 Amit Bansal
Amit Bansal Mai-Chi Trieu
Mai-Chi Trieu Kristin G. I. Mohn1,2
Kristin G. I. Mohn1,2 Rebecca Jane Cox
Rebecca Jane Cox
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol. , 06 October 2021
Sec. Vaccines and Molecular Therapeutics
Volume 12 - 2021 | https://doi.org/10.3389/fimmu.2021.744774
Annual influenza vaccination is often recommended for pregnant women and young children to reduce the risk of severe influenza. However, most studies investigating the safety, immunogenicity, and efficacy or effectiveness of influenza vaccines are conducted in healthy adults. In this evidence-based clinical review, we provide an update on the safety profile, immunogenicity, and efficacy/effectiveness of inactivated influenza vaccines (IIVs) in healthy pregnant women and children <5 years old. Six electronic databases were searched until May 27, 2021. We identified 3,731 articles, of which 93 met the eligibility criteria and were included. The IIVs were generally well tolerated in pregnant women and young children, with low frequencies of adverse events following IIV administration; however, continuous vaccine safety monitoring systems are necessary to detect rare adverse events. IIVs generated good antibody responses, and the seroprotection rates after IIVs were moderate to high in pregnant women (range = 65%–96%) and young children (range = 50%–100%), varying between the different influenza types/subtypes and seasons. Studies show vaccine efficacy/effectiveness values of 50%–70% in pregnant women and 20%–90% in young children against lab-confirmed influenza, although the efficacy/effectiveness depended on the study design, host factors, vaccine type, manufacturing practices, and the antigenic match/mismatch between the influenza vaccine strains and the circulating strains. Current evidence suggests that the benefits of IIVs far outweigh the potential risks and that IIVs should be recommended for pregnant women and young children.
Inactivated influenza (flu) vaccine is recommended by the WHO for all pregnant women and children aged 6 months to 5 years. Flu is more likely to cause severe illness in pregnant women, and young children are the main transmitters of the virus. Vaccination against influenza lowers the risk of severe complications from flu during pregnancy, infancy, and early childhood. The benefits of influenza vaccination to the mother and child outweigh the potential risks.
Influenza occurs in epidemics of variable impacts every year. Among the four types of viruses—A, B, C, and D—only influenza A and B viruses cause seasonal epidemics. Influenza A virus subtypes are divided by the two major viral membrane glycoproteins, namely, hemagglutinin (HA) and neuraminidase (NA), and influenza B viruses have two lineages (Victoria and Yamagata). Minor changes by point mutations in the RNA gene segments that code for the HA or NA of influenza A and B viruses (antigenic drift) may result in seasonal influenza epidemics of variable intensities and severities (1). Major changes in human influenza A viruses associated with the acquisition of novel HA with or without novel NA proteins occur through genetic reassortment with animal influenza viruses or, potentially, direct zoonotic transmission and are referred to as antigenic shift. Such events led to the emergence of novel viruses, which caused pandemics in 1918 (H1N1), 1957 (H2N2), 1968 (H3N2), and 2009 (H1N1pdm09) (1–3). Zoonotic influenza viruses infect humans through direct transmission, such as avian flu, but only are considered pandemic if they can spread from human to human. The continuous evolution of influenza viruses influences the severity of influenza seasons and poses a continuous threat to human health.
The influenza virus infects all age groups. However, pregnant women and young children are especially at high risk of influenza complications, resulting in serious illness, increased hospitalizations, and mortality (4, 5). The laboratory-confirmed influenza (LCI) hospitalization and mortality rates were 0.4–77 cases (6–9) and 0.3–6.9 cases (6, 8–10) per 100,000 pregnancies, respectively, during the 2009 pandemic. The annual global influenza attack rates are estimated to be higher in children (20%–30%) than that in adults (5%–10%) (11). Influenza accounts for 7%–13% of acute lower respiratory infections in children <5 years globally (5, 12). Unlike in temperate zones where a clear influenza activity peak occurs in the winter, influenza activity can occur year-round in tropical or subtropical countries, with a peak in the monsoon season. In Bangladesh, the influenza incidence among children <5 years old ranged from 6.3 episodes/1,000 child-years in January to 258.3 episodes/1,000 child-years in May during the 2004–2007 seasons (13), whereas in Finland (14), the influenza attack rates were 175 to 179 per 1,000 young children in the 2000–2002 seasons. The risk of influenza-related serious illness or hospitalizations (15–18) and all-cause mortality (19) is higher in young than that in older children, especially in children under 6 months of age (20, 21). The most common complications of pediatric influenza are pharyngitis (range = 31%–58% of LCI), acute otitis media (range = 0%–41%), and febrile seizures or convulsions (range = 0%–45%) (22). The majority of influenza-related deaths in young children occur in developing countries (5, 12). Furthermore, young children play an important role in the community spread of influenza (22).
The role of natural influenza infection in the protection against subsequent infection is not well studied, especially in pregnant women and young children, although most people will have been infected with influenza during early childhood. Influenza infection induces a multifaceted and long-lived immunity, whereas vaccination induces a more specific and short-lived immunity [review in (23)]. However, influenza viruses can escape the infection-established immunity and subsequent natural reinfection occurs (24). A human challenge study suggested that sequential infection with identical influenza A viruses can also occur (25). Therefore, influenza vaccination remains the best preventive method against influenza infection and its related complications (15, 16). Two types of influenza vaccines are available: inactivated influenza vaccines (IIVs) and live attenuated influenza vaccines (LAIVs). LAIVs are used in children >2 years (in Europe and the USA), but are contraindicated in pregnant women, children <2 years old, and immunosuppressed individuals, while IIVs are used in individuals >6 months old and in pregnant women. Influenza vaccine purity has been greatly improved over the last 60 years; however, the whole-virus IIVs were found to be significantly reactive in young children (26). This resulted in the development of split-virus IIVs in which reactogenicity was reduced by detergent treatment of the virus, which, in some cases, is further purified into surface antigen subunits (26).
Twice a year, the World Health Organization (WHO) makes recommendations on the composition of the influenza vaccine, currently including three or four influenza strains (A/H1N1, A/H3N2, and one or two influenza B strains) that are predicted to circulate in the upcoming seasons (trivalent or quadrivalent IIVs, TIV or QIV). Several countries recommend QIV for pregnant women and young children due to the high burden of influenza B illness and the potential of mismatch between the circulating influenza B viruses and the vaccine strains in TIV (27, 28). Pregnant women require one annual IIV dose, while children 6 months to 8 years old require two doses as a prime–boost regime to ensure adequate seroprotection against influenza (29, 30). Thereafter, only one annual dose is required. Comparing vaccine immunogenicity and vaccine effectiveness (VE) estimates between the different vaccines is challenging due to several factors, such as the IIV type (whole-virus, virosome, split-virus, or subunit), with/without adjuvant, and the manufacturing processes (eggs, cell culture, or recombinant protein) (31). Other confounding factors (31) are the vaccinee’s age, preexisting immunity, comorbidities, and antigenic match/mismatch between the vaccine strains and circulating viruses.
IIVs have been used for over 60 years and given to hundreds of millions of people, providing good safety and immunogenicity records (32–39). However, limited evidence exists from randomized controlled trials (RCTs) on the efficacy of maternal influenza vaccine against serious illnesses (4). Furthermore, the majority of VE studies originate from high-income countries (4), with low- and middle-income countries underrepresented, especially for young children. Here, we provide an evidence-based clinical review on the safety, immunogenicity, and efficacy/effectiveness of IIVs in healthy pregnant women and children <5 years old with an emphasis on data from low- and middle-income countries.
The electronic databases PubMed, Google Scholar, MEDLINE, Embase, WHO International Clinical Trials Registry Platform (ICTRP), and UpToDate were searched using these keywords: “influenza,” “maternal influenza vaccination,” “humans,” “pregnant women,” “young children,” “safety,” “adverse event/effect,” “immunogenicity,” “vaccine effectiveness,” and “inactivated influenza vaccines.” Eligible studies met the following inclusion criteria: 1) published from inception to May 27, 2021, and 2) evaluated the safety profile, immunogenicity, or effectiveness of IIVs in healthy pregnant women or children <5 years old. Studies were excluded based on the title and abstract. Articles resulting from these searches and relevant references cited in those articles were reviewed. We accessed 3,731 studies. After screening, 93 studies were included in this review (Figure 1), of which 36 studies were on IIV safety, 10 and 16 on immunogenicity, and 17 and 33 were on the efficacy/effectiveness of IIVs in pregnant women and children, respectively. Most of the randomized controlled trials in pregnant women included in this review were conducted in low- and middle-income countries, while observation studies were conducted in high-income countries.
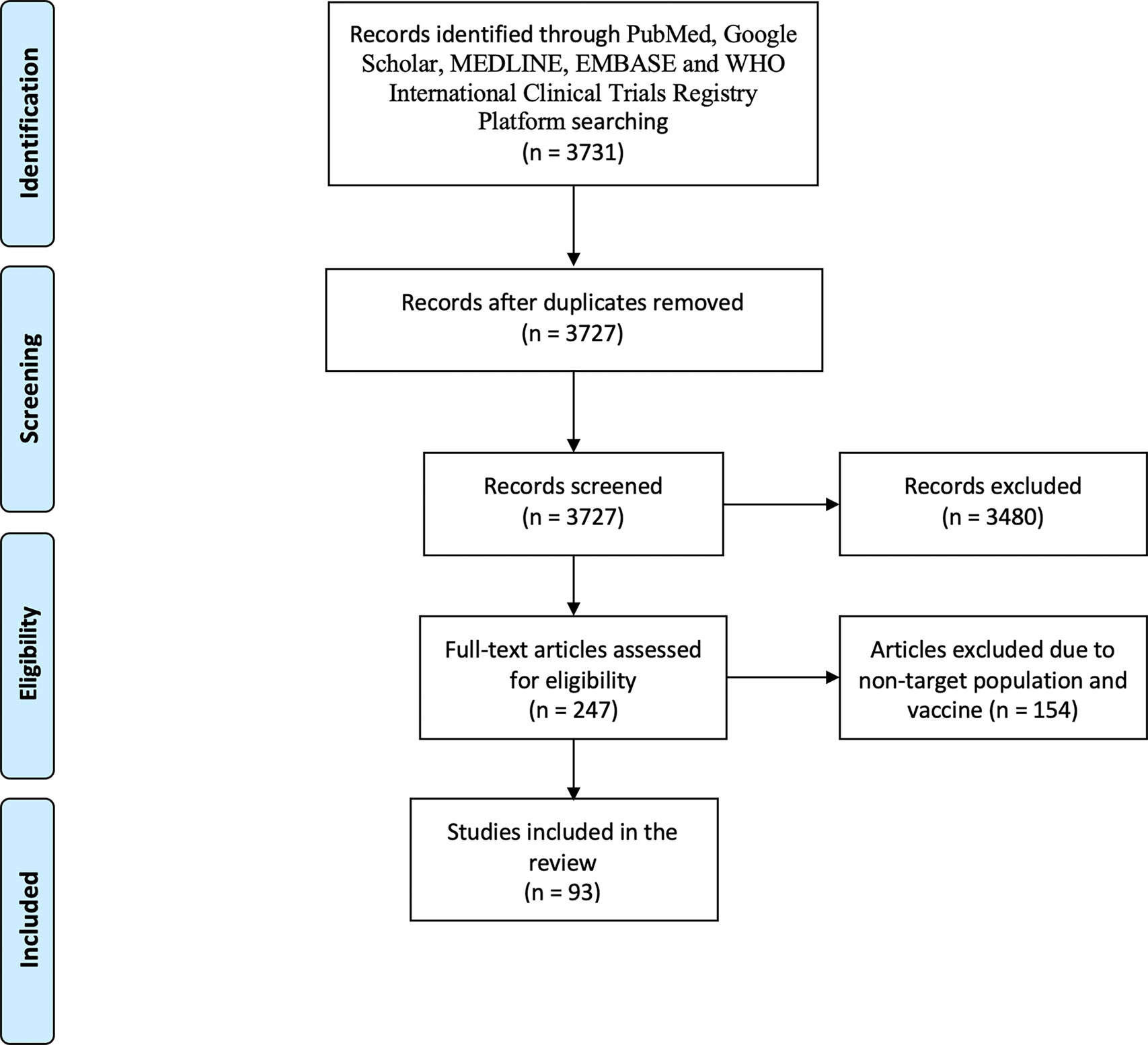
Figure 1 Flowchart of the included studies. We accessed 3,727 studies (titles and abstracts) following deletion of duplicates (n = 4). The literature search strategy included the following keywords: “influenza,” “maternal influenza vaccination,” “humans,” “pregnant women,” “young children,” “safety,” “adverse event/effect,” “immunogenicity,” “vaccine efficacy,” “vaccine effectiveness,” and “inactivated influenza vaccines” [and the Boolean operators (OR and AND)]. Eligible studies met the following inclusion criteria: 1) published from database inception to May 27, 2021, and 2) evaluated the safety profiles, immunogenicity, and effectiveness of inactivated influenza vaccines (IIVs) in healthy pregnant women and children <5 years old. Studies were excluded based on the title and abstract; non-peer-reviewed papers were not included. Large-scale studies were included only if the results were stratified for the target population. Studies in non-English language were also accessed. Most of the randomized controlled trials in pregnant women included in this review were conducted in low- and middle-income countries, while observation studies were conducted in high-income countries. Out of 93 suitable studies, the majority evaluated seasonal Northern Hemisphere IIVs, even when a study was conducted in the Southern Hemisphere, and 12 studies evaluated H1N1-pdm09 infection and/or vaccination. Of these 93 studies, 36 were on IIV safety, 10 on immunogenicity in pregnant women (two studies assessed both safety and immunogenicity), 16 on immunogenicity in young children (10 studies assessed both safety and immunogenicity), 17 studies for IIV effectiveness in pregnant women (three assessed both immunogenicity and effectiveness and one assessed both safety and effectiveness), and 33 studies for IIV effectiveness in young children (one on both safety and effectiveness and two on both immunogenicity and effectiveness).
Out of 93 studies, 36 were on the safety of IIVs in pregnant women and young children. Numerous studies have found that IIVs are safe for pregnant women (32, 33, 36, 39–49) and children <5 years old (34–37, 40–43, 45–47, 50, 51). In one study, no clinically significant difference was found in birth weight or gestational age at birth between infants of mothers who were vaccinated with IIV during any trimester of pregnancy and infants of unvaccinated mothers (32). There was no increased risk of either maternal complications or unwanted fetal outcomes after vaccination (33). In children, the most common adverse events after IIV were transient pain and irritability on the injection site, but no reaction persisted for more than 4 days (35). The majority of seasonal IIV studies report that adverse events requiring medical care are uncommon, and few children (up to 5.4%) experience febrile illness after IIV (36, 52–57), while some studies (34, 58–61) report transient fever in up to 18% of children. TIV has been temporally associated with hives (57), Henoch–Schönlein purpura (62), and pharyngitis (63) in children, but no causal evidence exists (64). Overall, the safety profiles are similar for the split-virion QIV and TIV in children 6–35 months old, except for more reactions on the injection site with QIV than with placebo or TIV (37).
There have been concerns over severe adverse events after IIV, such as narcolepsy and Guillain–Barré syndrome, but no indication of causality was found, although a weak correlation between IIV and narcolepsy, Guillain-Barré syndrome, or severe febrile illness was suggested in children (33–37, 65). A pre-registration pediatrics study (66) in the USA comparing two TIV formulations (TIV by CSL and Fluzone by Sanofi Pasteur Inc.) in 6- to 36-month-olds reported higher rates of fever (37.1% vs. 13.6%), severe fever (2.6% or 0%), irritability (58.5% or 37.3%), and loss of appetite (31.9% or 19.7%) after the first dose of the formulation approved for use in adults only, but the rates were lowered after the second dose. In 2010, there was a suspension of pediatric IIV use in Australia that lasted several years because Southern Hemisphere TIVs (manufactured by CSL Biotherapies, King of Prussia, PA, USA) were associated with severe febrile illness in children, but this was not found with the other IIVs (67). However, concomitant pneumococcal vaccination may further enhance the risk of febrile seizures in young children (68). Recent large-scale Australian cohort studies (69, 70) have found low rates of febrile illnesses in young children and pregnant women following QIV. Furthermore, IIV decreased the antepartum hospitalization risk of maternal influenza-like illness (ILI) by 39% (70). IIVs are not normally adjuvanted, but three main adjuvants have been used in pandemic IIVs (38): MF59, AS03, and AF03. Only MF59 is currently used in seasonal vaccines. The MF59-adjuvanted influenza vaccine was well tolerated in young children and induced greater, longer-lasting, and broader immune responses compared to the non-adjuvanted split vaccine (58, 71); however, transient and mild solicited reactions were more frequent after MF59-adjuvanted IIVs. Notably, the AS03-adjuvanted 2009 pandemic IIVs are no longer licensed for use in children <20 years old in Europe due to the association of the AS03-adjuvanted A/H1N1pdm09 vaccine with onset of narcolepsy in children in Scandinavia (36, 72). The whole-virus IIVs are also not used in Europe and North America due to safety concerns of increased reactogenicity (23). The prenatal 2009 pandemic A/H1N1pdm09 vaccination (with/without AS03) was weakly associated with increased risk of asthma and decreased rates of gastrointestinal infections in young children, which were attributed to confounding factors (50). A Danish retrospective cohort study (n = 61,359) concluded that the antenatal monovalent AS03-adjuvanted split-virion A/H1N1pdm09 IIVs were safe without any augmented early childhood morbidity risk (40). The adverse events of special interest for the AS03-A/H1N1pdm09 IIVs are generally rare, and no unexpected events during pregnancy were reported, but young children had higher reporting rates of adverse events (73). The risk of Guillain–Barré syndrome after IIV, particularly influenza A/H1N1pdm09, is very low (74–76) and lower than that with influenza infection (77). Furthermore, no significant links were found between H1N1pdm IIV and infectious diseases (e.g., pulmonary infections and otitis media), cancers, sensory disorders, use of hospital services, pediatric chronic diseases, and mortality (50).
This review may help physicians, pregnant women, and parents make informed choices about influenza immunization. IIVs are safe and well tolerated (36, 38, 40, 50, 51, 65) for pregnant women and children <5 years, but continued monitoring of adverse events is necessary to detect infrequent events.
The criteria of the European Committee for Medicinal Products for Human Use (CHMP) have been widely used to evaluate vaccine immunogenicity using the hemagglutination inhibition (HI) assay. Serum HI titer ≥40 is associated with >50% reduction in influenza infection or disease and is considered as a surrogate correlate of protection (COP) (78). However, this protective titer was established in healthy adults and not confirmed in children, with some experts recommending HI titres >110 (79) and others >160 (80). In adult vaccinees, as a part of registration requirements, three criteria (81) should be met, namely, >40% seroconversions or significant increase in HI titers, >2.5-fold increase in geometric mean HI titers (GMTs), and >70% seroprotection (achieving HI titer ≥40), for pandemic IIV and at least one of these criteria for seasonal IIV. HI and microneutralization (MN) titers are significantly correlated with each other; however, no MN titer level has been defined as a COP. In children, MN is the most sensitive for protection against seasonal A/H3N2 (82). Since 2017, new CHMP guidelines have recommended the measurement of neutralizing antibodies in addition to the HI titer and encouraged the assessment of broader immune response anti-neuraminidase antibodies, antibody kinetics, and cell-mediated immunity (83).
IIV induces strong humoral responses in pregnant women (84–88). After IIV administration, a 6- to 10-fold increase in GMTs (85, 88) and >72% seroconversions (85) were observed in pregnant women. A US cohort study (87) found that seasonal IIV led to 65%–95% and 75%–98% seroprotection rates for influenza A/H3N2 and A/H1N1, respectively, in pregnant women, with no significant difference by trimester or postpartum. However, the seroconversion rates were highest in the late third trimester and the postpartum period and lower in women with obesity (87). Higher pre-vaccination antibody levels and prior influenza vaccination were both linked to reduced odds of seroconversion rates, suggesting the antibody ceiling effect. Albeit a small study (n = 56), the seroprotection rates after TIV were largely comparable between pregnant and non-pregnant women for A/H1N1 (89% vs. 85%), A/H3N2 (81% vs. 93%), and B (83%% vs. 100%) during the 2011–2012 influenza season in the USA (89). Among pregnant TIV recipients in South Africa, Madhi et al. (84, 85) found 93%, 78%, and 96% seroprotection rates against A/H1N1pdm09, A/H3N2, and B/Victoria, respectively, and a 54% corresponding total vaccine efficacy against confirmed influenza. TIV induced significant enhancements of both the MN and HI titers against the three vaccine strains, and the MN titers were two to threefold higher than the HI titers, except against B/Victoria (90). Pregnant women vaccinated with QIV had similar safety and enhancement of GMTs for the strains included in TIV, but the GMTs were significantly higher for the second B strain (49). A Norwegian cohort study found durable antibody response after the 2009 AS03-adjuvanted monovalent pandemic IIV in pregnant women since the estimated waning of antibodies was slower in vaccinated pregnant women than that in ILI cases (HI titer half-life of 260 vs. 192 days) (39).
Importantly, infants born to vaccinated pregnant women received the complementary benefit of vertically transferred immunity against influenza (84, 85), a potentially cost-effective strategy. An RCT (n = 322) in South Africa (86) found that the percentages of infants with influenza-specific antibodies born to TIV-recipient mothers were significantly higher than those in saline placebo-recipient mothers (HI titers ≥40 at birth 78% vs. 34% against A/H1N1pdm09, 57% vs. 17% against A/H3N2, and 81% vs. 42% against B/Victoria, respectively). Yet, the percentage (86) of infants with seroprotective titers decreased from birth to 6 months (91). Passive immunity through placental transfer of maternal immunoglobulin G (IgG) antibodies to the fetus and IgA antibodies through breastfeeding is important to protect newborns against influenza infection (92), although transplacental antibody transfer seems to be the key mechanism in protecting newborns against influenza rather than through breast milk (93). Transplacental antibody transfer (94), primarily IgG, typically starts from 17 weeks of gestation and peaks at 37–41 weeks, with enhanced neonatal Fc receptor expression. Antibody decay occurs during the first 2–3 months (93, 95) in newborns. IIV immunization later in the trimester led to significantly higher seroprotection rates 2–3 days after delivery (effect sizes increase between the first and the third trimester), but no significant difference in the cord blood seroprotection rates was found between women vaccinated in the second or the third trimester (95). However, antibodies may wane faster in women vaccinated later in pregnancy, with some studies estimating antibody half-life of 7 weeks (95). Notably, there were fewer studies with the first trimester IIV immunogenicity results, where vaccination is often not recommended due to worries about temporal association with spontaneous abortion. The seroprotection and seroconversion rates at delivery were mostly high in pregnant women regardless of the vaccination timing (96).
Current limited evidence suggests that the IIV elicits similar good antibody responses in pregnant and non-pregnant women, and the antibodies can passively be transferred to their newborns. Although the vaccination timing may influence the antibody levels in pregnant women and their newborns, cumulative transfer of antibodies suggests the need for early IIV immunization of pregnant women (93).
A Canadian dose–response RCT (34) in 6- to 23-month-old children (n = 252) of the 2008–2009 Northern Hemisphere TIV found >85% seroprotection rates for all three vaccine strains in children aged 12–23 months without significant difference by dose (full vs. half dose), while the full dose induced higher antibody responses against all three vaccine strains without increasing reactogenicity in unprimed children aged 6–11 months. These results differ from an RCT (97) conducted in the USA in children 6–35 months of age, where increasing the antigen content of the 2010–2012 Northern Hemisphere TIV did not significantly increase the antibody responses to any of the three vaccine strains, except for the primed group who had been previously infected/vaccinated with A/H1N1 (as well as a subgroup analysis with infants only). Another Canadian RCT (35) evaluated the immunogenicity of the 2008–2009 Northern Hemisphere TIV in 6- to 35-month-old children (n = 374), reporting that two of the three serological criteria (>40% seroconversion rate and >2.5-fold increase in GMTs) were met for all vaccine strains and for both doses (full vs. half dose) in all TIV groups. Furthermore, antibody responses were significantly higher in children aged 24–35 months than those in 6–23 months. Similarly, higher antibody responses to TIV were reported with increasing age and after the second dose in healthy influenza-naive children 6–23 months old in the USA, albeit TIV was immunogenic in children 6–11 months old (98). Several RCTs in 2002–2003 (USA) (54, 55) and 2006–2009 (Europe) (58–60) found seroprotection rates ranging from 70% to 100% in children <5 years old following the Northern Hemisphere TIV. IIV is licensed for children from 6 months of age, and there are few studies evaluating the immunogenicity of IIV in children less than 12 months old. One study in infants reported >90% seroprotection rate in TIV recipients for at least one virus and 49.6% for two strains compared to 16.4% and 0.9%, respectively, in placebo recipients (57). Pilot data suggested that 6- to 12-week-old infants have significantly lower (99) antibody responses to TIV than do 6-month-old babies, with post-vaccination seroprotection rates of 46% vs. 69% against A/New Caledonia (H1N1), 59% vs. 79% against A/Wyoming (H3N2), and 5% vs. 22% against B/Jiangsu. In general, studies reported good immunogenicity profiles in children <5 years old (34, 35, 54–60, 66, 98, 99).
A multicenter phase III RCT (100) evaluated the immunogenicity of a split-virion QIV (2013–2014 Northern Hemisphere) in children 3–8 years old in Poland, Finland, Mexico, and Taiwan (n = 1,242) and found that the post-vaccination GMTs were augmented by more than sixfold for all vaccine strains (6.86 for A/H1N1, 7.49 for A/H3N2, 17.1 for B/Victoria, and 25.3 for B/Yamagata), regardless of the comparatively high baseline HI titers. The immunogenicity profile of QIV was comparable to that of TIV, with superiority for the second B strain (100, 101). More recently, a phase III RCT (37) evaluated the safety and efficacy of a split-virion QIV in healthy, previously unvaccinated children aged 6–35 months (n = 5,806) in Latin America, Asia, Africa, and Europe during the Northern Hemisphere and Southern Hemisphere 2014 and 2015 influenza seasons. The study found that most children were seronegative at baseline for each of the four vaccine strains, except only 50% of children from Asia were seronegative during the 2014 Southern Hemisphere season. After two doses of QIV, the seroconversion rates were >87% at day 56 for all four vaccine strains, and only <2% of participants remained seronegative (37). Moreover, the neutralizing antibody responses after IIV have not been extensively analyzed in children. One study found neutralizing antibodies against all homologous and heterologous H1 and H3 strains tested in all age groups, including children 2–8 years old receiving the 2009–2010 seasonal IIVs (102). Children aged 2–8 years also had higher seroprotection and seroconversion rates to homologous and heterologous strains compared to adults.
In conclusion, IIV elicits good HI antibody responses in children <5 years old, although there are no established HI protective titers for children and many studies rely on the adult criteria for HI titers (≥40 and a fourfold rise) when documenting seroprotection rates. Work is needed to evaluate protective HI titers and neutralizing antibodies in young children in order to better determine vaccine immunogenicity in this age group.
Vaccine efficacy and vaccine effectiveness (VE) measure the proportionate reduction in cases among vaccinated people under ideal (i.e., a randomized controlled trial) or typical field conditions, respectively. VE is now often assessed using a test-negative design in which patients with an ILI are tested for influenza. To estimate VE, vaccine coverage is compared between those testing positive versus those testing negative. Due to limited VE data on IIVs in pregnant women and children, we have included studies with both vaccine efficacy and VE below.
In an RCT in South Africa, Madhi et al. (4, 85) demonstrated that TIV partly protected pregnant women and their newborns, with vaccine efficacy values of 50% and 49%, respectively, against LCI during a 6-month postpartum follow-up period. Nunes et al. (86) conducted a secondary analyses of the data (85) and found that the vaccine efficacy against LCI decreased with age: 86% (95%CI = 38%–98%) efficacy in babies ≤8 weeks old, 25% (95%CI = −68% to 68%) in 8–16 weeks old, and 30% (95%CI = −155% to 83%) in 16–24 weeks old. Furthermore, the efficacy in newborns ranged from 30% in the Nepalese to 63% in Bangladeshi RCTs (103), confirming that maternal IgG antibodies can cross the placenta and protect newborns against influenza infection. Transplacental (and breast-milk-mediated) antibody transfer is an important means of protecting infants <6 months who are at high risk of hospitalization due to influenza (104) and IIV is not approved.
Observational data (36, 105, 106) showed that IIVs were 44%–65% effective against influenza among pregnant women, but the confidence intervals are wide, suggesting imprecise estimates (Table 1). Limited data exist on VE against severe influenza (requiring hospitalization) among pregnant women. A retrospective cohort study (118) in the USA from the 2005–2006 to 2013–2014 seasons concluded that infants born to vaccinated mothers, including those with comorbidities, had 70% risk reductions of LCI and 81% in influenza hospitalizations in the first 6 months of life. Similar results were reported in England during the 2013–2014 seasons, where antenatal IIVs were 71% effective (95%CI = 24%–89%) in preventing influenza infection and 64% effective (95%CI = 6%–86%) in preventing influenza hospitalization (113). A matched case–control study (115) in the USA reported that seasonal IIV immunization in pregnant women was 91.5% effective in preventing newborn hospitalization due to influenza. However, the selection bias might have overstated the VE estimates.
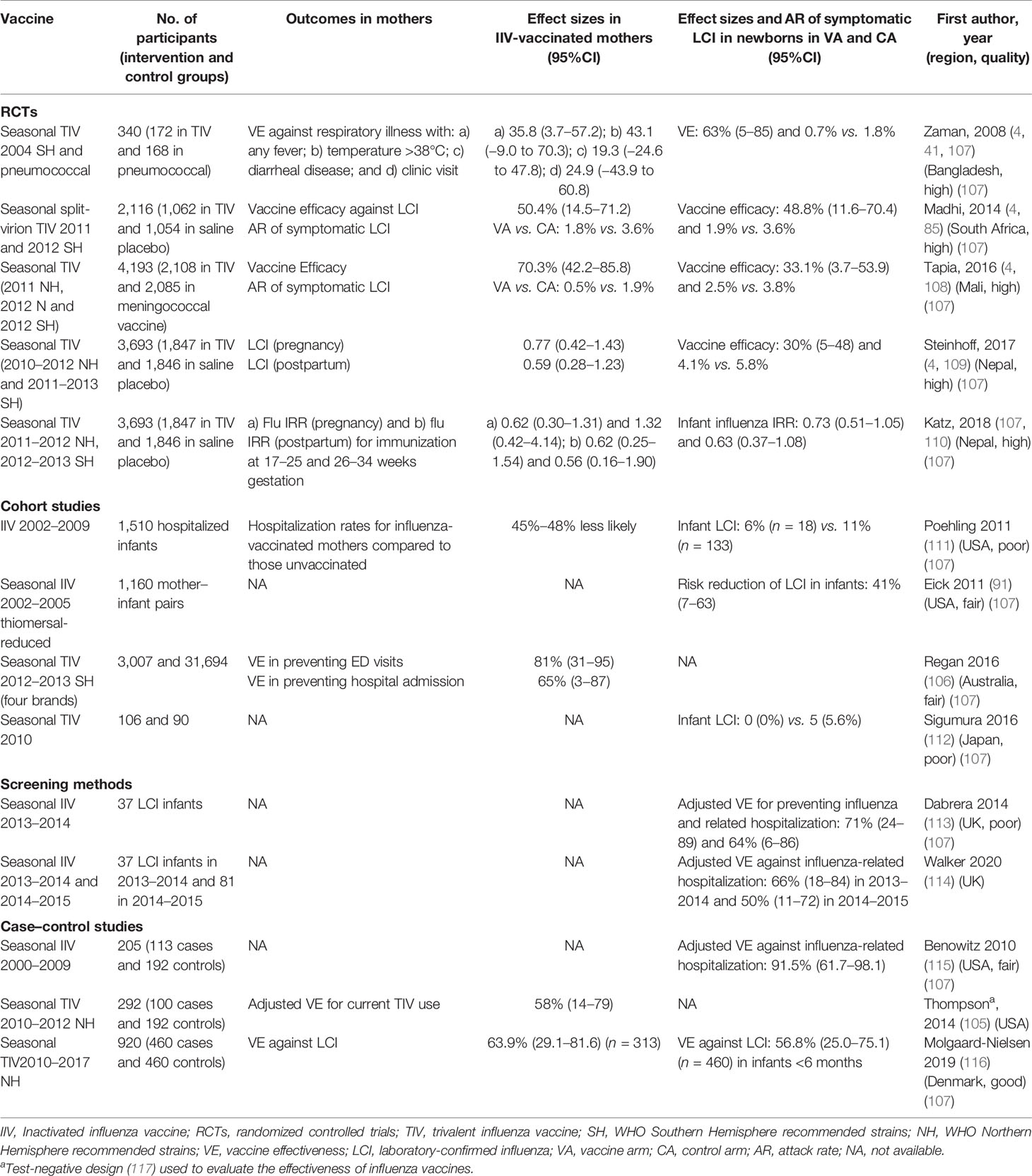
Table 1 Vaccine efficacy and effectiveness of influenza vaccination in healthy pregnant women.
In a Norwegian registry-based study (119), the pandemic monovalent H1N1pdm09 IIV with the AS03 adjuvant administered during pregnancy substantially reduced the risk of an influenza diagnosis (adjusted hazard ratio = 0.30), and it may have minimized the risk of influenza-related fetal demise during the pandemic. A Japanese questionnaire-based study (120) evaluating the 2009 H1N1 pandemic VE concluded that vaccination reduced infection by 89% in pregnant women.
In addition to the value of maternal–fetal transfer of influenza-specific antibodies (45, 84, 121) following antenatal IIV, there are also complementary benefits to vaccinated pregnant women. Women who received antenatal IIV had a lower risk of preterm delivery (13%) and low-birth-weight (26%) babies compared with unvaccinated pregnant women (70, 122). Furthermore, maternal influenza immunization has been linked to a decreased risk of having low-birth-weight babies in Bangladeshi and Nepalese RCTs (103).
Studies conducted in young children reported varying levels of vaccine efficacy/effectiveness primarily depending upon whether the circulating viruses match the vaccine strains and their preexisting immunity. Claeys et al. (123) conducted a multinational RCT of 12,018 healthy children aged 6–35 months and reported a 64% efficacy against moderate-to-severe influenza. In another large multinational RCT, Pepin et al. (37) reported QIV efficacy values of 51% (97%CI = 37%–62%) and 68% (97%CI = 47%–82%) against LCI caused by any influenza A or B strain and vaccine-similar strains, respectively. However, vaccine efficacy ranged from 41% to 60% during each of four influenza seasons, and the efficacy values for two QIV preparations were 46% (overall for the Southern Hemisphere 2014 and Northern Hemisphere 2014–2015 strains) and 58% (overall for the Southern 2015 and Northern 2015–2016 strains). A registry-based American study (124) in children aged 6–21 months carried out during the 2003–2004 season found that two doses of the vaccine were 69% and 87% effective against ILI and pneumonia/influenza office visits, respectively, but a single dose was not. Limited data on the efficacy estimates of IIVs exist in children <2 years. It is unclear whether the VE estimates are better for children <2 years old or those 2–5 years old (36) and impact indirect benefits for the communities by reducing transmission. Overall, data from test-negative design studies (29, 125–131) suggested moderate effectiveness of IIV against LCI in young children, but the confidence intervals are wide, suggesting imprecise estimates (Tables 2, 3). A Canadian test-negative design study (152) found that the adjusted VE rates against LCI hospitalization were 60% (95%CI = 44%–72%) for fully vaccinated 6- to 59-month-old children and 39% (95%CI = 17%–56%) for partially vaccinated children. Another test-negative design study (153) found that the VE against LCI hospitalization was 46% (95%CI = 19%–64%) among children 6 months to <5 years old. These two studies suggested that annual influenza vaccination is 40%–60% effective against LCI hospitalization in young children; however, the estimates included LAIVs and were not restricted to IIVs. More recent studies (146–151) have rather found high VE rates against LCI hospitalization (up to 81%) in young children (Table 2).
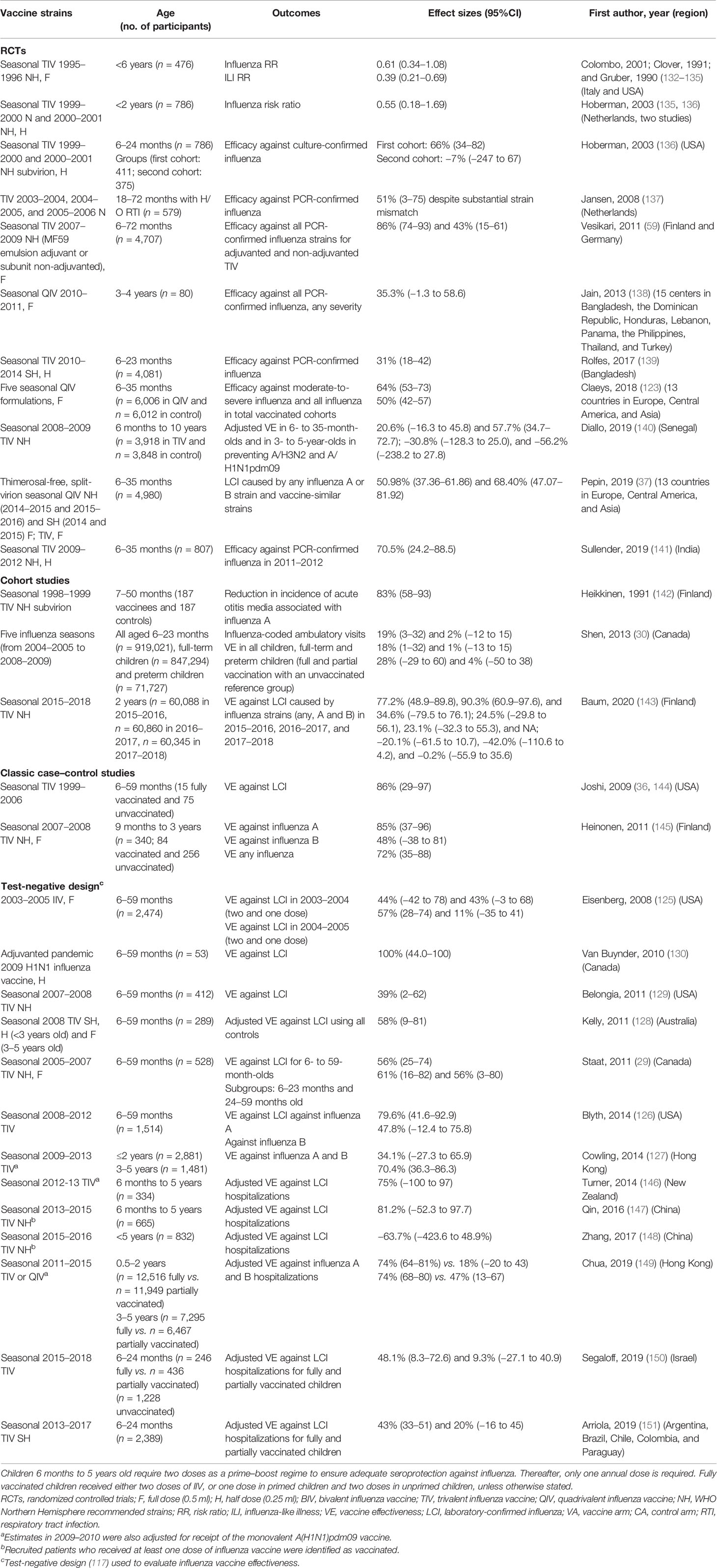
Table 2 Vaccine efficacy and effectiveness of influenza vaccination in healthy children under 5 years of age.
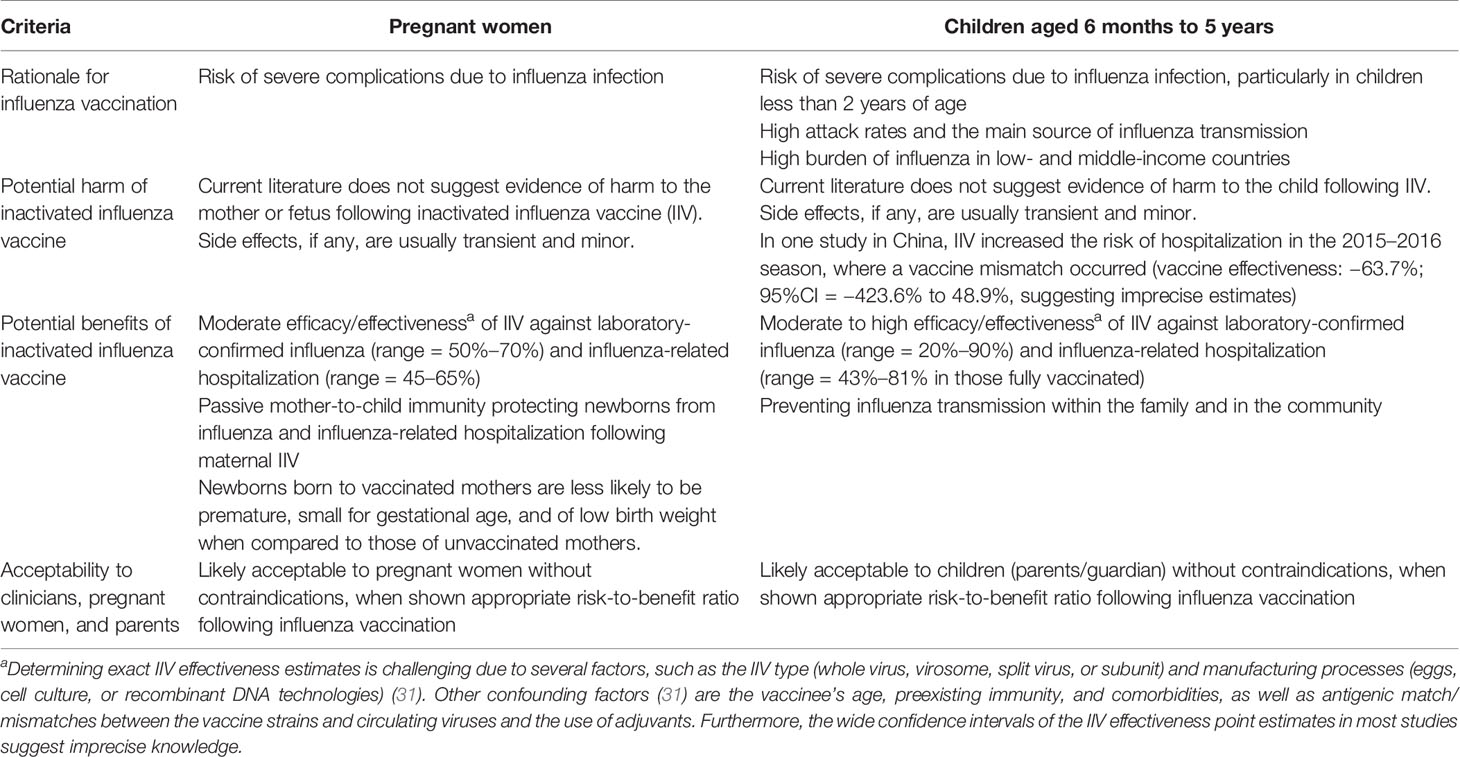
Table 3 Weighing of the potential benefits against risks of harm from the inactivated influenza vaccine in pregnant women and young children.
Diallo et al. (140) found that TIV-mediated VE estimates were lower in children <3 years old compared to those in 3–10 years old in Senegal (21% vs. 60% against the predominant seasonal A/H3N2 strain). However, the authors did not demonstrate noteworthy indirect effects among the entire study villages, which may be attributed to the study design, low vaccine coverage, and the high participant contact rates between extended families (140). Moreover, the indirect effect was assessed by comparing those vaccinated with control villages, and the study was undertaken in a year of vaccine mismatch. On the other hand, a Canadian study (154) in vaccinated children (from 36 months to 15 years old) showed an indirect VE of 60% (95%CI = 8%–83%) among the unvaccinated in 49 Hutterite communities, similar to a VE of 59% (95%CI = 5%–82%). IIV-mediated beneficial effects were also seen for other clinical outcomes in children (101, 155), such as reduced medical visits and antibiotic use. The influenza VE against nonspecific clinical outcomes such as acute otitis media is expected to be lower than its effectiveness against LCI because acute otitis media is primarily caused by viral or bacterial co-infection (156) in children. A 2017 Cochrane systematic review (157) found that the influenza vaccine resulted in a small reduction (risk ratio = 0.84) in at least one episode of acute otitis media over at least 6 months in 3,134 children aged 6–36 months. In summary, administration of IIV in young children prevents influenza complications in the vaccinees and may reduce the community transmission of influenza (141, 154).
Additionally, one recent study found that TIV was associated with lower coronavirus disease 2019 (COVID-19)-related severity and mortality in children <5 years old in Brazil (158). However, this retrospective observational study had selection bias and constrained data as it did not include potentially confounding factors such as other vaccines; thus, further investigations are required to confirm the findings.
A combined immunization strategy for pregnant women and young children who had IIVs may leverage both the direct protection of vaccinees and the indirect protection of non-vaccinees through vertically transmitted maternal antibodies and reduced person-to-person community transmission and mortality from influenza (4, 41, 159). However, conventional IIVs are grown in chicken eggs, with a long production time and impure contents. Previous literature suggested possible undesirable effects of egg-driven viral substitutions for optimal growth in eggs (31) and the induction of anti-egg antibodies in vaccinees (160, 161), which may have an impact on the vaccine efficacy, although no study has been done to evaluate this in pregnant women and young children. The long production times of IIVs could result in a vaccine antigen and circulating strain mismatch, affecting the VE estimates (162, 163), although studies have shown protection of IIVs in children despite vaccine strain mismatches (123). There is an urgent need for alternative methods for a more rapid production of vaccines. Cell-grown IIVs offer an alternative to egg-based vaccines. Cell-grown QIVs or TIVs have good immunogenicity profiles and may have a modest improvement over egg-based vaccines in children and adolescents (164, 165) while having similar safety profiles to those of egg-based IIVs in children (166, 167). One study found that the recombinant HA-based vaccine outperformed the virion-based IIV in both HA-specific cellular and serological responses in adults (168). However, to confirm these findings, larger RCTs are needed in pregnant women and younger children. In this review, the few relevant studies, along with major clinical, design, and statistical heterogeneities, precluded quantitative meta-analysis (4).
The ongoing COVID-19 pandemic has led to a paradigm shift in vaccinology, particularly with the use of new vaccine platforms that have not been previously licensed, especially messenger RNA (mRNA) vaccines. By 2019, 15 mRNA vaccine candidates, including three against influenza, were in clinical trials and none in phase III trials [review in (169)]. The COVID-19 pandemic has led to the most rapid vaccine development and approval of the mRNA COVID-19 vaccines to be used in humans. However, data on vaccine safety and efficacy in pregnant women are limited. Preliminary studies in pregnant and lactating women (170, 171) have suggested that the mRNA COVID-19 vaccines are safe, with immunogenicity and reactogenicity profiles similar to those observed in non-pregnant women. No data are yet available for young children since the mRNA COVID-19 vaccine clinical trials in children under 12 years of age are still ongoing. Nevertheless, the large safety database and good efficacy of the mRNA COVID-19 vaccines will accelerate the development of next-generation influenza vaccines, although it may well take over a decade before mRNA influenza vaccines will be licensed for pregnant women and young children. Therefore, the currently available IIVs should be continued to be recommended and used in pregnant women and young children until next-generation vaccines are available.
Overall, studies demonstrate that pregnant women and young children are protected against influenza illness and hospitalization by IIVs. Current evidence suggests that the benefits of IIVs outweigh the potential risks and that IIVs should be offered to pregnant women and young children. Moderate efficacy/effectiveness estimates after influenza vaccination, with acceptable tolerability profiles, are observed in pregnant women and young children, and the immunogenicity profile of pregnant women is comparable with healthy adults. Vaccine efficacy/effectiveness estimates are similar after both the second and the third trimester vaccination in pregnant women, while these estimates are lower in young children. Limited data on vaccine efficacy/effectiveness estimates exist for the first trimester and for younger children, although vertical transmission of antibodies may protect newborns who are at high risk of influenza-related complications. Robust trials should evaluate newer generations of influenza vaccines, especially cell-grown vaccines, in pregnant women and young children as even a modest vaccine efficacy/effectiveness enhancement could translate into major clinical benefits.
AB, M-CT, and RC contributed to the conception and design of the study. AB wrote the first draft and amended the manuscript. M-CT, KM, and RC reviewed the manuscript and suggested amendments. All authors contributed to the article and approved the submitted version.
This work was supported by a grant from the Research Council of Norway GLOBVAC program (284930) and the Ministry of Health and Care Services. AB and M-CT received research fellowships from the University of Bergen, Norway. This influenza center is funded by the Helse Vest (F-11628), the Trond Mohn Stiftelse (TMS2020TMT05), the European Union (EU IMI115672, FLUCOP, H2020 874866 INCENTIVE, and H2020 101037867 VACCELERATE), and Nanomedicines Flunanoair (ERA-NETet EuroNanoMed2 i JTC2016). The funders had no role in the preparation of the manuscript or in the decision to submit the manuscript for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Dolin R. Epidemiology of Influenza UpToDate. Waltham, MA: UpToDate (2020). Available at: https://www.uptodate.com/contents/epidemiology-of-influenza/print.
2. The Centers for Disease Control and Prevention. Past Pandemics (2021). Available at: https://www.cdc.gov/flu/pandemic-resources/basics/past-pandemics.html.
3. Krammer F, Smith GJD, Fouchier RAM, Peiris M, Kedzierska K, Doherty PC, et al. Influenza. Nat Rev Dis Primers (2018) 4(1):3. doi: 10.1038/s41572-018-0002-y
4. Fell DB, Azziz-Baumgartner E, Baker MG, Batra M, Beaute J, Beutels P, et al. Influenza Epidemiology and Immunization During Pregnancy: Final Report of a World Health Organization Working Group. Vaccine (2017) 35(43):5738–50. doi: 10.1016/j.vaccine.2017.08.037
5. Nair H, Brooks WA, Katz M, Roca A, Berkley JA, Madhi SA, et al. Global Burden of Respiratory Infections Due to Seasonal Influenza in Young Children: A Systematic Review and Meta-Analysis. Lancet (2011) 378(9807):1917–30. doi: 10.1016/S0140-6736(11)61051-9
6. Doyle TJ, Goodin K, Hamilton JJ. Maternal and Neonatal Outcomes Among Pregnant Women With 2009 Pandemic Influenza A(H1N1) Illness in Florida, 2009-2010: A Population-Based Cohort Study. PloS One (2013) 8(10):e79040. doi: 10.1371/journal.pone.0079040
7. Yates L, Pierce M, Stephens S, Mill AC, Spark P, Kurinczuk JJ, et al. Influenza A/H1N1v in Pregnancy: An Investigation of the Characteristics and Management of Affected Women and the Relationship to Pregnancy Outcomes for Mother and Infant. Health Technol Assess (2010) 14(34):109–82. doi: 10.3310/hta14340-02
8. Creanga AA, Johnson TF, Graitcer SB, Hartman LK, Al-Samarrai T, Schwarz AG, et al. Severity of 2009 Pandemic Influenza A (H1N1) Virus Infection in Pregnant Women. Obstet Gynecol (2010) 115(4):717–26. doi: 10.1097/AOG.0b013e3181d57947
9. Jamieson DJ, Honein MA, Rasmussen SA, Williams JL, Swerdlow DL, Biggerstaff MS, et al. H1N1 2009 Influenza Virus Infection During Pregnancy in the USA. Lancet (2009) 374(9688):451–8. doi: 10.1016/S0140-6736(09)61304-0
10. Knight M, Pierce M, Seppelt I, Kurinczuk JJ, Spark P, Brocklehurst P, et al. Critical Illness With AH1N1v Influenza in Pregnancy: A Comparison of Two Population-Based Cohorts. BJOG (2011) 118(2):232–9. doi: 10.1111/j.1471-0528.2010.02736.x
11. World Health Organization. WHO. Influenza 2019. Available at: http://www.who.int/biologicals/vaccines/influenza/en/.
12. Wang X, Li Y, O’Brien KL, Madhi SA, Widdowson MA, Byass P, et al. Global Burden of Respiratory Infections Associated With Seasonal Influenza in Children Under 5 Years in 2018: A Systematic Review and Modelling Study. Lancet Glob Health (2020) 8(4):e497–510. doi: 10.1016/S2214-109X(19)30545-5
13. Brooks WA, Goswami D, Rahman M, Nahar K, Fry AM, Balish A, et al. Influenza is a Major Contributor to Childhood Pneumonia in a Tropical Developing Country. Pediatr Infect Dis J (2010) 29(3):216–21. doi: 10.1097/INF.0b013e3181bc23fd
14. Heikkinen T, Silvennoinen H, Peltola V, Ziegler T, Vainionpaa R, Vuorinen T, et al. Burden of Influenza in Children in the Community. J Infect Dis (2004) 190(8):1369–73. doi: 10.1086/424527
15. Xu X, Blanton L, Elal AIA, Alabi N, Barnes J, Biggerstaff M, et al. Update: Influenza Activity in the United States During the 2018-19 Season and Composition of the 2019-20 Influenza Vaccine. MMWR Morb Mortal Wkly Rep (2019) 68(24):544–51. doi: 10.15585/mmwr.mm6824a3
16. Centers for Disease C, Prevention. Influenza Activity–United States, 2012-13 Season and Composition of the 2013-14 Influenza Vaccine. MMWR Morb Mortal Wkly Rep (2013) 62(23):473–9.
17. Heikkinen T, Tsolia M, Finn A. Vaccination of Healthy Children Against Seasonal Influenza: A European Perspective. Pediatr Infect Dis J (2013) 32(8):881–8. doi: 10.1097/INF.0b013e3182918168
18. Silvennoinen H, Peltola V, Vainionpää R, Ruuskanen O, Heikkinen T. Incidence of Influenza-Related Hospitalizations in Different Age Groups of Children in Finland: A 16-Year Study. Pediatr Infect Dis J (2011) 30(2):e24–8. doi: 10.1097/INF.0b013e3181fe37c8
19. Nielsen J, Krause TG, Molbak K. Influenza-Associated Mortality Determined From All-Cause Mortality, Denmark 2010/11-2016/17: The FluMOMO Model. Influenza Other Respir Viruses (2018) 12(5):591–604. doi: 10.1111/irv.12564
20. Zhou H, Thompson WW, Viboud CG, Ringholz CM, Cheng PY, Steiner C, et al. Hospitalizations Associated With Influenza and Respiratory Syncytial Virus in the United States, 1993-2008. Clin Infect Dis (2012) 54(10):1427–36. doi: 10.1093/cid/cis211
21. Poehling KA, Edwards KM, Weinberg GA, Szilagyi P, Staat MA, Iwane MK, et al. The Underrecognized Burden of Influenza in Young Children. N Engl J Med (2006) 355(1):31–40. doi: 10.1056/NEJMoa054869
22. Antonova EN, Rycroft CE, Ambrose CS, Heikkinen T, Principi N. Burden of Paediatric Influenza in Western Europe: A Systematic Review. BMC Public Health (2012) 12:968. doi: 10.1186/1471-2458-12-968
23. Krammer F. The Human Antibody Response to Influenza A Virus Infection and Vaccination. Nat Rev Immunol (2019) 19(6):383–97. doi: 10.1038/s41577-019-0143-6
24. Frank AL, Taber LH. Variation in Frequency of Natural Reinfection With Influenza A Viruses. J Med Virol (1983) 12(1):17–23. doi: 10.1002/jmv.1890120103
25. Memoli MJ, Han A, Walters KA, Czajkowski L, Reed S, Athota R, et al. Influenza A Reinfection in Sequential Human Challenge: Implications for Protective Immunity and "Universal" Vaccine Development. Clin Infect Dis (2020) 70(5):748–53. doi: 10.1093/cid/ciz281
26. Gross PA, Ennis FA, Gaerlan PF, Denson LJ, Denning CR, Schiffman D. A Controlled Double-Blind Comparison of Reactogenicity, Immunogenicity, and Protective Efficacy of Whole-Virus and Split-Product Influenza Vaccines in Children. J Infect Dis (1977) 136(5):623–32. doi: 10.1093/infdis/136.5.623
27. Young K GI, Harrison R, on behalf of the National Advisory Committee on Immunization (NACI). Summary of the NACI Seasonal Influenza Vaccine Statement for 2020–2021, (2020) 46:132–7. doi: 10.14745/ccdr.v46i05a06
28. Mak TK, Mangtani P, Leese J, Watson JM, Pfeifer D. Influenza Vaccination in Pregnancy: Current Evidence and Selected National Policies. Lancet Infect Dis (2008) 8(1):44–52. doi: 10.1016/S1473-3099(07)70311-0
29. Staat MA, Griffin MR, Donauer S, Edwards KM, Szilagyi PG, Weinberg GA, et al. Vaccine Effectiveness for Laboratory-Confirmed Influenza in Children 6-59 Months of Age, 2005-2007. Vaccine (2011) 29(48):9005–11. doi: 10.1016/j.vaccine.2011.09.037
30. Shen S, Campitelli MA, Calzavara A, Guttmann A, Kwong JC. Seasonal Influenza Vaccine Effectiveness in Pre- and Full-Term Children Aged 6-23 Months Over Multiple Seasons. Vaccine (2013) 31(29):2974–8. doi: 10.1016/j.vaccine.2013.05.011
31. Paules CI, Sullivan SG, Subbarao K, Fauci AS. Chasing Seasonal Influenza - The Need for a Universal Influenza Vaccine. N Engl J Med (2018) 378(1):7–9. doi: 10.1056/NEJMp1714916
32. McHugh L, Andrews RM, Lambert SB, Viney KA, Wood N, Perrett KP, et al. Birth Outcomes for Australian Mother-Infant Pairs Who Received an Influenza Vaccine During Pregnancy, 2012-2014: The FluMum Study. Vaccine (2017) 35(10):1403–9. doi: 10.1016/j.vaccine.2017.01.075
33. Tamma PD, Ault KA, del Rio C, Steinhoff MC, Halsey NA, Omer SB. Safety of Influenza Vaccination During Pregnancy. Am J Obstet Gynecol (2009) 201(6):547–52. doi: 10.1016/j.ajog.2009.09.034
34. Skowronski DM, Hottes TS, Chong M, De Serres G, Scheifele DW, Ward BJ, et al. Randomized Controlled Trial of Dose Response to Influenza Vaccine in Children Aged 6 to 23 Months. Pediatrics (2011) 128(2):e276–89. doi: 10.1542/peds.2010-2777
35. Langley JM, Vanderkooi OG, Garfield HA, Hebert J, Chandrasekaran V, Jain VK, et al. Immunogenicity and Safety of 2 Dose Levels of a Thimerosal-Free Trivalent Seasonal Influenza Vaccine in Children Aged 6-35 Months: A Randomized, Controlled Trial. J Pediatr Infect Dis Soc (2012) 1(1):55–63. doi: 10.1093/jpids/pis012
36. Sullivan SG, Price OH, Regan AK. Burden, Effectiveness and Safety of Influenza Vaccines in Elderly, Paediatric and Pregnant Populations. Ther Adv Vaccines Immunother (2019) 7:2515135519826481. doi: 10.1177/2515135519826481
37. Pepin S, Dupuy M, Borja-Tabora CFC, Montellano M, Bravo L, Santos J, et al. Efficacy, Immunogenicity, and Safety of a Quadrivalent Inactivated Influenza Vaccine in Children Aged 6-35months: A Multi-Season Randomised Placebo-Controlled Trial in the Northern and Southern Hemispheres. Vaccine (2019) 37(13):1876–84. doi: 10.1016/j.vaccine.2018.11.074
38. Del Giudice G, Rappuoli R, Didierlaurent AM. Correlates of Adjuvanticity: A Review on Adjuvants in Licensed Vaccines. Semin Immunol (2018) 39:14–21. doi: 10.1016/j.smim.2018.05.001
39. Tunheim G, Laake I, Robertson AH, Waalen K, Hungnes O, Naess LM, et al. Antibody Levels in a Cohort of Pregnant Women After the 2009 Influenza A(H1N1) Pandemic: Waning and Association With Self-Reported Severity and Duration of Illness. Influenza Other Respir Viruses (2019) 13(2):191–200. doi: 10.1111/irv.12623
40. Hviid A, Svanstrom H, Molgaard-Nielsen D, Lambach P. Association Between Pandemic Influenza A(H1N1) Vaccination in Pregnancy and Early Childhood Morbidity in Offspring. JAMA Pediatr (2017) 171(3):239–48. doi: 10.1001/jamapediatrics.2016.4023
41. Zaman K, Roy E, Arifeen SE, Rahman M, Raqib R, Wilson E, et al. Effectiveness of Maternal Influenza Immunization in Mothers and Infants. N Engl J Med (2008) 359(15):1555–64. doi: 10.1056/NEJMoa0708630
42. Munoz FM, Greisinger AJ, Wehmanen OA, Mouzoon ME, Hoyle JC, Smith FA, et al. Safety of Influenza Vaccination During Pregnancy. Am J Obstet Gynecol (2005) 192(4):1098–106. doi: 10.1016/j.ajog.2004.12.019
43. Black SB, Shinefield HR, France EK, Fireman BH, Platt ST, Shay D, et al. Effectiveness of Influenza Vaccine During Pregnancy in Preventing Hospitalizations and Outpatient Visits for Respiratory Illness in Pregnant Women and Their Infants. Am J Perinatol (2004) 21(6):333–9. doi: 10.1055/s-2004-831888
44. Yeager DP, Toy EC, Baker B. Influenza Vaccination in Pregnancy. Am J Perinatol (1999) 16(6):283–6. doi: 10.1055/s-2007-993873
45. Englund JA, Mbawuike IN, Hammill H, Holleman MC, Baxter BD, Glezen WP. Maternal Immunization With Influenza or Tetanus Toxoid Vaccine for Passive Antibody Protection in Young Infants. J Infect Dis (1993) 168(3):647–56. doi: 10.1093/infdis/168.3.647
46. Deinard AS, Ogburn P. A/NJ/8/76 Influenza Vaccination Program: Effects on Maternal Health and Pregnancy Outcome. Am J Obstet Gynecol (1981) 140(3):240–5. doi: 10.1016/0002-9378(81)90267-2
47. Sumaya CV, Gibbs RS. Immunization of Pregnant Women With Influenza A/New Jersey/76 Virus Vaccine: Reactogenicity and Immunogenicity in Mother and Infant. J Infect Dis (1979) 140(2):141–6. doi: 10.1093/infdis/140.2.141
48. Donahue JG, Kieke BA, King JP, Mascola MA, Shimabukuro TT, DeStefano F, et al. Inactivated Influenza Vaccine and Spontaneous Abortion in the Vaccine Safety Datalink in 2012-13, 2013-14, and 2014-15. Vaccine (2019) 37(44):6673–81. doi: 10.1016/j.vaccine.2019.09.035
49. Vesikari T, Virta M, Heinonen S, Eymin C, Lavis N, Chabanon AL, et al. Immunogenicity and Safety of a Quadrivalent Inactivated Influenza Vaccine in Pregnant Women: A Randomized, Observer-Blind Trial. Hum Vaccin Immunother (2020) 16(3):623–9. doi: 10.1080/21645515.2019.1667202
50. Walsh LK, Donelle J, Dodds L, Hawken S, Wilson K, Benchimol EI, et al. Health Outcomes of Young Children Born to Mothers Who Received 2009 Pandemic H1N1 Influenza Vaccination During Pregnancy: Retrospective Cohort Study. BMJ (2019) 366:l4151. doi: 10.1136/bmj.l4151
51. Sukumaran L, McCarthy NL, Kharbanda EO, Vazquez-Benitez G, Lipkind HS, Jackson L, et al. Infant Hospitalizations and Mortality After Maternal Vaccination. Pediatrics (2018) 141(3):e20173310. doi: 10.1542/peds.2017-3310
52. Pillsbury A, Cashman P, Leeb A, Regan A, Westphal D, Snelling T, et al. Real-Time Safety Surveillance of Seasonal Influenza Vaccines in Children, Australia, 2015. Euro Surveill (2015) 20(43):30050. doi: 10.2807/1560-7917.ES.2015.20.43.30050
53. Lina B, Fletcher MA, Valette M, Saliou P, Aymard M. A TritonX-100-Split Virion Influenza Vaccine Is Safe and Fulfills the Committee for Proprietary Medicinal Products (CPMP) Recommendations for the European Community for Immunogenicity, in Children, Adults and the Elderly. Biologicals (2000) 28(2):95–103. doi: 10.1006/biol.2000.0245
54. Englund JA, Walter EB, Fairchok MP, Monto AS, Neuzil KM. A Comparison of 2 Influenza Vaccine Schedules in 6- to 23-Month-Old Children. Pediatrics (2005) 115(4):1039–47. doi: 10.1542/peds.2004-2373
55. King JC, Cox MM, Reisinger K, Hedrick J, Graham I, Patriarca P. Evaluation of the Safety, Reactogenicity and Immunogenicity of FluBlok Trivalent Recombinant Baculovirus-Expressed Hemagglutinin Influenza Vaccine Administered Intramuscularly to Healthy Children Aged 6-59 Months. Vaccine (2009) 27(47):6589–94. doi: 10.1016/j.vaccine.2009.08.032
56. Walter EB, Neuzil KM, Zhu Y, Fairchok MP, Gagliano ME, Monto AS, et al. Influenza Vaccine Immunogenicity in 6- to 23-Month-Old Children: Are Identical Antigens Necessary for Priming? Pediatrics (2006) 118(3):e570–8. doi: 10.1542/peds.2006-0198
57. Englund JA, Walter E, Black S, Blatter M, Nyberg J, Ruben FL, et al. Safety and Immunogenicity of Trivalent Inactivated Influenza Vaccine in Infants: A Randomized Double-Blind Placebo-Controlled Study. Pediatr Infect Dis J (2010) 29(2):105–10. doi: 10.1097/INF.0b013e3181b84c34
58. Vesikari T, Pellegrini M, Karvonen A, Groth N, Borkowski A, O’Hagan DT, et al. Enhanced Immunogenicity of Seasonal Influenza Vaccines in Young Children Using MF59 Adjuvant. Pediatr Infect Dis J (2009) 28(7):563–71. doi: 10.1097/INF.0b013e31819d6394
59. Vesikari T, Knuf M, Wutzler P, Karvonen A, Kieninger-Baum D, Schmitt HJ, et al. Oil-in-Water Emulsion Adjuvant With Influenza Vaccine in Young Children. N Engl J Med (2011) 365(15):1406–16. doi: 10.1056/NEJMoa1010331
60. Esposito S, Marchisio P, Ansaldi F, Bianchini S, Pacei M, Baggi E, et al. A Randomized Clinical Trial Assessing Immunogenicity and Safety of a Double Dose of Virosomal-Adjuvanted Influenza Vaccine Administered to Unprimed Children Aged 6-35 Months. Vaccine (2010) 28(38):6137–44. doi: 10.1016/j.vaccine.2010.07.041
61. Li-Kim-Moy J, Yin JK, Rashid H, Khandaker G, King C, Wood N, et al. Systematic Review of Fever, Febrile Convulsions and Serious Adverse Events Following Administration of Inactivated Trivalent Influenza Vaccines in Children. Euro Surveill (2015) 20(24).
62. Watanabe T. Henoch-Schönlein Purpura Following Influenza Vaccinations During the Pandemic of Influenza A (H1n1). Pediatr Nephrol (2011) 26(5):795–8. doi: 10.1007/s00467-010-1722-8
63. Goodman MJ, Nordin JD, Harper P, Defor T, Zhou X. The Safety of Trivalent Influenza Vaccine Among Healthy Children 6 to 24 Months of Age. Pediatrics (2006) 117(5):e821–6. doi: 10.1542/peds.2005-2234
64. Halsey NA, Talaat KR, Greenbaum A, Mensah E, Dudley MZ, Proveaux T, et al. The Safety of Influenza Vaccines in Children: An Institute for Vaccine Safety White Paper. Vaccine (2015) 33(Suppl 5):F1–F67. doi: 10.1016/j.vaccine.2015.10.080
65. Stassijns J, Bollaerts K, Baay M, Verstraeten T. A Systematic Review and Meta-Analysis on the Safety of Newly Adjuvanted Vaccines Among Children. Vaccine (2016) 34(6):714–22. doi: 10.1016/j.vaccine.2015.12.024
66. Brady RC, Hu W, Houchin VG, Eder FS, Jackson KC, Hartel GF, et al. Randomized Trial to Compare the Safety and Immunogenicity of CSL Limited’s 2009 Trivalent Inactivated Influenza Vaccine to an Established Vaccine in United States Children. Vaccine (2014) 32(52):7141–7. doi: 10.1016/j.vaccine.2014.10.024
67. Armstrong PK, Dowse GK, Effler PV, Carcione D, Blyth CC, Richmond PC, et al. Epidemiological Study of Severe Febrile Reactions in Young Children in Western Australia Caused by a 2010 Trivalent Inactivated Influenza Vaccine. BMJ Open (2011) 1(1):e000016. doi: 10.1136/bmjopen-2010-000016
68. Tse A, Tseng HF, Greene SK, Vellozzi C, Lee GM, Group VRCAIW. Signal Identification and Evaluation for Risk of Febrile Seizures in Children Following Trivalent Inactivated Influenza Vaccine in the Vaccine Safety Datalink Project, 2010-2011. Vaccine (2012) 30(11):2024–31. doi: 10.1016/j.vaccine.2012.01.027
69. Pillsbury AJ, Glover C, Jacoby P, Quinn HE, Fathima P, Cashman P, et al. Active Surveillance of 2017 Seasonal Influenza Vaccine Safety: An Observational Cohort Study of Individuals Aged 6 Months and Older in Australia. BMJ Open (2018) 8(10):e023263. doi: 10.1136/bmjopen-2018-023263
70. Mohammed H, Roberts CT, Grzeskowiak LE, Giles LC, Dekker GA, Marshall HS. Safety and Protective Effects of Maternal Influenza Vaccination on Pregnancy and Birth Outcomes: A Prospective Cohort Study. EClinicalMedicine (2020) 26:100522. doi: 10.1016/j.eclinm.2020.100522
71. Vesikari T, Groth N, Karvonen A, Borkowski A, Pellegrini M. MF59-Adjuvanted Influenza Vaccine (FLUAD) in Children: Safety and Immunogenicity Following a Second Year Seasonal Vaccination. Vaccine (2009) 27(45):6291–5. doi: 10.1016/j.vaccine.2009.02.004
72. Wijnans L, Lecomte C, de Vries C, Weibel D, Sammon C, Hviid A, et al. The Incidence of Narcolepsy in Europe: Before, During, and After the Influenza A(H1N1)pdm09 Pandemic and Vaccination Campaigns. Vaccine (2013) 31(8):1246–54. doi: 10.1016/j.vaccine.2012.12.015
73. Folkenberg M, Callréus T, Svanström H, Valentiner-Branth P, Hviid A. Spontaneous Reporting of Adverse Events Following Immunisation Against Pandemic Influenza in Denmark November 2009-March 2010. Vaccine (2011) 29(6):1180–4. doi: 10.1016/j.vaccine.2010.12.008
74. Tokars JI, Lewis P, DeStefano F, Wise M, Viray M, Morgan O, et al. The Risk of Guillain-Barré Syndrome Associated With Influenza A (H1N1) 2009 Monovalent Vaccine and 2009-2010 Seasonal Influenza Vaccines: Results From Self-Controlled Analyses. Pharmacoepidemiol Drug Saf (2012) 21(5):546–52. doi: 10.1002/pds.3220
75. Wise ME, Viray M, Sejvar JJ, Lewis P, Baughman AL, Connor W, et al. Guillain-Barre Syndrome During the 2009-2010 H1N1 Influenza Vaccination Campaign: Population-Based Surveillance Among 45 Million Americans. Am J Epidemiol (2012) 175(11):1110–9. doi: 10.1093/aje/kws196
76. Greene SK, Rett M, Weintraub ES, Li L, Yin R, Amato AA, et al. Risk of Confirmed Guillain-Barre Syndrome Following Receipt of Monovalent Inactivated Influenza A (H1N1) and Seasonal Influenza Vaccines in the Vaccine Safety Datalink Project, 2009-2010. Am J Epidemiol (2012) 175(11):1100–9. doi: 10.1093/aje/kws195
77. Petráš M, Králová Lesná I, Dáňová J, Čelko AM. Is an Increased Risk of Developing Guillain–Barré Syndrome Associated With Seasonal Influenza Vaccination? A Systematic Review and Meta-Analysis. Vaccines (2020) 8(2):150. doi: 10.3390/vaccines8020150
78. Cox RJ. Correlates of Protection to Influenza Virus, Where do We Go From Here? Hum Vaccin Immunother (2013) 9(2):405–8. doi: 10.4161/hv.22908
79. Black S, Nicolay U, Vesikari T, Knuf M, Del Giudice G, Della Cioppa G, et al. Hemagglutination Inhibition Antibody Titers as a Correlate of Protection for Inactivated Influenza Vaccines in Children. Pediatr Infect Dis J (2011) 30(12):1081–5. doi: 10.1097/INF.0b013e3182367662
80. Gianchecchi E, Torelli A, Montomoli E. The Use of Cell-Mediated Immunity for the Evaluation of Influenza Vaccines: An Upcoming Necessity. Hum Vaccin Immunother (2019) 15(5):1021–30. doi: 10.1080/21645515.2019.1565269
81. The European Agency for the Evaluation of Medicinal Products. Committee for Proprietary Medicinal Products. Note for Guidance on Harmonization of Requirements for Influenza Vaccines (1997). Available at: http://www.emea.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500003945.pdf.
82. Wang B, Russell ML, Brewer A, Newton J, Singh P, Ward BJ, et al. Single Radial Haemolysis Compared to Haemagglutinin Inhibition and Microneutralization as a Correlate of Protection Against Influenza A H3N2 in Children and Adolescents. Influenza Other Respir Viruses (2017) 11(3):283–8. doi: 10.1111/irv.12450
83. Wijnans L, Voordouw B. A Review of the Changes to the Licensing of Influenza Vaccines in Europe. Influenza Other Respir Viruses (2016) 10(1):2–8. doi: 10.1111/irv.12351
84. Kay AW, Blish CA. Immunogenicity and Clinical Efficacy of Influenza Vaccination in Pregnancy. Front Immunol (2015) 6:289. doi: 10.3389/fimmu.2015.00289
85. Madhi SA, Cutland CL, Kuwanda L, Weinberg A, Hugo A, Jones S, et al. Influenza Vaccination of Pregnant Women and Protection of Their Infants. N Engl J Med (2014) 371(10):918–31. doi: 10.1056/NEJMoa1401480
86. Nunes MC, Cutland CL, Jones S, Hugo A, Madimabe R, Simoes EA, et al. Duration of Infant Protection Against Influenza Illness Conferred by Maternal Immunization: Secondary Analysis of a Randomized Clinical Trial. JAMA Pediatr (2016) 170(9):840–7. doi: 10.1001/jamapediatrics.2016.0921
87. Sperling RS, Engel SM, Wallenstein S, Kraus TA, Garrido J, Singh T, et al. Immunogenicity of Trivalent Inactivated Influenza Vaccination Received During Pregnancy or Postpartum. Obstet Gynecol (2012) 119(3):631–9. doi: 10.1097/AOG.0b013e318244ed20
88. Steinhoff MC, Omer SB, Roy E, Arifeen SE, Raqib R, Altaye M, et al. Influenza Immunization in Pregnancy–Antibody Responses in Mothers and Infants. N Engl J Med (2010) 362(17):1644–6. doi: 10.1056/NEJMc0912599
89. Christian LM, Porter K, Karlsson E, Schultz-Cherry S, Iams JD. Serum Proinflammatory Cytokine Responses to Influenza Virus Vaccine Among Women During Pregnancy Versus Non-Pregnancy. Am J Reprod Immunol (2013) 70(1):45–53. doi: 10.1111/aji.12117
90. Nunes MC, Weinberg A, Cutland CL, Jones S, Wang D, Dighero-Kemp B, et al. Neutralization and Hemagglutination-Inhibition Antibodies Following Influenza Vaccination of HIV-Infected and HIV-Uninfected Pregnant Women. PloS One (2018) 13(12):e0210124. doi: 10.1371/journal.pone.0210124
91. Eick AA, Uyeki TM, Klimov A, Hall H, Reid R, Santosham M, et al. Maternal Influenza Vaccination and Effect on Influenza Virus Infection in Young Infants. Arch Pediatr Adolesc Med (2011) 165(2):104–11. doi: 10.1001/archpediatrics.2010.192
92. Abbas AK, Lichtman AH, Pillai S, Baker DL, Baker A. Cellular and Molecular Immunology. Ninth edition. ed. Philadelphia, PA: Elsevier (2018). p. 565.
93. Nunes MC, Madhi SA. Prevention of Influenza-Related Illness in Young Infants by Maternal Vaccination During Pregnancy. F1000Res (2018) 7:122. doi: 10.12688/f1000research.12473.1
94. Malek A, Sager R, Kuhn P, Nicolaides KH, Schneider H. Evolution of Maternofetal Transport of Immunoglobulins During Human Pregnancy. Am J Reprod Immunol (1996) 36(5):248–55. doi: 10.1111/j.1600-0897.1996.tb00172.x
95. Cuningham W, Geard N, Fielding JE, Braat S, Madhi SA, Nunes MC, et al. Optimal Timing of Influenza Vaccine During Pregnancy: A Systematic Review and Meta-Analysis. Influenza Other Respir Viruses (2019) 13(5):438–52. doi: 10.1111/irv.12649
96. Kittikraisak W, Phadungkiatwatana P, Ditsungnoen D, Kaoiean S, Macareo L, Rungrojcharoenkit K, et al. Comparison of Influenza Antibody Titers Among Women Who Were Vaccinated in the 2. Vaccine (2021) 39(1):18–25. doi: 10.1016/j.vaccine.2020.11.032
97. Halasa NB, Gerber MA, Berry AA, Anderson EL, Winokur P, Keyserling H, et al. Safety and Immunogenicity of Full-Dose Trivalent Inactivated Influenza Vaccine (TIV) Compared With Half-Dose TIV Administered to Children 6 Through 35 Months of Age. J Pediatr Infect Dis Soc (2015) 4(3):214–24. doi: 10.1093/jpids/piu061
98. Walter EB, Rajagopal S, Zhu Y, Neuzil KM, Fairchok MP, Englund JA. Trivalent Inactivated Influenza Vaccine (TIV) Immunogenicity in Children 6 Through 23 Months of Age: Do Children of All Ages Respond Equally? Vaccine (2010) 28(27):4376–83. doi: 10.1016/j.vaccine.2010.04.058
99. Walter EB, Englund JA, Blatter M, Nyberg J, Ruben FL, Decker MD, et al. Trivalent Inactivated Influenza Virus Vaccine Given to Two-Month-Old Children: An Off-Season Pilot Study. Pediatr Infect Dis J (2009) 28(12):1099–104. doi: 10.1097/INF.0b013e3181b0c0ca
100. Pepin S, Szymanski H, Rochin Kobashi IA, Villagomez Martinez S, Gonzalez Zamora JF, Brzostek J, et al. Safety and Immunogenicity of an Intramuscular Quadrivalent Influenza Vaccine in Children 3 to 8 Y of Age: A Phase III Randomized Controlled Study. Hum Vaccin Immunother (2016) 12(12):3072–8. doi: 10.1080/21645515.2016.1212143
101. Montomoli E, Torelli A, Manini I, Gianchecchi E. Immunogenicity and Safety of the New Inactivated Quadrivalent Influenza Vaccine Vaxigrip Tetra: Preliminary Results in Children >/=6 Months and Older Adults. Vaccines (Basel) (2018) 6(1):14. doi: 10.3390/vaccines6010014
102. Wang W, Chen Q, Ford-Siltz LA, Katzelnick LC, Parra GI, Song HS, et al. Neutralizing Antibody Responses to Homologous and Heterologous H1 and H3 Influenza A Strains After Vaccination With Inactivated Trivalent Influenza Vaccine Vary With Age and Prior-Year Vaccination. Clin Infect Dis (2019) 68(12):2067–78. doi: 10.1093/cid/ciy818
103. Omer SB. Maternal Immunization. N Engl J Med (2017) 376(13):1256–67. doi: 10.1056/NEJMra1509044
104. Neuzil KM, Mellen BG, Wright PF, Mitchel EF Jr, Griffin MR. The Effect of Influenza on Hospitalizations, Outpatient Visits, and Courses of Antibiotics in Children. N Engl J Med (2000) 342(4):225–31. doi: 10.1056/NEJM200001273420401
105. Thompson MG, Li DK, Shifflett P, Sokolow LZ, Ferber JR, Kurosky S, et al. Effectiveness of Seasonal Trivalent Influenza Vaccine for Preventing Influenza Virus Illness Among Pregnant Women: A Population-Based Case-Control Study During the 2010-2011 and 2011-2012 Influenza Seasons. Clin Infect Dis (2014) 58(4):449–57. doi: 10.1093/cid/cit750
106. Regan AK, Klerk N, Moore HC, Omer SB, Shellam G, Effler PV. Effectiveness of Seasonal Trivalent Influenza Vaccination Against Hospital-Attended Acute Respiratory Infections in Pregnant Women: A Retrospective Cohort Study. Vaccine (2016) 34(32):3649–56. doi: 10.1016/j.vaccine.2016.05.032
107. Jarvis JR, Dorey RB, Warricker FDM, Alwan NA, Jones CE. The Effectiveness of Influenza Vaccination in Pregnancy in Relation to Child Health Outcomes: Systematic Review and Meta-Analysis. Vaccine (2020) 38(7):1601–13. doi: 10.1016/j.vaccine.2019.12.056
108. Tapia MD, Sow SO, Tamboura B, Tégueté I, Pasetti MF, Kodio M, et al. Maternal Immunisation With Trivalent Inactivated Influenza Vaccine for Prevention of Influenza in Infants in Mali: A Prospective, Active-Controlled, Observer-Blind, Randomised Phase 4 Trial. Lancet Infect Dis (2016) 16(9):1026–35. doi: 10.1016/S1473-3099(16)30054-8
109. Steinhoff MC, Katz J, Englund JA, Khatry SK, Shrestha L, Kuypers J, et al. Year-Round Influenza Immunisation During Pregnancy in Nepal: A Phase 4, Randomised, Placebo-Controlled Trial. Lancet Infect Dis (2017) 17(9):981–9. doi: 10.1016/S1473-3099(17)30252-9
110. Katz J, Englund JA, Steinhoff MC, Khatry SK, Shrestha L, Kuypers J, et al. Impact of Timing of Influenza Vaccination in Pregnancy on Transplacental Antibody Transfer, Influenza Incidence, and Birth Outcomes: A Randomized Trial in Rural Nepal. Clin Infect Dis (2018) 67(3):334–40. doi: 10.1093/cid/ciy090
111. Poehling KA, Szilagyi PG, Staat MA, Snively BM, Payne DC, Bridges CB, et al. Impact of Maternal Immunization on Influenza Hospitalizations in Infants. Am J Obstet Gynecol (2011) 204(6 Suppl 1):S141–8. doi: 10.1016/j.ajog.2011.02.042
112. Sugimura T, Nagai T, Kobayashi H, Ozaki Y, Yamakawa R, Hirata R. Effectiveness of Maternal Influenza Immunization in Young Infants in Japan. Pediatr Int (2016) 58(8):709–13. doi: 10.1111/ped.12888
113. Dabrera G, Zhao H, Andrews N, Begum F, Green H, Ellis J, et al. Effectiveness of Seasonal Influenza Vaccination During Pregnancy in Preventing Influenza Infection in Infants, England, 2013/14. Euro Surveill (2014) 19(45):20959. doi: 10.2807/1560-7917.ES2014.19.45.20959
114. Walker JL, Zhao H, Dabrera G, Andrews N, Thomas SL, Tsang C, et al. Assessment of Effectiveness of Seasonal Influenza Vaccination During Pregnancy in Preventing Influenza Infection in Infants in England, 2013-2014 and 2014-2015. J Infect Dis (2020) 221(1):16–20.
115. Benowitz I, Esposito DB, Gracey KD, Shapiro ED, Vazquez M. Influenza Vaccine Given to Pregnant Women Reduces Hospitalization Due to Influenza in Their Infants. Clin Infect Dis (2010) 51(12):1355–61. doi: 10.1086/657309
116. Molgaard-Nielsen D, Fischer TK, Krause TG, Hviid A. Effectiveness of Maternal Immunization With Trivalent Inactivated Influenza Vaccine in Pregnant Women and Their Infants. J Intern Med (2019) 286(4):469–80. doi: 10.1111/joim.12947
117. Sullivan SG, Feng S, Cowling BJ. Potential of the Test-Negative Design for Measuring Influenza Vaccine Effectiveness: A Systematic Review. Expert Rev Vaccines (2014) 13(12):1571–91. doi: 10.1586/14760584.2014.966695
118. Shakib JH, Korgenski K, Presson AP, Sheng X, Varner MW, Pavia AT, et al. Influenza in Infants Born to Women Vaccinated During Pregnancy. Pediatrics (2016) 137(6):e20152360. doi: 10.1542/peds.2015-2360
119. Haberg SE, Trogstad L, Gunnes N, Wilcox AJ, Gjessing HK, Samuelsen SO, et al. Risk of Fetal Death After Pandemic Influenza Virus Infection or Vaccination. N Engl J Med (2013) 368(4):333–40. doi: 10.1056/NEJMoa1207210
120. Yamada T, Yamada T, Morikawa M, Cho K, Endo T, Sato SS, et al. Pandemic (H1N1) 2009 in Pregnant Japanese Women in Hokkaido. J Obstet Gynaecol Res (2012) 38(1):130–6. doi: 10.1111/j.1447-0756.2011.01644.x
121. Jackson LA, Patel SM, Swamy GK, Frey SE, Creech CB, Munoz FM, et al. Immunogenicity of an Inactivated Monovalent 2009 H1N1 Influenza Vaccine in Pregnant Women. J Infect Dis (2011) 204(6):854–63. doi: 10.1093/infdis/jir440
122. Nunes MC, Aqil AR, Omer SB, Madhi SA. The Effects of Influenza Vaccination During Pregnancy on Birth Outcomes: A Systematic Review and Meta-Analysis. Am J Perinatol (2016) 33(11):1104–14. doi: 10.1055/s-0036-1586101
123. Claeys C, Zaman K, Dbaibo G, Li P, Izu A, Kosalaraksa P, et al. Prevention of Vaccine-Matched and Mismatched Influenza in Children Aged 6–35 Months: A Multinational Randomised Trial Across Five Influenza Seasons. Lancet Child Adolesc Health (2018) 2(5):338–49. doi: 10.1016/S2352-4642(18)30062-2
124. Allison MA, Daley MF, Crane LA, Barrow J, Beaty BL, Allred N, et al. Influenza Vaccine Effectiveness in Healthy 6- to 21-Month-Old Children During the 2003-2004 Season. J Pediatr (2006) 149(6):755–62. doi: 10.1016/j.jpeds.2006.06.036
125. Eisenberg KW, Szilagyi PG, Fairbrother G, Griffin MR, Staat M, Shone LP, et al. Vaccine Effectiveness Against Laboratory-Confirmed Influenza in Children 6 to 59 Months of Age During the 2003-2004 and 2004-2005 Influenza Seasons. Pediatrics (2008) 122(5):911–9. doi: 10.1542/peds.2007-3304
126. Blyth CC, Jacoby P, Effler PV, Kelly H, Smith DW, Robins C, et al. Effectiveness of Trivalent Flu Vaccine in Healthy Young Children. Pediatrics (2014) 133(5):e1218–25. doi: 10.1542/peds.2013-3707
127. Cowling BJ, Chan KH, Feng S, Chan EL, Lo JY, Peiris JS, et al. The Effectiveness of Influenza Vaccination in Preventing Hospitalizations in Children in Hong Kong, 2009-2013. Vaccine (2014) 32(41):5278–84. doi: 10.1016/j.vaccine.2014.07.084
128. Kelly H, Jacoby P, Dixon GA, Carcione D, Williams S, Moore HC, et al. Vaccine Effectiveness Against Laboratory-Confirmed Influenza in Healthy Young Children: A Case-Control Study. Pediatr Infect Dis J (2011) 30(2):107–11. doi: 10.1097/INF.0b013e318201811c
129. Belongia EA, Kieke BA, Donahue JG, Coleman LA, Irving SA, Meece JK, et al. Influenza Vaccine Effectiveness in Wisconsin During the 2007-08 Season: Comparison of Interim and Final Results. Vaccine (2011) 29(38):6558–63. doi: 10.1016/j.vaccine.2011.07.002
130. Van Buynder PG, Dhaliwal JK, Van Buynder JL, Couturier C, Minville-Leblanc M, Garceau R, et al. Protective Effect of Single-Dose Adjuvanted Pandemic Influenza Vaccine in Children. Influenza Other Respir Viruses (2010) 4(4):171–8. doi: 10.1111/j.1750-2659.2010.00146.x
131. Blyth CC, Cheng AC, Crawford NW, Clark JE, Buttery JP, Marshall HS, et al. The Impact of New Universal Child Influenza Programs in Australia: Vaccine Coverage, Effectiveness and Disease Epidemiology in Hospitalised Children in 2018. Vaccine (2020) 38(13):2779–87. doi: 10.1016/j.vaccine.2020.02.031
132. Clover RD, Crawford S, Glezen WP, Taber LH, Matson CC, Couch RB. Comparison of Heterotypic Protection Against Influenza A/Taiwan/86 (H1N1) by Attenuated and Inactivated Vaccines to A/Chile/83-Like Viruses. J Infect Dis (1991) 163(2):300–4. doi: 10.1093/infdis/163.2.300
133. Colombo C, Argiolas L, La Vecchia C, Negri E, Meloni G, Meloni T. Influenza Vaccine in Healthy Preschool Children. Rev Epidemiol Sante Publique (2001) 49(2):157–62.
134. Gruber WC, Taber LH, Glezen WP, Clover RD, Abell TD, Demmler RW, et al. Live Attenuated and Inactivated Influenza Vaccine in School-Age Children. Am J Dis Child (1990) 144(5):595–600. doi: 10.1001/archpedi.1990.02150290089035
135. Jefferson T, Rivetti A, Di Pietrantonj C, Demicheli V. Vaccines for Preventing Influenza in Healthy Children. Cochrane Database Syst Rev (2018) 2:CD004879. doi: 10.1002/14651858.CD004879.pub5
136. Hoberman A, Greenberg DP, Paradise JL, Rockette HE, Lave JR, Kearney DH, et al. Effectiveness of Inactivated Influenza Vaccine in Preventing Acute Otitis Media in Young Children - A Randomized Controlled Trial. JAMA-J Am Med Assoc (2003) 290(12):1608–16. doi: 10.1001/jama.290.12.1608
137. Jansen AG, Sanders EA, Hoes AW, van Loon AM, Hak E. Effects of Influenza Plus Pneumococcal Conjugate Vaccination Versus Influenza Vaccination Alone in Preventing Respiratory Tract Infections in Children: A Randomized, Double-Blind, Placebo-Controlled Trial. J Pediatr (2008) 153(6):764–70. doi: 10.1016/j.jpeds.2008.05.060
138. Jain VK, Rivera L, Zaman K, Espos RA, Sirivichayakul C, Quiambao BP, et al. Vaccine for Prevention of Mild and Moderate-to-Severe Influenza in Children. N Engl J Med (2013) 369(26):2481–91. doi: 10.1056/NEJMoa1215817
139. Rolfes MA, Goswami D, Sharmeen AT, Yeasmin S, Parvin N, Nahar K, et al. Efficacy of Trivalent Influenza Vaccine Against Laboratory-Confirmed Influenza Among Young Children in a Randomized Trial in Bangladesh. Vaccine (2017) 35(50):6967–76. doi: 10.1016/j.vaccine.2017.10.074
140. Diallo A, Diop OM, Diop D, Niang MN, Sugimoto JD, Ortiz JR, et al. Effectiveness of Seasonal Influenza Vaccination in Children in Senegal During a Year of Vaccine Mismatch: A Cluster-Randomized Trial. Clin Infect Dis (2019) 69(10):1780–8. doi: 10.1093/cid/ciz066
141. Sullender WM, Fowler KB, Gupta V, Krishnan A, Ram Purakayastha D, Srungaram Vln R, et al. Efficacy of Inactivated Trivalent Influenza Vaccine in Rural India: A 3-Year Cluster-Randomised Controlled Trial. Lancet Glob Health (2019) 7(7):e940–e50. doi: 10.1016/S2214-109X(19)30079-8
142. Heikkinen T, Ruuskanen O, Waris M, Ziegler T, Arola M, Halonen P. Influenza Vaccination in the Prevention of Acute Otitis Media in Children. Am J Dis Child (1991) 145(4):445–8. doi: 10.1001/archpedi.1991.02160040103017
143. Baum U, Kulathinal S, Auranen K, Nohynek H. Effectiveness of 2 Influenza Vaccines in Nationwide Cohorts of Finnish 2-Year-Old Children in the Seasons 2015-2016 Through 2017-2018. Clin Infect Dis (2020) 71(8):e255–e61. doi: 10.1093/cid/ciaa050
144. Joshi AY, Iyer VN, St Sauver JL, Jacobson RM, Boyce TG. Effectiveness of Inactivated Influenza Vaccine in Children Less Than 5 Years of Age Over Multiple Influenza Seasons: A Case-Control Study. Vaccine (2009) 27(33):4457–61. doi: 10.1016/j.vaccine.2009.05.038
145. Heinonen S, Silvennoinen H, Lehtinen P, Vainionpää R, Ziegler T, Heikkinen T. Effectiveness of Inactivated Influenza Vaccine in Children Aged 9 Months to 3 Years: An Observational Cohort Study. Lancet Infect Dis (2011) 11(1):23–9. doi: 10.1016/S1473-3099(10)70255-3
146. Turner N, Pierse N, Bissielo A, Huang QS, Baker MG, Widdowson MA, et al. The Effectiveness of Seasonal Trivalent Inactivated Influenza Vaccine in Preventing Laboratory Confirmed Influenza Hospitalisations in Auckland, New Zealand in 2012. Vaccine (2014) 32(29):3687–93. doi: 10.1016/j.vaccine.2014.04.013
147. Qin Y, Zhang Y, Wu P, Feng S, Zheng J, Yang P, et al. Influenza Vaccine Effectiveness in Preventing Hospitalization Among Beijing Residents in China, 2013-15. Vaccine (2016) 34(20):2329–33. doi: 10.1016/j.vaccine.2016.03.068
148. Zhang Y, Wu P, Feng L, Yang P, Pan Y, Feng S, et al. Influenza Vaccine Effectiveness Against Influenza-Associated Hospitalization in 2015/16 Season, Beijing, China. Vaccine (2017) 35(23):3129–34. doi: 10.1016/j.vaccine.2017.03.084
149. Chua H, Chiu SS, Chan ELY, Feng S, Kwan MYW, Wong JSC, et al. Effectiveness of Partial and Full Influenza Vaccination Among Children Aged <9 Years in Hong Kong, 2011-2019. J Infect Dis (2019) 220(10):1568–76. doi: 10.1093/infdis/jiz361
150. Segaloff HE, Leventer-Roberts M, Riesel D, Malosh RE, Feldman BS, Shemer-Avni Y, et al. Influenza Vaccine Effectiveness Against Hospitalization in Fully and Partially Vaccinated Children in Israel: 2015-2016, 2016-2017, and 2017-2018. Clin Infect Dis (2019) 69(12):2153–61. doi: 10.1093/cid/ciz125
151. Sofia Arriola C, El Omeiri N, Azziz-Baumgartner E, Thompson MG, Sotomayor-Proschle V, Fasce RA, et al. Influenza Vaccine Effectiveness Against Hospitalizations in Children and Older Adults-Data From South America, 2013-2017. A Test Negative Design. Vaccine X (2019) 3:100047. doi: 10.1016/j.jvacx.2019.100047
152. Buchan SA, Chung H, Campitelli MA, Crowcroft NS, Gubbay JB, Karnauchow T, et al. Vaccine Effectiveness Against Laboratory-Confirmed Influenza Hospitalizations Among Young Children During the 2010-11 to 2013-14 Influenza Seasons in Ontario, Canada. PloS One (2017) 12(11):e0187834. doi: 10.1371/journal.pone.0187834
153. Campbell AP, Ogokeh C, Lively JY, Staat MA, Selvarangan R, Halasa NB, et al. Vaccine Effectiveness Against Pediatric Influenza Hospitalizations and Emergency Visits. Pediatrics (2020) 146(5):e20201368. doi: 10.1542/peds.2020-1368
154. Loeb M, Russell ML, Moss L, Fonseca K, Fox J, Earn DJ, et al. Effect of Influenza Vaccination of Children on Infection Rates in Hutterite Communities: A Randomized Trial. JAMA (2010) 303(10):943–50. doi: 10.1001/jama.2010.250
155. Pepin S, Samson SI, Alvarez FP, Dupuy M, Gresset-Bourgeois V, De Bruijn I. Impact of a Quadrivalent Inactivated Influenza Vaccine on Influenza-Associated Complications and Health Care Use in Children Aged 6 to 35months: Analysis of Data From a Phase III Trial in the Northern and Southern Hemispheres. Vaccine (2019) 37(13):1885–8. doi: 10.1016/j.vaccine.2019.01.059
156. Ruohola A, Meurman O, Nikkari S, Skottman T, Salmi A, Waris M, et al. Microbiology of Acute Otitis Media in Children With Tympanostomy Tubes: Prevalences of Bacteria and Viruses. Clin Infect Dis (2006) 43(11):1417–22. doi: 10.1086/509332
157. Norhayati MN, Ho JJ, Azman MY. Influenza Vaccines for Preventing Acute Otitis Media in Infants and Children. Cochrane Database Syst Rev (2017) 10:CD010089. doi: 10.1002/14651858.CD010089.pub3
158. Fink G, Orlova-Fink N, Schindler T, Grisi S, Ferrer APS, Daubenberger C, et al. Inactivated Trivalent Influenza Vaccination Is Associated With Lower Mortality Among Patients With COVID-19 in Brazil. BMJ Evidence-Based Med (2021) 26:192–3. doi: 10.1136/bmjebm-2020-111549
159. Reichert TA, Sugaya N, Fedson DS, Glezen WP, Simonsen L, Tashiro M. The Japanese Experience With Vaccinating Schoolchildren Against Influenza. N Engl J Med (2001) 344(12):889–96. doi: 10.1056/NEJM200103223441204
160. Guthmiller JJ, Utset HA, Henry C, Li L, Zheng NY, Sun W, et al. An Egg-Derived Sulfated N-Acetyllactosamine Glycan Is an Antigenic Decoy of Influenza Virus Vaccines. mBio (2021) 12(3):e0083821. doi: 10.1128/mBio.00838-21
161. Jung J, Mundle ST, Ustyugova IV, Horton AP, Boutz DR, Pougatcheva S, et al. Influenza Vaccination in the Elderly Boosts Antibodies Against Conserved Viral Proteins and Egg-Produced Glycans. J Clin Invest (2021) 131(13):e148763. doi: 10.1172/JCI148763
162. Barr IG, Donis RO, Katz JM, McCauley JW, Odagiri T, Trusheim H, et al. Cell Culture-Derived Influenza Vaccines in the Severe 2017-2018 Epidemic Season: A Step Towards Improved Influenza Vaccine Effectiveness. NPJ Vaccines (2018) 3:44. doi: 10.1038/s41541-018-0079-z
163. DiazGranados CA, Denis M, Plotkin S. Seasonal Influenza Vaccine Efficacy and Its Determinants in Children and Non-Elderly Adults: A Systematic Review With Meta-Analyses of Controlled Trials. Vaccine (2012) 31(1):49–57. doi: 10.1016/j.vaccine.2012.10.084
164. Eun BW, Lee TJ, Lee J, Kim KH, Kim DH, Jo DS, et al. A Randomized, Double-Blind, Active-Controlled Phase III Trial of a Cell Culture-Derived Quadrivalent Inactivated Influenza Vaccine in Healthy South Korean Children and Adolescents 6 Months to 18 Years of Age. Pediatr Infect Dis J (2019) 38(9):e209–e15. doi: 10.1097/INF.0000000000002406
165. Oh CE, Choi UY, Eun BW, Lee TJ, Kim KH, Kim DH, et al. A Randomized, Double-Blind, Active-Controlled Clinical Trial of a Cell Culture-Derived Inactivated Trivalent Influenza Vaccine (NBP607) in Healthy Children 6 Months Through 18 Years of Age. Pediatr Infect Dis J (2018) 37(6):605–11. doi: 10.1097/INF.0000000000001973
166. Diez-Domingo J, de Martino M, Lopez JG, Zuccotti GV, Icardi G, Villani A, et al. Safety and Tolerability of Cell Culture-Derived and Egg-Derived Trivalent Influenza Vaccines in 3 to <18-Year-Old Children and Adolescents at Risk of Influenza-Related Complications. Int J Infect Dis (2016) 49:171–8. doi: 10.1016/j.ijid.2016.06.018
167. Nolan T, Chotpitayasunondh T, Capeding MR, Carson S, Senders SD, Jaehnig P, et al. Safety and Tolerability of a Cell Culture Derived Trivalent Subunit Inactivated Influenza Vaccine Administered to Healthy Children and Adolescents: A Phase III, Randomized, Multicenter, Observer-Blind Study. Vaccine (2016) 34(2):230–6. doi: 10.1016/j.vaccine.2015.11.040
168. Richards KA, Moritzky S, Shannon I, Fitzgerald T, Yang H, Branche A, et al. Recombinant HA-Based Vaccine Outperforms Split and Subunit Vaccines in Elicitation of Influenza-Specific CD4 T Cells and CD4 T Cell-Dependent Antibody Responses in Humans. NPJ Vaccines (2020) 5(1):77. doi: 10.1038/s41541-020-00227-x
169. Chaudhary N, Weissman D, Whitehead KA. mRNA Vaccines for Infectious Diseases: Principles, Delivery and Clinical Translation. Nat Rev Drug Discovery (2021) 1–22. doi: 10.1038/s41573-021-00283-5
170. Gray KJ, Bordt EA, Atyeo C, Deriso E, Akinwunmi B, Young N, et al. Coronavirus Disease 2019 Vaccine Response in Pregnant and Lactating Women: A Cohort Study. Am J Obstet Gynecol (2021) 225(3):303.e1–303.e17. doi: 10.1101/2021.03.07.21253094
Keywords: inactivated influenza vaccine (IIV), safety, immunogenicity, vaccine efficacy, vaccine effectiveness (VE), young children, pregnant women
Citation: Bansal A, Trieu M-C, Mohn KGI and Cox RJ (2021) Safety, Immunogenicity, Efficacy and Effectiveness of Inactivated Influenza Vaccines in Healthy Pregnant Women and Children Under 5 Years: An Evidence-Based Clinical Review. Front. Immunol. 12:744774. doi: 10.3389/fimmu.2021.744774
Received: 20 July 2021; Accepted: 08 September 2021;
Published: 06 October 2021.
Edited by:
Sofia A. Casares, Naval Medical Research Center, United StatesReviewed by:
Chang-Han Lee, Seoul National University, South KoreaCopyright © 2021 Bansal, Trieu, Mohn and Cox. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rebecca Jane Cox, cmViZWNjYS5jb3hAdWliLm5v; Amit Bansal, YW1pdC5iYW5zYWxAdWliLm5v
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.