 Agnieszka Tomaszewska1*†
Agnieszka Tomaszewska1*† Madan Jagasia2†Eric Beohou3Steffie van der Werf4
Madan Jagasia2†Eric Beohou3Steffie van der Werf4 Didier Blaise5Edward Kanfer6Noel Milpied7Péter Reményi8
Didier Blaise5Edward Kanfer6Noel Milpied7Péter Reményi8 Fabio Ciceri9
Fabio Ciceri9 Jean H. Bourhis10Patrice Chevallier11Carlos Solano12Gerard Socié13
Jean H. Bourhis10Patrice Chevallier11Carlos Solano12Gerard Socié13 Benedetto Bruno14Alessandro Rambaldi15
Benedetto Bruno14Alessandro Rambaldi15 Luca Castagna16
Luca Castagna16 Nicolaus Kröger17Paolo Corradini18Boris Afanasyev19Marco Ladetto20Dietger Niederwieser21Christof Scheid22Henrik Sengeloev23Frank Kroschinsky24
Nicolaus Kröger17Paolo Corradini18Boris Afanasyev19Marco Ladetto20Dietger Niederwieser21Christof Scheid22Henrik Sengeloev23Frank Kroschinsky24 Ibrahim Yakoub-Agha25
Ibrahim Yakoub-Agha25 Helene Schoemans26
Helene Schoemans26 Christian Koenecke27
Christian Koenecke27 Olaf Penack28
Olaf Penack28 Zinaida Perić29
Zinaida Perić29 Hildegard Greinix30
Hildegard Greinix30 Rafael F. Duarte31Grzegorz W. Basak1
Rafael F. Duarte31Grzegorz W. Basak1- 1Department of Hematology, Transplantology and Internal Medicine, Medical University of Warsaw, Warsaw, Poland
- 2Division of Hematology-Oncology, Vanderbilt University Medical Center, Nashville, TN, United States
- 3EBMT Paris Statistical Unit, Paris, France
- 4EBMT Data Office, Leiden, Netherlands
- 5Institut Paoli Calmettes, Marseille, France
- 6Hammersmith Hospital, Imperial College Healthcare, London, United Kingdom
- 7Hopital Haut-leveque, Bordeaux, France
- 8Dél-pesti Centrumkórház, Budapest, Hungary
- 9Ospedale San Raffaele s.r.l., Milan, Italy
- 10Gustave Roussy Institute de Cancérologie, Val de Marne, France
- 11CHU Nantes, Nantes, France
- 12Hospital Clínico Universitario, Valencia, Spain
- 13Hopital St. Louis, Paris, France
- 14A.O.U. Citta della Salute e della Scienza di Torino, Universita di Torino, Turin, Italy
- 15Azienda Ospedaliera Papa Giovanni XXIII, Bergamo, Italy
- 16Istituto Clinico Humanitas, Milan, Italy
- 17University Hospital Eppendorf, Hamburg, Germany
- 18Fondazione IRCCS Istituto Nazionale dei Tumori, University of Milano, Milan, Italy
- 19First State Pavlov Medical University of St. Petersburg, St. Petersburg, Russia
- 20H SS. Antonio e Biagio, Alessandria, Italy
- 21University Hospital Leipzig, Leipzig, Germany
- 22University of Cologne, Cologne, Germany
- 23Rigshospitalet, Copenhagen, Denmark
- 24Universitätsklinikum Dresden, Dresden, Germany
- 25Hôpital Huriez CHRU, Lille, France
- 26University Hospitals Leuven and KU Leuven, Leuven, Belgium
- 27Hannover Medical School, Hannover, Germany
- 28Department of Hematology, Oncology, and Tumor Immunology, Charité – Universitätsmedizin Berlin, Berlin, Germany
- 29University Hospital Center Rebro, Zagreb, Croatia
- 30Department of Hematology and Oncology, Medical University of Graz, Graz, Austria
- 31Hospital Universitario Puerta de Hierro Majadahonda, Madrid, Spain
Rituximab (R) is increasingly incorporated in reduced intensity conditioning (RIC) regimens for allogeneic hematopoietic cell transplantation (alloHCT) in patients with B-cell malignancies, not only to improve disease control, but also to prevent graft-versus-host disease (GVHD). There are no randomized prospective data to validate this practice, although single center data and the CIBMTR analysis have shown promising results. We aimed at validation of these findings in a large registry study. We conducted a retrospective analysis using the EBMT registry of 3,803 adult patients with B-cell malignancies undergoing alloHCT (2001–2013) with either rituximab (R-RIC-9%) or non-rituximab (RIC-91%) reduced intensity regimens respectively. Median age and median follow up were 55 years (range 19.1–77.3) and 43.2 months (range 0.3–179.8), respectively. There was no difference in transplant outcomes (R-RIC vs RIC), including 1-year overall survival (69.9% vs 70.7%), 1-year disease-free survival (64.4% vs 62.2%), 1-year non-relapse mortality (21% vs 22%), and day-100 incidence of acute GVHD 2-4° (12% vs 12%). In summary, we found that addition of rituximab in RIC regimens for B-cell malignancies had no significant impact on major transplant outcome variables. Of note, data on chronic GVHD was not available, limiting the conclusions that can be drawn from the present study.
Introduction
An optimal outcome after allogeneic hematopoietic cell transplantation (alloHCT), includes not only cure of the underlying malignancy, but minimizing the incidence of GVHD, both acute and chronic. Reduced intensity conditioning (RIC) allows patients in higher age groups and/or with significant comorbidities to access alloHCT, while minimizing transplant related mortality, and preserving graft-versus-tumor effect (1, 2).
RIC regimens have historically been designed to be unrelated to underlying disease, but at the same time, choice of agents used often has a scientific rationale for offering tumor-specific disease control (3, 4).
RIC regimens containing rituximab, an anti-CD20 antibody with anti-neoplastic activity, have been included for targeting B-cell malignancies and single center studies suggest a superior alloHCT outcome compared to center-specific historical cohorts (4–6). Recent data from the Center of International Blood and Marrow Transplant Registry (CIBMTR) suggests that the effect of rituximab may be confined to some subsets of patients or when specific preparative regimens are used (7). We studied the effect of rituximab using the European Society for Blood and Marrow Transplantation (EBMT) registry to attempt to cross validate the above mentioned findings.
Methods
Patient Selection and Treatment Plan
We analyzed 3,803 patients with B cell lymphoid malignancies (FL – follicular lymphoma, DLBCL – diffuse large B cell lymphoma, MCL – mantle cell lymphoma, CLL – chronic lymphocytic leukemia, SLL – small lymphocytic lymphoma), who received a RIC allo-HCT between 2001 and 2013 and were reported to the registry of the EBMT. Patients undergoing myeloablative HCT (total body irradiation > 6 Gy, or busulfan > 9 mg/kg) or alemtuzumab containing regimens were excluded. Umbilical cord and haploidentical HCT were excluded. All RIC or R-RIC regimens were included and were stratified as fludarabine (Flu), busulfan (Bu2), other FluBu regimens, other Flu containing regimens or other regimens.
Patients undergoing alloHCT often receive anti-T-cell globulin (ATG) as a part of the conditioning regimen for GVHD prophylaxis. Thus, regimens were stratified for ATG or non-ATG regimens, within each group of RIC or R-RIC, for analyses. Details of ATG dosing and schedule were not available. Similarly, the details of the dosing and schedule of rituximab were not available in the EBMT registry. GVHD prophylaxis details were captured as cyclosporine (CSA), mycophenolate mofetil (MMF), CSA plus MMF, CSA plus methotrexate (MTX), or other regimens.
Baseline demographics including follow-up, age at transplant, gender, diagnosis, disease status at alloHCT, year of alloHCT, donor type, recipient-donor gender match or mismatch, source of stem cells were obtained from the registry.
Maximum acute GVHD grade within the first 100 days was available in the majority of patients. In contrast, chronic GVHD status was available in a small minority of the patients and was not analyzed. Transplant outcomes of overall survival (OS), relapse incidence, and non-relapse mortality were available.
Statistical Analysis
Comparison of patient and transplant characteristics was conducted using the Mann-Whitney test for continuous variables and the chi-squared test for categorical variables. Overall survival, progression-free survival, and GVHD-free/relapse-free survival (GRFS) were estimated using the Kaplan-Meier method. Multivariable prediction models for continuous and binary outcomes were made using standard and logistic regression, respectively. Based on comparison of patient and transplant characteristics, age at HCT, year of HCT, preparative regimen, donor type, and GVHD prophylaxis were included in the multivariate analyses. Cumulative incidence functions were calculated using Gray’s Method (8). Cumulative incidence of relapse, and non-relapse mortality, were calculated. P values less than 0.05 were considered statistically significant. All statistical analyses were performed using R software by the EBMT statistical team.
Results
Patient Characteristics
Table 1 outlines patient and transplant characteristics. The overall cohort consisted of 3,803 patients (R-RIC: 350; RIC: 3,453) with a median follow up of 43.2 months (range, 0.3–179.8). Patients receiving R-RIC had a lower median age (54.2 y; range, 19.8–74.1) compared to RIC (55 y; range, 19.1–77.3) (p=0.01), and underwent transplant more recently (2001–2007: 35.2% RIC and 19.1% R-RIC, 2008–2013: 64.8% RIC, 80.9% R-RIC; median year of HCT: R-RIC vs. RIC; 2010 vs. 2009, p<0.0001). GVHD prophylaxis regimens were significantly different with higher incidence of CSA plus MMF in the RIC group and a higher incidence of CSA plus MTX in the R-RIC group. Preparative regimens varied significantly (p<0.0001) with fludarabine plus cyclophosphamide being more commonly used in the R-RIC group (46.3%) compared to the RIC group (23.9%).
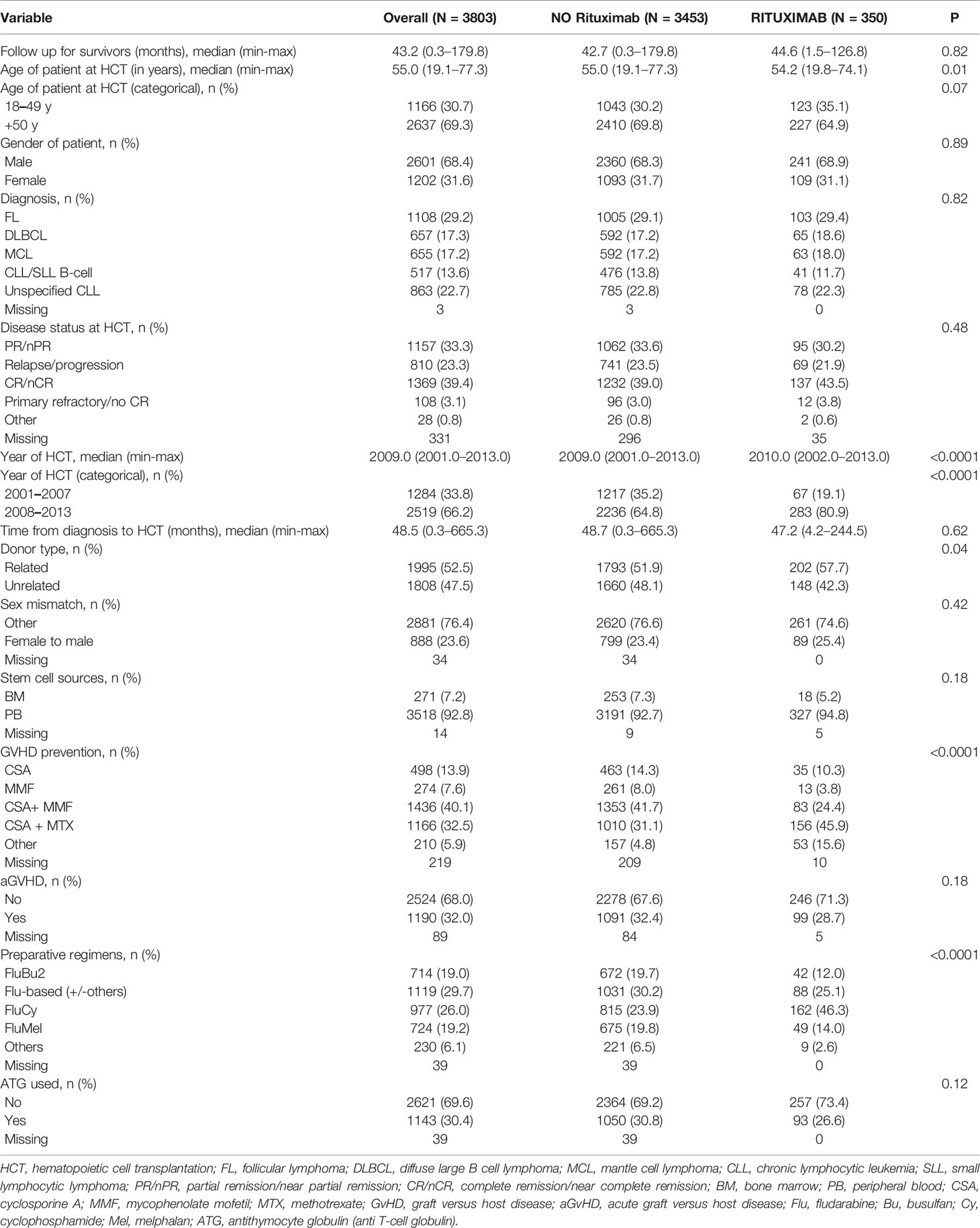
Table 1 Pre-transplant and transplant characteristics.
Survival, Relapse, Progression-Free Survival, Non-Relapse Mortality and 100-Day Cumulative Incidence of Acute GVHD
Table 2 outlines the above endpoints. There were no significant differences in the 1-year OS, 1-year relapse rate, 1-year non-relapse mortality, 1-year disease free survival, and the grade 2–4 aGvHD incidence between analysed cohorts of patients as well as there were no differing causes of death (Figure 1 in the manuscript and Table 3S in supplementary materials). Chronic GVHD analyses were not undertaken given the extent of missing data, and lack of data in the context of the NIH classification system.
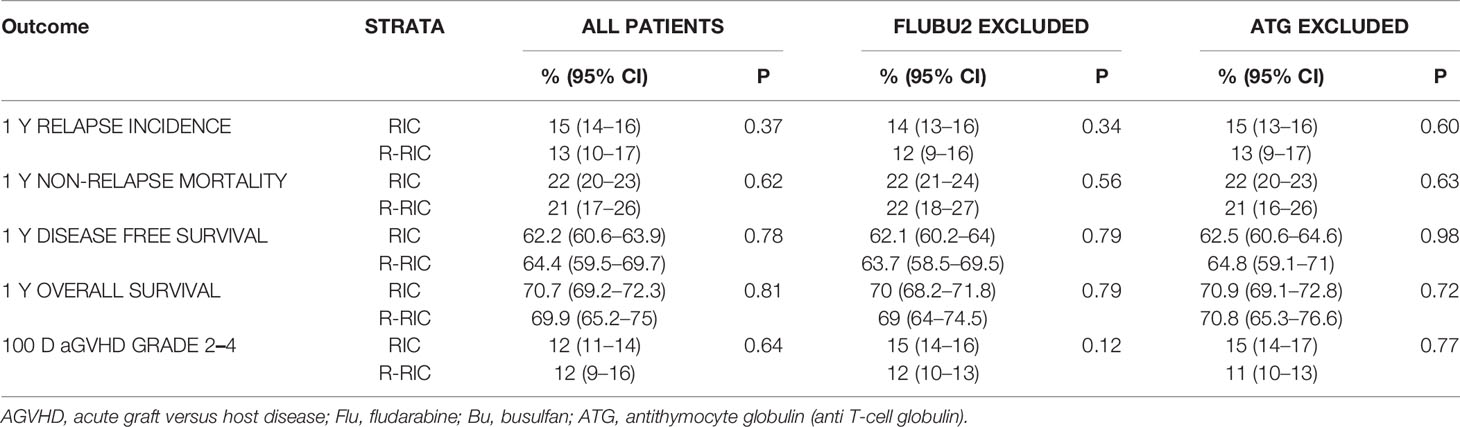
Table 2 Transplant outcomes for entire cohort, patients excluding those receiving fludarabine plus busulfan, and patients excluding those receiving anti-T-cell globulin.
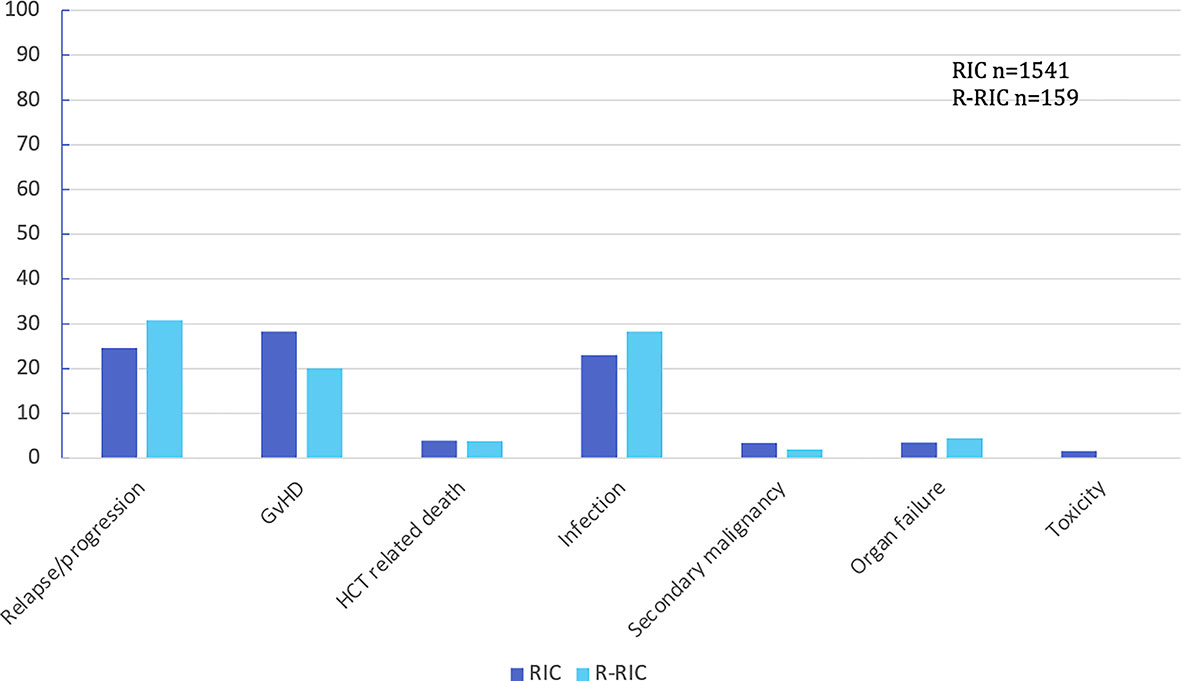
Figure 1 Main causes (percentages) of death in patients’ cohorts: RIC vs R-RIC. GvHD, graft versus host disease; HCT, hematopoietic cell transplantation.
Subset Analyses
Given the differential impact of preparative regimens on outcomes as reported by the CIBMTR (7), we studied two subsets (all patients excluding those receiving fludarabine plus busulfan [FluBu2 excluded]; and all patients excluding those receiving ATG [ATG excluded]). The percent of patients in these various subsets and use of GVHD prophylaxis in these subsets are outlined in supplementary materials Table 1S and 2S, respectively. Contrary to the findings in the CIBMTR cohort, there were no differences in the outcome endpoints in multivariable analyses, adjusted for age, year of HCT, GVHD prophylaxis and donor type (Table 3).
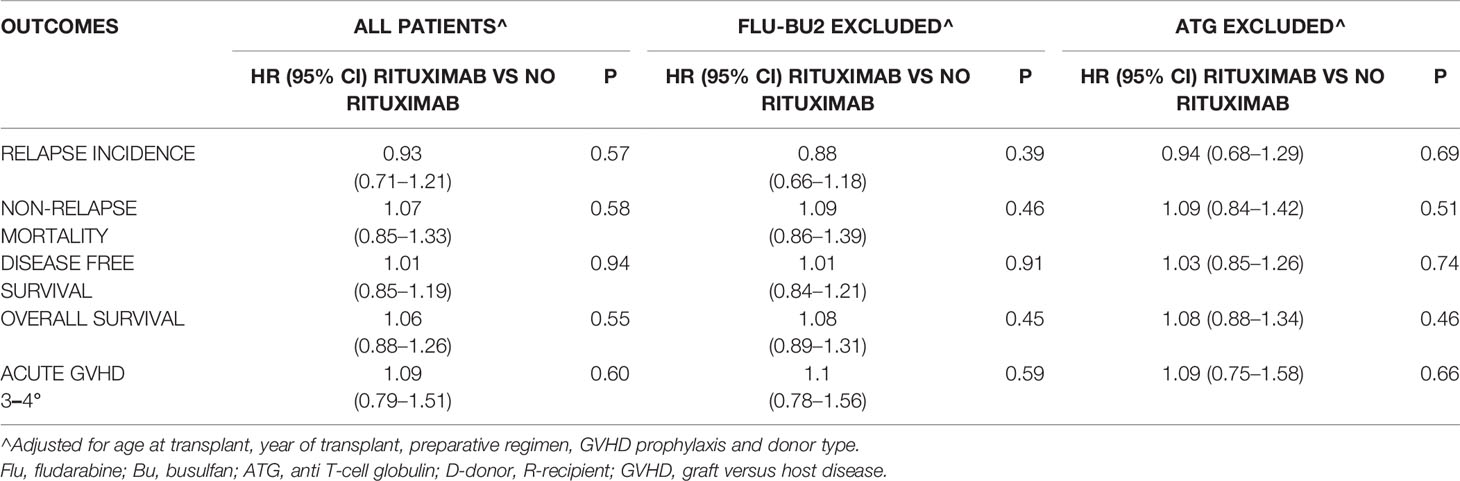
Table 3 Transplant outcomes: stratified by patients subsets.
Discussion
Historically, preparative regimens have remained unrelated to the underlying disease (1–3). The goal of the regimen is to achieve adequate immunoablation to facilitate donor cell engraftment, while maintaining adequate control of the underlying disease (1, 2). Although, there are a multitude of regimens in common practice, there is little prospective data that regimens truly affect HCT outcomes in patients with B-cell NHL. Clinical observations of reduced GVHD in patients having received rituximab in chemotherapy regimens preceding HCT were noted prior to the elucidation of B-cell biology and chronic GVHD (4, 5). Rituximab treatment within six months prior to RIC allo-HCT for any hematologic malignancy has been shown to reduce the incidence of extensive cGVHD from 45.8% to 20.1% (9).
In this study, we report that the addition of rituximab to RIC regimen had no incremental impact on outcomes of alloHCT in patients with B-cell malignancies. This study is in contrast to the CIBMTR analyses showing that the addition of rituximab was associated with improved PFS (7). It is interesting to note that although a PFS advantage was seen in the entire CIBMTR cohort, the survival benefit was confined only to patients not receiving fludarabine plus busulfan preparative regimen and with a higher cumulative dose of rituximab (7). In presented study the cohort of patients was larger than in the CIBMTR study (3,803 vs 1,401) but the prevalence of rituximab in preparative regimens for B-cell malignancies in our study was approximately 10% in contrast to 27% in the CIBMTR one.
In a separate CIBMTR study confined only to patients with follicular lymphoma, comparing the two most commonly used RIC approaches – fludarabine and busulfan (FluBu) versus fludarabine, cyclophosphamide, and rituximab (FCR) reported survival outcomes (OS, PFS, NRM) were not significantly different (10). The only noted benefit in this study was a decrease in incidence of chronic GVHD with R-RIC compared to RIC regimens (10). Data from the retrospective study of Kennedy et al. showed that use of RIC with FCR was associated with decreased chronic GVHD and improved OS (6).
In our study, data on chronic GVHD incidence and severity in the context of the NIH classification system was not available, limiting the conclusions that can be drawn.
Rituximab was used in the treatment of chronic GVHD and studied as a pre-emptive strategy in post-HCT setting for prevention of chronic GVHD (9, 11–13). It is an established second-line agent in the treatment of steroid-refractory cGVHD (12–16), and has been used in conjunction with corticosteroids as initial cGVHD therapy with moderate success (17). There is increasing evidence that B cells play a role in cGVHD pathogenesis (18–20), and it has been hypothesized that reducing B cell alloimmunity may decrease cGVHD incidence (16). Alloreactive antibodies against H-Y antigens are strongly associated with the occurrence of cGVHD (21, 22), and post-transplant rituximab has been shown to decrease allogeneic H-Y antibody development (16).
The above data may suggest that the effect of rituximab in modulating outcome is modest at the best and confined to regimens which are inherently associated with a slower rate of converting to full donor chimerism (non-busulfan containing regimens) (6, 7, 10). The survival benefit was noted in the high dose rituximab group (7).
Finally, what is the role of anti-thymocyte globulin in rituximab containing preparative regimens? The cumulative incidence of grade 3–4 acute GVHD, relapse, non-relapse mortality, disease-free, and overall survival did not show any significant differences in patients who did not receive ATG in the preparative regimen.
However, it does not answer the question if ATG can be safely omitted without compromising outcomes when rituximab containing preparative regimens are used for unrelated donor transplants. As preparative regimens are often “bundled” together with certain GVHD prophylaxis, it is challenging to study the differential impact of the regimen versus the GVHD prophylaxis. In our study, given the large sample size, we could adjust for the GVHD prophylaxis and did not see any interaction.
In conclusion, we could not demonstrate the benefit of adding rituximab to RIC regimens for B-cell malignancies on HCT outcomes. Although our study was limited by the absence of chronic GVHD data, the larger sample size in contrast to the positive the CIBMTR study, suggests that the effect of rituximab needs to be systematically re-examined. Many centers have adopted this institutional practice, despite the lack of well conducted mechanistic studies to optimize the dosage and schedule. The cost of rituximab is not trivial, and the transplant community needs to take a step back to re-examine the role of B-cell inhibitors in the preparative regimens. It is unlikely that a phase 3 study will ever be done to address this question. However, with the advent of more targeted B-cell receptor or signaling pathway inhibitors it is critical, that the transplant community should follow the conventional pathway of drug development with carefully conducted phase I studies, prior to accepting agents approved for other indications and integrating it into the preparative regimens.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author Contributions
AT and MJ contributed equally to writing this manuscript. EB analyzed the data. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2020.613954/full#supplementary-material
References
1. Khouri IF, Saliba RM, Giralt SA, Lee MS, Okoroji GJ, Hagemeister FB, et al. Nonablative allogeneic hematopoietic transplantation as adoptive immunotherapy for indolent lymphoma: low incidence of toxicity, acute graft-versus-host disease, and treatment-related mortality. Blood (2001) 98:3595–9. doi: 10.1182/blood.V98.13.3595
2. McSweeney PA, Niederwieser D, Shizuru JA, Sandmaier BM, Molina AJ, Maloney DG, et al. Hematopoietic cell transplantation in older patients with hematologic malignancies: replacing high-dose cytotoxic the rapy with graft-versus-tumor effects. Blood (2001) 97:3390–400. doi: 10.1182/blood.V97.11.3390
3. Slavin S, Nagler A, Naparstek E, Kapelushnik Y, Aker M, Cividalli G, et al. Nonmyeloablative stem cell transplantation and cell therapy as an alternative to conventional bone marrow transplantation with lethal cytoreduction for the treatment of malignant and nonmalignant hematologic diseases. Blood (1998) 91:756–63. doi: 10.1182/blood.V91.3.756.756_756_763
4. Khouri IF, McLaughlin P, Saliba RM, Hosing C, Korbling M, Lee MS, et al. Eight-year experience with allogeneic stem cell transplantation for relapsed follicular lymphoma after nonmyeloablative conditioning with fludarabine, cyclophosphamide, and rituximab. Blood (2008) 111:5530–6. doi: 10.1182/blood-2008-01-136242
5. Sauter CS, Barker JN, Lechner L, Zheng J, Devlin SM, Papadopoulos EB, et al. A phase II study of a nonmyeloablative allogeneic stem cell transplant with peritransplant rituximab in patients with B cell lymphoid malignancies: favorably durable event-free survival in chemosensitive patients. Biol Blood Marrow Transplant (2014) 20:354–60. doi: 10.1016/j.bbmt.2013.11.029
6. Kennedy VE, Savani BN, Greer JP, Kassim AA, Engelhardt BG, Goodman SA, et al. Reduced-Intensity Conditioning with fludarabine, cyclophosphamide, and rituximab is associated with improved outcomes compared with fludarabine and busulfan after allogeneic stem cell transplantation for B cell malignancies. Biol Blood Marrow Transplant (2016) 22:1801–7. doi: 10.1016/j.bbmt.2016.06.029
7. Epperla N, Ahn KW, Ahmed S, Jagasia M, DiGilio A, Devine SM, et al. Rituximab-containing reduced-intensity conditioning improves progression-free survival following allogeneic transplantation in B cell non-Hodgkin lymphoma. J Hematol Oncol (2017) 10:117–28. doi: 10.1186/s13045-017-0487-y
8. Scrucca L, Santucci A, Aversa F. Competing risk analysis using R: an easy guide for clinicians. Bone Marrow Transplant (2007) 40:381–7. doi: 10.1038/sj.bmt.1705727
9. van Dorp S, Pietersma F, Wolfl M, Verdonck LF, Petersen EJ, Lokhorst HM, et al. Rituximab treatment before reduced-intensity conditioning transplantation associates with a decreased incidence of extensive chronic GVHD. Biol Blood Marrow Transplant (2009) 15:671–8. doi: 10.1016/j.bbmt.2009.02.005
10. Epperla N, Ahn KW, Armand P, Jaglowski S, Ahmed S, Kenkre VP, et al. Fludarabine and Busulfan versus Fludarabine, Cyclophosphamide, and Rituximab as Reduced-Intensity Conditioning for Allogeneic Transplantation in Follicular Lymphoma. Biol Blood Marrow Transplant (2018) 24:78–85. doi: 10.1016/j.bbmt.2017.10.011
11. Cutler C, Kim HT, Bindra B, Sarantopoulos S, Ho VT, Chen YB, et al. Rituximab prophylaxis prevents corticosteroid-requiring chronic GVHD after allogeneic peripheral blood stem cell transplantation: results of a phase 2 trial. Blood (2013) 122:1510–7. doi: 10.1182/blood-2013-04-495895
12. Cutler C, Miklos D, Kim HT, Treister N, Woo SB, Bienfang D, et al. Rituximab for steroid-refractory chronic graft-versus-host disease. Blood (2006) 108:756–62. doi: 10.1182/blood-2006-01-0233
13. Kharfan-Dabaja MA, Mhaskar AR, Djulbegovic B, Cutler C, Mohty M, Kumar A. Efficacy of rituximab in the setting of steroid-refractory chronic graft-versus-host disease: a systematic review and meta-analysis. Biol Blood Marrow Transplant (2009) 15:1005–13. doi: 10.1016/j.bbmt.2009.04.003
14. Mohty M, Marchetti N, El-Cheikh J, Faucher C, Furst S, Blaise D. Rituximab as salvage therapy for refractory chronic GVHD. Bone Marrow Transplant (2008) 41:909–11. doi: 10.1038/bmt.2008.12
15. Ratanatharathorn V, Ayash L, Reynolds C, Silver S, Reddy P, Becker M, et al. Treatment of chronic graft-versus-host disease with anti-CD20 chimeric monoclonal antibody. Biol Blood Marrow Transplant (2003) 9:505–11. doi: 10.1016/S1083-8791(03)00216-7
16. Arai S, Sahaf B, Narasimhan B, Chen GL, Jones CD, Lowsky R, et al. Prophylactic rituximab after allogeneic transplantation decreases B-cell alloimmunity with low chronic GVHD incidence. Blood (2012) 119:6145–54. doi: 10.1182/blood-2011-12-395970
17. Sahaf B AS, Otani J, Schoenrock K, Logan A, Miklos DB. Rituximab provides steroid-sparing therapy in new-onset chronic graft-versus-host disease. BMT Tandem Meet Abstr (2013) 19:S140. doi: 10.1016/j.bbmt.2012.11.081
18. Kapur R, Ebeling S, Hagenbeek A. B-cell involvement in chronic graft-versus-host disease. Haematologica (2008) 93:1702–11. doi: 10.3324/haematol.13311
19. Sarantopoulos S, Blazar BR, Cutler C, Ritz J. B cells in chronic graft-versus-host disease. Biol Blood Marrow Transplant (2015) 21:16–23. doi: 10.1016/j.bbmt.2014.10.029
20. Shimabukuro-Vornhagen A, Hallek MJ, Storb RF, von Bergwelt-Baildon MS. The role of B cells in the pathogenesis of graft-versus-host disease. Blood (2009) 114:4919–27. doi: 10.1182/blood-2008-10-161638
21. Miklos DB, Kim HT, Miller KH, Guo L, Zorn E, Lee SJ, et al. Antibody responses to H-Y minor histocompatibility antigens correlate with chronic graft-versus-host disease and disease remission. Blood (2005) 105:2973–8. doi: 10.1182/blood-2004-09-3660
Keywords: transplantation, B-cell malignancy, conditioning, rituximab, non-relapse mortality after hematopoietic cell transplantation, graft-versus-host disease
Citation: Tomaszewska A, Jagasia M, Beohou E, van der Werf S, Blaise D, Kanfer E, Milpied N, Reményi P, Ciceri F, Bourhis JH, Chevallier P, Solano C, Socié G, Bruno B, Rambaldi A, Castagna L, Kröger N, Corradini P, Afanasyev B, Ladetto M, Niederwieser D, Scheid C, Sengeloev H, Kroschinsky F, Yakoub-Agha I, Schoemans H, Koenecke C, Penack O, Perić Z, Greinix H, Duarte RF and Basak GW (2021) Addition of Rituximab in Reduced Intensity Conditioning Regimens for B-Cell Malignancies Does Not Influence Transplant Outcomes: EBMT Registry Analyses Following Allogeneic Stem Cell Transplantation for B-Cell Malignancies. Front. Immunol. 11:613954. doi: 10.3389/fimmu.2020.613954
Received: 04 October 2020; Accepted: 16 December 2020;
Published: 02 February 2021.
Edited by:
Hermann Einsele, Julius Maximilian University of Würzburg, GermanyReviewed by:
Federico Simonetta, Geneva University Hospitals (HUG), SwitzerlandTomomi Toubai, Yamagata University, Japan
Copyright © 2021 Tomaszewska, Jagasia, Beohou, van der Werf, Blaise, Kanfer, Milpied, Reményi, Ciceri, Bourhis, Chevallier, Solano, Socié, Bruno, Rambaldi, Castagna, Kröger, Corradini, Afanasyev, Ladetto, Niederwieser, Scheid, Sengeloev, Kroschinsky, Yakoub-Agha, Schoemans, Koenecke, Penack, Perić, Greinix, Duarte and Basak. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Agnieszka Tomaszewska, YWduaWVzemthX3RvbWFzemV3c2thQG9uZXQuZXU=
†These authors have contributed equally to this work