 Chao Luo
Chao Luo Shunlin Peng
Shunlin Peng Mao Li
Mao Li Xudong Ao
Xudong Ao Zhiqing Liu
Zhiqing Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Immunol. , 19 May 2022
Sec. Microbial Immunology
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.848279
Background: Probiotics have proven beneficial in a number of immune-mediated and allergic diseases. Several human studies have evaluated the efficacy and safety of probiotics in allergic rhinitis; however, evidence for their use has yet to be firmly established.
Objective: We undertook a systematic review and meta-analysis aiming to address the effect and safety of probiotics on allergic rhinitis.
Methods: We systematically searched databases [MEDLINE (PubMed), Embase, and the Cochrane Central Register of Controlled Trials] from inception until June 1, 2021. Qualified literature was selected according to inclusion and exclusion criteria, the data were extracted, and a systematic review and meta-analysis was conducted.
Results: Twenty-eight studies were included. The results showed that probiotics significantly relieved allergic rhinitis symptoms (standardized mean difference [SMD], −0.29, 95% confidence interval (CI) [−0.44, −0.13]; p = 0.0003, I2 = 89%), decreased Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) scores compared with the control group (SMD, −0.64, 95% CI [−0.79, −0.49], p < 0.00001, I2 = 97%), and increased T helper cell 1(Th1)/Th2 ratio (mean difference [MD], −2.47, 95% CI [−3.27, −1.68], p < 0.00001, I2 = 72%). There was no significant change in overall or specific IgE levels between probiotic-treated and placebo-treated subjects (SMD, 0.09, 95% CI [−0.16, 0.34], I2 = 0%, and SMD, −0.03, 95% CI [−0.18, 0.13], p = 0.72, I2 = 0%, respectively).
Conclusions: To sum up, probiotic supplement seems to be effective in ameliorating allergic rhinitis symptoms and improving the quality of life, but there is high heterogeneity in some results after subgroup analysis and clinicians should be cautious when recommending probiotics in treating allergic rhinitis.
Systematic Review Registration: https://www.crd.york.ac.uk/PROSPERO/, PROSPERO (CRD42021242645).
Allergic rhinitis (AR) is characterized by a nasal sensitive inflammation, which is estimated to already affect 10%–40% of the worldwide population (1, 2). Common symptoms of AR are nasal itching, sneezing, rhinorrhea, and nasal congestion. In addition, some patients experience symptoms of allergic rhinoconjunctivitis, such as watery or itchy or red eyes. Severe AR can affect the quality of life, sleep, and work performance (1).
In 1989, Strachan found that the number of siblings was inversely related to the prevalence of hay fever among peers in the UK. Then, he proposed the “Hygiene hypothesis” (3), that the changed intestinal microbiota due to the lack of contact with infectious sources, parasites, and symbiotic microorganisms affects the normal development of immune system. The “Hygiene hypothesis” extends to the “Old Friends” and the “Microflora hypothesis” (4, 5). The “Microflora hypothesis” believes that a diverse gut microbiota plays an important role in shaping host immune development and that disruption or dysbiosis of the normal gut microbiota contributes to the development of immune disorders such as allergic diseases (6, 7). Host–microbes symbiosis plays a cardinal role in maintaining health and immune homeostasis. Changes in the intestinal flora are considered to be one of the most important indicators of allergic diseases (8, 9). Probiotics are live bacteria that colonize the gastrointestinal tract and they provide a health benefit to the host when administered in adequate amounts (10). Recent studies have shown that probiotics are non-pharmaceutical agents that can increase the production of systemic IFN, IL10, and IL12, improve the pre-Th1 immune response, and reduce Th2 cytokines (11), and thus have been proposed as modulators of the allergic response and advocated as therapeutic and preventive interventions for allergic disease (12, 13).
Probiotics include the Lactobacillus group (L. rhamnosus GG, L. sporogenes, L. reuteri RC-14, L. plantarum 299v, L. acidophilus, and L. lactis), the Bifidobacterium group (B. bifidum, B. longum, and B. infantis), the Streptococcus group (S. thermophilus, S. lactis, and S. fecalis), and non-bacterial organisms (non-pathogenic yeast Saccharomyces boulardii). The most common probiotics are the Lactobacillus and Bifidobacterium groups (14). Many studies have attempted to assess the role of probiotics in the treatment of AR with inconsistent findings. While some have found a protective effect of probiotics on AR (15–18), several others have found no association (19, 20). Given that there have been further published studies, we undertook a systematic review and meta-analysis aiming to address the effect and safety of probiotics on AR, and meanwhile, we attempted to explore the possible causes of between-study heterogeneity via subgroup.
The protocol of this systematic review and meta-analysis has been registered on the PROSPERO platform with an assigned registration number CRD42021242645, based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols statement guidelines. This research was conducted based on this protocol.
We have performed a search in MEDLINE (PubMed), Embase, and the Cochrane Central Register of Controlled Trials. Additional studies will be sought by manually checking the references of included studies and relevant reviews. Searches will be restricted to publications appearing from inception to June 1, 2021. We used subject (“Rhinitis, Allergic”, “Rhinitis, Allergic, Seasonal”, “Rhinitis, Allergic, perennial”, “prebiotics”,” probiotics”) and free words (“Seasonal Allergic Rhinitis”, “Pollen Allergy” “Pollinosis”, “Hay Fever”, “allergic rhinitis”, “Perennial Allergic Rhinitis”, “prebiotics”,” probiotics”) to search in the databases aforementioned. The search strategy was as follows, taking PubMed as an example:
(1) (Seasonal Allergic Rhinitis [MeSH Terms]) OR (Perennial Allergic Rhinitis [MeSH Terms]) OR (Allergic Rhinitides, Seasonal) OR (Allergic Rhinitis, Seasonal) OR (Rhinitides, Seasonal Allergic) OR (Rhinitis, Seasonal Allergic) OR (Seasonal Allergic Rhinitides) OR (Pollen Allergy)) OR (Allergies, Pollen) OR (Allergy, Pollen)) OR (Pollen Allergies) OR (Pollinosis)) OR (Pollinoses) OR (Hay Fever)) OR (Fever, Hay) OR (Perennial Allergic Rhinitis) OR (Allergic Rhinitis, Perennial).
(2) (Probiotics [MeSH Terms]) OR (Prebiotics [MeSH Terms]) OR(Probiotics) OR (Prebiotics).
(3) (1) AND (2).
Studies were included if they met all of the following criteria (1): study design: experimental (randomized and quasi-randomized controlled trials) studies (2); study participants: participants with AR (3); intervention: the intervention group/s should receive probiotics supplementation in any dosage, or regimen as decided by the trialists of the respective trials (4); comparator(s)/control: the participants in the comparison group/s might receive a placebo or other drugs (5); if other drugs were used in the treatment group, they must also be used in the control group in the same way; and (6) language: articles published in the English language.
Articles were excluded if they were published in the form of conference abstract, case report, case series, letter to the editor, correspondence, editorial, narrative reviews, systematic reviews, and meta-analyses.
Two investigators independently reviewed titles, abstracts, and full-text articles according to the aforementioned inclusion and exclusion criteria. Disagreement was resolved through discussion or a third investigator. The same two investigators extracted the following data from each selected study: literature characteristics (the first author’s name, journal, year of publication, and study design); participant information (age and sample size); intervention information (intervention duration and comparison group components); outcome (AR and related adverse events); and conclusion.
The risk of bias assessment was conducted through The Cochrane Risk of Bias Tool Version 1 (21) in Review manager 5.3.4 software by CL and ML. Any disagreement was settled through consultation with the author SP.
Statistical analyses were completed using Review Manager 5.3.4 software (RevMan; Version 5.3.4. Copenhagen, Denmark: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). We chose the mean difference (MD) and standardized mean difference (SMD) for continuous outcomes. MD is the difference between the two means, which eliminates the influence of the absolute value between multiple studies. SMD can be simply understood as the quotient of the difference between the two means divided by the combined standard deviation, which not only eliminates the influence of the absolute value of multiple studies, but also eliminates the different effects of multiple study measurement units. Statistical heterogeneity was judged using the inconsistency index (I2), and significant heterogeneity was reported if the I2 is over 50%. The fixed-effect model was be used in this meta-analysis because larger sample studies will receive greater weight and provide greater contributions to pooled effects. Subgroup analyses were conducted to explore the source of heterogeneity. Publication bias assessment was conducted through funnel plots if more than 10 trials were included. Sensitivity analysis was used to explore the stability of the results. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) Working Group was used to assess the evidence quality for outcomes across studies.
The initial search was completed on June 1, 2021. We have identified 245 potentially relevant publications from PubMed, 580 from Embase, and 129 from The Cochrane Central Register of Controlled Trials. Endnote was used to eliminate duplicate publications, resulting in 97 records for review. After excluding publications that did not meet the inclusion or the exclusion criteria, we included 28 studies for systematic review and meta-Analysis. A flow diagram illustrating the exclusion of articles with specific reasons is shown in Figure 1 (PRISMA flowchart).
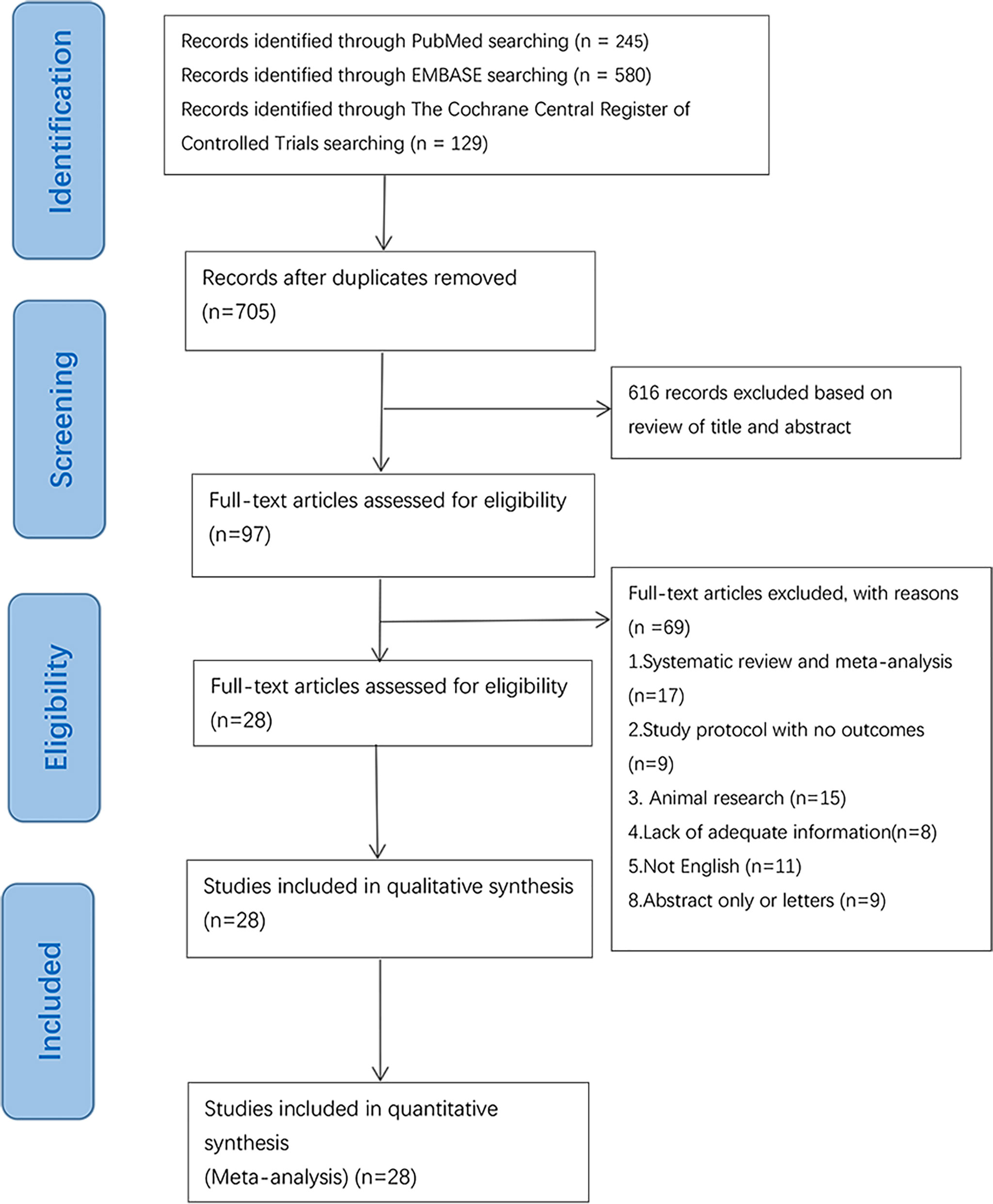
Figure 1 Flowchart of database searching and study identification.
Twenty-eight trials were included in the systematic analysis and meta-analysis. The main characteristics of the individual studies are shown in Table 1. Overall, one of these RCTs was a multicenter study (42). Twenty-eight studies included patients from 2 to 65 years of age. Fifteen studies included adults (age > 18 years old) (15–17, 25, 27, 28, 30, 32, 33, 36, 37, 40–42, 44), and eleven studies included children or teenagers (age < 18 years old) (18, 20, 23, 24, 26, 29, 34, 35, 38, 39, 43), and two studies included adults and children (22, 31). Fourteen studies included patients with seasonal allergic rhinitis (SAR) (15–18, 22, 25, 27, 29, 32, 33, 37, 39, 40, 44). Eleven studies included patients with perennial allergic rhinitis (PAR) (20, 23, 24, 28, 31, 32, 34, 36, 38, 41, 42) and three studies included patients with SAR and PAR (26, 30, 43). The intervention group of fourteen studies used Lactobacillus strains (17, 20, 22–24, 26–28, 30, 32, 33, 35, 37, 44), and four studies used Bifidobacterium strains (16, 25, 36, 39). Three studies used both Bifidobacterium strains and Lactobacillus strains (18, 40, 42). The other three studies used Tetragenococcus halophilus Th22 (31), E. coli Nissle 1917 (15), and Broncho-Vaxom (41), respectively. Three studies used probiotics combined with antihistamines (29, 34, 38). One study used Bifidobacterium strains and Enterococcus faecium (43). The treatment time of probiotics ranged from 6 weeks to 6 months.

Table 1 Study characteristics.
The risk of bias assessment is presented in Figures 2, 3. Most studies did not clearly show how to generate random sequences, nor did they clearly state whether association obfuscation was performed. In terms of masking method, most of the studies have insufficient information to permit judgment of “Low risk” or “High risk”. We assessed three trials having high risk of bias for different reasons. One of the trials did not report all the pre-specified primary outcome indicators (30). The random allocation method in one of the studies was incorrect (The patients were randomized according to the birth date) (41). Since Nagata reported that participants were all female college students from the same university in the trial (33), it was marked as “high risk” in other bias.
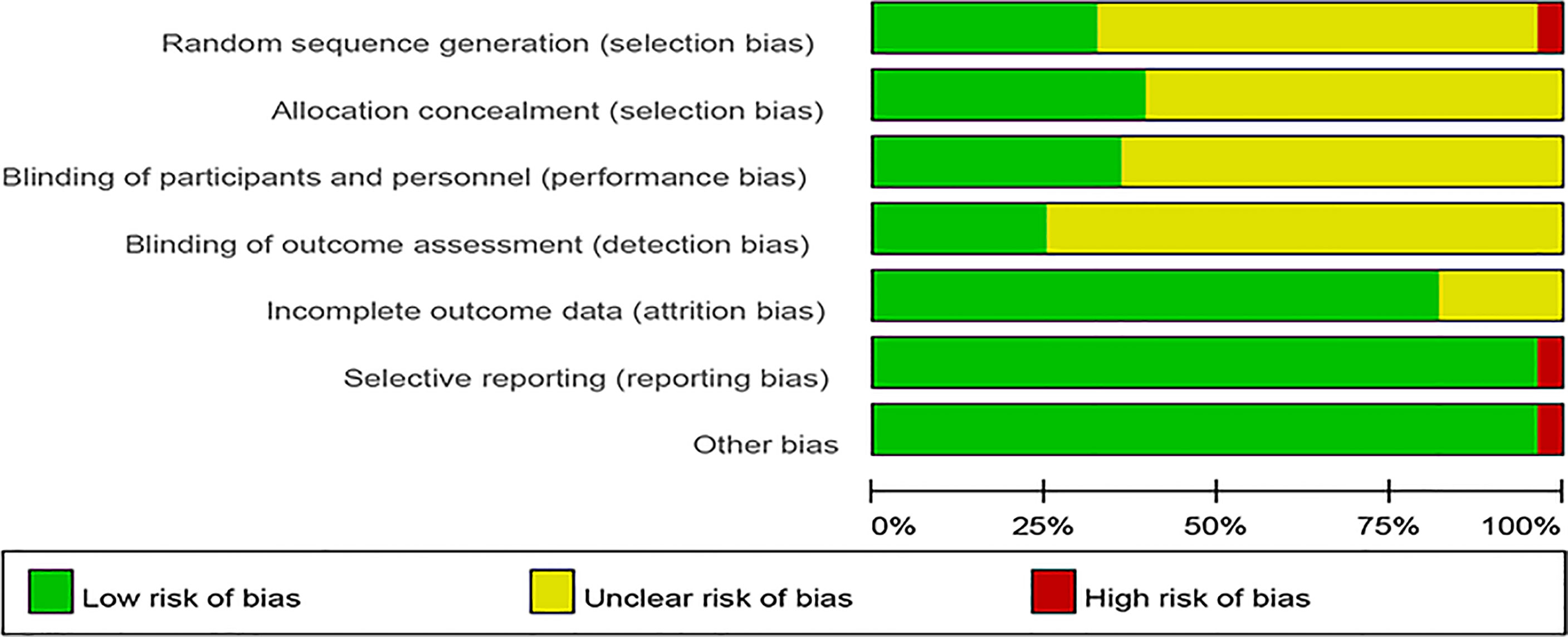
Figure 2 Risk of bias.
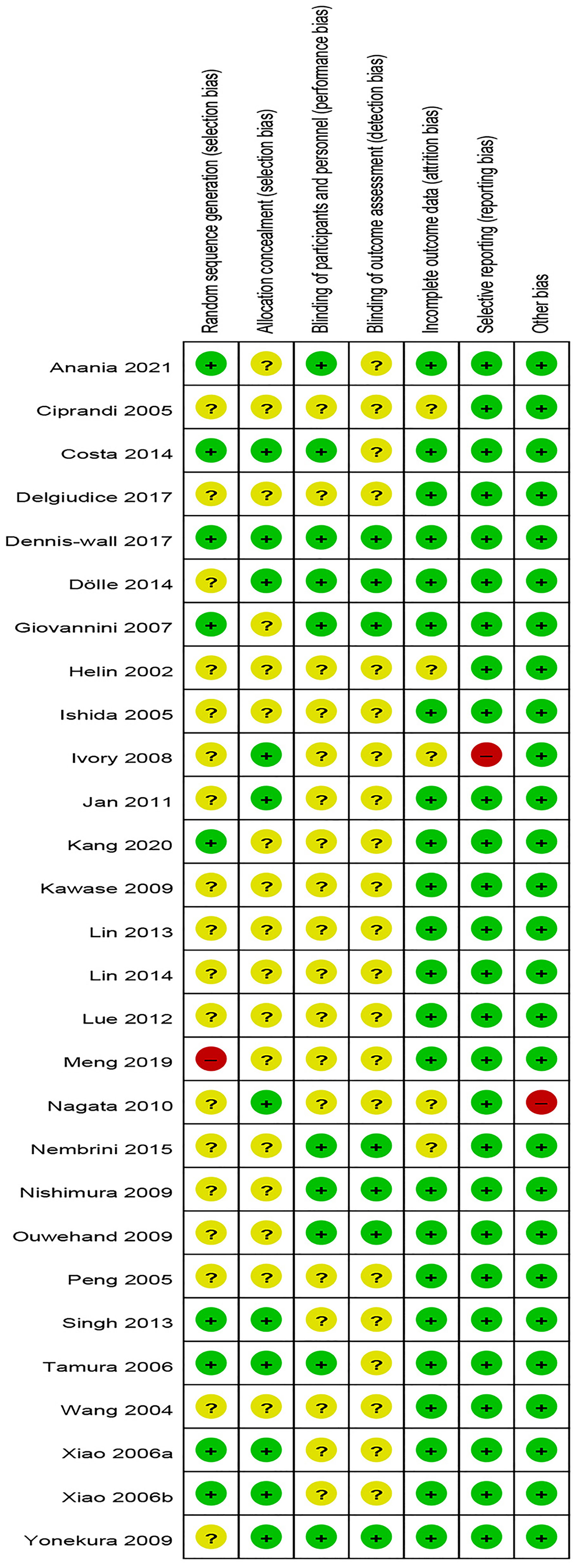
Figure 3 Summary of risk of bias.
AR symptoms score included rhinoconjunctivitis total symptom score (RTSS) and total nasal symptom scores (TNSS). RTSS includes five individual AR symptoms (nasal congestion, sneezing, rhinorrhea, nasal pruritus, and eye itching) noted from 0 (no symptom) to 3 (severe symptom). TNSS were expressed as the sum of the scores for the four symptoms (nasal congestion, rhinorrhea, nasal itching, and sneezing) noted from 0 (no symptom) to 3 (severe symptom). Seven trials reported pre- and post-treatment data of AR symptoms score available for meta-analysis. Compared with placebo, probiotics significantly improved AR symptoms score (SMD, −0.29, 95% CI [−0.44, −0.13]). There was high heterogeneity in the result (p = 0.0003, I2 = 89%) (Figure 4). Sensitivity analysis indicates that the result is robust (Supplementary Material 13). Due to the significantly statistical heterogeneity encountered in the analysis, several subgroup analyses were conducted separately according to the classification of AR, combination of drugs, and intervention of treatment group.
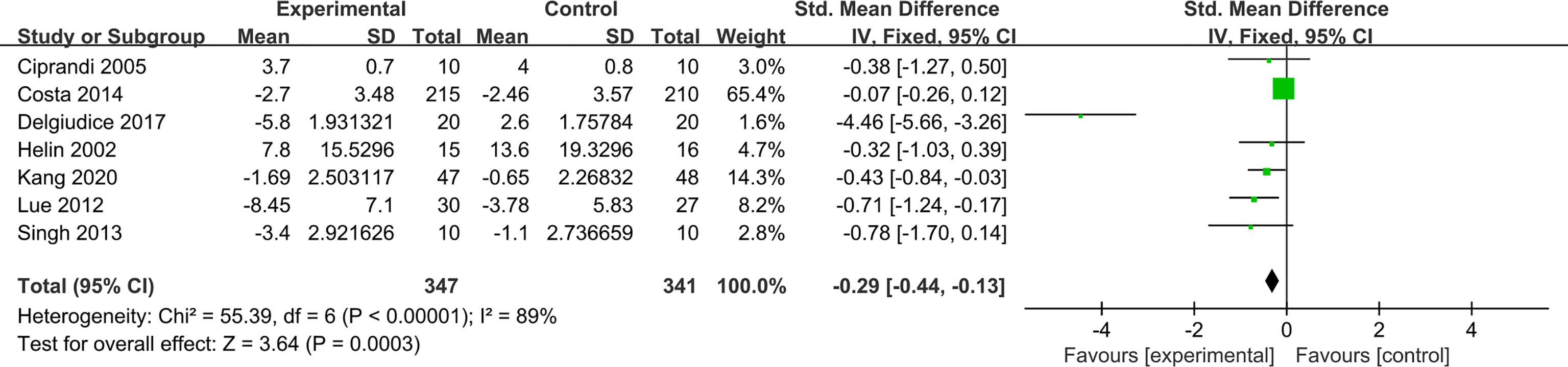
Figure 4 Forest plot for allergic rhinitis symptoms score.
With regard to classification of AR, probiotics can significantly relieve symptoms in patients with SAR (SMD −0.56, 95% CI [−0.87, −0.25]; p = 0.0003, I2 = 0%), and there was significant benefit that probiotics supplementation relieved PAR symptoms score (SMD,−0.19, 95% CI [−0.37, −0.01]; p = 0.03, I2 = 94%) (Supplementary Material 1). Subgroup analysis according to the combination of drugs again found some evidence of a protective effect of probiotics (monotherapy) in relieving AR symptoms compared with placebo (SMD, −0.73, 95% CI [−1.05, −0.42]; p < 0.00001, I2 = 93%). Compared with antihistamines, probiotics combined with antihistamines (combination therapy) have no significant relief of AR symptoms (SMD, −0.15, 95% CI [−0.32, 0.03]; p = 0.10, I2 = 61%) (Supplementary Material 2). The results of subgroup analysis showed that probiotics (single) compared with placebo cannot significantly relieve symptoms (SMD, −0.49, 95% CI [−1.05, 0.07], p = 0.09). Similarly, probiotics combined with antihistamines compared with antihistamines have no significant relief of AR symptoms (SMD, −0.15, 95% CI [−0.32, 0.03], p = 0.10, I2 = 61%). Probiotics (mixed) compared with placebo have significant relief of AR symptoms (SMD, −0.85, 95% CI [−1.23, −0.46], p < 0.0001, I2 = 97%) (Supplementary Material 3) (Table 2).
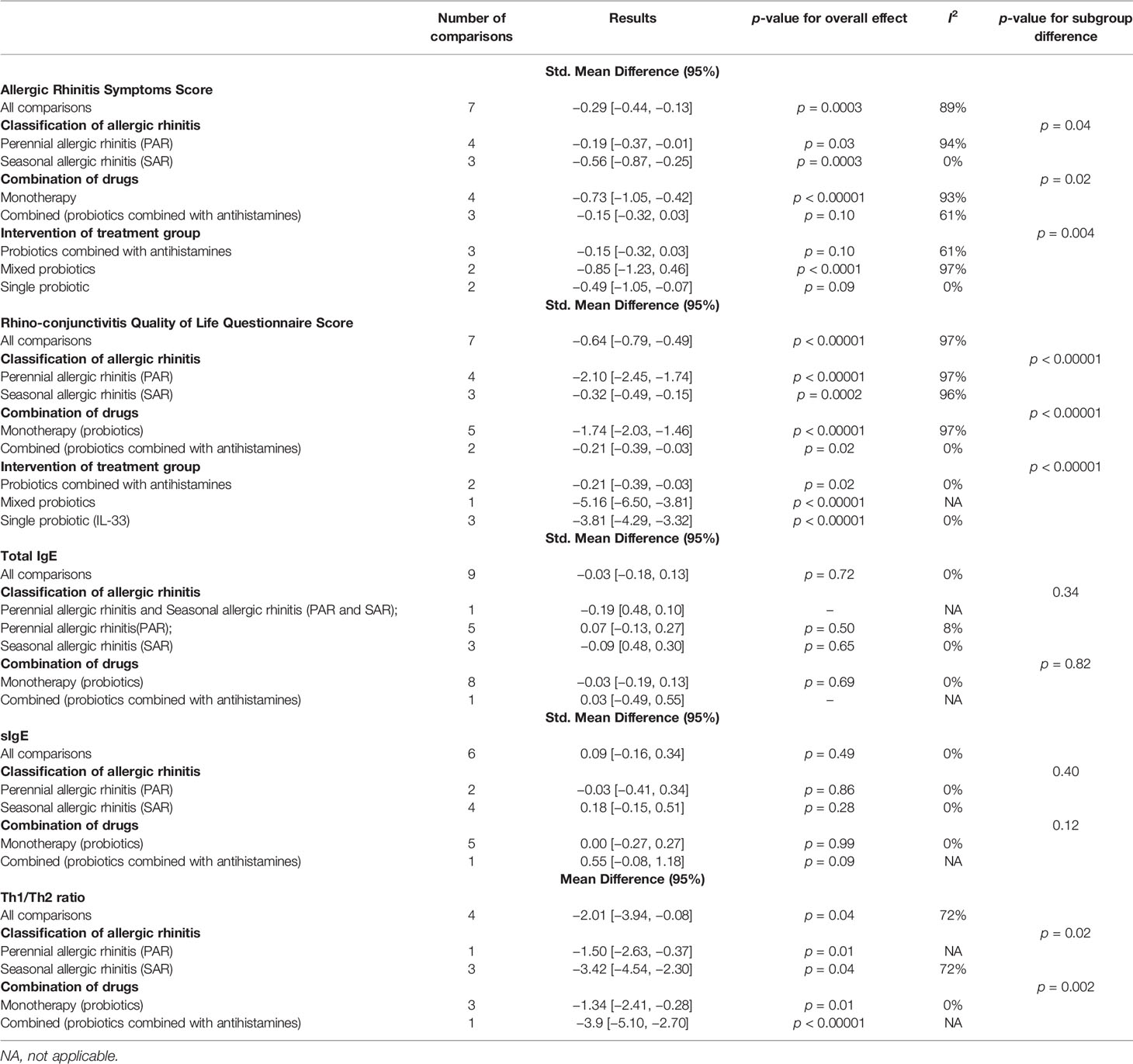
Table 2 Subgroup analysis for outcomes.
Seven trials reported pre- and post-treatment data of Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) scores available for meta-analysis. The results combined with the fixed-effect model showed a significant decrease in RQLQ scores in the probiotic group compared with the control group (−0.64, 95% CI [−0.79, −0.49], p < 0.00001, I2 = 97%) (Figure 5). Sensitivity analysis indicates that the result is stable (Supplementary Material 13).
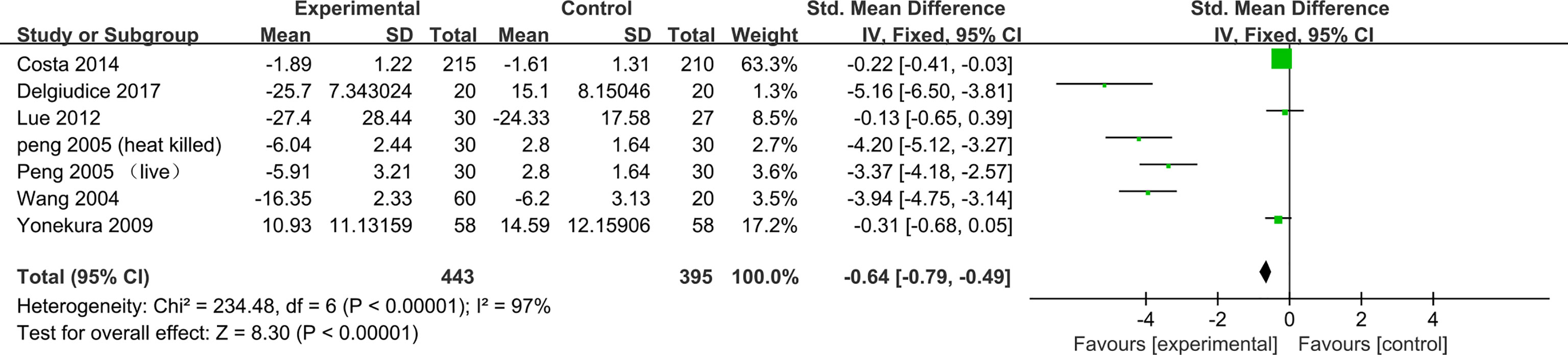
Figure 5 Forest plot for Rhinoconjunctivitis Quality of Life Questionnaire Score.
Subgroup analysis according to the classification of AR found some evidence of a significant decrease in RQLQ scores for SAR in the probiotic group compared with the control group (SMD, −0.32, 95% CI [−0.49, −0.15], p = 0.0002, I2 = 96%), and a greater beneficial effect in PAR (SMD, −2.10, 95% CI [-2.45, −1.74], p < 0.00001, I2 = 97%) (Supplementary Material 4). Subgroup analysis according to the combination of drugs again found some evidence of a protective effect of probiotics (monotherapy) in relieving AR symptoms compared with placebo (SMD, −1.74, 95% CI [−2.03, −1.46]; p < 0.00001, I2 = 97%). Compared with antihistamines, probiotics combined with antihistamines (combination therapy) have a significant relief of AR symptoms (SMD, −0.21, 95% CI [−0.39, −0.03]; p = 0.02, I2 = 0%) (Supplementary Material 5). The results of subgroup analysis showed that probiotics (single) comparing with placebo can significantly relieve symptoms (SMD, -3.81,95% CI [-4.29, -3.32], p<0.00001, I2=0%). Similarly, probiotics combined with antihistamines (combination therapy) compared with antihistamines showed significant improvement in RQLQ scores (SMD, −0.21, 95% CI [−0.39, −0.03], p = 0.02, I2 = 0%) (Supplementary Material 6) (Table 2).
Nine trials reported the effect of probiotics on total IgE. After pooling nine estimates, there was no difference found in total IgE between the probiotic group and the control group (SMD, −0.03, 95% CI [−0.18, 0.13], p = 0.72, I2 = 0%) (Figure 6). Sensitivity analysis indicates that the result is stable (Supplementary Material 13). Subgroup analyses were conducted according to the classification of AR and combination of drugs. The results of subgroup analysis showed that the effect of probiotics on total IgE could not be affected by the classification of AR (PAR or SAR) or combined with other drugs (Supplementary Materials 7 and 8) (Table 2).
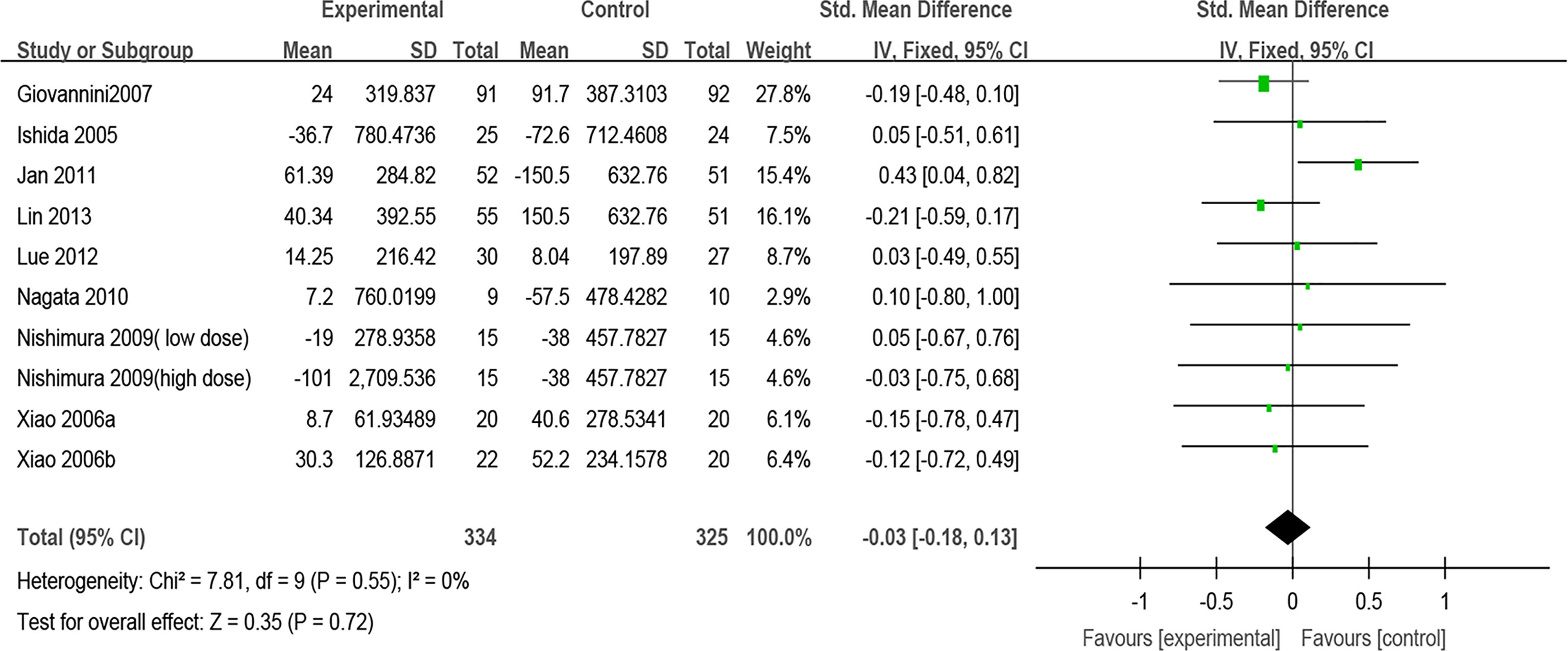
Figure 6 Forest plot for Total IgE.
Specific IgE was evaluated in six studies. After pooling six estimates, there was no difference found in sIgE between the probiotic group and the control group (SMD, 0.09, 95% CI [−0.16, 0.34], p = 0.49, I2 = 0%) (Figure 7). Sensitivity analysis indicates that the result is stable (Supplementary Material 13). Subgroup analyses were conducted according to the classification of AR and combination of drugs. The results of subgroup analysis showed that the effect of probiotics on sIgE could not be affected by the classification of AR (PAR or SAR) or combined with other drugs (Supplementary Materials 9 and 10) (Table 2).
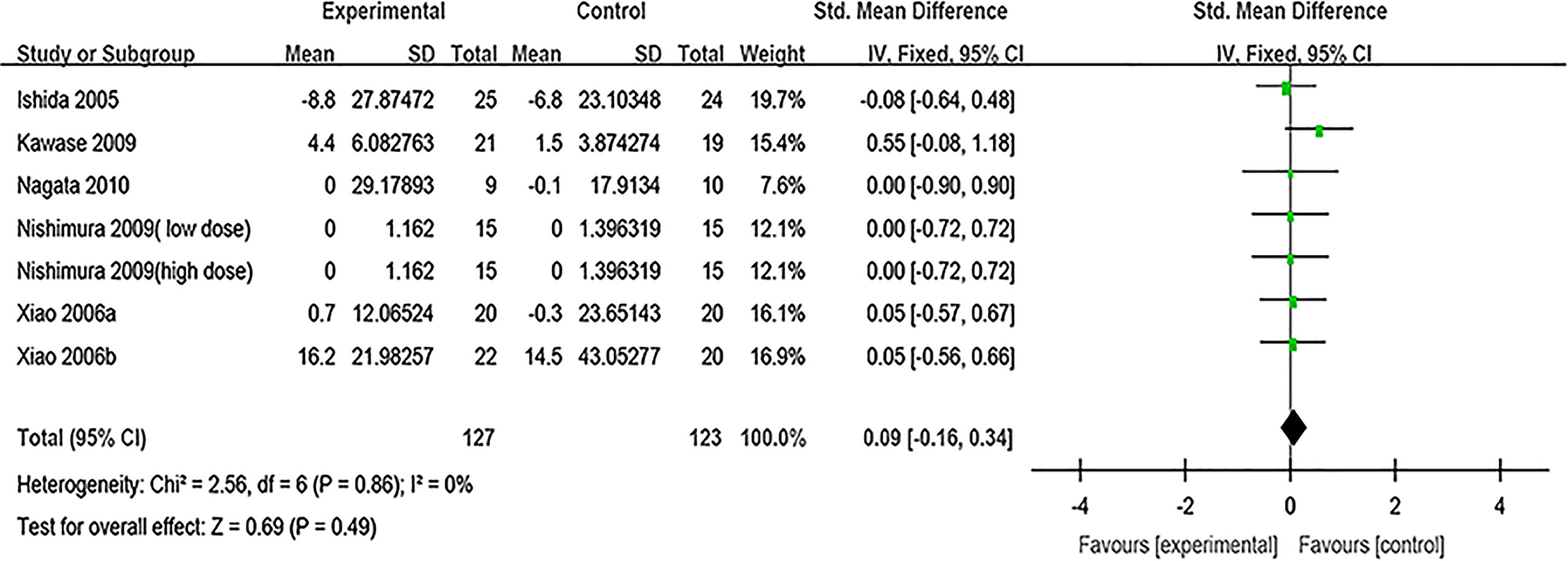
Figure 7 Forest plot for sIgE.
Four trials reported enough data to allow meta-analysis for the Th1/Th2 ratio. The results showed that the Th1/Th2 ratio was lower in the control group when the effect estimates from four trials were pooled (MD, −2.47, 95% CI [−3.27, −1.68], p < 0.00001, I2 = 72%) (Figure 8). Sensitivity analysis indicates that the result is stable (Supplementary Material 13). Subgroup analyses were conducted according to the classification of AR. The results of subgroup analysis showed that the effect of probiotics on the Th1/Th2 ratio could not be affected by the classification of AR (PAR or SAR) or treatment plan (monotherapy/combined) (Supplementary Materials 11 and 12) (Table 2).

Figure 8 Forest plot for Th1/Th2 ratio.
Of the twenty-eight studies included, seventeen RCTs mentioned that no obvious adverse events were found during the research, while seven RCTs did not mention whether any adverse events occurred. Four RCTs have reported adverse events including diarrhea, abdominal pain, flatulence, and fever episodes. One study reported that loose stools and diarrhea were observed in the active and placebo groups, which had no significant differences in adverse events between the two groups (chi-square test, p < 0.4) (17). Another study showed that subjects with these adverse drug reactions (diarrhea, abdominal pain, and flatulence) recovered within a few days. In this study, it was found that one subject’s adverse reaction was almost certainly related to the drug (15). One study reported slight abdominal pain in probiotic groups and all of the adverse events were spontaneously alleviated without drug treatment (41). One study revealed that abdominal symptoms (abdominal symptoms, diarrhea, and fever episodes) were reported in 56.5% versus 64.2% of children in intervention and control groups, respectively (p = 0.282) (26).
The quality of evidence applied for each outcome is summarized in Table 3. The quality of evidence on the Allergic Rhinitis Symptoms Score, Rhinoconjunctivitis Quality of Life Questionnaire Score, Total IgE, Antigen-specific IgE, and Th1/Th2 ratio was rated as very low, very low, low, low, and very low, respectively (Table 3).
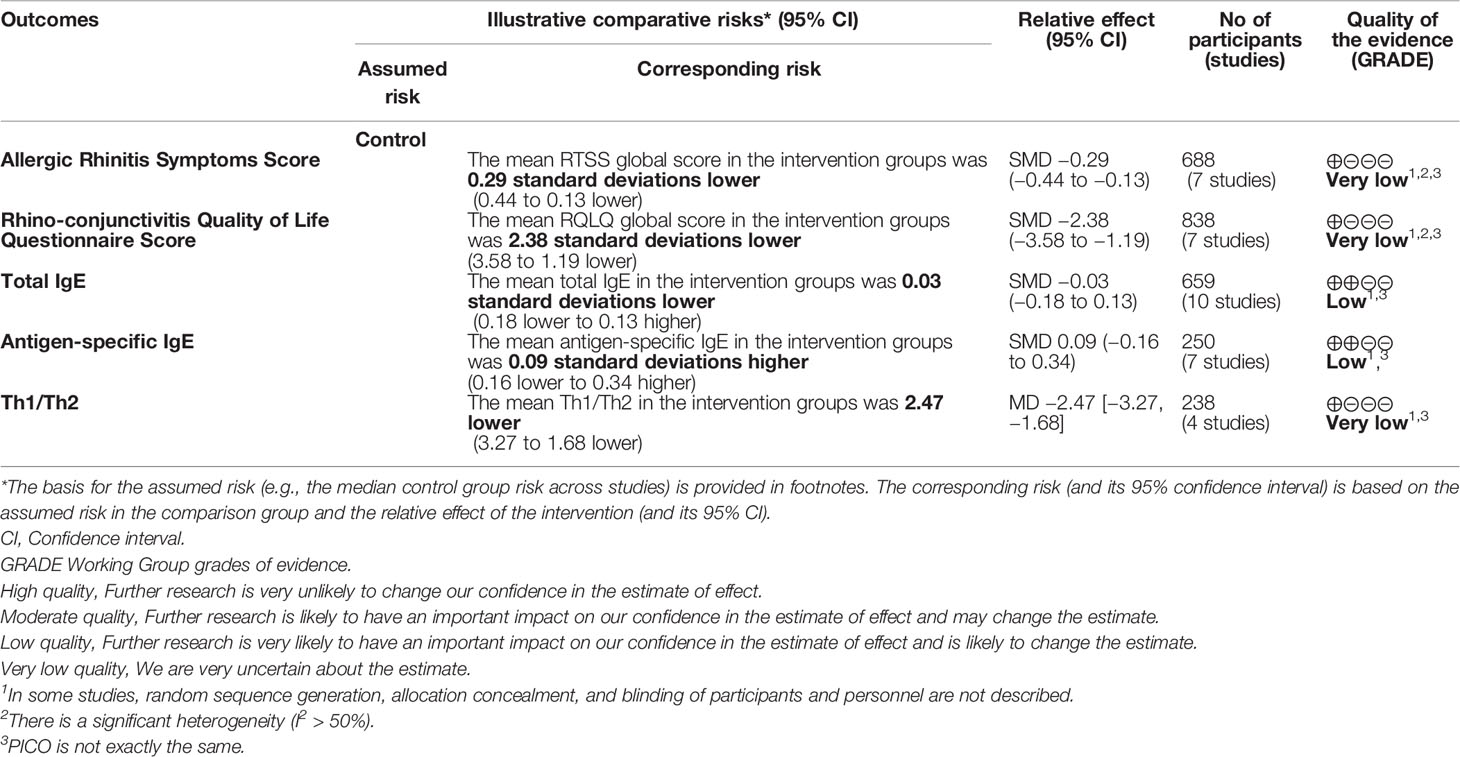
Table 3 GRADE assessment.
In this study, the clinical evidence of probiotics in the treatment of AR was systemically collated and analyzed so as to provide a better guidance for clinical practice. Our results showed that probiotics supplementation for patients with AR can ameliorate AR symptoms and improve the quality of life. Probiotics supplementation can correct the Th1/Th2 balance. There was no significant change in overall or antigen-specific IgE levels between probiotic-treated and placebo-treated subjects. The results of this study have significant heterogeneity, and the source of heterogeneity was explored by subgroup analysis. The results of subgroup analysis showed that probiotics can significantly relieve AR symptoms in patients with SAR. Subgroup analysis according to combination of drugs again found some evidence of a protective effect of probiotics (monotherapy) in relieving AR symptoms compared with placebo. Compared with antihistamines, probiotics combined with antihistamines (combination therapy) have no significant relief of AR symptoms. Subgroup analyses of these outcomes failed to find out the source of heterogeneity. The different doses, durations, and strains of probiotics may be the sources of heterogeneity. With regard to RQLQ score, the results of subgroup analysis according to combination of drugs showed that probiotics (single probiotic strain) compared with placebo can significantly improve the quality of life. Similarly, probiotics combined with antihistamines (combination therapy) compared with antihistamines showed a significant decrease in RQLQ scores, which means an improvement in the quality of life. As we all know, helper T cells play a key role in the adaptive immune response. Human T helper cells can be divided into two main subtypes, Th1 and Th2. The significant trend of immune response to Th2 lineage may lead to allergic diseases. Immunoglobin E (IgE)-mediated allergic inflammation is the main pathophysiological mechanism of AR and drives T helper 2 (Th2) cell polarized immune reactions (45).
The balance Th1/Th2 is associated with AR. Th2 induces the activation of B cells and IgE class switching, which leads to B-cell differentiation into plasma cells that produce allergen-specific IgE. IgE enters the circulation and binds through its Cϵ3 domain to the high-affinity IgE receptor (FcϵRI) on the surface of mast cells and basophils (46). Activated mast cells and basophils release inflammatory mediators (e.g., histamine and leukotrienes) that cause symptoms such as nasal itching, sneezing, and runny nose. At the same time, these inflammatory mediators lead to a predominance of Th2 immune responses, further exacerbating inflammation. Therefore, the predominance of Th2 and its related cytokines correlates with the severity of AR. The Th1/Th2 ratio can reflect the effect of improving allergy symptoms by drugs to a certain degree.
Our meta-analysis demonstrated that probiotics supplementation can correct the Th1/Th2 balance, which indicates that probiotic supplementation can ameliorate AR by regulating the balance of Th1/Th2. However, only four of the included studies reported the Th1/Th2 ratio.
The purpose of most systematic reviews or meta-analyses is to explore the preventive effect of probiotic supplementation on allergic diseases (47–50). There are less systematic reviews or meta-analyses to explore the therapeutic effect of probiotics on AR. A systematic review and meta-analysis of probiotics in the treatment of AR published in 2015 has shown that probiotics may be beneficial in improving symptoms and quality of life in patients with AR (51). One meta-analysis showed that probiotics have beneficial effects in the treatment of AR, especially with SAR and LP-33 strains (52). However, previous systematic reviews failed to explore the causes of heterogeneity as much as possible. Compared with previous systematic reviews and meta-analyses, our meta-analysis conducted subgroup analysis according to types of AR (PAR/SAR) and treatment plan (single probiotic strain/mixed probiotic strains/probiotics combined with antihistamines; monotherapy/combined). We found that a single probiotic strain (LP-33) can significantly improve the quality of life of patients with AR from the meta-analysis of three studies. Two studies used mixed probiotic strains. One study demonstrated that a Bifidobacteria mixture (B. longum BB536, B. infantis M-63, and B. breve M-16 V) was able to significantly improve AR symptoms and quality of life in children with pollen-induced AR and intermittent asthma (39). Another study showed that probiotic NVP-1703 (a mixture of B. longum and L. plantarum) relieves AR symptoms by prompting Treg cells to release IL-10 (42). However, there was a high heterogeneity from meta-analysis of two studies, which may be related to the use of different probiotics. The different strains of probiotics, doses, and durations may be the sources of heterogeneity. To date, no serious adverse events have been observed for probiotic treatment; thus, it appears to be safe.
To sum up, probiotic supplement seems to be effective in ameliorating AR symptoms and improving the quality of life, but there is high heterogeneity in some results after subgroup analysis, and clinicians should be cautious when recommending probiotics in treating AR.
There are some limitations in this meta-analysis. First, the sample size of some included RCTs was small. Second, airborne pollen concentrations are associated with symptom severity and recovery in patients with SAR. The pollen concentrations varied due to different regions in different trials. This is a source of clinical heterogeneity.
This study found that in spite of the positive results of some outcomes, there is weak evidence that probiotics have a potential benefit in the treatment of AR. More RCTs using specific probiotic strains and consistent outcome measures are also needed in the future to investigate efficacy and safety.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
CL, X-DA, and ML were involved in the methodological design of the systematic review, and conducted the acquisition of data, analyses, and interpretation. SP directed and organized the systematic review and the methodologist team, was involved in the initial concept and methodological design of the systematic review, and conducted data acquisition and interpretation. ZL was involved in the initial concept and methodological design of the systematic review, conducted data interpretation, and provided substantial feedback on the drafted manuscript. CL wrote the manuscript and SP revised the manuscript. All authors contributed to the article and approved the submitted version.
This project was funded by Foundation of Chengdu Science and Technology Bureau (No. 2021-YF05-01940-SN). The sponsors are not involved in the design, execution, or writing of the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.848279/full#supplementary-material
Supplementary Material 1 | Subgroup analysis according to classification of allergic rhinitis for allergic rhinitis symptoms score.
Supplementary Material 2 | Subgroup analysis according to combination of drugs for allergic rhinitis symptoms score.
Supplementary Material 3 | Subgroup analysis according to intervention of treatment group for allergic rhinitis symptoms score.
Supplementary Material 4 | Subgroup analysis according to classification of allergic rhinitis for rhinoconjunctivitis quality of life questionnaire score.
Supplementary Material 5 | Subgroup analysis according to combination of drugs for rhinoconjunctivitis quality of life questionnaire score.
Supplementary Material 6 | Subgroup analysis according to intervention of treatment group for rhinoconjunctivitis quality of life questionnaire score.
Supplementary Material 7 | Subgroup analysis according to classification of allergic rhinitis for total IgE.
Supplementary Material 8 | Subgroup analysis according to combination of drugs for total IgE.
Supplementary Material 9 | Subgroup analysis according to classification of allergic rhinitis for sIgE.
Supplementary Material 10 | Subgroup analysis according to combination of drugs for sIgE.
Supplementary Material 11 | Subgroup analysis according to classification of allergic rhinitis for Th1/Th2 ratio.
Supplementary Material 12 | Subgroup analysis according to combination of drugs for Th1/Th2 ratio.
1. Brożek JL, Bousquet J, Agache I, Agarwal A, Bachert C, Bosnic-Anticevich S, et al. Allergic Rhinitis and Its Impact on Asthma (ARIA) Guidelines-2016 Revision. J Allergy Clin Immunol (2017) 140(4):950–8. doi: 10.1016/j.jaci.2017.03.050
2. Chong SN, Chew FT. Epidemiology of Allergic Rhinitis and Associated Risk Factors in Asia. World Allergy Organ J (2018) 11(1):17. doi: 10.1186/s40413-018-0198-z
3. Strachan DP. Hay Fever, Hygiene, and Household Size. BMJ (Clinical Res ed) (1989) 299(6710):1259–60. doi: 10.1136/bmj.299.6710.1259
4. Rook GA, Adams V, Hunt J, Palmer R, Martinelli R, Brunet LR. Mycobacteria and Other Environmental Organisms as Immunomodulators for Immunoregulatory Disorders. Springer Semin immunopathol (2004) 25(3-4):237–55. doi: 10.1007/s00281-003-0148-9
5. Stiemsma LT, Reynolds LA, Turvey SE, Finlay BB. The Hygiene Hypothesis: Current Perspectives and Future Therapies. ImmunoTargets Ther (2015) 4:143–57. doi: 10.2147/ITT.S61528
6. Noverr MC, Huffnagle GB. The 'Microflora Hypothesis' of Allergic Diseases. Clin Exp Allergy J Br Soc Allergy Clin Immunol (2005) 35(12):1511–20. doi: 10.1111/j.1365-2222.2005.02379.x
7. Sbihi H, Boutin RC, Cutler C, Suen M, Finlay BB, Turvey SE. Thinking Bigger: How Early-Life Environmental Exposures Shape the Gut Microbiome and Influence the Development of Asthma and Allergic Disease. Allergy (2019) 74(11):2103–15. doi: 10.1111/all.13812
8. West CE, Jenmalm MC, Prescott SL. The Gut Microbiota and Its Role in the Development of Allergic Disease: A Wider Perspective. Clin Exp Allergy J Br Soc Allergy Clin Immunol (2015) 45(1):43–53. doi: 10.1111/cea.12332
9. McCoy KD, Köller Y. New Developments Providing Mechanistic Insight Into the Impact of the Microbiota on Allergic Disease. Clin Immunol (Orlando Fla) (2015) 159(2):170–6. doi: 10.1016/j.clim.2015.05.007
10. Nations F, Organization WH. Probiotics in Food - Health and Nutritional Properties and Guidelines for Evaluation: Probiotics in Food - Health and Nutritional Properties and Guidelines for Evaluation. Food and Agriculture Organization of the United Nations. (2006).
11. Hajavi J, Esmaeili SA, Varasteh AR, Vazini H, Atabati H, Mardani F, et al. The Immunomodulatory Role of Probiotics in Allergy Therapy. J Cell Physiol (2019) 234(3):2386–98. doi: 10.1002/jcp.27263
12. Isolauri E, Sütas Y, Kankaanpää P, Arvilommi H, Salminen S. Probiotics: Effects on Immunity. Am J Clin Nutr (2001) 73Suppl:444s–50s. doi: 10.1093/ajcn/73.2.444s
13. Fiocchi A, Burks W, Bahna SL, Bielory L, Boyle RJ, Cocco R, et al. Clinical Use of Probiotics in Pediatric Allergy (CUPPA): A World Allergy Organization Position Paper. World Allergy Organ J (2012) 5(11):148–67. doi: 10.1097/WOX.0b013e3182784ee0
14. Björkstén B. The Intrauterine and Postnatal Environments. J Allergy Clin Immunol (1999) 104(6):1119–27. doi: 10.1016/S0091-6749(99)70002-3
15. Dölle S, Berg J, Rasche C, Worm M. Tolerability and Clinical Outcome of Coseasonal Treatment With Escherichia Coli Strain Nissle 1917 in Grass Pollen-Allergic Subjects. Int Arch Allergy Immunol (2014) 163(1):29–35. doi: 10.1159/000356328
16. Xiao JZ, Kondo S, Yanagisawa N, Takahashi N, Odamaki T, Iwabuchi N, et al. Probiotics in the Treatment of Japanese Cedar Pollinosis: A Double-Blind Placebo-Controlled Trial. Clin Exp Allergy (2006) 36(11):1425–35. doi: 10.1111/j.1365-2222.2006.02575.x
17. Yonekura S, Okamoto Y, Okawa T, Hisamitsu M, Chazono H, Kobayashi K, et al. Effects of Daily Intake of Lactobacillus Paracasei Strain KW3110 on Japanese Cedar Pollinosis. Allergy Asthma Proc (2009) 30(4):397–405. doi: 10.2500/aap.2009.30.3256
18. Ouwehand AC, Nermes M, Collado MC, Rautonen N, Salminen S, Isolauri E. Specific Probiotics Alleviate Allergic Rhinitis During the Birch Pollen Season. World J Gastroenterol (2009) 15(26):3261–8. doi: 10.3748/wjg.15.3261
19. Nembrini C, Singh A, Vissers Y, Mercenier A, Nutten S, Blanchard C. Oral Administration of Lactobacillus Paracasei NCC2461 for the Modulation of Grass Pollen Allergic Rhinitis: A Randomized, Placebo-Controlled Study During the Pollen Season. Allergy: Eur J Allergy Clin Immunol (2015) 70:119–20. doi: 10.1186/s13601-015-0085-4
20. Jan RH, Chen CJ, Chen LK, Wen SH, Lin TY. Is the Effect of Probiotics on Allergic Rhinitis Confined to Dermatophagoides Farinae, Dermatophagoides Pteronyssinus, or Dust-Sensitive Children? A Randomized Prospective Double-Blind Controlled Trial. Tzu Chi Med J (2011) 23(2):51–4. doi: 10.1016/j.tcmj.2011.05.003
21. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's Tool for Assessing Risk of Bias in Randomised Trials. BMJ (Clinical Res ed) (2011) 343:d5928. doi: 10.1136/bmj.d5928
22. Helin T, Haahtela S, Haahtela T. No Effect of Oral Treatment With an Intestinal Bacterial Strain, Lactobacillus Rhamnosus (ATCC 53103), on Birch-Pollen Allergy: A Placebo-Controlled Double-Blind Study. Allergy: Eur J Allergy Clin Immunol (2002) 57(3):243–6. doi: 10.1034/j.1398-9995.2002.1s3299.x
23. Wang MF, Lin HC, Wang YY, Hsu CH. Treatment of Perennial Allergic Rhinitis With Lactic Acid Bacteria. Pediatr Allergy Immunol (2004) 15(2):152–8. doi: 10.1111/j.1399-3038.2004.00156.x
24. Peng GC, Hsu CH. The Efficacy and Safety of Heat-Killed Lactobacillus Paracasei for Treatment of Perennial Allergic Rhinitis Induced by House-Dust Mite. Pediatr Allergy Immunol (2005) 16(5):433–8. doi: 10.1111/j.1399-3038.2005.00284.x
25. Xiao JZ, Kondo S, Yanagisawa N, Takahashi N, Odamaki T, Iwabuchi N, et al. Effect of Probiotic Bifidobacterium Longum BBS36 in Relieving Clinical Symptoms and Modulating Plasma Cytokine Levels of Japanese Cedar Pollinosis During the Pollen Season. A Randomized Double-Blind, Placebo-Controlled Trial. J Investigational Allergol Clin Immunol (2006) 16(2):86–93.
26. Giovannini M, Agostoni C, Riva E, Salvini F, Ruscitto A, Zuccotti GV, et al. A Randomized Prospective Double Blind Controlled Trial on Effects of Long-Term Consumption of Fermented Milk Containing Lactobacillus Casei in Pre-School Children With Allergic Asthma and/or Rhinitis. Pediatr Res (2007) 62(2):215–20. doi: 10.1203/PDR.0b013e3180a76d94
27. Tamura M, Shikina T, Morihana T, Hayama M, Kajimoto O, Sakamoto A, et al. Effects of Probiotics on Allergic Rhinitis Induced by Japanese Cedar Pollen: Randomized Double-Blind, Placebo-Controlled Clinical Trial. Int Arch Allergy Immunol (2007) 143(1):75–82. doi: 10.1159/000098318
28. Ishida Y, Nakamura F, Kanzato H, Sawada D, Hirata H, Nishimura A, et al. Clinical Effects of Lactobacillus Acidophilus Strain L-92 on Perennial Allergic Rhinitis: A Double-Blind, Placebo-Controlled Study. J dairy scie (2005) 88(2):527–33. doi: 10.3168/jds.S0022-0302(05)72714-4
29. Ciprandi G, Vizzaccaro A, Cirillo I, Tosca MA. Bacillus Clausii Effects in Children With Allergic Rhinitis. Allergy (2005) 60(5):702–3. doi: 10.1111/j.1398-9995.2005.00722.x
30. Ivory K, Chambers SJ, Pin C, Prieto E, Arqués JL, Nicoletti C. Oral Delivery of Lactobacillus Casei Shirota Modifies Allergen-Induced Immune Responses in Allergic Rhinitis. Clin Exp Allergy (2008) 38(8):1282–9. doi: 10.1111/j.1365-2222.2008.03025.x
31. Nishimura I, Igarashi T, Enomoto T, Dake Y, Okuno Y, Obata A. Clinical Efficacy of Halophilic Lactic Acid Bacterium Tetragenococcus Halophilus Th221 From Soy Sauce Moromi for Perennial Allergic Rhinitis. Allergol Int (2009) 58(2):179–85. doi: 10.2332/allergolint.O-08-548
32. Kawase M, He F, Kubota A, Hiramatsu M, Saito H, Ishii T, et al. Effect of Fermented Milk Prepared With Two Probiotic Strains on Japanese Cedar Pollinosis in a Double-Blind Placebo-Controlled Clinical Study. Int J Food Microbiol (2009) 128(3):429–34. doi: 10.1016/j.ijfoodmicro.2008.09.017
33. Nagata Y, Yoshida M, Kitazawa H, Araki E, Gomyo T. Improvements in Seasonal Allergic Disease With Lactobacillus Plantarum No. 14. Biosci biotechnol Biochem (2010) 74(9):1869–77. doi: 10.1271/bbb.100270
34. Lue KH, Sun HL, Lu KH, Ku MS, Sheu JN, Chan CH, et al. A Trial of Adding Lactobacillus Johnsonii EM1 to Levocetirizine for Treatment of Perennial Allergic Rhinitis in Children Aged 7-12 Years. Int J Pediatr otorhinolaryngol (2012) 76(7):994–1001. doi: 10.1016/j.ijporl.2012.03.018
35. Lin TY, Chen CJ, Chen LK, Wen SH, Jan RH. Effect of Probiotics on Allergic Rhinitis in Df, Dp or Dust-Sensitive Children: A Randomized Double Blind Controlled Trial. Indian pediatrics (2013) 50(2):209–13. doi: 10.1007/s13312-013-0068-2
36. Singh A, Hacini-Rachinel F, Gosoniu ML, Bourdeau T, Holvoet S, Doucet-Ladeveze R, et al. Immune-Modulatory Effect of Probiotic Bifidobacterium Lactis NCC2818 in Individuals Suffering From Seasonal Allergic Rhinitis to Grass Pollen: An Exploratory, Randomized, Placebo-Controlled Clinical Trial. Eur J Clin Nutr (2013) 67(2):161–7. doi: 10.1038/ejcn.2012.197
37. Costa DJ, Marteau P, Amouyal M, Poulsen LK, Hamelmann E, Cazaubiel M, et al. Efficacy and Safety of the Probiotic Lactobacillus Paracasei LP-33 in Allergic Rhinitis: A Double-Blind, Randomized, Placebo-Controlled Trial (GA2LEN Study). Eur J Clin Nutr (2014) 68(5):602–7. doi: 10.1038/ejcn.2014.13
38. Lin WY, Fu LS, Lin HK, Shen CY, Chen YJ. Evaluation of the Effect of Lactobacillus Paracasei (HF.A00232) in Children (6-13 Years Old) With Perennial Allergic Rhinitis: A 12-Week, Double-Blind, Randomized, Placebo-Controlled Study. Pediatr Neonatol (2014) 55(3):181–8. doi: 10.1016/j.pedneo.2013.10.001
39. Del Giudice MM, Indolfi C, Capasso M, Maiello N, Decimo F, Ciprandi G. Bifidobacterium Mixture (B Longum BB536, B Infantis M-63, B Breve M-16V) Treatment in Children With Seasonal Allergic Rhinitis and Intermittent Asthma. Ital J Pediatrics (2017) 43(1):25. doi: 10.1186/s13052-017-0340-5
40. Dennis-Wall JC, Culpepper T, Nieves C Jr, Rowe CC, Burns AM, Rusch CT, et al. Probiotics (Lactobacillus Gasseri KS-13, Bifidobacterium Bifidum G9-1, and Bifidobacterium Longum MM-2) Improve Rhinoconjunctivitis-Specific Quality of Life in Individuals With Seasonal Allergies: A Double-Blind, Placebo-Controlled, Randomized Trial. Am J Clin Nutr (2017) 105(3):758–67. doi: 10.3945/ajcn.116.140012
41. Meng Q, Li P, Li Y, Chen J, Wang L, He L, et al. Broncho-Vaxom Alleviates Persistent Allergic Rhinitis in Patients by Improving Th1/Th2 Cytokine Balance of Nasal Mucosa. Rhinology (2019) 57(6):451–9. doi: 10.4193/Rhin19.161
42. Kang MG, Han SW, Kang HR, Hong SJ, Kim DH, Choi JH. Probiotic NVP-1703 Alleviates Allergic Rhinitis by Inducing IL-10 Expression: A Four-Week Clinical Trial. Nutrients (2020) 12(5):1427. doi: 10.3390/nu12051427
43. Anania C, Di Marino VP, Olivero F, De Canditiis D, Brindisi G, Iannilli F, et al. Treatment With a Probiotic Mixture Containing Bifidobacterium Animalis Subsp. Lactis BB12 and Enterococcus Faecium L3 for the Prevention of Allergic Rhinitis Symptoms in Children: A Randomized Controlled Trial. Nutrients (2021) 13(4):1315. doi: 10.3390/nu13041315
44. Nembrini C, Singh A, De Castro CA, Mercenier A, Nutten S. Oral Administration of Lactobacillus Paracasei NCC 2461 for the Modulation of Grass Pollen Allergic Rhinitis: A Randomized, Placebo-Controlled Study During the Pollen Season. Clin Trans Allergy (2015) 5(1). doi: 10.1186/s13601-015-0085-4
45. Baraniuk JN. Pathogenesis of Allergic Rhinitis. J Allergy Clin Immunol (1997) 99(2):S763–72. doi: 10.1016/S0091-6749(97)70125-8
46. Palomares O, Akdis M, Martín-Fontecha M, Akdis CA. Mechanisms of Immune Regulation in Allergic Diseases: The Role of Regulatory T and B Cells. Immunol Rev (2017) 278(1):219–36. doi: 10.1111/imr.12555
47. Du X, Wang L, Wu S, Yuan L, Tang S, Xiang Y, et al. Efficacy of Probiotic Supplementary Therapy for Asthma, Allergic Rhinitis, and Wheeze: A Meta-Analysis of Randomized Controlled Trials. Allergy Asthma Proc (2019) 40(4):250–60. doi: 10.2500/aap.2019.40.4227
48. Sestito S, D'Auria E, Baldassarre ME, Salvatore S, Tallarico V, Stefanelli E, et al. The Role of Prebiotics and Probiotics in Prevention of Allergic Diseases in Infants. Front Pediatrics (2020) 8. doi: 10.3389/fped.2020.583946
49. Meirlaen L, Levy EI, Vandenplas Y. Prevention and Management With Pro-, Pre and Synbiotics in Children With Asthma and Allergic Rhinitis: A Narrative Review. Nutrients (2021) 13(3):934. doi: 10.3390/nu13030934
50. Amalia N, Orchard D, Francis KL, King E. Systematic Review and Meta-Analysis on the Use of Probiotic Supplementation in Pregnant Mother, Breastfeeding Mother and Infant for the Prevention of Atopic Dermatitis in Children. Australas J Dermatol (2020) 61(2):e158–73. doi: 10.1111/ajd.13186
51. Zajac AE, Adams AS, Turner JH. A Systematic Review and Meta-Analysis of Probiotics for the Treatment of Allergic Rhinitis. Int Forum Allergy rhinol (2015) 5(6):524–32. doi: 10.1002/alr.21492
Keywords: probiotics, allergy rhinitis, allergy, systematic review, meta-analysis
Citation: Luo C, Peng S, Li M, Ao X and Liu Z (2022) The Efficacy and Safety of Probiotics for Allergic Rhinitis: A Systematic Review and Meta-Analysis. Front. Immunol. 13:848279. doi: 10.3389/fimmu.2022.848279
Received: 04 January 2022; Accepted: 14 April 2022;
Published: 19 May 2022.
Edited by:
Harry Wichers, Wageningen University and Research, NetherlandsReviewed by:
Mangesh Deshmukh, Fiona Stanley Hospital, AustraliaCopyright © 2022 Luo, Peng, Li, Ao and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shunlin Peng, c2h1bmxpbl9wZW5nQDE2My5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.