
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 04 January 2023
Sec. Autoimmune and Autoinflammatory Disorders : Autoimmune Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.1045523
This article is part of the Research Topic Insights in Autoimmune and Autoinflammatory Disorders: 2022 View all 14 articles
 Jakob Höppner1,2‡
Jakob Höppner1,2‡ Christoph Tabeling3,4,5‡
Christoph Tabeling3,4,5‡ Vincent Casteleyn1
Vincent Casteleyn1 Claudia Kedor1Wolfram Windisch2
Claudia Kedor1Wolfram Windisch2 Gerd Rüdiger Burmester1Dörte Huscher6†
Gerd Rüdiger Burmester1Dörte Huscher6† Elise Siegert1,5*†‡
Elise Siegert1,5*†‡Background: Systemic sclerosis (SSc) belongs to the group of connective tissue diseases and is associated with the occurrence of disease-specific autoantibodies. Although it is still controversial whether these antibodies contribute to pathogenesis, there are new insights into the development of these specific antibodies and their possible pathophysiological properties. Interestingly, they are associated with specific clinical manifestations, but for some rarer antibodies this association is not fully clarified. The aim of this study is a comprehensive analysis of the serum autoantibody status in patients with SSc followed by correlation analyses of autoantibodies with the clinical course of the disease.
Methods: Serum from SSc patients was analyzed using a line blot (EUROLINE, EUROIMMUN AG) for SSc-related autoantibodies. Autoantibodies to centromere, Topo-1, antimitochondrial antibodies (AMA) M2 subunit, angiotensin II type 1 receptors (AT1R) and endothelin-1 type-A-receptors (ETAR) were also determined by ELISA. We formed immunological clusters and used principal components analysis (PCA) to assign specific clinical characteristics to these clusters.
Results: A total of 372 SSc patients were included. 95.3% of the patients were antinuclear antibody positive and in 333 patients at least one SSc specific antibody could be detected. Four immunological clusters could be found by PCA. Centromere, Topo-1 and RP3 all formed own clusters, which are associated with distinct clinical phenotypes. We found that patients with an inverted phenotype, such as limited cutaneous SSc patients within the Topo-1 cluster show an increased risk for interstital lung disease compared to ACA positive patients. Anti-AT1R and anti-ETAR autoantibodies were measured in 176 SSc patients; no association with SSc disease manifestation was found. SSc patients with AMA-M2 antibodies showed an increased risk of cardiovascular events.
Conclusion: In our in large cluster analysis, which included an extended autoantibody profile, we were able to show that serologic status of SSc patients provides important clues to disease manifestation, co-morbidities and complications. Line blot was a reliable technique to detect autoantibodies in SSc and detected rarer autoantibodies in 42% of our patients.
Systemic Sclerosis (SSc), also called scleroderma, is a rare autoimmune-mediated rheumatic connective tissue disease (1, 2). Clinically it is a heterogenous condition that ranges from a chronic disease that can remain stable over decades to a life-threatening condition. Disease manifestations can include vasculopathic complications such as digital ulcers (DU), scleroderma renal crisis (SRC) and pulmonary arterial hypertension (PAH), as well as fibrotic complications such as skin fibrosis and interstitial lung disease (ILD) (1, 3). Anti-nuclear antibodies (ANA) are found in as many as 95% of patients with SSc (4). Many patients present with specific anti-centromeres antibodies (ACA), antibodies against topoisomerase 1 (Topo-1, also known as Scl-70) and/or RNA polymerase III (RP3) antibodies (5). The mechanisms underlying the development of these distinct antibodies in SSc are widely unclear, but accumulating data suggest a specific genetic background in combination with environmental and stochastic factors, as well as properties of the antigens themselves are key in antigen selection and antibody production (6–9). Moreover, the pathogenetic role of these autoantibodies in SSc is still a subject of ongoing research (10). Newer data suggest that antibodies could be pathogenic or at least contribute to the perennation of the disease (8, 11, 12). In addition, they have been established as strong predictors of disease outcome, of certain organ complications and therapeutic response (13–15). For example, Topo-1 and RP3 are more specific for dcSSc than ACA. In addition, ACA is associated with PAH without fibrosis while Topo-1 is frequently found in SSc patients with ILD (6). Moreover, RP3 autoantibodies are strongly associated with the incidence of SRC and malignancy. Interestingly, immunochemistry analysis of cancer tissue from anti-RNAP-positive patients revealed a strong RNAP3 staining (16). These data support the idea that cancer initiates a specific immune response which, however, contributes aberrantly to the pathogenesis of SSc with a specific phenotype (17).
Beside these typical associations, recently attention has been drawn to a phenomenon described as “inverted phenotype”, i.e, when there is a discordance between autoantibody and type of skin involvement, for example when a patient with anti-Topo-1 autoantibodies presents with limited skin disease (18). This group has been described as taking an intermediate risk position in terms of organ complications (18–20).
There are also less frequently detected serum autoantibodies that are known to be associated with SSc, such as antibodies against TRIM-21/Ro 52, NOR-90, PM-Scl-75, PM-Scl-100, Th/To, Ku, fibrillarin, and PDGFR. Their clinical associations and frequencies are less well defined, as is the significance of positivity for multiple autoantibodies (21). In addition to classical autoantibodies, which are important in the diagnosis of SSc, functional autoantibodies to angiotensin II-type1- and endothelin-type-A-receptors have also been described for SSc (22–25). Via G protein-coupled receptor stimulation, these functional autoantibodies may be potentially pathogenic and responsible for different clinical manifestations (22, 26). However, the associations with different SSc manifestations remain in parts controversial (26, 27).
As common for autoimmune diseases, SSc often coincides with other autoimmune diseases as Hashimoto thyroiditis or primary biliary cholangitis (PBC). PBC is a chronic cholestatic liver disease characterized by destruction of small intrahepatic bile ducts, leading to liver fibrosis and potential cirrhosis through resulting complications. The serological hallmark of primary biliary cirrhosis is the antimitochondrial antibody (AMA) (28). The prevalence of clinically significant PBC in patients with systemic sclerosis is estimated to be 2.5% (29, 30), and up to 25% of SSc patients are positive for AMA (31). Moreover a positive ACA is reported in 9 – 30% of PBC patients (29, 32, 33). Some reports suggest that PBC-SSc is associated with a more favorable prognosis of PBC whereas others report increased mortality due to SSc (29). In addition, several studies have concluded that patients with PBC may have an increased risk for cardiovascular complications (34, 35). However, these results are controversial (36–38). Concerning SSc, the cardiovascular effects of SSc-PBC or AMA positivity have not yet been defined.
Screening for antibodies is usually performed through indirect immunofluorescence staining (IIF). However, additional techniques, such as enzyme-linked immunosorbent assay (ELISA), immunodiffusion and immunoprecipitation, are used to identify specific SSc autoantibodies (13, 39, 40). Although, these immuno-assays may differ in terms of test characteristics and validation of results is crucial (41, 42).
In the present study, we investigated an extended autoantibody serum status in SSc patients using two different immunological methods and correlated the immunological phenotype of SSc patients with the clinical phenotype using cluster analysis. Here, we provide novel insights into the frequencies and associations of the antibodies especially with focus on inverted phenotypes, rarer antibodies as well as atypical antibodies such as AMA-M2.
SSc patients from our center at the Department of Rheumatology, Charité - Universitätsmedizin Berlin, Germany were recruited between April 2013 and October 2018. The study protocol was approved by the Charité - Universitätsmedizin Berlin Ethics Committee (EA1/179/17). Written informed consent was obtained from each patient. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Clinical parameters including sex, age, cutaneous subsets (43), age at onset of Raynaud’s phenomenon and age at onset of first non–Raynaud’s phenomenon symptom, disease duration and organ involvement were recorded. Variables collected included smoking history, digital ulcers, digital gangrene, calcinosis, highest modified Rodnan Skin Score (mRSS), systemic hypertension, hyperlipidemia, diabetes mellitus, myocardial infarction, angina pectoris, stroke, transitory ischemic attack (TIA), periphery arterial disease (PAD), PBC, PAH, ILD, SRC, heart involvement (defined as an increase in NT-proBNP and/or TropT and/or structural and/or functional damage diagnosed on echocardiography/cardiac MRI after excluding causes other than SSc) and myositis. Laboratory parameters (C-reactive protein [CRP], neutrophile count, hemoglobin, N-terminal pro-B-type natriuretic peptide [NT-proBNP]) were quantified from peripheral blood during clinical routine. Lung function was assessed via spirometry. Diffusing capacity for carbon monoxide (DLCO) was measured using the single-breath method. PAH was defined as a mean pulmonary artery pressure of ≥ 25 mmHg and a pulmonary capillary wedge pressure of ≤ 15 mmHg on right-sided heart catheterization. ILD was defined as the presence of pulmonary fibrosis on high-resolution computed tomography scan evaluated by experienced radiologists where HR-CT was performed upon clinical suspicion.
Serum aliquots were stored at -80°C prior to analyses. Sera were analyzed using commercially available ELISA and line immunoblot assay (all from EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, Germany) according to the manufacturer’s instructions. The EUROLINE Systemic sclerosis (Nucleoli) profile (IgG) contains 13 recombinant antigens: DNA-topoisomerase I (Scl‐70), centromere proteins A & B (CENP‐A and CENP‐B), RNA polymerase III (subunits RP11 and RP155), fibrillarin, NOR‐90, Th/To, PM-Scl‐100, PM-Scl‐75, Ku, platelet-derived growth factor receptors (PDGFR), and Ro-52. Samples were analyzed at a dilution of 1:101 for line immunoblot testing. Autoantibodies were detected using alkaline phosphatase–labeled anti‐human IgG. The EUROLINE flatbed scanner provides semi-quantitative results. Readings obtained with a signal intensity of 0-5 (-) and 6-10 (borderline) were considered negative. Positive measuring range was categorized as 11-25 (+), 26-50 (++), and above (+++).
ELISA detecting antibodies against M2-3E antigens were used with samples diluted 1:101. For Scl-70 or centromeres a dilution of 1:201 was applied. The Anti-M2-3E ELISA serves the serological detection of autoantibodies against mitochondria (AMA), precisely against AMA-M2, by an antigen mix of native M2 and a recombinant fusion protein. Anti-human-IgG HRP (EUROIMMUN) were used as the standard secondary antibody conjugate for all ELISA. Results were reported using a positive cut-off at ≥20 RU/ml. Anti-AT1R and Anti-ETAR antibody serum levels were measured by ELISA (CellTrend GmbH, Luckenwalde, Germany [since 2012, One Lambda, Inc., Canoga Park, CA]) as described (24), analogously to anti-ETB receptor autoantibody quantification performed earlier in a partially overlapping cohort (44).
In an explorative approach, two-step cluster analyses with automated selection of the numbers of clusters were conducted to identify patient clusters with specific antibody patterns, and to understand which antibodies determine those specific profiles. To investigate the underlying patterns in the dataset principal components analysis (PCA) of the autoantibody scores was performed in the MEDA package (R Library Facto-MineR) in Jamovi (45–47). Dimensions 1 and 2 were used for clustering of SSc patients into autoantibody-defined subgroups unsing K-means algorithm. The optimal number of clusters was determined using the elbow method. Clinical associations with these autoantibody clusters were explored using the v test function, which compares each group mean to the overall mean. Continuous data are shown as mean and standard deviation (SD) or median and interquartile range (IQR), categorical data as count and percentages. Depending on the distribution, for group comparisons of serum levels t-test or Mann-Whitney U test was performed, for categorical variables on autoantibody status the Chi-Square test or Fisher’s test. Chi-Square test or Fisher’s test was also performed for clinical associations of the less frequent autoantibodies. P-values <0.05 were considered statistically significant. Due to the exploratory nature of the study no adjustment for multiple testing was applied. For statistical analysis, IBM SPSS Statistics version 28.0 and Jamovi (45) were used.
372 patients fulfilled the ACR/EULAR 2013 classification criteria for SSc. 238 (64.0%) were defined as lcSSc, 104 (28.0%) dcSSc and 30 (8.0) as SSc sine scleroderma. Clinical data are summarized in Table 1. 87% of patients had Raynauds phenomenon. There was a prevalence of 34.9% of ILD when HR-CT was performed upon clinical suspicion and 12.4% of PAH when right heart catheter was performed upon clinical suspicion. Cardiac involvement was present in 8% of all patients, 35.8% had a history of DU. SRC was present in 2.7%. Arthritis was present in 9% of the patients, 8% had a history of calcinosis, and 7.8% had a history of malignancy.
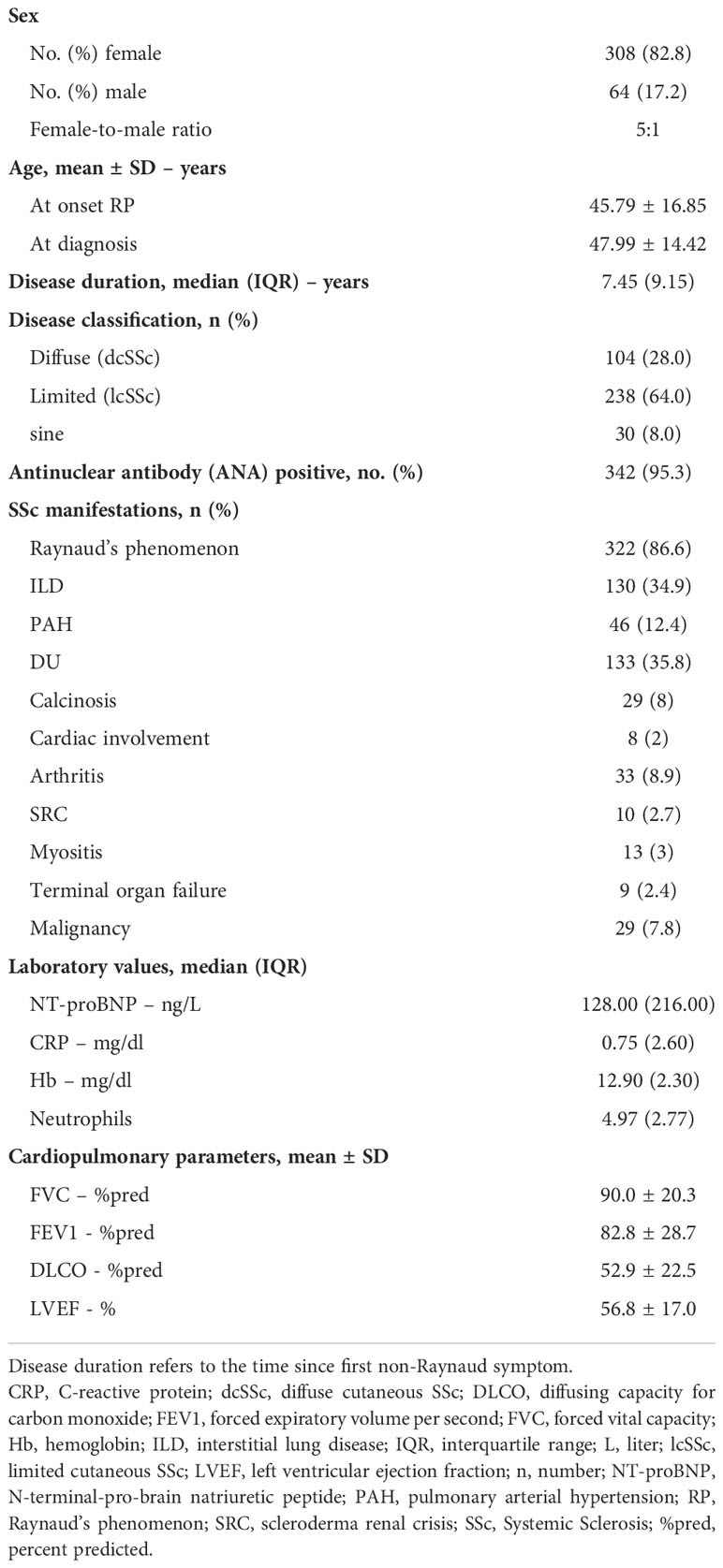
Table 1 Demographic, clinical, and serologic characteristics (n=372).
Counts of individual autoantibodies and their expression, either monospecific or the number of times they appeared in combination with other autoantibodies, are shown in Table 2. 125 patients (32.8%) had a monospecific autoantibody, while 138 (36.2%), 61 (16.0%), and 9 (2.4%) patients were positive for 2, 3, or more autoantibodies, respectively. The majority of patients were positive for ACA (ACA-CA or CB), Topo-1 or Ro52.
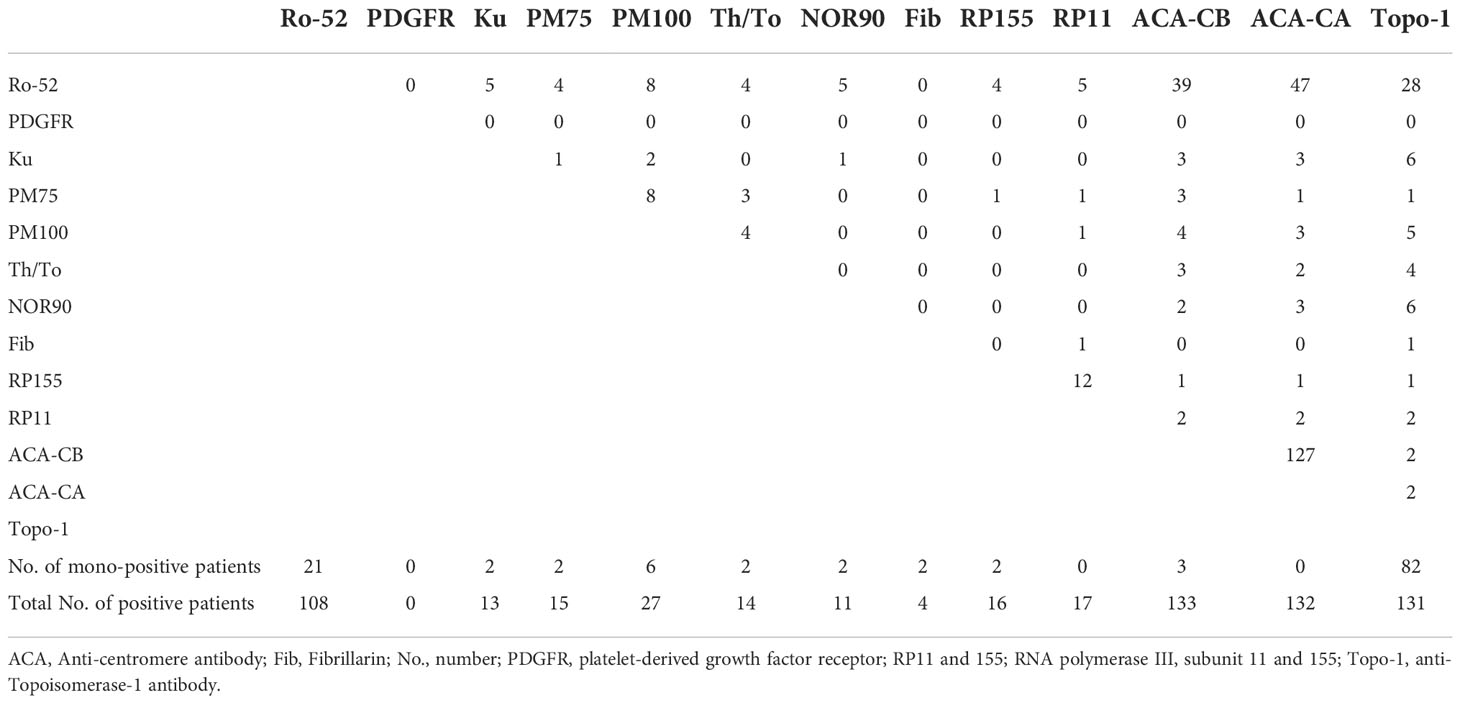
Table 2 Numbers and combinations of autoantibodies identified in the 372 SSc patients.
82 patients (22%) were monospecific for Topo-1 and 21 patients (5.6%) for Ro52. Co-expression of autoantibodies was common (Table 2 and Supplementary Figure 1). Ro52 was the most frequent autoantibody that occurred in combination with other autoantibodies. Topo-1 was detected in 131 patients and ACA (CA and CB) were observed in 138 patients. 132 patients were ACA-CA and 133 were ACA-CB positive. 21 patients were found positive for RP3 (RP11 and RP155). PDGFR was not found in any of our patients. Co-expression of ACA and Topo-1 occurred rarely (4 of 372), as well as co-expression of Topo-1 and RP3 (3 of 372), and co-expression of ACA and RP3 (3 of 372).
ACA and Topo-1 were measured both by ELISA and line blot. 132 patients were positive for anti-centromere antibodies in the ELISA and 138 patients were positive for ACA in the line blot (blot sensitivity for ACA 100%, blot specificity for ACA 97.5%). 125 patients were Topo-1 positive in the ELISA and 131 patients were Topo-1 positive in the line blot (blot sensitivity for Topo-1 100%, blot specificity for Topo-1 97.6%). Of the four patients double-positive for ACA and Topo-1 in the line blot, only one patient was also double-positive in the ELISA, three patients were ELISA-positive for Topo I only and one patient was both ACA and Topo-1 negative in the ELISA.
Principal component analysis is an unsupervised machine learning technique which is applied to reduce the dimensionality of the input data, thus provides valuable insights even in very complex multivariate data sets. PCA of autoantibody levels was performed to examine underlying patterns in the clinical data set. It revealed strong negative associations between the 3 major autoantibodies (Figure 1). Subsequently, K-means method was used to identify clusters in the data set. The K-means algorithm is an iterative method divides the data set into unique, non-overlapping subgroups (clusters), where each data point belongs to only one group. Using K-means clustering algorithm we were able to identify 4 autoantibody clusters, which we named after the assigned antibodies: RP3, Topo-1, Others and ACA (Figure 2).
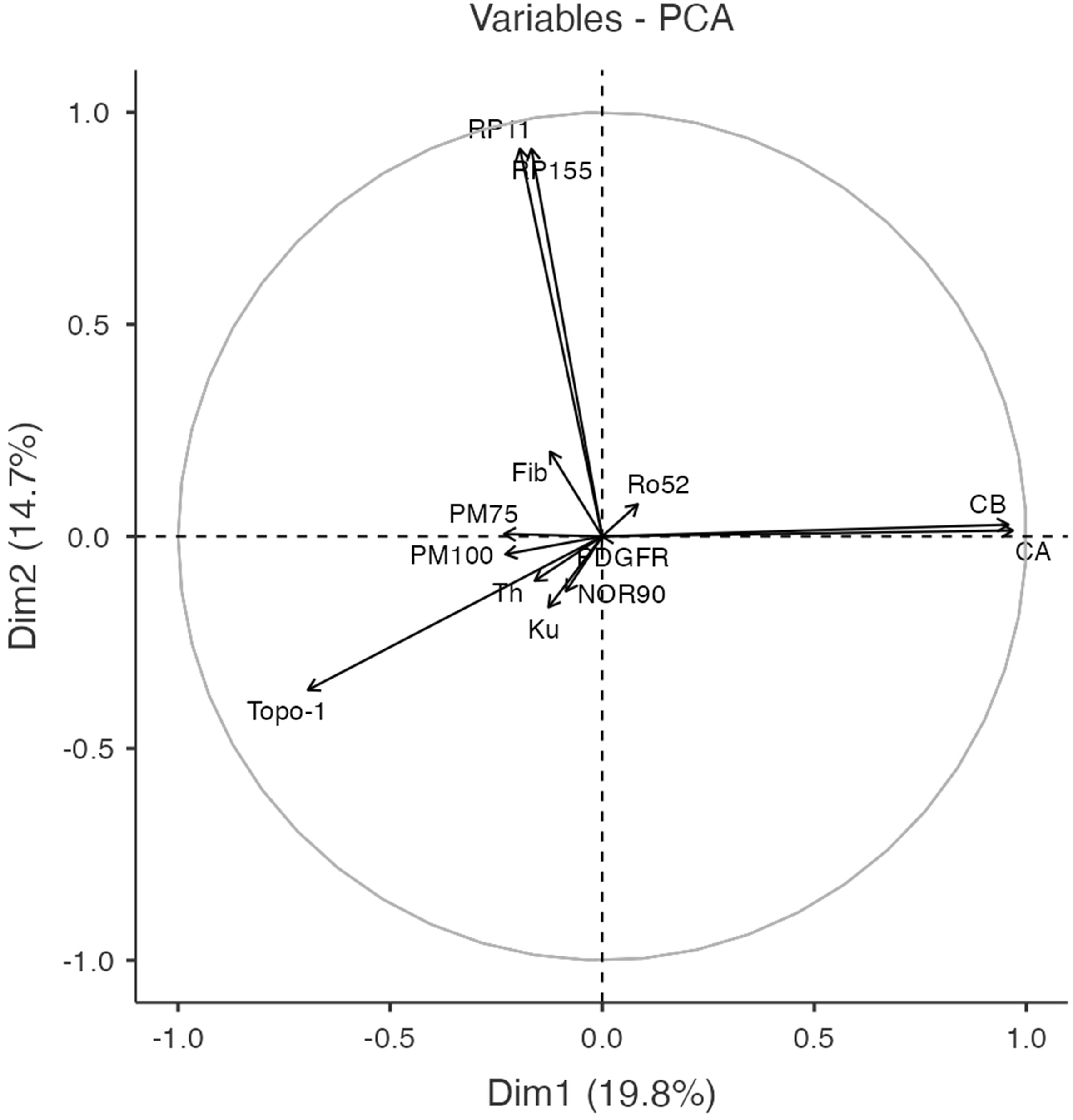
Figure 1 Correlation circle plot of the first 2 dimensions (Dim 1 and Dim 2) of the principal components analysis, which accounted for 34.5% of the total variance. This plot illustrates strong correlations between RNA polymerase 3 (RP3) epitope 11 and epitope 155 as well as between ACA epitopes.
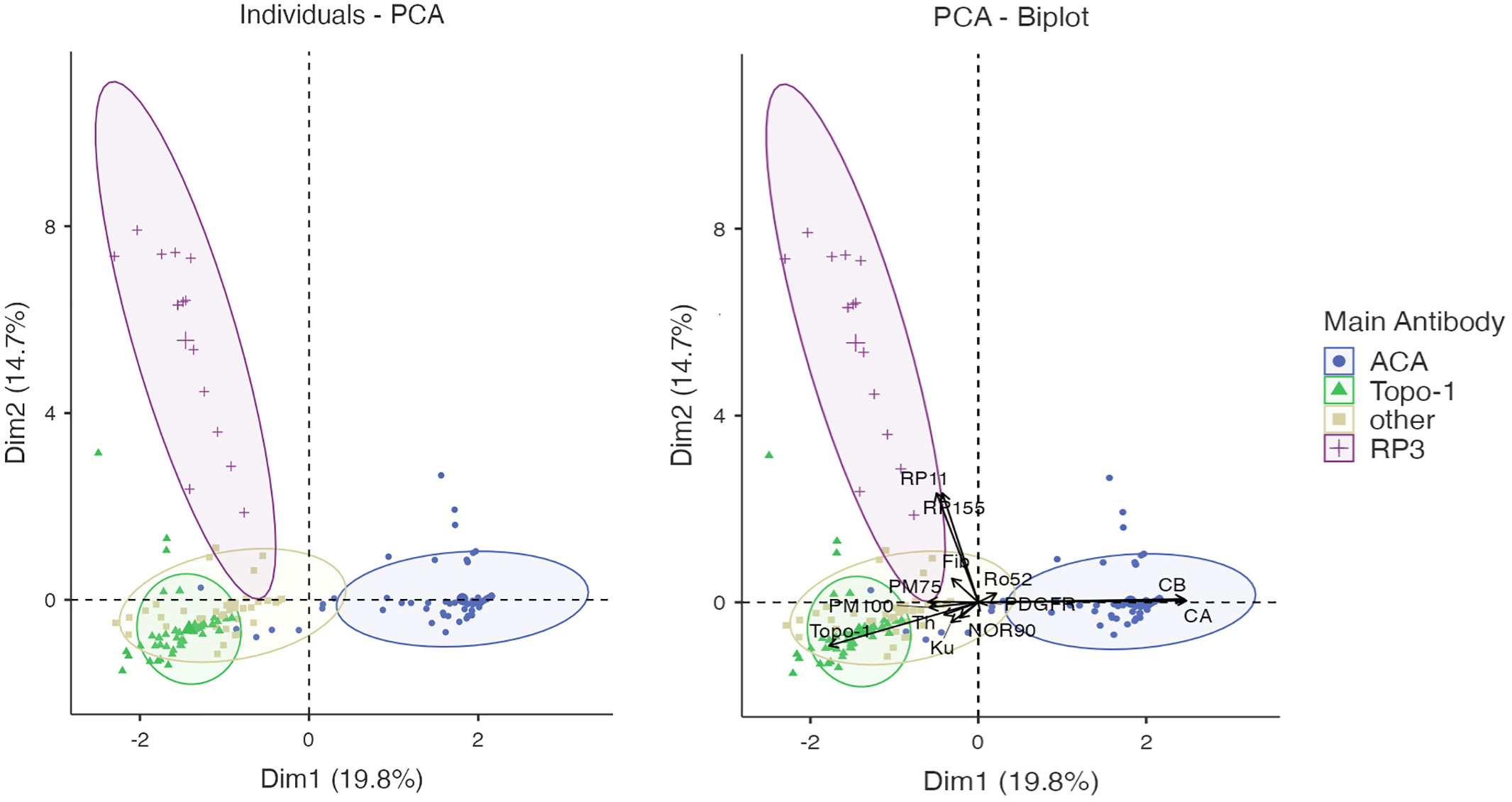
Figure 2 Clustering by K-means method revealed 4 autoantibody clusters: ACA, Topo-1, Others and RP3.
The 4 SSc clusters identified by principal components analysis were assessed with regard to their clinical characteristics. The results are shown in Table 3. Cluster ACA revealed many features consistent with limited cutaneous SSc, including female sex, lower neutrophil granulocyte count, PAD and coexisting PBC and was inversely associated with ILD, cardiac involvement, and impairment in lung function parameters. Cluster RP3 demonstrated multiple features of diffuse cutaneous SSc, including high mRSS, elevated NT-pro BNP, and SRC. Clusterc Topo-1 also shows several features of dcSSc, including ILD, DU, elevated mRSS, reduced FVC, cases of terminal organ failure, and elevated neutrophil granulocyte count. Cluster Others was positively associated with older age of RP onset, myositis, reduced FEV1 and DLCO and elevated NT-pro BNP and inversely associated lcSSc and DU.
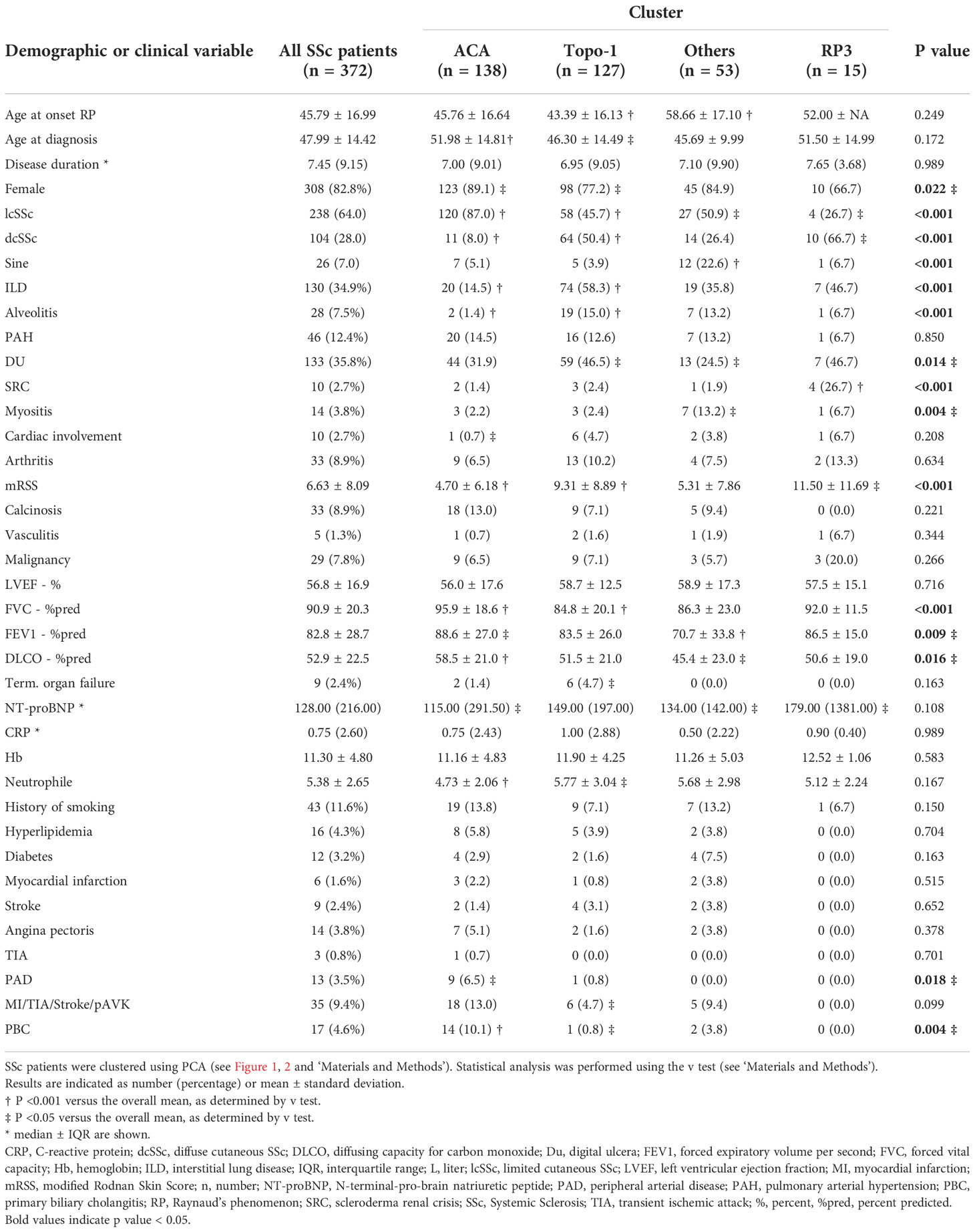
Table 3 Clinical manifestations of SSc clusters.
59 Topo-1 positive patients (45.0%) had lcSSc and 11 ACA positive patients had dcSSc (Table 4). Compared to Topo-1 dcSSc patients, Topo-1 lcSSc patients had a higher DLCO and FVC and less skin sclerosis. Moreover, they tended to have a higher prevalence of calcinosis, an increased risk for cardiovascular disease and a lower prevalence of ILD and less risk for myositis. Compared to ACA lcSSc patients, ILD was more prevalent in Topo-1 lcSSc than in ACA lcSSc patients and FVC was significantly decreased in Topo-1 lcSSc, compared with ACA lcSSc. Also, ILD was slightly less prevalent in the Topo-1 lcSSc than in Topo-1 dcSSc patients. Compared to ACA lcSSc patients, ACA dcSSc patients tended to develop calcinosis cutis less frequently. Compared to Topo-1 dcSSc, ACA dcSSc patients were less likely to suffer from ILD.
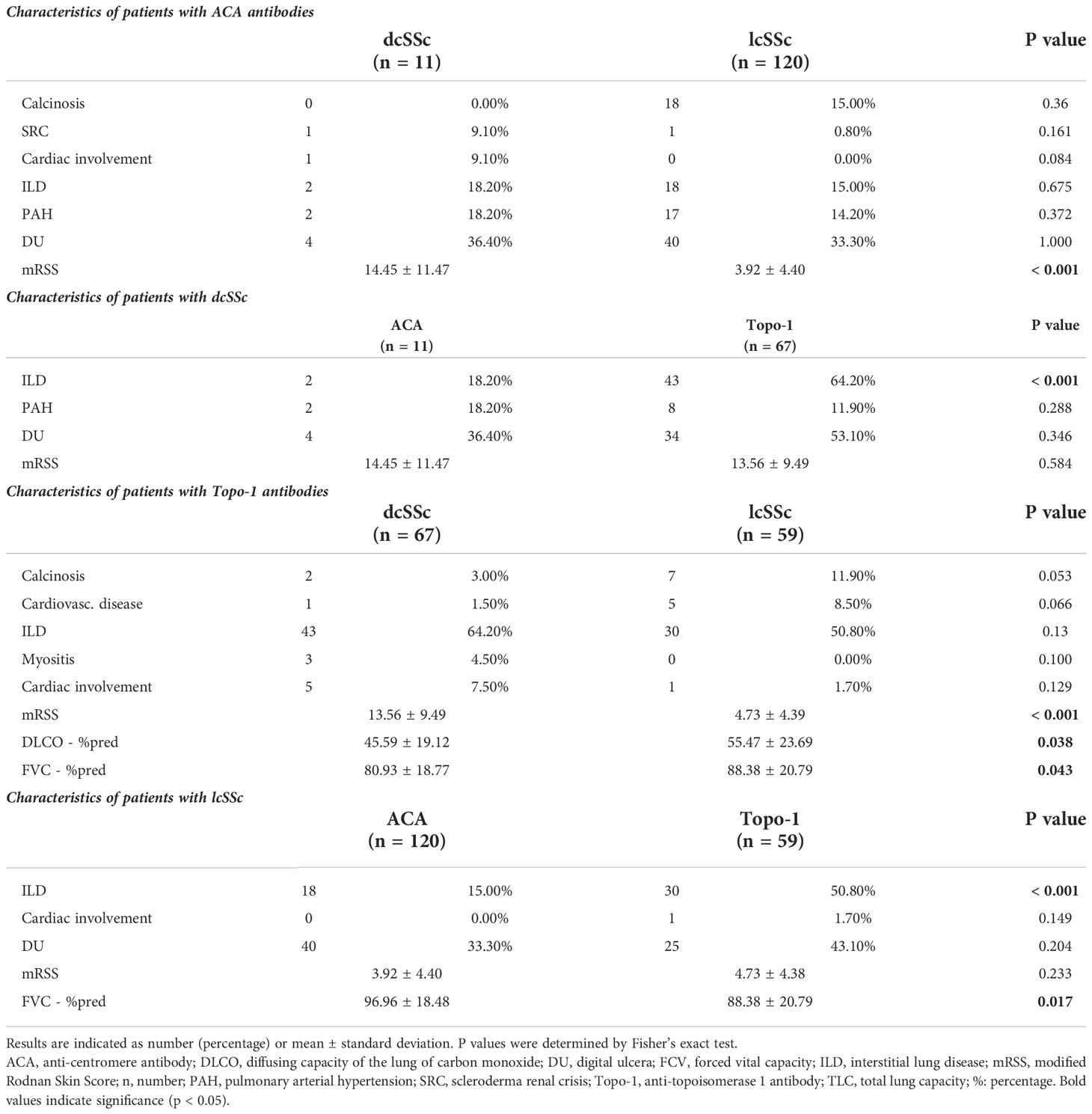
Table 4 Characteristics of patients with inverted phenotype.
Univariate analysis was performed to investigate clinical associations with the presence of TRIM-21/Ro52, NOR-90, PM-Scl-75, PM-Scl-100, Th/To, Ku, fibrillarin (fib, also known as U3RNP) and PDGFR. Statistically significant associations or those approaching statistical significance are summarized in Table 5.
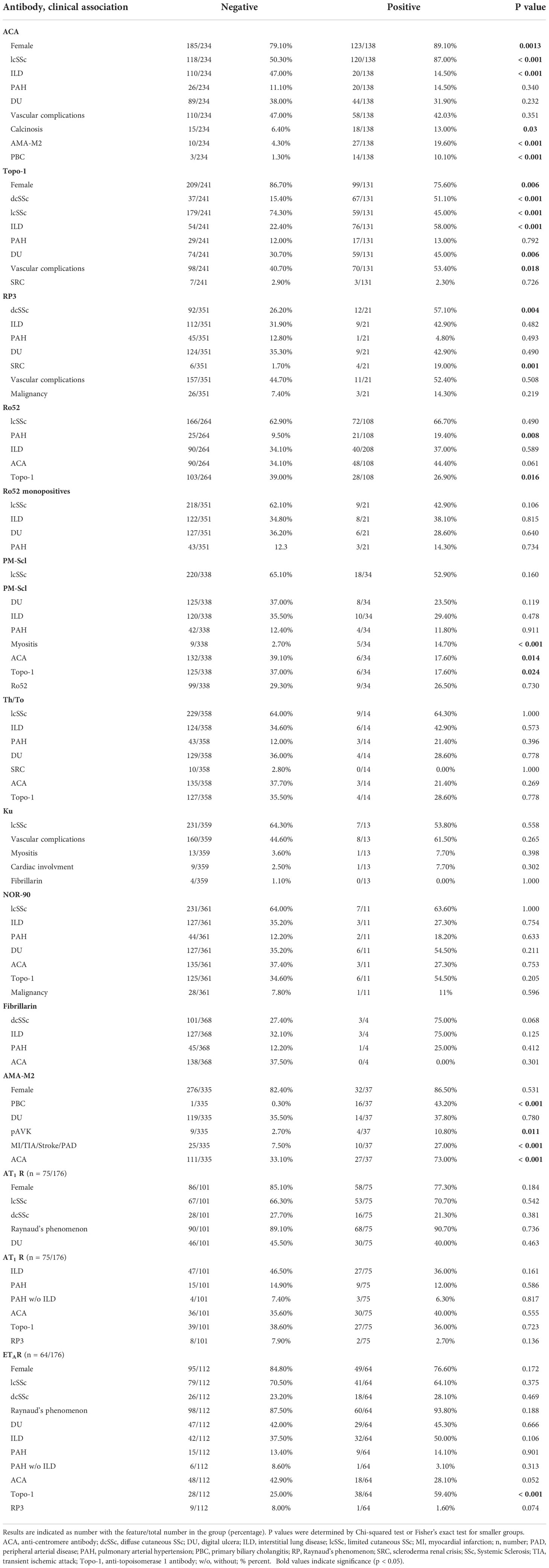
Table 5 Clinical characteristics of the SSc-associated autoantibodies.
Ro52 and PM-Scl-75 or PM-Scl-100 were the most common other SSc-associated autoantibodies. 108 patients were positive for Ro52. Ro52 was more commonly seen in the presence of ACA (48/108). Only 26.9% of the Ro52-positive patients were Topo-1 positive. 19.4% of the Ro52 positive patients were diagnosed with PAH, compared to 9.5% of Ro52 negative patients (p = 0.008). 32.40% of Ro52 positive patients were diagnosed with ILD, compared with 32.6% of the patients negative for Ro52. 21 patients (5.6%) were monospecifically positive for Ro52. However, monospecificity for Ro52 was not associated with a distinct clinical disease pattern.
Given the low numbers of patients with antibodies against PM-Scl-75/100 (34 of 372), Th/To (24 of 372), Ku (13 of 372), fibrillarin (4 of 372) and NOR- 90 (11 of 372), any associations reported should be interpreted with caution: In our cohort, 34 patients were positive for PM-Scl-75/100 (27 female, 7 male), and 12 were monospecifically positive for PM-Scl-75/100. PM-Scl was associated with myositis and inversely associated with coexisting ACA or Topo-1. In addition, there was a negative trend for DU. Ku was found in 13 patients equally in lcSSc and dcSSc. All patients had Raynaud’s phenomenon. However, no significant association with a distinct clinical pattern was found. Fib-positive patients had diffuse cutaneous involvement and a tended to have ILD. 21.4% (n=3) of Th/To positive patients had PAH. Patients with NOR90 tended to show an increased incidence of DU and a coexistence of Topo-1.
In 39 patients (10.5%) no specific autoantibody could be detected by line blot analysis. Of these 26 patients (66.7%) were positive for ANAs while 13 (33.3%) were negative for ANAs. Among the 26 patients positive for ANAs there were many different ANA patterns on HEp-2 indirect immunofluorescence assay. The most common patterns were AC-4 (nuclear fine speckled; n=9) and AC-8 (homogeneous nucleolar; n=9). Less common were AC-1 (nuclear homogeneous; n=3), AC-5 (nuclear large/coarse speckled; n=2, one of which was positive for anti-U1RNP antibodies), AC-3 (centromere; n=1) and AC-6 (nuclear dots; n=1); one pattern was not attributable to any of the defined ANA patterns. Of note, except for the one patient with AC-5 pattern who was found positive for anti-U1-RNP antibodies on routine diagnostics, none of the other patients showed any other SSc-associated antibodies such as anti-SSA, anti-SSB or anti-U1-RNP. Interestingly, 6 of these 26 ANA-positive patients showed cytoplasmatic antibodies in addition to ANAs. Of these 6 patients 3 presented with a pattern that suggests anti-centrosome antibodies. For the 13 ANA-negative patients information on HEp-2 indirect immunofluorescence patterns was available for 7/13 patients. Six samples showed staining consistent with cytoplasmatic autoantibodies of which three were directed against elements of the cytoskeleton and three showed other cytoplasmatic patterns; one sample did not show any evidence of cytoplasmatic autoantibodies.
In our cohort, 37 patients (9.9%) were positive for AMA-M2 (86% female) (Table 5). 73.0% patients were positive for ACA (p < 0.001), 5 patients were Topo-1 positive and 2 patients were positive for RP3. 16/37 AMA-M2 positive patients were diagnosed with PBC (p < 0.001). AMA-M2 positive patients with diagnosed PBC tended to have higher γ-glutamyltransferase (gGT), compared with AMA-M2 positive patients without a diagnosis of PBC (87.1 ± 98.8 vs. 43.7 ± 41.1; p = 0.076). 10.8% of AMA-M2 positive patients had PAD compared with 2.7% of AMA-M2 negative patients (p = 0.01) and 27.0% of AMA-M2 positive patients had cardiovascular disease (such as myocadial infarction, TIA, stroke or PAD), compared to 7.5% of AMA-M2 negative patients (p < 0.001). The increased cardiovascular risk applies both to AMA-M2 positive patients with and without PBC (p = 0.004 and p = 0.02).
Anti-AT1R and anti-ETAR autoantibodies were assessed in 176 SSc patients. Demographic data, clinical manifestations, disease duration and serology are shown in Supplementary Table 1. As described before, cut-off values were 9.2 units for anti-AT1R and 10.4 units for anti-ETAR antibodies (25). 42.6% of patients were positive for antibodies against AT1R and 36.4% were positive for anti-ETAR antibodies, respectively. A clear correlation between anti-AT1R and anti-ETAR auto- antibodies was present in patients with SSc (r = 0.75; Supplementary Figure 2A) as described before (25). In our SSc cohort, we did not find significant association between positive AT1R or ETAR status in the serum status of SSc patients with the presence of ILD or PAH (Table 4 and Supplementary Figures 2B, C). Interestingly, patients with anti-ETAR autoantibodies were significantly more often Topo-1 positive compared with patients without anti-ETAR autoantibodies (Table 5).
Autoantibodies are one of the strongest predictors of disease course, outcome and therapeutic response in patients with SSc (4, 15). Nevertheless, uncertainties remain in the clinical association for some autoantibodies. In the present study, we were able to demonstrate that the classical SSc antibodies (ACA, Topo-1 and RP3) show strong negative correlations and form their own clusters to which certain clinical manifestations of SSc can be assigned.
Traditionally, SSc has been classified according to the extent of skin fibrosis (43). However, dermatologic findings are a dynamic process, so the early classification of SSc as limited may need to be revised as the disease progresses (20, 21, 48). In contrast, autoantibodies are a consistent feature of the disease, and it is rare for an autoantibody to disappear. Thus, recent studies have tackled the issue showing that dermatologic evaluation only is not sufficient to classify patients. In our present study, which was performed in a representative cohort of Caucasian SSc patients (49), we could identify different clusters based on clinical features and autoantibody profiles, and thus confirm and further extend the results from others (21, 50).
Due to the nuclear nature of the targets of SSc specific antibodies, both the origin and the pathological role of these antibodies were unclear for a long time. Antibody generation includes the release of neoantigens, post-translational modifications and antigen presentation. In SSc, apoptotic blebs of endothelial cells and Topo-1 release from by apoptotic blebs are described (8, 51, 52). In addition, the release of neutrophil extracellular traps (NETs), also called NETosis, has also been highlighted in SLE as a contributor to autoimmunity and a source for autoantibodies. Recently, Didier et al. could demonstrate evidence for NETosis also in SSc (53). As previously reported, autoantibodies can also be induced as part of the immune response to malignancy (54). We were able to show in our cohort that patients in the RP3 cluster tend to have an increased prevalence of malignancies, which may be involved in the formation of these antibodies. For antigen presentation, major histocompatibility complex genes (human leukocyte antigen, HLA) are most relevant. In SSc, specific HLA-alleles may provide susceptibility to classical disease-specific autoantibodies. For example, Topo-1 was associated with DRB1*11:01/*11:04 in North American Caucasians, DPB1*13:01 in both African American and European-American patients (7). ACAs were found associated with DQB1*05:01/*26 alleles and RP3 with DRB1*04:04, DRB1*11 and DQB1*03 (7). These novel findings may explain why co-expression of multiple SSc-type antibodies is rare and why specific clinical clusters can be assigned to these antibodies (6, 55). In most instances we were able to confirm these associations:
ACA is the most frequently seen autoantibody in SSc patients (4). In our cohort, 37% of patients were ACA positive (Table 3). In literature, the frequency of ACA in patients with SSc has been reported to be 20–30% overall, however, it varies among different ethnic populations (13, 56, 57). Mierau et al. found 35.9% of patients to be ACA positive (49). The detection of ACA led to its inclusion in the ACA cluster in our analysis. In line with previous reports, ACA was associated with lcSSc and inversely associated with ILD. Moreover, ACA positive patients tended to have more PAH and calcinosis. The association of ACA with pulmonary hypertension has been observed in several previous reports (3, 5, 13, 14, 21, 49, 58–62), but not all of them (48, 49). In addition, 19.6% of ACA-positive SSc patients were positive for AMA-M2 and 10.1% were diagnosed with PBC (29).
The prevalence of Topo-1 in our cohort (34%) is in line with the numbers published by others (5, 49, 59). The presence of the Topo-1 led to its assignment to the Topo-1 cluster in our cluster analysis. Topo-1 was significantly associated with dcSSc, however, 44.9% of Topo-1 positive patients had lcSSc. These numbers slightly exceed those reported in the literature (39). Here, again the dynamic nature of skin involvement should be noted, and it cannot be excluded that some of these patients may develop diffuse skin involvement in the course of their disease. The cluster Topo-1 was associated with a higher risk for pulmonary fibrosis and digital ulcers. These results are in line with previous findings (21, 49). The value of Topo-1 as a predictor of SRC is uncertain and controversial in the literature (3, 21, 49, 63). In our cohort, we did not see an association between Topo-1 and SRC.
The third antibody that led to assignment to a clinical cluster was RP3. In line with previous reports, the RP3 cluster in our cohort was associated with dcSSc and higher risk for SRC (64–67).
In their study, Patterson et al. found 2 different autoantibody clusters, depending on the intensity of R3 staining (cluster RNAP III strong and cluster RNAP III weak) (21). Since RP3 titers may change over time (65), the authors concluded, that the clusters RNAP III strong and RNAP III weak may represent different temporal stages of SSc disease (21). However, we could not find this distinction of the cluster in our analysis. It should be noted that Patterson and colleagues included 81 patients with RP3, whereas we only included 21.
Co-expression of the 3 major autoantibodies was only rarely observed in this cohort (Table 2) but it has been also reported in previous reports (21, 49, 68–70). However, presence occasionally may represent a false-positive result. In our cohort, four patients were positive for ACA and Topo-1 in the line blot but only one patient in the ELISA. From an immunological point of view and considering that different genetic predispositions may result in different antibodies, laboratory errors are a reasonable explanation.
When multiple autoantibodies were examined in SSc patients in this study, ACA, Topo I, and RP3 remained the autoantibodies with the most pronounced inverse correlation with each other and are each associated with characteristic clinical features. While co-expression of any of these 3 major autoantibodies remained rare (Table 2), co-expression with other autoantibodies has been found to be frequent (21, 70).
Despite the common associations between specific SSc antibodies and clinical characteristics (Topo-1 and dcSSc, ACA and lcSSc), inverted phenotypes of SSc which refers to the phenomenon that ACA positive patients show a dcSSc phenotype or Topo-1 positive patients show a lcSSc phenotype have been described (19, 20, 71–73). In our study, Topo-1 lcSSc patients had less lung involvement than Topo-1 dcSSc patients. However, Topo-1 lcSSc patients had an increased risk for ILD, when compared with ACA lcSSc (Table 4). This indicates that inverted phenotypes should be considered as a separate group occupying an intermediate risk position in terms of organ complications and underlines the importance of antibody detection (20). In this context, the faSScinate study, which investigated tocilizumab in patients with dcSSc, indicated that the autoantibody status is important for the therapy. Tocilizumab showed significant decrease in rates of lung function decline in Topo-1 positive patients but not in Topo-1 negative patients in phase 2 and 3 studies (15, 74–76). This is further supported by recent studies that confirmed the relevance of the combination of antibodies and assessment of skin involvement for the prognostic assessment of SSc patients. Nihtyanova et al. (77) have shown that a combination of autoantibody status and extent of skin involvement allows a more precise risk stratification of SSc patients than the two single factors themselves (77).
The rarer SSc-associated autoantibodies were not found by principal components analysis to significantly contribute to subclassification. These patients were captured in cluster Other. This cluster was positive associated with higher risk of myositis and elevated NT-proBNP. Negative associations were found for lung function parameters (FVC and DLCO) and DU. Although, the rarer SSc-associated autoantibodies did not contribute to subclassification, clinical associations were assessed in this study (Table 5). In our cohort, Ro52 positivity was associated with presence of PAH. This association has also been discovered by others (21, 74, 75, 78).Others have reported an association between Ro52 and ILD (79). However, Patterson et al. (21) or Lee et al. (78) were not able to replicate these findings. In our study, we were neither able to find this association.
Anti-PM-Scl is reported to predict for lcSSc, myositis, calcinosis and no serious internal organ involvement with good prognosis (49, 80, 81). In our cohort, PM-Scl was associated with myositis, and by trend with lcSSc and DU. Moreover, PM-Scl was negatively associated with co-expression of both ACA and Topo-1. Autoantibodies to Th/To were reported to be specific for SSc or Raynaud’s disease with a short disease duration and lcSSc (82). Moreover, a high risk for severe organ involvement such as ILD and development of PAH and therefore a worse overall prognosis has been reported (83, 84). However, we did not find an association with ILD. For anti-NOR90 antibodies an association with malignancy is described in literature (85). In our cohort, we did not find this association. Moreover, case reports suggests that NOR90 might be associated with lcSSc, mild internal organ involvement and a favorable prognosis (86, 87). We can neither disprove nor confirm these observations. Anti-Ku has been reported in sera from patients with other connective tissue diseases, such as SLE and overlap syndrome, especially myositis (88, 89). However, we could not prove this association with myositis in our cohort. Likewise, others could not find this correlation, neigher (21). Patients with anti-fibrillarin are reported to have dcSSc and vasculopathy, including DU and PAH (4, 90, 91). We can confirm the association to dcSSc in our very small cohort of anti-fibrillarin positive SSc patient. In addition, we see a trend toward increased risk for ILD. Baroni et al. (92) reported autoantibodies against the platelet-derived growth factor receptor (PDGFR) in patients with SSc and for these autoantibodies a pathogenic role is suspected (93–95). However, we did not find any patient with this antibody in our cohort.
In addition to the antibodies included in our study, there are other antibodies that are associated with SSc, such as anti-SSA, anti-SSB and anti-U1RNP antibodies (96, 97). These antibodies may also have specific clinical and immunological associations but including those was beyond the scope of this study. However a previous study has shown a link between the presence of anti-U1RNP antibodies and ILD and joint involvement in SSc (96). That this association might be based on underlying immunological differences is supported by our previously published finding that patients with anti-U1RNP antibodies have a strong activation of the interferon signaling pathway (98). Further studies could elaborate on these findings to assess the pathogenic relevance and immunological implications of specific antibodies and guide personalized treatment decisions.
Also, we found no routinely detectable autoantibodies for SSc in 10.5% of our patients, which is in accordance with previous reports (99) and suggests the presence of yet unknown antibodies. Following the identification of a distinct pattern on immunofluorescence a hypothesis can be made against which cellular structure these antibodies are directed. In a next step, different techniques such as mass spectroscopy, electrophoresis and immunoblotting could be used to analyze the specific targets of these autoantibodies. Interestingly, we found evidence for cytoplasmic autoantibody patterns in both ANA-positive and ANA-negative patients. These were before discovered to be frequently associated to SSc with otherwise no SSc-specific antibodies (100), such as the recently discovered Anti-eIF2B (Eukaryotic initiation factor 2B) (101), which can be found in ANA-negative patients and has clinical associations with dcSSc and SSc-ILD (102).
AT1R- and ETAR-autoantibodies have been shown to be more frequently positive in patients with PAH secondary to SSc or other connective tissue disease when compared to patients with idiopathic PAH or chronic thromboembolic pulmonary hypertension (25). Moreover, their presence has been shown to be associated with vasculopathic changes like endothelial activation and smooth muscle contraction (23, 25, 103) and their presence was associated with SSc-related manifestations like PAH, SRC, DU, lung fibrosis, and mortality (24, 25). However, we were not able to confirm an association of AT1R- and/or ETAR-autoantibody positivity with PAH, SRC, DU or ILD. This might be due to the fact, that our cohort is significantly smaller than the cohort of Riemekasten et al. (24). On the other hand, our findings are in line with findings by Ilgen et al. (27) and Bankamp et al. (26) who were also not able to find these associations.
The significance of a coexisting PBC with SSc is not well understood. To our knowledge, we are the first who demonstrated that SSc patients with positive AMA-M2 had a significantly higher risk of cardiovascular events. No significant difference was found between AMA-M2 positive patients diagnosed with PBC and those without PBC. Both patient groups have an increased cardiovascular risk. Interestingly, as in SSc, also in PBC endothelial dysfunction is thought to be involved in the pathophysiology (104) and Fonollosa et al. found a high prevalence of nailfold capillary abnormalities characteristic of systemic sclerosis in patients with PBC (105).
For the determination of antibodies in SSc, different methods exist, each of which has strengths and weaknesses (106, 107). For clinical practice, simple and cost-efficient methods such as ELISA and immunoblotting have become established (108). In our study we used both methods for the determination of ACA and Topo-1 and could show a good agreement for the EUROLINE blot compared to ELISA. However, it should be noted that both methods are based on similar principles and thus share common sources of error, such as non-specific binding and cross-reactivity (42, 108). Furthermore, it has to be considered that the other antibodies we determined and on which our cluster analysis is based were only determined with a single technique. Mierau et al. analysed sera of 863 SSc patients using different methods including IIF, a comparable line immunoassay as we did, immunoprecipitation and immunodiffusion (49). These authors found a high concordance between the results from those different techniques and broadly similar results to ours on the frequencies and clinical associations of the different antibodies.
In our study, we could confirm and extend previously described correlation between certain autoantibodies and clinical phenotype in SSc in a well characterized Caucasian cohort by an unsupervised machine learning technique. We used line blot data that was partially validated by confirming results by ELISA to determine SSc associated autoantibodies. Although several antibodies were included in our analysis, we found, that the dominant SSc antibody most strongly predicted the clinical phenotype. However, we could highlight the importance of analyzing an extended spectrum of autoantibodies, including antibodies to AMA-M2, which were associated with a prior unknown elevated cardiovascular risk, to best assess clinical phenotypes, as well as organ complications and comorbidities. Despite the described advantages of determining antibody profiles, clinical examination is not obsolete. Especially for inverted phenotypes, we were able to show, that these patients form a special subgroup and that the antibody status of the patients must be evaluated in combination with the clinical examination.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed andapproved by Charité - Universitätsmedizin Berlin EthicsCommittee. The patients/participants provided their writteninformed consent to participate in this study (EA1/179/17).
Study design: JH, ES, DH, GB. Study conduct: JH, VC, CK, CT. Data collection: JH, VC, CK, CT. Data analysis: JH, DH, WW. Data interpretation: JH, CT, GB, DH, ES. Drafting manuscript: JH, GB, ES. Revising manuscript content: JH, VC, CT, CK, WW, GB, DH, ES. Approving final version of manuscript: JH, VC, CT, CK, WW, GB, DH, ES. JH, DH, ES take responsibility for the integrity of the data analysis.
This study was supported by the Edith Busch Foundation, Germany in the form of a research grant to ES. JH received a scholarship from the Daniela und Jürgen Westphal-Stiftung, Hamburg, Germany.
The authors would like to thank Daniel Grund and Udo Schneider for their support on patient recruitment. CT and ES are participants in the BIH-Charité Clinician Scientist Program funded by the Charité – Universitätsmedizin Berlin and the Berlin Institute of Health. The authors gratefully acknowledge Martina Lehmann and Christina Straßer for their excellent technical assistance and Dr. Alexander Kühnl for his valuable scientific communication.
CT received funding for research from Deutsche Gesellschaft für Pneumologie, Bayer HealthCare, Boehringer Ingelheim, and for lectures and advisory from Actelion Pharmaceuticals, Boehringer Ingelheim, GlaxoSmithKline, and for non-financial support from Actelion, ALK-Abelló, Bayer HealthCare, Boehringer Ingelheim and GlaxoSmithKline.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be constructed as a potential conflict of interest.
All clai ms expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.1045523/full#supplementary-material
1. Gabrielli A, Avvedimento EV, Krieg T. Scleroderma. N Engl J Med (2009) 360(19):1989–2003. doi: 10.1056/NEJMra0806188
2. Allanore Y, Simms R, Distler O, Trojanowska M, Pope J, Denton CP, et al. Systemic sclerosis. Nat Rev Dis Primers (2015) 1:15002. doi: 10.1038/nrdp.2015.2
3. Walker UA, Tyndall A, Czirják L, Denton C, Farge-Bancel D, Kowal-Bielecka O, et al. Clinical risk assessment of organ manifestations in systemic sclerosis: A report from the EULAR scleroderma trials and research group database. Ann Rheum Dis (2007) 66(6):754–63. doi: 10.1136/ard.2006.062901
4. Nihtyanova SI, Denton CP. Autoantibodies as predictive tools in systemic sclerosis. Nat Rev Rheumatol (2010) 6(2):112–6. doi: 10.1038/nrrheum.2009.238
5. Steen VD. Autoantibodies in systemic sclerosis. Semin Arthritis Rheumatol (2005) 35(1):35–42. doi: 10.1016/j.semarthrit.2005.03.005
6. Yang C, Tang S, Zhu D, Ding Y, Qiao J. Classical disease-specific autoantibodies in systemic sclerosis: Clinical features, gene susceptibility, and disease stratification. Front Med (Lausanne) (2020) 7:587773(November). doi: 10.3389/fmed.2020.587773
7. Gourh P, Safran SA, Alexander T, Boyden SE, Morgan ND, Shah AA, et al. HLA and autoantibodies define scleroderma subtypes and risk in African and European americans and suggest a role for molecular mimicry. Proc Natl Acad Sci USA (2020) 117(1):552–62. doi: 10.1073/pnas.1906593116
8. Chepy A, Bourel L, Koether V, Launay D, Dubucquoi S, Sobanski V. Can antinuclear antibodies have a pathogenic role in systemic sclerosis? Front Immunol (2022) 13:930970(June). doi: 10.3389/fimmu.2022.930970
9. Rosen A, Casciola-Rosen L. Autoantigens as partners in initiation and propagation of autoimmune rheumatic diseases. Annu Rev Immunol (2016) 34(February):395–420. doi: 10.1146/annurev-immunol-032414-112205
10. Melissaropoulos K, Iliopoulos G, Sakkas LI, Daoussis D. Pathogenetic aspects of systemic sclerosis: A view through the prism of b cells. Front Immunol (2022) 13:925741(June). doi: 10.3389/fimmu.2022.925741
11. Harris ML, Rosen A. Autoimmunity in scleroderma: The origin, pathogenetic role, and clinical significance of autoantibodies. Curr Opin Rheumatol (2003) 15(6):778–84. doi: 10.1097/00002281-200311000-00016
12. Senécal JL, Hoa S, Yang R, Koenig M. Pathogenic roles of autoantibodies in systemic sclerosis: Current understandings in pathogenesis. J Scleroderma Relat Disord (2020) 5(2):103–29. doi: 10.1177/2397198319870667
13. Hamaguchi Y. Autoantibody profiles in systemic sclerosis: Predictive value for clinical evaluation and prognosis. J Dermatol (2010) 37(1):42–53. doi: 10.1111/j.1346-8138.2009.00762.x
14. Hesselstrand R, Scheja A, Shen GQ, Wiik A, Åkesson A. The association of antinuclear antibodies with organ involvement and survival in systemic sclerosis. Rheumatology (2003) 42(4):534–40. doi: 10.1093/rheumatology/keg170
15. Shah S, Denton CP. Scleroderma autoantibodies in guiding monitoring and treatment decisions. Curr Opin Rheumatol (2022) 34:302–10. doi: 10.1097/BOR.0000000000000904
16. Shah AA, Casciola-Rosen L. Mechanistic and clinical insights at the scleroderma-cancer interface. J Scleroderma Relat Disord (2017) 2(3):153–9. doi: 10.5301/jsrd.5000250
17. Shah AA, Laiho M, Rosen A, Casciola-Rosen L. Protective effect against cancer of antibodies to the Large subunits of both RNA polymerases I and III in scleroderma. Arthritis Rheumatol (2019) 71(9):1571–9. doi: 10.1002/art.40893
18. Zanatta E, Huscher D, Ortolan A, Avouac J, Airò P, Balbir-Gurman A, et al. Phenotype of limited cutaneous systemic sclerosis patients with positive anti-topoisomerase I antibodies: data from EUSTAR cohort. Rheumatol (Oxf) (2022). doi: 10.1093/rheumatology/keac188
19. Desai RP, Assassi S. Anti-topoisomerase-positive limited systemic sclerosis has a propensity for interstitial lung disease but is linked to favorable prognosis. Rheumatol (Oxf) (2022) :1–2. doi: 10.1093/rheumatology/keac287
20. Tieu A, Chaigne B, Dunogué B, Dion J, Régent A, Casadevall M, et al. Autoantibodies versus skin fibrosis extent in systemic sclerosis: A case-control study of inverted phenotypes. Diagnostics (2022) 12(5):1067. doi: 10.3390/diagnostics12051067
21. Patterson KA, Roberts-Thomson PJ, Lester S, Tan JA, Hakendorf P, Rischmueller M, et al. Interpretation of an extended autoantibody profile in a well-characterized Australian systemic sclerosis (Scleroderma) cohort using principal components analysis. Arthritis Rheumatol (2015) 67(12):3234–44. doi: 10.1002/art.39316
22. Kill A, Riemekasten G. Functional autoantibodies in systemic sclerosis pathogenesis. Curr Rheumatol Rep (2015) 17(5):1–6. doi: 10.1007/s11926-015-0505-4
23. Kill A, Tabeling C, Undeutsch R, Kuhl AA, Gunther J, Radic M, et al. Autoantibodies to angiotensin and endothelin receptors in systemic sclerosis induce cellular and systemic events associated with disease pathogenesis. Arthritis Res Ther (2014) 16(1):R29. doi: 10.1186/ar4457
24. Riemekasten G, Philippe A, Näther M, Slowinski T, Müller DN, Heidecke H, et al. Involvement of functional autoantibodies against vascular receptors in systemic sclerosis. Ann Rheum Dis (2011) 70(3):530–6. doi: 10.1136/ard.2010.135772
25. Becker MO, Kill A, Kutsche M, Guenther J, Rose A, Tabeling C, et al. Vascular receptor autoantibodies in pulmonary arterial hypertension associated with systemic sclerosis. Am J Respir Crit Care Med (2014) 190(7):808–17. doi: 10.1164/rccm.201403-0442OC
26. Bankamp L, Preuß B, Pecher AC, Beucke N, Henes J, Klein R. Functionally active antibodies to the angiotensin II type 1-receptor measured by a luminometric bioassay do not correlate with clinical manifestations in systemic sclerosis: A comparison with antibodies to vascular receptors and topoisomerase I detected b. Front Immunol (2021) 12:786039(December). doi: 10.3389/fimmu.2021.786039
27. İlgen U, Yayla ME, Düzgün N. Anti-angiotensin II type 1 receptor autoantibodies (AT1R-AAs) in patients with systemic sclerosis: lack of association with disease manifestations. Rheumatol Int (2017) 37(4):593–8. doi: 10.1007/s00296-016-3639-4
28. Carey EJ, Ali AH, Lindor KD. Primary biliary cirrhosis. Lancet (2015) 386(10003):1565–75. doi: 10.1016/S0140-6736(15)00154-3
29. Rigamonti C, Shand LM, Feudjo M, Bunn CC, Black CM, Denton CP, et al. Clinical features and prognosis of primary biliary cirrhosis associated with systemic sclerosis. Gut (2006) 55(3):388–94. doi: 10.1136/gut.2005.075002
30. Norman GL, Bialek A, Encabo S, Butkiewicz B, Wiechowska-Kozlowska A, Brzosko M, et al. Is prevalence of PBC underestimated in patients with systemic sclerosis? Dig Liver Dis (2009) 41(10):762–4. doi: 10.1016/j.dld.2009.01.014
31. Gupta RC, Seibold JR, Krishnan MR, Steigerwald JC. Precipitating autoantibodies to mitochondrial proteins in progressive systemic sclerosis. Clin Exp Immunol (1984) 58(1):68–76.
32. Powell FC, Winkelmann RK, Venencie-Lemarchand F, Spurbeck JL, Schroeter AL. The anticentromere antibody: Disease specificity and clinical significance. Mayo Clin Proc (1984) 59(10):700–6. doi: 10.1016/S0025-6196(12)62059-X
33. Bernstein RM, Callender ME, Neuberger JM, Hughes GR, Williams R. Anticentromere antibody in primary biliary cirrhosis. Ann Rheum Dis (1982) 41(6):612–4. doi: 10.1136/ard.41.6.612
34. Jones DEJ, Hollingsworth K, Fattakhova G, MacGowan G, Taylor R, Blamire A, et al. Impaired cardiovascular function in primary biliary cirrhosis. Am J Physiol - Gastrointest Liver Physiol (2022) 298:764–73. doi: 10.1152/ajpgi.00501.2009
35. Ungprasert P, Wijarnpreecha K, Ahuja W, Spanuchart I, Thongprayoon C. Coronary artery disease in primary biliary cirrhosis: A systematic review and meta-analysis of observational studies. Hepatol Res (2015) 45(11):1055–61. doi: 10.1111/hepr.12452
36. Ungprasert P, Wijarnpreecha K, Thongprayoon C. Risk of cerebrovascular accident in patients with primary biliary cirrhosis: A systematic review. Eur J Gastroenterol Hepatol (2016), 28:90–4. doi: 10.1097/MEG.0000000000000493
37. Doycheva I. Asymptomatic primary biliary cirrhosis is not associated with increased frequency of cardiovascular disease. World J Hepatol (2011) 3(4):93. doi: 10.4254/wjh.v3.i4.93
38. Cash WJ, McCance DR, Young IS, McEneny J, Cadden IS, McDougall NI, et al. Primary biliary cirrhosis is associated with oxidative stress and endothelial dysfunction but not increased cardiovascular risk. Hepatol Res (2022) 40(11):1098–106. doi: 10.1111/j.1872-034X.2010.00717.x
39. Reveille JD, Solomon DH, Schur P, Kavanaugh A, Sherrer YRS, Lahita R. Evidence-based guidelines for the use of immunologic tests: Anticentromere, scl-70, and nucleolar antibodies. Arthritis Care Res (Hoboken) (2003) 49(3):399–412. doi: 10.1002/art.11113
40. van den Hoogen F, Khanna D, Fransen J, Johnson SR, Baron M, Tyndall A, et al. Classification criteria for systemic sclerosis: An American college of rheumatology/European league against rheumatism collaborative initiative. Ann Rheum Dis (2013) 72(11):1747–55. doi: 10.1136/annrheumdis-2013-204424
41. Damoiseaux J, Potjewijd J, Smeets RL, Bonroy C. Autoantibodies in the disease criteria for systemic sclerosis: The need for specification for optimal application. J Transl Autoimmun (2022) 5(December 2021):100141. doi: 10.1016/j.jtauto.2022.100141
42. Alkema W, Koenen H, Kersten BE, Kaffa C, Dinnissen JWB, Damoiseaux JGMC, et al. Autoantibody profiles in systemic sclerosis; a comparison of diagnostic tests. Autoimmunity (2021) 54(3):148–55. doi: 10.1080/08916934.2021.1907842
43. LeRoy EC, Black C, Fleischmajer R, Jablonska S, Krieg T, Medsger TA, et al. Scleroderma (systemic sclerosis): classification, subsets and pathogenesis. J Rheumatol (1988) 15(2):202–5.
44. Tabeling C, González Calera CR, Lienau J, Höppner J, Tschernig T, Kershaw O, et al. Endothelin b receptor immunodynamics in pulmonary arterial hypertension. Front Immunol (2022) 13:895501(June). doi: 10.3389/fimmu.2022.895501
45. The jamovi project. jamovi. (Version 2.3) [Computer Software] (2022). Retrieved from https://www.jamovi.org.
46. Tream RC. R: A language and enviroment for statistical computing. (2021). Retrieved from https://cran.r-project.org.
47. Lê S, Josse J, Husson F. FactoMineR: An r package for multivariate analysis. J Stat Soft (2008) 25(1 SE-Articles):1–18. doi: 10.18637/jss.v025.i01
48. Cottrell TR, Wise RA, Wigley FM, Boin F. The degree of skin involvement identifies distinct lung disease outcomes and survival in systemic sclerosis. Ann Rheum Dis (2014) 73(6):1060–6. doi: 10.1136/annrheumdis-2012-202849
49. Mierau R, Moinzadeh P, Riemekasten G, Melchers I, Meurer M, Reichenberger F, et al. Frequency of disease-associated and other nuclear autoantibodies in patients of the German network for systemic scleroderma: Correlation with characteristic clinical features. Arthritis Res Ther (2011) 13(5):R172. doi: 10.1186/ar3495
50. Sobanski V, Giovannelli J, Allanore Y, Riemekasten G, Airò P, Vettori S, et al. Phenotypes determined by cluster analysis and their survival in the prospective European scleroderma trials and research cohort of patients with systemic sclerosis. Arthritis Rheumatol (2019) 71(9):1553–70. doi: 10.1002/art.40906
51. Yamamoto T, Nishioka K. Possible role of apoptosis in the pathogenesis of bleomycin-induced scleroderma. J Invest Dermatol (2004) 122(1):44–50. doi: 10.1046/j.0022-202X.2003.22121.x
52. Racanelli V, Prete M, Musaraj G, Dammacco F, Perosa F. Autoantibodies to intracellular antigens: Generation and pathogenetic role. Autoimmun Rev (2011) 10(8):503–8. doi: 10.1016/j.autrev.2011.03.001
53. Didier K, Giusti D, le Jan S, Terryn C, Muller C, Pham BN, et al. Neutrophil extracellular traps generation relates with early stage and vascular complications in systemic sclerosis. J Clin Med (2020) 9(7):2136. doi: 10.3390/jcm9072136
54. Wooten M. Systemic sclerosis and malignancy: A review of the literature. South Med J (2008) 101(1):59–62. doi: 10.1097/SMJ.0b013e31815838ce
55. Arnett FC, Gourh P, Shete S, Ahn CW, Honey RE, Agarwal SK, et al. Major histocompatibility complex (MHC) class II alleles, haplotypes and epitopes which confer susceptibility or protection in systemic sclerosis: Analyses in 1300 Caucasian, African-American and Hispanic cases and 1000 controls. Ann Rheum Dis (2010) 69(5):822–7. doi: 10.1136/ard.2009.111906
56. Reveille JD, Fischbach M, McNearney T, Friedman AW, Aguilar MB, Lisse J, et al. Systemic sclerosis in 3 US ethnic groups: A comparison of clinical, sociodemographic, serologic, and immunogenetic determinants. Semin Arthritis Rheumatol (2001) 30(5):332–46. doi: 10.1053/sarh.2001.20268
57. McNeilage LJ, Youngchaiyud U, Whittingham S. Racial differences in antinuclear antibody patterns and clinical manifestations of scleroderma. Arthritis Rheumatol (1989) 32(1):54–60. doi: 10.1002/anr.1780320109
58. Mitri GM, Lucas M, Fertig N, Steen VD, Medsger TA. A comparison between anti-TH/To- and anticentromere antibody-positive systemic sclerosis patients with limited cutaneous involvement. Arthritis Rheumatol (2003) 48(1):203–9. doi: 10.1002/art.10760
59. Ferri C, Valentini G, Cozzi F, Sebastiani M, Michelassi C, la Montagna G, et al. Systemic sclerosis: Demographic, clinical, and serologic features and survival in 1,012 Italian patients. Medicine (2002) 81(2):139–53. doi: 10.1097/00005792-200203000-00004
60. Kuwana M, Kaburaki J, Okano Y, Tojo T, Homma M. Clinical and prognostic associations based on serum antinuclear antibodies in Japanese patients with systemic sclerosis. Arthritis Rheumatol (1994) 37(1):75–83. doi: 10.1002/art.1780370111
61. Ho KT, Reveille JD. The clinical relevance of autoantibodies in scleroderma. Arthritis Res Ther (2003) 5(2):80–93. doi: 10.1186/ar628
62. Hachulla E, Carpentier P, Gressin V, Diot E, Allanore Y, Sibilia J, et al. Risk factors for death and the 3-year survival of patients with systemic sclerosis: The French ItinérAIR-sclérodermie study. Rheumatology (2009) 48(3):304–8. doi: 10.1093/rheumatology/ken488
63. Tsuji H, Kuramoto N, Sasai T, Shirakashi M, Onizawa H, Kitagori K, et al. Autoantibody profiles associated with morbidity and mortality in scleroderma renal crisis. Rheumatol (Oxf) (2022) 61:4130–5. doi: 10.1093/rheumatology/keac047
64. Reimer G, Steen VD, Penning CA, Medsger TA, Tan EM. Correlates between autoantibodies to nucleolar antigens and clinical features in patients with systemic sclerosis (scleroderma). Arthritis Rheumatol (1988) 31(4):525–32. doi: 10.1002/art.1780310409
65. Nihtyanova SI, Parker JC, Black CM, Bunn CC, Denton CP. A longitudinal study of anti-RNA polymerase III antibody levels in systemic sclerosis. Rheumatol (Oxf) (2009) 48(10):1218–21. doi: 10.1093/rheumatology/kep215
66. Bhavsar SV, Carmona R. Anti-RNA polymerase III antibodies in the diagnosis of scleroderma renal crisis in the absence of skin disease. J Clin Rheumatol (2014) 20(7):379–82. doi: 10.1097/RHU.0000000000000167
67. Nikpour M, Hissaria P, Byron J, Sahhar J, Micallef M, Paspaliaris W, et al. Prevalence, correlates and clinical usefulness of antibodies to RNA polymerase III in systemic sclerosis: A cross-sectional analysis of data from an Australian cohort. Arthritis Res Ther (2011) 13(6):1–13. doi: 10.1186/ar3544
68. Graf SW, Hakendorf P, Lester S, Patterson K, Walker JG, Smith MD, et al. South Australian scleroderma register: Autoantibodies as predictive biomarkers of phenotype and outcome. Int J Rheum Dis (2012) 15(1):102–9. doi: 10.1111/j.1756-185X.2011.01688.x
69. Low AHL, Wong S, Thumboo J, Ng SC, Lim JY, Ng X, et al. Evaluation of a new multi-parallel line immunoassay for systemic sclerosis-associated antibodies in an Asian population. Rheumatol (United Kingdom) (2012) 51(8):1465–70. doi: 10.1093/rheumatology/kes055
70. Dick T, Mierau R, Bartz-Bazzanella P, Alavi M, Stoyanova-Scholz M, Kindler J, et al. Coexistence of antitopoisomerase I and anticentromere antibodies in patients with systemic sclerosis. Ann Rheum Dis (2002) 61(2):121–7. doi: 10.1136/ard.61.2.121
71. Kranenburg P, van den Hombergh WMT, Knaapen-Hans HKA, van den Hoogen FHJ, Fransen J, Vonk MC. Survival and organ involvement in patients with limited cutaneous systemic sclerosis and antitopoisomerase-I antibodies: Determined by skin subtype or auto-antibody subtype? a long-term follow-up study. Rheumatol (United Kingdom) (2016) 55(11):2001–8. doi: 10.1093/rheumatology/kew298
72. Caetano J, Nihtyanova SI, Harvey J, Denton CP, Ong VH. Distinctive clinical phenotype of anti-centromere antibody-positive diffuse systemic sclerosis. Rheumatol Adv Pract (2018) 2(1):1–6. doi: 10.1093/rap/rky002
73. Desai RP, Assassi S. Anti-topoisomerase-positive limited systemic sclerosis has a propensity for interstitial lung disease but is linked to favourable prognosis. Rheumatology (2022) 2022:1–2. doi: 10.1093/rheumatology/keac287
74. Roofeh D, Lin CJF, Goldin J, Kim GH, Furst DE, Denton CP, et al. Tocilizumab prevents progression of early systemic sclerosis associated interstitial lung disease. Arthritis Rheumatol (2021) 73:2021. doi: 10.1002/art.41668
75. Khanna D, Lin CJF, Furst DE, Goldin J, Kim G, Kuwana M, et al. Tocilizumab in systemic sclerosis: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir Med (2020) 8(10):963–74. doi: 10.1016/S2213-2600(20)30318-0
76. Khanna D, Denton CP, Jahreis A, van Laar JM, Frech TM, Anderson ME, et al. Safety and efficacy of subcutaneous tocilizumab in adults with systemic sclerosis (faSScinate): a phase 2, randomised, controlled trial. Lancet (2016) 387(10038):2630–40. doi: 10.1016/S0140-6736(16)00232-4
77. Nihtyanova SI, Sari A, Harvey JC, Leslie A, Derrett-Smith EC, Fonseca C, et al. Using autoantibodies and cutaneous subset to develop outcome-based disease classification in systemic sclerosis. Arthritis Rheumatol (2020) 72(3):465–76. doi: 10.1002/art.41153
78. Lee AYS, Patterson KA, Tan DJ, Wilson ME, Proudman SM, Stevens W, et al. Anti-Ro52/TRIM21 is independently associated with pulmonary arterial hypertension and mortality in a cohort of systemic sclerosis patients. Scand J Rheumatol (2021) 00(00):1–6. doi: 10.1080/03009742.2021.1887927
79. Hudson M, Pope J, Mahler M, Tatibouet S, Steele R, Baron M, et al. Clinical significance of antibodies to Ro52/TRIM21 in systemic sclerosis. Arthritis Res Ther (2012) 14(2):R50. doi: 10.1186/ar3763
80. Marguerie C, Bunn CC, Copier J, Bernstein RM, Gilroy JM, Black CM, et al. The clinical and immunogenetic features of patients with autoantibodies to the nucleolar antigen PM-scl. Med (United States) (1992) 71(6):327–36. doi: 10.1097/00005792-199211000-00001
81. D’Aoust J, Hudson M, Tatibouet S, Wick J, Mahler M, Baron M, et al. Clinical and serologic correlates of anti-pm/scl antibodies in systemic sclerosis: A multicenter study of 763 patients. Arthritis Rheumatol (2014) 66(6):1608–15. doi: 10.1002/art.38428
82. Yamane K, Ihn H, Kubo M, Kuwana M, Asano Y, Yazawa N, et al. Antibodies to Th/To ribonucleoprotein in patients with localized scleroderma. Rheumatology (2001) 40(6):683–6. doi: 10.1093/rheumatology/40.6.683
83. van Eenennaam H, Vogelzangs JHP, Bisschops L, te Boome LCJ, Seelig HP, Renz M, et al. Autoantibodies against small nucleolar ribonucleoprotein complexes and their clinical associations. Clin Exp Immunol (2002) 130(3):532–40. doi: 10.1046/j.1365-2249.2002.01991.x
84. Suresh S, Charlton D, Snell EK, Laffoon M, Medsger TA, Zhu L, et al. Over one-third of Th/To antibody positive scleroderma patients develop pulmonary hypertension in long-term follow-up. Arthritis Rheumatol (2022) 74:2022. doi: 10.1002/art.42152
85. Duffau P, Dimicoli S, Gensous N, Truchetet ME, Bordes C. Anti-NOR90 antibody associated with paraneoplastic systemic sclerosis. Clin Exp Rheumatol (2022) 40:2002–3. doi: 10.55563/clinexprheumatol/r6fqel
86. Dagher JH, Scheer U, Voit R, Grummt I, Lonzetti L, Raymond Y, et al. Autoantibodies to NOR 90/hUBF: Longterm clinical and serological followup in a patient with limited systemic sclerosis suggests an antigen driven immune response. J Rheumatol (2002) 29(7):1543–7.
87. Yamashita Y, Yamano Y, Muro Y, Ogawa-Momohara M, Takeichi T, Kondoh Y, et al. Clinical significance of anti-NOR90 antibodies in systemic sclerosis and idiopathic interstitial pneumonia. Rheumatol (Oxford) (2022) 61(4):1709–16. doi: 10.1093/rheumatology/keab575
88. Franceschini F, Cavazzana I, Generali D, Quinzanini M, Viardi L, Ghirardello A, et al. Anti-Ku antibodies in connective tissue diseases: Clinical and serological evaluation of 14 patients. J Rheumatol (2002) 29(7):1393–7.
89. Rozman B, Čučnik S, Sodin-Semrl S, Czirják L, Varjú C, Distler O, et al. Prevalence and clinical associations of anti-Ku antibodies in patients with systemic sclerosis: A European EUSTAR-initiated multi-centre case-control study. Ann Rheum Dis (2008) 67(9):1282–6. doi: 10.1136/ard.2007.073981
90. Tormey VJ, Bunn CC, Denton CP, Black CM. Anti-fibrillarin antibodies in systemic sclerosis. Rheumatology (2001) 40(10):1157–62. doi: 10.1093/rheumatology/40.10.1157
91. Aggarwal R, Lucas M, Fertig N, Oddis CV, Medsger TA. Anti-U3 RNP autoantibodies in systemic sclerosis. Arthritis Rheumatol (2009) 60(4):1112–8. doi: 10.1002/art.24409
92. Svegliati Baroni S, Santillo M, Bevilacqua F, Luchetti M, Spadoni T, Mancini M, et al. Stimulatory autoantibodies to the PDGF receptor in systemic sclerosis. New Engl J Med (2006) 354(25):2667–76. doi: 10.1056/NEJMoa052955
93. Loizos N, LaRiccia L, Weiner J, Griffith H, Boin F, Hummers L, et al. Lack of detection of agonist activity by antibodies to platelet-derived growth factor receptor α in a subset of normal and systemic sclerosis patient sera. Arthritis Rheumatol (2009) 60(4):1145–51. doi: 10.1002/art.24365
94. Gabrielli A, Moroncini G, Svegliati S, Avvedimento EB. Autoantibodies against the platelet-derived growth factor receptor in scleroderma: comment on the articles by classen et al. and loizos et al. Arthritis Rheumatol (2009) 60(11):3521–2. doi: 10.1002/art.27209
95. Classen JF, Henrohn D, Rorsman F, Lennartsson J, Lauwerys BR, Wikström G, et al. Lack of evidence of stimulatory autoantibodies to platelet-derived growth factor receptor in patients with systemic sclerosis. Arthritis Rheumatol (2009) 60(4):1137–44. doi: 10.1002/art.24381
96. Ihn H, Yamane K, Yazawa N, Kubo M, Fujimoto M, Sato S, et al. Distribution and antigen specificity of anti-U1RNP antibodies in patients with systemic sclerosis. Clin Exp Immunol (2001) 117(2):383–7. doi: 10.1046/j.1365-2249.1999.00961.x
97. Aye MP, Noaiseh G, Medsger TA Jr., Lafyatis RA, Laffoon M, Zhu L, et al. Anti-SSA (Ro52/Ro60) and SSB autoantibodies in patients with systemic sclerosis. In: ARTHRITIS & RHEUMATOLOGY, vol. 69. . 111 RIVER ST, HOBOKEN 07030-5774, NJ USA: WILEY (2017).
98. Höppner J, Casteleyn V, Biesen R, Rose T, Windisch W, Burmester GR, et al. SIGLEC-1 in systemic Sclerosis: A useful biomarker for differential diagnosis. Pharmaceuticals (2022) 15:1198. doi: 10.3390/ph15101198
99. Bussone G, Dib H, Tamby MC, Broussard C, Federici C, Woimant G, et al. Identification of new autoantibody specificities directed at proteins involved in the transforming growth factor β pathway in patients with systemic sclerosis. Arthritis Res Ther (2011) 13(3):1–13. doi: 10.1186/ar3336
100. Irure-Ventura J, Rodríguez C, Vergara-Prieto E, Vargas ML, Quirant B, Jurado A, et al. Rare immunofluorescence patterns of autoantibodies on HEp-2 cells defined by ICAP identify different autoimmune diseases in the absence of associated specificities: A Spanish multicentre study. Rheumatol (Oxf) (2021) 60(8):3904–12. doi: 10.1093/rheumatology/keaa831
101. Betteridge ZE, Woodhead F, Lu H, Shaddick G, Bunn CC, Denton CP, et al. Brief report: Anti-eukaryotic initiation factor 2B autoantibodies are associated with interstitial lung disease in patients with systemic sclerosis. Arthritis Rheumatol (2016) 68(11):2778–83. doi: 10.1002/art.39755
102. Pauling JD, Salazar G, Lu H, Betteridge ZE, Assassi S, Mayes MD, et al. Presence of anti-eukaryotic initiation factor-2B, anti-RuvBL1/2 and anti-synthetase antibodies in patients with anti-nuclear antibody negative systemic sclerosis. Rheumatol (United Kingdom) (2018) 57(4):712–7. doi: 10.1093/rheumatology/kex458
103. Gunther J, Kill A, Becker MO, Heidecke H, Rademacher J, Siegert E, et al. Angiotensin receptor type 1 and endothelin receptor type a on immune cells mediate migration and the expression of IL-8 and CCL18 when stimulated by autoantibodies from systemic sclerosis patients. Arthritis Res Ther (2014) 16(2):R65. doi: 10.1186/ar4503
104. Rigamonti C, Bogdanos DP, Mytilinaiou MG, Smyk DS, Rigopoulou EI, Burroughs AK. Primary biliary cirrhosis associated with systemic Sclerosis: Diagnostic and clinical challenges. Int J Rheumatol (2011) 2011:1–12. doi: 10.1155/2011/976427
105. Fonollosa V, Simeón CP, Castells L, Garcia F, Castro A, Solans R, et al. Morphologic capillary changes and manifestations of connective tissue diseases in patients with primary biliary cirrhosis. Lupus (2001) 10(9):628–31. doi: 10.1191/096120301682430212
106. Alsaed OS, Alamlih LI, Al-Radideh O, Chandra P, Alemadi S, Al-Allaf AW. Clinical utility of ANA-ELISA vs ANA-immunofluorescence in connective tissue diseases. Sci Rep (2021) 11(1):1–7. doi: 10.1038/s41598-021-87366-w
107. Orme ME, Andalucia C, Sjölander S, Bossuyt X. A comparison of a fluorescence enzyme immunoassay versus indirect immunofluorescence for initial screening of connective tissue diseases: Systematic literature review and meta-analysis of diagnostic test accuracy studies. Best Pract Res Clin Rheumatol (2018) 32(4):521–34. doi: 10.1016/j.berh.2019.03.005
Keywords: systemic sclerosis, scleroderma, autoantobodies, cluster analysis, primary biliary cholangitis (PBC)
Citation: Höppner J, Tabeling C, Casteleyn V, Kedor C, Windisch W, Burmester GR, Huscher D and Siegert E (2023) Comprehensive autoantibody profiles in systemic sclerosis: Clinical cluster analysis. Front. Immunol. 13:1045523. doi: 10.3389/fimmu.2022.1045523
Received: 15 September 2022; Accepted: 21 November 2022;
Published: 04 January 2023.
Edited by:
Raphaela Goldbach-Mansky, (NIH), United StatesReviewed by:
Devis Benfaremo, Marche Polytechnic University, ItalyCopyright © 2023 Höppner, Tabeling, Casteleyn, Kedor, Windisch, Burmester, Huscher and Siegert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elise Siegert, ZWxpc2Uuc2llZ2VydEBjaGFyaXRlLmRl
†These authors have contributed equally to this work
‡ORCID: Jakob Höppner, orcid.org/0000-0001-9908-2066
Christoph Tabeling, orcid.org/0000-0001-9189-4318
Elise Siegert, orcid.org/0000-0002-9594-0446
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.