
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 28 July 2022
Sec. Autoimmune and Autoinflammatory Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.915578
 Rosa Romero-Jimenez1,2
Rosa Romero-Jimenez1,2 Vicente Escudero-Vilaplana1,2*Esther Chamorro-de-Vega1,2Arantza Ais-Larisgoitia1,2Elena Lobato-Matilla1,2Beatriz Somoza-Fernández1,2Paula Ruiz-Briones1,2Carlos González2,3Ofelia Baniandrés2,4Luis Menchén2,5Carmen Lobo-Rodríguez2,6Ana Herranz1,2María Sanjurjo1,2
Vicente Escudero-Vilaplana1,2*Esther Chamorro-de-Vega1,2Arantza Ais-Larisgoitia1,2Elena Lobato-Matilla1,2Beatriz Somoza-Fernández1,2Paula Ruiz-Briones1,2Carlos González2,3Ofelia Baniandrés2,4Luis Menchén2,5Carmen Lobo-Rodríguez2,6Ana Herranz1,2María Sanjurjo1,2Background: Pharmacotherapeutic management of immune-mediated inflammatory diseases (IMID) has become more complex due to the development of new treatments, such as biological therapies. Mobile health, especially apps, can provide IMID patients with greater autonomy and facilitate communication with healthcare professionals. Our objective was to design and implement an app for remote monitoring and communication with IMID patients.
Methods: A multidisciplinary group was created to design and develop an app for IMID patients in a tertiary hospital. The app functionalities were identified through a focus group with IMID patients and through an observational, descriptive study of available apps for IMID patients at App Store and Play Store platforms. Once the app was designed and developed, we offered the app to IMID patients who initiated a new biological therapy. The inclusion period was from December 2020 to August 2021. We performed an observational, longitudinal study to assess the app’s impact on medication safety, communication, satisfaction, and usability.
Results: We designed an app (eMidCare®) with the following modules: My Medication, My Questionnaires, Adverse Events, Useful Information, Messages, and Patient Profile. A total of 85 patients were installed with the app. The median (range) follow-up time for app use was 123 (5-270) days. In the My Medication module, 100% of patients registered their biological therapy and 25.9% also used this module to record each dose of medication administered. A total of 82 adverse events (AEs) were registered. Thirty-two percent of the patients registered at least 1 AE. The most frequent AEs were fatigue, injection site reaction, headache, and nausea. Fifty-two percent of patients used the Messages module to communicate with healthcare professionals. The most frequent messages concerned doubts about managing AEs (26.2%) and drug interactions (18.9%). The satisfaction survey yielded a median (range) score of 9.1 (7-10) out of 10.
Conclusions: We developed an app, eMidCare®, which reminds patients to take their medication, enables them to record AEs, and helps them communicate with healthcare professionals. Approximately one-third of the patients registered the administration of the biological therapies and registered at least 1 AE. The most used and most satisfactory functionality was communication with health professionals.
The management of several immune-mediated inflammatory diseases (IMID) has changed dramatically owing to the development of biological therapies (1). These drugs resolve inflammatory processes quickly and effectively, thus improving prognosis. However, biological therapies continue to be associated with drug-related problems, such as adverse events and poor adherence (2). Furthermore, pharmacotherapeutic management of IMID has become more complex, and patients are now responsible for the correct administration of their treatment (3).
The quality of life of IMID patients is often affected by physical and psychological burdens (4–6). Therefore, it is essential to assess patient-reported outcomes (PROs) to complete clinical records and guarantee adequate care (4). Patient involvement is a crucial element in national health systems because of its impact on health outcomes and costs. Healthcare professionals should encourage the empowerment of IMID patients.
Information and communications technology, specifically mobile health (mHealth), can provide IMID patients with greater autonomy, facilitate communication with healthcare professionals, and increase the quality of patient care (7). Remote patient monitoring could lead to early identification of adverse events, early intervention for patients requiring their treatment to be adjusted, and reduced emergency room visits (7). IMID patients are younger than patients with other chronic diseases and, therefore, more familiar with these technologies (1). In addition, they are very eager to use mHealth to better understand their diseases (8). Apps represent an excellent opportunity to improve self-management of care and enable healthcare professionals to improve monitoring and patient care.
Our objective was to design and implement an app for self-management of disease and thus promote home monitoring and communication with IMID patients. We also assessed the usability of and satisfaction with the app.
A multidisciplinary working group comprising pharmacists, dermatologists, rheumatologists, gastroenterologists, and nurses was created to design and develop an app for IMID patients in a tertiary hospital. The functionalities of the app were based on the following: patients’ healthcare needs and their interest in the use of apps to manage their disease; and functionalities and uncertainties of currently available IMID apps.
1) Patients’ healthcare needs and their interest in the use of apps to manage their disease
We used the focus group methodology with IMID patients. A meeting was organized with 7 patients (2 diagnosed with psoriasis, 2 with psoriatic arthritis, and 3 with ankylosing spondylitis). The median age was 47.7 (SD= 10.3) years, and all patients were receiving biological therapy.
2) Functionalities and uncertainties characteristic of currently available IMID apps
We conducted a descriptive study of all apps for IMID patients to identify areas that could be improved with our new app. We searched the App Store (iOS) and Play Store (Android). The search terms used were “ankylosing spondylitis”, “Crohn’s disease”, “hidradenitis suppurativa”, “IBD”, “inflammatory bowel disease”, “immune-mediated inflammatory diseases”, “immune-mediated inflammatory disorders”, “juvenile idiopathic arthritis”, “psoriasis”, “psoriatic arthritis”, “rheumatoid arthritis”, and “ulcerative colitis”. The variables analyzed were app name, type of IMID, platform (Android or iOS), country of origin, language, category of the app, functionalities, date of the last update, downloads, and author affiliation.
The app was designed and developed considering the points mentioned above. In December 2020, we started offering the app to all IMID patients who initiated a new biological therapy. We performed an observational, longitudinal study of patients diagnosed with an IMID and followed using the app eMidCare to assess the tool’s impact on medication safety, communication, satisfaction, and usability. The inclusion period was from December 2020 to August 2021. The inclusion criteria were age ≥ 18 years, diagnosis of an IMID (ankylosing spondylitis, hidradenitis suppurativa, inflammatory bowel disease, juvenile idiopathic arthritis, psoriatic arthritis, psoriasis, and rheumatoid arthritis), and ownership of a Smartphone. Patients with language barriers were excluded. The study was approved by the Hospital Clinical Research Ethics Committee (code MSS-APP-2019). All patients signed an informed consent document.
Patients were offered the app by the pharmacist in the outpatient pharmaceutical care clinic. If the patient agreed to participate, the pharmacist registered the patient on the Content Management System (CMS) website, along with the delivery of the biological therapy and the usual information provided in the pharmaceutical care clinic. Once the patient downloaded the app, the pharmacist explained how to use it. Healthcare professionals then followed the patients up through the CMS. Health professionals can modify the contents of the app through the CMS (for example, they can add new PROs, change the recommendations for adverse events, or modify useful information when necessary).
Medication safety was evaluated through a descriptive analysis of the patient’s recording of adverse events (AE) using the app, the percentage of patients who registered an AE, type of AE, time of onset, and severity according to CTCAE (9).
Communication was evaluated through the messages sent through the app, the percentage of patients who used this module, whole messages, messages per patient, and type of messages.
Usability was evaluated using Google Analytics for Firebase®.
Satisfaction with the app was assessed through a specific survey on the app. The survey included items on usability, ease of communication with healthcare professionals, utility for the management of treatment, and grade of recommendation (Supplemental Material). The survey was delivered between 1 and 2 months after the app was installed.
1) Patients’ healthcare needs and their interest in the use of apps to manage their disease
The patients in the focus group highlighted the following issues:
General healthcare needs:
● Lack of information on diseases, lifestyles, and treatments
● Lack of knowledge on the part of healthcare professionals (e.g., general practitioners and surgeons) with respect to the disease and treatments
● Limited mobility owing to the consequences of the diseases
● Reduced possibility of communication with the medical specialist (only from Monday to Friday from 9 am to 2 pm)
● Considerable interest in using information and communication technologies, especially apps, to search for information about health
Desired health app functionalities:
● General information about the disease and treatments: symptoms, compatible medication, adverse effects, feeding, surgery, physical activity, vaccines, drug conservation, travel
● Specific information about AE management (e.g., when to go to the emergency room)
● Medication alarms
● Ability to register the injection site in the case of subcutaneous medication
● Diary to record AEs and symptoms
● Ability to take photographs of the skin and send them to specialists
● Questionnaires to assess and monitor physical and emotional states (patient-reported outcomes [PROs])
● Direct contact with health professionals to clarify doubts
Key elements of app design: Patients need information about their disease and treatments and must be able to communicate with healthcare professionals. They highlight different functionalities of the apps that will help them to manage their disease and should be incorporated in our app.
2) Functionalities and uncertainties characteristic of currently available IMID apps
We analyzed 243 apps (37.0% on Android, 27.2% on iOS, and 35.8% on both platforms). The main functionalities were as follows: general information about lifestyles, nutrition, and exercise (135/243, 55.6%), specific information about the disease or treatment (102/243, 42.0%) (although only 6 apps offered information specifically about biological therapies), recording adverse events (51/243, apps 21.0%), agenda/calendar (44/243, 18.1%), medication reminder (41/243, 16.9%), and recording of patient-reported outcomes (41/243, 16.9%). Healthcare professionals were involved in the development of 100 apps (41.1%). Only 110/243 apps (44.5%) had been updated in the previous year. The mean time between the date of the analysis and the date of the last update was 18.5 months (SD= 19.3).
Key points of app design: Functionalities and reliability were very heterogeneous. While most apps offer information, although information on biologic therapies is very scarce. Few apps allow patient interaction, such as recording AEs, setting alarms for medication, or recording PROs. Our app should have these functionalities under the supervision of healthcare professionals as a guarantee of reliability.
The content of the app was defined based on the above key points and the experience of the multidisciplinary group. The computer company Enredart®, which specializes in developing and implementing health apps, was contracted for development. A document was drawn up with the design and functional scope of the app, the support service, and the implementation plan. We decided to call the app eMidCare. The app was structured into 6 modules:
1) My Medication: This module enables the patient to record the medicines he/she is taking (biological therapies and concomitant medicines), with details of the type of intake, dose, unit of measurement, frequency, and quantity. An icon for biological therapies makes it possible to obtain more detailed information about each drug. The medicines can be included in the app by patients or by healthcare professionals. Patients can receive reminders when they have to administer the medicines. They can also record when they administer each medication to monitor adherence (e.g. at the time of administration, 10 minutes before, half an hour before…). In the case of subcutaneous biological therapies, the patients may also register the injection site.
2) My Questionnaires: Healthcare professionals can upload PRO measures (PROMs) in the app and define the frequency and the PROMs for each IMID (Table 1). The PROMs (questionnaires) are programmed to be sent to the patients at the start of treatment, after 3 months, and then every 6 months, except for the Morisky-Green test, which is sent every 3 months. However, this frequency can be modified in the web interface (CMS). The healthcare professionals can add new questionnaires, modify existing ones, and change the sending frequency. Patients receive a reminder when a new questionnaire is available.
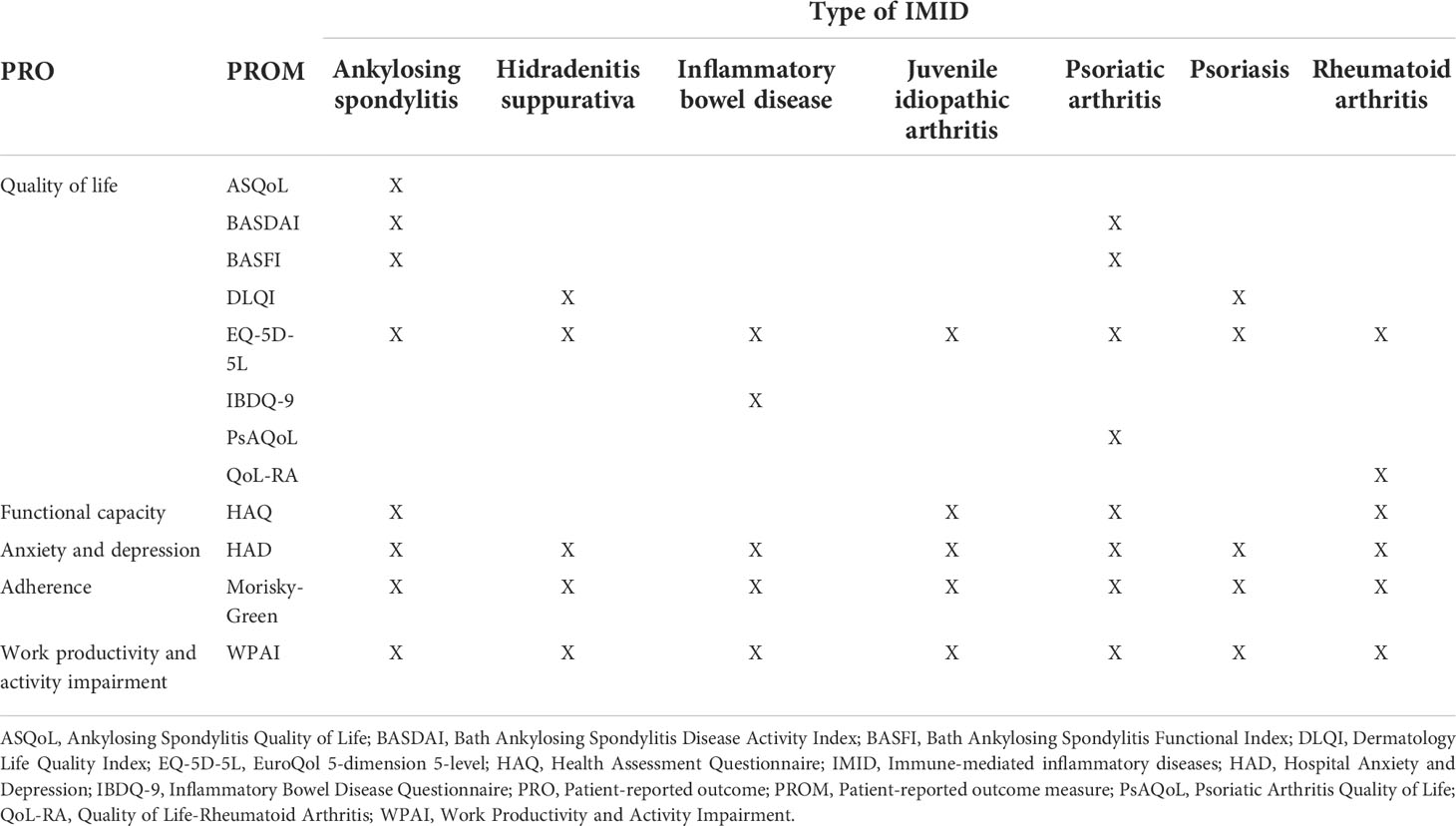
Table 1 Patient-reported outcomes assessed by the app.
3) Adverse Events: Patients can register the adverse events they experience, and the app offers various recommendations on the type of AE and its severity. The system acts based on a defined decision tree (Supplemental material), which guides the patient through a series of questions and classifies the severity of the AE (grades 1-4) (9). Then, depending on the severity, the app gives automatic recommendations on appropriate management. For example, when severity is low (grade 1), the app displays a brochure with information on the prevention and management of each AE. The decision tree is implemented in the CMS. The healthcare professionals can add new AEs to the decision tree or change the questions and recommendations provided by the app thanks to this tree.
The multidisciplinary group defined this decision tree for the most frequent AEs: diarrhea, fatigue, fever, headache, nausea, injection site reaction, vomiting, and other (recorded as free text).
4) Useful Information: This module contains recommendations and preventive information on various areas of treatment (especially on biological therapies) and IMIDs. The information is structured as Frequently Asked Questions, Adverse Events, General Information (recommendations on nutrition, conservation and stability of drugs, travel recommendations, and information about the hospital), web links of interest, and a tutorial about the app. All the information was adapted to a language that patients can understand and is periodically updated.
5) Messages: This module allows bidirectional communication between patients and healthcare professionals in real time.
6) Patient Profile: This module contains information about the patient: sex, date of birth, weight, smoking habits, type of IMID, date of diagnosis, and secondary IMID and date of diagnosis (if applicable). The Patient profile module contains a section entitled “My achievements”, where patients can obtain “trophies” and “medals” depending on their adherence and the registration of the questionnaires.
Figure 1 shows different eMidCare app screens.
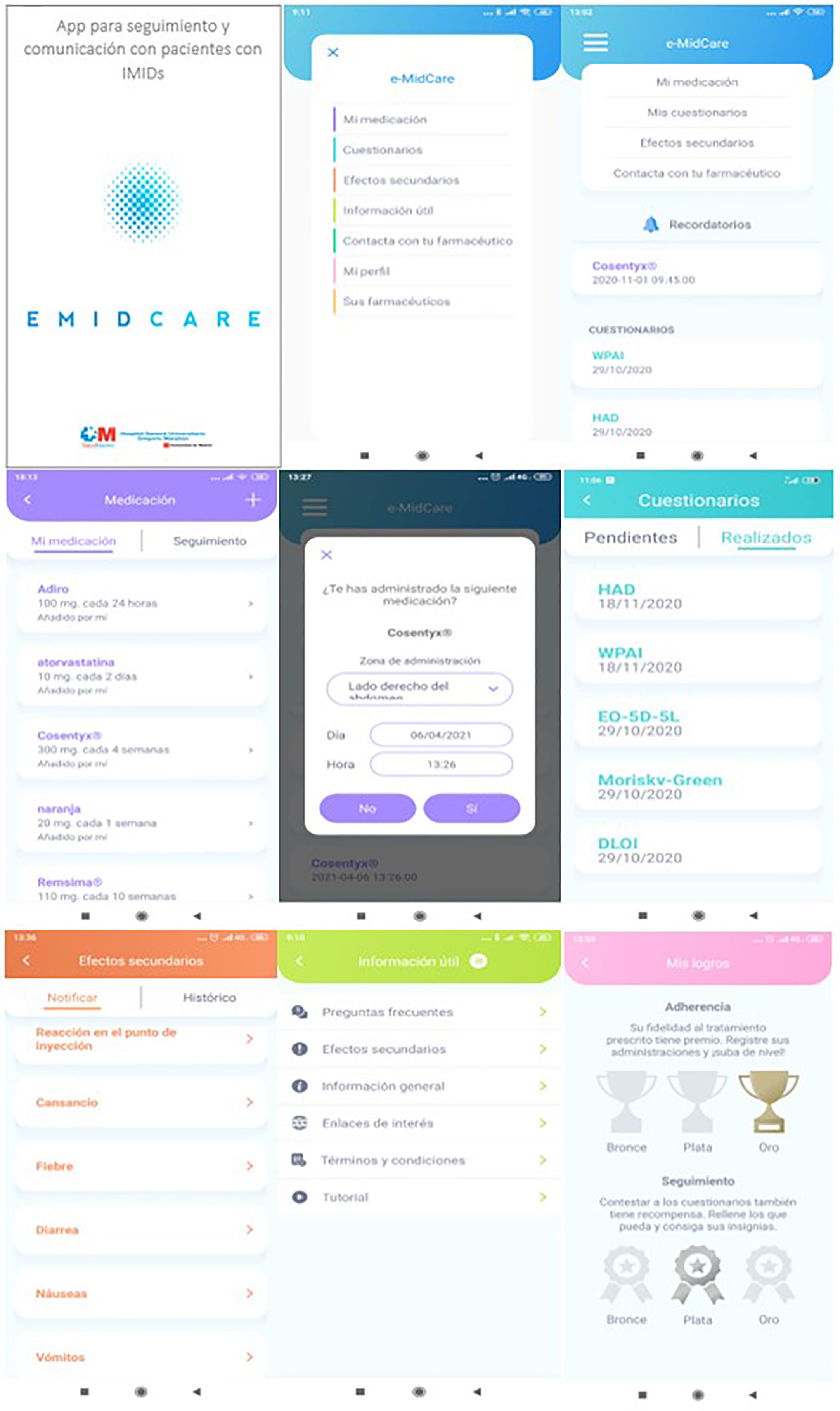
Figure 1 Functional diagram of eMidCare® app screens.
All the data registered in the app are recorded automatically in the web interface (CMS), which enables the healthcare professional to monitor patients in real time. The app also sends an automatic email to healthcare professionals when patients add a new medication, register an AE, or send a message. All the registered information can be exported to Excel® for analysis.
All the data contained in the eMidCare platform is considered confidential and has the highest level of protection according to General Data Protection Regulation (GDPR).
The app does not store data locally, so it is not possible to access it once the user is deactivated from the program. The data travels from the CMS on the server to the app through encrypted webservices. The platform is located in a hosting network at the company Gigas. The backup solution of the hosted data through advanced backup is implemented in virtual appliances R1Soft.
Other characteristics concerning privacy and security are as follows:
-The CMS and webservices will be under the Secure Sockets Layer (SSL) certificate.
-Email and password of the user will be encrypted
-The security password level is displayed to the user with a bar based on 3 factors: uppercase, lowercase, and numbers. The eMidCare prototypes for iOS and Android and the CMS were tested by end-users in a staging environment (alpha testing) and then in a production environment (beta testing). After 5 preliminary versions, the definitive version of the app was finally uploaded to the market in December 2020.
The app eMidCare was offered to 97 patients during the inclusion period, although 85 patients finally installed the app and were analyzed (Figure 2). A total of 53/85 patients (62.4%) were female. The median age (range) was 48.3 (18.1-79.4) years, and the median (range) weight was 70 (40-132) kg. Table 2 describes the type of immune-mediated inflammatory diseases and the biological therapies used.
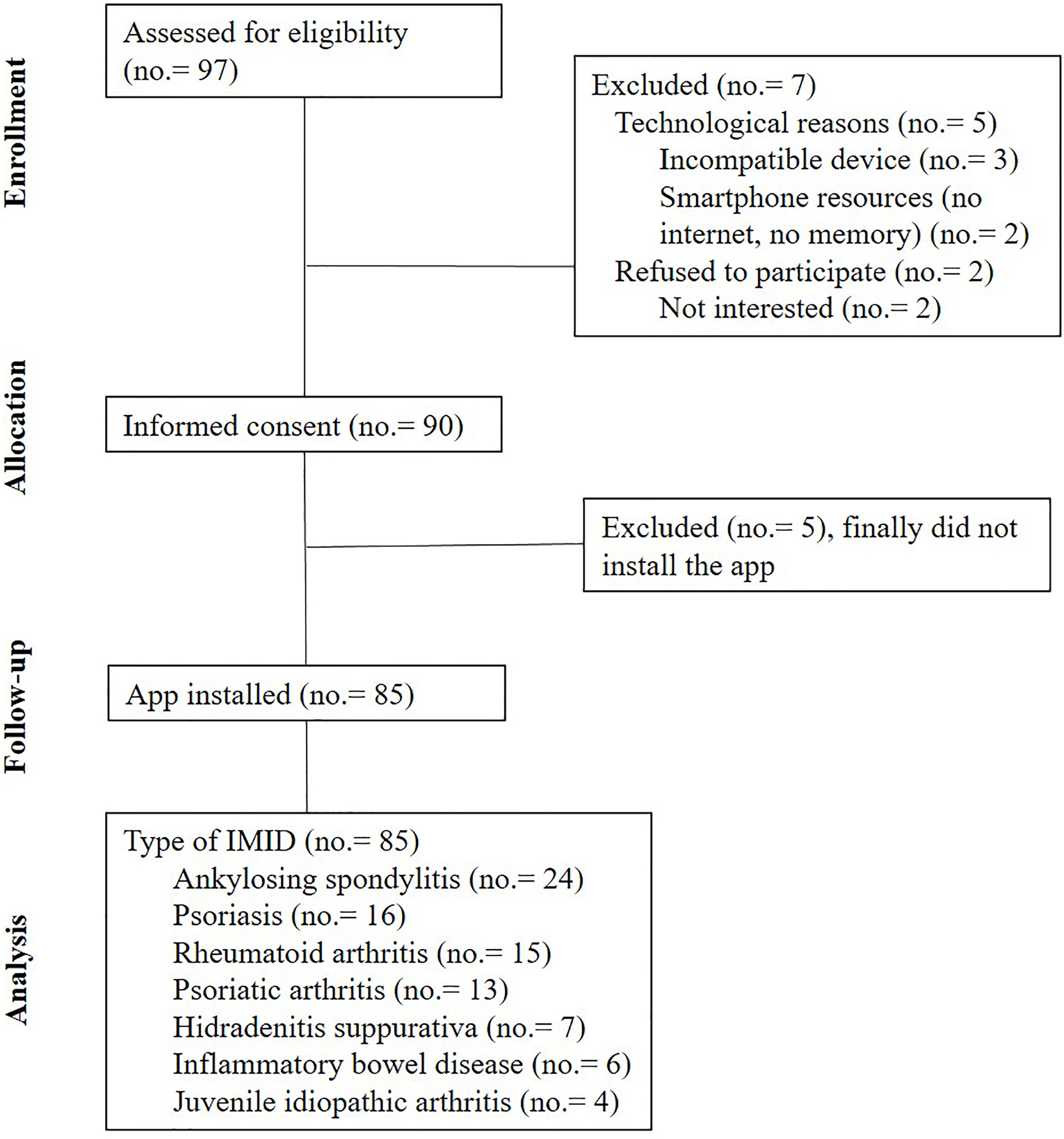
Figure 2 Patient inclusion diagram.
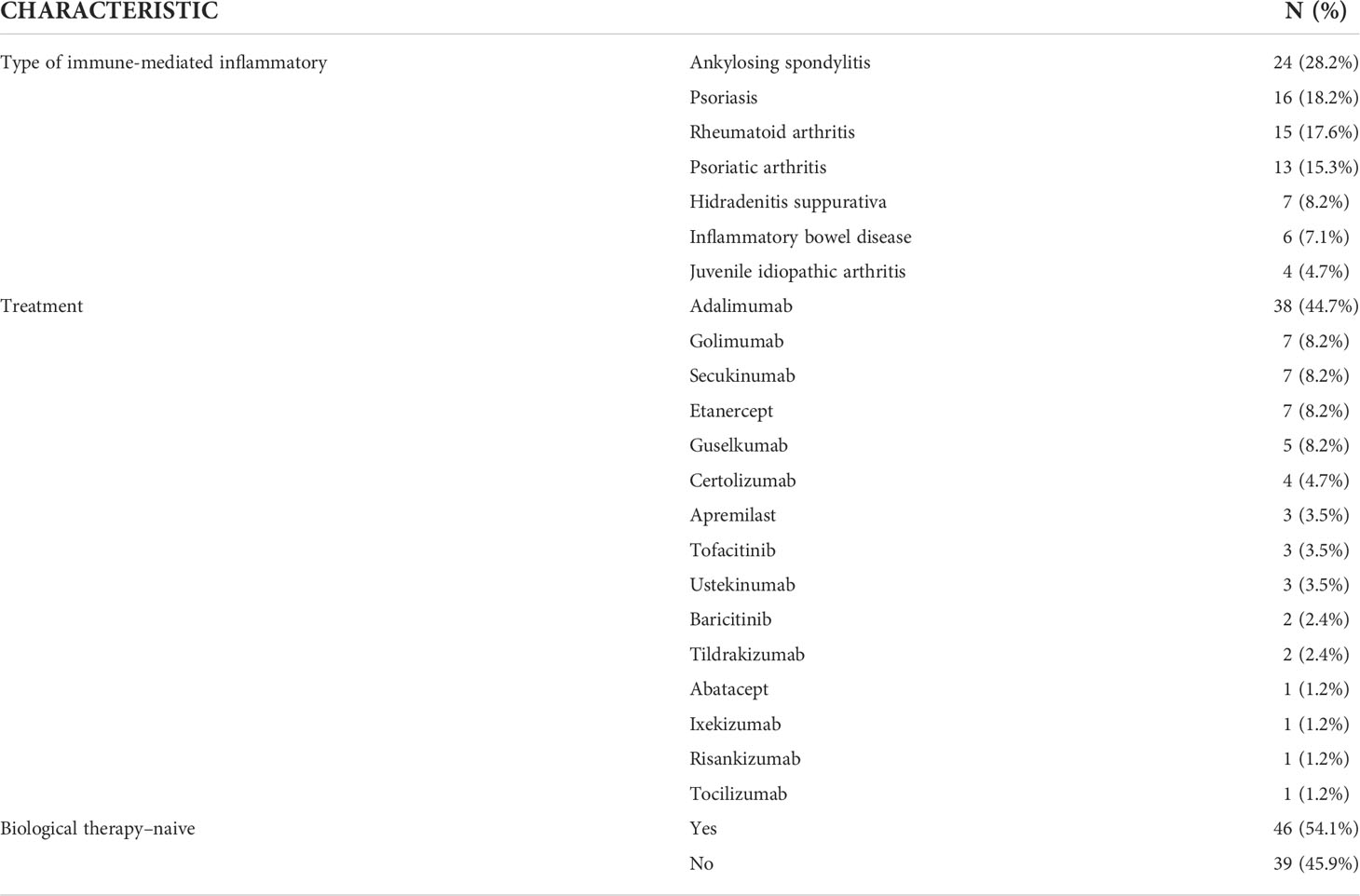
Table 2 Type of immune-mediated inflammatory diseases and biological therapy used.
In the My Medication module, all patients (85/85) registered their biological therapy (name, start date of treatment, dose, and administration frequency). Twenty-two (25.9%) also used this module to record each dose of medication administered. The median (range) adherence was 100% (50-100); adherence was >90% in 86.4% (19/22).
A total of 82 AEs were registered, and 31.8% (27/85) of patients registered at least 1 AE. The median (range) number of AEs per patient was 1 (1-17). The frequency and severity of AEs were as follows: fatigue, 26.8% (22/82; 9.1% [2/22] grade 1, 77.3% [17/22] grade 2, and 13.6% [3/22] grade 3); injection site reaction, 25.6% (21/82; 81.0% [17/21] grade 1 and 19.0% [4/21] grade 2); headache, 15.9% (13/82; 38.5% [5/13] grade 1, 38.5% [5/13] grade 2, and 23.1% [3/13] grade 3); nausea, 8.5% (7/82; 42.9% [3/7] grade 1, 42.9% [3/7] grade 2, and 14.3% [1/7] grade 3); diarrhea, 4.9% (4/82; 100% [4/4] grade 1); upper respiratory infection, 3.7% (3/82; 100% [3/3] grade 1); and other AEs, 14.6% (12/82; 75.0% [9/12] grade 1 and 25.0% [3/12] grade 2). There were no statistically significant differences in the recording of AEs between biological-naïve patients and biological-experienced patients (34.7% vs. 28.2%, respectively, p>.05). The median (range) time to the first AE was 16 (0-95) days.
Fifty-two percent of patients used the Messages module to communicate with healthcare professionals during the follow-up period. A total of 321 messages were sent (164 from patients and 157 from healthcare professionals). The most frequent messages concerned doubts about managing AEs and drug interactions (Table 3). A total of 56/164 (33.5%) messages were sent outside working hours.
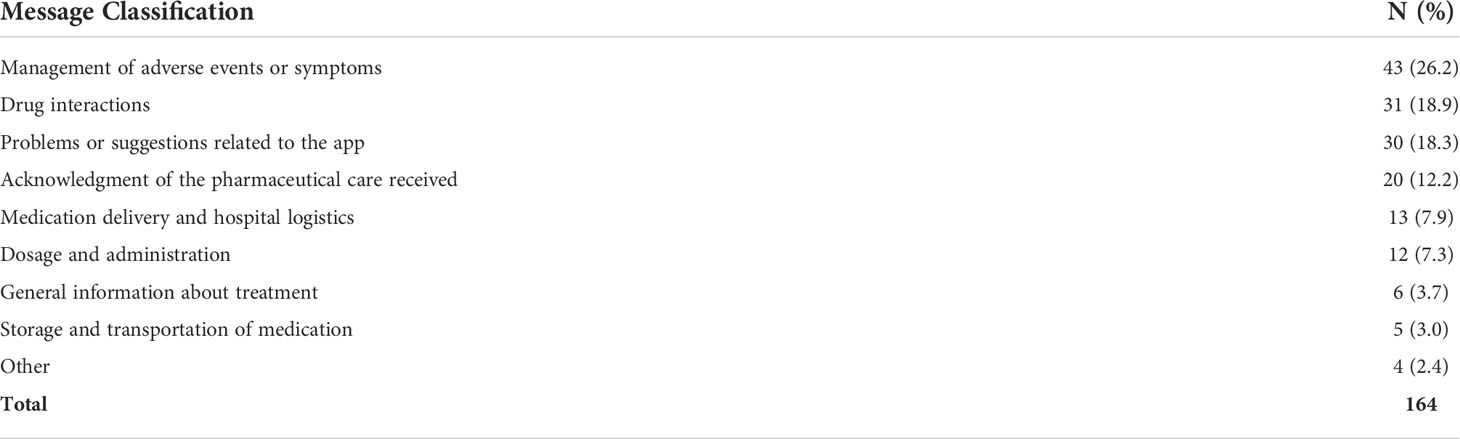
Table 3 Type of message sent by patients through eMidCare®.
The satisfaction survey yielded a median (range) score of 9.1 (7-10) out of 10. Figure 3 describes the score for the various functionalities.
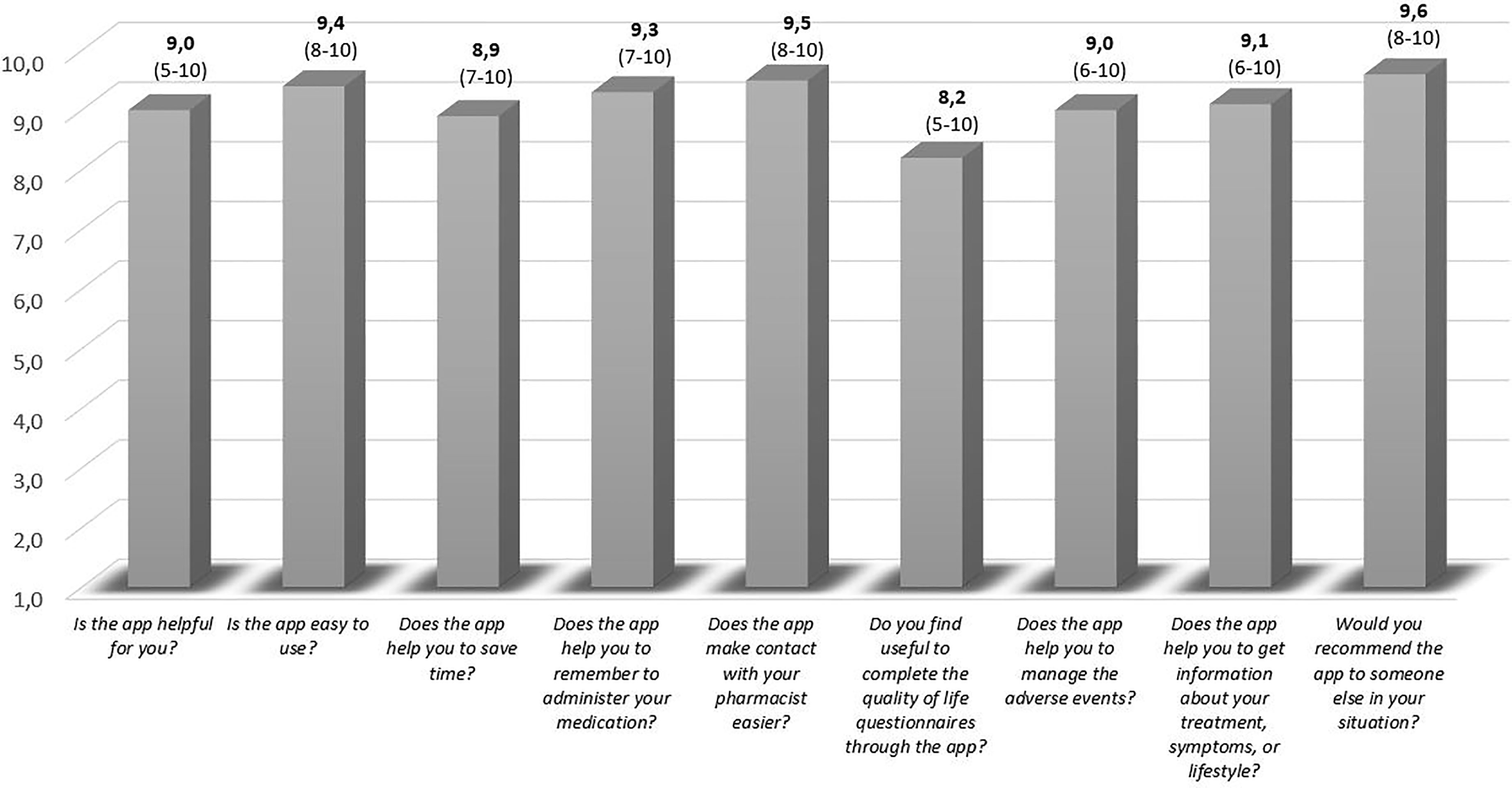
Figure 3 Patient satisfaction with eMidCare®. The score is expressed as the median (range).
The median (range) follow-up time for app use was 123 (5-270) days. The app sections that patients browsed for the longest time were Messages (21.9%), Start screen (20.9%), My questionnaires (20.4%), My medication (8.8%), Adverse events (7.1%), and reminders (5.7%). The median time per patient in each session with the app was 3.7 minutes.
The patients interacted an average of 1.4 times with the app each week. Table 4 shows the app retention rate during the follow-up period (Table 4).
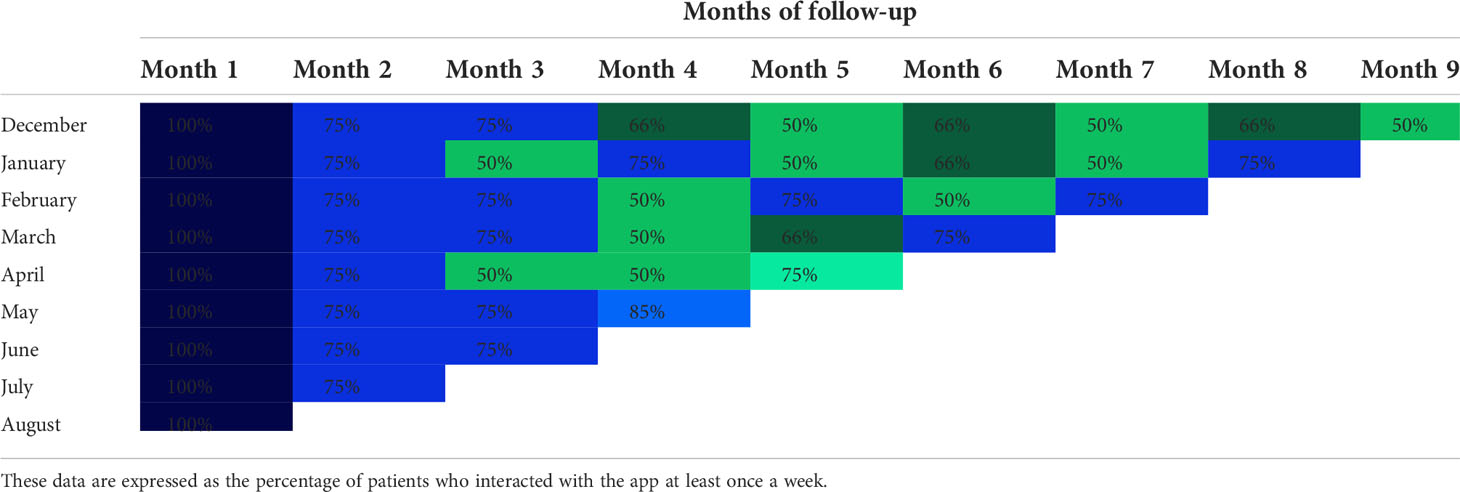
Table 4 App retention rate during the 9-month follow-up period.
We report on the design and successful implementation of the app eMidCare for the home follow-up of IMID patients undergoing treatment with biological therapies. We assessed the app impact in 85 IMID patients, with characteristics similar to those of patients treated with biologic therapies. Currently available apps for IMID patients are considerably heterogeneous with respect to functionalities and reliability. A recent review of similar apps for Android and iOS has shown that more than half of IMID-related apps are oriented toward offering information (10). Nevertheless, a few apps allow for active patient participation (e.g., recording AEs, managing medication, and communicating with healthcare professionals). However, active use of apps should be encouraged for several reasons, namely, to promote empowerment and self-care and monitor these continuously in real-time and to obtain more information for decision-making by health professionals. Patients’ active participation in their disease care has been associated with improved health adherence, medication safety, and quality of life (11).
Concerning reliability, only 15-42% of IMID patient apps have been developed by professionals, and approximately the half of the apps have not been updated recently (10, 12–14). This limitation generates considerable doubt among professionals when recommending apps to patients. Therefore, we believe that an app designed by healthcare professionals whose impact is evaluated in a controlled environment, such as a hospital, guarantees reliability.
eMidCare was designed based on the experience of the multidisciplinary team and on patients’ needs. Few IMID-related apps have taken patients into account in their design. The 6 modules defined in eMidCare—My Medication, My Questionnaires, Adverse Events, Useful Information, Messages, and Patient Profile—meet the requirements for achieving our ultimate goal of improving medication safety, adherence, and communication with patients.
Medication recording and reminders were the first functionalities incorporated into general health apps that enable patients to manage their pharmacotherapy. All patients included in the study recorded the biological therapy they were receiving. Consequently, they obtained specific information about each medication. In the market, there are very few apps with this functionality specific for this kind of therapies, only 5 out of 243 (2%) apps for IMID patients analyzed in a recent review had specific information on biologic therapies (10). Two of these apps (Remsimate®, MySIMPONI®) were oriented solely towards biologic therapy (infliximab and golimumab, respectively). However, this type of app should enable patients to record their complete treatment regimen, including monitoring of drug-drug interactions and adherence (13, 15, 16).
Apps are the preferred method for reminding patients to take their medication regularly (8), and numerous studies have shown that apps can improve adherence to treatment (13, 16–18). Alerts and reminders are the features that most frequently improve adherence. More than a quarter of our patients used this module to record each dose of medication administered. This could have influenced the high adherence observed (the median adherence was 100% and 86.4% of patients had an adherence >90%). Encouraging adherence is especially important in patients treated with biological therapies, since these medicines are not administered daily and it is easier to forget them. However, Romero-Jimenez et al. observed that only 16.9% of IMID-related apps enabled patients to record their medication and that only 11.1% enabled them to monitor adherence (10).
The Spanish Society of Hospital Pharmacy’s Rheumatoid Arthritis Guide references apps that have been used to improve adherence in IMID patients (RecuerdaMed®, MediSafe®, MyTherapy®, Dosecast®, Care4Today®) (19). However, none contain functionalities or information about IMID, but rather comprise general apps that aim only to remind patients to administer medication.
IMIDs have a high impact on patients’ quality of life (20). PROs enable the patient to provide subjective feedback on their disease, thus empowering the patient and enhancing patient-centred medicine (21). Monitoring PROs improves the follow-up of IMID patients and aids in decision-making, which improves health outcomes (22).
The use of apps can enhance recording and tracking of PROs’ by reducing limitations such as resource consumption, lack of time, and difficulties recording in real time and continuously (19). Riel et al. described different innovative electronic tools to monitor the management of arthritis (7). Sanoia® is an online interactive electronic e-health platform that enables self-assessment and self-monitoring in rheumatoid arthritis (23). iMonitor® is a software application that enables patients with rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis to report information about their disease state. The physician can review PROs and receive alerts when established thresholds are not met or if PROs are not completed on time. GoTreatIT Rheuma® is a software application that collects and displays data related to disease activity, health status, and quality of life. Despite these experiences, PRO recording is a rare functionality in apps for IMID patients. Romero-Jimenez et al. observed that only 11.5% of the apps for IMID patients enable recording of PROs (10). Another advantage of eMidCare is its versatility, which enables new PROMs to be incorporated. Healthcare professionals can easily incorporate PROMs directly into the CMS.
IMIDs can also have an impact on patients’ work activity. A cross-sectional online survey of spondyloarthritis patients from 13 European countries concluded that spondyloarthritis substantially impacts the working life of two-thirds of the actively employed population (24). Thus, we included the Work Productivity and Activity Impairment (WPAI) questionnaire in eMidCare.
New biological therapies are becoming increasingly safe (1), although they may produce AEs that diminish their effectiveness and patients’ quality of life (25). Consequently, adequate pharmacovigilance is essential for prevention and management of AEs associated with this type of drug. Almost one-third of our patients reported at least one AE. Hence the important role of eMidCare in the safety of these treatments. Besides, patients took a median of 16 days to register their first AE, thus enabling us to identify them before the first follow-up consultation with a specialist. This early detection may have contributed to the early management of adverse effects, hence only 8.5% of the AE’s recorded were graded ≥ 3. For example, the proportion of patients who discontinued treatment with adalimumab in pivotal studies was 5.9% (25). A similar experience in cancer patients helped to reduce the number of AEs and their severity (15). Using a decision tree to manage AEs helped to reduce visits to the emergency room. However, this functionality is not standard in apps for IMID patients. Romero-Jimenez et al. observed that only 21.0% of the apps for IMID patients made it possible to record symptoms or AEs (10), although the authors did not state whether these apps offered individualized recommendations. We were unable to find apps for IMID patients that enable self-management of AEs through automatic recommendations via a decision tree.
Atreja et al. reported that IMID patients feel insufficiently informed about their illness and treatment (26), as our focus group participants highlighted.
Approximately 60% of the apps available for IMID patients offer information about the disease, treatments, and lifestyle (10), thus making it the most frequent functionality of these types of apps. Besides, information on medication was the feature most desired by a cohort of 193 patients with rheumatic disease (8). Mollard et al. observed that 25% of apps available for rheumatoid arthritis were exclusively for patient education (27). One of the advantages of eMidCare is that it includes specific information on biological therapies, which is rare in these apps (22).
Doubts about the reliability of the apps’ authorship mean that the information provided should be used with caution. Even more important is the timing of updates, especially in a field such as IMIDs and biological therapies, where new scientific evidence is constantly appearing. The lack of specific legislation means that there are no guarantees with respect to the information obtained (28, 29). However, information that points to an app’s reliability includes authorship, date of update, whether the information is referenced, number of downloads, ratings, comments on the stores, or even if it has a quality seal (30).
In the focus group, we conducted prior to the development of the app, the most important point was to improve communication with healthcare professionals. This need has been confirmed with the use of eMidCare, as it has also been the most used functionality. The Messages module was used to communicate with the healthcare professional by 52% of patients. It was also the module most valued by patients, with a score of 9.5 out of 10. Messages was the most frequently accessed module, thus confirming the importance of these technologies in terms of communication. In addition, it was the most frequently used module in terms of time spent (21.9%).
We believe this app has greatly improved communication with our patients over the traditional model of care. The possibility of daily communication with health professionals reassures patients and gives them confidence. Thanks to eMidCare, we are helping patients who experience more difficulties contacting the health system and feel more helpless, since 33.5% of the queries answered through e-MidCare were made after 3:00 pm or at weekends. This communication proved to be worthwhile, since we likely avoided unscheduled visits.
In a French, multicenter, clinical trial, the interactive Sanoia® e-health platform was compared with traditional follow-up for 12 months (23). The authors observed a statistically significant improvement in patients’ perception of the quality of communication between IMID patients and their physicians.
The most innovative functionality of this module was gamification. The patient receives different awards according to the percentage of registration of medications and PROs. Gamification is a specific mHealth technique that favors behavioral change and increases users’ engagement. Haase et al. reported that gamification encourages adherence through personalized deals and promotions (18). In a revision of apps for IMID patients, only 1 of the 243 apps analyzed has a gamification module (10).
Finally, our results revealed a high degree of satisfaction with the aspects assessed. Those best rated were the ability to communicate with healthcare professionals, ease of app use, and reminders to administer medication. Patient satisfaction with this type of app is generally high (23, 31). Fifty-five patients with Crohn’s disease were satisfied (median VAS score 8) with an app for monitoring their intravenous biological treatment (31). The mean satisfaction with the Sanoia® platform was very high, although around a quarter of the patients never accessed the platform (12). The retention rate for eMidCare was high. We found no published studies on the usability of apps for IMID patients; however, 90-day retention has been reported to be 34% and annual retention 16% (32). The success of eMidCare was probably due to its ad hoc development based on patients’ needs and the possibility of communication with health professionals. Support from health professionals is key to increasing longer-term engagement with these tools. Besides, apps that involve the active participation of patients by data registration, messages, or gamification can improve usability. The possibility for healthcare professionals to adapt the contents of the app through the CMS for ease of reproducibility and acceptance by patients
While health apps encourage patients to take an active role in the management of their disease, this may lead them to overestimate their role in choosing medical treatment. It is essential that the app adequately detects “alarms” and that healthcare professionals have sufficient control mechanisms (33); hence the importance of the web interface, which enables continuous and real-time monitoring of patients. However, this supervisory role of healthcare professionals could increase their workload. eMidCare has a system for sending automatic emails to healthcare professionals when patients add a new medication, register an AE, or send a message. Consequently, health professionals know when these events occur without having to check the website, thus continuously reducing workload.
The limited size sample of patients diagnosed with IBD and JIA makes it difficult to draw conclusions in these pathologies. However, most treatments for these pathologies are common to other IMIDs. Thus, the information and questions about treatment and the adverse events that patients suffer are very similar.
We evaluated the use of our app through a prospective observational study. The descriptive evaluation of the results in our patients and the absence of a comparator group do not allow us to draw solid conclusions as to whether eMidCare improves certain aspects such as medication safety or adherence. Some review studies on the use of apps in IMID patients conclude that evidence on their impact is still lacking and that clinical trials with clearly predefined outcomes should be performed in a large cohort (33). However, the rapid advancement of mHealth makes this problematic owing to changes in technologies. The positive results we obtained serve as an incentive to continue using eMidCare with our patients, and we will continue to make improvements and carry out evaluations of this system.
We developed an app, eMidCare®, which enables remote and real-time follow-up of and communication with IMID patients receiving biological therapies. This new tool reminds patients to take their medication, enables them to record AEs, and helps them communicate with healthcare professionals. Approximately one-third of the patients registered the administration of the biological therapies and registered at least 1 AE. However, the most used and most satisfactory functionality was communication with health professionals. Patient satisfaction and retention were very high.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study was reviewed and approved by the Clinical Research Ethics Committee of Gregorio Marañón University Hospital (code MSS-APP-2019). All patients signed written informed consent.
RR-J wrote the first draft. RR-J, VE-V, AH, and MS defined the research question and objectives. RR-J, VE-V, EC-d-V, AA-L, EL-M, CG, OB, LM, CL-R, and AH defined the app’s functionalities. RR-J, VE-V, EC-d-V, AA-L, EL-M, BS-F, and PR-B included the patients and followed them up. RR-J, VE-V, AH, and MS were responsible for the research activity plan and its execution. All authors reviewed and approved the manuscript.
Novartis sponsored the technological development of the app. Novartis did not participate in the conception of the app, the inclusion and follow-up of patients, or the evaluation of results.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.915578/full#supplementary-material
1. Molinelli E, Campanati A, Ganzetti G, Offidani A. Biologic therapy in immune mediated inflammatory disease: Basic science and clinical concepts. Curr Drug Saf (2016) 11(1):35–43. doi: 10.2174/1574886310666151014115127
2. Maniadakis N, Toth E, Schiff M, Wang X, Nassim M, Szegvari B, et al. A targeted literature review examining biologic therapy compliance and persistence in chronic inflammatory diseases to identify the associated unmet needs, driving factors, and consequences. Adv Ther (2018) 35(9):1333–55. doi: 10.1007/s12325-018-0759-0
3. Martínez-López de Castro N, Álvarez-Payero M, Samartín-Ucha M, Martín-Vila A, Piñeiro-Corrales G, Pego Reigosa JM. Adherence to biological therapies in patients with chronic inflammatory arthropathies. Farm Hosp (2019) 43(4):134–9. doi: 10.7399/fh.11183
4. Blauvelt A, Wu JJ, Armstrong A, Menter A, Liu C, Jacobson A. Importance of complete skin clearance in psoriasis as a treatment goal: Implications for patient-reported outcomes. J Drugs Dermatol (2020) 19(5):487–92. doi: 10.36849/JDD.2020.4957
5. Law L, Beckman Rehnman J, Deminger A, Klingberg E, Jacobsson LTH, Forsblad-d'Elia H. Factors related to health-related quality of life in ankylosing spondylitis, overall and stratified by sex. Arthritis Res Ther (2018) 20:284. doi: 10.1186/s13075-018-1784-8
6. Korman NJ, Zhao Y, Li Y, Liao M, Tran MH. Clinical symptoms and self-reported disease severity among patients with psoriasis - implications for psoriasis management. J Dermatol Treat (2015) 26(6):514–9. doi: 10.3109/09546634.2015.1034074
7. van Riel P, Alten R, Combe B, Abdulganieva D, Bousquet P, Courtenay M, et al. Improving inflammatory arthritis management through tighter monitoring of patients and the use of innovative electronic tools. RMD Open (2016) 2(2):e000302. doi: 10.1136/rmdopen-2016-000302
8. Knitza J, Simon D, Lambrecht A, Raab C, Tascilar K, Hagen M, et al. Mobile health usage, preferences, barriers, and eHealth literacy in rheumatology: Patient survey study. JMIR Mhealth Uhealth (2020) 8(8):e19661. doi: 10.2196/19661
9. U.S. Department of Health and Human Services. Common terminology criteria for adverse events (CTCAE). version 5.00 (2017). Available at: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf (Accessed 2020-12-20).
10. Romero-Jimenez R, Escudero-Vilaplana V, Chamorro-De-Vega E, Ais-Larisgoitia A, Lobato Matilla ME, Herranz-Alonso A, et al. Characteristics and functionalities of mobile apps aimed at patients diagnosed with immune-mediated inflammatory diseases: systematic app search. J Med Internet Res (2022) 24(3):e31016. doi: 10.2196/31016
11. Yin AL, Hachuel D, Pollak JP, Scherl EJ, Estrin D. Digital health apps in the clinical care of inflammatory bowel disease: Scoping review. J Med Internet Res (2019) 21(8):e14630. doi: 10.2196/14630
12. Najm A, Gossec L, Weill C, Benoist D, Berenbaum F, Nikiphorou E. Mobile health apps for self-management of rheumatic and musculoskeletal diseases: Systematic literature review. JMIR Mhealth Uhealth (2019) 7(11):e14730. doi: 10.2196/14730
13. Tabi K, Randhawa AS, Choi F, Mithani Z, Albers F, Schnieder M, et al. Mobile apps for medication management: Review and analysis. JMIR Mhealth Uhealth (2019) 7(9):e13608. doi: 10.2196/13608
14. Luo D, Wang P, Lu F, Elias J, Sparks JA, Lee YC. Mobile apps for individuals with rheumatoid arthritis: A systematic review. J Clin Rheumatol (2019) 25(3):133–41. doi: 10.1097/RHU.0000000000000800
15. Collado-Borrell R, Escudero-Vilaplana V, Ribed A, Gonzalez-Anleo C, Martin-Conde M, Romero-Jimenez R, et al. Effect of a mobile app for the pharmacotherapeutic follow-up of patients with cancer on their health outcomes: Quasi-experimental study. JMIR Mhealth Uhealth (2020) 8(10):e20480. doi: 10.2196/20480
16. Timmers T, Janssen L, RB K, Kremer JA. Educating patients by providing timely information using smartphone and tablet apps: Systematic review. J Med Internet Res (2020) 22(4):e17342. doi: 10.2196/17342
17. Pérez-Jover V, Sala-González M, Guilabert M, Mira JJ. Mobile apps for increasing treatment adherence: Systematic review. J Med Internet Res (2019) 21(6):e12505. doi: 10.2196/12505
18. Haase J, Farris KB, Dorsch PD. Mobile applications to improve medication adherence. Telemed J E Health (2017) 23(2):75–9. doi: 10.1089/tmj.2015.0227
19. Guía de Práctica Farmacéutica en Artritis Reumatoide. SEFH. sociedad española de farmacia hospitalaria. (2020). Madrid
20. Puig L, Ruiz de Morales JG, Dauden E, Andreu JL, Cervera R, Adán A, et al. Prevalence of ten immune-mediated inflammatory diseases (IMID) in Spain. Rev Esp Salud Publica (2019) 93:e201903013.
21. US Department of Health and Human Services. Guidance for industry. patient-reported outcome measures: use in medical product development to support labeling claims. Food and Drug Administration (2009). Silver Spring
22. Butler S, Sculley D, Santos DS, Fellas A, Gironès X, Singh-Grewal D, et al. Usability of eHealth and mobile health interventions by young people living with juvenile idiopathic arthritis: Systematic review. JMIR Pediatr Parent (2020) 3(2):e15833. doi: 10.2196/15833
23. Gossec L, Cantagrel A, Soubrier M, Berthelot JM, Joubert JM, Combe B, et al. An e-health interactive self-assessment website (Sanoia®) in rheumatoid arthritis. a 12-month randomized controlled trial in 320 patients. Joint Bone Spine (2018) 85(6):709–14. doi: 10.1016/j.jbspin.2017.11.015
24. Garrido-Cumbrera M, Bundy C, Navarro-Compán V, Makri S, Sanz-Gómez S, Christen L, et al. Patient-reported impact of axial spondyloarthritis on working life: Results from the European map of axial spondyloarthritis survey. Arthritis Care Res (Hoboken) (2021) 73(12):1826–33. doi: 10.1002/acr.24426
25. European Public Assessment Reports. Adalimumab . Amsterdam: European Medicines Agency. Available at: https://www.ema.europa.eu/en/documents/product-information/humira-epar-product-information_en.pdf (Accessed 2021-08-01).
26. Atreja A, Otobo E, Ramireddy K, Deorocki A. Remote patient monitoring in IBD: Current state and future directions. Curr Gastroenterol Rep (2018) 20(2):6. doi: 10.1007/s11894-018-0611-3
27. Mollard E, Michaud K. Mobile apps for rheumatoid arthritis: Opportunities and challenges. Rheum Dis Clin North Am (2019) 45(2):197–209. doi: 10.1016/j.rdc.2019.01.011
28. Chan CX, Markowitz O. APPlying knowledge: evidence for and regulation of mobile apps for dermatologists. Cutis (2020) 106(2):76–8. doi: 10.12788/cutis.0036
29. Sharma A, Harrington RA, McClellan MB, Turakhia MP, Eapen ZJ, Steinhubl S, et al. Using digital health technology to better generate evidence and deliver evidence-based care. J Am Coll Cardiol (2018) 71:2680–90. doi: 10.1016/j.jacc.2018.03.523
30. AppSaludable Quality Seal. Agencia de calidad sanitaria de andalucía. Available at: http://www.calidadappsalud.com/en/distintivo-appsaludable/.
31. van Erp LW, Groenen MJM, Heida W, Wisse J, Roosenboom B, Wahab PJ. Mobile application to monitor inflammatory bowel disease patients on intravenous biologic treatment: a feasibility study. Scand J Gastroenterol (2021) 27:1–8. doi: 10.1080/00365521.2021.1966832
32. 2021 Mobile App Engagement Benchmark Report. Apptentive (2021). Available at: https://www.apptentive.com/2021-benchmark-report/.
Keywords: communication, immune-mediated inflammatory disease, mHealth, mobile app, monitoring
Citation: Romero-Jimenez R, Escudero-Vilaplana V, Chamorro-de-Vega E, Ais-Larisgoitia A, Lobato-Matilla E, Somoza-Fernández B, Ruiz-Briones P, González C, Baniandrés O, Menchén L, Lobo-Rodríguez C, Herranz A and Sanjurjo M (2022) Design and implementation of a mobile app for the pharmacotherapeutic follow-up of patients diagnosed with immune-mediated inflammatory diseases: eMidCare. Front. Immunol. 13:915578. doi: 10.3389/fimmu.2022.915578
Received: 08 April 2022; Accepted: 05 July 2022;
Published: 28 July 2022.
Edited by:
Giuseppe Murdaca, University of Genoa, ItalyReviewed by:
Yue Victor Zhang, Shenzhen Futian Hospital for Rheumatic Diseases, ChinaCopyright © 2022 Romero-Jimenez, Escudero-Vilaplana, Chamorro-de-Vega, Ais-Larisgoitia, Lobato-Matilla, Somoza-Fernández, Ruiz-Briones, González, Baniandrés, Menchén, Lobo-Rodríguez, Herranz and Sanjurjo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vicente Escudero-Vilaplana, dmljZW50ZS5lc2N1ZGVyb0BzYWx1ZC5tYWRyaWQub3Jn
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.