
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol., 12 July 2022
Sec. Alloimmunity and Transplantation
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.855730
This article is part of the Research TopicNovel treatments for Diffuse Large B-cell Lymphoma: the post-CART EraView all 6 articles
 Mariana Bastos-Oreiro1*
Mariana Bastos-Oreiro1* Antonio Gutierrez2
Antonio Gutierrez2 Juan Luís Reguera3
Juan Luís Reguera3 Gloria Iacoboni4Lucía López-Corral5
Gloria Iacoboni4Lucía López-Corral5 María José Terol6
María José Terol6 Valentín Ortíz-Maldonado7Jaime Sanz8
Valentín Ortíz-Maldonado7Jaime Sanz8 Luisa Guerra-Dominguez9Rebeca Bailen1
Luisa Guerra-Dominguez9Rebeca Bailen1 Alberto Mussetti10Pau Abrisqueta4Rafael Hernani6
Alberto Mussetti10Pau Abrisqueta4Rafael Hernani6 Hugo Luzardo9Juan-Manuel Sancho11Javier Delgado-Serrano3Antonio Salar12Carlos Grande13Leyre Bento2
Hugo Luzardo9Juan-Manuel Sancho11Javier Delgado-Serrano3Antonio Salar12Carlos Grande13Leyre Bento2 Sonia González de Villambrosía14Daniel García-Belmonte15
Sonia González de Villambrosía14Daniel García-Belmonte15 Anna Sureda10
Anna Sureda10 Antonio Pérez-Martínez16Pere Barba4Mi Kwon1Alejandro Martín García-Sancho5
Antonio Pérez-Martínez16Pere Barba4Mi Kwon1Alejandro Martín García-Sancho5Real-world evidence comparing the efficacy of chimeric antigen receptor (CAR) T-cell therapy against that of the previous standard of care (SOC) for refractory large B-cell lymphoma (LBCL) is scarce. We retrospectively collected data from patients with LBCL according to SCHOLAR-1 criteria treated with commercial CAR T-cell therapy in Spain (204 patients included and 192 treated, 101 with axicabtagene ciloleucel [axi-cel], and 91 with tisagenlecleucel [tisa-cel]) and compared the results with a historical refractory population of patients (n = 81) obtained from the GELTAMO-IPI study. We observed superior efficacy for CAR-T therapy (for both axi-cel and tisa-cel) over pSOC, with longer progression-free survival (PFS) (median of 5.6 vs. 4–6 months, p ≤ 0.001) and overall survival (OS) (median of 15 vs. 8 months, p < 0.001), independently of other prognostic factors (HR: 0.59 (95% CI: 0.44–0.80); p < 0.001] for PFS, and 0.45 [(95% CI: 0.31–0.64)] for OS). Within the CAR-T cohort, axi-cel showed longer PFS (median of 7.3 versus 2.8 months, respectively, p = 0.027) and OS (58% versus 42% at 12 months, respectively, p = 0.048) than tisa-cel. These differences were maintained in the multivariable analysis. On the other hand, axi-cel was independently associated with a higher risk of severe cytokine release syndrome and neurotoxicity. Our results suggest that the efficacy of CAR-T cell therapy is superior to pSOC in the real-world setting. Furthermore, axi-cel could be superior in efficacy to tisa-cel, although more toxic, in this group of refractory patients according to SCHOLAR-1 criteria.
Diffuse large B-cell lymphoma (DLBCL) is the most common non-Hodgkin’s lymphoma (NHL) (1, 2). The incorporation of the monoclonal antibody rituximab into first-line treatment regimens has led to improved survival of patients with DLBCL (3). However, approximately 40% of such patients will present refractory or relapsed (r/r) disease after the first-line treatment (4). Classically, the prognosis of patients with r/r DLBCL is poor, considering that salvage treatment followed by high-dose chemotherapy and autologous stem cell transplantation (auto-SCT) will be a curative option for only 20%–25% of patients (5–8).
The prognosis is especially poor for refractory patients, as was highlighted in the SCHOLAR-1 study, the largest retrospective analysis of this patient population (9). This study pooled data from two separate phase III clinical trials (the Lymphoma Academic Research Organization-CORAL and the Canadian Cancer Trials Group LY.12) and two observational cohorts (MD Anderson Cancer Center and the University of Iowa/Mayo Clinic Lymphoma Specialized Program of Research Excellence). Patients with DLBCL refractory to first-line or subsequent lines of therapy, or relapsing within 1 year after auto-SCT, had a very low chance of responding to the next line of treatment (26% overall response rate [ORR] and 7% complete response [CR]) and a median overall survival (OS) of only 6.3 months (9). These findings underscored the considerable unmet need for effective therapies for patients with refractory DLBCL and have served as benchmarks for assessing novel therapies in this patient population (10).
Chimeric antigen receptor (CAR) T-cell therapy constitutes a paradigm shift in the treatment of r/r DLBCL (11). Currently, two CAR T‐cell products targeting CD19 have been approved in Europe and three in the United States for treating r/r DLBCL after at least two lines of systemic therapy: axicabtagene ciloleucel (axi‐cel) (12, 13), tisagenlecleucel (tisa-cel) (14), and lisocabtagene maraleucel (liso-cel) (15) (16). The three pivotal single-arm phase II clinical trials evidenced highly encouraging results, showing complete response rates of 40%–58% and prolonged remission in 30%–40% of patients (12–16). These pivotal trials had important differences in the inclusion criteria as well as the study designs. In this sense, while the ZUMA-1 trial (axi-cel) included only refractory patients according to the SCHOLAR-1 criteria, the JULIET (tisa-cel) and TRANSFORM (liso-cel) trials included also non-refractory patients.
Real-world data on CAR-T therapy from various countries in Europe and the United States have shown similar efficacy to those of the pivotal trials (17–21). To date, there has been little evidence comparing CAR T-cell therapy in real world versus the previous standard of care (pSOC) of the pre-CAR era (17, 22). Moreover, none of the real-world evidence (RWE) studies have focused on analyzing refractory patients, the population of DLBCL with the highest unmet need.
In the present study, we aim to describe the global Spanish experience with CAR T-cell therapy in the commercial setting and compare these results with the historical treatment prior to the CAR T-cell therapy, focusing our analysis on refractory patients according to the Scholar-1 criteria.
We performed a multicenter, retrospective, observational study conducted in accordance with the Declaration of Helsinki and approved by the institutional ethics committee of Hospital Universitario Gregorio Marañón.
We included in the CAR-T cohort all adult patients treated with commercially available CAR-T cell products with aggressive B-cell lymphoma different from primary mediastinal large B-cell lymphoma (PMLBCL) who were registered in the GELTAMO/GETH-TC (Grupo Español de Linfomas y Trasplante Autólogo de Médula Ósea/Grupo Español de Trasplante Hematopoyético y Terapia Celular) database of patients treated with CAR T-cell therapy in eight Spanish centers between February 2019 and July 2021. All patients were judged eligible by the Expert Committee of the Spanish National Health System. Patients fulfilling SCHOLAR-1 criteria (9) for refractory disease (progressive disease as best response to any line of therapy, stable disease as best response to ≥4 cycles of first-line therapy or ≥2 cycles of later-line therapy, or relapse <12 months after auto-SCT) were identified and included in the primary analysis. Patient selection, supportive care, toxicity management, and response assessment followed institutional practices. Cytokine release syndrome (CRS) and neurotoxicity were graded according to the according to the ASTCT consensus criteria (23, 24).
This cohort was compared with a historical population of r/r DLBCL patients from the GELTAMO-IPI study, treated in the pre-CAR-T-cell therapy era (pSOC) (25). The GELTAMO-IPI study included patients from 20 academic and community hospitals in the GELTAMO network in Spain, diagnosed between 1998 and 2014, and treated with R-CHOP or more intense regimens with a curative intent. For the present study, centers were required to update the follow-up and additional data about the treatment at relapse or progression. Finally, nine centers (n = 9) agreed to participate in the present study. As previously mentioned for the CAR-T cohort, only patients who met at least one of the Sholar-1 refractory criteria were considered for this cohort as well.
The present analysis was based on a data cutoff on July 25, 2021, and March 1, 2019, for the CAR-T and pSOC cohorts, respectively. Descriptive statistics, including median, and interquartile range (IQR) for the continuous variables and percentages for the categorical variables, were obtained. To evaluate the association between two categorical variables, we employed Fisher’s exact test or the chi-squared test.
The median follow-up time (in months) was calculated for the surviving patients by the reverse Kaplan–Meier method. The time to event, overall survival (OS), and progression-free survival (PFS) were estimated using the Kaplan–Meier method, and comparisons between variables of interest were performed using the log-rank test. The OS for the ITT and infused populations was calculated from start of treatment for the pSOC cohort and apheresis and infusion date, respectively, until the date of death from any cause, censoring for patients alive at last contact. The PFS for the ITT and infused populations was calculated from failure to last treatment and infusion date, respectively, until the date of relapse, progression, or death from any cause, censoring for patients alive and progression-free at last contact. For the comparison analysis between the pSOC and ITT CAR-T cohorts, the survival was measured from the failure to last treatment in the patients fulfilling the Scholar-1 criteria. This analysis was exploratory, and p-values were not corrected for multiple testing. The specific cutoffs for several quantitative variables such as time to approval, apheresis or infusion, ferritin, and C-reactive protein (CRP) were calculated using receiver operating characteristic curves.
To assess the effect of important covariates on response and toxicity, we performed a multivariable logistic regression. We also performed a multivariate survival analysis with the variables that appeared to be significant in the univariate analysis (p < 0.05), according to the Cox proportional hazard regression model. All reported p-values were two-sided, and statistical significance was defined at p < 0.05. Analyses were performed using SPSS version 25 (SPSS, Chicago, IL).
From the initial population of 255 patients registered in the GELTAMO/GETH-TC database, 204 patients meeting the SCHOLAR-1 criteria for refractory disease were included in the intention-to-treat (ITT) analysis. Fifty-one patients were excluded due to non-refractory disease (15 patients), presence of PMLBCL histology (19 patients), histology different from aggressive B-cell lymphoma (4 patients), or lack of data or follow-up (13 patients) (Supplementary Figure 1).
Patient characteristics are shown in Table 1. Of the 204 refractory patients included in the ITT analysis, 192 (94%) were infused. The median time from official approval to infusion was 60 days (IQR: 49–73 days), and the median time from apheresis to infusion was 46.5 days (IQR: 39–55.7 days). For the infused patients, 101 were administered axi-cel and 91 were administered tisa-cel. Regarding the SCHOLAR-1 criteria in the ITT analysis, 64% of the patients were primary refractory, 82% were refractory to the last therapy, and 27% had an early relapse after auto-SCT. The most common histology included was DLBCL, not otherwise specified (NOS) (77%), followed by transformed follicular lymphoma (13%), high-grade B-cell lymphoma double or triple hit (9%), and high-grade B-cell lymphoma, NOS (1%). Seventeen patients (9%) had an Eastern Cooperative Oncology Group performance status (ECOG-PS) ≥2 pre-lymphodepletion, and 11 (5%) pre-apheresis. The revised IPI (R-IPI) was high (3–5) at diagnosis in 55% of the patients and pre-lymphodepletion in 54% of the patients. Bulky disease (more than 10 cm for the larger diameter) was present in 37% of the patients pre-apheresis. Almost one-third (29%) of the patients previously underwent auto-SCT. Eighty-two percent of the patients required bridging therapy. The most common bridging therapies were gemcitabine-based regimens (35%), cyclophosphamide-based regimens (24%), intense salvage regimens (R-ICE [rituximab plus ifosfamide, carboplatin, and etoposide], R-DHAP [rituximab plus dexamethasone, ara-C, and cisplatin], MINE [mesna, ifosfamide, mitoxantrone, and etoposide]) (13%), bendamustine-based regimens (10%), radiotherapy (5%), steroid monotherapy (5%), lenalidomide-based regimens (2%), nivolumab (1%), and brentuximab (1%).
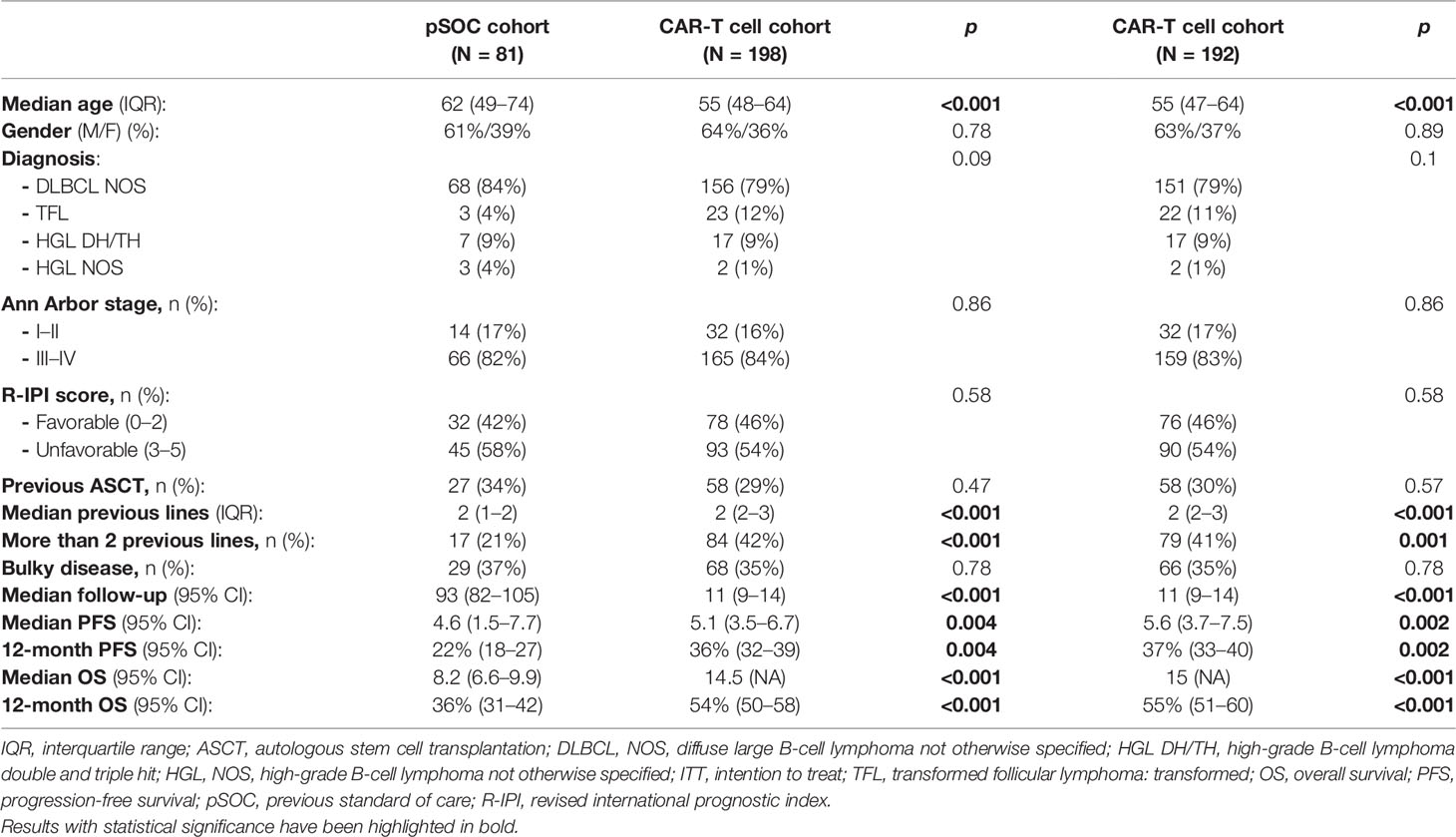
Table 1 Comparison of the previous standard-of-care (pSOC) cohort versus CAR-T cell, intention to treat (ITT), and infused cohorts.
As shown in Table 1, characteristics of the pSOC cohort were similar to those of the CAR-T cohort, except for age, which was significantly higher in the pSOC cohort. Similar to the CAR-T cohort, the most common histology included was DLBCL, NOS (84%). The R-IPI was high (3–5) at diagnosis in 58% of the patients. All patients received at least two lines of therapy, with 21% receiving more than three lines previous to the last therapy. Regarding the SCHOLAR-1 criteria, 50% of patients were primary refractory, 71% were refractory to the last therapy, and 17% had an early relapse after auto-SCT. The median number of lines was 2 (IQR: 1–2). The last therapies received were R-GemOx (19%), R-bendamustine (15%), R-ICE (13%), R-ESHAP (etoposide, methyl prednisolone, cytosine arabinoside, cisplatinum) (10%), mini-BEAM (BCNU, etoposide, cytosine arabinoside, melphalan) (5%), R-GIFOX (rituximab plus gemcitabine, ifosfamide, and oxaliplatin) (4%), lenalidomide (4%), and others (30%). One-third of the patients underwent hematopoietic auto-SCT (34%), and 8.6% underwent allogeneic transplantation.
The median follow-up was significantly longer for the pSOC cohort than for the CAR-T cohort (Table 1), 93 months vs. 11 months since start of treatment and apheresis, respectively. Refractory patients treated with CAR T-cells versus pSOC had significantly longer PFS (median of 5.1 and 5.6 vs. 4.6 months, p ≤ 0.001) and better OS (median of 14.5 and 15 vs. 8.2 months, p < 0.001), considering both the ITT and infused populations (Table 1; Figure 1). When analyzing separately by the various products versus pSOC, the differences were in favor of both products over the pSOC (Table 2; Figure 2), with a median PFS of 4.6 months (95% CI 2.9–8.5) for the pSOC cohort versus 8.5 months (95% CI 6.6–14.4) (p < 0.001) for axi-cel and 4.6 months (95% CI 4.3–8) (p = 0.074) for tisa-cel, and median OS of 8.2 months (95% CI 6.6–9.9) for the pSOC cohort versus not reached (p < 0.001) for axi-cel and 11.7 months (95% CI 7.8–15.6) (p = 0.015) for tisa-cel.
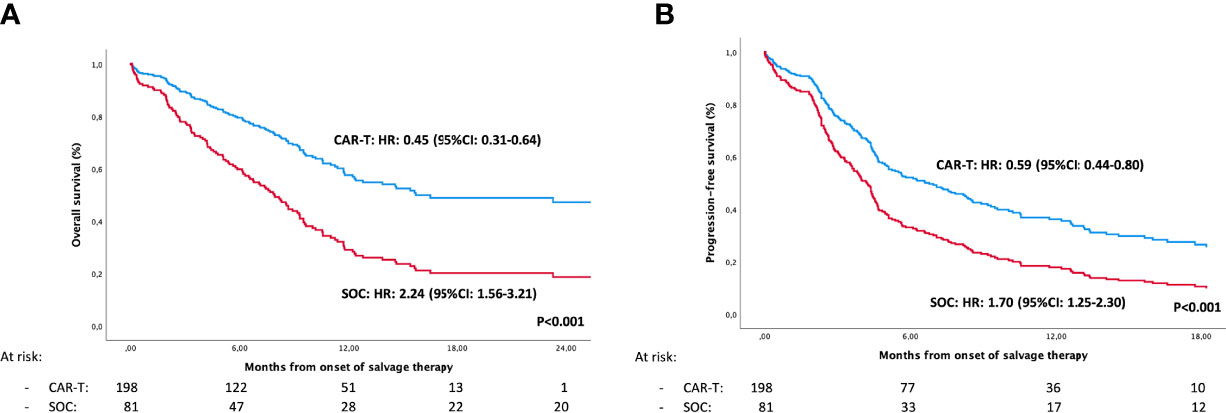
Figure 1 Intention to treat analysis of overall survival (A) and progression-free survival (B) in previous standard of care (pSOC) versus CAR-T cell cohorts, adjusted using a multivariable Cox regression model.
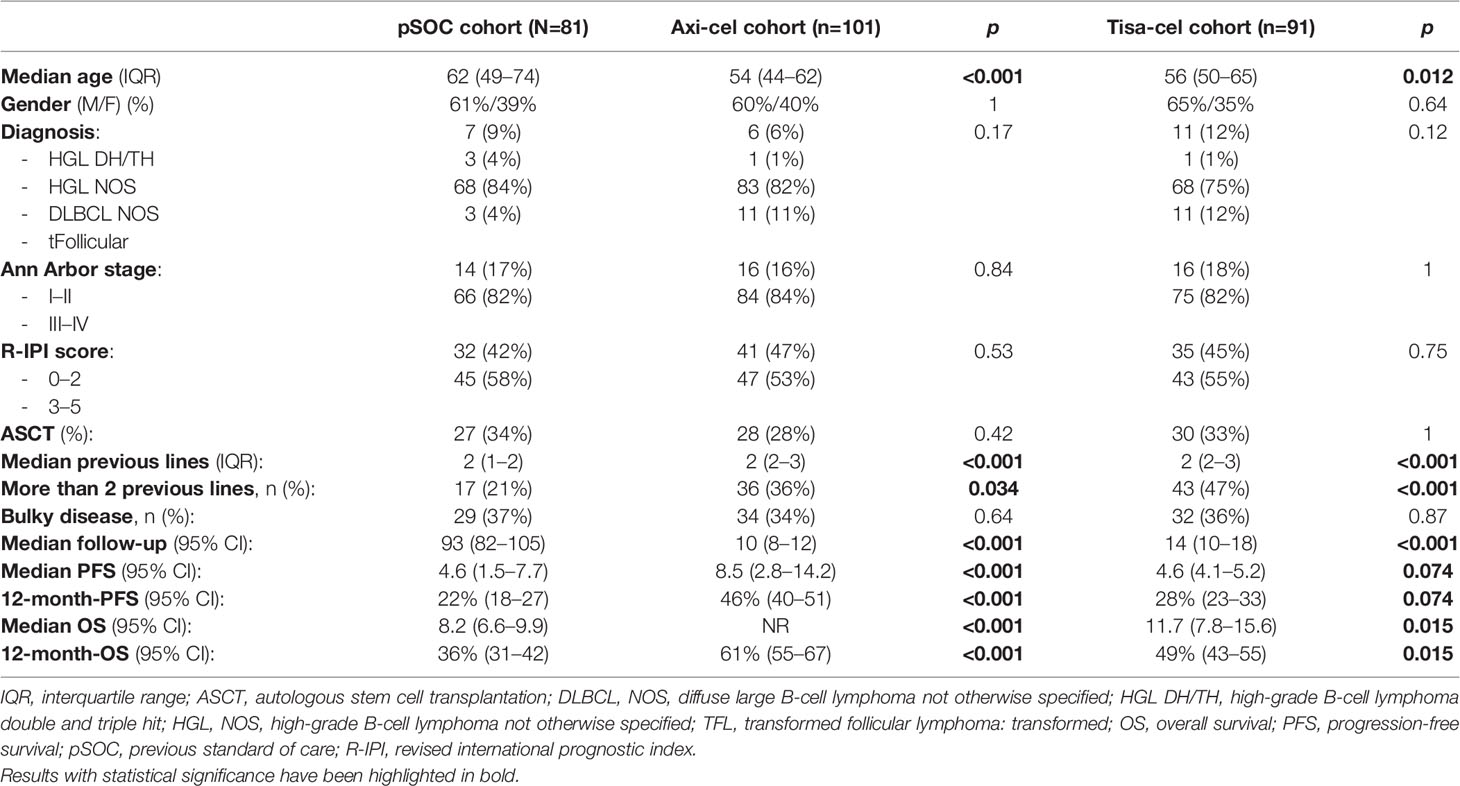
Table 2 Comparison of the previous standard-of-care (pSOC) cohort and infused CAR-T cell, axi-cell, and tisa-cel cohorts.
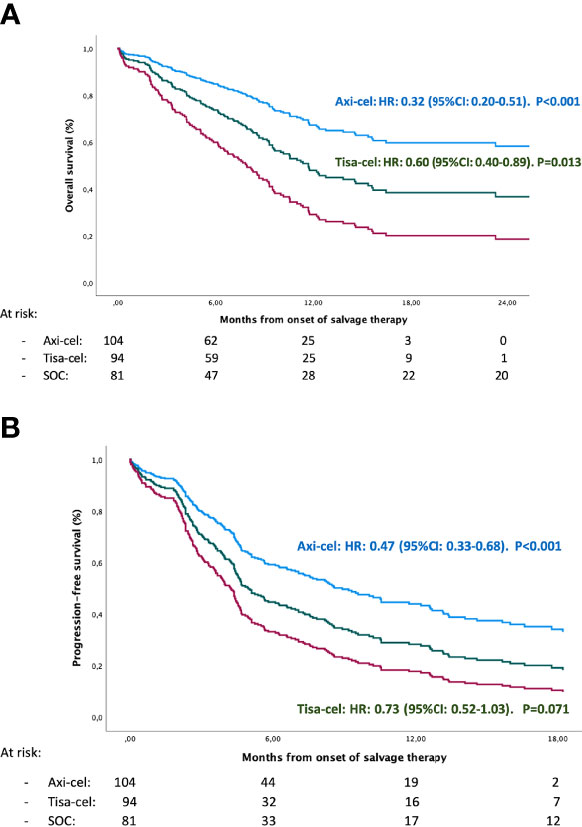
Figure 2 Overall survival (A) and progression-free survival (B) comparing: Axi-cel vs Tisa-cel vs previous Standardregression of care (pSOC) adjusted using a multivariable Cox regression model.
To account for possible imbalances between the groups, we performed a multivariate analysis using Cox regression, including all the patients from both cohorts. We found that pSOC therapy, as well as not having undergone auto-SCT, had a significant adverse impact on PFS and OS (Supplementary Table 1).
Table 3 shows the characteristics of the CAR-T cell cohort at diagnosis and at CAR T-cell therapy. The responses to CAR T-cell therapy are summarized in Supplementary Table 2. The best response rates after CAR T-cell infusion in this refractory group of patients meeting the Scholar-1 criteria (n = 192) were 36% for complete response, 24% for partial response, 7% for stable disease, and 22% for progressive disease (Supplementary Table 2).
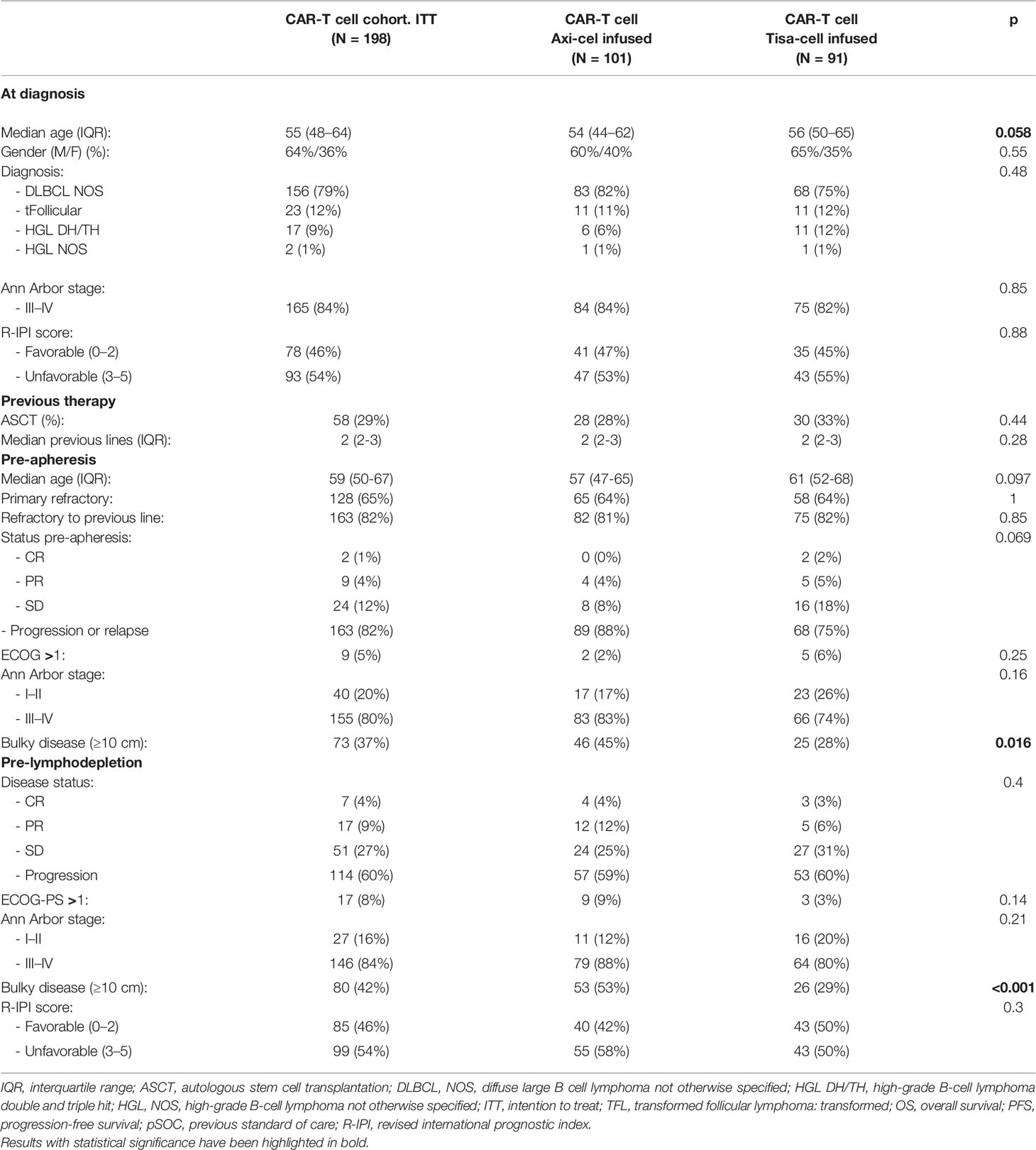
Table 3 CAR-T cell cohort characteristics: intention-to-treat and infused axi-cel and tisa-cel populations.
For all infused patients (n = 192), the median follow-up from infusion was 10 months (95% CI: 8–12 months), the median PFS was 3.3 months (95% CI 2–4.6), and the median OS was 11.8 months; the estimated 12-month PFS and OS were 35% (95% CI 27–42) and 50% (95% CI 41–59), respectively, and the 12-month PFS and OS for the patients who achieved complete response were 73% (95% CI 61–85) and 86% (95% CI 76–95), respectively. The factors affecting PFS and OS in the univariate analysis are shown in Table 4. In the multivariable analysis, the factors with independent adverse influence on PFS were CAR-T cell type (tisa-cel), unfavorable R-IPI at lymphodepletion, non-previous ASCT, and HCTCI (Hematopoietic Cell Transplantation-specific Comorbidity Index) 3–7 pre-lymphodepletion, and those for OS were CAR-T cell type (tisa-cel), unfavorable R-IPI at lymphodepletion, ECOG-PS 2–4 pre-apheresis, primary refractory disease, and HCTCI 3-7 pre-lymphodepletion (Table 5).
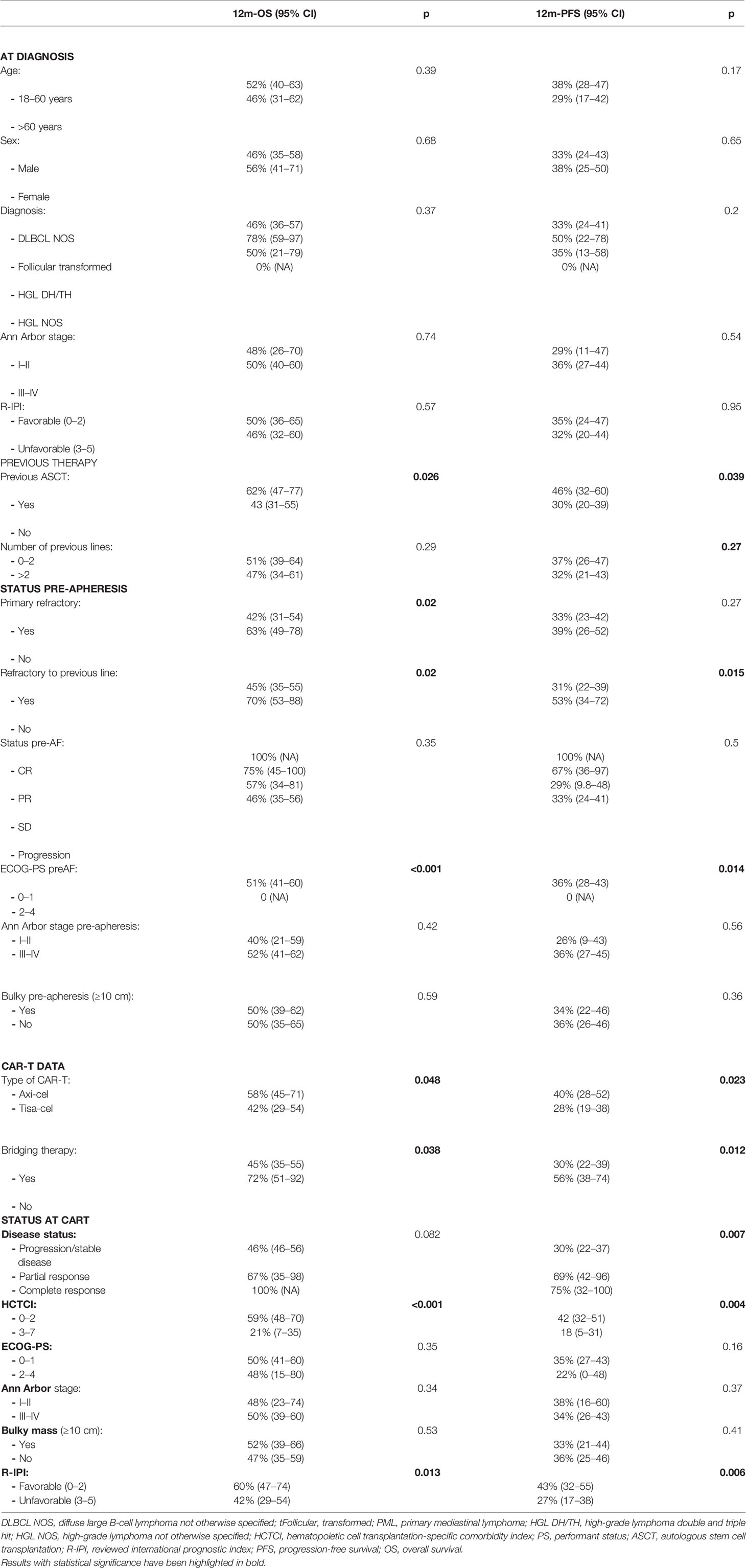
Table 4 Univariable analysis of survival in CAR-T-infused patients.
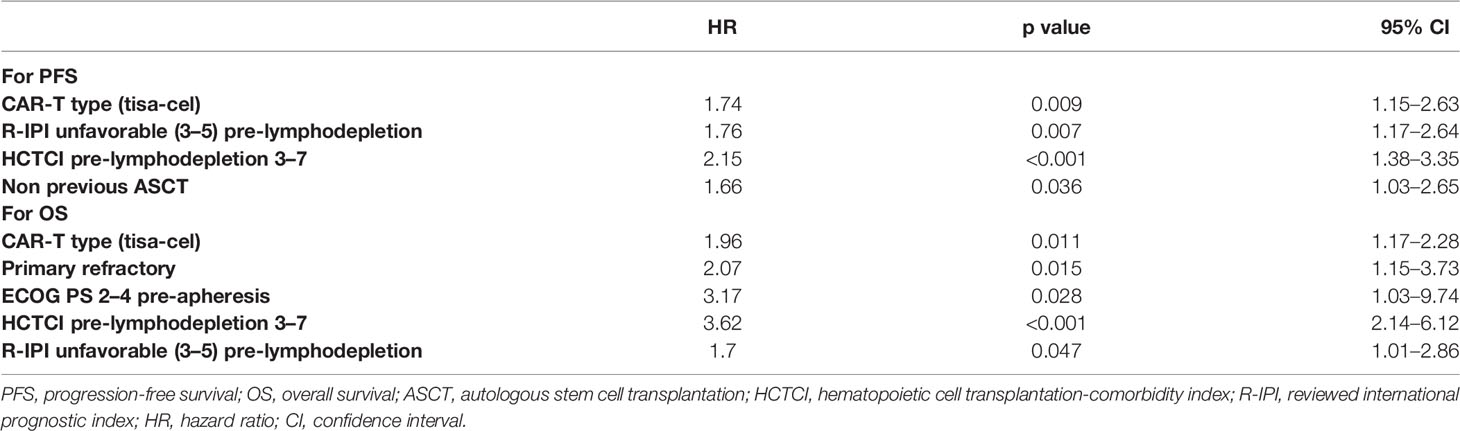
Table 5 Multivariable analysis of survival in CAR-T-infused patients.
For the infused patients (n = 192), axi-cel was superior to tisa-cel for PFS and OS, with a median PFS of 7.3 (95% CI 3.3–11.3) versus 2.8 months (95% CI 2.4–3.1) (p = 0.027), and median OS not reached (NR) versus 10 months (95% CI 6.6–13.4) (p = 0.048), respectively (Figure 3). Similarly, the 12-month PFS was 40% (95% CI 28–52) vs. 28% (95% CI 19–38) (p = 0.023), and the 12-month OS was 58% (95% CI 45–71) and 42% (95% CI 29–54) (p = 0.048) for axi-cel and tisa-cel cohorts, respectively (Tables 4, 5).
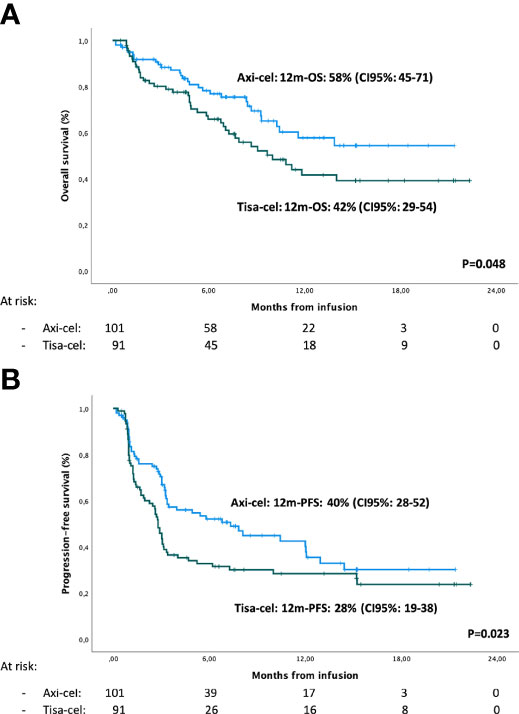
Figure 3 Overall survival (A) and progression-free survival (B) in axi-cel and tisa-cel cohorts.
A total of 78% of patients experienced some degree of CRS, with only 6% of cases grade 3 or more. The incidence of CRS was significantly higher in the patients treated with axi-cel than those treated with tisa-cel (90% vs. 65%, p < 0.001); however, the incidence of severe CRS did not differ between the two CAR-T cohorts (8% vs. 4%, p = 0.38). In terms of neurotoxicity, 29% of the patients had some degree of neurotoxicity, with 11% experiencing grade 3 or more. These events were more frequent with axi-cel than with tisa-cel: 42 (42%) vs. 13 (14%) patients, respectively (p < 0.001), and severe neurotoxicity occurred in 16 (16%) and 5 (5%) patients (p = 0.022), respectively. In the multivariable analysis, the factors identified as independently related to CRS were ferritin levels at lymphodepletion >673 UI/l (relative risk [RR] 2.5; 95% CI 1.1–5.6; p = 0.025) and having received axi-cel (RR 4.1; 95% CI 1.8–9.5; p = 0.001). For neurotoxicity, the factors were axi-cel (RR 5.4; 95% CI 2.3–12.5; p < 0.001) and a CRP >173 mg/l at lymphodepletion (RR 3.9; 95% CI 1.8–8.3; p < 0.001).
To our knowledge, this is the largest study comparing CAR T-cell therapy with pSOC in RWE. Although the clinical characteristics of the two cohorts differed, multivariate analysis identified an independent influence of treatment cohort on survival, suggesting a significant benefit of CAR-T cell therapy in patients with refractory DLBCL. In addition, as far as we know, we present the first series focused on refractory aBC-NHL patients according to SCHOLAR-1 criteria comparing axi-cel or tisa-cel in the RWE setting. The results of our multivariable analyses indicate better efficacy results for axi-cel compared with tisa-cel, but with increased toxicity.
Regarding the comparison with pSOC, the differences in favor of CAR T-cell therapy in terms OS were also maintained when comparing separately the two products (axi-cel and tisa-cel), although for PFS, statistically significant differences were only identified for axi-cel. In a recent single-center study, Sermer et al. analyzed the use of CAR T-cell therapy versus a historical control of alternative non-CAR T-cell regimens (22), and although they identified a clear benefit in favor of the former, the superiority of CAR T-cell therapy was not as clear in patients with unfavorable prognostic factors. However, in this study, the CAR-T arm had a small number of patients (n = 69) and a separate analysis of refractory patients was not performed. In the same vein, a recently published study compared the results of the SCHOLAR-1 study with the 2-year outcomes of ZUMA-1 (10). All patients in both cohorts fulfilled the SCHOLAR-1 refractoriness criteria, and propensity scoring was used to create balance between ZUMA-1 and SCHOLAR-1 patients. This study showed a notable benefit for axi-cel vs. non-CAR T-cell salvage regimens for patients with refractory DLBCL, with a 73% reduction in the risk of death for this group. In agreement with these results, our study found similar benefits for the CAR-T cohort, but without the selection bias that a clinical trial might incur, given that both cohorts of our study are from the real world. It is noteworthy that the follow-up of both cohorts is dissimilar, with less follow-up for the CAR-T cohort, which could result in a loss of late events in this cohort. However, it should be noted that 92% of the patients had at least 6 months of follow-up, and 68% at least 12 months.
A possible limitation of our study is that the historical cohort received treatment before 2014, mainly regimens based on chemotherapy and rituximab. However, this has been the only treatment available in Spain until very recently, since other options that are currently approved by the EMA, such as polatuzumab vedotin or tafasitamab, were not reimbursed in Spain at the time of designing this study. Further studies are needed to compare CAR-T cell treatment with these new treatment strategies. In addition, due to the high cost of these treatments, it would also be advisable to carry out pharmacoeconomic studies and try to identify the groups of patients that can benefit most from each treatment modality.
Regarding the efficacy and toxicity of CAR T-cell therapy, our results for response rates, PFS, and OS are similar to those of the pivotal trials (13–15) and other previously published RWE studies (17–20), with a best OR rate of 60%, a median PFS of 3.3 months, and a median OS of 11.8 months, with an estimated 12-month OS of 50%. We also observed similar rates of severe CRS (6%) and neurotoxicity (11%) than previously reported in RWE studies but rather less than those identified in the pivotal clinical trials, probably in relation to the anticipation of the use of tocilizumab and steroids. Notably, axi-cel was associated with a significantly higher risk of CRS and especially, severe neurotoxicity. This finding has been previously reported in the pivotal trials (13, 14) as well as in the RWE studies (17–20, 26), and several strategies to prevent neurotoxicity associated with axi-cel, such as prophylaxis with steroids or anakinra (27), are under investigation.
The multivariable analysis of prognostic factors in the CAR-T cell cohort showed, similarly to other studies (17, 18), that unfavorable R-IPI (3–5), ECOG-PS >1, and primary refractory disease had a negative impact on PFS and OS. Although the results in the primary refractory group were inferior, CAR T-cell therapy can lead to long-lasting remissions. Therefore, this subset of patients likely benefits the most from this therapy, if we take into account the poor results achieved with conventional therapy (9). Interestingly, an intermediate-/high-risk HCTCI score (28) was strongly associated with detrimental PFS and OS. This index, widely used in the context of allogeneic transplantation, has been little investigated in the CAR-T therapy setting and could be considered as a useful tool in this context of refractory patients.
When looking at the characteristics of the patients who received axi-cel and tisa-cel in our series, we found significant differences between the two cohorts. Younger patients and more frequently patients with bulky disease pre-apheresis were in the axi-cel group, which was probably related to a bias generated from the physician’s decision when indicating the therapy for this group of refractory patients. This bias could be detrimental to the axi-cel group, given that an association between bulky disease and poorer efficacy results has been identified (12, 17, 26). However, in our study, the efficacy of axi-cel was superior to that of tisa-cel, a finding confirmed in the multivariable analysis, suggesting that axi-cel could be a better option for patients with refractory disease according to SCHOLAR-1 criteria. This superior efficacy of axi-cel was also suggested in a recently published matching-adjusted indirect comparison between ZUMA-1 and JULIET trials, in which the authors concluded that axi-cel may have superior efficacy and greater toxicity than tisa-cel (29). However, this analysis had significant differences form ours because it evaluated clinical trials with different disease refractory definitions, inclusion and exclusion criteria, and study designs. In contrast, our study compared both products used in the commercial setting in a homogeneous population of refractory patients according to SCHOLAR-1 criteria.
The observational nature of our study implies that it is prone to unintentional bias and the effects of confounding variables. Overall and bearing in mind the study’s limitations, the data presented here indicate that the efficacy of CAR T-cell therapy in refractory patients, in terms of PFS and OS, is superior to that of the treatments available in the pre-CAR-T era. In addition, our analyses suggest that axi-cel could be more effective than tisa-cel in refractory patients according to SCHOLAR-1 criteria. Given the limitations of retrospective studies, these results should be confirmed in prospective randomized clinical trials.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the Gregorio Marañón Hospital Ethics Committee. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
MB-O, AMG-S, and AG were responsible for the conception and design. MB-O, AG, JR, GI, MT, VO-M, JS, LG-D, RB, AM, PA, RH, HL, J-MS, JD, ASa, CG, LB, SGdV, DG-B, AS, MK, and PB provided the patients and entered the data. MB-O, AMG-S, AG, MK, AS, PB, and AP-M were responsible for the data analysis and interpretation. MB-O, AMG-S, and AG wrote the manuscript. All authors reviewed the paper, gave final approval of the manuscript, and are accountable for all aspects of the work. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.855730/full#supplementary-material
Supplementary Table 1 | Univariable and Multivariable efficacy analysis including all patients, from pSOC and ITT CAR-T cohorts. DLBCL NOS: diffuse large B cell lymphoma not otherwise specified; PML: primary mediastinal lymphoma, HGL DH/TH: high-grade lymphoma doble and triple hit; HGL NOS high-grade lymphoma not otherwise specified. ASCT: autologous stem cell transplantation, R-IPI: reviewed international prognostic index. Multivariable analysis. All variables with a p value less than 0.05 were included in the multivariate analysis. PFS: progression free survival. OS: Overall survival; R-IPI: reviewed international prognostic index, ASCT autologous stem cell transplantation, SOC: standard of care; HR: haze ratio. CI confidence interval.
Supplementary Table 2 | Response rates in the CAR-T treated patients, including axi-cel and tisa-cel cohorts. ORR: overall response, CR: complete response, PR: partial response, SD: stable disease. PD: progressive disease, NA not available.
1. Teras LR, DeSantis CE, Cerhan JR, Morton LM, Jemal A, Flowers CR. 2016 US Lymphoid Malignancy Statistics by World Health Organization Subtypes. CA Cancer J Clin (2016) 66(6):443–459. doi: 10.3322/caac.21357
2. Bastos-Oreiro M, Muntañola A, Panizo C, Gonzalez-Barca E, de Villambrosia SG, Córdoba R, et al. RELINF: Prospective Epidemiological Registry of Lymphoid Neoplasms in Spain. A Project From the GELTAMO Group. Ann Hematol abril (2020) 99(4):799–808. doi: 10.1007/s00277-020-03918-6
3. Tilly H, Gomes da Silva M, Vitolo U, Jack A, Meignan M, Lopez-Guillermo A, et al. Diffuse Large B-Cell Lymphoma (DLBCL): ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Annals of Oncology. Annals of Oncology (2015) 26:v116–25. doi: 10.1093/annonc/mdv304
4. Bartlett NL, Wilson WH, Jung S-H, Hsi ED, Maurer MJ, Pederson LD, et al. Dose-Adjusted EPOCH-R Compared With R-CHOP as Frontline Therapy for Diffuse Large B-Cell Lymphoma: Clinical Outcomes of the Phase III Intergroup Trial Alliance/CALGB 50303. J Clin Oncol (2019) 37(21):1790–9. doi: 10.1200/JCO.18.01994
5. Martín A, Conde E, Arnan M, Canales MA, Deben G, Sancho JM, et al. R-ESHAP as Salvage Therapy for Patients With Relapsed or Refractory Diffuse Large B-Cell Lymphoma: The Influence of Prior Exposure to Rituximab on Outcome. A GEL/TAMO study Haematologica (2008) 93(12):1829–36. doi: 10.3324/haematol.13440
6. Gisselbrecht C, Glass B, Mounier N, Singh Gill D, Linch DC, Trneny M, et al. Salvage Regimens With Autologous Transplantation for Relapsed Large B-Cell Lymphoma in the Rituximab Era. J Clin Oncol (2010) 28(27):4184–90. doi: 10.1200/JCO.2010.28.1618
7. Crump M, Kuruvilla J, Couban S, MacDonald DA, Kukreti V, Kouroukis CT, et al. Randomized Comparison of Gemcitabine, Dexamethasone, and Cisplatin Versus Dexamethasone, Cytarabine, and Cisplatin Chemotherapy Before Autologous Stem-Cell Transplantation for Relapsed and Refractory Aggressive Lymphomas: NCIC-CTG LY.12. J Clin Oncol (2014) 32(31):3490–6. doi: 10.1200/JCO.2013.53.9593
8. van Imhoff GW, McMillan A, Matasar MJ, Radford J, Ardeshna KM, Kuliczkowski K, et al. Ofatumumab Versus Rituximab Salvage Chemoimmunotherapy in Relapsed or Refractory Diffuse Large B-Cell Lymphoma: The ORCHARRD Study. J Clin Oncol (2017) 35(5):544–51. doi: 10.1200/JCO.2016.69.0198
9. Crump M, Neelapu SS, Farooq U, Van Den Neste E, Kuruvilla J, Westin J, et al. Outcomes in Refractory Diffuse Large B-Cell Lymphoma: Results From the International SCHOLAR-1 Study. Blood (2017) 130(16):1800–8. doi: 10.1182/blood-2017-03-769620
10. Neelapu SS, Locke FL, Bartlett NL, Lekakis LJ, Reagan P, Miklos DB, et al. Comparison of 2-Year Outcomes With CAR T Cells (ZUMA-1) Versus Salvage Chemotherapy in Refractory Large B-Cell Lymphoma. Blood Adv (2021) 5(20):4149–55. doi: 10.1182/bloodadvances.2020003848
11. Sehn LH, Salles G. Diffuse Large B-Cell Lymphoma. N Engl J Med (2021) 384(9):842–58. doi: 10.1056/NEJMra2027612
12. Locke FL, Ghobadi A, Jacobson CA, Miklos DB, Lekakis LJ, Oluwole OO, et al. Long-Term Safety and Activity of Axicabtagene Ciloleucel in Refractory Large B-Cell Lymphoma (ZUMA-1): A Single-Arm, Multicentre, Phase 1-2 Trial. Lancet Oncol (2019) 20(1):31–42. doi: 10.1016/S1470-2045(18)30864-7
13. Neelapu SS, Locke FL, Bartlett NL, Lekakis LJ, Miklos DB, Jacobson CA, et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N Engl J Med (2017) 377(26):2531–44. doi: 10.1056/NEJMoa1707447
14. Schuster SJ, Bishop MR, Tam CS, Waller EK, Borchmann P, McGuirk JP, et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N Engl J Med (2019) 380(1):45–56. doi: 10.1056/NEJMoa1804980
15. Abramson JS, Palomba ML, Gordon LI, Lunning MA, Wang M, Arnason J, et al. Lisocabtagene Maraleucel for Patients With Relapsed or Refractory Large B-Cell Lymphomas (TRANSCEND NHL 001): A Multicentre Seamless Design Study. Lancet (2020) 396(10254):839–52. doi: 10.1016/S0140-6736(20)31366-0
16. Westin JR, Kersten MJ, Salles G, Abramson JS, Schuster SJ, Locke FL, et al. Efficacy and Safety of CD19-Directed CAR-T Cell Therapies in Patients With Relapsed/Refractory Aggressive B-Cell Lymphomas: Observations From the JULIET, ZUMA-1, and TRANSCEND Trials. Am J Hematol (2021) 96(10):1295–312. doi: 10.1002/ajh.26301
17. Nastoupil LJ, Jain MD, Feng L, Spiegel JY, Ghobadi A, Lin Y, et al. Standard-Of-Care Axicabtagene Ciloleucel for Relapsed or Refractory Large B-Cell Lymphoma: Results From the US Lymphoma CAR T Consortium. J Clin Oncol (2020) 38(27):3119–28. doi: 10.1200/JCO.19.02104
18. Jacobson CA, Hunter BD, Redd R, Rodig SJ, Chen P-H, Wright K, et al. Axicabtagene Ciloleucel in the Non-Trial Setting: Outcomes and Correlates of Response, Resistance, and Toxicity. J Clin Oncol (2020) 38(27):3095–106. doi: 10.1200/JCO.19.02103
19. Pasquini MC, Hu Z-H, Curran K, Laetsch T, Locke F, Rouce R, et al. Real-World Evidence of Tisagenlecleucel for Pediatric Acute Lymphoblastic Leukemia and non-Hodgkin Lymphoma. Blood Adv (2020) 4(21):5414–24. doi: 10.1182/bloodadvances.2020003092
20. Iacoboni G, Villacampa G, Martinez-Cibrian N, Bailén R, Lopez Corral L, Sanchez JM, et al. Real-World Evidence of Tisagenlecleucel for the Treatment of Relapsed or Refractory Large B-Cell Lymphoma. Cancer Med (2021) 10(10):3214–23. doi: 10.1002/cam4.3881
21. Sesques P, Ferrant E, Safar V, Wallet F, Tordo J, Dhomps A, et al. Commercial Anti-CD19 CAR T Cell Therapy for Patients With Relapsed/Refractory Aggressive B Cell Lymphoma in a European Center. Am J Hematol (2020) 95(11):1324–33. doi: 10.1002/ajh.25951
22. Sermer D, Batlevi C, Palomba ML, Shah G, Lin RJ, Perales M-A, et al. Outcomes in Patients With DLBCL Treated With Commercial CAR T Cells Compared With Alternate Therapies. Blood Adv (2020) 4(19):4669–78. doi: 10.1182/bloodadvances.2020002118
23. Neelapu SS, Tummala S, Kebriaei P, Wierda W, Gutierrez C, Locke FL, et al. Chimeric Antigen Receptor T-Cell Therapy - Assessment and Management of Toxicities. Nat Rev Clin Oncol (2018) 15(1):47–62. doi: 10.1038/nrclinonc.2017.148
24. Lee DW, Santomasso BD, Locke FL, Ghobadi A, Turtle CJ, Brudno JN, et al. ASTCT Consensus Grading for Cytokine Release Syndrome and Neurologic Toxicity Associated With Immune Effector Cells. Biol Blood Marrow Transpl (2019) 25(4):625–38. doi: 10.1016/j.bbmt.2018.12.758
25. Montalbán C, Díaz-López A, Dlouhy I, Rovira J, Lopez-Guillermo A, Alonso S, et al. Validation of the NCCN-IPI for Diffuse Large B-Cell Lymphoma (DLBCL): The Addition of β2 -Microglobulin Yields a More Accurate GELTAMO-IPI. Br J Haematol (2017) 176(6):918–28. doi: 10.1182/bloodadvances.2020003001
26. Vercellino L, Di Blasi R, Kanoun S, Tessoulin B, Rossi C, D’Aveni-Piney M, et al. Predictive Factors of Early Progression After CAR T-Cell Therapy in Relapsed/Refractory Diffuse Large B-Cell Lymphoma. Blood Adv (2020) 4(22):5607–15. doi: 10.1182/bloodadvances.2020003001
27. Park JH, Sauter CS, Palomba ML, Shah GL, Dahi PB, Lin RJ, et al. A Phase II Study of Prophylactic Anakinra to Prevent CRS and Neurotoxicity in Patients Receiving CD19 CAR T Cell Therapy for Relapsed or Refractory Lymphoma. Blood (2021) 138(Supplement 1):96. doi: 10.1182/blood-2021-150431
28. Sorror ML, Maris MB, Storb R, Baron F, Sandmaier BM, Maloney DG, et al. Hematopoietic Cell Transplantation (HCT)-Specific Comorbidity Index: A New Tool for Risk Assessment Before Allogeneic HCT. Blood (2005) 106(8):2912–9. doi: 10.1182/blood-2005-05-2004
Keywords: refractory aggressive B cell lymphoma, CAR-T cell therapy, standard of care (SOC), real world evidence (RWE), scholar-1 criteria
Citation: Bastos-Oreiro M, Gutierrez A, Reguera JL, Iacoboni G, López-Corral L, Terol MJ, Ortíz-Maldonado V, Sanz J, Guerra-Dominguez L, Bailen R, Mussetti A, Abrisqueta P, Hernani R, Luzardo H, Sancho J-M, Delgado-Serrano J, Salar A, Grande C, Bento L, González de Villambrosía S, García-Belmonte D, Sureda A, Pérez-Martínez A, Barba P, Kwon M and Martín García-Sancho A (2022) Best Treatment Option for Patients With Refractory Aggressive B-Cell Lymphoma in the CAR-T Cell Era: Real-World Evidence From GELTAMO/GETH Spanish Groups. Front. Immunol. 13:855730. doi: 10.3389/fimmu.2022.855730
Received: 15 January 2022; Accepted: 27 May 2022;
Published: 12 July 2022.
Edited by:
Christian Koenecke, Hannover Medical School, GermanyReviewed by:
Pouya Safarzadeh Kozani, Guilan University of Medical Sciences, IranCopyright © 2022 Bastos-Oreiro, Gutierrez, Reguera, Iacoboni, López-Corral, Terol, Ortíz-Maldonado, Sanz, Guerra-Dominguez, Bailen, Mussetti, Abrisqueta, Hernani, Luzardo, Sancho, Delgado-Serrano, Salar, Grande, Bento, González de Villambrosía, García-Belmonte, Sureda, Pérez-Martínez, Barba, Kwon and Martín García-Sancho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mariana Bastos-Oreiro, bWFyaWFuYWJlYXRyaXouYmFzdG9zQHNhbHVkLm1hZHJpZC5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.