 Marcela Araujo de Oliveira Santana1*
Marcela Araujo de Oliveira Santana1* Willian Vargas Tenório da Costa2
Willian Vargas Tenório da Costa2 Isadora Costa Celestino3
Isadora Costa Celestino3 Diogo Fernandes dos Santos1,2
Diogo Fernandes dos Santos1,2 Bruno de Carvalho Dornelas3,4
Bruno de Carvalho Dornelas3,4 Matthew Martin Pavelka5
Matthew Martin Pavelka5 Andrea De Martino Luppi1,3
Andrea De Martino Luppi1,3 Isabela Maria Bernardes Goulart1,2
Isabela Maria Bernardes Goulart1,2- 1National Reference Center for Sanitary Dermatology and Leprosy, Clinics’ Hospital, Faculty of Medicine, Federal University of Uberlândia, Uberlândia, Brazil
- 2Faculty of Medicine, Federal University of Uberlândia, Uberlândia, Brazil
- 3Post-Graduation Program in Health Science, Faculty of Medicine, Federal University of Uberlândia, Uberlândia, Brazil
- 4Pathology Department, Clinical Hospital, Faculty of Medicine, Federal University of Uberlândia, Uberlândia, Brazil
- 5School of Medicine, Indiana University, Terre Haute, IN, United States
Mycobacterium leprae, the etiologic agent of leprosy, is an acid-fast-staining and slow-growing bacilli that infect macrophages and Schwann cells individually or through forming globi. The clinical presentation of leprosy is broad and depends on the host immune response. We report a case of a 42-year-old Brazilian man presenting with fever of unknown origin (FUO), anemia, wasting syndrome, and neuropathy. The diagnosis of lepromatous leprosy was made after an extensive investigation revealed the presence of M. leprae in the bone marrow. Bone marrow involvement in leprosy is rare and some authors believe the presence of M. leprae in the bone marrow can act as a reservoir of the disease facilitating future relapses. It is important to investigate bone marrow involvement in leprosy, especially when the patient presents with cytopenias and positive epidemiologic history.
Introduction
Mycobacterium leprae, the etiologic agent of leprosy (Hansen’s disease), is an acid-fast-staining and slow-growing bacilli (1, 2). This intracellular bacteria infects macrophages and Schwann cells individually and could grow to form globi (1, 2).
The clinical presentation of leprosy is broad and depends on the host immune response (3). It usually involves the peripheral nervous system and skin, in addition to mucous membranes in some instances (3). The presentation of leprosy related to bone marrow infiltration is rare with only a few case reports in the literature diagnosing leprosy by bone marrow biopsy or aspiration (4–6).
We report a case of a patient presenting with fever of unknown origin (FUO), anemia, wasting syndrome, and neuropathy. The investigation revealed the presence of M. leprae in the bone marrow, and the diagnosis of lepromatous leprosy was made.
Case Description
A 42-year-old Brazilian man was admitted to the hospital due to wasting syndrome, fever of unknown origin (FUO), hyporexia, asthenia, and night sweats. The patient reported worsening of his condition during the last month to the point of becoming bedridden. He also reported edema up to his knees, skin peeling, and severe, bilateral lower extremity weakness.
One year before admission, the patient started presenting pain in his lower limbs that worsened during physical activities. Five months later, he started complaining of paresthesia and burning sensations from his knees to his feet. He reported no chronic conditions or significant past medical history and denied the use of any medications, drugs, alcohol, or tobacco. The family reported that his mother and brother were diagnosed with leprosy one year before the patient’s presentation.
The physical exam revealed weight loss of approximately 25 kg (55.11 lbs.) in five months, hepatosplenomegaly and lymphadenopathy confirmed with ultrasound, hypoesthesia to touch, and painful stimuli. Additional physical findings included the presence of bilaterally thickened neural trunks, inability to fully flex the fingers, and dactylitis. During the neurological exam, normal reflexes, motor coordination, and cranial nerve reactions were observed. The visual inspection yielded diffuse skin infiltration all over the body (especially on the face, hands, feet, and ears) and the presence of small lepromas on the posterior thighs and legs.
The laboratory exams revealed microcytic and hypochromic anemia (Table 1) and a normal pattern for serum protein electrophoresis (SPEP). Testing for HIV, T-Spot.TB, syphilis (VDRL), and hepatitis B and C were negative. The cerebral spinal fluid (CSF) analysis was normal (Table 2). The chest computed tomography (CT) was normal, and the abdomen CT revealed hepatosplenomegaly.
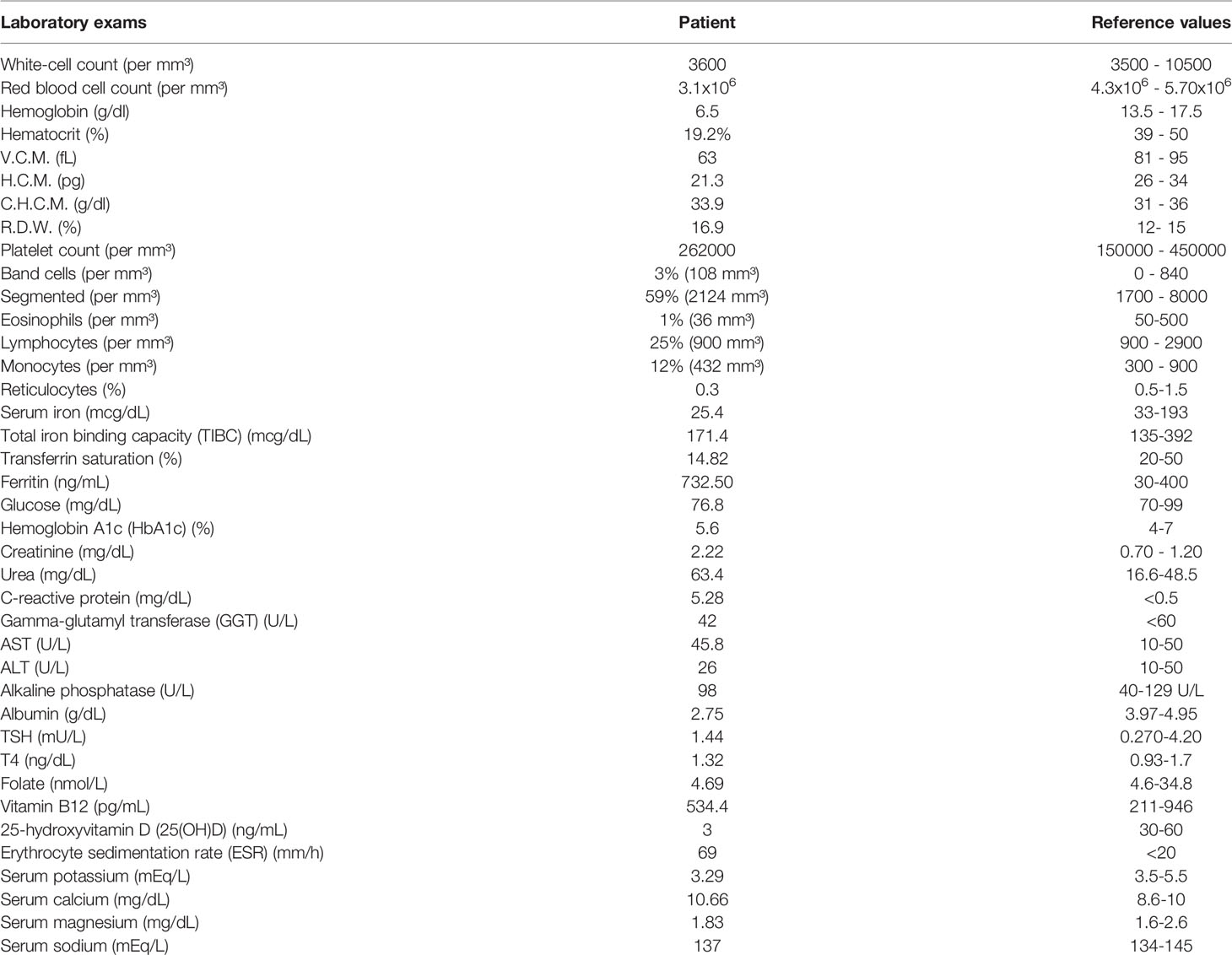
Table 1 Laboratory exams.
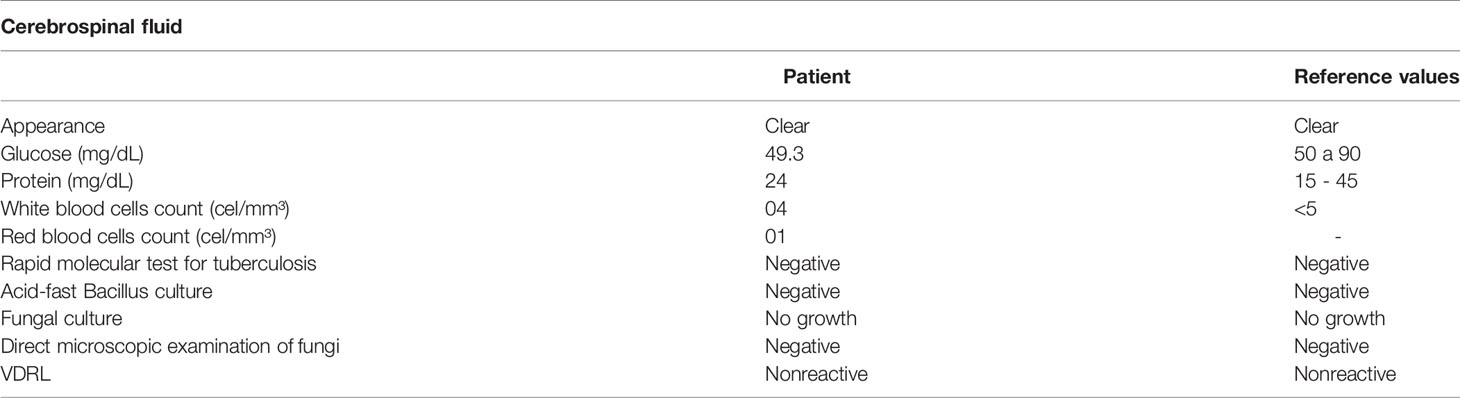
Table 2 Cerebrospinal fluid analysis.
Electroneuromyography showed an asymmetrical sensory and motor axonal neuropathy with focal slowing of conduction velocity and severe impairment of ulnar nerves in the elbow segment and tibial nerves in the ankle. Ultrasonography of peripheral nerves displayed echographic findings suggestive of hypertrophic neuropathy of the ulnar, median, left peroneal, and tibial nerves (more evident at pre-tunnel levels) in addition to signs of intraneural hyperemia in the left ulnar nerve at the pre-tunnel level and mild thickening of the right peroneal nerve.
A bone marrow biopsy (Figures 1, 2) revealed the presence of M. leprae forming globi. The ELISA anti-phenolic glycolipid I (PGL-I) IgM antibodies and M. leprae DNA were positive, with index 2.38 (normal values: <1 - negative) (7). The slit skin smear Bacilloscopy Index (BI) mean was 4.16 (Table 3).
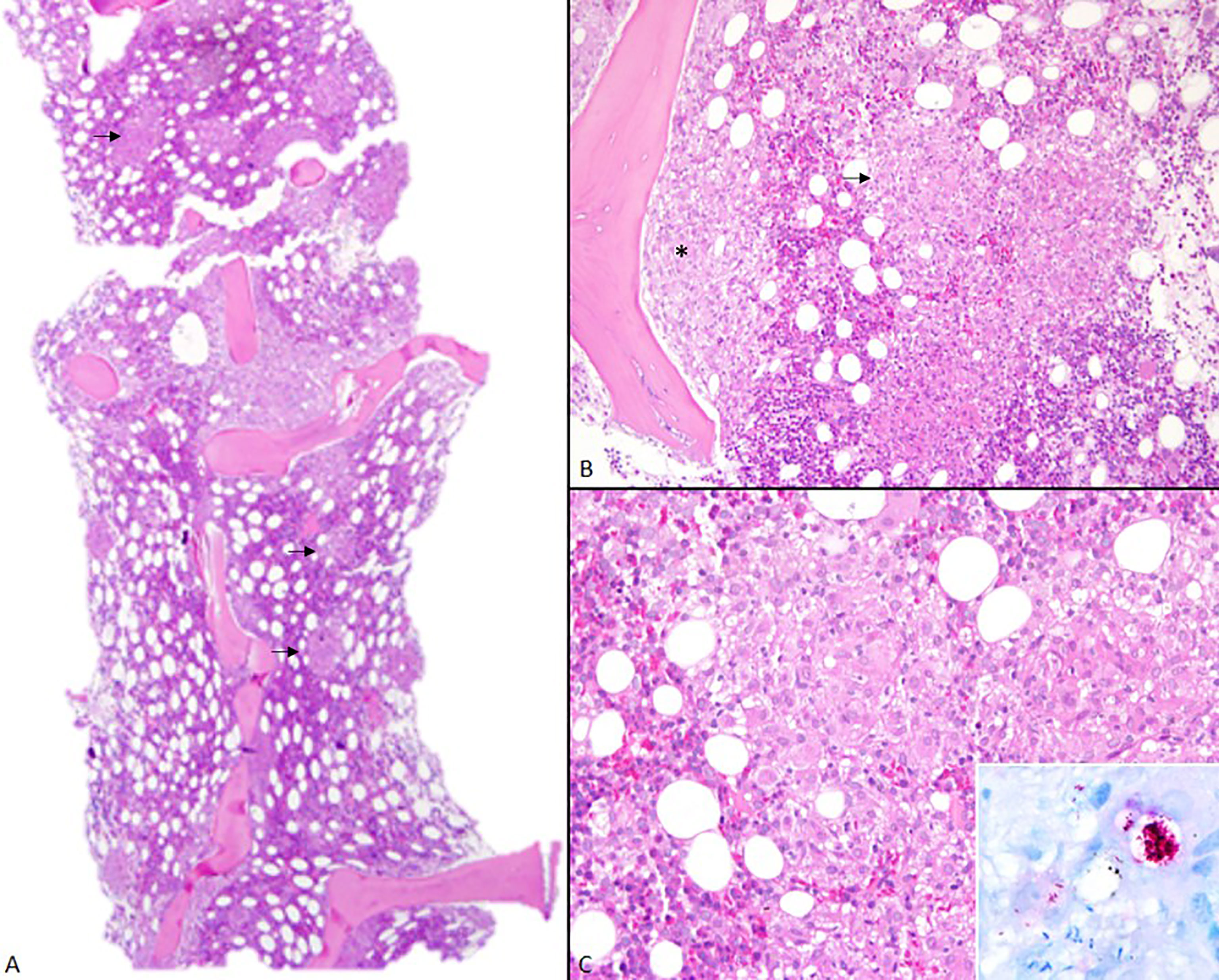
Figure 1 Bone marrow. (A) At low power, bone marrow microscopic examination shows hypercellularity in nodular pattern (arrows) (H&E, 2x). (B) Noncaseating epithelioid granulomas in interstitial (arrow) and paratrabecular loci (*) (H&E, 10x). (C) These granulomas are composed mostly of epithelioid macrophages and a few dispersed lymphocytes (20x, H&E). In detail, macrophages are enlarged by large collections of leprosy bacilli – globi (100x, Faraco-Fite).
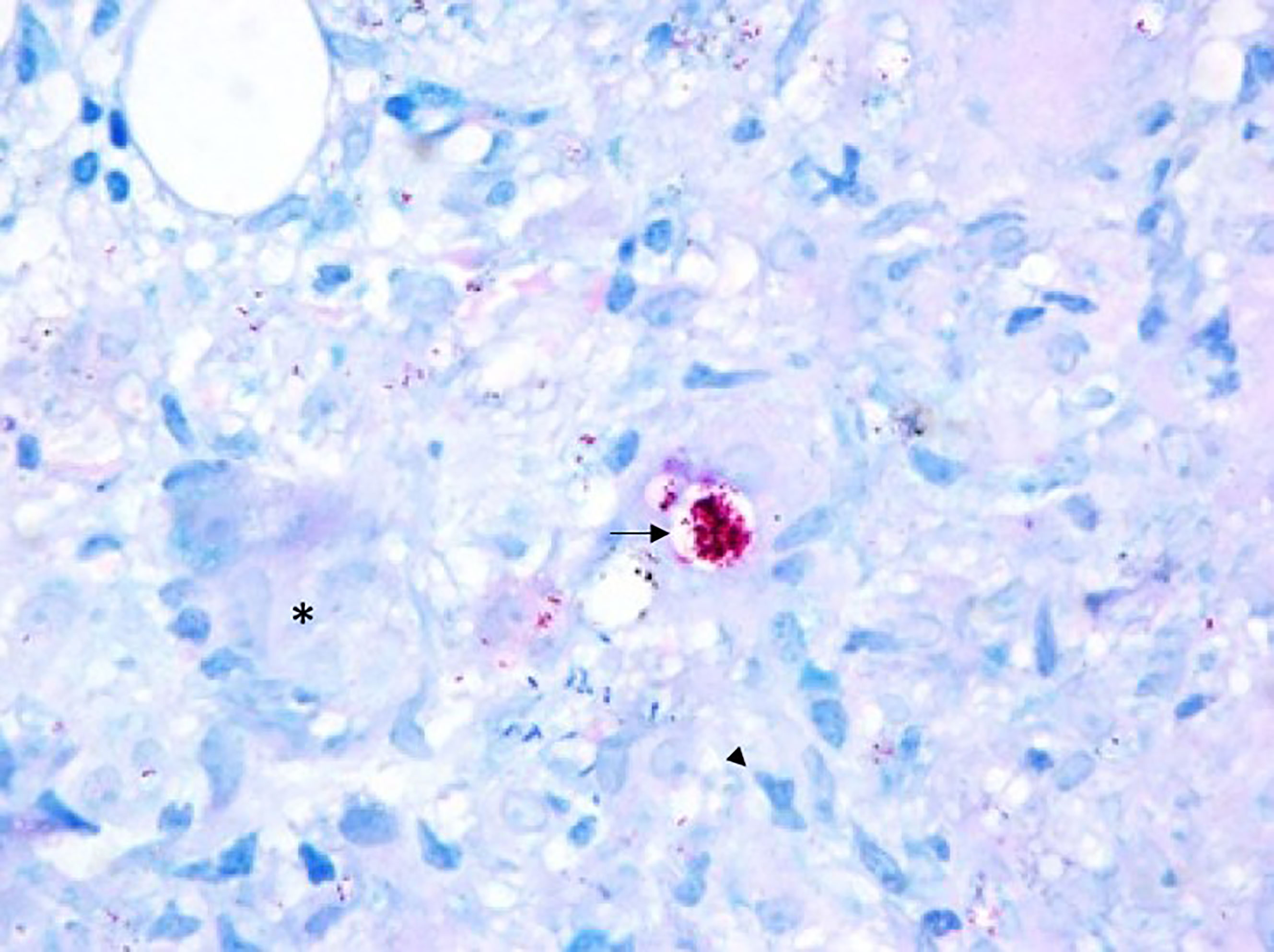
Figure 2 Bone Marrow - Epithelioid granuloma composed of macrophages (arrow head) and multinucleated giant cells (*) rich in bacilli, which may present in isolation or bound together forming globi (arrow), what distinguishes M. leprae from other mycobacteria (100x, Faraco-Fite).
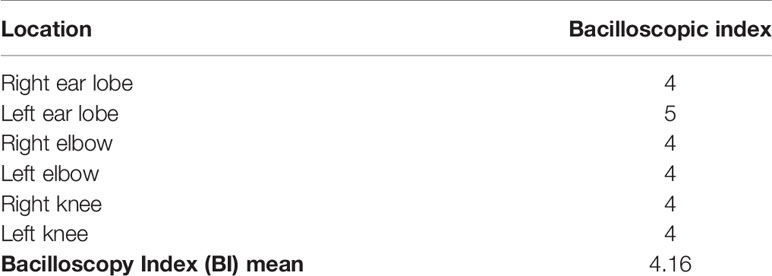
Table 3 Bacilloscopic index.
To detect M. leprae DNA, were used a real-time quantitative polymerase chain reaction (qPCR) primer/probe assay, described elsewhere, to target the M. leprae species-specific genomic element of dispersed repeats (RLEP) (ABI 7300 realtime PCR system; Applied Biosystems). The slit skin smear DNA M. leprae qPCR was positive Ct = 19 (normal values ≤ 35) with 3.8x108 copies/mL. The skin biopsy showed whole bacilli with BI equal to 6.0 and Ct = 21 (normal values ≤ 35) with 2.1x109 copies/gram. The diagnosis of lepromatous leprosy was made. The treatment was started with a supervised monthly dose of rifampin (600 mg), ofloxacin (400 mg), and minocycline (100 mg), and an unsupervised daily dose of ofloxacin (400 mg) and minocycline (100 mg). This treatment was chosen to avoid the use of dapsone, due to the possibility of drug-induced anemia worsening the patient’s condition.
During the first months of treatment, the patient gained weight, his nutritional status improved, and he was able to perform independent activities of daily living again. He has been followed up monthly by a multi-professional team at our outpatient clinic with good adherence to the proposed treatment.
Discussion
The presence of M. leprae in bone marrow aspirates or biopsies was already described in previous case reports (5, 6). Even though major studies are necessary, some authors believe the presence of M. leprae in the bone marrow, especially in lepromatous leprosy, can act as a reservoir of the disease facilitating future relapses (8).
Although bone marrow involvement in leprosy is rare, it is important to investigate bone marrow involvement in leprosy, especially when the patient presents with cytopenias (9). The differential diagnosis can be broad and variable depending on the clinical presentation. The majority of the cases involve the investigation of FUO, wasting syndrome, and cytopenias. In those cases, the main differential diagnosis was lymphoproliferative diseases that were considered less probable after the laboratory results revealed a normal pattern for serum protein electrophoresis (SPEP) and the absence of concerning findings for neoplasia on the abdomen and chest computerized tomography (CT) (4–6).
Shepard and Karat (1972) used the inoculation of mice to show bacilli in the bone marrow were viable and able to multiply. They hypothesized that the presence of M. leprae in the bone marrow could lead to inhibition of lymphocytes’ sensitivity for the mycobacteria, which diminishes the immune response in peripheral tissues for those with lepromatous leprosy (10).
Karat (1975) used footpads of mice to show that M. leprae remained viable in the bone marrow long after it ceased to be viable in the skin following treatment with oral dapsone or clofazimine (11). Since that time, leprosy treatment has evolved despite a lack of studies to clarify the relationship of the bacilli with the immune system and its presence in the bone marrow. The high number of leprosy relapses raises concern for a possible mechanism involving the persistence of bacilli multiplying in organs, such as bone marrow, after the standard treatment, especially in lepromatous leprosy (8, 12, 13).
The patient also developed cachexia, another contributor to the severe weakness presented by the patient. The weight loss in leprosy can be associated with the inflammatory state, especially during reactional episodes. High levels of tumor necrosis factor-alpha (TNF-α), interleukin-1 (IL-1), interferon-gamma (IFN-γ), and other cytokines are found in leprosy patients during reactional episodes (14, 15). Those same cytokines are related to the mechanisms of muscle wasting related to cachexia and weight loss (16). Besides that, TNF-α and IFN-γ may be involved in the pathogenesis of peripheral neuropathy (17), as seen in the severe neuropathy presented by our patient.
The laboratory exam revealed a remarkably low vitamin D level. There are studies associating vitamin D receptor (VDR) polymorphism with leprosy (18–20), but robust studies correlating serum vitamin D level, receptor polymorphism, and response to M. leprae are still needed. However, in this case, the low level of vitamin D can also be a consequence explained by the patient being bedridden without sun exposure, which is an important factor in the conversion of this vitamin. Furthermore, the cachexia, confirmed by observing the serum albumin and folate, may contribute to the low vitamin D.
Although a liver biopsy was not performed, we believe that hepatosplenomegaly was caused by lepromatous leprosy. It was either caused by the direct presence of the M. leprae or as part of an immune reaction to the pathogen. Previous studies have already shown leprosy as a cause of granulomatous hepatitis (21–25). Hepatosplenomegaly can also be present during a reaction episode showing a different histopathological pattern, similar to the one present on the reactionary erythema nodosum on the skin (25). The hepatic involvement in leprosy is usually with absent or mild increase on liver function tests, especially aminotransferases, but a previous case report shows the possibility of high serum aminotransferase levels from leprosy-induced liver disease (24, 25).
Another important aspect of this case is the delay in the diagnosis. The patient was evaluated at different points of the healthcare network without a previous diagnosis. The delay in diagnosis can be partly explained by the lack of appreciation of the family history of leprosy (mother and brother) as a risk factor for the patient’s illness. Evidence shows increased risk for developing leprosy among household contacts, especially for exposure to contacts diagnosed with multibacillary disease and older patients (26). Ideally, this patient should have been monitored since the first diagnosis of leprosy in his household. Brazilian guidelines emphasize the importance of epidemiological vigilance and surveillance of household and social contacts. It is suggested that the contacts should be evaluated every year for at least 5 years (27).
Unfortunately, leprosy has not been listed often among the differential diagnoses of FUO in the literature (28), which likely contributed to the delay in the diagnosis and clinical management of our patient. Therefore, leprosy should be considered in the differential diagnosis of FUO associated with neuropathies and wasting syndrome. The case shows the importance of the follow-up and active search for cases in household contacts. In this case, an early diagnosis could have prevented major sequelae and severe disease.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the local research ethics committee CAAE: 57585422200005152. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
MS, WC, BD, and IG conceived of the presented idea. MS, IG, WC, and IC contributed to the data collection. MS and IG took the lead in writing the manuscript with support from all the other authors. All authors contributed to manuscript revisions. All authors contributed to the final approval of the version to be published.
Funding
This study received funding from: FAPEMIG (Research Support Foundation of the State of Minas Gerais, Grant number: APQ - 02810-21) and the National Health Fund - Ministry of Health of Brazil. Grant number: TED 123/DIPOC 003/2020.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Chavarro-Portillo B, Soto CY, Guerrero MI. Mycobacterium Leprae’s Evolution and Environmental Adaptation. Acta Trop (2019) 197:105041. doi: 10.1016/j.actatropica.2019.105041
2. Scollard DM, Adams LB, Gillis TP, Krahenbuhl JL, Truman RW, Williams DL. The Continuing Challenges of Leprosy. Clin Microbiol Rev (2006) 19:338–81. doi: 10.1128/CMR.19.2.338-381.2006
3. Kundakci N, Erdem C. Leprosy: A Great Imitator. Clin Dermatol (2019) 37:200–12. doi: 10.1016/j.clindermatol.2019.01.002
4. Oliveira CC, Niéro-Melo L, Domingues MAC. Xanthomatous Macrophages in Bone Marrow Biopsies: Systemic Manifestation of Mycobacterioses. Ann Hematol (2017) 96:1237–8. doi: 10.1007/s00277-017-3018-6
5. Velasco D, Lozano S, Villarrubia J. Leprosy Diagnosed by Bone Marrow Aspiration. Br J Haematol (2013) 160:121–1. doi: 10.1111/bjh.12101
6. de Oliveira LR, Maltos AL. Mycobacterium Leprae in Bone Marrow. Rev Bras Hematol E Hemoter (2014) 36:300–1. doi: 10.1016/j.bjhh.2014.05.010
7. Lobato J, Costa MP, Reis EM, Gonçalves MA, Spencer JS, Brennan PJ, et al. Comparison of Three Immunological Tests for Leprosy Diagnosis and Detection of Subclinical Infection. Lepr Rev (2011) 82:389–401. doi: 10.47276/lr.82.4.389
8. Somanath P, Vijay KC. Bone Marrow Evaluation in Leprosy: Clinical Implications. Lepr Rev (2016) 87:122–3. doi: 10.47276/lr.87.1.122
9. Rastogi P, Chhabria BA, Sreedharanunni S, Pannu A, Varma N, Varma S. Leprosy and Bone Marrow Involvement. QJM (2016) 110:189–90. doi: 10.1093/qjmed/hcw204
10. Shepard CC, Karat ABA. Infectivity of Leprosy Bacilli From Bone Marrow and Liver of Patients With Lepromatous Leprosy. Lepr Rev (1972) 43:21–6. doi: 10.5935/0305-7518.19720003
11. Karat ABA. Viability of Myco. Leprae in the Skin and Bone Marrow of Patients With Lepromatous Leprosy While on Dapsone or Lamprene. Lepr Rev (1975) 46:69–72. doi: 10.5935/0305-7518.19750042
12. Kaimal S, Thappa D. Relapse in Leprosy. Indian J Dermatol Venereol Leprol (2009) 75:126–35. doi: 10.4103/0378-6323.48656
13. Nascimento ACM do, dos Santos DF, Antunes DE, Gonçalves MA, Santana MAO, Dornelas B de C, et al. Leprosy Relapse: A Retrospective Study on Epidemiologic, Clinical, and Therapeutic Aspects at a Brazilian Referral Center. Int J Infect Dis (2022) 118:44–51. doi: 10.1016/j.ijid.2022.01.009
14. Sarno EN, Grau GE, Vieira LM, Nery JA. Serum Levels of Tumour Necrosis Factor-Alpha and Interleukin-1 Beta During Leprosy Reactional States. Clin Exp Immunol (1991) 84:103–8.
15. Polycarpou A, Walker SL, Lockwood DNJ. A Systematic Review of Immunological Studies of Erythema Nodosum Leprosum. Front Immunol (2017) 8:233. doi: 10.3389/fimmu.2017.00233
16. Mitch WE, Goldberg AL. Mechanisms of Muscle Wasting. The Role of the Ubiquitin-Proteasome Pathway. N Engl J Med (1996) 335:1897–905. doi: 10.1056/nejm199612193352507
17. Sykam A, Gutlapalli VR, Tenali SP, Meena AK, Chandran P, Pratap DVS, et al. Association of Tumor Necrosis Factor-Alpha and Interferon Gamma Gene Polymorphisms and Their Plasma Levels in Leprosy, HIV and Other Peripheral Neuropathies. Cytokine (2015) 76:473–9. doi: 10.1016/j.cyto.2015.09.010
18. Goulart LR, Ferreira FR, Goulart IMB. Interaction of TaqI Polymorphism at Exon 9 of the Vitamin D Receptor Gene With the Negative Lepromin Response may Favor the Occurrence of Leprosy. FEMS Immunol Med Microbiol (2006) 48:91–8. doi: 10.1111/j.1574-695X.2006.00128.x
19. Singh I, Lavania M, Pathak VK, Ahuja M, Turankar RP, Singh V, et al. VDR Polymorphism, Gene Expression and Vitamin D Levels in Leprosy Patients From North Indian Population. PLoS Negl Trop Dis (2018) 12:e0006823. doi: 10.1371/journal.pntd.0006823
20. Pepineli AC, Alves HV, Tiyo BT, Macedo LC, Visentainer L, de Lima Neto QA, et al. Vitamin D Receptor Gene Polymorphisms Are Associated With Leprosy in Southern Brazil. Front Immunol (2019) 10:2157. doi: 10.3389/fimmu.2019.02157
21. Almaguer-Chavez J, Ocampo-Candiani J, Gomez-Flores M, Welsh O. An Unusual Case of Leprosy With Granulomatous Hepatitis. J Am Acad Dermatol (2009) 60(3):2301. doi: 10.1016/j.jaad.2008.11.475
22. Sabharwal BD, Malhotra N, Garg R, Malhotra V. Granulomatous Hepatitis: A Retrospective Study. Indian J Pathol Microbiol (1995) 38(4):413–6.
23. Braghiroli NAF, Oliveira PD, Sadigursky M, Machado PRL. Diagnosing Lepromatous Leprosy by Liver Biopsy: A Case of Granulomatous Hepatitis. Leprosy Rev (2018) 89(3):306–9. doi: 10.47276/lr.89.3.306
24. Karat ABA, Job CK, Rao PSS. Liver in Leprosy: Histological and Biochemical Findings. BMJ (1971) 1(5744):307–10. doi: 10.1136/bmj.1.5744.307
25. Ferrari TC, Araújo MG, Ribeiro MM. Hepatic Involvement in Lepromatous Leprosy. Lepr Rev (2002) 73(1):72–5. doi: 10.47276/lr.73.1.72
26. Teixeira CSS, Pescarini JM, Alves FJO, Nery JS, Sanchez MN, Teles C, et al. Incidence of and Factors Associated With Leprosy Among Household Contacts of Patients With Leprosy in Brazil. JAMA Dermatol (2020) 156:640–8. doi: 10.1001/jamadermatol.2020.0653
27. Brasil. Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Vigilância das Doenças Transmissíveis. Diretrizes Para Vigilância, Atenção E Eliminação Da Hanseníase Como Problema De Saúde Pública: Manual Técnico-Operacional (2016). Available at: http://www.credesh.ufu.br/sites/credesh.hc.ufu.br/arquivos/diretrizes-eliminacao-hanseniase-4fev16-web.pdf (Accessed November 25, 2021).
Keywords: lepromatous leprosy, bone marrow, neuropathy, fever of unknown origin, case report
Citation: Santana MAO, da Costa WVT, Celestino IC, dos Santos DF, Dornelas BdC, Pavelka MM, Luppi ADM and Goulart IMB (2022) Fever of Unknown Origin, Wasting Syndrome and Bone Marrow Involvement: A Leprosy Case Report. Front. Immunol. 13:916319. doi: 10.3389/fimmu.2022.916319
Received: 09 April 2022; Accepted: 03 June 2022;
Published: 07 July 2022.
Edited by:
Nicola Ivan Lorè, San Raffaele Scientific Institute (IRCCS), ItalyReviewed by:
Utpal Sengupta, The Leprosy Mission Trust India, IndiaDegang Yang, Tongji University, China
Copyright © 2022 Santana, da Costa, Celestino, dos Santos, Dornelas, Pavelka, Luppi and Goulart. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marcela Araujo de Oliveira Santana, bWFyY2VsYTIwc2FudGFuYUB1ZnUuYnI=