 Marta Dafne Cabañero-Navalon1
Marta Dafne Cabañero-Navalon1 Victor Garcia-Bustos1*
Victor Garcia-Bustos1* Maria Nuñez-Beltran1
Maria Nuñez-Beltran1 Pascual Císcar Fernández1
Pascual Císcar Fernández1 Lourdes Mateu2
Lourdes Mateu2 Xavier Solanich3
Xavier Solanich3 Juan Luis Carrillo-Linares4
Juan Luis Carrillo-Linares4 Ángel Robles-Marhuenda5Francesc Puchades-Gimeno6Ana Pelaez Ballesta7Nuria López-Osle8
Ángel Robles-Marhuenda5Francesc Puchades-Gimeno6Ana Pelaez Ballesta7Nuria López-Osle8 Miguel Ángel Torralba-Cabeza9
Miguel Ángel Torralba-Cabeza9 Ana María Bielsa Masdeu10Jorge Diego Gil11Nuria Tornador Gaya12Guillem Pascual Castellanos12Rosario Sánchez-Martínez13
Ana María Bielsa Masdeu10Jorge Diego Gil11Nuria Tornador Gaya12Guillem Pascual Castellanos12Rosario Sánchez-Martínez13 José Manuel Barragán-Casas14Andrés González-García15
José Manuel Barragán-Casas14Andrés González-García15 José Luís Patier de la Peña15Daniel López-Wolf16Antonia Mora Rufete17Alba Canovas Mora17
José Luís Patier de la Peña15Daniel López-Wolf16Antonia Mora Rufete17Alba Canovas Mora17 Maria José Forner Giner18Pedro Moral Moral1
Maria José Forner Giner18Pedro Moral Moral1- 1Department of Internal Medicine, University and Polytechnic Hospital LaFe, Valencia, Spain
- 2Department of Internal Medicine, Germans Trias i Pujol University Hospital, Badalona, Spain
- 3Department of Internal Medicine, Bellvitge University Hospital, Barcelona, Spain
- 4Department of Internal Medicine, Virgen de la Victoria University Hospital, Málaga, Spain
- 5Department of Internal Medicine, La Paz University Hospital, Madrid, Madrid, Spain
- 6Department of Internal Medicine, University General Hospital of Valencia, Valencia, Spain
- 7Department of Internal Medicine, Rafael Méndez University Hospital, Murcia, Spain
- 8Department of Internal Medicine, Cruces University Hospital, Bizkaia, Spain
- 9Department of Internal Medicine, Lozano Blesa University Clinical Hospital, Zaragoza, Spain
- 10Department of Internal Medicine, Miguel Servet University Hospital, Zaragoza, Spain
- 11Department of Internal Medicine, University Hospital October 12, Madrid, Spain
- 12Department of Internal Medicine, University General Hospital of Castellón, Castellón, Spain
- 13Department of Internal Medicine, University General Hospital of Alicante, Alicante, Spain
- 14Department of Internal Medicine, Complejo Asistencial de Ávila, Ávila, Spain
- 15Department of Internal Medicine, Santiago Ramón y Cajal University Hospital, Madrid, Spain
- 16Department of Internal Medicine, University Hospital Alcorcón Foundation, Madrid, Spain
- 17Department of Internal Medicine, General University Hospital of Elche, Alicante, Spain
- 18Department of Internal Medicine, Clinical University Hospital of Valencia, Valencia, Spain
Common variable immunodeficiency (CVID) constitutes a heterogenic group of primary immunodeficiency disorders with a wide-ranging clinical spectrum. CVID-associated non-infectious morbidity constitutes a major challenge requiring a full understanding of its pathophysiology and its clinical importance and global variability, especially considering the broad clinical, genetic, and regional heterogeneity of CVID disorders. This work aimed to develop a nationwide, multicenter, retrospective study over a 3-year period describing epidemiological, clinical, laboratory, therapeutic, and prognostic features of 250 CVID patients in Spain. The mean diagnostic delay was around 10 years and most patients initially presented with infectious complications followed by non-infectious immune disorders. However, infectious diseases were not the main cause of morbimortality. Non-infectious lung disease was extraordinarily frequent in our registry affecting approximately 60% of the patients. More than one-third of the patients in our cohort showed lymphadenopathies and splenomegaly in their follow-up, and more than 33% presented immune cytopenias, especially Evans’ syndrome. Gastrointestinal disease was observed in more than 40% of the patients. Among biopsied organs in our cohort, benign lymphoproliferation was the principal histopathological alteration. Reaching 15.26%, the global prevalence of cancer in our registry was one of the highest reported to date, with non-Hodgkin B lymphoma being the most frequent. These data emphasize the importance of basic and translational research delving into the pathophysiological pathways involved in immune dysregulation and diffuse lymphocytic infiltration. This would reveal new tailored strategies to reduce immune complications, and the associated healthcare burden, and ensure a better quality of life for CVID patients.
Introduction
Common variable immunodeficiency (CVID) constitutes a heterogenic group of primary immunodeficiency disorders (PID) with an estimated prevalence of 1:50.000 – 1:25.000 (1–3). It is characterized by decreased levels of serum IgG, together with decreased IgM and/or IgA, and it can be diagnosed after excluding secondary causes of hypogammaglobulinemia and other primary immunodeficiencies (1, 2). Infectious diseases were its main cause of morbidity and mortality until the introduction of immunoglobulin replacement therapy (IgRT) in the late 20th century. Due to this treatment, non-infectious complications such as autoimmune, benign lymphoproliferative disorders, and even cancer have emerged as comorbidities with a larger impact on prognosis than infections (4). These dysimmune phenomena may affect up to 70% of patients (5, 6) and imply an 11-fold increased risk of death (5, 7). In fact, IgRT does not seem to prevent or improve many of these conditions (5).
Therefore, the clinical spectrum of CVID is wide-ranging. Back in 2008, Chapel et al. already described five clinical phenotypes of CVID: those that showed polyclonal lymphocytic infiltration, those with autoimmune diseases, those that developed enteropathy, those showing malignant neoplasia, and those only suffering infectious diseases (8). These non-infectious phenomena can be the first symptom of CVID disease in some patients (9) or can appear over time. Polyclonal infiltration may affect lymph nodes, liver, spleen, skin, or lung -causing the well-known granulomatous-lymphocytic interstitial lung disease (GLILD)- although every organ might be virtually infiltrated (10). The most common autoimmune complications are blood cytopenias. Nevertheless, almost every autoimmune disease has been described in association with CVID (7, 11). Some patients with CVID present with non-infectious inflammatory gastrointestinal disease resulting in diarrhea, malabsorption, and weight loss (12). Additionally, hematologic, and solid organ malignancies have been more frequently described in CVID than in the rest of PIDs and are associated with poorer outcomes (4, 13).
Thus, CVID-associated non-infectious morbidity constitutes a major challenge requiring a full understanding of its pathophysiology and its clinical importance and variability worldwide, especially considering the wide clinical, genetic, and even regional heterogeneity of CVID disorders. Moreover, many of these complications might be part of a common altered immunological substrate resulting in a complex multisystemic disease that needs to be further characterized (14). The development of standardized targeted therapies is also required, as IgRT only plays a role in preventing infectious disorders. The use of other anti-inflammatory or immunosuppressant agents for immune complications is not exempt from serious adverse effects in these already immunocompromised patients and lacks a wide body of evidence (15).
Consequently, registries and large cohort studies are needed in order to provide an updated epidemiological overview of the clinical spectrum of CVID with less biased results considering high variability and even regional diversity of these disorders. The aim of this work was to develop a nationwide, multicenter, retrospective study over a 3-year period describing epidemiological, clinical, laboratory, therapeutic, and prognostic features of CVID patients in Spain.
Material and methods
Study design, setting, and population
A multicenter, cross-sectional, nationwide study of patients diagnosed with CVID was carried out in Spain from November 2019 to May 2022. A total of 17 hospitals treating PIDs participated in the creation of the GTEM-SEMI-CVID-Registry promoted by the Working Group of Minority Diseases of the Spanish Society of Internal Medicine (GTEM-SEMI). All patients aged 16 years and above with CVID diagnosis according to the European Society for Immunodeficiencies (ESID) registry working definitions (2) and who were or had been followed up by the participating units were considered eligible. By protocol, all selected patients for inclusion were initially screened to confirm CVID diagnosis according to the consensus ESID criteria, and patients with definite monogenic immunodeficiencies were not eligible for inclusion at the time of data collection.
Data collection and variables
The GTEM-SEMI-CVID-Registry systematically compiles sociodemographic and epidemiological data, genetic information, infectious and non-infectious comorbidities, imaging findings, laboratory and histopathological parameters, treatments, and patient outcomes. All data were collected by reviewing electronic medical records and included in a predesigned database.
Demographic data included sex, current age, or age at the time of death, age at diagnosis, age at clinical onset, diagnostic delay, first PID-related clinical complication (infection, dysimmunity, malignancy, or other), and time of follow-up. Genetic testing, family history, and consanguinity were recorded. All described genes with variants not listed under CVID and attributable to defined monogenic PIDs were compulsorily those of ‘uncertain significance’ or ‘likely benign’, according to the Standards and Guidelines for the Interpretation of Sequence Variants of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology.
History of major bacterial infections, opportunistic, and recurrent infections were collected, including chronic Epstein-Barr virus (EBV) and Helicobacter pylori infections. Non-infectious comorbidities included autoimmune cytopenias, lymphadenopathies, splenomegaly, hepatomegaly, and clinical or imaging findings of portal hypertension, systemic autoimmune disorders, lung, gastrointestinal, cutaneous, and neurological involvement, as well as cardiovascular comorbidity and malignancy (both solid and hematological neoplasia). Furthermore, clinical symptoms such as chronic cough, dyspnea, chronic diarrhea, and abdominal pain were recorded. Chronic enteropathy was considered, if the presence of chronic diarrhea, and/or diagnosed malabsorption were recorded in absence of documented infection.
Imaging findings were limited to chest CT scanning due to frequent and potentially severe lung involvement in CVID and according to the follow-up recommendations of the British Society for Immunology/United Kingdom Primary Immunodeficiency Network Consensus on managing non-infectious complications of CVID (16). Additionally, and following previous recommendations, lung function tests (LFT) and values of corrected diffusing capacity of the lungs for carbon monoxide (cDLCO) were also considered.
Laboratory variables included IgG (mg/dL), IgM (mg/dL), IgA (mg/dL), CD4 cell count (cell/µL), CD8 cell count (cell/µL), CD4/CD8 ratio, CD19 cell count (cell/µL), CD3 cell count (cell/µL), and natural killers (NK) cell count (cell/µL) both at diagnosis and last determination after treatment, first available LDL (mg/dL), HDL (mg/dL), triglycerides levels (mg/dL), positivity at any point of autoantibodies such as antinuclear antibodies (ANA) -only if titres exceed 1/80-, extractable nuclear antigens (ENA), rheumatoid factor (RF), antineutrophil cytoplasmic antibodies (ANCA), and myositis-related and systemic sclerosis-related antibodies. Due to the high prevalence of bowel disease, positivity at any point of coeliac-related antibodies, intrinsic factor, and gastric parietal cells antibodies (GPC), and HLA DQ2/DQ8 typing were also noted.
Histopathological results of lymph nodes, spleen, liver, lung, and digestive tract were compiled. In lymph node and spleen biopsies, the presence of granulomatosis, benign lymphoproliferation, lymphoma, or other features were collected. In liver biopsies, evidence of fibrosis or nodular regenerative hyperplasia (NRH) was registered too. For those patients who underwent lung biopsy, histologically relevant findings were classified as lymphoid interstitial pneumonia (LIP), GLILD, follicular bronchiolitis, granulomas, lymphoma, and their combinations. Gastric and bowel histology was comprehensively studied, including variables such as atrophic gastritis, nodular lymphoid hyperplasia (NLH), intestinal villous atrophy, lymphocytic infiltration, eosinophilic infiltration, absence of plasma cells, presence of granulomas, lymphocytic colitis, or findings compatible with Crohn’s disease or ulcerative colitis.
Treatment with IgRT, regime, and route of administration were also included. Moreover, therapy with all categories of immunosuppressant agents received at any point of the clinical history was considered. The GTEM-SEMI-CVID-Registry also collected the mortality rate, cause of death, and follow-up time until death in those deceased patients.
Statistics
Owing to the epidemiological and cross-sectional nature of the study, variables were mainly analyzed using descriptive statistics. The analyses were performed with R statistical software version 4.2.1 (R Development Core Team, 2022). Quantitative data were expressed as mean and standard deviation (SD). Qualitative data were expressed as absolute count and percentage of cases, without accounting for non available values. For subanalyses of variables of interest, significance was assessed with the χ2 or Fisher exact test for categorical variables and the Student t test for continuous variables after checking pertinent statistical assumptions. Two-tailed p-value below 0.05 was considered statistically significant.
Ethical statement
The creation and protocol of the GTEM-SEMI-CVID-Registry were independently approved by all institutional Ethical Committees of each participating hospital under their corresponding registry codes. Anonymity and data confidentiality of all included patients were ensured in accordance with the Spanish regulation of observational studies. The work was performed according to the Declaration of Helsinki and followed the STROBE guidelines (Supplementary Material).
Results
Demographics
As of May 2022, a total of 250 patients diagnosed with CVID were included in the GTEM-SEMI-CVID Spanish Registry. In our cohort, the mean age was 54.08 (SD 18.22) years old, and 121 patients (48.4%) were male. The mean age at diagnosis was 40.89 (SD 19.74) years old. However, the mean diagnostic delay was 10.01 (SD 13.21) years, while the global mean age at characteristic symptom onset was 29.8 (SD 20.08) years old. Most patients initially presented with infectious complications (158, 63.2%), followed by non-infectious or neoplastic complications (83, 33.2%). Two patients presented with non-Hodgkin lymphoma. Family history and consanguinity were registered in 226 and 193 patients, respectively. Twenty-seven (11.95%) patients had a previous family history of CVID. History of consanguinity was seen in 8 patients (4.14%). Genetic testing was performed in 99 (39.6%) patients. Genetic variants were found in 35 patients, and all of them were considered benign or of unknown significance (Table 1).
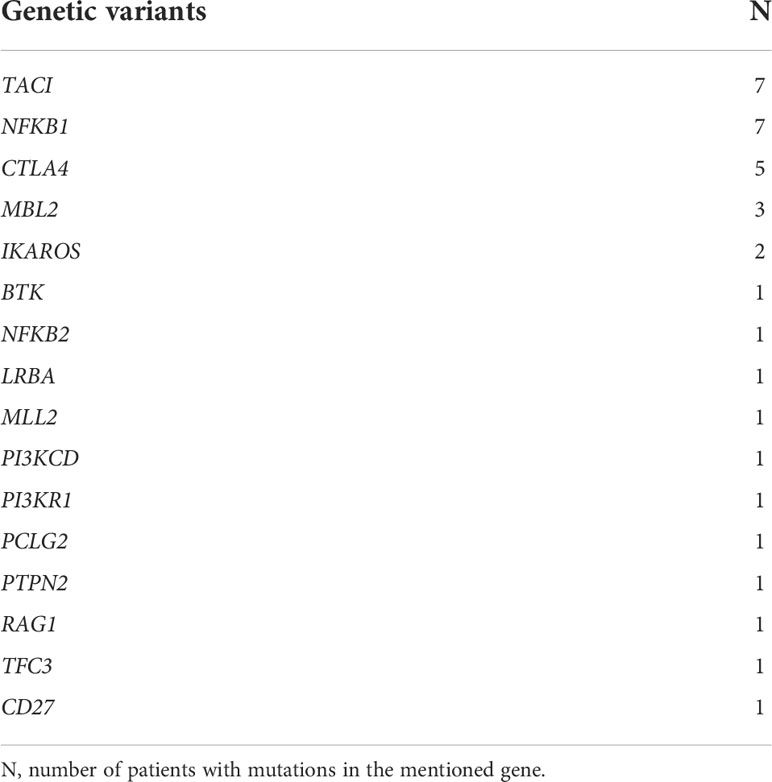
Table 1 List of genetic variants in the Spanish GTEM-SEMI-CVID Registry.
Infectious complications
Information on the history of infectious complications of CVID was available for all patients included in the cohort, with airway infections being the most common. Almost 65% had suffered at least one episode of a major bacterial infection, and pneumonia accounted for most episodes. A history of sepsis, nevertheless, was only reported in 31 patients. Of all respiratory infections, more than 50% were recurrent and around 70% of patients reported a previous history of recurrent upper respiratory tract infections. Skin, soft tissue, or musculoskeletal infections were less frequent than opportunistic infections (considering deep-seated candidiasis, cryptococcosis, tuberculosis (TBC), and infection by non-TBC mycobacteria, Pneumocystis jirovecii pneumonia, cytomegalovirus (CMV) infection, JC virus infection, leishmaniasis or toxoplasmosis among others). Noteworthy, there were 2 reported cases of TBC, 3 cases of disseminated CMV infection, and 1 case of visceral leishmaniasis. Further information is detailed in Table 2.
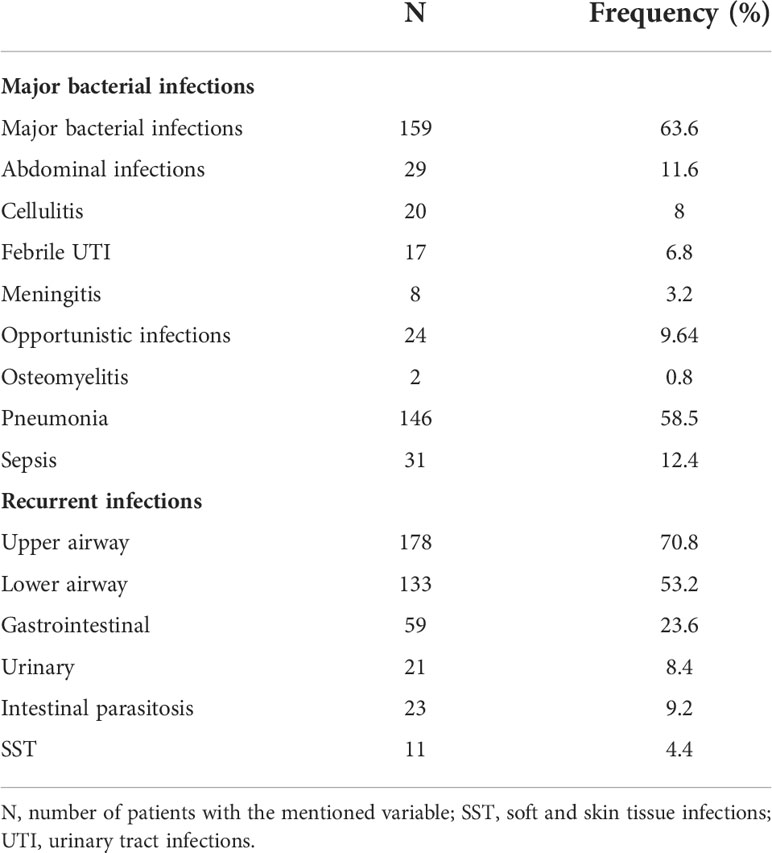
Table 2 Descriptive statistics of the major bacterial and the recurrent infections in the GTEM-SEMI-CVID Registry.
A significantly higher proportion of patients who suffered opportunistic infections had received or were under treatment with corticosteroids (68.2% versus 32.2%, χ2 p=0.002). Additionally, this was also significantly observed when considering treatment with azathioprine (31.8% versus 10.3%, χ2 p=0.01), as well as the combination of corticosteroids, azathioprine, and rituximab (20.8% versus 5.3%, χ2 p=0.015). No other significant differences were observed in relation to rituximab alone or other immunosuppressive treatments, or in relation to CD4+ cell count and genetic mutations. However, the genetic information is limited due to the absence of genetic analysis in a large part of the studied population.
Overview of non-infectious immune complications
Forty-three patients showed non-infectious immune complications as the first manifestation of the disease. During the mean follow-up time until data collection (8.90 years, SD 7.90), the most common immune complication was the presence of lymphadenopathies (35.2%), closely followed by the development of immune cytopenias (33.73%), non-infectious enteropathy (33.60%) and splenomegaly (33.06%). A total of 19.68% of patients had been previously diagnosed with a systemic autoimmune disease. Liver disease was less frequent, with hepatomegaly and liver nodules being found in 18.8% and 6.5% of patients, respectively (Figure 1). Considering GLILD as a severe lung immune complication in CVID, its presence was histologically confirmed in 7.69% of patients. Dysimmune neurological complications were also reported in 15 patients (6.02%) of the cohort.
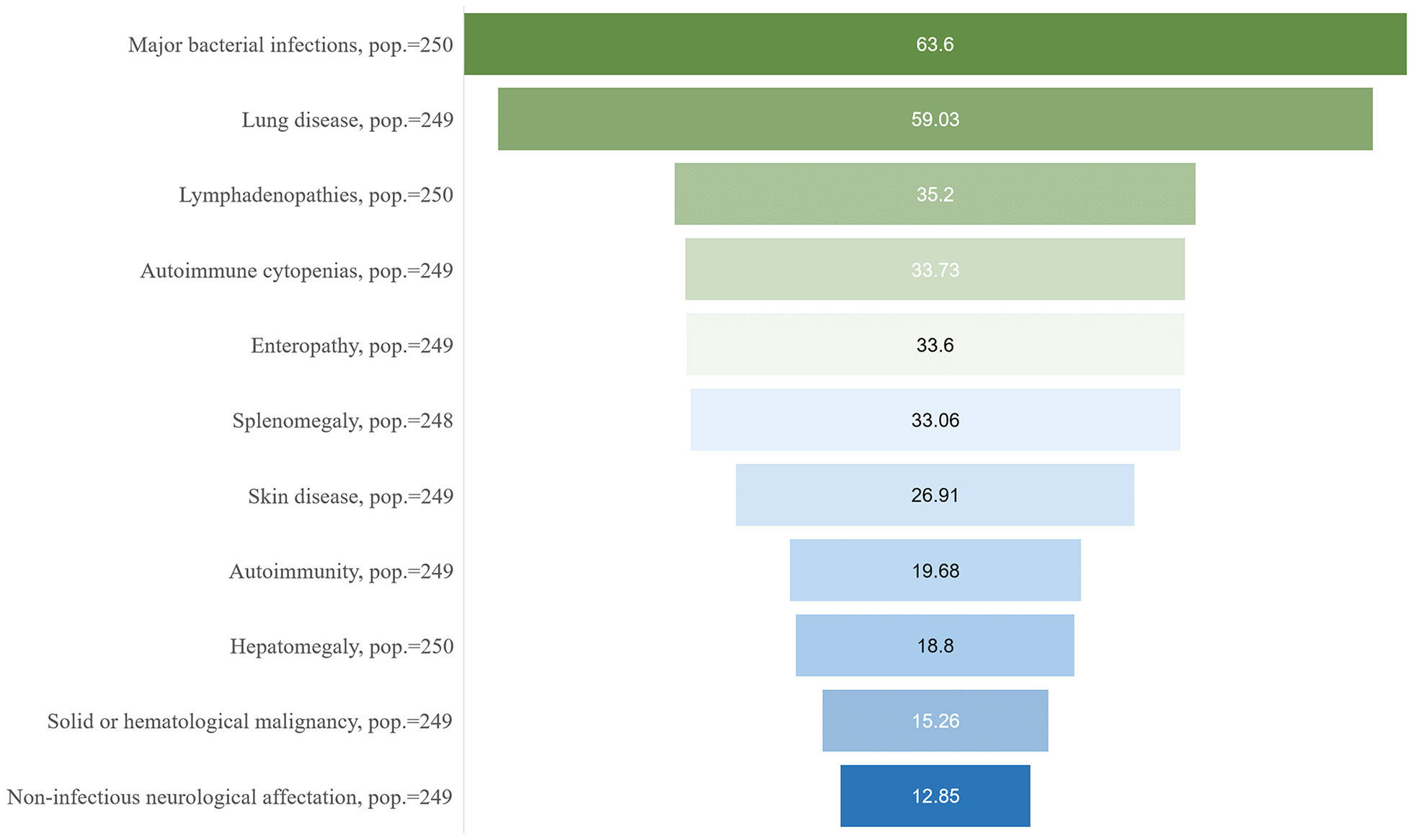
Figure 1 Summary of major comorbidities of the CVID patients included in the GTEM-SEMI-CVID Registry. Pop., number of patients for whom information on the specified variable was available.
Organ-specific manifestations will be described in detail below.
Systemic autoimmune diseases and immunosuppressant drugs
Cytopenias were present in 84 patients of the cohort. Two hundred and thirty-one patients were recorded for the specific presence of cytopenias. Evans’ syndrome, defined as both the simultaneous presence of immune anemia and thrombopenia, as well as leukopenia and thrombopenia were the most frequent cytopenias in our cohort, reported in 12 and 11 patients, respectively (5.19% and 4.76%). Isolated immune thrombopenia and hemolytic anemia were present in 6 (2.60%) and 4 (1.73%) patients, respectively. Isolated immune neutropenia was reported in 4 patients (1.73%).
Autoimmunity was present in 49 patients (19.68%) (Figure 1). The most common rheumatic disease in our cohort was ankylosing spondylitis, with a prevalence of 2.41% (6 cases), closely followed by sarcoidosis (2% and 5 cases). Systemic lupus erythematosus (SLE) and unspecified vasculitis had been diagnosed in 2 patients each (0.80%), and only 1 case of Sjögren syndrome and rheumatic polymyalgia were described (Figure 2). No reports on other autoimmune diseases such as systemic sclerosis or rheumatoid arthritis were seen. Type 1 diabetes mellitus was reported in 7 patients (2.81%) (Figure 2). Antinuclear antibodies (ANA), extractable nuclear antigen antibodies (ENA) and anti-neutrophil cytoplasmic antibodies (ANCA) were positive in 8.84% (17), 1.77% (2), and 2.86% (4) of determinations. Of all patients, 94 had received pharmacological immunosuppressant or immunomodulatory treatments (Table 3). Corticosteroids (34.17%), followed by azathioprine (12.24%) and rituximab (12.23%) were the most frequently used immunosuppressant agents, mainly targeting CVID immune complications such as cytopenias, lymphoproliferation, and autoimmune disorders
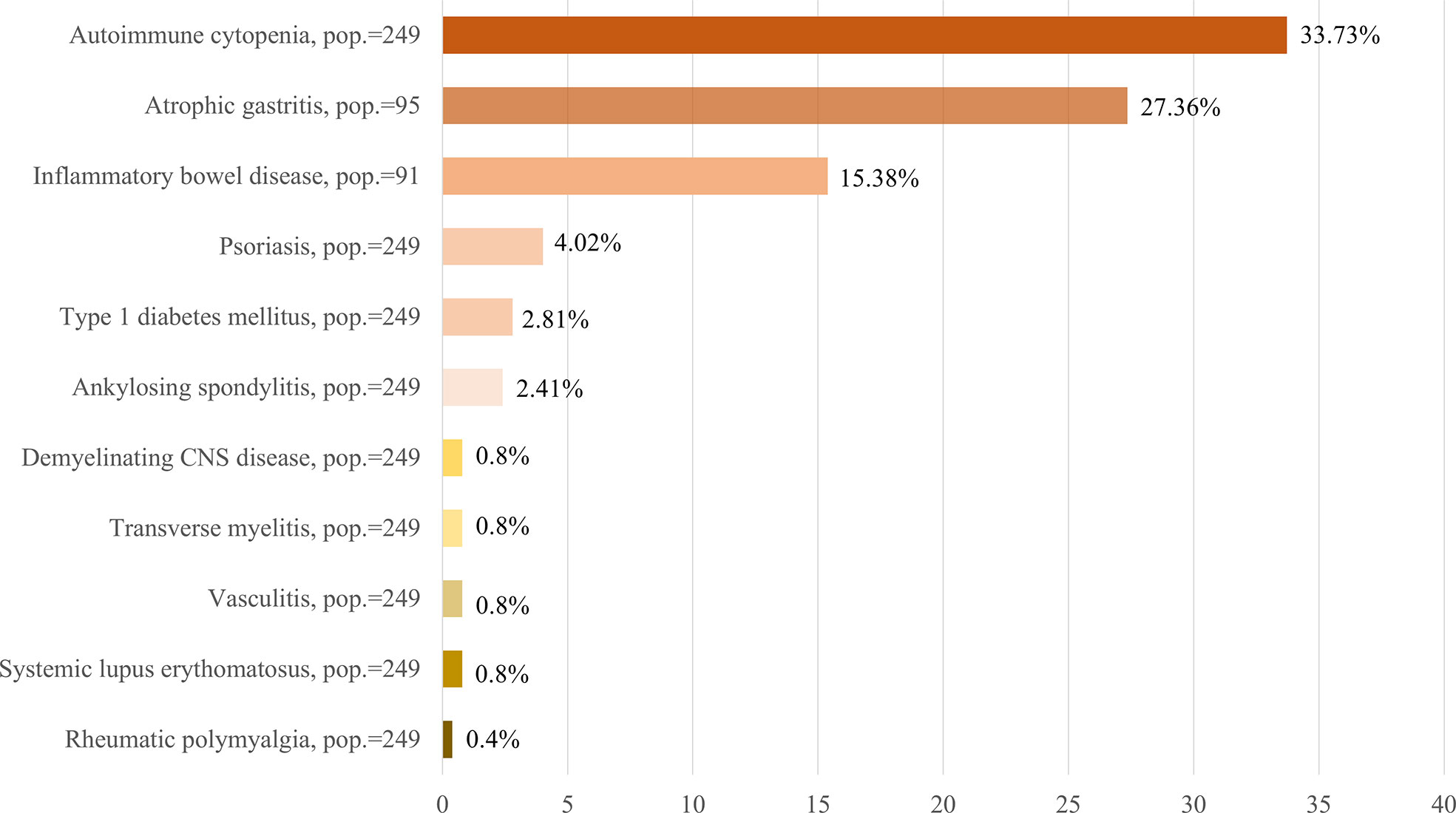
Figure 2 Summary of main immune complications of the CVID patients included in the GTEM-SEMI-CVID Registry. CNS, central nervous system. Pop., number of patients for whom information on the specified variable was available.
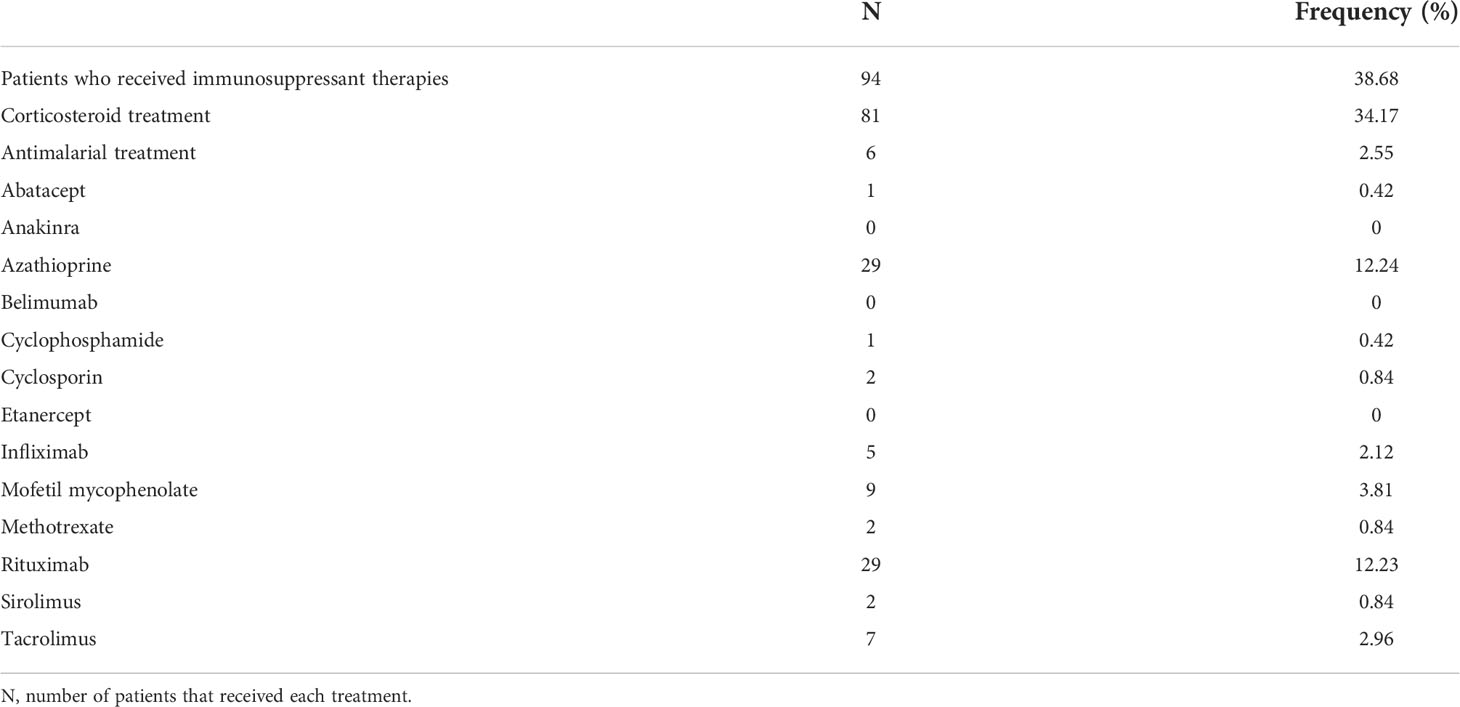
Table 3 History of immunosupressant treatment in the GTEM-SEMI-CVID Registry.
Eighty-one patients had received or were under corticosteroid treatment at the time of inclusion, of which 52 presented autoimmune cytopenias, 14 had histologically confirmed GLILD, and 24 patients suffered intestinal malabsorption. Azathioprine had been administered in 21 patients affected by immune cytopenias and 12 patients with confirmed GLILD. Rituximab therapy was the most used monoclonal antibody, and it had been administered in 24 patients with immune cytopenias, 14 patients with GLILD and in 6 patients who suffered non-Hodgkin lymphoma. Seventeen patients received treatment with all three agents, of which 10 patients presented coexistence of autoimmune cytopenias and GLILD. Further information on significant immunosuppressant therapies and the observed comorbidities in these patients can be consulted in the Supplementary S1 File.
Spleen and lymph node involvement
The presence of significant lymphadenopathies was observed in 88 patients. Half of them (18) had undergone a lymph node biopsy. Eighty-two patients (33.06%) presented splenomegaly (Figure 1), but a splenic biopsy was only performed in 4 patients due to high hemorrhagic risk. Benign lymphoproliferation (65.91% of lymph node biopsies and 50% of spleen biopsies) and node granulomatosis (44.45% of lymph node biopsies and 75% of spleen biopsies) were the most frequent histological findings for both organs. Further histological data are detailed in Table 4.
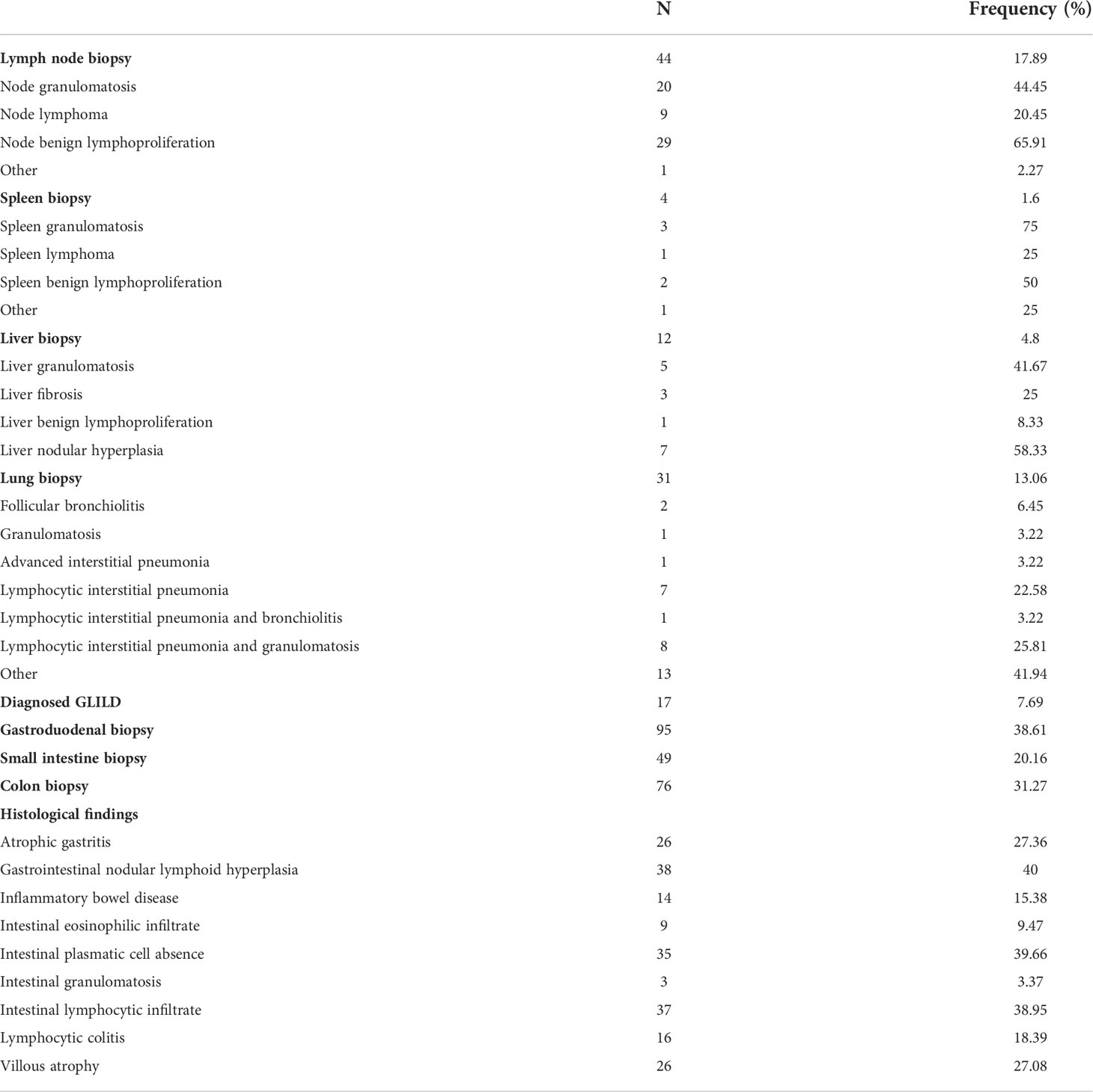
Table 4 Lymph node, spleen, liver, lung, and gastrointestinal histopathology of GTEM-SEMI-CVID Registry.
Liver involvement
In 47 patients (18.8%), hepatomegaly was documented on imaging tests regardless of the presence of splenomegaly. Liver nodules were observed in 16 patients (6.5%). Clinical, laboratory, imaging, or endoscopic evidence of portal hypertension was present in 19 patients (7.75%), and liver biopsy had been performed in 12 individuals (4.8%) during follow-up. As seen in Table 4, liver nodular hyperplasia was the most frequent histological finding (58.33%) followed by liver granulomatosis (41.67%).
Lung involvement
Non-infectious lung disease was extraordinarily frequent and was seen in almost 60% of CVID patients (Figure 1). Nevertheless, less than 25% of them reported chronic dyspnea or cough as the most frequent clinical manifestation (Table 5). High-resolution CT (HRCT) scanning had been performed for nearly 65% of the patients and isolated bronchial affectation, mainly bronchiectasis was the most frequent imaging finding (35%). Lung parenchymal involvement was observed in 15% of the patients, and the most regularly described radiological pattern was compatible with lymphoid interstitial pneumonia (13.83% of HRCT scans). Almost 80% of the patients had undergone LFT during follow-ups. Normal results were obtained in 56.90% of them and an obstructive spirometry pattern was seen in 27.59%. The mean cDLCO was 73.62 (21.28 SD). Further data are detailed in Table 5. Thirty-one patients underwent lung biopsy. Histological results concurred with imaging observations, and combined lymphocytic interstitial pneumonia and granulomatosis were the most frequent findings (25.81% of lung biopsies), as seen in Table 4. Confirmed GLILD according to the British Lung Foundation Criteria (15) was seen in 17 patients (Table 5).
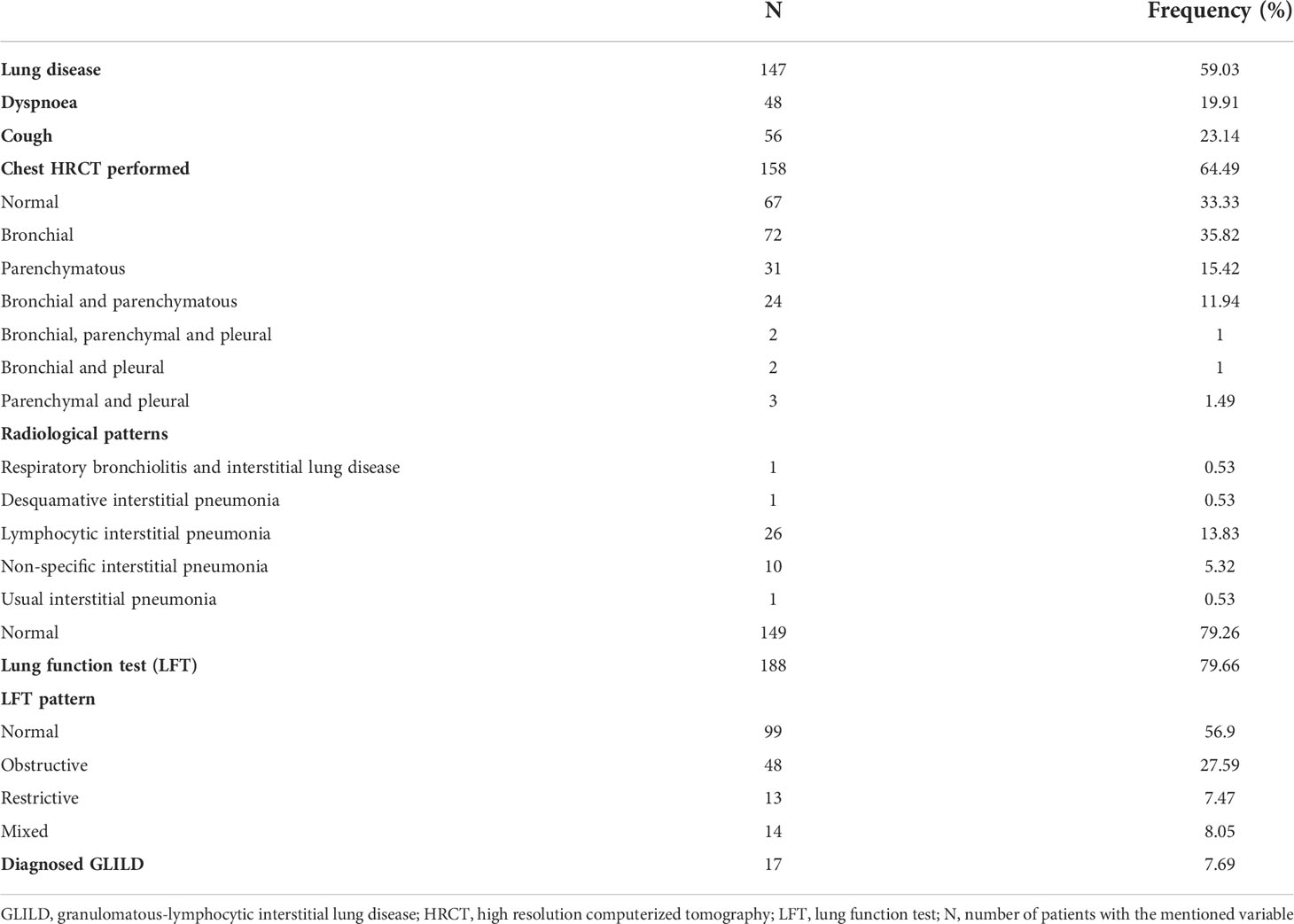
Table 5 Lung disease in the GTEM-SEMI-CVID Registry.
Digestive tract involvement
Gastrointestinal affectation was common (40.56%) but also highly variable. Non-infectious diarrhea was reported in 83 patients (33.60%) (Figure 1). However, proved malabsorption was diagnosed in 30 patients (23.81%). Determination of H. pylori infection was performed in 126 patients, with a prevalence in our population of 23.81%. Screening for coeliac, anti-gastric parietal, and anti-intrinsic factor antibodies, as well as screening for HLA DQ2/DQ8, was carried out in 241, 71, 53, and 33 patients obtaining a positive result in 3.73%, 19.72%, 3.77%, and 24.24%, respectively. Gastroduodenal, small intestine, and colon biopsies were performed in 95, 49, and 76 patients, correspondingly. Histological findings are detailed in Table 4. To highlight, lymphoid nodular hyperplasia, lymphocytic infiltrate, and intestinal absence of plasma cells were the most common traits. Atrophic gastritis was observed in 27.36% of the patients (Figure 2).
Involvement of other organs: cutaneous and neurological manifestations
Skin disorders were reported in 67 patients in our cohort (26.91%) (Figure 1). The most frequent lesions were eczema, in 22 patients (8.83%); psoriasis, in 10 patients (4.02%) (Figure 2); followed by vitiligo and alopecia, both recorded for 6 patients (2.41%). The presence of warts was registered for 3 patients (1.20%). However, the occurrence of other non-specified lesions of a wide nature (cutaneous neoplasms, nevi, among others) was reported in 37 individuals.
The presence of non-infectious neurological involvement was also studied. Five patients (2.01%) presented both intellectual disability and peripheral neuropathy of diverse severity and etiology. Of note, 4 patients suffered epilepsy (1.60%) and immune demyelinating lesions and transverse myelitis were described in 2 cases each (Figure 2). One episode of subacute sclerosing panencephalitis with severe sequelae was reported after measles vaccination in an undiagnosed CVID patient at that moment.
Neoplastic complications
Prevalence of both solid and hematological malignancies from inclusion to follow-up was 15.26% (38 cases) (Figure 1). Non-Hodgkin B lymphoma (11 cases and 4.41%) was the most frequent malignancy in our population. Gastric cancer and lung adenocarcinoma were reported in 5 (2.01%) and 3 (1.20%) patients, respectively. Interestingly, only 2 cases of colorectal cancer, as well as 1 case of breast cancer and prostate cancer were diagnosed. Of note, 3 patients reported basal cell carcinomas, and 1 patient was diagnosed with both basal cell and skin squamous cell carcinoma of the skin. The remaining 7 cases were diagnosed with other less frequent tumors (namely, myeloma, splenic lymphoma, thyroid, renal, uterine, or cervical cancer).
Other comorbidities
The prevalence of diseases resulting in increased cardiovascular events such as hypertension, type 2 diabetes mellitus (DM), dyslipidemia, and gout were seen in 52, 22, 41, and 4 individuals (namely, 20.88%, 8.84%, 16.65%, and 1.61%). Eighteen patients (7.23%) presented heart failure, 5 (2%) had suffered a stroke, and 3 (1.20%) reported peripheral arteriopathy. Chronic kidney disease was documented in 12 patients (4.82%). Venous thromboembolic disease was reported in 7 patients (2.81%).
Immunological parameters
Immunoglobulin levels at diagnosis as well as lymphocyte subpopulation cell count are detailed in Table 6. There was wide variation in the immunoglobulin levels and B and T cell subpopulations cell counts.
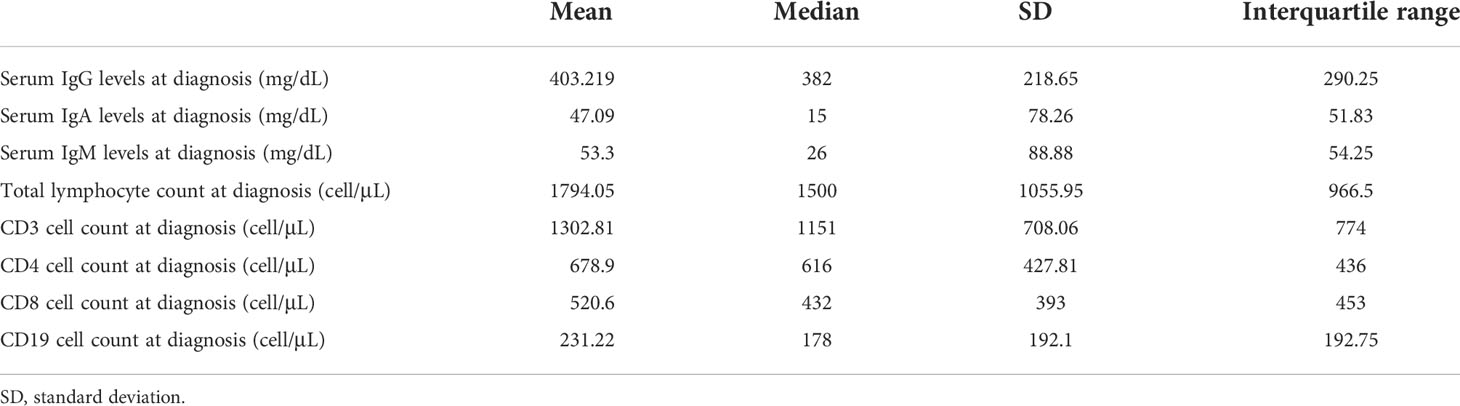
Table 6 Data on mmunoglobulin levels and lymphocyte subpopulations count in the GTEM-SEMI-CVID Registry.
IgRT and mortality
Two hundred and fourteen patients were under active treatment with IgRT. Remarkably, 29 patients were not being treated or had received IgRT at the time of data collection, and 3/29had already died. Therapeutic information was lacking for 8 patients in the national cohort. No differences were observed in the baseline epidemiological features of patients in the non-treated group, being only discretely younger than the treated group (46.10 vs 51.51 years). Intravenous route (IVIgRT) was preferred (124 patients, 57.94%) over subcutaneous (SCIgRT) (88, 41.12%) or intramuscular (IMIgRT) (1, 0.47%) routes. All patients received IVIgRT at the hospital, and most patients under SCIgRT (74 patients) administered it at home, or both (5).
Fifteen patients had died until the time of data collection, meaning a mortality rate of 6% in our cohort until data cut-off, with a mean age at death of 57 years old (SD 20.16) and a follow-up time until death of 7.6 years (SD 7.75). Non-infectious complications such as chronic respiratory failure (3 patients), solid or hematological malignancies (3 patients), or dysimmune complications (3 patients) were more frequent than infectious complications (3 patients) when analyzing the cause of death.
Discussion
The GTEM-SEMI-CVID-Registry systematically compiles the current clinical profile of 250 patients diagnosed with CVID in Spain on the basis of a nationwide multicentric approach. Hence, a complete, updated, and integrated view of the CVID clinical course is detailed in this study, which increases the available data provided by other CVID cohorts.
In line with previous reports, the mean diagnostic delay in our study was around 10 years (8, 19, 20), and most patients initially presented with infectious complications followed by non-infectious immune disorders. However, the current diagnostic delay appears higher than previously reported in partial cohorts in our country, which ranged from 4-6 years (4). More than one-third of the patients in our cohort showed lymphadenopathies and splenomegaly in their follow-up, and more than 30% presented immune cytopenias, with a higher prevalence than in other international cohorts, possibly due to a relatively higher mean age of our patients and longer disease evolution (8, 14, 17, 19) (Figures 1, 2). Remarkably, Evans’ syndrome was the most frequently described immune cytopenia instead of isolated ITP as previously described (5, 8, 14). Furthermore, systemic autoimmunity was reported in 20% of the patients, with anchylosing spondylitis being the most frequent rheumatic disease. This highlights the present need for developing referral protocols allowing an earlier diagnosis, which should include not only repeated infections as the main red flag for suspecting CVID and other immunodeficiencies (21, 22) but also immune disorders and organ lymphoproliferation.
Since the introduction of IgRT, infectious complications are not the main cause of morbimortality in CVID patients (5), as illustrated in this series. For more than a decade, SCIgRT has been introduced as a successful alternative to conventional IVIgRT with optimal IgG trough levels, fewer side effects, better health-related quality of life, patient empowerment, and faster functional recovery with less contact with the healthcare environment (23). Nevertheless, less than half of the patients received SCIgRT and IVIgRT was preferred by almost 60%. Through these data, practitioners should be encouraged to consider switching IVIgRT to SCIgRT for qualified patients with CVID.
Non-infectious lung disease was extraordinarily frequent in our registry affecting approximately 60% of the patients, which shows a higher prevalence than previously known (5, 8, 14) (Figure 1). Bronchiectasis was the most frequent imaging finding (35%) in consonance with previous studies (14). This could be due to chronic and repeated infections rather than local immune dysregulation (24). However, lung parenchymal involvement was observed in around 15% of the patients, mainly as lymphoid interstitial pneumonia. Despite the high prevalence of lung disease, less than 65% of the patients included in the cohort underwent a HRCT. This advocates that some patients with subclinical affectation may have been underdiagnosed in our cohort, as only around 20% experienced respiratory clinical manifestations such as cough or dyspnea. In line with this, histologically confirmed GLILD was only seen in 17 patients; a notably lesser prevalence than expected according to previous evidence (25, 26). This emphasizes the need for a further active search for chronic lung disease in the follow-up of these patients despite being asymptomatic or paucisymptomatic, as it has been associated with poorer clinical outcomes (8, 27).
In the GTEM-SEMI-CVID Registry, gastrointestinal disease was observed in more than 40%, which is the high end of previously reported data (range: 9 – 44%) (8, 14, 17, 19, 20, 28). Intestinal lymphocytic infiltration was the most common histological finding, being present in almost 40% of the biopsies, as recently published (14).
These results concur with growing evidence supporting disseminated benign lymphoproliferation and infiltration as one of the main characteristics of abnormal immunity in CVID patients, which may result in organ dysfunction at different levels. Among biopsied organs in our cohort, benign lymphoproliferation was the principal histopathological alteration, except for spleen and liver, where granulomatosis was observed in 75% and 42% of the biopsies, respectively. Interestingly, in non-lymphoid organs, lymphocytic infiltration was more frequent in gastrointestinal tract, probably due to the continuous antigen-lymphocyte interaction with local microbiota. Many studies have shown increased permeability of the gut barrier which results in microbial translocation and local inflammation, both endpoints of the systemic immune activation that was expressed in the histological findings of the patients in our cohort (29–31).
This coexistence of immunodeficiency and immune dysregulation with diffuse lymphocytic infiltration and autoimmune disorders in CVID patients seems paradoxical, requiring the use of immunosuppressant treatments on already immunosuppressed patients. In our case, almost 40% of the individuals had received immunosuppressant therapies, mainly corticosteroids followed by azathioprine and, notably, rituximab. These agents were mainly used to treat immune cytopenias, granulomatous or lymphocytic disorders, and other autoimmune complications. Given their risk of adverse effects, the need for these therapies reveals an important therapeutic complexity (32), especially considering the relatively high prevalence of opportunistic infections in our cohort, of up to 9.64% with clear relation to some of the most frequently used treatments. Further pathophysiological studies are needed to unravel the genetic and molecular pathways driving CVID dysimmunity that will allow the development of targeted therapies with fewer side effects.
In this regard, the presence of persistent abnormalities in immune activation and systemic inflammation have been related to an increased risk of cardiovascular disease (33, 34). Although the chronic proinflammatory state of CVID could be related to higher cardiovascular risk, evidence is still scarce (35–37). Nonetheless, the prevalence of cardiovascular comorbidities was not increased in our series when compared to the Spanish general population of the same age group. For instance, hypertension and type 2 DM are found in 42.6% and 14.8% of the Spanish adult population respectively, whereas in our study, the global prevalence of hypertension and type 2 DM was 20.88% and 8.84%, respectively. Chronic kidney disease (CKD) accounted for 4.82% of the patients in our registry, while the global prevalence of CKD is 15.1% for the Spanish adult population (38, 39). Studies aiming to profile the cardiovascular risk in CVID are needed to overcome this large knowledge gap.
Moreover, in the literature, patients with CVID have a significantly higher risk of both hematological and solid malignancies, with a described prevalence of approximately 10% (ranging from 1.5 – 20.7%). The overall prevalence of cancer in our registry was one of the highest reported to date, of up to 15.26% (5, 13, 14, 39–42) (Figure 1). As with immune complications, the higher mean age in the Registry as well as the diagnostic delay could partially explain these findings (13). In line with previous evidence, non-Hodgkin B lymphoma was the most frequently reported malignancy, followed by gastric cancer, lung tumors, and cutaneous malignancies. Despite the declining incidence of gastric cancer in older reports (43, 44), the prevalence of 2% in this series is significantly higher compared to the other recent studies (5, 14). The fact that approximately half of all patients had been actively investigated for the presence of H. pylori may have contributed to these higher figures and indicates the need for periodical screening for this infection in all CVID patients.
Several important limitations deserve mention. Firstly, this is a retrospective cohort study. Despite a systematic and closed form with clear instructions and definition of variables was provided, data were collected by a large number of researchers which could have led to heterogeneity in data input and validation. In fact, due to the retrospective approach based on the review of electronic clinical records, some information was not available, thus limiting its extrapolation to the general population with CVID. Secondly, despite the large number of clinical and complementary variables included in the registry, other important variables such as a complete cardiovascular risk evaluation, other received treatments apart from immunosuppressants and immunoglobulins, and complete lymphocyte subpopulation counts, among others, were not included. Noteworthy, only adult individuals were included, and many hospitals were not reference institutions for treating PIDs. This fact might have influenced the follow-up of CVID patients but is a clear reflection of the Spanish reality in the diagnosis, management, and treatment of this heterogeneous disease. Finally, this study was conceived from a descriptive approach, and no inferential analyses were performed. Data from the GTEM-SEMI-CVID Registry will be used for the design of further studies aiming to characterize and compare patient subpopulations.
Conclusion
This is the first nationwide multicentric study on CVID patients in Spain including both secondary and tertiary referral hospitals. The data provided by this work stress the need for developing national guidelines to optimize the diagnosis and management of these patients. Chronic dysimmune complications have emerged as the main cause of morbidity and mortality after the introduction of IgRT and pose a great challenge for clinicians treating PIDs. The lack of effective treatments and the use of immunosuppressants for the management of these disorders emphasizes the importance of basic and translational research delving into the pathophysiological pathways involved in immune dysregulation and diffuse lymphocytic infiltration. This would reveal new tailored strategies to reduce immune complications, the associated healthcare burden, and ensure a better quality of life for CVID patients. Moreover, evidence on cardiovascular disease in CVID is lacking and new studies should be designed to address this considerable knowledge gap. Finally, further studies with a large sample size in other regions, and meta-analyses of current evidence are needed to improve the epidemiological knowledge of this complex and heterogeneous disorder.
Data availability statement
The datasets presented in this article are not readily available because they belong to an institutional multicentric registry from the Spanish Society of Internal Medicine. Requests to access the datasets should be directed to the promotor of the registry, PMM: bW9yYWxfcGVkQGd2YS5lcw==.
Ethics statement
This study has been independently approved by the ethics comittees of all participating institutions. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements. All authors contributed to the article and approved the submitted version.
Author contributions
MC-N, VG-B, and PMM conceived the idea, searched the bibliographic materials, and reviewed the existing literature. MC-N, VG-B, and PMM developed the tables. VG-B performed the statistical analysis. MC-N, VG-B, MN-B and PMM contributed to the writing of the article. The rest of the authors contributed in data inclusion and variable collection in their respective centers. All authors are responsible for the care of the patients and provided their data to the GTEM-SEMI-CVID Registry.
Funding
The article processing charge for publication has been funded by CSL Behring. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Acknowledgments
We would like to thank the Working Group of Minority Diseases of the Spanish Society of Internal Medicine (GTEM), the Spanish Society of Internal Medicine (SEMI) and the Valencian Community Society of Internal Medicine (SMICV) for their support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.1033666/full#supplementary-material
References
1. Picard C, Bobby Gaspar H, Al-Herz W, Bousfiha A, Casanova JL, Chatila T, et al. International union of immunological societies: 2017 primary immunodeficiency diseases committee report on inborn errors of immunity. J Clin Immunol (2018) 38:96–128. doi: 10.1007/s10875-017-0464-9
2. Seidel MG, Kindle G, Gathmann B, Quinti I, Buckland M, van Montfrans J, et al. The European society for immunodeficiencies (ESID) registry working definitions for the clinical diagnosis of inborn errors of immunity. J Allergy Clin Immunol Pract (2019) 7(6):1763–70. doi: 10.1016/j.jaip.2019.02.004
3. Bonilla FA, Barlan I, Chapel H, Costa-Carvalho BT, Cunningham-Rundles C, de la Morena MT, et al. International consensus document (ICON): common variable immunodeficiency disorders. J Allergy Clin Immunol Pract (2016) 4:38–59. doi: 10.1016/j.jaip.2015.07.025
4. Gathmann B, Mahlaoui N CEREDIH, Gérard L, Oksenhendler E, Warnatz K, Schulze I, et al. Clinical picture and treatment of 2212 patients with common variable immunodeficiency. J Allergy Clin Immunol (2014) 134(1):116–26. doi: 10.1016/j.jaci.2013.12.1077
5. Resnick ES, Moshier EL, Godbold JH, Cunningham-Rundles C. Morbidity and mortality in common variable immune deficiency over 4 decades. Blood (2012) 119(7):1650–7. doi: 10.1182/blood-2011-09-377945
6. Orange JS, Grossman WJ, Navickis RJ, Wilkes MM. Impact of trough IgG on pneumonia incidence in primary immunodeficiency: A meta-analysis of clinical studies. Clin Immunol (2010) 137(1):21–30. doi: 10.1016/j.clim.2010.06.012
7. Fischer A, Provot J, Jais JP, Alcais A, Mahlaoui N, members of the CFPIDsg. Autoimmune and inflammatory manifestations occur frequently in patients with primary immunodeficiencies. J Allergy Clin Immunol (2017) 140:1388–93.e8. doi: 10.1016/j.jaci.2016.12.978
8. Chapel H, Lucas M, Lee M, Bjorkander J, Webster D, Grimbacher B, et al. Common variable immunodeficiency disorders: division into distinct clinical phenotypes. Blood (2008) 112:277–86. doi: 10.1182/blood-2007-11-124545
9. Azizi G, Abolhassani H, Asgardoon MH, Alinia T, Yazdani R, Mohammadi J, et al. Autoimmunity in common variable immunodeficiency: epidemiology, pathophysiology and management. Expert Rev Clin Immunol (2017) 13(2):101–15. doi: 10.1080/1744666X.2016.1224664
10. Cabanero-Navalon MD, Garcia-Bustos V, Forero-Naranjo LF, Baettig-Arriagada EJ, Núñez-Beltrán M, Cañada-Martínez AJ, et al. Integrating clinics, laboratory, and imaging for the diagnosis of common variable immunodeficiency-related granulomatous-lymphocytic interstitial lung disease. Front Immunol (2022) 13:813491. doi: 10.3389/fimmu.2022.813491
11. Rizvi FS, Zainaldain H, Rafiemanesh H, Jamee M, Hossein-Khannazer N, Hamedifar H, et al. Autoimmunity in common variable immunodeficiency: a systematic review and meta-analysis. Expert Rev Clin Immunol (2020) 16(12):1227–35. doi: 10.1080/1744666X.2021.1850272
12. Andersen IM, Jørgensen SF. Gut inflammation in CVID: causes and consequences. Expert Rev Clin Immunol (2022) 18(1):31–45. doi: 10.1080/1744666X.2021.2008241
13. Kiaee F, Azizi G, Rafiemanesh H, Zainaldain H, Sadaat Rizvi F, Alizadeh M, et al. Malignancy in common variable immunodeficiency: a systematic review and meta-analysis. Expert Rev Clin Immunol (2019) 15(10):1105–13. doi: 10.1080/1744666X.2019.1658523
14. Ho HE, Cunningham-Rundles C. Non-infectious complications of common variable immunodeficiency: Updated clinical spectrum, sequelae, and insights to pathogenesis. Front Immunol (2020) 11:149. doi: 10.3389/fimmu.2020.00149
15. Hurst JR, Verma N, Lowe D, Baxendale HE, Jolles S, Kelleher P, et al. British Lung Foundation/United kingdom primary immunodeficiency network consensus statement on the definition, diagnosis, and management of granulomatous-lymphocytic interstitial lung disease in common variable immunodeficiency disorders. J Allergy Clin Immunol Pract (2017) 5(4):938–45. doi: 10.1016/j.jaip.2017.01.021
16. Bethune C, Egner W, Garcez T, Huissoon A, Jolles S, Karim Y, et al. British Society for Immunology/United kingdom primary immunodeficiency network consensus statement on managing non-infectious complications of common variable immunodeficiency disorders. Clin Exp Immunol (2019) 196(3):328–35. doi: 10.1111/cei.13272
17. Mormile I, Punziano A, Riolo CA, Granata F, Williams M, de Paulis A, et al. Common variable immunodeficiency and autoimmune diseases: A retrospective study of 95 adult patients in a single tertiary care center. Front Immunol (2021) 12:652487. doi: 10.3389/fimmu.2021.652487
18. Hermaszewski RA, Webster AD. Primary hypogammaglobulinaemia: a survey of clinical manifestations and complications. Q J Med (1993) 86(1):31–42.
19. Wehr C, Kivioja T, Schmitt C, Ferry B, Witte T, Eren E, et al. The EUROclass trial: defining subgroups in common variable immunodeficiency. Blood (2008) 111(1):77–85. doi: 10.1182/blood-2007-06-091744
20. Ramírez-Vargas N, Arablin-Oropeza SE, Mojica-Martínez D, Yamazaki-Nakashimada MA, de la Luz García-Cruz M, Terán-Juárez LM, et al. Clinical and immunological features of common variable immunodeficiency in Mexican patients. Allergol Immunopathol (2014) 42(3):235–40. doi: 10.1016/j.aller.2013.01.007
21. Arslan S, Ucar R, Caliskaner AZ, Reisli I, Guner SN, Sayar EH, et al. How effective are the 6 European society of immunodeficiency warning signs for primary immunodeficiency disease? Ann Allergy Asthma Immunol (2016) 116(2):151–155.e1. doi: 10.1016/j.anai.2015.12.001
22. Arkwright PD, Gennery AR. Ten warning signs of primary immunodeficiency: a new paradigm is needed for the 21st century. Ann N Y Acad Sci (2011) 1238:7–14. doi: 10.1111/j.1749-6632.2011.06206.x
23. Abolhassani H, Sadaghiani MS, Aghamohammadi A, Ochs HD, Rezaei N. Home-based subcutaneous immunoglobulin versus hospital-based intravenous immunoglobulin in treatment of primary antibody deficiencies: systematic review and meta analysis. J Clin Immunol (2012) 32(6):1180–92. doi: 10.1007/s10875-012-9720-1
24. Schussler E, Beasley MB, Maglione PJ. Lung disease in primary antibody deficiencies. J Allergy Clin Immunol Pract (2016) 4(6):1039–52. doi: 10.1016/j.jaip.2016.08.005
25. Bates CA, Ellison MC, Lynch DA, Cool CD, Brown KK, Routes JM. Granulomatous-lymphocytic lung disease shortens survival in common variable immunodeficiency. J Allergy Clin Immunol (2004) 114(2):415–21. doi: 10.1016/j.jaci.2004.05.057
26. Morimoto Y, Routes JM. Granulomatous disease in common variable immunodeficiency. Curr Allergy Asthma Rep (2005) 5(5):370–5. doi: 10.1007/s11882-005-0008-x
27. Verma N, Grimbacher B, Hurst JR. Lung disease in primary antibody deficiency. Lancet Respir Med (2015) 3(8):651–60. doi: 10.1016/S2213-2600(15)00202-7
28. Farmer JR, Ong MS, Barmettler S, Yonker LM, Fuleihan R, Sullivan KE, et al. Common variable immunodeficiency non-infectious disease endotypes redefined using unbiased network clustering in Large electronic datasets. Front Immunol (2018) 8:1740. doi: 10.3389/fimmu.2017.01740
29. Jørgensen SF, Fevang B, Aukrust P. Autoimmunity and inflammation in CVID: a possible crosstalk between immune activation, gut microbiota, and epigenetic modifications. J Clin Immunol (2019) 39(1):30–6. doi: 10.1007/s10875-018-0574-z
30. Gereige JD, Maglione PJ. Current understanding and recent developments in common variable immunodeficiency associated autoimmunity. Front Immunol (2019) 10:2753. doi: 10.3389/fimmu.2019.02753
31. Varricchi G, Poto R, Ianiro G, Punziano A, Marone G, Gasbarrini A, et al. Gut microbiome and common variable immunodeficiency: Few certainties and many outstanding questions. Front Immunol (2021) 12:712915. doi: 10.3389/fimmu.2021.712915
32. Xiao X, Miao Q, Chang C, Gershwin ME, Ma X. Common variable immunodeficiency and autoimmunity–an inconvenient truth. Autoimmun Rev (2014) 13(8):858–64. doi: 10.1016/j.autrev.2014.04.006
33. Fioranelli M, Bottaccioli AG, Bottaccioli F, Bianchi M, Rovesti M, Roccia MG. Stress and inflammation in coronary artery disease: A review psychoneuroendocrineimmunology-based. Front Immunol (2018) 9:2031. doi: 10.3389/fimmu.2018.02031
34. So-Armah K, Benjamin LA, Bloomfield GS, Feinstein MJ, Hsue P, Njuguna B, et al. HIV And cardiovascular disease. Lancet HIV (2020) 7(4):e279–93. doi: 10.1016/S2352-3018(20)30036-9
35. Vieira DG, Costa-Carvalho BT, Hix S, da Silva R, Correia MSG, Sarni ROS. Higher cardiovascular risk in common variable immunodeficiency and X-linked agammaglobulinaemia patients. Ann Nutr Metab (2015) 66(4):237–41. doi: 10.1159/000435818
36. Ucar R, Arslan S, Turkmen K, Calıskaner AZ. Accelerated atherosclerosis in patients with common variable immunodeficiency: Is it overlooked or absent? Med Hypotheses (2015) 85(4):485–7. doi: 10.1016/j.mehy.2015.07.002
37. Macpherson ME, Halvorsen B, Yndestad A, Ueland T, Mollnes TE, Berge RK, et al. Impaired HDL function amplifies systemic inflammation in common variable immunodeficiency. Sci Rep (2019) 9(1):9427. doi: 10.1038/s41598-019-45861-1
38. Menéndez E, Delgado E, Fernández-Vega F, Prieto MA, Bordiú E, Calle A, et al. Prevalence, diagnosis, treatment, and control of hypertension in spain. results of theZGlAYmV0LmVzstudy. Rev Esp Cardiol (Engl Ed) (2016) 69(6):572–8. doi: 10.1016/j.rec.2015.11.034
39. Gorostidi M, Sánchez-Martínez M, Ruilope LM, Graciani A, de la Cruz JJ, Santamaría R. Chronic kidney disease in Spain: Prevalence and impact of accumulation of cardiovascular risk factors. Nefrologia (Engl Ed) (2018) 38(6):606–15. doi: 10.1016/j.nefro.2018.04.004
40. Cunningham-Rundles C, Bodian C. Common variable immunodeficiency: clinical and immunological features of 248 patients. Clin Immunol (1999) 92(1):34–48. doi: 10.1006/clim.1999.4725
41. Abolhassani H, Aghamohammadi A, Imanzadeh A, Mohammadinejad P, Sadeghi B, Rezaei N. Malignancy phenotype in common variable immunodeficiency. J Investig Allergol Clin Immunol (2012) 22(2):133–4.
42. Quinti I, Soresina A, Spadaro G, Martino S, Donnanno S, Agostini C, et al. Long-term follow-up and outcome of a large cohort of patients with common variable immunodeficiency. J Clin Immunol (2007) 27(3):308–16. doi: 10.1007/s10875-007-9075-1
43. Kinlen LJ, Webster AD, Bird AG, Haile R, Peto J, Soothill JF, et al. Prospective study of cancer in patients with hypogammaglobulinaemia. Lancet (1985) 1(8423):263–6. doi: 10.1016/s0140-6736(85)91037-2
Keywords: common variable immunodeficiency, CVID, cohort, dysimmunity, immune dysregulation, lymphoproliferation
Citation: Cabañero-Navalon MD, Garcia-Bustos V, Nuñez-Beltran M, Císcar Fernández P, Mateu L, Solanich X, Carrillo-Linares JL, Robles-Marhuenda Á, Puchades-Gimeno F, Pelaez Ballesta A, López-Osle N, Torralba-Cabeza MÁ, Bielsa Masdeu AM, Diego Gil J, Tornador Gaya N, Pascual Castellanos G, Sánchez-Martínez R, Barragán-Casas JM, González-García A, Patier de la Peña JL, López-Wolf D, Mora Rufete A, Canovas Mora A, Forner Giner MJ and Moral Moral P (2022) Current clinical spectrum of common variable immunodeficiency in Spain: The multicentric nationwide GTEM-SEMI-CVID registry. Front. Immunol. 13:1033666. doi: 10.3389/fimmu.2022.1033666
Received: 31 August 2022; Accepted: 11 October 2022;
Published: 28 October 2022.
Edited by:
Hans-Hartmut Peter, University of Freiburg Medical Center, GermanyReviewed by:
Ulrich Salzer, University of Freiburg Medical Center, GermanyJacqueline Kerr, Paul-Ehrlich-Institut (PEI), Germany
Copyright © 2022 Cabañero-Navalon, Garcia-Bustos, Nuñez-Beltran, Císcar Fernández, Mateu, Solanich, Carrillo-Linares, Robles-Marhuenda, Puchades-Gimeno, Pelaez Ballesta, López-Osle, Torralba-Cabeza, Bielsa Masdeu, Diego Gil, Tornador Gaya, Pascual Castellanos, Sánchez-Martínez, Barragán-Casas, González-García, Patier de la Peña, López-Wolf, Mora Rufete, Canovas Mora, Forner Giner and Moral Moral. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Victor Garcia-Bustos, dmljdG9yZ2FyY2lhYnVzdG9zQGdtYWlsLmNvbQ==