
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol., 28 September 2021
Sec. Immunological Tolerance and Regulation
Volume 12 - 2021 | https://doi.org/10.3389/fimmu.2021.636612
This article is part of the Research TopicAllergen Immunotherapy for Airborne and Food Allergens: Efficacy and Immunological MechanismsView all 5 articles
 Francesca Mori1†
Francesca Mori1† Mattia Giovannini1*†
Mattia Giovannini1*† Simona Barni1
Simona Barni1 Rodrigo Jiménez-Saiz2,3,4,5
Rodrigo Jiménez-Saiz2,3,4,5 Daniel Munblit6,7,8
Daniel Munblit6,7,8 Benedetta Biagioni9Giulia Liccioli1Lucrezia Sarti1Lucia Liotti10Silvia Ricci11
Benedetta Biagioni9Giulia Liccioli1Lucrezia Sarti1Lucia Liotti10Silvia Ricci11 Elio Novembre1
Elio Novembre1 Umit Sahiner12
Umit Sahiner12 Ermanno Baldo13
Ermanno Baldo13 Davide Caimmi14,15
Davide Caimmi14,15The prevalence of food allergy has increased in recent years, especially in children. Allergen avoidance, and drugs in case of an allergic reaction, remains the standard of care in food allergy. Nevertheless, increasing attention has been given to the possibility to treat food allergy, through immunotherapy, particularly oral immunotherapy (OIT). Several OIT protocols and clinical trials have been published. Most of them focus on children allergic to milk, egg, or peanut, although recent studies developed protocols for other foods, such as wheat and different nuts. OIT efficacy in randomized controlled trials is usually evaluated as the possibility for patients to achieve desensitization through the consumption of an increasing amount of a food allergen, while the issue of a possible long-term sustained unresponsiveness has not been completely addressed. Here, we evaluated current pediatric OIT knowledge, focusing on the results of clinical trials and current guidelines. Specifically, we wanted to highlight what is known in terms of OIT efficacy and effectiveness, safety, and impact on quality of life. For each aspect, we reported the pros and the cons, inferable from published literature. In conclusion, even though many protocols, reviews and meta-analysis have been published on this topic, pediatric OIT remains a controversial therapy and no definitive generalized conclusion may be drawn so far. It should be an option provided by specialized teams, when both patients and their families are prone to adhere to the proposed protocol. Efficacy, long-term effectiveness, possible role of adjuvant therapies, risk of severe reactions including anaphylaxis or eosinophilic esophagitis, and impact on the quality of life of both children and caregivers are all aspects that should be discussed before starting OIT. Future studies are needed to provide firm clinical and scientific evidence, which should also consider patient reported outcomes.
The worldwide prevalence of allergic disease has increased over the last decades (1, 2). Among allergic diseases, food allergy (FA) represents a major public health concern as the leading cause of anaphylaxis in the pediatric population (3–6) and and being associated to a higher risk of severe forms in asthmatic children (7). Such assumption should be carefully taken into consideration because the prevalence of FA in children in Europe is ~3.1% (8) and more than a third of food allergic children have asthma (9). In addition, FA causes a considerable psychological impact both to the allergic patients and their families (10). For example, a pan-European study showed that most peanut-allergic individuals had lifestyle restrictions regarding food, faced problems with socializing, holiday activities and the use of public transport. Remarkably, two‐thirds of them felt socially isolated and over 40% had been bullied because of their disease (11). Furthermore, FA is an economic burden with an estimated household-level out-of-pocket equivalent to $3,339 and an individual-level direct medical cost of ~$2,081 worldwide (12).
Food allergen avoidance remains the backbone of the FA management (13–15). In the past years, extensive research has focused on intervention strategies to manage FA. The potential methods of allergen immunotherapy for FA include subcutaneous, sublingual, epicutaneous and oral immunotherapy. Moreover, combinations of immunotherapy with biologics, such as anti-IgE (e.g., omalizumab) or anti-IL4 receptor α (IL4Rα; e.g., dupilumab), or probiotics were proposed as well in the management of FA (16, 17). Of these, subcutaneous immunotherapy (SCIT) was popular in the 90s, but clinical trials were not successful due to the high frequency of systemic side effects (18, 19), which led to the use of hypoallergenic recombinant proteins (20). Although the use of SCIT in IgE-mediated FA has not been popular, it has gained more interest recently, using safer innovative research approaches both in patients and in murine models (21, 22). Nevertheless, SCIT is not currently used in routine clinical practice. Oral immunotherapy (OIT), followed by epicutaneous immunotherapy (EPIT), is the most studied intervention (13, 23). Indeed, peanut OIT and EPIT were recently approved by the Food and Drug Administration (FDA) for the treatment of peanut-allergic children (24). On the other hand, the implementation of OIT in FA management is generally debated (25).
OIT efficacy in randomized controlled trials (RCTs) is usually evaluated as the achievement of desensitization through the consumption of an increasing amount of a food allergen; this last is a state of increased allergen reactivity threshold as compared with the pre-OIT eliciting dose. However, it is unclear if desensitization or sustained unresponsiveness (SU), which is, in previously desensitized patients, the ability to safely consume any amount of the offending food, even after a prolonged period of allergen avoidance may be considered as the best outcome in the assessment of OIT efficacy/effectiveness (26). The same consideration may apply to the use of immunological parameters, in assessing efficacy and effectiveness, because their applicability as potential OIT outcome measures remains unclear.
Recent systematic reviews suggest that a number of OIT trials had methodological limitations. This fact not only may have led to an overestimation of OIT efficacy and an underestimation of reactions rate during OIT but could also be associated to an inaccurate representation of changes in health-related quality of life (QoL) in treated patients (27, 28). Furthermore, the lack of defined outcomes in FA intervention trials causes inconsistencies in terms of data interpretation (29). Additional criticisms towards OIT include discrepancies in decision-making knowledge on allergen dosing schedules, risk of secondary effects due to the procedure, questions on long-term clinical efficacy, cost-efficacy, and the burden of a potential daily treatment lasting over several years (25). On the other hand, some growing evidence in favor of OIT prompted active discussions on a possible wider introduction of OIT into routine clinical practice (30, 31). Indeed, many RCTs of milk, egg and peanut OIT were published. In this review, we critically appraise available scientific literature and, based on up-to-date evidence, provide arguments for and against OIT in FA children.
Table 1 and Figure 1 summarize the pros and the cons with regards to efficacy and effectiveness of OIT in food-allergic children.
Table 1 Efficacy and effectiveness of OIT in children – pros and cons.
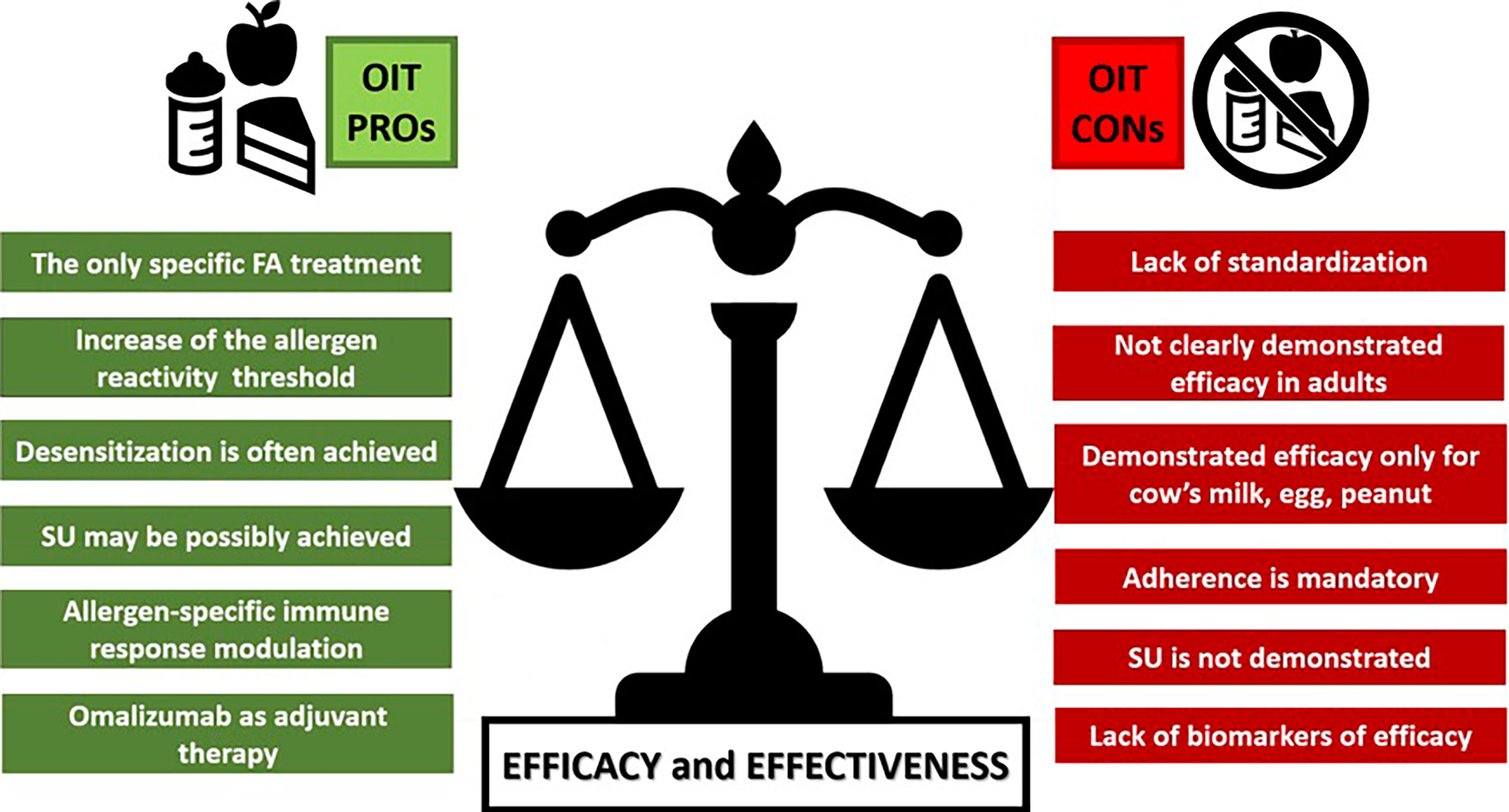
Figure 1 A comparison between the main PROs and CONs arguments on OIT Efficacy and Effectiveness. FA, food allergy; SU, sustained unresponsiveness.
OIT effectiveness is normally assessed using two possible outcomes: desensitization or SU (32, 33). As mentioned above, desensitization is the patient’s ability to increase the minimal amount of allergen required to elicit an allergic reaction; to be maintained, it requires daily allergen exposure (34). An allergen threshold increase provides a certain degree of protection on the accidental ingestion of the causative allergen (32). Moreover, some desensitized patients can regularly ingest a full serving dose without reactions. However, the ultimate OIT goal is the achievement of SU, which is, in previously desensitized patients, the ability to safely consume any amount of the offending food, even after a prolonged period of allergen avoidance (35). Desensitization does not preclude SU development. Indeed, desensitization is necessary to reach, afterwards, a state of SU.
It has long been established that 50% of cow’s milk allergic children and up to 80% of hen’s egg-allergic children develop tolerance by the age of 4-6 years (36–38). Moreover, recent studies showed that an increasing number of children tends to outgrow their cow’s milk and egg allergies after the preschool age (37, 39, 40). However, although FA often spontaneously resolves by preschool age, at least in patients allergic to cow’s milk and egg (41–43), the rate of patients outgrowing FA in adolescence is lower, with individuals suffering from persistent FA (37, 39, 40). Therefore, in these patients, immunotherapy represents a possible way to modify the natural course of their persistent FA.
A recent meta-analysis confirmed that OIT induces desensitization in most patients allergic to peanut, milk, and egg: 76.9% of OIT patients reached desensitization vs 8.1% of patients tolerating the foods following allergen avoidance or placebo (26). Although the capacity of OIT to induce SU has not been clearly demonstrated, this meta-analysis showed that SU developed in 31.8% of patients after OIT vs 11.1% after allergen avoidance or placebo (26). Of note, the likelihood of achieving SU appeared to be related to the duration of OIT. Indeed, 28% of egg-allergic patients reached SU after 22 months of egg OIT (35), compared to 50% after 4 years of treatment (44). Moreover, the rate of SU was higher in peanut-allergic patients when OIT was initiated at a younger age (9-36 months) (45). Although the ability of OIT to induce SU seems limited (26), in accordance to experts’ opinion, families may consider desensitization as an acceptable outcome, as it protects children from potentially severe allergic reactions due to accidental allergen exposure (46).
OIT efficacy/effectiveness is presumably dependent on its effects on the allergen-specific immune response (47, 48). The immunological basis underlying desensitization and SU during OIT are still poorly understood. This is in part due to the scarcity in studies on immunological mechanisms in OIT trials and to other possible limitations inherent to conducting research in FA pediatric patients (49). Notwithstanding, it is well established that OIT tends to reduce allergen-specific Ig (sIg)E (after an initial increase), and this is followed by a boost in sIgG4. The latter compete with sIgE for allergen binding, thus decreasing effector cell activation (i.e., basophils, mast cells), that release the mediators responsible for acute allergic reactions, including anaphylaxis (50). IgG4 has been the most studied sIg in OIT, but other subclasses may contribute to the overall blocking and inhibitory sIgG response in FA (50). Considering cellular immunity, the spotlight has mainly been on Treg cells, which typically increase during OIT and exert a beneficial, but transient, immunosuppressive function (48). Therefore, while there is evidence that OIT induces protective immunological mechanisms (47, 48, 50), our understanding of these circuits is still fairly limited, and therapeutic approaches to make them endure after OIT interruption remain to be clarified (49).
Recently, it has been shown that tolerance should not be considered as an “all-or-nothing phenomenon”. For example, some milk- and egg-allergic children tolerate baked forms of these foods (51, 52). This is due to the impact of heat-processing on the structure of immunodominant allergens of egg and milk (53, 54), which reduces the number of sIgE-binding sites (55, 56). Along this line, Esamaelizadeh et al. conducted a RCT in 84 children presenting with cow’s milk allergy but tolerant to baked milk. Patients were divided into a case (baked milk consumers) and a control group (baked milk avoiders) for one year: 88.1% of patients in the case group and 66.7% of those in the control group developed tolerance to unheated milk at the end of the study (57). Therefore, the use of cow’s milk as part of baked food in OIT may increase safety and may favor the resolution of allergies towards the native allergens (raw or unprocessed) (58–60). Nevertheless, further studies are needed to confirm this line of evidence and to ascertain involved mechanisms (57, 61, 62).
In addition to the use of baked or hypoallergenic foods, other approaches have been explored to improve OIT efficacy. One of them included the use of anti-IgE monoclonal antibodies as adjuvant treatment for OIT patients (63). Omalizumab was first used in combination with OIT in milk-allergic children (64). Subsequent studies showed that omalizumab facilitated a faster achievement of higher OIT maintenance doses as compared to regular OIT (32, 65–69). Importantly, while omalizumab used as an adjuvant to OIT improved its safety and tolerability, it did not lead to higher efficacy (67), although larger studies are required on this topic (70). In this context, biologics intended to block other pathways of the Th2 immune response, such as dupilumab have begun to be explored in FA patients (71). The idea of interfering with IL-4Rα, thus blocking IL-4/IL-13 signaling, would prevent IgE re-generation from any memory B cell reservoir that requires IgE class-switching and its commitment to a plasma cell lineage (49, 72, 73); in addition, de novo Th2 polarization would be hampered. Consequently, the concomitant interference with IL-4 and IL-13 signaling in FA, may not only impair the machinery re-generating IgE but also potentiate regulatory pathways leading to desensitization, SU or oral tolerance (72, 74, 75).
Even though OIT has been evaluated for different allergens through several trials, in most cases this approach still lacks standardized protocols and current evidence has been generated only in a selected proportion of pediatric FA patients and only for certain foods (20). As abovementioned, OIT efficacy in clinical trials should clearly distinguish between desensitization and SU. Furthermore, patient-reported outcomes measures should be included in the clinical trials as well, because they represent powerful and irreplaceable tools to quantify the patient’s perception of the disease status and of its improvement (32).
OIT trials have shown effective desensitization in many patients and SU in some, but it is still unclear if the most relevant and important outcomes were measured. At present, there is no consensus on the core outcome domains, and validated instruments to assess these domains are lacking as well (29). The heterogeneity in OIT products, protocols, outcomes, age and clinical features of the enrolled patients does not allow to adequately assess the treatment effectiveness (27). Some preliminary estimations may be drawn for certain FA (e.g., cow’s milk, egg, and peanut). However, these only apply to children, because OIT in adult patients appears to not lead to successful desensitization (26). Importantly, children have a considerable likelihood of spontaneously acquiring tolerance, particularly to cow’s milk and egg, which questions the utility of OIT in them (76). Therefore, in some cases, it may be more appropriate to wait for the natural development of tolerance before proposing such a challenging and time-consuming intervention. On the other hand, those children that do not spontaneously outgrow their FA and become adults, may have lost a sensible window to modify their hypersensitive immunological status.
Another line of criticism towards OIT considers that the evidence in support of OIT efficacy in FA is weak and relying on limited data for cow’s milk, egg, and peanut. At present, OIT is not recommended for many foods, neither in adults nor in children (20). Most OIT clinical trials assessing effectiveness do not consider adherence problems although such issues remain critical in real-life settings. Indeed, OIT is a very demanding therapeutic option, and its efficacy strictly depends on patients’ adherence to treatment (20). In addition, consistent clinical and laboratory data on SU are scarce (77) and OIT is currently not widely used in the adult population worldwide. SU may be clinically confirmed by performing a food challenge after OIT has been discontinued for a certain period of time. In most studies, SU has not been assessed and there is not enough information on the possible efficacy of OIT in acquiring it after treatment discontinuation (26). Moreover, there is no consensus on when SU should be assessed, especially on how much time after OIT cessation. The majority of studies addressing SU evaluate it up to 8 weeks after treatment discontinuation (34), which may be insufficient to reach a firm conclusion. Furthermore, even once SU is confirmed, it may be lost over time. For example, it has been demonstrated that after a 2-weeks proven SU, patients treated with OIT for cow’s milk, egg and wheat may still experience allergic clinical manifestations after longer periods of avoidance (78). The lack of evidence for SU implies that OIT patients should pursue a life-long “maintenance phase” to prevent potentially dangerous adverse reactions (ARs) after the consumption of the involved food. To date, protocols do not include accurate information on possible quantity and frequency of food intake after the end of the maintenance phase. Therefore, in most cases there is a lack of standardization and of recommendations on this aspect of patients’ after-treatment management.
Several immunological changes have been reported during OIT, some of which appear to be consistent across different allergens and OIT protocols (50). As indicated earlier, OIT studies usually show an increase in sIgG4 levels, and its persistence upon therapy cessation has been associated with SU (79). Other immunological changes reported during OIT include expansion of Treg cells, and reduction in total and sIgE levels (47, 50). However, reliable biological markers to assess the evolution of OIT patients or desensitization/SU persistence are still unavailable. The suppression of the immunologic response during OIT seems to be transient (80, 81) and unable to control persistent populations of pathogenic Th2-cells, which have been detected in patients with peanut allergy after 12 to 24 months of OIT (80). Hence it is unclear if immunological markers can serve as a practical and reliable outcome of OIT (48). A detailed characterization of the immune cells affected by OIT is required to uncover immunological changes indicative of durable SU or effective desensitization, which can be tracked after OIT discontinuation (48, 49, 77). In this context, reaching a better understanding on the immunological basis of persistent FA may lead to the identification of novel biomarkers that may help in better defining OIT outcomes (49, 72–74).
The use of omalizumab as adjuvant therapy for OIT showed some benefits in facilitating a faster achievement of higher maintenance doses, as discussed above. However, omalizumab failed to improve SU acquisition. This may be potentially connected to the fact that the benefit obtained is lost after the discontinuation of the treatment with this monoclonal antibody (69).
At present, OIT may be considered for recommendation only in cow’s milk, egg or peanut allergic children and desensitization is assured only if the adherence to the treatment is very high. In most cases, appropriate products and defined protocols for OIT are still lacking. OIT to baked foods may be particularly challenging in centres lacking expertise. To date, effectiveness in inducing SU has not been demonstrated neither clinically nor in terms of persistent immunological modifications. Therefore, post-desensitization strategy remains unclear and further studies are needed. New approaches such as the utilization of omalizumab to improve OIT effectiveness failed to achieve long-term SU. Of note, lack of agreed core outcomes in FA slows down the process of high-quality evidence collection and OIT effectiveness assessment.
Table 2 and Figure 2 summarize the pros and the cons with regards to safety of OIT in food-allergic children.

Table 2 Safety of OIT in children – pros and cons.
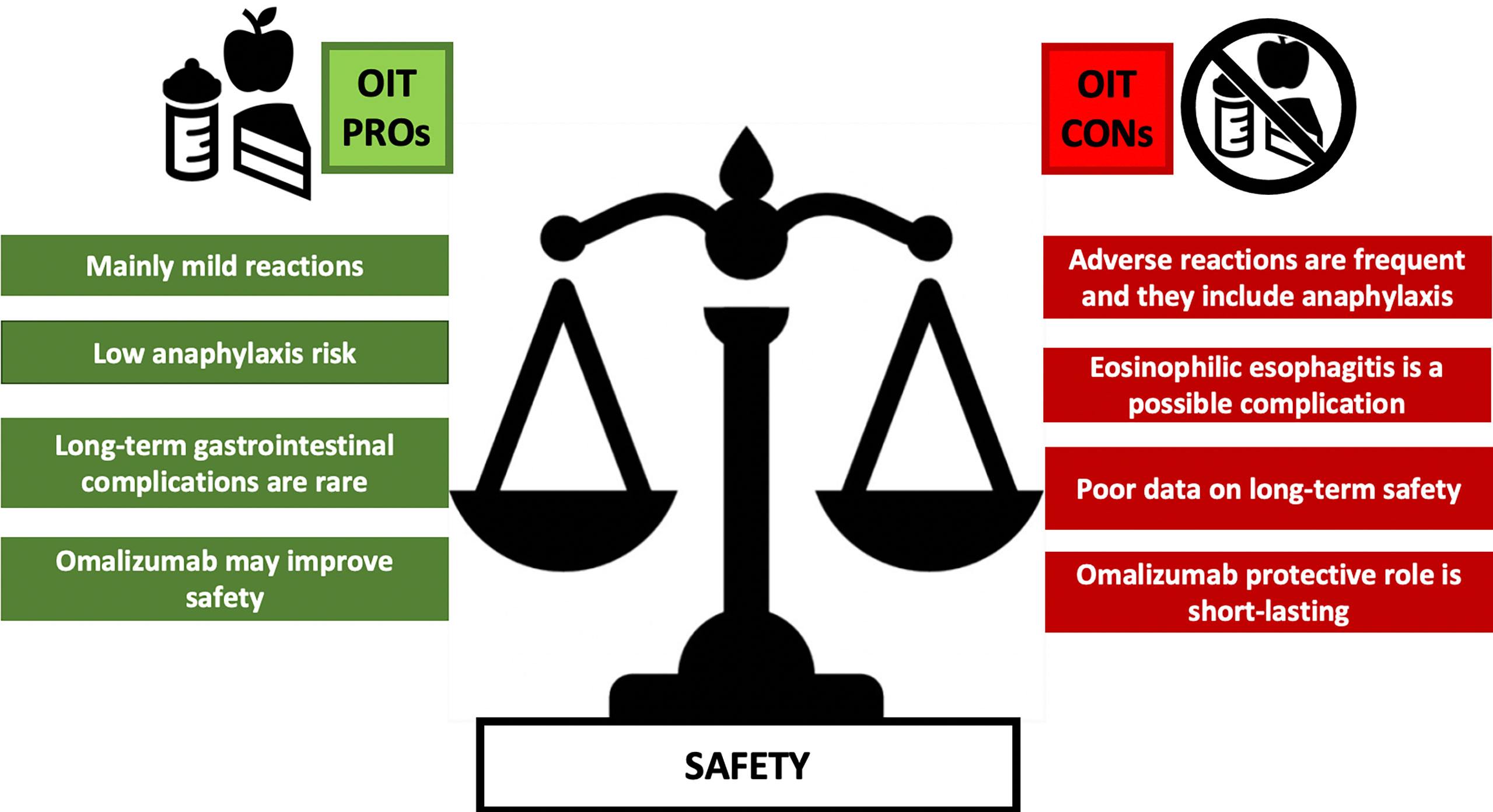
Figure 2 A comparison between the main PROs and CONs arguments on OIT Safety. ARs, adverse reactions; EoE, eosinophilic esophagitis; GI, gastrointestinal.
FA patients and their relatives should be always aware of the potential risks associated with OIT. Various studies assessed OIT safety comparing intervention data with patients on elimination diet. Almost all OIT patients experienced mild or moderate ARs (46), as perioral rash, local urticaria, rhinitis, or minor gastrointestinal clinical manifestations (26), and most ARs resolved without treatment or simply after administration of oral antihistamines (82).
The risk of systemic ARs during OIT is relatively uncommon, and no OIT-related deaths were reported in the literature. Still, all FA patients should be trained to use, and carry, emergency drugs (epinephrine auto injector), and should be accurately monitored, especially in the OIT up-dosing phase (83). A recent baked-milk OIT study reported ARs in 21 out of 63 patients, with only one of them developing anaphylaxis (84). Other studies confirmed a low incidence of ARs requiring epinephrine injection during peanut (30, 85) and egg (86) OIT. In contrast, Kauppila et al. reported that 14% of patients had anaphylaxis during raw milk OIT, but a cofactor was often considered as an element involved for inducing the AR, or the ARs appeared after a period of allergen elimination diet (87).
Cofactors may play a role in triggering an AR, which mainly occurs during the OIT build-up phase. Importantly, patients already tolerating a specific allergen dose, may sometimes experience an AR during the OIT maintenance phase. In those cases, a cofactor altering immune homeostasis (e.g., viral infections, fever, exercise, non-steroidal anti-inflammatory drugs intake, or hormonal changes) may be involved (46). Indeed, it is important to recommend avoidance of physical activity at least one hour before and three hours after the intake of a food allergen. Likewise, children suffering from fever or infectious diseases should suspend, or at least halve, the OIT maintenance dose for a few days (82). Other conditions contributing to ARs during OIT are poorly controlled asthma, seasonal pollen allergy, and circumstances such as consumption of the OIT on an empty stomach (82).
Once long-term secondary effects are concerned, it is still debated whether OIT might play a role in the onset of eosinophilic esophagitis (EoE) (82, 88, 89). A meta-analysis reported a not negligible prevalence of EoE in OIT-treated patients (90). However, EoE is a condition that can resolve following specific therapy or OIT discontinuation (89). Along this line, the results of a recent trial on 15 adults undergoing peanut OIT showed that possible OIT-induced EoE and gastrointestinal eosinophilia are usually transient and not always associated with gastrointestinal signs and symptoms (91). Recurrence of ARs may also be a cause of OIT withdrawal (92, 93). A recent meta-analysis reported an overall rate of OIT discontinuation of about 14%; only 4.7% was due to clinical manifestations possibly related to EoE (92). In addition, Blumchen et al. showed that, using a peanut OIT protocol with a low maintenance dose, the proportion of dropouts due to ARs was 6.7%, without need of epinephrine use and with no EoE development (31). Nevertheless, it is still unclear if OIT can induce EoE as a direct side effect of the treatment.
The decision to initiate OIT should be tailored on the patient’s allergic profile, and on personal choice of patients and their families. Awareness of the possible risks should be raised, and details of the heterogeneity of reported ARs should be clearly outlined and put into context of the specific treatment proposed (88, 94).
Patient safety is a critical issue for OIT. ARs, including life-threatening events, appear to be more frequent during OIT, in comparison with food allergen avoidance (28, 88, 89, 94). Studies report that 10–35% of FA children withdrew OIT trials because of anaphylaxis, acute or repeated ARs and especially chronic abdominal pain (95, 96). As mentioned above, many identifiable but often unavoidable factors may cause ARs (including fever or infections, exercise, temperature changes, dosing on an empty stomach, menstruation, seasonal allergies, asthma, and non-compliance), and some identifiable cofactors are often unknown (28, 82, 97, 98). For example, near-fatal reactions have been observed in asthmatic teenagers showing poor compliance (99). Therefore, the presence of cofactors requires frequent allergen dose adjustments to obtain a safe dosing profile (100). In this regard, the European Academy of Allergy and Clinical Immunology (EAACI) OIT guidelines suggest continuous surveillance of OIT patients for ARs and clinical manifestations of new-onset EoE, especially during the up-dosing phase (20).
EoE is a possible secondary effect of OIT, but the relationship between EoE and OIT remains controversial, being unclear whether OIT causes EoE or reveals a pre-existing condition (89, 101). The overall prevalence of EoE following OIT was reported as 2.7% (82, 90). However, a prospective food OIT study reported that EoE or eosinophilic gastroenteritis developed in 7 (7.2%) patients out of 97 children included in a milk OIT group and in 2 (6.4%) out of 31 patients in a egg OIT group (102). During OIT, sIgG and sIgA may enhance eosinophil activation and contribute to EoE onset (103). To evaluate the real EoE prevalence during and following OIT, it is necessary to consider that an esophagogastroduodenoscopy is not performed in all patients with dose-limiting gastrointestinal clinical manifestations. Therefore, the real EoE rate may be higher than reported (104). Furthermore, longitudinal data of EoE in food OIT are insufficient to study long-term safety (93). A recent comprehensive review analyzed data from 110 studies (92) and found that EoE-confirming biopsies were performed in 18 studies only, and EoE was diagnosed in 5.3% of OIT patients.
Many studies show that epinephrine use is variable and related to the OIT protocol (105). Wasserman et al. retrospectively reviewed charts from 352 patients evaluated in 5 allergy centres, and they found that epinephrine administration was necessary in 36 patients (10.2%) (106). A Cochrane systematic review on milk OIT reported ARs in 97 out of 106 patients (91%), while epinephrine was required in 9% of patients receiving milk OIT (107). A more recent prospective study on milk OIT registered 1,548 ARs, most of which occurring during the escalation phase (89.6%). Anaphylaxis and chronic late-onset gastrointestinal clinical manifestations accounted for 15.8% of ARs and represented the primary reason for protocol withdrawal. Interestingly, a higher rate of sIgE for α-lactalbumin and casein at baseline was associated with an increased risk of anaphylaxis during milk OIT, while patients with higher sIgE for β-lactoglobulin had a lower risk (108). Moreover, egg OIT was associated with serious ARs in all 10 RCTs included in a Cochrane systematic review. Epinephrine was required in 21 out of 249 (8.4%) of children in the egg OIT group but never in the control group (105). A recent systematic review of >1,000 peanut-allergic patients evidenced that peanut OIT increases the risk of ARs, anaphylaxis development and epinephrine use, either during the build-up or the maintenance phase. The authors estimated the risk of anaphylaxis in patients undergoing OIT about 22% in comparison with a baseline risk of 7% (28).
Some centres are using omalizumab during OIT because it may reduce the risk of ARs, especially in children with severe FA. However, the duration of the therapy with omalizumab is still debated, as well as the long-term outcomes after omalizumab discontinuation (66). Some experts consider the use of omalizumab as a helpful measure for rapid up-dosing but, when decreasing omalizumab doses, ARs become more frequent. Therefore, omalizumab appears to confer short-term protection from OIT-related ARs (109). Furthermore, the use of omalizumab may be associated with side reactions including skin inflammation and anaphylaxis in 0.1-0.2% of patients, likely due to its engagement with Fcγ receptors (110).
Further investigations on OIT safety should be carried on prior to routine OIT use in clinical practice (105, 111). A careful and complete explanation of the ARs risks vs OIT clinical benefits should be given before starting the therapy to both children and their families (83).
Table 3 and Figure 3 summarize the pros and the cons with regards to the impact on QoL of OIT in food-allergic children.
Table 3 Impact of food OIT in children’s QoL – pros and cons.
Figure 3 A comparison between the main PROs and CONs arguments on OIT quality of life. FA, food allergy.
Both FA and the consequent elimination diet have a negative impact on QoL due to food-related anxiety, fear of accidental exposures and the ever-present burden of social and dietary limitations (11, 95, 112–114). Allergen elimination diet remains the gold standard for FA management. This approach, however, requires constant responsibility from both patient and caregiver. FA children are vulnerable to unintentional allergen ingestion and possible anaphylaxis, which has a negative influence on the QoL (35).
OIT aims to increase the allergen reactivity threshold to reduce the risk of serious allergic reactions after inadvertent allergen exposure. This approach should provide a safer social life for FA children, with less fear of being accidentally exposed to the allergen, and eventually result in QoL improvement. A complete resolution of the allergy following OIT treatment remains the ultimate OIT goal, which would clearly improve patients’ QoL. An increasing number of studies evaluated the impact of OIT on children’s QoL, mainly for egg (115, 116), peanut (11, 31, 96, 117–119), and cow’s milk allergy (120), but also on patients suffering from multiple FA (121–124). The results of these studies are encouraging, even though most of them report major limitations mainly related to the small sample included in the study and the limited number of RCTs.
Most of the studies confirmed that desensitization correlates with an improvement in children’s QoL, as perceived by their caregivers (96, 115, 121, 122, 124, 125). Three factors were found to be associated with a more substantial improvement in QoL: having an allergy to a single food, presenting with a history of anaphylactic reactions prior to OIT initiation, and having a very low QoL before the beginning of OIT (124). Blumchen et al. found that achieving desensitization during OIT improved the QoL as perceived by caregivers and by patients in a double-blind RCT (31). After peanut OIT, there was a significant improvement in QoL in the domain of “risk of accidental exposure” and “emotional impact” in children, when compared with the placebo group. Other studies that evaluated the QoL during and/or at the end of OIT showed a more substantial improvement in children (116, 117) or adolescents (117) when compared to the caregiver-reported QoL. In contrast, Reier-Nielsen et al. found statistically significant improvements in QoL reported by caregivers, while no significant change was recorded in children (119).
Several studies evaluated QoL improvement by OIT, as perceived by caregivers, in patients achieving SU (11, 120, 126). Specifically, a double-blind placebo-controlled RCT (127) evaluated the impact of Probiotic and Peanut Oral Immunotherapy (PPOIT) on health-related QoL. The authors concluded that PPOIT had a sustained beneficial effect on the psychosocial impact of FA at 3 months and 12 months after completion of the treatment. The improved QoL was specifically associated with the acquisition of SU. Indeed, for this study, a post-hoc analysis revealed that no improvement in QoL was seen for either PPOIT-treated or placebo-treated patients who failed to achieve SU (128). A study assessed the impact of QoL evaluated by children and adolescents after achieving peanut SU (126); in this study, there was a general trend towards an improvement in QoL at the end of peanut OIT, but it did not reach statistical significance, probably because of the small sample size.
Studies assessing QoL as one of the outcomes in patients undergoing OIT are heterogeneous, use different methods, and are often limited to a small sample size. According to some experiences, compared to food allergen avoidance, OIT may be associated with an improvement in QoL for both patients and caregivers, especially at the end of the treatment and in the absence of ARs (122, 129). However, these data should be viewed with caution as additional evidence is needed.
FA patients present with a decreased QoL, with repercussions on their general health and lifestyle (20, 130). Although OIT is a promising therapeutic approach, it is demanding, especially in terms of protocol duration, adherence-related issues, and safety concerns (20). It is therefore evident that improvements in patients’ QoL throughout and after OIT must be carefully assessed (26, 131). The heterogeneity of factors possibly influencing QoL makes it difficult to achieve a uniform approach. Some important ones such as the perception of treatment burden, are rarely considered in OIT trials (31). Health-related QoL has only recently started to appear as a potential outcome in OIT clinical trials, hence data on the matter are limited (131) and a meta-analysis by Chu et al. found no evidence that OIT improves the QoL (28).
Improved QoL after OIT has been reported only in a few trials for egg (115, 116) and cow’s milk allergy (120), while a larger number of studies considering QoL is available regarding peanut (31, 96, 118, 119, 126, 127) and multiple food desensitization (121, 122, 124, 125). Most of these studies are characterized by substantial limitations in the reported results, being based only on parent-reported QoL (96, 121, 123, 128) or lacking a control group (117). As aforementioned, discrepancies between children self-assessment and parental reports have emerged, showing significantly better QoL scores reported by parents when compared to their children (119). These data suggest that parents may overestimate the impact of OIT on child’s QoL, calling into question the appropriateness of parental proxy reports use as a valid outcome of OIT effectiveness. In addition, OIT may also result in QoL worsening, for example in the build-up phase, as demonstrated by Ebstein-Rigbi et al., probably because of the occurrence of ARs in this treatment phase (122). The heterogeneity of the studies and of the methodology of QoL assessment, along with the very limited number of data do not allow for definitive conclusions but the most up to date meta-analysis does not add optimism (28).
FA is one of the most burdensome allergic disease in children (132). It affects both patients and caregivers, as there is always a risk of accidental exposure, and they should be ready to administer a treatment for the clinical manifestations, in case of a reaction, with the consequent impact on their daily life. Although food allergen avoidance and treatment of the signs and symptoms are still the mainstream of FA management, OIT has been proposed as an alternative approach aiming at the “disease treatment”, focusing on its natural history. Well-designed OIT clinical trials were initiated recently, making OIT a considerably novel approach in FA management; nevertheless, the first attempts of treating children by giving small and increasing amounts of the allergen, to stimulate immune tolerance, go back to the beginning of the 20th century (133). Most OIT trials were conducted over the last decade focusing on single allergens, predominantly on cow’s milk, egg, and peanut, but there is an increasing number of publications on other allergens, such as wheat (134–136) and nuts (137). Moreover, peanut OIT and EPIT were recently approved by the FDA for the treatment of peanut-allergic children (24). The novel approach of treating children suffering from multiple FAs with OIT is showing some promising results (138, 139), which is of a particular interest to practicing physicians as it is closer to routine clinical practice settings.
There is an intense debate over the utility of OIT in children: there is a substantial heterogeneity of study protocols with regards to administration schedules (e.g., starting doses, doses increase, delay between doses, and target maintenance dose); and they diverge on efficacy and safety profiles, as well as on QoL assessment in the treated population. Here, we reviewed existing evidence on this subject, highlighting discrepancies and summarizing the main findings. OIT is capable of increasing the allergen reactivity threshold dose. Although desensitization seems to be beneficial for the FA patient, the extent of this improvement is unknown as no agreement on core outcomes is in place (29). FA patients are facing the constant fear of developing a reaction after inadvertent consumption of the causative allergen, which remains one of the major issues for them and their caregivers. Increasing the allergen eliciting dose reduces, to some extent, the risk of allergic reactions, thus decreasing stress in FA patients and their relatives. While desensitization is an achievable OIT outcome, SU remains a distant prospect. In addition, studies thoroughly assessing SU are scarce and mainly focused on short-term effects.
The use of adjuvant therapies, as an OIT adjunct, may empower the effects of OIT. Adjuvant therapies currently under investigation include toll-like-receptor 4 and 9 agonists; nanoparticles encapsulating the allergen; Chinese medicine; antihistamines; leukotriene receptor antagonists; probiotics; and biologics, especially omalizumab and dupilumab (71, 140). The combination of OIT with omalizumab is believed to decrease the risk of ARs and/or allow faster desensitization with a better safety profile (66, 141).
A recent observational study assessing the effects of omalizumab in 15 asthmatic children showed 8.6-fold increase in food allergen threshold (142). The concomitant use of omalizumab during OIT seems to promote allergen desensitization through an initial omalizumab-dependent step that acutely depletes allergen-reactive T cells. This appears to be followed by an allergen-specific Treg cell activity increase due to the reversal of their Th2 cell-like program. Improved Treg cell function could therefore be the mechanism allowing an easier and faster OIT protocol in FA patients (143). Preliminary results are encouraging, but optimal duration of omalizumab use before/during/after OIT, and its role in the treatment of FA remain unknown. More clinical trials are therefore needed to determine the patients’ phenotype that is suitable for biologics therapy and optimal treatment regimens. A currently ongoing blinded study is comparing OIT with and without omalizumab (138). The results will possibly allow to single out the effect of omalizumab on OIT effectiveness and safety, hence providing novel prospective data to inform on the optimal and most cost-effective dosage for this indication (138). Lastly, the therapeutic value of dupilumab has begun to be assessed in FA patients (71). The blockade of IgE class-switching from IgG+ memory B cells and preventing the perpetuation of the Th2 program during OIT may yield safer therapies and favor the transition from desensitization to SU or even oral tolerance (72, 74, 75).
OIT safety has not been clearly determined. Most ARs occurring during the build-up phase are normally mild to moderate, but concerns remain regarding less frequent but potentially life-threatening ARs during OIT. Most studies report the occurrence of anaphylactic cases, especially during the OIT build-up phase. Furthermore, anaphylaxis is more common in patients undergoing OIT when compared with the control group, in clinical trials. It should be noted, however, that research settings may differ from the “real life scenario” as patients included in a study tend to meticulously follow investigator advice. Thus, studies evaluating the risk of anaphylaxis in “real-life settings” are needed. There are safety concerns due to the limited data and major methodological discrepancies between the trials and real-life populations in which patients having experienced anaphylaxis or suffering from severe asthma could be found. Indeed, although was shown that severe anaphylaxis is mainly associated with peanut allergy in children, most studies consider a history of severe anaphylaxis (or of repeated anaphylaxis episodes) (31, 65, 144–147), severe asthma (31, 65, 144–149) as an exclusion criteria. A limited number of trials did not exclude children with a history of severe and/or non-controlled asthma (96), or severe or repeated anaphylaxis (96, 148, 149). They did not find an increased risk of systemic/severe ARs in treated patients. Notwithstanding, the available data are not sufficient to establish an OIT safety profile in these particularly vulnerable groups of FA patients.
Because of the substantial heterogeneity of published studies, it is not possible to clearly define all the OIT pros and cons. ARs from OIT may be provoked by a wide range of factors including exercise, menses, colds, fever, alcohol, nonsteroidal anti-inflammatory drugs and other medications (46). Moreover, the frequency of ARs may affect OIT compliance resulting in patients to stop OIT over time. Another major problem is the absence of specific biomarkers predictive of OIT outcomes. Discussion with patients and their families, and meticulous explanation of the procedure including possible ARs, and the expected goals is pivotal. OIT outcomes should also be discussed and carefully analyzed by clinicians, patients, and their families together. An appropriate patients’ selection represents a cornerstone to increase the treatment’s probability of success and adherence. The latter choice appears really difficult, and it involves medical (e.g., sensitization, history of reaction) but also human factors, especially related to the estimated compliance of the patient/family.
The main OIT aim could be a decrease in the risk of ARs to trace contamination or accidental exposure, or introduction of the food to the regular diet. Importantly, patients and families should be well informed of the duration of maintenance. It is crucial to understand that this type of treatment is associated with daily ingestion of a given food for years, and consequent limitations, particularly related to physical activity and other cofactors. Furthermore, they should be aware of the prospect of not reaching SU. The food and the appropriate age for OIT initiation must be carefully considered, taking into account that most children eventually acquire natural tolerance to cow’s milk and hen’s egg. In some cases, it may be more appropriate to wait for the natural tolerance acquisition; on the other hand, the risk is that children who do not spontaneously outgrow FA may have lost a suitable window of OIT intervention.
One of the main OIT limitations is the lack of solid data on long-term QoL improvement in OIT patients and lack of consensus on what (and how) OIT outcomes should be assessed in OIT trials (29). OIT safety and efficacy may be dependent on the age of the patients, and some studies have suggested that desensitization in younger children may be associated with better outcomes (30). However, it is exceedingly difficult to confirm whether desensitization or SU are the result of OIT or the natural resolution of FA in some cases in this age group.
A final aspect on which the present review did not focus, due to the lack of substantial literature on the topic, is the cost-effectiveness of OIT in FA patients. OIT has already turned into a treatment for FA in some countries and potential for OIT to be cost-effective and cost-saving should be assessed in detail prior to a wider implementation.
As for today, many aspects of FA management do not seem cost-effective, such as not being able to provide a short delay for OFC for eligible patients, or not having good biomarkers to firmly diagnose FA without the need to perform an OFC (150). To affirm that OIT is cost-effective, there are 3 levels that need to be taken into account: patients’ health state utility improvement, reduction of the risk of anaphylaxis, and likelihood of achieving SU. It should also be considered the degree to which patients will perceive the benefit of OIT (e.g., depending on the level of protection from accidental exposure; the possible anxiety reduction in patients and caregivers; and the possibility of making dietary changes after a successful therapy) (151).
Two recent papers highlight the fact that peanut OIT (with a commercial product) shows more favorable cost-effectiveness, compared to avoidance, with greater improvements in health utility, particularly if SU can be achieved (150, 151). Further studies are needed to determine the degree of health state utility improvement, and whether OIT will induce durable SU, allowing discontinuation of OIT (150, 151). Also, identifying patients who poorly respond to OIT would prevent continuing the treatment, but more studies are essential to better understand the predictive capacities of food immunotherapy biomarkers, and longer-term data will contribute to reach more solid health and economic analyses (151).
In conclusion, OIT remains a controversial treatment option, requiring team decision making, with patient, family, and physician involved, and all potential risks and benefits should be reviewed. This therapeutic approach has benefits, and it is associated with effective results in terms of increasing the eliciting dose of allergens in many patients, but it also carries significant risks, such as a higher rate of ARs than patients following strict allergen avoidance. Moreover, the impact of OIT on patient-reported outcomes, including QoL remains an open question and it should be assessed in future studies. Further research may help to improve the safety and efficacy of OIT as well as to identify patients who will benefit the most from OIT and will experience minimal ARs. Emerging data from clinical trials suggest that food OIT is a promising treatment modality, which provide patients and their families with an alternative to allergen avoidance and use of rescue medications. However, OIT should be an option provided by specialized teams, when both patients and their families are prone to adhere to the proposed protocol. Finally, rigorous research using outcomes important to patients, including patient-reported outcome measures, is crucial to evaluate real-life effectiveness and safety of OIT.
MG and EB conceptualized the work. FM, MG, SB, DM, BB, GL, LS, LL, US and DC drafted the manuscript. FM, MG, SB, RJ-S, DM, BB, GL, LS, LL, SR, EN, US, EB and DC were responsible for literature search, analyzed, interpreted the data and critically revised the manuscript. All authors contributed to the article and approved the submitted version.
RJ-S acknowledges the support received by the Severo Ochoa Program (AEI/SEV-2017-0712), FSE/FEDER through the Instituto de Salud Carlos III (ISCIII; CP20/00043), The Nutricia Research Foundation (NRF-2021-13), New Frontiers in Research Fund (NFRFE-2019-00083), and SEAIC (BECA20A9). However, no significant funding source could have influenced the work in this paper.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AR, adverse reaction; EAACI, European Academy of Allergy and Clinical Immunology; EoE, eosinophilic esophagitis; EPIT, epicutaneous immuntherapy; FA, food allergy; FDA, Food and Drug Administration; IL4Rα, Interleukin 4 receptor α; OIT, oral immunotherapy; QoL, quality of life; RCT, randomized controlled trials; SCIT, subcutaneous immunotherapy; sIg, allergen-specific immunoglobulin; SU, sustained unresponsiveness.
1. Asher MI, Montefort S, Bjorksten B, Lai CK, Strachan DP, Weiland SK, et al. Worldwide Time Trends in the Prevalence of Symptoms of Asthma, Allergic Rhinoconjunctivitis, and Eczema in Childhood: ISAAC Phases One and Three Repeat Multicountry Cross-Sectional Surveys. Lancet (2006) 368(9537):733–43. doi: 10.1016/S0140-6736(06)69283-0
2. Harrison FC, Giovannini M, Kalaichandran A, Santos AF. Food Allergy. eLS (2020), 1–12. doi: 10.1002/9780470015902.a0028380
3. Barni S, Mori F, Giovannini M, de Luca M, Novembre E. In Situ Simulation in the Management of Anaphylaxis in a Pediatric Emergency Department. Intern Emerg Med (2019) 14(1):127–32. doi: 10.1007/s11739-018-1891-1
4. Foong RX, Giovannini M, du Toit G. Food-Dependent Exercise-Induced Anaphylaxis. Curr Opin Allergy Clin Immunol (2019) 19(3):224–8. doi: 10.1097/ACI.0000000000000531
5. Tanno LK, Demoly P. Anaphylaxis in Children. Pediatr Allergy Immunol (2020) 31 Suppl 26:8–10. doi: 10.1111/pai.13336
6. Nagakura KI, Sato S, Asaumi T, Yanagida N, Ebisawa M. Novel Insights Regarding Anaphylaxis in Children - With a Focus on Prevalence, Diagnosis, and Treatment. Pediatr Allergy Immunol (2020) 31(8):879–88. doi: 10.1111/pai.13307
7. Olabarri M, Vazquez P, Gonzalez-Posada A, Sanz N, Gonzalez-Peris S, Diez N, et al. Risk Factors for Severe Anaphylaxis in Children. J Pediatr (2020) 225:193–7 e5. doi: 10.1016/j.jpeds.2020.06.021
8. Lyons SA, Clausen M, Knulst AC, Ballmer-Weber BK, Fernandez-Rivas M, Barreales L, et al. Prevalence of Food Sensitization and Food Allergy in Children Across Europe. J Allergy Clin Immunol Pract (2020) 8(8):2736–46 e9. doi: 10.1016/j.jaip.2020.04.020
9. Simpson AB, Glutting J, Yousef E. Food Allergy and Asthma Morbidity in Children. Pediatr Pulmonol (2007) 42(6):489–95. doi: 10.1002/ppul.20605
10. Polloni L, Muraro A. Anxiety and Food Allergy: A Review of the Last Two Decades. Clin Exp Allergy (2020) 50(4):420–41. doi: 10.1111/cea.13548
11. DunnGalvin A, Blumchen K, Timmermans F, Regent L, Schnadt S, Podesta M, et al. APPEAL-1: A Multiple-Country European Survey Assessing the Psychosocial Impact of Peanut Allergy. Allergy (2020) 75(11):2899–908. doi: 10.1111/all.14363
12. Bilaver LA, Chadha AS, Doshi P, O’Dwyer L, Gupta RS. Economic Burden of Food Allergy: A Systematic Review. Ann Allergy Asthma Immunol (2019) 122(4):373–80.e1. doi: 10.1016/j.anai.2019.01.014
13. Muraro A, Werfel T, Hoffmann-Sommergruber K, Roberts G, Beyer K, Bindslev-Jensen C, et al. EAACI Food Allergy and Anaphylaxis Guidelines: Diagnosis and Management of Food Allergy. Allergy (2014) 69(8):1008–25. doi: 10.1111/all.12429
14. Ebisawa M, Ito K, Fujisawa T. Committee for Japanese Pediatric Guideline for Food Allergy TJSoPA, Clinical I, Japanese Society of A. Japanese Guidelines for Food Allergy 2020. Allergol Int (2020) 69(3):370–86. doi: 10.1016/j.alit.2020.03.004
15. Barni S, Liccioli G, Sarti L, Giovannini M, Novembre E, Mori F, et al. (IgE)-Mediated Food Allergy in Children: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Management. Med (Kaunas) (2020) 56(3):111. doi: 10.3390/medicina56030111
16. Sicherer SH, Sampson HA. Food Allergy: A Review and Update on Epidemiology, Pathogenesis, Diagnosis, Prevention, and Management. J Allergy Clin Immunol (2018) 141(1):41–58. doi: 10.1016/j.jaci.2017.11.003
17. Fleischer DM, Greenhawt M, Sussman G, Begin P, Nowak-Wegrzyn A, Petroni D, et al. Effect of Epicutaneous Immunotherapy vs Placebo on Reaction to Peanut Protein Ingestion Among Children With Peanut Allergy: The PEPITES Randomized Clinical Trial. JAMA (2019) 321(10):946–55. doi: 10.1001/jama.2019.1113
18. Oppenheimer JJ, Nelson HS, Bock SA, Christensen F, Leung DY. Treatment of Peanut Allergy With Rush Immunotherapy. J Allergy Clin Immunol (1992) 90(2):256–62. doi: 10.1016/0091-6749(92)90080-l
19. Nelson HS, Lahr J, Rule R, Bock A, Leung D. Treatment of Anaphylactic Sensitivity to Peanuts by Immunotherapy With Injections of Aqueous Peanut Extract. J Allergy Clin Immunol (1997) 99(6 Pt 1):744–51. doi: 10.1016/s0091-6749(97)80006-1
20. Pajno GB, Fernandez-Rivas M, Arasi S, Roberts G, Akdis CA, Alvaro-Lozano M, et al. EAACI Guidelines on Allergen Immunotherapy: IgE-Mediated Food Allergy. Allergy (2018) 73(4):799–815. doi: 10.1111/all.13319
21. Bindslev-Jensen C, de Kam P-J, van Twuijver E, Boot DB, El Galta R, Mose AP, et al. SCIT-Treatment With a Chemically Modified, Aluminum Hydroxide Adsorbed Peanut Extract (HAL-MPE1) Was Generally Safe And Well Tolerated And Showed Immunological Changes In Peanut Allergic Patients. J Allergy Clin Immunol (2017) 139(2):AB191. doi: 10.1016/j.jaci.2016.12.623
22. Li X-M, Song Y, Su Y, Heiland T, Sampson HA. Immunization With ARA H1,2,3-Lamp-Vax Peanut Vaccine Blocked IgE Mediated-Anaphylaxis in a Peanut Allergic Murine Model. J Allergy Clin Immunol (2015) 135(2):AB167. doi: 10.1016/j.jaci.2014.12.1482
23. OBH J, Beyer K, Abbas A, Fernandez-Rivas M, Turner PJ, Blumchen K, et al. Efficacy and Safety of Oral Immunotherapy With AR101 in European Children With a Peanut Allergy (ARTEMIS): A Multicentre, Double-Blind, Randomised, Placebo-Controlled Phase 3 Trial. Lancet Child Adolesc Health (2020) 4(10):728–39. doi: 10.1016/S2352-4642(20)30234-0
24. FDA. U.S. Food and Drug Administration. FDA Approves First Drug for Treatment of Peanut Allergy for Children 2020 (2020). Available at: https://www.fda.gov/news-events/press-announcements/fda-approves-first-drug-treatment-peanut-allergy-children (Accessed cited 2020 2020/02/18).
25. Soller L, Abrams EM, Chan ES. An Update on the Controversy Around Offering Oral Immunotherapy to Peanut-Allergic Children Outside of Research. Ann Allergy Asthma Immunol (2019) 122(6):559–62. doi: 10.1016/j.anai.2019.02.011
26. Nurmatov U, Dhami S, Arasi S, Pajno GB, Fernandez-Rivas M, Muraro A, et al. Allergen Immunotherapy for IgE-Mediated Food Allergy: A Systematic Review and Meta-Analysis. Allergy (2017) 72(8):1133–47. doi: 10.1111/all.13124
27. Rodriguez Del Rio P, Escudero C, Sanchez-Garcia S, Ibanez MD, Vickery BP. Evaluating Primary End Points in Peanut Immunotherapy Clinical Trials. J Allergy Clin Immunol (2019) 143(2):494–506. doi: 10.1016/j.jaci.2018.09.035
28. Chu DK, Wood RA, French S, Fiocchi A, Jordana M, Waserman S, et al. Oral Immunotherapy for Peanut Allergy (PACE): A Systematic Review and Meta-Analysis of Efficacy and Safety. Lancet (2019) 393(10187):2222–32. doi: 10.1016/S0140-6736(19)30420-9
29. Sim K, Mijakoski D, Stoleski S, Del Rio PR, Sammut P, Le TM, et al. Outcomes for Clinical Trials of Food Allergy Treatments. Ann Allergy Asthma Immunol (2020) 125(5):535–42. doi: 10.1016/j.anai.2020.06.023
30. Investigators PGoC, Vickery BP, Vereda A, Casale TB, Beyer K, du Toit G, et al. AR101 Oral Immunotherapy for Peanut Allergy. N Engl J Med (2018) 379(21):1991–2001. doi: 10.1056/NEJMoa1812856
31. Blumchen K, Trendelenburg V, Ahrens F, Gruebl A, Hamelmann E, Hansen G, et al. Efficacy, Safety, and Quality of Life in a Multicenter, Randomized, Placebo-Controlled Trial of Low-Dose Peanut Oral Immunotherapy in Children With Peanut Allergy. J Allergy Clin Immunol Pract (2019) 7(2):479–91 e10. doi: 10.1016/j.jaip.2018.10.048
32. Loh W, Tang M. Adjuvant Therapies in Food Immunotherapy. Immunol Allergy Clin North Am (2018) 38(1):89–101. doi: 10.1016/j.iac.2017.09.008
33. Sampath V, Sindher SB, Alvarez Pinzon AM, Nadeau KC. Can Food Allergy be Cured? What are the Future Prospects? Allergy (2020) 75(6):1316–26. doi: 10.1111/all.14116
34. Wood RA. Food Allergen Immunotherapy: Current Status and Prospects for the Future. J Allergy Clin Immunol (2016) 137(4):973–82. doi: 10.1016/j.jaci.2016.01.001
35. Burks AW, Jones SM, Wood RA, Fleischer DM, Sicherer SH, Lindblad RW, et al. Oral Immunotherapy for Treatment of Egg Allergy in Children. N Engl J Med (2012) 367(3):233–43. doi: 10.1056/NEJMoa1200435
36. Peters RL, Dharmage SC, Gurrin LC, Koplin JJ, Ponsonby AL, Lowe AJ, et al. The Natural History and Clinical Predictors of Egg Allergy in the First 2 Years of Life: A Prospective, Population-Based Cohort Study. J Allergy Clin Immunol (2014) 133(2):485–91. doi: 10.1016/j.jaci.2013.11.032
37. Sicherer SH, Wood RA, Vickery BP, Jones SM, Liu AH, Fleischer DM, et al. The Natural History of Egg Allergy in an Observational Cohort. J Allergy Clin Immunol (2014) 133(2):492–9. doi: 10.1016/j.jaci.2013.12.1041
38. Boyano-Martinez T, Garcia-Ara C, Diaz-Pena JM, Martin-Esteban M. Prediction of Tolerance on the Basis of Quantification of Egg White-Specific IgE Antibodies in Children With Egg Allergy. J Allergy Clin Immunol (2002) 110(2):304–9. doi: 10.1067/mai.2002.126081
39. Santos A, Dias A, Pinheiro JA. Predictive Factors for the Persistence of Cow’s Milk Allergy. Pediatr Allergy Immunol (2010) 21(8):1127–34. doi: 10.1111/j.1399-3038.2010.01040.x
40. Savage JH, Matsui EC, Skripak JM, Wood RA. The Natural History of Egg Allergy. J Allergy Clin Immunol (2007) 120(6):1413–7. doi: 10.1016/j.jaci.2007.09.040
41. Host A. Frequency of Cow’s Milk Allergy in Childhood. Ann Allergy Asthma Immunol (2002) 89(6 Suppl 1):33–7. doi: 10.1016/s1081-1206(10)62120-5
42. Saarinen KM, Pelkonen AS, Makela MJ, Savilahti E. Clinical Course and Prognosis of Cow’s Milk Allergy are Dependent on Milk-Specific IgE Status. J Allergy Clin Immunol (2005) 116(4):869–75. doi: 10.1016/j.jaci.2005.06.018
43. Savage J, Sicherer S, Wood R. The Natural History of Food Allergy. J Allergy Clin Immunol Pract (2016) 4(2):196–203. doi: 10.1016/j.jaip.2015.11.024
44. Jones SM, Burks AW, Keet C, Vickery BP, Scurlock AM, Wood RA, et al. Long-Term Treatment With Egg Oral Immunotherapy Enhances Sustained Unresponsiveness That Persists After Cessation of Therapy. J Allergy Clin Immunol (2016) 137(4):1117–27.e10. doi: 10.1016/j.jaci.2015.12.1316
45. Vickery BP, Berglund JP, Burk CM, Fine JP, Kim EH, Kim JI, et al. Early Oral Immunotherapy in Peanut-Allergic Preschool Children is Safe and Highly Effective. J Allergy Clin Immunol (2017) 139(1):173–81.e8. doi: 10.1016/j.jaci.2016.05.027
46. Anagnostou K. Food Immunotherapy for Children With Food Allergies: State of the Art and Science. Curr Opin Pediatr (2018) 30(6):798–805. doi: 10.1097/MOP.0000000000000684
47. Kulis MD, Patil SU, Wambre E, Vickery BP. Immune Mechanisms of Oral Immunotherapy. J Allergy Clin Immunol (2018) 141(2):491–8. doi: 10.1016/j.jaci.2017.12.979
48. Schoos AM, Bullens D, Chawes BL, Costa J, De Vlieger L, DunnGalvin A, et al. Immunological Outcomes of Allergen-Specific Immunotherapy in Food Allergy. Front Immunol (2020) 11:568598(2736). doi: 10.3389/fimmu.2020.568598
49. Jiménez-Saiz R, Chu DK, Waserman S, Jordana M. Initiation, Persistence and Exacerbation of Food Allergy. In: Schmidt-Weber CB, editor. Allergy Prevention and Exacerbation. Birkhäuser Advances in Infectious Diseases. Cham: Springer International Publishing (2017). p. 121–44.
50. Jimenez-Saiz R, Patil SU. The Multifaceted B Cell Response in Allergen Immunotherapy. Curr Allergy Asthma Rep (2018) 18(12):66. doi: 10.1007/s11882-018-0819-1
51. Nowak-Wegrzyn A, Bloom KA, Sicherer SH, Shreffler WG, Noone S, Wanich N, et al. Tolerance to Extensively Heated Milk in Children With Cow’s Milk Allergy. J Allergy Clin Immunol (2008) 122(2):342–7. doi: 10.1016/j.jaci.2008.05.043
52. Des Roches A, Nguyen M, Paradis L, Primeau MN, Singer S. Tolerance to Cooked Egg in an Egg Allergic Population. Allergy (2006) 61(7):900–1. doi: 10.1111/j.1398-9995.2006.01134.x
53. Jimenez-Saiz R, Benede S, Molina E, Lopez-Exposito I. Effect of Processing Technologies on the Allergenicity of Food Products. Crit Rev Food Sci Nutr (2015) 55(13):1902–17. doi: 10.1080/10408398.2012.736435
54. Jimenez-Saiz R, Pineda-Vadillo C, Lopez-Fandino R, Molina E. Human IgE Binding and In Vitro Digestion of S-OVA. Food Chem (2012) 135(3):1842–7. doi: 10.1016/j.foodchem.2012.06.044
55. Jimenez-Saiz R, Belloque J, Molina E, Lopez-Fandino R. Human Immunoglobulin E (IgE) Binding to Heated and Glycated Ovalbumin and Ovomucoid Before and After In Vitro Digestion. J Agric Food Chem (2011) 59(18):10044–51. doi: 10.1021/jf2014638
56. Jimenez-Saiz R, Rupa P, Mine Y. Immunomodulatory Effects of Heated Ovomucoid-Depleted Egg White in a BALB/c Mouse Model of Egg Allergy. J Agric Food Chem (2011) 59(24):13195–202. doi: 10.1021/jf202963r
57. Esmaeilzadeh H, Alyasin S, Haghighat M, Nabavizadeh H, Esmaeilzadeh E, Mosavat F. The Effect of Baked Milk on Accelerating Unheated Cow’s Milk Tolerance: A Control Randomized Clinical Trial. Pediatr Allergy Immunol (2018) 29(7):747–53. doi: 10.1111/pai.12958
58. Nowak-Wegrzyn A, Sampson HA. Future Therapies for Food Allergies. J Allergy Clin Immunol (2011) 127(3):558–73. doi: 10.1016/j.jaci.2010.12.1098
59. Urisu A, Komatsubara R, Hirata N, Kakami M, Kawada Y, Nakajima Y, et al. Oral Immunotherapy by Heated and Ovomucoid-Reduced Egg White to Children With Hen’s Egg Hypersensitivity. Allergy (2008) 63(s88):165. doi: 10.1111/j.1398-9995.2008.01760.x
60. Urisu A, Ando H, Morita Y, Wada E, Yasaki T, Yamada K, et al. Allergenic Activity of Heated and Ovomucoid-Depleted Egg White. J Allergy Clin Immunol (1997) 100(2):171–6. doi: 10.1016/s0091-6749(97)70220-3
61. Bird JA, Clark A, Dougherty I, Brown LS, Arneson A, Crain M, et al. Baked Egg Oral Immunotherapy Desensitizes Baked Egg Allergic Children to Lightly Cooked Egg. J Allergy Clin Immunol Pract (2019) 7(2):667–9.e4. doi: 10.1016/j.jaip.2018.07.013
62. Perez-Quintero O, Martinez-Azcona O, Balboa V, Vila L. Daily Baked Egg Intake may Accelerate the Development of Tolerance to Raw Egg in Egg-Allergic Children. Eur J Pediatr (2020) 179(4):679–82. doi: 10.1007/s00431-019-03488-4
63. Lin C, Lee IT, Sampath V, Dinakar C, DeKruyff RH, Schneider LC, et al. Combining Anti-IgE With Oral Immunotherapy. Pediatr Allergy Immunol (2017) 28(7):619–27. doi: 10.1111/pai.12767
64. Nadeau KC, Schneider LC, Hoyte L, Borras I, Umetsu DT. Rapid Oral Desensitization in Combination With Omalizumab Therapy in Patients With Cow’s Milk Allergy. J Allergy Clin Immunol (2011) 127(6):1622–4. doi: 10.1016/j.jaci.2011.04.009
65. Schneider LC, Rachid R, LeBovidge J, Blood E, Mittal M, Umetsu DT. A Pilot Study of Omalizumab to Facilitate Rapid Oral Desensitization in High-Risk Peanut-Allergic Patients. J Allergy Clin Immunol (2013) 132(6):1368–74. doi: 10.1016/j.jaci.2013.09.046
66. Takahashi M, Soejima K, Taniuchi S, Hatano Y, Yamanouchi S, Ishikawa H, et al. Oral Immunotherapy Combined With Omalizumab for High-Risk Cow’s Milk Allergy: A Randomized Controlled Trial. Sci Rep (2017) 7(1):17453. doi: 10.1038/s41598-017-16730-6
67. Wood RA, Kim JS, Lindblad R, Nadeau K, Henning AK, Dawson P, et al. A Randomized, Double-Blind, Placebo-Controlled Study of Omalizumab Combined With Oral Immunotherapy for the Treatment of Cow’s Milk Allergy. J Allergy Clin Immunol (2016) 137(4):1103–10.e11. doi: 10.1016/j.jaci.2015.10.005
68. Begin P, Dominguez T, Wilson SP, Bacal L, Mehrotra A, Kausch B, et al. Phase 1 Results of Safety and Tolerability in a Rush Oral Immunotherapy Protocol to Multiple Foods Using Omalizumab. Allergy Asthma Clin Immunol (2014) 10(1):7. doi: 10.1186/1710-1492-10-7
69. Lafuente I, Mazon A, Nieto M, Uixera S, Pina R, Nieto A. Possible Recurrence of Symptoms After Discontinuation of Omalizumab in Anti-IgE-Assisted Desensitization to Egg. Pediatr Allergy Immunol (2014) 25(7):717–9. doi: 10.1111/pai.12259
70. Manohar M, Dunham D, Gupta S, Yan Z, Zhang W, Minnicozzi S, et al. Immune Changes Beyond Th2 Pathways During Rapid Multifood Immunotherapy Enabled With Omalizumab. Allergy (2021) 76(9):2809–26. doi: 10.1111/all.14833
71. ClinicalTrials.gov. Study to Evaluate Dupilumab Monotherapy in Pediatric Patients With Peanut Allergy: Nct03793608 (2020). Available at: https://clinicaltrials.gov/ct2/show/study/NCT03793608 (Accessed cited 2020 07/11/2020).
72. Jimenez-Saiz R, Bruton K, Koenig JFE, Waserman S, Jordana M. The IgE Memory Reservoir in Food Allergy. J Allergy Clin Immunol (2018) 142(5):1441–3. doi: 10.1016/j.jaci.2018.08.029
73. Jimenez-Saiz R, Chu DK, Mandur TS, Walker TD, Gordon ME, Chaudhary R, et al. Lifelong Memory Responses Perpetuate Humoral TH2 Immunity and Anaphylaxis in Food Allergy. J Allergy Clin Immunol (2017) 140(6):1604–15 e5. doi: 10.1016/j.jaci.2017.01.018
74. Koenig JFE, Bruton K, Phelps A, Grydziuszko E, Jimenez-Saiz R, Jordana M. Memory Generation and Re-Activation in Food Allergy. Immunotarg Ther (2021) 10:171–84. doi: 10.2147/ITT.S284823
75. Bruton K, Spill P, Vohra S, Baribeau O, Manzoor S, Gadkar S, et al. Interrupting Reactivation of Immunologic Memory Diverts the Allergic Response and Prevents Anaphylaxis. J Allergy Clin Immunol (2021) 147(4):1381–92. doi: 10.1016/j.jaci.2020.11.042
76. Wood RA, Sicherer SH, Vickery BP, Jones SM, Liu AH, Fleischer DM, et al. The Natural History of Milk Allergy in an Observational Cohort. J Allergy Clin Immunol (2013) 131(3):805–12. doi: 10.1016/j.jaci.2012.10.060
77. Tang ML, Martino DJ. Oral Immunotherapy and Tolerance Induction in Childhood. Pediatr Allergy Immunol (2013) 24(6):512–20. doi: 10.1111/pai.12100
78. Manabe T, Sato S, Yanagida N, Hayashi N, Nishino M, Takahashi K, et al. Long-Term Outcomes After Sustained Unresponsiveness in Patients Who Underwent Oral Immunotherapy for Egg, Cow’s Milk, or Wheat Allergy. Allergol Int (2019) 68(4):527–8. doi: 10.1016/j.alit.2019.02.012
79. James LK, Shamji MH, Walker SM, Wilson DR, Wachholz PA, Francis JN, et al. Long-Term Tolerance After Allergen Immunotherapy is Accompanied by Selective Persistence of Blocking Antibodies. J Allergy Clin Immunol (2011) 127(2):509–16 e1-5. doi: 10.1016/j.jaci.2010.12.1080
80. Wisniewski JA, Commins SP, Agrawal R, Hulse KE, Yu MD, Cronin J, et al. Analysis of Cytokine Production by Peanut-Reactive T Cells Identifies Residual Th2 Effectors in Highly Allergic Children Who Received Peanut Oral Immunotherapy. Clin Exp Allergy (2015) 45(7):1201–13. doi: 10.1111/cea.12537
81. Gorelik M, Narisety SD, Guerrerio AL, Chichester KL, Keet CA, Bieneman AP, et al. Suppression of the Immunologic Response to Peanut During Immunotherapy is Often Transient. J Allergy Clin Immunol (2015) 135(5):1283–92. doi: 10.1016/j.jaci.2014.11.010
82. Gernez Y, Nowak-Wegrzyn A. Immunotherapy for Food Allergy: Are We There Yet? J Allergy Clin Immunol Pract (2017) 5(2):250–72. doi: 10.1016/j.jaip.2016.12.004
83. Calvani M, Bianchi A, Imondi C, Romeo E. Oral Desensitization in IgE-Mediated Food Allergy: Effectiveness and Safety. Pediatr Allergy Immunol (2020) 31 Suppl 24:49–50. doi: 10.1111/pai.13171
84. Gruzelle V, Juchet A, Martin-Blondel A, Michelet M, Chabbert-Broue A, Didier A. Benefits of Baked Milk Oral Immunotherapy in French Children With Cow’s Milk Allergy. Pediatr Allergy Immunol (2020) 31(4):364–70. doi: 10.1111/pai.13216
85. Nagakura KI, Sato S, Yanagida N, Nishino M, Asaumi T, Ogura K, et al. Oral Immunotherapy in Japanese Children With Anaphylactic Peanut Allergy. Int Arch Allergy Immunol (2018) 175(3):181–8. doi: 10.1159/000486310
86. Takaoka Y, Maeta A, Takahashi K, MI Y, Takahashi S, Muroya T, et al. Effectiveness and Safety of Double-Blind, Placebo-Controlled, Low-Dose Oral Immunotherapy With Low Allergen Egg-Containing Cookies for Severe Hen’s Egg Allergy: A Single-Center Analysis. Int Arch Allergy Immunol (2019) 180(4):244–9. doi: 10.1159/000502956
87. Kauppila TK, Paassilta M, Kukkonen AK, Kuitunen M, Pelkonen AS, Makela MJ. Outcome of Oral Immunotherapy for Persistent Cow’s Milk Allergy From 11 Years of Experience in Finland. Pediatr Allergy Immunol (2019) 30(3):356–62. doi: 10.1111/pai.13025
88. Burks AW, Sampson HA, Plaut M, Lack G, Akdis CA. Treatment for Food Allergy. J Allergy Clin Immunol (2018) 141(1):1–9. doi: 10.1016/j.jaci.2017.11.004
89. Babaie D, Mesdaghi M, Nishino M, Mansouri M, Ebisawa M. Oral and Sublingual Immunotherapy: Potential Causes for Eosinophilic Gastrointestinal Disorders? Int Arch Allergy Immunol (2017) 172(2):89–98. doi: 10.1159/000457796
90. Lucendo AJ, Arias A, Tenias JM. Relation Between Eosinophilic Esophagitis and Oral Immunotherapy for Food Allergy: A Systematic Review With Meta-Analysis. Ann Allergy Asthma Immunol (2014) 113(6):624–9. doi: 10.1016/j.anai.2014.08.004
91. Wright BL, Fernandez-Becker NQ, Kambham N, Purington N, Cao S, Tupa D, et al. Gastrointestinal Eosinophil Responses in a Longitudinal, Randomized Trial of Peanut Oral Immunotherapy. Clin Gastroenterol Hepatol (2021) 19(6):1151–9.e14. doi: 10.1016/j.cgh.2020.05.019
92. Petroni D, Spergel JM. Eosinophilic Esophagitis and Symptoms Possibly Related to Eosinophilic Esophagitis in Oral Immunotherapy. Ann Allergy Asthma Immunol (2018) 120(3):237–40.e4. doi: 10.1016/j.anai.2017.11.016
93. Cafone J, Capucilli P, Hill DA, Spergel JM. Eosinophilic Esophagitis During Sublingual and Oral Allergen Immunotherapy. Curr Opin Allergy Clin Immunol (2019) 19(4):350–7. doi: 10.1097/ACI.0000000000000537
94. Vazquez-Cortes S, Jaqueti P, Arasi S, Machinena A, Alvaro-Lozano M, Fernandez-Rivas M. Safety of Food Oral Immunotherapy: What We Know, and What We Need to Learn. Immunol Allergy Clin North Am (2020) 40(1):111–33. doi: 10.1016/j.iac.2019.09.013
95. Burbank AJ, Sood P, Vickery BP, Wood RA. Oral Immunotherapy for Food Allergy. Immunol Allergy Clin North Am (2016) 36(1):55–69. doi: 10.1016/j.iac.2015.08.007
96. Anagnostou K, Islam S, King Y, Foley L, Pasea L, Bond S, et al. Assessing the Efficacy of Oral Immunotherapy for the Desensitisation of Peanut Allergy in Children (STOP II): A Phase 2 Randomised Controlled Trial. Lancet (2014) 383(9925):1297–304. doi: 10.1016/S0140-6736(13)62301-6
97. Virkud YV, Burks AW, Steele PH, Edwards LJ, Berglund JP, Jones SM, et al. Novel Baseline Predictors of Adverse Events During Oral Immunotherapy in Children With Peanut Allergy. J Allergy Clin Immunol (2017) 139(3):882–8 e5. doi: 10.1016/j.jaci.2016.07.030
98. Vickery BP, Ebisawa M, Shreffler WG, Wood RA. Current and Future Treatment of Peanut Allergy. J Allergy Clin Immunol Pract (2019) 7(2):357–65. doi: 10.1016/j.jaip.2018.11.049
99. Vazquez-Ortiz M, Alvaro M, Piquer M, Giner MT, Dominguez O, Lozano J, et al. Life-Threatening Anaphylaxis to Egg and Milk Oral Immunotherapy in Asthmatic Teenagers. Ann Allergy Asthma Immunol (2014) 113(4):482–4. doi: 10.1016/j.anai.2014.07.010
100. Blumchen K, Ulbricht H, Staden U, Dobberstein K, Beschorner J, de Oliveira LC, et al. Oral Peanut Immunotherapy in Children With Peanut Anaphylaxis. J Allergy Clin Immunol (2010) 126(1):83–91 e1. doi: 10.1016/j.jaci.2010.04.030
101. Burk CM, Dellon ES, Steele PH, Virkud YV, Kulis M, Burks AW, et al. Eosinophilic Esophagitis During Peanut Oral Immunotherapy With Omalizumab. J Allergy Clin Immunol Pract (2017) 5(2):498–501. doi: 10.1016/j.jaip.2016.11.010
102. Echeverria-Zudaire LA, Fernandez-Fernandez S, Rayo-Fernandez A, Munoz-Archidona C, Checa-Rodriguez R. Primary Eosinophilic Gastrointestinal Disorders in Children Who Have Received Food Oral Immunotherapy. Allergol Immunopathol (Madr) (2016) 44(6):531–6. doi: 10.1016/j.aller.2016.05.002
103. Muraki M, Gleich GJ, Kita H. Antigen-Specific IgG and IgA, But Not IgE, Activate the Effector Functions of Eosinophils in the Presence of Antigen. Int Arch Allergy Immunol (2011) 154(2):119–27. doi: 10.1159/000320226
104. Hsieh FH. Oral Food Immunotherapy and Iatrogenic Eosinophilic Esophagitis: An Acceptable Level of Risk? Ann Allergy Asthma Immunol (2014) 113(6):581–2. doi: 10.1016/j.anai.2014.09.008
105. Romantsik O, Tosca MA, Zappettini S, Calevo MG. Oral and Sublingual Immunotherapy for Egg Allergy. Cochrane Database Syst Rev (2018) 4:CD010638. doi: 10.1002/14651858.CD010638.pub3
106. Wasserman RL, Factor JM, Baker JW, Mansfield LE, Katz Y, Hague AR, et al. Oral Immunotherapy for Peanut Allergy: Multipractice Experience With Epinephrine-Treated Reactions. J Allergy Clin Immunol Pract (2014) 2(1):91–6. doi: 10.1016/j.jaip.2013.10.001
107. Yeung JP, Kloda LA, McDevitt J, Ben-Shoshan M, Alizadehfar R. Oral Immunotherapy for Milk Allergy. Cochrane Database Syst Rev (2012) 11:CD009542. doi: 10.1002/14651858.CD009542.pub2
108. De Schryver S, Mazer B, Clarke AE, St Pierre Y, Lejtenyi D, Langlois A, et al. Adverse Events in Oral Immunotherapy for the Desensitization of Cow’s Milk Allergy in Children: A Randomized Controlled Trial. J Allergy Clin Immunol Pract (2019) 7(6):1912–9. doi: 10.1016/j.jaip.2019.02.007
109. Brandstrom J, Vetander M, Sundqvist AC, Lilja G, Johansson SGO, Melen E, et al. Individually Dosed Omalizumab Facilitates Peanut Oral Immunotherapy in Peanut Allergic Adolescents. Clin Exp Allergy (2019) 49(10):1328–41. doi: 10.1111/cea.13469
110. Balbino B, Herviou P, Godon O, Stackowicz J, Goff OR, Iannascoli B, et al. The Anti-IgE mAb Omalizumab Induces Adverse Reactions by Engaging Fcgamma Receptors. J Clin Invest (2020) 130(3):1330–5. doi: 10.1172/JCI129697
111. Vazquez-Ortiz M, Turner PJ. Improving the Safety of Oral Immunotherapy for Food Allergy. Pediatr Allergy Immunol (2016) 27(2):117–25. doi: 10.1111/pai.12510
112. Flokstra-de Blok BM, Dubois AE, Vlieg-Boerstra BJ, Oude Elberink JN, Raat H, DunnGalvin A, et al. Health-Related Quality of Life of Food Allergic Patients: Comparison With the General Population and Other Diseases. Allergy (2010) 65(2):238–44. doi: 10.1111/j.1398-9995.2009.02121.x
113. Antolin-Amerigo D, Manso L, Caminati M, de la Hoz Caballer B, Cerecedo I, Muriel A, et al. Quality of Life in Patients With Food Allergy. Clin Mol Allergy (2016) 14:4. doi: 10.1186/s12948-016-0041-4
114. Wassenberg J, Cochard MM, Dunngalvin A, Ballabeni P, Flokstra-de Blok BM, Newman CJ, et al. Parent Perceived Quality of Life is Age-Dependent in Children With Food Allergy. Pediatr Allergy Immunol (2012) 23(5):412–9. doi: 10.1111/j.1399-3038.2012.01310.x
115. Itoh-Nagato N, Inoue Y, Nagao M, Fujisawa T, Shimojo N, Iwata T, et al. Desensitization to a Whole Egg by Rush Oral Immunotherapy Improves the Quality of Life of Guardians: A Multicenter, Randomized, Parallel-Group, Delayed-Start Design Study. Allergol Int (2018) 67(2):209–16. doi: 10.1016/j.alit.2017.07.007
116. Vazquez-Ortiz M, Alvaro M, Piquer M, Dominguez O, Giner MT, Lozano J, et al. Impact of Oral Immunotherapy on Quality of Life in Egg-Allergic Children. Pediatr Allergy Immunol (2015) 26(3):291–4. doi: 10.1111/pai.12355
117. Factor JM, Mendelson L, Lee J, Nouman G, Lester MR. Effect of Oral Immunotherapy to Peanut on Food-Specific Quality of Life. Ann Allergy Asthma Immunol (2012) 109(5):348–52 e2. doi: 10.1016/j.anai.2012.08.015
118. Kukkonen AK, Uotila R, Malmberg LP, Pelkonen AS, Makela MJ. Double-Blind Placebo-Controlled Challenge Showed That Peanut Oral Immunotherapy was Effective for Severe Allergy Without Negative Effects on Airway Inflammation. Acta Paediatr (2017) 106(2):274–81. doi: 10.1111/apa.13668
119. Reier-Nilsen T, Carlsen KCL, Michelsen MM, Drottning S, Carlsen KH, Zhang C, et al. Parent and Child Perception of Quality of Life in a Randomized Controlled Peanut Oral Immunotherapy Trial. Pediatr Allergy Immunol (2019) 30(6):638–45. doi: 10.1111/pai.13066
120. Carraro S, Frigo AC, Perin M, Stefani S, Cardarelli C, Bozzetto S, et al. Impact of Oral Immunotherapy on Quality of Life in Children With Cow Milk Allergy: A Pilot Study. Int J Immunopathol Pharmacol (2012) 25(3):793–8. doi: 10.1177/039463201202500329
121. Otani IM, Begin P, Kearney C, Dominguez TL, Mehrotra A, Bacal LR, et al. Multiple-Allergen Oral Immunotherapy Improves Quality of Life in Caregivers of Food-Allergic Pediatric Subjects. Allergy Asthma Clin Immunol (2014) 10(1):25. doi: 10.1186/1710-1492-10-25
122. Epstein-Rigbi N, Goldberg MR, Levy MB, Nachshon L, Elizur A. Quality of Life of Food-Allergic Patients Before, During, and After Oral Immunotherapy. J Allergy Clin Immunol Pract (2019) 7(2):429–36 e2. doi: 10.1016/j.jaip.2018.06.016
123. Rigbi NE, Goldberg MR, Levy MB, Nachshon L, Golobov K, Elizur A. Changes in Patient Quality of Life During Oral Immunotherapy for Food Allergy. Allergy (2017) 72(12):1883–90. doi: 10.1111/all.13211
124. Epstein Rigbi N, Katz Y, Goldberg MR, Levy MB, Nachshon L, Elizur A. Patient Quality of Life Following Induction of Oral Immunotherapy for Food Allergy. Pediatr Allergy Immunol (2016) 27(3):263–8. doi: 10.1111/pai.12528
125. Arasi S, Otani IM, Klingbeil E, Begin P, Kearney C, Dominguez TL, et al. Two Year Effects of Food Allergen Immunotherapy on Quality of Life in Caregivers of Children With Food Allergies. Allergy Asthma Clin Immunol (2014) 10(1):57. doi: 10.1186/1710-1492-10-57
126. Zhong Y, Chew JL, Tan MM, Soh JY. Efficacy and Safety of Oral Immunotherapy for Peanut Allergy: A Pilot Study in Singaporean Children. Asia Pac Allergy (2019) 9(1):e1. doi: 10.5415/apallergy.2019.9.e1
127. Dunn Galvin A, McMahon S, Ponsonby AL, Hsiao KC, Tang MLK. Team Ps. The Longitudinal Impact of Probiotic and Peanut Oral Immunotherapy on Health-Related Quality of Life. Allergy (2018) 73(3):560–8. doi: 10.1111/all.13330
128. Dunn Galvin A, Hourihane JO. Psychosocial Mediators of Change and Patient Selection Factors in Oral Immunotherapy Trials. Clin Rev Allergy Immunol (2018) 55(2):217–36. doi: 10.1007/s12016-018-8700-5
129. Feuille E, Nowak-Wegrzyn A. Oral Immunotherapy for Food Allergies. Ann Nutr Metab (2016) 68 Suppl 1:19–31. doi: 10.1159/000445391
130. Saleh-Langenberg J, Goossens NJ, Flokstra-de Blok BM, Kollen BJ, van der Meulen GN, Le TM, et al. Predictors of Health-Related Quality of Life of European Food-Allergic Patients. Allergy (2015) 70(6):616–24. doi: 10.1111/all.12582
131. Pajno GB, Castagnoli R, Muraro A, Alvaro-Lozano M, Akdis CA, Akdis M, et al. Allergen Immunotherapy for IgE-Mediated Food Allergy: There is a Measure in Everything to a Proper Proportion of Therapy. Pediatr Allergy Immunol (2019) 30(4):415–22. doi: 10.1111/pai.13042
132. Logan K, Du Toit G, Giovannini M, Turcanu V, Lack G. Pediatric Allergic Diseases, Food Allergy, and Oral Tolerance. Annu Rev Cell Dev Biol (2020) 36:511–28. doi: 10.1146/annurev-cellbio-100818-125346
133. Schofield AT. A Case of Egg Poisoning. Lancet (1908) 1:716–. doi: 10.1016/S0140-6736(00)67313-0
134. Sugiura S, Kitamura K, Makino A, Matsui T, Furuta T, Takasato Y, et al. Slow Low-Dose Oral Immunotherapy: Threshold and Immunological Change. Allergol Int (2020) 69(4):601–9. doi: 10.1016/j.alit.2020.03.008
135. Nowak-Wegrzyn A, Wood RA, Nadeau KC, Pongracic JA, Henning AK, Lindblad RW, et al. Multicenter, Randomized, Double-Blind, Placebo-Controlled Clinical Trial of Vital Wheat Gluten Oral Immunotherapy. J Allergy Clin Immunol (2019) 143(2):651–61 e9. doi: 10.1016/j.jaci.2018.08.041
136. Kulmala P, Pelkonen AS, Kuitunen M, Paassilta M, Remes S, Schultz R, et al. Wheat Oral Immunotherapy was Moderately Successful But was Associated With Very Frequent Adverse Events in Children Aged 6-18 Years. Acta Paediatr (2018) 107(5):861–70. doi: 10.1111/apa.14226
137. Elizur A, Appel MY, Nachshon L, Levy MB, Epstein-Rigbi N, Pontoppidan B, et al. Walnut Oral Immunotherapy for Desensitisation of Walnut and Additional Tree Nut Allergies (Nut CRACKER): A Single-Centre, Prospective Cohort Study. Lancet Child Adolesc Health (2019) 3(5):312–21. doi: 10.1016/S2352-4642(19)30029-X
138. Langlois A, Lavergne MH, Leroux H, Killer K, Azzano P, Paradis L, et al. Protocol for a Double-Blind, Randomized Controlled Trial on the Dose-Related Efficacy of Omalizumab in Multi-Food Oral Immunotherapy. Allergy Asthma Clin Immunol (2020) 16:25. doi: 10.1186/s13223-020-00419-z
139. Eapen AA, Lavery WJ, Siddiqui JS, Lierl MB. Oral Immunotherapy for Multiple Foods in a Pediatric Allergy Clinic Setting. Ann Allergy Asthma Immunol (2019) 123(6):573–81.e3. doi: 10.1016/j.anai.2019.08.463
140. Virkud YV, Wang J, Shreffler WG. Enhancing the Safety and Efficacy of Food Allergy Immunotherapy: A Review of Adjunctive Therapies. Clin Rev Allergy Immunol (2018) 55(2):172–89. doi: 10.1007/s12016-018-8694-z
141. Labrosse R, Graham F, Des Roches A, Begin P. The Use of Omalizumab in Food Oral Immunotherapy. Arch Immunol Ther Exp (Warsz) (2017) 65(3):189–99. doi: 10.1007/s00005-016-0420-z
142. Fiocchi A, Artesani MC, Riccardi C, Mennini M, Pecora V, Fierro V, et al. Impact of Omalizumab on Food Allergy in Patients Treated for Asthma: A Real-Life Study. J Allergy Clin Immunol Pract (2019) 7(6):1901–9 e5. doi: 10.1016/j.jaip.2019.01.023
143. Abdel-Gadir A, Schneider L, Casini A, Charbonnier LM, Little SV, Harrington T, et al. Oral Immunotherapy With Omalizumab Reverses the Th2 Cell-Like Programme of Regulatory T Cells and Restores Their Function. Clin Exp Allergy (2018) 48(7):825–36. doi: 10.1111/cea.13161
144. Soller L, Abrams EM, Carr S, Kapur S, Rex GA, Leo S, et al. First Real-World Safety Analysis of Preschool Peanut Oral Immunotherapy. J Allergy Clin Immunol Pract (2019) 7(8):2759–67 e5. doi: 10.1016/j.jaip.2019.04.010
145. Bird JA, Spergel JM, Jones SM, Rachid R, Assa’ad AH, Wang J, et al. Efficacy and Safety of AR101 in Oral Immunotherapy for Peanut Allergy: Results of ARC001, a Randomized, Double-Blind, Placebo-Controlled Phase 2 Clinical Trial. J Allergy Clin Immunol Pract (2018) 6(2):476–85.e3. doi: 10.1016/j.jaip.2017.09.016
146. Varshney P, Jones SM, Scurlock AM, Perry TT, Kemper A, Steele P, et al. A Randomized Controlled Study of Peanut Oral Immunotherapy: Clinical Desensitization and Modulation of the Allergic Response. J Allergy Clin Immunol (2011) 127(3):654–60. doi: 10.1016/j.jaci.2010.12.1111
147. Narisety SD, Frischmeyer-Guerrerio PA, Keet CA, Gorelik M, Schroeder J, Hamilton RG, et al. A Randomized, Double-Blind, Placebo-Controlled Pilot Study of Sublingual Versus Oral Immunotherapy for the Treatment of Peanut Allergy. J Allergy Clin Immunol (2015) 135(5):1275–82.e1-6. doi: 10.1016/j.jaci.2014.11.005
148. Chinthrajah RS, Purington N, Andorf S, Long A, O’Laughlin KL, Lyu SC, et al. Sustained Outcomes in Oral Immunotherapy for Peanut Allergy (POISED Study): A Large, Randomised, Double-Blind, Placebo-Controlled, Phase 2 Study. Lancet (2019) 394(10207):1437–49. doi: 10.1016/S0140-6736(19)31793-3
149. Nagakura KI, Yanagida N, Sato S, Nishino M, Asaumi T, Ogura K, et al. Low-Dose Oral Immunotherapy for Children With Anaphylactic Peanut Allergy in Japan. Pediatr Allergy Immunol (2018) 29(5):512–8. doi: 10.1111/pai.12898
150. Shaker M, Greenhawt M. Providing Cost-Effective Care for Food Allergy. Ann Allergy Asthma Immunol (2019) 123(3):240–8 e1. doi: 10.1016/j.anai.2019.05.015
Keywords: food allergy, oral immunotherapy, IgE, reaction, anaphylaxis, pediatrics
Citation: Mori F, Giovannini M, Barni S, Jiménez-Saiz R, Munblit D, Biagioni B, Liccioli G, Sarti L, Liotti L, Ricci S, Novembre E, Sahiner U, Baldo E and Caimmi D (2021) Oral Immunotherapy for Food-Allergic Children: A Pro-Con Debate. Front. Immunol. 12:636612. doi: 10.3389/fimmu.2021.636612
Received: 01 December 2020; Accepted: 03 September 2021;
Published: 28 September 2021.
Edited by:
Kenneth Beaman, Rosalind, alind Franklin University of Medicine and Science, United StatesReviewed by:
Alice Gilman-Sachs, Rosalind Franklin University of Medicine and Science, United StatesCopyright © 2021 Mori, Giovannini, Barni, Jiménez-Saiz, Munblit, Biagioni, Liccioli, Sarti, Liotti, Ricci, Novembre, Sahiner, Baldo and Caimmi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mattia Giovannini, bWF0dGlhZzg4QGhvdG1haWwuaXQ=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.