 Allen Cheng-Wei Li
Allen Cheng-Wei Li Chen Dong
Chen Dong Soon-Tzeh Tay
Soon-Tzeh Tay Ashwin Ananthakrishnan4*†
Ashwin Ananthakrishnan4*† Kevin Sheng-Kai Ma
Kevin Sheng-Kai Ma
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Immunol. , 11 November 2022
Sec. Alloimmunity and Transplantation
Volume 13 - 2022 | https://doi.org/10.3389/fimmu.2022.1025350
This article is part of the Research Topic Novel Mechanism and Strategies to Overcome Relapse after Allogeneic Stem Cell Transplantation View all 6 articles
Objective: To determine the safety and efficacy of vedolizumab for the prophylaxis and treatment of gastrointestinal involvement of acute graft-versus-host disease (GVHD) (GI-aGVHD).
Methods: Literature search within PubMed, EMBASE, Web of Science, and Cochrane Library for observational studies and clinical trials that evaluated the effect of vedolizumab on GI-aGVHD was done through 17 May 2022. A bivariate and random-effect meta-analysis derived the pooled observational percentages and pooled risk ratios (RRs) from baseline of primary endpoints including overall response, complete response, mortality, and adverse events.
Results: There was a total of 122 participants in eight eligible studies, including one study on the prophylactic use of vedolizumab and seven studies on vedolizumab for the treatment of GI-aGVHD. Of seven studies that reported details on baseline grades of GI-aGVHD, a total of 47 patients (47.95%) were of stage 4, 31 patients (31.63%) were of stage 3, 10 patients (10.2%) were of stage 2, and 10 patients (10.2%) were of stage 1. The use of vedolizumab for the treatment of GI-aGVHD yielded a significantly improved objective response rate (ORR) at 14 days (pooled ORR = 60.53%, pooled RR = 14.14, 95% CI: 2.95–67.71), 28 days (pooled ORR = 50%, RR = 7.36, 95% CI = 2.14–25.37), and 12 months (pooled ORR = 76.92%, RR = 13.66, 95% CI = 3.5–53.35) from baseline. Likewise, the use of vedolizumab was followed by a significantly improved complete response (CR) at 12 months (pooled CR = 27.27%, RR = 5.50, 95% CI = 1.01–29.95), yet the CR at 14 days and 28 days did not reach statistical significance. Fifty-seven out of 87 (pooled overall survival, OS = 34.5%) and 46 out of 65 (pooled OS = 29.2%) patients expired at 6 and 12 months after the use of vedolizumab, respectively. Prophylactic use of vedolizumab was not associated with any specific type of reported adverse events, while patients with GI-aGVHD on vedolizumab presented with significantly increased risks of adverse events including infections (RR = 7.55) and impaired metabolism or nutritional complications (RR = 9.00). All analyses were of a low heterogeneity (all I-squares = 0%).
Conclusion: Vedolizumab was safe and effective for the prophylaxis and management of early grade GI-aGVHD. More clinical evidence is warranted to validate these findings.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=345584, identifier CRD42022345584.
Hematopoietic cell transplantation (HSCT) is a medical procedure in which stem cells are infused into patients following short-term courses of chemotherapy or radiotherapy for hematopoietic malignancies or benign hematologic conditions (1, 2). Despite its success, severe graft-versus-host disease (GVHD) as a result of HSCT remains an unmet medical challenge, whose incidence ranges from 20% to 80% (3). The mechanisms by which acute GVHD occurs involve donor-activated T cells that recognize the recipient as foreign, which initiate immune reactions in various organs including skin, liver, lungs, and the gastrointestinal (GI) tract; as such, immunosuppressive medications are used for its prophylaxis (4). aGVHD is staged from grades I to IV according to the extent of organ involvement and the number of involved organs. Common risk factors for aGVHD include unrelated donors, mismatched donors, graft types, multiparous female donors, older ages of donors, and recipients (4). Although skin is the most common affected organ, cumulative evidence from previous studies has suggested the GI involvement of aGVHD (GI-aGVHD), manifested as persistent anorexia, diarrhea, abdominal pain, and hemorrhage, that is associated with great all-cause mortality (70%–90%) (5–7).
Existing options for the first-line treatment of grade II or above aGVHD other than corticosteroids are limited, with the compromised efficacy of corticosteroids resulting in fewer than 50% of patients having durable remission following treatments that only involved corticosteroids (8). For this, several combinations of steroids and additional systemic therapies have been used to treat steroid-refractory (SR) aGVHD (SR-aGVHD), although significant adverse events are as well noted. For instance, despite previous studies on cyclosporine, mycophenolate mofetil (MMF), ruxolitinib, extracorporeal photopheresis (ECP), tacrolimus, sirolimus, basiliximab, daclizumab, and infliximab have demonstrated the efficacy of these agents for GI symptoms of aGVHD, long-term use of these immunosuppressive agents is associated with high infection rate and poor life quality (9–11). As such, patients suffering from GI-aGVHD remained of poor prognosis and survival due to a lack of management that allows for both high treatment response and low infectious adverse events, following which damage to GI tract amplifies the severity of aGVHD through microbiota-triggered activation of inflammatory pathways (12, 13).
Vedolizumab, a monoclonal antibody that inhibits the interaction between α4β7 integrins on T lymphocytes and mucosal vascular addressin cell adhesion molecule 1 (MADCAM1) on gut endothelial cells, was reported to exert favorable efficacy and safety profile in bio-naïve patients with inflammatory bowel disease (IBD) including both ulcerative colitis and Crohn’s disease (14, 15) through blocking the homing of TH1, TH2, TH17, and Treg cells to inflamed colon and their subsequent accumulation in the tissue. The activation of α4β7 integrins by antigen-presenting cells (APC) in the GI tract is crucial for the trafficking of immunocompetent donor T lymphocytes to GI mucosa and gut-associated lymphoid tissues (GALT), which is also involved in the pathogenesis of GI-aGVHD (16, 17). However, clinical studies on vedolizumab for the treatment of GI-aGVHD were of limited sample sizes, with each studies typically enrolling less than 30 participants; thus, the efficacy cannot be robustly concluded (18). Moreover, there is a lack of studies on whether vedolizumab may be used as standard prophylaxis for GI-aGVHD in patients undergoing HSCT (19). Thus, the present systematic review and meta-analysis was designed to determine the safety and efficacy of vedolizumab for the prophylaxis and treatment of GI-aGVHD, respectively.
Studies on vedolizumab for the management of GI-aGVHD were retrieved and reviewed. We searched the following databases: MEDLINE, EMBASE, Web of science, and the Cochrane Library on May 17th, 2022 in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyzes (PRISMA) statement (20). The search strategy was developed using a combination of keywords as follows: (“biologics” OR “biological” OR “vedolizumab” OR “α4β7” OR “alpha4beta7”) AND (“graft versus host disease” OR “graft-versus-host disease” OR “gvhd”). We manually searched for further references to included research that were relevant.
Two investigators extracted all data independently to ensure accuracy and consistency. Disagreements were settled by consensus or by seeking an independent third viewpoint (21–48). Eligible studies were clinical studies on vedolizumab for GVHD including either aGVHD or chronic GVHD (cGVHD). Letters to editor, expert comments, and studies without recorded treatment course were excluded (Figure 1).
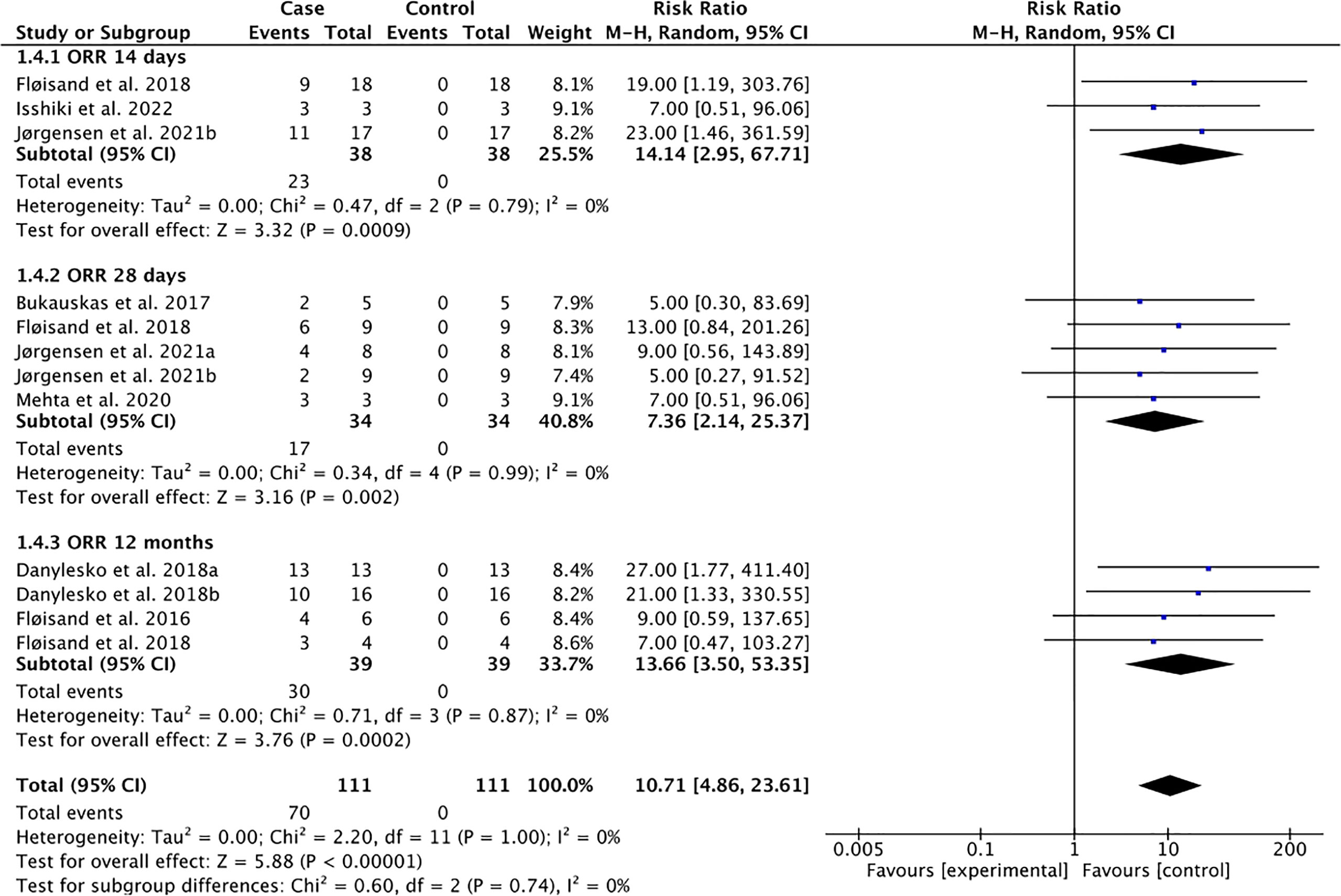
Figure 1 Overall response rate (ORR) following the use of vedolizumab for GI-aGVHD.
Two reviewers independently selected studies by screening titles and abstracts to identify those potentially relevant to our study question. Reported results of the included studies were extracted and analyzed. Disagreement was settled by discussion and review of the articles. The quality of included studies was assessed according to the Newcastle–Ottawa Scale (NOS) and NOS modified for single-arm cohorts (25). The ratings were made based on the quality of selection (up to four points), comparability (up to two points), and outcome of study participants (up to three points). The overall quality of study was defined as poor (scores 0–3), fair (scores, 4–6), or good (scores, 7–9). The quality assessment was carried out independently by two investigators. If there was a disagreement, it was resolved through discussion.
Data on baseline demographics including country in which the study was conducted, study population, age, sex, and disease characteristics for the indication of HSCT, the grade and organs involved in aGVHD, and the usage, dose, intervention time, and duration of treatment of vedolizumab were extracted. Outcomes recorded during the follow-up period included main treatment response such as overall response, complete response, mortality, skin involvement, intestinal involvement, and hepatic involvement. Specifically, partial response was defined as an improvement of one aGVHD grade in at least one organ without progression in any other organs, while complete response was defined as the resolution of all signs and symptoms of aGVHD, according to the criteria described by Martin et al. (26). Overall response rate (ORR) included partial response rate plus complete response rate (CRR), as obtained on day 14, day 28, and 12 months after the initiation of vedolizumab treatment. Adverse events related to vedolizumab were also recorded.
A bivariate meta-analysis was used to derive the pooled estimates of outcomes including overall response, complete response, mortality, and adverse events following the use of vedolizumab in patients with GI-aGVHD, measured as pooled observational percentages of all participants and pooled Mantel–Haenszel (M–H) risk ratios with 95% confidence intervals (CIs) in the random-effect model using RevMan5 software (Cochrane Collaboration). For single-arm studies, the outcomes were compared with that at baseline, with which all outcomes at day 0 were set as zero. I-square was derived to determine the heterogeneity of all analyses, with I-square values less than 50% indicating between-study homogeneity. A p-value less than 0.05 in tests for overall effect indicated significant differences after the use of vedolizumab from baseline.
A total of 7,432 studies were identified through initial search. After screening the studies with titles and abstracts, 98 studies were further assessed, during which 90 studies were excluded due to duplicated study population or not human subjects research. Eight studies met the inclusion criteria (Figure S1), for which the study design and primary outcomes were summarized (Table 1).
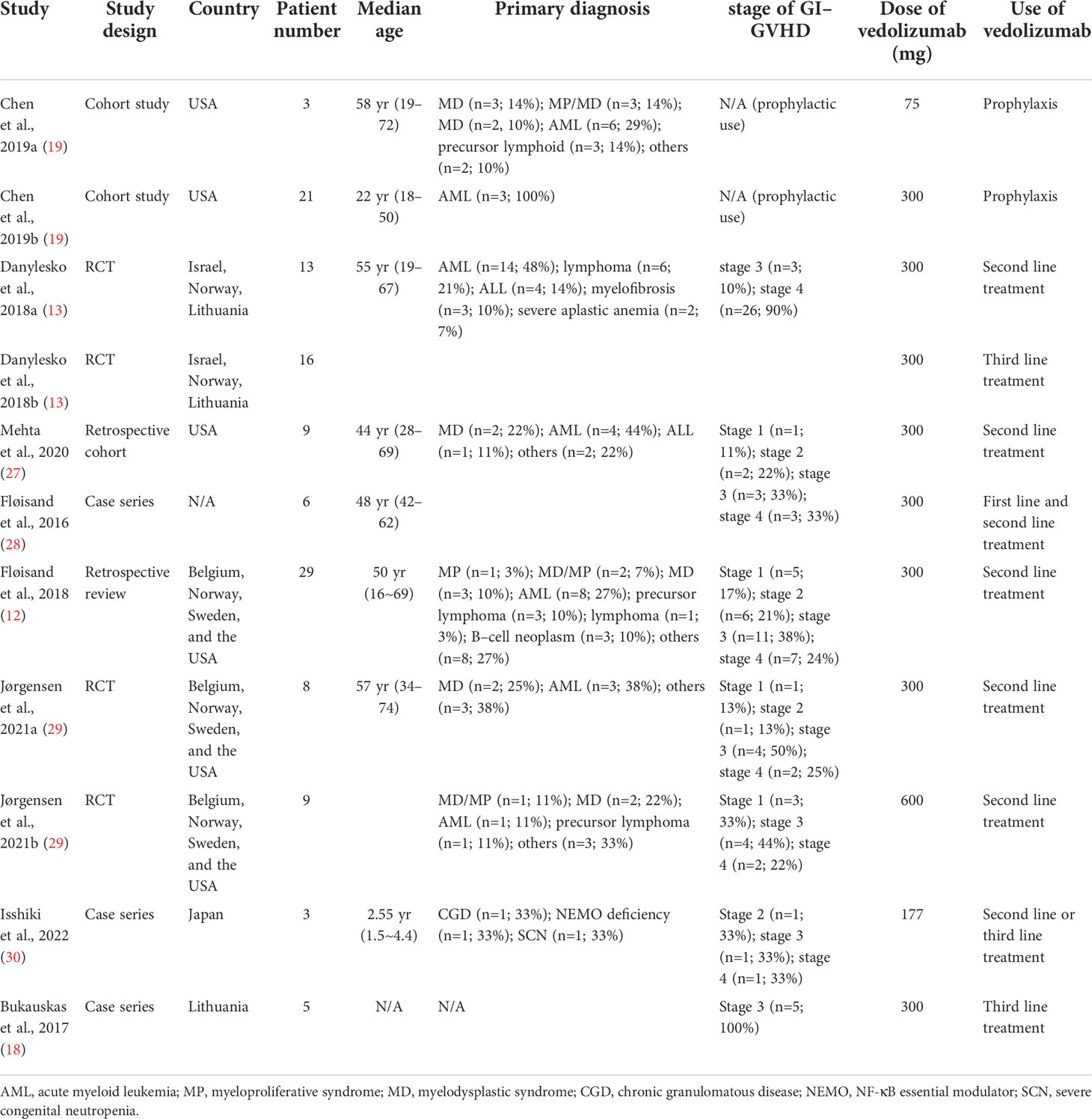
Table 1 Overview of studies included in the systemic review.
There was a total of 122 patients who developed GI-aGVHD following HSCT from the included eight included studies. Acute GVHD was diagnosed according to the Glucksberg–Seattle criteria (27) and clinically graded according to the modified Glucksberg criteria (27). The median age of patients across studies ranged from 2.55 to 59 years (Table 1).
Of seven studies that reported details on stages of GI-aGVHD in patients undergoing vedolizumab treatment for GVHD, a total of 47 patients (pooled rate = 47.95%) were of stage 4, 31 patients (pooled rate = 31.63%) were of stage 3, 10 patients (10.2%) were of stage 2, and 10 patients (10.2%) were of stage 1. In addition, patients in one study on vedolizumab for the prophylaxis of GI-aGVHD (19) did not have baseline GI-aGVHD. Accordingly, the seven (12, 13, 18, 28–31) studies on vedolizumab for the treatment of GI-aGVHD were included in the meta-analysis on the efficacy of vedolizumab, while the study (19) on prophylactic use of vedolizumab was not considered in the meta-analysis on the efficacy of vedolizumab.
The type of transplant was matched related donor (MSD) in 71 patients (pooled rate = 86.58%), mismatched related donor (MMRD) in eight adults (pooled rate = 9.75%), and haploidentical in three adults (pooled rate = 3.65%) across studies. Three studies (12, 18, 29) did not report details of the transplant type. Of three studies that reported details of conditioning regimens, 41 patients (pooled rate = 58.57%) used the non-myeloablative conditioning (NMA) regimen and 29 patients (pooled rate = 41.42%) used the myeloablative conditioning (MAC) regimen, while five studies (13, 18, 28, 29, 31) did not report details on the conditioning regimen (Table 1). Overall, three studies were assessed as good quality, and the rest were fair (Table 2).
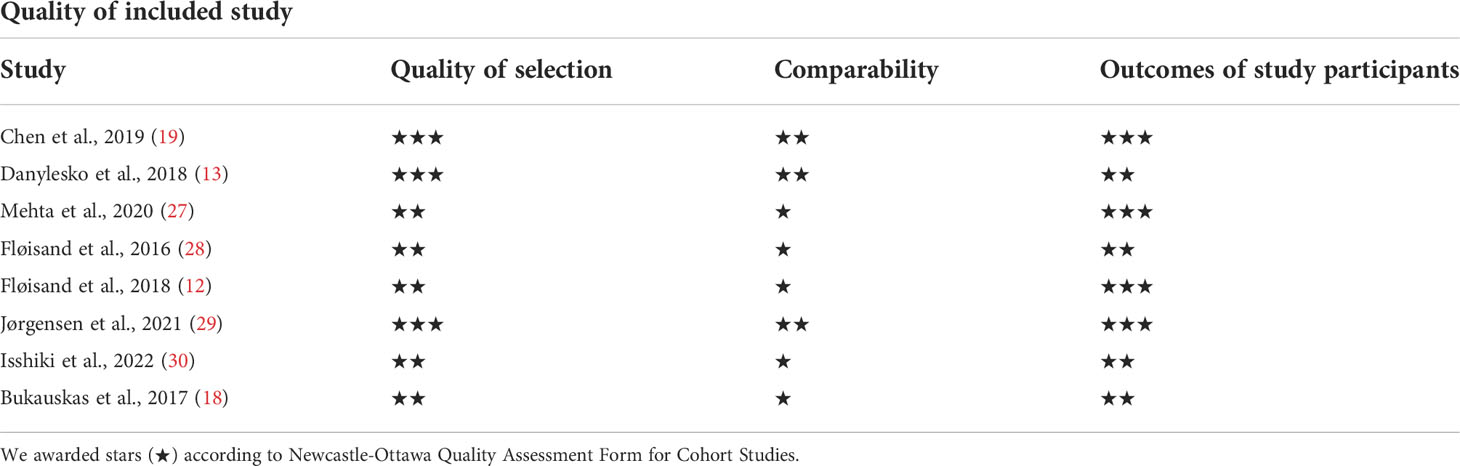
Table 2 Quality assessment of the included studies.
The pooled overall response to vedolizumab indicated significant overall response rate (ORR) at 14 days (pooled ORR = 60.53%, pooled risk ratio, RR =14.14, 95% CI: 2.95–67.71), 28 days (pooled ORR = 50.00%, pooled RR = 7.36, 95% CI: 2.14–25.37), and 12 months (pooled ORR = 76.92%, pooled RR = 13.66, 95% CI: 3.50–53.35) with low heterogeneity across studies (Tau-square = 0.00; I-square = 0%) (Figure 1).
Patients with GI-aGVHD showed a statistically significant complete response to vedolizumab at 12 months (pooled CRR = 27.27%, pooled RR = 5.50, 95% CI: 1.01–29.95) from baseline with low heterogeneity across studies (Tau-square = 0.00; I-square = 0%) (Figure 2). To the contrary, the pooled complete response at 14 days (pooled CRR = 16.67%, pooled RR = 5.00, 95% CI: 0.34–74.52) and at 28 days (pooled CRR = 17.24%, pooled RR = 4.24, 95% CI: 0.80–22.55) did not reach statistical significance (Figure 2). Collectively, these findings demonstrate possible long-term benefits of vedolizumab for patients with persistent GI-GVHD.
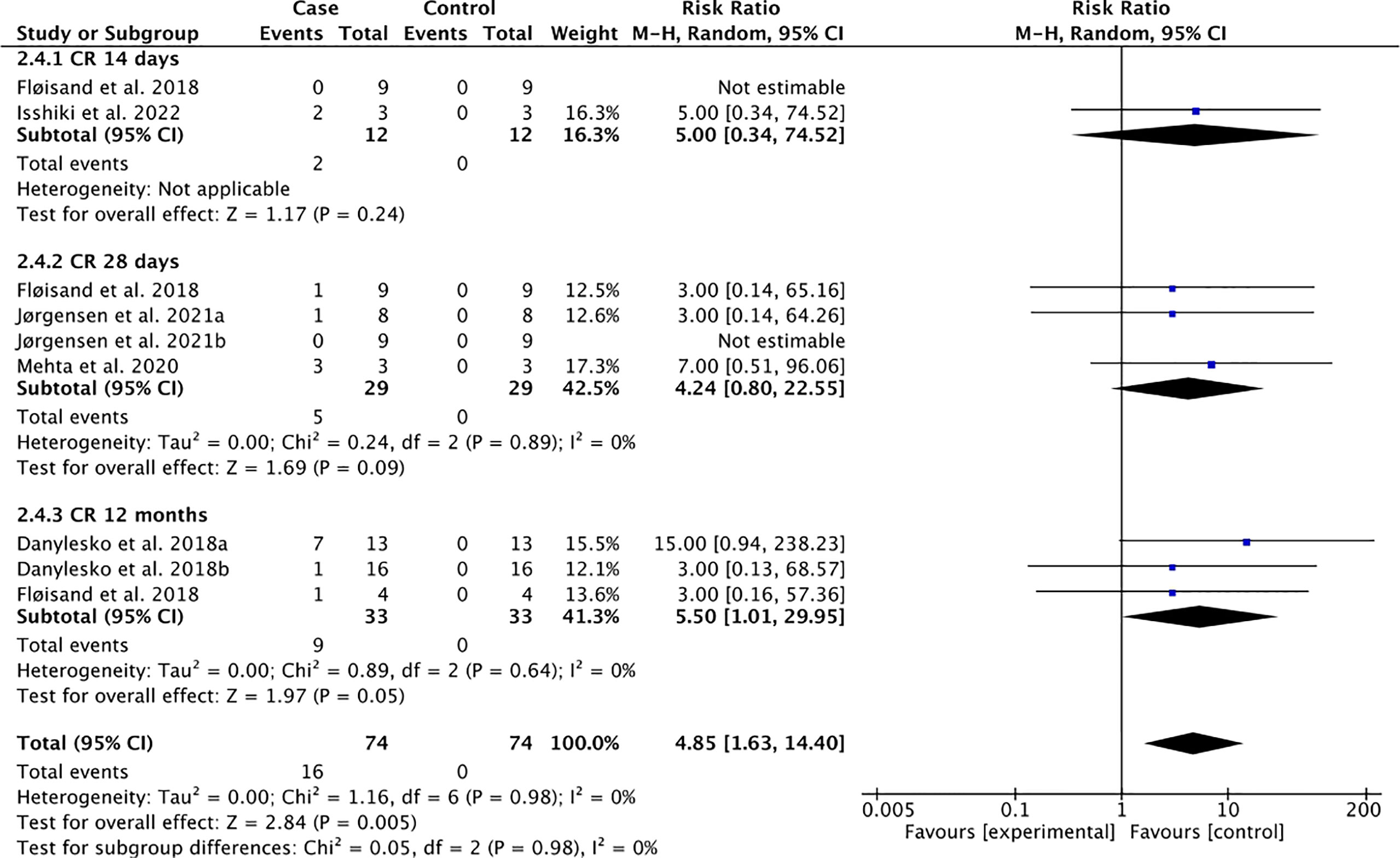
Figure 2 Complete response (CR) following the use of vedolizumab for GI-aGVHD.
The pooled mortality rate at 6 months (65.51%) and 12 months (70.76%) were derived from seven studies of 87 patients and six studies of 89 patients, respectively, with low heterogeneity (Tau-square = 0.00; I-square = 0%) (Figure 3).
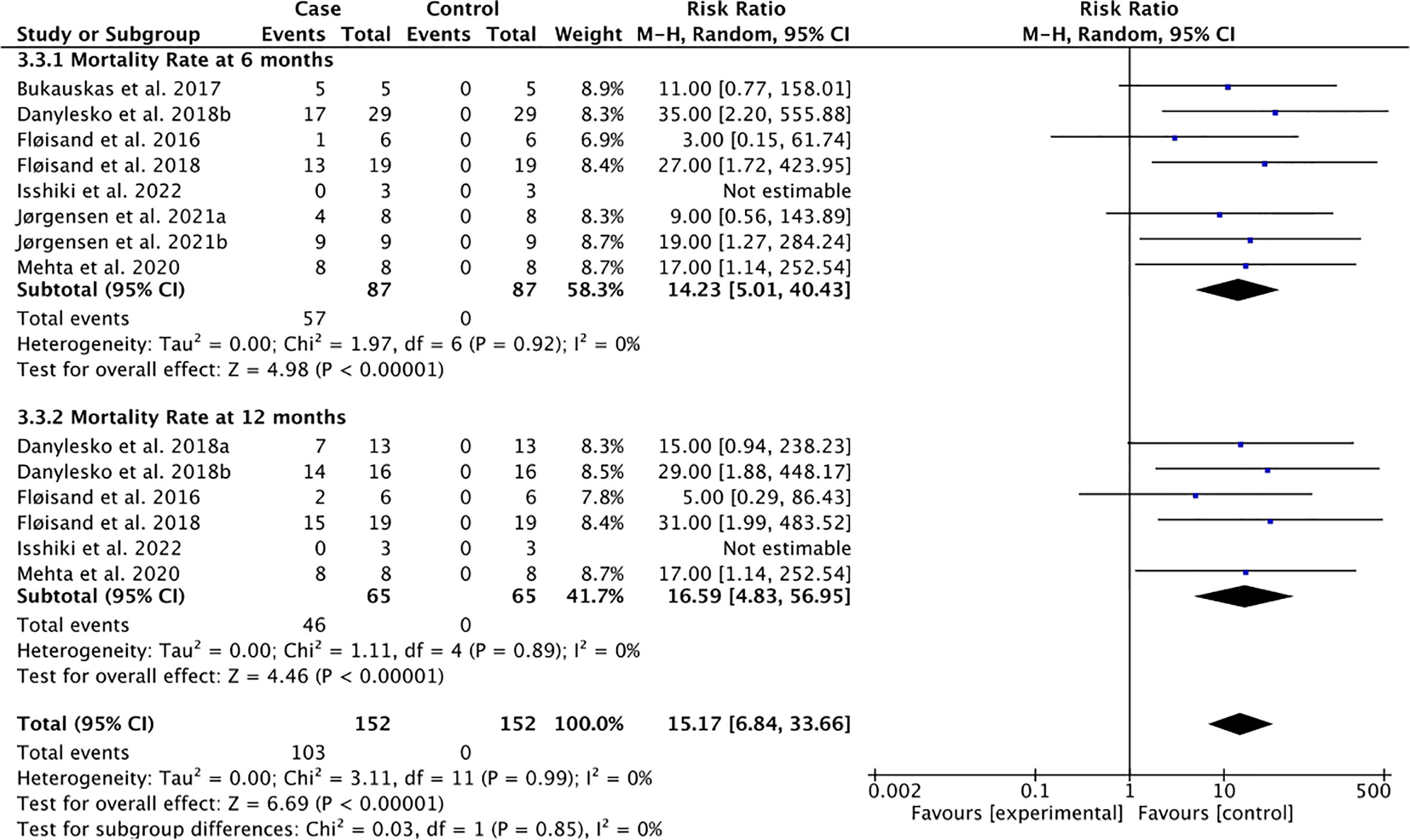
Figure 3 Mortality rate following the use of vedolizumab for GI-aGVHD.
There were five studies (13, 19, 28–30) that recorded patients’ causes of death. The deaths were attributed to sepsis (n = 10), aGVHD (n = 7), the relapse of underlying diseases (n = 5), failure (n = 2), peritonitis (n = 1), thrombotic microangiopathy (n = 1), and mediastinitis (n = 1).
Pooled risks for adverse events including blood and lymphatic, renal and urinary, GI tract, nervous, musculoskeletal, hepatic, infectious, respiratory and thoracic, metabolic and nutritional, and cutaneous adverse events following prophylactic use of vedolizumab (Figure 4) and vedolizumab treatment for GI-aGVHD (Figure 5) were estimated in a total of 24 patients and 114 patients across studies, respectively. The risk of adverse events following prophylactic use of vedolizumab did not reach statistical significance (Figure 4), suggesting the safety of vedolizumab for the prevention of GI-aGVHD in patients undergoing HSCT. Despite the non-significant risk of most adverse events, the pooled risks for infections (pooled rate = 22.22% of 81 included participants, pooled RR = 7.55, 95% CI: 2.11–27.05) and metabolic and nutritional side effects (pooled rate = 47.06% of 17 included participants, pooled RR = 9.00, 95% CI: 1.26–64.24) were observed following the use of vedolizumab in patients with GI-aGVHD (Figure 5).
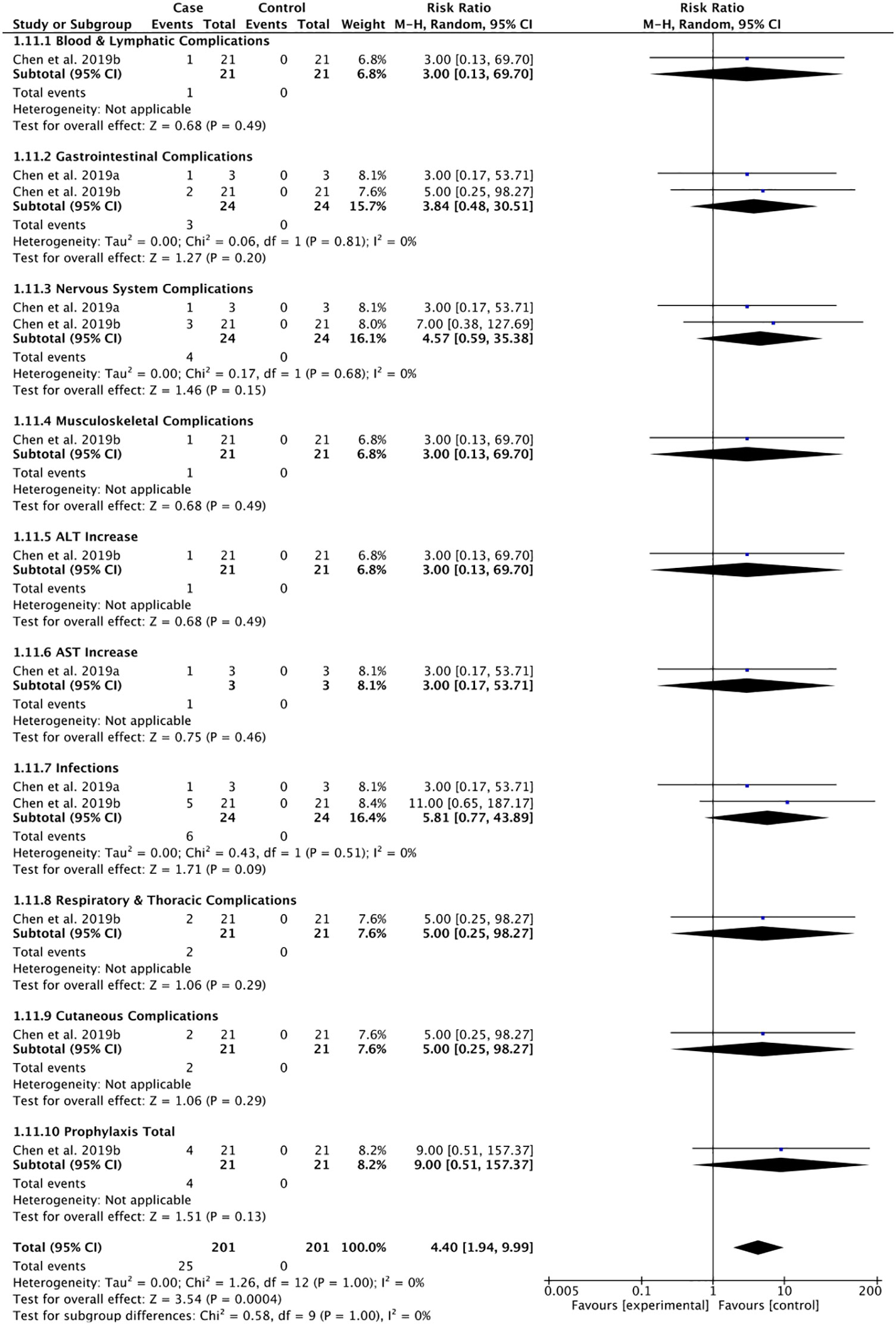
Figure 4 Adverse events following the use of vedolizumab to prevent GI-aGVHD.
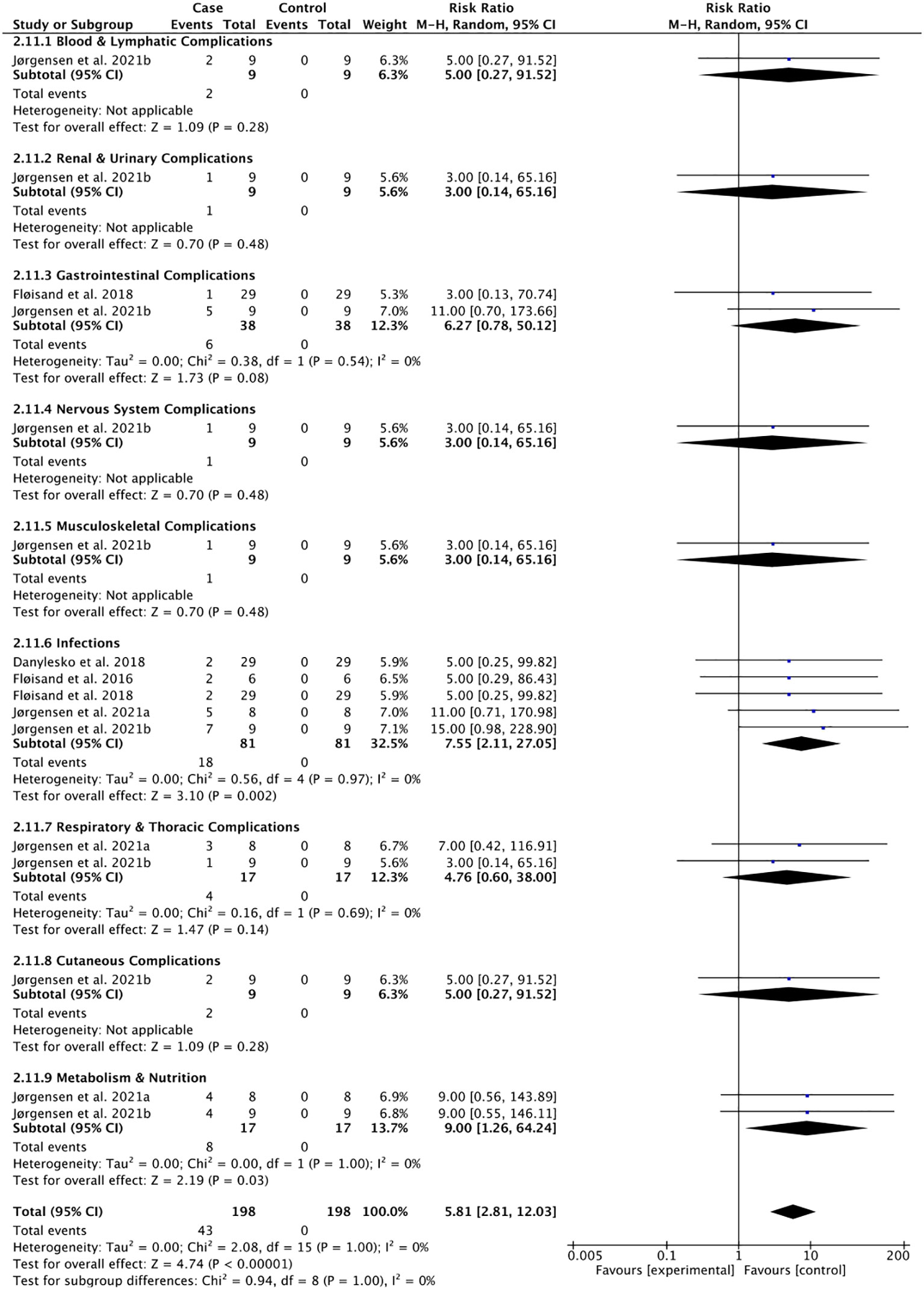
Figure 5 Adverse events following the use of vedolizumab to treat GI-aGVHD.
In reports of infections following the use of vedolizumab, one study (30) specified the numbers of each type of bacterial infections in patients with GI-aGVHD, with frequent pathogenic infections including Enterococcus (11.7%), Escherichia (11.1%), Citrobacter (11.11%), and cytomegalovirus (7.7%) infections. On the other hand, one study reported Staphylococcus infections in patients with GI-aGVHD (29). Stratifying the infected sites by organs (19, 30), it was pinpointed that the most common infections in patients with aGVHD were mediastinitis (11.1%), peritonitis (11.11%), pneumonia (6.8%), bronchitis (4.76%), cellulitis (4.76%), and mucosal infection (4.76%). Lastly, five out of 52 patients (9.6%) from three studies experienced sepsis (12, 29, 30). All in all, the risk of all treatment-related adverse events except infectious, metabolic, and nutritional complications following the use of vedolizumab in patients with GI-aGVHD did not reach statistical significance, providing the safety profile of vedolizumab for the treatment of GI-aGVHD.
The present study was the first systematic review and meta-analysis that assessed the safety and efficacy of vedolizumab for the prevention and the of GI-aGVHD. Results of clinical studies were comprehensively identified, evaluated, and summarized to determine the pooled efficacy of vedolizumab as an effective prophylaxis or therapeutic approach to GI-aGVHD. Despite experiencing adverse events including infections and metabolic or nutritional complications, patients on vedolizumab for the treatment of GI-aGVHD had significant overall response and complete response from baseline. While no significant adverse events were reported following prophylactic use of vedolizumab, more studies were warranted to reach a conclusive statement for its overall response rate and complete response rate and to address whether vedolizumab can be used for the standard prophylaxis of GI-aGVHD in patients undergoing allogenic HSCT.
As for the efficacy of vedolizumab for the treatment of GI-aGVHD, findings of the present meta-analysis demonstrated that the pooled overall response rate at 14 days, 28 days, and 12 months and pooled complete response at 12 months from baseline were evident, in which 70% of patients achieved an overall response on 12 months after first dose of vedolizumab. This finding was consistent with that reported by Coltoff et al. (28). In our findings, owing to the generally poor prognosis at baseline of GI-aGVHD, many patients on vedolizumab died in the first month of follow-up, while a remarkable clinical response was evident in patients who survived passing that time point. Furthermore, compared to the scenario in which vedolizumab was used as later-line treatments (13, 30), early administration of vedolizumab following steroid failure exerted a faster response and better overall response rate. Application of multiple immunosuppressive agents prior to the use of vedolizumab could result in microbiome imbalance, leading to unsatisfied prognosis following the use of later-line medications (32). At the same time, patients who used vedolizumab earlier were less likely to be immunosuppressed and develop subsequent infections (12, 13, 28). On the contrary, a few studies suggested poor overall outcomes following vedolizumab treatments in advanced aGVHD (13, 18, 30), which was explained by theories conjecturing that α4β7 integrins were no longer needed for the propagation of aGVHD after tissue injury and systemic injury occurred (13). In such theories, it was proposed that α4β7–MAdCAM-1 interactions were mainly involved in the early recruitment of T cells to the intestinal stem cell compartment (33). It warrants further studies to elucidate whether the expression of the α4β7 integrins can be a prognostic biomarker for GI-aGVHD and may be used to guide the use of vedolizumab in gastrointestinal inflammatory complications associated with GVHD. Another potential parameter for the early detection of GI-aGVHD is the calprotectin fecal level. Following the activation of leukocytes, calprotectin is released. Hence, the level of calprotectin is positively correlated to bowel inflammation. Moreover, it retains high stability and concentration under room temperature in feces, making it a reliable biomarker for GI inflammation detection aGVHD (34).
When it comes to whether vedolizumab can prevent GI-aGVHD in patients undergoing HSCT, there was one included clinical trial that addressed low risk of infection and no impairment of the graft-versus-tumor effect following the prophylactic use of vedolizumab (19). In particular, it was demonstrated that 300 mg intravenous vedolizumab in conjunction with tacrolimus and methotrexate (MTX) was well tolerated by adult patients who had undergone HSCT, among which only 12.5% of the participants receiving vedolizumab experienced lower-intestinal aGVHD and no dose-limiting toxicity was observed (19). Although there was limited evidence that supported vedolizumab as a standard prophylactic pharmacologic therapy for GVHD, the promising results of this study (19) enlightened the need for future studies that may ascertain the efficacy of prophylactic use of vedolizumab in patients receiving HSCT.
The present study provided the pooled safety profile of vedolizumab for the prophylaxis and treatment of GI-aGVHD, in which infections or metabolic and nutritional adverse events following vedolizumab as the second-line or above treatments were observed. This was in accordance with findings in a previous review that reported upper airway infections, nausea, and fatigue in over 2,000 patients on vedolizumab (35). Although it was suggested that theimmune suppressing effect of vedolizumab was local and was limited in the GI tract, which may not diminish immune responses to parenteral administered antigens (13, 36), still treatment-related infections were reported following the use of vedolizumab across studies. Nonetheless, the pooled rate of infections following vedolizumab treatment was lower than that following other systemic therapies. Compared with an infection rate of 59.09% following daclizumab and infliximab injection for GI-aGVHD (11), and an infection rate of 24% following the use of ruxolitinib for the treatment of GI-aGVHD (9), the present meta-analysis suggested a comparatively low pooled infection rate of 22% following vedolizumab treatment for GI-aGVHD. Furthermore, safety profiles in five out of eight included studies (12, 13, 19, 29, 30) specified the incidence of cytomegalovirus (CMV) infection following vedolizumab treatments. The mechanism of which may involve the preexisting inflammatory microenvironment in the bowel of patients with GI-aGVHD. To elaborate, CMV was dormant after its initial infection in most organs including the colon, while it can be reactivated upon inflammation or immunosuppression in the microenvironment (37, 38), for which the association between IBD and CMV infection had been suggested per extensively secreted proinflammatory cytokines in the bowel that caused the reactivation of CMV infection (39). Due to the shared immune-related pathogenesis between GI-aGVHD and IBD (14, 15, 40, 41), it was possible that CMV infections following vedolizumab treatments were attributed to the preexisting but not treatment-induced inflammatory microenvironment in GI-aGVHD.
Compared with a previous phase II trial which reported a 22±7% rate of developing aGVHD (grade II to IV) following the prophylactic use of CCR5 antagonists at 90 days after HSCT (42), the present meta-analysis showed a lower incidence of aGVHD (grade II to III) following the prophylactic use of vedolizumab (19.2%), with no participant experiencing grade IV aGVHD during the 6-month follow-up. Compared with the previously reported 12-month survival of 25% and 77% of overall response rate of 77% following pentostatin treatment in 12 patients with grade IV aGVHD (pooled rate = 60%) and eight patients with grade III aGVHD (pooled rate = 40%) (43), and another study demonstrating 12-month survival of 38% and overall response rate of 67% following the use of daclizumab and infliximab in 18 patients with grade IV aGVHD (pooled rate = 72%) and 7 patients with grade III aGVHD (pooled rate=28%) of grade III aGVHD (11), the present meta-analysis suggested a pooled 12-month overall survival of 29.23% and a pooled overall response rate of 76.92% following vedolizumab treatment in patients with stage 3 (31.63%) or stage 4 (47.95%) GI-aGVHD, for which the advantages of vedolizumab over pentostatin, daclizumab, and infliximab for advanced grades aGVHD were indicated. On the contrary, a retrospective cohort study (44) on the overall survival of 79 patients with SR-aGVHD using anti-thymocyte globulin (ATG) reported an estimated 6-month overall survival rate of 44%, while another phase III randomized clinical trial (45) comparing ATG with inolimomab found a 12-month overall survival rate of approximately 45% in all patients with aGVHD. The relatively higher mortality in the present meta-analysis than that in those studies (44, 45) was due mainly to the fact that most patients in the present study were of stage 3 or stage 4 GI-aGVHD at baseline, for which the more advanced grades with multiorgan involvement contributed to the worse prognosis (46–48). Overall, findings in the present study suggested that most deaths occurred in the first 6 months during the course of vedolizumab treatment. Juxtaposing the mortality profile and safety profile of vedolizumab for the prophylaxis and treatment of GI-aGVHD provided in the present study, it was suggested that patients should be closely monitored in the first 6 months after starting vedolizumab to prevent and to timely manage potential concomitant infections and metabolic or nutritional adverse events including decreased appetite, electrolyte imbalance, and hypoglycemia.
Limitations of the present meta-analysis included a lack of unified definition of SR-aGVHD across studies, which resulted in different criteria for the initiation of vedolizumab treatment. Second, due to the limited quantity of existing studies, not only clinical trials but also real-world studies and case series were included in the meta-analysis, which might compromise the external validity of our estimation on the effect of vedolizumab. Third, due to the limited sample size of each study, underlying conditions of aGVHD such as the primary disease, conditioning regimen, the status of human leukocyte antigen (HLA) matching, and comorbidities were not matched in the included studies, with which the lack of information might result in residual confounding bias. That said, since the heterogeneity across studies through all analyses in the present study was low, it was inferred that all abovementioned potential biases were optimally controlled.
In summary, the use of vedolizumab was safe and effective in patients with GI-aGVHD, especially when administered earlier in the disease course of GI-aGVHD. Further studies are warranted to elucidate its efficacy for the prophylaxis of GI-aGVHD in patients undergoing HSCT.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
KSM and AA contribute to the conception and design of the study. ACWL, CD, and STT performed the literature search. ACWL and CD further completed the data screening and data extraction. ACWL analyzed the data and wrote the first draft of the manuscript. KSM created the tables and figures of this study. ACWL, CD, STT, AA, and KSM contributed to manuscript revision and read and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.1025350/full#supplementary-material
1. Reshef R, Porter DL. Reduced-intensity conditioned allogeneic SCT in adults with AML. Bone Marrow Transplant (2015) 50(6):759–69. doi: 10.1038/bmt.2015.7
2. Shen M-Z, Li J-X, Zhang X-H, Xu L-P, Wang Y, Liu K-Y, et al. Meta-analysis of interleukin-2 receptor antagonists as the treatment for steroid-refractory acute graft-Versus-Host disease. Front Immunol (2021) 12(3815). doi: 10.3389/fimmu.2021.749266
3. Storb R. Allogeneic hematopoietic stem cell transplantation–yesterday, today, and tomorrow. Exp Hematol (2003) 31(1):1–10. doi: 10.1016/S0301-472X(02)01020-2
4. Reddy P, Ferrara JLM. Mouse models of graft-versus-host disease. In: Pavan R, Ferrara JLM, editors. StemBook. Cambridge (MA: Harvard Stem Cell Institute (2008).
5. Zeiser R, Blazar BR. Acute graft-versus-Host disease - biologic process, prevention, and therapy. N Engl J Med (2017) 377(22):2167–79. doi: 10.3389/fimmu.2018.01087
6. Yu J, Parasuraman S, Shah A, Weisdorf D. Mortality, length of stay and costs associated with acute graft-versus-host disease during hospitalization for allogeneic hematopoietic stem cell transplantation. Curr Med Res Opin (2019) 35(6):983–8. doi: 10.1080/03007995.2018.1551193
7. Zhang L, Yu J, Wei W. Advance in targeted immunotherapy for graft-Versus-Host disease. Front Immunol (2018) 9:1087. doi: 10.1080/17474086.2020.1738214
8. Jagasia M, Arora M, Flowers M. E, N, Chao J, McCarthy PL, Cutler CS, et al. Risk factors for acute GVHD and survival after hematopoietic cell transplantation. Blood (2012) 119(1):296–307. doi: 10.1182/blood-2011-06-364265
9. Hui L, Qi L, Guoyu H, Xuliang S, Meiao T. Ruxolitinib for treatment of steroid-refractory graft-versus-host disease in adults: a systematic review and meta-analysis. Expert Rev Hematol (2020) 13(5):565–75. doi: 10.1038/bmt.2010.117
10. Zhang H, Chen R, Cheng J, Jin N, Chen B. Systematic review and meta-analysis of prospective studies for ECP treatment in patients with steroid-refractory acute GVHD. Patient Prefer Adherence (2015) 9:105–11. doi: 10.2147/PPA.S76563
11. Rager A, Frey N, Goldstein SC, Reshef R, Hexner EO, Loren A, et al. Inflammatory cytokine inhibition with combination daclizumab and infliximab for steroid-refractory acute GVHD. Bone Marrow Transplant (2011) 46(3):430–5. doi: 10.1038/s41409-018-0364-5
12. Fløisand Y, Lazarevic VL, Maertens J, Mattsson J, Shah NN, Zachée P, et al. Safety and effectiveness of vedolizumab in patients with steroid-refractory gastrointestinal acute graft-versus-Host disease: A retrospective record review. Biol Blood Marrow Transplant (2019) 25(4):720–7. doi: 10.1016/j.bbmt.2018.11.013
13. Danylesko I, Bukauskas A, Paulson M, Peceliunas V, Gedde-Dahl DYT, Shimoni A, et al. Anti-α4β7 integrin monoclonal antibody (vedolizumab) for the treatment of steroid-resistant severe intestinal acute graft-versus-host disease. Bone Marrow Transplant (2019) 54(7):987–93. doi: 10.1038/nrgastro.2016.208
14. Attauabi M, Madsen G.R, Bendtsen F, Seidelin JB, Burisch J. Vedolizumab as the first line of biologic therapy for ulcerative colitis and Crohn's disease - a systematic review with meta-analysis. Dig Liver Dis. 2022 54(9):1168–78. doi: 10.1016/j.dld.2021.11.014
15. Neurath MF. Current and emerging therapeutic targets for IBD. Nat Rev Gastroenterol Hepatol (2017) 14(5):269–78. doi: 10.1182/blood-2003-03-0957
16. Dutt S, Ermann J, Tseng D, Liu YP, George TI, Fathman C. G, et al. L-selectin and beta7 integrin on donor CD4 T cells are required for the early migration to host mesenteric lymph nodes and acute colitis of graft-versus-host disease. Blood (2005) 106(12):4009–15. doi: 10.1016/j.bbmt.2017.05.028
17. Petrovic A, Alpdogan O, Willis LM, Eng JM, Greenberg AS, Kappel BJ, et al. LPAM (alpha 4 beta 7 integrin) is an important homing integrin on alloreactive T cells in the development of intestinal graft-versus-host disease. Blood (2004) 103(4):1542–7. doi: 10.1182/blood-2003-03-0957
18. Bukauskas A, Griskevicius L, Peceliunas V. Lessons learned from early experiences with vedolizumab for steroid-refractory acute graft- versus-host disease with gastrointestinal involvement. Biol Blood Marrow Transplant (2017) 23(9):1597. doi: 10.1016/j.ijsu.2010.02.007
19. Chen YB, Shah NN, Renteria AS, Cutler C, Jansson J, Akbari M, et al. Vedolizumab for prevention of graft-versus-host disease after allogeneic hematopoietic stem cell transplantation. Blood Adv (2019) 3(23):4136–46. doi: 10.1182/bloodadvances.2019000893
20. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg (2010) 8(5):336–41. doi: 10.1016/j.bbmt.2009.03.012
21. Socié G, Vigouroux S, Yakoub-Agha I, Bay JO, Fürst S, Bilger K, et al. A phase 3 randomized trial comparing inolimomab vs usual care in steroid-resistant acute GVHD. Blood (2017) 129(5):643–9. doi: 10.1053/bbmt.2002.v8.pm12171485
22. Holtan SG, Pasquini M, Weisdorf DJ. Acute graft-versus-host disease: a bench-to-bedside update. Blood (2014) 124(3):363–73. doi: 10.1038/bmt.2014.69
23. MacMillan ML, Weisdorf DJ, Wagner JE, DeFor TE, Burns LJ, Ramsay NK, et al. Response of 443 patients to steroids as primary therapy for acute graft-versus-host disease: comparison of grading systems. Biol Blood Marrow Transplant (2002) 8(7):387–94. doi: 10.1056/NEJMra1609337
24. Castilla-Llorente C, Martin PJ, McDonald GB, Storer BE, Appelbaum FR, Deeg HJ, et al. Prognostic factors and outcomes of severe gastrointestinal GVHD after allogeneic hematopoietic cell transplantation. Bone Marrow Transplant (2014) 49(7):966–71. doi: 10.1038/bmt.2014.69
25. Lee IT, Shen CH, Tsai FC, Chen CB, Ma KS. Cancer-Derived Extracellular Vesicles as Biomarkers for Cutaneous Squamous Cell Carcinoma: A Systematic Review. Cancers (Basel). (2022) 14(20):5098. doi: 10.3390/cancers14205098
26. Ma KS, Lee CC, Liu KJ, Wei JC, Lee YT, Wang LT. Safety and Seroconversion of Immunotherapies against SARS-CoV-2 Infection: A Systematic Review and Meta-Analysis of Clinical Trials. Pathogens. (2021) 10(12):1537. doi: 10.3390/pathogens10121537
27. Ma KS, Wang LT, Blatz MB. Efficacy of Adhesive Strategies for Restorative Dentistry: A Systematic Review and Network Meta-analysis of Double-blind Randomized Controlled Trials Over 12 Months of Follow-up. J Prosthodont Res.( 2022). doi: 10.2186/jpr.JPR_D_21_00279
28. Chiang CH, Tang PU, Lee GH, Chiang TH, Chiang CH, Ma KS, et al. Prevalence of Nontuberculous Mycobacterium Infections versus Tuberculosis among Autopsied HIV Patients in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Am J Trop Med Hyg. (2020) 104(2):628–33. doi: 10.4269/ajtmh.20-0973
29. Wells GA, Wells G, Shea B, Shea B, O'Connell D, Peterson J, et al. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Environ. Sci. (2014).
30. Martin PJ, Bachier C.R, Klingemann HG, McCarthy PL, Szabolcs P, Uberti JP, et al. Endpoints for clinical trials testing treatment of acute graft-versus-host disease: A joint statement. Biol Blood Marrow Transplant (2009) 15(7):777–84. doi: 10.1038/s41409-018-0094-8
31. Glucksberg H, Storb R, Fefer A, Buckner CD, Neiman PE, Clift RA, et al. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-a-matched sibling donors. Transplantation (1974) 18(4):295–304. doi: 10.1016/j.bbmt.2016.10.009
32. Coltoff A, Lancman G, Kim S, Steinberg A. Vedolizumab for treatment of steroid-refractory lower gastrointestinal acute graft-versus-host disease. Bone Marrow Transplant (2018) 53(7):900–4.
33. Fløisand Y, Lundin KEA, Lazarevic V, Kristiansen JD, Osnes LTN, Tjønnfjord GE, et al. Targeting integrin α4β7 in steroid-refractory intestinal graft-versus-Host disease. Biol Blood Marrow Transplant (2017) 23(1):172–5. doi: 10.1007/s12185-021-03245-0
34. Fløisand Y, Schroeder MA, Chevallier P, Selleslag D, Devine S, Renteria AS, et al. A phase 2a randomized clinical trial of intravenous vedolizumab for the treatment of steroid-refractory intestinal acute graft-versus-host disease. Bone Marrow Transplant (2021) 56(10):2477–88. doi: 10.1038/s41409-021-01356-0
35. Isshiki K, Kamiya T, Endo A, Okamoto K, Osumi T, Kawai T, et al. Vedolizumab therapy for pediatric steroid-refractory gastrointestinal acute graft-versus-host disease. Int J Hematol (2021) 115:590–4. doi: 10.1007/s12185-021-03245-0
36. Bull MJ, Plummer NT. Part 1: The human gut microbiome in health and disease. Integr Med (Encinitas) (2014) 13(6):17–22. doi: 10.3892/br.2016.751
37. Fu YY, Egorova A, Sobieski C, Kuttiyara J, Calafiore M, Takashima S, et al. T Cell recruitment to the intestinal stem cell compartment drives immune-mediated intestinal damage after allogeneic transplantation. Immunity (2019) 51(1):90–103.e3. doi: 10.1111/apt.16060
38. Chatzikonstantinou M, Konstantopoulos P, Stergiopoulos S, Kontzoglou K, Verikokos C, Perrea D, et al. Calprotectin as a diagnostic tool for inflammatory bowel diseases. BioMed Rep (2016) 5(4):403–7. doi: 10.1016/S0140-6736(09)60237-3
39. Loftus EV Jr., Feagan BG, Panaccione R, Colombel J-F, Sandborn WJ, Sands BE, et al. Long-term safety of vedolizumab for inflammatory bowel disease. Alimentary Pharmacol Ther (2020) 52(8):1353–65. doi: 10.1007/s11894-012-0266-4
40. Ferrara JL, Levine JE, Reddy P, Holler E. Graft-versus-host disease. Lancet (2009) 373(9674):1550–61. doi: 10.3748/wjg.v22.i6.2030
41. You DM, Johnson MD. Cytomegalovirus infection and the gastrointestinal tract. Curr Gastroenterol Rep (2012) 14(4):334–42. doi: 10.1016/S2468-1253(16)30159-5
42. Pillet S, Pozzetto B, Roblin X. Cytomegalovirus and ulcerative colitis: Place of antiviral therapy. World J Gastroenterol (2016) 22(6):2030–45. doi: 10.1016/j.bbmt.2009.05.003
43. Siegmund B. Cytomegalovirus infection associated with inflammatory bowel disease. Lancet Gastroenterol Hepatol (2017) 2(5):369–76.
44. Chen Y-B, Kim HT, McDonough S, Odze RD, Yao X, Lazo-Kallanian S, et al. Up-regulation of alpha4beta7 integrin on peripheral T cell subsets correlates with the development of acute intestinal graft-versus-host disease following allogeneic stem cell transplantation. Biol Blood marrow Transplant J Am Soc Blood Marrow Transplant (2009) 15(9):1066–76. doi: 10.1016/j.bbmt.2018.09.034
45. Ueha S, Murai M, Yoneyama H, Kitabatake M, Imai T, Shimaoka T, et al. Intervention of MAdCAM-1 or fractalkine alleviates graft-versus-host reaction associated intestinal injury while preserving graft-versus-tumor effects. J Leukoc Biol (2007) 81(1):176–85. doi: 10.1189/jlb.0306231
46. Reshef R, Ganetsky A, Acosta EP, Blauser R, Crisalli L, McGraw J, et al, et al. Extended CCR5 blockade for graft-versus-Host disease prophylaxis improves outcomes of reduced-intensity unrelated donor hematopoietic cell transplantation: A phase II clinical trial. Biol Blood Marrow Transplant (2019) 25(3):515–21. doi: 10.1038/bmt.2010.146
47. Pidala J, Kim J, Roman-Diaz J, Shapiro J, Nishihori T, Bookout R, et al. Pentostatin as rescue therapy for glucocorticoid-refractory acute and chronic graft-versus-host disease. Ann Transplant (2010) 15(4):21–9. doi: 10.1182/blood-2016-09-738625
Keywords: vedolizumab, graft-versus-host disease, biologics, alpha-4-beta-7 integrins, acute GVHD
Citation: Li AC-W, Dong C, Tay S-T, Ananthakrishnan A and Ma KS-K (2022) Vedolizumab for acute gastrointestinal graft-versus-host disease: A systematic review and meta-analysis. Front. Immunol. 13:1025350. doi: 10.3389/fimmu.2022.1025350
Received: 22 August 2022; Accepted: 26 September 2022;
Published: 11 November 2022.
Edited by:
Liangding Hu, Fifth Medical Center of the PLA General Hospital, ChinaReviewed by:
Jan Styczynski, Nicolaus Copernicus University in Toruń, PolandCopyright © 2022 Li, Dong, Tay, Ananthakrishnan and Ma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ashwin Ananthakrishnan, YWFuYW50aGFrcmlzaG5hbkBtZ2guaGFydmFyZC5lZHU=; Kevin Sheng-Kai Ma, a2V2aW5zaGVuZ2thaW1hQGcuaGFydmFyZC5lZHU=
†These authors have contributed equally to this work
‡ORCID: Kevin Sheng-Kai Ma, orcid.org/0000-0002-9394-4144
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.