
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Immunol. , 20 December 2021
Sec. Primary Immunodeficiencies
Volume 12 - 2021 | https://doi.org/10.3389/fimmu.2021.760019
 Martin Martinot1*
Martin Martinot1* Anne Sophie Korganow2Mathieu Wald1Julie Second3Elodie Birckel3Antoine Mahé3Laurent Souply4Mahsa Mohseni-Zadeh1Laure Droy5Julien Tarabeux6Satoshi Okada7Mélanie Migaud8
Anne Sophie Korganow2Mathieu Wald1Julie Second3Elodie Birckel3Antoine Mahé3Laurent Souply4Mahsa Mohseni-Zadeh1Laure Droy5Julien Tarabeux6Satoshi Okada7Mélanie Migaud8 Anne Puel7,9,10
Anne Puel7,9,10 Aurelien Guffroy2
Aurelien Guffroy2Purpose: Heterozygous missense STAT1 mutations leading to a gain of function (GOF) are the most frequent genetic cause of chronic mucocutaneous candidiasis (CMC). We describe the case of a patient presenting a new GOF mutation of STAT1 with the clinical symptoms of CMC, recurrent pneumonia, and persistent central erythema with papulopustules with ocular involvement related to rosacea-like demodicosis.
Methods: Genetic analysis via targeted next-generation sequencing (NGS; NGS panel DIPAI v.1) exploring the 98 genes most frequently involved in primary immunodeficiencies, including STAT1, was performed to identify an underlying genetic defect.
Results: NGS identified a novel variant of STAT1, c.884C>A (exon 10), p.T295Y, not previously described. This variant was found to be gain of function using an in vitro luciferase reporter assay. Rosacea-like demodicosis was confirmed by substantial Demodex proliferation observed via the microscopic examination of a cutaneous sample. A review of literature retrieved 20 other cases of STAT1 GOF mutations associated with early-onset rosacea-like demodicosis, most with ocular involvement.
Conclusion: We describe a new STAT1 GOF mutation associated with a phenotype of CMC and rosacea-like demodicosis. Rosacea-like demodicosis appears as a novel and important clinical phenotype among patients with STAT1 GOF mutation.
Chronic mucocutaneous candidiasis (CMC) is characterized by increased susceptibility to skin, mucosa, and nail infections caused by Candida species and dermatophytes. CMC is found in patients with various acquired or inherited immune disorders (1, 2). The autosomal dominant (AD) signal transducer and activator of transcription protein (STAT) 1 gain of function (STAT1 GOF) is the most frequent genetic cause of CMC (3, 4). STATs are critical signaling molecules downstream of interferons (IFNs), cytokines, growth factors, and hormones, which upon binding to their receptors lead to the activation of Janus kinases, which recruit and phosphorylate cytoplasmic STAT proteins (JAK–STAT signaling pathway). Phosphorylated STATs form homo- or heterodimers and translocate to the nucleus where they bind to specific promoters to initiate transcription (5). Most of the STAT1 GOF variants are located in the coiled-coil and DNA-binding domains of STAT1 (6). These variants result in enhanced STAT1 phosphorylation, as compared to wild-type STAT1, due to impaired nuclear dephosphorylation (4), and enhanced STAT1 signaling downstream of STAT1-dependant cytokines, such as IFN-α/β, IFN-γ, and interleukin (IL)-27, as well as downstream STAT3-dependent cytokines, such as IL-6 and IL-21, resulting in impaired Th17 cell development (4, 7). Patients with STAT1 GOF present heterogeneous symptoms; CMC is present in nearly all cases often associated with other infectious (bacterial, fungal, or viral) and noninfectious (autoimmunity/inflammatory, aneurysm, and tumor) clinical features (6, 8). Rosacea-like demodicosis is an emerging manifestation reported among the patients with STAT1 GOF, with only a few cases recently described in the literature (9–14), related to Demodex proliferation. We report the case of a patient with a novel heterozygous STAT1 mutation, shown by functional study to be GOF, who presented CMC associated with recurrent pneumonia and florid rosacea-like demodicosis affecting the center of the face and the eyelids.
A 40-year-old woman has been hospitalized in our department of infectious diseases in February 2018 for fever and cough. Her medical history included CMC since 7 years of age which had never been explored, and esophageal candidiasis in 2015 showing recurrence despite treatment with fluconazole. She had a 3-year-old healthy boy, and no other case was reported in her family.
Upon admission, the patient was diagnosed with pneumonia associated with bronchiectasis via clinical and radiological examinations. Microbiological examination revealed Streptococcus pneumoniae in the sputum. On clinical exam, marked oral candidiasis and diffuse inflammatory papules on the face associated with bilateral blepharitis were noted (Figure 1). The patient was successfully treated with ceftriaxone but experienced another episode of pneumonia in June 2018, which resolved after further treatment with ceftriaxone. The patient denied receiving any treatment for CMC.

Figure 1 Chronic oral candidiasis (left, photo taken in February 2018) associated with diffuse inflammatory papules and blepharitis along with cutaneous and ocular rosacea-like demodicosis (right, photo taken in June 2018).
A direct examination of the eyelashes revealed the presence of Demodex folliculorum (Supplementary Material, Appendix 2). Skin biopsy also revealed non-granulomatous peripilar inflammation with the presence of numerous Demodex within the follicles (Figure 2). A diagnosis of florid rosacea-like demodicosis was therefore established. Treatment with oral doxycycline (100 mg/day) led to the partial improvement of the lesions. Similarly, oral ivermectin (200 µg/kg, thrice a week) in combination with a daily topical application of ivermectin led to the partial improvement of the lesions. Finally, lasting remission was achieved with the resumption of doxycycline in combination with the local application of 1.5% metronidazole.
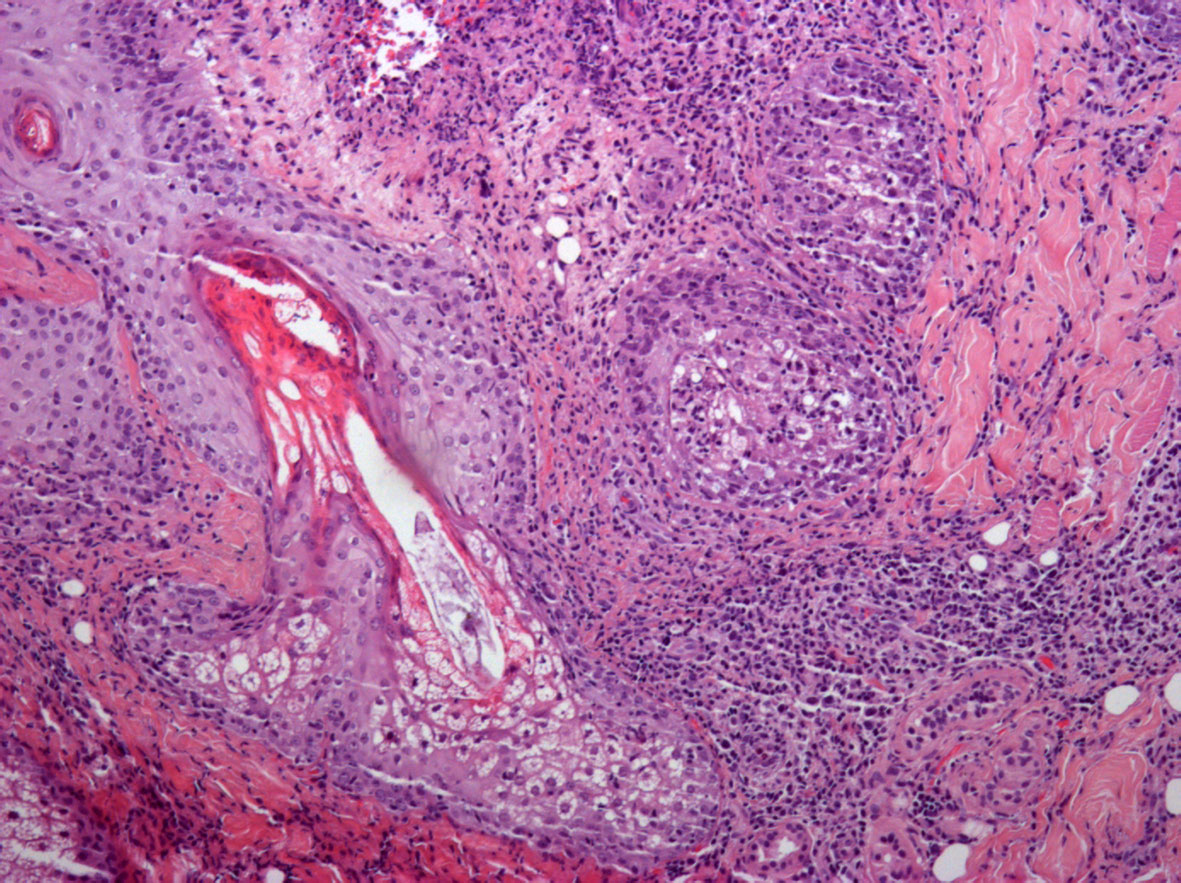
Figure 2 Skin biopsy (hematoxylin and eosin staining, ×10). A mixed inflammatory infiltrate (arrow), without granuloma, related to pilosebaceous units, containing Demodex (star).
The absolute lymphocyte count was 1,650/mm3, with 1.070/mm3 T CD3+ lymphocytes (601 T CD4+, 454 T CD8+, with a CD4/CD8 ratio of 1.32). The natural killer cell count was 166/mm3, and the B lymphocyte count was low, with a CD19+ cell count of 58/mm3, corresponding to 4% of the total lymphocyte count. Immunoglobulin levels were in the normal range [10.16 g/l (IgG), 2.14 g/L (IgA), and 0.9 g/L (IgM)]. Serologic testing for human immunodeficiency virus was negative. The results of plasma protein electrophoresis for determining immunoglobulin levels (including IgG subclasses) and complement assay were in the normal range, as was the control of tetanus vaccination. The results of autoimmune assay were also negative.
Genetic analysis by targeted next-generation sequencing (NGS; NGS panel DIPAI v.1) exploring the 98 genes most frequently involved in primary immunodeficiencies, including STAT1, was performed (Supplementary Material, Appendix 1). DNA samples were extracted from the peripheral blood. For high-throughput sequencing, targeted libraries were prepared with an individual in-solution SureSelect capture reaction for each DNA sample using a QXT protocol and custom design for genes known to be involved in primary immunodeficiencies (Agilent, Santa Clara, California, USA). Capture experiments were performed using probes corresponding to a panel of 98 genes.
Paired-end sequencing (2 × 75 bp) was performed on Illumina NextSeq 550, multiplexing an average of 25 samples per run. Read mapping, variant calling, and annotation were performed using an in-house bioinformatics pipeline. Detected variants, short indels, and single-nucleotide variants were annotated and ranked using the VaRank software (15).
NGS identified a novel nucleotide change c.884C>A (exon 10) of STAT1, at the heterozygous state, resulting in a private missense mutation (p.T295K). The mutation was not confirmed by Sanger sequencing, but we controlled the concordance between NGS data and the individual using TaqMan assay with identitovigilance single-nucleotide polymorphism on an independent sample. Parents’ DNA samples were not available. The mutation was predicted to be deleterious in silico (SIFT score = 0.04, CADD score = 20.1) and was not yet described in public databases (1000 Genome Project, gnomAD v2.1.1).
Assessment of the mutation impact was performed in vitro using a luciferase reporter assay. U3C cells were plated into 96-well plates (1 × 104/well) and transfected with reporter plasmids (Cignal GAS and ISRE Reporter Assay kit; SA Biosciences) together with plasmids encoding various STAT1 proteins (wild type, WT, or mutant: p.T295K, patient’s mutation, p.R274Q, already reported as GOF, and Y701C, a loss-of-function protein) or an empty vector in the presence of Lipofectamine LTX (Invitrogen, Massachusetts, United States). After 6 h of transfection, cells were washed and incubated in RPMI/10% fetal bovine serum for 24 additional hours. Cells were then stimulated or not with IFN-γ (10 and 1,000 IU/ml) for 16 h, followed by luciferase assay using the Dual-Glo luciferase assay system (Promega, Wisconsin, United States). Experiments were performed in triplicate, and firefly luciferase activity was normalized with Renilla luciferase activity. In this GAS reporter luciferase assay, the patient’s p.T295K-encoding STAT1 allele showed enhanced luciferase activity upon IFN-γ stimulation, as compared to the WT encoding STAT1 allele or even more when compared to the loss-of-function p.Y701C-encoding STAT1 mutant allele, comparable to the p.R274Q-encoding STAT1 mutant allele, previously shown to be GOF (4, 7) (Figure 3). We did not assess pSTAT1 in the patient’s cells.
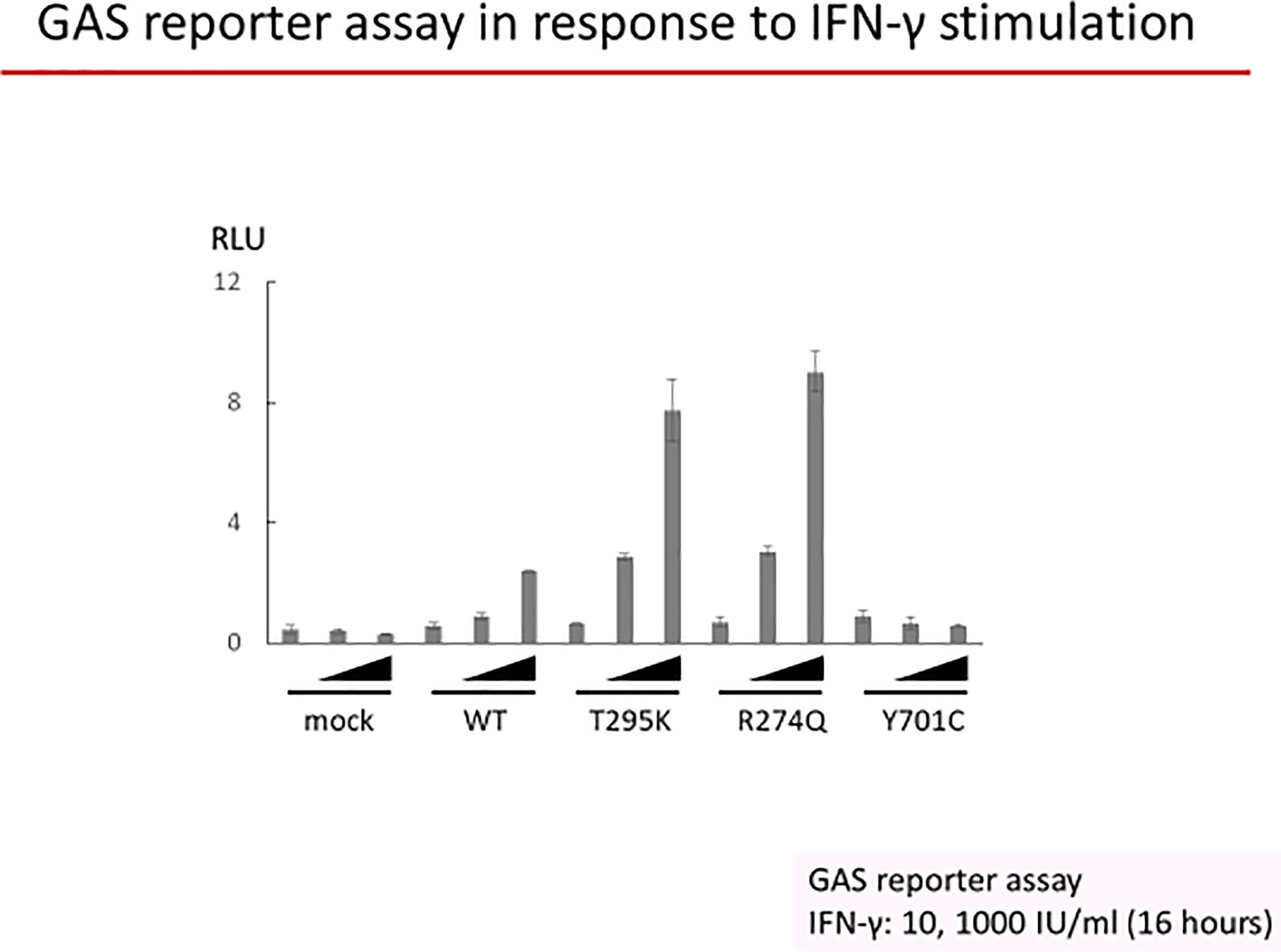
Figure 3 U3C cells were transfected with a mock vector, a WT allele, or three mutant alleles of STAT1 (encoding T295K, R274Q, or Y701C STAT1). Luciferase activity under a GAS promoter was evaluated after 16 h of stimulation with 10 or 1,000 IU/ml of IFN-γ or without stimulation.
Inherited CMC has been reported in many inborn errors of immunity impairing the IL-17A/F axis (2, 7). Up to now, the genetic defect responsible for most of the reported cases of CMC is autosomal dominant STAT1 GOF, described in 2011, with various heterozygous mutations located in the coiled-coil domain of STAT1 associated with exaggerated IFN-α/β and IFN-γ responses and low Th17 cell proportions (3, 4, 7). As many as 105 mutations at 72 amino acid residues, including 65 recurrent mutations, have already been reported in more than 400 patients worldwide (7). STAT1 GOF can lead to a wide variety of clinical manifestations, with CMC being nearly constantly observed (3, 4, 6, 8). However, rosacea was not reported in the first descriptions of STAT1 GOF in 2011 (3, 4). A cohort of 26 patients with STAT1 GOF reported skin infections, such as pustules, furunculosis, or folliculitis, but not rosacea (6). However, some cases of demodicosis can manifest with folliculitis (16). In 2016, a large international cohort of 274 patients with STAT1 GOF from 167 kindreds originating across 40 countries was described (8). CMC was found in almost all patients (98%); however, the patients displayed a much broader and heterogeneous clinical phenotype, including other skin and invasive infectious diseases, autoimmune diseases (37%), cerebral aneurysm (6%), and/or cancers (6%) (8). Our patient presented CMC, pneumonia, and bronchiectasis, as well as florid rosacea, a clinical form not reported in the two series, but only in 20 other cases among 6 different families (Table 1) (9–14). The pathophysiology causing rosacea in STAT1 GOF remains unknown. However, it is suspected that the immunodeficiency related to STAT1 GOF facilitates Demodex mite and bacterial proliferation involved in rosacea affecting the face and, even more frequently, the eyelids. There is a link between Demodex and rosacea (17) explaining the success of ivermectin treatment in some patients with STAT1 GOF (9, 10). We did not perform a density count for Demodex, but the Demodex load appeared high and the presence of Demodex infection was easily confirmed. However, the antiparasitic treatment was not effective, and it is only in combination with more conventional rosacea therapies that the treatment ultimately achieved the patient’s lasting remission. Other microbes, especially bacteria such as Bacillus oleronius, whether they are harbored or not by Demodex are involved in the pathophysiology of rosacea. This finding may explain the success of the patient’s treatment with tetracyclines (18). Rosacea is a chronic inflammatory skin disease affecting typically the convexities of the face, with the possibility of ocular involvement (subtype 4) (19). A retrospective study of 115 cases of demodicosis reported three cases related to immunodeficiencies (20). Demodicosis in patients with human immunodeficiency virus infection (21–24), with an immune reconstitution inflammatory syndrome (25–28), or in a patient with ataxia-telangiectasia (29) has been reported. The impaired IL-17-mediated immunity, with low Th17 cell proportions, in STAT1 GOF patients may explain the proliferation of Demodex (30), leading to the occurrence of demodicosis, especially rosacea-like demodicosis (31). Rosacea-like demodicosis could also be more prevalent but under-recognized in those with inborn errors of immunity.
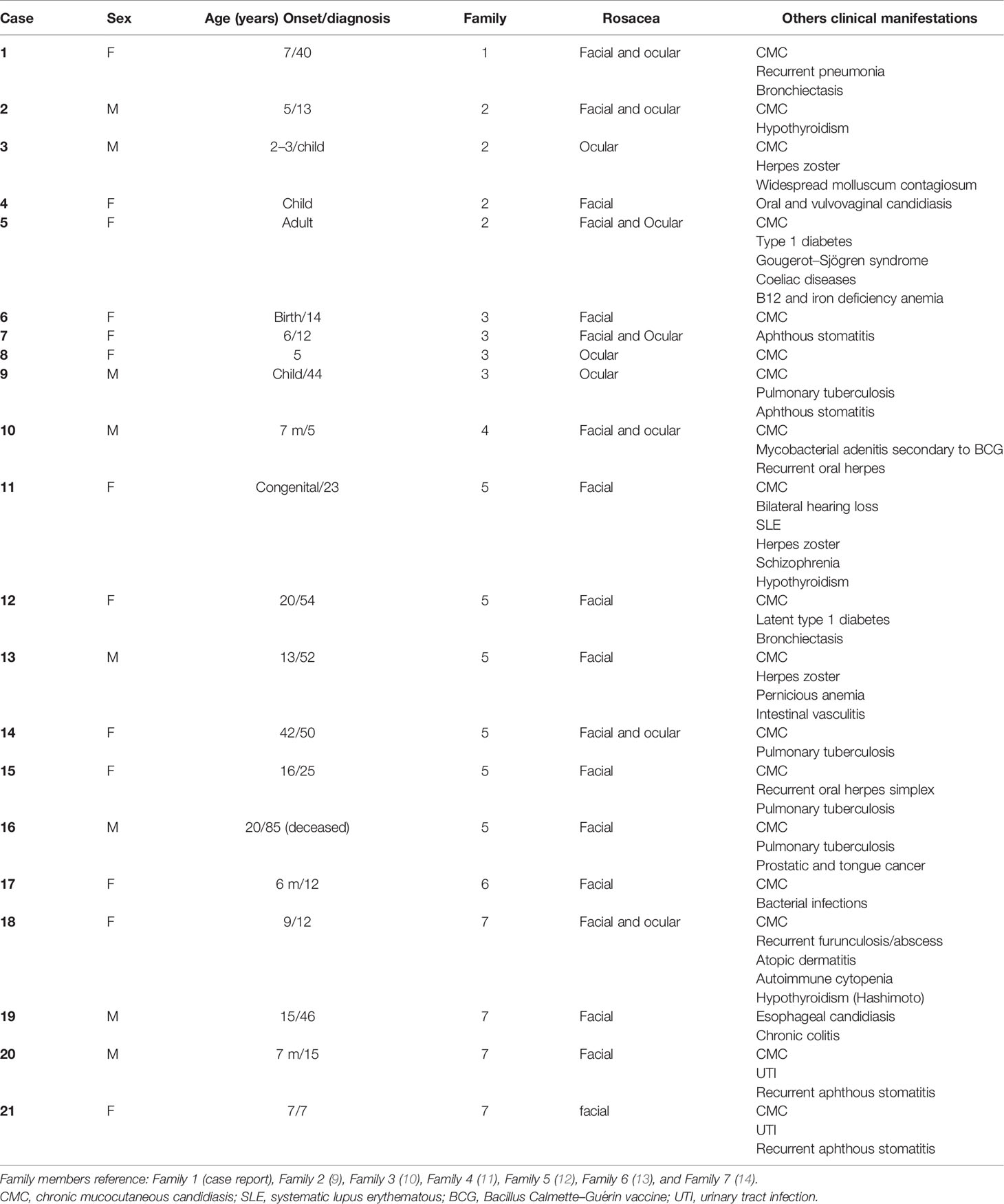
Table 1 Clinical characteristics of the 19 patients with rosacea and STAT1 GOF mutation.
In conclusion, we describe a patient heterozygous for a novel STAT1 GOF mutation. The phenotype includes CMC, bacterial pneumonia, and florid rosacea-like demodicosis with ocular involvement. Rosacea-like demodicosis appears as an increasingly recognized clinical feature among individuals with STAT1 GOF mutations. Therefore, a thorough cutaneous examination of patients with STAT1 GOF should carefully evaluate the presence of rosacea-like demodicosis, which can be easily omitted in clinical practice, and rosacea related to chronic demodicosis should be considered among symptoms suggestive of STAT1 GOF.
The datasets presented in this article are not readily available because the consent obtained did not include making this publicly available. However, the variant data can be found at https://www.ncbi.nlm.nih.gov/clinvar/ under the accession number SCV001885896. Requests to access the datasets should be directed to the corresponding author.
Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.
MM, AK, and AG conceived and designed the case report, contributed to the clinical and pathology diagnosis, collected all data, and wrote the manuscript. AP, AK, MM, LS, SO and JT contributed to the pathology diagnosis, immunohistochemistry, and its photographic material. EB, JS, AM, and LD contributed to the dermatologic evaluation and skin biopsies. All authors critically revised the manuscript for important intellectual content, provided approval of the final version, and agreed to be accountable for all aspects of the work. All authors contributed to the article and approved the submitted version.
The work was funded by the French National Research Agency (ANR) under the “Investments for the future” program (ANR-10-IAHU-01), the ANR-18-CE93-0008-01, the Integrative Biology of Emerging Infectious Diseases Laboratory of Excellence (ANR-10-LABX-62-IBEID), and the National Institute of Allergy and Infectious Diseases of the NIH (grant no. R01AI127564). This study was supported by the European Reference Networks for Rare Diseases (ERN) Rare Immunodeficiency, Autoinflammatory, and Autoimmune Diseases (RITA).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors thank Jamel Chelly, Raphaël Carapito, and Benedicte Gerard from the DIPAI group who helped with the DIPAI genetic analysis.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2021.760019/full#supplementary-material
1. Tangye SG, Al-Herz W, Bousfiha A, Chatila T, Cunningham-Rundles C, Etzioni A, et al. Human Inborn Errors of Immunity: 2019 Update on the Classification From the International Union of Immunological Societies Expert Committee. J Clin Immunol (2020) 40(1):24–64. doi: 10.1007/s10875-019-00737-x
2. Puel A. Human Inborn Errors of Immunity Underlying Superficial or Invasive Candidiasis. Hum Genet (2020) 139(6-7):1011–22. doi: 10.1007/s00439-020-02141-7
3. van de Veerdonk FL, Plantinga TS, Hoischen A, Smeekens SP, Joosten LA, Gilissen C, et al. STAT1 Mutations in Autosomal Dominant Chronic Mucocutaneous Candidiasis. N Engl J Med (2011) 365(1):54–61. doi: 10.1056/NEJMoa1100102
4. Liu L, Okada S, Kong XF, Kreins AY, Cypowyj S, Abhyankar A, et al. Gain-Of-Function Human STAT1 Mutations Impair IL-17 Immunity and Underlie Chronic Mucocutaneous Candidiasis. J Exp Med (2011) 208(8):1635–48. doi: 10.1084/jem.20110958
5. Olbrich P, Freeman AF. STAT1 and STAT3 Mutations: Important Lessons for Clinical Immunologists. Expert Rev Clin Immunol (2018) 14(12):1029–41. doi: 10.1080/1744666X.2018.1531704
6. Depner M, Fuchs S, Raabe J, Frede N, Glocker C, Doffinger R, et al. The Extended Clinical Phenotype of 26 Patients With Chronic Mucocutaneous Candidiasis Due to Gain-Of-Function Mutations in STAT1. J Clin Immunol (2016) 36(1):73–84. doi: 10.1007/s10875-015-0214-9
7. Okada S, Asano T, Moriya K, Boisson-Dupuis S, Kobayashi M, Casanova JL, et al. Human STAT1 Gain-Of-Function Heterozygous Mutations: Chronic Mucocutaneous Candidiasis and Type I Interferonopathy. J Clin Immunol (2020) 40(8):1065–81. doi: 10.1007/s10875-020-00847-x
8. Toubiana J, Okada S, Hiller J, Oleastro M, Lagos Gomez M, Aldave Becerra JC, et al. Heterozygous STAT1 Gain-of-Function Mutations Underlie an Unexpectedly Broad Clinical Phenotype. Blood (2016) 127(25):3154–64. doi: 10.1182/blood-2015-11-679902
9. Second J, Korganow AS, Jannier S, Puel A, Lipsker D. Rosacea and Demodicidosis Associated With Gain-of-Function Mutation in STAT1. J Eur Acad Dermatol Venereol (2017) 31(12):e542–4. doi: 10.1111/jdv.14413
10. Molho-Pessach V, Meltser A, Kamshov A, Ramot Y, Zlotogorski A. STAT1 Gain-of-Function and Chronic Demodicosis. Pediatr Dermatol (2020) 37(1):153–5. doi: 10.1111/pde.14011
11. Baghad B, Benhsaien I, El Fatoiki FZ, Migaud M, Puel A, Chiheb S, et al. [Chronic Mucocutaneous Candidiasis With STAT1 Gain-of-Function Mutation Associated With Herpes Virus and Mycobacterial Infections]. Ann Dermatol Venereol (2019) 147(1):41–5. doi: 10.1016/j.annder.2019.09.597
12. Saez-de-Ocariz M, Suarez-Gutierrez M, Migaud M, OF-R P, Casanova JL, Segura-Mendez NH, et al. Rosacea as a Striking Feature in Family Members With a STAT1 Gain-of-Function Mutation. J Eur Acad Dermatol Venereol (2020) 34(6):e265–7. doi: 10.1111/jdv.16241
13. Baghad B, El Fatoiki FZ, Benhsaien I, Bousfiha AA, Puel A, Migaud M, et al. Pediatric Demodicosis Associated With Gain-Of-Function Variant in STAT1 Presenting as Rosacea-Type Rash. J Clin Immunol (2021) 41(3):698–700. doi: 10.1007/s10875-020-00942-z
14. Shamriz O, Lev A, Simon AJ, Barel O, Javasky E, Matza-Porges S, et al. Chronic Demodicosis in Patients With Immune Dysregulation: An Unexpected Infectious Manifestation of Signal Transducer and Activator of Transcription (STAT)1 Gain-of-Function. Clin Exp Immunol (2021) 206(1):56–67. doi: 10.1111/cei.13636
15. Geoffroy V, Pizot C, Redin C, Piton A, Vasli N, Stoetzel C, et al. VaRank: A Simple and Powerful Tool for Ranking Genetic Variants. PeerJ (2015) 3:e796. doi: 10.7717/peerj.796
16. Forton FMN, De Maertelaer V. Rosacea and Demodicosis: Little-Known Diagnostic Signs and Symptoms. Acta Derm Venereol (2019) 99(1):47–52. doi: 10.2340/00015555-3041
17. Zhao YE, Wu LP, Peng Y, Cheng H. Retrospective Analysis of the Association Between Demodex Infestation and Rosacea. Arch Dermatol (2010) 146(8):896–902. doi: 10.1001/archdermatol.2010.196
18. Ciccarese G, Parodi A, Rebora A, Drago F. The Usefulness of Investigating the Possible Underlying Conditions in Rosacea. J Eur Acad Dermatol Venereol (2018) 32(3):e88–9. doi: 10.1111/jdv.14547
19. Vera N, Patel NU, Seminario-Vidal L. Rosacea Comorbidities. Dermatol Clin (2018) 36(2):115–22. doi: 10.1016/j.det.2017.11.006
20. Forton F, Germaux MA, Brasseur T, De Liever A, Laporte M, Mathys C, et al. Demodicosis and Rosacea: Epidemiology and Significance in Daily Dermatologic Practice. J Am Acad Dermatol (2005) 52(1):74–87. doi: 10.1016/j.jaad.2004.05.034
21. Sanchez-Viera M, Hernanz JM, Sampelayo T, Gurbindo MD, Lecona M, Soto-Melo J. Granulomatous Rosacea in a Child Infected With the Human Immunodeficiency Virus. J Am Acad Dermatol (1992) 27(6 Pt 1):1010–1. doi: 10.1016/s0190-9622(08)80268-x
22. Jansen T, Kastner U, Kreuter A, Altmeyer P. Rosacea-Like Demodicidosis Associated With Acquired Immunodeficiency Syndrome. Br J Dermatol (2001) 144(1):139–42. doi: 10.1046/j.1365-2133.2001.03794.x
23. Brutti CS, Artus G, Luzzatto L, Bonamigo RR, Balconi SN, Vettorato R. Crusted Rosacea-Like Demodicidosis in an HIV-Positive Female. J Am Acad Dermatol (2011) 65(4):e131–2. doi: 10.1016/j.jaad.2011.05.037
24. Vocks E, Engst R, Worret WI. [Exacerbation of Rosacea in HIV Infection]. Z Hautkr (1989) 64(6):452–4.
25. Scott C, Staughton RC, Bunker CJ, Asboe D. Acne Vulgaris and Acne Rosacea as Part of Immune Reconstitution Disease in HIV-1 Infected Patients Starting Antiretroviral Therapy. Int J STD AIDS (2008) 19(7):493–5. doi: 10.1258/ijsa.2008.008026
26. Aquilina C, Viraben R, Sire S. Ivermectin-Responsive Demodex Infestation During Human Immunodeficiency Virus Infection. A Case Report and Literature Review. Dermatology (2002) 205(4):394–7. doi: 10.1159/000066430
27. Redondo Mateo J, Soto Guzman O, Fernandez Rubio E, Dominguez Franjo F. Demodex-Attributed Rosacea-Like Lesions in AIDS. Acta Derm Venereol (1993) 73(6):437. doi: 10.2340/0001555573437
28. Hachfi W, Slama D, Ben Lasfar N, Mnif K, Bellazreg F, Fathallah A, et al. Demodicosis Revealing an HIV Infection. New Microbes New Infect (2019) 31:100525. doi: 10.1016/j.nmni.2019.100525
29. Cantarutti N, Claps A, Angelino G, Chessa L, Callea F, El Hachem M, et al. Multi-Drugs Resistant Acne Rosacea in a Child Affected by Ataxia-Telangiectasia: Successful Treatment With Isotretinoin. Ital J Pediatr (2015) 41:23. doi: 10.1186/s13052-015-0125-7
30. Kim JH, Chun YS, Kim JC. Clinical and Immunological Responses in Ocular Demodecosis. J Korean Med Sci (2011) 26(9):1231–7. doi: 10.3346/jkms.2011.26.9.1231
Keywords: STAT1 GOF, mutation, IL-17, rosacea, Demodex, demodicosis, inborn error of immunity, rosacea-like demodicosis
Citation: Martinot M, Korganow AS, Wald M, Second J, Birckel E, Mahé A, Souply L, Mohseni-Zadeh M, Droy L, Tarabeux J, Okada S, Migaud M, Puel A and Guffroy A (2021) Case Report: A New Gain-of-Function Mutation of STAT1 Identified in a Patient With Chronic Mucocutaneous Candidiasis and Rosacea-Like Demodicosis: An Emerging Association. Front. Immunol. 12:760019. doi: 10.3389/fimmu.2021.760019
Received: 17 August 2021; Accepted: 15 November 2021;
Published: 20 December 2021.
Edited by:
Antonio Condino-Neto, University of São Paulo, BrazilCopyright © 2021 Martinot, Korganow, Wald, Second, Birckel, Mahé, Souply, Mohseni-Zadeh, Droy, Tarabeux, Okada, Migaud, Puel and Guffroy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martin Martinot, bWFydGluLm1hcnRpbm90QGNoLWNvbG1hci5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.