
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol., 25 May 2022
Sec. Systems Immunology
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.862742
 Isis Ricaño-Ponce1†
Isis Ricaño-Ponce1† Toon Peeters1,2,3†
Toon Peeters1,2,3† Vasiliki Matzaraki1
Vasiliki Matzaraki1 Bert Houben4Ruth Achten4Peter Cools5
Bert Houben4Ruth Achten4Peter Cools5 Mihai G. Netea1,6
Mihai G. Netea1,6 Inge C. Gyssens1,2,3
Inge C. Gyssens1,2,3 Vinod Kumar1,7,8*
Vinod Kumar1,7,8*Background: Acute appendicitis is one of the most common abdominal emergencies worldwide. Both environmental and genetic factors contribute to the disease. C-reactive protein (CRP) is an important biomarker in the diagnosis of acute appendicitis. CRP concentrations are significantly affected by genetic variation. However, whether such genetic variation is causally related to appendicitis risk remains unclear. In this study, the causal relationship between single-nucleotide polymorphisms (SNPs) associated with circulating CRP concentrations and the risk and severity of acute appendicitis was investigated.
Methods: CRP concentrations in serum of appendicitis patients (n = 325) were measured. Appendicitis was categorized as complicated/uncomplicated and gangrenous/non-gangrenous. Imputed SNP data (n = 287) were generated. A genome-wide association study (GWAS) on CRP concentrations and appendicitis severity was performed. Intersection and colocalization of the GWAS results were performed with appendicitis and CRP-associated loci from the Pan-UKBB cohort. A functional-genomics approach to prioritize genes was employed.
Results: Thirteen percent of significant CRP quantitative trait loci (QTLs) that were previously identified in a large cohort of healthy individuals were replicated in our small patient cohort. Significant enrichment of CRP-QTLs in association with appendicitis was observed. Among these shared loci, the two top loci at chromosomes 1q41 and 8p23.1 were characterized. The top SNP at chromosome 1q41 is located within the promoter of H2.0 Like Homeobox (HLX) gene, which is involved in blood cell differentiation, and liver and gut organogeneses. The expression of HLX is increased in the appendix of appendicitis patients compared to controls. The locus at 8p23.1 contains multiple genes, including cathepsin B (CTSB), which is overexpressed in appendix tissue from appendicitis patients. The risk allele of the top SNP in this locus also increases CTSB expression in the sigmoid colon of healthy individuals. CTSB is involved in collagen degradation, MHC class II antigen presentation, and neutrophil degranulation.
Conclusions: The results of this study prioritize HLX and CTSB as potential causal genes for appendicitis and suggest a shared genetic mechanism between appendicitis and CRP concentrations.
Acute appendicitis is one of the most common surgical emergencies worldwide (1). The lifetime risk is estimated at between 6% and 17% (2, 3). Acute appendicitis involves inflammation of the appendix and can be associated with serious complications such as localized abscess, peritonitis, and perforation. Depending on the severity of the disease and presence of complications, appendicitis is often referred to as complicated or uncomplicated. Based on histological examination for the presence of necrosis, the disease can also be classified as gangrenous or non-gangrenous.
The etiology of the disease is likely multifactorial. Positive family history is often observed in patients, indicating that appendicitis can be a consequence of both genetic and environmental risk factors. Segregation analyses have shown that appendicitis is inherited by a polygenic model in which several genetic loci, in addition to environmental triggers, contribute to the disease phenotype (4). Twin studies and population-based studies also show familial transmission of acute appendicitis through genetic as well as environmental effects (5–7).
The role of genetic factors in the development of acute appendicitis has been confirmed in a number of candidate gene-based as well as genome-wide association studies (GWASs). Although inconsistent associations exist between the severity of appendicitis and single-nucleotide polymorphisms (SNPs) at NOD2/CARD15 (8) and IL-6 genes (9, 10), a significant association at SNP rs2129979 near PITX2 gene has been observed in adults (11). This finding was confirmed in another study, and a number of additional susceptibility genes were identified (12). Among other genes, PITX2 was also differentially expressed in different categories of appendiceal inflammation, suggesting a potential genetic link between inflammation regulation and appendicitis phenotypes.
The etiology of appendicitis is not yet well understood; however, several observations point to the pathogenic pathways related to inflammation. C-reactive protein (CRP) is one of the most abundant systemic markers of inflammation and one of the most important biomarkers in the diagnosis of acute appendicitis. In addition, serum CRP concentrations appear to be associated with disease severity (13–16). With the use of QTL mapping strategies in large population-based cohorts, it has been shown that the CRP concentrations are significantly affected by host genetic variation (17, 18). However, whether such CRP-QTLs are causally related to appendicitis risk remains unclear. Therefore, in this study, the causal relationship between SNPs associated with circulating CRP concentrations and the risk and severity of acute appendicitis was investigated.
All patients included in this study gave written informed consent before participation; in the case of children, informed consent was obtained from parents or guardians. The study was approved by the Medical Ethics Committee of Jessa Hospital, Hasselt, Belgium. The study was registered at Clinicaltrials.gov under identifier NCT02391675. The study population consisted of 374 appendicitis patients (Table 1). A total of 325 patients were prospectively recruited in the HAPPIEST population at Jessa Hospital, Hasselt, Belgium, between June 2012 and October 2016. An additional 49 patients were recruited at Sint-Vincentius Hospital, Antwerp, Belgium, between September 2015 and March 2017. Patients between the ages of 5 and 85 were considered possible candidates. All included patients had an appendectomy in the first 5 days after diagnosis. Exclusion criteria were patients with an appendectomy more than 5 days after onset of symptoms, pregnant, and immunocompromised patients.

Table 1 Demographics of patients in the HAPPIEST cohort.
Acute appendicitis was diagnosed based on clinical symptoms, laboratory results, and ultrasound and/or CT scan. Clinical data and medical history of patients were recorded. Patients received standard-of-care treatment. CRP concentrations were measured as routine at the time of admission at Jessa Hospital. Upon surgery, the appendix was sectioned, and appendicitis was classified by the surgeon according to ICD-9 codes. Samples from a 1-cm part of the tip, the middle, and the base were sent to the pathology department to confirm the diagnosis and assign histological severity (gangrenous vs. non-gangrenous). Acute appendicitis with general peritonitis (540.0) or peritoneal abscess (540.1) was considered complicated; patients with no data on abscess or peritonitis (540.9) were considered uncomplicated. In the HAPPIEST population, microbiological and immunological factors contributing to the risk and severity of acute appendicitis were studied previously (16, 19).
During surgery, EDTA blood was collected (3 × 10 ml in the case of adults and 2 × 10 ml in the case of children). Samples were aliquoted and frozen at −80°C at the University Biobank Limburg (UBiLim). DNA isolation from whole blood was performed using the DNeasy Blood and Tissue kit (Qiagen, Venlo, the Netherlands) according to the manufacturer’s instructions. DNA samples were stored at −20°C until further analysis.
The study design is presented in Supplementary Figure 1 (Additional File 1). DNA samples from 331 individuals who passed quality control (QC) were hybridized on the Infinium CoreExome v3 SNP chip from Illumina. Genotype calling was performed using optiCall 0.7.0 using default settings (20). Non-polymorphic markers and markers within sexual chromosomes were excluded for further analysis. Chromosome coordinates are given in human Build 37 (hg19). QC checks and filters were performed using PLINK version 1.09 (21). Samples with a call rate <99% and SNPs with a call rate <99%, Hardy–Weinberg equilibrium exact test ≤0.001, and minor allele frequency (MAF) ≤0.001 were discarded. Three individuals were removed because of an excess of homozygosity rate. Two individuals were removed due to hidden relatedness calculated by identity-by-descent estimates. Thirty-nine population outliers were detected by multidimensional scaling (MDS) plots using R Studio and removed for further analysis. After QC, the dataset comprised 287 samples and 272,017 SNPs. Strands of variants were aligned and identified against the 1000 Genomes reference panel using Genotype Harmonizer (22). Genotype imputation was performed on the Michigan Imputation Server using the human reference consortium as a reference panel, and variants with an R2 ≤ 0.3 and MAF ≤ 0.10 were excluded for imputation QC (23).
GWAS on complicated versus uncomplicated appendicitis and gangrenous vs. non-gangrenous was performed using SNPtest version 2.5.2 (24). A frequentist additive model was run including age and sex as covariates. To control for genotype uncertainty, the parameter score was selected to include a missing data likelihood score test.
To test whether CRP and appendicitis had shared genetic loci, the summary statistics from the Pan-ancestry genetic analysis of the UK Biobank (Pan-UKBB) were used (25). The files were extracted according to their phenotype manifest. The Pan-UKBB ID in the manifest for the CRP-QTLs in the general population is “biomarkers-30710” and for acute appendicitis “phecode-540.1”. All analyses were focused on the results from individuals with European ancestry. The CRP-QTL study was a population-based study (n = 400,094), where the appendicitis cohort comprised 3,490 acute appendicitis cases and 416,195 controls. SNP IDs were annotated based on the variant manifest file provided by Pan-UKBB.
Expression QTLs were obtained from the GTEx portal (26) on February 13, 2020. Microarray gene expression from the appendix of 9 appendicitis cases and 4 individuals who were undergoing intra-abdominal surgery for a non-inflammatory condition has been generated previously (27), and it is publicly available at Gene Expression Omnibus with ID “GSE9579.” Expression values were obtained using GEO2R on the same website; the probe selected for HLX was 214,438_AT, and for CTSB, it was 200838_AT. The expression values were compared using a t-test. Chromatin states were annotated using data from sigmoid colon and colon smooth muscle reported by the Roadmap Epigenomics Mapping Consortium (28). These data were obtained and visualized on the WashU epigenome browser (29).
CRP concentrations and genotypes for 285 individuals were available. Normalization of CRP concentrations was done by inverse rank quantile normalization. The correlation between normalized CRP concentrations and genotype was assessed with a linear regression model including age and sex as covariables using the eQTLMatrix package in R. Significance was considered as p < 0.05.
CRP concentrations in different age groups were compared by dividing the cohort into four different age range groups. The difference in CRP concentrations was assessed using the non-parametrical Kruskal–Wallis sum rank test, followed by a Dunn’s test to compare between groups. To assess the shared genetic variants between appendicitis and CRP concentrations, the genome-wide significant CRP-QTLs were extracted from the Pan-UKBB and intersected with the results from the appendicitis GWAS performed in the same cohort. The enrichment was calculated based on the quantification of the degree of inflation between the observed and expected p-values from a uniform distribution in the QQ plot. Statistical analysis and plots were generated using R Studio. Genome-wide significance was defined as p < 5 × 10−8, suggestive association as p < 1 × 10−5, and significance as p < 0.05. All top SNPs in the loci were functionally annotated using SNP Nexus (https://snp-nexus.org/), including the predicted effect of non-synonymous coding SNPs on protein function by SIFT and PolyPhen. Gene Ontology (GO) terms and PathCard information for the candidate genes were extracted from GeneCards®: The Human Gene Database (https://www.genecards.org).
From the 374 appendicitis patients included in the study, the mean age was 32.8 (range 5–81), and 198 patients (52.9%) were male. Table 1 shows the age and sex of patients with complicated appendicitis, non-complicated appendicitis, and gangrenous and non-gangrenous appendicitis. To assess the difference in CRP concentration at different ages, we stratified the cohort into four different groups, as shown in Supplementary Figure 2 (Additional File 2). CRP concentration was significantly different between groups (p = 3.24 × 10−6) and seems to be increasing with age. All groups showed significant differences, except when the group below 20 years old was compared with the group between 20 and 40 years old (p = 0.14) and patients between 40 and 60 years old were compared with patients between 60 and 80 years old.
To test whether the previously reported genetic causes of CRP concentrations (CRP-QTLs) in healthy individuals can be replicated in appendicitis patients, QTL mapping in the cohort was performed. The analysis included 256 individuals in whom we had imputed SNP data and CRP measurements. After 4,416,143 SNPs were tested, 8 loci with suggestive association were identified. Our results were compared with significant CRP-QTLs from the European population in the Pan-UKBB cohort (n = 400,094). Of 65,457 SNPs significantly associated with CRP concentrations in the Pan-UKBB cohort, 36,042 SNPs were present in our analysis, and 4,754 (13.2%) were replicated with a p < 0.05 (Supplementary Table 1).
To test whether CRP concentrations are genetically related to acute appendicitis, we looked for enrichment of CRP-associated SNPs in appendicitis GWAS. For this analysis, 65,457 genome-wide significant CRP-QTLs from the Pan-UKBB cohort were intersected with the summary statistics from the appendicitis GWAs performed in the same cohort. The analysis revealed significant enrichment of CRP-associated SNPs in appendicitis GWAS (inflation factor of 1.19), as shown in Figure 1.
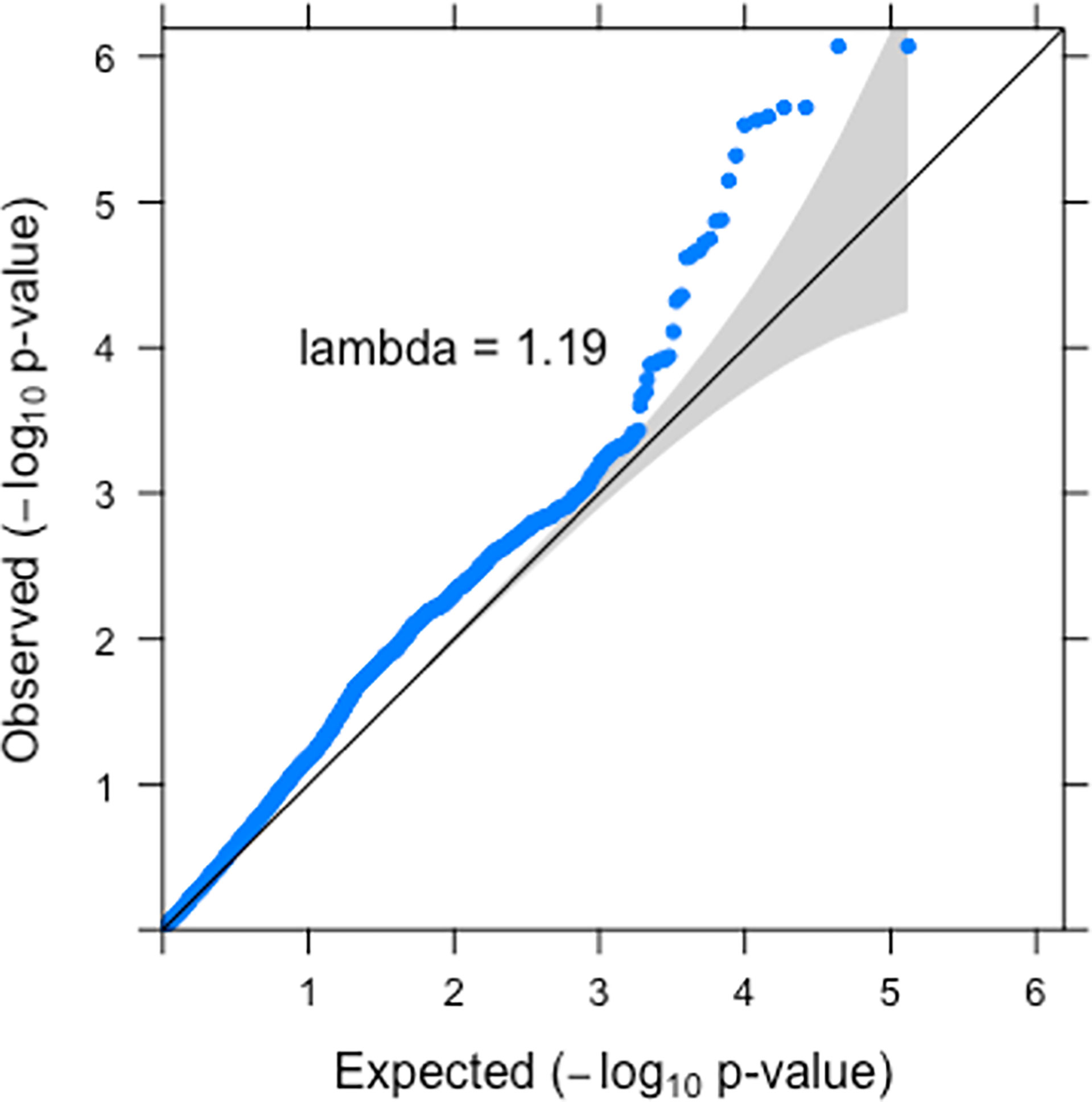
Figure 1 Enrichment of CRP-QTLs in appendicitis GWAS. CRP, C-reactive protein; QTLs, quantitative trait loci; GWAS, genome-wide association study.
From the 65,457 SNPs, two loci on chromosomes 1q41 and 8p23.1 reached suggestive association (p < 1 × 10−5) in appendicitis GWAS. To further characterize these loci, functional annotation of the SNPs was performed using literature as well as genomic information from the publicly available databases.
The strongest association in chromosome 1q41 was SNP rs67420025 (p = 7.15 × 10−6). This SNP is located in the promoter region of the H2.0 Like Homeobox (HLX) gene and overlaps a transcription start site characterized in sigmoid colon and colon smooth muscle, as depicted in Figure 2. rs67420025 is in high linkage disequilibrium (LD) (r2 = 0.928) with rs2738755, a missense variant in HLX that leads to amino acid proline-to-arginine change or proline-to-leucine change, depending on the transcript (NP_068777.1:p.Pro356Arg and NP_068777.1:p.Pro356Leu). While the change from proline to arginine is predicted to be benign by PolyPhen and tolerated by SIFT, the change to leucine is predicted to be deleterious by SIFT.
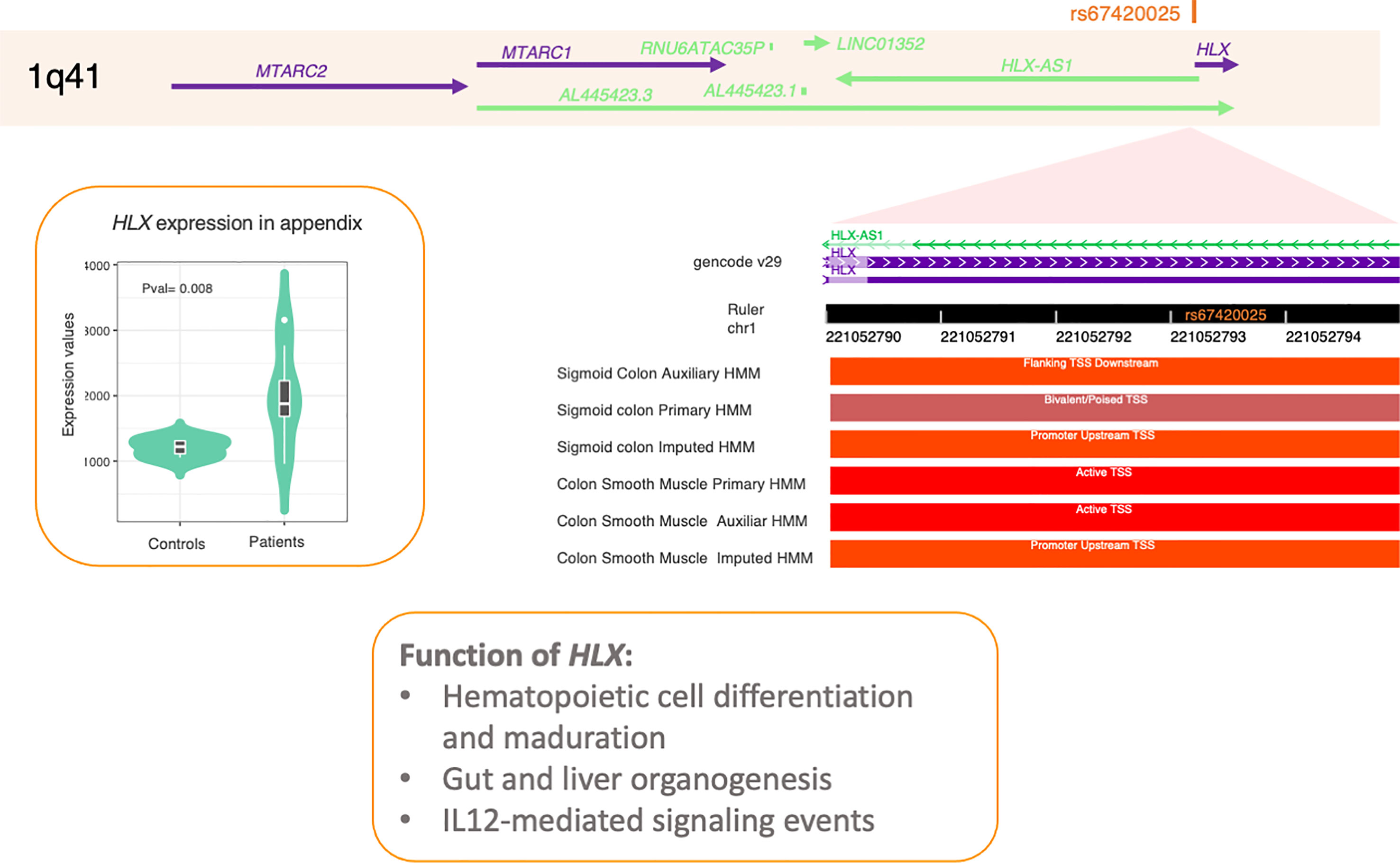
Figure 2 Locus on chromosome 1q41. SNP rs67420025 shows a suggestive association to appendicitis in the Pan-UKBB cohort, and it is located in the promoter region of HLX and overlaps a transcription start site (TSS) in colon smooth muscle. The right panel shows a significant increase in HLX expression in the appendix of 9 appendicitis patients and 4 controls. The box at the bottom shows the function of HLX as reported in the literature and PathCards. SNP, single-nucleotide polymorphism.
Moreover, gene expression of HLX is significantly higher in the appendix of appendicitis patients compared to that of individuals who were undergoing intra-abdominal surgery for a non-inflammatory condition (p = 0.008, Figure 2). According to the GO biological process, HLX is involved in cell differentiation, embryonic digestive tract morphogenesis, enteric nervous system development, liver development, multicellular organism development, negative regulation of T-helper 2 cell differentiation, positive regulation of cell population proliferation, positive regulation of organ growth, positive regulation of T-helper 1 cell differentiation, and skeletal muscle tissue development. A study using a mouse model with deficient expression of HLX revealed that HLX is also involved in liver and gut morphogenesis (30). Additionally, PathCards reports HLX as part of the IL-12-mediated signaling events SuperPath.
In an independent acute appendicitis GWAS performed on the FinnGen cohort (31), the HLX locus on chromosome 1q41 has reached genome-wide significance (top SNP = rs3738182, p = 7.1 × 10−10). Although the top SNP rs67420025 was not tested in the FinnGen cohort, its proxy rs2738755 reaches genome-wide significance in the FinnGen analysis (p = 3.6 × 10−8). These observations indicate the highly likely causal role of HLX in conferring susceptibility to appendicitis.
The top SNP on chromosome 8p32.1 locus is rs2686198 (p = 8.48 × 10−7). This SNP is located in an intron of the farnesyl-diphosphate farnesyltransferase 1 (FDFT1) gene. The locus contains multiple genes including cathepsin B (CTSB) gene (Figure 3). The expression of CTSB was significantly higher in the appendix of appendicitis patients compared to individuals who were undergoing intra-abdominal surgery for a non-inflammatory condition (p = 0.0004). None of the other genes within the locus showed a significant difference in this comparison. Additionally, the risk allele (C) of rs2686198 significantly increases the expression of CTSB in the sigmoid colon of individuals from the GTEx project (p = 2.7 × 10−11) and the CTSB concentrations in plasma (p = 1.9 × 10−28) (32).
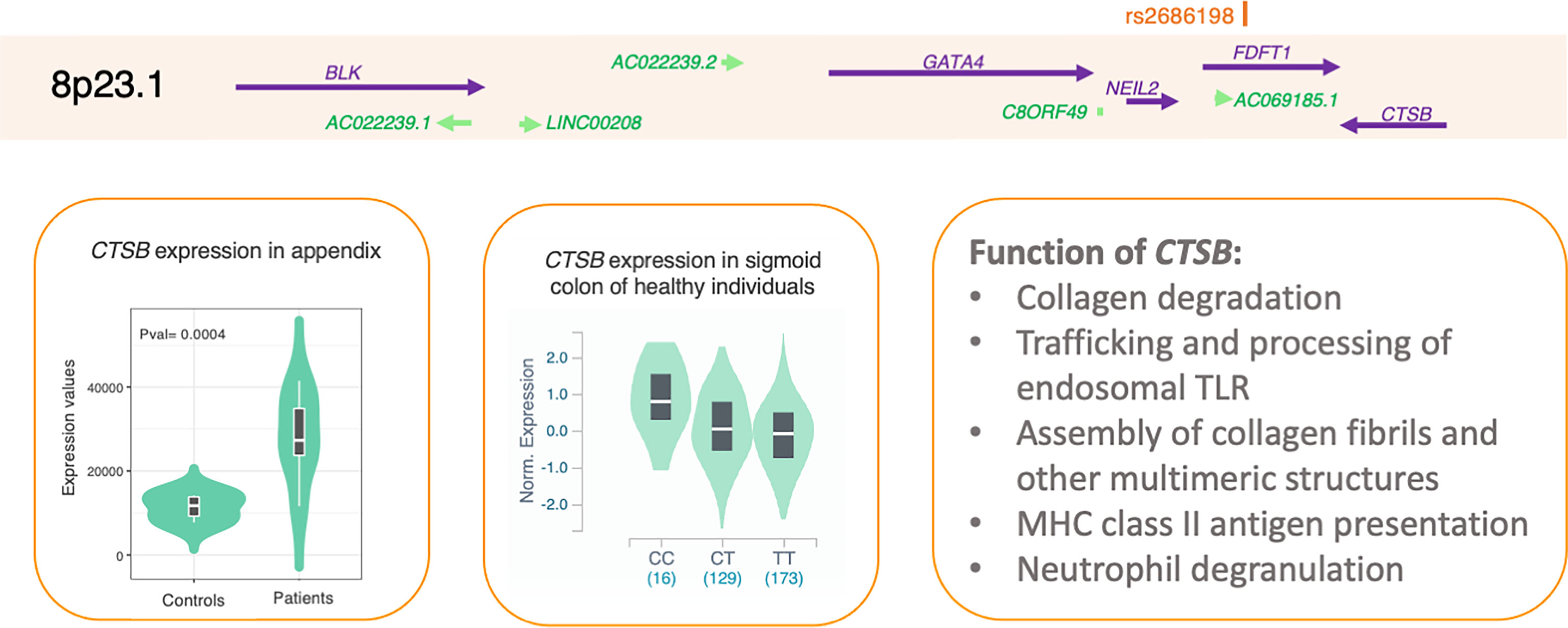
Figure 3 Locus on chromosome 8p32.1. The strongest association in this locus corresponds to SNP rs2686198 with a p-value of 8.48 × 10−7 in the Pan- UKBB cohort. There are multiple genes in the locus, but only cathepsin B (CTSB) is significantly overexpressed in the appendix of patients compared to individuals who were undergoing intra-abdominal surgery for a non-inflammatory condition, as depicted in the left panel. The risk allele of rs2686198*C is associated with higher expression of CTSB in sigmoid colon in healthy individuals. The left panel shows the function of CTSB according to Reactome. SNP, single-nucleotide polymorphism.
According to Reactome, CTSB is involved in collagen degradation, trafficking and processing of endosomal TLR, assembly of collagen fibrils and other multimeric structures, MHC class II antigen presentation, and neutrophil degranulation. The inflammasome pathway, which includes CTSB, was significantly upregulated in plasma from appendicitis patients compared to patients with sexually transmitted infection-induced endometritis (adjusted p = 0.0017) (33). These observations point to the important role of CTSB in regulating inflammation and in turn affecting susceptibility to appendicitis.
In order to establish whether genetic variants associated with appendicitis also predispose to disease severity, a GWAS was performed on our Belgian cohort, comparing complicated patients with uncomplicated appendicitis patients and gangrenous with non-gangrenous appendicitis. A total of 331 individuals in whom DNA was available were genotyped. After QC filtering per sample and per SNPs, 287 individuals were imputed. After imputation QC, 430,122 SNPs and 285 individuals were available for the GWAS analysis.
For the GWAS on appendicitis complications, the individuals were split into complicated appendicitis cases (n = 82) and uncomplicated cases (n = 203). No loci reaching genome-wide significance were identified, although 11 loci showed a suggestive association (p < 1 × 10−5, Supplementary Table 2).
To assess the genetic influence on the development of gangrenous appendicitis, a GWAS was performed including 91 patients with gangrenous appendicitis and 194 patients with non-gangrenous appendicitis. Although ten loci with suggestive associations were found, none of them reached genome-wide significance (Supplementary Table 3).
The 585 SNPs showing suggestive associations with appendicitis identified in the PAN-UKBB cohort were intersected with our results. Out of 277 SNPs tested in this cohort, only 46 SNPs showed a nominal association. One SNP (rs61571009, p in the Belgian cohort = 0.037, p in the PAN-UKBB = 1.13 × 10−7) was associated with appendicitis complications, while 45 comprising two loci were associated with gangrenous appendicitis (Supplementary Table 4).
Given the pleiotropic nature of many molecular phenotypes, one of the important observations of this study is the identification of shared genetic loci between CRP concentrations and appendicitis. The fact that 13.2% of significant CRP-QTLs that were identified previously in a large cohort of healthy individuals could be replicated in a small patient cohort and the significant enrichment of CRP-QTLs in appendicitis GWAS suggests the causal role of CRP in the disease and bridge a knowledge gap regarding SNP–disease associations in appendicitis.
Among the two prioritized causal genes, the strongest association was found in HLX gene. A recent study in the FinnGen cohort (with a four times higher sample size than the Pan-UKBB; 12,476 acute appendicitis patients and 163,396 controls) has also identified this locus to be associated with appendicitis, confirming its causal role in the disease. In this study HLX was prioritized as a potential causal gene at this locus, using multiple lines of evidence. The top SNP overlaps a transcription start site of HLX, and the gene is overexpressed in the appendix of appendicitis patients. Additionally, one of the proxies is a missense variant in the same gene. Although we found that one of the proxies of the top SNP had multiple expression QTLs (eQTLs) reported, including HLX in the brain, so far there are no eQTLs determined in the appendix. As eQTLs are highly tissue- and context-specific, such associations in the appendix should be considered in future studies.
The second prioritized gene, CTSB, encodes cathepsin B protein. We found that the top SNP at this locus increases the expression of CTSB in the sigmoid colon in healthy individuals, showing a regulatory effect of this SNP. Moreover, this SNP also increases the concentrations of CTSB protein in the plasma of healthy individuals. Interestingly, CTSB is predicted to interact with the previously established appendicitis gene PITX2 by the Integrated Interactions Database version 2021-05 (11, 12, 34). Therefore, it is tempting to speculate that CTSB and PITX2 may affect similar molecular pathways to cause appendicitis.
There are also a number of limitations to this study. Firstly, the patient sample size is relatively small, which limited the ability to draw strong conclusions from GWAS of appendicitis complications. Although the shared genetics between appendicitis susceptibility and disease severity was assessed, only 46 SNPs reached a nominal significance in our cohort. As it is shown in the context of immune diseases—for example, in inflammatory bowel disease (IBD) and celiac disease, SNPs conferring risk to disease susceptibility are different from the ones predisposing to disease severity (35, 36)—it could be interesting for future research to test this hypothesis in a larger appendicitis cohort, as it might reflect the difference in the tested sample sizes. Secondly, the gene expression data from the appendix of appendicitis patients and controls were generated using micro-array technology that did not include the majority of non-coding genes. Therefore, their role in appendicitis cannot be excluded. Finally, our cohort comprises patients within an age range from 5 to 81 years, although correcting for age in our analysis addresses this issue; by pooling all age groups together, we might dilute the power to identify age-specific genetic effects. This could potentially affect the comparison that we performed with the Pan-UKBB cohort, as the age range from this cohort is 40 to 69. The age restriction in this cohort was due to the primary aim of the study: to improve the prevention, diagnosis, and treatment of serious illnesses that typically onset later in life, including diabetes, cancer, arthritis, heart disease, stroke, and dementia. Similarly, previous GWASs in appendicitis susceptibility have been performed only using adult patients. Thus, further studies need to be performed in different age ranges to assess if the extent of shared genetics of appendicitis and CRP varies with different age groups.
Our results prioritize HLX and CTSB as potential causal genes for appendicitis and suggest a shared genetic mechanism between appendicitis and CRP concentrations.
The datasets presented in this article are not readily available because the informed consent did not include permission for genotype sharing. Requests to access the datasets should be directed to Vinod Kumar at Vi5LdW1hckByYWRib3VkdW1jLm5s.
The studies involving human participants were reviewed and approved by the Medical Ethics Committee of Jessa Hospital, Hasselt, Belgium. The patients/participants provided their written informed consent to participate in this study. In the case of children informed consent was obtained from parents or guardians.
ICG and VK designed and supervised the study. BH, PC, TP recruited the patients, BH and PC collected the samples and coded the clinical severity and RA performed the histological analysis. IR-P, TP and VM performed the analyses. IR-P and TP wrote the initial manuscript, MGN, ICG, BH, PC, RA, VM and VK reviewed and edited the manuscript. All authors read and approved the final manuscript.
This study is part of the Limburg Clinical Research Program (LCRP) UHasselt-ZOL-Jessa, supported by the foundation Limburg Sterk Merk, province of Limburg, Flemish government, Hasselt University, Ziekenhuis Oost-Limburg, and Jessa Hospital. Part of the work was funded by a research grant (2017) from the European Society of Clinical Microbiology and Infectious Diseases, a Radboudumc Hypatia Grant (2018), and a grant from the research program ZonMw COVID-19 call by the Netherlands Organisation for Health Research and Development (ZonMw) to VK.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank the UK Biobank for the collection and public availability of the data, as well as the Pan-UK Biobank team for the analysis and again public availability of the results.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.862742/full#supplementary-material
1. Stewart B, Khanduri P, McCord C, Ohene-Yeboah M, Uranues S, Vega Rivera F, et al. Global Disease Burden of Conditions Requiring Emergency Surgery. Br J Surg (2014) 101(1):e9–22. doi: 10.1002/bjs.9329
2. Williams JG, Roberts SE, Ali MF, Cheung WY, Cohen DR, Demery G, et al. Gastroenterology Services in the UK. The Burden of Disease, and the Organisation and Delivery of Services for Gastrointestinal and Liver Disorders: A Review of the Evidence. Gut (2007) 56(Suppl 1):1–113. doi: 10.1136/gut.2006.117598
3. Lee JH, Park YS, Choi JS. The Epidemiology of Appendicitis and Appendectomy in South Korea: National Registry Data. J Epidemiol (2010) 20(2):97–105. doi: 10.2188/jea.JE20090011
4. Basta M, Morton NE, Mulvihill JJ, Radovanovic Z, Radojicic C, Marinkovic D. Inheritance of Acute Appendicitis: Familial Aggregation and Evidence of Polygenic Transmission. Am J Hum Genet (1990) 46(2):377–82.
5. Sadr AO, Andren-Sandberg A, Larsson H. Genetic and Environmental Influences on the Risk of Acute Appendicitis in Twins. Br J Surg (2009) 96(11):1336–40. doi: 10.1002/bjs.6736
6. Oldmeadow C, Mengersen K, Martin N, Duffy DL. Heritability and Linkage Analysis of Appendicitis Utilizing Age at Onset. Twin Res Hum Genet (2009) 12(2):150–7. doi: 10.1375/twin.12.2.150
7. Li HM, Yeh LR, Huang YK, Hsieh MY, Yu KH, Kuo CF. Familial Risk of Appendicitis: A Nationwide Population Study. J Pediatr (2018) 203:330–5.e3. doi: 10.1016/j.jpeds.2018.07.071
8. Yazdanyar S, Nordestgaard BG. NOD2/CARD15 Genotype and Common Gastrointestinal Diseases in 43,600 Individuals. J Intern Med (2010) 267(2):228–36. doi: 10.1111/j.1365-2796.2009.02137.x
9. Sarsu SB, Yilmaz SG, Bayram A, Denk A, Kargun K, Sungur MA. Polymorphisms in the IL-6 and IL-6R Receptor Genes as New Diagnostic Biomarkers of Acute Appendicitis: A Study on Two Candidate Genes in Pediatric Patients With Acute Appendicitis. Ital J Pediatr (2015) 41:100. doi: 10.1186/s13052-015-0206-7
10. Rivera-Chavez FA, Peters-Hybki DL, Barber RC, Lindberg GM, Jialal I, Munford RS. Innate Immunity Genes Influence the Severity of Acute Appendicitis. Ann Surg (2004) 240(2):269–77. doi: 10.1097/01.sla.0000133184.10676.26
11. Kristjansson RP, Benonisdottir S, Oddsson A, Galesloot TE, Thorleifsson G, Aben KK, et al. Sequence Variant at 4q25 Near PITX2 Associates With Appendicitis. Sci Rep (2017) 7(1):3119. doi: 10.1038/s41598-017-03353-0
12. Orlova E, Yeh A, Shi M, Firek B, Ranganathan S, Whitcomb DC, et al. Genetic Association and Differential Expression of PITX2 With Acute Appendicitis. Hum Genet (2019) 138(1):37–47. doi: 10.1007/s00439-018-1956-2
13. Mikaelsson C, Arnbjornsson E. The Value of C-Reactive Protein (CRP) Determinations in Patients With Suspected Acute Appendicitis. Ann Chir Gynaecol (1984) 73(5):281–4.
14. Shommu NS, Jenne CN, Blackwood J, Joffe AR, Martin DA, Thompson GC, et al. Metabolomic and Inflammatory Mediator Based Biomarker Profiling as a Potential Novel Method to Aid Pediatric Appendicitis Identification. PLoS One (2018) 13(3):e0193563. doi: 10.1371/journal.pone.0193563
15. Yang J, Liu C, He Y, Cai Z. Laboratory Markers in the Prediction of Acute Perforated Appendicitis in Children. Emerg Med Int (2019) 2019:4608053. doi: 10.1155/2019/4608053
16. Peeters T, Martens S, D’Onofrio V, Stappers MHT, van der Hilst JCH, Houben B, et al. An Observational Study of Innate Immune Responses in Patients With Acute Appendicitis. Sci Rep (2020) 10(1):17352. doi: 10.1038/s41598-020-73798-3
17. Ligthart S, Vaez A, Võsa U, Stathopoulou MG, de Vries PS, Prins BP, et al. Genome Analyses of >200,000 Individuals Identify 58 Loci for Chronic Inflammation and Highlight Pathways That Link Inflammation and Complex Disorders. Am J Hum Genet (2018) 103(5):691–706. doi: 10.1016/j.ajhg.2018.09.009
18. Han X, Ong JS, An J, Hewitt AW, Gharahkhani P, MacGregor S. Using Mendelian Randomization to Evaluate the Causal Relationship Between Serum C-reactive Protein Levels and Age-Related Macular Degeneration. Eur J Epidemiol (2020) 35(2):139–46. doi: 10.1007/s10654-019-00598-z
19. Peeters T, Penders J, Smeekens SP, Galazzo G, Houben B, Netea MG, et al. The Fecal and Mucosal Microbiome in Acute Appendicitis Patients: An Observational Study. Future Microbiol (2019) 14:111–27. doi: 10.2217/fmb-2018-0203
20. Shah TS, Liu JZ, Floyd JAB, Morris JA, Wirth N, Barrett JC, et al. optiCall: A Robust Genotype-Calling Algorithm for Rare, Low-Frequency and Common Variants. Bioinf (Oxford England) (2012) 28(12):1598–603. doi: 10.1093/bioinformatics/bts180
21. Chang CC, Chow CC, Tellier LC, Vattikuti S, Purcell SM, Lee JJ. Second-Generation PLINK: Rising to the Challenge of Larger and Richer Datasets. GigaScience (2015) 4:7. doi: 10.1186/s13742-015-0047-8
22. Deelen P, Bonder MJ, van der Velde KJ, Westra HJ, Winder E, Hendriksen D, et al. Genotype Harmonizer: Automatic Strand Alignment and Format Conversion for Genotype Data Integration. BMC Res Notes (2014) 7:901. doi: 10.1186/1756-0500-7-901
23. McCarthy S, Das S, Kretzschmar W, Delaneau O, Wood AR, Teumer A, et al. A Reference Panel of 64,976 Haplotypes for Genotype Imputation. Nat Genet (2016) 48(10):1279–83. doi: 10.1038/ng.3643
24. Marchini J, Howie B, Myers S, McVean G, Donnelly P. A New Multipoint Method for Genome-Wide Association Studies by Imputation of Genotypes. Nat Genet (2007) 39(7):906–13. doi: 10.1038/ng2088
25. Team P-U. (2020). Available at: https://pan.ukbb.broadinstitute.org.
26. Aguet F, Barbeira AN, Bonazzola R, Brown A, Castel SE, Jo B, et al. The GTEx Consortium Atlas of Genetic Regulatory Effects Across Human Tissues. Science (2020) 369(6509):1318–30. doi: 10.1126/science.aaz1776
27. Murphy CG, Glickman JN, Tomczak K, Wang YY, Beggs AH, Shannon MW, et al. Acute Appendicitis Is Characterized by a Uniform and Highly Selective Pattern of Inflammatory Gene Expression. Mucosal Immunol (2008) 1(4):297–308. doi: 10.1038/mi.2008.13
28. Roadmap Epigenomics Consortium, Kundaje A, Meuleman W, Ernst J, Bilenky M, Yen A, et al. Integrative Analysis of 111 Reference Human Epigenomes. Nature (2015) 518(7539):317–30. doi: 10.1038/nature14248
29. Li D, Hsu S, Purushotham D, Sears RL, Wang T. Washu Epigenome Browser Update 2019. Nucleic Acids Res (2019) 47(W1):W158–65. doi: 10.1093/nar/gkz348
30. Hentsch B, Lyons I, Li R, Hartley L, Lints TJ, Adams JM, et al. Hlx Homeo Box Gene is Essential for an Inductive Tissue Interaction That Drives Expansion of Embryonic Liver and Gut. Genes Dev (1996) 10(1):70–9. doi: 10.1101/gad.10.1.70
31. Finngen. Documentation of R5 Release. (2021). Available at: https://finngen.gitbook.io/documentation/.
32. Sun BB, Maranville JC, Peters JE, Stacey D, Staley JR, Blackshaw J, et al. Genomic Atlas of the Human Plasma Proteome. Nature (2018) 558(7708):73–9. doi: 10.1038/s41586-018-0175-2
33. Zheng X, O’Connell CM, Zhong W, Poston TB, Wiesenfeld HC, Hillier SL, et al. Gene Expression Signatures Can Aid Diagnosis of Sexually Transmitted Infection-Induced Endometritis in Women. Front Cell Infect Microbiol (2018) 8:307. doi: 10.3389/fcimb.2018.00307
34. Kotlyar M, Pastrello C, Malik Z, Jurisica I. IID 2018 Update: Context-Specific Physical Protein-Protein Interactions in Human, Model Organisms and Domesticated Species. Nucleic Acids Res (2019) 47(D1):D581–9. doi: 10.1093/nar/gky1037
35. Lee JC, Biasci D, Roberts R, Gearry RB, Mansfield JC, Ahmad T, et al. Genome-Wide Association Study Identifies Distinct Genetic Contributions to Prognosis and Susceptibility in Crohn’s Disease. Nat Genet (2017) 49(2):262–8. doi: 10.1038/ng.3755
Keywords: C-reactive protein (CRP), appendicitis, functional genetics, biomarker, quantitative trait
Citation: Ricaño-Ponce I, Peeters T, Matzaraki V, Houben B, Achten R, Cools P, Netea MG, Gyssens IC and Kumar V (2022) Impact of Human Genetic Variation on C-Reactive Protein Concentrations and Acute Appendicitis. Front. Immunol. 13:862742. doi: 10.3389/fimmu.2022.862742
Received: 26 January 2022; Accepted: 25 April 2022;
Published: 25 May 2022.
Edited by:
Ferhat Ay, La Jolla Institute for Immunology (LJI), United StatesReviewed by:
Lyubov E. Salnikova, Russian Academy of Sciences, RussiaCopyright © 2022 Ricaño-Ponce, Peeters, Matzaraki, Houben, Achten, Cools, Netea, Gyssens and Kumar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vinod Kumar, Vi5LdW1hckByYWRib3VkdW1jLm5s
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.