 Laura Lambert
Laura Lambert Fiona J. Culley
Fiona J. Culley- Faculty of Medicine, Respiratory Infections Section, National Heart and Lung Institute, Imperial College London, London, United Kingdom
Early life is a period of particular susceptibility to respiratory infections and symptoms are frequently more severe in infants than in adults. The neonatal immune system is generally held to be deficient in most compartments; responses to innate stimuli are weak, antigen-presenting cells have poor immunostimulatory activity and adaptive lymphocyte responses are limited, leading to poor immune memory and ineffective vaccine responses. For mucosal surfaces such as the lung, which is continuously exposed to airborne antigen and to potential pathogenic invasion, the ability to discriminate between harmless and potentially dangerous antigens is essential, to prevent inflammation that could lead to loss of gaseous exchange and damage to the developing lung tissue. We have only recently begun to define the differences in respiratory immunity in early life and its environmental and developmental influences. The innate immune system may be of relatively greater importance than the adaptive immune system in the neonatal and infant period than later in life, as it does not require specific antigenic experience. A better understanding of what constitutes protective innate immunity in the respiratory tract in this age group and the factors that influence its development should allow us to predict why certain infants are vulnerable to severe respiratory infections, design treatments to accelerate the development of protective immunity, and design age specific adjuvants to better boost immunity to infection in the lung.
Introduction
Respiratory infection is one of the leading causes of mortality in children under 5 years of age (1, 2). Early life respiratory viral infections are most commonly caused by rhinovirus, respiratory syncytial virus (RSV), influenza, parainfluenza virus, and coronavirus (3). Infection is frequently restricted to the upper respiratory tract but may develop into severe lower respiratory tract infection, such as RSV bronchiolitis, the leading cause of hospitalization of infants worldwide (4–7). Bacterial pneumonia in infants, caused by agents such as Haemophilus influenzae and Streptococcus pneumoniae, is estimated to cause a million deaths in infants under 5 years of age annually (8, 9). Maternal antibodies afford some protection against infection but wane over the first months of life, and neonates and infants respond poorly to vaccination, leaving early life as a window of particular vulnerability to respiratory infection (10, 11). Experiences during the crucial neonatal and infant window may shape respiratory health in the long term (12–14). Severe RSV infection in infants is associated with the development of wheeze and asthma in childhood (15–19) and even respiratory disease that occur late in life, such as chronic obstructive pulmonary disease, are associated with early life events (20–24).
At birth, the neonate emerges from the sheltered intrauterine environment into a plethora of antigenic challenges from pathogens, commensals, and harmless environmental antigens. Neonatal immunity is, in general, attenuated compared to that of adults (4, 25–29). Differences in immunity in early life are due to tissue leukopenia, cell intrinsic hyporesponsiveness, and inhibitory mechanisms, such as CD71+ immunosuppressive erythroid cells and high levels of adenosine in extracellular fluids (26, 28–31). Protective Th1 polarized responses and antibodies are produced less well in early life than in adults, along with a propensity to develop unwanted, Th2 or Th17 biased, or dysregulated inflammation (28, 31–33), for example, following vaccination or allergen exposure (34, 35). TLR stimulation of cord blood leukocytes results in a lower production of proinflammatory, Th1-associated cytokines (IL-12p70, TNF-α, IFN-α), and greater production of IL-10 and the Th17-promoting IL-6 and IL-23 when compared to stimulation of adult blood cells, although equivalent responses to TLR 7/8 ligand R848 occur (29, 36, 37). Over the first few years of life, antiviral and Th1-biasing cytokine production increases (38, 39).
In the face of an inexperienced adaptive response, innate immunity is likely to play a more dominant role in protection against infection in early life than in adulthood. This is supported by the findings that many gene polymorphisms associated with severe RSV infection in infants encode components of the innate immune response (4, 40–43). The importance of TLR signaling in early life is illustrated by individuals with genetic deficiencies in components of the TLR signaling pathway such as MyD88 or IRAK-4. These patients are at high risk of bacterial infection in childhood, including in the respiratory tract; however, their condition improves dramatically with age (44). This review will focus on describing our current knowledge of innate immunity in the neonatal lung as a first line of defense against infection. Some potentially important mechanisms underlying susceptibility to lung infection in infants are summarized in Figure 1.
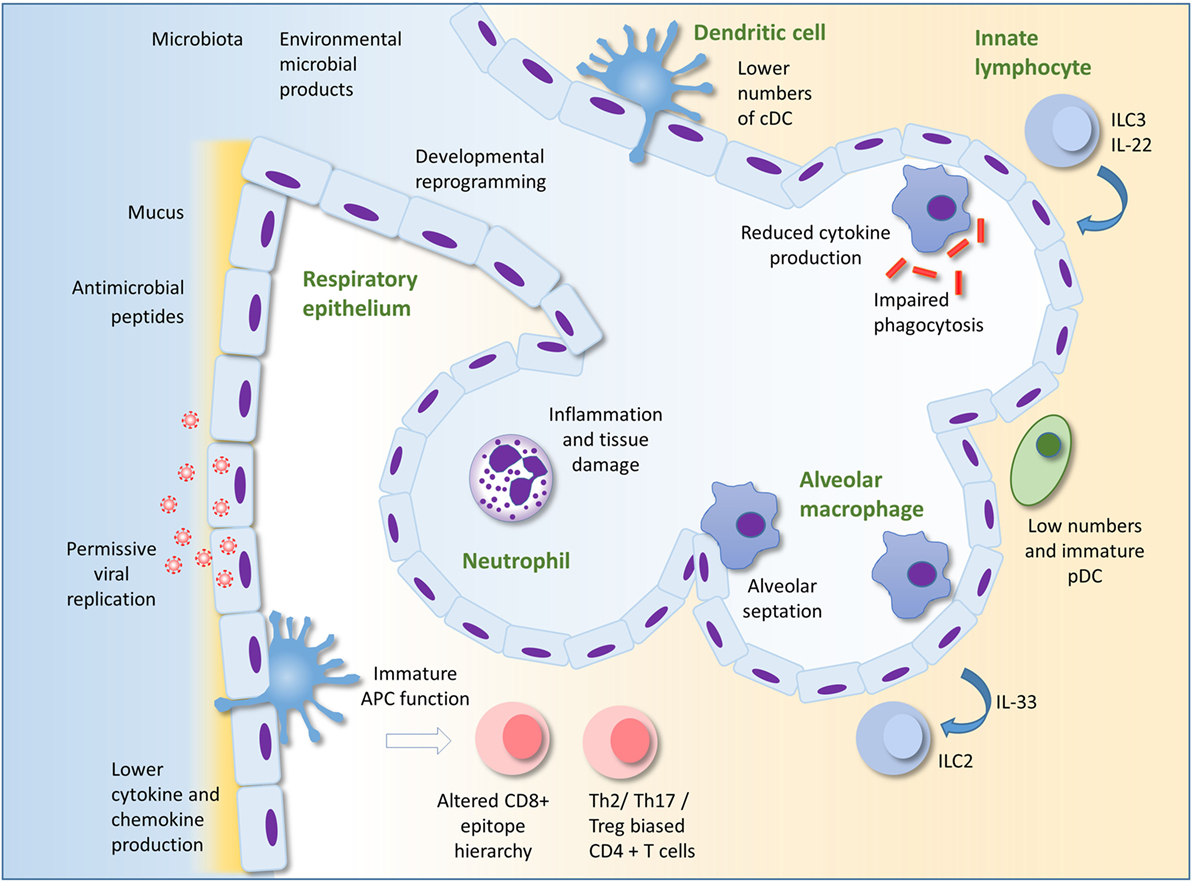
Figure 1. Innate immunity to infection in the lung in early life. Alveolar macrophages (AM) are the most numerous leukocyte in the lungs in early life. Reduced cytokine production and phagocytic ability in AM in early life compared to those of adults could underlie susceptibility to infection. AM also promote pre- and post-natal lung development and remodeling. The respiratory epithelium protects against infection through the production of mucus and antimicrobial peptides. Production of type I IFNs may be lower in infant than adult epithelial cells, perhaps permitting greater viral replication. Epithelial cells may interact with innate lymphocytes to both initiate and regulate inflammation. Developmental reprograming in the epithelium in early life may also alter the nature of the epithelial response to infection. There are low numbers of pDC in the lungs compared to adults. Recruitment of neutrophils to the lung occurs less readily in early life compared to adults in some circumstances, but in other situations, excessive recruitment of inflammatory cells can lead to lung inflammation, tissue damage, and impairment of gaseous exchange. Immaturity and lower numbers of dendritic cells, the environment as well as intrinsic differences in T cells in early life may result in the development of skewed helper T cell responses and an altered epitope hierarchy in CD8+ T cells. Innate immunity in the lung in early life is influenced by acquisition of the microbiota, exposure to microbial products and other environmental factors, as well as the infant genome. Adapted by permission from Macmillan Publishers Ltd: Nature Reviews Immunology (45), copyright 2014.
Respiratory Immunity in Early Life
It is relatively difficult to obtain samples from the lower airways of healthy infant subjects, so many studies have been carried out in murine and other animal models. Information on the cellular composition of the neonatal lung in humans has come from analysis of bronchoalveolar lavage fluid composition (46–49), immunohistochemistry (50), and more recently, extensive phenotypic analysis of leukocyte subsets in pediatric tissues (51–53).
Adaptive Immunity
Fetal airways are essentially devoid of lymphocytes, they are seeded from birth, and lymphocytes increase as a proportion of airway cells over the first few years of life (48, 54). There is a relative paucity in CD4+ cells (46, 50), and memory T cells are less abundant in infant lungs than in adults, though they are more abundant in the lungs than many other tissues (51). Tregs are relatively abundant in pediatric tissues and may have a higher suppressive capacity than those from adults (28, 51) and a transient increase in regulatory T cells, associated with microbial colonization, protects from hyperresponsiveness to allergen (35). A failure of regulation may underlie excessive inflammation in infection, as in RSV bronchiolitis (43), and RSV infection in early life can increase susceptibility to allergic inflammation in the mouse model through an impairment of regulatory T cells (4, 55). CD8+ T cells in the lung correlate with disease severity in infants with respiratory failure due to respiratory viral infection (52) and in neonatal mice infected with RSV, a CD8+ T cell epitope hierarchy emerges, which is distinct to that of adults (56). Distinct phenotypes of adaptive lymphocytes are found in early life. A subset of Th cells in human cord blood produce the neutrophil chemoattractant interleukin-8 upon activation (57) and, during RSV infection, a regulatory phenotype in the neonatal B cell compartment may dampen protective immunity (58).
Lung Dendritic Cells (DCs)
There is some evidence that neonatal T cells have the capacity to mount adult-like protective responses to lung infection. Adoptive transfer of neonatal CD4+ T cells into Pneumocystis carinii-infected adult SCID mice allowed for adult-level pathogen clearance and cytokine production (59, 60), suggesting that the neonatal environment in the lung influences T cell responses. This may be due in part to the function of neonatal antigen-presenting cells. Neonatal mouse lungs contain relatively fewer conventional DCs (cDCs), which are immature and poorly functional (56, 61, 62), although mature functions ex vivo have been reported (63). During neonatal RSV infection, migratory cDCs are dominated by CD103+ DCs, while the CD11b+ contribution increases with age (64). These CD103+ DCs are phenotypically immature and poorly functional (65), and this may influence the magnitude and epitope hierarchy of the CD8+ T cell response (64–66), although these are also influenced by T cell intrinsic differences and regulatory T cells (56, 67). As well as stimulating protective responses, lung DCs in neonates must promote tolerance to harmless environmental antigens. CD11b+ cDCs in the lung induce Th2 responses to allergens, but transiently express high levels of PD-L1, which promotes tolerance, following acquisition of the microbiota (35, 68). In contrast to murine studies, the relative frequency of different DC subsets in the human lung appears to be relatively stable over the life course (53).
In the murine neonatal lung, potent IFN-α-producing pDC cells are scarce (61), and there is limited recruitment of pDCs and IFN-α production following RSV infection (69).
Alveolar Macrophages (AM)
Lung resident macrophages, which include AM and the less well-characterized interstitial macrophages (70–72), are an important component of the first line of defense in the lung. In the steady state, AMs remove debris and maintain a tolerogenic environment; during infection, they secrete proinflammatory cytokines and contribute to pathogen clearance; and after infection, they aid resolution of inflammation (45). AMs are the predominant cell type in the neonatal airway, they appear in the alveolar compartment from just before birth and throughout the first week of life, and are relatively abundant and self-renewing, persisting for at least 11 weeks in mice (47–50, 73, 74).
Stimulation of cultured cells has been used to interrogate the relative antimicrobial functions of neonatal and adult AMs. LPS stimulation of rodent or ovine AMs results in similar or even enhanced upregulation of TNF-α and CXC-chemokines in neonatal compared to adult cells (75–77), though others demonstrated a reduced translocation of NF-κB to the nucleus of AM from neonatal mice (78). Enhanced phagocytosis by neonatal compared to adult rat AM has been observed (75), but others have reported impaired phagocytosis and subsequent killing of yeast particles in neonatal rhesus monkey AMs; and impaired phagocytosis of opsonized red blood cells in neonatal rat AMs in comparison to adults (79, 80). In a murine model of Pneumocystis infection, neonatal AMs were delayed in their expression of activation markers in vivo in comparison to adults (81). Similarly, during murine neonatal RSV infection, there was reduced and delayed AM activation compared to adult infection (82), but intranasal IFN-γ was able to promote AM maturation (82). Little is known about responses in human infant AMs. Cultured cells obtained by bronchoalveolar lavage from infants <2 years of age produce lower IL-1 and TNF-α following LPS stimulation compared with cells from children aged 2–17 (54). The apparent contradictions in the data on AM function in early life may reflect differences in the species, age, experimental conditions, and assays used. Various macrophage functions are likely to mature at different rates. Neonatal and adult AMs are likely to behave differently in their respective lung environments, which is a limitation of these in vitro studies.
Respiratory Epithelial Cells
The respiratory epithelium is the principal site of replication of respiratory viruses. It is in close communication with AM and acts an immune sentinel producing inflammatory mediators, such as type I and III interferons, mucus, and antimicrobial proteins (45, 83). Relatively little is known about the immunological functions of the airway epithelium in early life. In cultured tracheobronchial epithelial cells from Rhesus macaques of different ages (infant, juvenile, and adult), IL-8 production on exposure to LPS positively correlated with age (84). Furthermore, epithelial cells from juveniles housed in filtered air produced higher cytokine responses than those in conventional housing suggesting the microbial richness of the environment may influence epithelial responsiveness. The same group demonstrated that infant Rhesus monkey primary epithelial cell cultures are more permissive for the H1N1 influenza virus than those from adult airways, while producing less IL-1α (85).
In humans, type I IFNs are detected at only low levels in the airways of RSV-bronchiolitic infants. This may be due to inhibition of the host anti-viral response by the viral non-structural proteins but alternatively may reflect the timing of sampling, and an IFN-induced gene signature is detectable in blood (86–88). Pediatric nasal and airway epithelial cells cultured from bronchial brushings are readily infected with RSV (89–91) and poor induction of type I IFNs by RSV is reflected in these cultures (92, 93). Instead, the type III interferon IL-29 (IFN-λ) is detected both in the airways of bronchiolitic infants and in cultures of RSV infected airway epithelial cells, and IL-29 pretreatment of cultured epithelial cells attenuates RSV growth (92, 93). Epithelial cells are probably a key source of inflammatory cytokines in respiratory tract secretions of infants with acute RSV (92, 94, 95), including the type-2 immunity promoting cytokine IL-33 (96). The cells used in many in vitro experiments on pediatric respiratory epithelial cells were originally taken from the conducting airway and data surrounding lower airway and ATII cells in early life is even sparser.
Antimicrobial proteins are a first line of defense at barrier sites and are produced primarily by epithelial cells and innate leukocytes, particularly neutrophils (97, 98). In the lung, they include surfactants as well as S100s, β-defensins, and cathelicidin and they may provide protection against important infant respiratory infections, including RSV (99–102). Cathelicidin has direct antiviral activity against RSV, can prevent infection in vitro and in vivo and in children hospitalized with bronchiolitis, those with low serum cathelicidin were significantly more likely to have RSV infection and a longer hospital stay (97, 103–107).
Innate Lymphocytes
Neonatal murine lungs show no quantitative deficiency in γδ T cells as a proportion of CD3+ T cells (61, 108). Exposure to allergen in neonatal mice can stimulate innate ILC2 lymphocytes, a major source of type 2 cytokines (109). Colonization by the microbiota in neonates protects against the accumulation of potentially pro-inflammatory mucosal iNKT cells in the lung and gut (110). Colonization of the gut of neonatal mice can also lead to intestinal DC mediated upregulation of CCR4 on IL-22 producing ILC3, which allows their migration into the lungs of neonatal mice, and promotes protection against bacterial pneumonia (111).
Neutrophils
Recruitment of innate leukocytes and, in particular, neutrophils, is likely to play an important role in the innate response to infection in the neonatal lung following microbial recognition. Both TLR4 gene and protein expression are present in the murine lung in the fetus and increase with age through to adulthood (112, 113). TLR2 expression is also present in the human fetal lung and increases with gestational age (114). It appears that there is an immaturity of chemokine production at baseline in the respiratory mucosa. Expression of CXCL2 is low in neonatal mice compared with adults (115) and in uninfected infants (newborn to 18 months), the concentration of IL-8 in nasal washes positively correlates with age (116). There is a dramatically reduced and delayed neutrophil influx in neonatal lung in response to administration of LPS or bacteria in comparison to adult animals (75, 117–119). In the neonatal murine lung, infection with the paramyxovirus Sendai virus results in a minimal early influx of neutrophils and low production of pro-inflammatory cytokines compared with the adult lung; similarly in murine RSV infection, early pro-inflammatory cytokine production is impaired (108, 115). Diminished recruitment of neutrophils may also be due to an impaired chemotaxic ability of infant neutrophils (25, 120, 121).
In severe RSV bronchiolitis in infants, neutrophils can account for the majority of cells recovered from the airways, associated with increased neutrophil elastase (122–125) and IL-8 (94, 126), although others have reported a lower inflammatory cytokine response in infants with severe vs mild RSV bronchiolitis (127). There is a considerable influx of neutrophils into S. pneumoniae-infected lungs of neonatal and adult mice, with the neonatal influx even occurring at a lower bacterial dose (128). It is unclear under what circumstances the neonatal lung will produce an equivalent or exacerbated inflammatory response compared to that of adults, whether this simply requires a high level of stimulation or whether additional factors are involved.
Factors Influencing the Development and Maturation of Lung Immunity
Despite the apparent absence of a mature adult-like immune system, neonates are able to produce effective immune responses that defend against infection and indeed excessive inflammation can occur. The neonate must strike a balance between protection against infection and potential damage to the developing lung and may use alternative mechanisms of protection against infection to those that predominate in adults.
Exposure to microbial products from the environment, the microbiota, or infection may be beneficial in terms of their ability to promote immune maturation and more adult like innate and adaptive immunity (28, 30). Treatment with TLR agonists CpG or LPS during RSV infection alters the CD8+ T cell response toward a more adult-like immunodominance (66) and treatment of neonatal mice with CpG prior to RSV infection shifts the secondary response to re-infection away from a type 2 response (129). Furthermore, administration of BCG shifts lung CD4+ responses away from a Th2 bias and cDC from BCG treated lungs promote Th1 responses (61).
The microbiota is acquired from the mother at birth and in early life and an adult-like microbiome is established by around 3 years of age (130). The composition of the microbiota and microbial richness of the environment in which children develop have been linked to susceptibility to severe respiratory infections and the development of wheeze and asthma (131–133). Environmental microbial exposure may influence lung health by establishing the set-point of immunological responsiveness of the lung, as seen by the attenuation of allergic lung inflammation by airway exposure to LPS or endotoxin rich dust samples (133, 134). Additionally, commensal bacteria may influence neonatal respiratory immunity indirectly. For example, sensing of commensal bacteria by gut DCs promotes resistance to bacterial pneumonia in neonatal mice (111). Factors that shape the microbiota, such as delivery by cesarean section and antibiotic use in early life and pregnancy, are likely to profoundly influence the developing immune system (14, 135). Other environmental factors that regulate the balance of immunity in the infant respiratory tract may include diet, vitamin D status, breast feeding, maternal immunity, and exposure to environmental pollutants.
Significant stages of lung development occur both before and after birth and hyporesponsiveness to immune stimuli may have evolved to protect the developing lung from the disruptive and damaging effects of inflammation (136, 137). This is evidenced in mouse models of chorioamnionitis, where exposure of the fetal lung to LPS results in abnormal development of the distal airways (138, 139). In addition, IL-1β expression in the fetal or newborn lung impairs normal postnatal development (140). Reciprocally, the developmental programmes active in resident lung cells, which drive cell growth and differentiation may also influence immune responses (141, 142). Macrophages take on important roles in lung development and remodeling including septation and vascularization of the alveoli after birth (137, 143). Macrophages associate with sites of branching morphogenesis where they assume a tissue remodeling phenotype and promote development through production of growth factors and matrix metalloproteases (143). Polarization of macrophages away from this phenotype might, therefore, be a mechanism by which pro-inflammatory signals disrupt lung development (138, 140). As with lung macrophages, the respiratory epithelium will be subject to lung developmental programmes extending into the postnatal period, which regulate epithelial cell proliferation and differentiation, and these may potentially also alter epithelial immunological function. Foxa2 is an epithelially expressed member of the forkhead family of transcription factors. In the developing lung, it regulates epithelial differentiation and controls goblet cell hyperplasia. It also has immunoregulatory functions and limits type-2 immunity through inhibition of the cysteinyl LT signaling pathway (83, 141, 144).
Conclusion
The mechanisms that regulate inflammatory responses to microbial stimulation in the lung need to be more fully elucidated. Increasing our knowledge of how the developing immune system responds to infectious challenge is of importance for development of neonatal vaccines and treatments for exaggerated respiratory inflammation during infection. In certain circumstances, the immune system in early life is capable of adult-level responses, and perhaps boosting responses in at-risk infants—in treatment for acute infectious disease or as adjuvant for vaccination—would be a beneficial protective strategy. Additionally, selectively harnessing the protective innate mechanisms that are already expressed at adult or greater than adult levels in the neonate could be a safe therapeutic method. Thus, while early life is clearly a period of immunological vulnerability for the developing lung, it is also an opportunity for effective intervention strategies, which could benefit respiratory health not only in infancy, but into adulthood.
Author Contributions
LL researched the literature and wrote the review. FC wrote the review, edited, and updated it.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Some of the content of this manuscript first appeared in Lambert (2015) (145), Immunology of the Neonatal Lung and the Long Term Consequences of Neonatal Respiratory Virus Infection for Pulmonary Innate Immunity. Ph.D. thesis: Imperial College London. We thank Dr. Spiros Makris for critical reading of the manuscript. This work was supported by a Medical Research Council New Investigator Research Grant to FC (G1001763).
References
1. Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, et al. Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet (2015) 385(9966):430–40. doi:10.1016/S0140-6736(14)61698-6
2. Walker CLF, Rudan I, Liu L, Nair H, Theodoratou E, Bhutta ZA, et al. Global burden of childhood pneumonia and diarrhoea. Lancet (2013) 381(9875):1405–16. doi:10.1016/S0140-6736(13)60222-6
3. Tregoning JS, Schwarze J. Respiratory viral infections in infants: causes, clinical symptoms, virology, and immunology. Clin Microbiol Rev (2010) 23(1):74–98. doi:10.1128/CMR.00032-09
4. Lambert L, Sagfors AM, Openshaw PJM, Culley FJ. Immunity to RSV in early-life. Front Immunol (2014) 5:466. doi:10.3389/fimmu.2014.00466
5. Nair H, Nokes DJ, Gessner BD, Dherani M, Madhi SA, Singleton RJ, et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: a systematic review and meta-analysis. Lancet (2010) 375(9725):1545–55. doi:10.1016/S0140-6736(10)60206-1
6. Hall CB, Weinberg GA, Iwane MK, Blumkin AK, Edwards KM, Staat MA, et al. The burden of respiratory syncytial virus infection in young children. N Engl J Med (2009) 360(6):588–98. doi:10.1056/NEJMoa0804877
7. Meissner HC. Viral bronchiolitis in children. N Engl J Med (2016) 374(1):62–72. doi:10.1056/NEJMra1413456
8. O’Brien KL, Wolfson LJ, Watt JP, Henkle E, Deloria-Knoll M, McCall N, et al. Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: global estimates. Lancet (2009) 374(9693):893–902. doi:10.1016/S0140-6736(09)61204-6
9. Watt JP, Wolfson LJ, O’Brien KL, Henkle E, Deloria-Knoll M, McCall N, et al. Burden of disease caused by Haemophilus influenzae type b in children younger than 5 years: global estimates. Lancet (2009) 374(9693):903–11. doi:10.1016/S0140-6736(09)61203-4
10. Mohr E, Siegrist C-A. Vaccination in early life: standing up to the challenges. Curr Opin Immunol (2016) 41:1–8. doi:10.1016/j.coi.2016.04.004
11. Heath PT, Culley FJ, Jones CE, Kampmann B, Le Doare K, Nunes MC, et al. Group B streptococcus and respiratory syncytial virus immunisation during pregnancy: a landscape analysis. Lancet Infect Dis (2017) 17(7):e223–34. doi:10.1016/S1473-3099(17)30232-3
12. Renz H, Brandtzaeg P, Hornef M. The impact of perinatal immune development on mucosal homeostasis and chronic inflammation. Nat Rev Immunol (2011) 12(1):9–23. doi:10.1038/nri3112
13. Lloyd CM, Marsland BJ. Lung homeostasis: influence of age, microbes, and the immune system. Immunity (2017) 46(4):549–61. doi:10.1016/j.immuni.2017.04.005
14. Man WH, de Steenhuijsen Piters WAA, Bogaert D. The microbiota of the respiratory tract: gatekeeper to respiratory health. Nat Rev Microbiol (2017) 15(5):259–70. doi:10.1038/nrmicro.2017.14
15. Biesbroek G, Tsivtsivadze E, Sanders EAM, Montijn R, Veenhoven RH, Keijser BJF, et al. Early respiratory microbiota composition determines bacterial succession patterns and respiratory health in children. Am J Respir Crit Care Med (2014) 190(11):1283–92. doi:10.1164/rccm.201407-1240OC
16. De Steenhuijsen Piters WAA, Heinonen S, Hasrat R, Bunsow E, Smith B, Suarez-Arrabal M-C, et al. Nasopharyngeal microbiota, host transcriptome, and disease severity in children with respiratory syncytial virus infection. Am J Respir Crit Care Med (2016) 194(9):1104–15. doi:10.1164/rccm.201602-0220OC
17. Sigurs N, Gustafsson PM, Bjarnason R, Lundberg F, Schmidt S, Sigurbergsson F, et al. Severe respiratory syncytial virus bronchiolitis in infancy and asthma and allergy at age 13. Am J Respir Crit Care Med (2005) 171(2):137–41. doi:10.1164/rccm.200406-730OC
18. Sigurs N, Aljassim F, Kjellman B, Robinson PD, Sigurbergsson F, Bjarnason R, et al. Asthma and allergy patterns over 18 years after severe RSV bronchiolitis in the first year of life. Thorax (2010) 65(12):1045–52. doi:10.1136/thx.2009.121582
19. Caballero MT, Serra ME, Acosta PL, Marzec J, Gibbons L, Salim M, et al. TLR4 genotype and environmental LPS mediate RSV bronchiolitis through Th2 polarization. J Clin Invest (2015) 125(2):571–82. doi:10.1172/JCI75183
20. Svanes C, Sunyer J, Plana E, Dharmage S, Heinrich J, Jarvis D, et al. Early life origins of chronic obstructive pulmonary disease. Thorax (2010) 65(1):14–20. doi:10.1136/thx.2008.112136
21. Shaheen SO, Barker DJ, Holgate ST. Do lower respiratory tract infections in early childhood cause chronic obstructive pulmonary disease? Am J Respir Crit Care Med (1995) 151(5):1649–51. doi:10.1164/ajrccm/151.5_Pt_1.1649
22. Narang I, Bush A. Early origins of chronic obstructive pulmonary disease. Semin Fetal Neonatal Med (2012) 17(2):112–8. doi:10.1016/j.siny.2012.01.002
23. Bui DS, Burgess JA, Lowe AJ, Perret JL, Lodge CJ, Bui M, et al. Childhood lung function predicts adult chronic obstructive pulmonary disease and asthma-chronic obstructive pulmonary disease overlap syndrome. Am J Respir Crit Care Med (2017) 196(1):39–46. doi:10.1164/rccm.201606-1272OC
24. Martinez FD. The origins of asthma and chronic obstructive pulmonary disease in early life. Proc Am Thorac Soc (2009) 6(3):272–7. doi:10.1513/pats.200808-092RM
25. Levy O. Innate immunity of the newborn: basic mechanisms and clinical correlates. Nat Rev Immunol (2007) 7(5):379–90. doi:10.1038/nri2075
26. Siegrist C-A, Aspinall R. B-cell responses to vaccination at the extremes of age. Nat Rev Immunol (2009) 9(3):185–94. doi:10.1038/nri2508
27. Prendergast AJ, Klenerman P, Goulder PJR. The impact of differential antiviral immunity in children and adults. Nat Rev Immunol (2012) 12(9):636–48. doi:10.1038/nri3277
28. Kollmann TR, Kampmann B, Mazmanian SK, Marchant A, Levy O. Protecting the newborn and young infant from infectious diseases: lessons from immune ontogeny. Immunity (2017) 46(3):350–63. doi:10.1016/j.immuni.2017.03.009
29. Kollmann TR, Levy O, Montgomery RR, Goriely S. Innate immune function by Toll-like receptors: distinct responses in newborns and the elderly. Immunity (2012) 37(5):771–83. doi:10.1016/j.immuni.2012.10.014
30. Torow N, Marsland BJ, Hornef MW, Gollwitzer ES. Neonatal mucosal immunology. Mucosal Immunol (2017) 10(1):5–17. doi:10.1038/mi.2016.81
31. Adkins B, Leclerc C, Marshall-Clarke S. Neonatal adaptive immunity comes of age. Nat Rev Immunol (2004) 4(7):553–64. doi:10.1038/nri1394
32. Zaghouani H, Hoeman CM, Adkins B. Neonatal immunity: faulty T-helpers and the shortcomings of dendritic cells. Trends Immunol (2009) 30(12):585–91. doi:10.1016/j.it.2009.09.002
33. PrabhuDas M, Adkins B, Gans H, King C, Levy O, Ramilo O, et al. Challenges in infant immunity: implications for responses to infection and vaccines. Nat Immunol (2011) 12(3):189–94. doi:10.1038/ni0311-189
34. Saglani S, Mathie SA, Gregory LG, Bell MJ, Bush A, Lloyd CM. Pathophysiological features of asthma develop in parallel in house dust mite-exposed neonatal mice. Am J Respir Cell Mol Biol (2009) 41(3):281–9. doi:10.1165/rcmb.2008-0396OC
35. Gollwitzer ES, Saglani S, Trompette A, Yadava K, Sherburn R, McCoy KD, et al. Lung microbiota promotes tolerance to allergens in neonates via PD-L1. Nat Med (2014) 20(6):642–7. doi:10.1038/nm.3568
36. Levy O, Zarember KA, Roy RM, Cywes C, Godowski PJ, Wessels MR. Selective impairment of TLR-mediated innate immunity in human newborns: neonatal blood plasma reduces monocyte TNF-alpha induction by bacterial lipopeptides, lipopolysaccharide, and imiquimod, but preserves the response to R-848. J Immunol (2004) 173(7):4627–34. doi:10.4049/jimmunol.173.7.4627
37. Kollmann TR, Crabtree J, Rein-Weston A, Blimkie D, Thommai F, Wang XY, et al. Neonatal innate TLR-mediated responses are distinct from those of adults. J Immunol (2009) 183(11):7150–60. doi:10.4049/jimmunol.0901481
38. Corbett NP, Blimkie D, Ho KC, Cai B, Sutherland DP, Kallos A, et al. Ontogeny of Toll-like receptor mediated cytokine responses of human blood mononuclear cells. PLoS One (2010) 5(11):e15041. doi:10.1371/journal.pone.0015041
39. Belderbos ME, van Bleek GM, Levy O, Blanken MO, Houben ML, Schuijff L, et al. Skewed pattern of Toll-like receptor 4-mediated cytokine production in human neonatal blood: low LPS-induced IL-12p70 and high IL-10 persist throughout the first month of life. Clin Immunol (2009) 133(2):228–37. doi:10.1016/j.clim.2009.07.003
40. Faber TE, Schuurhof A, Vonk A, Koppelman GH, Hennus MP, Kimpen JLL, et al. IL1RL1 gene variants and nasopharyngeal IL1RL-a levels are associated with severe RSV bronchiolitis: a multicenter cohort study. PLoS One (2012) 7(5):e34364. doi:10.1371/journal.pone.0034364
41. Janssen R, Bont L, Siezen CLE, Hodemaekers HM, Ermers MJ, Doornbos G, et al. Genetic susceptibility to respiratory syncytial virus bronchiolitis is predominantly associated with innate immune genes. J Infect Dis (2007) 196(6):826–34. doi:10.1086/520886
42. Tulic MK, Hurrelbrink RJ, Prêle CM, Laing IA, Upham JW, Le Souef P, et al. TLR4 polymorphisms mediate impaired responses to respiratory syncytial virus and lipopolysaccharide. J Immunol (2007) 179(1):132–40. doi:10.4049/jimmunol.179.1.132
43. Openshaw PJM, Chiu C, Culley FJ, Johansson C. Protective and harmful immunity to RSV infection. Annu Rev Immunol (2017) 35(1):501–32. doi:10.1146/annurev-immunol-051116-052206
44. Picard C, Casanova J-L, Puel A. Infectious diseases in patients with IRAK-4, MyD88, NEMO, or IκBα deficiency. Clin Microbiol Rev (2011) 24(3):490–7. doi:10.1128/CMR.00001-11
45. Hussell T, Bell TJ. Alveolar macrophages: plasticity in a tissue-specific context. Nat Rev Immunol (2014) 14(2):81–93. doi:10.1038/nri3600
46. Ratjen F, Bredendiek M, Zheng L, Brendel M, Costabel U. Lymphocyte subsets in bronchoalveolar lavage fluid of children without bronchopulmonary disease. Am J Respir Crit Care Med (1995) 152(1):174–8. doi:10.1164/ajrccm.152.1.7599820
47. Riedler J, Grigg J, Robertson CF. Role of bronchoalveolar lavage in children with lung disease. Eur Respir J (1995) 8(10):1725–30. doi:10.1183/09031936.95.08101725
48. Grigg J, Riedler J. Developmental airway cell biology. The “normal” young child. Am J Respir Crit Care Med (2000) 162(2 Pt 2):S52–5. doi:10.1164/ajrccm.162.supplement_1.maic-14
49. Ratjen F, Bredendiek M, Brendel M, Meltzer J, Costabel U. Differential cytology of bronchoalveolar lavage fluid in normal children. Eur Respir J (1994) 7(10):1865–70. doi:10.1183/09031936.94.07101865
50. Dos Santos ABG, Binoki D, Silva LFF, de Araujo BB, Otter ID, Annoni R, et al. Immune cell profile in infants’ lung tissue. Ann Anat (2013) 195(6):596–604. doi:10.1016/j.aanat.2013.05.003
51. Thome JJC, Bickham KL, Ohmura Y, Kubota M, Matsuoka N, Gordon C, et al. Early-life compartmentalization of human T cell differentiation and regulatory function in mucosal and lymphoid tissues. Nat Med (2016) 22(1):72–7. doi:10.1038/nm.4008
52. Connors TJ, Ravindranath TM, Bickham KL, Gordon CL, Zhang F, Levin B, et al. Airway CD8(+) T cells are associated with lung injury during infant viral respiratory tract infection. Am J Respir Cell Mol Biol (2016) 54(6):822–30. doi:10.1165/rcmb.2015-0297OC
53. Granot T, Senda T, Carpenter DJ, Matsuoka N, Weiner J, Gordon CL, et al. Dendritic cells display subset and tissue-specific maturation dynamics over human life. Immunity (2017) 46(3):504–15. doi:10.1016/j.immuni.2017.02.019
54. Grigg J, Riedler J, Robertson CF, Boyle W, Uren S. Alveolar macrophage immaturity in infants and young children. Eur Respir J (1999) 14(5):1198–205. doi:10.1183/09031936.99.14511989
55. Krishnamoorthy N, Khare A, Oriss TB, Raundhal M, Morse C, Yarlagadda M, et al. Early infection with respiratory syncytial virus impairs regulatory T cell function and increases susceptibility to allergic asthma. Nat Med (2012) 18(10):1525–30. doi:10.1038/nm.2896
56. Ruckwardt TJ, Malloy AMW, Gostick E, Price DA, Dash P, McClaren JL, et al. Neonatal CD8 T-cell hierarchy is distinct from adults and is influenced by intrinsic T cell properties in respiratory syncytial virus infected mice. PLoS Pathog (2011) 7(12):e1002377. doi:10.1371/journal.ppat.1002377
57. Gibbons D, Fleming P, Virasami A, Michel M-L, Sebire NJ, Costeloe K, et al. Interleukin-8 (CXCL8) production is a signatory T cell effector function of human newborn infants. Nat Med (2014) 20(10):1206–10. doi:10.1038/nm.3670
58. Zhivaki D, Lemoine S, Lim A, Morva A, Vidalain P-O, Schandene L, et al. Respiratory syncytial virus infects regulatory B cells in human neonates via chemokine receptor CX3CR1 and promotes lung disease severity. Immunity (2017) 46(2):301–14. doi:10.1016/j.immuni.2017.01.010
59. Qureshi MH, Garvy BA. Neonatal T cells in an adult lung environment are competent to resolve Pneumocystis carinii pneumonia. J Immunol (2001) 166(9):5704–11. doi:10.4049/jimmunol.166.9.5704
60. Garvy BA, Qureshi MH. Delayed inflammatory response to Pneumocystis carinii infection in neonatal mice is due to an inadequate lung environment. J Immunol (2000) 165(11):6480–6. doi:10.4049/jimmunol.165.11.6480
61. Roux X, Remot A, Petit-Camurdan A, Nahori M-A, Kiefer-Biasizzo H, Marchal G, et al. Neonatal lung immune responses show a shift of cytokines and transcription factors toward Th2 and a deficit in conventional and plasmacytoid dendritic cells. Eur J Immunol (2011) 41(10):2852–61. doi:10.1002/eji.201041224
62. Nelson DJ, Holt PG. Defective regional immunity in the respiratory tract of neonates is attributable to hyporesponsiveness of local dendritic cells to activation signals. J Immunol (1995) 155(7):3517–24.
63. Fach SJ, Brockmeier SL, Hobbs LA, Lehmkuhl HD, Sacco RE. Pulmonary dendritic cells isolated from neonatal and adult ovine lung tissue. Vet Immunol Immunopathol (2006) 112(3–4):171–82. doi:10.1016/j.vetimm.2006.02.012
64. Ruckwardt TJ, Malloy AMW, Morabito KM, Graham BS. Quantitative and qualitative deficits in neonatal lung-migratory dendritic cells impact the generation of the CD8+ T cell response. PLoS Pathog (2014) 10(2):e1003934. doi:10.1371/journal.ppat.1003934
65. Ruckwardt TJ, Morabito KM, Bar-Haim E, Nair D, Graham BS. Neonatal mice possess two phenotypically and functionally distinct lung-migratory CD103(+) dendritic cell populations following respiratory infection. Mucosal Immunol (2017). doi:10.1038/mi.2017.28
66. Malloy AMW, Ruckwardt TJ, Morabito KM, Lau-Kilby AW, Graham BS. Pulmonary dendritic cell subsets shape the respiratory syncytial virus-specific CD8+ T cell immunodominance hierarchy in neonates. J Immunol (2017) 198(1):394–403. doi:10.4049/jimmunol.1600486
67. Ruckwardt TJ, Bonaparte KL, Nason MC, Graham BS. Regulatory T cells promote early influx of CD8+ T cells in the lungs of respiratory syncytial virus-infected mice and diminish immunodominance disparities. J Virol (2009) 83(7):3019–28. doi:10.1128/JVI.00036-09
68. Herbst T, Sichelstiel A, Schär C, Yadava K, Bürki K, Cahenzli J, et al. Dysregulation of allergic airway inflammation in the absence of microbial colonization. Am J Respir Crit Care Med (2011) 184(2):198–205. doi:10.1164/rccm.201010-1574OC
69. Cormier SA, Shrestha B, Saravia J, Lee GI, Shen L, DeVincenzo JP, et al. Limited type I interferons and plasmacytoid dendritic cells during neonatal respiratory syncytial virus infection permit immunopathogenesis upon reinfection. J Virol (2014) 88(16):9350–60. doi:10.1128/JVI.00818-14
70. Guilliams M, Lambrecht BN, Hammad H. Division of labor between lung dendritic cells and macrophages in the defense against pulmonary infections. Mucosal Immunol (2013) 6(3):464–73. doi:10.1038/mi.2013.14
71. Bedoret D, Wallemacq H, Marichal T, Desmet C, Quesada Calvo F, Henry E, et al. Lung interstitial macrophages alter dendritic cell functions to prevent airway allergy in mice. J Clin Invest (2009) 119(12):3723–38. doi:10.1172/JCI39717
72. Sabatel C, Radermecker C, Fievez L, Paulissen G, Chakarov S, Fernandes C, et al. Exposure to bacterial CpG DNA protects from airway allergic inflammation by expanding regulatory lung interstitial macrophages. Immunity (2017) 46(3):457–73. doi:10.1016/j.immuni.2017.02.016
73. Alenghat E, Esterly JR. Alveolar macrophages in perinatal infants. Pediatrics (1984) 74(2):221–3.
74. Guilliams M, De Kleer I, Henri S, Post S, Vanhoutte L, De Prijck S, et al. Alveolar macrophages develop from fetal monocytes that differentiate into long-lived cells in the first week of life via GM-CSF. J Exp Med (2013) 210(10):1977–92. doi:10.1084/jem.20131199
75. Lee PT, Holt PG, McWilliam AS. Role of alveolar macrophages in innate immunity in neonates: evidence for selective lipopolysaccharide binding protein production by rat neonatal alveolar macrophages. Am J Respir Cell Mol Biol (2000) 23(5):652–61. doi:10.1165/ajrcmb.23.5.4016
76. Empey KM, Hollifield M, Garvy BA. Exogenous heat-killed Escherichia coli improves alveolar macrophage activity and reduces Pneumocystis carinii lung burden in infant mice. Infect Immun (2007) 75(7):3382–93. doi:10.1128/IAI.00174-07
77. Fach SJ, Olivier A, Gallup JM, Waters TE, Ackermann MR, Lehmkuhl HD, et al. Differential expression of cytokine transcripts in neonatal and adult ovine alveolar macrophages in response to respiratory syncytial virus or toll-like receptor ligation. Vet Immunol Immunopathol (2010) 136(1–2):55–64. doi:10.1016/j.vetimm.2010.02.008
78. Kurkjian C, Hollifield M, Lines JL, Rogosky A, Empey KM, Qureshi M, et al. Alveolar macrophages in neonatal mice are inherently unresponsive to Pneumocystis murina infection. Infect Immun (2012) 80(8):2835–46. doi:10.1128/IAI.05707-11
79. Ballinger MN, Peters-Golden M, Moore BB. Impaired neonatal macrophage phagocytosis is not explained by overproduction of prostaglandin E2. Respir Res (2011) 12:155. doi:10.1186/1465-9921-12-155
80. Kurland G, Cheung AT, Miller ME, Ayin SA, Cho MM, Ford EW. The ontogeny of pulmonary defenses: alveolar macrophage function in neonatal and juvenile rhesus monkeys. Pediatr Res (1988) 23(3):293–7. doi:10.1203/00006450-198803000-00013
81. Empey KM, Hollifield M, Schuer K, Gigliotti F, Garvy BA. Passive immunization of neonatal mice against Pneumocystis carinii f. sp. muris enhances control of infection without stimulating inflammation. Infect Immun (2004) 72(11):6211–20. doi:10.1128/IAI.72.11.6211-6220.2004
82. Empey KM, Orend JG, Peebles RS, Egaña L, Norris KA, Oury TD, et al. Stimulation of immature lung macrophages with intranasal interferon gamma in a novel neonatal mouse model of respiratory syncytial virus infection. PLoS One (2012) 7(7):e40499. doi:10.1371/journal.pone.0040499
83. Whitsett JA, Alenghat T. Respiratory epithelial cells orchestrate pulmonary innate immunity. Nat Immunol (2015) 16(1):27–35. doi:10.1038/ni.3045
84. Maniar-Hew K, Clay CC, Postlethwait EM, Evans MJ, Fontaine JH, Miller LA. Innate immune response to LPS in airway epithelium is dependent on chronological age and antecedent exposures. Am J Respir Cell Mol Biol (2013) 49(5):710–20. doi:10.1165/rcmb.2012-0321OC
85. Clay CC, Reader JR, Gerriets JE, Wang TT, Harrod KS, Miller LA. Enhanced viral replication and modulated innate immune responses in infant airway epithelium following H1N1 infection. J Virol (2014) 88(13):7412–25. doi:10.1128/JVI.00188-14
86. Hall CB, Kopelman AE, Douglas RG, Geiman JM, Meagher MP. Neonatal respiratory syncytial virus infection. N Engl J Med (1979) 300(8):393–6. doi:10.1056/NEJM197902223000803
87. Isaacs D. Production of interferon in respiratory syncytial virus bronchiolitis. Arch Dis Child (1989) 64(1):92–5. doi:10.1136/adc.64.1.92
88. Mejias A, Dimo B, Suarez NM, Garcia C, Suarez-Arrabal MC, Jartti T, et al. Whole blood gene expression profiles to assess pathogenesis and disease severity in infants with respiratory syncytial virus infection. PLoS Med (2013) 10(11):e1001549. doi:10.1371/journal.pmed.1001549
89. Villenave R, Thavagnanam S, Sarlang S, Parker J, Douglas I, Skibinski G, et al. In vitro modeling of respiratory syncytial virus infection of pediatric bronchial epithelium, the primary target of infection in vivo. Proc Natl Acad Sci U S A (2012) 109(13):5040–5. doi:10.1073/pnas.1110203109
90. Fonceca AM, Flanagan BF, Trinick R, Smyth RL, McNamara PS. Primary airway epithelial cultures from children are highly permissive to respiratory syncytial virus infection. Thorax (2012) 67(1):42–8. doi:10.1136/thoraxjnl-2011-200131
91. Villenave R, Shields MD, Power UF. Respiratory syncytial virus interaction with human airway epithelium. Trends Microbiol (2013) 21(5):238–44. doi:10.1016/j.tim.2013.02.004
92. Villenave R, Broadbent L, Douglas I, Lyons JD, Coyle PV, Teng MN, et al. Induction and antagonism of antiviral responses in respiratory syncytial virus-infected pediatric airway epithelium. J Virol (2015) 89(24):12309–18. doi:10.1128/JVI.02119-15
93. Okabayashi T, Kojima T, Masaki T, Yokota S-I, Imaizumi T, Tsutsumi H, et al. Type-III interferon, not type-I, is the predominant interferon induced by respiratory viruses in nasal epithelial cells. Virus Res (2011) 160(1–2):360–6. doi:10.1016/j.virusres.2011.07.011
94. McNamara PS, Flanagan BF, Hart CA, Smyth RL. Production of chemokines in the lungs of infants with severe respiratory syncytial virus bronchiolitis. J Infect Dis (2005) 191(8):1225–32. doi:10.1086/428855
95. McNamara PS, Fonceca AM, Howarth D, Correia JB, Slupsky JR, Trinick RE, et al. Respiratory syncytial virus infection of airway epithelial cells, in vivo and in vitro, supports pulmonary antibody responses by inducing expression of the B cell differentiation factor BAFF. Thorax (2013) 68(1):76–81. doi:10.1136/thoraxjnl-2012-202288
96. Saravia J, You D, Shrestha B, Jaligama S, Siefker D, Lee GI, et al. Respiratory syncytial virus disease is mediated by age-variable IL-33. PLoS Pathog (2015) 11(10):e1005217. doi:10.1371/journal.ppat.1005217
97. Hasegawa K, Mansbach JM, Ajami NJ, Petrosino JF, Freishtat RJ, Teach SJ, et al. Serum cathelicidin, nasopharyngeal microbiota, and disease severity among infants hospitalized with bronchiolitis. J Allergy Clin Immunol (2017) 139(4):1383.e–6.e. doi:10.1016/j.jaci.2016.09.037
98. Starner TD, Agerberth B, Gudmundsson GH, McCray PB. Expression and activity of beta-defensins and LL-37 in the developing human lung. J Immunol (2005) 174(3):1608–15. doi:10.4049/jimmunol.174.3.1608
99. Schaller-Bals S, Schulze A, Bals R. Increased levels of antimicrobial peptides in tracheal aspirates of newborn infants during infection. Am J Respir Crit Care Med (2002) 165(7):992–5. doi:10.1164/ajrccm.165.7.200110-020
100. LeVine AM, Gwozdz J, Stark J, Bruno M, Whitsett J, Korfhagen T. Surfactant protein-A enhances respiratory syncytial virus clearance in vivo. J Clin Invest (1999) 103(7):1015–21. doi:10.1172/JCI5849
101. Derscheid RJ, Ackermann MR. The innate immune system of the perinatal lung and responses to respiratory syncytial virus infection. Vet Pathol (2013) 50(5):827–41. doi:10.1177/0300985813480216
102. Battersby AJ, Khara J, Wright VJ, Levy O, Kampmann B. Antimicrobial proteins and peptides in early life: ontogeny and translational opportunities. Front Immunol (2016) 7:309. doi:10.3389/fimmu.2016.00309
103. Mansbach JM, Piedra PA, Stevenson MD, Sullivan AF, Forgey TF, Clark S, et al. Prospective multicenter study of children with bronchiolitis requiring mechanical ventilation. Pediatrics (2012) 130(3):e492–500. doi:10.1542/peds.2012-0444
104. Mansbach JM, Piedra PA, Borregaard N, Martineau AR, Neuman MI, Espinola JA, et al. Serum cathelicidin level is associated with viral etiology and severity of bronchiolitis. J Allergy Clin Immunol (2012) 130(4):1007.e–8.e. doi:10.1016/j.jaci.2012.07.044
105. Currie SM, Gwyer Findlay E, McFarlane AJ, Fitch PM, Böttcher B, Colegrave N, et al. Cathelicidins have direct antiviral activity against respiratory syncytial virus in vitro and protective function in vivo in mice and humans. J Immunol (2016) 196(6):2699–710. doi:10.4049/jimmunol.1502478
106. Currie SM, Findlay EG, McHugh BJ, Mackellar A, Man T, Macmillan D, et al. The human cathelicidin LL-37 has antiviral activity against respiratory syncytial virus. PLoS One (2013) 8(8):e73659. doi:10.1371/journal.pone.0073659
107. Harcourt JL, McDonald M, Svoboda P, Pohl J, Tatti K, Haynes LM. Human cathelicidin, LL-37, inhibits respiratory syncytial virus infection in polarized airway epithelial cells. BMC Res Notes (2016) 9(1):11. doi:10.1186/s13104-015-1836-y
108. Huang H, Saravia J, You D, Shaw AJ, Cormier SA. Impaired gamma delta T cell-derived IL-17A and inflammasome activation during early respiratory syncytial virus infection in infants. Immunol Cell Biol (2015) 93(2):126–35. doi:10.1038/icb.2014.79
109. Castanhinha S, Sherburn R, Walker S, Gupta A, Bossley CJ, Buckley J, et al. Pediatric severe asthma with fungal sensitization is mediated by steroid-resistant IL-33. J Allergy Clin Immunol (2015) 136(2):312.e–22.e. doi:10.1016/j.jaci.2015.01.016
110. Olszak T, An D, Zeissig S, Vera MP, Richter J, Franke A, et al. Microbial exposure during early life has persistent effects on natural killer T cell function. Science (2012) 336(6080):489–93. doi:10.1126/science.1219328
111. Gray J, Oehrle K, Worthen G, Alenghat T, Whitsett J, Deshmukh H. Intestinal commensal bacteria mediate lung mucosal immunity and promote resistance of newborn mice to infection. Sci Transl Med (2017) 9(376):eaaf9412. doi:10.1126/scitranslmed.aaf9412
112. Harju K, Glumoff V, Hallman M. Ontogeny of Toll-like receptors Tlr2 and Tlr4 in mice. Pediatr Res (2001) 49(1):81–3. doi:10.1203/00006450-200101000-00018
113. Harju K, Ojaniemi M, Rounioja S, Glumoff V, Paananen R, Vuolteenaho R, et al. Expression of toll-like receptor 4 and endotoxin responsiveness in mice during perinatal period. Pediatr Res (2005) 57(5 Pt 1):644–8. doi:10.1203/01.PDR.0000156212.03459.A9
114. Petrikin JE, Gaedigk R, Leeder JS, Truog WE. Selective Toll-like receptor expression in human fetal lung. Pediatr Res (2010) 68(4):335–8. doi:10.1203/PDR.0b013e3181ed1134
115. Bhattacharya S, Beal BT, Janowski AM, Shornick LP. Reduced inflammation and altered innate response in neonates during paramyxoviral infection. Virol J (2011) 8:549. doi:10.1186/1743-422X-8-549
116. Gern JE, Martin MS, Anklam KA, Shen K, Roberg KA, Carlson-Dakes KT, et al. Relationships among specific viral pathogens, virus-induced interleukin-8, and respiratory symptoms in infancy. Pediatr Allergy Immunol (2002) 13(6):386–93. doi:10.1034/j.1399-3038.2002.01093.x
117. Martin TR, Ruzinski JT, Wilson CB, Skerrett SJ. Effects of endotoxin in the lungs of neonatal rats: age-dependent impairment of the inflammatory response. J Infect Dis (1995) 171(1):134–44. doi:10.1093/infdis/171.1.134
118. Martin TR, Rubens CE, Wilson CB. Lung antibacterial defense mechanisms in infant and adult rats: implications for the pathogenesis of group B streptococcal infections in the neonatal lung. J Infect Dis (1988) 157(1):91–100. doi:10.1093/infdis/157.1.91
119. McGrath-Morrow SA, Lee S, Gibbs K, Lopez A, Collaco JM, Neptune E, et al. Immune response to intrapharyngeal LPS in neonatal and juvenile mice. Am J Respir Cell Mol Biol (2015) 52(3):323–31. doi:10.1165/rcmb.2014-0100OC
120. Anderson DC, Rothlein R, Marlin SD, Krater SS, Smith CW. Impaired transendothelial migration by neonatal neutrophils: abnormalities of Mac-1 (CD11b/CD18)-dependent adherence reactions. Blood (1990) 76(12):2613–21.
121. Harris MC, Shalit M, Southwick FS. Diminished actin polymerization by neutrophils from newborn infants. Pediatr Res (1993) 33(1):27–31. doi:10.1203/00006450-199301000-00006
122. Smith PK, Wang SZ, Dowling KD, Forsyth KD. Leucocyte populations in respiratory syncytial virus-induced bronchiolitis. J Paediatr Child Health (2001) 37(2):146–51. doi:10.1046/j.1440-1754.2001.00618.x
123. McNamara PS, Ritson P, Selby A, Hart CA, Smyth RL. Bronchoalveolar lavage cellularity in infants with severe respiratory syncytial virus bronchiolitis. Arch Dis Child (2003) 88(10):922–6. doi:10.1136/adc.88.10.922
124. Abu-Harb M, Bell F, Finn A, Rao WH, Nixon L, Shale D, et al. IL-8 and neutrophil elastase levels in the respiratory tract of infants with RSV bronchiolitis. Eur Respir J (1999) 14(1):139–43. doi:10.1034/j.1399-3003.1999.14a23.x
125. Everard ML, Swarbrick A, Wrightham M, McIntyre J, Dunkley C, James PD, et al. Analysis of cells obtained by bronchial lavage of infants with respiratory syncytial virus infection. Arch Dis Child (1994) 71(5):428–32. doi:10.1136/adc.71.5.428
126. Noah TL, Ivins SS, Murphy P, Kazachkova I, Moats-Staats B, Henderson FW. Chemokines and inflammation in the nasal passages of infants with respiratory syncytial virus bronchiolitis. Clin Immunol (2002) 104(1):86–95. doi:10.1006/clim.2002.5248
127. Nicholson EG, Schlegel C, Garofalo RP, Mehta R, Scheffler M, Mei M, et al. Robust cytokine and chemokine response in nasopharyngeal secretions: association with decreased severity in children with physician diagnosed bronchiolitis. J Infect Dis (2016) 214(4):649–55. doi:10.1093/infdis/jiw191
128. Garvy BA, Harmsen AG. Susceptibility to Pneumocystis carinii infection: host responses of neonatal mice from immune or naive mothers and of immune or naive adults. Infect Immun (1996) 64(10):3987–92.
129. Yamaguchi Y, Harker JA, Wang B, Openshaw PJ, Tregoning JS, Culley FJ. Preexposure to CpG protects against the delayed effects of neonatal respiratory syncytial virus infection. J Virol (2012) 86(19):10456–61. doi:10.1128/JVI.01082-12
130. Yatsunenko T, Rey FE, Manary MJ, Trehan I, Dominguez-Bello MG, Contreras M, et al. Human gut microbiome viewed across age and geography. Nature (2012) 486(7402):222–7. doi:10.1038/nature11053
131. Ege MJ, Bieli C, Frei R, van Strien RT, Riedler J, Ublagger E, et al. Prenatal farm exposure is related to the expression of receptors of the innate immunity and to atopic sensitization in school-age children. J Allergy Clin Immunol (2006) 117(4):817–23. doi:10.1016/j.jaci.2005.12.1307
132. Braun-Fahrländer C, Riedler J, Herz U, Eder W, Waser M, Grize L, et al. Environmental exposure to endotoxin and its relation to asthma in school-age children. N Engl J Med (2002) 347(12):869–77. doi:10.1056/NEJMoa020057
133. Stein MM, Hrusch CL, Gozdz J, Igartua C, Pivniouk V, Murray SE, et al. Innate immunity and asthma risk in amish and hutterite farm children. N Engl J Med (2016) 375(5):411–21. doi:10.1056/NEJMoa1508749
134. Schuijs MJ, Willart MA, Vergote K, Gras D, Deswarte K, Ege MJ, et al. Farm dust and endotoxin protect against allergy through A20 induction in lung epithelial cells. Science (2015) 349(6252):1106–10. doi:10.1126/science.aac6623
135. Schulfer A, Blaser MJ. Risks of antibiotic exposures early in life on the developing microbiome. PLoS Pathog (2015) 11(7):e1004903. doi:10.1371/journal.ppat.1004903
136. Kramer BW, Kallapur S, Newnham J, Jobe AH. Prenatal inflammation and lung development. Semin Fetal Neonatal Med (2009) 14(1):2–7. doi:10.1016/j.siny.2008.08.011
137. Warburton D, El-Hashash A, Carraro G, Tiozzo C, Sala F, Rogers O, et al. Lung organogenesis. Curr Top Dev Biol (2010) 90:73–158. doi:10.1016/S0070-2153(10)90003-3
138. Blackwell TS, Hipps AN, Yamamoto Y, Han W, Barham WJ, Ostrowski MC, et al. NF-κB signaling in fetal lung macrophages disrupts airway morphogenesis. J Immunol (2011) 187(5):2740–7. doi:10.4049/jimmunol.1101495
139. Prince LS, Dieperink HI, Okoh VO, Fierro-Perez GA, Lallone RL. Toll-like receptor signaling inhibits structural development of the distal fetal mouse lung. Dev Dyn (2005) 233(2):553–61. doi:10.1002/dvdy.20362
140. Bry K, Whitsett JA, Lappalainen U. IL-1beta disrupts postnatal lung morphogenesis in the mouse. Am J Respir Cell Mol Biol (2007) 36(1):32–42. doi:10.1165/rcmb.2006-0116OC
141. Whitsett JA, Haitchi HM, Maeda Y. Intersections between pulmonary development and disease. Am J Respir Crit Care Med (2011) 184(4):401–6. doi:10.1164/rccm.201103-0495PP
142. Wan H, Kaestner KH, Ang S-L, Ikegami M, Finkelman FD, Stahlman MT, et al. Foxa2 regulates alveolarization and goblet cell hyperplasia. Development (2004) 131(4):953–64. doi:10.1242/dev.00966
143. Jones CV, Williams TM, Walker KA, Dickinson H, Sakkal S, Rumballe BA, et al. M2 macrophage polarisation is associated with alveolar formation during postnatal lung development. Respir Res (2013) 14:41. doi:10.1186/1465-9921-14-41
144. Tang X, Liu XJ, Tian C, Su Q, Lei Y, Wu Q, et al. Foxa2 regulates leukotrienes to inhibit Th2-mediated pulmonary inflammation. Am J Respir Cell Mol Biol (2013) 49(6):960–70. doi:10.1165/rcmb.2013-0122OC
Keywords: respiratory, neonatal, infection, respiratory syncytial virus, innate immunity
Citation: Lambert L and Culley FJ (2017) Innate Immunity to Respiratory Infection in Early Life. Front. Immunol. 8:1570. doi: 10.3389/fimmu.2017.01570
Received: 06 June 2017; Accepted: 01 November 2017;
Published: 14 November 2017
Edited by:
Arnaud Marchant, Free University of Brussels, BelgiumReviewed by:
Camille Locht, INSERM, FranceGiuseppe Lofano, Ragon Institute of MGH, MIT and Harvard, United States
Copyright: © 2017 Lambert and Culley. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fiona J. Culley, Zi5jdWxsZXlAaW1wZXJpYWwuYWMudWs=