
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol. , 30 April 2021
Sec. Alloimmunity and Transplantation
Volume 12 - 2021 | https://doi.org/10.3389/fimmu.2021.676756
This article is part of the Research Topic Managing Chronic GvHD in the Era of Personalized Medicine View all 8 articles
 Antonela Lelas1
Antonela Lelas1 Hildegard Theresia Greinix2
Hildegard Theresia Greinix2 Daniel Wolff3
Daniel Wolff3 Günther Eissner4
Günther Eissner4 Steven Zivko Pavletic5
Steven Zivko Pavletic5 Drazen Pulanic1,6*
Drazen Pulanic1,6*Chronic graft-versus-host disease (cGvHD) is an immune mediated late complication of allogeneic hematopoietic stem cell transplantation (alloHSCT). Discovery of adequate biomarkers could identify high-risk patients and provide an effective pre-emptive intervention or early modification of therapeutic strategy, thus reducing prevalence and severity of the disease among long-term survivors of alloHSCT. Inflammation, endothelial injury, and endothelial dysfunction are involved in cGvHD development. Altered levels of acute phase reactants have shown a strong correlation with the activity of several immune mediated disorders and are routinely used in clinical practice. Since elevated von Willebrand factor (VWF) and factor VIII (FVIII) levels have been described as acute phase reactants that may indicate endothelial dysfunction and inflammation in different settings, including chronic autoimmune diseases, they could serve as potential candidate biomarkers of cGvHD. In this review we focused on reported data regarding VWF and FVIII as well as other markers of inflammation and endothelial dysfunction, evaluating their potential role in cGvHD.
Chronic graft-versus-host disease (cGvHD) is an iatrogenic, immune mediated complication of allogeneic hematopoietic stem cell transplantation (alloHSCT) with clinical features resembling aspects of several autoimmune disorders. With its high incidence of approximately 50% (1) and mortality of approximately 25% (2), cGvHD is a major burden on quality of life and long-term survival following alloHSCT. Considering the fact that improvement of transplantation techniques allowed an increased number of patients to undergo alloHSCT and resulted in longer survival, the future incidence of cGvHD is expected to become even higher (1). Despite tremendous efforts of the scientific community put into research of cGvHD biology, a significant breakthrough in treatment strategies has not been achieved yet. One of the major obstacles for further progress is the absence of biomarkers suitable for clinical use. An ideal biomarker would be a specific agent that is active early in cGvHD development and that reliably identifies high-risk patients. This biomarker would allow developing of effective pre-emptive intervention, thus reducing incidence and severity of cGvHD. Furthermore, a specific marker that could provide earlier and more accurate initial assessment of disease intensity, or detect therapeutic response before improvement or worsening of clinical manifestations, could revolutionize the therapeutic approach. For all these reasons, along with the search for an effective treatment, the search for a biomarker that has satisfactory specificity and sensitivity has become one of the top priorities of researchers and clinicians (3, 4). However, the elusive etiology of cGvHD significantly hinders this search so far, especially when masked by multifarious impacts that can modulate course of illness. It is widely known that both inflammation and endothelial injury persist long after alloHSCT, and are involved in cGvHD development (5–8). Von Willebrand factor (VWF) and factor VIII (FVIII) are coagulation factors, as well as acute phase reactants indicating endothelial dysfunction and inflammation in different settings. Therefore, they could serve as potentially interesting candidate biomarkers of cGvHD. In this review we focused on reported data regarding VWF and FVIII, and other markers of inflammation and endothelial dysfunction, evaluating their potential role in cGvHD.
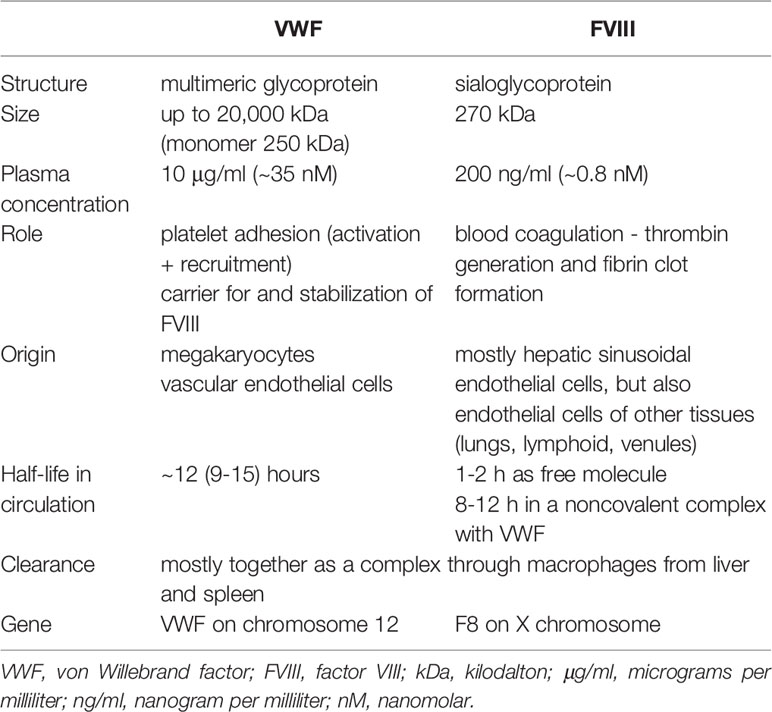
Von Willebrand factor and FVIII are widely known as coagulation factors that play an important role in hemostasis. Beside the critical role of VWF in “platelet plug” formation (bridging molecule for platelet adhesion and promoting platelet aggregation) at sites of vascular injury, it also serves as a carrier of FVIII, protecting it from proteolytic degradation and transporting it to sites of injury, thus enhancing fibrin formation (9). A detailed overview of VWF and FVIII physiology is shown in Table 1. In this review we will focus on the fact that both VWF and FVIII are considered positive acute phase reactants in settings of inflammation and endothelial activation (11).
Although synthesis regulation of VWF and FVIII is yet to be completely elucidated, it seems that different endothelial cells produce each of them, with an additional production of VWF by megakaryocytes. While most of VWF is synthesized in endothelium of larger extrahepatic vessels, FVIII is synthesized mostly in hepatic sinusoidal endothelial cells. Interestingly, murine models have shown predominant distribution of VWF mRNA in lung and brain, indicating that VWF is differently expressed in different tissues (12). It should be emphasized that VWF and FVIII are the only coagulation factors that are not being produced by liver hepatocytes. Upon synthesis VWF is stored in specialized organelles; in smaller quantities as α granules of platelets, but mostly as Weibel-Palade bodies in vascular endothelial cells. Since endothelium represents the first line of defense from noxious stimuli, its activation caused by vascular injury of any etiology, results in secretion of VWF from Weibel-Palade bodies into the plasma. Secretion can be provoked by different inflammatory mediators released from resident immune cells, mostly tissue macrophages (13), and it results not only in direct adhesive interaction of VWF with leukocytes and trans-endothelial migration (14), but also in stimulation of other proinflammatory pathways such as complement and neutrophil extracellular traps (15). Moreover, proinflammatory agents, such as P-selectin are also released from Weibel-Palade bodies (16) further supporting the inflammatory response.
While VWF is well-recognized as the carrier of FVIII in plasma and protector of its degradation, the possible impact of FVIII on VWF plasma levels is poorly resolved. Some studies described a synergistic role of FVIII and platelets on the cleavage of VWF multimers by a disintegrin and metalloproteinase with ADAMTS13 (a thrombospondin type 1 motif, member 13) (17), while study with FVIII deficient mouse model revealed increased VWF content in the liver endothelium and increased VWF plasma levels, which was associated with hepatic low-grade inflammation (18).
The clinical utility of VWF and FVIII as biomarkers has been questioned due to a possible influence by many extrinsic patient related parameters, such as age, body weight, ABO antigen status, diet, smoking, ethnicity, and even exercise (10, 19–21). However, possible benefits of such a relatively cost-effective and non-invasive diagnostic tool encouraged extensive research in the field of cardiovascular diseases, resulting in clear distinction of patients at risk for major adverse cardiovascular events (22–24). Significant elevation of both biomarkers has been described in different states of acute stress, and lately a lot of attention has been given to the investigation of their role in connection between inflammation and procoagulant state caused by coronavirus 2019 (SARS-CoV-2) infection (25, 26). Elevation of VWF and FVIII was also reported in many long-lasting clinical conditions, including chronic autoimmune rheumatic diseases, pregnancy, malignancy, hyperthyroidism, hyperglycemia, hypertriglyceridemia, liver and renal disease (19, 27, 28). All these findings directed current research of VWF and FVIII toward elucidation of association between hemostasis, thrombosis, endothelial injury, and inflammation in a process jointly named as “thromboinflammation”. Although increase of these coagulation factors has been described in many vasculopathies and other states of hypoxia, this review mainly focusses on autoimmune diseases that clinically resemble cGvHD. Available knowledge of biomarker utility in different settings regarding VWF is summarized in Table 2, while one regarding FVIII is shown in Table 3. It is interesting to note that both VWF and FVIII level increase correlates with activity of autoimmune connective tissue diseases. In systemic sclerosis and systemic lupus erythematosus it has shown to be predictive of pulmonary involvement (31), which can be connected to localized endothelial synthesis of these factors. Pathogenesis of both of these diseases includes inflammation and microvascular changes that lead to hypoxia and, consequently, fibrosis which is similar as in cGvHD. From these studies it can be concluded that inflammation caused by autoimmune disease is a consequence of endothelial injury. However, a detailed analysis of the biomarker potential regarding VWF and FVIII, including their sensitivity and specificity, has not been performed yet.
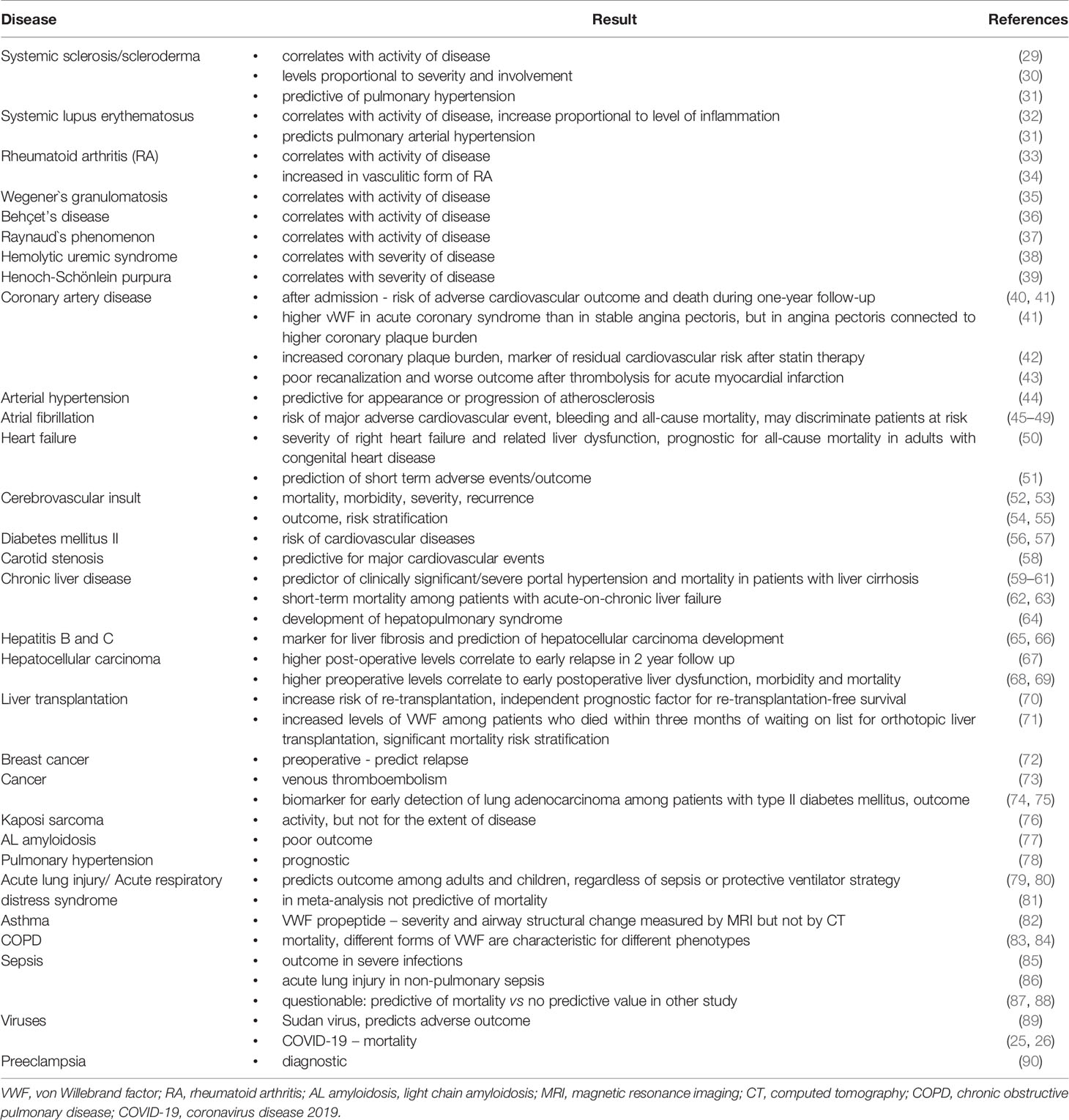
Table 2 Reported biomarker potential of elevated VWF levels in different diseases/conditions.
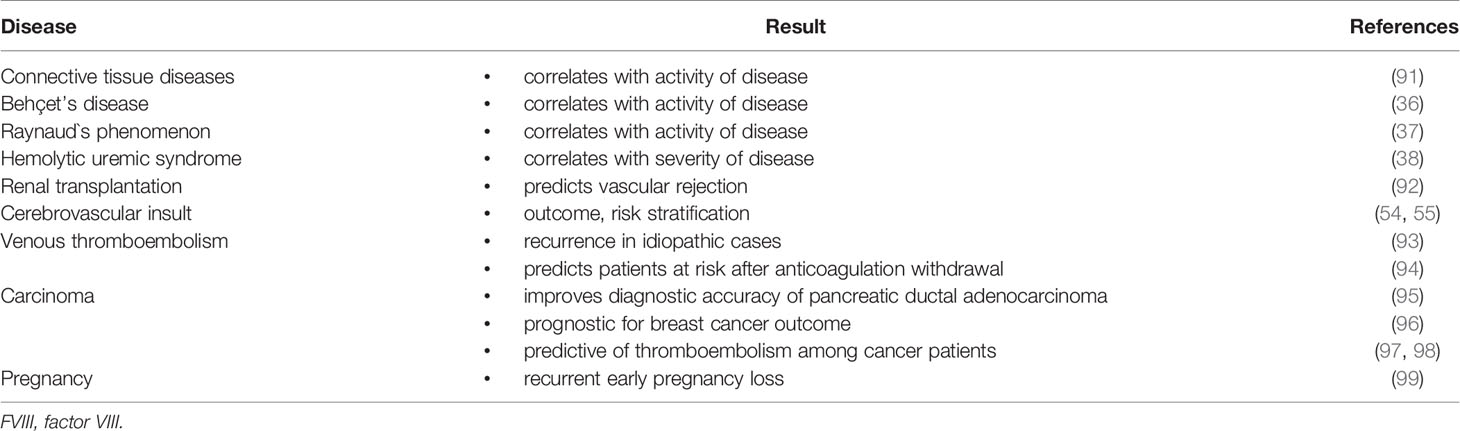
Table 3 Reported biomarker potential of elevated FVIII levels in different diseases/conditions.
Despite the fact that increase of VWF and FVIII can also be caused by hematologic malignancies (100, 101), chemotherapy or autologous HSCT, their levels following alloHSCT are significantly more prominent (102, 103). It is considered that such increase in a post-alloHSCT setting reflects endothelial injury in addition to acute phase reaction. Endothelium is the first-line barrier against various transplant related toxic effects including cytostatic therapy, radiation, immunosuppression, and alloreactivity. Increase of VWF has already shown prognostic value for acute GvHD (aGvHD) development (104). Moreover, it has been reported that elevated levels of VWF and FVIII among patients diagnosed with aGvHD strongly correlate with endothelial activation but their role in aGvHD biology has not yet been defined (102, 105–108). Such findings suggest that the endothelium has a pathophysiological role in aGvHD development which goes beyond cytokine-mediated cell-to-cell communication. Interestingly, an increase of VWF level was proposed as a diagnostic marker of cGvHD among alloHSCT long-term survivors also (108), with its potential utility as sensitive biomarker of cGvHD activity (109). These reports, though, had a limited number of subjects and lacking methodology. However, recent preliminary results of a prospective study on a well-defined cohort of alloHSCT patients conducted by Pulanic at al. showed significantly higher levels of VWF and FVIII in the cGvHD group in comparison to patients who did not develop cGvHD (110). Further analysis revealed a close association between cGvHD activity and elevated levels of VWF, suggesting a potential causal relationship. It should also be noticed that thromboembolic events, including venous thromboembolism, have been associated with presence of both acute and chronic GvHD even 50 months after alloHSCT (111). Such observations could suggest a potential role of inflammation induced increase of coagulation factors FVIII and VWF in the pathogenesis of these events. Additionally, elevated levels of VWF were described as predictive of poor outcome for some vascular endothelial syndromes such as transplant-associated thrombotic microangiopathy (112, 113), and FVIII seems to be involved in the pathophysiology of sinusoidal obstruction syndrome/veno-occlusive disease (SOS/VOD) after alloHSCT (114). The prognostic role of FVIII and VWF plasma levels in SOS/VOD has been investigated, but the results were too ambiguous for clinical use (115).
The term acute-phase reactants (APRs) relates to all markers whose measured plasma concentrations increase or decrease by at least 25% during inflammation or tissue injury (116). Most of APRs are proteins produced by the liver. Their production is regulated by cytokines like interleukin-2 (IL-2), tumor necrosis factor alpha (TNF-α) and interferon gamma (IFNγ) which are being produced by immune cells during the inflammation process. As already mentioned earlier, inflammation and endothelial injury are closely connected. Also, both processes have been described in the cGvHD setting, although less extensively studied than in aGVHD. The most comprehensive study addressing inflammation in cGvHD was performed by Grkovic and NCI group who investigated clinical laboratory markers of inflammation as determinants of cGvHD activity and severity (6). The authors proposed that reactive thrombocytosis, mediated by interleukin-6 (IL-6), might contribute to the pathogenesis of transforming growth factor beta (TGF-β) and platelet-derived growth factor (PDGF)-induced fibrosis and vascular thickening. Namely, though thrombocytopenia measured at time of diagnosis of cGvHD is among the strongest predictors of poor survival across many studies (117), this study has shown an association of increased platelets with cGvHD activity and with more severe skin and joint/fascia cGvHD involvement over a longer follow-up period after cGvHD presentation (6). This is in line with other studies identifying platelets as key regulators of the inflammatory response (118). In addition to that, strong association of low platelet counts at time of diagnosis of cGvHD and poor survival could be partly due to development of microangiopathic hemolytic anemia (defined by appearance of schistocytes in peripheral blood smears and thrombocytopenia) in some cases, and impaired splenic function may cause thrombocytopenia in others (117).
Endothelial injury caused by inflammation, on the other hand, has not been extensively studied in cGvHD so far. However, an increase of vascular inflammation markers, such as endothelin-1, gelsolin, and anti-LG3 (autoantibodies against perlecan/LG3), was observed, confirming thus important role of endothelial injury and inflammation in the onset of cGvHD (119). Of note, endothelial injury is usually characterized by induction of proinflammatory cytokines (TNF-α, IL-6, IL-10, IL-1β, etc.) and by decreased levels of anti-inflammatory cytokines (TGF-β, IL-15), increased release of coagulation factors (VWF and FVIII), and overexpression of soluble and membrane-bound adhesion molecules (ICAM-1 (intercellular adhesion molecule 1), VCAM-1 (vascular cell adhesion protein 1), E-selectin) (120, 121). Interestingly, in contrast to multitude reports in aGvHD, there is no cGvHD data available even on basic hemostatic APRs, such as fibrinogen, D-dimer, thrombomodulin, and plasminogen activator inhibitor (PAI-1), a well-known marker of endothelial damage in SOS/VOD. Moreover, although inadequate activation of natural anticoagulants has been reported among patients following HSCT (107), no studies with longer follow-ups, describing changes among cGvHD patients in particular, were found. Aside from hemostatic APRs, great progress in omnics technique resulted in a number of novel potential cGvHD biomarkers, further reflecting the complex biology of cGvHD. For example, an interesting study with a panel of four markers (C-X-C motif chemokine ligand 9 (CXCL9), suppression of tumorigenicity 2 (ST2), osteopontin (OPN) and matrix metalloproteinase-3 (MMP3) measured 100 days after alloHSCT showed predictability for cGvHD development (122). The most important APRs and markers of endothelial dysfunction that have been investigated as potential cGvHD biomarkers are summarized in Table 4. However, it has to be stated that there is lack of standardized methods to separate inflammation in general from endothelial injury.
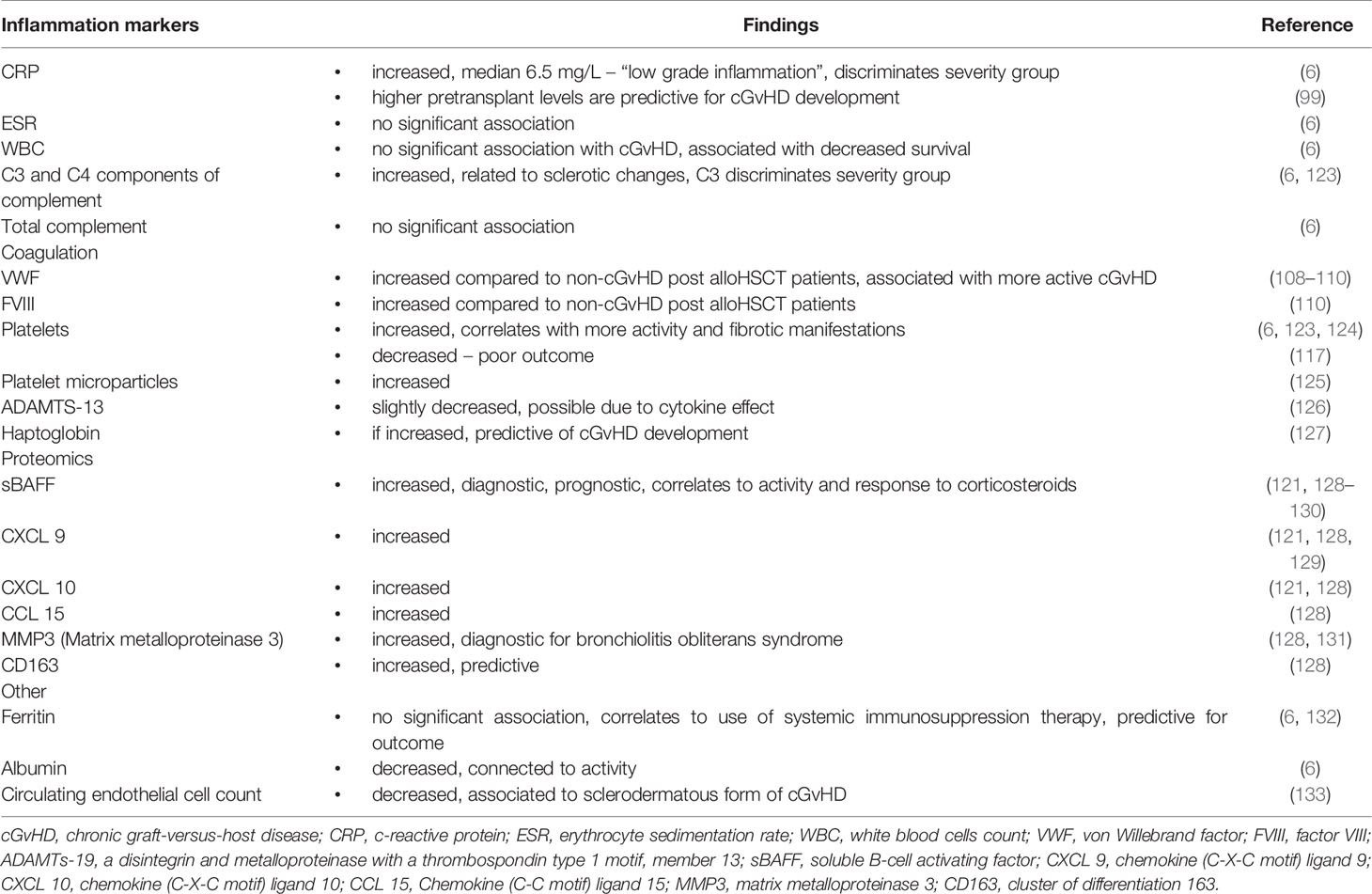
Table 4 Acute phase reactants and markers of endothelial dysfunction in cGvHD.
Elucidation of immunological processes in the recovery period following alloHSCT remains challenging, especially in context of aGvHD and cGvHD. It is well established that endothelial activation and injury enhance the occurrence of aGvHD (134). Furthermore, an increasing number of scientists advocate the existence of an endothelial form of GvHD (135). Pioneers of this thinking, Tichelli and Gratwohl, supported the hypothesis of the vascular endothelium as a target of GvHD-mediated immune responses, which were previously described by Biedermann and colleagues (108). In addition, there is also in vitro evidence that some of the endothelium targeting immunological effector cells are in fact endothelial-, not just allo-specific (136, 137). Moreover, Tichelli and Gratwohl proposed that vascular endothelial syndromes should be considered as different forms of aGvHD which are reflected by organ-related injury. Another support to this opinion was given by connecting endothelial damage to steroid-refractory aGvHD (138). More recently publications demonstrate a reduction of aGvHD severity by experimentally using the endothelium-protecting agents sildenafil and defibrotide (139–141). Of note, defibrotide can also reduce the allogenicity of endothelial cells towards CD8+ T cells (142).
As for cGvHD, although it is characterized by impaired immune tolerance mechanisms affecting innate and adaptive immunity, elevated levels of inflammation and endothelial injury are also present, albeit less well elaborated so far (6, 108). Although the role of endothelial injury in cGvHD biology is not fully elucidated yet, it is clear that disease activity correlates with activation of the endothelium. Such activation cannot be attributed to acute conditioning toxicity or engraftment, considering the long period of time passing between these events and cGvHD diagnosis. Taking into consideration the proportional increase of VWF in relation to cGvHD activity and severity, the most probable reason for endothelial activation must be immune-related mechanisms. It was proposed earlier that endothelial cells of small vessels can act as antigen presenting cells (APC), even in the absence of professional APC (143). Activated endothelial cells (EC) show increased surface histocompatibility antigens and co-stimulatory molecules, rendering them more susceptible to a direct immune attack by alloreactive donor T cells. The resulting EC activation and injury can facilitate the passage of donor-derived cellular and soluble effectors from the blood and into recipient tissues (5). Biedermann et al. described infiltration of alloreactive cytotoxic T lymphocytes in the upper dermis of cGvHD patient with sclerotic form of skin involvement and subsequent rarefaction of small vessels, which argues in favor of this observation (108). Moreover, it has been suggested that neovascularization inhibition supported by activated donor T cells may contribute to a graft-versus-leukemia (GvL) effect, which can explain the protective role of active GvHD in prevention of tumor relapse (144). Another investigation showed partial reconstitution of microvessels among long-term survivors after alloHSCT (median follow-up was 17 years in this study), with complete recovery of microvascular remodeling after resolution of skin cGvHD (145). In an interesting study performed by Willemze et al. percentage of EC chimerism was higher when measured over a longer period of time after alloHSCT (146). It can be concluded that microvascular loss and resultant tissue ischemia may contribute to target organ fibrosis characteristic of cGvHD and that the effect may be reversible if treated on time, pointing to a possible role for donor derived EC in repair of damaged blood vessels. Tichelli and Gratwohl additionally suggested a causative link between inflammation, endothelial injury and the increased risk of cardiovascular diseases reported among long-term alloHSCT survivors. They actually used a simple and logical explanation, connecting an accelerated atherosclerosis to endothelial injury which is caused by persistent vascular inflammation and provoked by immunological mechanisms of cGvHD (135). Considering all the facts, endothelium-protecting agents could significantly diminish this vicious circle of chronic inflammation, endothelial damage, and ischemia, and for their possible beneficial effect, low side-effect profile and preservation of GVL effect, their usage should definitely be taken into consideration for future treatment strategies in cGvHD. However, there are some limitations of this concept: there is lack of markers that differentiate between endothelial damage and acute phase reaction well, as well as lack of drugs that are endothelial protective and that are tested in sufficiently large studies to prove that endothelial protection is a goal that can be achieved.
To conclude, in search for much needed biomarkers of cGvHD for clinical use, this review draws attention to acute phase reactants that may be associated with cGvHD activity and severity of cGvHD organ involvement. As non-invasive, readily available, and cost-efficient markers of endothelial activation, VWF and FVIII could provide valuable insight into cGvHD activity. Their elevation has a promising biomarker potential for an early diagnosis and as surrogate for activity of the disease. This concept is further underpinned by their proven good prognostic value in chronic autoimmune diseases clinically resembling cGvHD. In addition to the aforementioned factors it may also be helpful to assess endothelium-derived microvesicles for endothelial injury and procoagulant activity (147). Still, the influence of patient-related parameters should definitely be taken into consideration, and for that reason further prospective studies addressing this issue and the precise role of endothelial injury in cGvHD in general are needed.
AL: drafting of the manuscript, acquisition and interpretation of data. HG: interpretation of data, critical revision of the manuscript for important intellectual content. DW: interpretation of data, critical revision of the manuscript for important intellectual content. GE: interpretation of data, critical revision of the manuscript for important intellectual content. SP: interpretation of data, critical revision of the manuscript for important intellectual content. DP: designed and coordinated the preparation of the manuscript, interpretation of data, critical revision of the manuscript for important intellectual content. All authors contributed to the article and approved the submitted version.
This work was supported by European Cooperation in Science & Technology under the COST Action CA17138 (Integrated European Network on Chronic Graft Versus Host Disease) and by the Croatian Science Foundation Project IP-2016-06-8046 entitled “New biomarkers for chronic Graft-versus-Host disease”.
The opinions expressed here are those of the authors and do not represent the official position of the National Institutes of Health or the US Government.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Arai S, Arora M, Wang T, Spellman SR, He W, Couriel DR, et al. Increasing Incidence of Chronic Graft-Versus-Host Disease in Allogeneic Transplantation: A Report From the Center for International Blood and Marrow Transplant Research. Biol Blood Marrow Transplant (2015) 21(2):266–74. doi: 10.1016/j.bbmt.2014.10.021
2. Grube M, Holler E, Weber D, Holler B, Herr W, Wolff D. Risk Factors and Outcome of Chronic Graft-Versus-Host Disease After Allogeneic Stem Cell Transplantation—Results From a Single-Center Observational Study. Biol Blood Marrow Transplant (2016) 22(10):1781–91. doi: 10.1016/j.bbmt.2016.06.020
3. Wolff D, Greinix H, Lee SJ, Gooley T, Paczesny S, Pavletic S, et al. Biomarkers in Chronic Graft-Versus-Host Disease: Quo Vadis? Bone Marrow Transplant (2018) Jul 153(7):832–7. doi: 10.1038/s41409-018-0092-x
4. Paczesny S, Hakim FT, Pidala J, Cooke KR, Lathrop J, Griffith LM, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-Versus-Host Disease: III. The 2014 Biomarker Working Group Report. Biol Blood Marrow Transplant (2015) 21(5):780–92. doi: 10.1016/j.bbmt.2015.01.003
5. Cooke KR, Luznik L, Sarantopoulos S, Hakim FT, Jagasia M, Fowler DH, et al. The Biology of Chronic Graft-versus-Host Disease: A Task Force Report From the National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-Versus-Host Disease. Biol Blood Marrow Transplant (2017) 23(2):211–34. doi: 10.1016/j.bbmt.2016.09.023
6. Grkovic L, Baird K, Steinberg SM, Williams KM, Pulanic D, Cowen EW, et al. Clinical Laboratory Markers of Inflammation as Determinants of Chronic Graft-Versus-Host Disease Activity and NIH Global Severity. Leukemia (2012) 26(4):633–43. doi: 10.1038/leu.2011.254
7. Penack O, Luft T. Editorial: Endothelial Dysfunction During Inflammation and Alloimmunity. Front Immunol (2018) 9:2886. doi: 10.3389/fimmu.2018.02886
8. Medinger M, Tichelli A, Bucher C, Halter J, Dirnhofer S, Rovo A, et al. GVHD After Allogeneic Haematopoietic SCT for AML: Angiogenesis, Vascular Endothelial Growth Factor and VEGF Receptor Expression in the BM. Bone Marrow Transplant (2013) 48(5):715–21. doi: 10.1038/bmt.2012.200
9. Pipe SW, Montgomery RR, Pratt KP, Lenting PJ, Lillicrap D. Life in the Shadow of a Dominant Partner: The FVIII-VWF Association and its Clinical Implications for Hemophilia a. Blood Am Soc Hematol (2016) 128:2007–16. doi: 10.1182/blood-2016-04-713289
10. Terraube V, O’Donnell JS, Jenkins PV. Factor VIII and Von Willebrand Factor Interaction: Biological, Clinical and Therapeutic Importance. Haemophilia (2010) 16:3–13. doi: 10.1111/j.1365-2516.2009.02005.x
11. Kawecki C, Lenting PJ, Denis CV. Von Willebrand Factor and Inflammation. J Thromb Haemost (2017) 15(7):1285–94. doi: 10.1111/jth.13696
12. Yamamoto K, de Waard V, Fearns C, Loskutoff DJ. Tissue Distribution and Regulation of Murine Von Willebrand Factor Gene Expression In Vivo. Blood (1998) 92(8):2791–801. doi: 10.1182/blood.V92.8.2791.420k24_2791_2801
13. Chen J, Chung DW. Inflammation, Von Willebrand Factor, and ADAMTS13. Blood (2018) 132(2):141–7. doi: 10.1182/blood-2018-02-769000
14. Petri B, Broermann A, Li H, Khandoga AG, Zarbock A, Krombach F, et al. Von Willebrand Factor Promotes Leukocyte Extravasation. Blood (2010) 116(22):4712–9. doi: 10.1182/blood-2010-03-276311
15. Gragnano F, Sperlongano S, Golia E, Natale F, Bianchi R, Crisci M, et al. The Role of Von Willebrand Factor in Vascular Inflammation: From Pathogenesis to Targeted Therapy. Mediators Inflamm (2017) 2017:5620314. doi: 10.1155/2017/5620314
16. Pendu R, Terraube V, Christophe OD, Gahmberg CG, De Groot PG, Lenting PJ, et al. P-Selectin Glycoprotein Ligand 1 and β2-Integrins Cooperate in the Adhesion of Leukocytes to Von Willebrand Factor. Blood (2006) 108(12):3746–52. doi: 10.1182/blood-2006-03-010322
17. Skipwith CG, Cao W, Zheng XL. Factor VIII and Platelets Synergistically Accelerate Cleavage of Von Willebrand Factor by ADAMTS13 Under Fluid Shear Stress. J Biol Chem (2010) 285:28596–603. doi: 10.1074/jbc.M110.131227
18. Kiouptsi K, Grill A, Mann A, Döhrmann M, Lillich M, Jäckel S, et al. Mice Deficient in the Anti-Haemophilic Coagulation Factor VIII Show Increased Von Willebrand Factor Plasma Levels. PLoS One (2017) 12(8):e0183590. doi: 10.1371/journal.pone.0183590
19. Conlan MG, Folsom AR, Finch A, Davis CE, Sorlie P, Marcucci G, et al. Associations of Factor VIII and Von Willebrand Factor With Age, Race, Sex, and Risk Factors for Atherosclerosis: The Atherosclerosis Risk in Communities (ARIC) Study. Thromb Haemost (1993) 70(3):380–5. doi: 10.1055/s-0038-1649589
20. Ingerslev J. A Sensitive ELISA for Von Willebrand Factor (Vwf:Ag). Scand J Clin Lab Invest (1987) 47(2):143–9. doi: 10.3109/00365518709168882
21. Cohen RJ, Epstein SE, Cohen LS, Dennis LH. Alterations of Fibrinolysis and Blood Coagulation Induced by Exercise, and the Role of Beta-Adrenergic-Receptor Stimulation. Lancet (1968) 2(7581):1264–6. doi: 10.1016/S0140-6736(68)91760-1
22. Alonso A, Tang W, Agarwal SK, Soliman EZ, Chamberlain AM, Folsom AR. Hemostatic Markers are Associated With the Risk and Prognosis of Atrial Fibrillation: The ARIC Study. Int J Cardiol (2012) 155(2):217–22. doi: 10.1016/j.ijcard.2010.09.051
23. Sonneveld MAH, Franco OH, Ikram MA, Hofman A, Kavousi M, De Maat MPM, et al. Von Willebrand Factor, ADAMTS13, and the Risk of Mortality: The Rotterdam Study. Arterioscler Thromb Vasc Biol (2016) 36(12):2446–51. doi: 10.1161/ATVBAHA.116.308225
24. Folsom AR, Rosamond WD, Shahar E, Cooper LS, Aleksic N, Nieto FJ, et al. Prospective Study of Markers of Hemostatic Function With Risk of Ischemic Stroke. Circulation (1999) 100(7):736–42. doi: 10.1161/01.CIR.100.7.736
25. Ladikou EE, Sivaloganathan H, Milne KM, Arter WE, Ramasamy R, Saad R, et al. Von Willebrand Factor (vWF): Marker of Endothelial Damage and Thrombotic Risk in COVID-19? Clin Med (2020) 20(5):e178–82. doi: 10.7861/clinmed.2020-0346
26. Goshua G, Pine AB, Meizlish ML, Chang CH, Zhang H, Bahel P, et al. Endotheliopathy in COVID-19-associated Coagulopathy: Evidence From a Single-Centre, Cross-Sectional Study. Lancet Haematol (2020) 7(8):e575–82. doi: 10.1016/S2352-3026(20)30216-7
27. Habe K, Wada H, Matsumoto T, Ohishi K, Ikejiri M, Tsuda K, et al. Plasma ADAMTS13, Von Willebrand Factor (VWF), and VWF Propeptide Profiles in Patients With Connective Tissue Diseases and Antiphospholipid Syndrome. Clin Appl Thromb (2017) 23(6):622–30. doi: 10.1177/1076029615625832
28. Danesh J, Wheeler JG, Hirschfield GM, Eda S, Eiriksdottir G, Rumley A, et al. C-Reactive Protein and Other Circulating Markers of Inflammation in the Prediction of Coronary Heart Disease. N Engl J Med (2004) 350(14):1387–97. doi: 10.1056/NEJMoa032804
29. Scheja A, Åkesson A, Geborek P, Wildt M, Wollheim CB, Wollheim FA, et al. Von Willebrand Factor Propeptide as a Marker of Disease Activity in Systemic Sclerosis (Scleroderma). Arthritis Res (2001) 3(3):178–82. doi: 10.1186/ar295
30. Herrick AL, Illingworth K, Blann A, Hay CRM, Hollis S, Jayson MIV. Von Willebrand Factor, Thrombomodulin, Thromboxane, β-Thromboglobulin and Markers of Fibrinolysis in Primary Raynaud’s Phenomenon and Systemic Sclerosis. Ann Rheum Dis (1996) 55(2):122–7. doi: 10.1136/ard.55.2.122
31. Barnes T, Gliddon A, Doré CJ, Maddison P, Moots RJ. Baseline vWF Factor Predicts the Development of Elevated Pulmonary Artery Pressure in Systemic Sclerosis. Rheumatology (United Kingdom) (2012) 51(9):1606–9. doi: 10.1093/rheumatology/kes068
32. Nossent JC, Raymond WD, Eilertsen GØ. Increased Von Willebrand Factor Levels in Patients With Systemic Lupus Erythematosus Reflect Inflammation Rather Than Increased Propensity for Platelet Activation. Lupus Sci Med (2016) 3(1):e000162. doi: 10.1136/lupus-2016-000162
33. Gürol G, Ciftci IH, Harman H, Karakece E, Kamanli A, Tekeoglu I. Roles of Claudin-5 and Von Willebrand Factor in Patients With Rheumatoid Arthritis. Int J Clin Exp Pathol (2015) 8(2):1979–84.
34. Lau CS, McLaren M, Hanslip J, Kerr M, Belch JJF. Abnormal Plasma Fibrinolysis in Patients With Rheumatoid Arthritis and Impaired Endothelial Fibrinolytic Response in Those Complicated by Vasculitis. Ann Rheum Dis (1993) 52(9):643–9. doi: 10.1136/ard.52.9.643
35. D’Cruz D, Direskeneli H, Khamashta M, Hughes GRV. Lymphocyte Activation Markers and Von Willebrand Factor Antigen in Wegener’s Granulomatosis: Potential Markers for Disease Activity. J Rheumatol (1999) 26(1):103–9.
36. Alkaabi JK, Gravell D, Al-Haddabi H, Pathare A. Haemostatic Parameters in Patients With Behçet’s Disease. Sultan Qaboos Univ Med J (2014) 14(2):e190–6.
37. Lau CS, Mclaren M, Belch JJF. Factor VIII Von Willebrand Factor Antigen Levels Correlate With Symptom Severity in Patients With Raynaud’s Phenomenon. Rheumatology (1991) 30(6):433–6. doi: 10.1093/rheumatology/30.6.433
38. Rose PE, Kavi J, Chant I, Taylor CM, Struthers GS, Robertson M. Factor VIII Von Willebrand Protein in Haemolytic Uraemic Syndrome and Systemic Vasculitides. Lancet (1990) 335(8688):500–2. doi: 10.1016/0140-6736(90)90736-O
39. De Mattia D, Penza R, Giordano P, Del Vecchio GC, Aceto G, Altomare M, et al. Von Willebrand Factor and Factor XIII in Children With Henoch-Schonlein Purpura. Pediatr Nephrol (1995) 9(5):603–5. doi: 10.1007/BF00860949
40. Fan M, Wang X, Peng X, Feng S, Zhao J, Liao L, et al. Prognostic Value of Plasma Von Willebrand Factor Levels in Major Adverse Cardiovascular Events: A Systematic Review and Meta-Analysis. BMC Cardiovasc Disord (2020) 20. doi: 10.1186/s12872-020-01375-7
41. Sonneveld MAH, Cheng JM, Oemrawsingh RM, de Maat MPM, Kardys I, Garcia-Garcia HM, et al. Von Willebrand Factor in Relation to Coronary Plaque Characteristics and Cardiovascular Outcome Results of the Atheroremo-Ivus Study. Thromb Haemost (2014) 113(3):577–84. doi: 10.1160/TH14-07-0589
42. Kato Y, Iwata A, Futami M, Yamashita M, Imaizumi S, Kuwano T, et al. Impact of Von Willebrand Factor on Coronary Plaque Burden in Coronary Artery Disease Patients Treated With Statins. Medicine (United States) (2018) 97(17):e0589. doi: 10.1097/MD.0000000000010589
43. Lip GYH, Lydakis C, Nuttall SL, Landray MJ, Watson RDS, Blann AD. A Pilot Study of Streptokinase-Induced Endothelial Injury and Platelet Activation Following Acute Myocardial Infarction. J Intern Med (2000) 248(4):316–8. doi: 10.1046/j.1365-2796.2000.00738.x
44. Blann AD, Waite MA. Von Willebrand Factor and Soluble E-selectin in Hypertension: Influence of Treatment and Value in Predicting the Progression of Atherosclerosis. Coron Artery Dis (1996) 7(2):143–7. doi: 10.1097/00019501-199602000-00008
45. Zhong C, Xin M, He L, Sun G, Shen F. Prognostic Value of Von Willebrand Factor in Patients With Atrial Fibrillation. Medicine (United States) (2018) 97:e11269. doi: 10.1097/MD.0000000000011269
46. Krishnamoorthy S, Khoo CW, Lim HS, Lane DA, Pignatelli P, Basili S, et al. Prognostic Role of Plasma Von Willebrand Factor and Soluble E-selectin Levels for Future Cardiovascular Events in a “Real-World” Community Cohort of Patients With Atrial Fibrillation. Eur J Clin Invest (2013) 43(10):1032–8. doi: 10.1111/eci.12140
47. Freynhofer MK, Gruber SC, Bruno V, Höchtl T, Farhan S, Zaller V, et al. Prognostic Value of Plasma Von Willebrand Factor and its Cleaving Protease ADAMTS13 in Patients With Atrial Fibrillation. Int J Cardiol (2013) 168(1):317–25. doi: 10.1016/j.ijcard.2012.09.056
48. Ye YZ, Chang YF, Wang BZ, Ma YT, Ma X. Prognostic Value of Von Willebrand Factor for Patients With Atrial Fibrillation: A Meta-Analysis of Prospective Cohort Studies. Postgrad Med J (2020) 96:267–76. doi: 10.1136/postgradmedj-2019-136842
49. Ancedy Y, Berthelot E, Lang S, Ederhy S, Boyer-Chatenet L, Di Angelantonio E, et al. Is Von Willebrand Factor Associated With Stroke and Death At Mid-Term in Patients With non-Valvular Atrial Fibrillation? Arch Cardiovasc Dis (2018) 111(5):357–69. doi: 10.1016/j.acvd.2017.08.004
50. Ohuchi H, Hayama Y, Miike H, Suzuki D, Nakajima K, Iwasa T, et al. Prognostic Value of Von Willebrand Factor in Adult Patients With Congenital Heart Disease. Heart (2020) 106(12):910–5. doi: 10.1136/heartjnl-2019-316007
51. Gombos T, Makó V, Cervenak L, Papassotiriou J, Kunde J, Hársfalvi J, et al. Levels of Von Willebrand Factor Antigen and Von Willebrand Factor Cleaving Protease (ADAMTS13) Activity Predict Clinical Events in Chronic Heart Failure. Thromb Haemost (2009) 102(3):573–80. doi: 10.1160/TH09-01-0036
52. Catto AJ, Carter AM, Barrett JH, Bamford J, Rice PJ, Grant PJ. Von Willebrand Factor and Factor VIII:C in Acute Cerebrovascular Disease. Relationship to Stroke, Subtype and Mortality. Thromb Haemost (1997) 77(6):1104–8. doi: 10.1055/s-0038-1656120
53. Buchtele N, Schwameis M, Gilbert JC, Schörgenhofer C, Jilma B. Targeting Von Willebrand Factor in Ischaemic Stroke: Focus on Clinical Evidence. Thromb Haemost (2018) 118:959–78. doi: 10.1055/s-0038-1648251
54. Samai A, Monlezun D, Shaban A, George A, Dowell L, Kruse-Jarres R, et al. Von Willebrand Factor Drives the Association Between Elevated Factor VIII and Poor Outcomes in Patients With Ischemic Stroke. Stroke (2014) 45(9):2789–91. doi: 10.1161/STROKEAHA.114.006394
55. Tóth NK, Székely EG, Czuriga-Kovács KR, Sarkady F, Nagy O, Lánczi LI, et al. Elevated Factor VIII and Von Willebrand Factor Levels Predict Unfavorable Outcome in Stroke Patients Treated With Intravenous Thrombolysis. Front Neurol (2018) 8(JAN):721. doi: 10.3389/fneur.2017.00721
56. Frankel DS, Meigs JB, Massaro JM, Wilson PWF, O’Donnell CJ, D’Agostino RB, et al. Von Willebrand Factor, Type 2 Diabetes Mellitus, and Risk of Cardiovascular Disease: The Framingham Offspring Study. Circulation (2008) 118(24):2533–9. doi: 10.1161/CIRCULATIONAHA.108.792986
57. Peng X, Wang X, Fan M, Zhao J, Lin L, Liu J. Plasma Levels of Von Willebrand Factor in Type 2 Diabetes Patients With and Without Cardiovascular Diseases: A Meta-Analysis. Diabetes Metab Res Rev (2020) 36:e3193. doi: 10.1002/dmrr.3193
58. Kovacevic KD, Mayer FJ, Jilma B, Buchtele N, Obermayer G, Binder CJ, et al. Von Willebrand Factor Antigen Levels Predict Major Adverse Cardiovascular Events in Patients With Carotid Stenosis of the ICARAS Study. Atherosclerosis (2019) 290:31–6. doi: 10.1016/j.atherosclerosis.2019.09.003
59. Ferlitsch M, Reiberger T, Hoke M, Salzl P, Schwengerer B, Ulbrich G, et al. Von Willebrand Factor as New Noninvasive Predictor of Portal Hypertension, Decompensation and Mortality in Patients With Liver Cirrhosis. Hepatology (2012) 56(4):1439–47. doi: 10.1002/hep.25806
60. Zou Z, Yan X, Li C, Li X, Ma X, Zhang C, et al. Von Willebrand Factor as a Biomarker of Clinically Significant Portal Hypertension and Severe Portal Hypertension: A Systematic Review and Meta-Analysis. BMJ Open (2019) 9:e025656. doi: 10.1136/bmjopen-2018-025656
61. Ding X-C, Ma W-L, Li M-K, Liu S-W, Liu X-Y, Hai L, et al. A Meta-Analysis of the Value of vWF in the Diagnosis of Liver Cirrhosis With Portal Hypertension. J Clin Transl Hepatol (2018) 6(4):1–6. doi: 10.14218/JCTH.2018.00036
62. Prasanna KS, Goel A, Amirtharaj GJ, Ramachandran A, Balasubramanian KA, Mackie I, et al. Plasma Von Willebrand Factor Levels Predict in-Hospital Survival in Patients With Acute-on-Chronic Liver Failure. Indian J Gastroenterol (2016) 35(6):432–40. doi: 10.1007/s12664-016-0708-2
63. Eidelberg A, Kirubakaran R, Nair SC, Eapen CE, Elias E, Goel A. Systematic Review: Role of Elevated Plasma von-Willebrand Factor as Predictor of Mortality in Patients With Chronic Liver Disease. Eur J Gastroenterol Hepatol (2019) 31(10):1184–91. doi: 10.1097/MEG.0000000000001491
64. Horvatits T, Drolz A, Roedl K, Herkner H, Ferlitsch A, Perkmann T, et al. Von Willebrand Factor Antigen for Detection of Hepatopulmonary Syndrome in Patients With Cirrhosis. J Hepatol (2014) 61(3):544–9. doi: 10.1016/j.jhep.2014.04.025
65. Takaya H, Kawaratani H, Tsuji Y, Nakanishi K, Saikawa S, Sato S, et al. Von Willebrand Factor is a Useful Biomarker for Liver Fibrosis and Prediction of Hepatocellular Carcinoma Development in Patients With Hepatitis B and C. United European Gastroenterol J (2018) 6(9):1401–9. doi: 10.1177/2050640618779660
66. Maieron A, Salzl P, Peck-Radosavljevic M, Trauner M, Hametner S, Schöfl R, et al. Von Willebrand Factor as a New Marker for Non-Invasive Assessment of Liver Fibrosis and Cirrhosis in Patients With Chronic Hepatitis C. Aliment Pharmacol Ther (2014) 39(3):331–8. doi: 10.1111/apt.12564
67. Aryal B, Yamakuchi M, Shimizu T, Kadono J, Furoi A, Gejima K, et al. Bivalent Property of Intra-Platelet VWF in Liver Regeneration and HCC Recurrence: A Prospective Multicenter Study. Cancer Biomark (2019) 26(1):51–61. doi: 10.3233/CBM-190168
68. Starlinger P, Pereyra D, Haegele S, Braeuer P, Oehlberger L, Primavesi F, et al. Perioperative Von Willebrand Factor Dynamics are Associated With Liver Regeneration and Predict Outcome After Liver Resection. Hepatology (2018) 67(4):1516–30. doi: 10.1002/hep.29651
69. Schwarz C, Fitschek F, Mittlböck M, Saukel V, Bota S, Ferlitsch M, et al. Von Willebrand Factor Antigen Predicts Outcomes in Patients After Liver Resection of Hepatocellular Carcinoma. Gut Liver (2020) 14(2):218–24. doi: 10.5009/gnl17115
70. Wannhoff A, Rauber C, Friedrich K, Rupp C, Stremmel W, Weiss KH, et al. Von Willebrand Factor and Alkaline Phosphatase Predict Re-Transplantation-Free Survival After the First Liver Transplantation. United European Gastroenterol J (2017) 5(1):86–93. doi: 10.1177/2050640616650060
71. Györi GP, Pereyra D, Rumpf B, Hackl H, Köditz C, Ortmayr G, et al. The Von Willebrand Factor Facilitates Model for End-Stage Liver Disease–Independent Risk Stratification on the Waiting List for Liver Transplantation. Hepatology (2020) 72(2):584–94. doi: 10.1002/hep.31047
72. Rhone P, Zarychta E, Bielawski K, Ruszkowska-Ciastek B. Pre-Surgical Level of Von Willebrand Factor as an Evident Indicator of Breast Cancer Recurrence. Cancer Biomark (2020) 29(3):359–72. doi: 10.3233/CBM-191096
73. Obermeier HL, Riedl J, Ay C, Koder S, Quehenberger P, Bartsch R, et al. The Role of ADAMTS-13 and Von Willebrand Factor in Cancer Patients: Results From the Vienna Cancer and Thrombosis Study. Res Pract Thromb Haemost (2019) 3(3):503–14. doi: 10.1002/rth2.12197
74. Yao J, Song A, Cao W, Chen S, Zhou L, Cao S, et al. Clinical Significance of Anti-Endothelial Cell Antibody in Allogeneic Hematopoietic Stem Cell Transplantation Recipients With Graft-Versus-Host Disease. Int J Hematol (2014) 99(3):329–37. doi: 10.1007/s12185-014-1517-y
75. Guo R, Yang J, Liu X, Wu J, Chen Y. Increased Von Willebrand Factor Over Decreased ADAMTS-13 Activity is Associated With Poor Prognosis in Patients With Advanced Non-Small-Cell Lung Cancer. J Clin Lab Anal (2018) 32(1):e22219. doi: 10.1002/jcla.22219
76. Hodak E, Trattner A, David M, Kornbrot N, Modan B, Lurie H, et al. Quantitative and Qualitative Assessment of Plasma Von Willebrand Factor in Classic Kaposi’s Sarcoma. J Am Acad Dermatol (1993) 28(2):217–21. doi: 10.1016/0190-9622(93)70030-W
77. Kastritis E, Papassotiriou I, Terpos E, Roussou M, Gavriatopoulou M, Komitopoulou A, et al. Clinical and Prognostic Significance of Serum Levels of Von Willebrand Factor and ADAMTS-13 Antigens in AL Amyloidosis. Blood (2016) 128(3):405–9. doi: 10.1182/blood-2016-02-702696
78. Lopes AAB, Maeda NY. Circulating Von Willebrand Factor Antigen as a Predictor of Short-Term Prognosis in Pulmonary Hypertension. Chest (1998) 114(5):1276–82. doi: 10.1378/chest.114.5.1276
79. Ware LB, Eisner MD, Thompson BT, Parsons PE, Matthay MA. Significance of Von Willebrand Factor in Septic and Nonseptic Patients With Acute Lung Injury. Am J Respir Crit Care Med (2004) 170(7):766–72. doi: 10.1164/rccm.200310-1434OC
80. El Basset Abo El Ezz AA, Abd El Hafez MA, El Amrousy DM, El Momen Suliman GA. The Predictive Value of Von Willebrand Factor Antigen Plasma Levels in Children With Acute Lung Injury. Pediatr Pulmonol (2017) 52(1):91–7. doi: 10.1002/ppul.23518
81. Van Der Zee P, Rietdijk W, Somhorst P, Endeman H, Gommers D. A Systematic Review of Biomarkers Multivariately Associated With Acute Respiratory Distress Syndrome Development and Mortality. Crit Care (2020) 24:243. doi: 10.1186/s13054-020-02913-7
82. Johansson MW, Kruger SJ, Schiebler ML, Evans MD, Sorkness RL, Denlinger LC, et al. Markers of Vascular Perturbation Correlate With Airway Structural Change in Asthma. Am J Respir Crit Care Med (2013) 188(2):167–78. doi: 10.1164/rccm.201301-0185OC
83. Rønnow SR, Langholm LL, Karsdal MA, Manon-Jensen T, Tal-Singer R, Miller BE, et al. Endotrophin, an Extracellular Hormone, in Combination With Neoepitope Markers of Von Willebrand Factor Improves Prediction of Mortality in the ECLIPSE COPD Cohort. Respir Res (2020) 21(1):202. doi: 10.1186/s12931-020-01461-6
84. Langholm LL, Rønnow SR, Sand JMB, Leeming DJ, Tal-Singer R, Miller BE, et al. Increased Von Willebrand Factor Processing in COPD, Reflecting Lung Epithelium Damage, is Associated With Emphysema, Exacerbations and Elevated Mortality Risk. Int J COPD (2020) 15:543–52. doi: 10.2147/COPD.S235673
85. Kayal S, Jaïs JP, Aguini N, Chaudière J, Labrousse J. Elevated Circulating E-selectin, Intercellular Adhesion Molecule 1, and Von Willebrand Factor in Patients With Severe Infection. Am J Respir Crit Care Med (1998) 157(3 PART I):776–84. doi: 10.1164/ajrccm.157.3.9705034
86. Rubin DB, Wiener-Kronish JP, Murray JF, Green DR, Turner J, Luce JM, et al. Elevated Von Willebrand Factor Antigen is an Early Plasma Predictor of Acute Lung Injury in Nonpulmonary Sepsis Syndrome. J Clin Invest (1990) 86(2):474–80. doi: 10.1172/JCI114733
87. Hyseni A, Kemperman H, De Lange DW, Kesecioglu J, De Groot PG, Roest M. Active Von Willebrand Factor Predicts 28-Day Mortality in Patients With Systemic Inflammatory Response Syndrome. Blood (2014) 123(14):2153–6. doi: 10.1182/blood-2013-08-508093
88. Hovinga JAK, Zeerleder S, Kessler P, Romani De Wit T, Van Mourik JA, Hack CE, et al. ADAMTS-13, Von Willebrand Factor and Related Parameters in Severe Sepsis and Septic Shock. J Thromb Haemost (2007) 5(11):2284–90. doi: 10.1111/j.1538-7836.2007.02743.x
89. McElroy AK, Erickson BR, Flietstra TD, Rollin PE, Towner JS, Nichol ST, et al. Von Willebrand Factor is Elevated in Individuals Infected With Sudan Virus and is Associated With Adverse Clinical Outcomes. Viral Immunol (2015) 28(1):71–3. doi: 10.1089/vim.2014.0072
90. Alpoim PN, Gomes KB, Godoi LC, Rios DR, Carvalho MG, Fernandes AP, et al. ADAMTS13, FVIII, Von Willebrand Factor, ABO Blood Group Assessment in Preeclampsia. Clin Chim Acta (2011) 412(23–24):2162–6. doi: 10.1016/j.cca.2011.07.030
91. James JP, Stevens TRJ, Hall ND, Maddison PJ, Goulding NJ, Silman A, et al. Factor VIII Related Antigen in Connective Tissue Disease Patients and Relatives. Rheumatology (1990) 29(1):6–9. doi: 10.1093/rheumatology/29.1.6
92. Van Son WJ, Brijker F, Elema JD, Tegzess AM, Van Der Meer J. Elevated Factor VIII as a Marker for Vascular Type of Rejection After Renal Transplantation. Transplant Proc (1997) 29(1–2):161–3. doi: 10.1016/S0041-1345(96)00049-8
93. Jenkins PV, Rawley O, Smith OP, O’Donnell JS. Elevated Factor VIII Levels and Risk of Venous Thrombosis. Br J Haematol (2012) 157(6):653–63. doi: 10.1111/j.1365-2141.2012.09134.x
94. Cosmi B, Legnani C, Cini M, Favaretto E, Palareti G. D-dimer and Factor VIII are Independent Risk Factors for Recurrence After Anticoagulation Withdrawal for a First Idiopathic Deep Vein Thrombosis. Thromb Res (2008) 122(5):610–7. doi: 10.1016/j.thromres.2007.12.024
95. Mattila N, Seppänen H, Mustonen H, Przybyla B, Haglund C, Lassila R. Preoperative Biomarker Panel, Including Fibrinogen and FVIII, Improves Diagnostic Accuracy for Pancreatic Ductal Adenocarcinoma. Clin Appl Thromb (2018) 24(8):1267–75. doi: 10.1177/1076029618779133
96. Vormittag R, Simanek R, Ay C, Dunkler D, Quehenberger P, Marosi C, et al. High Factor VIII Levels Independently Predict Venous Thromboembolism in Cancer Patients: The Cancer and Thrombosis Study. Arterioscler Thromb Vasc Biol (2009) 29(12):2176–81. doi: 10.1161/ATVBAHA.109.190827
97. Castellón Rubio VE, Segura PP, Muñoz A, Farré AL, Ruiz LC, Lorente JA. High Plasma Levels of Soluble P-Selectin and Factor VIII Predict Venous Thromboembolism in Non-Small Cell Lung Cancer Patients: The Thrombo-Nsclc Risk Score. Thromb Res (2020) 196:349–54. doi: 10.1016/j.thromres.2020.09.021
98. Dossenbach-Glaninger A, van Trotsenburg M, Krugluger W, Dossenbach MR, Oberkanins C, Huber J, et al. Elevated Coagulation Factor VIII and the Risk for Recurrent Early Pregnancy Loss. Thromb Haemost (2004) 91(4):694–9. doi: 10.1160/TH03-09-0554
99. Sakamoto S, Kawabata H, Kanda J, Uchiyama T, Mizumoto C, Kondo T, et al. Differing Impacts of Pretransplant Serum Ferritin and C-Reactive Protein Levels on the Incidence of Chronic Graft-Versus-Host Disease After Allogeneic Hematopoietic Stem Cell Transplantation. Int J Hematol (2013) 97(1):109–16. doi: 10.1007/s12185-012-1229-0
100. Minnema MC, Fijnheer R, De Groot PG, Lokhorst HM. Extremely High Levels of Von Willebrand Factor Antigen and of Procoagulant Factor VIII Found in Multiple Myeloma Patients are Associated With Activity Status But Not With Thalidomide Treatment. J Thromb Haemost (2003) 1(3):445–9. doi: 10.1046/j.1538-7836.2003.00083.x
101. Mohren M, Jentsch-Ullrich K, Koenigsmann M, Kropf S, Schalk E, Lutze G. High Coagulation Factor VIII and Von Willebrand Factor in Patients With Lymphoma and Leukemia. Int J Hematol (2016) 103(2):189–95. doi: 10.1007/s12185-015-1913-y
102. Collins P, Gutteridge C, O’Driscoll A, Blair S, Jones L, Aitchison R, et al. Von Willebrand Factor as a Marker of Endothelial Cell Activation Following BMT. Bone Marrow Transplant (1992) 10(6):499–506.
103. Vannucchi A, Rafanelli D, Longo G, Bosi A, Guidi S, Saccardi R, et al. Early Hemostatic Alterations Following Bone Marrow Transplantation: A Prospective Study. Haematologica (1994) 79:519–25.
104. Mir E, Palomo M, Rovira M, Pereira A, Escolar G, Penack O, et al. Endothelial Damage is Aggravated in Acute GvHD and Could Predict its Development. Bone Marrow Transplant (2017) 52(9):1317–25. doi: 10.1038/bmt.2017.121
105. Buser TA, Martinez M, Drexler B, Tschan-Plessl A, Heim D, Passweg J, et al. Biological Markers of Hemostasis and Endothelial Activation in Patients With a Hematological Malignancy With or Without Stem Cell Transplants. Eur J Haematol (2019) 103(5):472–7. doi: 10.1111/ejh.13310
106. Salat C, Holler E, Kolb H-J, Pihusch R, Reinhardt B, Hiller E. Endothelial Cell Markers in Bone Marrow Transplant Recipients With and Without Acute Graft-Versus-Host Disease. Bone Marrow Transplant (1997) 19(9):909–14. doi: 10.1038/sj.bmt.1700767
107. Przybyla B, Pinomäki A, Petäjä J, Joutsi-Korhonen L, Strandberg K, Hillarp A, et al. Coordinated Responses of Natural Anticoagulants to Allogeneic Stem Cell Transplantation and Acute GVHD - A Longitudinal Study. PLoS One (2017) 12(12):e0190007. doi: 10.1371/journal.pone.0190007
108. Biedermann BC, Sahner S, Gregor M, Tsakiris DA, Jeanneret C, Pober JS, et al. Endothelial Injury Mediated by Cytotoxic T Lymphocytes and Loss of Microvessels in Chronic Graft Versus Host Disease. Lancet (2002) 359(9323):2078–83. doi: 10.1016/S0140-6736(02)08907-9
109. Biedermann BC, Tsakiris DA, Gregor M, Pober JS, Gratwohl A. Combining Altered Levels of Effector Transcripts in Circulating T Cells With a Marker of Endothelial Injury is Specific for Active Graft-Versus-Host Disease. Bone Marrow Transplant (2003) 32(11):1077–84. doi: 10.1038/sj.bmt.1704258
110. Pulanic D, Samardzic A, Desnica L, Zadro R, Milosevic M, Serventi Seiwerth R, et al. High Levels of FVIII and Von Willebrand Factor in Chronic Graft-versus-Host Disease. The 45th Annual Meeting of the European Society for Blood and Marrow Transplantation: Physicians – Poster Session. Bone Marrow Transplant (2019) 54:303. doi: 10.1038/s41409-019-0559-4
111. Kekre N, Kim HT, Ho VT, Cutler C, Armand P, Nikiforow S, et al. Venous Thromboembolism is Associated With Graft-Versus-Host Disease and Increased non-Relapse Mortality After Allogeneic Hematopoietic Stem Cell Transplantation. Haematologica (2017) 102(7):1185–91. doi: 10.3324/haematol.2017.164012
112. Xu Z, Luo C, Lai P, Ling W, Wu S, Huang X, et al. Von Willebrand Factor as a Predictor for Transplant-Associated Thrombotic Microangiopathy. Clin Appl Thromb (2020) 26:1–7. doi: 10.1177/1076029619892684
113. Ito-Habe N, Wada H, Matsumoto T, Ohishi K, Toyoda H, Ishikawa E, et al. Elevated Von Willebrand Factor Propeptide for the Diagnosis of Thrombotic Microangiopathy and for Predicting a Poor Outcome. Int J Hematol (2011) 93(1):47–52. doi: 10.1007/s12185-010-0732-4
114. Shulman HM, Gown AM, Nugent DJ. Hepatic Veno-Occlusive Disease After Bone Marrow Transplantation. Immunohistochemical Identification of the Material Within Occluded Central Venules. Am J Pathol (1987) 127(3):549–58.
115. Mohty M, Malard F, Abecassis M, Aerts E, Alaskar AS, Aljurf M, et al. Revised Diagnosis and Severity Criteria for Sinusoidal Obstruction Syndrome/Veno-Occlusive Disease in Adult Patients: A New Classification From the European Society for Blood and Marrow Transplantation. Bone Marrow Transplant (2016) 51(7):906–12. doi: 10.1038/bmt.2016.130
116. Gabay C, Kushner I. Acute-Phase Proteins and Other Systemic Responses to Inflammation. N Engl J Med (1999) 340:448–54. doi: 10.1056/NEJM199902113400607
117. Pulanic D, Lozier JN, Pavletic SZ. Thrombocytopenia and Hemostatic Disorders in Chronic Graft Versus Host Disease. Bone Marrow Transplant (2009) 44(7):393–403. doi: 10.1038/bmt.2009.196
118. Rayes J, Bourne JH, Brill A, Watson SP. The Dual Role of Platelet-Innate Immune Cell Interactions in Thrombo-Inflammation. Res Pract Thromb Haemost (2020) 4(1):23–35. doi: 10.1002/rth2.12266
119. Matsuda Y, Hara J, Osugi Y, Tokimasa S, Fujisaki H, Takai K, et al. Serum Levels of Soluble Adhesion Molecules in Stem Cell Transplantation-Related Complications. Bone Marrow Transplant (2001) 27(9):977–82. doi: 10.1038/sj.bmt.1703026
120. Kariminia A, Holtan SG, Ivison S, Rozmus J, Hebert M-J, Martin PJ, et al. Heterogeneity of Chronic Graft-Versus-Host Disease Biomarkers: Association With CXCL10 and CXCR3+ NK Cells. Blood (2016) 127(24):3082–91. doi: 10.1182/blood-2015-09-668251
121. Pidala J, Sarwal M, Roedder S, Lee SJ. Biologic Markers of Chronic GVHD. Bone Marrow Transplant (2014) 49:324–31. doi: 10.1038/bmt.2013.97
122. Yu J, Storer BE, Kushekhar K, Zaid MA, Zhang Q, Gafken PR, et al. Biomarker Panel for Chronic Graft-Versus-Host Disease. J Clin Oncol (2016) 34(22):2583–90. doi: 10.1200/JCO.2015.65.9615
123. Martires KJ, Baird K, Steinberg SM, Grkovic L, Joe GO, Williams KM, et al. Sclerotic-Type Chronic GVHD of the Skin: Clinical Risk Factors, Laboratory Markers, and Burden of Disease. Blood (2011) 118(15):4250–7. doi: 10.1182/blood-2011-04-350249
124. Bat T, Steinberg SM, Childs R, Calvo KR, Barrett AJ, Battiwalla M, et al. Active Thrombopoiesis is Associated With Worse Severity and Activity of Chronic GVHD. Bone Marrow Transplant (2013) 48(12):1569–73. doi: 10.1038/bmt.2013.95
125. Pihusch R, Wegner H, Salat C, Pihusch M, Holler E, Kolb HJ, et al. Flow Cytometric Findings in Platelets of Patients Following Allogeneic Hematopoietic Stem Cell Transplantation. Bone Marrow Transplant (2002) 30(6):381–7. doi: 10.1038/sj.bmt.1703663
126. Bozdag SC, Gunaltay S, Dalva K, Ozcan M. Follow-Up of ADAMTS13 Enzyme and its Relationship With Clinical Events After Allogeneic Hematopoietic Stem Cell Transplantation. Blood Coagul Fibrinolysis (2009) 20(3):165–9. doi: 10.1097/MBC.0b013e3283177b30
127. McGuirk J, Hao G, Hou W, Abhyankar S, Williams C, Yan W, et al. Serum Proteomic Profiling and Haptoglobin Polymorphisms in Patients With GVHD After Allogeneic Hematopoietic Cell Transplantation. J Hematol Oncol (2009) 2(1):17. doi: 10.1186/1756-8722-2-17
128. Ren H-G, Adom D, Paczesny S. The Search for Drug-Targetable Diagnostic, Prognostic and Predictive Biomarkers in Chronic Graft-Versus-Host Disease. Expert Rev Clin Immunol (2018) 14(5):389–404. doi: 10.1080/1744666X.2018.1463159
129. Kitko CL, Levine JE, Storer BE, Chai X, Fox DA, Braun TM, et al. Plasma CXCL9 Elevations Correlate With Chronic GVHD Diagnosis. Blood (2014) 123(5):786–93. doi: 10.1182/blood-2013-08-520072
130. Saliba RM, Sarantopoulos S, Kitko CL, Pawarode A, Goldstein SC, Magenau J, et al. B-Cell Activating Factor (BAFF) Plasma Level At the Time of Chronic GvHD Diagnosis is a Potential Predictor of non-Relapse Mortality. Bone Marrow Transplant (2017) 52(7):1010–5. doi: 10.1038/bmt.2017.73
131. Liu X, Yue Z, Yu J, Daguindau E, Kushekhar K, Zhang Q, et al. Proteomic Characterization Reveals That MMP-3 Correlates With Bronchiolitis Obliterans Syndrome Following Allogeneic Hematopoietic Cell and Lung Transplantation. Am J Transplant (2016) 16(8):2342–51. doi: 10.1111/ajt.13750
132. Großekatthöfer M, Güclü ED, Lawitschka A, Matthes-Martin S, Mann G, Minkov M, et al. Ferritin Concentrations Correlate to Outcome of Hematopoietic Stem Cell Transplantation But do Not Serve as Biomarker of Graft-Versus-Host Disease. Ann Hematol (2013) 92(8):1121–8. doi: 10.1007/s00277-013-1737-x
133. Shimura K, Ashihara E, Shimazaki C, Matsunaga S, Taniguchi K, Uchiyama H, et al. Circulating Endothelial Progenitor Cells Decreased in Patients With Sclerodermatous Chronic Graft-versus-Host Disease. Biol Blood Marrow Transplant (2008) 14(4):426–37. doi: 10.1016/j.bbmt.2008.02.001
134. Hildebrandt GC, Chao N. Endothelial Cell Function and Endothelial-Related Disorders Following Haematopoietic Cell Transplantation. Br J Haematol (2020) 190:508–19. doi: 10.1111/bjh.16621
135. Tichelli A, Gratwohl A. Vascular Endothelium as ‘Novel’ Target of Graft-Versus-Host Disease. Best Pract Res Clin Haematol (2008) 21(2):139–48. doi: 10.1016/j.beha.2008.02.002
136. Biedermann BC, Pober JS. Human Vascular Endothelial Cells Favor Clonal Expansion of Unusual Alloreactive CTL. J Immunol (1999) 162:7022–30.
137. Eissner G, Hartmann I, Kesikli A, Holler E, Haffner S, Sax T, et al. CD4+CD25+FoxP3+ Regulatory T-Cells Enhance the Allogeneic Activity of Endothelial-Specific CD8+/CD28- Cytotoxic T Lymphocytes. Int Immunol (2011) 23:485–92. doi: 10.1093/intimm/dxr041
138. Luft T, Dietrich S, Falk C, Conzelmann M, Hess M, Benner A, et al. Steroid-Refractory GVHD: T-Cell Attack Within a Vulnerable Endothelial System. Blood (2011) 118(6):1685–92. doi: 10.1182/blood-2011-02-334821
139. Cordes S, Mokhtari Z, Bartosova M, Mertlitz S, Riesner K, Shi Y, et al. Endothelial Damage and Dysfunction in Acute Graft-Versus-Host Disease. Haematologica (2020) 105. doi: 10.3324/haematol.2020.253716
140. Martinez-Sanchez J, Hamelmann H, Palomo M, Mir E, Moreno-Castaño AB, Torramade S, et al. Acute Graft-vs.-Host Disease-Associated Endothelial Activation In Vitro Is Prevented by Defibrotide. Front Immunol (2019) 10:2339. doi: 10.3389/fimmu.2019.02339
141. García-Bernal D, Palomo M, Martínez CM, Millán-Rivero JE, García-Guillén AI, Blanquer M, et al. Defibrotide Inhibits Donor Leucocyte-Endothelial Interactions and Protects Against Acute Graft-Versus-Host Disease. J Cell Mol Med (2020) 24(14):8031–44. doi: 10.1111/jcmm.15434
142. Eissner G, Multhoff G, Gerbitz A, Kirchner S, Haffner S, Sondermann D, et al. Fludarabine Induces Apoptosis, Activation and Allogenicity in Human Endothelial and Epithelial Cells, Protective Role of Defibrotide. Blood (2002) 100:334–40. doi: 10.1182/blood.V100.1.334
143. Kreisel D, Krupnick AS, Gelman AE, Engels FH, Popma SH, Krasinskas AM, et al. Non-Hematopoietic Allograft Cells Directly Activate CD8+ T Cells and Trigger Acute Rejection: An Alternative Mechanism of Allorecognition. Nat Med (2002) 8:233–9. doi: 10.1038/nm0302-233
144. Penack O, Socié G, Van Den Brink MRM. The Importance of Neovascularization and its Inhibition for Allogeneic Hematopoietic Stem Cell Transplantation. Blood (2011) 117:4181–9. doi: 10.1182/blood-2010-10-312934
145. Haeusermann P, Kump E, Rovo A, Tichelli A, Itin P, Gratwohl A, et al. Partial Reconstitution of Cutaneous Microvessels in Long-Term Survivors After Allogeneic Bone Marrow Transplantation. Dermatology (2009) 219(1):32–41. doi: 10.1159/000216934
146. Willemze AJ, Bakker AC, Von Dem Borne PA, Bajema IM, Vossen JM. The Effect of Graft-Versus-Host Disease on Skin Endothelial and Epithelial Cell Chimerism in Stem-Cell Transplant Recipients. Transplantation (2009) 87(7):1096–101. doi: 10.1097/TP.0b013e31819d340f
Keywords: endothelial dysfunction, inflammation, factor VIII, Von Willeband factor, chronic graft-versus-host disease (cGvHD), allogeneic hematopoietic stem cell transplantation
Citation: Lelas A, Greinix HT, Wolff D, Eissner G, Pavletic SZ and Pulanic D (2021) Von Willebrand Factor, Factor VIII, and Other Acute Phase Reactants as Biomarkers of Inflammation and Endothelial Dysfunction in Chronic Graft-Versus-Host Disease. Front. Immunol. 12:676756. doi: 10.3389/fimmu.2021.676756
Received: 05 March 2021; Accepted: 12 April 2021;
Published: 30 April 2021.
Edited by:
Ralf Dressel, University Medical Center Göttingen, GermanyReviewed by:
Jakob Passweg, University Hospital of Basel, SwitzerlandCopyright © 2021 Lelas, Greinix, Wolff, Eissner, Pavletic and Pulanic. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Drazen Pulanic, ZHJhemVuLnB1bGFuaWNAa2JjLXphZ3JlYi5ocg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.