 Xiao-Mei Chen1†
Xiao-Mei Chen1† Hui Li
Hui Li Yu Wu
Yu Wu Yang-Juan Bai
Yang-Juan Bai
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Immunol., 29 November 2022
Sec. Alloimmunity and Transplantation
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.1049444
This article is part of the Research TopicRole of the Immune System in Renal Transplantation: Importance, Mechanism, and TherapyView all 12 articles
Anti-erythropoietin (anti-EPO) antibody-mediated pure red cell aplasia (PRCA) is a rarely seen disease. Anti-EPO antibodies were mostly found in patients with chronic kidney disease who received recombinant human erythropoietin (rHuEPO) injections subcutaneously. The treatment against anti-EPO antibody-mediated PRCA included discontinuation of rHuEPO, immunosuppressive agents, intravenous immunoglobulin, plasmapheresis, or kidney transplantation. We reported a case of kidney transplant recipient with anti-EPO antibody-mediated PRCA, who had no trend of recovery after stopping rHuEPO, receiving regular induction and maintenance immunosuppressive regimens. He was further given 6 consecutive plasmapheresis sessions, cyclophosphamide, and adjusted maintenance immunosuppressive regimen into cyclosporine, sirolimus and prednisone. We monitored his anti-EPO antibody levels with a self-created simple mixing test. At 10 months post kidney transplant, his anti-EPO antibody finally turned negative, and his reticulocyte count dramatically increased. Cyclosporine, sirolimus and prednisone combined with roxadustat eventually alleviated the patient’s anti-EPO antibody-mediated PRCA. Our self-created simple mixing test for anti-EPO antibody titer was very helpful in disease monitoring and therapeutic guidance.
Anti-EPO antibody-mediated PRCA is a very rare but severe transfusion-dependent anemia with an incidence of 0.02 to 0.03 per 1000 person-years (1). The incidence rate may be underestimated due to the availability of anti-EPO antibody testing. A slight modification in the production process of rHuEPO leads to some antigenicity of the manufactured hormone, which induces the generation of anti-EPO antibody (2–4). Causes of this disease included formulations without human serum albumin, subcutaneous administration, and uncoated rubber stoppers (1). The median duration of rHuEPO treatment prior to the occurrence of PRCA was 9-25 months (5). There was no guideline on the treatment for anti-EPO antibody-mediated PRCA, because there were too limited cases to perform prospective cohort studies and the patients in most case reports experienced rapid remission after kidney transplant (6). Since kidney transplant itself was an effective treatment for anti-EPO antibody-mediated PRCA, cases with prolonged course after kidney transplant were rarely reported. We reported a case of anti-EPO antibody-mediated PRCA diagnosed after kidney transplant with an abnormally prolonged course, and we successfully created a simple mixing test to monitor anti-EPO antibody titer and guide our treatment adjustment effectively.
A 38-year-old Chinese man who was diagnosed with end-stage renal disease (ESRD) due to chronic glomerulonephritis started maintenance hemodialysis three times a week in a local hospital since 2018. He received rHuEPO (Epiao, 3SBio, Shenyang, China) subcutaneously at 10,000 IU twice a week and roxadustat was added later due to his hemoglobin (Hb) below the target range (Figure 1). In June 2020, his Hb level suddenly decreased from 100 g/L to 34 g/L without evidence of active bleeding or hemolysis, and he required blood transfusion every month to maintain Hb around 60g/L ever since then. He underwent his first bone marrow aspirate and biopsy in February 2021 in West China Hospital, and his bone marrow smear showed hypercellularity with no red blood cell precursors. His blood routine examination showed that reticulocyte count was 0.0020×1012/L and Hb was 50 g/L. His erythropoietin level was <0.60 mIU/mL and his ferritin level was >2000 ng/mL. In May 2021, he received a kidney transplant donated by his 58-year-old mother in West China Hospital of Sichuan University, and his Hb was enhanced to 90 g/L by transfusing leukodepleted red cell suspension prior to the surgery. Induction therapy including intravenous basiliximab and methylprednisolone pulse therapy was given, and the standard triple immunosuppressive regimen consisting of mycophenolate mofetil (MMF), tacrolimus (Tac), and prednisone was immediately applied. Trimethoprim-sulfamethoxazole and ganciclovir were administered as the general prophylaxis for pneumocystis pneumonia and cytomegalovirus (CMV) infection, respectively. The kidney graft functioned immediately after the surgery, and roxadustat combined with rHuEPO injection subcutaneously were continued for his anemia (Figure 1).
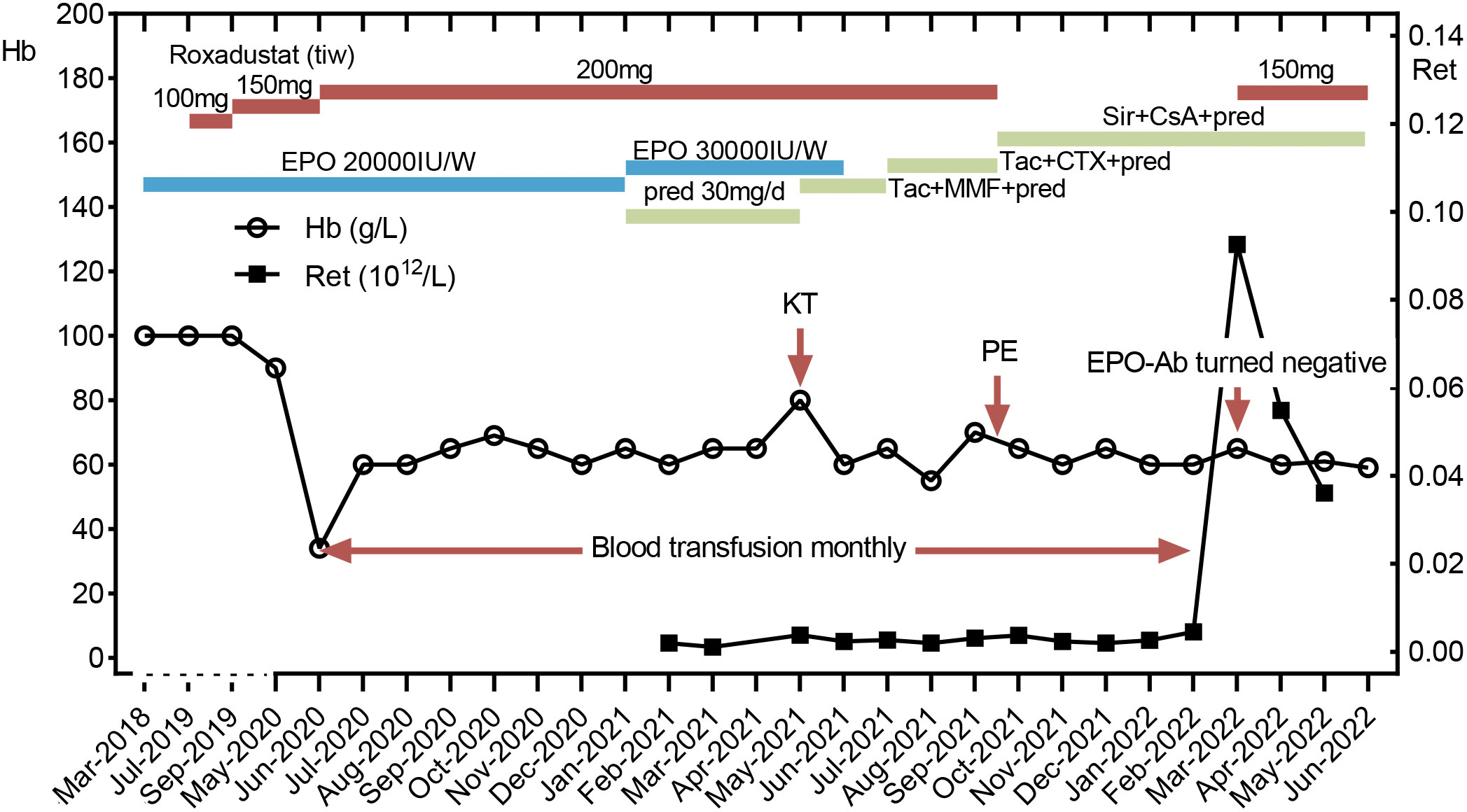
Figure 1 Clinical course. A kidney transplantation was performed in May 2021. Plasma exchange was performed in September 15, 2021. After the EPO antibody turned negative, the patient didn’t rely on blood transfusion any more. Hb, hemoglobin; Ret, reticulocyte; Tac, tacrolimus; MMF, mycophenolate mofetil; pred, prednisone; CTX, cyclophosphamide; Sir, sirolimus; CsA, cyclosporine; KT, kidney transplant; PE, plasma exchange.
Approximately one month after kidney transplant, the patient was readmitted to the hospital due to severe anemia. His blood routine examination showed that reticulocyte count was 0.0020×1012/L, Hb was 49 g/L, platelet (PLT) count was 60×109/L and white blood cell (WBC) count was 2.8×109/L with normal differentials. His graft function was stable with a creatinine level of 144 µmol/L. The erythropoietin and ferritin levels were similar to those before the transplant. Examinations to exclude other possible causes of anemia, including tumor markers, serum protein electrophoresis, serum immunofixation electrophoresis, anti-nuclear antibodies (ANA), extractable nuclear antigens (ENA), Coombs test, serum cytomegalovirus (CMV) DNA polymerase chain reaction (PCR) and Epstein-Barr virus (EBV) DNA PCR, were all negative. Computed tomography of the chest did not reveal thymoma. Fecal occult blood testing and DNA quantification of parvovirus B19 were also negative. No suspected family history or history of using drugs that might interfere hematopoietic function was found. Tacrolimus trough concentration was 6.86ng/mL. A second bone marrow biopsy was performed, and the bone marrow smear showed hypercellularity with 0.5% red blood cell precursors. Bone marrow biopsy revealed severe erythroid hypoplasia. The patient was diagnosed with PRCA accordingly. His serum was sent to 3SBio Pharmaceutical Company for the anti-EPO antibody examination, which showed positive by enzyme-linked immunosorbent assay (ELISA). The neutralization test of anti-EPO antibody was performed by a bioassay based on the fact that rHuEPO-neutralizing antibodies could inhibit the proliferation of rHuEPO on UT7/EPO-dependent cell lines. The patient was eventually diagnosed with anti-EPO antibody-mediated PRCA.
Due to the limited availability and long turn-around time of the anti-EPO antibody test, as well as the need for dynamic monitoring of the therapeutic effect, we created a simple mixing test to quantify the antibody titer (Supplementary Figure 1). The operating steps were as follows: the sera of both the patient and the health control were collected and then mixed in different proportions, which were used for the testing of EPO concentrations (IMMULITE 1000, SIEMENS). The maximum dilution multiple at which a positive EPO result was obtained was defined as the antibody titer, which was based on the fact that the neutralizing IgG antibodies against the protein component of exogenous erythropoiesis-stimulating agents (ESAs) would cross-react with endogenous hormones. The result of the simple mixing test was consistent with the neutralization test of anti-EPO antibodies from the 3SBio Pharmaceutical Company, which revealed a titer of 1:10 at diagnosis. Then, we adopted this simple method for the monthly anti-EPO antibody monitoring. It should be noted that the EPO level of the selected health control in each test must be fixed and above the upper limit of normal value to reduce errors. In our experiment, the fixed EPO level was 200mIU/ml. The dynamic changes of anti-EPO antibody titers and EPO levels of the patient are shown in Figure 2.
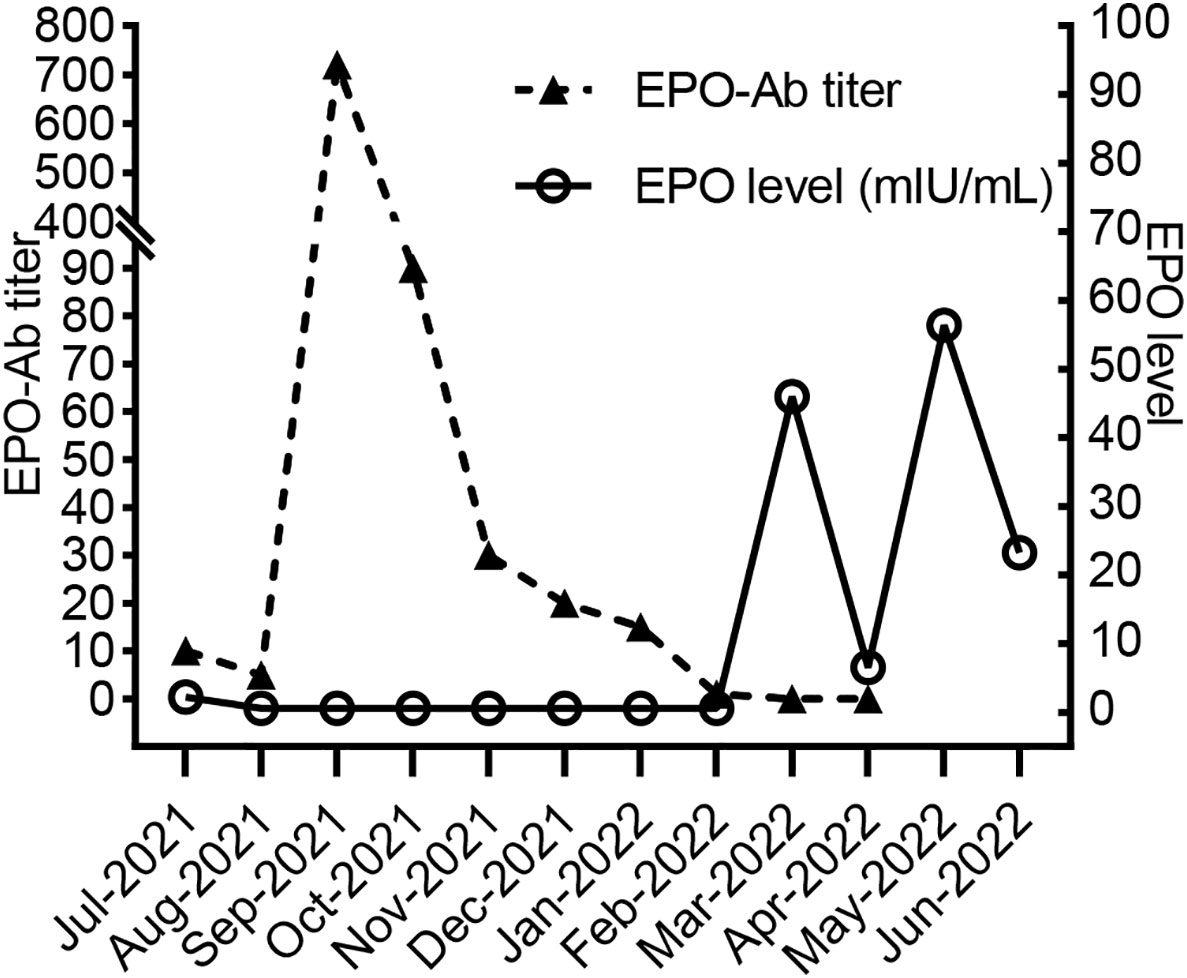
Figure 2 EPO antibody titer and EPO levels of the patient.
Once diagnosed in July 2021, rHuEPO was stopped immediately. The detailed treatment course is shown in Figure 1. Recombinant human granulocyte colony-stimulating factors were administered and Trimethoprim-sulfamethoxazole as well as ganciclovir were discontinued due to leukopenia. The antibody titer decreased to 1:5 in August 2021, and then suddenly increased to 1:720 one month later after he received massive transfusion of 10 U leukodepleted red blood cell suspension in the local hospital. It was speculated that EPO existed in a small amount of plasma contained in the leukodepleted red blood cells, which may activate immunological memory response and induce the massive production of anti-EPO antibodies. In comparison, the residual plasma volume in washed red blood cells was less than that in leukodepleted red blood cell suspension (7). Therefore, we replaced the leukodepleted red blood cell suspension with a restrictive washed red blood cell transfusion. At the same time, the cumulative dose of cyclophosphamide reached 6 g but no effect was observed. Then, we performed plasmapheresis 6 times and adjusted immunosuppressive regimen into cyclosporine, sirolimus and methylprednisolone (because of mild liver dysfunction). The trough concentration of cyclosporine was maintained at 100-150 ng/ml, and sirolimus was maintained at 6-8 ng/ml. By the fifth month of the above treatment, antibodies were finally undetectable using the simple mixing test, and laboratory results were as follows: a Hb level of 51 g/L, a reticulocyte count of 0.0926×1012/L, an EPO level of 46 mIU/mL, a creatinine level of 146 µmol/L, and an eGFR of 51.46 mL/min/1.73 m2. A serum sample of the patient was sent to 3SBio Pharmaceutical company again for anti-EPO antibody test, which also confirmed the negative result. We did not schedule any more blood transfusions but started roxadustat treatment. For the following three months, although the patient’s hemoglobin still fluctuated around 60 g/L, he no longer relied on blood transfusions. During the whole treatment, the graft function of the patient remained stable with serum creatinine level around 120-140umol/L, and no acute rejection or severe infection was occurred except a mild urinary tract infection and a herpes zoster infection.
The main treatments for anti-EPO antibody-mediated PRCA include immediate cessation of rHuEPO, restrictive transfusion and immunosuppressive therapies (8). However, long-term blood transfusions are resource-consuming and may increase the risk of infection and antibody development. Kidney transplant appears to be a viable option for ESRD patients with PRCA (9). There may be antigenic differences between endogenous and exogenous erythropoietin, and kidney transplantation can inhibit the production of antibodies and restore EPO secretion from the transplanted kidney (10, 11). A retrospective study collected anti-EPO antibody-mediated PRCA cases in French and German from 1998 to 2003, which found that there were 6 cases in total and they all got recovered one month after undergoing kidney transplant (6). We also reviewed other case reports published afterward and found that 6 (85.7%) out of 7 ESRD cases with anti-EPO antibody-mediated PRCA got recovered with Hb levels above 100 g/L within 3 months after kidney transplantation (12–15). Only one case reported partial recovery at 28 months after transplantation with persistent anti-EPO antibodies but independent of blood transfusion (13). The clinical characteristics of 13 reported cases of anti-rHuEPO antibody-mediated PRCA who underwent kidney transplant were summarized in Table 1. Unlike previous reports, anemia in our case did not recover quickly after kidney transplant and intense immunosuppressive regimen. Instead, the antibodies disappeared after plasmapheresis therapy and immunosuppressive regimen adjustment. Although the anemia in this case was not completely corrected, we still consider the treatment to be successful because of the negative antibody result, increased reticulocyte count and detectable EPO concentration.
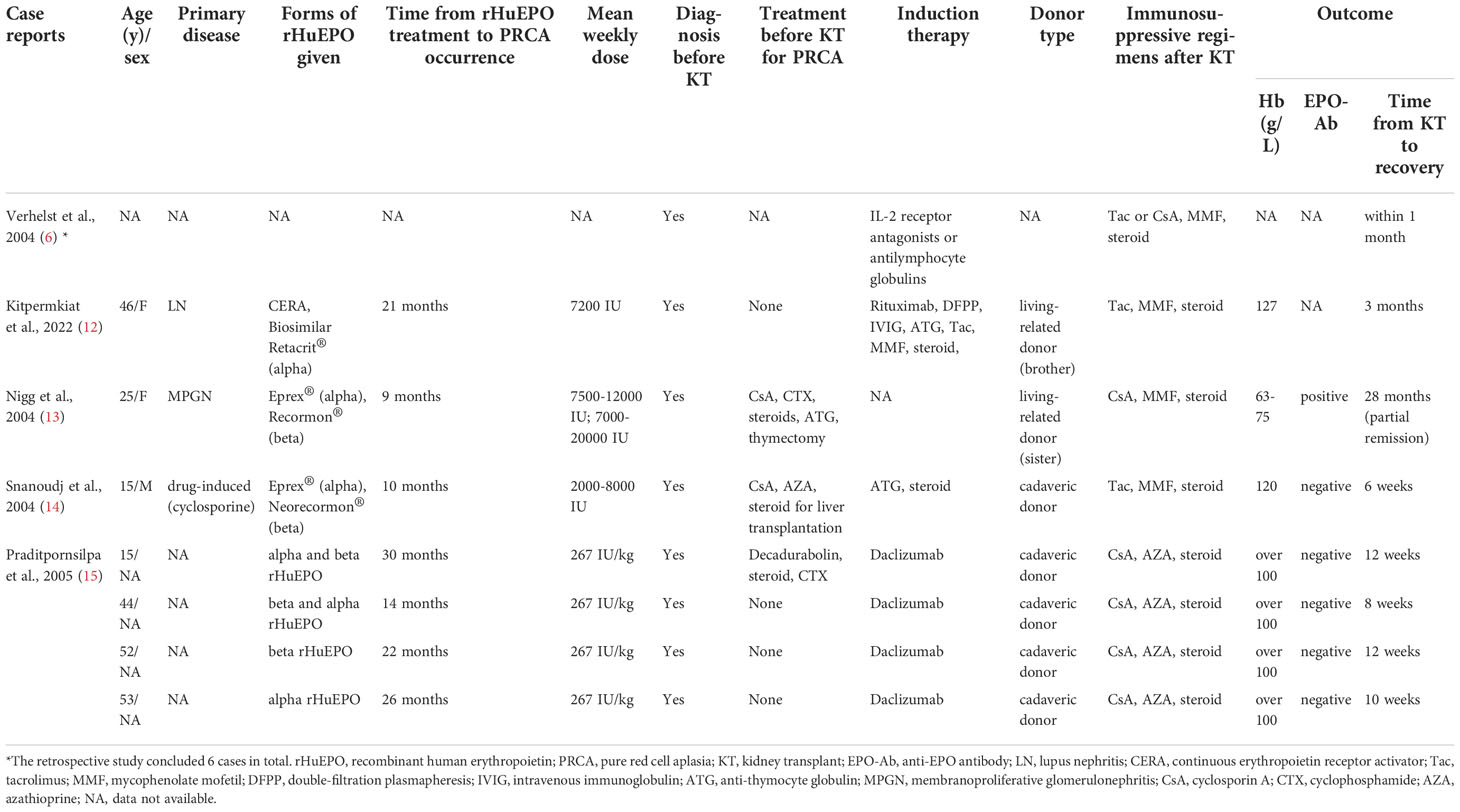
Table 1 Clinical characteristics of 13 reported cases of anti-rHuEPO antibody-mediated PRCA who underwent kidney transplantation.
The patient was diagnosed 1 month after kidney transplantation after identifying anti-EPO antibodies, which highlights the importance of the timely detection of anti-EPO antibodies in suspected patients (16). The timely diagnosis before renal transplant can not only prevent the accumulation of rHuEPO but also guide the selection of immunosuppressive agents for subsequent treatment. Current assays for anti-EPO antibody examination include radioimmunoprecipitation (RIP), enzyme linked immunosorbent assay (ELISA), surface plasmon resonance (BIAcore) and bioassays that measure the proliferation of EPO-dependent primary erythroid cells or cell lines. Characteristics of the four assays used to measure anti-EPO antibodies are shown in Table 2. No single assay can both detect and fully characterize the presence of Abs and determine their neutralizing capabilities of them. Each assay has its own particular level of sensitivity and specificity for detecting Ab isotypes or binding affinities. At least two assays must be used for the analysis of EPO Abs, one assay for confirming the existence of Abs and the other (a bioassay) to demonstrate the Abs’ ability to inhibit the biological activity of epoetin in living cells. Various laboratories have used different assays for detecting anti-EPO Abs. Due to the lack of standardized processes and reagents, it is difficult to compare the test results from different laboratories directly. In addition, laboratories capable of carrying out such tests were quite few, which leads to the extremely long turn-around-time for the anti-EPO antibody detection. Only a few previous cases have reported antibody titer monitoring during treatment with sophisticated bioassay methods. We recommended the aforementioned simple mixing test for the diagnosis and therapeutic monitoring of PRCA mediated by anti-EPO antibodies. Our simple mixing test is time-and cost-effective, which can be used for rapid differential diagnosis and timely therapeutic effect evaluation.
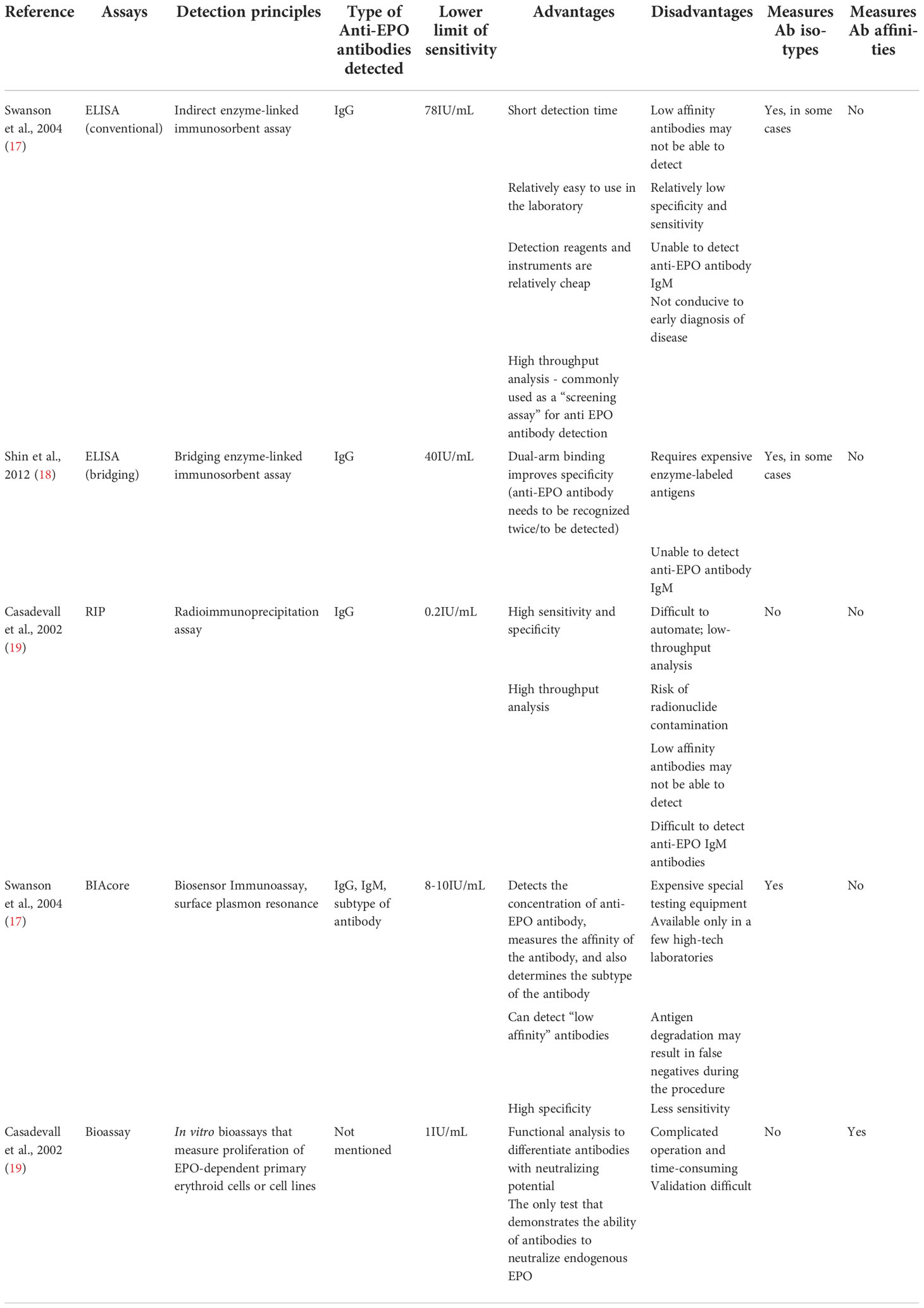
Table 2 Characteristics of the four assays used to measure anti-EPO antibodies.
In this case, a large number of antibodies were removed from a titer of 1:720 to 1:30 after 6 rounds of plasmapheresis. To protect the graft kidney function, preventing the production of EPO-neutralizing antibodies and eliminating residual antibodies is essential. Therefore, we finally chose cyclosporine, sirolimus and prednisone for immunosuppressive treatment. After four-month treatment of the adjusted regimen, the antibody titer dropped to 1:1, the reticulocyte count began to rise, and the transfusion frequency began to drop. At the fifth month of the treatment, EPO could be detected in the patient’s serum, and the reticulocyte count was higher than the normal range, indicating that the bone marrow began to restore hematopoiesis. To our knowledge, this was the first reported case of successful remission of persistent PRCA after kidney transplantation using such treatment regimen. Moreover, this patient’s PRCA was refractory with an abnormally prolonged disease course. Recently, studies had recommended initial treatment, including cyclosporine or cyclophosphamide combined with prednisone in PRCA (9, 11, 20). Tacrolimus may be considered as a substitute for cyclosporine (21). Chen et al. also reported the therapeutic effect of sirolimus in PRCA patients with a complete response of 58.3% and a median time of 4 (1–7) months to achieve the optimal effect (22).
In addition, roxadustat is an oral hypoxia-inducible factor prolyl hydroxylase inhibitor that simulates intracellular hypoxia to promote the production of endogenous EPO. Successful treatment with roxadustat in anti-EPO antibody-mediated PRCA has been noted in some case reports (23–25). However, it was reported that anti-EPO antibodies were found in patients who had never received rHuEPO (26), indicating that endogenous EPO may also induce the development of autoantibodies. Therefore, considering the possible interference of roxadustat in antibody production and its limited therapeutic effect when massive anti-EPO antibodies still existed, we stopped roxadustat treatment when anti-EPO antibody titer increased dramatically in Sep 2021 and restarted roxadustat when anti-EPO antibodies were below the lower limit of detection in Mar 2022. Our result demonstrated the safety of roxadustat in PRCA because no reproduction of anti-EPO antibody was found after restarting roxadustat. However, the data of our patient did not show the effectiveness of roxadustat, which may be related to the short observation time.
In conclusion, we reported a case of anti-EPO antibody-mediated persistent PRCA after renal transplant. Cyclosporine, sirolimus and methylprednisolone could be considered as maintenance immunosuppressive regimen and washed red blood cells should be used instead of leukodepleted red blood cells if transfusion was needed. Plasmapheresis was useful when anti-EPO antibody titers reached quite high. We created a simple mixing test for anti-EPO antibody titer, which was helpful in dynamic antibody monitoring especially when the examination of anti-EPO antibodies with RIPA, ELISA or biosensor assay was not available.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Committee on Medical Ethics of West China Hospital, Sichuan University. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
The original manuscript was written by HL and X-MC and reviewed by Y-YS, Y-JB, L-LW and YW, while YW and Y-YS participated in the treatments for the patients. The test for anti-EPO antibodies were conducted by X-MC and Y-JB. All authors contributed to the article and approved the submitted version.
Supported by 1·3·5 project for disciplines of excellence Clinical Research Incubation Project, West China Hospital, Sichuan University (ZYJC18004).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.1049444/full#supplementary-material
Supplementary Figure 1 | The flow chart of experiment
1. McKoy JM, Stonecash RE, Cournoyer D, Rossert J, Nissenson AR, Raisch DW, et al. Epoetin-associated pure red cell aplasia: Past, present, and future considerations. Transfusion (2008) 48(8):1754–62. doi: 10.1111/j.1537-2995.2008.01749.x
2. Casadevall N. Antibodies against rhuepo: Native and recombinant. Nephrol Dialysis Transplant (2002) 17(suppl_5):42–7.
3. Means RT Jr. Pure red cell aplasia. Blood (2016) 128(21):2504–9. doi: 10.1182/blood-2016-05-717140
4. Boven K, Knight J, Bader F, Rossert J, Eckardt KU, Casadevall N. Epoetin-associated pure red cell aplasia in patients with chronic kidney disease: Solving the mystery. Nephrol Dial Transplant (2005) 20 Suppl 3:iii33–40. doi: 10.1093/ndt/gfh1072
5. Bennett CL, Luminari S, Nissenson AR, Tallman MS, Klinge SA, McWilliams N, et al. Pure red-cell aplasia and epoetin therapy. N Engl J Med (2004) 351:1403–8. doi: 10.1056/NEJMoa040528
6. Verhelst D, Rossert J, Casadevall N, Krüger A, Eckardt KU, Macdougall IC. Treatment of erythropoietin-induced pure red cell aplasia: A retrospective study. Lancet (London England) (2004) 363(9423):1768–71. doi: 10.1016/s0140-6736(04)16302-2
7. Dameshek W, Neber J. Transfusion reactions to plasma constituent of whole blood; their pathogenesis and treatment by washed red blood cell transfusions. Blood (1950) 5(2):129–47. doi: 10.1182/blood.V5.2.129.129
8. Sawada K, Fujishima N, Hirokawa M. Acquired pure red cell aplasia: Updated review of treatment. Br J Haematology (2008) 142(4):505–14. doi: 10.1111/j.1365-2141.2008.07216.x
9. Rossert J, Macdougall I, Casadevall N. Antibody-mediated pure red cell aplasia (Prca) treatment and re-treatment: Multiple options. Nephrol Dial Transplant (2005) 20 Suppl 4:iv23–6. doi: 10.1093/ndt/gfh1090
10. Shingu Y, Nakata T, Sawai S, Tanaka H, Asai O, Tamagaki K, et al. Antibody-mediated pure red cell aplasia related with epoetin-beta pegol (C.E.R.A.) as an erythropoietic agent: Case report of a dialysis patient. BMC Nephrol (2020) 21(1):275. doi: 10.1186/s12882-020-01934-2
11. Bennett CL, Cournoyer D, Carson KR, Rossert J, Luminari S, Evens AM, et al. Long-term outcome of individuals with pure red cell aplasia and antierythropoietin antibodies in patients treated with recombinant epoetin: A follow-up report from the research on adverse drug events and reports (Radar) project. Blood (2005) 106(10):3343–7. doi: 10.1182/blood-2005-02-0508
12. Kitpermkiat R, Thotsiri S, Arpornsujaritkun N, Sangkum P, Chantrathammachart P, Kitpoka P, et al. A 46-Year-Old Thai woman with secondary acquired pure red cell aplasia due to treatment with recombinant erythropoietin while on dialysis for end-stage renal disease who recovered following abo-incompatible kidney transplantation. Am J Case Rep (2022) 23:e935451. doi: 10.12659/ajcr.935451
13. Nigg L, Schanz U, Ambühl PM, Fehr J, Bachli EB. Prolonged course of pure red cell aplasia after erythropoietin therapy. Eur J Haematology (2004) 73(5):376–9. doi: 10.1111/j.1600-0609.2004.00317.x
14. Snanoudj R, Beaudreuil S, Arzouk N, Jacq D, Casadevall N, Charpentier B, et al. Recovery from pure red cell aplasia caused by anti-erythropoietin antibodies after kidney transplantation. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surgeons (2004) 4(2):274–7. doi: 10.1046/j.1600-6143.2003.00297.x
15. Praditpornsilpa K, Buranasot S, Bhokaisuwan N, Avihingsanon Y, Pisitkul T, Kansanabuch T, et al. Recovery from anti-Recombinant-Human-Erythropoietin associated pure red cell aplasia in end-stage renal disease patients after renal transplantation. Nephrology dialysis Transplant Off Publ Eur Dialysis Transplant Assoc - Eur Renal Assoc (2005) 20(3):626–30. doi: 10.1093/ndt/gfh666
16. KDIGO Clinical Practice Guideline Working Group. Chapter 1: Diagnosis and evaluation of anemia in ckd. Kidney Int Suppl (2011) (2012) 2(4):288–91. doi: 10.1038/kisup.2012.33
17. Swanson SJ, Ferbas J, Mayeux P, Casadevall N. Evaluation of methods to detect and characterize antibodies against recombinant human erythropoietin. Nephron Clin Pract (2004) 96(3):c88–95. doi: 10.1159/000076746
18. Shin SK, Moon SJ, Ha SK, Jo YI, Lee TW, Lee YS, et al. Immunogenicity of recombinant human erythropoietin in Korea: A two-year cross-sectional study. Biologicals J Int Assoc Biol Standardization (2012) 40(4):254–61. doi: 10.1016/j.biologicals.2012.02.003
19. Casadevall N, Nataf J, Viron B, Kolta A, Kiladjian JJ, Martin-Dupont P, et al. Pure red-cell aplasia and antierythropoietin antibodies in patients treated with recombinant erythropoietin. New Engl J Med (2002) 346(7):469–75. doi: 10.1056/NEJMoa011931
20. Gurnari C, Maciejewski JP. How I manage acquired pure red cell aplasia in adults. Blood (2021) 137(15):2001–9. doi: 10.1182/blood.2021010898
21. Hashimoto K, Harada M, Kamijo Y. Pure red cell aplasia induced by anti-erythropoietin antibodies, well-controlled with tacrolimus. Int J Hematol (2016) 104(4):502–5. doi: 10.1007/s12185-016-2047-6
22. Chen Z, Liu X, Chen M, Yang C, Han B. Successful sirolimus treatment of patients with pure red cell aplasia complicated with renal insufficiency. Ann Hematol (2020) 99(4):737–41. doi: 10.1007/s00277-020-03946-2
23. Cai KD, Zhu BX, Lin HX, Luo Q. Successful application of roxadustat in the treatment of patients with anti-erythropoietin antibody-mediated renal anaemia: A case report and literature review. J Int Med Res (2021) 49(4):3000605211005984. doi: 10.1177/03000605211005984
24. Wu R, Peng Y. Roxadustat on anti-erythropoietin antibody-related pure red cell aplasia in the patient with end-stage renal disease. Semin Dial (2021) 34(4):319–22. doi: 10.1111/sdi.12991
25. Xu B, Liu S, Li Y, Zhao L, Song X, Chen T. Roxadustat in the treatment of a hemodialysis patient with anti-erythropoietin antibody-mediated pure red cell aplasia. Clin Kidney J (2021) 14(11):2444–5. doi: 10.1093/ckj/sfab134
Keywords: anti-erythropoietin (anti-EPO) antibody, pure red cell aplasia, kidney transplant, immunosuppressive therapy, roxadustat
Citation: Chen X-M, Li H, Wu Y, Wang L-L, Bai Y-J and Shi Y-Y (2022) Case report: Dynamic antibody monitoring in a case of anti-recombinant human erythropoietin-mediated pure red cell aplasia with prolonged course after kidney transplantation. Front. Immunol. 13:1049444. doi: 10.3389/fimmu.2022.1049444
Received: 20 September 2022; Accepted: 11 November 2022;
Published: 29 November 2022.
Edited by:
Xuanchuan Wang, Zhongshan Hospital, Fudan University, ChinaReviewed by:
Wei Wang, Tongji University, ChinaCopyright © 2022 Chen, Li, Wu, Wang, Bai and Shi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yun-Ying Shi, c2hpeXVueWluZ0B3Y2hzY3UuY24=; Yang-Juan Bai, d2hpdGV3Y3Vtc0AxMjYuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.