 Sriram Kumar1,2
Sriram Kumar1,2 Duygu Merve Çalışkan1,2
Duygu Merve Çalışkan1,2 Josua Janowski1,3Aileen Faist1,4Beate Claudine Gisela Conrad1
Josua Janowski1,3Aileen Faist1,4Beate Claudine Gisela Conrad1 Julius Lange1
Julius Lange1 Stephan Ludwig1,2,4,5
Stephan Ludwig1,2,4,5 Linda Brunotte1,5*
Linda Brunotte1,5*- 1Institute of Virology, University of Münster, Münster, Germany
- 2EvoPAD Research Training Group 2220, University of Münster, Münster, Germany
- 3SP BioSciences Graduate Program, University of Münster, Münster, Germany
- 4CiM-IMPRS Graduate Program, University of Münster, Münster, Germany
- 5Interdisciplinary Centre for Medical Research, University of Münster, Münster, Germany
Since November 2019 the SARS-CoV-2 pandemic has caused nearly 200 million infection and more than 4 million deaths globally (Updated information from the World Health Organization, as on 2nd Aug 2021). Within only one year into the pandemic, several vaccines were designed and reached approval for the immunization of the world population. The remarkable protective effects of the manufactured vaccines are demonstrated in countries with high vaccination rates, such as Israel and UK. However, limited production capacities, poor distribution infrastructures and political hesitations still hamper the availability of vaccines in many countries. In addition, due to the emergency of SARS-CoV-2 variants with immune escape properties towards the vaccines the global numbers of new infections as well as patients developing severe COVID-19, remains high. New studies reported that about 8% of infected individuals develop long term symptoms with strong personal restrictions on private as well as professional level, which contributes to the long socioeconomic problems caused by this pandemic. Until today, emergency use-approved treatment options for COVID-19 are limited to the antiviral Remdesivir, a nucleoside analogue targeting the viral polymerase, the glucocorticosteroide Dexamethasone as well as neutralizing antibodies. The therapeutic benefits of these treatments are under ongoing debate and clinical studies assessing the efficiency of these treatments are still underway. To identify new therapeutic treatments for COVID-19, now and by the post-pandemic era, diverse experimental approaches are under scientific evaluation in companies and scientific research teams all over the world. To accelerate clinical translation of promising candidates, repurposing approaches of known approved drugs are specifically fostered but also novel technologies are being developed and are under investigation. This review summarizes the recent developments from the lab bench as well as the clinical status of emerging therapeutic candidates and discusses possible therapeutic entry points for the treatment strategies with regard to the biology of SARS-CoV-2 and the clinical course of COVID-19.
SARS-CoV2 Replication Cycle
Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) is a positive-sense, single-stranded RNA virus that belongs to the lineage β-coronavirus-2b the family Coronaviridae and the order Nidovirales (1). The name coronavirus is derived from the crown-like appearance of the spike proteins of the virus particles under an electron microscope. The viral genome measures approximately 30 kb, and contains fourteen Open Reading Frames (ORF) coding for twenty-seven viral proteins, some of which are not-yet functionally characterized. The virion consists of four structural proteins: Spike (S), Envelope (E), Membrane (M), and Nucleocapsid (N). The S protein, located on the virion surface, primarily binds to the cell-surface receptor Angiotensin Converting Enzyme 2 (ACE2). Due to its strong antigenicity and indispensable role during virus entry, the S protein serves as a target for antiviral treatments and vaccine design. It contains two functional subunits: The S1 subunit binds to and interacts with the cell-surface receptors, while the S2 subunit mediates membrane fusion (2, 3). Alongside S protein binding, cleavage of S proteins at the polybasic cleavage-sites by the membrane-associated Transmembrane Protease Serine 2 (TMPRSS2) and the lysosomal cysteine protease Cathepsin-L facilitates membrane-fusion and virus entry at the cellular endosomes (4, 5). The released viral genomic RNA (gRNA), which carries a cap-structure and a polyA-tail, serves as a direct template for the cellular ribosome-mediated translation of the two large ORFs: ORF1a and ORF1b. The polyprotein products pp1a and pp1ab are independently cleaved by the viral proteases nsp3 and nsp5, which are also prominent drug targets, and post-translationally processed into sixteen non-structural proteins (nsps). Of these sixteen nsps, nsp12 assembles the other nsps to constitute the viral replication-transcription machinery, and also confers catalytic activity to the RNA-dependent RNA polymerase (RdRp), which then catalyzes genome replication and RNA processing (6). The encapsidated progeny gRNAs are then assembled into viral particles in the Endoplasmic Reticulum (ER)-Golgi complex, together mediated by the membrane proteins. The fully assembled virus particles then bud out of the ER-Golgi complex and are released out of the host-cell by membrane exocytosis.
COVID-19 Clinical Manifestation
SARS-CoV-2 is mainly transmitted by aerosols and infects the cells in the upper respiratory tract (7). However, depending on the viral load, replication speed and local immune response, it is further disseminated to the lower respiratory tract and other organs within days or weeks post infection, by which it is reported to cause severe damage to lungs, stomach, intestine, kidney, heart, blood vessels, liver, brain and skin (8–10). Early symptoms appear after an incubation period of 1-14 days but many infected individuals can remain asymptomatic despite high viral loads, which promotes viral transmission even before the clinical diagnosis of positive infection. Most common early symptoms include fever, dry cough, myalgia, fatigue, and loss of smell and taste. In addition, some patients manifest sputum production, hemoptysis, headache, sore throat, chest pain and gastrointestinal symptoms like diarrhea, nausea and vomiting (7, 11, 12). Dyspnea and pneumonia can develop in a median time span of eight days after symptom onset. In laboratory examinations, leukopenia, lymphopenia, anemia, thrombocytopenia, elevated ferritin and d-dimer level such as an elevated CRP, which were recognized to correlate with severity. Likewise, elevated plasma concentrations of pro-inflammatory cytokines IL-2, IL-6, IL-7, IL-10, GCSF, IP10, MCP1, MIP1A, and TNF-α are predictive for a severe outcome (11, 13). Due to the lack of wide-spread pre-existing adaptive immunity towards the newly emerged zoonotic SARS-CoV-2 virus, the human innate immune response poses the first critical barrier against the infection and is an important determinant of the disease trajectories.
In general, the immune response to SARS-CoV-2 infection can be broadly described in three phases (14). The early phase is predominated by virus replication in the upper respiratory epithelium, but also involve the intestinal epithelium and vascular endothelium, due to the high expression of ACE2 receptors in these linings (15, 16). This phase is often accompanied by mild respiratory and systemic symptoms. The quality and potency of the induced early immune response is critical in this phase and decisive for further disease development. The second phase is characterized by both, viral replication and development of lung inflammation with massive recruitment of cytokine-expressing immune cells to the site of infection. Patients often experience first signs of hypoxia and are admitted to hospital during this phase. The third phase describes severe COVID-19 and is specified by systemic hyper-inflammation with high blood levels of inflammatory cytokines. The systemic involvement causes symptoms like septic shock, respiratory failure, cardiopulmonary collapse and may even lead to multi-organ dysfunction and death (11).
Even though all age groups can be infected by SARS-CoV-2, particularly elderly patients have an increased risk of mortality. Comorbidities such as obesity, hypertension, chronic obstructive pulmonary diseases (COPD), diabetes, cardiovascular and cerebrovascular diseases have been reported as risk factors for severe COVID-19 (10, 17). These patients required more intensive care and experienced more often complications like Acute Respiratory Distress Syndrome (ARDS), coagulation dysfunction, sepsis, and death (10–12, 18). Additionally, immunosuppressed patients as well as cancer patients have been reported as a highly vulnerable group due to low protective antibody responses (19, 20).
Clearly, these dynamics in viral replication and immune activation as well as the patient’s individual constitution require specified therapeutic strategies that are aligned to the disease phase and time of treatment onset. Here, we summarize the current state of development and experiences from first in-human applications of the many antiviral and immunomodulatory drugs that are under investigation in single or combinatorial approaches for the treatment and prevention of COVID-19.
Direct-Acting Antivirals (DAA)
According to their essential enzymatic functions for the replication of SARS-CoV-2, the S protein, the viral polymerase as well as the viral proteases are the most prominent targets for diverse virus-targeting antiviral strategies.
Umifenovir
Umifenovir (Arbidol) has been previously applied against some enveloped and non-enveloped viruses especially Influenza A and B, and recently against hepatitis C virus (HCV) (21). Although the mechanism of action of Umifenovir is not exactly understood, it was suggested to inhibit trimerization of the SARS-CoV-2 S protein (22). Molecular simulations indicated that it stabilizes the RBD-ACE2 complex, thus limiting conformational rearrangements associated with membrane fusion and virus entry (23). While some clinical studies showed that Umifenovir positively affects patient recovery and mortality, other studies reported that treatment of patients not requiring intensive care does not show different results than the control group in terms of recovery and virus clearance (24–26). A study comparing Arbidol and Lopinavir/ritonavir (LPV/r) treatments reported that Arbidol had a significantly positive effect on clinical and laboratory improvements on COVID-19 patients (24, 25). Another study comparing Arbidol and LPV/r combined therapy with LPV/r therapy alone shows that the group receiving the combination therapy was associated with a higher rate of coronavirus test negative conversions rate on day 7 (combination group %75, control group %35) and on day 14 (combination group %94, control group %52,9) and significant improvement in chest CT scans (combination group %69, control group %29) at day 7 (24, 25). In contrast, a meta-analysis of 137 reports on the efficacy and safety concludes that Umifenovir is safe, led to higher negative PCR rates after 14 days but had no positive effects on patient recovery (27). Despite these contradictory results, further combinatorial studies with different antivirals and interferons (IFN) are planned (Clinical study identifier: NCT04350684, NCT04273763).
Clofazimine
Clofazimine is an orally available and FDA (Food and Drug Administration)-approved anti-leprosy drug and has been shown to reduce SARS-CoV-2 infection by inhibiting spike-dependent cell fusion and the activity of the viral helicase in many in vitro, ex vivo and in vivo systems (28). Interestingly, it demonstrated synergistic antiviral activity in combination with Remdesivir. A Phase-II clinical trial (NCT04465695) is ongoing, evaluating dual therapy with Clofazimine and IFN-β1b for treatment of hospitalized COVID-19 patients in China.
Convalescent Sera and Monoclonal Antibodies
Like for other virus infections, the therapeutic value of convalescent sera that contain neutralizing antibodies to SARS-CoV-2 was evaluated. Although early clinical studies demonstrated improvement of symptoms and viral clearance within an average of 5-6 days in patients receiving convalescent plasma treatment (29–32), results from recent large-scale trials, such as the RECOVERY Collaborative Group, report the absence of positive outcomes (33, 34). With respect to the general associated risks of convalescent plasma therapy regarding blood product transfusion (e.g. blood-borne infections, allergic reactions), transfusion-related acute lung injury and the potential for antibody-dependent infection enhancement (ADE), this treatment option is considered with care (35). Importantly, convalescent sera treatment of immunosuppressed patients with chronic SARS-CoV-2 infections resulted in the evolution of virus variants with immune escape mutations (36). Similar problems occurred during treatment of patients with mild to moderate COVID-19 with the monoclonal antibody Bamlavinimab that targets the S protein Receptor Binding Domain (RBD) and was given Emergency Use Authorization (EUA) in November 2020. However, due to complications and rapid resistance development, the EUA was withdrawn in April 2021 (FDA News release, April 2021). More promising is the use of monoclonal antibody cocktails. Combination of Bamlanivimab and Etesevimab, which are both human immunoglobulin G1 (IgG1) kappa antibodies that target different epitopes of the SARS-CoV-2 spike protein (37, 38) showed a significant decrease in viral load in nose and upper respiratory tract on the 11th day post treatment in a randomized Phase-II study performed with 577 mild/moderate COVID-19 patients (39). The combination was given EUA by the FDA for the use in patients with a high risk of developing severe COVID-19. Also, the European Medicines Agency (EMA) initiated a rolling review process for approval.
Another antibody cocktail named REGN-COV2 contains the two non-competing neutralizing antibodies Casirivimab and Imdevimab, both targeting the S protein RBD (40). Results from a clinical study with 275 patients showed that REGN-COV2 reduced viral loads with a greater effect in patients whose immune response was not yet initiated or had a high initial viral load. No side effects were seen and its use was considered safe (41). In addition, recent clinical trials tested use of REGN-COV2 for preventive treatment. This demonstrated 73% protection of household contacts from symptomatic infections (NCT04452318). Another approach is based on an engineered, double acting recombinant human antibody VIR-7831 (Sotrovimab). This engineered antibody is derived from a parental antibody (S309) that was isolated from the memory B cells of a SARS-CoV-2 survivor. Sotrovimab targets a highly conserved glycan in the S protein that is part of a region not competing with ACE2 binding and does not cover any of the reported positions that are mutated in the current SARS-CoV-2 variants of concern. To improve serum half-life and mucosal distribution, Sotrovimab contains several modifications in the Fc region. In addition, VIR-7832, which is otherwise identical to VIR-7831, contains a GAALIE mutation to promote the induction of CD8+ T-cells during viral respiratory infections. Importantly, both antibodies demonstrated efficient neutralization of SARS-CoV-2 including the Alpha, Beta and Gamma variants in the context of a VSV-pseudotype model (42). EUA application was filed to the FDA for VIR-7831 in March 2021 according to the observed 85% reduction of hospitalization or death in Phase-III clinical trials and EMA has started a rolling review for treatment of patients with mild to moderate COVID-19, which do not require oxygenation but are at risk to develop severe disease. In addition, VIR-7831 is currently investigated in a randomized multi-centre Phase-II/III clinical study for treatment of mild COVID-19 in outpatients (NTC04545060).
Human Recombinant Soluble ACE2 (hrsACE2)
ACE2 is the major receptor for SARS-CoV-2 and a regulator of the renin-angiotensin system that protects many tissues, including the lung, from injuries and has a role on blood pressure regulation and electrolyte homeostasis. Because of these functions, it is seen as a good therapeutic candidate for COVID-19 by using it as a decoy receptor and immune regulator (43, 44). A soluble version of the human ACE2 protein (hrsACE2, APN01) reduces the SARS-CoV-2 viral load 1000-5000- fold in cell cultures and shows an inhibitory effect on cell attachment in human blood vessel and kidney organoids. In addition, the combination therapy with Remdesivir and human soluble ACE2 reduced the dose of Remdesivir and human ACE2 required for treatment, as it inhibited both, the binding of the virus to the cell and its replication (45). Clinical studies confirmed safety and tolerability of hrsACE2 and demonstrated clinical benefits, such as more ventilation-free days and reduced RNA loads (NCT00886353, NCT01597635) (NCT04335136) (45). Based on these positive outcomes it was announced that APN01 will be included in the large-scale NIH-funded ACTIV Phase-II clinical trial (ACTIV-4d RAAS). Furthermore, combination of recombinant soluble human ACE with Remdesivir was shown to enhance its antiviral effects in vitro (46). An alternative approach utilizes the therapeutic molecule obtained by binding the human Fc region to the ACE2 receptor by antibody engineering techniques (47). Fusion of the human IgG Fc moiety to the ACE2 ectodomain moiety results in an extended half-life. A version of ACE2 IgG1 Fc is currently evaluated in a Phase-I clinical trial. Developing this therapeutic candidate, it has been optimized with IgG4-Fc to facilitate Fc receptor activation and prevention of antibody-dependent disease development (48).
Remdesivir
Remdesivir is metabolized in host cells to form a nucleoside triphosphate that competes with ATP for incorporation into progeny viral RNA by the viral polymerase (4) and has proven effectiveness against coronaviruses in vitro and in vivo (49–51). Studies of the ACTT-1 trial (NCT04280705) showed that Remdesivir shortens the recovery time (median 11 days compared to 15 days in the placebo group) (52, 53) of ventilated COVID-19 patients and was granted EUA for use in severe COVID-19 patients in the US and the EU. Considering the results of other clinical studies, FDA gave full approval of Remdesivir for COVID-19 treatment a few month later in the US (52–54). However, the WHO SOLIDARITY study reported that Remdesivir had little or no effect on the length of hospitalization, transition to ventilation, or overall mortality and recommended against the use of it for COVID-19 treatment (55). In line with this study, in patients with mild to moderate COVID-19 without respiratory support, Remdesivir does not provide a significant benefit but can shorten the recovery time in patients with an early diagnosis (≤10 days) (56). Despite the controversial results of the available clinical trials, Remdesivir is widely used as standard care in combination with dexamethasone for critically ill COVID-19 patients (56). Further clinical studies evaluating time of application, effect on comorbidities and diverse drug combination are still ongoing.
Favipiravir
Favipiravir is a prodrug and acts by transforming into a metabolite of ribofuranosyl 5’triphosphate (57) that inhibits viral RNA polymerases (58, 59). It is effective against many RNA viruses such as Lassa, Marburg and Nipah virus, and is approved for the treatment of influenza in Japan (60). Many clinical studies have assessed the effectiveness of Favipiravir for treatment of COVID-19 and it was approved in several countries. However, data availability of the results of these studies is difficult preventing proper meta-analysis (61). Previous studies reported teratogenicity and embryotoxicity in different study models, thus use in pregnant women should be avoided (60, 62). Clinical studies in patients with mild and moderate COVID-19, comparing Favipiravir, Umifenovir and LPV/r treatments have shown that time of viral clearance and recovery of radiological findings are faster in patients using Favipiravir (63, 64). In a clinical study investigating the effectiveness of chloroquine and Favipiravir, no significant difference was found between the two drugs (65). Currently, clinical studies for at-home medication are underway within the PRINCIPLE trial (66).
Molnupiravir
Molnupiravir (MK-4482) is an orally available nucleoside analogue with similar mechanism to Favipiravir and inhibits effectively SARS-CoV-2 in in vitro and in vivo (67, 68). It is currently evaluated in Phase-II/III trials for outpatients and inpatients with COVID-19 (NCT04405739, NCT04405570, NCT04575584). In combination with Favipiravir in hamster models of SARS-Cov-2, Molnupiravir was able to reduce the viral load in the lungs of infected hamsters by approximately 5 log10 (68, 69). Molnupiravir increased the frequency of mutations in MERS-CoV viral RNA in infected mice, and in the SARS-Cov-2 treatment study, the number of these mutations in the Molnupiravir/Favipiravir combination group was found to be significantly higher than that in the highest dose group of Molnupiravir alone. These results indicate a similar mode of action for the marked decrease in infectious viral loads observed in the combination therapy group for SARS-CoV-2 (68).
Lopinavir/ritonavir (LPV/r)
LPV/r is a broad-spectrum protease inhibitor used in the treatment of AIDS. Due to its low bioavailability when taken orally, it is used in combination with the pharmacokinetic enhancer ritonavir. LPV/r is supposed to target the SARS-CoV-2 C-like proteinase (3CLpro) substrate binding site, which is highly conserved among all coronaviruses (69). Despite this expected broad-spectrum effect, clinical studies have not shown a significant difference in clinical improvement between patients receiving standard therapy with/without LPV/r or Umifenovir (70, 71). Although the results have reduced the trust in LPV/r therapy, other studies reported that adding ribavirin and IFN-β1b to LPV/r therapy results in faster recovery and virus clearance in SARS-CoV-2 patients (72, 73). Most patients using LPV/r experienced non-serious side effects (mostly gastrointestinal problems). However, it has been reported in clinical studies that some patients were unable to continue treatment due to serious side effects (74). In addition, it is known that it may cause hypertriglyceridemia, hypercholesterolemia, pancreatitis, hepatotoxicity and cardiac problems. The use of LPV/r, especially with drugs that prolong the QT interval (time from the start of a Q wave to the end of the next T wave in an electrocardiogram), which describes the time taken by the cardiac ventricles to depolarize and repolarize, is one of the important issues to be considered (75).
Host-Directed Antivirals (HDA)
All viruses, including SARS-CoV-2, exploit the host cell resources to replicate and ensure transmission to other hosts. Virus-host interactions occur at all stages of the viral life cycle and provide numerous factors that are crucial for virus survival and therefore may represent targets for antiviral approaches. A major advantage of targeting the host rather than the virus is the low risk of resistance development and the high potential of broad use against other pathogens that rely on related cellular proteins or processes.
(Hydroxy-) Chloroquine
Huge efforts have been taken to systematically screen existing drug libraries in order to find treatments for COVID-19 (76). This revealed a number of repurposed candidates such as (Hydroxy-) Chloroquine (HCQ), which has previously shown beneficial effects in the treatment of malaria and autoimmune diseases and displayed controversially discussed antiviral properties against HIV and SARS-CoV (77). HCQ increases the pH of cellular endosomes and vacuoles and thereby affects the activity of many enzymes, including Cathepsin L, which is needed to mediate cleavage of the SARS-CoV-2 S protein, followed by membrane fusion and release of the viral genome into the host cell (78, 79). Even though chloroquine exhibited antiviral effects against both SARS-CoV and SARS-CoV-2 in vitro, and also in mice using the common-cold corona virus OC43 (80–83), all clinical trials failed to protect patients from severe COVID-19 (84–86). This discrepancy might be explained by the dependency of SARS-CoV-2 on another protease, namely TMPRSS2, which is important for virus entry and remains unaffected by HCQ (79). Due to the lack of efficacy, the FDA revoked the EUA for HCQ in June 2020 (87).
Camostat and Nafamostat
Direct targeting of the host cell protease TMPRSS2, which cleaves and thus activates the S protein (88, 89), Camostat mesylate or its active metabolite 4-(4-guanidinobenzyloxy)phenylacetic acid (GBPA) demonstrated efficient antiviral activity against SARS-CoV and SARS-CoV-2 in vitro (4, 90). Currently, Camostat, which is approved in Japan for the treatment of chronic pancreatitis, is evaluated in diverse international clinical trials of all phases for the treatment of hospitalized and non-hospitalized COVID-19 patients in various disease stages and comorbidities for single or combination treatments with other drugs (NCT04455815, NCT04321096) (91).
In a comparative in vitro study with Nafamostat mesylate, another protease inhibitor targeting TMPRSS2, inhibition of SARS-CoV-2 entry was 15-fold higher compared to treatment with Camostat mesylate. In addition, Nafamostat mesylate showed higher inhibition of SARS-CoV-2 infection in vitro (92). Several Phase-II/III clinical trials with Nafamostat mesylate for treatment of hospitalized COVID-19 patients are currently ongoing (NCT04352400, NCT04473053, NCT04623021). However, whether the required concentrations of these inhibitors can be attained in the human lung remain to be determined (93). Nevertheless, these studies demonstrate that targeting the main host proteases involved in the virus lifecycle provides a promising approach to inhibit viral replication and thus have initiated numerous studies that aim to characterize host protease in various stages of virus infection, as reviewed previously (94, 95).
Fluoxetine
Recently, the therapeutic effect of Functional Inhibitors of Acid Sphingomyelinase (FIASMA) such as the antidepressant Fluoxetine to inhibit SARS-CoV-2 cell entry has been investigated by several groups. This revealed, that Fluoxetine treatment efficiently reduced viral entry and replication without cytotoxic effects in vitro (96, 97). A follow-up study further showed pronounced drug synergism of Fluoxetine and Remdesivir, thereby providing additional therapeutic options for COVID-19 treatment (98). In addition to endolysosomal acidification, Fluoxetine was shown to disrupt the NFkB/IL-6 axis, which is associated with cytokine-induced pathologies during COVID-19 (99). On this basis, a pharmacokinetic study estimated efficient inhibition of SARS-CoV-2 at a commonly well-tolerated concentration of Fluoxetine used for treatment of depression (100). A retrospective observational study investigated a potential beneficial effect of anti-depressant intake, including Fluoxetine, during COVID-19. The results indicated a significant reduction in the risk of intubation and death in hospitalized COVID-19 patients (101). Furthermore, an ongoing Phase-IV clinical trial investigates the potential of Fluoxetine treatment to reduce intubation and death from SARS-CoV-2 infection (NCT04377308).
Plitidepsin
For translation of viral proteins, SARS-CoV-2 relies on the host cellular translation machinery. Recently, a well-described inhibitor of the eukaryotic translation elongation factor 1 alpha (eEF1A), called Plitidepsin (Brandname: Aplidin) was discovered and characterized to have potent antiviral effects against SARS-CoV-2 (102–104). Intriguingly, Plitidepsin inhibited virus infections more efficient than Remdesivir by a factor of 27.5 in vitro. Moreover, SARS-CoV-2 titers in lungs of mice expressing human ACE2 were significantly reduced upon prophylactic treatment with Plitidepsin, facilitated by eEF1A inhibition (105). Furthermore, it exhibits antiviral potential against the SARS-CoV-2 Alpha variant (106). Plitidepsin has originally been developed for the treatment of multiple myeloma (103). Interestingly, in earlier studies with myeloma patients, Plitidepsin has also been used in combination with the anti-inflammatory drug dexamethasone (107). This provides already existing data for drug tolerance in combination therapies of dexamethasone and Plitidepsin in COVID-19 patients as well. However, EMA refused marketing authorization of Plitidepsin as an anti-cancer medication twice, in 2017 and 2018. The safety and tolerability of Plitidepsin was recently evaluated in COVID-19 patients in a Phase-I trial (NCT04382066) but results have not been released yet. In addition, a Phase-III trial for use of Plitidepsin in patients with moderate COVID-19 was filed but not yet started (NCT04784559).
MEK Inhibitor ATR-002
Host kinases represent another group of cellular targets against SARS-CoV-2 infection (108). The RAF/MEK/ERK-signaling cascade is known to be a central pathway involved in virus replication of several RNA viruses, including influenza, RSV and coronavirus (109–112). Previous studies using the MEK inhibitor ATR-002 demonstrated reduced influenza viral titers by preventing export of viral ribonucleoprotein complexes during the viral infection cycle (109, 113). Moreover, there are indications that treatment with ATR-002 reduced cytokine expression, such as TNF-α, IL-1β, and IP-10 in vitro and in vivo and thereby could help to counteract or rebalance the SARS-CoV-2 induced hyperactivation of the immune response (114). A Phase-I clinical trial demonstrated that ATR-002 is safe and very well tolerated in humans with little or no drug related side effects (NCT04385420). Currently, ATR-002 is tested in a Phase-II clinical trial RESPIRE for treatment of COVID-19 (NCT04776044).
Ivermectin
Ivermectin is an antiparasitic drug that has been used for years, thus providing well described pharmacokinetic data, is readily available and quite inexpensive. Even though several studies demonstrated promising positive aspects of Ivermectin treatment (115), being anti-inflammatory properties (116), prophylaxis treatment (NCT04668469), inhibition of virus replication (117), and patient survival (118), Ivermectin is not recommended as a COVID-19 drug by the FDA, EMA, and WHO. This is mainly explained by methodological limitations of various studies such as small sample sizes, the use of concomitant medications and controversial data (119). Further studies showed that up to 100-fold higher concentrations will be needed to achieve a concentration necessary for an antiviral effect (120). To finally clarify whether Ivermectin has beneficial effects in COVID-19 treatment the University of Oxford announced to add Ivermectin to the PRINCIPLE trial.
Emerging Drug Candidates
Besides large drug screens, many research groups focused on the identification of novel virus-host interactions using genome wide-CRISPR/Cas screens (121–124). This revealed several factors that play a central role in various host pathways during infection, such as the cholesterol and phosphatidylinositol pathway, inflammatory signaling, cell cycle regulation or PML nuclear body formation and might represent new targets for antiviral approaches. One of the most prominent targets identified was the lysosomal transmembrane protein TMEM106B. Upon knock out (KO), SARS-CoV-2 replication was impaired (121). Consistent with this finding another research group further found TMEM106B expression to be induced during SARS-CoV-2 infection in patients and suggested a role of TMEM106B in virus entry (125). Another top-ranked protein was the membrane trafficking factor Rab7A. Knockout of Rab7A resulted in the sequestration of the SARS-CoV-2 receptor molecule ACE2 inside the cell and thereby led to reduced viral entry (121). In the light of emerging mutations that potentially reduce vaccine efficacy and the lack of specific antiviral therapeutics against SARS-CoV-2, these studies lay the ground for broadly active antivirals in the future.
Interferons
IFNs are host cell-secreted signaling molecules that stimulate the concerted expression of antiviral restriction factors in infected and neighboring cells in an autocrine or paracrine manner, to restrict replication and prevent transmission of the invading pathogens. As other viruses, SARS-CoV-2 also antagonizes IFN-induction in infected cells, thereby calling for exogenous IFN-administration as a therapeutic strategy, which is already being exploited for treating diverse virus infections (126, 127). IFNs exist in three different types: Type-I, Type-II and Type-III, with distinct biological and antiviral properties. Despite its potential to antagonize IFN-induction, SARS-CoV-2 intriguingly demonstrates remarkable sensitivity towards lower doses of exogenous IFNs (128, 129), suggesting that early therapeutic application, and possibly prophylaxis with IFNs could be clinically promising. Thus, already early in the pandemic, the therapeutic potential of exogenous IFNs, mostly in combination with other treatments, was subject to clinical investigations.
Type-I IFNs
Although many clinical studies have investigated the benefits of type I IFNs for the treatment of SARS-CoV-2 infections and COVID-19, the outcomes were highly diverse. This is facilitated by the differences in the study design, involving combinations with diverse other treatments as well as the selection of individual therapeutic entry points during the disease course, which strongly affect the antiviral actions of IFNs.
Two open-labelled trials assessed the efficacy of cotherapy of IFN-β1b (NCT04276688) or IFN-β1a (IRCT20151227025726N12) with LPV/r on mild-moderate COVID-19 hospitalized patients. The multicentre trial reported that the early triple cotherapy involving systemic administration of IFN-β1b with LPV/r was superior and safe compared to LPV/r alone, in attenuating the disease symptoms, and in reducing the clinical duration of viral shedding and hospital admission (73). Similarly, another single-centre retrospective trial (IRCT20151227025726N12) also reported favourable clinical outcomes of systemic IFN-β1a-addition with standard medications (LPV/r) and stated that although the mortality rates of the two groups were comparable, multivariate analysis showed that not-receiving IFN-β1a was significantly associated with all-cause mortality, alongside others factors like comorbidities and non-invasive ventilation (130), further corroborating the clinical benefits of early systemic IFN-β1b administration in cotreatment settings.
Only two associated clinical trials were performed on severe COVID-19 patients to assess the clinical benefits of IFN-β as therapeutic additive to standard medications (HCQ plus LPV/r or atazanavir/ritonavir) and reported favorable clinical outcomes. The trial administering IFN-β1b (IRCT20100228003449N27) reported that the test group had a shorter time to clinical improvement and discharge day and a lower 28-days mortality rate than the control group not receiving IFN-β1b (131). Although the other trial (IRCT20100228003449N28) reported that addition of IFN-β1a did not significantly accelerate the time to clinical improvement, it significantly accelerated the hospital discharge rate to day-14, lowered the 28-days mortality rate, and also improved the survival rates when administered during the early phase of the disease (132). In contrast to systemic administration, two clinical trials evaluated the therapeutic benefits of administering nebulized IFN early during mild COVID-19 and reported clinical benefits. An uncontrolled exploratory study found that nebulized IFN-α2b, alone or combined with Arbidol, reduced the time of quantifiable virus in the upper respiratory tract and reduced the duration of elevated inflammatory markers like IL-6 and CRP in the blood (133). In line with this, the multi-center trial (NCT04385095) on moderate hospitalized and ambulatory patients reported that nebulized IFN-β1a favored faster recovery than the control group, quantified based on the WHO Ordinal Scale for Clinical Improvement (OSCI) (134).
The timing of IFN-administration is likely a strong influential factor on the disease trajectory of COVID-19. Therefore, a retrospective multicenter cohort study carried-out in COVID-19 patients investigated the association between the timing of IFN-α2b administration with its clinical outcomes through regression analysis (135). Importantly, the study found that early administration was significantly associated with reduced in-hospital mortality and confers positive clinical outcomes. Similarly, a single-center retrospective-cohort clinical trial evaluated the therapeutic potency of IFN-β1b administration on moderate/severe pneumonia-positive hospitalized COVID-19 patients. The study reported that IFN-β1b-treatment did not significantly decrease in-hospital mortality at this disease stage, highlighting that IFN administration in the later stages of disease progression would have minimal to no significant clinical benefits (136). While several smaller clinical trials have reported mixed results based on diverse primary and secondary outcomes on the therapeutic benefits of IFN administration in single or cotreatment regimens in mild-moderate as well as on severe hospitalized and ambulatory patients, the WHO SOLIDARTY Consortium Trial is the largest clinical trial till-date that evaluated the therapeutic effects of IFN-β1a administration (and other drugs including HCQ, Remdesivir and LPV) in several thousand COVID-19 patients. The interim results from their multicenter trial at 405 hospitals in 30 countries conclude that there are no beneficial effects of IFN-administration, in terms of reducing in-patient mortality, initiation of mechanical ventilation, or hospitalization duration (Interim Results of WHO Solidarity Consortium Trial, Feb 2021).
Although more Type I IFNs exist in humans, currently only IFN-β (IFN-β1a and IFN-β1b) and IFN-α2 (IFN-α2b) as well as some engineered forms of IFNs are of clinical relevance. However, recent studies investigated the activity against SARS-CoV-2 of all twelve existing IFN-α subtypes, and demonstrated highly efficient and subtype-specific antiviral properties (137, 138), which strongly emphasizes that IFN-α subtypes should be included in clinical investigations in order to increase our IFN-therapeutic arsenal.
Type-III IFNs
Encouraged by the preclinical evidences on the inhibitory potential of IFN-λ1 on SARS-CoV-2 replication in vitro and in vivo (139, 140), two Phase-II clinical trials evaluated the therapeutic efficacy of single-dose subcutaneous administration of pegylated (peg) IFN-λ1a in ambulatory uncomplicated COVID-19 patients. While the COVID-LAMBDA trial (NCT04331899) reported that the treatment regimen neither reduced the duration of virus shedding, nor alleviated disease symptoms (141), the ILIAD trial (NCT04354259) reported that the treatment regimen significantly accelerated virus clearance as quantified by qRT-PCR of SARS-CoV-2 vRNA in nasopharyngeal swabs, concluding that peg-IFN-λ1a administration has therapeutic benefits to shorten virus shedding and prevent clinical progression (142). Currently ongoing trials aim to further evaluate the therapeutic efficacy of single dose (NCT04343976) or double-dose (NCT04534673 and Phase-IIb of NCT04354259) subcutaneous administration of peg-IFN-λ1a in hospitalized moderate COVID-19 patients, in terms of clinical time to reach negative qRT-PCR outcome, mortality rate and recovery period. Results from these trials would likely throw light for choosing optimal treatment regimen to achieve favorable clinical outcomes in hospitalized patients.
Other IFNs
Several clinical trials investigated the therapeutic benefits of other non-conventional IFN subtypes. For instance, a non-randomized clinical trial (ChiCTR2000030262) on mild COVID-19 patients tested the therapeutic efficacy of aerosol inhalation of IFN-κ with Topical Trefoil Factor Family-2 (TFF2), which is a peptide isoform demonstrating proven therapeutic benefits against gastrointestinal disorders associated with mucosal damage (143). This treatment regimen significantly improved clinical outcomes, including cough-relief, CT-imaging, and vRNA negativity, altogether favoring an early discharge from hospitalization (144). Another Phase-II clinical trial (ChiCTR2000029638) was conducted on moderate to severe COVID-19 patients to evaluate the safety and efficacy of Recombinant Super-Compound Interferon (rSIFN-co) versus traditional nebulized IFNα-2b, alongside standard antivirals (LPV/r or Umifenovir) (145). The trial observed that co-treatment with rSIFN-co was safer and more efficacious than traditional IFNα-2b for treating moderate to severe COVID-19, warranting further clinical trials of rSIFN, alone or in combination with other antiviral agents.
While the concept of cotreatment classically revolves around the use of two different drugs, or currently with a drug combined with an IFN-type, to accomplish improved clinical benefits at lower doses of the individual agents, encouraging results came out of clinical trials evaluating combinations of two different IFN types. For instance, based on the synergic inhibition of SARS-CoV-2 replication by type-I and type-II IFN combinations (146–149), a controlled clinical trial was conducted to assess the efficacy and safety of subcutaneous IFN-α2b and IFN-γ coadministration along standard medication (LPV/r), in SARS-CoV-2-positive hospitalized patients (150). The trial reported that IFN-α2b+IFN-γ cotreatment eliminated the virus earlier than IFN-α2b standalone treatment, although the latter also demonstrated appreciable efficacy for SARS-CoV-2 treatment.
IFN Prophylaxis
While several trials evaluated the therapeutic benefits of IFN administration, preliminary trials are also being deployed on a prophylactic setting to prevent infections. Inspired by the preclinical studies on the high maintenance of IFN concentration as nasal droplets (129, 151), a prospective open-label clinical trial (NCT04320238) evaluated the prophylactic administration of recombinant human IFN-α (rhIFNα) nasal droplets on medical staff in Hubei, China. From the trial the authors concluded that prophylactic application was remarkably effective in preventing COVID-19 in medical staff that are at a high risk of acquiring infection, which was confirmed by negative pulmonary CT scans and the absence of other clinical symptoms (152). Along the same line, the PROTECT Trial (NCT04344600) currently evaluates the prophylactic potential of a single subcutaneous peg-IFN-λ1 administration on non-hospitalized individuals that are at a high risk of SARS-CoV-2 infection due to household exposure.
Immunomodulators
Because the development of COVID-19 is strongly driven by a dysregulated, often overshooting immune response, different immune modulatory treatments are considered for early and late phases of COVID-19 and several promising approaches for immuno-therapeutic treatments are under clinical investigations.
Dexamethasone
Glucocorticoids such as Dexamethasone constitute a frequently used class of anti-inflammatory drugs and have been used to treat chronic rhinosinusitis, chronic respiratory diseases or autoimmune disorders like rheumatoid arthritis (153, 154). Apart from their extensive use, they are very well-studied, widely available and also inexpensive (155). Dexamethasone disrupts inflammatory processes by decreasing the peripheral concentration and function of immune cells and limits the release of cytokines such as TNF-α and IL-1 from macrophages and other antigen-presenting cells (156, 157). The preliminary results from RECOVERY trial indicated that an oral or intravenous Dexamethasone dose of 6 mg given once daily for up to 10 days resulted in 35% less COVID-19 related deaths in patients on ICU who require mechanical ventilation and 20% less in non-ventilated patients on oxygen therapy (158). In addition, hospitalization time was significantly reduced. In contrast, there was no benefit for patients who do not receive respiratory aid. Based on this preliminary report the FDA and EMA endorsed the use of Dexamethasone for treatment of COVID-19 in late 2020. Later trials in COVID-19 patients with ARDS support this finding and report reduced overall mortality, and an increase in ventilation-free days (159, 160) Since November 2020, the Adaptive COVID-19 Treatment Trial 4 (ACTT-4) is active for a Phase-III study evaluating combinational therapy using Dexamethasone and Remdesivir in hospitalized patients (NCT04640168) as previous studies showed that combining Dexamethasone and Remdesivir enhances the positive effect of Remdesivir, leading to reduced mortality in hospitalized patients (161). Despite the promising results in ARDS and COVID-19 patients, there is still uncertainty about the overall effectiveness of glucocorticoids for COVID-19 patients as corticosteroids can also induce unwanted adverse effects, such as hyperglycemia, bacterial, fungal and viral infections, skin changes, adrenal suppression, myopathy and effects on wound healing and bone metabolism. Furthermore, there are potential ophthalmic, gastrointestinal, cardiovascular and psychiatric side effects (154).
IL-6 Receptor Antagonists
The proinflammatory cytokine IL-6 is one of the hallmark cytokines upregulated during severe COVID-19 and represents a predictive marker for the need of mechanical ventilation in accordance with CRP levels (162). Based on the critical role of IL-6 signaling, therapeutic approaches employed strategies to inhibit IL-6 signaling to reduce inflammation.
Tocilizumab and Sarilumab are both monoclonal antibodies, which inhibit the membrane-bound and the soluble form of the IL-6 receptor (163). Tocilizumab is already widely used for the treatment of diverse chronic and autoinflammatory diseases like rheumatoid arthritis, systemic juvenile idiopathic arthritis and others (164–167). The benefit of Tocilizumab treatment for hospitalized COVID-19 patients has been investigated in several clinical studies, however, early clinical trials conducted in Brazil were terminated due to safety issues (168). The first successful study was conducted in China with a cohort of only 15 COVID-19 patients. After administration of Tocilizumab, IL-6 levels first spiked but then decreased in 66.7% of the patients. A repeated dose of Tocilizumab was suggested to be more likely to improve the status of critically ill patients (169). Another study showed that Tocilizumab immediately improved the clinical outcome in severe and critical COVID-19 patients while no adverse side effects were registered (170). Since 2020, Roche is conducting three trials investigating the effect of Tocilizumab on COVID-19. The COVACTA trial showed a reduction in hospitalization time in COVID-19 patients treated with Tocilizumab, but there was no significant clinical improvement nor mortality reduction [NCT04320615; (171)]. The EMPACTA trial dealt with ethnic minorities and observed a reduction of mechanical ventilation by day 28, but also no difference in mortality between treated and non-treated patients [NCT04372186; (172)]. Lastly, the REMDACTA trial was enrolled to evaluate the safety and efficacy of the combination of Tocilizumab and Remdesivir in patients hospitalized with severe COVID-19 pneumonia, but did not meet the primary endpoint of earlier hospital discharge with treatment (NCT04409262). Additionally, other studies (NCT4356937, NCT04331808, NCT04346355) could also not show a benefit of Tocilizumab in preventing death (173–175). Critics also point out the high price of Tocilizumab, turning it to a drug only available in wealthy countries instead of a global treatment approach (176). Despite these disappointing results, the large-scale REMAP-CAP and RECOVERY trials concluded that for hospitalized, critically-ill COVID-19 patients, treatment with either Tocilizumab or Sarilumab improved the survival and other clinical outcomes, suggesting a superiority to standard care and an additive benefit when administered in combination with Dexamethasone (REMAP-CAP NCT02735707; RECOVERY Collaborative Group NCT04381936). Since 26th of June 2021, the FDA gave an EUA for Tocilizumab (Actemra) for the treatment of hospitalized pediatric or adult COVID-19 patients, when they are in need for supplemental oxygen, mechanical ventilation or ECMO. Later, at the 6th of July 2021, the WHO officially recommended the usage of IL-6 receptor blockers based on a network meta-analysis with data from clinical trial investigators in 28 countries (WHO).
Anti-IL-6 Antibodies
Siltuximab is a human-mouse chimeric monoclonal antibody against IL-6, which is approved for treatment in HIV-negative patients with multicentric Castleman’s disease (177). Preliminary data from a study with 21 COVID-19 patients suffering from ARDS indicated an improvement of the clinical condition after treatment with Siltuximab in 7 of the patients, while 9 patients stabilized with no clinically relevant improvement and the condition of the remaining 5 patients worsened [NCT04322188; (178)] Ongoing studies investigate the efficacy and safety of Siltuximab for COVID-19 treatment in comparison and in combination with corticosteroids such as methylprednisolone (NCT04329650, NCT04486521).
MAPK p38 Inhibitors
The mitogen-activated protein kinase (MAPK) p38 is associated with dysbalanced inflammatory processes in different pathologies and well-studied in animal models of acute lung and myocardial injury (179, 180). Mechanistically, p38-mediated phosphorylation of downstream kinases regulates the expression of proinflammatory cytokines such as IL-6, TNF-α and IL-1β. In the context of a dysbalanced immune response, such as in severe COVID-19 (11, 181), overexpression of these cytokines is suspected to contribute to organ damage and the described immunopathologies, suggesting that therapeutic interventions that reduce the expression of these cytokines could provide beneficial treatments for COVID-19. Recent work has demonstrated that p38 is activated during SARS-CoV-2 infection in vitro (180, 182, 183) and that blocking of p38 signaling by using pharmacological inhibitors that bind to the ATP binding pocket of this kinase resulted in decreased cytokine levels in vitro (182). Based on this observation Grimes et al. suggested p38 signaling as a promising therapeutic target for immunomodulatory therapeutic approaches of COVID-19 (184). In August 2020, Fulcrum Therapeutics initiated a Phase-III clinical trial with losmapimod, a clinically pre-evaluated but non-licensed, orally available p38 inhibitor, to investigate its effect on mortality and clinical outcome in hospitalized patients with moderate COVID-19, which are at risk to develop severe disease (NCT04511819). The results of this study are not yet released.
JAK Inhibitors
The Janus Kinase (JAK) family members play an essential role for the intracellular cytokine receptor signaling (185). They closely interact with signal transducer and activator of transcription (STAT) proteins and thereby contribute to inflammation and antiviral responses (186). Already in February 2020, Richardson et al. introduced Baricitinib, a JAK kinase inhibitor, to be trialed in COVID-19 patients (187) as it showed inhibitory properties against IL-6 and STAT3 phosphorylation and is approved for treatment of rheumatoid arthritis (188). Consistently, rhesus macaques had reduced inflammation in the lung upon treatment during SARS-CoV-2 infection, however, virus titers remained unaffected, demonstrating that it has immunomodulatory but not antiviral properties (189). However, in combination with Remdesivir, Baricitinib reduced the recovery time of patients receiving high-flow oxygen or noninvasive ventilation (190). Of note, patients also underwent standard treatment with corticosteroids, which limits the validity of the effect of Baricitinib. Nevertheless, on November 19th 2020, Baricitinib received EUA from the FDA in combination with Remdesivir (191).
Similar to Baricitinib, the JAK inhibitor Tofacitinib is also approved as an anti-rheumatic drug (192). When applied to COVID-19 patients with high levels of CRP within the TOFA-COV-2 trial, Tofacitinib treatment lowered the lung damage and CRP levels, increased the oxygen saturation and thus was suggested as an effective medication for managing the cytokine levels during COVID-19 (193) (NCT04750317).
In June 2021, a clinical trial using JAK inhibitor Ruxolitinib for treatment of COVID-19 patients was completed (RUXCOVID NCT04362137). Ruxolitinib is already an approved medication for myelofibrosis since 2012 (194). Unfortunately, the RUXCOVID trial sponsored by Novartis Pharmaceuticals could not meet the primary outcome of reducing the number of COVID-19 patients with severe complication such as ICU care, mechanical ventilation or death (NCT04362137). Before, a small study in 2020 indicated significant clinical improvement of patients with hyperinflammation during COVID-19 without signals of Ruxolitinib-induced toxicity (195). Based on these results, a Phase-II clinical trial has been completed, but only comprised 3 patients and did not publish any results (NCT04331665). More studies are currently recruiting participants to further assess the efficiency of Ruxolitinib for treating COVID-19 patients suffering from hyperinflammation and dysregulated immune responses (NCT04334044, NCT04338958, NCT04581954).
Emerging Immunomodulatory Treatment Strategies
Based on the rationale that the reduction of the overly activated proinflammatory response during COVID-19 improves clinical outcomes, many studies investigate approaches to target proinflammatory processes and other cytokines. Similar to the mechanism of IL-6 antagonists, antagonists of the IL-1 family and TNF blockers were investigated. The IL-1β antagonist Anakinra could successfully ameliorate the cytokine storm in infected patients with severe sepsis (196). A completed meta-analysis of clinical publications could already demonstrate a reduced mortality rate in treated patients (197),NCT04443881). Hence, new clinical trials with Anakinra are planned, injecting 100 mg Anakinra subcutaneously for up to 10 days (NCT04357366, NCT04643678, NCT04362111 (198, 199). Other potential measures focus on targeting mononuclear macrophage recruitment and their function or even stem cell therapy (200, 201) NCT04366063; NCT04486001; NCT04252118; NCT04437823), but there is no clinical information yet whether this is of benefit in COVID-19 patients.
Long COVID
In addition to the treatment of acute COVID-19, the need for efficient therapeutic options for the long-term consequences of the infection rapidly increases as many infected individuals suffer from Long COVID (202). Reports on the symptoms of Long COVID range from pulmonary manifestations such as shortness of breath, persistent cough and declined lung function to extrapulmonary manifestation like fatigue, anxiety and depression, memory loss, anosmia as well as declined kidney function, gastrointestinal complaints and heart damage (203–206).
Whilst this condition was first described as post COVID-19 syndrome or chronic COVID-19, the patient-derived name Long COVID or Long-haul COVID has recently been favored within the literature to draw attention to its severity (207, 208). The National Institute for Health and Care Excellence (NICE) further divides Long COVID into three separate groups according to the time of symptom duration: (I) acute COVID-19 (for up to 4 weeks) (II) ongoing symptomatic COVID-19 (4 to 12 weeks) (III) post-COVID-19 syndrome (more than 12 weeks) (COVID-19 Rapid Guideline, Dec 2020) (209, 210).
The knowledge of Long COVID is still rather small and it is not even clear if all reports of long-lasting effects on patient´s health describe the same entity (211). There are multiple different hypotheses of what may trigger Long COVID that still remain to be investigated. Ideas range from a post-viral syndrome similar to myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), a potential persistence of the virus in certain organs, an auto-immune triggered disease mechanism and post-intensive care syndrome (212). It was recently shown that a median of 4 months after COVID-19 diagnosis the SARS-CoV-2 N-protein could be detected within enterocytes in 5 out of 14 intestinal biopsies illustrating that antigen-persistence could potentially play a role in the development of Long COVID (213). Another disease mechanism that was recently suggested is that of an orthostatic intolerance syndrome caused by a disruption of the autonomic nervous system through infection with the SARS-CoV-2 virus (214). In 31 patients suffering from Long COVID symptoms two to seven different functional autoantibodies against G-coupled receptors could be detected illustrating that autoimmunity might play a role in the development of Long COVID (215). There is also a lack of information on how to best treat Long COVID patients. In a recent not yet peer-reviewed prospective observational study receiving the vaccination seemed to be beneficial to the recovery process at a median of 32 days after the vaccination. In 5.6% of the 44 vaccinated participants, symptoms increased, whilst 14.2% of the 22 not-vaccinated participants reported such an increase. Symptom resolution was experienced in 23.2% of those vaccinated in comparison to 15.4% of those not vaccinated. A difference between the Biontech-Pfizer or the AstraZeneca vaccine used in this study could not be observed (216).
The largest survey about the impact of different vaccines on the symptoms of patients suffering from Long COVID was conducted by the patient advocacy group LongCOVIDSOS via an online questionnaire with 900 participants. In 56.7% of all participants, symptoms overall improved after vaccination, while 18.7% experienced a deterioration. Only in 2.9% of participants all symptoms worsened. Interestingly, the Moderna mRNA vaccine appeared to be especially beneficial in relieving symptoms (217). Accordingly, it appears that receiving the vaccine is at least not harmful for those suffering from Long COVID. It has recently been suggested that an infection with SARS-CoV-2 results in an increasing amount of double negative B memory cells, which are dysfunctional. RNA vaccination reduced the number of those cells. This could be a potential reason why RNA vaccination seems to relieve the symptom burden in some patients (218).
To gain more insight into Long COVID the post-hospitalization study (PHOSP-COVID) has been set up in the UK and will recruit 10.000 patients that have been hospitalized with COVID-19, in order to better understand the short-, medium- and long-term consequences of infection via collecting patient data and material for one year after discharge from hospital (www.phosp.org).
Concluding Remarks
More than one and a half years into the SARS-CoV-2 pandemic, the treatment options for severe COVID-19 are still very limited. However, as this review highlights, the number of new drug candidates that are in clinical development or have already received EUA and are on the way to full approval is constantly growing. This include the immunomodulatory JAK inhibitor Baricitinib and the IL-6 receptor blocker tocilizumab, which both targets prevent signaling pathways that are involved in the expression levels of proinflammatory cytokines. The success of such approaches in the treatment of COVID-19 emphasizes that immunomodulatory and not primarily antiviral treatments are the key to COVID-19 therapies as the late-stage clinical manifestation of this disease is dominated by imbalanced inflammatory responses rather than by virus replication itself (Figure 1).
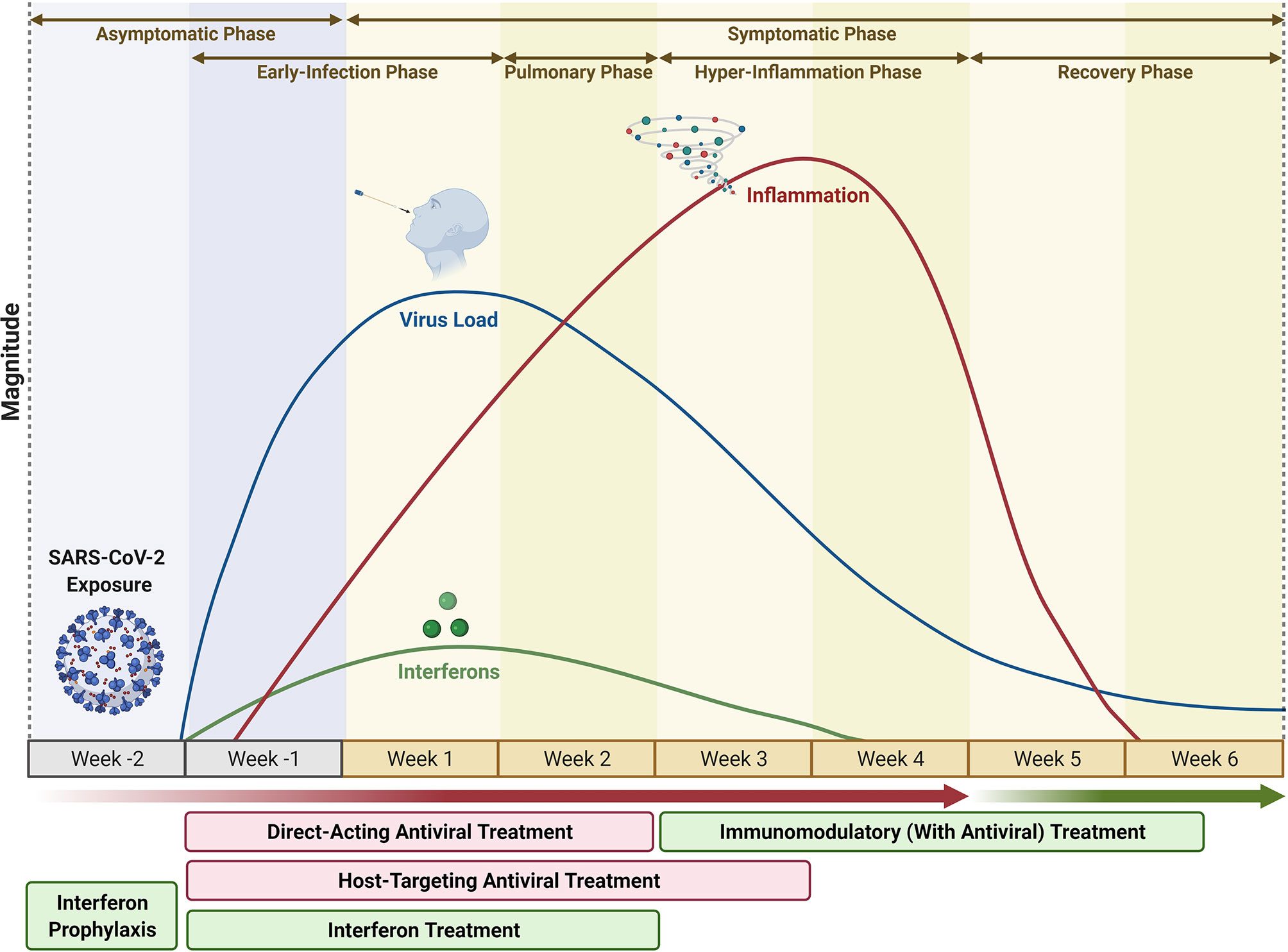
Figure 1 COVID-19 Progression vs Treatment Options. The infection phase of COVID-19 begins 1-week post exposure to SARS-CoV2 (Asymptomatic phase) and lasts for 4 weeks from the time of onset of symptoms, marked by a steady increase and resolution in virus titer between the first 2 weeks, during which Direct-Acting Antivirals (DAA), alone or in combination with Host-Targeting Antivirals (HTA) or Recombinant Interferons, could be potential treatment options. Week-2 until week-4 marks the resolution of infection phase, and onset of pulmonary phase (week-1, week-2) followed by inflammatory phase (week-3, week-4), during which Immunomodulators, mostly in combination with Antivirals, could be potential treatment options. Interferon Prophylaxis could be a preventive strategy on suspected exposure to SARS-CoV2 during the asymptomatic, pre-infection phase. (Timecourse not to be exactly scaled; varies depending on patient heterogeneity and virus variant). Figure modified from (135), and created with BioRender.com.
However, antiviral approaches aiming to reduce viral replication are similarly required to prevent the development of COVID-19 which is most successful in the earlier stages of the disease and can prevent further systemic dissemination of the virus and development of systemic inflammation. Under these considerations, combination of antiviral and immunomodulatory drugs or drugs that comprise both actions offers the broadest treatment window and appears most promising to achieve positive clinical outcomes in COVID-19 patients.
Clearly, the majority of the new therapeutic options are constituted of repurposed drugs or derived from classical therapeutic strategies such as treatment with convalescent sera or monoclonal antibodies, that are already in clinical use for other diseases and for which the route of administration, safety and side effects in humans is already well characterized. Nevertheless, as this review summarizes, there are also novel strategies, such as the ACE2-Fc fusion protein. Next to clinical therapeutics, home-treatment options are also being assessed for several drugs with the aim to reduce the time of viral shedding and the burden of milder disease. Another advantage of an increased arsenal of treatment options against SARS-CoV-2 and COVID-19 can be seen in potential to prevent the development of long-term complications like Long COVID.
Author Contributions
LB is responsible for the concept and structure of the review. SK, DC, JJ, AF, BC, and JL collected the literature articles and drafted the individual sections. SK edited the initial draft and designed the final figure. LB and SL reviewed and revised the final draft. All authors contributed to the article and approved the submitted version.
Funding
This work was financially supported by the German Research Foundation (DFG) through the Clinical Research Unit CRU342 (for Project-P6 to LB and SL); the Federal Ministry of Education and Research (BMBF) for the project CoIMMUNE (Grant No. 01KI20218 to LB), and through the Network University Medicine (NUM) for the COVID-19 project Organo-Strat (Grant No. 01KX2021 to LB and SL); and by the Faculty of Medicine, University of Muenster, through the Interdisciplinary Centre for Clinical Research (IZKF) (Grant No. Bru2/015/19 to LB) and the Innovative Medizinische Forschung (IMF) (Grant No. BR111905 to LB). DC is financially supported through a Study Abroad Program by the Ministry of National Education (Law: 1416), Republic of Turkey.
Conflict of Interest
SL is a founder, shareholder and board member of Atriva Therapeutics GmbH, Tübingen, Germany, a pharmaceutical company developing novel HTA against respiratory viral diseases including COVID-19.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We are grateful for the suggestions from André Schreiber, Angeles Mecate Zambrano and Franziska Günl, and for the assistance from Anmari Christersson. We acknowledge the valuable work of all the other researchers that aren’t cited here due to space constraints.
Abbreviations
ACTT, Adaptive COVID-19 Treatment Trial; ADE, Antibody-dependent Infection Enhancement; ARDS, Acute Respiratory Distress Syndrome; CFS, Chronic Fatigue Syndrome; COPD, Chronic Obstructive Pulmonary Diseases; DAA, Direct-Acting Antivirals; eEF1A, eukaryotic translation Elongation Factor 1 Alpha; EMA, European Medicines Agency; EUA, Emergency Use Authorization; FDA, Food and Drug Administration; FIASMA, Functional Inhibitors of Acid Sphingomyelinase; GBPA, 4-(4-Guanidinobenzyloxy)Phenylacetic Acid; HCQ, Hydroxy-Chloroquine; hrsACE2, Recombinant human soluble ACE2; LPV/r, Lopinavir/ritonavir; ME, Myalgic Encephalomyelitis; NICE, National Institute for Health and Care Excellence; NSP, Non-Structural Proteins; ORF, Open Reading Frames; OSCI, Ordinal Scale for Clinical Improvement; RdRp, RNA-dependent RNA Polymerase; rhIFNα, Recombinant Human IFN-α; rSIFN, Recombinant Super-Compound Interferon; HTA, Host-Targeting Antivirals; SARS-CoV-2, Severe Acute Respiratory Syndrome Coronavirus 2.
References
1. Lai CC, Shih TP, Ko WC, Tang HJ, Hsueh PR. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Coronavirus Disease-2019 (COVID-19): The Epidemic and the Challenges. Int J Antimicrobial Agents (2020) 55:105924. doi: 10.1016/j.ijantimicag.2020.105924
2. Lu R, Zhao X, Li J, Niu P, Yang B, Wu H, et al. Genomic Characterisation and Epidemiology of 2019 Novel Coronavirus: Implications for Virus Origins and Receptor Binding. Lancet (2020) 395(10224):565–74. doi: 10.1016/S0140-6736(20)30251-8
3. Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell (2020) 181(2):281–92. doi: 10.1016/j.cell.2020.02.058
4. Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell (2020) 181(2):271–80. doi: 10.1016/j.cell.2020.02.052
5. Blaess M, Kaiser L, Sommerfeld O, Csuk R, Deigner HP. Drugs, Metabolites, and Lung Accumulating Small Lysosomotropic Molecules: Multiple Targeting Impedes Sars-Cov-2 Infection and Progress to Covid-19. Int J Mol Sci (2021) 22(4):1797. doi: 10.3390/ijms22041797
6. Xu X, Liu Y, Weiss S, Arnold E, Sarafianos SG, Ding J. Molecular Model of SARS Coronavirus Polymerase: Implications for Biochemical Functions and Drug Design. Nucleic Acids Res (2003) 31(24):7117–30. doi: 10.1093/nar/gkg916
7. Hu B, Guo H, Zhou P, Shi ZL. Characteristics of SARS-CoV-2 and COVID-19. Nat Rev Microbiol (2021) 19:141–54. doi: 10.1038/s41579-020-00459-7
8. Lee IC, Huo TI, Huang YH. Gastrointestinal and Liver Manifestations in Patients With COVID-19. J Chin Med Assoc (2020) 83:521–3. doi: 10.1097/JCMA.0000000000000319
9. Gavriatopoulou M, Korompoki E, Fotiou D, Ntanasis-Stathopoulos I, Psaltopoulou T, Kastritis E, et al. Organ-Specific Manifestations of COVID-19 Infection. Clin Exp Med (2020) 20:493–506. doi: 10.1007/s10238-020-00648-x
10. Chen T, Wu D, Chen H, Yan W, Yang D, Chen G, et al. Clinical Characteristics of 113 Deceased Patients With Coronavirus Disease 2019: Retrospective Study. BMJ (2020) 368:m1091. doi: 10.1136/bmj.m1091
11. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical Features of Patients Infected With 2019 Novel Coronavirus in Wuhan, China. Lancet (2020) 395(10223):497–506. doi: 10.1016/S0140-6736(20)30183-5
12. Guo YR, Cao QD, Hong ZS, Tan YY, Chen SD, Jin HJ, et al. The Origin, Transmission and Clinical Therapies on Coronavirus Disease 2019 (COVID-19) Outbreak- A N Update on the Status. Military Med Res (2020) 7:11. doi: 10.1186/s40779-020-00240-0
13. Tang L, Yin Z, Hu Y, Mei H. Controlling Cytokine Storm Is Vital in COVID-19. Front Immunol (2020) 11. doi: 10.3389/fimmu.2020.570993
14. Siddiqi HK, Mehra MR. COVID-19 Illness in Native and Immunosuppressed States: A Clinical–Therapeutic Staging Proposal. J Heart Lung Transplant (2020) 39:405–7. doi: 10.1016/j.healun.2020.03.012
15. Hamming I, Timens W, Bulthuis MLC, Lely AT, Navis GJ, van Goor H. Tissue Distribution of ACE2 Protein, the Functional Receptor for SARS Coronavirus. A First Step in Understanding SARS Pathogenesis. J Pathol (2004) 203(2):631–7. doi: 10.1002/path.1570
16. Ortiz ME, Thurman A, Pezzulo AA, Leidinger MR, Klesney-Tait JA, Karp PH, et al. Heterogeneous Expression of the SARS-Coronavirus-2 Receptor ACE2 in the Human Respiratory Tract. EBioMedicine (2020) 60:102976. doi: 10.1016/j.ebiom.2020.102976
17. Chen Y, Klein SL, Garibaldi BT, Li H, Wu C, Osevala NM, et al. Aging in COVID-19: Vulnerability, Immunity and Intervention. Ageing Res Rev (2021) 65:101205. doi: 10.1016/j.arr.2020.101205
18. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA - J Am Med Assoc (2020) 323(11):1061–9. doi: 10.1001/jama.2020.1585
19. Liu C, Zhao Y, Okwan-Duodu D, Basho R, Cui X. COVID-19 in Cancer Patients: Risk, Clinical Features, and Management. Cancer Biol Med (2020) 17:519–27. doi: 10.20892/j.issn.2095-3941.2020.0289
20. Chen J, Qi T, Liu L, Ling Y, Qian Z, Li T, et al. Clinical Progression of Patients With COVID-19 in Shanghai, China. J Infect (2020) 80(5):e1–6. doi: 10.1016/j.jinf.2020.03.004
21. Nojomi M, Yassin Z, Keyvani H, Makiani MJ, Roham M, Laali A, et al. Effect of Arbidol (Umifenovir) on COVID-19: A Randomized Controlled Trial. BMC Infect Dis (2020) 20(1):954–64. doi: 10.1186/s12879-020-05698-w
22. Vankadari N. Arbidol: A Potential Antiviral Drug for the Treatment of SARS-CoV-2 by Blocking Trimerization of the Spike Glycoprotein. Int J Antimicrobial Agents (2020) 56(2):105998. doi: 10.1016/j.ijantimicag.2020.105998
23. Padhi AK, Seal A, Khan JM, Ahamed M, Tripathi T. Unraveling the Mechanism of Arbidol Binding and Inhibition of SARS-CoV-2: Insights From Atomistic Simulations. Eur J Pharmacol (2021) 894:173836. doi: 10.1016/j.ejphar.2020.173836
24. Lian N, Xie H, Lin S, Huang J, Zhao J, Lin Q. Umifenovir Treatment is Not Associated With Improved Outcomes in Patients With Coronavirus Disease 2019: A Retrospective Study. Clin Microbiol Infect (2020) 26(7):917–21. doi: 10.1016/j.cmi.2020.04.026
25. Deng L, Li C, Zeng Q, Liu X, Li X, Zhang H, et al. Arbidol Combined With LPV/r Versus LPV/r Alone Against Corona Virus Disease 2019: A Retrospective Cohort Study. J Infect (2020) 81(1):e1–5. doi: 10.1016/j.jinf.2020.03.002
26. Jomah S, Asdaq SMB, Al-Yamani MJ. Clinical Efficacy of Antivirals Against Novel Coronavirus (COVID-19): A Review. J Infect Public Health (2020) 13:11871195. doi: 10.1016/j.jiph.2020.07.013
27. Huang D, Yu H, Wang T, Yang H, Yao R, Liang Z. Efficacy and Safety of Umifenovir for Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis. J Med Virol (2021) 93(1):481–90. doi: 10.1002/jmv.26256
28. Yuan S, Yin X, Meng X, Chan J, Ye Z-W, Riva L, et al. Clofazimine is a Broad-Spectrum Coronavirus Inhibitor That Antagonizes SARS-CoV-2 Replication in Primary Human Cell Culture and Hamsters. Res Square (2020). doi: 10.21203/rs.3.rs-86169/v1
29. Duan K, Liu B, Li C, Zhang H, Yu T, Qu J, et al. Effectiveness of Convalescent Plasma Therapy in Severe COVID-19 Patients. Proc Natl Acad Sci USA (2020) 117(17):9490–6. doi: 10.1073/pnas.2007408117
30. Shen C, Wang Z, Zhao F, Yang Y, Li J, Yuan J, et al. Treatment of 5 Critically Ill Patients With COVID-19 With Convalescent Plasma. JAMA - J Am Med Assoc (2020) 323(16):1582–9. doi: 10.1001/jama.2020.4783
31. Ahn JY, Sohn Y, Lee SH, Cho Y, Hyun JH, Baek YJ, et al. Use of Convalescent Plasma Therapy in Two Covid-19 Patients With Acute Respiratory Distress Syndrome in Korea. J Korean Med Sci (2020) 35(14):e149. doi: 10.3346/jkms.2020.35.e149
32. Salazar E, Perez KK, Ashraf M, Chen J, Castillo B, Christensen PA, et al. Treatment of Coronavirus Disease 2019 (COVID-19) Patients With Convalescent Plasma. Am J Pathol (2020) 190(8):1680–90. doi: 10.1016/j.ajpath.2020.05.014
33. Li L, Zhang W, Hu Y, Tong X, Zheng S, Yang J, et al. Effect of Convalescent Plasma Therapy on Time to Clinical Improvement in Patients With Severe and Life-Threatening COVID-19: A Randomized Clinical Trial. JAMA - J Am Med Assoc (2020) 324(5):460–70. doi: 10.1001/jama.2020.12607
34. Liu STH, Aberg JA. Convalescent Plasma in Patients Hospitalised With COVID-19. Lancet (2021) 397:2024–5. doi: 10.1016/S0140-6736(21)01064-3
35. Casadevall A, Pirofski LA. The Convalescent Sera Option for Containing COVID-19. J Clin Invest (2020) 130:1545–8. doi: 10.1172/JCI138003
36. Kemp SA, Collier DA, Datir RP, Ferreira IATM, Gayed S, Jahun A, et al. SARS-CoV-2 Evolution During Treatment of Chronic Infection. Nature (2021) 592(7853):277–82. doi: 10.1038/s41586-021-03291-y
37. Bamlanivimab. Drugs and Lactation Database. Bethesda (MD): National Library of Medicine (2021) (US. 2006–2021 Apr 19 [Internet].
38. Etesevimab and Bamlanivimab. Drugs and Lactation Database. Bethesda (MD): National Library of Medicine (2021) (US. 2006–2021 Apr 19; PMID: 33630482 [Internet].
39. Gottlieb RL, Nirula A, Chen P, Boscia J, Heller B, Morris J, et al. Effect of Bamlanivimab as Monotherapy or in Combination With Etesevimab on Viral Load in Patients With Mild to Moderate COVID-19: A Randomized Clinical Trial. JAMA - J Am Med Assoc (2021) 325(7):632–44. doi: 10.1001/jama.2021.0202
40. Baum A, Fulton BO, Wloga E, Copin R, Pascal KE, Russo V, et al. Antibody Cocktail to SARS-CoV-2 Spike Protein Prevents Rapid Mutational Escape Seen With Individual Antibodies. Science (2020) 369(6506):1014–8. doi: 10.1126/science.abd0831
41. Weinreich DM, Sivapalasingam S, Norton T, Ali S, Gao H, Bhore R, et al. REGN-COV2, a Neutralizing Antibody Cocktail, in Outpatients With Covid-19. N Engl J Med (2021) 384(3):238–51. doi: 10.1056/NEJMoa2035002
42. Cathcart AL, Havenar-Daughton C, Lempp FA, Ma D, Schmid MA, Agostini ML, et al. The Dual Function Monoclonal Antibodies VIR-7831 and VIR-7832 Demonstrate Potent In Vitro and 2 In Vivo Activity Against SARS-CoV-2 3 4 5. bioRxiv (2021). doi: 10.1101/2021.03.09.434607
43. Zoufaly A, Poglitsch M, Aberle JH, Hoepler W, Seitz T, Traugott M, et al. Human Recombinant Soluble ACE2 in Severe COVID-19. Lancet Respir Med (2020) 8(11):e78. doi: 10.1016/S2213-2600(20)30418-5
44. Pang X, Cui Y, Zhu Y. Recombinant Human ACE2: Potential Therapeutics of SARS-CoV-2 Infection and Its Complication. Acta Pharmacol Sin (2020) 41:1255–7. doi: 10.1038/s41401-020-0430-6
45. Monteil V, Dyczynski M, Lauschke VM, Kwon H, Wirnsberger G, Youhanna S, et al. Human Soluble ACE2 Improves the Effect of Remdesivir in SARS-CoV-2 Infection. EMBO Mol Med (2021) 13(1):e13426. doi: 10.15252/emmm.202013426
46. Rodell CB. An ACE Therapy for COVID-19. Sci Trans Med (2020) 12(541):eabb5676. doi: 10.1126/scitranslmed.abb5676
47. Kruse RL. Therapeutic Strategies in an Outbreak Scenario to Treat the Novel Coronavirus Originating in Wuhan, China. F1000Research (2020) 9. doi: 10.12688/f1000research.22211.1
48. Svilenov HL, Sacherl J, Reiter A, Wolff L, Chen CC, Wachs FP, et al. Efficient Inhibition of SARS-CoV-2 Strains by a Novel ACE2-IgG4-Fc Fusion Protein With a Stabilized Hinge Region. bioRxiv (2020). doi: 10.1101/2020.12.06.413443
49. Frediansyah A, Nainu F, Dhama K, Mudatsir M, Harapan H. Remdesivir and Its Antiviral Activity Against COVID-19: A Systematic Review. Clin Epidemiol Global Health (2021) 9:2213–3984. doi: 10.1016/j.cegh.2020.07.011
50. de Wit E, Feldmann F, Cronin J, Jordan R, Okumura A, Thomas T, et al. Prophylactic and Therapeutic Remdesivir (GS-5734) Treatment in the Rhesus Macaque Model of MERS-CoV Infection. Proc Natl Acad Sci USA (2020) 117(12):6771–6. doi: 10.1073/pnas.1922083117
51. Holshue ML, DeBolt C, Lindquist S, Lofy KH, Wiesman J, Bruce H, et al. First Case of 2019 Novel Coronavirus in the United States. New Engl J Med (2020) 382(10):929–36. doi: 10.1056/NEJMoa2001191
52. Pagliano P, Scarpati G, Sellitto C, Conti V, Spera AM, Ascione T, et al. Experimental Pharmacotherapy for Covid-19: The Latest Advances. J Exp Pharmacol (2021) 13:1–13. doi: 10.2147/JEP.S255209
53. Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, Kalil AC, et al. Remdesivir for the Treatment of Covid-19 — Final Report. New Engl J Med (2020) 383(19):1813–26. doi: 10.1056/NEJMc2022236
54. Twomey JD, Luo S, Dean AQ, Bozza WP, Nalli A, Zhang B. COVID-19 Update: The Race to Therapeutic Development. Drug Resistance Updates (2020) 53:100733. doi: 10.1016/j.drup.2020.100733
55. Pan H, Peto R, Karim QA, Alejandria M, Henao-Restrepo AM, García CH, et al. Repurposed Antiviral Drugs for COVID-19 –Interim WHO SOLIDARITY Trial Results. N Engl J Med (2020) 348(6):497–511. doi: 10.1056/NEJMoa2023184
56. Young B, Tan TT, Leo YS. The Place for Remdesivir in COVID-19 Treatment. Lancet Infect Dis (2021) 21:20–1. doi: 10.1016/S1473-3099(20)30911-7
57. Agrawal U, Raju R, Udwadia ZF. Favipiravir: A New and Emerging Antiviral Option in COVID-19. Med J Armed Forces India (2020) 76:370–6. doi: 10.1016/j.mjafi.2020.08.004
58. Naesens L, Guddat LW, Keough DT, van Kuilenburg ABP, Meijer J, vande Voorde J, et al. Role of Human Hypoxanthine Guanine Phosphoribosyltransferase in Activation of the Antiviral Agent T-705 (Favipiravir). Mol Pharmacol (2013) 84(4):615–29. doi: 10.1124/mol.113.087247
59. Joshi S, Parkar J, Ansari A, Vora A, Talwar D, Tiwaskar M, et al. Role of Favipiravir in the Treatment of COVID-19. Int J Infect Dis (2021) 102:501–8. doi: 10.1016/j.ijid.2020.10.069
60. Kramer DG, da Silva MJL, da, Silva GSE, de, Moura AMMA, et al. Favipiravir as a Potential Drug in the Treatment of COVID-19. Int J Res - GRANTHAALAYAH (2020) 8(4):7–12. doi: 10.29121/granthaalayah.v8.i4.2020.2
61. Kelleni MT. Tocilizumab, Remdesivir, Favipiravir, and Dexamethasone Repurposed for COVID-19: A Comprehensive Clinical and Pharmacovigilant Reassessment. SN Compr Clin Med (2021) 3(4):1–5. doi: 10.1007/s42399-021-00824-4
62. Pilkington V, Pepperrell T, Hill A. A Review of the Safety of Favipiravir – a Potential Treatment in the COVID-19 Pandemic? J Virus Eradication (2020) 6:45–51. doi: 10.1016/S2055-6640(20)30016-9
63. Chen C, Zhang Y, Huang J, Yin P, Cheng Z, Wu J, et al. Favipiravir Versus Arbidol for COVID-19: A Randomized Clinical Trial. Front Pharmacol (2021) 12:683296. doi: 10.1101/2020.03.17.20037432
64. Cai Q, Yang M, Liu D, Chen J, Shu D, Xia J, et al. Experimental Treatment With Favipiravir for COVID-19: An Open-Label Control Study. Engineering (2020) 6(10):1192–8. doi: 10.1016/j.eng.2020.03.007
65. Dabbous HM, Abd-Elsalam S, El-Sayed MH, Sherief AF, Ebeid FFS, Ghafar MSA, et al. Efficacy of Favipiravir in COVID-19 Treatment: A Multi-Center Randomized Study. Arch Virol (2021) 166(3):949–54. doi: 10.1007/s00705-021-04956-9
66. PRINCIPLE. Favipiravir to be Investigated as a Possible COVID-19 Treatment for at-Home Recovery in the PRINCIPLE Trial — PRINCIPLE Trial. (2021). (https://www.principletrial.org/news/favipiravir-to-be-investigated-as-a-possible-covid-19-treatment-for-at-home-recovery-in-the-principle-trial [Accessed September 23,2021]
67. Painter WP, Holman W, Bush JA, Almazedi F, Malik H, Eraut NCJE, et al. Human Safety, Tolerability, and Pharmacokinetics of Molnupiravir, a Novel Broad-Spectrum Oral Antiviral Agent With Activity Against SARS-CoV-2. Antimicrobial Agents Chemother (2021) 65(5):e02428–20. doi: 10.1128/AAC.02428-20
68. Abdelnabi R, Foo CS, Kaptein SJF, Zhang X, Langendries L, Vangeel L, et al. The Combined Treatment of Molnupiravir and Favipiravir Results in a Marked Potentiation of Antiviral Efficacy in a SARS-CoV-2 Hamster Infection Model. bioRxiv (2021). doi: 10.1101/2020.12.10.419242
69. Uzunova K, Filipova E, Pavlova V, Vekov T. Insights Into Antiviral Mechanisms of Remdesivir, Lopinavir/Ritonavir and Chloroquine/Hydroxychloroquine Affecting the New SARS-CoV-2. Biomed Pharmacother (2020) 131:110668. doi: 10.1016/j.biopha.2020.110668
70. Cao B, Wang Y, Wen D, Liu W, Wang J, Fan G, et al. A Trial of Lopinavir–Ritonavir in Adults Hospitalized With Severe Covid-19. New Engl J Med (2020) 382(19):1787–99. doi: 10.1056/NEJMc2008043
71. Li Y, Xie Z, Lin W, Cai W, Wen C, Guan Y, et al. Efficacy and Safety of Lopinavir/Ritonavir or Arbidol in Adult Patients With Mild/Moderate COVID-19: An Exploratory Randomized Controlled. Trial Med (2020) 1(1):105–13. doi: 10.1016/j.medj.2020.04.001
72. Sheahan TP, Sims AC, Leist SR, Schäfer A, Won J, Brown AJ, et al. Comparative Therapeutic Efficacy of Remdesivir and Combination Lopinavir, Ritonavir, and Interferon Beta Against MERS-CoV. Nat Commun (2020) 11(1):222. doi: 10.1038/s41467-019-13940-6
73. Hung IFN, Lung KC, Tso EYK, Liu R, Chung TWH, Chu MY, et al. Triple Combination of Interferon Beta-1b, Lopinavir–Ritonavir, and Ribavirin in the Treatment of Patients Admitted to Hospital With COVID-19: An Open-Label, Randomised, Phase 2 Trial. Lancet (2020) 395(10238):1695–704. doi: 10.1016/S0140-6736(20)31042-4
74. Srinivas P, Sacha GL, Koval C. Antivirals for COVID-19. Cleveland Clin J Med (2020). doi: 10.3949/ccjm.87a.ccc030
75. Cvetkovic RS, Goa KL. Lopinavir/ritonavir: A Review of Its Use in the Management of HIV Infection. Drugs (2003) 63:769–802. doi: 10.2165/00003495-200363080-00004
76. Wang X, Guan Y. COVID-19 Drug Repurposing: A Review of Computational Screening Methods, Clinical Trials, and Protein Interaction Assays. Med Res Rev (2021) 41:5–28. doi: 10.1002/med.21728
77. Savarino A, Boelaert JR, Cassone A, Majori G, Cauda R. Effects of Chloroquine on Viral Infections: An Old Drug Against Today’s Diseases? Lancet Infect Dis (2003) 3:722–7. doi: 10.1016/S1473-3099(03)00806-5
78. Gomes CP, Fernandes DE, Casimiro F, da Mata GF, Passos MT, Varela P, et al. Cathepsin L in COVID-19: From Pharmacological Evidences to Genetics. Front Cell Infect Microbiol (2020) 10. doi: 10.3389/fcimb.2020.589505
79. Ou T, Mou H, Zhang L, Ojha A, Choe H, Farzan M. Hydroxychloroquine-Mediated Inhibition of SARS-CoV-2 Entry is Attenuated by TMPRSS2. PloS Pathogens (2021) 17(1 January):e1009212. doi: 10.1371/journal.ppat.1009212
80. Vincent MJ, Bergeron E, Benjannet S, Erickson BR, Rollin PE, Ksiazek TG, et al. Chloroquine is a Potent Inhibitor of SARS Coronavirus Infection and Spread. Virol J (2005) 2:69. doi: 10.1186/1743-422X-2-69
81. Yao X, Ye F, Zhang M, Cui C, Huang B, Niu P, et al. In Vitro Antiviral Activity and Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin Infect Dis (2020) 71(15):732–9. doi: 10.1093/cid/ciaa237
82. Liu J, Cao R, Xu M, Wang X, Zhang H, Hu H, et al. Hydroxychloroquine, a Less Toxic Derivative of Chloroquine, is Effective in Inhibiting SARS-CoV-2 Infection In Vitro. Cell Discov (2020) 6:16. doi: 10.1038/s41421-020-0156-0
83. Keyaerts E, Li S, Vijgen L, Rysman E, Verbeeck J, van Ranst M, et al. Antiviral Activity of Chloroquine Against Human Coronavirus OC43 Infection in Newborn Mice. Antimicrobial Agents Chemother (2009) 53(8):3416–21. doi: 10.1128/AAC.01509-08
84. Mitjà O, Corbacho-Monné M, Ubals M, Alemany A, Suñer C, Tebé C, et al. A Cluster-Randomized Trial of Hydroxychloroquine for Prevention of Covid-19. New Engl J Med (2021) 384(5):417–27. doi: 10.1056/NEJMoa2021801
85. Self WH, Semler MW, Leither LM, Casey JD, Angus DC, Brower RG, et al. Effect of Hydroxychloroquine on Clinical Status at 14 Days in Hospitalized Patients With COVID-19: A Randomized Clinical Trial. JAMA - J Am Med Assoc (2020) 324(21):2165–76. doi: 10.1001/jama.2020.22240
86. Geleris J, Sun Y, Platt J, Zucker J, Baldwin M, Hripcsak G, et al. Observational Study of Hydroxychloroquine in Hospitalized Patients With Covid-19. New Engl J Med (2020) 382(25):2411–8. doi: 10.1056/NEJMoa2012410
87. Thomson K, Nachlis H. Emergency Use Authorizations During the COVID-19 Pandemic: Lessons From Hydroxychloroquine for Vaccine Authorization and Approval. JAMA - J Am Med Assoc (2020) 324:1282–3. doi: 10.1001/jama.2020.16253
88. Hussain M, Jabeen N, Amanullah A, Baig AA, Aziz B, Shabbir S, et al. Structural Basis of SARS-CoV-2 Spike Protein Priming by TMPRSS2. AIMS Microbiol (2020) 6(3):350–60. doi: 10.3934/microbiol.2020021
89. Benton DJ, Wrobel AG, Xu P, Roustan C, Martin SR, Rosenthal PB, et al. Receptor Binding and Priming of the Spike Protein of SARS-CoV-2 for Membrane Fusion. Nature (2020) 588(7837):327–30. doi: 10.1038/s41586-020-2772-0
90. Hoffmann M, Hofmann-Winkler H, Smith JC, Krüger N, Arora P, Sørensen LK, et al. Camostat Mesylate Inhibits SARS-CoV-2 Activation by TMPRSS2-Related Proteases and Its Metabolite GBPA Exerts Antiviral Activity. EBioMedicine (2021) 65:103255. doi: 10.1016/j.ebiom.2021.103255
91. Kupferschmidt K. These Drugs Don’t Target the Coronavirus—They Target Us. Science (2020). doi: 10.1126/science.abc0405
92. Hoffmann M, Schroeder S, Kleine-Weber H, Müller MA, Drosten C, Pöhlmann S. Nafamostat Mesylate Blocks Activation of SARS-CoV-2: New Treatment Option for COVID-19. Antimicrobial Agents Chemother (2020) 64(6):e00754–20. doi: 10.1128/AAC.00754-20
93. Breining P, Frølund AL, Højen JF, Gunst JD, Staerke NB, Saedder E, et al. Camostat Mesylate Against SARS-CoV-2 and COVID-19—Rationale, Dosing and Safety. Basic Clin Pharmacol Toxicol (2021) 128(2):204–12. doi: 10.1111/bcpt.13533
94. Luan B, Huynh T, Cheng X, Lan G, Wang HR. Targeting Proteases for Treating COVID-19. J Proteome Res (2020) 19:4316–26. doi: 10.1021/acs.jproteome.0c00430
95. Seth S, Batra J, Srinivasan S. COVID-19: Targeting Proteases in Viral Invasion and Host Immune Response. Front Mol Biosci (2020) 7. doi: 10.3389/fmolb.2020.00215
96. Schloer S, Brunotte L, Goretzko J, Mecate-Zambrano A, Korthals N, Gerke V, et al. Targeting the Endolysosomal Host-SARS-CoV-2 Interface by Clinically Licensed Functional Inhibitors of Acid Sphingomyelinase (FIASMA) Including the Antidepressant Fluoxetine. Emerging Microbes Infect (2020) 9(1):2245–55. doi: 10.1080/22221751.2020.1829082
97. Zimniak M, Kirschner L, Hilpert H, Geiger N, Danov O, Oberwinkler H, et al. The Serotonin Reuptake Inhibitor Fluoxetine Inhibits SARS-CoV-2 in Human Lung Tissue. Sci Rep (2021) 11(1):5890. doi: 10.1038/s41598-021-85049-0
98. Schloer S, Brunotte L, Mecate-Zambrano A, Zheng S, Tang J, Ludwig S, et al. Drug Synergy of Combinatory Treatment With Remdesivir and the Repurposed Drugs Fluoxetine and Itraconazole Effectively Impairs SARS-CoV-2 Infection In Vitro. Br J Pharmacol (2021) 178(11):2339–50. doi: 10.1111/bph.15418
99. Creeden JF, Imami AS, Eby HM, Gillman C, Becker KN, Reigle J, et al. Fluoxetine as an Anti-Inflammatory Therapy in SARS-CoV-2 Infection. Biomed Pharmacother (2021) 138:111437. doi: 10.1016/j.biopha.2021.111437
100. Eugene AR. Fluoxetine Pharmacokinetics and Tissue Distribution Suggest a Possible Role in Reducing SARS-CoV-2 Titers [version 1; peer review: 2 approved with reservations]. F1000Research (2021) 10:477. doi: 10.12688/f1000research.53275.1
101. Hoertel N, Sánchez-Rico M, Vernet R, Beeker N, Jannot AS, Neuraz A, et al. Association Between Antidepressant Use and Reduced Risk of Intubation or Death in Hospitalized Patients With COVID-19: Results From an Observational Study. Mol Psychiatry (2021). doi: 10.1038/s41380-021-01021-4
102. Gordon DE, Jang GM, Bouhaddou M, Xu J, Obernier K, White KM, et al. A SARS-CoV-2 Protein Interaction Map Reveals Targets for Drug Repurposing. Nature (2020) 583(7816):459–68. doi: 10.1038/s41586-020-2286-9
103. Delgado-Calle J, Kurihara N, Atkinson EG, Nelson J, Miyagawa K, Galmarini CM, et al. Aplidin (Plitidepsin) is a Novel Anti-Myeloma Agent With Potent Anti-Resorptive Activity Mediated by Direct Effects on Osteoclasts. Oncotarget (2019) 10(28):2709–21. doi: 10.18632/oncotarget.26831
104. Wong JP, Damania B. SARS-CoV-2 Dependence on Host Pathways. Science (2021) 371:884–5. doi: 10.1126/science.abg6837
105. White KM, Rosales R, Yildiz S, Kehrer T, Miorin L, Moreno E, et al. Plitidepsin has Potent Preclinical Efficacy Against SARS-CoV-2 by Targeting the Host Protein Eef1a. Science (2021) 371(6532):926–31. doi: 10.1126/science.abf4058
106. Reuschl A-K, Thorne L, Zuliani Alvarez L, Bouhaddou M, Obernier K, Soucheray M, et al. Host-Directed Therapies Against Early-Lineage SARS-CoV-2 Retain Efficacy Against B.1.1.7 Variant. bioRxiv: Preprint Server Biol (2021). doi: 10.1101/2021.01.24.427991
107. Spicka I, Ocio EM, Oakervee HE, Greil R, Banh RH, Huang SY, et al. Randomized Phase III Study (ADMYRE) of Plitidepsin in Combination With Dexamethasone vs. Dexamethasone Alone in Patients With Relapsed/Refractory Multiple Myeloma. Ann Hematol (2019) 98(9):2139–50. doi: 10.1007/s00277-019-03739-2
108. Planz O. Development of Cellular Signaling Pathway Inhibitors as New Antivirals Against Influenza. Antiviral Res (2013) 98:457–68. doi: 10.1016/j.antiviral.2013.04.008
109. Pleschka S, Wolff T, Ehrhardt C, Hobom G, Planz O, Rapp UR, et al. Influenza Virus Propagation is Impaired by Inhibition of the Raf/MEK/ERK Signalling Cascade. Nat Cell Biol (2001) 3(3):301–5. doi: 10.1038/35060098
110. Schreiber A, Boff L, Anhlan D, Krischuns T, Brunotte L, Schuberth C, et al. Dissecting the Mechanism of Signaling-Triggered Nuclear Export of Newly Synthesized Influenza Virus Ribonucleoprotein Complexes. Proc Natl Acad Sci USA (2020) 117(28):16557–66. doi: 10.1073/pnas.2002828117
111. Preugschas HF, Hrincius ER, Mewis C, Tran GVQ, Ludwig S, Ehrhardt C. Late Activation of the Raf/MEK/ERK Pathway is Required for Translocation of the Respiratory Syncytial Virus F Protein to the Plasma Membrane and Efficient Viral Replication. Cell Microbiol (2019) 21(1):e12955. doi: 10.1111/cmi.12955
112. Cai Y, Liu Y, Zhang X. Suppression of Coronavirus Replication by Inhibition of the MEK Signaling Pathway. J Virol (2007) 81(2):446–56. doi: 10.1128/JVI.01705-06
113. Laure M, Hamza H, Koch-Heier J, Quernheim M, Müller C, Schreiber A, et al. Antiviral Efficacy Against Influenza Virus and Pharmacokinetic Analysis of a Novel MEK-Inhibitor, ATR-002, in Cell Culture and in the Mouse Model. Antiviral Res (2020) 178:104806. doi: 10.1016/j.antiviral.2020.104806
114. Pinto R, Herold S, Cakarova L, Hoegner K, Lohmeyer J, Planz O, et al. Inhibition of Influenza Virus-Induced NF-kappaB and Raf/MEK/ERK Activation can Reduce Both Virus Titers and Cytokine Expression Simultaneously In Vitro and In Vivo. Antiviral Res (2011) 92(1):45–56. doi: 10.1016/j.antiviral.2011.05.009
115. Zaidi AK, Dehgani-Mobaraki P. The Mechanisms of Action of Ivermectin Against SARS-CoV-2: An Evidence-Based Clinical Review Article. J Antibiotics (2021). doi: 10.1038/s41429-021-00430-5
116. Matsuyama T, Kubli SP, Yoshinaga SK, Pfeffer K, Mak TW. An Aberrant STAT Pathway is Central to COVID-19. Cell Death Different (2020) 27:3209–25. doi: 10.1038/s41418-020-00633-7
117. Caly L, Druce JD, Catton MG, Jans DA, Wagstaff KM. The FDA-Approved Drug Ivermectin Inhibits the Replication of SARS-CoV-2 In Vitro. Antiviral Res (2020) 178:104787. doi: 10.1016/j.antiviral.2020.104787
118. Kory P, Meduri GU, Varon J, Iglesias J, Marik PE. Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of COVID-19. Am J Ther (2021) 28(3):e299–318. doi: 10.1097/MJT.0000000000001377
119. Camprubí D, Almuedo-Riera A, Martí-Soler HI, Soriano A, Hurtado JC, Subirà C, et al. Lack of Efficacy of Standard Doses of Ivermectin in Severe COVID-19 Patients. PloS One (2020) 15(11):e0242184. doi: 10.1371/journal.pone.0242184
120. Chaccour C, Hammann F, Ramón-García S, Rabinovich NR. Ivermectin and COVID-19: Keeping Rigor in Times of Urgency. Am J Trop Med Hygiene (2020) 102:1156–7. doi: 10.4269/ajtmh.20-0271
121. Wang R, Simoneau CR, Kulsuptrakul J, Bouhaddou M, Travisano KA, Hayashi JM, et al. Genetic Screens Identify Host Factors for SARS-CoV-2 and Common Cold Coronaviruses. Cell (2021) 184(1):106–19. doi: 10.1016/j.cell.2020.12.004
122. Daniloski Z, Jordan TX, Wessels HH, Hoagland DA, Kasela S, Legut M, et al. Identification of Required Host Factors for SARS-CoV-2 Infection in Human Cells. Cell (2021) 184(1):92–105. doi: 10.1016/j.cell.2020.10.030
123. mac Kain A, Maarifi G, Aicher S-M, Arhel N, Baidaliuk A, Vallet T, et al. Identification of DAXX As A Restriction Factor Of SARS-CoV-2 Through A CRISPR/Cas9 Screen. bioRxiv (2021) 58(12). doi: 10.1101/2021.05.06.442916
124. Biering SB, Sarnik SA, Wang E, Zengel JR, Sathyan V, Nguyenla X, et al. Genome-Wide, Bidirectional CRISPR Screens Identify Mucins as Critical Host Factors Modulating SARS-CoV-2 Infection. bioRxiv (2021). doi: 10.1101/2021.04.22.440848
125. Baggen J, Persoons L, Vanstreels E, Jansen S, van Looveren D, Boeckx B, et al. Genome-Wide CRISPR Screening Identifies TMEM106B as a Proviral Host Factor for SARS-CoV-2. Nat Genet (2021) 53(4):435–44. doi: 10.1038/s41588-021-00805-2
126. Lazear HM, Schoggins JW, Diamond MS. Shared and Distinct Functions of Type I and Type III Interferons. Immunity (2019) 50:907–23. doi: 10.1016/j.immuni.2019.03.025
127. Gibbert K, Schlaak JF, Yang D, Dittmer U. IFN-α Subtypes: Distinct Biological Activities in Anti-Viral Therapy. Br J Pharmacol (2013) 168:1048–58. doi: 10.1111/bph.12010
128. Lokugamage KG, Hage A, de Vries M, Valero-Jimenez AM, Schindewolf C, Dittmann D, et al. Type I Interferon Susceptibility Distinguishes SARS-CoV-2 from SARS-CoV. J Virol (2020) 94(23):e01410–20. doi: 10.1128/JVI.01410-20
129. Mantlo E, Bukreyeva N, Maruyama J, Paessler S, Huang C. Antiviral Activities of Type I Interferons to SARS-CoV-2 Infection. Antiviral Res (2020) 179:104811. doi: 10.1016/j.antiviral.2020.104811
130. Baghaei P, Dastan F, Marjani M, Moniri A, Abtahian Z, Ghadimi S, et al. Combination Therapy of Ifnβ1 With Lopinavir–Ritonavir, Increases Oxygenation, Survival and Discharging of Sever COVID-19 Infected Inpatients. Int Immunopharmacol (2021) 92:107329. doi: 10.1016/j.intimp.2020.107329
131. Rahmani H, Davoudi-Monfared E, Nourian A, Khalili H, Hajizadeh N, Jalalabadi NZ, et al. Interferon β-1b in Treatment of Severe COVID-19: A Randomized Clinical Trial. Int Immunopharmacol (2020) 88:106903. doi: 10.1016/j.intimp.2020.106903
132. Davoudi-Monfared E, Rahmani H, Khalili H, Hajiabdolbaghi M, Salehi M, Abbasian L, et al. A Randomized Clinical Trial of the Efficacy and Safety of Interferon β-1a in Treatment of Severe COVID-19. Antimicrobial Agents Chemother (2020) 64(9):e01061–20. doi: 10.1128/AAC.01061-20
133. Zhou Q, Chen V, Shannon CP, Wei XS, Xiang X, Wang X, et al. Interferon-α2b Treatment for COVID-19. Front Immunol (2020) 11. doi: 10.3389/fimmu.2020.01061
134. Monk PD, Marsden RJ, Tear VJ, Brookes J, Batten TN, Mankowski M, et al. Safety and Efficacy of Inhaled Nebulised Interferon Beta-1a (SNG001) for Treatment of SARS-CoV-2 Infection: A Randomised, Double-Blind, Placebo-Controlled, Phase 2 Trial. Lancet Respir Med (2021) 9(2):196–206. doi: 10.1016/S2213-2600(20)30511-7
135. Wang N, Zhan Y, Zhu L, Hou Z, Liu F, Song P, et al. Retrospective Multicenter Cohort Study Shows Early Interferon Therapy Is Associated With Favorable Clinical Responses in COVID-19 Patients. Cell Host Microbe (2020) 28(3):455–64. doi: 10.1016/j.chom.2020.07.005
136. Estébanez M, Ramírez-Olivencia G, Mata T, Martí D, Gutierrez C, de Dios B, et al. Clinical Evaluation of IFN Beta1b in COVID-19 Pneumonia: A Retrospective Study. bioRxiv (2020). doi: 10.1101/2020.05.15.20084293
137. Schuhenn J, Meister TL, Todt D, Bracht T, Schork K, Billaud J-N, et al. Differential Interferon-α Subtype Immune Signatures Suppress SARS-CoV-2 Infection. bioRxiv (2021). doi: 10.1101/2021.05.20.444757
138. Guo K, Barrett BS, Mickens KL, Hasenkrug KJ, Santiago M. Interferon Resistance of Emerging SARS-CoV-2 Variants. bioRxiv (2021). doi: 10.1101/2021.03.20.436257
139. Vanderheiden A, Ralfs P, Chirkova T, Upadhyay AA, Zimmerman MG, Bedoya S, et al. Type I and Type III Interferons Restrict SARS-CoV-2 Infection of Human Airway Epithelial Cultures. J Virol (2020) 94(19):e00985–20. doi: 10.1128/JVI.00985-20
140. Dinnon KH, Leist SR, Schäfer A, Edwards CE, Martinez DR, Montgomery SA, et al. A Mouse-Adapted Model of SARS-CoV-2 to Test COVID-19 Countermeasures. Nature (2020) 586(7830):560–6. doi: 10.1038/s41586-020-2708-8
141. Jagannathan P, Andrews JR, Bonilla H, Hedlin H, Jacobson KB, Balasubramanian V, et al. Peginterferon Lambda-1a for Treatment of Outpatients With Uncomplicated COVID-19: A Randomized Placebo-Controlled Trial. Nat Commun (2021) 12(1):1967. doi: 10.21203/rs.3.rs-110659/v1
142. Feld JJ, Kandel C, Biondi MJ, Kozak RA, Zahoor MA, Lemieux C, et al. Peginterferon Lambda for the Treatment of Outpatients With COVID-19: A Phase 2, Placebo-Controlled Randomised Trial. Lancet Respir Med (2021) 9(5):498–510. doi: 10.1016/S2213-2600(20)30566-X
143. Braga Emidio N, Hoffmann W, Brierley SM, Muttenthaler M. Trefoil Factor Family: Unresolved Questions and Clinical Perspectives. Trends Biochem Sci (2019) 44:387–90. doi: 10.1016/j.tibs.2019.01.004
144. Fu W, Liu Y, Liu L, Hu H, Cheng X, Liu P, et al. An Open-Label, Randomized Trial of the Combination of IFN-κ Plus TFF2 With Standard Care in the Treatment of Patients With Moderate COVID-19. EClinicalMedicine (2020) 27:100547. doi: 10.1016/j.eclinm.2020.100547
145. Li C, Luo F, Liu C, Xiong N, Xu Z, Zhang W, et al. Effect of a Genetically Engineered Interferon-Alpha Versus Traditional Interferon-Alpha in the Treatment of Moderate-to-Severe COVID-19: A Randomised Clinical Trial. Ann Med (2021) 53(1):391–401. doi: 10.1080/07853890.2021.1890329
146. Scagnolari C, Vicenzi E, Bellomi F, Stillitano MG, Pinna D, Poli G, et al. Increased Sensitivity of SARS-Coronavirus to a Combination of Human Type I and Type II Interferons. Antiviral Ther (2004) 9(6):1003–11.
147. Sainz B, Mossel EC, Peters CJ, Garry RF. Interferon-Beta and Interferon-Gamma Synergistically Inhibit the Replication of Severe Acute Respiratory Syndrome-Associated Coronavirus (SARS-CoV). Virology (2004) 329(1):11–7. doi: 10.1016/j.virol.2004.08.011
148. Mossel EC, Sainz B, Garry RF, Peters CJ. Synergistic Inhibition of SARS-Coronavirus Replication by Type I and Type II IFN. Adv Exp Med Biol (2006) 581:503–6. doi: 10.1007/978-0-387-33012-9_89.
149. Yoshikawa T, Hill TE, Yoshikawa N, Popov VL, Galindo CL, Garner HR, et al. Dynamic Innate Immune Responses of Human Bronchial Epithelial Cells to Severe Acute Respiratory Syndrome-Associated Coronavirus Infection. PloS One (2010) 5(1):e8729. doi: 10.1371/journal.pone.0008729
150. Esquivel-Moynelo II, Vazquez-Blonquist DD, Cervantes CL, Campa-Legra II, Vizcaino TM, Lucila Muzio-Gonzalez VV, et al. Title: Effect of Combination of Interferon Alpha-2b and Interferon-Gamma or Interferon Alpha-2b Alone for Elimination of SARS-CoV-2 Viral RNA. Preliminary Results of a Randomized Controlled Clinical Trial. Available at: https://doi.org/10.1101/2020.07.29.20164251.
151. Kumaki Y, Ennis J, Rahbar R, Turner JD, Wandersee MK, Smith AJ, et al. Single-Dose Intranasal Administration With Mdef201 (Adenovirus Vectored Mouse Interferon-Alpha) Confers Protection From Mortality in a Lethal SARS-CoV BALB/c Mouse Model. Antiviral Res (2011) 89(1):75–82. doi: 10.1016/j.antiviral.2010.11.007
152. Meng Z, Wang T, Chen L, Chen X, Li L, Qin X, et al. The Effect of Recombinant Human Interferon Alpha Nasal Drops to Prevent COVID-19 Pneumonia for Medical Staff in an Epidemic Area. Curr Top Med Chem (2021) 21(10):920–7. doi: 10.2174/1568026621666210429083050
153. Schäcke H, Döcke WD, Asadullah K. Mechanisms Involved in the Side Effects of Glucocorticoids. Pharmacol Ther (2002) 96:23–43. doi: 10.2174/1568026621666210429083050
154. Poetker DM, Reh DD. A Comprehensive Review of the Adverse Effects of Systemic Corticosteroids. Otolaryngol Clin North Am (2010) 43:753–68. doi: 10.1016/j.otc.2010.04.003
155. Ledford H. Coronavirus Breakthrough: Dexamethasone is First Drug Shown to Save Lives. Nature (2020) 582:469. doi: 10.1038/d41586-020-01824-5
156. Bertram K, Susan M, Chrousos G.Chapter 39: Adrenocorticosteroids & Adrenocortical Antagonists. Basic and Clinical Pharmacology: Edition 12 (Access Medicine). Edited by Katzung BG, Kruidering-Hall M, Trevor AJ (2012).
157. Segal BH, Sneller MC. Infectious Complications of Immunosuppressive Therapy in Patients With Rheumatic Diseases. Rheumatic Dis Clinics North Am (1997) 23(2):219–23. doi: 10.1016/S0889-857X(05)70327-6
158. RECOVERY Collaborative Group, Horby P, Lim WS, Emberson J, Mafham M, Bell J, et al. Dexamethasone in Hospitalized Patients with Covid-19. N Engl J Med (2020) 384(8):693–704. doi: 10.1056/NEJMoa2021436
159. Villar J, Ferrando C, Martínez D, Ambrós A, Muñoz T, Soler JA, et al. Dexamethasone Treatment for the Acute Respiratory Distress Syndrome: A Multicentre, Randomised Controlled Trial. Lancet Respir Med (2020) 8(3):267–76. doi: 10.1016/S2213-2600(19)30417-5
160. Tomazini BM, Maia IS, Cavalcanti AB, Berwanger O, Rosa RG, Veiga VC, et al. Effect of Dexamethasone on Days Alive and Ventilator-Free in Patients With Moderate or Severe Acute Respiratory Distress Syndrome and COVID-19: The CoDEX Randomized Clinical Trial. JAMA - J Am Med Assoc (2020) 324(13):1307–16. doi: 10.1001/jama.2020.17021
161. Garibaldi BT, Wang K, Robinson ML, Zeger SL, Roche KB, Wang M-C, et al. Effectiveness of Remdesivir With and Without Dexamethasone in Hospitalized Patients With COVID-19. medRxiv (2020). doi: 10.1101/2020.11.19.20234153
162. Herold T, Jurinovic V, Arnreich C, Hellmuth J, von Bergwelt-Baildon M, Klein M, et al. Level of IL-6 Predicts Respiratory Failure in Hospitalized Symptomatic COVID-19 Patients. J Allergy Clin Immunol (2020) 146(1):128–36.e4. doi: 10.1016/j.jaci.2020.05.008
163. Saha A, Sharma AR, Bhattacharya M, Sharma G, Lee SS, Chakraborty C. Tocilizumab: A Therapeutic Option for the Treatment of Cytokine Storm Syndrome in COVID-19. Arch Med Res (2020) 51(6):595–7. doi: 10.1016/j.arcmed.2020.05.009
164. Hennigan S, Kavanaugh A. Interleukin-6 Inhibitors in the Treatment of Rheumatoid Arthritis. Ther Clin Risk Manage (2008) 4:767–75. doi: 10.2147/TCRM.S3470
165. Brunner HI, Ruperto N, Zuber Z, Keane C, Harari O, Kenwright A, et al. Efficacy and Safety of Tocilizumab in Patients With Polyarticular-Course Juvenile Idiopathic Arthritis: Results From a Phase 3, Randomised, Double-Blind Withdrawal Trial. Ann Rheumatic Dis (2015) 74(6):1110–7. doi: 10.1136/annrheumdis-2014-205351
166. Stone JH, Tuckwell K, Dimonaco S, Klearman M, Aringer M, Blockmans D, et al. Trial of Tocilizumab in Giant-Cell Arteritis. N Engl J Med (2017) 377(4):317–28. doi: 10.1056/NEJMoa1613849
167. Tanaka T, Narazaki M, Kishimoto T. Anti-Interleukin-6 Receptor Antibody, Tocilizumab, for the Treatment of Autoimmune Diseases. FEBS Lett (2011) 585:3699–709. doi: 10.1016/j.febslet.2011.03.023
168. Beneficencia Portuguesa de Sao Paulo. Safety and Efficacy of Tocilizumab in Moderate to Severe COVID-19 With Inflammatory Markers (TOCIBRAS). (2020). (https://clinicaltrials.gov/ct2/show/NCT04403685) [Accessed March 30,2021]
169. Luo P, Liu Y, Qiu L, Liu X, Liu D, Li J. Tocilizumab Treatment in COVID-19: A Single Center Experience. J Med Virol (2020) 92(7):814–8. doi: 10.1002/jmv.25801
170. Xu X, Han M, Li T, Sun W, Wang D, Fu B, et al. Effective Treatment of Severe COVID-19 Patients With Tocilizumab. Proc Natl Acad Sci USA (2020) 117(20):10970–5. doi: 10.1073/pnas.2005615117
171. Rosas IO, Bräu N, Waters M, Go RC, Hunter BD, Bhagani S, et al. Tocilizumab in Hospitalized Patients With Severe Covid-19 Pneumonia. N Engl J Med (2021) 384(16):1503–16. doi: 10.1056/NEJMc2100217
172. Salama C, Han J, Yau L, Reiss WG, Kramer B, Neidhart JD, et al. Tocilizumab in Patients Hospitalized With Covid-19 Pneumonia. N Engl J Med (2021) 384(1):20–30. doi: 10.1056/NEJMoa2030340
173. Hermine O, Mariette X, Tharaux PL, Resche-Rigon M, Porcher R, Ravaud P. Effect of Tocilizumab vs Usual Care in Adults Hospitalized With COVID-19 and Moderate or Severe Pneumonia: A Randomized Clinical Trial. JAMA Internal Med (2021) 181(1):144. doi: 10.1001/jamainternmed.2021.2209
174. Salvarani C, Dolci G, Massari M, Merlo DF, Cavuto S, Savoldi L, et al. Effect of Tocilizumab vs Standard Care on Clinical Worsening in Patients Hospitalized With COVID-19 Pneumonia: A Randomized Clinical Trial. JAMA Internal Med (2021) 181(1):24–31. doi: 10.1001/jamainternmed.2021.0404
175. Stone JH, Frigault MJ, Serling-Boyd NJ, Fernandes AD, Harvey L, Foulkes AS, et al. Efficacy of Tocilizumab in Patients Hospitalized With Covid-19. New Engl J Med (2020) 383(24):2333–44. doi: 10.1056/NEJMoa2028836
176. Kupferschmidt K. World’s Largest COVID-19 Drug Trial Identifies Second Compound That Cuts Risk of Death. Science (2021). doi: 10.1126/science.abh0459
177. van Rhee F, Wong RS, Munshi N, Rossi JF, Ke XY, Fosså A, et al. Siltuximab for Multicentric Castleman’s Disease: A Randomised, Double-Blind, Placebo-Controlled Trial. Lancet Oncol (2014) 15(9):966–74. doi: 10.1016/S1470-2045(14)70319-5
178. Gritti G, Raimondi F, Ripamonti D, Riva I, Landi F, Alborghetti L, et al. Use of Siltuximab in Patients With COVID-19 Pneumonia Requiring Ventilatory Support. medRxiv (2020). doi: 10.1101/2020.04.01.20048561
179. Fang W, Cai SX, Wang CL, Sun XX, Li K, Yan XW, et al. Modulation of Mitogen-Activated Protein Kinase Attenuates Sepsis-Induced Acute Lung Injury in Acute Respiratory Distress Syndrome Rats. Mol Med Rep (2017) 16(6):9652–8. doi: 10.3892/mmr.2017.7811
180. Ma XL, Kumar S, Gao F, Louden CS, Lopez BL, Christopher TA, et al. Inhibition of P38 Mitogen-Activated Protein Kinase Decreases Cardiomyocyte Apoptosis and Improves Cardiac Function After Myocardial Ischemia and Reperfusion. Circulation (1999) 99(13):1685–91. doi: 10.1161/01.CIR.99.13.1685
181. Zarubin T, Han J. Activation and Signaling of the P38 MAP Kinase Pathway. Cell Res (2005) 15:11–8. doi: 10.1038/sj.cr.7290257
182. Bouhaddou M, Memon D, Meyer B, White KM, v RV, Correa Marrero M, et al. The Global Phosphorylation Landscape of SARS-CoV-2 Infection. Cell (2020) 182(3):685–712. doi: 10.1016/j.cell.2020.06.034
183. Stukalov A, Girault V, Grass V, Karayel O, Bergant V, Urban C, et al. Multilevel Proteomics Reveals Host Perturbations by SARS-CoV-2 and SARS-CoV. Nature (2021) 594(7862):246–52. doi: 10.1038/s41586-021-03493-4
184. Grimes JM, Grimes KV. P38 MAPK Inhibition: A Promising Therapeutic Approach for COVID-19. J Mol Cell Cardiol (2020) 144:63–5. doi: 10.1016/j.yjmcc.2020.05.007
185. Babon JJ, Lucet IS, Murphy JM, Nicola NA, Varghese LN. The Molecular Regulation of Janus Kinase (JAK) Activation. Biochem J (2014) 462:1–13. doi: 10.1042/BJ20140712
186. Renauld JC. Class II Cytokine Receptors and Their Ligands: Key Antiviral and Inflammatory Modulators. Nat Rev Immunol (2003) 3:667–76. doi: 10.1038/nri1153
187. Richardson P, Griffin I, Tucker C, Smith D, Oechsle O, Phelan A, et al. Baricitinib as Potential Treatment for 2019-Ncov Acute Respiratory Disease. Lancet (2020) 395:e30–1. doi: 10.1016/S0140-6736(20)30304-4
188. McInnes IB, Byers NL, Higgs RE, Lee J, Macias WL, Na S, et al. Comparison of Baricitinib, Upadacitinib, and Tofacitinib Mediated Regulation of Cytokine Signaling in Human Leukocyte Subpopulations. Arthritis Res Ther (2019) 21(1):183. doi: 10.1186/s13075-019-1964-1
189. Hoang TN, Pino M, Boddapati AK, Viox EG, Starke CE, Upadhyay AA, et al. Baricitinib Treatment Resolves Lower-Airway Macrophage Inflammation and Neutrophil Recruitment in SARS-CoV-2-Infected Rhesus Macaques. Cell (2021) 184(2):460–75. doi: 10.1016/j.cell.2020.11.007
190. Kalil AC, Patterson TF, Mehta AK, Tomashek KM, Wolfe CR, Ghazaryan V, et al. Baricitinib Plus Remdesivir for Hospitalized Adults With Covid-19. N Engl J Med (2021) 384(9):795–807. doi: 10.1056/NEJMoa2031994
191. The U.S. Food and Drug Administration (FDA). Fact Sheet for Healthcare Providers Emergency Use Authorization (EUA) of Baricitinib [Internet]. Available at: www.lillytrade.com.
192. Kucharz EJ, Stajszczyk M, Kotulska-Kucharz A, Batko B, Brzosko M, Jeka S, et al. Tofacitinib in the Treatment of Patients With Rheumatoid Arthritis: Position Statement of Experts of the Polish Society for Rheumatology. Reumatologia (2018) 56(4):203–11. doi: 10.5114/reum.2018.77971
193. Maslennikov R, Ivashkin V, Vasilieva E, Chipurik M, Semikova P, Semenets V, et al. Tofacitinib Reduces Mortality in Coronavirus Disease 2019 Tofacitinib in COVID-19. Pulmonary Pharmacol Ther (2021) 69:102039. doi: 10.1016/j.pupt.2021.102039
194. Verstovsek S, Mesa RA, Gotlib J, Levy RS, Gupta V, DiPersio JF, et al. A Double-Blind, Placebo-Controlled Trial of Ruxolitinib for Myelofibrosis. N Engl J Med (2012) 366(9):799–807. doi: 10.1056/NEJMoa1110557
195. la Rosée F, Bremer HC, Gehrke I, Kehr A, Hochhaus A, Birndt S, et al. The Janus Kinase 1/2 Inhibitor Ruxolitinib in COVID-19 With Severe Systemic Hyperinflammation. Leukemia (2020) 34(7):1805–15. doi: 10.1038/s41375-020-0891-0
196. Shakoory B, Carcillo JA, Chatham WW, Amdur RL, Zhao H, Dinarello CA, et al. Interleukin-1 Receptor Blockade Is Associated With Reduced Mortality in Sepsis Patients With Features of Macrophage Activation Syndrome: Reanalysis of a Prior Phase III Trial∗. Crit Care Med (2016) 44(2):275–81. doi: 10.1097/CCM.0000000000001402
197. Kyriazopoulou E, Panagopoulos P, Metallidis S, Dalekos GN, Poulakou G, Gatselis N, et al. An Open Label Trial of Anakinra to Prevent Respiratory Failure in Covid-19. eLife (2021) 10:e66125. doi: 10.7554/eLife.66125
198. Qiu P, Cui X, Sun J, Welsh J, Natanson C, Eichacker PQ. Antitumor Necrosis Factor Therapy is Associated With Improved Survival in Clinical Sepsis Trials: A Meta-Analysis. Crit Care Med (2013) 41:2419–29. doi: 10.1097/CCM.0b013e3182982add
199. McDermott JE, Mitchell HD, Gralinski LE, Eisfeld AJ, Josset L, Bankhead A, et al. The Effect of Inhibition of PP1 and Tnfα Signaling on Pathogenesis of SARS Coronavirus. BMC Syst Biol (2016) 10(1):93. doi: 10.1186/s12918-016-0336-6
200. Leuschner F, Dutta P, Gorbatov R, Novobrantseva TI, Donahoe JS, Courties G, et al. Therapeutic siRNA Silencing in Inflammatory Monocytes in Mice. Nat Biotechnol (2011) 29(11):1005–10. doi: 10.1038/nbt.1989
201. Uccelli A, de Rosbo NK. The Immunomodulatory Function of Mesenchymal Stem Cells: Mode of Action and Pathways. Ann New York Acad Sci (2015) 1351(1):114–26. doi: 10.1111/nyas.12815
202. Marshall M. The Lasting Misery of Coronavirus Long-Haulers. Nature (2020) 585(7825):339–41. doi: 10.1038/d41586-020-02598-6
203. Carfì A, Bernabei R, Landi F, for the Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA (2020) 324(6):603–5. doi: 10.1001/jama.2020.12603
204. Mandal S, Barnett J, Brill SE, Brown JS, Denneny EK, Hare SS, et al. Long-Covid’: A Cross-Sectional Study of Persisting Symptoms, Biomarker and Imaging Abnormalities Following Hospitalisation for COVID-19. Thorax (2021) 76(4):396–8. doi: 10.1136/thoraxjnl-2020-215818
205. Huang C, Huang L, Wang Y, Li X, Ren L, Gu X, et al. 6-Month Consequences of COVID-19 in Patients Discharged From Hospital: A Cohort Study. Lancet (2021) 397(10270):220–32. doi: 10.1016/S0140-6736(20)32656-8
206. Dennis A, Wamil M, Alberts J, Oben J, Cuthbertson DJ, Wootton D, et al. Multiorgan Impairment in Low-Risk Individuals With Post-COVID-19 Syndrome: A Prospective, Community-Based Study. BMJ Open (2021) 11(3):e048391. doi: 10.1136/bmjopen-2020-048391
207. Editorial. Long COVID: Let Patients Help Define Long-Lasting COVID Symptoms. Nature (2020) 586. doi: 10.1038/d41586-020-02796-2
208. Callard F, Perego E. How and Why Patients Made Long Covid. Soc Sci Med (2021) 268:113426. doi: 10.1016/j.socscimed.2020.113426
210. Venkatesan P. NICE Guideline on Long COVID. Lancet Respir Med (2021) 9(2):129. doi: 10.1016/S2213-2600(21)00031-X
211. NIHR. Living With Covid-19. A Dynamic Review of the Evidence Around Ongoing Covid-19 Symptoms (Often Called Long Covid) (https://evidence.nihr.ac.uk/themedreview/living-with-covid19/). Accessed: October 15, 2020. doi: 10.3310/themedreview_41169
212. Editorial. Meeting the Challenge of Long COVID. Nat Med (2020) 26. doi: 10.1038/s41591-020-01177-6
213. Gaebler C, Wang Z, Lorenzi JCC, Muecksch F, Finkin S, Tokuyama M, et al. Evolution of Antibody Immunity to SARS-CoV-2. Nature (2021) 591(7851):639–44. doi: 10.1101/2020.11.03.367391
214. Dani M, Dirksen A, Taraborrelli P, Torocastro M, Panagopoulos D, Sutton R, et al. Autonomic Dysfunction in ‘Long COVID’: Rationale, Physiology and Management Strategies. Clin Med J R Coll Phys London (2021) 21(1):e63–7. doi: 10.7861/clinmed.2020-0896
215. Wallukat G, Hohberger B, Wenzel K, Fürst J, Schulze-Rothe S, Wallukat A, et al. Functional Autoantibodies Against G-Protein Coupled Receptors in Patients With Persistent Long-COVID-19 Symptoms. J Trans Autoimmun (2021) 4:100100. doi: 10.1016/j.jtauto.2021.100100
216. Arnold DT, Milne A, Samms E, Stadon L, Maskell NA, Hamilton FW. Are Vaccines Safe in Patients With Long COVID? A Prospective Observational Study. medRxiv (2021). doi: 10.1101/2021.03.11.21253225
217. LongCovidSOS. The Impact of COVID Vaccination on Symptoms of Long Covid. An International Survey of 900 People With Lived Experience. (2021). (https://www.longcovidsos.org/post/longcovidsos-publish-results-of-their-survey-into-the-impact-of-vaccination-on-long-covid-symptoms) [Accessed May 18,2021].
Keywords: SARS-CoV-2, COVID-19, interferons, antivirals, immunomodulators, Long COVID
Citation: Kumar S, Çalışkan DM, Janowski J, Faist A, Conrad BCG, Lange J, Ludwig S and Brunotte L (2021) Beyond Vaccines: Clinical Status of Prospective COVID-19 Therapeutics. Front. Immunol. 12:752227. doi: 10.3389/fimmu.2021.752227
Received: 02 August 2021; Accepted: 14 September 2021;
Published: 01 October 2021.
Edited by:
Mauro Martins Teixeira, Federal University of Minas Gerais, BrazilReviewed by:
Eizo Takashima, Ehime University, JapanMarc Paul Girard, Université Paris Diderot, France
Copyright © 2021 Kumar, Çalışkan, Janowski, Faist, Conrad, Lange, Ludwig and Brunotte. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Linda Brunotte, YnJ1bm90dGVAdW5pLW11ZW5zdGVyLmRl