 Federica Defendi1*
Federica Defendi1* Corentin Leroy2,3
Corentin Leroy2,3 Olivier Epaulard4,5
Olivier Epaulard4,5 Giovanna Clavarino1
Giovanna Clavarino1 Antoine Vilotitch2Marion Le Marechal4Marie-Christine Jacob1Tatiana Raskovalova1Martine Pernollet1
Antoine Vilotitch2Marion Le Marechal4Marie-Christine Jacob1Tatiana Raskovalova1Martine Pernollet1 Audrey Le Gouellec5,6Jean-Luc Bosson5Pascal Poignard7,8
Audrey Le Gouellec5,6Jean-Luc Bosson5Pascal Poignard7,8 Matthieu Roustit9,10
Matthieu Roustit9,10 Nicole Thielens7
Nicole Thielens7 Chantal Dumestre-Pérard1,7†Jean-Yves Cesbron1†
Chantal Dumestre-Pérard1,7†Jean-Yves Cesbron1†- 1Laboratoire d’Immunologie, Institut de Biologie et Pathologie, Centre Hospitalier Universitaire Grenoble Alpes, Grenoble, France
- 2Cellule d’Ingénierie des Données, Centre Hospitalier Universitaire Grenoble Alpes, Grenoble, France
- 3Centre d’Investigation Clinique de l’Innovation et de la Technologie (CIC-IT), Centre Hospitalier Universitaire Grenoble Alpes, Grenoble, France
- 4Service des Maladies Infectieuses et Tropicales, Centre Hospitalier Universitaire Grenoble Alpes, Grenoble, France
- 5Université Grenoble Alpes, TIMC-IMAG, Grenoble, France
- 6Laboratoire de Biochimie, Institut de Biologie et Pathologie, Centre Hospitalier Universitaire Grenoble Alpes, Grenoble, France
- 7Université Grenoble Alpes, CNRS, CEA, Institut de Biologie Structurale (IBS), Grenoble, France
- 8Laboratoire de Virologie, Institut de Biologie et Pathologie, Centre Hospitalier Universitaire Grenoble Alpes, Grenoble, France
- 9Département de Pharmacologie Clinique INSERM CIC 1406, Centre Hospitalier Universitaire Grenoble Alpes, Grenoble, France
- 10Université Grenoble Alpes, UMR 1042-HP2, INSERM, Grenoble, France
Background: The SARS-CoV-2 infection triggers excessive immune response resulting in increased levels of pro-inflammatory cytokines, endothelial injury, and intravascular coagulopathy. The complement system (CS) activation participates to this hyperinflammatory response. However, it is still unclear which activation pathways (classical, alternative, or lectin pathway) pilots the effector mechanisms that contribute to critical illness. To better understand the immune correlates of disease severity, we performed an analysis of CS activation pathways and components in samples collected from COVID-19 patients hospitalized in Grenoble Alpes University Hospital between 1 and 30 April 2020 and of their relationship with the clinical outcomes.
Methods: We conducted a retrospective, single-center study cohort in 74 hospitalized patients with RT-PCR-proven COVID-19. The functional activities of classical, alternative, and mannose-binding lectin (MBL) pathways and the antigenic levels of the individual components C1q, C4, C3, C5, Factor B, and MBL were measured in patients’ samples during hospital admission. Hierarchical clustering with the Ward method was performed in order to identify clusters of patients with similar characteristics of complement markers. Age was included in the model. Then, the clusters were compared with the patient clinical features: rate of intensive care unit (ICU) admission, corticoid treatment, oxygen requirement, and mortality.
Results: Four clusters were identified according to complement parameters. Among them, two clusters revealed remarkable profiles: in one cluster (n = 15), patients exhibited activation of alternative and lectin pathways and low antigenic levels of MBL, C4, C3, Factor B, and C5 compared to all the other clusters; this cluster had the higher proportion of patients who died (27%) and required oxygen support (80%) or ICU care (53%). In contrast, the second cluster (n = 19) presented inflammatory profile with high classical pathway activity and antigenic levels of complement components; a low proportion of patients required ICU care (26%) and no patient died in this group.
Conclusion: These findings argue in favor of prominent activation of the alternative and MBL complement pathways in severe COVID-19, but the spectrum of complement involvement seems to be heterogeneous requiring larger studies.
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection drives sustained inflammatory response considered to be a major cause of disease severity and death in patients with COVID-19 (1). Growing evidence suggests that the complement system (CS) activation instigates this dysregulated inflammatory reaction in COVID-19: elevated levels of the anaphylatoxin C5a have been reported to be proportional to disease severity (2); the membrane attack complex concentration has been linked with respiratory failure and systemic inflammation in infected patients (3); and deposits of mannose-binding lectin (MBL) and MBL-associated protease MASP-2 have been found in the microvasculature of critical patients with SARS CoV-2 infection (4). On the other hand, patients treated with complement blockers (anti-C5a mAb [eculizumab] or C3-inhibitor) exhibited a drop in inflammatory markers and significant clinical improvement (5–9). However, it is still not fully understood which of the three complement activation pathways (classical, alternative, or lectin pathway) drives the effector mechanisms that contribute to the tissue injury. To address these questions, we performed extensive analysis of CS activation pathways and components in samples collected from hospitalized COVID-19 patients and their relationship with the clinical outcomes.
Methods
Study Participants
This retrospective, single center study included 74 patients with RT-PCR-proven COVID-19 admitted to Grenoble Alpes University Hospital from April 1 to 30, 2020. Samples were collected during hospitalization in infectious/pneumology/internal medicine department or intensive care unit (ICU) of our hospital. The study was performed in accordance with the Declaration of Helsinki, Good Clinical Practice guidelines, and CNIL (Commission Nationale de l’Informatique et des Libertés) methodology reference. Patients were informed and consent was obtained, according to French law. Demographic, clinical characteristics (oxygen requirements, ICU admission, mortality, steroid treatment) and laboratory data were collected from electronic clinical records and included in an anonymized database. Patients were classified as severe on the basis of oxygen requirement (>2 L O2/min), ICU admission, limitation of therapeutic effort (LTE), and mortality, according to (10).
Complement Testing
Peripheral blood samples were collected in citrate anticoagulated or without anticoagulant tubes for hemolytic and functional assays or antigenic level measurement, respectively. Total hemolytic assays for classical pathway (CP, TH50c) and alternative pathway (AP, TH50a) were assessed as previously published (11); 100% lysis is defined by the TH50c/TH50a of the control sample. Reference values (TH50c: 86–126%; TH50a: 84–150%) were established by testing samples from 50 blood donors.
Antigenic levels of C1q, C4, C3, C5, and Factor B proteins in the serum samples were measured using a laser nephelometer BNII (Dade Behring, GmbH, Marburg, Germany). Reference intervals (RI; C1q: 154–258 mg/L; C4: 100–380 mg/L; C3: 880–1650 mg/L; C5: 120–220 mg/L; Factor B: 216–504 mg/L) were obtained by testing samples from 50 blood donors.
Determination of MBL protein concentration and function was realized by an enzyme-linked immunosorbent assay (ELISA) as described previously (12). The characterization of MBL protein expression deficiency was established by the combination of three assays: ELISA for antigen and functional MBL and hemolytic activity of C4 (C4H) (13) normal values of C1q confirmed the absence of CP activation. Low values of antigenic (<100 µg/L) (14) and functional MBL associated with a normal value of C4H defined patients with MBL protein expression deficiency. Low levels of antigenic and functional MBL associated with decreased value of C4H identified patients with MBL pathway activation. Reference values for MBL protein concentration and function and C4H were determined from 50 blood donors (MBL antigen: 30–3000 µg/L; MBL function: 35–115%; C4H: 70–130%).
Statistical Analysis
Statistical analysis was performed using hierarchical ascendant clustering (HAC) in order to identify groups of COVID-19 patients with similar characteristics (“clusters”) in terms of complement variables: TH50c, TH50a, C1q, C4, C3, C5, Factor B, and MBL antigen. Age was included in the model (Supplementary Methods).
The biological significance of the clusters was analyzed by comparing the values of every complement parameter between the clusters. The ANOVA F-test was performed for variables with a Gaussian distribution, and the Kruskal-Wallis test for the variables with other distribution. Mean (standard deviation [sd]) or median (interquartile range [IQR]) were presented for the parametric or non-parametric variables, respectively. For the markers with a significant difference between the clusters, specific cluster by cluster tests were performed using Student or Wilcoxon tests to identify the cluster significantly different from the others. Post-hoc analysis with the Fisher’s exact test was used to test specific difference between the clusters.
Results
Table 1 details the main demographic and clinical characteristics of our cohort. The median age of patients was 72 years (IQR: 62;82; range: 32–96); more than half of patients were men (58%). Of the 74 patients, 43 (58%) were severe, 8 (11%) died, 23 (31%) were admitted in the ICU, 3 (4%) were with LTE, and 23 (31%) required treatment by corticoids.
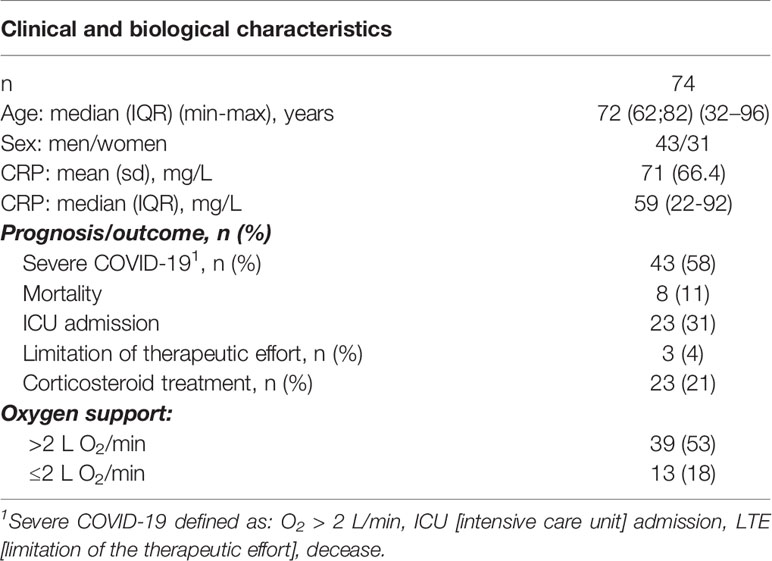
Table 1 Patient characteristics.
The results of complement proteins and activation pathways analysis performed in samples collected during hospitalization are summarized in Table 2.
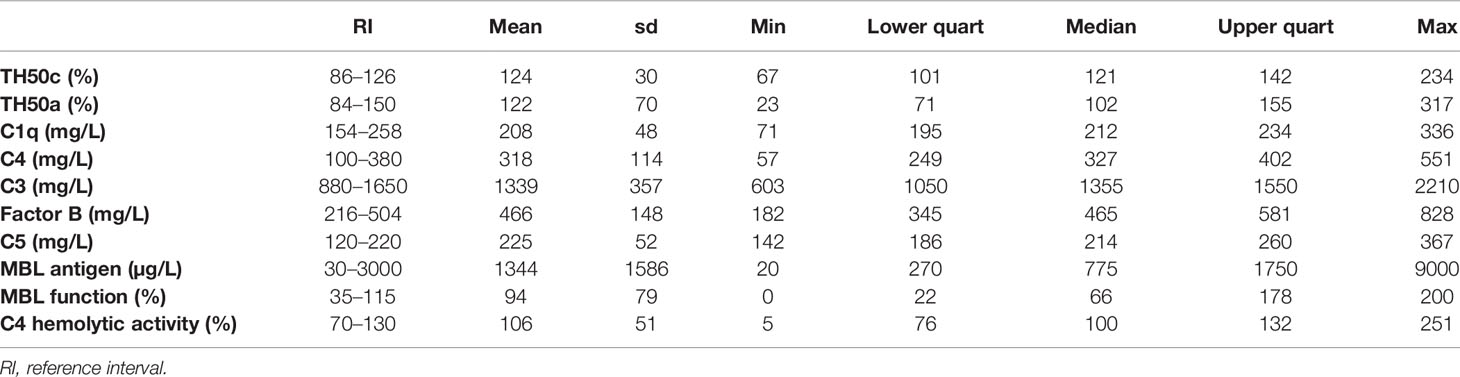
Table 2 Complement parameters.
Four clusters of individuals were identified in the studied cohort by HAC analysis according to the complement data (Supplementary Figure S1). The comparison between the clusters (cluster 2 against others and/or cluster 4 against others) is presented in Figure 1 and Table 3. There was no statistically significant difference among the four clusters for sex, age, CRP, severity, ICU admission, O2 requirement, or corticoid treatment (Table 4).
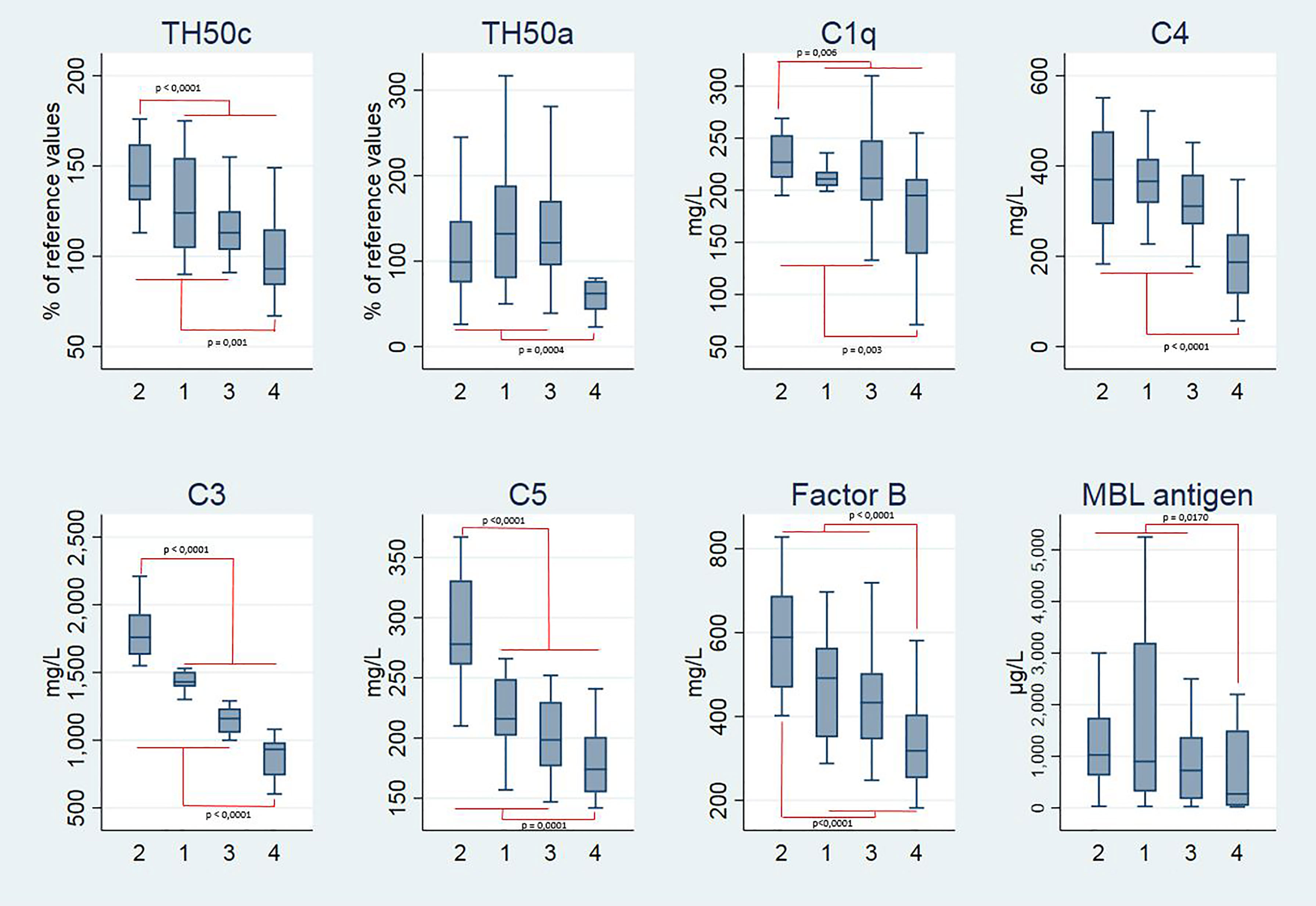
Figure 1 Boxplots representing the complement parameters of the four clusters of patients. Statistical analysis by hierarchical ascendant clustering discriminates the 74 patients with COVID-19 of the cohort in four distinct clusters according to complement variables: TH50c, TH50a, C1q, C4, C3, C5, Factor B, and MBL antigen. Age was included in the model. Boxplots represent the median and 25th to 75th percentiles, the whiskers denote the maximum and minimum values, and the horizontal bars indicate the medians. Outside values were excluded.
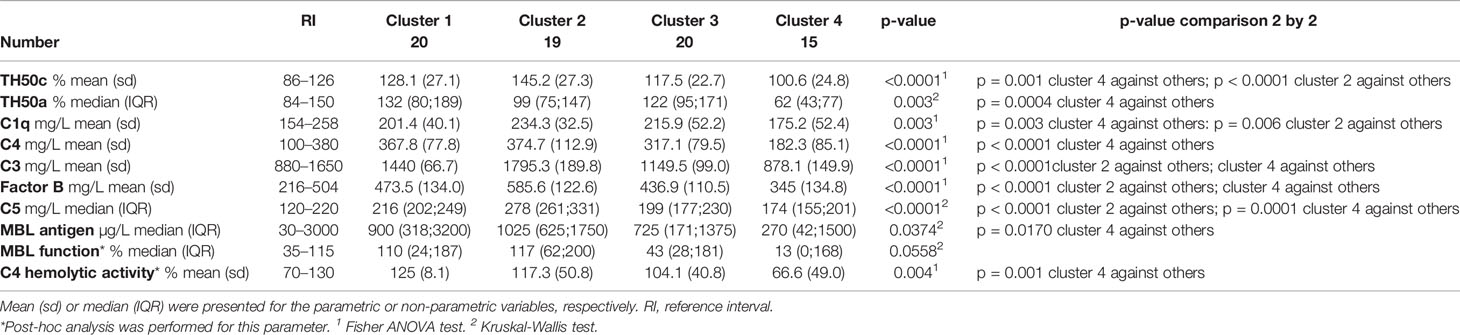
Table 3 Clusters of COVID-19 patients according to complement parameters.
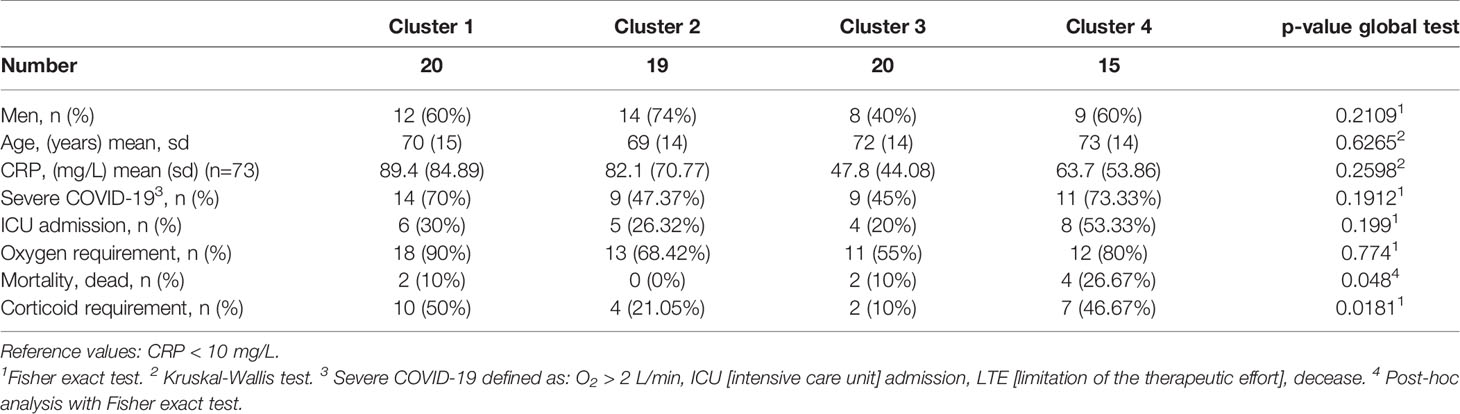
Table 4 Overall comparison of clinical and biological characteristics between the clusters.
For patients of the first cluster (n = 20; 27%), the complement profile was overall without anomalies (TH50c: 128%; TH50a: 132%; C1q: 201 mg/L; C4: 368 mg/L; C3: 1440 mg/L; C5: 216 mg/L; Factor B: 474 mg/L; MBL antigen: 900 µg/L; MBL function: 110%; C4H: 125%; Table 3). A large percentage of patients in this cluster was severe (n = 14; 70%) and required corticoid treatment (n = 10; 50%) (Table 4).
Patients of cluster 2 (n = 19; 26%) exhibited an inflammatory profile: high values of CP, LP, and C4 activities (TH50c: 145%; MBL function: 117%; C4H: 118%) and increased antigenic levels of C3 (1795 mg/L), C5 (278 mg/L), Factor B (586 mg/L), and MBL (1025 µg/L) were observed in this cluster compared to other clusters (Table 3). The majority of patients of the second cluster were men (men/women: 14/5). Interestingly, none of the patients died in this cluster (Table 4).
In cluster 3 (n = 20; 27%), most complement markers were within reference interval (TH50c: 118%; TH50a: 122%; C1q: 216 mg/L; C4: 317 mg/L; C3: 1150 mg/L; C5: 199 mg/L; Factor B: 437 mg/L; MBL antigen: 725 µg/L; C4H: 104%); only MBL function was decreased (43%) (Table 3). The third cluster was characterized by the lowest rate of ICU admission (20%) and by the lowest rate of patients having required corticoid treatment (10%); the rate of mortality was also low in this cluster (10%) (Table 4).
Finally, the fourth cluster (n = 15; 20%) (Tables 3, 4; Supplementary Table S1) was specifically characterized by significant activation of alternative (TH50a: 62%; p = 0.0004 against other clusters) and lectin (MBL antigen: 270 µg/L: p = 0.0170 against other clusters) complement pathways. Decreased MBL concentration was associated with reduced MBL function (13%) and C4H (67%) confirming the MBL pathway activation. TH50c was also decreased compared to the other clusters (101%; p = 0.001), but remained in the RI (86–126%). Interestingly, in this cluster, 13 patients (87%) exhibited AP activation and 7 patients (47%) exhibited MBL pathway activation; 6 (40%) patients presented simultaneously AP and MBL pathway activation (Supplementary Table S1). A large percentage of patients of the fourth cluster was severe (73%) and required ICU admission (53%) and corticoid treatment (47%) (Table 4). Among the 11 severe patients, 10 exhibited AP activation; 6 exhibited MBL pathway activation, and 5 presented at the same time AP and MBL pathway activation (Supplementary Table S1). Of note, cluster 4 was characterized by a higher mortality rate (27% versus 10%, 0% and 10% in clusters 1, 2, and 3, respectively; p = 0.048) (Table 4). Among the four patients who died, three presented AP activation, two exhibited MBL pathway activation, and two patients showed concurrent activation of alternative and MBL pathways (Supplementary Table S1). Regarding the four other patients who died, all presented a normal complement profile except patient 1 who exhibited an MBL deficiency (Supplementary Table S2).
Discussion
SARS-CoV-2 infection triggers an innate immune response including CS activation which is a key weapon both implicated in disease resolution and organ damage depending on the time of infection (15).
Recent studies addressing the role of complement in the pathogenesis of COVID-19 have shown a relationship between respiratory failure, intravascular coagulopathy, and complement overactivation in COVID-19 patients (3, 16). There are several lines of evidence for local deposition of complement proteins and activation products in lung, skin, and other tissues showing activation of the three pathways, CP, LP, and AP (17–21). Furthermore, systemic complement activation and consumption were related to severe COVID-19 and predictive of in-hospital mortality (22). However, despite in vitro lines of evidence suggesting that the SARS-CoV-2 spike proteins activate the AP (23), it remains incompletely understood which complement activation pathways contribute to critical illness in COVID-19.
Concerning the possible involvement of MBL in coronavirus infection, it has been described so far for SARS-CoV in several studies. Among those, two in vitro studies demonstrated binding of MBL to SARS-CoV or viral particles pseudotyped with SARS-CoV spike protein and activation of the lectin complement pathway (24, 25). More recently, Ali and al showed binding of LP recognition molecules to S- and N- proteins of SARS-CoV-2, as also robust LP activation on the surface of HEK 293 cells expressing SARS-CoV-2 S protein (26).
One of the limitation of the study is that it reports data about the original variant of the virus, while the delta variant is now a majority among the infected patients. The crucial mutations leading to delta variant concern the S1 subunit (intimately involved in the initiation of infection) for which we have no data concerning its molecular interaction with complement components. However, the replication rate of delta strain is much higher. It would therefore be interesting to compare our results with samples collected from patients infected with the delta variant of the virus.
Using an original, unsupervised statistical approach by hierarchical clustering on complement and clinical parameters, this study reveals for the first time the association between AP and LP activation, and the mortality in COVID-19 patients (cluster 4). Our data are in line with Ma et al. showing increased AP components in COVID-19 patients with worse prognosis (27) and with Sinkovits et al. relating significant association between AP activity and COVID-19 severity (22).
Furthermore, our results provide additional evidence for an association between MBL pathway activation and mortality, supported by the data of Eriksson et al. (4). In contrast, Sinkovits et al. reported that the LP activity showed no difference between severity groups (22). Our data are consistent with recent reports describing deposits of MBL and MASP2 in affected tissues of COVID-19 patients and in vitro MBL pathway activation by recombinant SARS-CoV2 proteins (17, 28). Collectively, these findings are consistent with the CS implication in the pathogenesis of severe COVID-19 infection. As consequences of unrestrained complement activation, the strong pro-inflammatory C5a-C5aR axis promotes neutrophil/monocyte infiltration and the “cytokine storm” driving lung inflammation and injury, responsible for complications in hospitalized COVID-19 patients (2).
If complement activation is evident from our results and associated with the severity of the disease, the spectrum of involvement of the complement cascade in COVID-19 seems to be heterogeneous and depending on patients: notably, complement activation could be deleterious in some ones and expression of the severity of the disease in other ones. A recent review summarizes the current knowledge about modulating complement cascade as therapeutic approach in COVID-19 patients (29). In brief, despite nonconclusive studies, the available data suggested favorable outcomes in a small number of patients with severe COVID-19 treated either with C1 inhibitor, MASP-2 monoclonal antibodies, compstatin-based complement C3 inhibitor, anti-C5 drugs, or C5a-C5aR1 antagonists. Clinical trials of complement inhibitors in COVID-19 are ongoing (NCT04288713, NCT04414631, NCT04395456). However, awaiting final results from the clinical trials, the potential benefits from complement inhibition in COVID-19 remain to be elucidated.
Interestingly, we found high incidence of MBL expression deficiency in patients of our cohort (16%, established as described in Methods), all clusters combined. Further studies based on MBL genotyping would be of interest to support biochemical data. MBL deficiency is fairly common, affecting approximately 5–10% of individuals and usually associated with increased susceptibility to bacterial infections of the upper respiratory in young children (30).
Our results highlight the dichotomous nature of the complement MBL pathway: on one hand, MBL appears to contribute to the pathogenesis of disease because it mediates complement activation that is related to clinical deterioration of patients; on the other hand, MBL could have a protective role against SARS-CoV-2 infection by promoting phagocytosis and virus lysis or neutralization. Further in vitro studies using pseudoviral particles or the SARS-CoV-2 virus are necessary to check the latter hypothesis.
In summary, our study suggests that alternative and lectin pathways assessment might be useful as biomarker of disease severity. Extensive investigations of complement pathways have to be performed on a larger cohort of patients with SARS-CoV-2 infection to help rationalize therapeutic choices.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Commission Nationale de l'Informatique et des Libertés (CNIL). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
Study conception: FD, CD-P, and J-YC. Immunological determinations: FD, CD-P, M-CJ, TR, and MP. Methodology: MR. Statistical analysis: CL, AV, and J-LB. Collection of patients’ samples and clinical information: OE and MM. Funding acquisition: FD, CD-P, NT, OE, GC, AG, and PP. Writing original draft: FD and CD-P. Review manuscript: J-YC and NT. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by funding from the Université Grenoble Alpes (projects COMPLEC-COV and BIOMARCOVID).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors are grateful for the excellent work from the staff of technicians at Complement Laboratory of Grenoble-Alpes University Hospital: Marion Allegret-Cadet, Véronique Bergerot, Nadège Fondraz, Marie-Anne Pasquier and from Pierre Audoin for help in project conception.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2021.742446/full#supplementary-material
Abbreviations
AP, alternative pathway; COVID-19, coronavirus disease 19; CP, classical pathway; CS, Complement system; C4H, C4 hemolytic activity; LTE, limitation of the therapeutic effort; LP, lectin pathway; MBL, mannose-binding lectin; RI, reference interval.
References
1. Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ. HLH Across Speciality Collaboration, UK. COVID-19: Consider Cytokine Storm Syndromes and Immunosuppression. Lancet (2020) 395:1033–4. doi: 10.1016/S0140-6736(20)30628-0
2. Carvelli J, Demaria O, Vély F, Batista L, Benmansour NC, Fares J, et al. Association of COVID-19 Inflammation With Activation of the C5a-C5aR1 Axis. Nature (2020) 588:146–50. doi: 10.1038/s41586-020-2600-6
3. Holter JC, Pischke SE, de Boer E, Lind A, Jenum S, Holten AR, et al. Systemic Complement Activation is Associated With Respiratory Failure in COVID-19 Hospitalized Patients. Proc Natl Acad Sci USA (2020) 117:25018–25. doi: 10.1073/pnas.2010540117
4. Eriksson O, Hultström M, Persson B, Lipcsey M, Ekdahl KN, Nilsson B, et al. Mannose-Binding Lectin Is Associated With Thrombosis and Coagulopathy in Critically Ill COVID-19 Patients. Thromb Haemost (2020) 120:1720–4. doi: 10.1055/s-0040-1715835
5. Diurno F, Numis FG, Porta G, Cirillo F, Maddaluno S, Ragozzino A, et al. Eculizumab Treatment in Patients With COVID-19: Preliminary Results From Real Life ASL Napoli 2 Nord Experience. Eur Rev Med Pharmacol Sci (2020) 24:4040–7. doi: 10.26355/eurrev_202004_20875
6. Laurence J, Mulvey JJ, Seshadri M, Racanelli A, Harp J, Schenck EJ, et al. Anti-Complement C5 Therapy With Eculizumab in Three Cases of Critical COVID-19. Clin Immunol (2020) 219:108555. doi: 10.1016/j.clim.2020.108555
7. Peffault de Latour R, Bergeron A, Lengline E, Dupont T, Marchal A, Galicier L, et al. Complement C5 Inhibition in Patients With COVID-19 - A Promising Target? Haematologica (2020) 105:2847–50. doi: 10.3324/haematol.2020.260117
8. Annane D, Heming N, Grimaldi-Bensouda L, Frémeaux-Bacchi V, Vigan M, Roux A-L, et al. Eculizumab as an Emergency Treatment for Adult Patients With Severe COVID-19 in the Intensive Care Unit: A Proof-of-Concept Study. EClinicalMedicine (2020) 28:100590. doi: 10.1016/j.eclinm.2020.100590
9. Mastaglio S, Ruggeri A, Risitano AM, Angelillo P, Yancopoulou D, Mastellos DC, et al. The First Case of COVID-19 Treated With the Complement C3 Inhibitor AMY-101. Clin Immunol (2020) 215:108450. doi: 10.1016/j.clim.2020.108450
10. WHO. COVID-19 Therapeutic Trial Synopsis World Health Organisation. (2020). Novel Coronavirus. Available at: https://www.who.int/publications/i/item/covid-19-therapeutic-trial-synopsis [Accessed June 9, 2020].
11. Dumestre-Pérard C, Lamy B, Aldebert D, Lemaire-Vieille C, Grillot R, Brion J-P, et al. Aspergillus Conidia Activate the Complement by the Mannan-Binding Lectin C2 Bypass Mechanism. J Immunol (2008) 181:7100–5. doi: 10.4049/jimmunol.181.10.7100
12. Dumestre-Perard C, Ponard D, Arlaud GJ, Monnier N, Sim RB, Colomb MG. Evaluation and Clinical Interest of Mannan Binding Lectin Function in Human Plasma. Mol Immunol (2002) 39:465–73. doi: 10.1016/s0161-5890(02)00119-0
13. Dumestre-Perard C, Ponard D, Drouet C, Leroy V, Zarski J-P, Dutertre N, et al. Complement C4 Monitoring in the Follow-Up of Chronic Hepatitis C Treatment. Clin Exp Immunol (2002) 127:131–6. doi: 10.1046/j.1365-2249.2002.01729.x
14. Garred P, Madsen HO, Hofmann B, Svejgaard A. Increased Frequency of Homozygosity of Abnormal Mannan-Binding-Protein Alleles in Patients With Suspected Immunodeficiency. Lancet (1995) 346:941–3. doi: 10.1016/S0140-6736(95)91559-1
15. Kim AHJ, Wu X, Atkinson JP. The Beneficial and Pathogenic Roles of Complement in COVID-19. Cleve Clin J Med (2020) 88:1–4. doi: 10.3949/ccjm.87a.ccc065
16. de Nooijer AH, Grondman I, Janssen NAF, Netea MG, Willems L, van de Veerdonk FL, et al. RCI-COVID-19 Study Group. Complement Activation in the Disease Course of Coronavirus Disease 2019 and Its Effects on Clinical Outcomes. J Infect Dis (2021) 223:214–24. doi: 10.1093/infdis/jiaa646
17. Magro C, Mulvey JJ, Berlin D, Nuovo G, Salvatore S, Harp J, et al. Complement Associated Microvascular Injury and Thrombosis in the Pathogenesis of Severe COVID-19 Infection: A Report of Five Cases. Transl Res (2020) 220:1–13. doi: 10.1016/j.trsl.2020.04.007
18. Prendecki M, Clarke C, Medjeral-Thomas N, McAdoo SP, Sandhu E, Peters JE, et al. Temporal Changes in Complement Activation in Haemodialysis Patients With COVID-19 as a Predictor of Disease Progression. Clin Kidney J (2020) 13:889–96. doi: 10.1093/ckj/sfaa192
19. Macor P, Durigutto P, Mangogna A, Bussani R, D’Errico S, Zanon M, et al. Multi-Organ Complement Deposition in COVID-19 Patients. medRxiv (2021) 9:1–15. doi: 10.1101/2021.01.07.21249116
20. Satyam A, Tsokos MG, Brook OR, Hecht JL, Moulton VR, Tsokos GC. Activation of Classical and Alternative Complement Pathways in the Pathogenesis of Lung Injury in COVID-19. Clin Immunol (2021) 226:108716. doi: 10.1016/j.clim.2021.108716
21. Pfister F, Vonbrunn E, Ries T, Jäck H-M, Überla K, Lochnit G, et al. Complement Activation in Kidneys of Patients With COVID-19. Front Immunol (2020) 11:594849. doi: 10.3389/fimmu.2020.594849
22. Sinkovits G, Mező B, Réti M, Müller V, Iványi Z, Gál J, et al. Complement Overactivation and Consumption Predicts In-Hospital Mortality in SARS-CoV-2 Infection. Front Immunol (2021) 12:663187. doi: 10.3389/fimmu.2021.663187
23. Yu J, Yuan X, Chen H, Chaturvedi S, Braunstein EM, Brodsky RA. Direct Activation of the Alternative Complement Pathway by SARS-CoV-2 Spike Proteins is Blocked by Factor D Inhibition. Blood (2020) 136:2080–9. doi: 10.1182/blood.2020008248
24. Zhou Y, Lu K, Pfefferle S, Bertram S, Glowacka I, Drosten C, et al. A Single Asparagine-Linked Glycosylation Site of the Severe Acute Respiratory Syndrome Coronavirus Spike Glycoprotein Facilitates Inhibition by Mannose-Binding Lectin Through Multiple Mechanisms. J Virol (2010) 84:8753–64. doi: 10.1128/JVI.00554-10
25. Ip WKE, Chan KH, Law HKW, Tso GHW, Kong EKP, Wong WHS, et al. Mannose-Binding Lectin in Severe Acute Respiratory Syndrome Coronavirus Infection. J Infect Dis (2005) 191:1697–704. doi: 10.1086/429631
26. Ali YM, Ferrari M, Lynch NJ, Yaseen S, Dudler T, Gragerov S, et al. Lectin Pathway Mediates Complement Activation by SARS-CoV-2 Proteins. Front Immunol (2021) 12:2645–52. doi: 10.3389/fimmu.2021.714511
27. Ma L, Sahu SK, Cano M, Kuppuswamy V, Bajwa J, McPhatter J, et al. Increased Complement Activation is a Distinctive Feature of Severe SARS-CoV-2 Infection. Sci Immunol (2021) 6:1–18. doi: 10.1126/sciimmunol.abh2259
28. Gao T, Hu M, Zhang X, Li H, Zhu L, Dong Q, et al. Highly Pathogenic Coronavirus N Protein Aggravates Lung Injury by MASP-2-Mediated Complement Over-Activation. medRxiv [preprint]. doi: 10.1101/2020.03.29.20041962v3.
29. Fodil S, Annane D. Complement Inhibition and COVID-19: The Story So Far. Immunotargets Ther (2021) 10:273–84. doi: 10.2147/ITT.S284830
Keywords: COVID-19, complement, alternative pathway, MBL, lectin pathway
Citation: Defendi F, Leroy C, Epaulard O, Clavarino G, Vilotitch A, Le Marechal M, Jacob M-C, Raskovalova T, Pernollet M, Le Gouellec A, Bosson J-L, Poignard P, Roustit M, Thielens N, Dumestre-Pérard C and Cesbron J-Y (2021) Complement Alternative and Mannose-Binding Lectin Pathway Activation Is Associated With COVID-19 Mortality. Front. Immunol. 12:742446. doi: 10.3389/fimmu.2021.742446
Received: 16 July 2021; Accepted: 23 August 2021;
Published: 10 September 2021.
Edited by:
Zoltán Prohászka, Semmelweis University, HungaryReviewed by:
Lubka T. Roumenina, INSERM U1138 Centre de Recherche des Cordeliers (CRC), FranceMarten Trendelenburg, University Hospital of Basel, Switzerland
Copyright © 2021 Defendi, Leroy, Epaulard, Clavarino, Vilotitch, Le Marechal, Jacob, Raskovalova, Pernollet, Le Gouellec, Bosson, Poignard, Roustit, Thielens, Dumestre-Pérard and Cesbron. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Federica Defendi, ZmRlZmVuZGlAY2h1LWdyZW5vYmxlLmZy
†These authors have contributed equally to this work