
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 14 December 2021
Sec. Alloimmunity and Transplantation
Volume 12 - 2021 | https://doi.org/10.3389/fimmu.2021.771449
 Chrysanthi Tsamadou1,2†Daphne Engelhardt2,3†Uwe Platzbecker4Elisa Sala5Thomas Valerius6Eva Wagner-Drouet7Gerald Wulf8Nicolaus Kröger9Niels Murawski10Hermann Einsele11Kerstin Schaefer-Eckart12Sebastian Freitag13Jochen Casper14Martin Kaufmann15Mareike Dürholt16Bernd Hertenstein17Stefan Klein18Mark Ringhoffer19Sandra Frank20Christine Neuchel1,2Hubert Schrezenmeier1,2Joannis Mytilineos20,21Daniel Fuerst1,2*
Chrysanthi Tsamadou1,2†Daphne Engelhardt2,3†Uwe Platzbecker4Elisa Sala5Thomas Valerius6Eva Wagner-Drouet7Gerald Wulf8Nicolaus Kröger9Niels Murawski10Hermann Einsele11Kerstin Schaefer-Eckart12Sebastian Freitag13Jochen Casper14Martin Kaufmann15Mareike Dürholt16Bernd Hertenstein17Stefan Klein18Mark Ringhoffer19Sandra Frank20Christine Neuchel1,2Hubert Schrezenmeier1,2Joannis Mytilineos20,21Daniel Fuerst1,2*The HLA-DRB3/4/5 loci are closely linked to the HLA-DRB1 gene. Mismatches in these loci occur with a frequency of about 8%–12% in otherwise 10/10 HLA-matched transplant pairs. There is preliminary evidence that these disparities may associate with increased acute graft-versus-host disease (GvHD) rates. The aim of this study was to analyze a large cohort of German patients and their donors for HLA-DRB3/4/5 compatibility and to correlate the HLA-DRB3/4/5 matching status with the outcome of unrelated hematopoietic stem cell transplantation (uHSCT). To this end, 3,410 patients and their respective donors were HLA-DRB3/4/5 and HLA-DPB1 typed by amplicon-based next-generation sequencing (NGS). All patients included received their first allogeneic transplant for malignant hematologic diseases between 2000 and 2014. Mismatches in the antigen recognition domain (ARD) of HLA-DRB3/4/5 genes were correlated with clinical outcome. HLA-DRB3/4/5 incompatibility was seen in 12.5% (n = 296) and 17.8% (n = 185) of the 10/10 and 9/10 HLA-matched cases, respectively. HLA-DRB3/4/5 mismatches in the ARD associated with a worse overall survival (OS), as shown in univariate (5-year OS: 46.1% vs. 39.8%, log-rank p = 0.038) and multivariate analyses [hazard ratio (HR) 1.25, 95% CI 1.02–1.54, p = 0.034] in the otherwise 10/10 HLA-matched subgroup. The worse outcome was mainly driven by a significantly higher non-relapse mortality (HR 1.35, 95% CI 1.05–1.73, p = 0.017). In the 9/10 HLA-matched cases, the effect was not statistically significant. Our study results suggest that mismatches within the ARD of HLA-DRB3/4/5 genes significantly impact the outcome of otherwise fully matched uHSCT and support their consideration upon donor selection in the future.
HLA-DRB3/4/5 genes are closely linked to the HLA-DRB1 locus (1). They exhibit a strong linkage disequilibrium in often conserved HLA-class II haplotypes (2). Within such haplotypes, the HLA-DRB1 antigen determines the presence or absence of an HLA-DRB3/4/5 gene. The three loci HLA-DRB3, HLA-DRB4, and HLA-DRB5 show a lower expression as compared to HLA-DRB1 but are still detectable by serological methods on account of which they are designated as HLA-DR52, -DR53, and -DR51 antigens, respectively (3). The HLA-DR51 (i.e., DRB5*) antigen is commonly present when HLA-DRB1*15 or -DRB1*16 alleles are also present. The HLA-DR52 (i.e., DRB3*) antigen is linked to HLA-DRB1*03, *11, *12, *13, and *14 alleles, while the HLA-DR53 (i.e., DRB4*) antigen is found together with HLA-DRB1*04, *07, and *09. Generally, alleles from the HLA-DRB1*01, *08, and *10 antigen groups do not associate with any of the HLA-DRB3/4/5 genes (4). Additionally, non-expressed alleles are quite frequent within the HLA-DRB3/4/5 genes, particularly HLA-DRB4*01:03:01:02N, which is the most frequent HLA-null allele recognized with an overall allele frequency of about 3.5% (5, 6). Despite the strong linkage disequilibrium, unusual HLA-DRB1-DRB3/4/5 associations do occur, leading to unexpected absence or presence of an HLA-DR52/53/51 antigen. This is sometimes observed in HLA-DRB1*01 that occasionally associates with HLA-DRB5 (7). In addition, HLA-DRB3/4/5 typing can be challenging due to the presence of unusual associations and non-expressed variants caused by polymorphisms in non-coding regions (e.g., HLA-DRB4*01:03:01:02N or HLA-DRB4*01:14N) (8, 9).
Due to the strong linkage between HLA-DRB1 and HLA-DRB3/4/5, mismatches at the HLA-DRB3/4/5 loci have been reported in only a fraction of transplant pairs (10, 11) with frequencies between 9.5% and 12.8% in different retrospective cohorts (10–12). The relevance of HLA-DRB3/4/5 discrepancies on outcome of uHSCT is still controversial. Some case studies showed that severe graft-versus-host disease (GvHD) may be induced by mismatches in these genes, while others speculated that the lower level of expression precludes any significant effects (12, 13). That said, preliminary cohort studies suggest that HLA-DRB3/4/5 differences do associate with increased mortality and GvHD events. There is evidence that factors beyond expression may influence alloreactivity such as, for instance, the cumulative number of mismatches and/or the direction of mismatches (i.e., antigen missing in donor or recipient or bidirectional if different allotypes in patient and donor are present (12, 14).
In order to investigate the potential role of HLA-DRB3/4/5 differences in GvHD incidence and mortality after uHSCT, we retrospectively analyzed a large cohort of German transplant pairs for differences within the antigen recognition domain (ARD) (exon 2) and/or exon 3 of HLA-DRB4 genes and correlated these mismatches with outcome.
This study included a total of 3,410 patients who underwent first allo-HSCT between 2000 and 2014 for malignant hematological diseases (i.e., acute and chronic leukemia, Myelodysplastic syndrome (MDS), Non-Hodgkin Lymphoma (NHL), and myeloma) with peripheral blood stem cells (PBSCs) or bone marrow (BM) from an unrelated donor at German transplant centers. Stem cell donor searches for cooperating transplant centers were conducted by the search unit in Ulm.
Clinical data were obtained from the German registry for stem cell transplantation (DRST) that is a subset of the EBMT ProMISe database for German patients. Treatment decisions and follow-up information from day 0, day 100, and yearly afterward were collected by the cooperating transplant centers based on EBMT surveys (MED-AB-Survey). Missing data in the EBMT files were retrieved directly from the centers when possible.
In the stem cell donor search setting, high-resolution HLA typing of the classical HLA gene loci HLA-A, -B, -C, -DRB-1, and -DQB1 had already been performed up front in the tissue typing laboratory of the search unit in Ulm. Retrospective typing for HLA-DPB1 and HLA-DRB3/4/5 loci was performed using an in-house-developed CE-certified next-generation sequencing (NGS)-amplicon sequencing protocol based on the Illumina MiSeq platform (San Diego, CA, USA) (15) in both patients and donors (n = 6,820). Matching status between donor and patient was defined by the identity of the protein sequence in the ARD, which is determined by exon 2 sequences for these loci (16). Additionally, differences in HLA-DRB4 exon 3 were determined and evaluated separately in this analysis.
Definition of the disease status prior to transplantation was classified according to definitions previously used by the EBMT study group (17). Myeloablative conditioning (MAC) was classified according to the EBMT MED-AB manual Appendix III and published consensus suggestions and compared to less intense regimen termed reduced-intensity conditioning (RIC) (18). The primary endpoints for the analysis in this study were defined according to the EBMT statistical recommendations (19). Overall survival (OS) was defined as the time from stem cell transplantation to death or last follow-up. Disease-free survival (DFS) was defined as the time to relapse or death from any cause or last follow-up. GvHD and relapse-free survival (GRFS) was defined as the time from the transplantation to the development of acute GvHD (aGvHD), relapse, or death, whichever occurred first. Non-relapse mortality (NRM) was defined as the time from transplantation until any cause of death without previous relapse, with disease relapse serving as a competing risk. Acute GvHD incidence was defined as the time to first occurrence of aGvHD grades II–IV, with death from other causes and disease relapse constituting competing risks. Relapse incidence was defined as the time to the event of a relapse, with death from other causes as a competing risk.
Statistical analysis of patient characteristics was performed by chi-square test for categorical variables and Mann–Whitney U test for continuous variables. For univariate analysis, Kaplan–Meier analysis with log-rank testing was used. Cox proportional hazards regression models were used for multivariate analysis of the endpoints OS, DFS, and GRFS. For the endpoints NRM, aGvHD, chronic GvHD (cGvHD), and relapse, competing risk regression according to the Fine and Gray model was used (20). Models were stratified for diagnosis and included adjustments for a center effect. Models for the variables of interests were checked for interactions, and none was found. Significance level was set at p = 0.05.
This study is a retrospective analysis of the impact of HLA-DRB3/4/5 matching status between patient and donor on the outcome after uHSCT. The endpoints mentioned above were analyzed in the context of relevant clinical and immunobiological variables. All patients and donors provided consent for HLA typing. Consent for recording and scientific analysis of the clinical data was obtained prior to registration of patients in the EBMT ProMISe database. The study was approved by the ethical committee of the University of Ulm.
Patients’ characteristics with respect to overall HLA and HLA-DRB3/4/5 compatibility are summarized in Table 1. The distribution as to clinical predictors within the respective subgroups was balanced, with only mild differences observed for HLA-DPB1 matching status (p = 0.035 and 0.037 for the 10/10 and 9/10 HLA-matched cohorts, respectively). Median patient age for the whole cohort was 54 years, and acute myeloid leukemia (AML) was the most frequent diagnosis (n = 1,255, 36.8%). Disease status at the time of transplantation was for most of the patients either early stage (n = 1,343, 39.4%) or intermediate stage (n = 1,177, 34.5%). The majority of the patients received in vivo T-cell depletion consisting of anti-thymocyte globulin (ATG) or alemtuzumab (n = 2,273, 66.7%). MAC was performed in 62.2% of the patients (n = 2,122). In this cohort, 2,371 (69.5%) patients underwent a 10/10 HLA-matched transplantation, while 1,039 (30.5%) patients received a 9/10 HLA-matched transplant. Median follow-up time was 52 months.
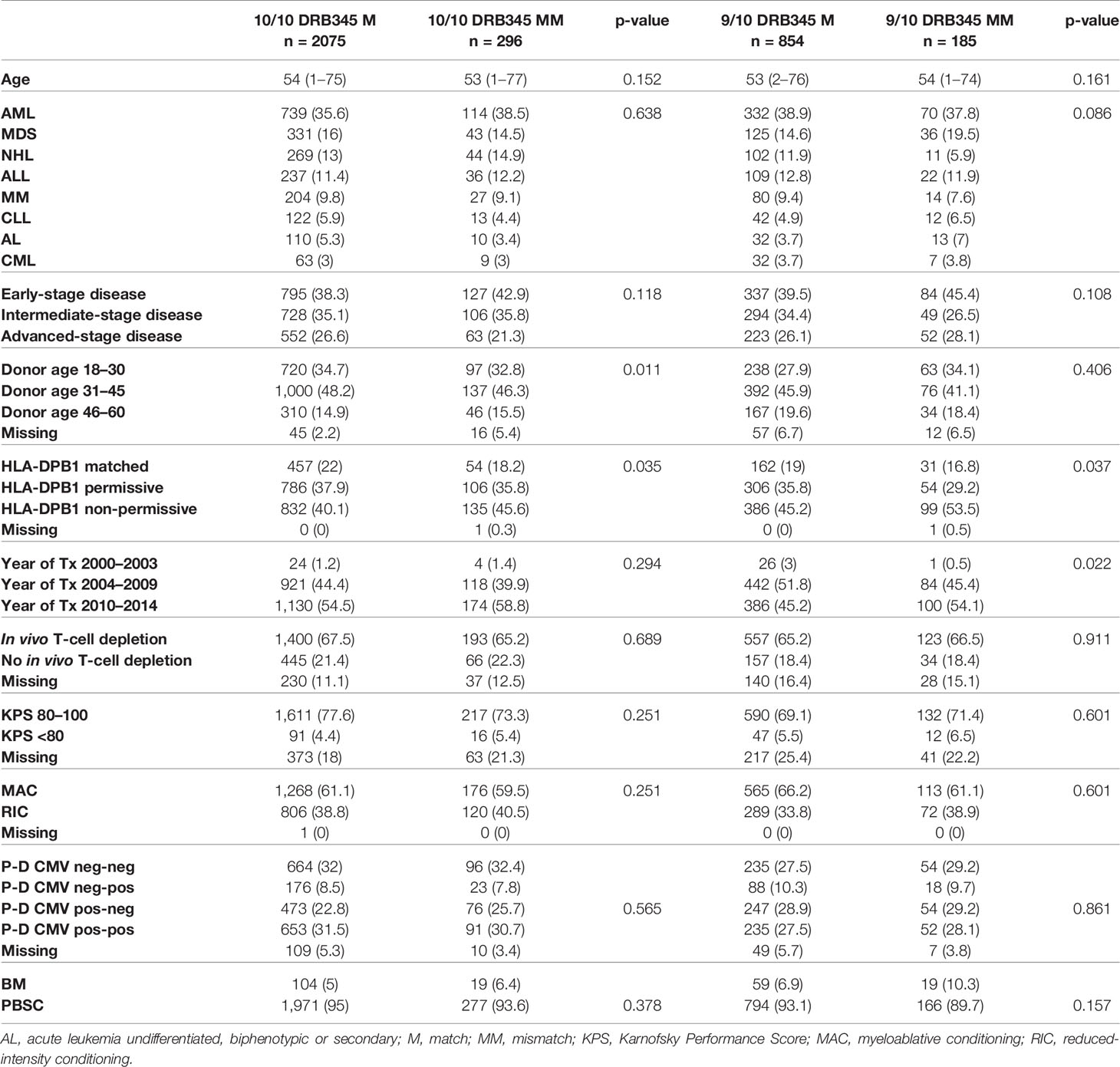
Table 1 Cohort characteristics.
Due to the diversity of HLA-class II haplotypes, different mismatch combinations had to be considered in the analyses. In 10/10 matched transplantations, 2,075 (87.5%) were HLA-DRB3/4/5 matched and 296 (12.5%) mismatched. A similar distribution was observed in the 9/10 group, with 854 (82.2%) HLA-DRB3/4/5 matched and 185 (17.8%) HLA-DRB3/4/5 mismatched transplantations. Identified HLA-DRB3/4/5 mismatches occurred within the ARD of HLA-DRB3/4/5 and/or HLA-DRB4 exon 3. Current consensus is that mismatches in the ARD are clinically relevant, so only differences within the ARD were included in the univariate models. As mismatches in HLA-DRB4 exon 3 were suggested as relevant in one previous study12, we incorporated HLA-DRB4 exon 3 mismatches as a separate variable in multivariate analysis to assess any additional risk conferred by such differences. In an overall 481 identified HLA-DRB3/4/5 mismatched cases, 334 (69.4%) concerned the ARD (exon 2) and 147 (30.6%) related to differences in HLA-DRB4 exon 3 only. Some ARD mismatches were combined with additional HLA-DRB4 exon 3 mismatches (Table 2). Mismatches due to missing or additional antigens were classified as ARD discrepancies. These were most often caused by the presence of HLA-DRB4*01:03:01:02N in donor or recipient (n = 29, 0.85%, missing antigen) and due to the uncommon association of HLA-DRB5 with HLA-DRB1*01 (n = 9, 0.27%, additional antigen). A detailed overview of the mismatch combinations is given in Table 2.
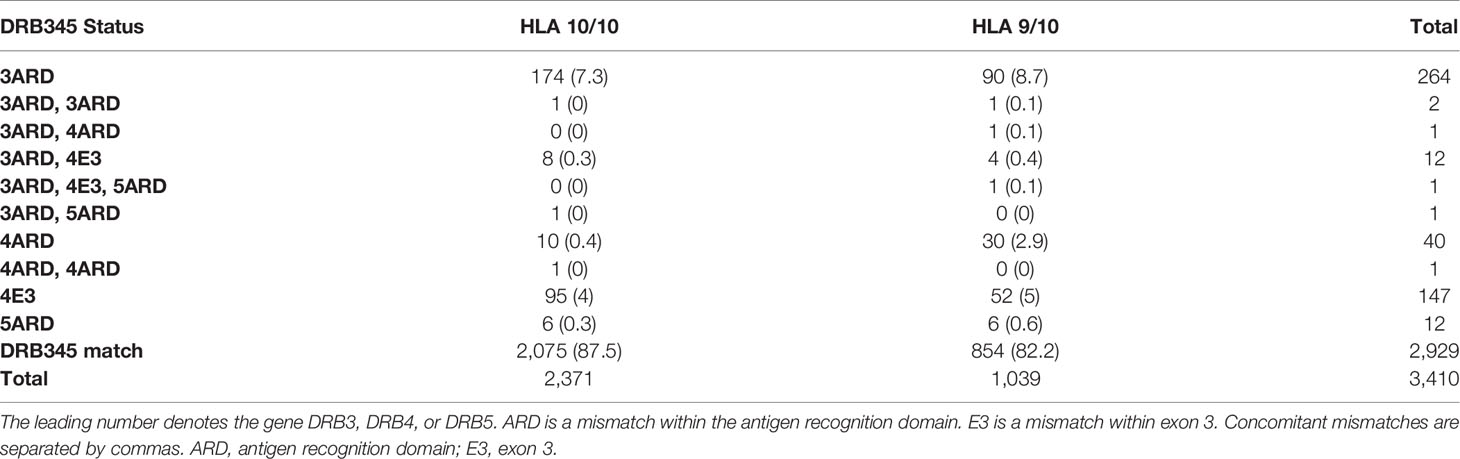
Table 2 HLA-DRB345 mismatch status.
OS in univariate analysis showed a significantly better outcome for 10/10 HLA-A, -B, -C, -DRB1, and -DQB1-matched transplants when HLA-DRB3/4/5 were also matched compared to HLA-DRB3/4/5 ARD-mismatched (MM) cases (log-rank p = 0.038; Figure 1A). Estimates at 1, 3, and 5 years posttransplantation were 64.2% (62.1–66.5), 50.4% (48.0–52.8), and 46.1% (43.6–48.6) for the HLA-DRB3/4/5-matched group vs. 58.0% (51.1–65.7), 48.0% (40.9–56.3), and 39.8% (32.5–48.7) for the HLA-DRB3/4/5 ARD-MM group. This association was not statistically significant in the subgroup of 9/10 HLA-matched transplanted patients, n = 1,039 (log-rank p = 0.237; Figure 1B). Specifically, in this subgroup (n = 1,039), estimates for OS at 1, 3, and 5 years posttransplantation were at 54.5% (51.2–58.1), 42.3% (38.9–46.1), and 38.0% (34.5–41.9) for the HLA-DRB345-matched group vs. 52.7% (44.4–62.7), 32.8% (24.8–43.3), and 30.3% (22.5–40.9) for the HLA-DRB3/4/5 ARD-MM group.
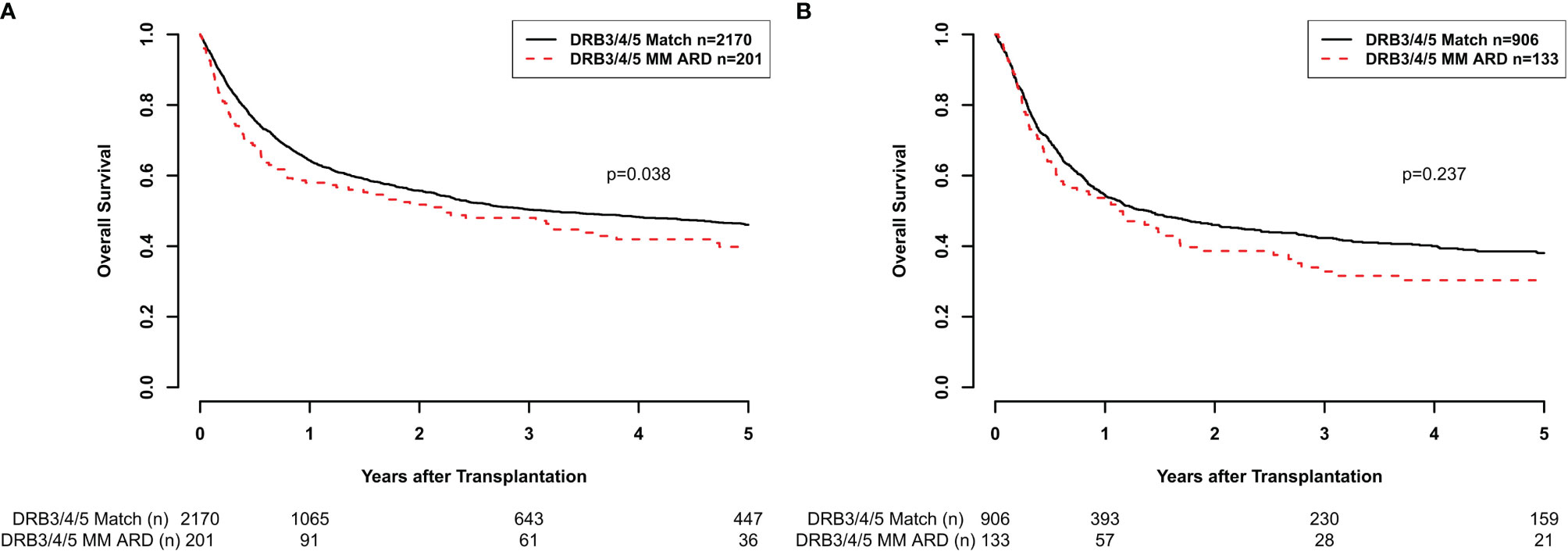
Figure 1 (A) Overall survival (OS) according to HLA-DRB3/4/5 matching status (M = match, MM = mismatch) considering the antigen recognition domain (ARD) only in the subgroup of 10/10-matched transplant pairs (p = 0.038). (B) OS according to HLA-DRB3/4/5 matching status (M, MM) considering the ARD only in the subgroup of 9/10-matched transplant pairs (p = 0.237).
In the multivariate analysis of 10/10 HLA-matched cases, HLA-DRB3/4/5 ARD-MM showed a significantly higher overall mortality risk [OS: hazard ratio (HR) 1.25, 95% CI 1.02–1.54, p = 0.034; Table 3]. For DFS and GFRS, no significant differences were seen between the groups (Table 3). Results for 9/10-matched cases and combined models concerning HLA-DRB3/4/5 ARD and HLA-DRB4 E3 differences are shown in the Supplementary Material.

Table 3 Survival endpoints 10/10 HLA-matched group.
The aforementioned adverse survival outcomes were predominantly caused by a higher risk of NRM in HLA-DRB3/4/5 ARD-mismatched cases (NRM: 1.35, 95% CI 1.05–1.73, p = 0.017; Table 4). No statistically significant risk estimates were observed regarding the incidence rates of aGvHD and cGvHD (aGvHD II–IV: HR 1.16, 95% CI 0.89–1.52, p = 0.277 and cGvHD: HR 1.12, 95% CI 0.85–1.47, p = 0.433). Additional analysis focused on severe aGvHD (i.e., III–IV) incidence rates also failed to reveal any significant association (aGvHD III–IV: HR 1.19, 95% CI 0.79–1.79, p = 0.412). Similarly, exon 3 mismatches at HLA-DRB4 were not associated with a significantly increased risk (Table 4). However, grouping ARD and exon 3 mismatches together resulted in a significantly higher aGvHD risk in a model encompassing all transplant pairs (aGvHD II–IV: HR 1.21, 95% CI 1.02–1.43, p = 0.027; Supplementary Material). No significant difference on relapse rates could be identified for HLA-DRB3/4/5 mismatches, regardless of gene region concerned (i.e., ARD or HLA-DRB4 exon 3; Table 4). In line with numerous previous reports, single HLA mismatches associated with an increased risk for all endpoints except relapse incidence. Non-permissive HLA-DPB1 mismatches correlated with inferior GRFS and higher aGvHD risk but had no statistically significant impact on either OS or DFS. Last, increasing donor age was also highly predictive of mortality. Other clinically relevant covariates that were included in the final models are reported in Tables 3, 4.

Table 4 Competing risk endpoints 10/10 HLA-matched group.
Histocompatibility assessment for classical HLA (HLA-A, HLA-B, HLA-C, HLA-DRB1, HLA-DQB1) alleles is currently the consensus for unrelated donor HSCT in Germany (21–24). Among HLA-class II molecules, the HLA-DRB1 gene shows the highest diversity and highest cell surface expression (25). However, next to the aforementioned highly expressed and polymorphic loci, there are also low expressed genes that appear to be less diverse. Among these are the HLA-DRB3/4/5 genes, which are genetically linked to the HLA-DRB1 gene and form the serologically defined DR52, DR53, and DR51 antigens. Because of the strong linkage disequilibrium with the HLA-DRB1 gene, incompatibilities for HLA-DRB3/4/5 are only observed in a relatively small fraction of transplant pairs when classical HLA alleles are otherwise matched (2). Therefore, there is currently only limited data on the role of HLA-DRB3/4/5 incompatibility in HSCT. In this study, we sought to investigate this parameter in a retrospective analysis of 3,410 patients who received their first unrelated allogeneic transplant between 2000 and 2014 in a malignant hematologic disease setting.
As shown in Figure 1A, HLA-DRB3/4/5-incompatible transplants with a mismatch in the ARD region in an otherwise 10/10 HLA-matched setting had a significantly worse OS when compared to HLA-DRB3/4/5 ARD-compatible transplants. This could be observed in both univariate and multivariate analyses (Table 3). HLA-DRB1 mismatches have shown high relative risks for overall mortality and GvHD incidences in other independent (21, 24) and non-independent large studies (23). This may be partly explained by the fact that DRB1 mismatches often associate with HLA-DRB3/4/5 mismatches, which in turn exert an additional effect on top of HLA-DRB1 disparity. Moreover, lower surface expression of these loci compared to HLA-DRB1 may account for the apparently reduced immunogenicity of HLA-DRB3/4/5 mismatches. No significant results were seen in the 9/10 HLA-matched setting as shown in Figure 1B. The post-hoc power for this subanalysis was 44%, indicating that the case numbers in this subgroup were possibly insufficient to show a putative effect in a statistically significant manner.
An impact of HLA-DRB3/4/5 mismatch on OS has not yet been described in other studies (11, 12). This might be attributed to the relatively high percentage of older patients included in this study (i.e., 30% >60 years and 54 years median age), given that HLA-associated risk increases with age particularly with regard to transplant-related morbidity (26). In our cohort, the effect on OS was in fact mainly driven by an increased NRM (HR 1.35, p = 0.017; Table 4). Although statistical significance was not reached in the aGvHD models including only HLA-DRB3/4/5 ARD-mismatched cases, the analysis in a model encompassing all types of HLA-DRB3/4/5 mismatches revealed a statistically significant higher risk of aGvHD II–IV in the complete cohort (HR 1.21, 95% CI 1.02–1.43, p = 0.027). The inability to clearly identify this effect in the HLA-DRB3/4/5 ARD-mismatched cases alone is more likely due to a lack of statistical power rather than lack of association, considering that previous studies have already shown a significantly higher risk of aGvHD in patients receiving HLA-DRB3/4/5-mismatched grafts (10, 11). Having said that, an additive effect of HLA-DRB4 E3 mismatches cannot be excluded (11), despite the common perception that mismatches not affecting the ARD have a low impact on alloreactivity (27). According to a recently published study, HLA mismatches outside the ARD that were newly detected after retrospective ultrahigh-resolution HLA genotyping of 5,140 10/10 HLA-matched transplant pairs did associate with a higher risk of aGvHD and TRM but no inferior survival (28). The fact thatHLA-DRB3/4/5 incompatibility increased less the risk of aGvHD when compared to HLA-DRB1 or other single HLA incompatibility, as reported in this (i.e., HLA mismatch GvHD II–IV: HR 1.38, p < 0.001; Supplementary Table S4) but also in other studies conducted in Europe and the United States (21, 24, 29–31), indicates that the effect of HLA-DRB3/4/5 mismatch is more subtle and thus more difficult to detect.
Regarding the increased NRM observed, it is of note that death due to infections was more frequent in the HLA-DRB3/4/5 ARD-mismatched group (10/10 HLA: 38.6% vs. 30.7%), something that warrants further investigation (32).
In multivariate analysis, HLA-DRB3/4/5 incompatibility was associated with a significantly higher risk of GRFS. Contrary to the other endpoints, GRFS is informative of both disease and transplant-related morbidity, which gives a better understanding about the patients’ quality of life after HSCT. Ducreux etal. (11) also described a lower GRFS in HLA-DRB3/4/5-mismatched patients—something that was confirmed in this study. As already mentioned, a higher risk of aGvHD in DRB3/4/5-mismatched cases was also observed in our study when all types of DRB3/4/5 mismatches were grouped and analyzed together in the whole of our cohort (n = 3,410).
Our study differs from previously published studies in several aspects. Fernandez-Vina etal. (12) analyzed mismatches in low expressing loci (LEL) alleles in general, namely, without segregating the impact of HLA-DQ or HLA-DP mismatches, which appear to have different immunobiological properties (33–35). We, on the other hand, analyzed the impact of HLA-DRB3/4/5 mismatches independently from other LEL.
Furthermore, since matching for HLA-DP epitopes has been shown to play an important role in HSCT, we analyzed the distribution of HLA-DP-matched/permissive and non-permissive transplantations among HLA-DRB3/4/5-matched and -mismatched cases, respectively (33–35). As shown in Table 1, the distribution was similar between the subgroups analyzed, with mild differences observed only in a relatively small fraction of cases (i.e., 5.5% and 8.3% more cases with DPB1 non-permissive mismatches in the DRB3/4/5-mismatched transplant pairs compared to the DRB3/4/5-matched ones in the 10/10 and 9/10 HLA-matched subgroups, respectively). Moreover, no interaction between HLA-DPB1 and HLA-DRB3/4/5 mismatches was observed in the multivariate analysis, which justified the independent analysis of HLA-DRB3/4/5 mismatches on the outcome of HSCT. Previously published studies limited their cohort only to HLA-DPB1-mismatched transplants due to the low numbers of HLA-DPB1-matched cases (11). Because of the independent effect of HLA-DPB1 and HLA-DRB3/4/5 mismatches, we chose to include HLA-DPB1-matched transplants and to account for both variables in the multivariate analysis.
Limitations of this study were the heterogeneity of the cohort regarding in vivo T-cell depletion and the relatively high proportion of older patients, where the impact of HLA mismatches may be more pronounced (26). Furthermore, although various possible HLA-DRB3/4/5 disparities were identified (Table 2), the cohort size precluded analysis at individual combination levels in order to predict the risk for each one of those separately. This means that, unavoidably, the respective HLA-DRB3, -DRB4, and -DRB5 genes were considered in the analysis as one uniform locus, and thus, no comparison between HLA-DRB3, -DRB4, and -DRB5-mismatched cases was sought, considering as well that in some cases, multiple HLA-DRB3/4/5 mismatches were observed. Last, another limitation of our study was that HLA differences outside the ARD and incompatibilities in additional genes like HLA-DQA, -DPA, -MICA, -MICB, -E, -F, and –G were not considered. Such an approach could perhaps clarify if the associations observed should be attributed to an independent HLA-DRB3/4/5 mismatch effect or rather an HLA-haplotype incompatibility impact. Moreover, subanalysis for the vector of mismatches could not be performed due to power considerations.
An aspect that could be investigated in future studies is whether factors influencing the expression levels of HLA-DRB3/4/5 antigens may also influence the effect of HLA-DRB3/4/5 incompatibilities on HSCT outcome, as this has been shown to be the case for HLA-DP (36, 37).
In conclusion, our study suggests that HLA-DRB3/4/5 incompatibilities in a setting of otherwise 10/10 and possibly also 9/10 HLA-matched uHSCT may increase the risk of adverse outcomes especially in more frail patients who face a higher risk of developing transplant-related complications and should therefore be avoided when possible.
The datasets presented in this article are not readily available because of data safety and confidentiality regulations denoted in the patient consent forms and the application for ethical approval. Requests to access the datasets should be directed to d.fuerst@blutspende.de.
The studies involving human participants were reviewed and approved by the ethical committee of the University of Ulm. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
CT, DE, HS, JM, and DF are principal investigators. They designed the study, performed data analysis/interpretation, and wrote the article. SaF and CN contributed to the data analysis and writing of the article. CT and DE contributed equally. DF and JM contributed equally. UP, ES, TV, EW-D, GW, NK, NM, HE, KS-E, SeF, JC, MK, MD, BH, SK, and MR contributed patients, reviewed the data, and edited the article. All authors contributed to the article and approved the submitted version.
This work was supported by the Wilhelm Sander-Stiftung (Grant No. 2018.092.1).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors thank Anita Richter for performing the HLA class II typing.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2021.771449/full#supplementary-material
1. Rollini P, Mach B, Gorski J. Linkage Map of Three HLA-DR Beta-Chain Genes: Evidence for a Recent Duplication Event. Proc Natl Acad Sci USA (1985) 82:7197–201. doi: 10.1073/pnas.82.21.7197
2. Maiers M, Gragert L, Klitz W. High-Resolution HLA Alleles and Haplotypes in the United States Population. Hum Immunol (2007) 68:779–88. doi: 10.1016/j.humimm.2007.04.005
3. Nunez G, Ball EJ, Myers LK, Stastny P. Allostimulating Cells in Man. Quantitative Variation in the Expression of HLA-DR and HLA-DQ Molecules Influences T-Cell Activation. Immunogenetics (1985) 22:85–91. doi: 10.1007/BF00430597
4. Hurley CK, Nunez G, Winchester R, Finn OJ, Levy R, Capra JD. The Human HLA-DR Antigens are Encoded by Multiple Beta-Chain Loci. J Immunol (1982) 129:2103–8.
5. Mack SJ, Cano P, Hollenbach JA, He J, Hurley CK, Middleton D, et al. Common and Well-Documented HLA Alleles: 2012 Update to the CWD Catalogue. Tissue Antigens (2013) 81:194–203. doi: 10.1111/tan.12093
6. Sutton VR, Kienzle BK, Knowles RW. An Altered Splice Site is Found in the DRB4 Gene That is Not Expressed in HLA-DR7,Dw11 Individuals. Immunogenetics (1989) 29:317–22. doi: 10.1007/BF00352841
7. Fernandez-Vina MA, Gao XJ, Moraes ME, Moraes JR, Salatiel I, Miller S, et al. Alleles at Four HLA Class II Loci Determined by Oligonucleotide Hybridization and Their Associations in Five Ethnic Groups. Immunogenetics (1991) 34:299–312. doi: 10.1007/BF00211994
8. Fuerst D, Tsamadou C, Gowdavally S, Schrezenmeier H, Mytilineos J. HLA-DRB4*01:14 is a Null Allele, and Renamed HLA-DRB4*01:14N. HLA (2020) 95:73–5. doi: 10.1111/tan.13701
9. Kotsch K, Wehling J, Blasczyk R. Sequencing of HLA Class II Genes Based on the Conserved Diversity of the non-Coding Regions: Sequencing Based Typing of HLA-DRB Genes. Tissue Antigens (1999) 53:486–97. doi: 10.1034/j.1399-0039.1999.530505.x
10. Detrait M, Morisset S, Chalandon Y, Yakoub-Agha I, Dufossé F, Labalette M, et al. Suggestive Evidence of a Role of HLA-DRB4 Mismatches in the Outcome of Allogeneic Hematopoietic Stem Cell Transplantation With HLA-10/10-Matched Unrelated Donors: A French-Swiss Retrospective Study. Bone Marrow Transplant (2015) 50:1316–20. doi: 10.1038/bmt.2015.157
11. Ducreux S, Dubois V, Amokrane K, Yakoub-Agha I, Labalette M, Michallet M, et al. HLA-DRB3/4/5 Mismatches are Associated With Increased Risk of Acute GVHD in 10/10 Matched Unrelated Donor Hematopoietic Cell Transplantation. Am J Hematol (2018) 93:994–1001. doi: 10.1002/ajh.25133
12. Fernandez-Vina MA, Klein JP, Haagenson M, Spellman SR, Anasetti C, Noreen H, et al. Multiple Mismatches at the Low Expression HLA Loci DP, DQ, and DRB3/4/5 Associate With Adverse Outcomes in Hematopoietic Stem Cell Transplantation. Blood (2013) 121:4603–10. doi: 10.1182/blood-2013-02-481945
13. van Balen P, van Luxemburg-Heijs SAP, van de Meent M, van Bergen CAM, Halkes CJM, Jedema I, et al. Mismatched HLA-DRB3 Can Induce a Potent Immune Response After HLA 10/10 Matched Stem Cell Transplantation. Transplantation (2017) 101:2850–4. doi: 10.1097/TP.0000000000001713
14. Hurley CK, Woolfrey A, Wang T, Haagenson M, Umejiego J, Aljurf M, et al. The Impact of HLA Unidirectional Mismatches on the Outcome of Myeloablative Hematopoietic Stem Cell Transplantation With Unrelated Donors. Blood (2013) 121:4800–6. doi: 10.1182/blood-2013-01-480343
15. Gabriel C, Furst D, Fae I, Wenda S, Zollikofer C, Mytilineos J, et al. HLA Typing by Next-Generation Sequencing - Getting Closer to Reality. Tissue Antigens (2014) 83:65–75. doi: 10.1111/tan.12298
16. Nunes E, Heslop H, Fernandez-Vina M, Taves C, Wagenknecht DR, Eisenbrey AB, et al. Definitions of Histocompatibility Typing Terms: Harmonization of Histocompatibility Typing Terms Working Group. Hum Immunol (2011) 72:1214–6. doi: 10.1016/j.humimm.2011.06.002
17. Gratwohl A. The EBMT Risk Score. Bone Marrow Transplant (2012) 47:749–56. doi: 10.1038/bmt.2011.110
18. Bacigalupo A, Ballen K, Rizzo D, Giralt S, Lazarus H, Ho V, et al. Defining the Intensity of Conditioning Regimens: Working Definitions. Biol Blood Marrow Transplant (2009) 15:1628–33. doi: 10.1016/j.bbmt.2009.07.004
19. Iacobelli S. Suggestions on the Use of Statistical Methodologies in Studies of the European Group for Blood and Marrow Transplantation. Bone Marrow Transplant (2013) 48 Suppl 1:S1–37. doi: 10.1038/bmt.2012.282
20. Zhou B, Fine J, Latouche A, Labopin M. Competing Risks Regression for Clustered Data. Biostatistics (2012) 13:371–83. doi: 10.1093/biostatistics/kxr032
21. Ayuk F, Beelen DW, Bornhauser M, Stelljes M, Zabelina T, Finke J, et al. Relative Impact of HLA Matching and Non-HLA Donor Characteristics on Outcomes of Allogeneic Stem Cell Transplantation for Acute Myeloid Leukemia and Myelodysplastic Syndrome. Biol Blood Marrow Transplant (2018) 24:2558–67. doi: 10.1016/j.bbmt.2018.06.026
22. Flomenberg N, Baxter-Lowe LA, Confer D, Fernandez-Vina M, Filipovich A, Horowitz M, et al. Impact of HLA Class I and Class II High-Resolution Matching on Outcomes of Unrelated Donor Bone Marrow Transplantation: HLA-C Mismatching is Associated With a Strong Adverse Effect on Transplantation Outcome. Blood (2004) 104:1923–30. doi: 10.1182/blood-2004-03-0803
23. Furst D, Muller C, Vucinic V, Bunjes D, Herr W, Gramatzki M, et al. High-Resolution HLA Matching in Hematopoietic Stem Cell Transplantation: A Retrospective Collaborative Analysis. Blood (2013) 122:3220–9. doi: 10.1182/blood-2013-02-482547
24. Lee SJ, Klein J, Haagenson M, Baxter-Lowe LA, Confer DL, Eapen M, et al. High-Resolution Donor-Recipient HLA Matching Contributes to the Success of Unrelated Donor Marrow Transplantation. Blood (2007) 110:4576–83. doi: 10.1182/blood-2007-06-097386
25. Brooks CF, Moore M. Differential MHC Class II Expression on Human Peripheral Blood Monocytes and Dendritic Cells. Immunology (1988) 63:303–11.
26. Furst D, Niederwieser D, Bunjes D, Wagner EM, Gramatzki M, Wulf G, et al. Increased Age-Associated Mortality Risk in HLA-Mismatched Hematopoietic Stem Cell Transplantation. Haematologica (2017) 102:796–803. doi: 10.3324/haematol.2016.151340
27. Roelen D, de Vaal Y, Vierra-Green C, Waldvogel S, Spellman S, Claas F, et al. HLA Mismatches That are Identical for the Antigen Recognition Domain are Less Immunogenic. Bone Marrow Transplant (2018) 53:729–40. doi: 10.1038/s41409-018-0108-6
28. Mayor NP, Wang T, Lee SJ, Kuxhausen M, Vierra-Green C, Barker DJ, et al. Impact of Previously Unrecognized HLA Mismatches Using Ultrahigh Resolution Typing in Unrelated Donor Hematopoietic Cell Transplantation. J Clin Oncol (2021) 39:2397–409. doi: 10.1200/JCO.20.03643
29. Kanda Y, Kanda J, Atsuta Y, Maeda Y, Ichinohe T, Ohashi K, et al. Impact of a Single Human Leucocyte Antigen (HLA) Allele Mismatch on the Outcome of Unrelated Bone Marrow Transplantation Over Two Time Periods. A Retrospective Analysis of 3003 Patients From the HLA Working Group of the Japan Society for Blood and Marrow Transplantation. Br J Haematol (2013) 161:566–77. doi: 10.1111/bjh.12279
30. Verneris MR, Lee SJ, Ahn KW, Wang HL, Battiwalla M, Inamoto Y, et al. HLA Mismatch Is Associated With Worse Outcomes After Unrelated Donor Reduced-Intensity Conditioning Hematopoietic Cell Transplantation: An Analysis From the Center for International Blood and Marrow Transplant Research. Biol Blood Marrow Transplant (2015) 21:1783–9. doi: 10.1016/j.bbmt.2015.05.028
31. Woolfrey A, Klein JP, Haagenson M, Spellman S, Petersdorf E, Oudshoom M, et al. HLA-C Antigen Mismatch is Associated With Worse Outcome in Unrelated Donor Peripheral Blood Stem Cell Transplantation. Biol Blood Marrow Transplant (2011) 17:885–92. doi: 10.1016/j.bbmt.2010.09.012
32. Servais S, Lengline E, Porcher R, Carmagnat M, de Latour RP, Robin M, et al. Long-Term Immune Reconstitution and Infection Burden After Mismatched Hematopoietic Stem Cell Transplantation. Biol Blood Marrow Transplant (2014) 20:507–17. doi: 10.1016/j.bbmt.2014.01.001
33. Crivello P, Zito L, Sizzano F, Zino E, Maiers M, Mulder A, et al. The Impact of Amino Acid Variability on Alloreactivity Defines a Functional Distance Predictive of Permissive HLA-DPB1 Mismatches in Hematopoietic Stem Cell Transplantation. Biol Blood Marrow Transplant (2015) 21:233–41. doi: 10.1016/j.bbmt.2014.10.017
34. Fleischhauer K, Shaw BE, Gooley T, Malkki M, Bardy P, Bignon JD, et al. Effect of T-Cell-Epitope Matching at HLA-DPB1 in Recipients of Unrelated-Donor Haemopoietic-Cell Transplantation: A Retrospective Study. Lancet Oncol (2012) 13:366–74. doi: 10.1016/S1470-2045(12)70004-9
35. Zino E, Frumento G, Marktel S, Sormani MP, Ficara F, Di Terlizzi S, et al. A T-Cell Epitope Encoded by a Subset of HLA-DPB1 Alleles Determines Nonpermissive Mismatches for Hematologic Stem Cell Transplantation. Blood (2004) 103:1417–24. doi: 10.1182/blood-2003-04-1279
36. Petersdorf EW, Gooley TA, Malkki M, Bacigalupo AP, Cesbron A, Du Toit E, et al. HLA-C Expression Levels Define Permissible Mismatches in Hematopoietic Cell Transplantation. Blood (2014) 124:3996–4003. doi: 10.1182/blood-2014-09-599969
Keywords: HLA-DRB3, HLA-DRB4, HLA-DRB5, HLA-DRB3/4/5, unrelated hematopoietic stem cell transplantation (uHSCT), HLA-matched, DRB3/4/5 matching
Citation: Tsamadou C, Engelhardt D, Platzbecker U, Sala E, Valerius T, Wagner-Drouet E, Wulf G, Kröger N, Murawski N, Einsele H, Schaefer-Eckart K, Freitag S, Casper J, Kaufmann M, Dürholt M, Hertenstein B, Klein S, Ringhoffer M, Frank S, Neuchel C, Schrezenmeier H, Mytilineos J and Fuerst D (2021) HLA-DRB3/4/5 Matching Improves Outcome of Unrelated Hematopoietic Stem Cell Transplantation. Front. Immunol. 12:771449. doi: 10.3389/fimmu.2021.771449
Received: 06 September 2021; Accepted: 18 November 2021;
Published: 14 December 2021.
Edited by:
Eric Spierings, Utrecht University, NetherlandsReviewed by:
Valerie Dubois, Etablissement Français du Sang Auvergne Rhône Alpes, FranceCopyright © 2021 Tsamadou, Engelhardt, Platzbecker, Sala, Valerius, Wagner-Drouet, Wulf, Kröger, Murawski, Einsele, Schaefer-Eckart, Freitag, Casper, Kaufmann, Dürholt, Hertenstein, Klein, Ringhoffer, Frank, Neuchel, Schrezenmeier, Mytilineos and Fuerst. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel Fuerst, d.fuerst@blutspende.de
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.