figure S1 | Longitudinal development of daily laboratory values in stab injury patients. (A) hemoglobin/erythrocyte count, (B) leukocyte count/platelet count, (C) total bilirubin/ALT/AST, (D) creatinine/urea, (E) CK/K+, and (F) INR/aPTT. Data are presented as median box plots with interquartile range and whiskers from minimum to maximum. ALT, alanine transaminase; aPTT, activated partial thromboplastin time; AST, aspartate transaminase; CK, creatine kinase; INR, International Normalized Ratio.
1. Malik NS, Munoz B, de Courcey C, Imran R, Lee KC, Chernbumroong S, et al. Violence-related knife injuries in a UK city; epidemiology and impact on secondary care resources. EClinicalMedicine (2020) 20:100296. doi: 10.1016/j.eclinm.2020.100296
2. Rikken QGH, Chadid A, Peters J, Geeraedts LMG, Giannakopoulos GF, Tan ECTH. Epidemiology of penetrating injury in an urban versus rural level 1 trauma center in the Netherlands. Hong Kong J Emergency Med (2020) 29(1):38–45. doi: 10.1177/1024907920904190
3. Bieler D, Kollig E, Hackenberg L, Rathjen JH, Lefering R, Franke A, et al. Penetrating injuries in Germany - epidemiology, management and outcome an analysis based on the TraumaRegister DGU(R). Scand J Trauma Resusc Emerg Med (2021) 29(1):80. doi: 10.1186/s13049-021-00895-1
4. Bäckström D, Wladis A. A cohort study of trauma patients in Sweden during the first months of the COVID-19 pandemic: a small reduction in trauma admissions. Scand J Trauma Resusc Emergency Med (2022) 30(1):12. doi: 10.1186/s13049-022-01001-9
5. Sotiropoulou M, Vailas M, Kapiris S. COVID-19 and impact on trauma injuries. a janus facing in opposite directions? Injury (2021) 53(7):2671–2. doi: 10.1016/j.injury.2021.02.069
6. Chodos M, Sarani B, Sparks A, Bruns B, Gupta S, Michetti CP, et al. Impact of COVID-19 pandemic on injury prevalence and pattern in the Washington, DC metropolitan region: a multicenter study by the American college of surgeons committee on trauma, Washington, DC. Trauma Surg Acute Care Open (2021) 6(1):e000659. doi: 10.1136/tsaco-2020-000659
7. Ratnasekera AM, Seng SS, Jacovides CL, Kolb R, Hanlon A, Stawicki SP, et al. Rising incidence of interpersonal violence in Pennsylvania during COVID-19 stay-at home order. Surgery (2022) 171(2):533–40. doi: 10.1016/j.surg.2021.06.024
8. Ghafil C, Matsushima K, Ding L, Henry R, Inaba K. Trends in trauma admissions during the COVID-19 pandemic in Los Angeles county, California. JAMA Netw Open (2021) 4(2):e211320. doi: 10.1001/jamanetworkopen.2021.1320
9. Pelzl CE, Salottolo K, Banton K, Madayag RM, Hamilton D, Duane TM, et al. COVID-19 and trauma: how social distancing orders altered the patient population using trauma services during the 2020 pandemic. Trauma Surg Acute Care Open (2021) 6(1):e000645. doi: 10.1136/tsaco-2020-000645
10. Hanna K, Asmar S, Ditillo M, Chehab M, Khurrum M, Bible L, et al. Readmission with major abdominal complications after penetrating abdominal trauma. J Surg Res (2021) 257:69–78. doi: 10.1016/j.jss.2020.07.060
11. Zhang Q, Raoof M, Chen Y, Sumi Y, Sursal T, Junger W, et al. Circulating mitochondrial DAMPs cause inflammatory responses to injury. Nature (2010) 464(7285):104–7. doi: 10.1038/nature08780
12. Huber-Lang M, Lambris JD, Ward PA. Innate immune responses to trauma. Nat Immunol (2018) 19(4):327–41. doi: 10.1038/s41590-018-0064-8
13. Lord JM, Midwinter MJ, Chen YF, Belli A, Brohi K, Kovacs EJ, et al. The systemic immune response to trauma: an overview of pathophysiology and treatment. Lancet (2014) 384(9952):1455–65. doi: 10.1016/S0140-6736(14)60687-5
14. Gearing RE, Mian IA, Barber J, Ickowicz A. A methodology for conducting retrospective chart review research in child and adolescent psychiatry. J Can Acad Child Adolesc Psychiatry (2006) 15(3):126–34.
15. Hagebusch P, Faul P, Naujoks F, Klug A, Hoffmann R, Schweigkofler U. Trauma-team-activation in Germany: how do emergency service professionals use the activation due to trauma mechanism? results from a nationwide survey. Eur J Trauma Emerg Surg (2022) 48:393–9. doi: 10.1007/s00068-020-01425-x
16. Pham HP, Shaz BH. Update on massive transfusion. Br J Anaesth. (2013) 111 Suppl 1:i71–82. doi: 10.1093/bja/aet376
17. VanDerHeyden N, Cox TB. CHAPTER 6 - TRAUMA SCORING. In: Asensio JA, Trunkey DD, editors. Current therapy of trauma and surgical critical care. Philadelphia: Mosby (2008). p. 26–32.
18. Brown M, Nassoiy S, Plackett T, Luchette F, Posluszny J Jr. Red blood cell distribution width and outcome in trauma patients. J Osteopath Med (2021) 121(2):221–8. doi: 10.1515/jom-2020-0089
19. Mukaka MM. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med J (2012) 24(3):69–71.
20. Heinze G, Dunkler D. Five myths about variable selection. Transpl Int (2017) 30(1):6–10. doi: 10.1111/tri.12895
21. Tibshirani R. Regression shrinkage and selection Via the lasso. J R Stat Society: Ser B (Methodological). (1996) 58(1):267–88. doi: 10.1111/j.2517-6161.1996.tb02080.x
22. Heinze G, Wallisch C, Dunkler D. Variable selection - a review and recommendations for the practicing statistician. Biom J (2018) 60(3):431–49. doi: 10.1002/bimj.201700067
23. Friedman J, Hastie T, Tibshirani R. Regularization paths for generalized linear models via coordinate descent. J Stat Software (2010) 33(1):1–22. doi: 10.18637/jss.v033.i01
24. Salehi O, Tabibzadeh Dezfuli SA, Namazi SS, Dehghan Khalili M, Saeedi M. A new injury severity score for predicting the length of hospital stay in multiple trauma patients. Trauma Mon (2016) 21(1):e20349. doi: 10.5812/traumamon.20349
25. Lavoie A, Moore L, LeSage N, Liberman M, Sampalis JS. The injury severity score or the new injury severity score for predicting intensive care unit admission and hospital length of stay? Injury (2005) 36(4):477–83. doi: 10.1016/j.injury.2004.09.039
26. Pino EC, Gebo E, Dugan E, Jay J. Trends in violent penetrating injuries during the first year of the COVID-19 pandemic. JAMA Netw Open (2022) 5(2):e2145708. doi: 10.1001/jamanetworkopen.2021.45708
27. Hickland MM, Massouh P, Sutthakorn RE, Greenslade C, Jennings C, Cantle F, et al. The impact of the COVID-19 pandemic on the number of presentations of penetrating injuries to a UK major trauma centre. J Public Health (Oxf). (2022) 44(1):e126–e32. doi: 10.1093/pubmed/fdab333
28. Nivette AE, Zahnow R, Aguilar R, Ahven A, Amram S, Ariel B, et al. A global analysis of the impact of COVID-19 stay-at-home restrictions on crime. Nat Hum Behav (2021) 5(7):868–77. doi: 10.1038/s41562-021-01139-z
29. Liao Z, Zhang X, Wang Y, Wang T, Li X, Zhao M, et al. Delayed-onset PTSD and coping strategies of Chinese college students during the COVID-19 pandemic. Front Sociol (2021) 6:734738. doi: 10.3389/fsoc.2021.734738
30. Gan Y, Ma J, Wu J, Chen Y, Zhu H, Hall BJ. Immediate and delayed psychological effects of province-wide lockdown and personal quarantine during the COVID-19 outbreak in China. Psychol Med (2020), 1–12. doi: 10.1017/S0033291720003116
31. Balmori de la Miyar JR, Hoehn-Velasco L, Silverio-Murillo A. The U-shaped crime recovery during COVID-19: evidence from national crime rates in Mexico. Crime Sci (2021) 10(1):14. doi: 10.1186/s40163-021-00147-8
32. Gearhart S, Perez-Patron M, Hammond TA, Goldberg DW, Klein A, Horney JA. The impact of natural disasters on domestic violence: An analysis of reports of simple assault in Florida (1999–2007). Violence Gender (2018) 5(2):87–92. doi: 10.1089/vio.2017.0077
33. Thurston AM, Stockl H, Ranganathan M. Natural hazards, disasters and violence against women and girls: a global mixed-methods systematic review. BMJ Glob Health (2021) 6(4):e004377. doi: 10.1136/bmjgh-2020-004377
34. Ho VP, Towe CW, Chan J, Barie PS. How's the weather? relationship between weather and trauma admissions at a level I trauma center. World J Surg (2015) 39(4):934–9. doi: 10.1007/s00268-014-2881-8
35. Vulliamy P, Faulkner M, Kirkwood G, West A, O'Neill B, Griffiths MP, et al. Temporal and geographic patterns of stab injuries in young people: a retrospective cohort study from a UK major trauma centre. BMJ Open (2018) 8(10):e023114. doi: 10.1136/bmjopen-2018-023114
36. Kutcher ME, Redick BJ, McCreery RC, Crane IM, Greenberg MD, Cachola LM, et al. Characterization of platelet dysfunction after trauma. J Trauma acute Care surg (2012) 73(1):13–9. doi: 10.1097/TA.0b013e318256deab
37. Jacoby RC, Owings JT, Holmes J, Battistella FD, Gosselin RC, Paglieroni TG. Platelet activation and function after trauma. J Trauma. (2001) 51(4):639–47. doi: 10.1097/00005373-200110000-00003
38. Cardenas JC, Zhang X, Fox EE, Cotton BA, Hess JR, Schreiber MA, et al. Platelet transfusions improve hemostasis and survival in a substudy of the prospective, randomized PROPPR trial. Blood Adv (2018) 2(14):1696–704. doi: 10.1182/bloodadvances.2018017699
39. Yang Z, Simovic MO, Liu B, Burgess MB, Cap AP, DalleLucca JJ, et al. Indices of complement activation and coagulation changes in trauma patients. Trauma Surg Acute Care Open (2022) 7(1):e000927. doi: 10.1136/tsaco-2022-000927
40. Raffee LA, Oteir AO, Alawneh KZ, Alustath AMI. Relationship between initial arterial blood gases and coagulation profiles - analyzing the prognosis and outcomes in patients with multiple Injuries/Trauma. Open Access Emerg Med (2020) 12:87–92. doi: 10.2147/OAEM.S244941
41. Kamarova M, Kendall R. 13 prophylactic antibiotics for penetrating injury: a review of practice at a major trauma centre, literature review and recommendations. Emergency Med J (2017) 34(12):A869. doi: 10.1136/emermed-2017-207308.13
42. Ho KM, Lee KY, Dobb GJ, Webb SA. C-reactive protein concentration as a predictor of in-hospital mortality after ICU discharge: a prospective cohort study. Intensive Care Med (2008) 34(3):481–7. doi: 10.1007/s00134-007-0928-0
43. Kaben A, Correa F, Reinhart K, Settmacher U, Gummert J, Kalff R, et al. Readmission to a surgical intensive care unit: incidence, outcome and risk factors. Crit Care (2008) 12(5):R123. doi: 10.1186/cc7023
44. Gulcher SS, Bruins NA, Kingma WP, Boerma EC. Elevated c-reactive protein levels at ICU discharge as a predictor of ICU outcome: a retrospective cohort study. Ann Intensive Care (2016) 6(1):5. doi: 10.1186/s13613-016-0105-0
45. Dupre A, Gagniere J, Samba H, Rivoire M, Slim K. CRP predicts safe patient discharge after colorectal surgery. Ann Surg (2018) 267(2):e33. doi: 10.1097/SLA.0000000000001983
46. Silvestre J, Coelho L, Povoa P. Should c-reactive protein concentration at ICU discharge be used as a prognostic marker? BMC Anesthesiol (2010) 10:17. doi: 10.1186/1471-2253-10-17
47. Al-Subaie N, Reynolds T, Myers A, Sunderland R, Rhodes A, Grounds RM, et al. C-reactive protein as a predictor of outcome after discharge from the intensive care: a prospective observational study. Br J Anaesth. (2010) 105(3):318–25. doi: 10.1093/bja/aeq171
48. Simon L, Gauvin F, Amre DK, Saint-Louis P, Lacroix J. Serum procalcitonin and c-reactive protein levels as markers of bacterial infection: a systematic review and meta-analysis. Clin Infect Dis (2004) 39(2):206–17. doi: 10.1086/421997
49. Nuutila J, Hohenthal U, Oksi J, Jalava-Karvinen P. Rapid detection of bacterial infection using a novel single-tube, four-colour flow cytometric method: Comparison with PCT and CRP. EBioMedicine (2021) 74:103724. doi: 10.1016/j.ebiom.2021.103724
50. Ookuma T, Miyasho K, Kashitani N, Beika N, Ishibashi N, Yamashita T, et al. The clinical relevance of plasma potassium abnormalities on admission in trauma patients: a retrospective observational study. J Intensive Care (2015) 3(1):37. doi: 10.1186/s40560-015-0103-6
51. Perkins RM, Aboudara MC, Abbott KC, Holcomb JB. Resuscitative hyperkalemia in noncrush trauma: a prospective, observational study. Clin J Am Soc Nephrol. (2007) 2(2):313–9. doi: 10.2215/CJN.03070906
52. Stewart IJ, Snow BD, Clemens MS, Sosnov JA, Ross JD, Howard JT, et al. Hyperkalemia in combat casualties: Implications for delayed evacuation. Mil Med (2017) 182(11):e2046-e51. doi: 10.7205/MILMED-D-17-00119
53. Messerer DAC, Halbgebauer R, Nilsson B, Pavenstadt H, Radermacher P, Huber-Lang M. Immunopathophysiology of trauma-related acute kidney injury. Nat Rev Nephrol. (2021) 17(2):91–111. doi: 10.1038/s41581-020-00344-9
54. Assanangkornchai N, Akaraborworn O, Kongkamol C, Kaewsaengrueang K. Characteristics of creatine kinase elevation in trauma patients and predictors of acute kidney injury. J Acute Med (2017) 7(2):54–60. doi: 10.6705/j.jacme.2017.0702.002
55. Perkins ZB, Captur G, Bird R, Gleeson L, Singer B, O'Brien B. Trauma induced acute kidney injury. PloS One (2019) 14(1):e0211001. doi: 10.1371/journal.pone.0211001
56. Mohsenin V. Practical approach to detection and management of acute kidney injury in critically ill patient. J Intensive Care (2017) 5:57. doi: 10.1186/s40560-017-0251-y
57. Alobaidi R, Morgan C, Basu RK, Stenson E, Featherstone R, Majumdar SR, et al. Association between fluid balance and outcomes in critically ill children: A systematic review and meta-analysis. JAMA Pediatr (2018) 172(3):257–68. doi: 10.1001/jamapediatrics.2017.4540
58. Payen D, de Pont AC, Sakr Y, Spies C, Reinhart K, Vincent JL, et al. A positive fluid balance is associated with a worse outcome in patients with acute renal failure. Crit Care (2008) 12(3):R74. doi: 10.1186/cc6916
59. St John AE, McCoy AM, Moyes AG, Guyette FX, Bulger EM, Sayre MR. Prehospital lactate predicts need for resuscitative care in non-hypotensive trauma patients. West J Emerg Med (2018) 19(2):224–31. doi: 10.5811/westjem.2017.10.34674
60. Qi J, Bao L, Yang P, Chen D. Comparison of base excess, lactate and pH predicting 72-h mortality of multiple trauma. BMC Emerg Med (2021) 21(1):80. doi: 10.1186/s12873-021-00465-9
61. Bilgic I, Gelecek S, Akgun AE, Ozmen MM. Predictive value of liver transaminases levels in abdominal trauma. Am J Emerg Med (2014) 32(7):705–8. doi: 10.1016/j.ajem.2014.03.052
Keywords: trauma, knife, penetrating, blood, serum biochemistry, coagulation, hemostasis, inflammation
Citation: Maleitzke T, Zhou S, Zocholl D, Fleckenstein FN, Back DA, Plewe JM, Weber J, Winkler T, Stöckle U, Tsitsilonis S and Märdian S (2023) Routine laboratory parameters predict intensive care unit admission and hospitalization in patients suffering stab injuries. Front. Immunol. 13:959141. doi: 10.3389/fimmu.2022.959141
Received: 17 June 2022; Accepted: 21 November 2022;
Published: 05 January 2023.
Edited by:
Markus Huber-Lang, Ulm University Medical Center, GermanyReviewed by:
Hayley Louise Letson, James Cook University, AustraliaCopyright © 2023 Maleitzke, Zhou, Zocholl, Fleckenstein, Back, Plewe, Weber, Winkler, Stöckle, Tsitsilonis and Märdian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sven Märdian, c3Zlbi5tYWVyZGlhbkBjaGFyaXRlLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.