 Lifang Wen
Lifang Wen Susanne Krauss-Etschmann2,3
Susanne Krauss-Etschmann2,3 Xinhua Yu
Xinhua Yu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Immunol. , 25 January 2018
Sec. Immunological Tolerance and Regulation
Volume 9 - 2018 | https://doi.org/10.3389/fimmu.2018.00066
This article is part of the Research Topic Autoantibodies View all 89 articles
Chronic obstructive pulmonary disease (COPD), the fourth leading cause of death worldwide, is characterized by irreversible airflow limitation based on obstructive bronchiolitis, emphysema, and chronic pulmonary inflammation. Inhaled toxic gases and particles, e.g., cigarette smoke, are major etiologic factors for COPD, while the pathogenesis of the disease is only partially understood. Over the past decade, an increasing body of evidence has been accumulated for a link between COPD and autoimmunity. Studies with clinical samples have demonstrated that autoantibodies are present in sera of COPD patients and some of these antibodies correlate with specific disease phenotypes. Furthermore, evidence from animal models of COPD has shown that autoimmunity against pulmonary antigens occur during disease development and is capable of mediating COPD-like symptoms. The idea that autoimmunity could contribute to the development of COPD provides a new angle to understand the pathogenesis of the disease. In this review article, we provide an advanced overview in this field and critically discuss the role of autoantibodies in the pathogenesis of COPD.
Chronic obstructive pulmonary disease (COPD) is a major public health problem affecting more than 200 million people worldwide and leading to millions of death annually (1). COPD patients suffer from a progressive and not fully reversible airflow limitation. Pathologically, COPD is characterized by persistent pulmonary inflammation, obstruction of the small airways (obstructive bronchiolitis) and structural changes of the airways (emphysema) (2). It is widely accepted that COPD is triggered by inhaled toxic gases and particles. However, the pathogenesis of COPD remains largely unclear (2, 3).
Cigarette smoking (CS) is the major etiologic and risk factor for COPD (4, 5), and smoking cessation is beneficial for patients in terms of lung function (6). However, smoke cessation does not attenuate the pulmonary inflammation once COPD is established in patients (7, 8). The persistence of the pulmonary inflammation after smoking cessation and the presence of well-organized lymphoid follicles around small airways and lung parenchyma of COPD patients (9–11) implicate that there are memory adaptive immune responses to non-cigarette antigens, such as autoantigens, commensal microbiota, and infectious pathogens (8, 12, 13). Among these candidates, autoantigens are of specific interest because both clinical and experimental evidence suggest that CS is capable of triggering autoimmunity. Thus, the exploration of the contribution of autoimmune responses to the development of COPD could provide a new angle for understanding the pathogenesis of this disease.
In 2002, Cosio et al. proposed a novel concept that COPD could be considered as an autoimmune disease triggered by smoking (14). In 2007, Lee et al. reported that emphysema is characterized by the presence of humoral and cellular autoimmune responses against elastin, an extracellular protein important for lung integrity (12), for the first time showing evidence for a role of autoimmunity in COPD pathogenesis. Thereafter, many efforts have been made to determine the role of autoimmunity in the development of COPD by the use of clinical samples and animal models. In this review article, we aim to summarize recent advances in this field, discuss the contribution of autoimmunity to COPD, and outline prospects for future research. Since the role of self-reactive T cells in COPD has been reviewed elsewhere (14–16), we focus here on autoantibodies in COPD and its animal models.
According to their targets, studies investigating the presence of autoantibodies in COPD can be roughly categorized into two groups, those addressing autoantibodies against undefined and those addressing defined antigens (Table 1).
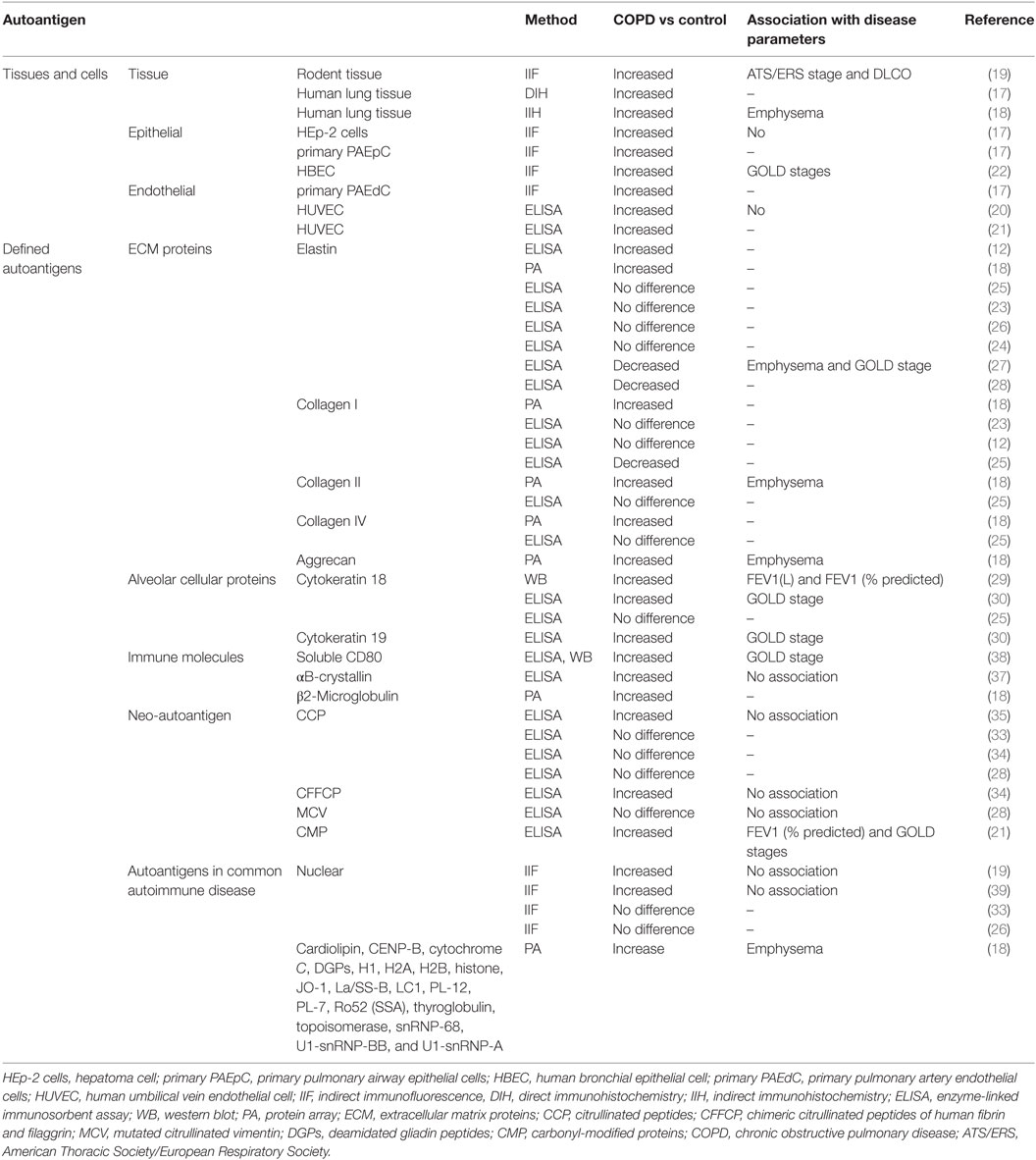
Table 1. Summary of autoantibodies in COPD.
The first group consists of studies in which autoantibodies against undefined autoantigens, such as tissues or cells were investigated. Given that the majority of autoantigens in COPD is probably unknown, determination of autoantibodies against lung tissue or its major cell types, e.g., epithelial or endothelial cells provides a proof-of-principle evidence for the presence of autoantibodies in this disease. In 2008, Feghali-Bostwick and colleagues detected IgG deposition within alveolar septa and small airway walls by immunohistochemical staining in six out of six of patients with severe COPD, but in none of six controls (17) indicating for the first time that anti-tissue antibodies are present in COPD patients. Such anti-tissue antibodies in COPD were also described in another study using indirect immunohistochemical staining in which Packard et al. showed that IgG from COPD patients have a higher binding capability to non-smoker lung tissue section than IgG from healthy smokers (18). In addition, anti-tissue antibodies in COPD could also be detected using rodent tissues as antigen (19) confirming the presence of anti-tissue antibodies.
Aside from studying anti-tissue autoantibodies, Feghali-Bostwick et al. went on to investigate autoantibodies more specifically directed against epithelial and endothelial cells (17). Their results showed that the prevalence of autoantibodies against epithelial cells, including both hepatoma (HEp-2) cell and primary pulmonary artery epithelial cells, is significantly higher in COPD patients as compared with smoker or non-smoker (17). In addition, 50% of the COPD patients are also characterized by autoantibodies against primary pulmonary artery endothelial cells (17). This study shows for the first time the presence of anti-epithelial and anti-endothelial autoantibodies in COPD patients. By using a cell-based enzyme-linked immunosorbent assay with human umbilical vein endothelial cells (HUVECs) as coated antigen, two independent research groups confirmed the presence of anti-endothelial IgG in COPD patients (20, 21). Recently, the presence of anti-epithelial IgG has also been shown in a study using human bronchial epithelial cells as target (22). Taken together, these studies demonstrate convincingly that autoantibodies against lung tissue as well as pulmonary epithelial and endothelial cells are detectable in patients with COPD.
In the second group of studies, autoantibodies against defined antigens suspected to be present in or functionally related to the disease were investigated. This group includes extracellular matrix (ECM) proteins, cellular proteins from pulmonary cells, neo-autoantigens, immune molecules, and autoantigens in common autoimmune diseases.
The main function of cellular matrix proteins is to maintain the structure and integrity of the lung. Since degradation of matrix proteins is a hallmark of emphysema, these proteins are promising candidates for autoantigens in COPD. As mentioned earlier, autoantibodies against elastin have been detected in emphysema patients, showing for the first time the presence of autoantibodies in COPD (12). However, beside one exception (18), all following studies failed to confirm levels of anti-elastin antibodies in COPD patients surmounting those of healthy controls (23–26). Moreover, results from two independent groups showed that levels of anti-elastin antibodies are even lower in COPD patients than in healthy controls (27, 28). Beside elastin, collagens have been also extensively investigated as candidate autoantigens for COPD. Using an autoantigen array with 70 proteins, Packard and colleagues showed that levels of autoantibodies reactive to a broad spectrum of self-antigens are significantly higher in COPD patients involving emphysema than in healthy controls, including autoantibodies against collagen I, collagen II, and collagen IV (18). However, similar to the findings for anti-elastase antibodies, these results were not confirmed by other groups (12, 23, 25), keeping this issue under debate. Moreover, autoantibodies against aggrecan, another ECM protein, have been detected in patients with COPD (18).
In addition to ECM proteins, cellular proteins from pulmonary cells have also been regarded as potential autoantigens in COPD. Using immunoblotting assays with lysates prepared from alveolar cells as targets, Kuo et al. showed that autoantibodies against multiple cellular antigens are more frequently present in sera of COPD patients than in controls (29). Among those antigens, a 45-kDa cellular protein was identified as cytokeratin 18 (CK-18), an intermediate filament protein located in the intracytoplasmic cytoskeleton of epithelial tissue. Although this interesting finding has not been observed in a report based on a small number of samples (25), it has been confirmed in a recent study where 228 COPD patients and 136 controls were included (30). Here, Xiong et al. could show that the levels of circulating IgG, IgA, and IgM autoantibodies against CK-18 are elevated in COPD patients as compared with healthy controls (30). Furthermore, they also demonstrated that COPD patient express autoantibodies against another intermediate filament protein, CK-19, suggesting another cellular autoantigen for the diseases (30).
Neo-autoantigens are antigens expressed under specific pathophysiological conditions and are not ubiquitously in our body (31). Well-known neo-autoantigens in autoimmune diseases such as rheumatoid arthritis (RA) are citrullinated peptides or proteins which are generated by a posttranslational modification process occurring under certain inflammatory conditions (32). Results from several studies using different citrullinated peptides or proteins as antigens have shown that the frequencies of sera with anti-citrullinated protein antibody (ACPA) are very low in both COPD patients and healthy controls and without significant difference between these two groups (33–35). When the concentrations of ACPA are used for comparison, levels of anti-cyclic citrullinated peptide antibodies (CCP2) have been shown to be higher in sera of COPD patients than controls in one study (35), which was not confirmed by three other groups (28, 33, 34). Carbonyl-modified proteins (CMP) represent another type of neo-autoantigen, which are investigated in COPD. Oxidants, a major constituent of cigarette smoke, can cause the formation of carbonyl adducts on proteins in vivo (36), making it conceivable that autoantibodies against CMP are generated in COPD patients. To verify this hypothesis, Kirkham et al. determined levels of autoantibodies against CMP in the sera of COPD patients and controls. They found that antibody titers against carbonyl-modified self-protein were significantly increased in patients with COPD as compared with controls (21) showing the presence of such autoantibodies.
Apart from molecules from cells residing in the lung, some molecules from immune cells have also been shown to act as autoantigens in COPD. In 2012, Cherneva and colleagues reported that concentrations of autoantibodies against αB-crystallin (HspB5), a marker of innate immune activation, were increased in patients with COPD (37). Notably, according to this study, those autoantibodies are also present in inflammatory lung diseases suggesting that they are not COPD specific. Very recently, Luo et al. investigated autoantibodies against a soluble form of CD80 (sCD80), a co-stimulatory molecule for T cell activation, in sera of patients with COPD (38). They found that serum levels of anti-sCD80 were higher in patients with COPD than in controls and were positively correlated to inflammatory cytokines, e.g., IL-6 and IL-8 (38). Another immune molecule, β2-microglobulin that is a component of MHC class I molecules, has also been identified as an autoantigen in COPD (18).
Finally, autoantigens that have already been described in some common autoimmune diseases have also been investigated in COPD. For example, using indirect immunofluorescence staining, two independent groups have demonstrated that antinuclear antibodies are more prevalent in patients with COPD than healthy controls (19, 39). Although this difference has not been found in two other studies using the same detection method (26, 33), a study using protein arrays carrying 70 different antigens has confirmed that sera of patients with emphysema have autoantibodies reactive to many common nuclear antigens (18). In this study, the reactivity of sera derived from patients suffering from systemic lupus erythematosus (SLE) and RA was analyzed in comparison. Interestingly, emphysema-associated COPD was characterized by a lower autoantibody reactivity than SLE, but a higher than RA (18), suggesting COPD is indeed associated with a substantial level of autoimmunity.
Taken together, a number of previous studies have demonstrated that autoantibodies are present in patients with COPD. However, their determination and visualization appear to be autoantigen and method depending.
Aside from demonstrating the mere presence of autoantibodies, their potential correlation with disease parameters is important for their clinical relevance as biomarkers and could provide further evidence for a role of autoantibodies in COPD. Therefore, some studies with well characterized patients investigated the correlation between autoantibodies and clinical parameters of COPD.
By comparing subgroups of COPD patients categorized by clinical parameters, Nunez and colleagues demonstrated that the prevalence of anti-tissue antibodies are significantly different among patients groups with various disease severity as indicated by American Thoracic Society/European Respiratory Society (ATS/ERS) stage or diffusing capacity of carbon monoxide (DLCO). Patients with more severe disease showed higher prevalence of anti-tissue antibodies (19), suggesting an association between the presence of anti-tissue antibodies and an increased disease severity. In another study, Packard and colleagues described that sera from COPD patients with emphysema showed a higher anti-tissue antibody reactivity than sera from COPD patients without emphysema, suggesting an association of this autoantibody with emphysematous disease.
Recently, an association between severity of COPD and anti-epithelial antibodies has been demonstrated by Cheng et al. (22). They found that the prevalence of both anti-epithelial IgG and IgA are elevated in patients with severe disease (GOLD stage III or IV) as compared with patients with milder symptoms (GOLD stage I or II) (22). However, the association of anti-epithelial antibodies with disease severity has not been observed in a study with a rather small number of patients (17). Based on these inconsistent results from current studies, it remains unclear whether anti-epithelial antibodies are indeed associated with severity of COPD.
The correlation with clinical parameters of COPD has also been shown for autoantibodies directed against some defined antigens. For example, in Packard’s study, they found that serum levels of autoantibodies against many antigens are significantly higher than in COPD patients without emphysema (18). Disease severity is also reported to be associated with autoantibodies against several other antigens. In 2010, Kuo et al. reported that levels of autoantibodies against CK-18 were inversely correlated with lung function parameters (29). This correlation is confirmed by investigations of Xiong et al. who showed that circulating levels of both anti-CK-18 and anti-CK-19 autoantibodies correlate significantly with the severity of the disease (30). Besides anti-CK-18 and anti-CK-19, two other autoantibodies have been reported to correlate with disease severity in COPD. While the presence of anti-sCD80 antibodies was shown to be associated with a high GOLD stage (38), autoantibodies against CMP correlated with a high GOLD stage and were inversely correlated with lung function parameters (21).
Notably, anti-elastin antibodies are also associated with disease parameters, but in contrast to all autoantibodies mentioned earlier, in the opposite direction where a lower antibody titer was associated with more severe disease and emphysema (27).
Animal models are powerful research tools for investigating the pathogenesis of human diseases. For COPD, such models have been established in many species, including mice, rat, dog, monkey, and guinea pig (40). In consistence with findings in COPD patients, evidence from animal models also supports a role of autoantibodies in the pathogenesis of COPD, especially in those with emphysema (Table 2).
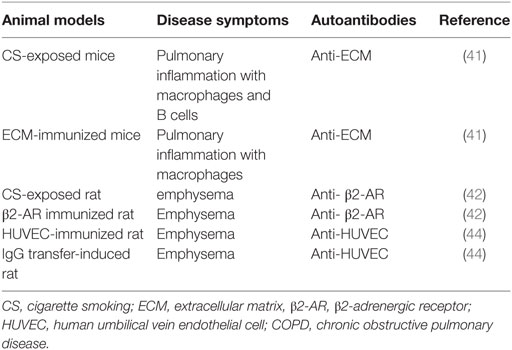
Table 2. Autoantibodies in animal models of COPD.
In 2010, Brandsma and colleagues reported that chronic CS-exposure leads to the pulmonary inflammation and production of autoantibodies against multiple ECM components in mice (41). To further explore the role of autoantibodies against ECM in this mouse model, the authors immunized mice with a mixture of lung ECM. As expected, mice immunized with ECM produced high levels of autoantibodies against different ECM components. In addition, the immunization alone increased the number of macrophage in the lung tissue suggesting a proinflammatory role of autoimmunity against ECM (41). Unfortunately, emphysema, which is associated with autoantibodies in human COPD, was not observed in their model disabling the evaluation of a potential association between autoimmunity against ECM and emphysema development (41). Very recently, a study investigating CS-induced rat model of COPD shed some new light on this field (42). In this study, Hu et al. reported that CS-exposed rats produce higher levels of autoantibodies against β2-adrenergic receptors (β2-ARs) than control rats (42). Moreover, autoantibodies against β2-ARs are associated with severity of CS-induced emphysema suggesting that the autoimmunity might be involved in the formation of emphysema. To confirm this notion, the authors immunized rats with the peptide of the second extracellular loop of β2-ARs which contains an epitope recognized by agnostic autoantibodies against β2-ARs (42, 43). Rat immunized with the β2-ARs peptide produces autoantibodies against β2-ARs and development of emphysema, confirming the role of autoimmunity against β2-ARs in pathogenesis of COPD-like disease (42). Therefore, evidence from CS-induced animal models demonstrates that CS-exposure triggers autoimmunity against multiple autoantigens in the lung and such autoimmunity contribute to COPD-like symptoms.
Beside CS-expose induced approaches, models induced by active immunization also provide evidence for a role of autoimmunity in the pathogenesis of COPD. In 2005, Taraseviciene-Stewart and colleagues reported a new animal model for COPD in rats (44). Rats immunized with HUVECs raised antibodies against HUVECs and developed emphysema. Interestingly, adoptive transfer of either serum or CD4+ T cells from the HUVECs-immunized rat into naive immunocompetent rats induced subsequent emphysema (44). These results suggest an autoimmune-driven mechanism beneath the disease manifestation in experimental COPD which involves both autoreactive T cells and autoantibodies.
In summary, the abovementioned clinical and experimental studies provide some evidence for the role of autoantibodies in COPD. First, autoantibodies are present in both COPD patients and in corresponding animal models, particularly those involving emphysema. This notion is supported by the finding that severe COPD with emphysema is associated with HLA II alleles which is associated with most autoimmune diseases (45). Second, correlation between autoantibodies and disease severity has been described but appears not to be consistent among different studies. Third, autoantibodies in animal models of COPD are capable of inducing a COPD-like disease phenotype. Those evidence, alone with the fact that COPD patients are characterized by increased numbers of B cells, plasma cells, and B cell-rich lymphoid follicles that correlate directly with disease severity (11, 46), support a role of autoantibodies in the development of COPD. Besides humoral autoimmunity, it is important to mention that cellular autoimmunity might also contribute to COPD pathogenesis. As aforementioned, human autoreactive CD8+ and CD4+ T cells have been suggested to contribute to COPD (14–16). In addition, transfer of CD4+ T cells from the HUVECs-immunized rat is able to induce emphysema, supporting a role of autoreactive CD4+ T cells in experimental COPD (44).
With immunodeficient mice which lack both T- and B-cells, the role of adaptive immunity in experimental COPD can be explored. In 2010, Motz et al. reported that transfer of T cells from CS-exposed mice, but not T cells from fresh air-exposed mice, into Rag2−/− mice led to the development of pulmonary inflammation and emphysema in the recipient mice (47), suggesting that adaptive immune responses are capable to mediate COPD-like symptoms. However, by directly exposing immunodeficient mice to CS, two research groups have demonstrated that immunodeficient mice develop comparable COPD-like disease as wild-type controls mice (48, 49), indicating that adaptive immune responses are not required for CS-induced COPD in mice. Since autoimmunity is a part of adaptive immune responses, the abovementioned experimental evidence suggests that autoimmunity is potentially pathogenic but dispensable for CS-induced COPD in animals. However, since human differ from animals in many aspects, findings from animal models might not sufficiently reflect human diseases. Therefore, whether autoimmunity is a pathogenic or an indispensable event in the development of COPD remains elucidative.
In conclusion, previous studies have suggested a potential role of autoimmunity in COPD and its animal models, opening a new field for exploring the pathogenesis of the diseases. Further investigations in this field will not only help for understanding the pathogenesis of COPD but also help for both diagnostic and treatment of the disease.
LW was involved in search and identification of relevant literatures. XY and LW were involved in drafting the manuscript. SK-E and FP critically read the manuscript and contributed with significant revision.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This work was supported by the Deutsche Forschungsgemeinschaft, German Center for Lung Research (DZL) and Research Training Group GRK1727 Modulation of Autoimmunity, as well as by the National Natural Science Foundation of China (No.81371325).
1. Mannino DM. COPD: epidemiology, prevalence, morbidity and mortality, and disease heterogeneity. Chest (2002) 121(5 Suppl):121S–6S. doi:10.1378/chest.121.5_suppl.121S
2. Hogg JC, Timens W. The pathology of chronic obstructive pulmonary disease. Annu Rev Pathol (2009) 4:435–59. doi:10.1146/annurev.pathol.4.110807.092145
3. Tuder RM, Petrache I. Pathogenesis of chronic obstructive pulmonary disease. J Clin Invest (2012) 122(8):2749–55. doi:10.1172/JCI60324
4. Brusselle GG, Joos GF, Bracke KR. New insights into the immunology of chronic obstructive pulmonary disease. Lancet (2011) 378(9795):1015–26. doi:10.1016/S0140-6736(11)60988-4
5. Caramori G, Casolari P, Barczyk A, Durham AL, Di SA, Adcock I. COPD immunopathology. Semin Immunopathol (2016) 38(4):497–515. doi:10.1007/s00281-016-0561-5
6. Kohansal R, Martinez-Camblor P, Agusti A, Buist AS, Mannino DM, Soriano JB. The natural history of chronic airflow obstruction revisited: an analysis of the Framingham offspring cohort. Am J Respir Crit Care Med (2009) 180(1):3–10. doi:10.1164/rccm.200901-0047OC
7. Gamble E, Grootendorst DC, Hattotuwa K, O’Shaughnessy T, Ram FS, Qiu Y, et al. Airway mucosal inflammation in COPD is similar in smokers and ex-smokers: a pooled analysis. Eur Respir J (2007) 30(3):467–71. doi:10.1183/09031936.00013006
8. Rutgers SR, Postma DS, ten Hacken NH, Kauffman HF, van Der Mark TW, Koeter GH, et al. Ongoing airway inflammation in patients with COPD who do not currently smoke. Thorax (2000) 55(1):12–8. doi:10.1136/thorax.55.1.12
9. Brusselle GG, Demoor T, Bracke KR, Brandsma CA, Timens W. Lymphoid follicles in (very) severe COPD: beneficial or harmful? Eur Respir J (2009) 34(1):219–30. doi:10.1183/09031936.00150208
10. Hogg JC, Chu F, Utokaparch S, Woods R, Elliott WM, Buzatu L, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med (2004) 350(26):2645–53. doi:10.1056/NEJMoa032158
11. Seys LJ, Verhamme FM, Schinwald A, Hammad H, Cunoosamy DM, Bantsimba-Malanda C, et al. Role of B cell-activating factor in chronic obstructive pulmonary disease. Am J Respir Crit Care Med (2015) 192(6):706–18. doi:10.1164/rccm.201501-0103OC
12. Lee SH, Goswami S, Grudo A, Song LZ, Bandi V, Goodnight-White S, et al. Antielastin autoimmunity in tobacco smoking-induced emphysema. Nat Med (2007) 13(5):567–9. doi:10.1038/nm1583
13. Sze MA, Dimitriu PA, Suzuki M, McDonough JE, Campbell JD, Brothers JF, et al. Host response to the lung microbiome in chronic obstructive pulmonary disease. Am J Respir Crit Care Med (2015) 192(4):438–45. doi:10.1164/rccm.201502-0223OC
14. Cosio MG, Majo J, Cosio MG. Inflammation of the airways and lung parenchyma in COPD: role of T cells. Chest (2002) 121(5 Suppl):160S–5S. doi:10.1378/chest.121.5_suppl.160S
15. Cosio MG, Saetta M, Agusti A. Immunologic aspects of chronic obstructive pulmonary disease. N Engl J Med (2009) 360(23):2445–54. doi:10.1056/NEJMra0804752
16. Kheradmand F, Shan M, Xu C, Corry DB. Autoimmunity in chronic obstructive pulmonary disease: clinical and experimental evidence. Expert Rev Clin Immunol (2012) 8(3):285–92. doi:10.1586/eci.12.7
17. Feghali-Bostwick CA, Gadgil AS, Otterbein LE, Pilewski JM, Stoner MW, Csizmadia E, et al. Autoantibodies in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med (2008) 177(2):156–63. doi:10.1164/rccm.200701-014OC
18. Packard TA, Li QZ, Cosgrove GP, Bowler RP, Cambier JC. COPD is associated with production of autoantibodies to a broad spectrum of self-antigens, correlative with disease phenotype. Immunol Res (2013) 55(1–3):48–57. doi:10.1007/s12026-012-8347-x
19. Nunez B, Sauleda J, Anto JM, Julia MR, Orozco M, Monso E, et al. Anti-tissue antibodies are related to lung function in chronic obstructive pulmonary disease. Am J Respir Crit Care Med (2011) 183(8):1025–31. doi:10.1164/rccm.201001-0029OC
20. Karayama M, Inui N, Suda T, Nakamura Y, Nakamura H, Chida K. Antiendothelial cell antibodies in patients with COPD. Chest (2010) 138(6):1303–8. doi:10.1378/chest.10-0863
21. Kirkham PA, Caramori G, Casolari P, Papi AA, Edwards M, Shamji B, et al. Oxidative stress-induced antibodies to carbonyl-modified protein correlate with severity of chronic obstructive pulmonary disease. Am J Respir Crit Care Med (2011) 184(7):796–802. doi:10.1164/rccm.201010-1605OC
22. Cheng G, Zhang N, Wang Y, Rui J, Yin X, Cui T. Antibodies of IgG, IgA and IgM against human bronchial epithelial cell in patients with chronic obstructive pulmonary disease. Clin Lab (2016) 62(6):1101–8. doi:10.7754/Clin.Lab.2015.151020
23. Brandsma CA, Kerstjens HA, Geerlings M, Kerkhof M, Hylkema MN, Postma DS, et al. The search for autoantibodies against elastin, collagen and decorin in COPD. Eur Respir J (2011) 37(5):1289–92. doi:10.1183/09031936.00116710
24. Cottin V, Fabien N, Khouatra C, Moreira A, Cordier JF. Anti-elastin autoantibodies are not present in combined pulmonary fibrosis and emphysema. Eur Respir J (2009) 33(1):219–21. doi:10.1183/09031936.00140208
25. Daffa NI, Tighe PJ, Corne JM, Fairclough LC, Todd I. Natural and disease-specific autoantibodies in chronic obstructive pulmonary disease. Clin Exp Immunol (2015) 180(1):155–63. doi:10.1111/cei.12565
26. Greene CM, Low TB, O’Neill SJ, McElvaney NG. Anti-proline-glycine-proline or antielastin autoantibodies are not evident in chronic inflammatory lung disease. Am J Respir Crit Care Med (2010) 181(1):31–5. doi:10.1164/rccm.200904-0545OC
27. Rinaldi M, Lehouck A, Heulens N, Lavend’homme R, Carlier V, Saint-Remy JM, et al. Antielastin B-cell and T-cell immunity in patients with chronic obstructive pulmonary disease. Thorax (2012) 67(8):694–700. doi:10.1136/thoraxjnl-2011-200690
28. Wood AM, de PP, Buckley CD, Ahmad A, Stockley RA. Smoke exposure as a determinant of autoantibody titre in alpha(1)-antitrypsin deficiency and COPD. Eur Respir J (2011) 37(1):32–8. doi:10.1183/09031936.00033710
29. Kuo YB, Chang CA, Wu YK, Hsieh MJ, Tsai CH, Chen KT, et al. Identification and clinical association of anti-cytokeratin 18 autoantibody in COPD. Immunol Lett (2010) 128(2):131–6. doi:10.1016/j.imlet.2009.12.017
30. Xiong Y, Gao S, Luo G, Cheng G, Huang W, Jiang R, et al. Increased circulating autoantibodies levels of IgG, IgA, IgM against cytokeratin 18 and cytokeratin 19 in chronic obstructive pulmonary disease. Arch Med Res (2017) 48(1):79–87. doi:10.1016/j.arcmed.2017.01.007
31. Rosen A, Casciola-Rosen L. Autoantigens in systemic autoimmunity: critical partner in pathogenesis. J Intern Med (2009) 265(6):625–31. doi:10.1111/j.1365-2796.2009.02102.x
32. Darrah E, Andrade F. Rheumatoid arthritis and citrullination. Curr Opin Rheumatol (2018) 30(1):72–8. doi:10.1097/BOR.0000000000000452
33. Newkirk MM, Mitchell S, Procino M, Li Z, Cosio M, Mazur W, et al. Chronic smoke exposure induces rheumatoid factor and anti-heat shock protein 70 autoantibodies in susceptible mice and humans with lung disease. Eur J Immunol (2012) 42(4):1051–61. doi:10.1002/eji.201141856
34. Ruiz-Esquide V, Gomara MJ, Peinado VI, Gomez Puerta JA, Barbera JA, Canete JD, et al. Anti-citrullinated peptide antibodies in the serum of heavy smokers without rheumatoid arthritis. A differential effect of chronic obstructive pulmonary disease? Clin Rheumatol (2012) 31(7):1047–50. doi:10.1007/s10067-012-1971-y
35. Sigari N, Moghimi N, Shahraki FS, Mohammadi S, Roshani D. Anti-cyclic citrullinated peptide (CCP) antibody in patients with wood-smoke-induced chronic obstructive pulmonary disease (COPD) without rheumatoid arthritis. Rheumatol Int (2015) 35(1):85–91. doi:10.1007/s00296-014-3083-2
36. le-Donne I, Aldini G, Carini M, Colombo R, Rossi R, Milzani A. Protein carbonylation, cellular dysfunction, and disease progression. J Cell Mol Med (2006) 10(2):389–406. doi:10.1111/j.1582-4934.2006.tb00407.x
37. Cherneva RV, Georgiev OB, Petrova DS, Trifonova NL, Stamenova M, Ivanova V, et al. The role of small heat-shock protein alphaB-crystalline (HspB5) in COPD pathogenesis. Int J Chron Obstruct Pulmon Dis (2012) 7:633–40. doi:10.2147/COPD.S34929
38. Luo XM, Liu XY, Tang JH, Yang W, Ni ZH, Chen QG, et al. Autoantibodies against CD80 in patients with COPD. Clin Transl Immunology (2016) 5(10):e103. doi:10.1038/cti.2016.57
39. Bonarius HP, Brandsma CA, Kerstjens HA, Koerts JA, Kerkhof M, Nizankowska-Mogilnicka E, et al. Antinuclear autoantibodies are more prevalent in COPD in association with low body mass index but not with smoking history. Thorax (2011) 66(2):101–7. doi:10.1136/thx.2009.134171
40. Ghorani V, Boskabady MH, Khazdair MR, Kianmeher M. Experimental animal models for COPD: a methodological review. Tob Induc Dis (2017) 15:25. doi:10.1186/s12971-017-0130-2
41. Brandsma CA, Timens W, Geerlings M, Jekel H, Postma DS, Hylkema MN, et al. Induction of autoantibodies against lung matrix proteins and smoke-induced inflammation in mice. BMC Pulm Med (2010) 10:64. doi:10.1186/1471-2466-10-64
42. Hu JY, Liu BB, Du YP, Zhang Y, Zhang YW, Zhang YY, et al. Increased circulating beta2-adrenergic receptor autoantibodies are associated with smoking-related emphysema. Sci Rep (2017) 7:43962. doi:10.1038/srep43962
43. Kohr D, Singh P, Tschernatsch M, Kaps M, Pouokam E, Diener M, et al. Autoimmunity against the beta2 adrenergic receptor and muscarinic-2 receptor in complex regional pain syndrome. Pain (2011) 152(12):2690–700. doi:10.1016/j.pain.2011.06.012
44. Taraseviciene-Stewart L, Scerbavicius R, Choe KH, Moore M, Sullivan A, Nicolls MR, et al. An animal model of autoimmune emphysema. Am J Respir Crit Care Med (2005) 171(7):734–42. doi:10.1164/rccm.200409-1275OC
45. Faner R, Nunez B, Sauleda J, Garcia-Aymerich J, Pons J, Crespi C, et al. HLA distribution in COPD patients. COPD (2013) 10(2):138–46. doi:10.3109/15412555.2012.729621
46. Polverino F, Seys LJ, Bracke KR, Owen CA. B cells in chronic obstructive pulmonary disease: moving to center stage. Am J Physiol Lung Cell Mol Physiol (2016) 311(4):L687–95. doi:10.1152/ajplung.00304.2016
47. Motz GT, Eppert BL, Wesselkamper SC, Flury JL, Borchers MT. Chronic cigarette smoke exposure generates pathogenic T cells capable of driving COPD-like disease in Rag2-/- mice. Am J Respir Crit Care Med (2010) 181(11):1223–33. doi:10.1164/rccm.200910-1485OC
48. Botelho FM, Gaschler GJ, Kianpour S, Zavitz CC, Trimble NJ, Nikota JK, et al. Innate immune processes are sufficient for driving cigarette smoke-induced inflammation in mice. Am J Respir Cell Mol Biol (2010) 42(4):394–403. doi:10.1165/rcmb.2008-0301OC
Keywords: autoimmunity, autoantibodies, chronic obstructive pulmonary disease, biomarkers, emphysema, experimental models, pathogenesis
Citation: Wen L, Krauss-Etschmann S, Petersen F and Yu X (2018) Autoantibodies in Chronic Obstructive Pulmonary Disease. Front. Immunol. 9:66. doi: 10.3389/fimmu.2018.00066
Received: 23 October 2017; Accepted: 10 January 2018;
Published: 25 January 2018
Edited by:
Falk Nimmerjahn, University of Erlangen-Nuremberg, GermanyReviewed by:
Simon Fillatreau, Deutsches Rheuma-Forschungszentrum (DRFZ), GermanyCopyright: © 2018 Wen, Krauss-Etschmann, Petersen and Yu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xinhua Yu, eGluaHVheXVAZnotYm9yc3RlbC5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.