
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Immunol., 17 February 2021
Sec. Viral Immunology
Volume 12 - 2021 | https://doi.org/10.3389/fimmu.2021.632119
This article is part of the Research TopicImmune Evasion Mechanisms by RNA VirusesView all 32 articles
 Yang Zhang1,2,3†
Yang Zhang1,2,3† Taiyi Jiang1†
Taiyi Jiang1† Aixin Li1†
Aixin Li1† Zhen Li1,2
Zhen Li1,2 Jianhua Hou1,2Meixia Gao1Xiaojie Huang1
Jianhua Hou1,2Meixia Gao1Xiaojie Huang1 Bin Su1,2Hao Wu1,2*Tong Zhang1,2*
Bin Su1,2Hao Wu1,2*Tong Zhang1,2* Wei Jiang3,4*
Wei Jiang3,4*Background: HIV infection results in immune homeostasis perturbations, which is characterized by CD4+ T-cell depletion, immune activation, and inflammation. Effective antiretroviral therapy (ART) does not fully restore immunologic and clinical health in people living with HIV (PLWH). Various drugs have been used to improve their immune status and CD4+ T-cell counts, but no measures have been tested effective. Here we conduct a systematic review and meta-analysis of existing clinical studies on improving CD4+ T-cell count while decreasing inflammation and immune activation.
Methods: We retrieved possible relevant publications from a total of five electronic databases and selected eligible studies, which dealt with outcomes of medical therapy for CD4+ T-cell count recovery, inflammation, and immune activation with or without ART. We paid particular attention to immunologic non-responders with a favorable treatment regimen.
Results: Thirty-three articles were included in the systematic review and meta-analysis. However, there were no safe and effective medications specific for improving CD4+ T-cell reconstitution. The immunological benefits or adverse events mainly depend on the safety, dosage, and duration of the candidate medication use, as well as whether it is combined with ART.
Conclusion: Under the “safe, combined, adequate and long (SCAL)” principles, alternative approaches are needed to accelerate the recovery of CD4+ T-cells, and to prevent adverse long-term outcomes in PLWH with standard ART treatment.
Since 1996, the morbidity and mortality of HIV-related diseases were dramatically declined by the wide use of antiretroviral therapy (ART) (1). ART is a standardized combination of several anti-HIV drugs (1), being classified as etiological therapy. Theoretically, treatment-experienced people living with HIV (PLWH) persistently suppress the HIV viral load, and their CD4+ T-cell counts increase gradually. However, PLWH fail to achieve normalization of CD4+ T-cell counts despite persistent blood virological suppression, especially in immunological non-responder (INR, usually defined as PLWH under ART with viremia and CD4+ T-cell counts < 350/μl in the blood) showing severe immunological dysfunction (2). This immunological dysfunction involves chronic immune activation and systemic inflammation (3), and is thought to contribute not only to HIV disease progression, but also to mortality and emerging non-AIDS morbidity (4, 5). To date, there is still a lack of effective adjunct medical therapy to further enhance CD4+ T-cell counts for PLWH, including INRs.
For over two decades, researchers have tested multiple medication candidates to recover CD4+ T-cell count. Montaner et al. have assessed the effect of hydroxyurea in PLWH in 1997; However, the CD4+ T-cell counts did not change significantly; or even significantly decreased during the washout phase (6). Because the level of immune activation and inflammation were independently associated with the subsequent rate of CD4+ T-cell losses (7, 8), the immunomodulators or immunosuppressants such as glucocorticoid (9) and cyclosporine (10), may be beneficial to PLWH or INRs. In recent years, PLWH may have more benefits by “early treatment” (11), and they will not go through the process from immunological destruction to reconstruction, which means that INRs may be fewer and fewer. However, although their CD4+ T-cell count was high, it did not reach normalization (1). Besides, ART does not eliminate inflammation and immune activation (4, 5), so researchers have paid more attention to other traditionally non-AIDS-related morbidities (12, 13). In other words, hypertension, hyperglycemia, and hyperlipidemia may be similar to the low CD4+ T-cell count, which may be the adverse consequences of inflammation and immune activation. Besides, some candidate drugs also show anti-inflammatory and inhibitory effects on excessive immune activation in the general population. Take rosuvastatin (14) and sitagliptin (15) as examples, scientists hypothesized that the CD4+ T-cell recovery over time could be explained by the improved use of non-HIV-specific preventive interventions. Unfortunately, even though some candidates could reduce immune activation or chronic inflammation to varying degrees, they cannot directly increase CD4+ T-cell count recovery, and the mechanisms underlying these candidates are far from known.
Therefore, we searched and summarized the literature on the case-control study of medication-assisted treatment of CD4+ T-cell count recovery. The second aim was to summarize biomarkers of inflammation and immune activation in PLWH. An intervention that decreased immune activation or inflammation or both in PLWH might therefore be beneficial. Besides, for CD4+ T-cell count recovery in INRs, we separately analyzed articles related to incomplete immune reconstitution in PLWHs. We hope to put forward the therapeutic principle of adjunct therapy for CD4+ T-cell recovery, and provide a basis for further searching for an inexpensive, safe, and well-tolerated candidate intervention.
The protocol in this study has been deposited and registered in the PROSPERO database (CRD42020210393).
Adult PLWH with or without ART.
Any auxiliary medicine treatment in junction with or without ART, but not including inaccurate dose or non-drug treatment studies (e.g., immunotherapy and cell therapy).
PLWH with or without ART + adjunct treatment vs. PLWH with or without ART (placebo or blank control).
Searches were limited to data published before February 29, 2020 using a combination of population-related terms (HIV OR AIDS), immunology-related terms (“immune reconstitution” OR “CD4+ T-cell recovery”), and treatment-related terms (treatment OR therapy). All searches were limited to peer-reviewed journal articles in English.
Comprehensive searches were conducted in PubMed, Web of Science, and Cochrane library. Besides, Google Scholar and GeenMedical were used as supplementary sources.
We included [1] studies conducted in PLWH; [2] any auxiliary medicine treatment in junction with or without ART treatment; [3] studies with at least two groups (adjunct therapy group vs. control group) including randomized controlled trials (RCT) and non-RCTs; (4) the results of the research which should include the CD4+ T-cell count; and (5) articles were written in English and excluded those studies without peer-review process, case reports, theoretic studies, conference abstracts and samples overlapped with the other included studies. We also excluded studies that did not include accurate doses (e.g., probiotics/prebiotics, fish oil, and chocolate) and non-drug treatment studies (e.g., immunotherapy and cell therapy). Two authors (Yang Zhang and Taiyi Jiang) used an Excel spreadsheet to independently screen for eligibility.
Two authors (Yang Zhang and Jianhua Hou) used an Excel spreadsheet to independently extract data from each study. The opinions on the included data were resolved by consensus after consulting a 3rd reviewer (Aixin Li). The summary statistics of each outcome were means, standard deviations (SD), and the number of participants. We also coded the mean change and SD of mean change if necessary. Related information from other studies was coded for use as well.
We considered using meta-analytical methods when three or more studies with the same treatment, or systematic review was used to summarize the results.
For the meta-analysis, random-effect models were adopted to estimate the pooled estimation of effect sizes. The variation in effect sizes across studies was assessed by the Cochrane Q with a threshold of P < 0.1. The I2 statistic was calculated to estimate the proportion of true heterogeneity in observed variance. The funnel plot and Egger's regression intercept test were used to estimate publication bias. If the P-value for Egger's test is larger than 0.1, publication bias exists, and we should draw cautious conclusions. Besides, we calculated Egger's test only if three or more comparisons are included in specific outcomes.
For the systematic review, we grouped our results classified by types of treatment. The outcomes of interest were changes in CD4+ T-cell count, viral load, other immune system biomarkers such as inflammation or immune activation, and medical side effects.
Our literature searches returned 29,556 records, including 11,263 in the web of science, 7,293 in Pubmed, and 11,000 in Embase. After duplicates removal, 15,521 studies were remained. Of these, 14,447 were excluded during the title and abstract screening, leaving 174 publications for full-text evaluation. Of these, 141 were excluded for various reasons after full-text review, as detailed in the flow chart. Thirty-three studies were included in the final review (Figure 1, Table 1).
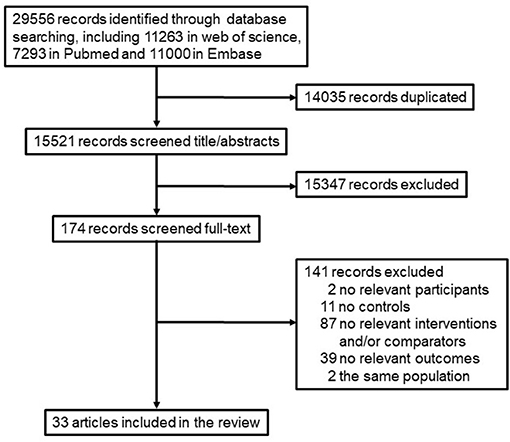
Figure 1. A flow diagram of the studies retrieved for the review.
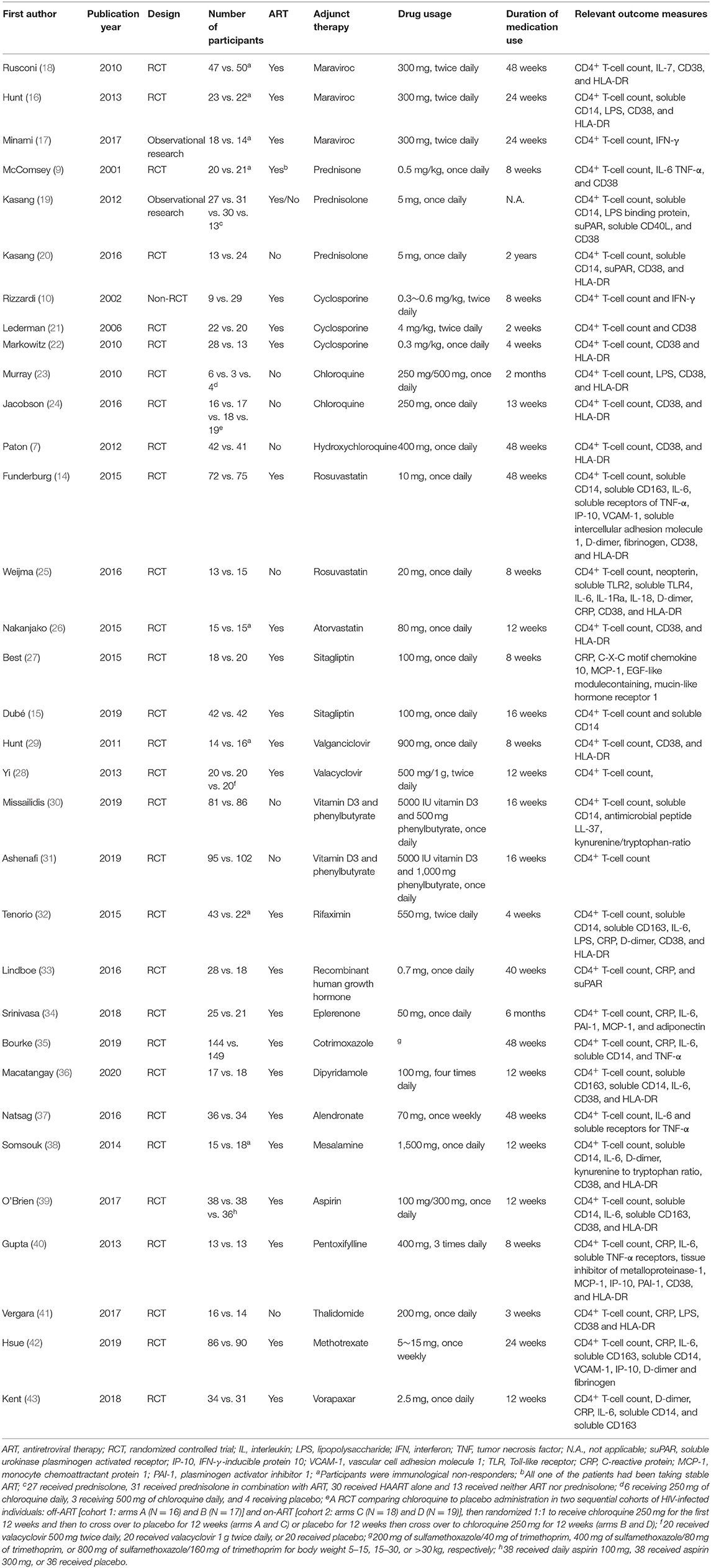
Table 1. Characteristic of included articles.
Among 33 studies, one study was a non-randomized intervention study, two were observational studies, and others were RCTs. Regarding ART, 30 studies used ART in combination with these auxiliary treatments. In addition, the visit period for all studies ranged from 3 to 48 weeks. The reported outcomes included CD4+ T-cell count, viral load, inflammation biomarkers, and medical side effects. The detailed information of each treatment was reviewed and summarized below.
The CC chemokine receptor type 5 inhibitor maraviroc has been hypothesized to decrease T-cell activation in PLWH (16), and associated with an enhanced CD4+ T-cell response independent of virological suppression (17). Two RCTs (16, 18) and one observational study (17) reported the effects of maraviroc on CD4+ T-cell counts. The pooled estimate of effects on CD4+ T-cell count was 0.184, 95% CI 0.13 ~ 0.499, p = 0.254, Figure 2. The heterogeneity across studies was not significant and small [Q(2) = 2.153, p = 0.341, I2 = 7.122%]. The publication bias was not significant (Intercept = 2.177, p = 0.57).
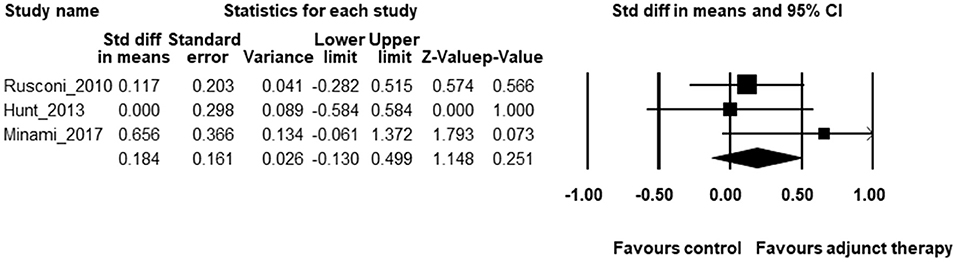
Figure 2. The forest plot for the effects of maraviroc on CD4+ T-cell counts.
Unexpectedly, Hunt et al. found that compared with the placebo group, maraviroc-treated patients with ART experienced a tremendous median increase in CD38+HLA-DR+CD8+ T cells (16). Furthermore, Rusconi et al. also reported that PLWH accepted maraviroc showed higher levels of HLA-DR+CD38+CD8+ T cells as compared to those without maraviroc (18). These studies suggest that maraviroc does not effectively reduce immune activation, at least in INRs.
McComsey et al. reported a double-blinded RCT of prednisone in 41 patients (40 with ART) with HIV-1 infection (9). They found that 8 weeks of prednisone administration is reasonably safe in advanced HIV-1 disease, and decreases immune activation (tumor necrosis factor α levels and percentages of CD38+CD8+ T cells). However, there was no effect on HIV-1 RNA levels or CD4+ T-cell count.
An observational study demonstrates that although PLWH without ART-treated with low-dose prednisolone display significantly lower general immune activation, prednisolone was not beneficial to CD4+ T-cell recovery and viral load controls (19). In double-blinded RCT, prednisolone could increase the odds of CD4+ T-cell count recovery as well as decrease immune activation and increase HIV viral load (20). These studies have shown that, without the escort of ART, the benefits of glucocorticoids on CD4+ T-cell reconstitution and the risk of viral activation may coexist.
An RCT evaluating the immune-modulating effects of combining cyclosporine treatment with ART during primary HIV-1 infection has shown that the net increase over baseline values in both CD4+ T-cell count and CD4/CD8 ratio was significantly greater in PLWH receiving cyclosporine in combination with ART than those receiving ART alone (10). However, two other cyclosporine RCTs have shown no significant differences between treatment arms in levels of CD4+ T-cell counts (21, 22). Interestingly, treatment with cyclosporin A (4 mg/kg, bid) for 2 weeks provided only a transient enhancement in circulating CD4+ T-cell restoration (21). However, adjunctive therapy with cyclosporine (0.3 mg/kg, qd) even for 4 weeks did not provide apparent virologic or immunologic benefits (22), suggesting that adequate doses of cyclosporine are needed to suppress immune activation.
Three RCTs have tested the effects of chloroquine and its derivatives on CD4+ T-cell counts in PLWH. One double-blind RCT indicated that treatment with chloroquine could reduce the systemic T-cell immune activation in participants without ART, but they did not report CD4+ T-cell counts and viral load (23). Another double-blind RCT in PLWH off and on ART demonstrated no significant differences in the changes of CD4+ T-cell counts between the chloroquine arm and the placebo arm in either cohort (24). However, chloroquine modestly reduced the proportions of CD8+T cells co-expressing CD38 and HLA-DR in ART-treated HIV-infected participants. In contrast, this effect on immune activation was not found in the off-ART group during chloroquine use. This study showed that even if chloroquine could not increase CD4+ T-cell count, it should be combined with ART to reduce immune activation in PLWH.
Moreover, a double-blind RCT performed in the United Kingdom indicated that among HIV-infected patients not taking ART, hydroxychloroquine compared with placebo did not reduce CD8+ T cell activation, but did significantly decrease CD4+ T-cell count and increase HIV-RNA replication (7). These studies indicated that adjuvant treatments with immune modulators to increase CD4+ T-cell count should consider the combination with ART. Otherwise, it would bring about the risk of increased HIV replication and even further the decline of CD4+ T-cell counts.
Statins, or 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors, have anti-inflammatory effects, licensed and widely marketed for the treatment of dyslipidemia (14). There are two RCTs on rosuvastatin and one RCT on atorvastatin involving statins in PLWH, which indicated that statins could not increase CD4+ T-cell counts in PLWH on ART. However, rosuvastatin may significantly reduce several inflammatory markers, and lymphocyte and monocyte activation in ART-treated subjects in a 48-week follow up (14) rather than 8-weeks (25). Besides, atorvastatin could also reduce the T-cell immune activation among ART-experienced adults in a 24-week study (26). These studies have shown that statins are needed for a long period to reduce immune activation and inflammation among PLWH.
Dipeptidyl peptidase-4 inhibitors (e.g., sitagliptin) are a relatively new class of oral antidiabetes medications. In animal models and clinical studies of type 2 diabetes, dipeptidyl peptidase-4 inhibitors appear to have many cardiometabolic, anti-inflammatory, and immunoregulatory benefits in addition to their glucoregulatory actions (15). Both 8 (27) and 16 weeks (15) of sitagliptin had pleiotropic anti-inflammatory and immune regulatory effects in PLWH during ART. However, there were no significant between-arm differences in CD4+ T-cell counts.
Herpes simplex virus type 2 is a common HIV coinfection, contributing to the increased systematic inflammation and immune activation despite suppressive ART (28). Either RCTs of anti-herpes simplex virus medication valganciclovir (29) or valacyclovir (28) could not increase CD4+ T-cell counts in PLWH. Still, valganciclovir-treated participants had a significantly greater reduction in CD8+ T-cell activation than those from the placebo group, which was not observed in the study of valacyclovir.
Poor nutritional status is common among PLWH (30, 31). Vitamin D3 and phenylbutyrate possess pleiotropic immunomodulatory functions that could simultaneously prevent chronic immune activation and dysregulation (30, 31). Two double-blinded RCTs in treatment-naive HIV patients indicated that daily nutritional supplementation with Vitamin D3 and phenylbutyrate could not change the viral load, CD4+ T-cell counts, and levels of inflammation (30, 31).
Some candidates were conducted in one RCT, which was demonstrated the anti-inflammatory and immunomodulatory effects by rifaximin (32), recombinant human growth hormone (33), eplerenone (34), cotrimoxazole (35), and dipyridamole (36) decreased immune activation significantly among persons with HIV-1 infection receiving ART. Further studies are necessary to uncover the clinical potential of these candidates on CD4+ T-cell count recovery in PLWH.
However, HIV-associated changes of CD4+ T-cell counts and immune activation are not impacted by alendronate (37), mesalamine (38), and aspirin (39). More frustratingly, the pentoxifylline (40), thalidomide (41), methotrexate (42), and vorapaxar (43) had no benefits on immune activation, inflammation, and CD4+ T-cell count recovery in PLWH receiving ART but at risk of poor outcomes.
There are eight studies on INRs in the above research. For maraviroc, only one study proved that maraviroc could increase the CD4+ T-cell counts (17). One study reported that maraviroc could reduce inflammation (18), but another study showed that maraviroc increased immune activation (16). However, two studies showed that maraviroc has serious adverse events (17, 18).
For the other five candidates, which were only conducted in one study, prednisone (9), valganciclovir (29), atorvastatin (26), and rifaximin (32) have all been reported to reduce inflammation and immune activation to varying degrees, except for mesalamine (38). As expected, prednisone has been reported more adverse events (9).
HIV is associated with increased systematic inflammation and immune activation that persist despite suppressive ART (44). The elevated immune activation and inflammation are associated with an increased risk of non-AIDS diseases and mortality among PLWH (12, 13). While ART reduces the level of inflammatory biomarkers, it does not result in normalization of CD4+ T-cell counts and host immunity (45). Interventions reducing immune activation request a deep understanding of pathogenesis and a balance thought of therapeutic benefit or side effects. In this systematic review, only maraviroc can be used for meta-analysis. However, maraviroc does not significantly increase the CD4+ T-cell counts of INR. Moreover, most of the included studies have shown that the maraviroc and other target drugs could reduce inflammation or immune activation based on different biomarkers. Besides, we have also evaluated the safety of candidates, especially in HIV load and CD4+ T-cell counts. In general, there is no well-established adjunct therapy to increase CD4+ T-cell counts.
In this systematic review and meta-analysis, the use of research drugs that bring immunological benefits in PLWH usually has the following characteristics, which may also be the principle of searching for ideal candidates in the future. First, this clinical study design should be based on the combined ART (i.e., principle “combined”). Hydroxychloroquine (7) and thalidomide (41) did not reduce inflammation and immune activation without ART, but led to a greater decline in CD4+ T-cell counts and an increase in viral replication. In contrast, even if other studies did not bring immunological or virological benefits, or even showed the adverse effects of the candidate drug, the candidates combined with ART would not lead to the poor outcomes such as a decrease in CD4+ T-cell counts or an increase in HIV RNA load.
Second, the preexisting immune system abnormalities in the setting of HIV infection may overpower the immunomodulatory effects of the overwhelming majority of candidates (3). Moreover, ART, low-level HIV replication, microbial translocation across damaged mucosal surfaces, and chronic coinfections may contribute to persistent inflammation during influential virologic ART (4, 5). Accordingly, an adequate dose for an extended period of candidate interventions is needed to moderate them (i.e., principle “adequate” and “long”). Two cyclosporine studies indicated that adequate cyclosporine doses (21) could suppress immune activation rather than fewer doses (22). Besides, insufficient use of a loading vorapaxar dose in PLWH may not achieve the general effect, as some cardiovascular studies have shown (43). Similarly, the 48-week treatment of rosuvastatin (13) may significantly reduce immune activation and inflammation among PLWH in the 8-week study (7).
Finally, immune activation and inflammation persist in most ART-suppressed PLWH (5). Therefore, reducing persistent immune activation has emerged as a major priority (4). Considering the principles of “combined, adequate and long,” as well as drug interaction with ART, evidently and most importantly, a “safe” intervention that suppresses immune activation and increases CD4+ T-cell counts would be attractive. Our review indicated that the vast majority of candidates above might not be studied further as a treatment to increase the CD4+ T-cell counts in PLWH. Therefore, we propose the four principles of adjunct therapy for CD4+ T-cell recovery in PLWH, namely the “SCAL” principles of safe, combined, adequate, and long. Maybe existing proven interventions in HIV-negative populations to modify inflammation and immune activation risks remain the best available methods to reduce non-AIDS disease in PLWH.
So how do we screen drug candidates to increase CD4+ T-cell counts of PLWH? Much has been learnt about candidates since assessing the effect on hydroxyurea in PLWH in 1997 (6). Although the exact proinflammatory mechanisms are unclear, interventions that reduce inflammation and immune activation are believed to reduce non-AIDS disease risk in PLWH (4, 5). Bioinformatics technology should be used to explore the potential differences in the immune system between PLWH and healthy controllers, especially in INRs. Next, chemoinformatics could be further used to match candidates that meet the “SCAL” principles, just like scientists' outstanding performance during the SARS-CoV-2 epidemic (46). Given the potential for complex and unpredictable effects, interventions for immune activation and CD4+ T-cell recovery must be evaluated rigorously and comprehensively in adequately powered randomized controlled trials. Also, in the context of fully suppressive ART, multifarious immunotherapeutic approaches such as vaccines or cytokines (47), dietary supplements (48), might further reduce immune activation, and improve CD4+ T-cell count in PLWH. However, because the intervention was difficult to standardize or the number of subjects was small, the safety and effectiveness of these methods need to be further verified.
The use of different biomarkers in this included literature above might miss biological effects with the potential for clinical importance. Still, it is much more efficient than devoting the resources for CD4+ T-cell count recovery as a clinical endpoint study. Besides, we focused on individuals with incomplete CD4+ T-cell count recovery. They tend to have the higher persistent immune activation levels and are at the highest risk for morbidity and mortality. However, despite a large number of candidates, few studies adopt the control group, so we didn't include these studies, which also excluded the effect of the slow increase in CD4+ T-cell count among PLWH or INR.
To date, there are no safe and effective medications specific to improving CD4+ T-cell reconstitution. There are still considerable challenges in the adjuvant treatment of CD4+ T-cell count recovery, as well as the interventions of inflammation and immune activation. The immunological benefits or adverse events mainly depend on the safety, dosage, and duration of the candidate medication use, and whether it is combined with ART. Therefore, we propose the four principles of the “SCAL” principles. Under the guidance of “SCAL” principles, it is necessary to develop effective drugs and design rigorous clinical trials to verify in PLWH treated with standard ART in the future.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
YZ, TJ, AL, HW, TZ, and WJ had full access to all of the data in the study and are responsible for the integrity of data and the accuracy of data analysis. YZ, HW, TZ, and WJ study concept and design. YZ, TJ, AL, JH, and MG acquisition, analysis, and interpretation of data. YZ, TJ, and AL drafting the manuscript. ZL, XH, BS, HW, TZ, and WJ critical revision of the manuscript for important intellectual content. YZ, ZL, XH, BS, HW, TZ, and WJ obtained funding. YZ, HW, TZ, and WJ study supervision. All of the authors gave the publishing approval.
This work was supported by the National Natural Science Foundation of China (NSFC)-NIH Biomedical collaborative research program (81761128001 to HW), the NSFC (81772165 and 81974303 to BS, 81901089 to YZ, 82072271 to TZ, 82072294 to ZL), the National Institutes of Allergy and Infectious Diseases (AI128864 to WJ), the China Postdoctoral Science Foundation (2019M660718 to YZ), the Chinese Government under the 13th Five-Year Plan (2017ZX10202101 to TZ, 2018ZX10301 to ZL), the Major Project of Beijing Municipal Science and Technology Committee (D161100000416003 to HW), the Beijing International Postdoctoral Exchange Fellowship Program (2019PC-11 to YZ), the Peak Talent Program of Beijing Hospital Authority (DFL20191701 to TZ), the Beijing Excellent Talent Plan (2018000021223ZK04 to XH), the Beijing Key Laboratory for HIV/AIDS Research (BZ0089) and the Open Project funded by Beijing Key Laboratory of HIV/AIDS Research (BJYAHKF2019001 to YZ).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Fauci AS, Lane HC. Four decades of HIV/AIDS - much accomplished, much to do. N Engl J Med. (2020) 383:1–4. doi: 10.1056/NEJMp1916753
2. Yang X, Su B, Zhang X, Liu Y, Wu H, Zhang T. Incomplete immune reconstitution in HIV/AIDS patients on antiretroviral therapy: challenges of immunological non-responders. J Leukoc Biol. :10.1002. doi: 10.1002/JLB.4MR1019-189R
3. Kuller LH, Tracy R, Belloso W, De Wit S, Drummond F, Lane HC, et al. Inflammatory and coagulation biomarkers and mortality in patients with HIV infection. PLoS Med. (2008) 5:e203. doi: 10.1371/journal.pmed.0050203
4. Smith CJ, Ryom L, Weber R, Morlat P, Pradier C, Reiss P, et al. Trends in underlying causes of death in people with HIV from 1999 to 2011 (D:A:D): a multicohort collaboration. Lancet. (2014) 384:241–8. doi: 10.1016/S0140-6736(14)60604-8
5. Lebrun D, Hentzien M, Cuzin L, Rey D, Joly V, Cotte L, et al. Epidemiology of autoimmune and inflammatory diseases in a French nationwide HIV cohort. Aids. (2017) 31:2159–66. doi: 10.1097/QAD.0000000000001603
6. Montaner JS, Zala C, Conway B, Raboud J, Patenaude P, Rae S, et al. A pilot study of hydroxyurea among patients with advanced human immunodeficiency virus (HIV) disease receiving chronic didanosine therapy: Canadian HIV trials network protocol 080. J Infect Dis. (1997) 175:801–6. doi: 10.1086/513974
7. Paton NI, Goodall RL, Dunn DT, Franzen S, Collaco-Moraes Y, Gazzard BG, et al. Effects of hydroxychloroquine on immune activation and disease progression among hiv-infected patients not receiving antiretroviral therapy a randomized controlled trial. JAMA-J Am Med Assoc. (2012) 308:353–61. doi: 10.1001/jama.2012.6936
8. Deeks SG, Kitchen CMR, Liu L, Guo H, Gascon R, Narváez AB, et al. Immune activation set point during early HIV infection predicts subsequent CD4+ T-cell changes independent of viral load. Blood. (2004) 104:942–7. doi: 10.1182/blood-2003-09-3333
9. McComsey GA, Whalen CC, Mawhorter SD, Asaad R, Valdez H, Patki AH, et al. Placebo-controlled trial of prednisone in advanced HIV-1 infection. AIDS. (2001) 15:321–7. doi: 10.1097/00002030-200102160-00004
10. Rizzardi GP, Harari A, Capiluppi B, Tambussi G, Ellefsen K, Ciuffreda D, et al. Treatment of primary HIV-1 infection with cyclosporin A coupled with highly active antiretroviral therapy. J Clin Invest. (2002) 109:681–8. doi: 10.1172/JCI14522
11. Song AX, Liu XC, Huang XJ, Meyers K, Oh DY, Hou JH, et al. From CD4-based initiation to treating all HIV-infected adults immediately: an evidence-based meta-analysis. Front Immunol. (2018) 9:212. doi: 10.3389/Fimmu.2018.00212
12. Hsue PY, Scherzer R, Hunt PW, Schnell A, Bolger AF, Kalapus SC, et al. Carotid intima-media thickness progression in HIV-infected adults occurs preferentially at the carotid bifurcation and is predicted by inflammation. J Am Heart Assoc. (2012) 1:jah3-e000422. doi: 10.1161/JAHA.111.000422
13. Lazarus JV, Safreed-Harmon K, Barton SE, Costagliola D, Dedes N, Del Amo Valero J, et al. Beyond viral suppression of HIV - the new quality of life frontier. BMC Med. (2016) 14:94. doi: 10.1186/s12916-016-0640-4
14. Funderburg NT, Jiang Y, Debanne SM, Labbato D, Juchnowski S, Ferrari B, et al. Rosuvastatin reduces vascular inflammation and T-cell and monocyte activation in HIV-infected subjects on antiretroviral therapy. J Acquir Immune Defic Syndr. (2015) 68:396–404. doi: 10.1097/QAI.0000000000000478
15. Dubé MP, Chan ES, Lake JE, Williams B, Kinslow J, Landay A, et al. A randomized, double-blinded, placebo-controlled trial of sitagliptin for reducing inflammation and immune activation in treated and suppressed human immunodeficiency virus infection. Clin Infect Dis. (2019) 69:1165–72. doi: 10.1093/cid/ciy1051
16. Hunt PW, Shulman NS, Hayes TL, Dahl V, Somsouk M, Funderburg NT, et al. The immunologic effects of maraviroc intensification in treated HIV-infected individuals with incomplete CD4+ T-cell recovery: a randomized trial. Blood. (2013) 121:4635–46. doi: 10.1182/blood-2012-06-436345
17. Minami R, Takahama S, Kaku Y, Yamamoto M. Addition of maraviroc to antiretroviral therapy decreased interferon-γ mRNA in the CD4+ T cells of patients with suboptimal CD4+ T-cell recovery. J Infect Chemother. (2017) 23:29–34. doi: 10.1016/j.jiac.2016.09.003
18. Rusconi S, Vitiello P, Adorni F, Colella E, Focà E, Capetti AF, et al. Maraviroc intensification for HIV-1-positive immunological non-responders (INRs) despite virological suppression during HAART. J Int AIDS Soc. (2010) 13:044. doi: 10.1186/1758-2652-13-S4-O44
19. Kasang C, Ulmer A, Donhauser N, Schmidt B, Stich A, Klinker H, et al. HIV patients treated with low-dose prednisolone exhibit lower immune activation than untreated patients. BMC Infect Dis. (2012) 2012:14. doi: 10.1186/1471-2334-12-14
20. Kasang C, Kalluvya S, Majinge C, Kongola G, Mlewa M, Massawe I, et al. Effects of prednisolone on disease progression in antiretroviral-untreated HIV infection: A 2-year randomized, double-blind placebo-controlled clinical trial. PLoS ONE. (2016) 11:e0146678-e. doi: 10.1371/journal.pone.0146678
21. Lederman MM, Smeaton L, Smith KY, Rodriguez B, Pu M, Wang H, et al. Cyclosporin A provides no sustained immunologic benefit to persons with chronic HIV-1 infection starting suppressive antiretroviral therapy: results of a randomized, controlled trial of the AIDS clinical trials group A5138. J Infect Dis. (2006) 194:1677–85. doi: 10.1086/509261
22. Markowitz M, Vaida F, Hare CB, Boden D, Mohri H, Hecht FM, et al. The virologic and immunologic effects of cyclosporine as an adjunct to antiretroviral therapy in patients treated during acute and early HIV-1 infection. J Infect Dis. (2010) 201:1298–302. doi: 10.1086/651664
23. Murray SM, Down CM, Boulware DR, Stauffer WM, Cavert WP, Schacker TW, et al. Reduction of immune activation with chloroquine therapy during chronic HIV infection. J Virol. (2010) 84:12082–6. doi: 10.1128/JVI.01466–10
24. Jacobson JM, Bosinger SE, Kang M, Belaunzaran-Zamudio P, Matining RM, Wilson CC, et al. The effect of chloroquine on immune activation and interferon signatures associated with HIV-1. AIDS Res Hum Retroviruses. (2016) 32:636–47. doi: 10.1089/AID.2015.0336
25. Weijma RGM, Vos ERA, Ten Oever J, Van Schilfgaarde M, Dijksman LM, Van der Ven A, et al. The effect of rosuvastatin on markers of immune activation in treatment-naive human immunodeficiency virus-patients. Open Forum Infect Dis. (2016) 3:ofv201. doi: 10.1093/ofid/ofv201
26. Nakanjako D, Ssinabulya I, Nabatanzi R, Bayigga L, Kiragga A, Joloba M, et al. Atorvastatin reduces T-cell activation and exhaustion among HIV-infected cART-treated suboptimal immune responders in Uganda: a randomised crossover placebo-controlled trial. Trop Med Int Health. (2015) 20:380–90. doi: 10.1111/tmi.12442
27. Best C, Struthers H, Laciny E, Royal M, Reeds DN, Yarasheski KE. Sitagliptin reduces inflammation and chronic immune cell activation in HIV+ adults with impaired glucose tolerance. J Clin Endocrinol Metab. (2015) 100:2621–9. doi: 10.1210/jc.2015-1531
28. Yi TJ, Walmsley S, Szadkowski L, Raboud J, Rajwans N, Shannon B, et al. A randomized controlled pilot trial of valacyclovir for attenuating inflammation and immune activation in hiv/herpes simplex virus 2-coinfected adults on suppressive antiretroviral therapy. Clin Infect Dis. (2013) 57:1331–8. doi: 10.1093/cid/cit539
29. Hunt PW, Martin JN, Sinclair E, Epling L, Teague J, Jacobson MA, et al. Valganciclovir reduces T cell activation in HIV-infected Individuals with Incomplete CD4(+) T cell recovery on antiretroviral therapy. J Infect Dis. (2011) 203:1474–83. doi: 10.1093/infdis/jir060
30. Missailidis C, Sørensen N, Ashenafi S, Amogne W, Kassa E, Bekele A, et al. Vitamin D and phenylbutyrate supplementation does not modulate gut derived immune activation in HIV-1. Nutrients. (2019) 11:1675. doi: 10.3390/nu11071675
31. Ashenafi S, Amogne W, Kassa E, Gebreselassie N, Bekele A, Aseffa G, et al. Daily nutritional supplementation with vitamin D(3) and phenylbutyrate to treatment-naive HIV patients tested in a randomized placebo-controlled trial. Nutrients. (2019) 11:133. doi: 10.3390/nu11010133
32. Tenorio AR, Chan ES, Bosch RJ, Macatangay BJC, Read SW, Yesmin S, et al. Rifaximin has a marginal impact on microbial translocation, T-cell activation and inflammation in HIV-positive immune non-responders to antiretroviral therapy - ACTG A5286. J Infect Dis. (2015) 211:780–90. doi: 10.1093/infdis/jiu515
33. Lindboe JB, Langkilde A, Eugen-Olsen J, Hansen BR, Haupt TH, Petersen J, et al. Low-dose growth hormone therapy reduces inflammation in HIV-infected patients: a randomized placebo-controlled study. Infect Dis. (2016) 48:829–37. doi: 10.1080/23744235.2016.1201722
34. Srinivasa S, Fitch KV, Wong K, O'Malley TK, Maehler P, Branch KL, et al. Randomized, Placebo-Controlled Trial to Evaluate Effects of Eplerenone on Metabolic and Inflammatory Indices in HIV. J Clin Endocrinol Metab. (2018) 103:2376–84. doi: 10.1210/jc.2018-00330
35. Bourke CD, Gough EK, Pimundu G, Shonhai A, Berejena C, Terry L, et al. Cotrimoxazole reduces systemic inflammation in HIV infection by altering the gut microbiome and immune activation. Sci Transl Med. (2019) 11:aav0537. doi: 10.1126/scitranslmed.aav0537
36. Macatangay BJC, Jackson EK, Abebe KZ, Comer D, Cyktor J, Klamar-Blain C, et al. A randomized, placebo-controlled, pilot clinical trial of dipyridamole to decrease human immunodeficiency virus-associated chronic inflammation. J Infect Dis. (2020) 221:1598–606. doi: 10.1093/infdis/jiz344
37. Natsag J, Kendall MA, Sellmeyer DE, McComsey GA, Brown TT. Vitamin D, osteoprotegerin/receptor activator of nuclear factor-kappaB ligand (OPG/RANKL) and inflammation with alendronate treatment in HIV-infected patients with reduced bone mineral density. HIV Med. (2016) 17:196–205. doi: 10.1111/hiv.12291
38. Somsouk M, Dunham RM, Cohen M, Albright R, Abdel-Mohsen M, Liegler T, et al. The immunologic effects of mesalamine in treated HIV-infected individuals with incomplete CD4+ T cell recovery: a randomized crossover trial. PLoS ONE. (2014) 9:e116306. doi: 10.1371/journal.pone.0116306
39. O'Brien MP, Hunt PW, Kitch DW, Klingman K, Stein JH, Funderburg NT, et al. A randomized placebo controlled trial of aspirin effects on immune activation in chronically human immunodeficiency virus-infected adults on virologically suppressive antiretroviral therapy. Open Forum Infect Dis. (2017) 4:ofw278-ofw. doi: 10.1093/ofid/ofw278
40. Gupta SK, Mi D, Dubé MP, Saha CK, Johnson RM, Stein JH, et al. Pentoxifylline, inflammation, and endothelial function in HIV-infected persons: a randomized, placebo-controlled trial. PLoS ONE. (2013) 8:e60852. doi: 10.1371/journal.pone.0060852
41. Vergara TRC, Samer S, Santos-Oliveira JR, Giron LB, Arif MS, Silva-Freitas ML, et al. Thalidomide is associated with increased T cell activation and inflammation in antiretroviral-naive HIV-infected individuals in a randomised clinical trial of efficacy and safety. EBioMedicine. (2017) 23:59–67. doi: 10.1016/j.ebiom.2017.08.007
42. Hsue PY, Ribaudo HJ, Deeks SG, Bell T, Ridker PM, Fichtenbaum C, et al. Safety and impact of low-dose methotrexate on endothelial function and inflammation in individuals with treated human immunodeficiency virus: AIDS clinical trials group study A5314. Clin Infect Dis. (2019) 68:1877–86. doi: 10.1093/cid/ciy781
43. Kent SJ, Hough S, Kelleher AD, Law MG, Hutchinson J, Catalfarmo M, et al. Vorapaxar for HIV-associated inflammation and coagulopathy (ADVICE): a randomised, double-blind, placebo-controlled trial. Lancet HIV. (2018) 5:e553–e9. doi: 10.1016/S2352-3018(18)30214-5
44. Cao W, Mehraj V, Kaufmann DE, Li T, Routy J-P. Elevation and persistence of CD8 T-cells in HIV infection: the achilles heel in the ART era. J Int AIDS Soc. (2016) 19:20697. doi: 10.7448/IAS.19.1.20697
45. Hearps AC, Maisa A, Cheng WJ, Angelovich TA, Lichtfuss GF, Palmer CS, et al. HIV infection induces age-related changes to monocytes and innate immune activation in young men that persist despite combination antiretroviral therapy. AIDS. (2012) 26:843–53. doi: 10.1097/QAD.0b013e328351f756
46. Cao Y, Su B, Guo X, Sun W, Deng Y, Bao L, et al. Potent neutralizing antibodies against SARS-CoV-2 identified by high-throughput single-cell sequencing of convalescent patients' B cells. Cell. (2020) 182:73–84.e16. doi: 10.1016/j.cell.2020.05.025
47. Herasimtschuk A, Downey J, Nelson M, Moyle G, Mandalia S, Sikut R, et al. Therapeutic immunisation plus cytokine and hormone therapy improves CD4 T-cell counts, restores anti-HIV-1 responses and reduces immune activation in treated chronic HIV-1 infection. Vaccine. (2014) 32:7005–13. doi: 10.1016/j.vaccine.2014.09.072
48. Winter FS, Emakam F, Kfutwah A, Hermann J, Azabji-Kenfack M, Krawinkel MB. The effect of Arthrospira platensis capsules on CD4 T-cells and antioxidative capacity in a randomized pilot study of adult women infected with human immunodeficiency virus not under HAART in Yaoundé, Cameroon. Nutrients. (2014) 6:2973–86. doi: 10.3390/nu6072973
Keywords: CD4+ T-cell, immune activation, inflammation, immunologic non-responder, people living with HIV, adjunct therapy
Citation: Zhang Y, Jiang T, Li A, Li Z, Hou J, Gao M, Huang X, Su B, Wu H, Zhang T and Jiang W (2021) Adjunct Therapy for CD4+ T-Cell Recovery, Inflammation and Immune Activation in People Living With HIV: A Systematic Review and Meta-Analysis. Front. Immunol. 12:632119. doi: 10.3389/fimmu.2021.632119
Received: 22 November 2020; Accepted: 22 January 2021;
Published: 17 February 2021.
Edited by:
Serge Benichou, Centre National de la Recherche Scientifique (CNRS), FranceReviewed by:
Suresh Pallikkuth, University of Miami, United StatesCopyright © 2021 Zhang, Jiang, Li, Li, Hou, Gao, Huang, Su, Wu, Zhang and Jiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hao Wu, d2hkb2NAY2NtdS5lZHUuY24=; Tong Zhang, enRfZG9jQGNjbXUuZWR1LmNu; Wei Jiang, amlhbndAbXVzYy5lZHU=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.