 Aining Qin
Aining Qin Jing Sun2*
Jing Sun2*
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Immunol. , 18 July 2022
Sec. Autoimmune and Autoinflammatory Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.950641
Objectives: The aim of this research is to discuss the research status, hotspots, frontiers and development trends in the field of adult-onset Still’s disease (AOSD) based on bibliometrics and visual analysis by CiteSpace software.
Methods: The relevant research articles on AOSD from 1921 to 2021 were retrieved from the Scopus database. CiteSpace software was used to form a visual knowledge map and conduct analysis for the countries/regions, journals, authors, keywords, clusters, research hotspots and frontiers of the included articles.
Results: There were 2,373 articles included, and the number of articles published during 1921-2021 is increasing. The country with the highest number of articles published was Japan (355, 14.96%), followed by the United States (329, 13.86%) and France (215, 9.06%). The author with the highest number of publications is Ansell, Barbara M. (30, 1.26%), and the author with the highest co-citation frequency is Yamaguchi, Masaya (703). Clinical Rheumatology is the journal with the highest publication frequency. The top five cluster groups were “joint”, “differential diagnosis”, “prednisolone”, “methotrexate” and “macrophage activation syndrome”. The diagnosis, treatment and pathogenesis of AOSD form the main research fields, and prognosis and complications are the research hotspots and trends.
Conclusions: The global research field in AOSD has expanded in the past 100 years. The complications and new pathogenesis of AOSD are hotspots in this field and need further study in the future.
Adult-onset Still’s disease (AOSD) is a kind of systemic inflammatory disease with unknown etiology that can accumulate in various systems of the whole body, with a global incidence rate of (0.16–0.40)/100,000 and an estimated prevalence rate of (1-34)/1,000,000 (1). The incidence rate of males in Japan is 0.22/100,000 and that of females is 0.34/100,000 (2). Due to the low prevalence of AOSD, there is still a lack of extensive and reliable epidemiological data in clinics at the present stage (3). A study on Poland revealed that the incidence of AOSD in urban areas of Poland (0.33/100,000) was significantly higher than that in rural areas (0.29/100,000) (4). The age distribution of the AOSD is bimodal, with one peak occurring between 15-25 years and the other between 36-45 years (5). The typical clinical manifestations of AOSD mainly include fever (60-100%), arthritis or arthralgia (70-100%) and maculopapular red rash (60-80%) (6). Atypical clinical manifestations such as sore throat or pharyngitis, myalgia, lymphadenopathy, and hepatosplenomegaly may also occur in some patients (7). In addition, the prevalence of mental disorders in AOSD patients is increased due to the long-term chronic course of the disease, which especially affects their emotions (8). In general, the prognosis of AOSD is good (9), but there is still a mortality rate of 3% (3, 10), and some serious complications can also lead to death (11), such as macrophage activation syndrome (MAS) (12–14%) (12), thrombotic thrombocytopenic purpura (<1%) (13), disseminated intravascular coagulation disease (14), and acute respiratory distress syndrome (15).
Many factors, including genetic factors (16), infection (17), and immune dysfunction (18) may be possible causative factors of AOSD. Several studies have shown that Human leucocyte antigen is closely related to the occurrence of AOSD (19, 20), and the Macrophage migration inhibitory factor gene may increase susceptibility to the disease (21). Bacterial, viral, or parasitic infections may also cause AOSD (22). At present, the pathogenesis is still controversial, and pathophysiology studies are rare (23). Studies have shown that chemokines and pro-inflammatory cytokines, such as interferon (IFN)-γ, tumor necrosis factor (TNF)-α and interleukin (IL) are involved in the pathogenesis of AOSD (24). In the absence of markers for specific diagnosis and curative effect evaluation (25), AOSD is primarily diagnosed by excluding other diseases (26). For the possibility of misdiagnosis in AOSD (27), the average delay time of diagnosis is about four months (28). Yamaguchi criteria (29) have the highest diagnostic sensitivity of 92%, followed by Fautrel criteria (30) (87%) and Cush criteria (31) (80%). AOSD has been treated symptomatically mainly by using non-steroidal anti-inflammatory drugs (NSAIDs), steroids and disease-modifying anti-rheumatic drugs (DMARDs) (26). With the in-depth understanding of the pathogenesis, Biological Response Modifiers are gradually trying to be used for treatment (32). However, the effect of traditional treatment schemes is not satisfactory, with more than 80% of patients not relieved after only using NSAIDs (33) and 45% of patients developing hormone dependence after the use of steroids (34). At the same time, new treatments, such as Biological Response Modifiers still lack more effective clinical experimental data to verify (35).
In the past few years, a number of scholars have carried out basic and clinical studies on the pathogenesis and treatment of AOSD (36). However, few reports have analyzed the characteristics and development trend of the AOSD over a long period of time, which is not conducive for researchers to accurately grasp the occurrence, development rules and characteristics of the AOSD (37). With an increasing number of reports on the AOSD research, retrieving the research status quickly and efficiently in related fields has become a more realistic problem faced by researchers (38). Bibliometrics and visual analysis provide an important, feasible and systematic method for judging the importance of published literature by showing the author’s networks and academic exchanges, connections between scholars and the development in the field of knowledge (39). Using the results of the bibliometric analysis will not only help researchers understand the global research trends of AOSD and master the information sources of AOSD research but also help researchers understand the advantages and disadvantages of their research and quickly capture the research priorities, hotspots, and trends (40).
In this study, the research articles related to adult-onset Still’s disease in the Scopus database were selected and analyzed by using CiteSpace software. From the perspectives of bibliometrics and visual analysis, the research progress of AOSD is discussed, aiming to understand the research development trends and new trends of AOSD, identify the hotspots in this research field, and provide a reference and basis for better research on AOSD.
Scopus is a multi-disciplinary abstract index database launched by Elsevier in 2004 (http://www.scopus.com), which contains nearly 25,000 active titles from more than 7,000 publishing houses worldwide, covering 240 disciplinary fields such as engineering, agriculture and environmental science, biomedicine, social science, art and humanities (41). Scopus is currently the largest database of abstracts and citations in the world, providing a one-stop platform for researchers to obtain scientific and technological literature (42), which can provide a reliable data basis for this study.
We retrieved the Scopus database core dataset, and the search formula is as follows: TITLE-ABS-KEY (“adult onset still disease”) OR TITLE-ABS-KEY (“still disease”). The search time range was from 1921 to 2021. The last retrieval date was November 30, 2021.
The periodical articles with research contents related to the theme of “adult-onset Still’s disease” were included by reading the titles, abstracts and keywords of the detected articles. Articles with incomplete research information, conference articles, degree papers, review articles, book content, and duplicate articles were excluded.
CiteSpace is a web-based Java application for analyzing and visualizing co-citation networks (43). CiteSpace analyzes the research by using the information contained in the articles and predicts the future development of this field (44). The visual co-occurrence network is constructed with CiteSpace software.
In the CiteSpace software parameter setting, the time span is set to be from November 1921 to November 2021, the time slice of 1 year, the threshold item is selected as “Top N”, and the data of the top 10 high frequency nodes are selected for each time slice. “Pathfinder” is selected as the cutting connection mode to simplify the network structure and highlight important features.
A total of 2,378 articles were retrieved, and duplicated articles in the imported articles were deleted by using CiteSpace software. Finally, 2,373 articles were included. The number of articles published in the past decade has shown a steady growth trend. See Figure 1 for details. In 2021 (173), the number of publications was approximately 2.3 times that in 2011 (74), reflecting the increased attention given by the academic community to adult-onset Still’s disease. The main research areas of AOSD are Medicine, Immunology and Microbiology, Biochemistry, Genetics and Molecular biology, accounting for 95.69% of the total frequency, and Medicine is the most frequently reported (2,291, 75.54%). See Table 1 for details. Among the 2,373 retrieved articles, the total citation frequency was 17,968, the average citation frequency of each article was 7.57 times, and the highest citation frequency of a single article was 1,252 times. The top 10 most frequently cited articles are shown in Table 2.
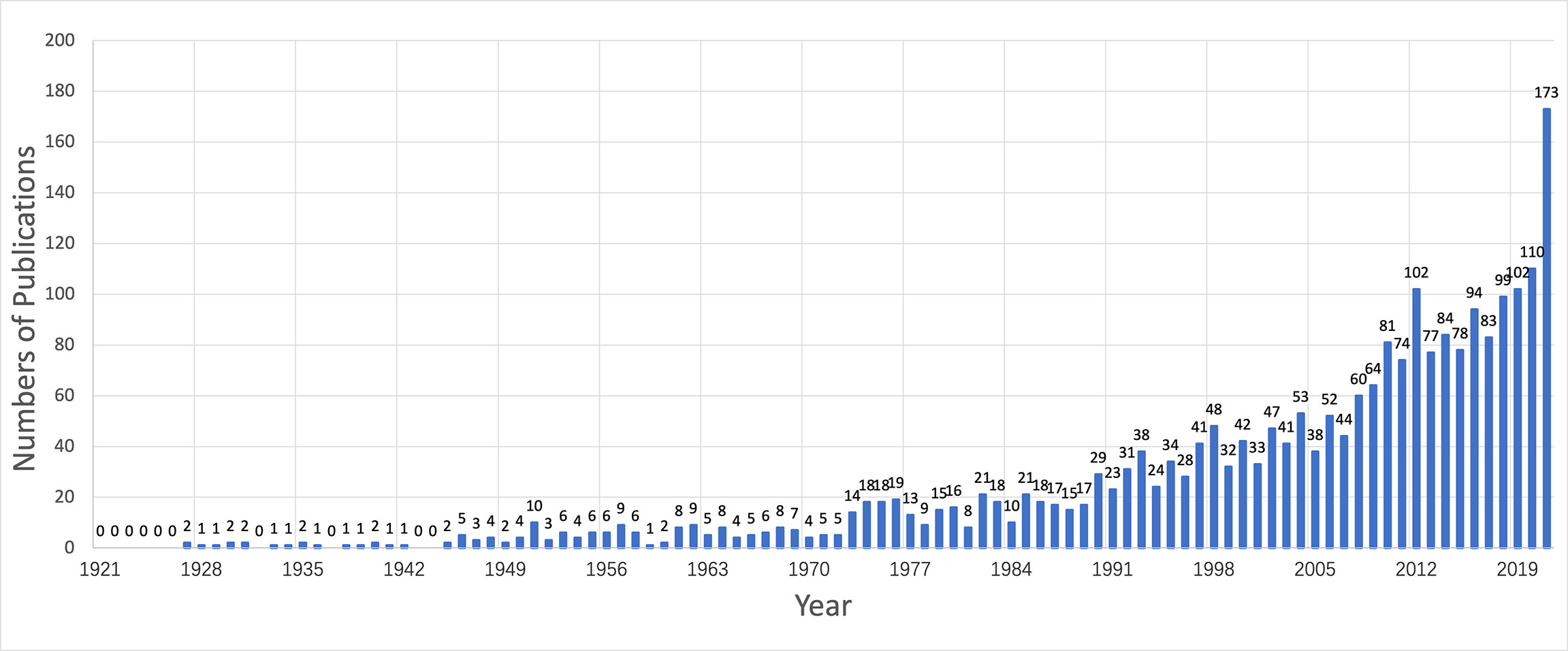
Figure 1 The annual quantities of adult-onset Still’s disease articles from 1921 to 2021.
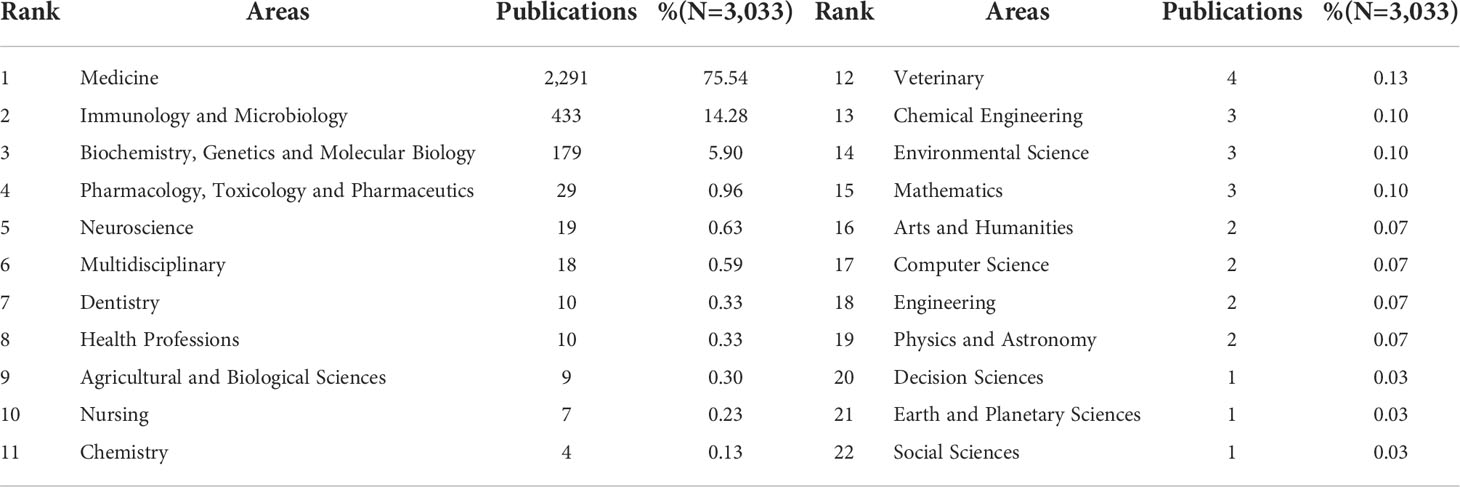
Table 1 The research areas of adult-onset Still’s disease articles from 1921 to 2021.
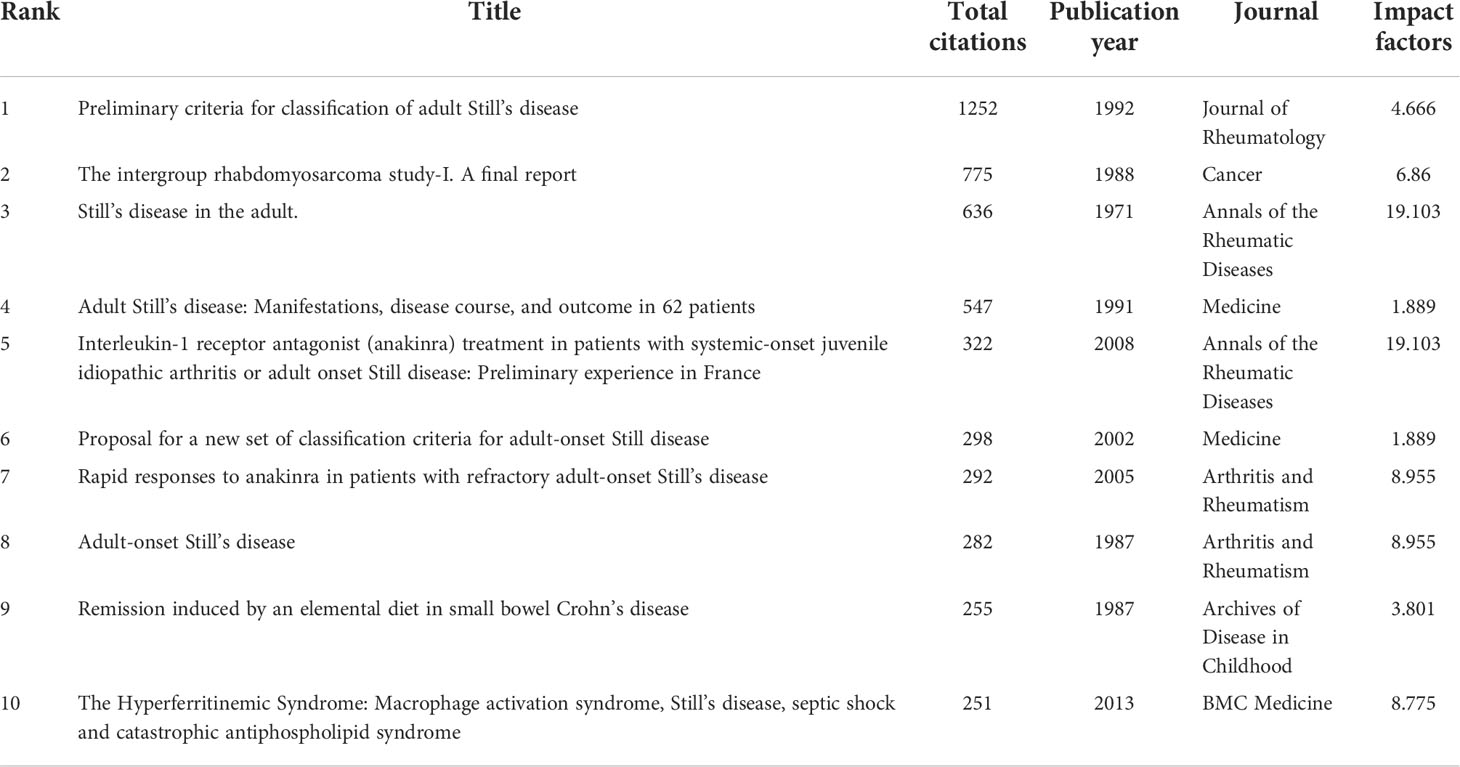
Table 2 Top 10 highly cited articles from 1921 to 2021.
These articles are published in 649 journals, with an average published volume of 3.66 articles. The journal with the most published articles is Clinical Rheumatology, with 80 articles, accounting for 3.37% of the total. The journals with the top 5 articles included 314 articles, accounting for 13.2% of the total, as shown in Table 3.

Table 3 Top 5 journals with the largest number of articles from 1921 to 2021.
Figure 2 is the co-citation network of journals, in which the number of nodes is 649 and the number of links is 2,679. The top 5 cited journals are Journal of Rheumatology (1,081, 40.4%), Annals of The Rheumatic Diseases (893, 33.3%), Arthritis Rheumatism (687, 25.6%), Clinical Rheumatology (316, 11.8%), and Clinical and Experimental Rheumatology (184, 6.9%). Centrality reflects the importance of nodes, which is shown as a purple circle in the figure. The higher the centrality is, the more important the node is. The top 3 journals in centrality are Arthritis Rheumatism (0.10), Journal of Rheumatology (0.04), and Annals of The Rheumatic Diseases (0.03).
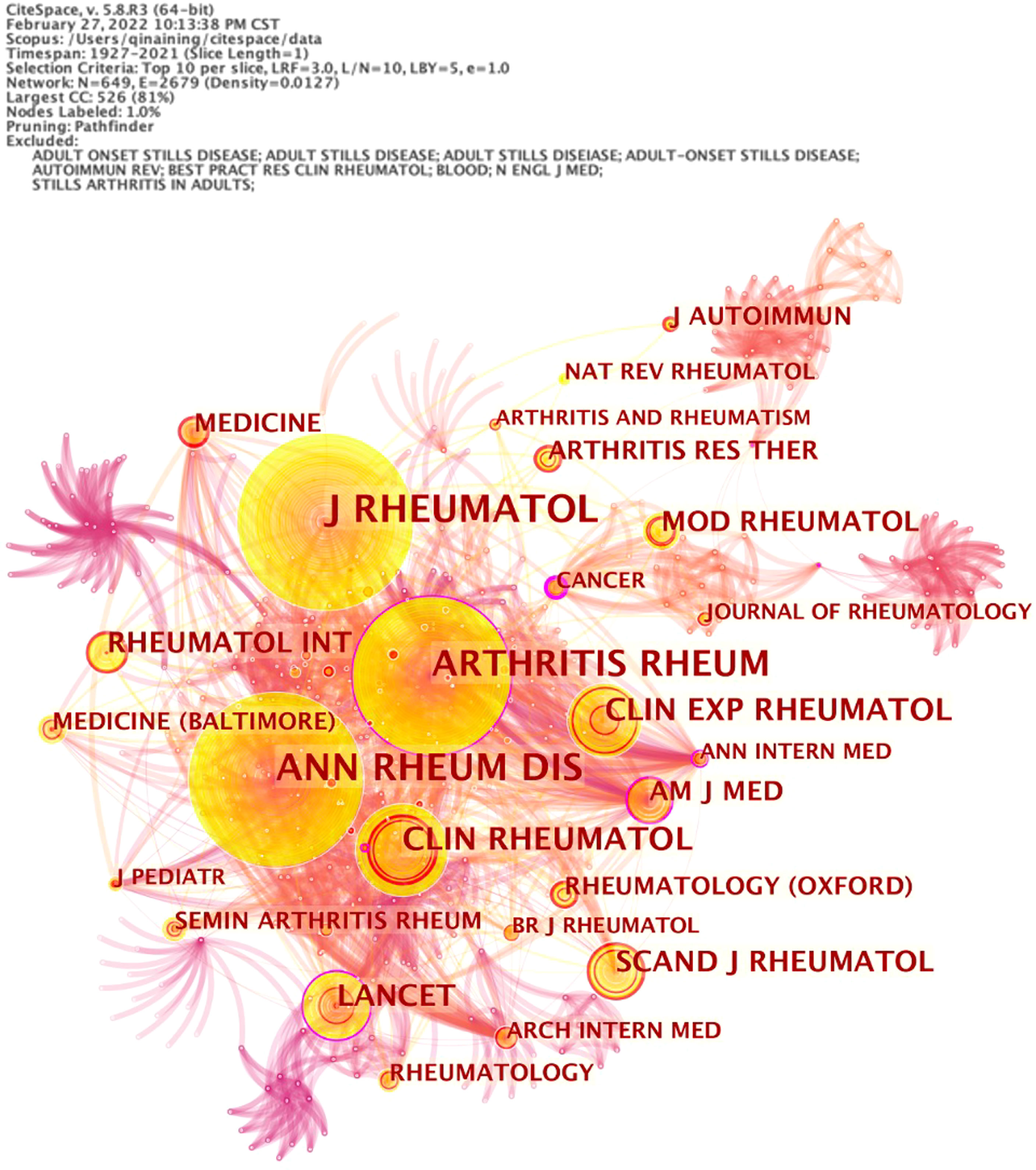
Figure 2 The co-citation network of adult-onset Still’s disease articles from 1921 to 2021.
A total of 4,308 authors are involved in the publication of articles related to adult-onset Still’s disease. Three authors write more than 20 articles, and among them, Ansell, Barbara M. from Clinica Pediatrica ranks first with 30 articles. See Table 4 for details.
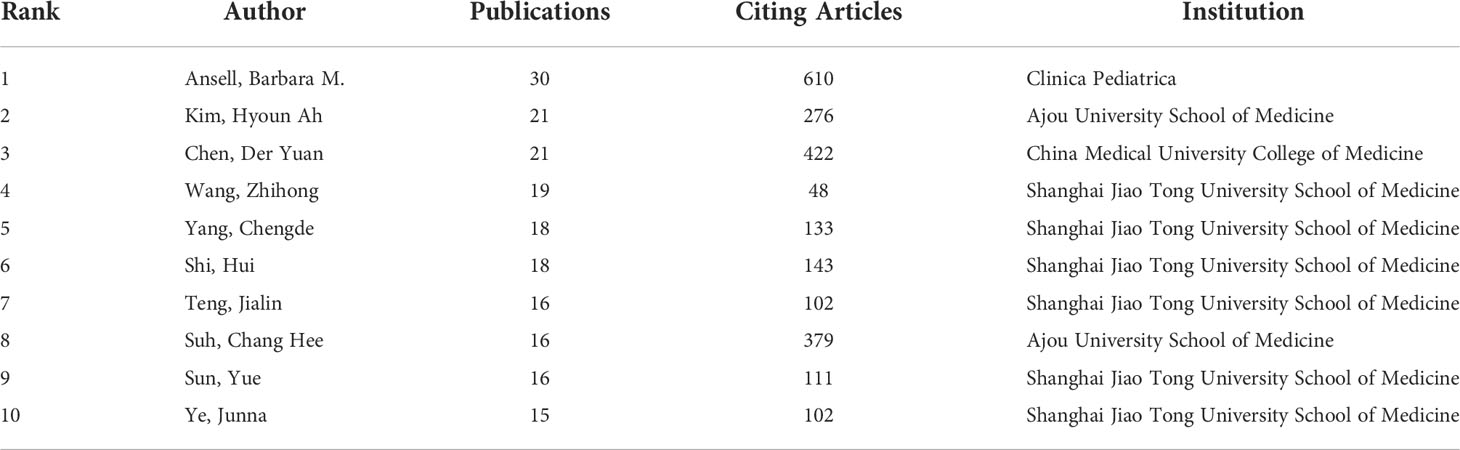
Table 4 Top 10 authors by number of published works from 1921 to 2021.
In the network map of cooperation between authors, the number of nodes is 4,308, and the number of links is 12,056, in which one node represents an author and the size of the circle represents the number of published articles by the author. The larger the node diameter is, the more published articles there are. The connection between the nodes indicates that the authors have a cooperative relationship, as shown in Figure 3A.
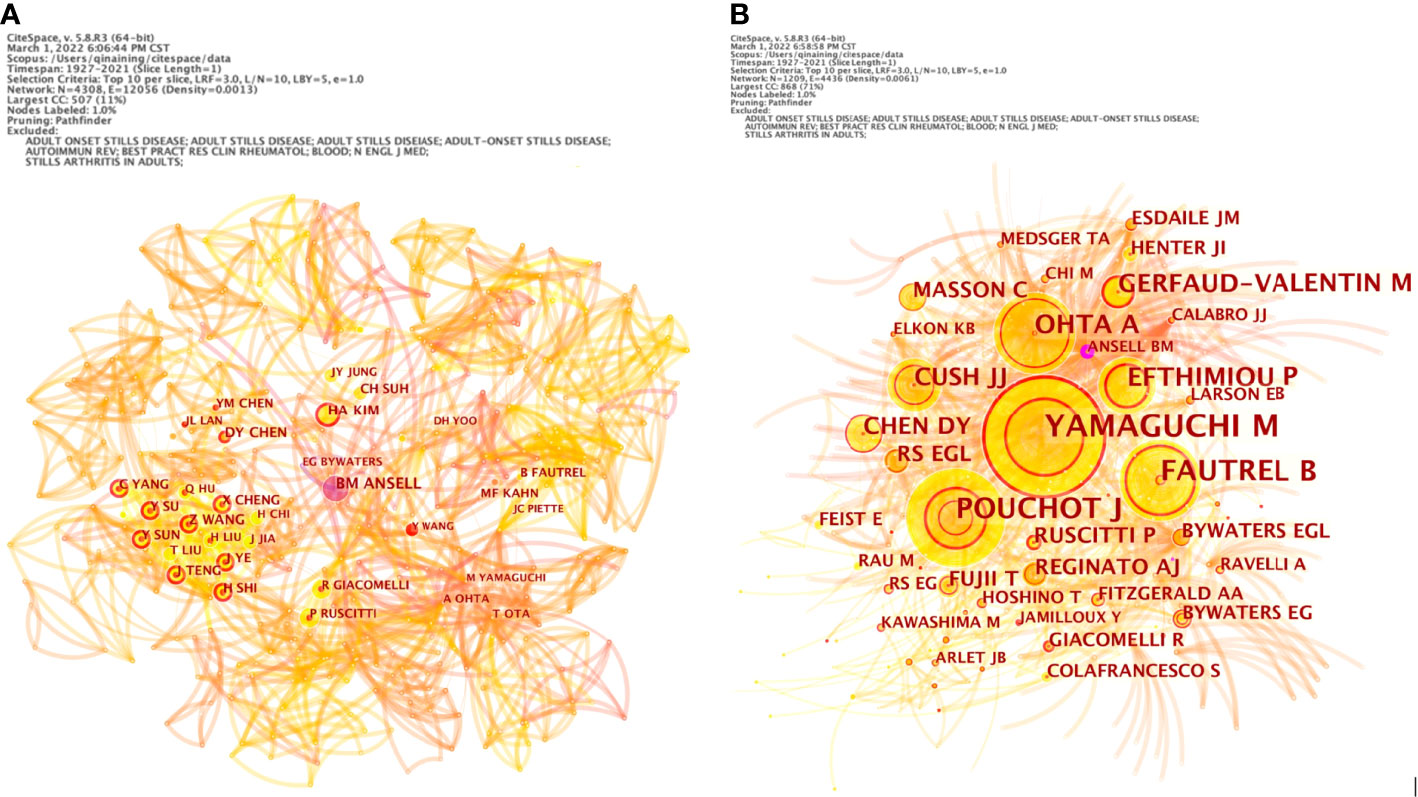
Figure 3 The network map of cooperation between authors (A) and co-authorship (B) of adult-onset Still’s disease articles from 1921 to 2021.
The results show that Ansell, Barbara M., Kim, Hyoun Ah, Chen, Der Yuan, Wang, Zhihong and other authors with high publication volumes each formed several independent core author groups, with close cooperation within the core author group and relatively few connections between different author groups. These authors’ research topics reflect the hot topics in the field to a certain extent, so paying attention to the research direction and content of these core author groups can better understand the development frontier and trend of adult-onset Still’s disease research.
The number of nodes in the co-authorship network is 1,229, and the number of links is 4,436. The top 5 co-authorship times ranking are Yamaguchi, Masaya (703), Pouchot, Jacques (374), Fautrel, Bruno J. (366), Ohta, Akihide (240) and Efthimiou, Petros (229), as shown in Figure 3B.
There are 90 countries/regions around the world paying attention to the research on adult-onset Still’s disease. Five countries have published more than 140 articles, and the top 10 countries/regions have 1,603 articles, accounting for 67.55% of the total published articles. Among them, Japan ranks first with 355 articles, accounting for 14.96% of the total number of articles, followed by the United States (329, 13.86%). See Table 5 for details.
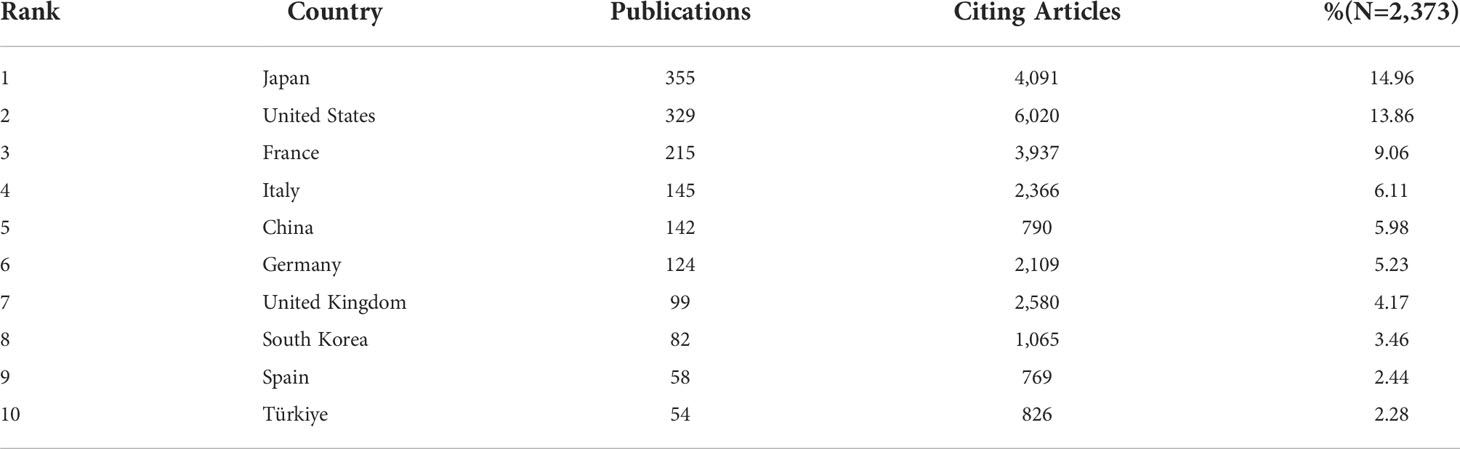
Table 5 Top 10 countries/regions with the largest number of articles from 1921 to 2021.
As shown in Figure 4, the number of nodes in the network of cooperation among countries/regions is 91, and the number of links is 232. The top 3 countries in the centrality ranking are the United States (0.31), France (0.06) and the United Kingdom (0.05), indicating that these 3 countries have close cooperation with other countries/regions.
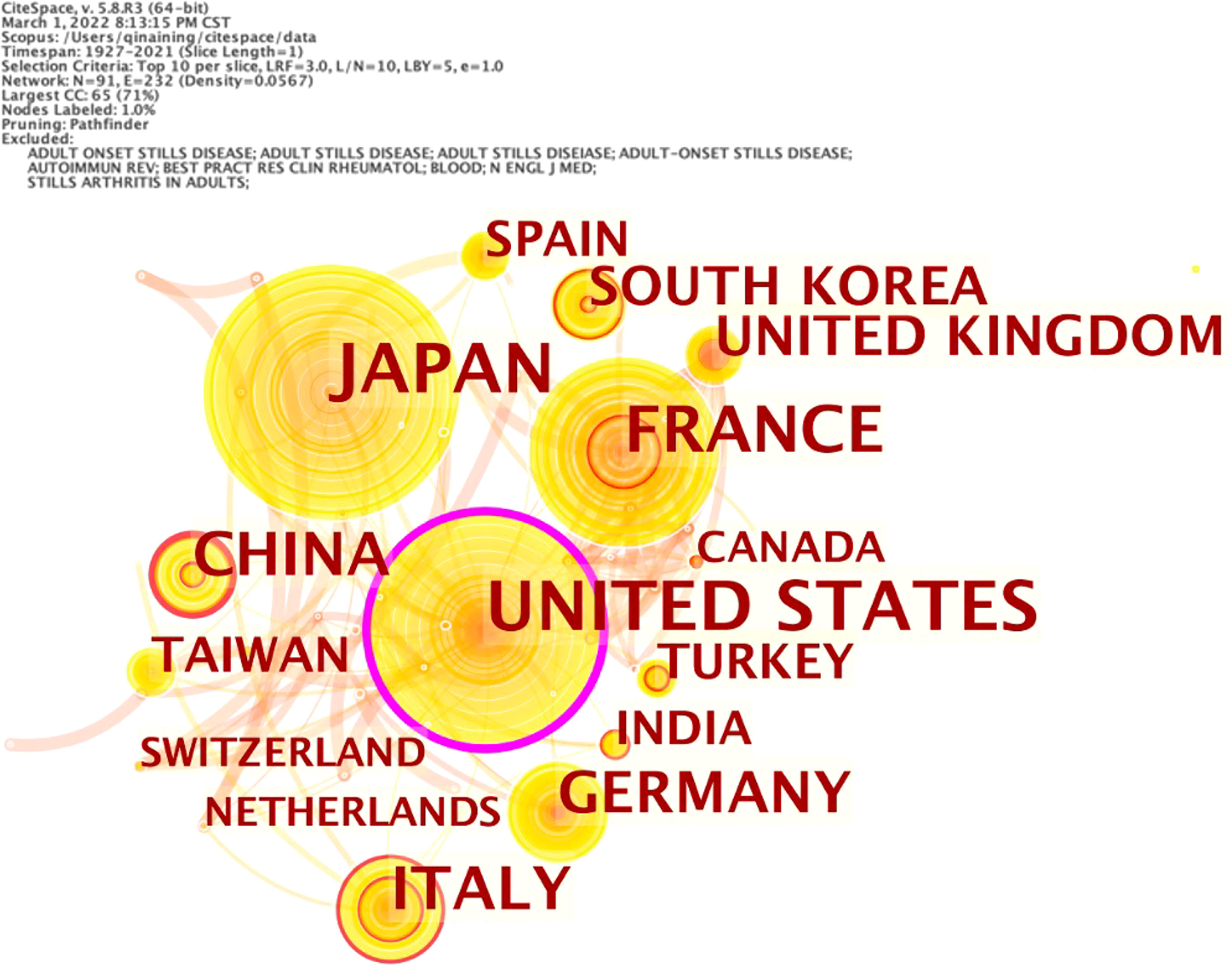
Figure 4 Network of cooperation among countries/regions of adult-onset Still’s disease articles from 1921 to 2021.
Using CiteSpace software to visually analyze the keywords, we obtain the network of co-occurrence among keywords, as shown in Figure 5A. The number of nodes in the keyword co-occurrence network is 395, and the number of links is 1,348. As shown in Table 6, the high frequency keywords in the top 5 are “adult onset Still disease” (1501), “juvenile rheumatoid arthritis” (701), “fever” (663), “arthritis” (605) and “diagnosis” (437).
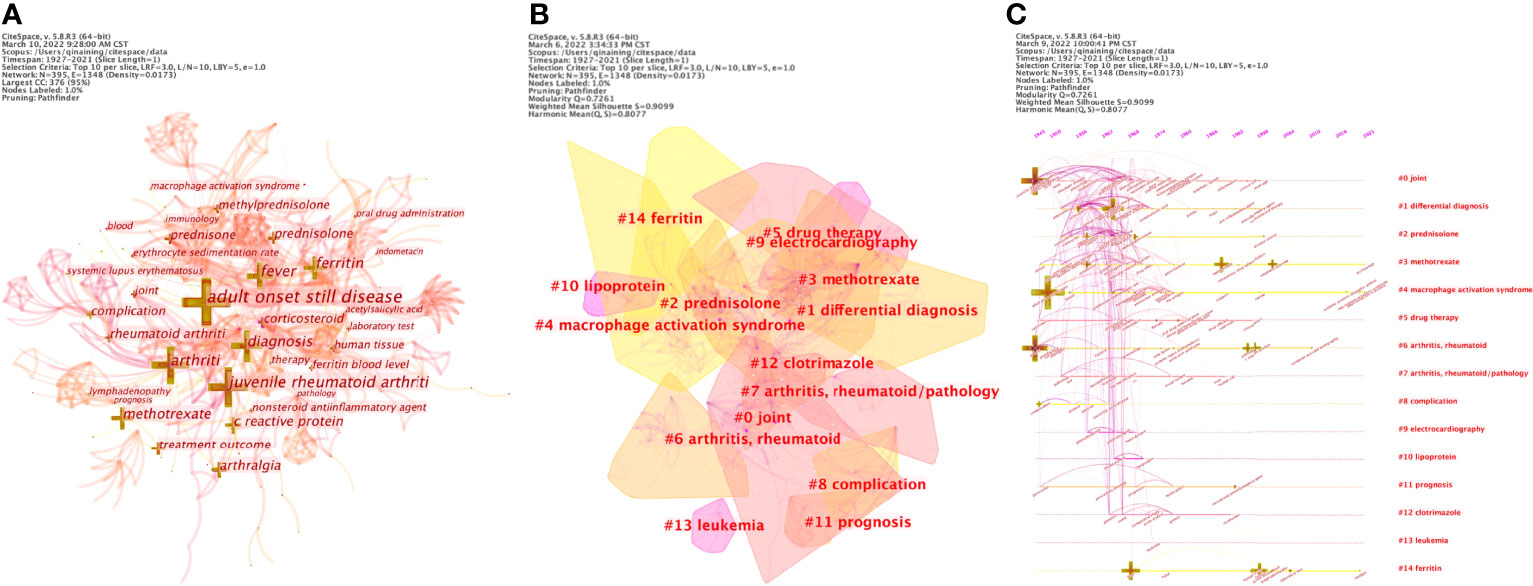
Figure 5 (A) Network of co-occurrence among keywords of adult-onset Still’s disease articles from 1921 to 2021 (B) Keyword clusters analysis of adult-onset Still’s disease articles from 1921 to 2021 (C) The timeline view of keyword clusters of adult-onset Still’s disease articles from 1921 to 2021.
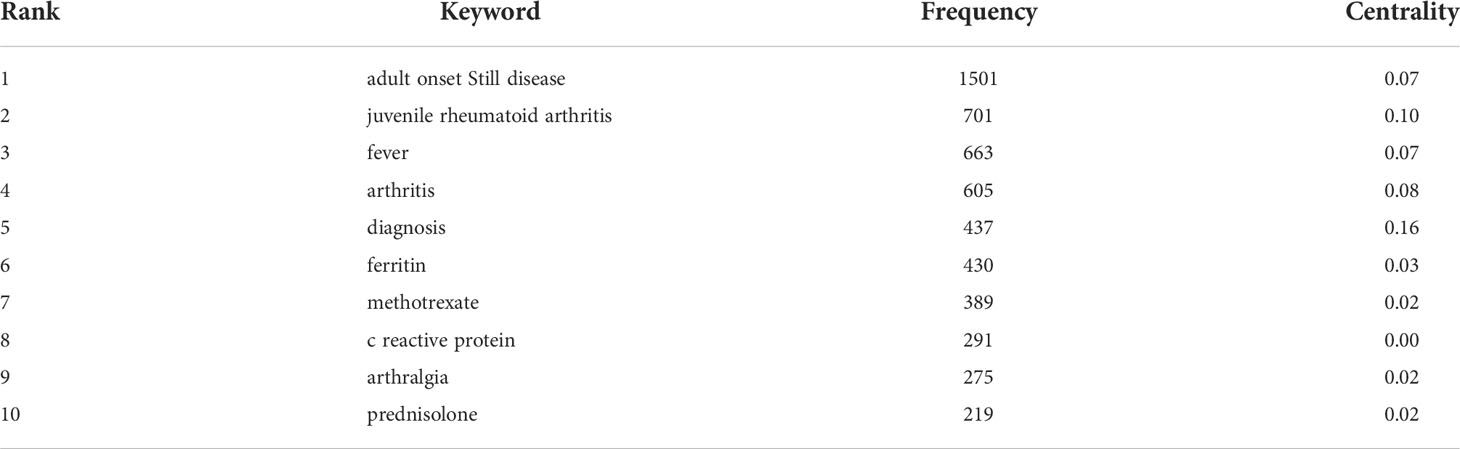
Table 6 High frequency keywords (>200) of adult-onset Still’s disease articles from 1921 to 2021.
Using the log-likelihood ratio (LLR) method in keyword clustering, a total of 28 clustering groups are obtained. Each module represents a cluster, and the larger the module is, the greater the number of keywords in the cluster. The first five cluster groups are as follows: #0 joint, #1 differential diagnosis, #2 prednisolone, #3 methotrexate, and #4 macrophage activation syndrome, as shown in Figure 5B. The clustering groups reflect that the research hotspots are mainly focused on the lesion location, differential diagnosis and therapeutic medication. The timeline view of keyword clusters mainly reflects the relationship between different clustering groups and the changing trend of keywords in the research process. A horizontal line represents a clustering group, and different keywords are arranged on the horizontal line in chronological order. Timeline View in CiteSpace was selected to visually analyze the keywords, and the results are shown in Figure 5C.
Burstness refers to keywords with a sudden or significant increase in frequency in a short time (45). The larger the burst strength is, the more active the field is, and the better it can focus on research hotpots. Using the keyword burst detection function of CiteSpace software, a total of 56 burst keywords are detected, of which the top 25 are shown in Figure 6. Among them, “arthritis” (94) has the strongest burst strength. The keywords with strong burst strength in the past 8 years are “methylprednisolone” (2013-2014), “complication” (2014-2021), “human tissue” (2015-2019), “adult onset Still disease” (2017-2019), and “blood” (2018-2019). The change in that keyword with time can be roughly divided into three stages, in which the keywords of each stage are shown in Table 7.

Figure 6 Top 25 keywords with the strongest citation bursts of adult-onset Still’s disease articles from 1921 to 2021.

Table 7 Keywords during different periods.
In this study, 2,373 articles related to AOSD from the Scopus database were analyzed by bibliometric methods. From 1921 to 2021, the number of published articles showed an overall upward trend (Figure 1), which can be divided into two stages. Before 1972, it was in the initial research period of AOSD, with a few articles published and a slow growth rate of literature. The basic research in this period laid a solid theoretical foundation for the development of AOSD. Since 1972, the number of articles published has increased rapidly, and there is no obvious trend of slowing down, which indicates that the research has not yet entered the mature stage, and the research of AOSD still has great space and potential. For countries, Japan, the United States and France publish the largest number of articles (Table 5), and the United States, France and the United Kingdom engage in relatively more international cooperation (Figure 4), which is basically consistent with the results of other studies (46). This may be because the improvement of gross domestic product and rapidly expanding economies result in more research funding support, thereby increasing scientific productivity (47). In addition, because developed countries have advanced medical levels and abundant scientific research resources, cooperation with developed countries can promote the improvement of scientific productivity. The results show that in scientifically weaker regions, internal cooperation will be more efficient than international cooperation (48). Therefore, we suggest that developed countries strengthen cooperation with wider countries/regions and strengthen internal cooperation and contact in relatively underdeveloped areas to promote the improvement of global standards at the AOSD medical level.
Clinical Rheumatology is the journal with the largest number of published articles, and Journal of Rheumatology is the journal with the most citations (Table 3 and Figure 1). The impact factors of the two journals are above 2, indicating that the quality of AOSD-related research papers is high and has certain academic value. The article Preliminary criteria for classification of adult Still’s disease published by Yamaguchi, Masaya in Journal of Rheumatology in 1992 has the most citations (Table 2). This article describes a preliminary diagnostic criteria of AOSD (29), namely Yamaguchi criteria, which are now widely used.
The most representative and influential authors in the field of AOSD research have formed their own core author groups with little cooperation among them (Figure 3). Ansell, Barbara M.’s group focuses on the pathophysiological changes of AOSD (49, 50). Their study showed that IgG antiglobulin factor levels are elevated in AOSD patients (51). In the FII haemagglutination test for serum antigammaglobulin factors of AOSD patients, the mean FII tube titre increased, and severe incapacity was associated with higher FII titres (52). The group of Kim, Hyoun Ah pointed out that the neutrophil-to-lymphocyte ratio (NLR) can be used as a diagnostic tool and predictor of AOSD recurrence (53). Serum CXCL10, CXCL13 (54) and S100A12 (55) levels can be used as clinical markers to assess the disease activity of AOSD. Chen, D.Y’s team found that there is a fine-tuned mechanism between inflammatory and anti-inflammatory factors in AOSD (56), and IL-18 is an important predictor of active AOSD (57). In addition, galectin-3 (58), C-Type Lectin Domain Family 5-Member A (59), B19-NS1 (60), microRNA-134 (61), and the NLRP3 inflammasome (62) are involved in the pathogenesis of AOSD. Since 2018, the core research team formed by Wang, Zhihong, et al. from Shanghai Jiao Tong University has performed research on biomarkers of AOSD (63) and illustrated the pathogenesis, diagnosis, treatment and nursing of AOSD through clinical case data (64, 65). Their case study pointed out that neutrophils-derived lipocalin-2 can serve as an effective biomarker to identify AOSD with systemic inflammation (66).
The research field of AOSD can be divided into three phases in terms of time (Figure 6 and Table 7) to better determine the research hotspots in different periods and the obvious change in research direction (67). In the early stage of research (1921–1997), researchers paid more attention to the therapeutic medication of disease. JACQUES M. G. W. WOUTERS et al.’s research shows that glucocorticoids can effectively relieve systemic and/or joint symptoms (68). Aydintuǧ, A. Olcay et al. showed that low-dose methotrexate (MTX) can treat AOSD and reduce the dosage of steroids (69). Researchers began to explore the pathological mechanism of disease and biomarkers related to disease in the middle of the research (1998-2011). Chen, Der Yuan’s research showed that Th1 cytokines may promote the pathogenesis of AOSD (70). In the recent stage (2012-2021), the complications of the disease became a hot topic for researchers. As seen, the focus of research has gradually changed from symptoms and treatment of AOSD to the complications and prognosis of diseases. Research on complications and new pathogenesis will become a research trend and hotspot in the future. However, slightly different from our research results, the research results of Xue Zhang et al. show that the research focus in the recent 10 years has mainly been on the treatment of AOSD and its serious complications (46). This difference may be mainly caused by the different literature source databases selected, different data analysis software used, and different literature data time spans included.
Combining the keyword frequency and keyword clustering analysis, the research hotspots and frontier are as follows (Table 6 and Figure 5):
Joints are the commonly affected areas of the AOSD and can occur singly or in combination. Joint problems are difficult to distinguish from other diseases, especially at the early stage of the disease (71). Common affected joints include the knee (43.9-82%), wrist (31.7-73%), ankle (31.7-55%), proximal interphalangeal (21.4-47%), metacarpophalangeal (21.4-46.3%) and other parts (72, 73). The heart is also one of the affected sites of AOSD, usually presenting as pericarditis (37%) (19), cardiac tamponade and myocarditis (74). Heart failure is the most serious manifestation of cardiac involvement, which may lead to death (75). Electrocardiogram (ECG) is a relatively simple and main method for diagnosing and monitoring cardiac involvement (76), and it is widely used in clinical practice. ECG can preliminarily judge whether patients have heart involvement and the degree of involvement to better help improve the follow-up examination and treatment, which are useful noninvasive diagnostic tools (74).
The diagnosis of AOSD primarily depends on the identification of other diseases. Rheumatoid arthritis is a common disease of the rheumatic immune system, with the main symptoms affecting the joints (77). AOSD is mainly distinguished from rheumatoid arthritis by the negative laboratory results of anti-citrullinated peptids autoantibodies and rheumatoid factor (16, 78). Other diseases that need to be identified mainly include Polyarteritis nodosa or other vasculitis, Polymyositis and systemic lupus (22).
Treatment of AOSD begins with NSAIDs, but the response rate to these drugs is only 20–25% (79). Steroids are characterized by their ability to improve systemic manifestations in the acute phase, and they have a good therapeutic effect with a response rate of 76–95% (26), making them the first-line therapeutic drug in clinical practice at the present stage. However, about 45% of patients have steroid dependence and need DMARDs such as MTX to control the dose of steroids (80). At present, MTX is widely used in clinics and has good tolerance (28), about 70% of patients recover completely after MTX treatment (81). In addition, the treatment of prednisone refractory diseases with intravenous pulse methylprednisolone has been verified in some cases (82). The response rate of 60-80% can also be achieved by oral administration of glucocorticoids, such as prednisolone (71). Clotrimazole is an anti-fungal drug (83) that might produce an anti-inflammatory effect by stimulating the adrenal glands, which has been confirmed to be able to improve the symptoms of rheumatoid arthritis (84) and is a potential therapeutic drug for autoimmune diseases (85). Currently, many experiments have proven the feasibility of targeted biologic therapies (34). For example, targeted therapy is carried out by using drugs such as Tocilizumab (86), anti-human IL6 monoclonal antibody (87) and Anti-TNF-α (88).
MAS is one of the most common complications of AOSD, with an incidence rate of over 10% (89). The main symptoms include persistent fever, methemoglobinemia, pancytopenia and hepatic dysfunction (90). MAS is a potentially fatal inflammatory disease that lacks targeted therapy and relies primarily on combination immunosuppressive agents to relieve symptoms (91). Patients with hematopoietic malignancies, such as leukemia, may present with systemic symptoms consistent with AOSD (92). Therefore, to exclude hematological malignancies, the researchers suggest bone marrow aspiration and lymph node biopsy (93). In addition, a case reported that a patient was diagnosed with chronic myeloid leukemia two years after being diagnosed with AOSD, which also suggests the possibility of the development of complications (94). The prognosis of AOSD mainly depends on the severity of visceral involvement and the degree of joint erosion (7). Studies have shown that early diagnosis can improve prognosis, arthritis at diagnosis is an important predictor of disease chronicity, and high fever is a good predictor of systemic disease course (28). Few studies have discussed the prognosis of AOSD alone, which is mainly due to the heterogeneity of the disease (7).
Studies have shown that the chronic inflammatory response and joint destruction symptoms of RA are caused by genetic, environmental and immunological factors (95). Lipoprotein (a) is related to inflammatory reactions, and its monocytes can increase the production of pro-inflammatory cytokines after stimulation (96). Therefore, the increase in lipoprotein(a) levels in AOSD patients may also reflect a high inflammatory state (97). One of the clinical features of AOSD is a significant increase in serum ferritin levels (16). Ferritin is a pro-inflammatory mediator that can induce the expression of inflammatory molecules (98). High levels of ferritin are not only the product of inflammation but also contribute to the development of cytokine storms (99), which may lead to diseases (100). Cytokines such as IL-1β, IL-18, TNF, IFN-γ, and IL-6, which are all involved in the pathogenesis of AOSD, regulate the synthesis of ferritin (78). This finding indicates that ferritin may not only be a biomarker of AOSD but also be involved in the pathogenesis process of AOSD.
To the best of our knowledge, little research systematically and comprehensively discusses the research progress and changing trends in the AOSD field. Therefore, to eliminate this limitation, we used CiteSpace software to visualize information such as authors, journals, and keywords. This study is the first time to analyze the literature in the field of AOSD in the past 100 years. By retrieving the Scopus database with a large amount of data in the field of AOSD, almost all the original studies in this field were included, and the history, current situation and trend analysis of the field of AOSD were conducted. On the one hand, this research provides valuable information for scholars in this field, which helps them understand the development process of AOSD and master the hot topics at the forefront; on the other hand, it also provides new research perspectives and ideas for exploring the development direction of AOSD.
However, this research inevitably has limitations that need to be solved in the future. Due to the continuous updating of the database and the limited analysis year span of CiteSpace software, only the articles from 1921 to November 30, 2021, were selected for this research, and articles published after that were not included in this research. Therefore, there will be discrepancies between bibliometric analysis and actual publication. Restricted by the capabilities of the analysis software, only articles in the Scopus core database are included in this research, which may result in potentially incomplete analytical data. Due to the limitation of CiteSpace software, a lack of unified parameter setting standards, data loss and partial data overlap will inevitably occur in the process of software clustering, which will also lead to the deviation of analysis results. In addition, according to the general process of bibliometrics research, this study adopts an accurate literature search strategy to ensure the correlation between downloaded literature and research topics and uses Cite Space software to remove duplicate literature. However, it is still possible to have subtle errors due to the database or software issues, which are slightly insufficient in artificial induction.
The number of AOSD-related articles is generally on the rise. Developed countries have more research achievements and closer cooperation among countries and lack cooperation with other countries. The diagnosis and treatment of AOSD have always been the focus of researchers’ attention. In the future, the complications and new pathogenesis of AOSD will become research trends and hotspots.
The original contributions presented in the study are included in the article/supplementary material, Further inquiries can be directed to the corresponding author.
AQ wrote the first draft of the manuscript. JS, CG wrote sections of the manuscript. CL contribute to the search strategy of the study. All authors contributed to manuscript revision, read, and approved the submitted version
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Thanks to the teachers at Peking University Health Science Library for their help and support in the process of literature retrieval. Thanks to the doctors and nurses in the Rheumatology and Immunology Department of Peking University People’s Hospital for their clinical guidance in the process of literature collation and analysis.
1. Giacomelli R, Ruscitti P, Shoenfeld Y. A comprehensive review on adult onset still's disease. J Autoimmun (2018) 93:24–36. doi: 10.1016/j.jaut.2018.07.018
2. Wakai K, Ohta A, Tamakoshi A, Ohno Y, Kawamura T, Aoki R, et al. Estimated prevalence and incidence of adult still's disease: findings by a nationwide epidemiological survey in japan. J Epidemiol (1997) 7(4):221–5. doi: 10.2188/jea.7.221
3. Mehta BY, Ibrahim S, Briggs W, Efthimiou P. Racial/Ethnic variations in morbidity and mortality in adult onset still's disease: an analysis of national dataset. Semin Arthritis Rheum (2019) 49(3):469–73. doi: 10.1016/j.semarthrit.2019.04.004
4. Bogdan M, Nitsch-Osuch A, Samel-Kowalik P, Gorynski P, Tyszko P, Kanecki K. Adult-onset still's disease in poland - a nationwide population-based study. Ann Agr Env Med (2021) 28(2):250–4. doi: 10.26444/aaem/132451
5. Magadurjoly G, Billaud E, Barrier JH, Pennec YL, Masson C, Renou P, et al. Epidemiology of adult stills disease - estimate of the incidence by a retrospective study in west france. Ann Rheum Dis (1995) 54(7):587–90. doi: 10.1136/ard.54.7.587
6. Crnogaj MR, Cubelic D, Babic A, Mayer M, Anic B. Treatment of refractory adult onset still's disease with tocilizumab-a single centre experience and literature review. Rheumatol Int (2020) 40(8):1317–25. doi: 10.1007/s00296-020-04622-4
7. Mitrovic S, Fautrel B. Complications of adult-onset still's disease and their management. Expert Rev Clin Immunol (2018) 14(5):351–65. doi: 10.1080/1744666x.2018.1465821
8. Chi HH, Jin HY, Wang ZH, Feng TA, Zeng T, Shi H, et al. Anxiety and depression in adult-onset still's disease patients and associations with health-related quality of life. Clin Rheumatol (2020) 39(12):3723–32. doi: 10.1007/s10067-020-05094-4
9. Fauter M, Gerfaud-Valentin M, Delplanque M, Georgin-Lavialle S, Seve P, Jamilloux Y. Adult-onset still's disease complications. Rev Med Interne (2020) 41(3):168–79. doi: 10.1016/j.revmed.2019.12.003
10. Sakata N, Shimizu S, Hirano F, Fushimi K. Epidemiological study of adult-onset still's disease using a japanese administrative database. Rheumatol Int (2016) 36(10):1399–405. doi: 10.1007/s00296-016-3546-8
11. Sugiyama T, Furuta S, Hiraguri M, Ikeda K, Inaba Y, Kagami SI, et al. Latent class analysis of 216 patients with adult-onset still's disease. Arthritis Res Ther (2022) 24(1):10. doi: 10.1186/s13075-021-02708-3
12. Efthimiou P, Kadavath S, Mehta B. Life-threatening complications of adult-onset still's disease. Clin Rheumatol (2014) 33(3):305–14. doi: 10.1007/s10067-014-2487-4
13. Ben Salah R, Bouattour Y, Turki C, Frikha F, Bahloul Z. Coexistence of thrombotic thrombocytopenic purpura and adult-onset still's disease. Clin Case Rep (2022) 10(2):e05474. doi: 10.1002/ccr3.5474
14. Mimura T, Shimodaira M, Kibata M, Tsukadaira A, Shirahata K. Adult-onset still's disease with disseminated intravascular coagulation and hemophagocytic syndrome: a case report. BMC Res Notes (2014) 7:940. doi: 10.1186/1756-0500-7-940
15. Lowther GH, Chertoff J, Cope J, Alnuaimat H, Ataya A. Pulmonary arterial hypertension and acute respiratory distress syndrome in a patient with adult-onset stills disease. Pulm Circ (2017) 7(4):797–802. doi: 10.1177/2045893217712710
16. Gerfaud-Valentin M, Jamilloux Y, Iwaz J, Seve P. Adult-onset still's disease. Autoimmun Rev (2014) 13(7):708–22. doi: 10.1016/j.autrev.2014.01.058
17. Kaneko Y, Takeuchi T. Interleukin-6 inhibition: A therapeutic strategy for the management of adult-onset still's disease. Expert Opin Biol Ther (2022) 22(1):79–85. doi: 10.1080/14712598.2021.1942832
18. Mitrovic S, Fautrel B. New markers for adult-onset still's disease. Joint Bone Spine (2018) 85(3):285–93. doi: 10.1016/j.jbspin.2017.05.011
19. Pouchot J, Sampalis JS, Beaudet F, Carette S, Decary F, Salusinskysternbach M, et al. Adult stills disease - manifestations, disease course, and outcome in 62 patients. Med (Baltimore) (1991) 70(2):118–36. doi: 10.1097/00005792-199103000-00004
20. Joung CI, Lee HS, Lee SW, Kim CG, Song YH, Jun JB, et al. Association between hla-Dr B1 and clinical features of adult onset still's disease in Korea. Clin Exp Rheumatol (2003) 21(4):489–92.
21. Wang FF, Huang XF, Shen N, Leng L, Bucala R, Chen SL, et al. A genetic role for macrophage migration inhibitory factor (Mif) in adult-onset still's disease. Arthritis Res Ther (2013) 15(3):8. doi: 10.1186/ar4239
22. Fautrel B. Adult-onset still disease. Best Pract Res Clin Rheumatol (2008) 22(5):773–92. doi: 10.1016/j.berh.2008.08.006
23. Girard-Guyonvarc'h C, Gabay C. Biological agents in the management of adult-onset still's disease. Joint Bone Spine (2019) 86(1):5–7. doi: 10.1016/j.jbspin.2018.03.010
24. Kaneko Y. Interluekin-6 inhibitors for the treatment of adult-onset still's disease. Mod Rheumatol (2022) 32(1):12–5. doi: 10.1093/mr/roab004
25. Wang M-Y, Jia J-C, Yang C-D, Hu Q-Y. Pathogenesis, disease course, and prognosis of adult-onset still's disease: An update and review. Chin Med J (2019) 132(23):2856–64. doi: 10.1097/cm9.0000000000000538
26. Efthimiou P, Paik PK, Bielory L. Diagnosis and management of adult onset still's disease. Ann Rheum Dis (2006) 65(5):564–72. doi: 10.1136/ard.2005.042143
27. Mahmood K, Mahmood S, Marsia S. Paving a shorter path towards diagnosis: A case on adult onset still's disease from Pakistan. Cureus (2018) 10(9):5. doi: 10.7759/cureus.3255
28. Gerfaud-Valentin M, Maucort-Boulch D, Hot A, Iwaz J, Ninet J, Durieu I, et al. Adult-onset still disease manifestations, treatment, outcome, and prognostic factors in 57 patients. Med (Baltimore) (2014) 93(2):91–9. doi: 10.1097/md.0000000000000021
29. Yamaguchi M, Ohta A, Tsunematsu T, Kasukawa R, Mizushima Y, Kashiwagi H, et al. Preliminary criteria for classification of adult stills disease. J Rheumatol (1992) 19(3):424–30.
30. Lebrun D, Mestrallet S, Dehoux M, Golmard JL, Granger B, Georgin-Lavialle S, et al. Validation of of the fautrel classification criteria for adult-onset still's disease. Semin Arthritis Rheum (2018) 47(4):578–85. doi: 10.1016/j.semarthrit.2017.07.005
31. Cush JJ, Medsger TA, Christy WC, Herbert DC, Cooperstein LA. Adult-onset stills disease - clinical course and outcome. Arthritis Rheum (1987) 30(2):186–94. doi: 10.1002/art.1780300209
32. Kadavath S, Efthimiou P. Adult-onset still's disease–pathogenesis, clinical manifestations, and new treatment options. Ann Med (2015) 47(1):6–14. doi: 10.3109/07853890.2014.971052
33. Siddiqui M, Putman MS, Dua AB. Adult-onset still's disease: Current challenges and future prospects. Open Access Rheumatol Res Rev (2016) 8:17–22. doi: 10.2147/OARRR.S83948
34. Jamilloux Y, Gerfaud-Valentin M, Henry T, Seve P. Treatment of adult-onset still's disease: A review. Therap Clin Risk Manag (2015) 11:33–43. doi: 10.2147/tcrm.S64951
35. Gabay C, Fautrel B, Rech J, Spertini F, Feist E, Kotter I, et al. Open-label, multicentre, dose-escalating phase ii clinical trial on the safety and efficacy of tadekinig Alfa (Il-18bp) in adult-onset still's disease. Ann Rheum Dis (2018) 77(6):840–7. doi: 10.1136/annrheumdis-2017-212608
36. Kim S, Kim H-R, Lee S-H, Min HK. Diagnosis and treatment of adult-onset still’s disease. Korean J Med (2021) 96(1):30–5. doi: 10.3904/kjm.2021.96.1.30
37. Zhu S, Feng X, Xu W. Bibliometrics analysis on the research status of ankylosing spondylitis from 2009 to 2018. Acad J Second Military Med Univ (2020) 41(4):455–60. doi: 10.16781/j.0258-879x.2020.04.0455
38. Bornmann L. Bibliometrics-based decision trees (Bbdts) based on bibliometrics-based heuristics (Bbhs): Visualized guidelines for the use of bibliometrics in research evaluation. Quant Sci Stud (2020) 1(1):171–82. doi: 10.1162/qss_a_00012
39. Wang H, Tian XM, Wang XR, Wang Y. Evolution and emerging trends in depression research from 2004 to 2019: A literature visualization analysis. Front Psychiatry (2021) 12:705749. doi: 10.3389/fpsyt.2021.705749
40. Zupic I, Cater T. Bibliometric methods in management and organization. Organizational Res Methods (2015) 18(3):429–72. doi: 10.1177/1094428114562629
41. Scopus. Elsevier (2022). Available at: https://www.elsevier.com/solutions/scopus/how-scopus-works Accessed June 12, 2022.
42. de Granda-Orive JI, Alonso-Arroyo A, Garcia-Rio F, Solano-Reina S, Jimenez-Ruiz CA, Aleixandre-Benavent R. Certain advantages of scopus compare with web of science in a bibliometric analysis related to smoking. Rev Esp Doc Cient (2013) 36(2):9. doi: 10.3989/redc.2013.2.941
43. Chen CM. Searching for intellectual turning points: Progressive knowledge domain visualization. Proc Natl Acad Sci U.S.A. (2004) 101:5303–10. doi: 10.1073/pnas.0307513100
44. Liu S, Sun YP, Gao XL, Sui Y. Knowledge domain and emerging trends in alzheimer's disease: A scientometric review based on citespace analysis. Neural Regener Res (2019) 14(9):1643–50. doi: 10.4103/1673-5374.255995
45. Chen BY, Shin S. Bibliometric analysis on research trend of accidental falls in older adults by using citespace-focused on web of science core collection (2010-2020). Int J Environ Res Public Health (2021) 18(4):17. doi: 10.3390/ijerph18041663
46. Zhang X, Yang QY, Yu H, Yin F, He Y, Peng LH, et al. Bibliometric analysis of the global literature productivity of adult-onset still's disease (2011-2020). Rheumatol Int (2022) 42(4):707–16. doi: 10.1007/s00296-022-05097-1
47. Cheng T, Zhang GY. Worldwide research productivity in the field of rheumatology from 1996 to 2010: A bibliometric analysis. Rheumatology (2013) 52(9):1630–4. doi: 10.1093/rheumatology/ket008
48. Scarazzati S, Wang LL. The effect of collaborations on scientific research output: The case of nanoscience in Chinese regions. Scientometrics (2019) 121(2):839–68. doi: 10.1007/s11192-019-03220-x
49. Schaller JG, Johnson GD, Holborow EJ, Ansell BM, Smiley WK. Association of antinuclear antibodies with chronic iridocyclitis of juvenile rheumatoid-arthritis (Stills disease). Arthritis Rheum (1974) 17(4):409–16. doi: 10.1002/art.1780170411
50. Zutshi DW, Friedman M, Ansell BM. Corticotrophin therapy in juvenile chronic polyarthritis (Stills disease) and effect on growth. Arch Dis Child (1971) 46(249):584. doi: 10.1136/adc.46.249.584
51. Torrigiani G, Ansell BM, Chown EEA, Roitt IM. Raised igg antiglobulin factors in stills disease. Ann Rheum Dis (1969) 28(4):424. doi: 10.1136/ard.28.4.424
52. Zutshi DW, Ansell BM, Bywaters EG, Epstein WV, Holborow EJ, Reading CA. Fii haemagglutination test for serum antigammaglobulin factors in stills disease. Ann Rheum Dis (1969) 28(5):541. doi: 10.1136/ard.28.5.541
53. Seo JY, Suh CH, Jung JY, Kim AR, Yang JW, Kim HA. The neutrophil-to-Lymphocyte ratio could be a good diagnostic marker and predictor of relapse in patients with adult-onset still's disease a strobe-compliant retrospective observational analysis. Med (Baltimore) (2017) 96(29):6. doi: 10.1097/md.0000000000007546
54. Han JH, Suh CH, Jung JY, Nam JY, Kwon JE, Yim H, et al. Association of Cxcl10 and Cxcl13 levels with disease activity and cutaneous manifestation in active adult-onset still's disease. Arthritis Res Ther (2015) 17:9. doi: 10.1186/s13075-015-0773-4
55. Bae CB, Suh CH, An JM, Jung JY, Jeon JY, Nam JY, et al. Serum S100a12 may be a useful biomarker of disease activity in adult- onset still's disease. J Rheumatol (2014) 41(12):2403–8. doi: 10.3899/jrheum.140651
56. Liao TL, Chen YM, Tang KT, Chen PK, Liu HJ, Chen DY. Microrna-223 inhibits neutrophil extracellular traps formation through regulating calcium influx and small extracellular vesicles transmission. Sci Rep (2021) 11(1):17. doi: 10.1038/s41598-021-95028-0
57. Chen PK, Lan JL, Huang PH, Hsu JL, Chang CK, Tien N, et al. Interleukin-18 is a potential biomarker to discriminate active adult-onset still's disease from covid-19. Front Immunol (2021) 12:719544. doi: 10.3389/fimmu.2021.719544
58. Chen PK, Lan OL, Li JP, Chang CK, Chang SH, Huang PH, et al. Elevated plasma galectin-3 levels and their correlation with disease activity in adult-onset still's disease. Clin Rheumatol (2020) 39(6):1945–52. doi: 10.1007/s10067-020-04946-3
59. Chen PK, Hsieh SL, Lan JL, Lin CC, Chang SH, Chen DY. Elevated expression of c-type lectin domain family 5-member a (Clec5a) and its relation to inflammatory parameters and disease course in adult-onset still's disease. J Immunol Res (2020) 2020:11. doi: 10.1155/2020/9473497
60. Chen DY, Chen YM, Chen HH, Hsieh CW, Gung NR, Hung WT, et al. Human parvovirus B19 nonstructural protein Ns1 activates Nlrp3 inflammasome signaling in adult-onset still's disease. Mol Med Rep (2018) 17(2):3364–71. doi: 10.3892/mmr.2017.8275
61. Liao TL, Chen YM, Hsieh CW, Chen HH, Lee HC, Hung WT, et al. Upregulation of circulating microrna-134 in adult-onset still's disease and its use as potential biomarker. Sci Rep (2017) 7:12. doi: 10.1038/s41598-017-04086-w
62. Hsieh CW, Chen YM, Lin CC, Tang KT, Chen HH, Hung WT, et al. Elevated expression of the Nlrp3 inflammasome and its correlation with disease activity in adult-onset still disease. J Rheumatol (2017) 44(8):1142–50. doi: 10.3899/jrheum.161354
63. Wang ZH, Chi HH, Sun Y, Teng JL, Feng TN, Liu HL, et al. Serum strem-1 in adult-onset still's disease: A novel biomarker of disease activity and a potential predictor of the chronic course. Rheumatology (2020) 59(11):3293–302. doi: 10.1093/rheumatology/keaa135
64. Hu QY, Wang MY, Jia JC, Teng JL, Chi HH, Liu TT, et al. Tofacitinib in refractory adult-onset still's disease: 14 cases from a single centre in China. Ann Rheum Dis (2020) 79(6):842. doi: 10.1136/annrheumdis-2019-216699
65. Meng JF, Chi HH, Wang ZH, Zhang H, Sun Y, Teng JL, et al. Characteristics and risk factors of relapses in patients with adult-onset still's disease: A long-term cohort study. Rheumatology (2021) 60(10):4520–9. doi: 10.1093/rheumatology/keab023
66. Jia JC, Yang LY, Cao ZJ, Wang MY, Ma YN, Ma X, et al. Neutrophil-derived lipocalin-2 in adult-onset still's disease: A novel biomarker of disease activity and liver damage. Rheumatology (2021) 60(1):304–15. doi: 10.1093/rheumatology/keaa368
67. Yu DJ, Xu ZS, Wang WR. Bibliometric analysis of fuzzy theory research in China: A 30-year perspective. Knowledge Based Syst (2018) 141:188–99. doi: 10.1016/j.knosys.2017.11.018
68. Wouters J, Vandeputte LBA. Adult-onset stills disease - clinical and laboratory features, treatment and progress of 45 cases. Q J Med (1986) 61(235):1055–65. doi: 10.1093/oxfordjournals.qjmed.a068061
69. Aydintug AO, Dcruz D, Cervera R, Khamashta MA, Hughes GRV. Low-dose methotrexate treatment in adult stills disease. J Rheumatol (1992) 19(3):431–5.
70. Chen DY, Lan JL, Lin FJ, Hsieh TY, Wen MC. Predominance of Th1 cytokine in peripheral blood and pathological tissues of patients with active untreated adult onset still's disease. Ann Rheum Dis (2004) 63(10):1300–6. doi: 10.1136/ard.2003.013680
71. Baerlecken NT, Schmidt RE. Adult onset still's disease, fever, diagnosis and therapy. Z Rheumatol (2012) 71(3):174. doi: 10.1007/s00393-011-0859-6
72. Lin SJ, Chao HC, Yan DC. Different articular outcomes of still's disease in Chinese children and adults. Clin Rheumatol (2000) 19(2):127–30. doi: 10.1007/s100670050030
73. Priori R, Colafrancesco S, Gattamelata A, Di Franco M, Di Tondo U, Valesini G. Adult-onset still disease: A rare disorder with a potentially fatal outcome. Auto Immun Highlights (2010) 1(1):53–9. doi: 10.1007/s13317-010-0009-1
74. Gracia-Ramos AE, Contreras-Ortiz JA. Myocarditis in adult-onset still's disease: Case-based review. Clin Rheumatol (2020) 39(3):933–47. doi: 10.1007/s10067-019-04814-9
75. Neel A, Wahbi A, Tessoulin B, Boileau J, Carpentier D, Decaux O, et al. Diagnostic and management of life-threatening adult-onset still disease: A French nationwide multicenter study and systematic literature review. Crit Care (2018) 22:10. doi: 10.1186/s13054-018-2012-2
76. Bazzani C, Cavazzana I, Ceribelli A, Vizzardi E, Dei Cas L, Franceschini F. Cardiological features in idiopathic inflammatory myopathies. J Cardiovasc Med (2010) 11(12):906–11. doi: 10.2459/JCM.0b013e32833cdca8
77. Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet (2016) 388(10055):2023–38. doi: 10.1016/s0140-6736(16)30173-8
78. Feist E, Mitrovic S, Fautrel B. Mechanisms, biomarkers and targets for adult-onset still's disease. Nat Rev Rheumatol (2018) 14(10):603–18. doi: 10.1038/s41584-018-0081-x
79. Sfriso P, Priori R, Valesini G, Rossi S, Montecucco CM, D'Ascanio A, et al. Adult-onset still's disease: An Italian multicentre retrospective observational study of manifestations and treatments in 245 patients. Clin Rheumatol (2016) 35(7):1683–9. doi: 10.1007/s10067-016-3308-8
80. Sfriso P, Bindoli S, Galozzi P. Adult-onset still's disease: Molecular pathophysiology and therapeutic advances. Drugs (2018) 78(12):1187–95. doi: 10.1007/s40265-018-0956-9
81. Franchini S, Dagna L, Salvo F, Aiello P, Baldissera E, Sabbadini MG. Efficacy of traditional and biologic agents in different clinical phenotypes of adult-onset still's disease. Arthritis Rheum (2010) 62(8):2530–5. doi: 10.1002/art.27532
82. Khraishi M, Fam AG. Treatment of fulminant adult stills disease with intravenous pulse methylprednisolone therapy. J Rheumatol (1991) 18(7):1088–90. doi: 10.1002/art.1780340728
83. Crowley PD, Gallagher HC. Clotrimazole as a pharmaceutical: Past, present and future. J Appl Microbiol (2014) 117(3):611–7. doi: 10.1111/jam.12554
84. Wojtulewski JA, Gow PJ, Walter J, Grahame R, Gibson T, Panayi GS, et al. Clotrimazole in rheumatoid-arthritis. Ann Rheum Dis (1980) 39(5):469–72. doi: 10.1136/ard.39.5.469
85. Jensen BS, Hertz M, Christophersen P, Madsen LS. The Ca2+-activated k+ channel of intermediate Conductance:A possible target for immune suppression. Expert Opin Ther Targets (2002) 6(6):623–36. doi: 10.1517/14728222.6.6.623
86. Kishida D, Okuda Y, Onishi M, Takebayashi M, Matoba K, Jouyama K, et al. Successful tocilizumab treatment in a patient with adult-onset still's disease complicated by chronic active hepatitis b and amyloid a amyloidosis. Mod Rheumatol (2011) 21(2):215–8. doi: 10.1007/s10165-010-0365-8
87. Iwamoto M, Nara H, Hirata D, Minota S, Nishimoto N, Yoshizaki K. Humanized monoclonal anti-Interieukin-6 receptor antibody for treatment of intractable adult-onset still's disease. Arthritis Rheum (2002) 46(12):3388–9. doi: 10.1002/art.10620
88. Husni ME, Maier AL, Mease PJ, Overman SS, Fraser P, Gravallese EM, et al. Etanercept in the treatment of adult patients with still's disease. Arthritis Rheum (2002) 46(5):1171–6. doi: 10.1002/art.10231
89. Arlet JB, Huong DLT, Marinho A, Amoura Z, Wechsler B, Papo T, et al. Reactive haemophagocytic syndrome in adult-onset still's disease: A report of six patients and a review of the literature. Ann Rheum Dis (2006) 65(12):1596–601. doi: 10.1136/ard.2005.046904
90. Crayne CB, Albeituni S, Nichols KE, Cron RQ. The immunology of macrophage activation syndrome. Front Immunol (2019) 10:119. doi: 10.3389/fimmu.2019.00119
91. Carter SJ, Tattersall RS, Ramanan AV. Macrophage activation syndrome in adults: Recent advances in pathophysiology, diagnosis and treatment. Rheumatology (2019) 58(1):5–17. doi: 10.1093/rheumatology/key006
92. Delplanque M, Aouba A, Hirsch P, Fenaux P, Graveleau J, Malard F, et al. Usaid associated with myeloid neoplasm and vexas syndrome: Two differential diagnoses of suspected adult onset still's disease in elderly patients. J Clin Med (2021) 10(23):13. doi: 10.3390/jcm10235586
93. Hofheinz K, Schett G, Manger B. Adult onset still's disease associated with malignancy-cause or coincidence? Semin Arthritis Rheum (2016) 45(5):621–6. doi: 10.1016/j.semarthrit.2015.10.003
94. Nakagawa Y, Furusyo N, Taniai H, Henzan H, Tsuchihashi T, Hayashi J. Chronic myelogenous leukemia that occurred two years after the diagnosis of adult still's disease. Intern Med (2005) 44(9):994–7. doi: 10.2169/internalmedicine.44.994
95. Lin YJ, Anzaghe M, Schulke S. Update on the pathomechanism, diagnosis, and treatment options for rheumatoid arthritis. Cells (2020) 9(4):43. doi: 10.3390/cells9040880
96. Tsimikas SA. Test in context: Lipoprotein(a) diagnosis, prognosis, controversies, and emerging therapies. J Am Coll Cardiol (2017) 69(6):692–711. doi: 10.1016/j.jacc.2016.11.042
97. Yanai H, Moriyama S, Hirowatari Y, Kaneko H. Very low density lipoprotein, chylomicron, and lipoprotein (a) are more useful to detect the development of macrophage activation syndrome in adult-onset still's disease as compared with cytokines and triglyceride. Am J Hematol (2013) 88(9):828–30. doi: 10.1002/ajh.23517
98. Ruddell RG, Hoang-Le D, Barwood JM, Rutherford PS, Piva TJ, Watters DJ, et al. Ferritin functions as a proinflammatory cytokine Via iron-independent protein kinase c Zeta/Nuclear factor kappab-regulated signaling in rat hepatic stellate cells. Hepatology (2009) 49(3):887–900. doi: 10.1002/hep.22716
99. Jamilloux Y, Gerfaud-Valentin M, Martinon F, Belot A, Henry T, Seve P. Pathogenesis of adult-onset still's disease: New insights from the juvenile counterpart. Immunol Res (2015) 61(1-2):53–62. doi: 10.1007/s12026-014-8561-9
Keywords: Still’s disease, adult-onset, scopus, bibliometrics [MeSH], trends, epidemiology
Citation: Qin A, Sun J, Gao C and Li C (2022) Bibliometrics analysis on the research status and trends of adult-onset Still’s disease: 1921-2021. Front. Immunol. 13:950641. doi: 10.3389/fimmu.2022.950641
Received: 23 May 2022; Accepted: 27 June 2022;
Published: 18 July 2022.
Edited by:
Chang-Hee Suh, Ajou University, South KoreaReviewed by:
Ourlad Alzeus Gaddi Tantengco, University of the Philippines Manila, PhilippinesCopyright © 2022 Qin, Sun, Gao and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jing Sun, c3VuamluZzk5QGJqbXUuZWR1LmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.