 Noémi Zádori1,2
Noémi Zádori1,2 Lajos Szakó1,2
Lajos Szakó1,2 Szilárd Váncsa1,2,3
Szilárd Váncsa1,2,3 Nóra Vörhendi1,2
Nóra Vörhendi1,2 Eduard Oštarijaš1
Eduard Oštarijaš1 Szabolcs Kiss1,4,5
Szabolcs Kiss1,4,5 Levente Frim1
Levente Frim1 Péter Hegyi1,2,3,6
Péter Hegyi1,2,3,6 József Czimmer1,7*
József Czimmer1,7*- 1Institute for Translational Medicine, Medical School, University of Pécs, Pécs, Hungary
- 2János Szentágothai Research Centre, University of Pécs, Pécs, Hungary
- 3Centre for Translational Medicine, Semmelweis University, Budapest, Hungary
- 4Doctoral School of Clinical Medicine, University of Szeged, Szeged, Hungary
- 5Heim Pál National Pediatric Institute, Budapest, Hungary
- 6Division of Pancreatic Diseases, Heart and Vascular Center, Semmelweis University, Budapest, Hungary
- 7Division of Gastroenterology, First Department of Medicine, Medical School, University of Pécs, Pécs, Hungary
Background: Gastric cancer is one of the most common cancers worldwide, with a high mortality rate. The potential etiological role of autoimmune (AI) disorders has been described in gastric cancer; however, the literature is controversial. This study aims to provide a comprehensive summary of the association between autoimmune disorders and the incidence of gastric cancer.
Methods: This study was registered on PROSPERO under registration number CRD42021262875. The systematic literature search was conducted in four scientific databases up to May 17, 2021. Studies that reported standardized incidence rate (SIR) of gastric cancer in autoimmune disorders were eligible. We calculated pooled SIRs with 95% confidence intervals (CIs) in this meta-analysis.
Results: We included 43 articles describing 36 AI disorders with data of 499,427 patients from four continents in our systematic review and meta-analysis. Significantly increased incidence of gastric cancer was observed in dermatomyositis (SIR = 3.71; CI: 2.04, 6.75), pernicious anemia (SIR = 3.28; CI: 2.71, 3.96), inflammatory myopathies (SIR = 2.68; CI:1.40; 5.12), systemic lupus erythematosus (SIR = 1.48; CI: 1.09, 2.01), diabetes mellitus type I (SIR = 1.29; CI:1.14, 1,47), and Graves’ disease (SIR = 1.28; CI: 1.16, 1.41). No significant associations could be found regarding other AI disorders.
Conclusions: Pernicious anemia, Graves’ disease, dermatomyositis, diabetes mellitus type I, inflammatory myopathies, and systemic lupus erythematosus are associated with higher incidence rates of gastric cancer. Therefore, close gastroenterological follow-up or routinely performed gastroscopy and application of other diagnostic measures may be cost-effective and clinically helpful for patients diagnosed with these autoimmune diseases.
Introduction
Malignant neoplasm of the stomach is one of the most common cancers worldwide, affecting over 20,000 patients yearly in the USA. The average 5-year survival rate is less than 20%, underlining the importance of the disease (1, 2). This poor prognosis can be improved by early diagnosis. If the tumor is detected and treated before reaching the muscular layer of the stomach (T1), the 5-year survival rate can be up to 90% (3).
A significant decline in incidence and mortality can be observed over the past few decades (4), which can be attributed to the recognition of certain causative factors, decreased incidence of Helicobacter pylori infection, and decreased use of tobacco and dietary salt (2, 5). While the overall rate of gastric cancer has been declining, the distribution of its subtype was changing neoplasms of the cardia and gastro-esophagal junction became more frequent, and an unexplained increased incidence among younger than 50 years of age, particularly in females, could be observed (5–8).
Despite the effective H. pylori eradication strategies, gastric cancer remains the fifth most common cancer worldwide (9), highlighting the possibility of further etiological factors. Besides H. pylori, autoimmune gastritis is another common cause of gastric cancer, reflecting 7.8%–19.5% of the cases, and thought to be another possible cause of the rising incidence of gastric cancer in females younger than 50 years of age (5, 7, 10).
The incidence of autoimmune gastritis and generally autoimmune diseases has increased in the past few decades (11–13). Several previous studies have described the potential association of autoimmunity and gastric cancer (14, 15), but up to date, data have been controversial regarding cause-effect relationships and underlying pathomechanism. Our study aims to provide a comprehensive summary of the potential association between autoimmune disorders and the incidence of gastric cancer in the form of a meta-analysis and systematic review.
Methods and Materials
This meta-analysis was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 Statement (16). The protocol of this analysis was registered on the PROSPERO International Prospective Register of Systematic Reviews in advance (CRD42021262875). We did not deviate from the protocol.
Systematic Search
The systematic literature search was conducted in four scientific databases—MEDLINE via PubMed; Cochrane Central Register of Controlled Trials (CENTRAL); Embase; and Web of Science, Latin American and Caribbean Health Sciences Literature (LILACS)—up to May 17, 2021. The following search terms were used without any restriction to language or other filters: (stomach OR gastric) AND (neoplas* OR malign* OR cancer OR carcinoma OR lymphoma OR tumor OR tumour) AND (“autoimmun*” OR autoaggressive OR autoantibody OR lupus OR rheuma* OR Addison* OR celiac OR “gluten sensitive” OR dermatomyositis OR Hashimoto OR graves OR sclerosis OR scleroderma OR myasthenia OR arthritis OR Sjögren*). Additionally, reference lists of the citing and cited articles were screened for eligibility.
Selection and Eligibility of Studies
Duplicates were removed with EndNote X9 software (Clarivate Analytics, Philadelphia, PA, USA) manually. Two investigators (NV, NZ) screened the titles and abstracts and full texts to identify eligible articles. Disagreements were resolved by another investigator (LF, JC).
We included any peer-reviewed studies reporting the standardized incidence ratio (SIR) (O) of gastric cancer in an autoimmune disorder (E) in the general population (P). There were no restrictions on the type of gastric cancer, language, or study design eligible for inclusion. Only full texts were included. Studies with no event rate of SIR were excluded.
Data Extraction
Two independent researchers (NZ, NV) extracted data from the eligible studies into a standardized data collection form. Extracted data were validated by a third reviewer (LF). All disagreements were resolved by a fourth independent author (SV). The following data were extracted from each included study: title, first author, year of publication, country, study design, age of the population (mean, standard deviation (SD), median, interquartile ranges), gender distribution, the total number of patients (with autoimmune disorders), type of autoimmune disorders, follow-up time, and standardized incidence ratios of gastric cancer (observed, expected, SIR, confidence interval).
Data Synthesis
We provided summaries of the rate of gastric cancer in each autoimmune disorder (frequency of gastric cancer in each autoimmune disease) by pooling standardized incidence ratios (SIRs) as an outcome for selected autoimmune disorders. SIRs were first extracted and then pooled using the inverse variance method and random-effects model with the restricted maximum-likelihood (REML) estimation. Subsequently, the results were displayed on forest plots. Summary SIR estimation, p-value, and 95% confidence interval (CI) were calculated.
Statistical heterogeneity was analyzed using the I² statistic and the χ² test to acquire probability values; p < 0.1 is defined to indicate significant heterogeneity. As suggested by the Cochrane Handbook, I2 values were interpreted as moderate (30%–60%), substantial (50%–90%), and considerable (75%–100%) heterogeneity (17). Publication bias was checked by Funnel plot and Egger’s test (alpha = 0·1) (18). The Eggers test was performed for each autoimmune disorder, where there were more than 10 studies included.
Subgroup analyzes were performed considering high-incidence or low-incidence countries for gastric cancer (10) and based on gender. A minimum number of studies were three for performing quantitative synthesis. Otherwise, findings were summarized in the qualitative synthesis.
All analyses were performed using R statistical software (R Foundation, Vienna, Austria) with the meta package (Guido Schwarzer, v4.18-2).
Risk of Bias Assessment in Individual Studies
Based on the recommendations of Cochrane Prognosis Methods Group (PMG), the Quality in Prognostic Studies (QUIPS) tool was used by two independent investigators (NV, LF) to assess the quality of the studies included, focusing on the definition of prognostic factors and outcomes (19). Disagreements were resolved by a third investigator (NZ). Details of the QUIPS are shown in Supplementary Table S2.
Results
Search and Selection
The systemic search yielded 18,206 records, of which 12,420 remained after duplicate removal. Following the selection process, 43 articles were included in the systematic review and meta-analysis. Results of the selection are presented in Figure 1.
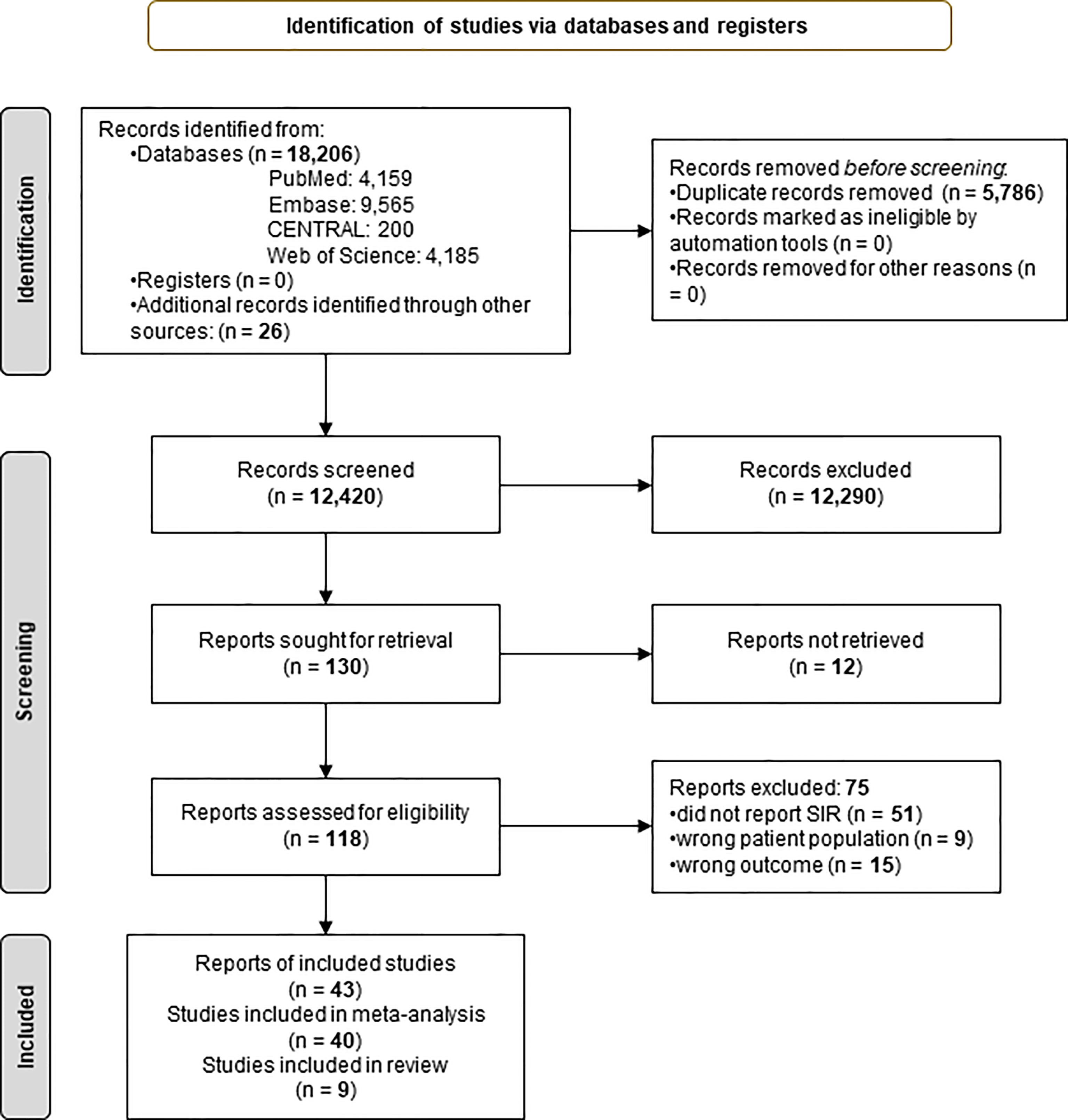
Figure 1 Preferred Reporting in Systematic Reviews and Meta-analyses 2020 (PRISMA) flowchart showing the selection process (16).
Basic Characteristics of the Included Studies
Four studies were retrospective from the included 43 articles, and 39 were prospective, describing 36 autoimmune disorders altogether. The overall work, including the qualitative and quantitative synthesis, contains 499,427 patients from four continents (America, Europe, Asia, and Australia) and 15 countries. The general characteristics of the included articles are presented in Table 1.
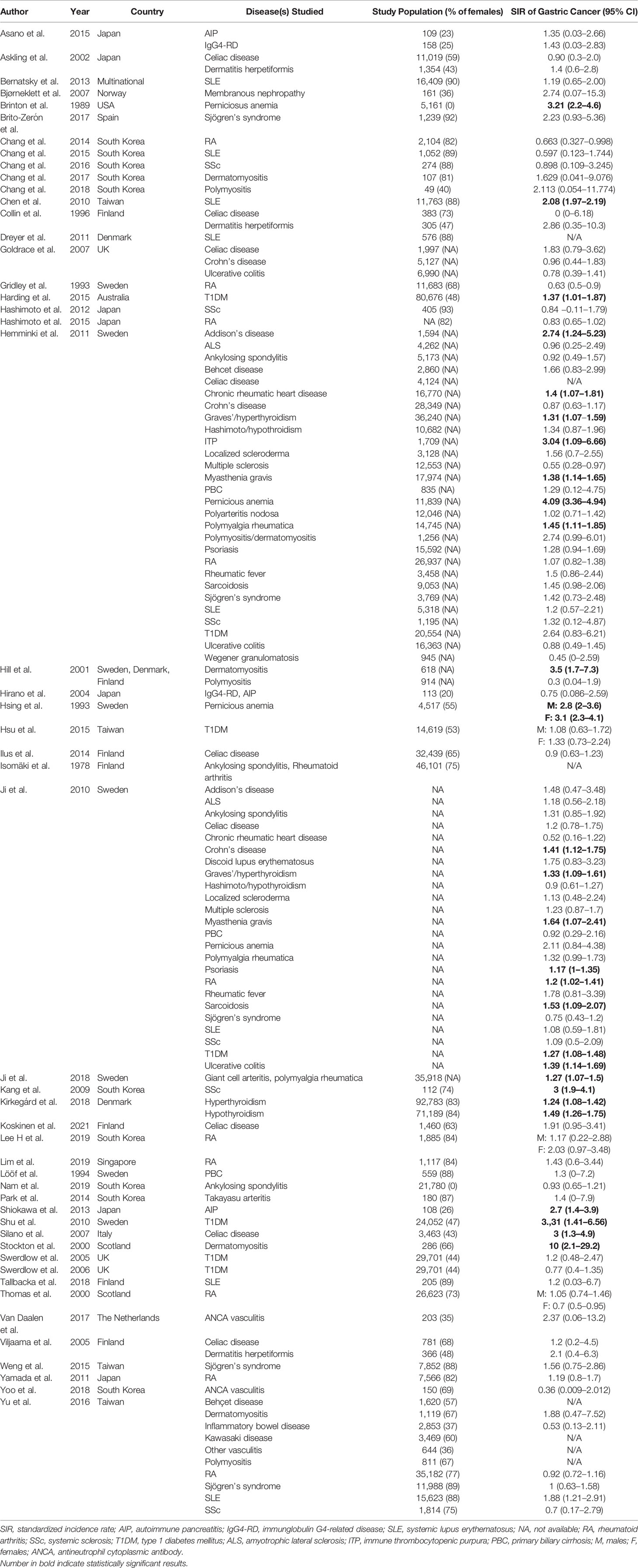
Table 1 Basic characteristics of included studies.
Analytical Results of Associations of Autoimmune Diseases and Gastric Cancer
Significantly increased incidence of gastric cancer was observed in the cases dermatomyositis (SIR = 3.71; 95% CI: 2.04, 6.75; p < 0.0001) based on four studies, pernicious anemia (SIR = 3.28; 95% CI: 2.71, 3.96; p < 0.0001) based on five studies, inflammatory myopathies (SIR = 2.68; 95% CI:1.40; 5.12; p = 0.0029) based on seven articles, systemic lupus erythematosus (SIR = 1.48; 95% CI: 1.09, 2.01; p = 0.0116) according to the analysis of seven records, diabetes mellitus type I (SIR = 1.29; 95% CI:1.14, 1.47; p < 0.0001) according to eight studies, and Graves’ disease (SIR = 1.28; 95% CI: 1.16, 1.41; p < 0.0001) in the analysis of three studies. No significant differences could be found regarding autoimmune vasculitis, celiac disease, systemic sclerosis, dermatitis herpetiformis, Hashimoto thyroiditis, Sjogren’s syndrome, inflammatory bowel disease, Crohn’s disease, rheumatoid arthritis, ulcerative colitis, ankylosing spondylitis, and primary biliary cirrhosis. Detailed results are presented in Figure 2.
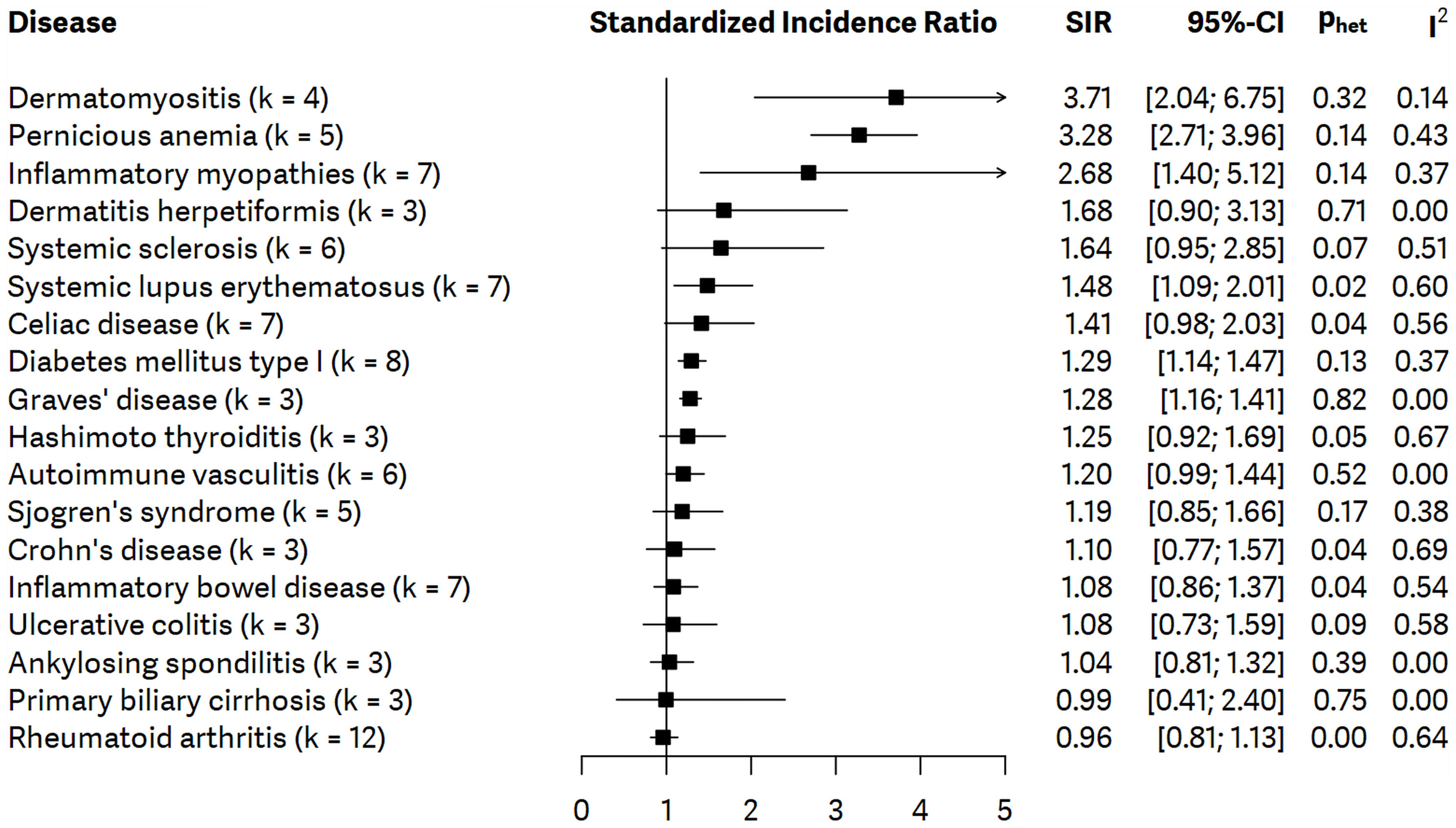
Figure 2 Summarizing forest plot with pooled standardized incidence ratios (SIRs), representing the incidence of gastric cancer in all patients with autoimmune disorders included in meta-analysis; number of studies – k.
Subgroup Analysis Based on Gender
Diabetes mellitus type I increased the incidence of gastric cancer in female patients (SIR = 1.62; 95% CI: 1.20, 2.18) but not in male patients. Rheumatoid arthritis did not increase the incidence of gastric cancer in male or female patients. Subgroup analysis could not be performed regarding other autoimmune diseases. Results of the subgroup analysis based on gender are presented in Supplementary Figures S39, S40.
Subgroup Analysis Based on the Incidence of Gastric Cancer
Pernicious anemia (SIR = 3.28; 95% CI: 2.71, 3.96), diabetes mellitus type I (SIR = 1.41; 95% CI: 1.02, 1.95), Graves’ disease (SIR = 1.28; 95% CI: 1.61, 1.41), and autoimmune vasculitis (SIR = 1.21; 95% CI: 1.01, 1.44) were associated with gastric cancer in low-incidence countries.
Systemic lupus erythematosus (SIR = 1.69; 95% CI: 1.21, 2.36) was associated with increased incidence of gastric cancer in high-incidence countries. However, in the case of dermatomyositis, subgroup analysis could not be performed, it was also associated with gastric cancer (SIR = 5.10; 95% CI: 1.90, 13.67) in low-incidence countries, based on two studies. We did not find significant statistical difference concerning the other autoimmune diseases. The detailed results of the subgroup analysis are presented in Supplementary Figures S41–S56.
Qualitative Synthesis
Eighteen other autoimmune disorders were included in the qualitative synthesis. The individual articles found an increased incidence of gastric cancer in the cases of immune thrombocytopenic purpura (20), membranous nephropathy (21), Addison’s disease (20, 22), discoid lupus (22), Bechet’s disease (20, 23), sarcoidosis (20, 22), myasthenia gravis (20, 22), Takayasu arteritis (24), polymyalgia rheumatica (20, 22), localized scleroderma (20, 22), and psoriasis (20, 22). Chronic rheumatic heart disease (20, 22), IgG4-related disease (25, 26), ANCA-vasculitis (27, 28), multiple sclerosis (20, 22), and granulomatosis with polyangiitis (20) seem not to be associated with elevated incidence of gastric cancer. The detailed results of the qualitative synthesis are presented in Figure 3.
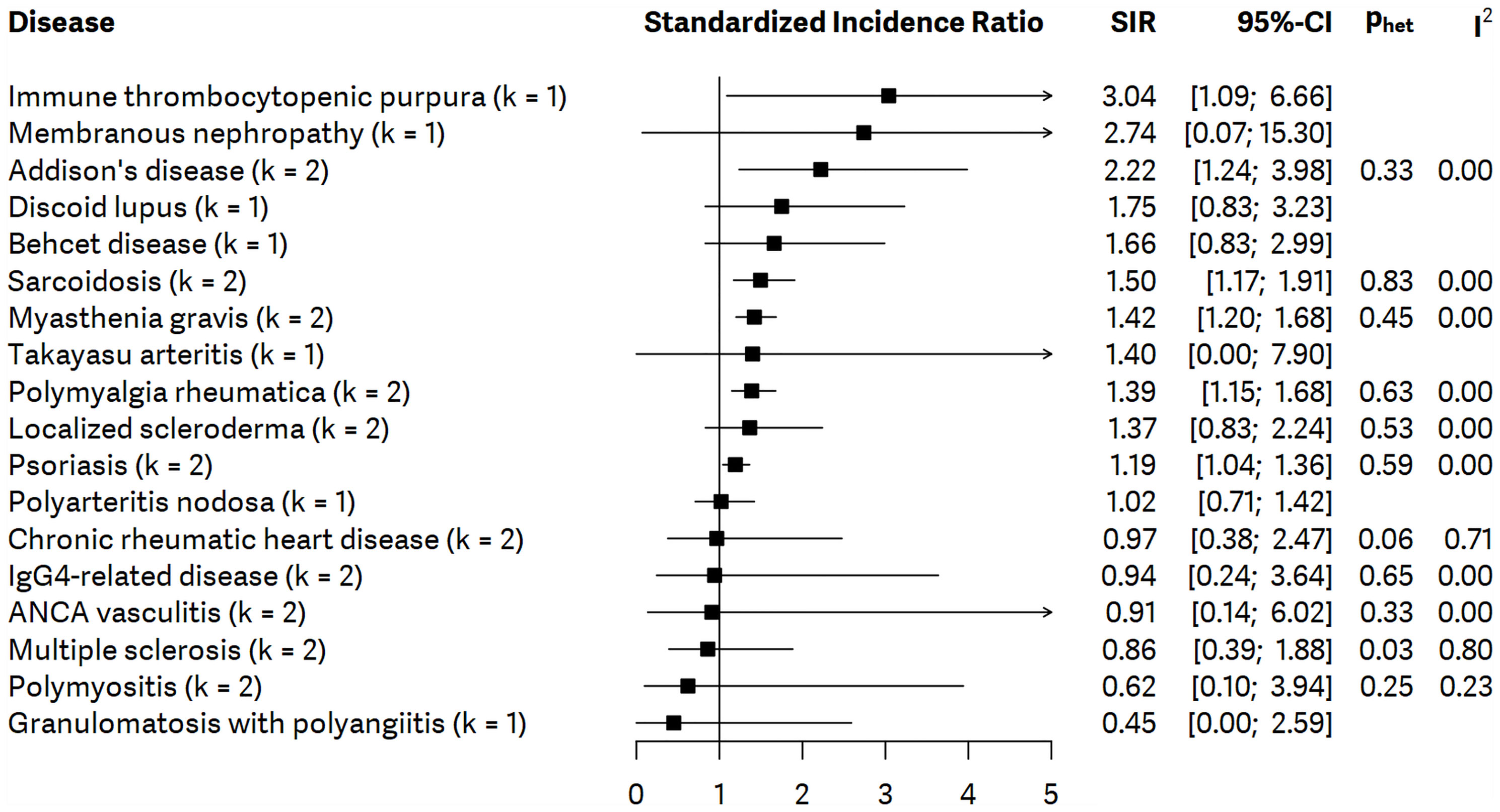
Figure 3 Summarizing forest plot with pooled standardized incidence ratios (SIRs), representing the incidence of gastric cancer in all patients with autoimmune disorders included in qualitative synthesis; number of studies – k.
Risk of Bias Assessment
Results and a detailed description of the risk of bias assessment according to the QUIPS tool are presented in Supplementary Table S2.
Publication bias was assessed for rheumatoid arthritis by the Egger’s test, which does not indicate the presence of Funnel plot asymmetry. Therefore, we concluded that no publication bias was present. Funnel plot is presented in Supplementary Figure S57.
Statistical Heterogeneity
The heterogeneity analysis proved to be significant in the analysis of rheumatoid arthritis (I2 = 0.64; p = 0.00), inflammatory bowel disease (I2 = 0.54; p = 0.04), systemic lupus erythematosus (I2 = 0.60; p = 0.02), coeliac disease (I2 = 0.56; p = 0.04), Crohn’s disease (I2 = 0.69; p = 0.04), and rheumatoid arthritis in the case of subgroup analysis of female patients (I2 = 0.69; p=0.01). Other comparisons did not prove to be significant regarding heterogeneity. Detailed results of heterogeneity are presented in Supplementary Figure S1.
Discussion
This meta-analysis, including data of 499,427 patients collected from 43 studies, was conducted to understand the relationship between autoimmunity and gastric cancer. Based on our results, the incidence of gastric cancer significantly increased in patients with pernicious anemia, Graves’ disease, dermatomyositis, diabetes mellitus type I, inflammatory myopathies, and systemic lupus erythematosus.
In line with our results, the literature suggests that patients with dermatomyositis, rheumatoid arthritis, scleroderma, systemic lupus erythematosus, or diabetes mellitus type I may have an increased risk for developing multiple cancers (29–34). Positive associations have been observed between various gastrointestinal tumors and rheumatoid arthritis, systemic lupus erythematosus, Sjögren’s syndrome, celiac disease, idiopathic inflammatory myositis, and systemic sclerosis (35–39).
A recent meta-analysis described a correlation between autoimmune disorders and increased risk of gastric cancer (40). Song et al. concluded that patients with dermatomyositis, pernicious anemia, Addison’s disease, dermatitis herpetiformis, IgG4-related disease, primary biliary cirrhosis, diabetes mellitus type I, systemic lupus erythematosus, and Graves’ disease had elevated risk for developing gastric neoplasms.
Pernicious anemia has been demonstrated as a risk factor for gastric cancer (41) since it correlates with autoimmune gastritis and results from gastric mucosal damage. This pathomechanism has been modeled in mice and has suggested an association between autoimmunity and carcinogenesis (14). Autoimmune thyroiditis, diabetes mellitus type I, vitiligo, and Addison disease are frequently associated with pernicious anemia.
An increase in the incidence of autoimmune diseases has been observed recently parallelly with the increasing incidence of cancers. The autoimmune inflammation often correlates with the tumorous disorder of the affected organ. This phenomenon is most conspicuous in people below 50 years of age, and it affects females more considering the development of gastric cancer (7, 8).
Although autoimmune processes can play a significant role in developing different cancers, the exact pathomechanisms remain unclear. Several common factors can be identified, such as immunosuppression/dysregulation, infections, dietary habits, environmental factor, and chronic inflammation. These factors can induce chronic cell damage and can trigger either autoimmune conditions or cancer (12). Autoimmune disorders may lead to antigen specificity-driven tissue damage causing chronic inflammation, whose role in carcinogenesis is well known and precedes the tumor formation in time (42).
Regarding the strengths of our meta-analysis, we included a large number of cohort studies. Many of our analytical results proved to be significant. This comprehensive work contains wide coverage of AI disorders from 15 different countries and four continents of the currently available literature so far. Following the PRISMA Statement and a rigorous methodology, the quality is secured. The key questions of this study were not widely investigated recently; thus, most of our findings are novel.
The formerly mentioned meta-analysis (40) discussing the question of interest had several limitations. Compared with that work, a more general search key was used in our study, which allowed us to find a higher number of relevant records. Our search was conducted in four databases compared with the two in the previous work, which also contributed to the identification of further eligible studies. They calculate pooled relative risk ratios (RR) with 95% CI; however, hazard ratios, SIRs, RRs, and standardized mortality rates were pooled into RR. Statistical analysis of our study is also more coherent as only SIR-s were calculated consistently (43, 44).
However, our analysis has some limitations, which should be considered for a correct interpretation. Firstly, other risk factors for gastric cancer, such as H. pylori infection status, smoking, dietary habits, obesity, occupational exposure to dust, high-temperature particulates, and metals such as chromium VI, gastric surgery (by-pass), and Epstein-Barr infection could be present that were not measured or reported. We also did not have information about drugs taken for autoimmune disorders, so how it may affect the outcome is unknown. However, according to 10 included articles, the mean time interval from the diagnosis of AI disorder to the diagnosis of cancer is 2–7.4 years. Although, the mentioned time intervals refer to the development of any type of cancer in general, not only to gastric cancer.
The diagnosis of AI diseases in countries could be different, which could create significant heterogeneity in some of the analyses. The presence of ascertainment cannot be ruled out, since people with an autoimmune disease are subjected to medical examinations more frequently, than the general population, which may lead to a greater number of cancer diagnoses. The low number of enrolled studies regarding certain autoimmune disorders, which could not be meta-analyzed, is also a further limitation. The risk of bias assessment deemed in case of multiple domains as not low overall risk of bias too.
Subgroup analyses regarding the type of gastric cancer could not be performed, because there were no details available on histological type, or location of cancer. However, Ji et al. described that a few autoimmune diseases is an important risk factor for gastric cancer, mainly for corpus cancer (22). Sensitivity analysis was carried out to define the strength of confounding factors, such as H. pylori infection, which results suggest the examined association is unlikely to be solely because of confounding.
Most of the included studies originate from either North Europe (where incidence of autoimmunity could be higher compared with other populations) or Asia (where H. pylori infection and/or gastric cancer could be more prevalent). To address this problem, we performed subgroup analyses based on low- or high-incidence countries of gastric cancer. The results of the subgroup analysis reassert our main results, namely pernicious anemia, diabetes mellitus type I, Graves’ disease, and autoimmune vasculitis were associated with gastric cancer in low-incidence countries.
Conclusion
Our meta-analysis of 39 articles concludes that pernicious anemia, Graves’ disease, dermatomyositis, diabetes mellitus type I, inflammatory myopathies, and systemic lupus erythematosus are associated with higher incidence rates of gastric cancer. For clinical practice, close gastroenterological follow-up or routinely performed gastroscopy and application of other diagnostic measures may be cost-effective and clinically helpful for patients diagnosed with these six autoimmune diseases. Based on the importance of the problem, conducting further clinical trials on this topic is essential.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author Contributions
NZ: conceptualization, project administration, formal analysis, and writing—original draft. EO: conceptualization, methodology, and statistical analysis. PH: conceptualization and writing—review and editing. SV: conceptualization, data curation, and writing—review and editing. NV: conceptualization, data curation, and writing—review and editing. SK: conceptualization, methodology, and writing—review and editing. LF: conceptualization, visualization, and writing—review and editing. LS: conceptualization, methodology, visualization, and writing—original draft. JC: conceptualization, supervision, and writing—original draft. All authors have participated sufficiently to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2021.750533/full#supplementary-material
References
1. Siegel R, Ma J, Zou Z, Jemal A. Cancer Statistics, 2014. CA: Cancer J Clin (2014) 64:9–29. doi: 10.3322/caac.21208
2. Correa P. Gastric Cancer: Overview. Gastroenterol Clin North Am (2013) 42:211–7. doi: 10.1016/j.gtc.2013.01.002
3. Miyahara R, Niwa Y, Matsuura T, Maeda O, Ando T, Ohmiya N, et al. Prevalence and Prognosis of Gastric Cancer Detected by Screening in a Large Japanese Population: Data From a Single Institute Over 30 Years. J Gastroenterol Hepatol (2007) 22:1435–42. doi: 10.1111/j.1440-1746.2007.04991.x
4. Brenner H, Rothenbacher D, Arndt V. Epidemiology of Stomach Cancer. Methods Mol Biol (Clifton N.J.) (2009) 472:467–77. doi: 10.1007/978-1-60327-492-0_23
5. Blaser MJ, Chen Y. A New Gastric Cancer Among Us. J Natl Cancer Institute (2018) 110:549–50. doi: 10.1093/jnci/djx279
6. Anderson WF, Camargo MC, Fraumeni JF Jr, Correa P, Rosenberg PS, Rabkin CS. Age-Specific Trends in Incidence of Noncardia Gastric Cancer in US Adults. Jama (2010) 303:1723–8. doi: 10.1001/jama.2010.496
7. Anderson WF, Rabkin CS, Turner N, Fraumeni JF Jr, Rosenberg PS, Camargo MC. The Changing Face of Noncardia Gastric Cancer Incidence Among US non-Hispanic Whites. J Natl Cancer Institute (2018) 110:608–15. doi: 10.1093/jnci/djx262
8. Kehm RD, Yang W, Tehranifar P, Terry MB. 40 Years of Change in Age- and Stage-Specific Cancer Incidence Rates in US Women and Men. JNCI Cancer Spectr (2019) 3:pkz038. doi: 10.1093/jncics/pkz038
9. Ferlay J. GLOBOCAN 2008 V1. 2, Cancer Incidence and Mortality World-Wide. Lyon, France: International Agency for Research on Cancer. (2010).
10. Rawla P, Barsouk A. Epidemiology of Gastric Cancer: Global Trends, Risk Factors and Prevention. Przeglad Gastroenterologiczny (2019) 14:26–38. doi: 10.5114/pg.2018.80001
11. Bach JF. The Effect of Infections on Susceptibility to Autoimmune and Allergic Diseases. New Engl J Med (2002) 347:911–20. doi: 10.1056/NEJMra020100
12. Agmon-Levin N, Lian Z, Shoenfeld Y. Explosion of Autoimmune Diseases and the Mosaic of Old and Novel Factors. Cell Mol Immunol (2011) 8:189–92. doi: 10.1038/cmi.2010.70
13. Selmi C. The Worldwide Gradient of Autoimmune Conditions. Autoimmun Rev (2010) 9:A247–50. doi: 10.1016/j.autrev.2010.02.004
14. Nguyen TL, Khurana SS, Bellone CJ, Capoccia BJ, Sagartz JE, Kesman RA Jr, et al. Autoimmune Gastritis Mediated by CD4+ T Cells Promotes the Development of Gastric Cancer. Cancer Res (2013) 73:2117–26. doi: 10.1158/0008-5472.CAN-12-3957
15. Miska J, Lui JB, Toomer KH, Devarajan P, Cai X, Houghton J, et al. Initiation of Inflammatory Tumorigenesis by CTLA4 Insufficiency Due to Type 2 Cytokines. J Exp Med (2018) 215:841–58. doi: 10.1084/jem.20171971
16. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ (2021) 372:n71. doi: 10.1136/bmj.n71
17. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring Inconsistency in Meta-Analyses. Bmj (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
18. Egger M, Smith GD, Schneider M, Minder C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
19. Hayden JA, van der Windt DA, Cartwright JL, Côté P, Bombardier C. Assessing Bias in Studies of Prognostic Factors. Ann Internal Med (2013) 158:280–6. doi: 10.7326/0003-4819-158-4-201302190-00009
20. Hemminki K, Liu X, Ji J, Sundquist J, Sundquist K. Autoimmune Disease and Subsequent Digestive Tract Cancer by Histology. Ann Oncol (2012) 23:927–33. doi: 10.1093/annonc/mdr333
21. Bjørneklett R, Vikse BE, Svarstad E, Aasarød K, Bostad L, Langmark F, et al. Long-Term Risk of Cancer in Membranous Nephropathy Patients. Am J Kidney Dis (2007) 50:396–403. doi: 10.1053/j.ajkd.2007.06.003
22. Ji J, Sundquist J, Sundquist K. Family History of Autoimmune Diseases and Risk of Gastric Cancer: A National Cohort Study. Eur J Cancer Prev (2018) 27:221–6. doi: 10.1097/CEJ.0000000000000420
23. Yu K-H, Kuo C-F, Huang LH, Huang W-K, See L-C. Cancer Risk in Patients With Inflammatory Systemic Autoimmune Rheumatic Diseases: A Nationwide Population-Based Dynamic Cohort Study in Taiwan. Medicine (2016) 95(18):e3540. doi: 10.1097/MD.0000000000003540
24. Park JK, Choi IA, Lee EY, Song YW, Lee EB. Incidence of Malignancy in Takayasu Arteritis in Korea. Rheumatol Int (2014) 34:517–21. doi: 10.1007/s00296-013-2887-9
25. Hirano K, Tada M, Sasahira N, Isayama H, Mizuno S, Takagi K, et al. Incidence of Malignancies in Patients With Igg4-Related Disease. Internal Med (2014) 53:171–6. doi: 10.2169/internalmedicine.53.1342
26. Asano J, Watanabe T, Oguchi T, Kanai K, Maruyama M, Ito T, et al. Association Between Immunoglobulin G4–Related Disease and Malignancy Within 12 Years After Diagnosis: An Analysis After Longterm Followup. J Rheumatol (2015) 42:2135–42. doi: 10.3899/jrheum.150436
27. van Daalen EE, Rahmattulla C, Wolterbeek R, Bruijn JA, Bajema IM. Incidence of Malignancy Prior to Antineutrophil Cytoplasmic Antibody–Associated Vasculitis Compared to the General Population. J Rheumatol (2017) 44:314–8. doi: 10.3899/jrheum.160885
28. Yoo J, Ahn SS, Jung SM, Song JJ, Park Y-B, Lee S-W. Cancer Development in Korean Patients With ANCA-Associated Vasculitis: A Single Centre Study. Clin Exp Rheumatol (2018) 36:73–7.
29. Simon TA, Thompson A, Gandhi KK, Hochberg MC, Suissa S. Incidence of Malignancy in Adult Patients With Rheumatoid Arthritis: A Meta-Analysis. Arthritis Res Ther (2015) 17:212. doi: 10.1186/s13075-015-0728-9
30. Hill CL, Nguyen AM, Roder D, Roberts-Thomson P. Risk of Cancer in Patients With Scleroderma: A Population Based Cohort Study. Ann Rheumatic Dis (2003) 62:728–31. doi: 10.1136/ard.62.8.728
31. Bae EH, Lim SY, Han KD, Jung JH, Choi HS, Kim CS, et al. Systemic Lupus Erythematosus is a Risk Factor for Cancer: A Nationwide Population-Based Study in Korea. Lupus (2019) 28:317–23. doi: 10.1177/0961203319826672
32. Cobo-Ibáñez T, Urruticoechea-Arana A, Rúa-Figueroa I, Martín-Martínez MA, Ovalles-Bonilla JG, Galindo M, et al. Hormonal Dependence and Cancer in Systemic Lupus Erythematosus. Arthritis Care Res (2020) 72:216–24. doi: 10.1002/acr.24068
33. Carstensen B, Read SH, Friis S, Sund R, Keskimäki I, Svensson AM, et al. Cancer Incidence in Persons With Type 1 Diabetes: A Five-Country Study of 9,000 Cancers in Type 1 Diabetic Individuals. Diabetologia (2016) 59:980–8. doi: 10.1007/s00125-016-3884-9
34. Lau L, Huang L, Fu E, Tan TC, Kong KO, Lim MY. Nasopharyngeal Carcinoma in Dermatomyositis. Clin Otolaryngology: Off J ENT-UK; Off J Netherlands Soc Oto-Rhino-Laryngol Cervico-Facial Surg (2021) 46(5):1082–8. doi: 10.1111/coa.13764
35. Solans-Laque R, Perez-Bocanegra C, Salud-Salvia A, Fonollosa-Plá V, Rodrigo M, Armadans L, et al. Clinical Significance of Antinuclear Antibodies in Malignant Diseases: Association With Rheumatic and Connective Tissue Paraneoplastic Syndromes. Lupus (2004) 13:159–64. doi: 10.1191/0961203304lu521oa
36. Moinzadeh P, Fonseca C, Hellmich M, Shah AA, Chighizola C, Denton CP, et al. Association of Anti-RNA Polymerase III Autoantibodies and Cancer in Scleroderma. Arthritis Res Ther (2014) 16:1–10. doi: 10.1186/ar4486
37. Mellemkjér L, Andersen V, Linet MS, Gridley G, Hoover R, Olsen JH. Non-Hodgkin’s Lymphoma and Other Cancers Among a Cohort of Patients With Systemic Lupus Erythematosus. Arthritis Rheumatism: Off J Am Coll Rheumatol (1997) 40:761–8. doi: 10.1002/art.1780400424
38. Konstadoulakis MM, Syrigos KN, Albanopoulos C, Mayers G, Golematis B. The Presence of Anti-Carcinoembryonic Antigen (CEA) Antibodies in the Sera of Patients With Gastrointestinal Malignancies. J Clin Immunol (1994) 14:310–3. doi: 10.1007/BF01540984
39. Atalay C, Atalay G, Yilmaz K, Altinok M. The Role of Anti-CENP-B and Anti-SS-B Antibodies in Breast Cancer. Neoplasma (2005) 52:32–5.
40. Song M, Latorre G, Ivanovic-Zuvic D, Camargo MC, Rabkin CS. Autoimmune Diseases and Gastric Cancer Risk: A Systematic Review and Meta-Analysis. Cancer Res Treat (2019) 51:841–50. doi: 10.4143/crt.2019.151
41. Hsing AW, Hansson LE, McLaughlin JK, Nyren O, Blot WJ, Ekbom A, et al. Pernicious Anemia and Subsequent Cancer. A Population-Based Cohort Study. Cancer (1993) 71:745–50. doi: 10.1002/1097-0142(19930201)71:3<745::AID-CNCR2820710316>3.0.CO;2-1
42. Li CM, Chen Z. Autoimmunity as an Etiological Factor of Cancer: The Transformative Potential of Chronic Type 2 Inflammation. Front Cell Dev Biol (2021) 9:664305–5. doi: 10.3389/fcell.2021.664305
43. Becher H, Winkler V. Estimating the Standardized Incidence Ratio (SIR) With Incomplete Follow-Up Data. BMC Med Res Method (2017) 17:55. doi: 10.1186/s12874-017-0335-3
Keywords: : autoimmune disease, gastric cancer, autoimmunity, risk, standardized incidence rate
Citation: Zádori N, Szakó L, Váncsa S, Vörhendi N, Oštarijaš E, Kiss S, Frim L, Hegyi P and Czimmer J (2021) Six Autoimmune Disorders Are Associated With Increased Incidence of Gastric Cancer: A Systematic Review and Meta-Analysis of Half a Million Patients. Front. Immunol. 12:750533. doi: 10.3389/fimmu.2021.750533
Received: 30 July 2021; Accepted: 01 November 2021;
Published: 23 November 2021.
Edited by:
José Carlos Crispín, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán (INCMNSZ), MexicoReviewed by:
Jose Maria Remes-Troche, Universidad Veracruzana, MexicoChan-Na Zhao, Anhui Provincial TB Institute, China
Isaac Núñez, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán (INCMNSZ), Mexico
Copyright © 2021 Zádori, Szakó, Váncsa, Vörhendi, Oštarijaš, Kiss, Frim, Hegyi and Czimmer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: József Czimmer, Y3ppbW1lci5qb3pzZWZAcHRlLmh1