 Scott M. Krummey
Scott M. Krummey Alison J. Gareau
Alison J. Gareau
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol., 05 August 2022
Sec. Alloimmunity and Transplantation
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.916200
This article is part of the Research TopicNew advances in matching and donor selection for HCTView all 6 articles
Advances in hematopoietic stem cell transplant (HSCT) have led to changes in the approach to donor selection. Many of these new approaches result in greater HLA loci mismatching, either through the selection of haploidentical donors or permissive HLA mismatches. Although these approaches increase the potential of transplant for many patients by expanding the number of acceptable donor HLA genotypes, they add the potential barrier of donor-specific HLA antibodies (DSA). DSA presents a unique challenge in HSCT, as it can limit engraftment and lead to graft failure. However, transient reduction of HLA antibodies through desensitization treatments can limit the risk of graft failure and facilitate engraftment. Thus, the consideration of DSA in donor selection and the management of DSA prior to transplant are playing an increasingly important role in HSCT. In this review, we will discuss studies addressing the role of HLA antibodies in HSCT, the reported impact of desensitization on DSA levels, and the implications for selecting donors for patients with DSA. We found that there is a clear consensus that moderate strength DSA should be avoided, while desensitization strategies are reported to be effective in most cases at reducing DSA to amenable levels. There is limited information regarding the impact of specific characteristics of DSA, such as HLA loci or overall level of sensitization, which could further aid in donor selection for sensitized HSCT candidates.
Hematopoietic stem cell transplantation (HSCT) is a life-saving therapeutic option for a wide range of malignant and non-malignant hematologic disorders. Historically, bone marrow transplant was performed on human leukocyte antigen (HLA) matched related or unrelated donors, due to the significant morbidity and mortality of graft-versus-host-disease (GVHD) associated with HLA mismatch (1–3). Advances in conditioning regimens, graft-versus-host prophylaxis, and HLA genotyping technology instigated new approaches for donor selection in order to increase the successful identification of donors and improve post-transplant outcomes. In cases where an HLA identical related donor is not an option, either haploidentical related or mismatched unrelated donors are often available.
In recent years, advances in HLA genotyping and clinical management have led to the successful use of mismatched donors in the form of haploidentical related transplant and permissively HLA mismatched transplants (3). While haploidentical HSCT has gained traction in recent years due to advances in the approach to manage engraftment and mitigate intense alloreactivity in both the graft and host directions. In addition, recent work has elucidated situations where mismatches of specific HLA loci carry a reduced risk of graft failure or GVHD. These “permissive” mismatches have been described based on the HLA-DPB1 allele and HLA-B leader sequence dimorphisms.
These advances have expanded access to transplant for many patients, particularly those from non-Caucasian ethnic groups where matched unrelated donors are less abundant (4). However, both HLA haploidentical and mismatched donors introduce the complication of donor-specific HLA antibodies (DSA), which can be a barrier to transplantation. Thus, increasing the use of HLA-mismatched donors in HSCT places increased importance on overcoming the barrier of DSA in HSCT. In contrast to solid organ transplant, HLA antibodies in HSCT represent a unique challenge in that the source of those antibodies, the host immune system, is replaced by the process of transplantation. Thus, if the deleterious effect of HLA antibodies on donor cell engraftment can be transiently reduced, there is a significant chance of long-term success. This has led to the routine use desensitization in HSCT programs using HLA mismatched donor-recipient pairing in the setting of DSA.
In this article, we will review the role of DSA in HSCT, the efficacy of desensitization approaches in mitigating DSA. From the perspective of HLA, we will discuss the conclusions and knowledge gaps that exist when considering DSA against potential HSCT donors.
Among unrelated HSCT donors, multiple seminal studies established that minimizing the number of HLA mismatches is advantageous for survival and GVHD mitigation (5). Expert CIBMTR guidelines recently codified that there is no advantage to mismatch at any specific locus among HLA-A, -B, -C, or DRB1 (5, 6). Elegant work by Fernandez-Vina and colleagues found that mismatching at the low expression loci HLA-DRB3/4/5, -DQB1, and -DPB1 was associated with worse overall survival and transplant-related mortality among 7/8 matched unrelated cases, and had little impact among 8/8 matched cases (7). Thus, for unrelated mismatched HSCT, there is little consensus about the preference of HLA loci mismatch.
Recently, two bodies of work have begun to establish a hierarchy of outcomes related to HLA mismatch. HLA locus-specific algorithms have been identified to identify so-called permissive mismatches for HLA-DPB1 and HLA-B that do not carry an increased risk of GVHD or graft failure. HLA-DPB1 has historically not been included in HSCT genotyping and matching consideration. With advances in genotyping technology, many centers have access to HLA-DPB1 genotyping. Using an elegant series of in vitro experiments and bioinformatics, Zino and colleagues classified HLA-DPB1 alleles into groups based on the presence of alloreactive T cell epitopes, leading to the algorithmic assessment of permissive and non-permissive HLA-DPB1 mismatching between donors and recipients (8). Non-permissive HLA-DPB1 mismatching has been shown to be associated with worse outcomes, primarily non-relapse mortality and rates of GVHD (6, 9).
More recently, studies have uncovered the importance of HLA-B exon 1 sequence matching in HSCT outcomes. The HLA-B exon 1 encodes a nonamer peptide leader sequence that can be presented by HLA-E, which binds to T and NK cell receptors. The HLA-B leader sequence position two, unlike HLA-A and -C, is dimorphic, encoding either a methionine (M) or a threonine (T) (10). Recent work has evaluated the patient genotype and B leader sequence mismatch on GVHD and transplant outcomes. The International Histocompatibility Working Group evaluated nearly 34,000 unrelated HSCTs and found that among those with a single HLA-B locus mismatch, HLA-B leader mismatching was associated with greater GVHD risk versus leader matching, and that a shared T leader haplotype was lower risk than a shared M leader haplotype (11). Another study of unrelated HSCT cases with one mismatch at HLA-A, -B, -C, -DRB1, or -DQB1, found associations between HLA-B leader mismatch and genotype with mismatches at either HLA-DQB1 or -DRB1 that were associated with increased non-relapse mortality and GVHD (12). Thus, for unrelated mismatched donors, identifying the permissiveness of HLA-B leader mismatches is emerging as a way to improve outcomes in HLA mismatched unrelated HSCT. For unrelated donors, while the 10/10 HLA matching is ideal, this recent work has elucidated a hierarchy of mismatches that can lower the risk of GVHD and mortality.
The use of related HLA haploidentical transplantation has gained traction in recent years because of the significant expansion of the potential donor pool. While only 20-30% of patients have a potential HLA matched sibling, nearly all patients have haploidentical family members that could serve as donors (4). Multiple approaches are currently used to successfully manage the alloreactivity associated with haploidentical HSCT that result in high rates of engraftment and limited GVHD (4, 13, 14). Our center has reported successful outcomes using post-transplant cyclophosphamide in haploidentical HSCT versus matched related donors (15, 16). For these reasons, along with the speed at which donors can be evaluated for transplant, the use of haploidentical donors has been rising worldwide and represents another area in which HLA mismatch is increasingly being confronted (17).
Together, these developments have established new algorithms for HSCT donor selection. Transplant of mismatched donors by either approach, however, increases the likelihood of DSA complicating donor selection.
The HLA genes are the most polymorphic in the human genome, which have evolved to allow the immune system to sense foreign pathogens and provide wide-ranging protection (18, 19). The classical HLA genes are comprised of the Class I and Class II genes that present peptide antigen to T cells. To date, over 30,000 Class I and Class II alleles have been identified. The Class I HLA-A, -B, and -C genes are expressed on all nucleated cells, while the Class II HLA-DR, -DQ, and -DP genes are expressed on antigen presenting cells. Expression of Class II can be induced on other cell types, particularly in the setting of inflammation. Historically, HLA matching for HSCT patients and donors was performed for HLA-A, -B, -C, and -DR (8/8 loci matching), owing to limited typing methods that precluded typing at HLA-DQ and -DP (19). Currently, with the widespread and growing use of next-generation sequencing to perform genotyping, matching is clinically assessed at HLA-A, -B, -C, -DR, -DQ (10/10 loci matching) although data is available for donors and recipients at all HLA loci, including HLA-DP, -DRB345, -DQA1, and -DPA1.
Due to the high degree of polymorphism and the necessity of transplanting across HLA antigen mismatches in some cases, the presence of HLA antibodies directed against mismatched donor antigens has been recognized as a significant barrier to graft acceptance (20, 21). For HSCT patients, HLA antibodies can form through multiple mechanisms that activate HLA-specific humoral immunity. Major avenues include pregnancy, blood transfusion, and prior organ transplant. Blood transfusions are a common source of sensitization for patients undergoing HSCT, due to the effects of chemotherapeutic treatments for hematologic malignancy. In addition, inflammatory events such as vaccination, infection, or trauma can result in the formation of HLA antibodies, potentially due to cross-reactivity or bystander activation (22). Studies have estimated that approximately half of transplant candidates are positive for HLA antibody (20, 23, 24). Among HSCT candidates, multiparous females are more likely to be HLA sensitized than nulliparous females or males (20, 23).
Testing of patient sera prior to incompletely HLA-matched transplantation is critical to detect DSA that can impact engraftment, and to characterize the breadth and strength of DSA. DSA detection with solid-phase and cell-based assays is routinely performed in most HLA laboratories to inform clinical practice and stratify immune risk for patients, for both solid organ and bone marrow transplant programs (Table 1). Solid phase assays have been pioneered through the linkage of purified recombinant class I and II protein to microparticles labeled with fluorescent markers (25). Single-antigen bead (SAB) assays allow for the detection of DSA against each potential HLA mismatch, and the level of DSA in patient serum can be interpreted in a semi-quantitative manner using mean fluorescent intensity (MFI) values detected with Luminex-based technology (23, 26–28). However, due to the high sensitivity of this assay and the potential for false-positive reactions, cell-based crossmatch assays can be used to complement SAB results as they correlate with the ability of DSA to bind to donor cells in vitro (27). Traditionally, complement-dependent cell-based crossmatches were used to assess donor-recipient compatibility, but they have been largely replaced by crossmatches using flow cytometry because of the increased sensitivity. A flow crossmatch can provide valuable information in cases where patients have DSA that would be too low for detection by a complement-dependent crossmatch. Results from solid-phase and cell-based assays are invaluable in helping guide donor selection in the setting of mismatched HCT.
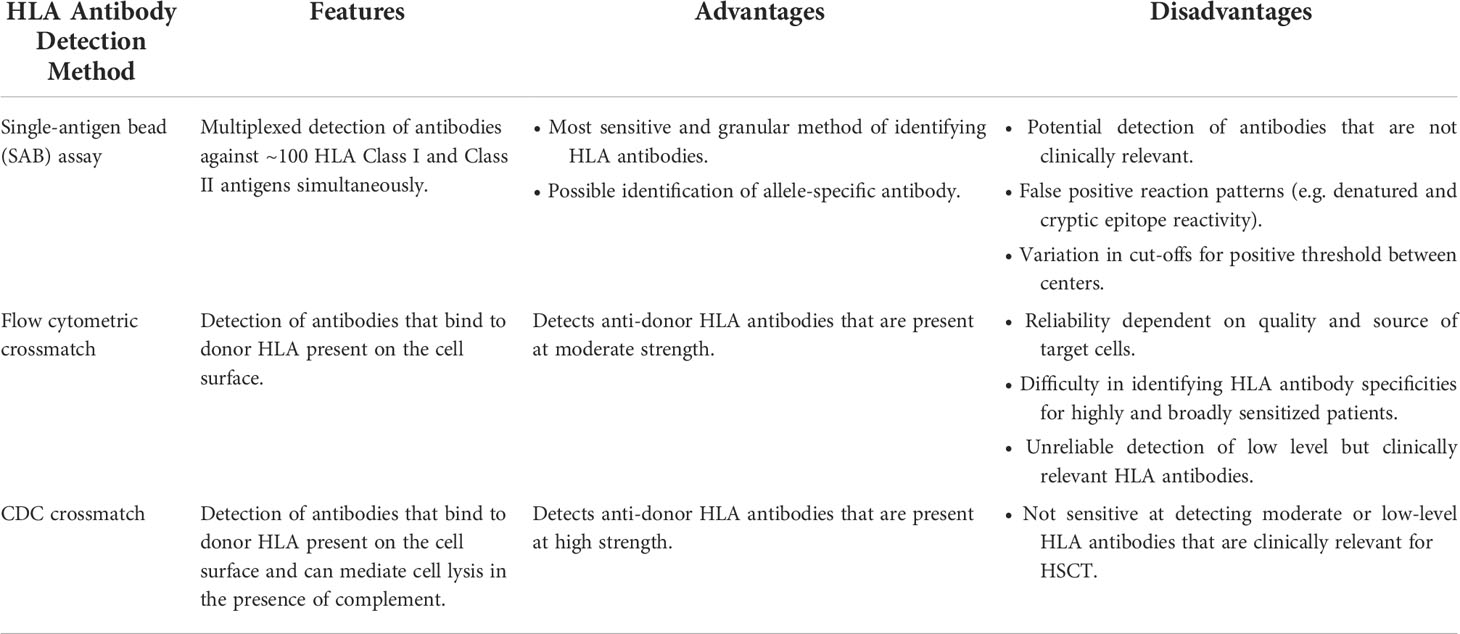
Table 1 Overview of methods used to detect donor-recipient compatibility and identify DSA.
The relationship between the presence of DSA prior to mismatched allogeneic HSCT and negative impact on primary engraftment and graft survival is now well-established (20, 29). While early studies evaluating the role of DSA in HSCT confirmed that a positive crossmatch was a risk factor for primary graft failure, a group of studies in the modern era of DSA detection using SAB results has provided more granular detail about the risk of high-level DSA in HSCT in various transplant settings (20, 21).
Among matched unrelated donor transplants, Ciurea et al. evaluated the impact of DSA in a cohort of 592 patients. Among the 19.6% of patients with HLA antibodies, eight had DSA against DPB1 (24). While the rate of primary graft failure was 3.2% among patients without DSA, three of eight patients with DSA had graft failure. In a retrospective case-control study of HSCT cohorts with or without failed transplants (groups of thirty-seven and seventy-eight patients, respectively), Spellman et al. found that 24% of the failed transplants had DSA against HLA-A, -B, or –DP, compared with 1% of the control group (30).
In umbilical cord blood transplants, Takanashi et al. found that the presence of DSA in twenty patients was associated with delayed time to neutrophil and platelet recovery (31). Among double unit umbilical cord blood transplants, Cutler et al. found that the presence of DSA was associated with an increased incidence of graft failure, prolonged time to neutrophil engraftment, and excess 100-day mortality or relapse (32).
Ciurea and colleagues at MD Anderson have conducted several seminal studies on the role of HLA antibodies and DSA in haploidentical HSCT. The 2009 study was the first to report a link between single antigen bead testing and primary graft failure in haploidentical HSCT patients (33). Among twenty-four consecutive transplant patients, the authors reported that three of four patients with DSA undergoing haploidentical HSCT failed to engraft, compared with one of twenty in a control cohort with no DSA. All patients with primary graft failure had one or more DSA with an MFI above 3,000. (Two of these patients were treated with TPE and rituximab, and one maintained DSA above 1,500 MFI).
A follow up study in 2015 evaluated 122 transplant recipients and found that twenty-two had DSA. Seven of eleven patients with DSA above 5,000 MFI failed to engraft (median DSA MFI 10,055), compared with none of the eleven with DSA below 5,000 MFI (median DSA MFI 2,471) (24). Five of the seven patients who experienced graft failure with DSA were also C1q positive. This study was central in establishing that DSA above threshold on single antigen bead testing carries a significant risk of graft failure. A recent study by this group evaluated the impact of desensitization of high-level DSA. The authors evaluated 37 patients who underwent desensitization for DSA versus a control cohort without DSA (n=345) (34). Patients with initial DSA >20,000 MFI and positive C1q after desensitization had lower engraftment rate, higher non-relapse mortality, and worse overall survival than controls. However, graft outcome and survival of patients with initial DSA <20,000 and those with negative C1q after desensitization were comparable with no DSA controls.
The removal of HLA antibodies in sensitized patients has been widely used for HSCT and solid organ transplantation. There are a number of modalities and protocols that are often used in various combinations. The major goals of therapies are to target B cells and plasma cells, physically remove antibodies from circulation, and to modulate the pathogenic functions of antibodies (21, 35). Here we will summarize the major therapeutic modalities and provide some context of how they are used in HSCT programs.
Depletion of circulating B cells is one major component of desensitization strategies. The chimeric anti-CD20 monoclonal antibody Rituximab is the most widely-used agent, although several other agents are in development (36, 37). Targeted depletion of B cells with agents such as Rituximab has the advantage of not only physically removing alloreactive B cells, but also has tolerogenic effects, such as resetting the peripheral B cell pool away from a pro-inflammatory profile and altering the balance of the immunoregulatory plasma cell populations in the bone marrow and tissues (36).
Plasma cells are a major source of anti-HLA IgG. The proteasome inhibitor bortezomib, originally developed to treat multiple myeloma, has gained use in transplantation because it targets plasma cells. In pre-clinical models and kidney transplant patients, bortezomib has been shown to be effective in desensitization protocols in combination with other agents (38, 39). Additional proteasome inhibitory agents, such as carfilzomib, which has a reduced toxicity profile, are in development and being explored in the setting of HSCT (40).
Therapeutic plasma exchange (TPE) uses mechanical separation of the blood components to replace plasma with colloidal fluid. TPE has a wide range of indications and is generally well-tolerated. TPE is a mainstay approach to reduce the concentration of IgG in circulation during desensitization for several decades (41). In transplantation, TPE is also used to reduce antibody levels for solid organ transplant patients who are experiencing antibody-mediated rejection (41). There is no standard number of TPE procedures for desensitization, but typically patients undergo multiple rounds of plasmapheresis based on the levels of DSA as determined by the transplant center. Antibody levels are typically monitored with serial solid phase HLA antibody testing after treatments.
In addition to TPE, transfusion-based strategies have been employed to absorb circulating anti-HLA IgG. Two approaches are to use donor platelets or buffy coat infusion prior to transplantation to provide a target for the binding and clearance of anti-HLA antibodies (34, 41, 42).
Intravenous immunoglobulin (IVIG) is a preparation of polyclonal and polyspecific immunoglobulins. While initially developed to provide passive immunity in cases of immunodeficiency, high dose IVIG has immunosuppressive properties. High dose IVIG exerts several effects on immune cells via Fc receptors that attenuate innate and adaptive immune activation (41, 43). IVIG has been paired with TPE to prevent rebound of DSA by rapidly restoring the homeostatic levels of immunoglobulins in circulation. IVIG is used both for desensitization in solid organ and HSCT, as well as for treatment of antibody-mediated rejection after solid organ transplant.
While a number of agents and strategies are used to desensitize patients prior to transplantation, these protocols and philosophies vary widely between transplant centers. There are both pre-transplant and post-transplant features that can be used to assess the efficacy of desensitization in HSCT patients (Table 2). While there are many larger studies that have reported the clinical outcomes of patients after desensitization, less information is available about the impact of treatment modalities on HLA antibodies and DSA. In addition, HLA antibody removal is frequently used in the setting of solid organ transplantation prior to transplant or for antibody-mediated rejection. Although there are caveats to extrapolating this information for HSCT patients (discussed below), there are many similarities between the two clinical scenarios. Here, we will review the available studies that have reported HLA antibody level information in the context of desensitization of both HSCT and solid organ transplant patients.
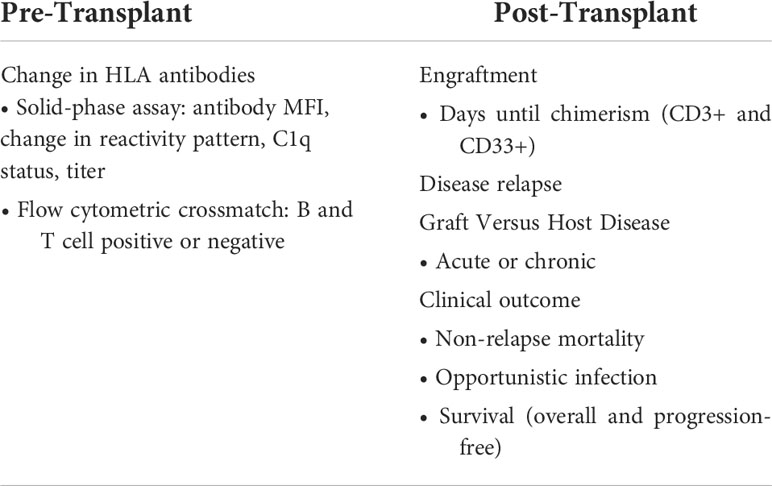
Table 2 Factors available to assess the efficacy of HLA antibody desensitization.
Leffell et al. evaluated fifteen HSCT patients with DSA who underwent desensitization (35). Based on levels of antibody corresponding to either a positive flow cytometric crossmatch (generally >10,000 MFI) or CDC crossmatch (generally >10,000 MFI at 1:8 serum dilution), patients underwent multiple rounds of desensitization with TPE, along with treatment with IVIG, tacrolimus, and mycophenolate mofetil. This cohort of patients each had from one to three DSA, with nine patients having Class I DSA, five possessing Class II DSA, and one patient having DSA against both Class I and II antigens. Three patients had DSA that were below the level of a positive flow cytometric crossmatch, eleven had DSA at a positive flow cytometric crossmatch level, and one was at a positive CDC crossmatch level. Those with DSA below flow crossmatch underwent one round of plasmapheresis, while flow crossmatch positive DSA patients received three to eleven rounds of TPE (average 5.6 TPE). After desensitization, the mean reduction for DSA was 64.4% (range 40.2-93.3%), with fifteen patients experiencing reduction in DSA levels. There was no reported association with the HLA specificity (loci or number of DSA) and the reduction in DSA. Three patients did experience a rebound in DSA level during the conditioning period. All fourteen patients who were transplanted engrafted by day 60; seven suffered relapses from 3-12 months after transplantation (29).
Bailen et al. evaluated nineteen haploidentical HSCT patients with DSA who underwent variable desensitization treatments with rituximab, IVIG, plasma exchange, incompatible platelets, and buffy coat treatments (44). Overall, twelve patients had DSA >5,000 MFI, six against Class I, 1 against Class II alone, and five against Class I and II. The mean reduction in MFI after desensitization was 74%, with a range from 20-100%. Ten of the twelve patients with pre-desensitization DSA >5,000 had DSA reduced below 5,000 MFI prior to transplant, although one patient had an increase in DSA levels prior to infusion to levels above 5,000 MFI (38).
A recent study by Ciurea et al. evaluated the impact of desensitization on thirty-seven patients at two institutions (34). Patients were treated with three sessions of plasma exchange followed by rituximab and high dose IVIG. Most patients received irradiated donor buffy coat as well. The mean DSA was 10,198 MFI, which was reduced to a mean of 5,937 after desensitization treatments. HLA antibody information was not reported by Class or loci. Patients were also evaluated for C1q positivity, which generally correlates with MFI. Fourteen of these patients had C1q positivity prior to treatment, and six became C1q negative after desensitization.
Although there are multiple differences in the patient populations undergoing HSCT versus solid organ transplantation, desensitization of HLA antibodies has been used extensively in solid organ transplant with many of the same therapeutic modalities. Here, we highlight two detailed studies that have evaluated the impact of desensitization with plasmapheresis-based approaches on HLA antibodies.
Noble et al. evaluated the impact of desensitization in two cohorts of patients undergoing living donor kidney transplantation or deceased donor kidney transplantation and provided a careful evaluation of the impact of desensitization on HLA antibody MFI reduction (45). Patients were treated with rituximab, tacrolimus, mycophenolate mofetil, and steroids, as well as plasmapheresis protocols based on the strength of DSA. Seventeen living donor candidates were treated with plasmapheresis 4-5 times per week prior to transplant, and immunoadsorption was used if DSA was greater than 12,000 MFI. This cohort had a mean Class I DSA MFI of 6,195 and 2,191 for Class II. Twenty-seven deceased donor candidates with cPRA >80% underwent desensitization with the above agents plus multiple weeks of 4-5 sessions per week. This cohort had a mean Class I DSA MFI of 13,929 and 5,508 for Class II. For these patients, the mean decrease in MFI was 88% for Class I and 59% for Class II. Factors that were found to correlate with a greater decrease in MFI were the volume of treated plasma. Thus, these results demonstrate a similar reduction in Class I and Class II DSA by these desensitization protocols.
Yamada et al. reported the impact of desensitization in sixty-four renal transplant recipients who underwent TPE for AMR (46). Patients underwent approximately six procedures every other day followed by one dose of IVIG. HLA antibody testing by single antigen bead testing was reported at two time points, time point 1 after the third TPE, and time point 2, after the sixth TPE. Overall, the authors found that most of the reduction in DSA levels occurred over the first three procedures (time point 1), with smaller and more variable reductions occurring between time point 1 and time point 2. When compared with pre-treatment levels, Class I and Class II specificities had similar reductions at each time point, 25.7% and 25.1%, respectively, after the first set of procedures, and 37.1% and 34.2% after the second set. Among Class I loci, the largest reduction after all procedures was for HLA-A (48.6%) versus HLA-B and -C (27.2% and 32.2%, respectively). Among Class II specificities, HLA-DR, DQ, and DP had similar levels of reduction (39.8%, 33.6%, and 41.6%, respectively), while HLA-DR51-53 antibodies were only reduced by 19.9%. Interestingly, the authors found that for two specificities, the impact of treatments 4-6 (time point 1 to time point 2), HLA-DR51-53 and -DQ did not decrease, while all other loci did. Overall, this study provides a very detailed reporting of the impact of TPE desensitization on HLA antibodies by loci and number of procedures.
Several case studies have reported on HSCT in the face of high-level class I DSA in multiple donor-recipient scenarios, with most DSA directed at HLA-A and B antigens (Table 3). A patient undergoing evaluation for HCT had a 9/10 matched sibling donor with an HLA-A locus mismatch (patient A*32:01, donor A*24:02). The patient was highly sensitized, with A*24:02 DSA at 18,000 MFI. Desensitization with several TPE and IVIG treatments, plus two rituximab doses resulted in a decrease to an MFI of 2,233, predictive of a negative flow crossmatch (47). This treatment was also effective in reducing third-party MFI values. Spriewald and colleagues reported on a 53 year-old female patient with a CDC-level HLA-A2 DSA at 20,000 MFI that was treated with platelet infusions in combination with rituximab and bortezomib, reducing the HLA-A2 DSA to less than 5,000 MFI. This patient engrafted by day 10 with a 9/10 matched unrelated donor and remained in complete remission over 1 year post-transplant (48).
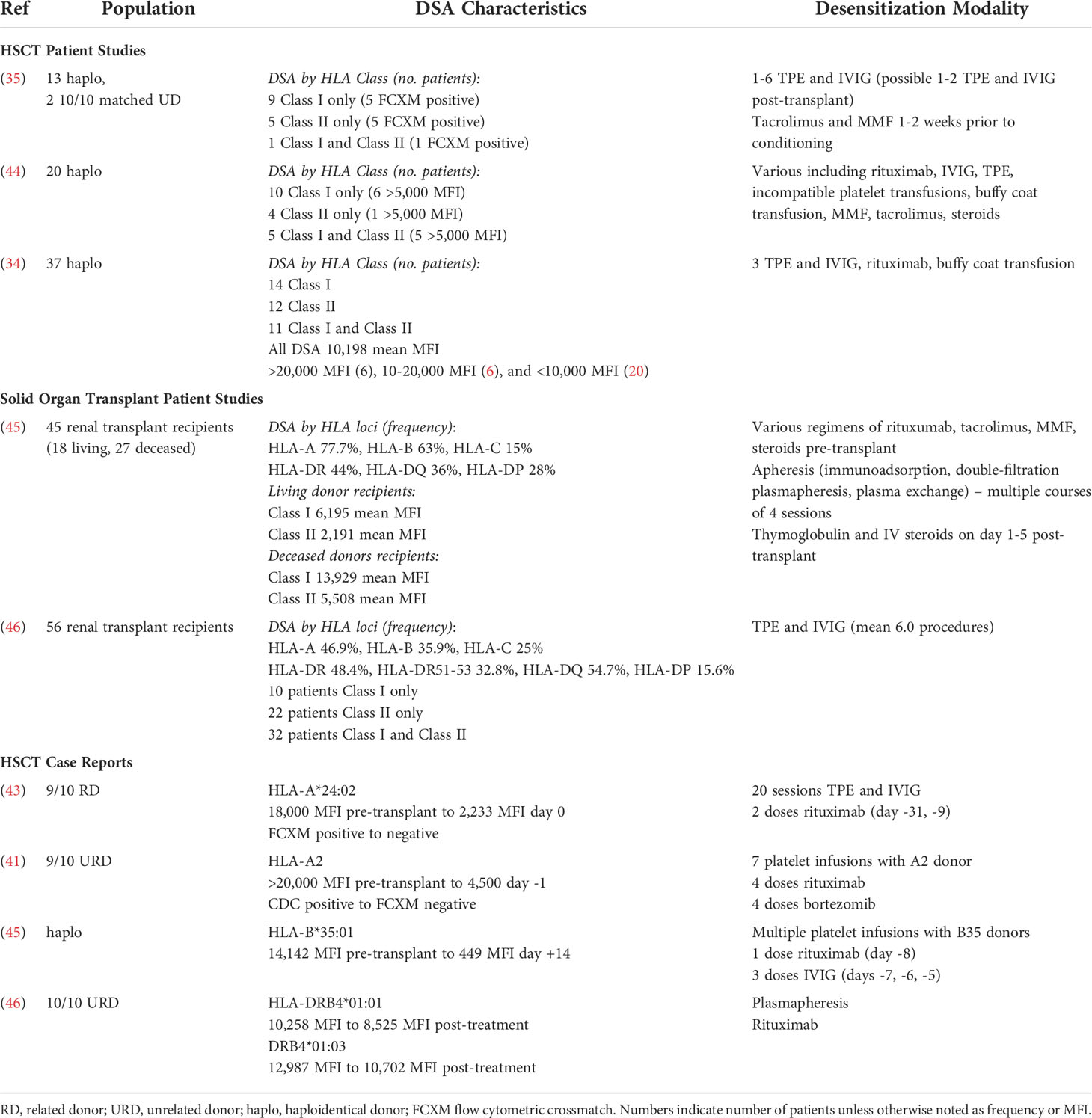
Table 3 Summary of DSA and desensitization methods used in HSCT and solid organ transplant studies.
In cases where DSA testing is completed prior to the administration of blood products and not repeated prior to transplantation, new sensitization can present challenges and lead to graft failure. Following administration of eighteen platelet transfusions, a 58-year old male patient with no DSA detected previously developed high level DSA against his haploidentical donor (A*26:02, MFI 26,978; B*48:01, MFI 5,228) that was only detected post-transplant and resulted in graft failure and the necessity of a second salvage transplant (49). A similar case reported graft failure in a 64 year-old male on day 28 due to a de novo DSA against the donor’s A*11:01 (MFI 21,564) following haploidentical HSCT from the patient’s daughter (50). The only available donor for a second transplant was the patient’s brother, where a DSA to the donor’s B*35:01 (MFI 14,142) was also present. Desensitization with rituximab, IVIG, and multiple infusions with platelets bearing the donor’s HLA-B35 were successful in reducing the DSA to <500 MFI.
While less commonly found in the literature, cases reporting Class II DSA causing graft failure have also been published. DR53 antibody (DRB4*01:01, MFI 10,258; DRB4*01:03, MFI 12,987), detected pre-transplant in a patient undergoing transplant with a 10/10 matched unrelated donor. Although the DSA was reduced with plasmapheresis and rituximab, it was resistant to treatment and present at the time of transplant (DRB4*01:01, MFI 8,525; DRB4*01:03, MFI 10,702). This patient experienced secondary graft failure twice due to the HLA-DRB4 DSA, and a new donor with a DRB4*03:01N allele was used successfully (51). DPB1 DSA leading to graft failure following HCT from a 10/10 matched unrelated donor in a 53 year-old male has also been reported (52). In this case, the DPB1 mismatch (patient DPB1*04:01, 04:01; donor DPB1*01:01, 04:01) resulted in the development of DPB1*01:01 de novo DSA (MFI 13,752) leading to a strongly positive flow crossmatch that was predicted to be CDC positive as well based on the laboratory’s cutoff. This patient required a second HCT and the DPB1 DSA had a predictable impact on the donor search.
New approaches to HSCT have expanded the role of DSA evaluation in the process of donor selection. A strong body of work has established that HLA antibodies, and DSA particularly, is a significant barrier to successful HSCT. The major factor that has been shown to correlate with outcome is the strength of HLA antibody. Despite some ambiguity due to differences between techniques and laboratories, the overall consensus is that DSA above a value of 5,000 MFI, or at levels consistent with a positive flow cytometric crossmatch, is associated with worse outcomes for HSCT patients (24, 33). Additionally, based on a physical crossmatch-based assessment of compatibility, antibody at a level that would cause a CDC crossmatch is considered to be a contraindication to successful HCT. Thus, studies and case reports of desensitization mostly focus on antibodies that are above the flow cytometric crossmatch threshold of clinical relevance.
In other areas of histocompatibility and transplantation literature, there is evolving evidence of the importance of certain HLA loci mismatches and DSA formation over others. For example, multiple HSCT studies have evaluated the relative risk of HLA mismatches on survival and graft failure and failed to uncover an impact of mismatches at specific HLA loci (5). In solid organ transplantation, HLA-DRB1 and -DQB1 mismatches are associated with worse outcomes, and the degree of HLA-DRB1 and -DQB1 molecular mismatch load is associated with the development of post-transplant DSA (53–55). For the sake of choosing between donors in an HLA sensitized HSCT patients, the existing literature does not provide specific guidance beyond the importance of DSA strength. While some case studies have reported the specificities of DSA, there is little consensus about additional clinical or HLA-based factors that portent worse outcomes in HSCT patients with DSA. For example, we did not find any discernible evidence that Class I versus Class II DSA (or DSA against a specific loci) is associated with lower rates of engraftment or graft failure.
In the case of approaches to desensitization, existing studies provide evidence that reduction of DSA is a safe approach to transplant sensitized patients. In other words, the physical strength of the antibody at the time of transplant seems to be critical to the outcome of the transplant, not the characteristics of DSA prior to desensitization. Multiple studies have reported an association between successful transplantation and reduction in DSA strength of over 50% versus a starting level, with several reporting average MFI reductions in the 70-80% (34, 35, 44). This appears to be true across multiple desensitization protocols and institutions. Thus, for programs considering the outcome of desensitization against a given donor, the literature provides evidence to expect a reduction by over half of the starting level. However, as discussed below, there is relatively limited information provided about the impact HLA loci or other characteristics of the DSA on this outcome.
For example, at our center the presence and strength of DSA is a crucial factor that is considered when selecting among haploidentical donors (13, 56) Donors against whom DSA is present at high level (CDC crossmatch positive) are not considered further, while DSA at moderate levels (generally >3,000 MFI) are considered for desensitization. Desensitization consists of tacrolimus and mycophenolate mofetil along with a course of 3-6 IVIG and plasma exchange that depends on the strength of DSA (13, 20, 56). This regimen employs a wide range of treatment modalities and has been used successfully with minor variations for several years at our center.
The current studies that evaluate the potential for desensitization have established that the presence of DSA above a moderate strength is predictive of a greater risk for graft failure. This work has provided important guidance for sensitized HSCT patients, and certainly has advanced the field for haploidentical and HLA mismatched transplants. From the perspective of DSA and histocompatibility, many of these studies have published limited HLA antibody data and overall there is little consensus on several areas related to histocompatibility. We find that the main factors that limit the strength of these findings and application to new HLA matching algorithms in HSCT:
- Variable classification of antibody strength. HLA laboratories use SAB testing from a limited number of vendors; however, there is variability in how assays are conducted, analyzed, and reported. As with most studies in histocompatibility, this makes the broad interpretation of HLA antibody levels (as defined by MFI) across different centers difficult.
- Limited reporting of HLA loci in clinical studies. The HLA system uses a complex nomenclature that makes interpretation difficult for non-HLA laboratory professionals. Many of the studies evaluated in this review provide very limited information regarding the HLA specificities and strength of DSA. This is probably due to a number of factors, but it precludes more detailed meta-analysis of the impact of HLA antibody characteristics in HSCT. Similarly, while the level of sensitization is frequently reported in studies of solid organ transplantation, most often as cPRA, this type of more global HLA antibody information is not included in HSCT studies. Again, while there is likely to be a relatively low level of HLA sensitization compared with solid organ transplantation and most studies would be underpowered to make strong conclusions, this data in aggregate could prove useful, particularly for multiparous females.
- Limited statistical power to assess impact of DSA on clinical outcomes. One inherent limitation in studying DSA in HSCT is the limited number of patients who both have DSA and experience graft failure. Even among the largest studies to date, the number of patients who experience graft failure with DSA is often less than a few dozen. Thus, no reliable conclusions can be drawn about loci-specific DSA (for example, is HLA-B DSA more associated with graft failure than DSA against other HLA loci? Is it more or less resistant to desensitization)?. As discussed above, more detailed reporting would potentially allow some idea of whether DSA directed against certain HLA loci are more problematic for engraftment or desensitization outcomes.
In future studies, it would be highly beneficial for more detailed HLA antibody information to be provided. Data in most studies evaluating desensitization is often limited to mean or median reductions in MFI among cohorts. More complete HLA antibody information might elucidate trends or patterns that are clinically useful. Examples of relevant data that could be included are: criteria for how HLA antibodies are defined at the study centers as well as more complete understanding of the sensitization status of patients, e.g. patient history, how many DSA are present, which HLA Classes, specific MFIs or MFI ranges, the presence of third-party antibody and cPRA classification.
It would also be informative to have more granular information regarding the impact of multiple low level DSA on outcomes. This would be valuable in the case of haploidentical transplantation, in which due to sensitization from pregnancy, multiparous female patients are more likely to have multiple DSA against related donors. It would be useful to know, for example, if there is a higher risk of transplanting across multiple DSA in this setting or if there is an increased risk of worse outcomes due to the relative durability of this mode of sensitization (e.g. the presence of high numbers of memory B cells). Fossey and colleagues provided some evidence that low level DSA in haploidentical transplant patients is not clinically detrimental. The authors reported on a group of five haploidentical HSCT recipients that were transplanted across borderline DSA (MFI between 1,700 and 4,200) with an overall survival of 80%, with only slightly longer neutrophil and platelet engraftment periods compared to patients with no DSA (57). It would be useful to expand upon this type of study, with reporting of the number and loci of DSA. However, there does not appear to be systematic studies of the impact of multiple low level DSA
As the use of HLA mismatched donors grows, however, more granular assessment of factors that impact desensitization for HSCT would be valuable. For example, when choosing between haploidentical donors with different DSA. In addition, when choosing HLA mismatched unrelated donors with DSA against HLA-B or HLA-DBP1, are there particular patient or HLA antibody characteristics that make desensitization more challenging? Assessment of loci-specific success of desensitization is difficult due to the range of HLA genes that precludes identification of cohorts with narrowly defined HLA antibody profiles. Demographic factors (sex, age) as well as immunologic/HLA factors (cPRA, etc.), could be considered.
In summary, the HSCT field is evolving in several key ways that make HLA mismatch and DSA an important consideration for donor selection. The existing literature has established that DSA can be a barrier to successful transplantation. In the future, the field will need to generate more specific information in order to continue to improve outcomes for patients undergoing HLA mismatched transplantation.
SMK and AJG wrote and edited the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by NIH R00 AI46271 (SMK).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Petersdorf EW, Hansen JA, Martin PJ, Woolfrey A, Malkki M, Gooley T, et al. Major-Histocompatibility-Complex class I alleles and antigens in hematopoietic-cell transplantation. New Engl J Med (2001) 345(25):1794–800. doi: 10.1056/NEJMoa011826
2. Lee SJ, Klein J, Haagenson M, Baxter-Lowe LA, Confer DL, Eapen M, et al. High-resolution donor-recipient HLA matching contributes to the success of unrelated donor marrow transplantation. Blood (2007) 110(13):4576–83. doi: 10.1182/blood-2007-06-097386
3. Granot N, Storb R. History of hematopoietic cell transplantation: challenges and progress. Haematologica (2020) 105(12):2716–29. doi: 10.3324/haematol.2019.245688
4. Kanakry CG, Fuchs EJ, Luznik L. Modern approaches to HLA-haploidentical blood or marrow transplantation. Nat Rev Clin Oncol (2016) 13(1):10–24. doi: 10.1038/nrclinonc.2015.128
5. Dehn J, Spellman S, Hurley CK, Shaw BE, Barker JN, Burns LJ, et al. Selection of unrelated donors and cord blood units for hematopoietic cell transplantation: guidelines from the NMDP/CIBMTR. Blood (2019) 134(12):924–34. doi: 10.1182/blood.2019001212
6. Pidala J, Lee SJ, Ahn KW, Spellman S, Wang HL, Aljurf M, et al. Nonpermissive HLA-DPB1 mismatch increases mortality after myeloablative unrelated allogeneic hematopoietic cell transplantation. Blood (2014) 124(16):2596–606. doi: 10.1182/blood-2014-05-576041
7. Fernández-Viña MA, Klein JP, Haagenson M, Spellman SR, Anasetti C, Noreen H, et al. Multiple mismatches at the low expression HLA loci DP, DQ, and DRB3/4/5 associate with adverse outcomes in hematopoietic stem cell transplantation. Blood (2013) 121(22):4603–10. doi: 10.1182/blood-2013-02-481945
8. Zino E. A T-cell epitope encoded by a subset of HLA-DPB1 alleles determines nonpermissive mismatches for hematologic stem cell transplantation. Blood (2003) 103(4):1417–24. doi: 10.1182/blood-2003-04-1279
9. Fleischhauer K, Shaw BE, Gooley T, Malkki M, Bardy P, Bignon JD, et al. Effect of T-cell-epitope matching at HLA-DPB1 in recipients of unrelated-donor haemopoietic-cell transplantation: a retrospective study. Lancet Oncol (2012) 13(4):366–74. doi: 10.1016/S1470-2045(12)70004-9
10. Sajulga R, Bolon YT, Maiers M, Petersdorf EW. Assessment of HLA-b genetic variation with an HLA-b leader tool and implications in clinical transplantation. Blood Advances (2021) 6(1):270–80. doi: 10.1182/bloodadvances.2021004561
11. Petersdorf EW, Carrington M, O’hUigin C, Bengtsson M, de Santis D, Dubois V, et al. Role of HLA-b exon 1 in graft-versus-host disease after unrelated haemopoietic cell transplantation: a retrospective cohort study. Lancet Haematol (2020) 7(1):e50–60. doi: 10.1016/S2352-3026(19)30208-X
12. Petersdorf EW, Stevenson P, Bengtsson M, de Santis D, Dubois V, Gooley T, et al. HLA-b leader and survivorship after HLA-mismatched unrelated donor transplantation. Blood (2020) 136(3):362–9. doi: 10.1182/blood.2020005743
13. Chang YJ, Luznik L, Fuchs EJ, Huang XJ. How do we choose the best donor for T-cell-replete, HLA-haploidentical transplantation? J Hematol Oncol (2016) 9(1):35. doi: 10.1186/s13045-016-0265-2
14. Luznik L, O’Donnell PV, Fuchs EJ. Post-transplantation cyclophosphamide for tolerance induction in HLA-haploidentical bone marrow transplantation. Semin Oncol (2012) 39(6):683–93. doi: 10.1053/j.seminoncol.2012.09.005
15. Meybodi MA, Cao W, Luznik L, Bashey A, Zhang X, Romee R, et al. HLA-haploidentical vs matched-sibling hematopoietic cell transplantation: a systematic review and meta-analysis. Blood Advances (2019) 3(17):2581–5. doi: 10.1182/bloodadvances.2019000614
16. McCurdy SR, Kasamon YL, Kanakry CG, Bolaños-Meade J, Tsai HL, Showel MM, et al. Comparable composite endpoints after HLA-matched and HLA-haploidentical transplantation with post-transplantation cyclophosphamide. Haematologica (2017) 102(2):391–400. doi: 10.3324/haematol.2016.144139
17. Passweg JR, Baldomero H, Bader P, Bonini C, Duarte RF, Dufour C, et al. Use of haploidentical stem cell transplantation continues to increase: the 2015 European society for blood and marrow transplant activity survey report. Bone Marrow Transplantation (2017) 52(6):811–7. doi: 10.1038/bmt.2017.34
18. Klein J, Sato A. The HLA system. New Engl J Med (2000) 343(10):702–9. doi: 10.1056/NEJM200009073431006
19. Spencer Mangum D, Caywood E. A clinician’s guide to HLA matching in allogeneic hematopoietic stem cell transplant. Hum Immunol (2022). doi: 10.1016/j.humimm.2022.03.002
20. Gladstone DE, Bettinotti MP. HLA donor-specific antibodies in allogeneic hematopoietic stem cell transplantation: challenges and opportunities. Hematology (2017) 2017(1):645–50. doi: 10.1182/asheducation-2017.1.645
21. File B, Huang Y, Peedin A, Gergis U. The impact of HLA donor-specific antibodies on engraftment and the evolving desensitization strategies. Bone Marrow Transplantation (2022)57:526–31. doi: 10.1038/s41409-022-01578-w
22. Locke JE, Zachary AA, Warren DS, Segev DL, Houp JA, Montgomery RA, et al. Proinflammatory events are associated with significant increases in breadth and strength of HLA-specific antibody. Am J Transplantation (2009) 9(9):2136–9. doi: 10.1111/j.1600-6143.2009.02764.x
23. McKenna R, Takemoto S, Terasaki P. Anti-HLA antibodies after solid organ transplantation. Transplantation (2000) 69(3):319–26. doi: 10.1097/00007890-200002150-00001
24. Ciurea SO, Thall PF, Milton DR, Barnes TH, Kongtim P, Carmazzi Y, et al. Complement-binding donor-specific anti-HLA antibodies and risk of primary graft failure in hematopoietic stem cell transplantation. Biol Blood Marrow Transplantation (2015) 21(8):1392–8. doi: 10.1016/j.bbmt.2015.05.001
25. Liwski RS, Gebel HM. Of cells and microparticles. Transplantation (2018) 102(1S):S1–6. doi: 10.1097/TP.0000000000001818
26. Gebel HM, Bray RA. HLA antibody detection with solid phase assays: Great expectations or expectations too great? Am J Transplantation (2014) 14(9):1964–75. doi: 10.1111/ajt.12807
27. Bettinotti MP, Zachary AA, Leffell MS. Clinically relevant interpretation of solid phase assays for HLA antibody. Curr Opin Organ Transplantation (2016) 21(4):453–8. doi: 10.1097/MOT.0000000000000326
28. Tait BD. Detection of HLA antibodies in organ transplant recipients – triumphs and challenges of the solid phase bead assay. Front Immunol (2016) 7. doi: 10.3389/fimmu.2016.00570
29. Ciurea SO, Champlin RE. Donor selection in T cell–replete haploidentical hematopoietic stem cell transplantation: Knowns, unknowns, and controversies. Biol Blood Marrow Transplantation (2013) 19(2):180–4. doi: 10.1016/j.bbmt.2012.08.007
30. Spellman S, Bray R, Rosen-Bronson S, Haagenson M, Klein J, Flesch S, et al. The detection of donor-directed, HLA-specific alloantibodies in recipients of unrelated hematopoietic cell transplantation is predictive of graft failure. Blood (2010) 115(13):2704–8. doi: 10.1182/blood-2009-09-244525
31. Takanashi M, Atsuta Y, Fujiwara K, Kodo H, Kai S, Sato H, et al. The impact of anti-HLA antibodies on unrelated cord blood transplantations. Blood (2010) 116(15):2839–46. doi: 10.1182/blood-2009-10-249219
32. Cutler C, Kim HT, Sun L, Sese D, Glotzbecker B, Armand P, et al. Donor-specific anti-HLA antibodies predict outcome in double umbilical cord blood transplantation. Blood (2011) 118(25):6691–7. doi: 10.1182/blood-2011-05-355263
33. Ciurea SO, de Lima M, Cano P, Korbling M, Giralt S, Shpall EJ, et al. High risk of graft failure in patients with anti-HLA antibodies undergoing haploidentical stem-cell transplantation. Transplantation (2009) 88(8):1019–24. doi: 10.1097/TP.0b013e3181b9d710
34. Ciurea SO, Al Malki MM, Kongtim P, Zou J, Aung FM, Rondon G, et al. Treatment of allosensitized patients receiving allogeneic transplantation. Blood Advances (2021) 5(20):4031–43. doi: 10.1182/bloodadvances.2021004862
35. Leffell MS, Jones RJ, Gladstone DE. Donor HLA-specific abs: to BMT or not to BMT? Bone Marrow Transplantation (2015) 50(6):751–8. doi: 10.1038/bmt.2014.331
36. Lee DSW, Rojas OL, Gommerman JL. B cell depletion therapies in autoimmune disease: advances and mechanistic insights. Nat Rev Drug Discovery (2021) 20(3):179–99. doi: 10.1038/s41573-020-00092-2
37. Schinstock C, Tambur A, Stegall M. Current approaches to desensitization in solid organ transplantation. Front Immunol (2021), 12:686271. doi: 10.3389/fimmu.2021.686271
38. Ezekian B, Schroder PM, Mulvihill MS, Barbas A, Collins B, Freischlag K, et al. Pretransplant desensitization with costimulation blockade and proteasome inhibitor reduces DSA and delays antibody-mediated rejection in highly sensitized nonhuman primate kidney transplant recipients. J Am Soc Nephrol (2019) 30(12):2399–411. doi: 10.1681/ASN.2019030304
39. Woodle ES, Shields AR, Ejaz NS, Sadaka B, Girnita A, Walsh RC, et al. Prospective iterative trial of proteasome inhibitor-based desensitization. Am J Transplantation (2015) 15(1):101–18. doi: 10.1111/ajt.13050
40. Tremblay S, Driscoll JJ, Rike-Shields A, Hildeman DA, Alloway RR, Girnita AL, et al. A prospective, iterative, adaptive trial of carfilzomib-based desensitization. Am J Transplantation (2020) 20(2):411–21. doi: 10.1111/ajt.15613
41. Choi AY, Manook M, Olaso D, Ezekian B, Park J, Freischlag K, et al. Emerging new approaches in desensitization: Targeted therapies for HLA sensitization. Front Immunol (2021) 12. doi: 10.3389/fimmu.2021.694763
42. Yamashita T, Ikegame K, Kojima H, Tanaka H, Kaida K, Inoue T, et al. Effective desensitization of donor-specific HLA antibodies using platelet transfusion bearing targeted HLA in a case of HLA-mismatched allogeneic stem cell transplantation. Bone Marrow Transplantation (2017) 52(5):794–6. doi: 10.1038/bmt.2017.10
43. Durandy A, Kaveri SV, Kuijpers TW, Basta M, Miescher S, Ravetch JV, et al. Intravenous immunoglobulins – understanding properties and mechanisms. Clin Exp Immunol (2009) 158(Supplement_1):2–13. doi: 10.1111/j.1365-2249.2009.04022.x
44. Bailén R, Vicario JL, Solán L, Sánchez-Vadillo I, Herrera P, Calbacho M, et al. Management of donor-specific antibodies in haploidentical transplant: Multicenter experience from the Madrid group of hematopoietic transplant. Front Immunol (2021) 12. doi: 10.3389/fimmu.2021.674658
45. Noble J, Metzger A, Naciri Bennani H, Daligault M, Masson D, Terrec F, et al. Apheresis efficacy and tolerance in the setting of HLA-incompatible kidney transplantation. J Clin Med (2021) 10(6):1316. doi: 10.3390/jcm10061316
46. Yamada C, Ramon DS, Cascalho M, Sung RS, Leichtman AB, Samaniego M, et al. Efficacy of plasmapheresis on donor-specific antibody reduction by HLA specificity in post-kidney transplant recipients. Transfusion (Paris) (2015) 55(4):727–35. doi: 10.1111/trf.12923
47. Misra MK, Xin JJ, Brown NK, Weidner JG, Upchurch RL, Bishop MR, et al. Effective desensitization for a strong donor-specific HLA antibody in a case of HLA-mismatched allogeneic hematopoietic cell transplantation. HLA (2019) 94(3):307–11. doi: 10.1111/tan.13627
48. Spriewald BM, Bach C, Zingsem J, Strobel J, Winkler J, Mackensen A, et al. Depletion of donor-specific anti-HLA A2 alloantibodies in a hematopoietic cell transplant recipient using directed mismatched platelet transfusions. Bone Marrow Transplantation (2018) 53(6):791–4. doi: 10.1038/s41409-018-0220-7
49. Pelobello de Leon M, Takahashi S, Onozawa M, Ito M, Nakano M, Senjo H, et al. Salvage transplantation with cord blood for graft rejection of peripheral blood stem cells due to donor specific antibody. Blood Cell Ther (2020) 3(3):74–7. doi: 10.31547/bct-2020-004
50. Minami M, Matsushima T, Mori Y, Ishihara D, Jinnnouchi F, Takenaka K, et al. Successful rescue transplantation with desensitization procedure after primary graft failure due to donor-specific antibody. Bone Marrow Transplantation (2019) 54(8):1374–6. doi: 10.1038/s41409-019-0486-4
51. Blennerhassett R, Moses JH, Coulits N, Horne A, Simpson J, Marshall J, et al. Recurrent secondary graft failure likely due to a DRB4 donor-specific antibody in a patient with aplastic anemia and DRB4 null allele. Bone Marrow Transplantation (2021) 56(10):2603–5. doi: 10.1038/s41409-021-01402-x
52. Hefazi M, Hogan WJ, Wakefield LL, Gandhi MJ. The association of de novo anti-HLA-DPB1 donor-specific antibody formation and primary graft failure after allogeneic hematopoietic cell transplantation. Hum Immunol (2018) 79(12):861–4. doi: 10.1016/j.humimm.2018.08.009
53. Wiebe C, Pochinco D, Blydt-Hansen TD, Ho J, Birk PE, Karpinski M, et al. Class II HLA epitope matching-a strategy to minimize De novo donor-specific antibody development and improve outcomes. Am J Transplantation (2013) 13(12):3114–22. doi: 10.1111/ajt.12478
54. Wiebe C, Rush DN, Nevins TE, Birk PE, Blydt-Hansen T, Gibson IW, et al. Class II eplet mismatch modulates tacrolimus trough levels required to prevent donor-specific antibody development. J Am Soc Nephrol (2017) 28:3353–62. doi: 10.1681/ASN.2017030287
55. Wiebe C, Nickerson PW. Human leukocyte antigen molecular mismatch to risk stratify kidney transplant recipients. Curr Opin Organ Transplantation (2020) 25(1):8–14. doi: 10.1097/MOT.0000000000000714
56. McCurdy SR, Luznik L. How we perform haploidentical stem cell transplantation with posttransplant cyclophosphamide. Blood (2019) 134(21):1802–10. doi: 10.1182/blood.2019001323
Keywords: hematopoietic (stem) cell transplantation, HLA, donor-specific alloantibody, desensitization, haploidentical stem cell transplant
Citation: Krummey SM and Gareau AJ (2022) Donor specific HLA antibody in hematopoietic stem cell transplantation: Implications for donor selection. Front. Immunol. 13:916200. doi: 10.3389/fimmu.2022.916200
Received: 08 April 2022; Accepted: 13 July 2022;
Published: 05 August 2022.
Edited by:
Brent Logan, Medical College of Wisconsin, United StatesReviewed by:
Saurabh Chhabra, Medical College of Wisconsin, United StatesCopyright © 2022 Krummey and Gareau. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Scott M. Krummey, c2tydW1tZTFAamhtaS5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.