 Liliane Maria Vidal Siqueira1
Liliane Maria Vidal Siqueira1 Carolina Senra2Áureo Almeida de Oliveira1Nidia Francisca de Figueiredo Carneiro3Luciana Inácia Gomes2Ana Rabello2Paulo Marcos Zech Coelho1
Carolina Senra2Áureo Almeida de Oliveira1Nidia Francisca de Figueiredo Carneiro3Luciana Inácia Gomes2Ana Rabello2Paulo Marcos Zech Coelho1 Edward Oliveira2*
Edward Oliveira2*- 1Diagnosis and Therapy of Infectious and Oncologic Diseases, Instituto René Rachou, Oswaldo Cruz Foundation, Belo Horizonte, Brazil
- 2Clinical Research and Public Politics in Infectious and Parasitic Diseases, Instituto René Rachou, Oswaldo Cruz Foundation, Belo Horizonte, Brazil
- 3School of Medicine, Universidade Estadual de Montes Claros (UNIMONTES), Montes Claros, Brazil
The laboratorial diagnosis of the intestinal schistosomiasis is always performed using Kato-Katz technique. However, this technique presents low sensitivity for diagnosis of individuals with low parasite burden, which constitutes the majority in low endemicity Brazilian locations for the disease. The objective of this study was developed and to validate a real-time PCR assay (qPCR) targeting 121 bp sequence to detect Schistosoma spp. DNA for the diagnosis of intestinal schistosomiasis and a sequence of the human β-actin gene as internal control. Firstly, the qPCR was standardized and next it was evaluated for diagnosis and cure assessment of intestinal schistosomiasis in the resident individuals in Tabuas and Estreito de Miralta, two locations in Brazil endemic for intestinal schistosomiasis. The qPCR assay results were compared with those of the Kato-Katz (KK) test, examining 2 or 24 slides, Saline Gradient (SG) and “reference test” (24 KK slides + SG). The cure assessment was measured by these diagnostic techniques at 30, 90, and 180 days post-treatment. In Tabuas, the positivity rates obtained by the qPCR was 30.4% (45/148) and by “reference test” was of 31.0% (46/148), with no statistical difference (p = 0.91). The presumed cure rates at 30, 90, and 180 days post-treatment were 100, 94.4, and 78.4% by the analysis of 24 KK slides, 100, 94.4, and 78.4% by the SG, and 100, 83.3, and 62.1% by the qPCR assay. In Estreito de Miralta, the positivity obtained by qPCR was 18.3% (26/142) and with “reference test” was 24.6% (35/142), with no statistical difference (p = 0.20). The presumed cure rates were 93.3, 96.9, and 96.5% by the KK, 93.3, 96.9, and 100% by the SG, and 93.3, 93.9, and 96.5% by the qPCR at 30, 90, and 180 days post-treatment, respectively. This study showed that the diagnostic techniques presented different performance in the populations from the two districts (Tabuas and Estreito de Miralta) and reinforces the need of combining techniques to improve diagnosis accuracy, increasing the detection of individuals with low parasite burden. This combination of techniques consists an important strategy for controlling the disease transmission.
Introduction
In Brazil, intestinal schistosomiasis is caused by Schistosoma mansoni, the only species with established transmission. Despite the prevalence and parasite burden having decreased over the years after implanting the preventive measurements of the Schistosomiasis Control Program, in 1975, the disease still occurs in Brazil. Intestinal schistosomiasis is currently found in low, moderate, and high endemicity areas of 19 Brazilian federal units (1). The last national prevalence survey (INPEG 2010–2015) estimated 1,500,000 positive individuals for intestinal schistosomiasis in Brazil, which remains an important public health issue (2).
This situation could be partly attributed to the lack of accurate diagnostic techniques to detect intestinal schistosomiasis in endemic areas. The use of the Kato-Katz technique to detect S. mansoni eggs (3) with one or two slides from a single fecal sample per individual is extensively employed in prevalence surveys and individual diagnosis due to its practicability and low cost (4). This technique is sensitive to the diagnosis of S. mansoni infection when applied in fecal samples from individuals with moderate and high parasite burden. However, the lack of sensitivity presented by this technique occurs when it is used to diagnose individuals with low parasite burden, who are mostly present in low endemicity area (5–11). The S. mansoni infected individuals who were not diagnosed contribute to maintain the local transmission or to establish new outbreak when they migrate to a non-endemic area, hindering the efficacy of the control measures.
Serological assays have been used for schistosomiasis diagnosis by detecting antibodies against schistosomal antigens. However, they are unable to discriminate between active infections and past exposures, especially in individuals living in regions endemic for schistosomiasis (12). A lateral flow cassette assay was developed to overcome the limitation of parasitological and serological techniques to detect circulating cathodic antigen in urine from the Schistosoma infected individuals (POC-CCA®, Rapid Medical Diagnostics, Pretoria, South Africa). This test became available in 2003 and seems to be more sensitive than the Kato-Katz technique when applied in areas highly endemic for S. mansoni (13). However, there are controversies regarding the sensitivity of the POC-CCA when applied in individuals from low endemicity areas. In these cases, the POC-CCA has showed larger sensitivity only in patients with moderate or high parasite burden (14, 15).
Alternatively, the detection of schistosome DNA through DNA amplification techniques provides advantages compared to the many parasitological techniques and serological tests, due their high sensitivity, specificity, and accuracy. Furthermore, DNA amplification techniques can detect early pre-patent infections. Although the PCR assay is widely used for laboratory diagnosis of many infectious and parasitic diseases, its application for schistosomiasis was reported for the first time for our research group. We showed that PCR targeting 121 bp, described by Hamburger et al. (16) achieved a limit of detection (LOD) of 1 fg of S. mansoni egg template DNA and absence of amplification of the DNA from Ascaris lumbricoides, Ancylostoma duodenale, Taenia solium, and Trichiuris trichiuria, helminths commonly found in the same endemic areas.
Since then, we have extensively worked with this 121 bp sequence as a target in the PCR assays for diagnosing intestinal schistosomiasis. The 121 bp sequence was used successfully in conventional PCR (17, 18), PCR-ELISA (19, 20), obtaining consistent results. Furthermore, other studies show the 121 bp sequence as a target in a real-time PCR and oligochromatography-polymerase chain reaction with higher sensitivity than the Kato-Katz technique for diagnosing intestinal schistosomiasis (21, 22). Moreover, the 121 bp DNA sequence was targeted to detect Schistosoma DNA in plasma (23) and urine samples (24, 25) using conventional PCR.
Thus, the main goal of this study was to develop a qPCR assay targeting 121 bp sequence to detect S. mansoni DNA in fecal samples to diagnose intestinal schistosomiasis and assess the post-treatment cure for individuals with low parasite burden. In addition, a 92 bp sequence from the human β-actin gene too was amplified in the same reaction as internal control for ensure the efficiency of DNA extraction and PCR-amplification.
Material and Methods
qPCR Assay Standardization
Extraction of S. mansoni DNA
In this study we tried contaminate negative fecal samples with S. mansoni eggs and we did not have success. The S. mansoni eggs are relatively big ones and we had difficulties to count the S. mansoni eggs in Neubauer chamber and then recover it to contaminate negative fecal samples.
To contorn this limitation, genomic DNA was extracted from adult S. mansoni worms (BH strain) obtained from the liver of Swiss albino mice 60 days after infection with 150 cercariae using QlAamp DNA Mini and Blood Mini Handbook (QIAGEN, GmbH, Hilden, Germany), following the manufacturer`s protocol.
As negative controls we used DNA extracted from three negative S. mansoni fecal samples collected from children resident in non-endemic area who had negative results by Kato-Katz technique. The total DNA was extracted using the QIAamp DNA Stools Mini Kit (Qiagen GmbH, Hilden, Germany), according to the manufacturer’s recommendations and following the protocols of DNA Isolation from Stool for Pathogen Detection and DNA Isolation from Large Amounts of Stool. The DNA concentration and A260/A280 absorbance ratio was measured in a Nanodrop ND-1000 spectrophotometer (Thermo Fisher Scientific, Wilmington, DE, USA) to ensure the efficiency of the DNA extraction and to verify the purity of the DNA obtained.
Primers and Probes
A forward 5′-CCG ACC AAC CGT TCT ATG A-3′ and reverse 5′-CAC GCT CTC GCA AAT AAT CTA AA-3′ primers and a 5′-6[FAM]/TCG TTG TAT CTC CGA AACCAC TGG ACG/[3BHQ1] probe were designed to amplify and detect a 90 bp fragment of a highly repetitive 121 bp sequence of S. mansoni (GenBank: M61098). A forward 5’-CCA TCT ACG AGG GGT ATG-3’ and reverse 3’-GGT GAG GAT CTT CAT GAG GTA-5’ primers, and the 56-JOE/CCT GCG TCT GGA CCT GGC TG/[3BHQ1] probe were designed to amplify and detect a 92 pb of the human β-actin gene (GenBank: AY582799.1) as internal control (Figure 1). All primers and probes were designed in the Primer3-web program 0.4.0 (26) and submitted to homology searches on the National Center for Biotechnology Information website with nucleotide BLAST program using the Nucleotide collection and Megablast option database. The primers and probes were purchased from Integrated DNA Technologies Inc. (Coralville, IO, USA). Initially, we tried S. mansoni primers at 0.1, 0.2, 0.3 μM and S. mansoni probe at 0.1, 0.25, and 0.5 μM in different combinations in the simplex qPCR assay using 38 ng, 3.8 ng, 380 pg, 38 pg, 3.8 pg, 380 fg, 0.38 fg, and 0.038 fg genomic DNA of S. mansoni diluted 1:5 in linear acrylamide solution [30 μg/ml (w/v) in DEPC treat H2O]. Next, we tried the human β-actin gene primers at 0.1, 0.15, and 0.2 μM and human β-actin gene probe at 0.1, 0.25, and 0.5 μM in a simplex qPCR assay using DNA extracted from negative S. mansoni fecal samples diluted 1:5 in linear acrylamide solution. In this way, the best qPCR protocol was defined as:

Figure 1 Diagram showing anneling positions of the primers and probes in the 121 bp and human β-actin gene sequences. SnapGene software (from Insightful Science; available at snapgene.com).
The reaction was performed with a final volume of 25 μl containing 12.5 μl of TaqMan® Universal PCR Master Mix (Life Technologies, Thermo Fisher Scientific Inc., USA), S. mansoni specific primers at 0.1 μM, 5′-6[FAM]—[3BHQ1] probe at 0.25 μM, β-actin specific primers at 0.15 μM and 56-JOE—[3BHQ1] probe at 0.25 μM, BSA 0.01 μg/μl, MgCl2 at 2 μM and 4 μl of DNA diluted 1:5 in linear acrylamide solution. Two controls were used for each reaction, a positive control (PCR mix plus DNA extracted from adult worms) and a negative control consisting of PCR mix (No Template Control). The assays were performed in duplicate using microplates (MicroAmp® Fast Optical/Applied Biosystems Foster City, CA, USA) sealed with adhesive film (Optical Adhesive Covers/Applied Biosystems) on the StepOnePlus™ Real-Time PCR System (Thermo Fisher Scientific Inc., USA) under the universal cycling program with 45 cycles and annealing temperature of 60 °C. Based on a standard curve produced with serial dilutions of S. mansoni DNA, samples presenting Ct ⩽ 42 were classified as positives. Samples that did not presented internal control JOE (β-actin Probe) amplification were retested and a new DNA sample was reextracted when necessary.
Extraction and amplification protocols were performed in different rooms to minimize the possibility of contamination. All experiments were performed in a laminar flow chamber, previously irradiated with ultraviolet light, and employing only sterile disposable products, including barrier tips.
Analytical Sensitivity (Limit of Detection)
The lower LOD of the qPCR was defined by the amplification curve of a positive control containing 38 ng, 3.8 ng, 380 pg, 38 pg, 3.8 pg, 380 fg, 0.38 fg, and 0.038 fg of genomic DNA of adult worms diluted 1:5 in linear acrylamide solution, in triplicate. The mean of Ct from the triplicates was used to define the point in the amplification curve. The amplification efficiency assay was analyzed according to the amplification efficiency (E), Slope, and R2, following recommendations of Johnson et al. (27).
Analytical Specificity
DNA from Ancylostoma duodenale, Ascaris lumbricoides, and Fasciola hepatica, ceded by professors from the Department of Parasitology, Biology Institute, of the Universidade Federal de Minas Gerais, was used in the qPCR assay to evaluate the analytical specificity. A. duodenale and A. lumbricoides are frequently found in S. mansoni co-infections and F. hepatica is a worm phylogenetically next to the S. mansoni.
Precision Tests
The repeatability test was carried out using six DNA samples extracted from human feces (three negatives and three positives for the presence of S. mansoni eggs), according to the Kato-Katz technique. The repeatability test was measured by the coefficient of variation (CV) by retesting four times the same samples in a single assay (intra-assay test). The reproducibility test was measured by the coefficient of variation (CV) of retesting positive control containing 38 ng, 3.8 ng, 380 pg, 38 pg, 3.8 pg, 380 fg and 0.38 fg of genomic DNA of adult worms diluted 1:5 in linear acrylamide solution in three different days.
qPCR Validation
The validation of the qPCR was performed through a cross-sectional-based study carried out in the Tabuas and Estreito de Miralta districts (Figure 2), two communities endemic for schistosomiasis from the rural area of the municipality of Montes Claros, in the northern region of the state of Minas Gerais, Brazil. The prevalence in Tabuas in 2010 was estimated in 29.1% using two slides in the Kato-Katz technique in the Zoonozis Control Center of Montes Claros. There were no prevalence data from the Estreito de Miralta. However, this community was close to Tabuas and no control has been placed in these communities in the 2 years prior to the current study.
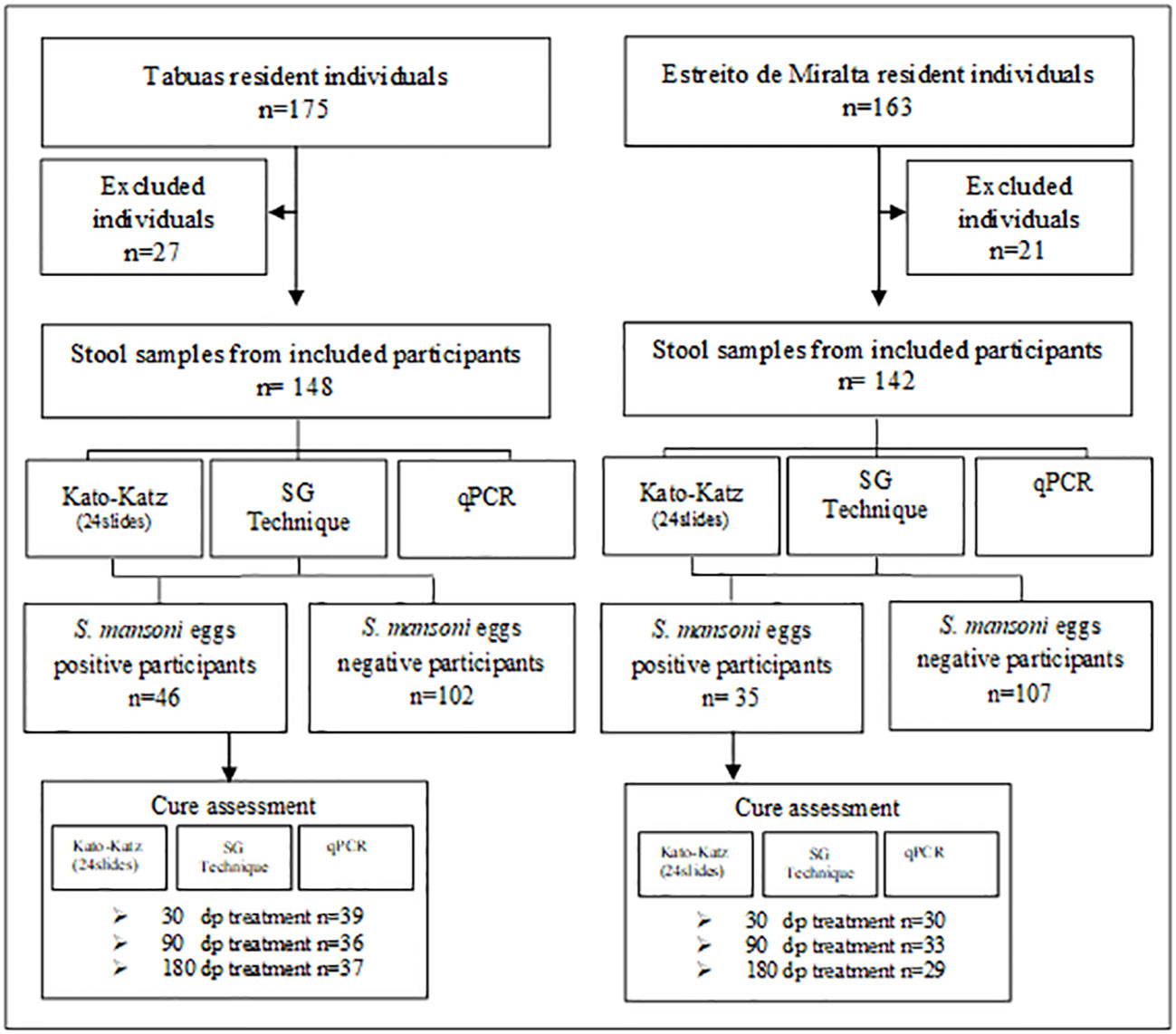
Figure 2 STARD flow diagram followed to select the studied groups.
All residents of the mentioned locations with over 1 year of age, of both gender, and who agreed to participate in the study and signed the informed consent form were included. Furthermore, the diagnostic tests were applied to assess the cure after specific treatment of low parasite burden individuals.
Stool Samples
The stools samples were provided by the participants at day 0 and examined using the Kato-Katz and Saline Gradient techniques in both locations. The participants who presented S. mansoni eggs in their stools were treated with 60 mg/kg of praziquantel for children and 50 mg/kg for adults. New stools samples were collected at 30, 90, and 180 days post-treatment, totalizing four samples by participant until the study end. The participants who presented eggs or cyst of other parasites were treated with 400 mg of albendazole (single oral dose) as recommended by the Brazilian Ministry of Health.
Kato–Katz Technique
The fecal samples from the residents of Tabuas and Estreito de Miralta were submitted to the Kato-Katz technique using the Helm-Test® produced by BioManguinhos-Fiocruz (Rio de Janeiro, RJ, Brazil). Twenty-four slides of the same stools sample, which correspond to the 1,000 mg of feces, were examined to perform a quantitative comparison between the parasitological tests. Infection intensity was calculated by the number of S. mansoni eggs found in 24 slides, resulting in eggs per gram of feces (epg). According to WHO (4), the S. mansoni infection intensity is classified as light (1–100 epg), moderate (101–400 epg), and high (>400).
Saline Gradient Technique
The Saline Gradient technique was performed according to the protocol published by Coelho et al. (28). Fecal samples were filtered through nylon screen (150 µm) and two portions of 500 mg were quantified using a metal plate. The portions were subjected to a slow flow of a 3% saline solution for 1 h. Subsequently, the system was closed and all remaining material transferred to a Falcon® tube (15 ml), after which 20% formaldehyde was added to the sediment obtained (approximately 2 ml of sediment). The final solution was examined in an optical microscope. All sediment was examined, the helminth eggs were counted, and the S. mansoni eggs were separated in two preparations (500 mg + 500 mg) representing eggs per gram of feces (epg).
qPCR Assay
The DNA of 1,000 mg fecal samples obtained from residents of Tabuas and Estreito de Miralta was extracted using the QIAamp DNA Stools Mini Kit (Qiagen GmbH, Hilden, Germany), according to the manufacturer’s recommendations and following the protocols of DNA Isolation from Stool for Pathogen Detection and DNA Isolation from Large Amounts of Stool. The DNA concentration was measured by absorbance at 260 nm in a Nanodrop ND-1000 spectrophotometer (Thermo Fisher Scientific, Wilmington, DE, USA). The A260/A280 absorbance ratio was analyzed to verify the purity of the DNA obtained.
The qPCR assay was performed using fecal samples according to the conditions standardized. The DNA samples that did not present amplification for the human β-actin gene were retested for ensure the efficiency of DNA extraction and PCR-amplification.
Data Analysis
The database was built in Microsoft Office Excel 2007 spreadsheets and analyzed using GraphPad Prism version 6.0 (San Diego, CA, USA) or Open Epi software version 3.0 (29). The positivity, sensitivity, specificity, and accuracy rates of the parasitological and molecular tests were calculated using the Open Epi software. The chi-square test was used for comparisons between proportions considering a 5% significance level (30). The degree of agreement between diagnostic tests was determined by the Kappa index and interpreted according to Landis & Koch (31). Correlations between epg from the KK and Ct from the qPCR test results were tested using the Spearman’s coefficiency of correlation.
Ethical Approval
The use of human samples was approved following the standards of the Ethical Review Committee of the IRR/FIOCRUZ, Brazil (CEPSH 03/2008) and National Committee of Ethical Research (784/2008, CONEP 14886) in accordance with the Brazilian legislation (RDC 466/2012). The written informed consent was obtained from all the participants/parents or guardians before collecting the samples.
Results
qPCR Assay Standardization
A standard curve was constructed and the analytical sensitivity assay showed that the S. mansoni DNA was detected up to the seventh dilution, which corresponds to 0.38 fg. Moreover, repeatability and linearity in the standard curve were obtained up to Ct 41 (CV ranging from 0.05 to 2.7%; Slope: −3.222; E: 104%, and R²: 0.98).
The analytical specificity was assessed using DNA from Ancylostoma duodenale, Ascaris lumbricoides, and Fasciola hepática adult worms. The results showed no unspecific amplifications when using genomic DNA in the qPCR assay. The repeatability test presented acceptable Ct variations in the four replicates of three S. mansoni negative and three S. mansoni positive samples. In this assay the coefficient of variation (CV) were 1.74, 2.18, and 2.33% for the target (FAM probe) and 0.69, 0.48, and 0.40% for internal control (JOE probe). Likewise, the reproducibility test presented Ct consistent, resulting CV ranging from 1.6 to 5.4%.
qPCR Validation in Tabuas
Positivity Rates for S. mansoni and Other Parasites
In Tabuas, 84.5% (148/175) of the population participated of this study. From these, 73 were females and 75 males, aged between 1 and 86 years. Ninety-six individuals were residents in the Tabuas district and 52 in the Ribeirão de Tabuas, an adjacent location. The reasons for non-participation in the study were: 1) refusal; 2) insufficient biological sample for performing all techniques, and 3) health reasons.
The Table 1 shows the positivity rates found in the population from Tabuas. The positivity rate of the KK technique was 12.1% (18/148), 15.5% (23/148), 16.9% (25/148), 19.6% (29/148), 19.6% (29/148), and 20.6% (31/148) for 1, 2, 3, 6, 12, and 24 slides examined, respectively. The higher positivity rates were found in individuals with 10 to 19 (47.6%) and 20–29 years of age (30%) (Figure 3). Of the 31 positive participants, 25 (80.7%) presented low parasite load (1–100), five (16.1%) presented moderate load (101–400), and one (3.2%) presented high parasite load (>400 epg).

Table 1 Positivity rates of intestinal schistosomiasis found by parasitological techniques and qPCR in the population from Tabuas district, Minas Gerais state, Brazil.
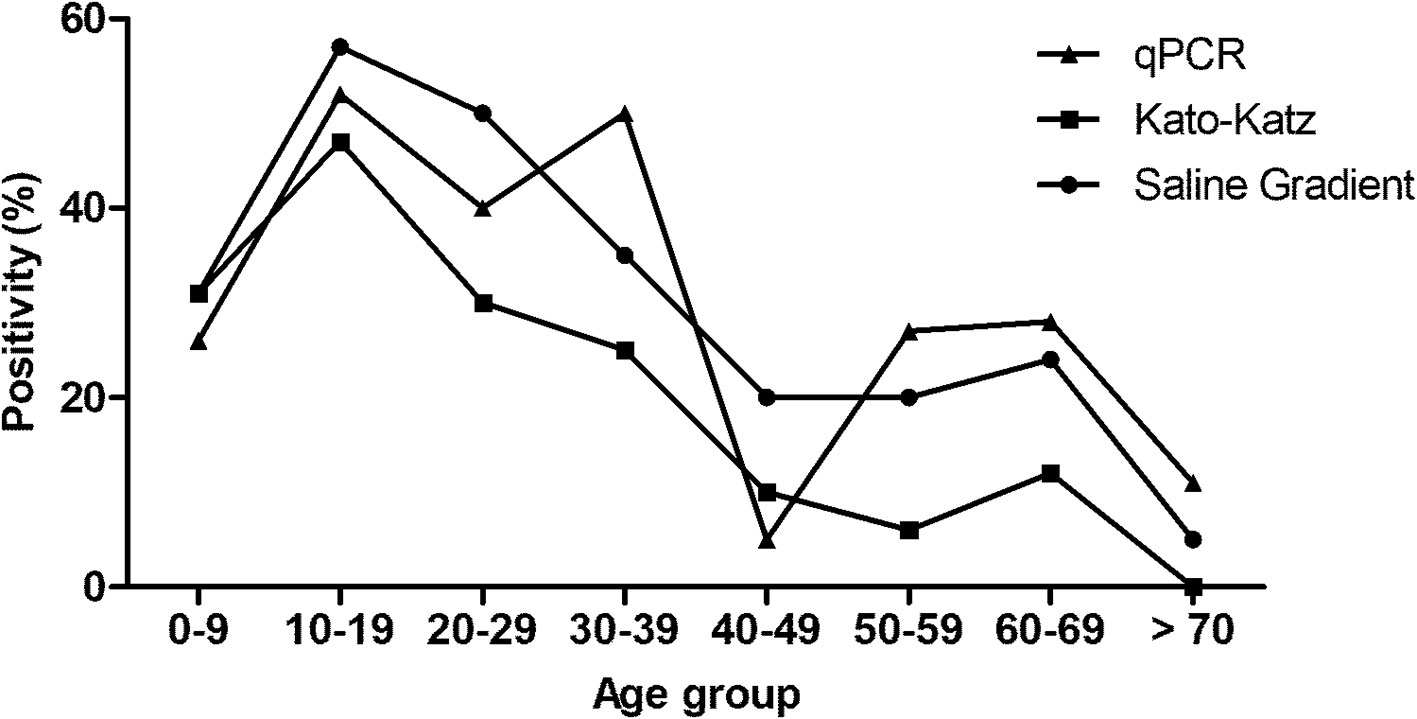
Figure 3 Positivity of intestinal schistosomiasis in the participants from Tabuas district, diagnosed by Kato-Katz (24 slides), Saline Gradient, and qPCR and distributed by age ranges.
The SG technique detected 43/148 participants with S. mansoni eggs in their stools, producing a positivity rate of 29.0%. Likewise, the SG technique showed higher positivity rates in the age range from 10 to 19 (57.1) followed by 20–29 years (50%) (Figure 3). Of the 43 positive participants, 40 had low parasite load and only three presented moderate loads.
To create a “reference test,” the results obtained by KK (24 slides) and SG were combined and the positivity increased to 31.0% (46/148), with a statistical difference regarding the previous KK positivity (p = 0.04), although without statistical difference compared to SG (p = 0.70). The positivity rate obtained by the qPCR assay was 30.4%, represented by 45/148 positive participants. All samples (148/148) presented amplification of the internal control. The highest positivity rates for this assay occurred in the age ranges from 10 to 19 (52%) and 30 to 39 years (50%) (Figure 3).
Besides S. mansoni, the two combined techniques detected 37 positive participants for other parasites, 16 (10.8%) positive for hookworms, eight (5.4%) for Enterobius vermicularis, eight (5.4%) for Ascaris lumbricoides, six (4%) for Giardia sp., 20 (13.5%) for Entamoeba coli, two (1.4%) for Trichuris trichiura, one (0.68%) for Taenia sp., and two (1.4%) for Hymenolepis nana. Of the participants infected with S. mansoni, six presented co-infection with hookworms and E. vermicularis.
qPCR Performance in Different Scenarios
Considering the results of the KK technique with two slides as a definitive diagnostic, the qPCR presented 95.7% sensitivity (95% CI: 79–99.2), 81.6% specificity (95% CI: 73.9–87.4), and 83.8% accuracy (95% CI: 77–88.9). Considering the results of the KK technique with 24 slides, the qPCR presented 96.7% sensitivity (95% CI: 83.8–99.4), 87.2% specificity (95% CI: 79.9–92.0), and 89.2% accuracy (95% CI: 83.2–93.2).
Considering the SG results, the qPCR presented 81.4% sensitivity (95% CI: 67.3–90.2), 90.5% specificity (95% CI: 83.3–94.7), and 87.8% accuracy (95% CI: 81.6–92.2). Based in the results from the “reference test,” the qPCR presented 82.6% (95% CI: 69.3–90.9), 93.1% (95% CI: 86.5–96.6), and 89.8% (95% CI: 83.9–93.7) of sensitivity, specificity, and accuracy rates, respectively (Table 2).

Table 2 Performance of qPCR considering the parasitological techniques and “reference test” applied in the population from Tabuas district, Minas Gerais state, Brazil.
Table 3 shows the agreement ratios between the parasitological techniques and qPCR results. Among the 45 participants positive to S. mansoni by the qPCR assay, 22 were consistent with the KK technique (two slides), one presented positive KK and negative qPCR results (with positive amplification of human β-actin gene), and 23 were positive only by the qPCR (Kappa index: 0.56). On the other hand, 30 participants were consistent with the KK technique (24 slides), one presented positive KK and negative qPCR results (with positive amplification of human β-actin gene), and 15 were positive only by qPCR (Kappa índice: 0.72). Furthermore, there is a negative correlation between the microscopic egg counts (epg) and Ct (r: −0.404) obtained by the KK technique (24 slides) and qPCR assay, respectively.

Table 3 Agreement analysis of the qPCR results in relation to the parasitological techniques and reference test in the population from Tabuas district, Minas Gerais state, Brazil.
In the crosstabulation between SG and qPCR, eight participants presented positive results with the SG technique and negative with the qPCR (with positive amplification of human β-actin gene). On the other hand, 10 participants presented negative results with the SG technique but were positive with the qPCR. Thirty-five positive and 95 negative results were consistent between the SG technique and qPCR assay (Kappa index: 0.71). Forty-five individuals were positive by the qPCR, of which seven cases were not detected by the “reference test.” In contrast, eight cases were positive by the “reference test” and were not detected by the qPCR (with positive amplification of human β-actin gene), resulting in a Kappa index of 0.76.
Cure Assessment in Tabuas
Table 4 shows the follow-up for cure assessment. Of the 46 positive participants treated with praziquantel, 39 participated of the follow-up for cure assessment at 30 days post-treatment. Of these individuals, all presented negative results by the parasitological techniques and qPCR assay, resulting in a presumed cure rate of 100%. At 90 days post-treatment, 36 participants were reexamined for cure assessment. Among these, three participants were positive for S. mansoni eggs, one of which was diagnosed by both techniques (KK and SG) and two identified separately by each parasitological technique. qPCR diagnosed six positive participants at 90 days. Therefore, the presumed cure rates at 90 days post-treatment were 94.4% for the KK and SG techniques and 83.3% for the qPCR assay. At 180 days post-treatment, new stool samples were collected from 37 participants for cure assessment, of which eight were positive for S. mansoni eggs by both parasitological techniques and 14 were positive for S. mansoni DNA by the qPCR. The presumed cure rates were 78.4% for the KK and SG techniques and 62.1% for the qPCR assay.
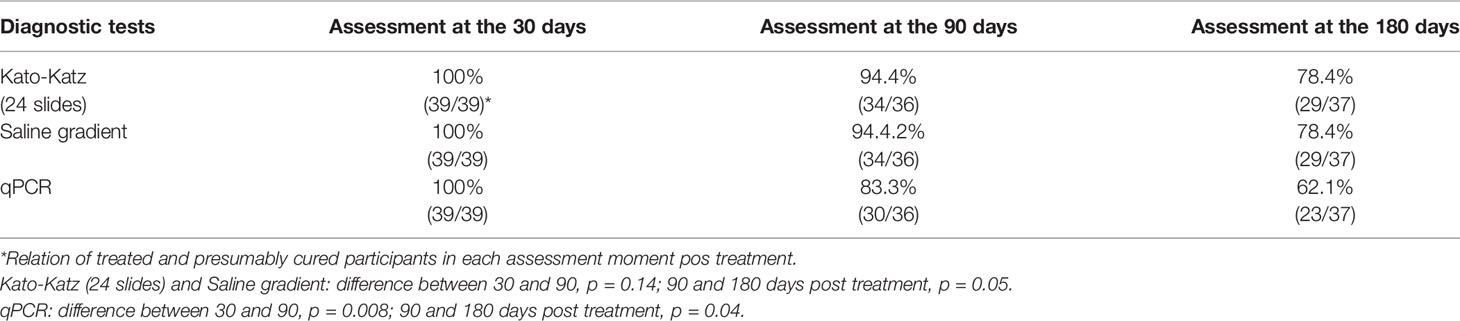
Table 4 Presumed cure rates measured by parasitological techniques and qPCR 30, 90, and 180 days pos treatment of the S. mansoni positive participants from Tabuas district, Minas Gerais state, Brazil.
qPCR Validation in Estreito de Miralta Positivity Rates for S. mansoni and Other Parasites
In Estreito de Miralta, 87.1% (142/163) of the population was included in this study, of which 77 were females and 65 males, aged from 01 to 86 years, 96 residents of the Estreito de Miralta and 46 of Serra Verde, an adjacent location. The reasons for non-participation in the study were the same as those considered for the Tabuas location.
The positivity rates obtained by the KK technique were 9.2% (13/142), 10.5% (15/142), 11.3% (16/142), 12% (17/142), 16.2% (23/142), and 19.7% (28/142) using 1, 2, 3, 6, 12, and 24 slides, respectively (Table 5). The higher positivity rates of the KK (24 slides) technique occurred from 10 to 19 years (44.4%) and 50 to 59 years (30%) (Figure 4). All positive participants presented low parasitic load (1–100 epg). The SG technique detected 26/142 participants positive for S. mansoni eggs, with a positivity rate of 18.3% concentrated at ages from 10 to 19 (51.9%) and 20 to 29 years (50%) (Figure 4).

Table 5 Positivity rates of intestinal schistosomiasis found by parasitological techniques and qPCR in the population from Estreito de Miralta district, Minas Gerais state, Brazil.
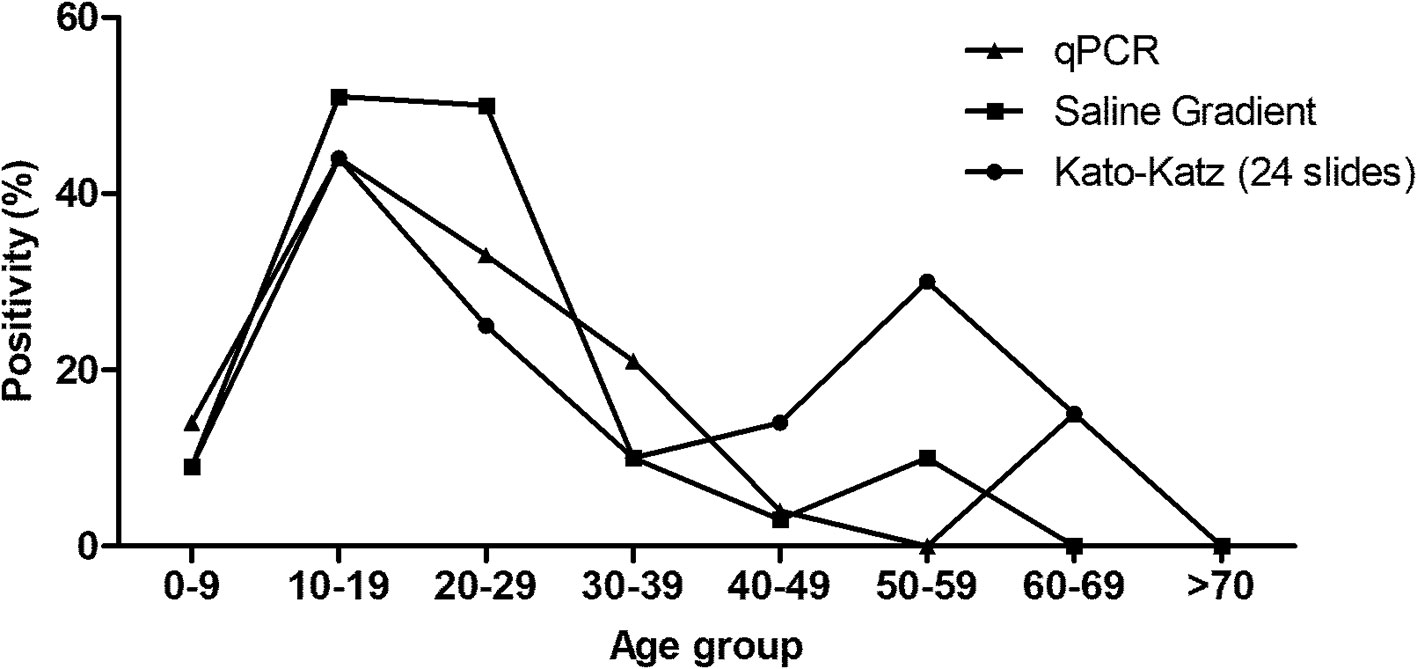
Figure 4 Positivity of intestinal schistosomiasis in the participants from Estreito de Miralta district, diagnosed by Kato–Katz (24 slides), Saline Gradient, and qPCR and distributed by the age ranges.
Likewise, “reference test” was created with the results obtained by the KK (24 slides) and SG techniques. The positivity increased to 24.6% (35/142), with no statistical difference regarding the previous KK (p = 0.32) and SG (p = 0.20) positivity rates. The positivity rate obtained by the qPCR assay was equal to the one obtained with the SG technique (18.3%), represented by 26/142 positive participants. The higher positivity rates with qPCR occurred in the age ranges from 10 to 19 years (44.4%) (Figure 4).
Other intestinal parasites were also detected by both parasitological techniques. The KK and SG techniques detected 14 (9.9%) individuals positive for hookworms, eight (5.6%) for Enterobius vermicularis, one (0.7%) for Ascaris lumbricoides, and three (2.1%) for Hymenolepis nana. Five participants presented co-infection with S. mansoni and hookworms and two with S. mansoni and E. vermicularis.
qPCR Performance in Different Scenarios
Table 6 shows the sensitivity, specificity, and accuracy rates. Considering the results of the KK technique with two slides as a true diagnosis, the qPCR showed 80% sensitivity (95% CI: 54.8–93), 89% specificity (95% CI: 82.3–93.3), and 88% accuracy (95% CI: 81.7–92.4). On the other hand, considering the results of the KK technique with 24 slides as a true diagnosis, the qPCR assay presented 64.3% sensitivity (95% CI: 45.8–79.3), 92.9% specificity (95% CI: 86.7–96.4), and 87.3% accuracy (95% CI: 80.9–91.8). Considering the SG results as reference, the qPCR presented 69.2% sensitivity (95% CI: 50–83.5), 93.1% specificity (95% CI: 87–96.5), and 88.7% accuracy (95% CI: 82.5–92.9). However, if the “reference test” results are considered as a true diagnosis, the qPCR presented 57.1% sensitivity (95% CI: 40.8–72), 94.4% specificity (95% CI: 88.3–97.4), and 85.2% accuracy (95% CI: 78.4–90.1) (Table 6).

Table 6 Performance of qPCR considering the parasitological techniques and “reference test” applied in the population from Estreito de Miralta district, Minas Gerais state, Brazil.
The qPCR results were crosstabulated with the parasitological techniques and the results are presented in the Table 7. Of the 142 participants, 12 were co-positive and 113 were co-negative with the KK technique (two slides) and qPCR assay, three were positive by the KK technique and negative by the qPCR assay (with positive amplification for the human β-actin gene), and 14 were positive only by the qPCR assay (Kappa index: 0.52). Twenty-six participants were positive for the qPCR assay, of which eight were not detected by the KK 24 slides. On other hand, there were 10 positive cases detected by the KK technique that the qPCR assay could not detect (Kappa index: 0.59). Moreover, is important highlight that the results of the Ct from the qPCR assay showed negative correlation (r: −0.427) with the microscopic egg counts (epg) obtained by KK technique (24 slides).

Table 7 Agreement analysis of the qPCR results in relation to the parasitological techniques and “reference test” in the population from Estreito de Miralta district, Minas Gerais state, Brazil.
The crosstabulation of the SG and qPCR results showed that 126 were consistent and 16 discordants. Among the discordant results, eight were qPCR positive and SG negative and eight were qPCR negative (with positive amplification for the human β-actin gene) and SG positive (Kappa index: 0.62). There were 21/142 qPCR and “reference test” discordant results, of which six presented positive qPCR and negative “reference test” results. In contrast, 15 individuals presented negative qPCR (with positive amplification of human β-actin gene) and positive “reference test” results, resulting in a Kappa index of 0.56 (Table 7).
Cure Assessment in Estreito de Miralta
In the follow-up for cure assessment 30 days post-treatment, new stool samples were collected from 30/35 positive participants. This evaluation showed two participants diagnosed as positive for S. mansoni infection by the KK, SG techniques and qPCR assay, resulting in a presumed cure rate of 93.3%. In the evaluation 90 days post-treatment, of the 35 participants positive for S. mansoni who were treated with praziquantel, 33 were sampled to evaluate cure assessment. The KK and SG techniques detected two positive participants, one by each technique. The qPCR assay diagnosed both participants as positive for S. mansoni DNA. The presumed cure rates were 97% measured by the KK and SG techniques and 93.3% by the qPCR assay.
The follow-up at 180 days post-treatment consisted of 29/35 samples for new stool samples for the last cure assessment. This evaluation showed only one participant diagnosed with intestinal schistosomiasis by the KK technique and qPCR, resulting in a presumed cure rate of 96.5% (Table 8).
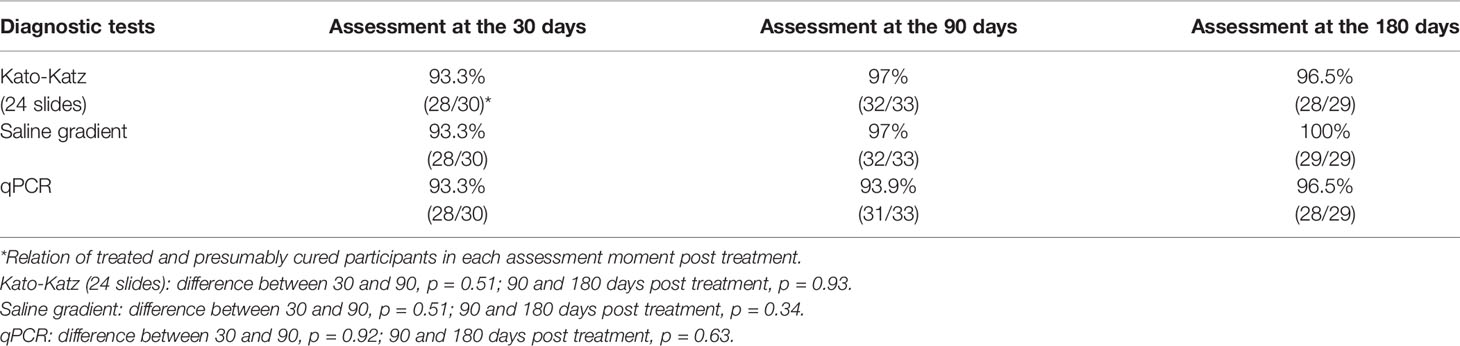
Table 8 Presumed cure rates measured by parasitological techniques and qPCR 30, 90, and 180 days post treatment of the S. mansoni positive individuals from Estreito de Miralta district, Minas Gerais state, Brazil.
Discussion
Despite the parasitological technique presenting the best cost-benefit conditions, the assessment of more sensitive techniques is essential for an efficient diagnosis in endemic areas. Current scenarios show that molecular tests are a promising tool for diagnosis and cure assessment of intestinal schistosomiasis in individuals of low parasite burden (17–20, 32, 33). One of the advantages of the qPCR assay is its potential for high throughput, elimination of post-PCR handling, and possible quantification. Moreover, the qPCR can be multiplexed to detect other parasites in the feces using primers highly specific for each parasite of interest (33). In this study, the qPCR assay was duplexed to detect S. mansoni and the human β-actin gene to diagnose the intestinal schistosomiasis and to secure the optimal conditions of amplification, respectively.
In the conditions defined in this study, the qPCR was extremally sensitive and capable of detecting 0.38 fg of S. mansoni DNA, which corresponds to approximately 0.00065 times its genome, that contains ~580 fg of DNA (34). Thus, the LOD defined in this study (0.38 fg) corresponds to less than a single cell of this multi-cellular parasite. Among the PCR assays described in the literature, those targeting 121 bp have presented lower LOD, ranging from 1 to 3 fg of total DNA (18–20, 35).
The qPCR assay was highly specific for detecting S. mansoni DNA. The primers used in the qPCR are genus-specific and did not amplify the DNA of Ancylostoma duodenale, Ascaris lumbricoides, Fasciola hepatica, and Ancylostoma duodenale. Furthermore, there were no false-positive results in the stool samples collected from the participants infected with Enterobius vermicularis, Giardia sp., Entamoeba coli, Trichuris trichiura, Taenia sp., and Hymenolepis nana.
In Tabuas, the positivity rate presented by the KK technique increased until six slides and kept relatively constant from 6 to 24 slides examined of the same fecal sample (Table 1). This behavior was also observed by other authors, who emphasize that the positivity rate is directly proportional to the number of slides and fecal samples examined. Enk et al. (7) showed that the positivity rate of schistosomiasis in an experimental group of 305 participants increased from 13.8 to 19% when one and six KK slides were examined. Moreover, an increase of 20.7 to 27.2% in the prevalence of schistosomiasis occurred when these authors examined three stool samples. Likewise, Siqueira et al. (8) found an expressive increase of the positivity rate from 8 to 9.5% and from 12.4 to 14.8.9% when one, three, six, and 12 KK slides were examined in individuals from the Buriti Seco and Morro Grande communities from Pedra Preta, a small village located in the rural area of Montes Claros, state of Minas Gerais, Brazil. These findings demonstrate the importance of evaluating a larger number of samples and slides to reduce the number of false-negative results, given that there is consensus on the limitation of the parasitological technique in detecting individuals with low parasitic burden. Nevertheless, this approach is not applicable in the epidemiological inquiry due to the lack of operability in field.
The positivity of qPCR was higher than that of the KK (24 slides, p = 0.053) and SG techniques (p = 0.79) and like the “reference test,” with no statistical difference (p = 0.91). Espírito-Santo et al. (21) also reported a qPCR positivity rate 6.8 times greater than that obtained by the results of the Kato-Katz and Spontaneous Sedimentation (HPJ) techniques combined (0.9%), in a study performed with 572 residents of a low endemicity area. These discrepant positivity rates were also described in other studies using conventional PCR (17) and PCR-ELISA (19, 20), as well as LAMP targeting 121 bp (36).
The sensitivity of the qPCR was high (96.7%) but the specificity was low (87.2%) when the KK (24 slides) results were taken as reference. Only one participant positive with eggs diagnosed by the Kato-Katz technique was not identified by the qPCR assay, which can be explained by the absence of eggs in the sample examined. The qPCR detected 15 positive participants not identified by the Kato-Katz, by examining 24 slides. This discordance was probably due to the limitation of parasitological technique for detecting parasite eggs in stools samples from residents of low endemicity areas, where most of the carriers present low parasite burden (<100 epg). In these cases, the PCR assay detects more cases of infection than the evaluations of many slides by the Kato-Katz technique, suggesting that it can be a useful diagnostic tool. In contrast, the sensitivity rates were lower (81.4 and 82.6%) and the specificity rates were high (90.4 and 93.4%) when the SG or “reference test” were considered as a reference. Thus, the accuracy ranged from 87.8 to 89.8%, with no statistical difference (p = 0.59).
In a cross-sectional population-based study, the qPCR targeting 121 bp was compared with POC-CCA®, KK (18 slides), Saline Gradient, and Helmintex techniques. The qPCR assay presented sensitivity of 91.4%, specificity of 86.9%, and Kappa index of 0.71, when the results of the three parasitological techniques were considered as a “reference test.” Moreover, the qPCR assay diagnosed 86.9% of the participants with very low parasite burden (<12 epg) while the POC-CCA® diagnosed 50.8% (37). Other studies with qPCR targeting the Schistosoma cytochrome oxidase gene (38), internal transcriber-spacer-2 sequence (ITS2) (39), SSU rRNA from S. mansoni (34), and 28S ribosomal RNA (40) have showed better performance of the qPCR compared to the parasitological techniques. Schistosoma spp. 28S ribosomal RNA can be quantitatively detected in stool, serum, and urine (40) with higher sensitivity than the Kato-Katz technique.
Furthermore, retrotransposon (SjR2), a portion of a mitochondrial gene (nad1) and cell-free parasite DNA (cfDNA) detection by Droplet Digital PCR (ddPCR) has shown to be applicable to the diagnosis of schistosomiasis (41, 42). Also, the authors highlight that the capacity to measure infection intensity have important implications for schistosomiasis control.
It is difficult to obtain a valid comparison between parasitological techniques and PCR assays since they are methodologies with different principles. These discrepant results may be related to irregular distribution of eggs in the feces when the number of eggs per gram of feces (epg) is small (43). Although the Kato-Katz technique is considered the choice test to diagnose schistosomiasis in fecal samples, it is not characteristic of a “reference test.” A study showed that the qPCR targeting Schistosoma ITS2 applied in a population from Senegal (n = 197) and Kenia (n = 760), high and low endemicity areas, respectively, presented 13–15% more positivity regarding the KK technique (two slides) of a single stool sample (39). Moreover, the authors reported that the positivity of the qPCR assay was very similar in both areas.
The presumed cure rate of 100% post-treatment was expected. However, we observed that 5.6, 21.6 and 16.7, 37.9% of the individuals from Tabuas were positive for S. mansoni eggs in the stool or with qPCR at 90 and 180 days post-treatment. Similar data were found in a study performed in the residents from the Pedra Preta community, in the municipality of Montes Claros, Minas Gerais, Brazil (44). An explanation for these findings might be the possible reinfection by S. mansoni. Moreover, one must consider the possibility of therapeutic failure caused by an incomplete cure due the sub-curative effect of praziquantel when used at usual doses (45). In this study, the sequential qPCR assay from praziquantel-treated participants showed a long persistence of S. mansoni circulating DNA, with a negative correlation between the microscopic egg counts (epg) using the KK technique (24 slides) and Ct obtained by the qPCR assay. In contrast, a qPCR assay for the quantitative detection of S. mansoni and S. haematobium DNA in stool samples in the Senegal population showed significant correlation between the qPCR Ct values and microscopic eggs counts for both Schistosoma species (38). In this case, we believe that the high positivity rate of 79.5% found by the microscopic egg counts performed on duplicate stool samples favored the positive correlation.
There are insufficient data regarding the clearance of Schistosoma DNA post-treatment. However, is necessary to consider the possibility of unisexual Schistosome infection. In this case, male or female worms will be able to release antigens and DNA that could be detected by immunological and molecular techniques, respectively (46). It is possible that Schistosoma DNA could continue to be released from eggs or killed worms that are withheld in tissue granulomes. Thus, circulating DNA from schistosomiasis patients is not entirely cleared and might be detected by qPCR assays. Wichman et al. (23, 47) proposed that circulating free DNA may be detected in more than 1 year since inactive eggs may release DNA very slowly. In some patients with chronic schistosomiasis, presenting a higher number of Schistosoma eggs, circulating free DNA may remain for considerably longer (48). Moreover, the authors highlight that the decrease of Schistosoma circulating free DNA pre- and post-treatment may be useful for monitoring patients under therapy.
In Estreito de Miralta, the positivity obtained by the KK technique (24 slides) was high than the SG technique (p = 0.76) and qPCR assay (p = 0.76). In this district the positivity rate increases constantly according to number of slides examined, disagreeing with the behavior shown in Tabuas. In Estreito de Miralta all participants presented low parasite load and possibly this fact influenced the correlation between the number of slides and positivity rates (Table 5).
In both districts (Tabuas and Estreito de Miralta), the high positivity rates for schistosomiasis were found in participants aged from 10 to 19 years, followed by participants aged between 20 and 29 (Figures 3 and 4). Burlandy-Soares et al. (49) also found high positivity when using the KK technique in these age ranges for the population of Pedro de Toledo, a low endemicity area of the state of São Paulo, Brazil. These findings clearly show the relevance of these age groups for the disease epidemiology.
Despite the low parasite load presented by the infected participants in Estreito de Miralta, the qPCR presented a positivity rate of 18.3%, approximately twice as high as that obtained by the Kato-Katz technique (two slides), as is performed in the Brazilian Schistosomiasis Program Control. Thus, approximately 50% of the individuals infected with S. mansoni continue to eliminate eggs and contribute for maintaining the transmission of the disease in the area. This evidence emphasizes the urgent need for a more sensitive diagnostic method for surveilling schistosomiasis cases in low transmission areas (25).
Apparently, the sensitivity rates of the qPCR assay (64.3, 69.2, 57.1%) were impaired and the specificity (92.9, 93.1, 94.4%) were favored when considering the KK (24 slides) and SG techniques or “reference test” as true results. These data indicate the influence of individual parasite burden in the performance of the diagnostic techniques used. Some authors reported that false negative results obtained by PCR may be due to a few factors such as inhibition of the amplification reaction by fecal compounds or DNA degradation during transportation of the sample from the field (19, 43). However, all samples from Estreito de Miralta presented amplification of the human β-actin gene, ensuring that negative results correspond to true negative samples for the Schistosoma DNA obtained with the qPCR assay. It is a consensus that the specificity of any diagnostic test benefits when it is applied in individuals from low endemicity areas. Also, it is well established that the sensitivity of a diagnostic test benefits when it is applied in individuals from high endemicity areas.
In contrast to the presumed cure rate observed in the population from Tabuas, the presumed cure rates in Estreito de Miralta were high and more consistent in the follow up at 30, 90, and 180 days post-treatment, with no statistical difference (Table 8). Surprisingly, the presumed cure rate in the population of Estreito de Miralta district at 30 days post-treatment measured by parasitological techniques and qPCR was only 93.3%. It is opportune to highlight that none of these participants received treatment during the acute phase of the disease, where the juvenile schistosomes are less susceptible to praziquantel (50). Furthermore, an experimental study using the qPCR assay showed that adult schistosomes with 6 weeks post-infection were susceptible to the praziquantel and those juvenile schistosomes with 4 weeks post-infection were not (51).
In conclusion, the diagnostic techniques presented different performance in the populations from two districts (Tabuas and Estreito de Miralta). In Tabuas, the positivity rate was higher, with the participants presenting low, moderate, and high parasite burdens and a considerable percentage of participants positive with S. mansoni eggs evaluated by the qPCR assay after undergoing treatment with the recommended dose of praziquantel. In contrast, all participants in Estreito de Miralta were classified as low parasite burden carriers, with less therapeutic failure during the cure assessment performed in this study. Based in these data, we can to suggest that the transmission force of the parasite in Tabuas is higher than that in Estreito de Miralta.
The qPCR was an acceptable diagnostic tool, with added value to microscopy in low endemicity areas for the diagnosis of intestinal schistosomiasis in fecal samples, which makes it particularly useful in low transmission areas, and consequently, in post-treatment settings. Moreover, the qPCR can be multiplexed for the diagnosis of other intestinal parasites making the assay more useful. On other hand, because of the relative high costs, the qPCR assay is not cost-effective for the routine diagnosis of schistosomiasis in endemic countries. However, the qPCR assay has become less expensive over time, with increase of the number of research centers with qPCR infrastructure. Thus, the qPCR assay can be used in the routine diagnosis of helminth infections in countries of low economic power.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
LMVS aided with the field work and parasitological techniques, and performed the molecular techniques and analyzed the results. CS assisted with the qPCR assay and analyzed the results. ÁAO aided with the enrollment of the participants, assisted with the parasitological techniques, and assisted with the field work. NFFC assisted with the enrollment of the participants and field work. LG assisted with the qPCR assay and critically reviewed the manuscript for intellectual content. AR supported with the study design and critically reviewed the manuscript for intellectual content. PMZC supported with the study design and critically reviewed the manuscript for intellectual content. EO assisted with the study design, data analysis, drafted the manuscript, and critically reviewed the manuscript for intellectual content. All authors contributed to the article and approved the submitted version.
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001; DECIT/CNPq program 2012 #404405/2012-6; PROEP/Pesquisa Clínica Program MCT-CNPq/FIOCRUZ No 03/2012. EO is supported by CNPq-Brazil (Conselho Nacional de Desenvolvimento Científico e Tecnológico, (Proc. 301159/2016-5).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
LMVS thanks the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for the PhD-scholarship.
References
1. Nascimento GL, Pegado HM, Domingues ALC, Ximenes RAA, Itria A, Cruz LN, et al. The cost of a disease targeted for elimination in Brazil: the case of schistosomiasis mansoni. Mem Inst Oswaldo Cruz (2019) 2019) 114:e180347. doi: 10.1590/0074-02760180347
2. Katz N. Inquerito Nacional de Prevalência da Esquistossomose mansoni e Geo-helmintoses (2018). Available at: http://tabnet.datasus.gov.br/cgi/sinan/inpeg/RelatorioINPEG.pdf (Accessed 15 out 2019).
3. Katz N, Chaves A, Pellegrino J. A simple device for quantitative stools thrick smear technique in schistosomiasis mansoni. Rev Inst Med Trop São Paulo (1972) 14:397–400.
4. World Health Organization (WHO). The control of schistosomiasis. Second report of the WHO expert committee. Technical Report series 830. Geneva: World Health Organization (1993) 86 p.
5. Utzinger J, Booth M, Goran EKN, Muller I, Tanner M, Lengeler C. Relative contribution of day-to-day and intra-specimen variation in faecal egg counts of Schistosoma mansoni before and after treatment with praziquantel. Parasitol (2001) 122:537–44. doi: 10.1017/S0031182001007752
6. Berhe N, Medhina G, Erkoa B, Smithc T, Gedamuc S, Berededc D, et al. Variations in helminth faecal egg contours in Kato-Katz thick smears and their implications in assessing infection status with Schistosoma mansoni. Acta Trop (2004) 92(3):205–12. doi: 10.1016/j.actatropica.2004.06.011
7. Enk MJ, Lima AC, Massara CL, Coelho PM, Schall VT. A combined strategy to improve the control of Schistosoma mansoni in areas of low prevalence in Brazil. Am J Trop Med Hyg (2008) 78:140–46. doi: 10.4269/ajtmh.2008.78.140
8. Siqueira LMV, Coelho PMZ, Oliveira AA, Massara CL, Carneiro NFF, Lima ACL, et al. Evaluation of two coproscopic techniques for the diagnosis of schistosomiasis in a low-transmission area in the state of Minas Gerais, Brazil. Mem Inst Oswaldo Cruz (2011) 106:844–50. doi: 10.1590/S0074-02762011000700010
9. Cavalcanti MG, Silva LF, Peralta RHS, Barreto MGM, Peralta JM. Schistosomiasis in areas of low endemicity: a new era in diagnosis. Trends Parasitol (2013) 29(2):75–82. doi: 10.1016/j.pt.2012.11.003
10. Carneiro TR, Peralta RHS, Pinheiro MCC, Oliveira SM, Peralta JM, Bezerra FSM. A conventional polymerase chain reaction-based method for the diagnosis of human schistosomiasis in stool samples from individuals in a low-endemicity area. Mem Inst Oswaldo Cruz (2013) 108(8):1037–44. doi: 10.1590/0074-0276130202
11. Lamberton PH, Kabatereine NB, Oguttu DW, Fenwick A, Webster JP. Sensitivity and specificity of multiple Kato-Katz thick smears and a circulating cathodic antigen test for Schistosoma mansoni diagnosis pre and post-repeated-praziquantel treatment. PloS Negl Trop Dis (2014) 8(9):e3139. doi: 10.1371/journal.pntd.0003139
12. Hinz R, Schwarz NG, Hahn A, Frickmann H. Serological approaches for the diagnosis of schistosomiasis: A review. Mol Cell Probes (2017) 31:2–21. doi: 10.1016/j.mcp.2016.12.003
13. Colley DG, Binder S, Campbell C, King CH, Tchuem Tchuente LA, N’Goran EK, et al. A five-country evaluation of a point-of-care circulating cathodic antigen urine assay for the prevalence of Schistosoma mansoni. Am J Trop Med Hyg (2013) 88:426–32. doi: 10.4269/ajtmh.12-0639
14. Coulibaly JT, Knopp S, N’Guessan NA, Silue KD, Furst T, Lohourignon LK, et al. Accuracy of urine circulating cathodic antigen (CCA) test for Schistosoma mansoni diagnosis in different settings of Cote d’Ivoire. PloS Negl Trop Dis (2011) 5(11):e1384. doi: 10.1371/journal.pntd.0001384
15. Tchuenté LAT, Fouodo CJK, Ngassam RIK, Sumo L, Noumedem CD, Kenfack CM, et al. Evaluation of circulating cathodic antigen (CCA) urine-tests for diagnosis of Schistosoma mansoni infection in Cameroon. PloS Negl Trop Dis (2012) 6(7):e1758. doi: 10.1371/journal.pntd.0001758
16. Hamburger J,H-N, Xin XY, Ramzy RM, Jourdane J, Ruppel A. A polymerase chain reaction assay for detecting snails infected with bilharzia parasites (Schistosoma mansoni) from very early prepatency. Am J Trop Med Hyg (1998) 59(6):872–6. doi: 10.4269/ajtmh.1998.59.872
17. Pontes LA, Oliveira MC, Katz N, Dias-Neto E, Rabello A. Comparison of a polymerase chain reaction and the Kato-Katz technique for diagnosing infection with Schistosoma mansoni. Am J Trop Med Hyg (2003) 68(6):652–6. doi: 10.4269/ajtmh.2003.68.652
18. Gomes LI, Marques LH, Enk MJ, Coelho PM, Rabello A. Further evaluation of an updated PCR assay for the detection of Schistosoma mansoni DNA in human stool samples. Mem Inst Oswaldo Cruz (2009) 104(8):1194–6. doi: 10.1590/S0074-02762009000800021
19. Gomes LI, Dos Santos Marques LH, Enk MJ, de Oliveira MC, Coelho PM, Rabello A. Development and evaluation of a sensitive PCR-ELISA system for detection of Schistosoma infection in feces. PloS Negl Trop Dis (2010) 4(4):e664. doi: 10.1371/journal.pntd.0000664
20. Senra C, Gomes LI, Siqueira LMV, Coelho PMZ, Rabello A, Oliveira E. Development of a laboratorial platform for diagnosis of schistosomiasis mansoni by PCR-ELISA. BMC Res Notes (2018) 11(1):455. doi: 10.1186/s13104-018-3571-7
21. Espírito-Santo MCC, Alvarado-Mora MV, Dias-Neto E, Botelho-Lima LS, Moreira JP, Amorim M, et al. Evaluation of real-time PCR assay to detect Schistosoma mansoni infections in a low endemic setting. BMC Infect Dis (2014) 14:558. doi: 10.1186/s12879-014-0558-4
22. Akinwale OP, Laurent T, Mertens P, Leclipteux T, Rollinson D, Kane R, et al. Detection of schistosomes polymerase chain reaction amplified DNA by oligochromatographic dipstick. Mol Biochem Parasitol (2008) 160:167–70. doi: 10.1016/j.molbiopara.2008.04.003
23. Wichmann D, Panning M, Quack T, Kramme S, Burchard GD, Grevelding C, et al. Diagnosing schistosomiasis by detection of cell-free parasite DNA in human plasma. PloS Negl Trop Dis (2009) 3:e422. doi: 10.1371/journal.pntd.0000422
24. Enk MJ, Oliveira e Silva G, Rodrigues NB. A salting out and resin procedure for extracting Schistosoma mansoni DNA from human urine samples. BMC Res Notes (2010) 3:115. doi: 10.1186/1756-0500-3-115
25. Enk MJ, Oliveira e Silva G, Rodrigues NB. Diagnostic accuracy and applicability of a PCR system for the detection of Schistosoma mansoni DNA in human urine samples from an endemic area. PloS One (2012) 7(6):e38947. doi: 10.1371/journal.pone.0038947
26. Rozen S, Skaletsky H. Primer3 on the WWW for general users and for biologist programmers. Methods Mol Biol (2000) 132:365–86. doi: 10.1385/1-59259-192-2:365
27. Johnson G, Nour AA, Nolan T, Huggett J, Bustin S. Minimum information necessary for quantitative real-time PCR experiments. Methods Mol Biol (2014) 1160:5–17. doi: 10.1007/978-1-4939-0733-5_2
28. Coelho PM, Jurberg AD, Oliveira AA, Katz N. Use of a saline gradient for the diagnosis of schistosomiasis. Mem Inst Oswaldo Cruz (2009) 104(5):720–3. doi: 10.1590/S0074-02762009000500010
29. Dean AG, Sullivan KM, Soe MM. OpenEpi: Open Source Epidemiologic Statistics for Public Health. Available at: www.OpenEpi.com (Accessed 15 out 2019).
30. Bhattacharyya GK, Johnson RA. Statistical concepts and methods. New York: John Wiley & Sons, Inc. (1977).
31. Landis JR, Koch GG. An application of hierarchical kappa-type statistics in the assessment of majority agreement among multiple observers. Biometrics (1977) 33:363–74. doi: 10.2307/2529786
32. Sandoval N, Siles-Lucas M, Perez-Arellano JL, Carranza C, Puente S, López-Abán J, et al. A new PCR-based approach for the specific amplification of DNA from different Schistosoma species applicable to human urine samples. Parasitol (2006) 133:581–7. doi: 10.1017/S0031182006000898
33. Cunningham LJ, Stothard JR, Osei-Atweneboana M, Armoo S, Verweij JJ, Adams ER. Developing a real-time PCR assay based on multiplex high-resolution melt curve analysis: a pilot study in detection and discrimination of soil-transmitted helminth and schistosome species. Parasitology (2018) 145(13):1733–38. doi: 10.1017/S0031182018001361
34. Gomes ALV, Melo FL, Werkhauser RP, Abath FGC. Development of a real time polymerase chain reaction for quantitation of Schistosoma mansoni DNA. Mem Inst Oswaldo Cruz (2006) 101:133–6. doi: 10.1590/S0074-02762006000900021
35. Pontes LA, Dias-Neto E, Rabello A. Detection by polymerase chain reaction of Schistosoma mansoni DNA in human serum and feces. Am J Trop Med Hyg (2002) 66(2):157–62. doi: 10.4269/ajtmh.2002.66.157
36. Mwangi IN, Mugambi RM, Shiraho EA, Mkoji GM. Development and evaluation of a loop-mediated isothermal amplification assay for diagnosis of Schistosoma mansoni infection in faecal samples. J Parasitol Res (2018) 2018:1267826. doi: 10.1155/2018/126826
37. Magalhães FC, Resende SD, Senra C, Graeff-Teixeira C, Enk MJ, Coelho PMZ, et al. Accuracy of real-time polymerase chain reaction to detect Schistosoma mansoni-infected individuals from an endemic area with low parasite loads. Parasitology (2020) 147(10):1140–8. doi: 10.1017/S003118202000089X
38. Ten Hove RJ, Verweij JJ, Vereecken K, Polman K, Dieye L, van Lieshout L. Multiplex real-time PCR for the detection and quantification of Schistosoma mansoni and S. haematobium infection in stool samples collected in northern Senegal. Trans R Soc Trop Med Hyg (2008) 102(2):179–85. doi: 10.1016/j.trstmh.2007.10.011
39. Meurs L, Brienen E, Mbow M, Ochola EA, Mboup S, Karanja DM, et al. Is PCR the next reference standard for the diagnosis of Schistosoma in stool? A comparison with microscopy in Senegal and Kenya. PloS Negl Trop Dis (2015) 9(7):e0003959. doi: 10.1371/journal.pntd.0003959
40. Cnops L, Tannich E, Polman K, Clerinx J, Van Esbroeck M. Schistosoma real-time PCR as diagnostic tool for international trvellers and migrants. Trop Med Int Health (2012) 17(10):1208–16. doi: 10.1111/j.1365-3156.2012.03060.x
41. Weerakoon KG, Gordon CA, Gobert GN, Cai P, McManus DP. Optimisation of a droplet digital PCR assay for the diagnosis of Schistosoma japonicum infection: A duplex approach with DNA binding dye chemistry. J Microbiol Methods (2016) 125:19–27. doi: 10.1016/j.mimet.2016.03.012
42. Weerakoon KG, Gordon CA, Williamas GM, Cai P, Gobert GN, Olveda RM, et al. Droplet digital PCR diagnosis of human schistosomiasis: Parasite cell-free DNA detection in diverse clinical samples. J Infect Dis (2017) 216:1611–22. doi: 10.1093/infdis/jix521
43. Engels D, Sinzinkayo E, Gryseels B. Day-to-day egg count fluctuation in Schistosoma mansoni infection and its operational implications. Am J Trop Med Hyg (1996) 54:319–24. doi: 10.4269/ajtmh.1996.54.319
44. Siqueira LM, Gomes LI, Oliveira E, Oliveira ER, Oliveira ÁA, Enk MJ, et al. Evaluation of parasitological and molecular techniques for the diagnosis and assessment of cure of schistosomiasis mansoni in a low transmission area. Mem Inst Oswaldo Cruz (2015) 110(2):209–14. doi: 10.1590/0074-02760140375
45. Guegan H, Fillaux J, Charpentier E, Robert-Gangneux F, Chauvin P, Guemas E, et al. Real-time PCR for diagnosis of imported schistosomiasis. PloS Negl Trop Dis (2019) 13(9):e0007711. doi: 10.1371/journal.pntd.0007711
46. Doenhoff MJ. Is Schistosomicidal chemotherapy sub-curative? Implications for drug resistance. Parasitol Today (1998) 14(10):434–5. doi: 10.1016/S0169-4758(98)01315-5
47. Wichmann D, Poppert S, Von Thien H, Clerinx J, Dieckmann S, Jensenius M, et al. Prospective European-wide multicentre study on a blood based real-time PCR for the diagnosis of acute schistosomiasis. BMC Infect Dis (2013) 13:55. doi: 10.1186/1471-2334-13-55
48. Lu D-B, Deng Y, Ding H, Liang Y-S, Webster JP. Simgle-sex schistosome infections of definitive hosts: implications for epidemiology and disease control in a changing word. PloS Pathog (2018) 14(3):e1006817. doi: 10.1371/journal.ppat.1006817
49. Burlandy-Soares LC, Dias LCS, Kanamura HY, Oliveira EJ, Ciaravolo RM. Schistosomiasis mansoni: follow-aup of control program based on parasitologic and serologic methods in a Brazilian community of low endemicity. Mem Inst Oswaldo Cruz (2003) 98(6):853–9. doi: 10.1590/S0074-02762003000600025
50. Pica-Mattoccia L, Cioli D. Sex and stage related sensitivity of Schistosoma mansoni to in vivo and in vitro praziquantel treatment. Int J Parasitol (2004) 34(4):527–33. doi: 10.1016/j.ippara.2003
Keywords: intestinal schistosomiasis, laboratory diagnosis, Kato–Katz technique, saline gradient technique, real-time PCR
Citation: Siqueira LMV, Senra C, de Oliveira ÁA, Carneiro NFF, Gomes LI, Rabello A, Coelho PMZ and Oliveira E (2021) A Real-Time PCR Assay for the Diagnosis of Intestinal Schistosomiasis and Cure Assessment After the Treatment of Individuals With Low Parasite Burden. Front. Immunol. 11:620417. doi: 10.3389/fimmu.2020.620417
Received: 22 October 2020; Accepted: 24 December 2020;
Published: 16 March 2021.
Edited by:
Thiago Almeida Pereira, Stanford University, United StatesReviewed by:
Jose Mauro Peralta, Federal University of Rio de Janeiro, BrazilBonnie Webster, Natural History Museum, United Kingdom
Copyright © 2021 Siqueira, Senra, de Oliveira, Carneiro, Gomes, Rabello, Coelho and Oliveira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Edward Oliveira, ZWR3YXJkLm9saXZlaXJhQGZpb2NydXouYnI=